Embed Size (px)
Citation preview
Interesting Spine CasesInteresting Spine Cases
M. Castillo, MD, FACR
University of North Carolina
Chapel Hill
Case # 1
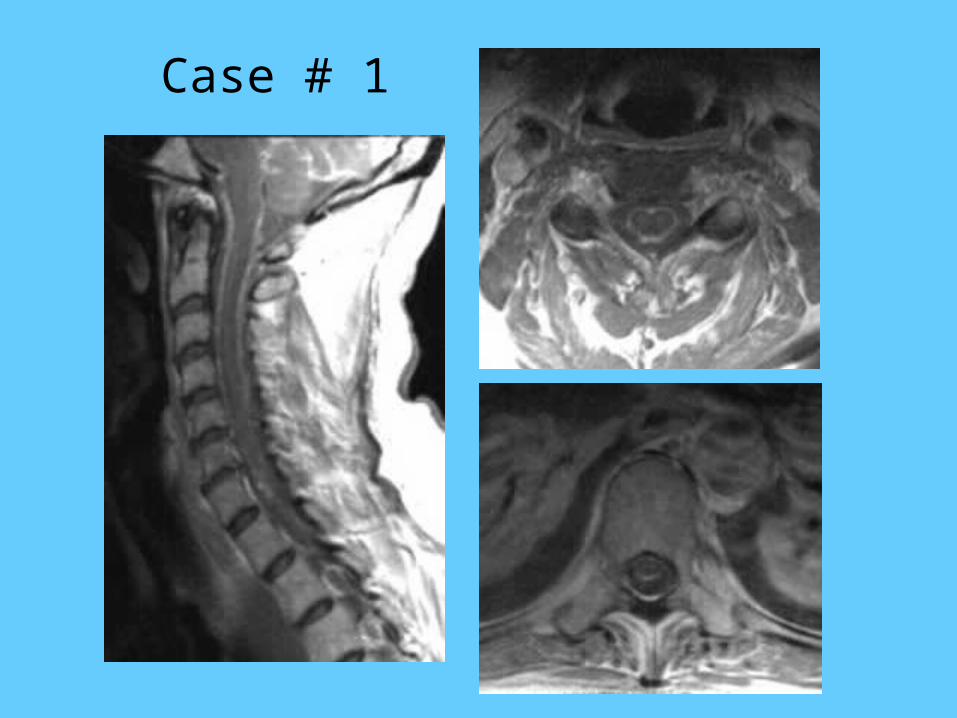
• 43-year-old male with a chronic history of dysesthesias and hypesthesias in all extremities. He has a chronic disease of which the most important findings are liver failure and decreased vision. Several members of his family had a similar history.
Case # 1
Case # 1
Case # 1. Which of the following is/are cause(s) of pial enhancement?
• 1. Metastases
• 2. Sarcoidosis
• 3. Amyloidosis
• 4. Lymphoma
• 5. All of the above

Case # 1. Regarding amyloidosis involving the spinal cord, which is true:
1. It predominantly involves the intrame-
dullary veins
2. It predominantly involves the arteries in
the subarachnoid space
3. It never results in cord contrast enhance-
ment
4. It affects heavy myelinated fibers
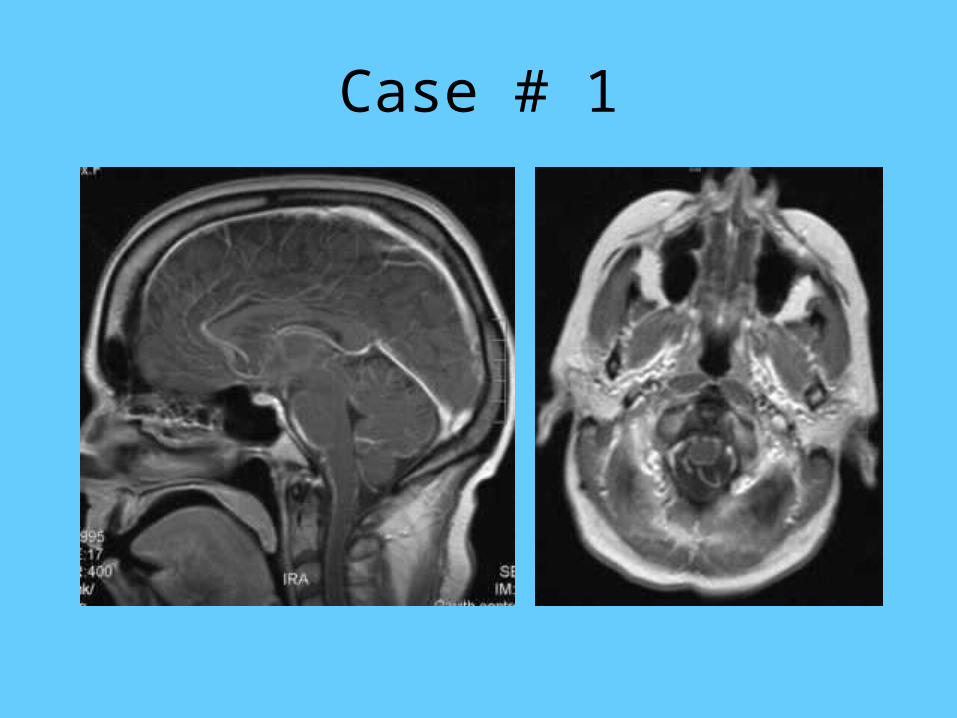
Case # 1. Dx: Amyloidosis involving Amyloidosis involving the piathe pia.
Familial amyloid polyneuropathy:– Deposition of amyloid in pial/subarachnoid
arteries & arterioles• Results in destruction of the blood-cord-barrier
– Sensory nerves & unmyelinated fibers most affected
– Precursors of FAP are metabolized by liver, thus liver transplantation is useful
» AJNR 2004; 25: 1599
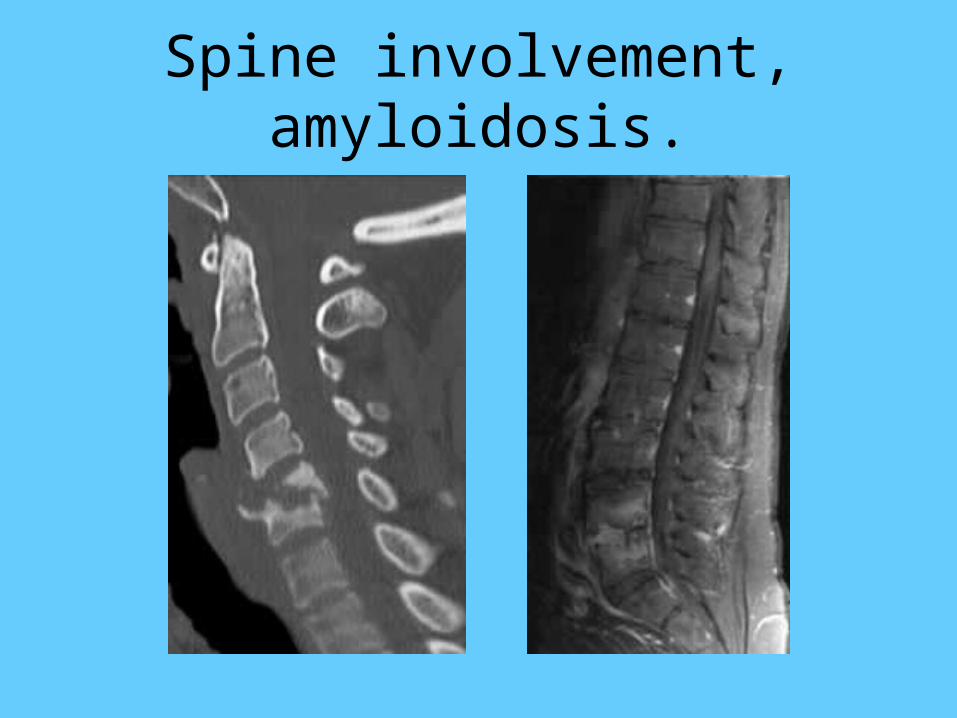
Spine involvement, amyloidosis.
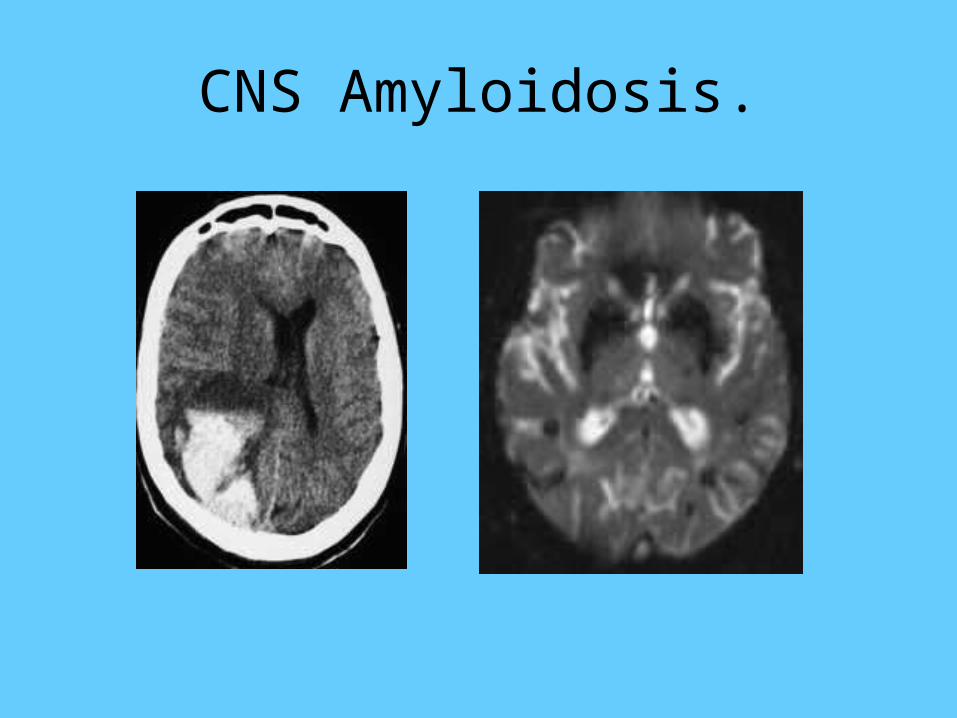
CNS Amyloidosis.
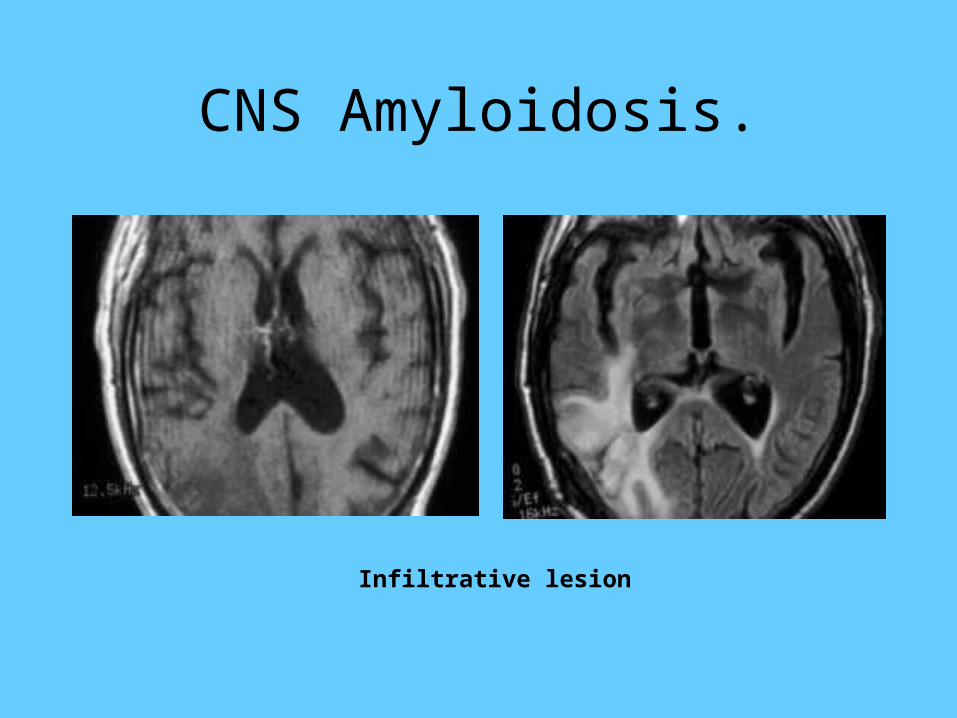
CNS Amyloidosis.
Infiltrative lesion

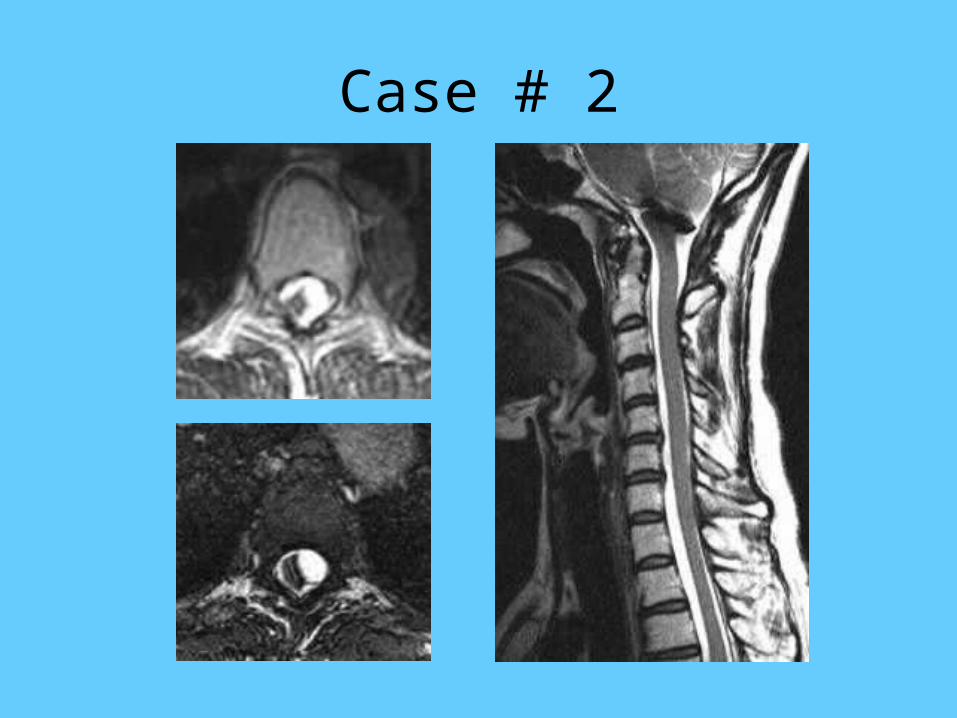
Case # 2
Young patient presenting with a myelopathy 2 years after a ‘stroke’.
Case # 2

Case # 2. The following may result in spinal ‘cysts’:
• A. Cysticercosis
• B. Exophytic syrinxes
• C. Post trauma arachnoid tears
• D. Post SAH arachnoid cysts
• E. All of the above
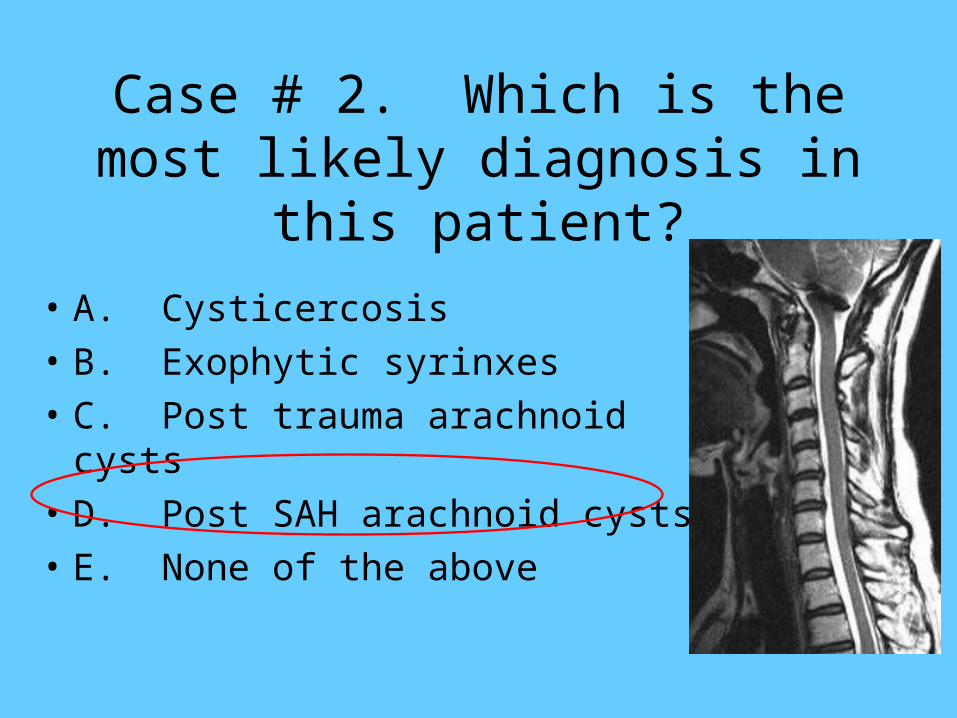
Case # 2. Which is the most likely diagnosis in this patient?
• A. Cysticercosis
• B. Exophytic syrinxes
• C. Post trauma arachnoid cysts
• D. Post SAH arachnoid cysts
• E. None of the above
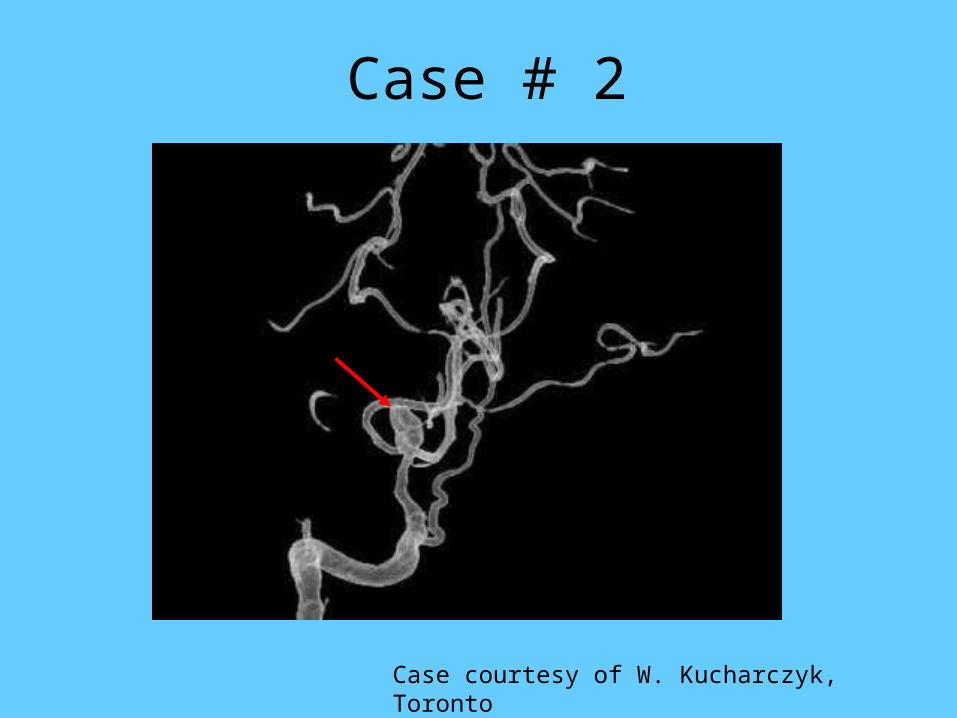
Case # 2
Case courtesy of W. Kucharczyk, Toronto
Case # 2. Dx: Multiple spinal Multiple spinal ‘arachnoid’ cysts following aneurysmal ‘arachnoid’ cysts following aneurysmal
SAH.SAH.• Cysts may develop after hemorrhage, trauma
& inflammation
• Pre-existing or de novo? may have hemosiderin
• Composed of single layer of meningothelial cells
• May produce back pain/myelopathy that may be intermittent (syrinx)
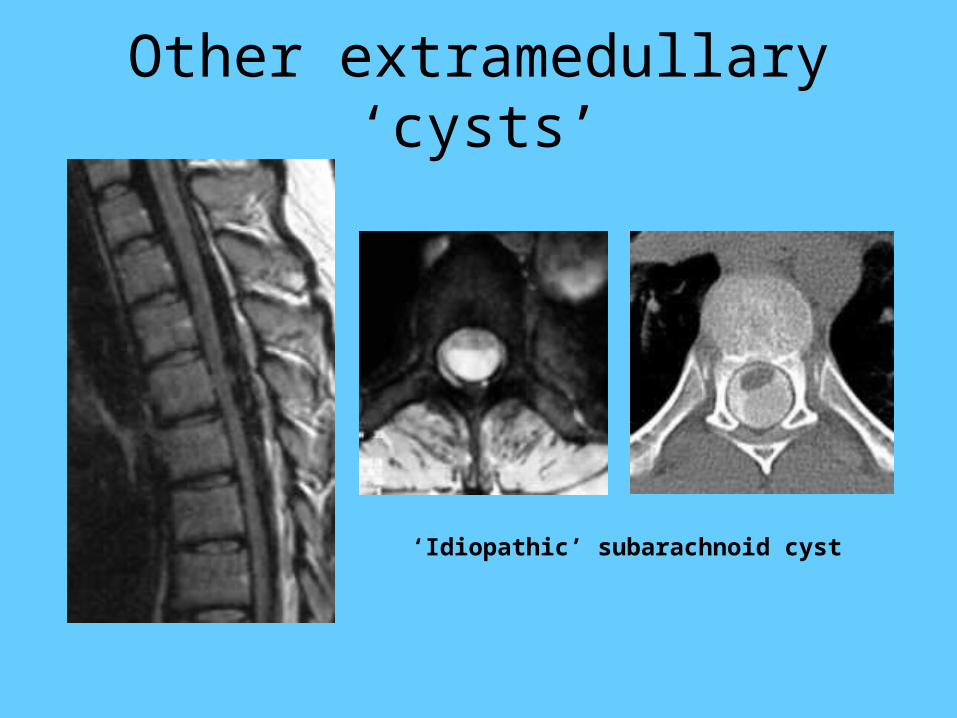
Other extramedullary ‘cysts’
‘Idiopathic’ subarachnoid cyst
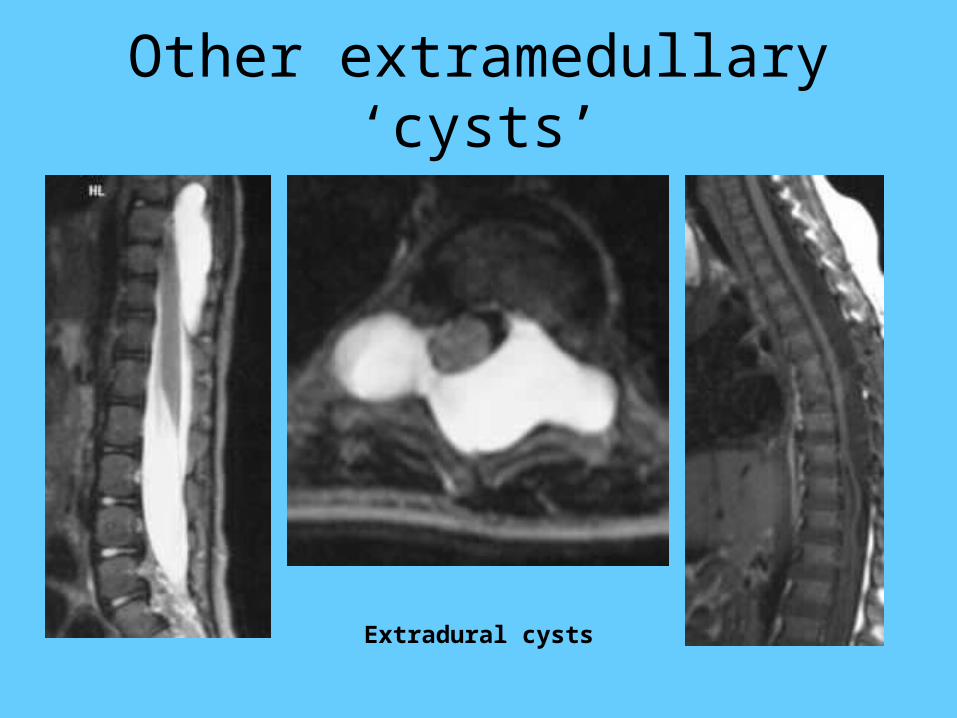
Other extramedullary ‘cysts’
Extradural cysts
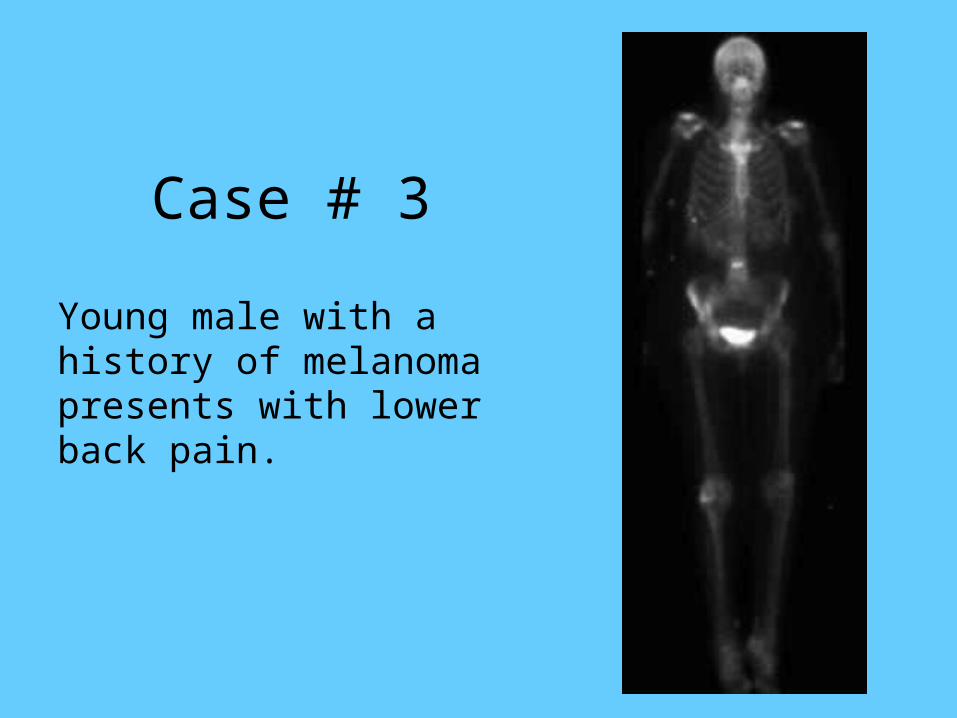
Case # 3
Young male with a history of melanoma presents with lower back pain.
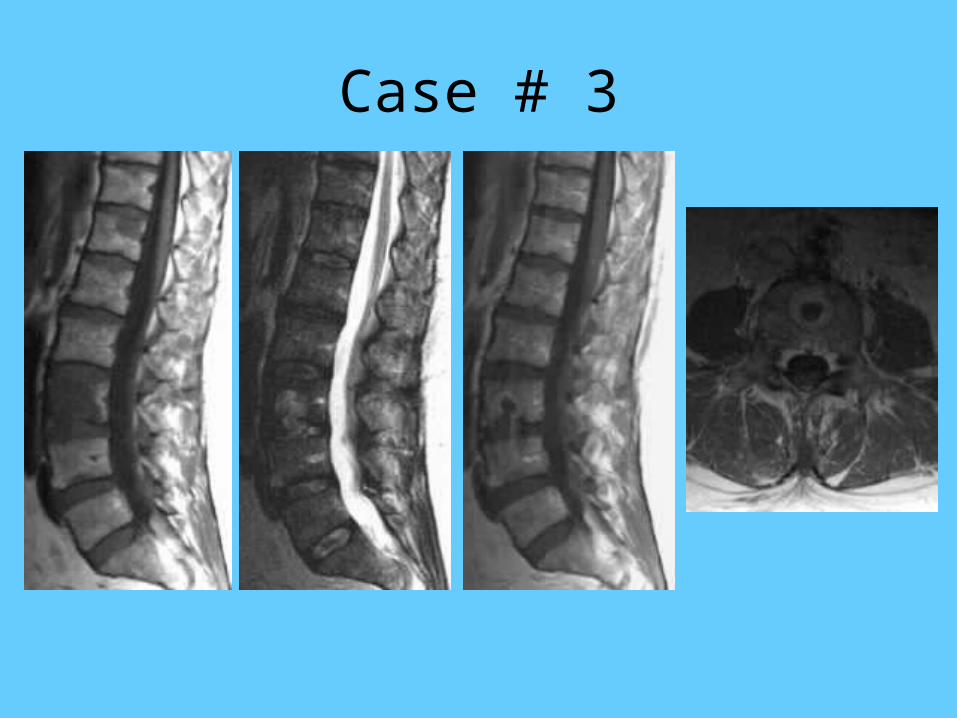
Case # 3

Case # 3. The most likely diagnosis is related to which
category of disease:
• A. Metastasis
• B. Infection
• C. Degenerative disease
• D. Congenital
• E. None of the above
Case # 3. Which is false regarding the abnormality shown here:
• A. Trauma is a predisposing factor
• B. Disc herniation is a part of it
• C. Weakening of the end-plate may be a secondary factor
• D. Contrast enhancement may occur
• E. Infection plays a role
Case # 3. Dx: Acute enhancing Acute enhancing Schmorl node.Schmorl node.
• Pre-requisites: soft end-plate/bone trabeculae– Congenital: nutrient blood vessels– Metabolic diseases, tumors– Scheuermann disease
• May appear ‘cystic’ due to:– Intra-nodal hemorrhage, mucous degeneration
• Contrast enhancement: granulation tissues• Cause pain before MRI findings, pain
disappears by 3 years & node ‘stabilizes”
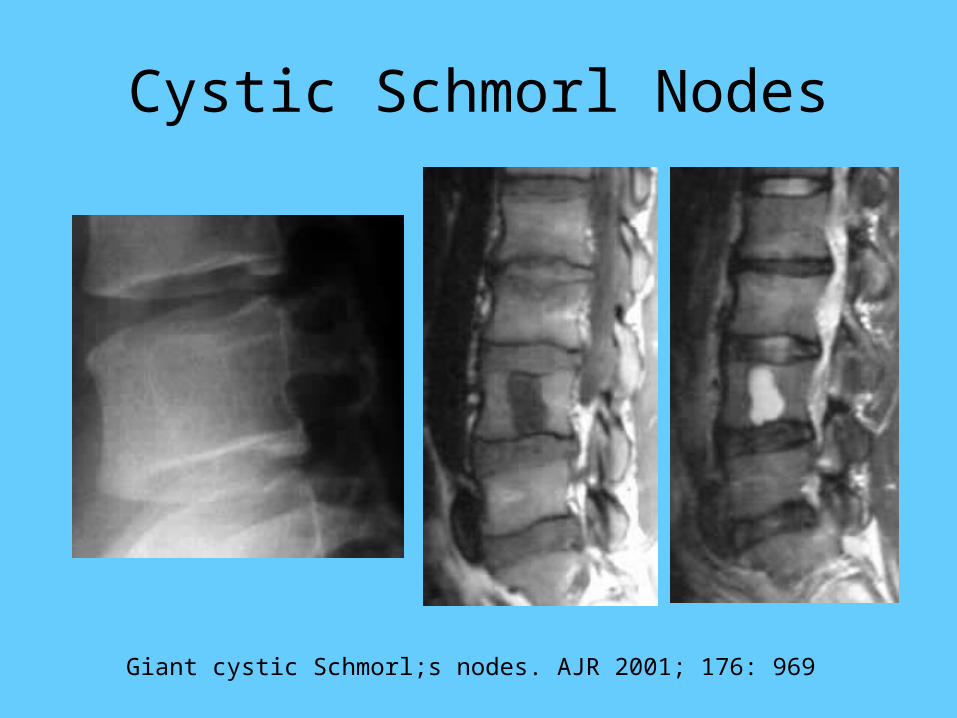
Cystic Schmorl Nodes
Giant cystic Schmorl;s nodes. AJR 2001; 176: 969

11-year-old boy with back pain of 2-months duration.
CASE # 4
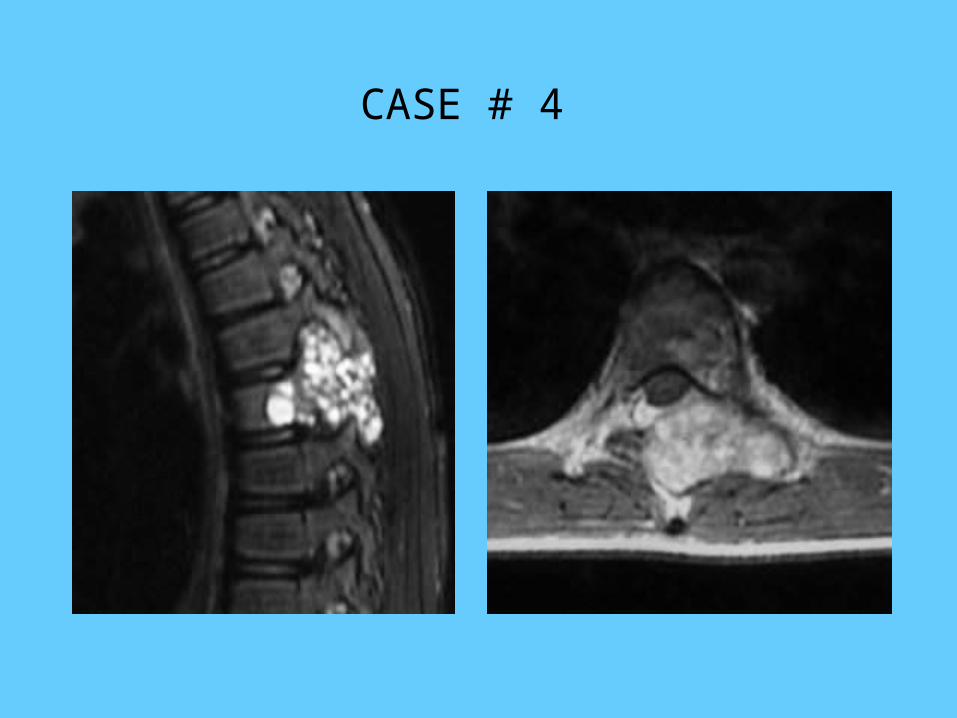
CASE # 4
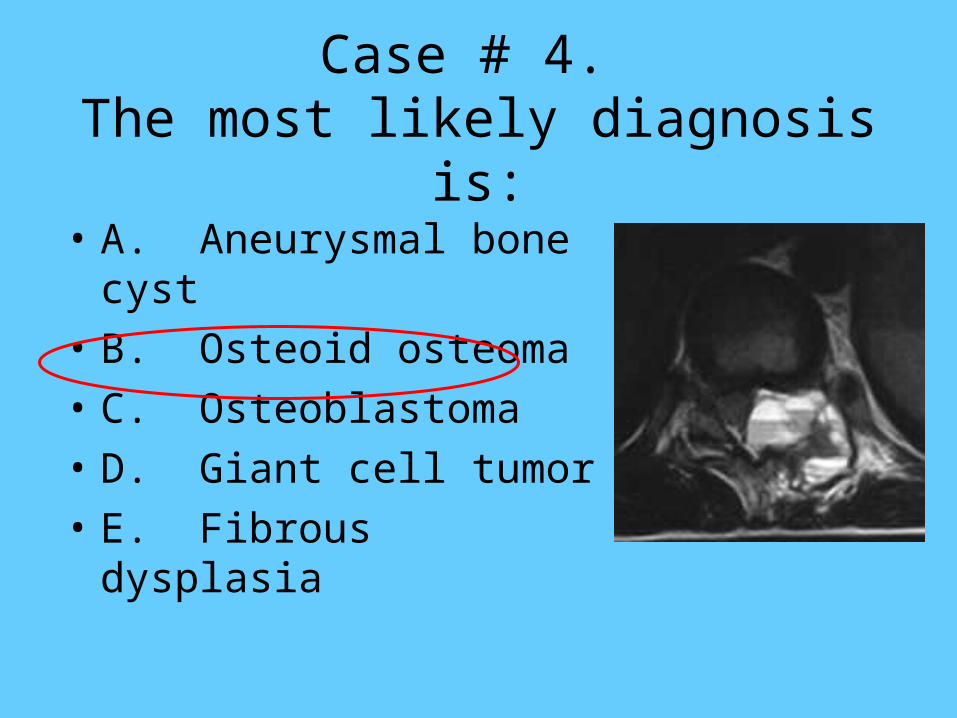
Case # 4. The most likely diagnosis is:
• A. Aneurysmal bone cyst
• B. Osteoid osteoma
• C. Osteoblastoma
• D. Giant cell tumor
• E. Fibrous dysplasia
Case # 5. Which is false regarding spinal osteoblastoma:
• A. If predominantly affects the posterior elements
• B. It may occasionally cross intervertebral space
• C. It is a benign process
• D. It is a lesion found in middle age and older individuals
Case # 4. Dx: Osteoblastoma.Osteoblastoma.
• Rare tumor (0.5-2%) comprised of osteoid, primitive woven bone amidst fibrovascular connective tissues
• Chronic pain, salicylates not helpful
• Sclerotic or lucent lesion, 25% have aggressive features
• Choice of Tx: en bloc resection, curettage with bone packing, XRT for malignant ones
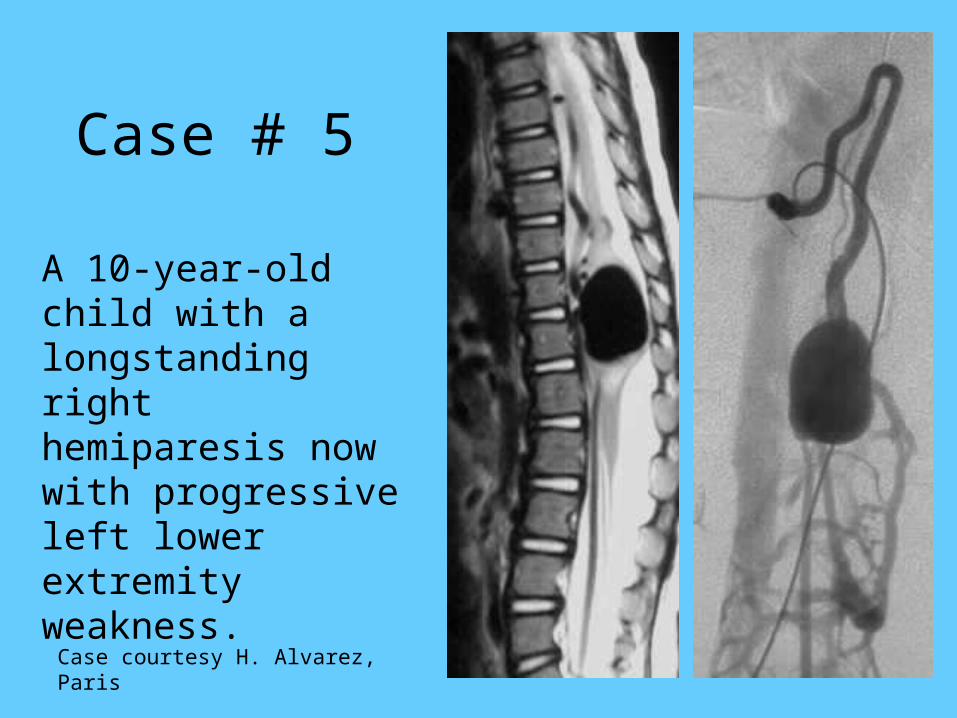
Case # 5
A 10-year-old child with a longstanding right hemiparesis now with progressive left lower extremity weakness.
Case courtesy H. Alvarez, Paris
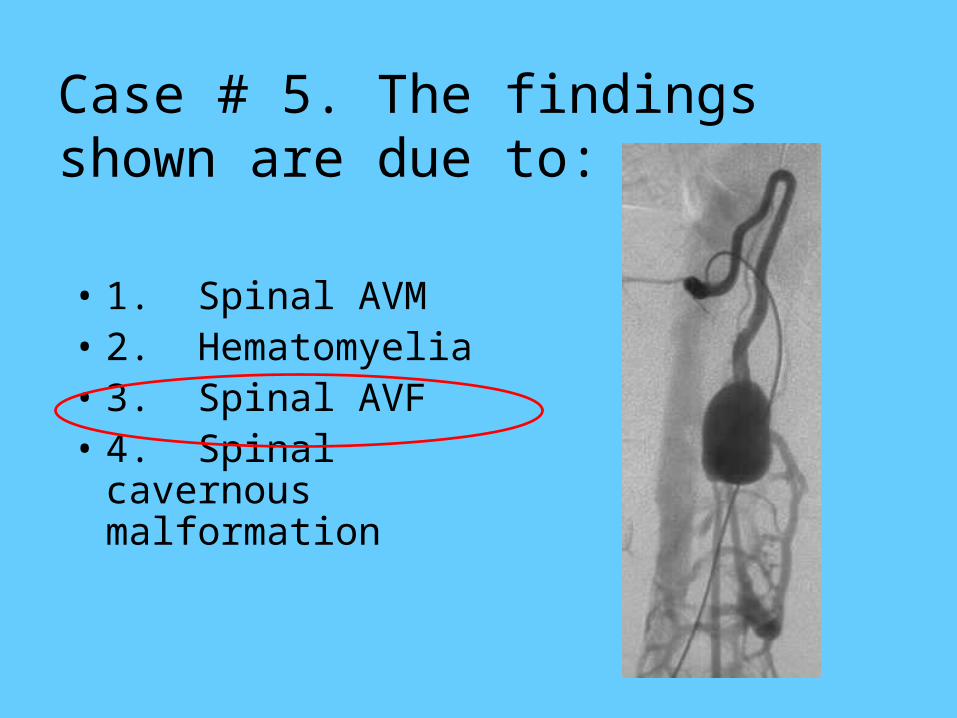
Case # 5. The findings shown are due to:
• 1. Spinal AVM• 2. Hematomyelia• 3. Spinal AVF• 4. Spinal cavernous
malformation
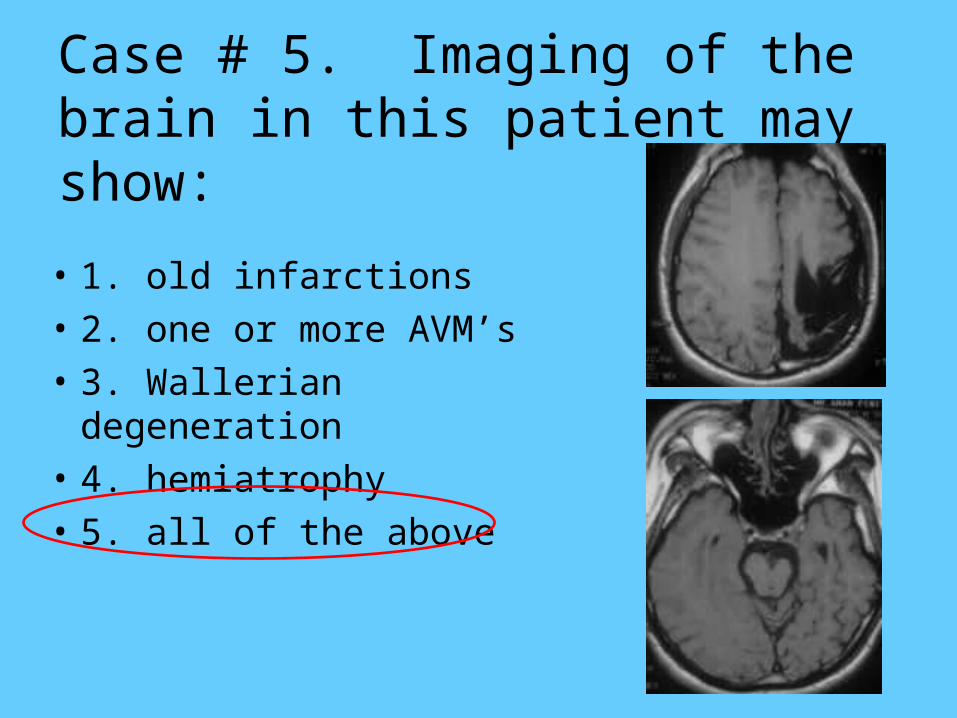
Case # 5. Imaging of the brain in this patient may show:
• 1. old infarctions
• 2. one or more AVM’s
• 3. Wallerian degeneration
• 4. hemiatrophy
• 5. all of the above
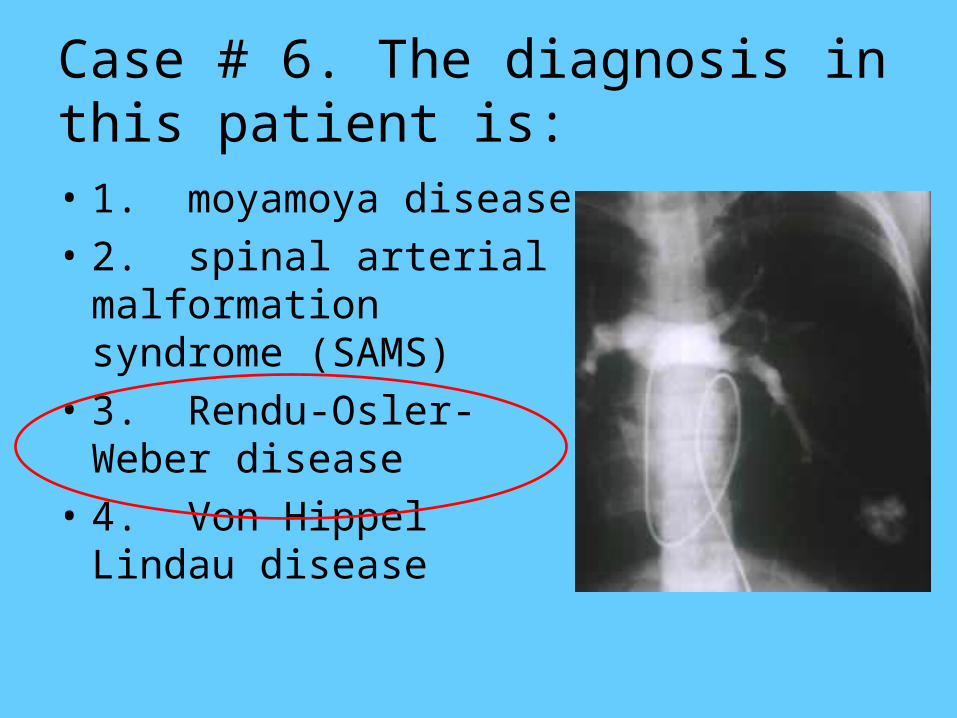
Case # 6. The diagnosis in this patient is:• 1. moyamoya disease
• 2. spinal arterial malformation syndrome (SAMS)
• 3. Rendu-Osler-Weber disease
• 4. Von Hippel Lindau disease
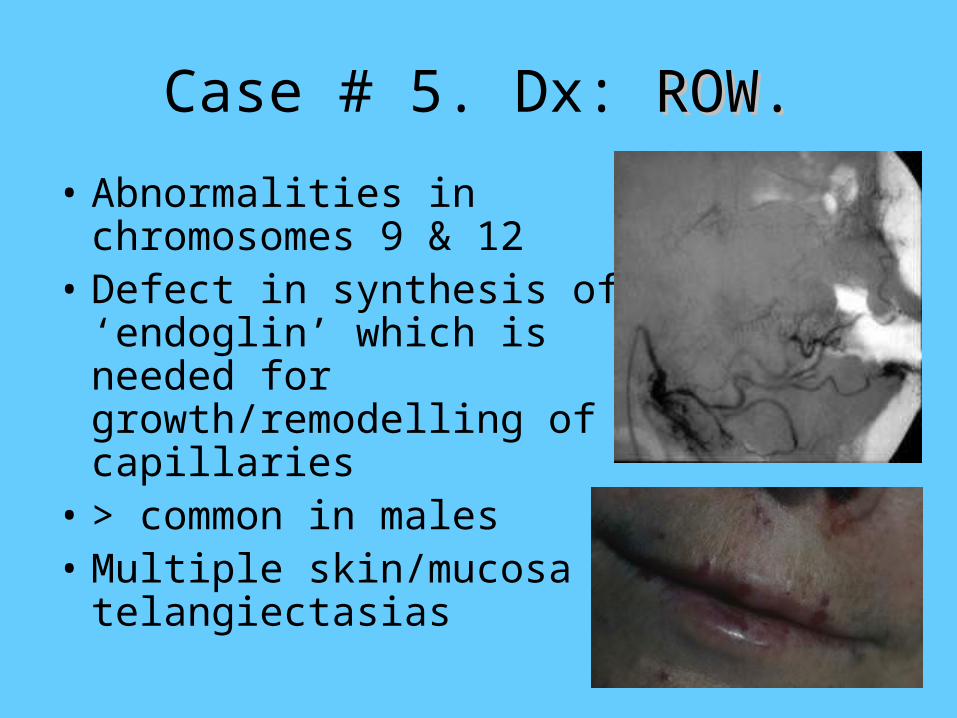
Case # 5. Dx: ROW.ROW.
• Abnormalities in chromosomes 9 & 12
• Defect in synthesis of ‘endoglin’ which is needed for growth/remodelling of capillaries
• > common in males• Multiple skin/mucosa
telangiectasias
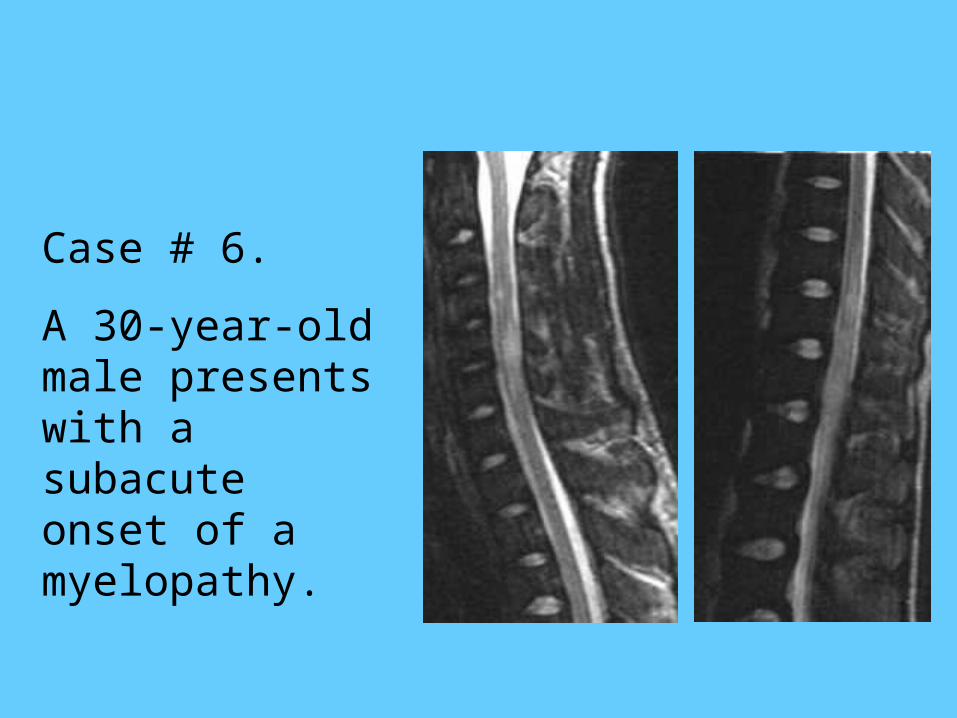
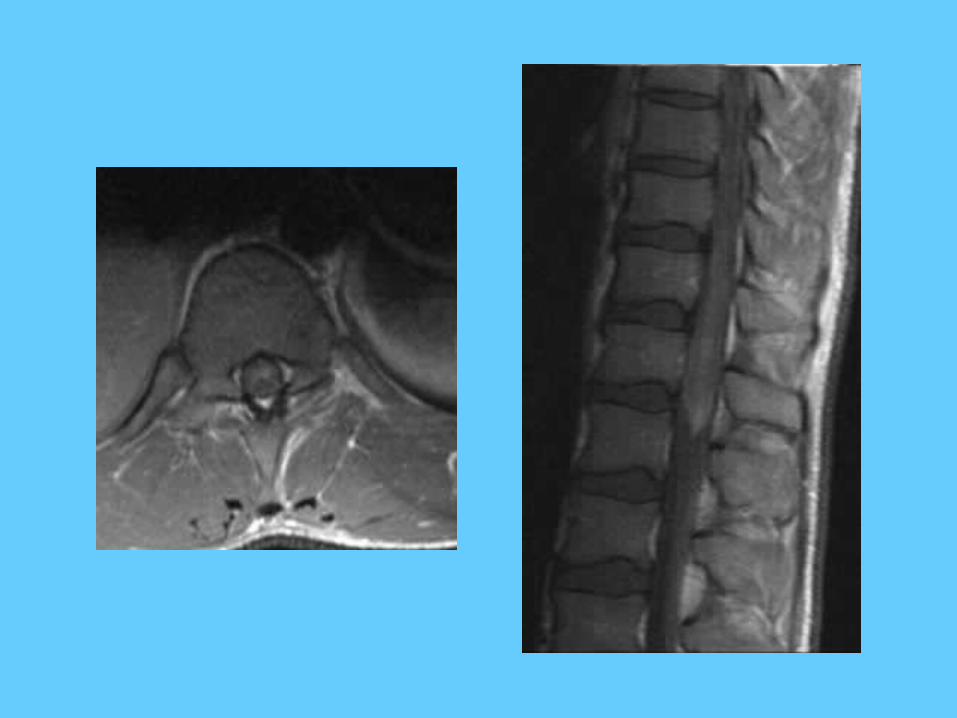
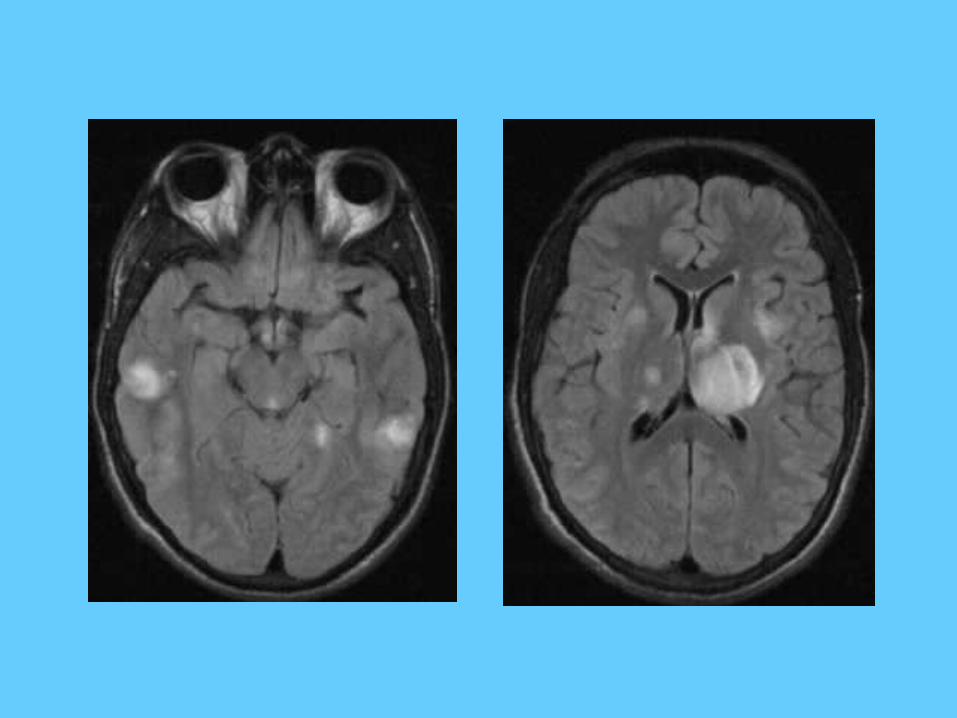
Case # 6.
A 30-year-old male presents with a subacute onset of a myelopathy.
Case # 6. The differential diagnosis in this case includes:
• 1. Multiple sclerosis
• 2. Acute disseminated encephalomyelitis
• 3. Vasculitis
• 4. Sarcoidosis
• 5. All of the above
Case # 6. Primary Angiitis of the Primary Angiitis of the CNS.CNS.
• Spinal cord vasculitis: idiopathic, associated with Hodgkin, thyroiditis, drug allergy, Sjogren, viral-induced, hepatitis
• Perivascular (artery & vein) infiltration by lymphocytes, cavitation, pial inflammation
• Prognosis is very poor, some temporary symptom relief with steroids, necrosis of spinal cord

45-year-old man with a chronic disorder now with a cauda equina syndrome.
CASE # 7
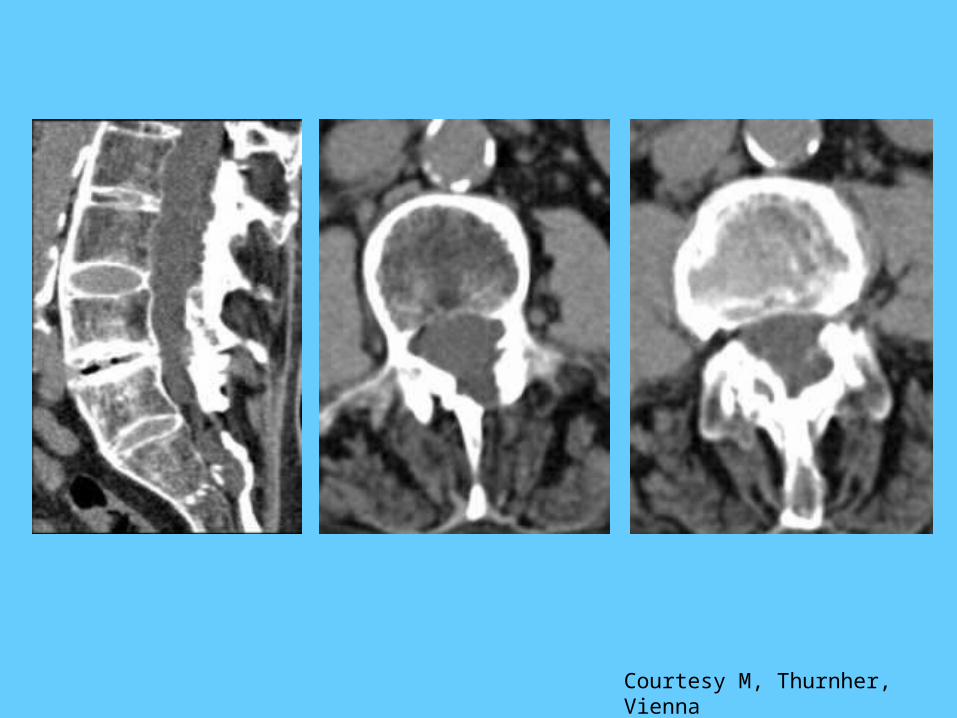
Courtesy M, Thurnher, Vienna
Case # 7. The most likely diagnosis is:
• A. Neurofibromatosis I with dural ectasia
• B. Marfan syndrome with dural ectasia
• C. Ankylosing spondylitis with erosive dural ectasia
• D. Epidermoid with bone scalloping
Case # 7.All but one of the following are complications of ankylosing
spondylitis:
• A. “Banana” type fractures
• B. Erosive dural ectasia w/cauda equina syndrome
• C. Epidural hematomas
• D. Infectious diskitis/osteomyelitis
• E. Non-infectious diskitis/osteomyelitis (amyloidosis?)
Case # 7.Ankylosing Spondylitis, Newer Concepts
• B27 gene:– 95% of Europeans, only 25% in Middle East– Antiviral properties high in American Indians
who survived European viruses during conquest
• Bowel infection is a predisposing factor– Antibodies with cross reaction to joints
• Spine disease is not improved with anti-inflammatory drugs or methotrexate, need blockers of TNF