Embed Size (px)
Citation preview

Six Weeks of Strength and ProprioceptionTraining Does Not Affect Muscle Fatigue andStatic Balance in Functional Ankle Instability
Michael E. Powers, Bernadette D. Buckley, Thomas W. Kaminski,Tricia |. Hubbard, and Cindy OrtizContext: The combined effects of strength and proprioception training, especially inindividuals with ankle instability, have not been studied extensively. Objective: Toexamine the Influence of 6 weeks of strength and proprioception training on mea-sures of muscle fatigue and static balance in those with unilateral functional ankleinstability (FAI). Design: Pretest-posttest, randomized groups. Setting: A climate-controlled sports-medicine research laboratory. Subjects: 38 subjects witb self-reportedunilateral FAL Measurements: Muscle fatigue was determined using the median powerfrequency {f^^^^) from an electromyographic signal, and static balance was assessedusing center-of-pressure values obtained from a triaxial force plate. Results: Tberewere no significant effects of tbe strength or proprioception training on our measuresof muscle fatigue and static balance. Conclusions: Strength training, proprioceptiontraining, and the combination of the 2 failed to improve postural-stability characteris-tics in a group of subjects with FAI. Key Words: chronic ankle dysfunction, posturalstability, subtalar joint, motor control
Powers ME, Buckley BD, Kaminski TW, Hubbard T|, Ortiz C. Six weeks of strength .ind proprioception trainingdoes not affect muscie fatigue and slaticb.iUnce in functional ,inklp instability. I Sport Rehahil. 2004; 1 3:201-227. © 2004 Human Kinetics Publishers, Inc.
The lateral ankle sprain is one of the most common injuries suffered intoday's athletic population, and these injuries are most prevalent in cut-ting and jumping sports such as volleyball, football, soccer, and basket-ball.'^ It has been reported that the recurrence rate after a lateral anklesprain is as high as 80%. -'' This is a primary concern for athletic trainersand physical therapists, because individuals are more susceptible to long-term disability and degeneration after the initial traumatic episode.'''' ** Fur-thermore, athletes who experience more ankle sprains present with more
Powers is with the Division of Athletic Training, Shenandoah University, Winchester,VA 22601. Buckley, Kaminski, Hubbard, and Ortiz University of Delaware. Buckley is withthe College of Health, University of North Florida, Jacksonville, FL 32224. Kaminski is withthe Sports Medicine and Athletic Training Dept, Southwest Missouri State University, Spring-field, MO 65804. Hubbard is with the Dept of Kinesiology, The Pennsylvania State University,University Park, PA 16802. Ortiz is with Gainesville Health and Fitness Center, Newberry Rd,Gainesville, FL 32652.
201

202 Powers et al
severe residual symptoms than those less frequently injured do.'' Yeungand colleagues'' reported that pain was the most common residual symp-tom, and a subject's reported sense of instability was rated second.
Although speculations have been made regarding the cause of long-termpain, dysfunction, and disability associated with lateral ankle sprains andreferred to as chronic instability, the exact reason for these problems re-mains unclear. The source of the chronic ankle dysfunction has tradition-ally been described as an either mechanical or functional instability. Theterm functional mikle instability (FAI) was first coined by Freeman'" and de-scribes the subjective feeling of "giving way" of the foot and ankle. A con-temporary definition characterizes the condition as a history of ankle inse-curity. Recently, a refinement of the criteria used to classify individuals asfunctionally unstable was published." Conversely, mechanical ankle in-stability involves structural damage to the support network (ligaments,tendons, neurovascular components) surrounding the ankle-subtalar-jointcomplex and is best labeled ligamentous laxity.' Hertel'^ best summarizesthe relationship between the 2 entities by saying that "mechanical instabil-ity and functional instability are probably not mutually exclusive entitiesbut more likely form a continuum of pathologic contributions to chronicinstability"!''^
Bosien et al'^ were the first to report that peroneal muscle weakness wasthe most significant factor contributing to recurrent ankle sprains. Sincethat time, a number of others have reported similar strength deficits inindividuals with FAI. ''"^ Thus, peroneal strengthening has been advocatedfor many years in the rehabilitation of both acute and chronic anklesprains.' '"^ Strength deficits are not always observed, however, in thosewith FAI, ^ ' so factors other than muscle weakness must be involved inthis condition.
Reestablishing neuromuscular control is a primary part of the rehabili-tation process after lateral ankle sprains and plays a pivotal role in hasten-ing retum to activity and preventing reinjury and long-term dysfunction. ' - 'Proprioceptive and kinesthetic sensations are part of the 4 basic elementsnecessary for reestablishing neuromuscular control and functional stabil-ity. Fxamples of these rehabilitation techniques include joint-repositioningtasks, functional range-of-motion activities, axial loading, and closed ki-netic chain exercises.^" One specific ankle exercise involves balance taskson a wobble board. Ultimately, the clinician varies the visual and supportconditions to challenge and alter the feedback systems needed to performsuch movements. It is recommended that variation in speed and intensityof the proprioceptive tasks be initiated to appropriately challenge the neu-romuscular system at the highest level.-'
Relationships between FAI and deficits in joint-position sense (JPS) andbalance have also been observed.''*' ^-'' Because of this, deficits in neuro-muscular control have been suggested as a cause of FAI. Like muscle weak-ness, however, these deficits are not always present in those suffering from

Functional Ankle Instability 203
-^ Despite contradictory findings, the improvement or restoration ofneuromuscular control has become a common component of ankle reha-bilitation.^^ Although the effects of proprioception training in those withand without FAI have been investigated, - • ^ ' few have examined the ef-fects of strength training alone-™ or the combination of both.^' In one study,6 weeks of elastic-band strengthening significantly improved JPS in subjectswith FAI.^ Proprioception exercises were not performed in that study, socomparisons between protocols could not be made. More recently, a 4-weekbalance-training program consisting of both static and dynamic balancingwas shown to improve dynamic balance in both control and experimentalgroups.^''
It has also been shown that muscle fatigue can significantly impair pos-tural control. ' '' Thus, it is likely that improvements in muscle strengthand endurance through training would improve stability. Generally, fa-tigue is considered a failure to maintain a required or expected force. It iswell accepted that the inability to maintain this force is associated withchanges in muscle electrical activity. Because of this, electromyography(EMG) is commonly used to assess fatigue. As a muscle fatigues, changesin EMG frequency characteristics (eg, median power frequency) that canbe used to quantify the rate of fatigue occur. Whereas EMG ampHtude in-creases during fatigue, the median power frequency actually decreases,reflecting decreases in muscle-fiber conduction velocity.^^''
Studies involving a combination of both proprioception and strengthtraining in those with ankle instability have not been pursued, Thus, weset out to examine the influence of 6 weeks of strength and proprioceptiontraining on muscle fatigue and static balance in individuals suffering fromunilateral FAI. We hypothesized that the subjects participating in a com-bined program of strength and proprioception training would show greaterimprovement in postural stability than any of the other groups.
MethodsDesign
A pretest-posttest randomized-groups design was used for this investiga-tion. All testing was performed in a single-blind fashion, in which the ex-aminers were unaware of which training group each subject had been as-signed to. The dependent measures were static balance and muscle fatigue.The independent variables were training group, test (pretraining andposttraining), and time interval during a 1-minute single-leg stance.
Subjects
Thirty-eight male (22) and female (16) subjects (age 21.6 ± 2.9 years, height174.1 ± 9.8 cm, mass 78.2 ± 16.6 kg) suffering from FAI volunteered to par-ticipate in this study. They were physically active, college-age individuals

204 Powers et al
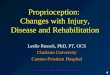
who were able to maintain their activity level regardless of their FAI sta-tus. Before participating, the subjects read and signed an informed-consentagreement (#2000-274) that was approved by the university's institutionalreview board. All subjects were examined by the same clinician and werecleared from having any mechanical instability before participating. Subjectswere excluded from participation if they did not meet the stringent FAIcriteria established by Hubbard and Kaminski (Figure 1)."
Instrumentation
Electromyography. A Myopac EMG system (Run Technologies, LagunaHills, Galif) was used to collect the raw EMG signal. The unit specifica-tions for the EMG included a frequency bandwidth of 10-1000 Hz, CMRR110 dB, input resistance of 1 MW, and a sampling rate of 2000 Hz. Aftersampling, EMG data underwent an analogue-to-digital conversion and werestored on a PG-type computer using the DATAPAG 2000 (Run Technolo-gies) analogue data-acquisition, -processing, and -analysis system.
Force Plate. Deviation from the center of pressure (GOP) was measuredat a frequency of 50 Hz using a triaxial force plate (Bertec Gorp, Golumbus,Ohio). The force plate uses a series of force transducers to record the ground-reaction force and its point of application, or GOP. The raw signals fromthe force plate underwent an analog-to-digital conversion and were storedon the same PG-type computer using the DATAPAG 2000 software men-tioned previously.
MeasurementsMuscle Fatigue. We examined muscle fatigue using the median power
frequency (/ j) of the EMG signal. It is well accepted that muscle-fiberpropagation velocity decreases with fatigue.-^^ As the propagation veloc-ity slows, there is a shift in the EMG-signal power spectrum and a decreasein the median frequency of that spectrum. Thus, an observed decrease inthe/^.j would indicate muscle fatigue. To begin this procedure, eachsubject's skin was shaved and cleaned with isopropyl alcohol to reduceskin impedance. Immediately afterward, bipolar 1-cm Ag/AgGI surfaceelectrodes were placed in parallel with the muscle fibers at a midpoint be-tween the motor point and the musculotendinous junction of the tibialisanterior (TA) and peroneus longus (PL), with an interelectrode distance of1.5 cm. All electrode placements were confirmed with manual muscle test-ing and checked for cross-talk with real-tin^e oscilloscope displays.
Once electrode placements were confirmed, we positioned the subjectsin a double-leg stance with the test leg centered on the force plate. We theninstructed them to keep their hands on their hips and focus on a visualtarget aligned at eye level 2 m in front of the platform while they assumeda single-leg stance and maintained balance for 60 seconds. If at any time asubject lost balance and touched the other foot down, he or she was told toimmediately return to the test position.

Functional Ankle Instability 205
Part 1: BjnctlOfMl Ankto inttabm^ QuMtlonnaira
1. Concerning your purporMd anM* insMMity. doesttiia (nfury invoM only ona arM»7 Y NIf yM. ( M th» Inilial apltod* involv* your ankle-roUng inwarcT? Y Nif no. do not oontimw to M out (Ms question-
2. WNcti ankle suffers tfw instabiMy?3. Did m« initial injury to your anMe reqtire
immobttzation. or b ( ^ . of any torm (cast, brac-es, etc)? Y N
4. htove you had any fractures (brvtfts) in either c4your ankles? Y N
5. Is the intured/unstable ankle funcbonally wesdter,mora painfU, looser," and less functional thanyour uninvotved ankle? Y N
6. Do you ever have episodes of your ankle "givingway" or "roMng over" difftr>g d a ^ activity (ath-tetk; or othenvtoe)? Y N
7. Oo you attribute your current rnstabiHty to past in-juries to the affected ankle? Y N
B. Have you had an episode ot ir^wy ("your anklewas hurt," "you were in great painl to the af-fected ankle within the last 3 months? Y N
9. Have you been watkmg around unassisted withouta lirnp." for at least the past 3 months? Y N
10. Are you cunwitfy invoh/ed in a "formal" rehatMiita-tkxi program for tt>e affected ankle? Y N
tf you answered yes. pleaae dascribe hera.
11. Can you describe a symptorT^s) 0* your ankle"giving way"?
Part il: Clinical Examinatk>n of Ankle Stability
Is than sweMng present? Y NIs there ecchynwsis presmt? Y N
Anterior Drawer TestRightankleLeft ankle
Talar Tltt Test
Right ankle +Left ankle +
Cleared for partidpatkin m the study? Y NSignature ___ „ _„
'To qualify as functional ankle irtstabillty. questions 3. 5. 6. 7, and 9should be answered "yes." Questions 4, 8, arKJ 10 should be answered"no." and no dintcal stgns ot mechanical Instability can be present
Figure 1 Criteria for functional ankle instability (reproduced with permission from
Hubbard TJ, Kaminski TW. Kinesthesia is not affected by functional ankle instability
status. /AfWe(/c Train. 2002;37:481-486).

206 F'owers et al
values for each 5-second interval during the 60-second collec-tion period were obtained from the DATAPAC 2000 software and recorded.Because there are a number of variables that can affect the raw EMG sig-nal, a general representation of the signal must contain a formulation thatallows a comparison between different individuals and testing sessions.This is commonly achieved by normalizing the variables of the EMG sig-nal with respect to their maximal measurable value in a particular experi-mental procedure. For the current investigation, we normalized the /^^from each of the 5-second intervals to the/ ,_^ of the first 5-second interval,which we considered the nonfatigued, or baseline, interval. Thus, the datafor the final 11 intervals (5 through 60 seconds) were calculated relative tothe first 5-second interval and used for statistical analysis.
Static Balance. Static balance was assessed during the same single-legstance using the Bertec triaxial force plate. COP (point of application of theground-reaction vector) can be directly related to the motion of body cen-ter of mass, or body sway (postural stability or balance). As the body cen-ter of mass deviates (as the body sways), the COP also deviates. Thus, theamount of deviation from the mean COP (measured in centimeters) pro-vides a measure of motion of the body center of mass and a quantificationof body sway. The mean migration of the COP over the base of support inthe anterior/posterior and medial/lateral directions and the mean overalldeviations from COP (calculated using the average length of the diagonalor hypotenuse between each COP point and the mean COP) were obtainedfrom the force-plate module of the DATAPAC 2000 software. Static bal-ance was assessed in 2 ways. Eirst, a mean COP was calculated for theentire 60-second collection period, and the mean deviation from that cen-ter point was detennined for each direction and used in the statistical analy-sis. Second, a mean COP was calculated for each 5-second interval of the60-second period. The mean deviation for each direction that occurredduring that interval was then determined and used in the analysis. Thiswas done to provide a way to observe changes in balance over the courseof the 1-minute period.
Training Protocols
Subjects were randomly assigned to 1 of 4 treatment groups: strength train-ing (S), proprioception training (P), strength and proprioception training(SP), and control. The S group participated in 6 weeks of plan tar-flexion,dorsiflexion, inversion, and eversion strength training using Theraband®(Hygenic Corp, Akron, Ohio) elastic bands. The P group participated in 6weeks of proprioception training that involved T-band kicks. The SP groupperformed a combination of both training protocols, whereas the controlgroup refrained from all formal ankle training. The S and P protocols werebased on common clinical practice and experiences; each protocol involvedthe application of ordinary strength and proprioception rehab techniques.All 3 training groups exercised 3 times a week for 6 weeks. The time spent

Functional Ankle Instability 207
in each session, however, varied according to group. All subjects trainedusing their EAI ankle only, and each training session was supervised by amember of the research team. Subjects assigned to the control group re-frained from any ankle training during the 6-week period.
Stretigth Training. The S group trained using a progressive resistanceprotocol utilizing Theraband elastic bands. Subjects progressed weekly insets and/or resistance throughout the training period (Table 1). Thestrength-training session was performed with the subject seated on the floorwith the knee extended. The elastic bands were doubled and attached to ahook on the wall. The looped end was secured to the foot while the subjectperformed the plantar-flexion, dorsiflexion, inversion, and eversion mo-tions. Subjects were instructed to concentrate on performing only the move-ments at the ankle joint and not add any extraneous movements from ei-ther the knee or the hip joint. The training resistance was determined bycalculating 70% of the resting length of the doubled Theraband elastic band.This distance was then added to the resting length of the band and a subse-quent mark placed on the floor, to which the elastic band had to be stretchedfor the subject to perform the exercise routine. Regardless of the color (re-sistance) of the band, all strength-training exercises were performed withthe bands elongated to 70%. This protocol was designed to ensure that allsubjects trained with a consistent and progressive amount of resistive force.Using a set/rep protocol similar to that described by Docherty et al, " eachsubject performed 10 reps per set and progressed uniformly throughoutthe 6-week training period.
Propriocqition Training. The P group trained using a progressive proto-col with Theraband elastic bands. A T-band-kicks protocol modified fromthat originally described by Tomaszewski^^ was used in our study. The elas-tic bands were attached to a hook on the wall but were not double loopedlike the bands that were used in the S protocol. The subject placed theuninvoived foot through the loop in the band opposite the loop attached tothe wall. The subject then stood barefoot while balancing on the EAI ankle.
Table 1 Strength-Training Protocol
Week
1
2
3
4
5
6
Color
red
red
green
green
blue
blue
Sets
3
4
3
4
3
4
Reps
10
10
10
10
10
10

208 Powers et al
The uninvoived foot was used to perform the kicking motions only. Thekicking motions consisted of short, quick oscillations. Consistency of oscil-lations was controlled by having the subject perform the T-band kicks tothe beat of a metronome set at 80 beats/min. While balancing on the FAIankle, the subject was then asked to perform 2 sets of 25 T-band kicks in 4different directions of hip motion (flexion, extension, abduction, and ad-duction). If subjects were able to complete 2 sets of 25 reps in each direc-tion without losing balance or touching the uninvoived foot to the ground,they would increase the resistance (color) of the elastic band at their nexttraining session. All subjects began using the red-color Theraband. Once asubject reached the highest resistance (gold color), repetitions were in-creased by 10 if further progression was necessary.
CoDibined Training. Subjects in the SP training group performed the Sand P exercise protocols in conjunction with one another. As expected, thistraining session required more time on the part of the subjects to completethe entire routine. The order of training (strength vs proprioception) wasrandomized at each session.
Procedures
On reporting to the athletic training/sports-medicine research laboratory,each subject completed a questionnaire detailing his or her activity leveland demographic information. We then assessed the subjects for TA andPL muscle fatigue and static balance while they performed a single-legstance on the unstable limb for 60 seconds. After testing, we randomly as-signed each subject to 1 of the 4 groups. If assigned to one of the traininggroups, subjects trained 3 days per week for 6 weeks. Immediately afterthe training period, the subjects returned and were reassessed using a pro-tocol identical to the one used during pretesting.
Statistical Analysis
SPSS® 10.0 for Windows® (SPSS, Inc, Chicago, 111) was used for statisticalanalysis. An alpha level of P < .05 was set a priori for all analyses. Six mixed-design analyses of variance (ANOVAs) with repeated measures were usedto determine whether there were differences between pretest and posttestn:\easures for deviation from COP (cm). Three 4 x 2 mixed-design ANOVAswere used to analyze the dependent measures involving a single COPmeasure over the entire 60-second period. The between-subjects factor forthose analyses was group status (S, P, SP, or C), and the within-subject fac-tor was test (pre vs post). Three 4 x 2 x 12 mixed-design ANOVAs wereused to analyze the COP measures involving the 5-second time intervals.In addition to the factors used in the previously mentioned ANOVA, asecond within-subject factor, time (twelve 5-second intervals), was added.Two 4 X 2 X 11 mixed-design ANOVAs were used to determine whether

Functional Ankle Inslabilily 209
there were differences between pretest and posttest measures for/ ^ ,. Thebetween-subjects factor was group status (S, P, SP, or C), and the within-subject factors were test (pre vs post) and time (eleven 5-second intervals).Tukey's honestly significant difference (HSD) post hoc analyses were usedto examine differences of interest.
Results
Muscle Fatigue
Peroneus Loti<?us. Normalized f , values for the PL can be found inTables 2(a) and 2(b). No significant test (P = .418) or group (P - .594) maineffects were observed, but a significant time main effect was observed (P -.024); the/_^ ^ during the final time interval (93.26 ± 19.97%) was signifi-cantly less than the/^^ during the initial time interval (99.65 ± 15.52%).Likewise, a significant Test X Time interaction (P - .028) was observed forthe PL; the/^_^ progressively decreased during the 60-second static-balancetest at pretesting and at posttesting (Table 2), but the decline only reachedsignificance during pretesting. The Tukey HSD post hoc analysis deter-mined that a difference of 9.17% w as required for statistical significance.Training had no effect on this measure—no significant Group x Time (P =.807), Group x Test (P = .269), or Group X Test X Time (P = .559) interac-tions were observed.
Tibialis Anterior. Normalized/^^ values for the TA can be found in Tables3(a) and 3(b). No significant testT? = .877), time (P - .124), or group (P =.695) main effects and no significant Group X Time (P - .117) or Group XTest (P - .346) interactions were observed. Unlike the PL, no significantchanges in/^^ (P - .418) were observed for the TA during the 60-secondstatic-balance test at both pretesting and posttesting. Likewise, no signifi-cant changes were observed from pretraining to posttraining, regardless ofgroup (P = .325).
Static Balance
There was only 1 occasion when a subject lost balance and touched theother foot down. This occurred during pretesting, and the subject was ran-domly assigned to the P group. Removing this subject's data did not affectthe results, so the data were included in the analyses. At no other timeduring pretesting or posttesting did a subject lose balance to the extentthat the other foot touched down.
Anterior/Posterior. No significant test (P = .964) or group (P = .598) maineffects were observed for anterior and posterior deviation from COP whenthe means over the entire 60-second balancing period were analyzed. Train-ing also had no effect on this measure; the Group X Test (P = .734) interac-tion failed to be significant (Table 4). Likewise, no significant test (P = .591),

210 Powers etal
PJZu
300co
oQ-I-lc01
Ic5
•o01N
u
3U l
<
+1
CO
o
+1rsrodo
I V
+1ino
00.
rv
+1LA
98.
m
+1
98.
+1
97.
o
+1
96.
rv
+1mLn
96.
+1 +1 +
rM O
•auclaoU
a.p
DOc0)
oU
rororo
+1
57
LnCO
+1
63r v
+1
63oc^
+[15
COCO
+1
42
IVIVO
+1
56
CO
+1
79
Lnfv
+1
07
rvrv
o
+1
62
r v
o
+1Ln
rNrs
+1
21
M
rvLn
oo ,_:
oCO
1—
r o
Orvro
ro
ro
rvm" '
rvCO
d
+1mcn
+1i nro
+\rvCO
rs
+1'•0
+1nrv
+1 +1
rs
+1T f
ro+1rM1 "
-HroCO
+1roro
fN Oo o
+1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1f N " — r O r O O ~ i ' — O ^ l v r v - r J - O
rv
M
94
f Nrv
+1
58
LO
rv• ^
+1
93
fNrN
+1
33
ro"^
+1
34
en
+1
10
inrorv
+1
61
rv
+1
68
roO•~D
+1
87
rs
M
99
rs
+1
61
E 1/1
o1
LO
LnT
orM
Ln
1/1
i nf N
cirs
ly i
Or^
Lnrs
i / l
3121/1 1/1
O Ln oLn Ln ^
I I ILn o Ln

Functional Ankle Instability 211
Of
p-g
oQ
+1c
Ic
N
(N
-ac
15EoU
"5.
O
oU
E
rsroO
03 ±
-
44 ±
ro
27 +
rM• -
37 +
fSrv• -
38 ±
roCO
02 ±
rotrio
36 ±
70 ±
orv—
07 ±
tCO• -
47 +
rMCOLn
77 ±
oo
+1
.42
CO
-H
53
l=v
rv
+1
60orv
+1
64in
+181
?ro
72
ro
+1
00
fv
(N
+1
56
CO
+1
84
+1
15
roCTi
+1
86
+1 +1 +1
K
+1tn
in
+1CD
rv
+1 +1• - o
+1 +1rv \.D
>— ro ro o+1 +1 +1 +1
^ cq1- orv o
+1 +1 +1 +1 +1CO Ln
+1 +1
o1
in—
Ln
ors
Oro1
in
in
0-3
ro
O
Tmro
rv ocq ^cn fN
+1 +1fN ro -— rofN cn ro ro. p in ^^ ^fCTi Q^ O^ CTl
ro ro rvrv ro CO cn
+1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1'^ ^D L-O ^N •»o (*o CO ^r o^ ^ ^^

212 Powers et al
.215P
o
Q
+1cra
3
O
o
at
•o
-—-- rara .*-
PO
3
c15Eou
"S.a>u
Q.O
CO
+1 +1 +1 +1 +1 +1 +1 +1 +1 +1
+1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1
o ^ ^ i d r s o r ^ O nI - M O O - - O O O O O O O
CM O O
ro ro ro
C
24
+1
34
13
+1
29
18
+1
81
15
+106
23
+1
63
14
+1
44
22
+1
36
20
+1
23
25
+1
41
23
+1
72
?1
+
3S
roCT^
+1 +1 +1 +1
ro cnr o CTl
oaro in r-
I— -— I— .— rM -—
cnrs
CO o <nrf rv >XI^ ^ 1..DCTl CTl CTl CTl
+1 +1 +1 +1 +1 +1ro '«O "T 'T ro
rocn CO i n CO
cn CO
cn CO o i V.DCO '.D CO ro
V.O rM
Ln rv
O
O inoo ro
I ILO O m o m
m inci
rMm+1
oCO
LTi C> '—
ro in ro
c n c n o o c n o c n o
Con
tr
•V
+1
LO
ro
+1
SOL
ro
+1
SOL
ro
+1
102
ro
+1
107
m
+1
cn
+1
102
c^
+1
103
CO
+1
in
CT^
+1
ro
rM
+
o

Functional Ankle Instability 213
a;Pura
P
+1c
0
01
I
0) . -
ito oZ ^
il
3
loou
9
p(A
cnro
+1ro
104
CO
rs
10
±10
4
ror
+1fv
102
inCOun
+1fv
o
103
i n
Ln
+1fv
100
f Nrv
+1cn
101
rorv
+1
100
om
+1oro
100
orom
+1
o
"-
+1cnCO
100
CO
rs |
+1mro
99
cnCO
+1CO
CO
rv
+1ro
roro
+1mo
rM+1
o
ro
rs+1
r f
ors+1
z
rvcnr s
+1
f N
rocnr v
+1rvoo
CO
f N
+1fNro
CTlO
f N
+1O
m
(Nro
+1mK
in rsO O
ro rv
o oO O rM fN -—O O O O O
m
+1rs
107
11 ±
6.9
108
o
+1rv
104
i n
+1rv
105
CO
+1o
o
ro
+1rv
ZOL
m
+1m
104
CO
+1ro
104
f N
+1rv
105
o
+1in
106
+(
cn
i n
cqLn
+1O
o
r fi n
d-—+1,_roi n
o
Lnf vCO
+1vXJ
ro,—o
cnr—
rs
+1CT^m,—o
—v£lCT^
+1CTlroCTlCTl
<DCTi
ror -
+1rororoCTl
vn
cn+1vn•rfr v
cn
r o
CO
+1I V
mf So
,—
d+1,
mo
rv•.£
+\,CTl
roCTl
(T>
cn+1rororMo
23
+1
21
rM• ^
+1
45
"^
+1
52
mvTiro
+1
31
cnroro
+1
94
roo
+1roro
rfcno
+1
83
orM
+1—
•rfmm
+1
83
roro
+1
32
oi n
+1
52
LOrM rM
I ILo o1— fN
cncn
fN ro ro

214 Powers etal
Table 4 Anterior/Posterior Deviation From Center of Pressure(Mean ± SD) for the Entire 60-Second Trial for Each Group FromPretesting to Posttesting*
Group Pretest Posttest
Strength 5.26 ± 0.95 5.23 ± 0.70
Proprioception 5.25 ± 0.98 5.00 + 0.78
Strength and proprioception 5.30 ± 0.52 5.39 ± 0.25
Control 5.59 ± 1.07 5.00 + 0.78
*Center-of-pressure values are in centimeters.
time (P - .365), or group (P = .669) main effects were observed when the 60-second period was separated into 5-second intervals and analyzed using asecond within-subject variable of time. Training had no effect on this mea-sure either; no significant Group X Test (P = .172), Group X Time (P - .967),Test X Time (P - .254), or Group X Test X Time (P - .358) interactions wereobserved (Tables 5[al and 5Ib]).
Medial/Lateral. No significant test (P = .178) or group (P - .911) maineffects were observed for medial and lateral deviation from COP when themeans over the entire 60-second balancing period were analyzed. Trainingalso had no effect on this measure; the Group X Test (P = .352) interactionwas not significant (Table 6). Likewise, no significant test (P = .746), time (P=.871), or group (P - .308) main effects were observed when the 60-secondperiod was separated into 5-second intervals and analyzed using a secondwithin-subject variable of time. Training had no effect on this measure; nosignificant Group X Test (P - .307), Group x Time (P - .653), Test X Time(P - .884), or Group X Test X Time (P = .175) interactions were observed(Tables 7ta] and 7Ib]).
OveraU. No significant test (P = .681) or group (P - .713) main effectswere observed for deviation from COP in all directions when the meansover the entire 60-second balancing period were analyzed. Training alsohad no effect on this measure; the Group x Test (P - .737) interaction failedto be significant (Table 8). Likewise, no significant test (P = .591), time (P =.565), or group (P - .669) main effects were observed when the 60-secondperiod was separated into 5-second intervals and analyzed using a secondwithin-subject variable of time. Training had no effect on this measure; nosignificant Group X Test (P = .172), Group x Time (P = .967), Test X Time(P = .254), or Group X Test X Time (P = .358) interactions were observed(Tables 9ta] and lb]).

Functional Ankle Instability 215
Of
x:u
E
-Hc
oOf
c
Eo
.2*>Go
C 00< _c
re ,^
"5 5
<
cIEEou
c_o
a;uO
c(/I
coU
01EP
+1 +1 +\ +1 +1 +1 +1 +1 +1 -I-l -H -H
+1 +1 +1 -H -HI +1 +1 +1 +1 -H -H +\
i n
(N
rs - ^ Ln 00CTl CO CO CO r s
CTl OCT> O
o o o o o — • - • -+1 +1 +1 -H -H +1 -H +1m ^ O Q*i G* ^ ^~ O
+1 +1 +1OI T - .—rs CO o
CO COCO o o i n
CO m r n r^ r^ >—CO -XJ CO .— r s CO
i / i i / j Ul 1/1
O Ln O Ln(N fN rn rn
I I I J .Ln o in o.— rs rg m
O in
t TLn o
-H +1 +1 +1 +1 +1 -H -H -H +1 +1 +1
•.0 ^.O CTl CTl
.— d - — d - — r s i ^ ^ ^ d d d+\ +1 +1 +1 +1 +1 -H -H -H +1 -H +1
rg "tj- O r r~. OO O m rs rn rn
O in Oin in ^
LTi d Ln

216 Powers et al
re
01* -
IH
reLU
00
—3G
5"+1cre
101
3(/><fiZi
mte
r
EO
LU
C
rt>01G
?ri
or
OS
t(
a.
01
i n
t2
*OA.S'E
rrai
» * -o
TS.Si.IH'(/)
<
claEou
ion
ept
ioc
CL
Pro
ac*•t / 1
"o
cou
uE
Tes
t/Ti
+i
19
o
+1
07
oCTl
+1
08
o
+1
87
o
+1
06
KO
-H
23
•.Dm
-H
22
rj0
-H
94
otN
-H
02
c
+1
04
LO
+1
34
COCTl
-H
24
CTl r s jCO CTi
CO txIx q rx cq oS IX. cqci ^ dl CD (5 d d+1 +1 -HI +1 +1 +1 +1
m inCTl IX
-Ho o —+1 +1 4-1
-O •XiCO ^
ro ^•XJ O
O IXI x <T>
O inro ro
I ILn O
o in o in
T t "[m o m
Ln
O
COCTl
d41
m m' ^ CTl
o-H
89
- -
-H
92
o-H
11
O
-l-l
86
o-HvD
O
-H
n
o-H
63
• -
-H
01
o+1
63
o-H
06—
+145
o+1
95
ro
O
+1
85
.—+1
.55
COIx
O
+1
12
+1
92
o.—-H
90
mCTl
O
41
23
.—41
- -
rorx
o41
05
=0CO
o41
83
oClo+1
07
+1
25
t'Z
T —
+1
52
• o
1 411 •—1 Ln
o41i n
M
+1,>vO
o+1mCO
o+1,_o
--41I X•XJ
o-Ha iI X
O
41mm
+1i nm
—
41Krn
o+1
f N

Functional Ankle Instability 217
Table 6 Medial/Lateral Deviation From Center of Pressure(Mean + SD) for the Entire 60-Second Trial for Each Group EromPretesting to Posttesting*
Group Pretest Posttest
Strength 5.47 4 1.21 5.34 ± 0.55
Proprioception 5.92 ± 4.60 5.09 ± 1.80
Strength and proprioception 5.24 ± 0.93 5.74 ± 1.03
Control 6.03 ± 1.00 6.40 ± 2.25
*Center-of-pressure values are in centimeters.
Discussion
Neuromuscular training has become a major component of ankle rehabili-tation. Although numerous rehabilitation protocols have been developedand used clinically, few have been shown to be effective through scientificinvestigation. Table 10 provides a summary of studies investigating theefficacy of these training protocols. For the present investigation, we hy-pothesized that fatigue would be reduced and static balance would im-prove after 6 weeks of intensive strength and proprioception training. Wehad further hypothesized that this improvement would be greatest in theSP group. This did not occur; none of the groups showed improvement oneither of the variables assessed. We only used 1 trial of the single-leg-stancetest at pretesting and at posttesting. Had we used multiple trials and takenthe means of those trials, the results might have been different, but it ispossible that a learning or practice effect would result in an improved bal-ance on consecutive trials (this has been shown to be a source of intrasubjectvariability). ** Likewise, it is possible that fatigue would result in an im-paired balance on consecutive trials." Thus, we thought that using only 1trial would eliminate confounding variables and provide us with the in-formation needed for this investigation.
Theraband resistance training and T-band kicks are commonly used toimprove strength and proprioception during rehabilitation of the unstableankle. • ' ''• '•'''*'''" Thus, the training protocols used in the present investiga-tion were primarily chosen based on clinical practice. One of the greatestdifficulties we encountered in developing our training protocols is the lackof objective evidence that supports the use of elastic-band resistance train-ing. The material properties of Theraband have been examined in order toquantify the amount of force that is applied with a given color and length.*'This has enabled therapists and clinicians to develop strength and pro-prioception training protocols with a more objective method of resistance

218 Powers ct al
Zi
oa
I
BPureLUeo.£
Q
Q
+1cre
13( / ]tnSJ
•a
cL£Eou
c_0
'Q.a;u
_O
O.o£a.
Zi
cU
o
Zi
G"20)re
; - ' DO
u013
ou
^ D c o o r ^ i — c o > i ) r v c 6 ' — r o o ^
t — I — ( N . — r s ) . — ,— ,— r s j r s j r j r -
+1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 -HrN ^ rN O ^ ro ^ rn ^ O ^
CTl LT)O
oCO Ln CTl
+1 +1 +1 +1 +1 -H +\ +1 +1 +1 +1 +1
CO CO
CO O •^ O rsj' ^ in Lfi Ln in
CT^ CO
• T ^ ^
mm m
o COrN O
fNCO
OCO
CO r o COT f CO -rf-
•— r s j m r o r n r s j i — t N L O r o r o r s j
-H -I-l -H -H -H -H -H -H +\ +\ +\ +\• . O ' — T f . — o r - v r o c o o c o m
-H -H -I-l -H +\ +\ -t-l -H -H -H -H +\
Lfi t rJ- rf m ' ^
COCTl
+1
51
IV.Ln
+1
15
Ln
+1
06
+1
64
CO
+1CO
rorsj
+1
22
i n
+1
98
o
+1
31
Ln
+1Lnrv.
m
+1
01
oCO
+1
19
,—
+1
82
LO
oor s j
LOrsj
Orsi
om1
r-j
i n
oro
O
5-4
ro
i n
ooi n
m
0-5
Ln
o1
Ln

Functional Ankle Instability 219
if^ ^<
rval
1\=unLU0 0
3
O
cts
:Ul
All
1.£lcEou
+1cre
. 2a;Q
"2
ra *
"I
a.o
coU
-H +1 +1 +1 +1 -H -H -fl +1 +1 -H -H
-H -H +1 -H +1 -H +1 +1 -t-l -l-l +1 +1
-H -l-l +1 +1 +1 -H -H -+-I +1 -t-l -H -t-l
-t-l +1 -H -l-l -t-l +1 +1 -t-l -fl -H -t-l +1O ' . o ^ c o r v O C T i L o r v O ^ r v i —O ^ r v r o L n T r c q i ^ o c q c q - — cq
OO
r-1
+1
65
r -
+1
88
o-t-l
04
f N
-t-l
87
- -
-t-l
15
+1
57
r -
+1
36
. --H
65
f N
-t-l
74
- -
-H
63
+1
77
+1
91
in Ln T • ^
1/) 1/1 i/i t/1 i/i (/I 1/1 1/1

220 Powers et al
Table 8 Overall Deviation From Center of Pressure (Mean ± SD)for the Entire 60-Second Trial for Each Croup From Pretestingto Posttesting*
Group Pretest Posttest
Strength 8.42 ±1.15 8.28 ±0.74
Proprioception 8.82 ± 4.37 7.92 ± 1.90
Strength and proprioception 8.23 ± 0.90 8,72 ± 0.88
Control 9.11 ±1.14 8.96 ±2.25
*Center-of-pressure values are in centimeters.
progression. Docherty et al^ used this principle and reported improve-ments in eversion and dorsiflexion strength after 6 weeks of progressiveelastic-band training. As in our study, their subjects had a history of unilat-eral FAI. In addition, their subjects demonstrated improvements in JPSmeasures, a finding they attributed to enhancements in muscle-spindleactivity. We did not assess jPS in the present investigation but did assesspostural stability, another measure of neuromuseular control. Although weused a strength-training protocol similar to Docherty's, improvements inpostural stability were not observed. It is difficult to make comparisonsbetween the 2 studies, however, because of the differing measures of neu-romuseular control. The exercises we used during strength training andthose used by Docherty employed open kinetic chain movements. Thus,the motions were limited to the ankle and were identical to those usedduring JPS testing. We would expect greater improvements to occur whentesting is performed in a similar manner as training. Our postural stabilitytest was performed in the closed kinetic chain position and required hipand knee, as well as ankle, stability. It is possible that the single-leg-stancetest we used was not sensitive enough to detect isolated improvements inankle function achieved through open kinetic chain strength training. Im-provements would have been expected after proprioception training, how-ever, which was performed in a closed kinetic chain position similar totesting. This did not occur. One explanation for this might be a lack of defi-cit. We did not assess the unaffected limb in our subjects. Thus, we areunsure if there were deficits when the subjects balanced on the unstableankle as compared with the healthy ankle. Some authors have reporteddeficits in postural stability when comparing subjects' unstable and healthy
but others have not.'''-^ Furthermore, impairments in TA andot been reported in those with FAI. To our knowledge, the
EMG-frequency characteristics of the TA and PL have not been investi-gated in that population. Thus, it is possible that we did not observe sig-

Functional Ankle Instability 221
C
!s/a
lBnte
n
• "
01
E
ura
uueo
uri
Q
Q
+1c
^ 1
surf
cn
(JE2c
iati
>01
Q
2
O
Table
~>u•u15"
Jlsu
• aV
15Eou
c
tio
a.U
.9a.
sa.
gth
c
itrei
"pcou
I
Tes
t/n
--+1
79
--+1
25
(N
-H
73
-l-l
35
f N
-l-l
CO
f N
-H
61
r -
-H
74
. -
+1
62
• -
+1
62
--+1
67
rs
+1
61
f S
-H
06
+1 +1 -H -H -H +1 +1 +1 -H -H -H
COCO
'—
+1
98
oCOf N
+1
89
ooro
-1-1
87
r-
c-f s
- f
fN
cr
CO(-Jro
-H
90
-^f N
+\
r-i
rN
-H
64
Ln
rM
+1
06
COrof N
+1
07
• -
+1
78
' t
+1
31
m
-1-
n
^ r o L n i n ^ . — c O r o r N C N O Oc o i n - — ^ ^ ^ ( r ) ^ c t j i f o r s , N ,
. — ^ f N - — I— r ^ " — T — >— f N i — t—
-H +1 +1 +1 -H -H -l-l -I-! -H -H +1 +1
m COro O
-H -H +1 -H +1 -l-l
fM LO rs
r-i >— CN-H -H -H
t n
o
o1—
1Ln
Ln'—
o1
in
i nrs
ci
+1 +1• * ^ N O O ^ O ^ ^ ^ r ^ | ' — (Ti'd'fMc q i ^ < T i ^ c q c q ^ ' - ; ( N L n C T ir ^ r ^ " \ O c d r ^ r ^ a D c d r ^ r ^ r ^
O in o Lo o Ln o
0-3
roLn
mTo
Ln
Ln
Ln
oIT)
1mLn

222 Powers et al
ii
V
01
p
DC
3G
+1cfl
0)ciiUEo
2
'E2
" 4 -
o
15"3
1 —
-HI
(Nf N
33 ±
t —
-HI
Pvr -
-HI
rn
+1'—
45 +
'—<N
+1
'—(N
87 ±
orN
63 ±
Lnr -
62 ±
I N
+1
r*!-—
12 ±
V
15Eou
a.0)u
a.p
to
ou
I
rsi
-HIO
cn
.83
+1rv
cn
.12
-HICO
.34
-HImo
-HI!N0^
.09
IN-HI
cn
.89
-HI
.62
-HI
CO
.09
-HIO
-HICTi
rv
.70
-HI
m
.29
+1
+1 +1 +1 +1 +1 +1 -HI -HI -HI -H -HI -HI
-HI -HI -HI -HI -Hi -HI -HI -HI -HI -HI +1 +1
<j^ *ji <yi fj^
rsi
+1
44
'it'—-HI
41
o'—-HI
98
r s j
+\
47
oLnI —
-HI06
•rf
T—
-HI
28
Ln
f N
-HI
49
-HI
43
of N
-HI
31
-HI
23
(N
o+i
54
C3
T—
+(
t / 1
L O
6o
1Ln
LnT
r—
o(N1
, F
i n( N
ci=(N
oLn
i n
<im
o Ln
t toLnLA
IT)
oL O
o1
.9-
u

Functional Ankle Instability 223
Ouoofa.
D.
oc
.EflDC
<UQ.
ra
E3(/I
a.ao
Pro
pr
"G
ra
Fret
dur:
^ ->
'% ^
m m•s
DO=
z
1-0
occ
ain
i
rara
C
inat
0ou
craflc
a;
3o
ra
OJ
J—
raCD
Q .
-oC
ern
m
raQJ
lar
CO
o o o
•a "D • •
^1
c co oa> QJu uc cra ra
"ra "ra
^-^ *.ml IJ\1/1 Ul
^ ^ ra
ii il "ra^ ^ 03
. b . b Jit/) W-) I—
00c0
- C
U
roOJ
X0U
^ ^ o o ^CO ^ 1— .— CO
O .0 .O .O .O
OJ>.
cher
t
oQ
raQJ
uffin
raO
ra
QJ1/1
QJI
I—
ffm
ai
oX
tsus
a
.h O

224 Powers el al
nificant improvements because deficits in muscle function and posturalstability did not exist to begin with. It is important to note that the sensitiv-ity of this type of testing in detecting these deficiencies remains largelyunknown at this time.
The efficacy of the T-band-kick exercise has also been previously inves-tigated. ***" In a comparison of exercises developed to enhance neuromus-eular function, Cordova et al^' observed greater EMG activity in the PL andTA when the subjects performed T-band kicks. Unfortunately, measures ofneuromuseular function were not assessed in that study. Baker et al, ' how-ever, examined the effects of a 6-week T-band-kick training protocol onpostural sway. Their protocol consisted of performing the kicks with theeyes open and progressing to eyes closed with repetitions that ranged from30 to 50. They concluded that the resistive-tubing kicks did not signifi-cantly improve postural sway and suggested that a greater intensity oftraining might be necessary. The repetitions were increased over the courseof the study; they began with 30 repetitions during week 1 and progressedto 50 repetitions during week 6, while the resistance remained the samethroughout the protocol. In the present investigation, we progressively in-creased the resistance (changing the color of the band) while the repeti-tions remained constant. We thought that this intensity would be greaterthan that used in the Baker et aP'' study. Like that study, however, traininghad no effect on postural stability. Observations by Chong et al" suggestthat improvements in postural stability cannot be explained by improve-ments in ankle strength and proprioception alone and are likely the resultof improvements in other body segments such as the knees, hips, spine,and upper extremities. Thus, rehabilitation protocols targeting only theankle might not be as effective for improving postural stability.
It might also be suggested that the 6-week duration of our training pro-tocol was not sufficient for noticeable effects to occur. Likewise, a trainingfrequency of 3 days per week might also be insufficient. Por example, shortertraining protocols (4 weeks) have been previously shown to have no effecton postural stability in healthy subjects *^ and subjects suffering from PAL*"Blackburn et al, ' however, theorized that a combination of strength andproprioception training would provide a greater stimulus for enhancedneural adaptation during a brief 6-week period than either type of trainingalone. This was partially supported in that they observed improvementsin dynamic stability after training, but improvements were also observedafter strength and proprioception training alone. Purthermore, like ourstudy, no improvements in static balance were observed. We did not assessdynamic balance in the present investigation, so it is unknown whether ornot improvements occurred. As mentioned previously, Docherty observedsignificant improvements in JPS after 6 weeks of strength training. It ispossible that our single-leg-stance test was more difficult than the open-chain repositioning used in that study. Thus, the 6-week training protocolwas not sufficient to produce remarkable changes. Had our protocol beenlonger, had a greater frequency, or a combination of the 2, changes n:\ight

Functional Ankle Instability 225
have been observed. Once again, it is important to note that the sensitivityof the deviation from COP measure in detecting changes that might occurafter only 6 weeks of training remains unknown at this time.
Other types of neuromuseular training have been shown to help im-prove neuromuseular control. ' ' '"^^ Bemier and Perrin' '' developed aprotocol specifically for balance and coordination training and observedconflicting results after 6 weeks of training. Their subjects, who were alsosuffering from PAI, showed improvements in static and dynamic balancewhen assessed with their eyes closed and open, respectively, but static bal-ance assessed with the eyes open and dynamic balance assessed with theeyes closed did not improve. No changes in JPS were observed, either. Shethet aP demonstrated that 8 weeks of ankle-disk training influenced reac-tion times of selected muscles during a simulated ankle sprain. Unlike inthe present investigation, the subjects in that study were not suffering fromany type of ankle instability. Likewise, static stability was not assessed, soit is difficult to compare their results with ours. Nonetheless, in similarstudies, subjects with PAI experienced improved postural sway after 8weeks"^^ and 10 weeks ** of ankle-disk training. This type of training hasalso been shown to decrease postural sway in healthy subjects. " It is pos-sible that the type of training used in these other studies provided a greaterstimulus for stability improvements than the protocols we used in thepresent investigation. Our subjects were suffering from PAI but were notin an acute stage after injury at the time of the testing and training. Thus,the elastic-band strengthening and proprioception exercises nright haveprovided only a modest stimulus for adaptation. Had our subjects been inthe early stages of rehabilitation, the exercises would have been more chal-lenging, and remarkable changes might have occurred.
In conclusion, strength training, proprioception training, and a combi-nation of the 2 failed to improve postural stability in subjects sufferingfrom PAL This study adds to an already conflicting body of literature re-garding optimal treatment protocols for this condition. It would be of ben-efit for future studies to investigate the effects of these protocols duringthe more acute stages of injury (once the subject has achieved full weight-bearing ability). It would also be of benefit to examine the effects of morestrenuous training protocols when the subjects are beyond the acute stage.
References
1. Ekstrand J, Gillquist J. Soccer injuries and their mechanisms: a prospectivestudy Med Sci Sports Exerc. 1983; 15:267-270.
2. Garrick JG, Requa RK. The epidemiology of foot and ankle injuries in sports.Clin Podiatr Med Surg. 1989;6:629-637.
3. Poweil JW, Barber-Foss KD. Injury patterns in selected high school sports: areview of the 1995-1997 seasons. / Athletic Train. 1999;34:277-284.
4. Sn\ith RW, ReischI SF. Treatinent of ankle sprains in young athletes. Am } SportsMcrf. 1986;14:465-471.

226 Powers et al
5. Stanitski CL. Common injuries in preadolescent and adolescent athletes. SportsMed. \9S9;7:32-4l.
6. Yeung MS, Chan K, So CH, et al. An epidemiological survey on ankle sprain.Br} Sports Med. 1994;28:112-n6.
7. Hertel J. Functional instability following lateral ankle sprain. Sports Med.2000;29:361-371.
8. Kannus P, Renstrom P. Current concepts review: treatment for acute tears ofthe lateral ligaments of the ankle. / Bone Joint Surg Am. 1991;73:305-312.
9. Barker HB, Beynnon BD, Renstrom AFH. Ankle injury risk factors in sports.Sports Med.'[997;23:b9-74.
10. PreemanMAR, Dean MRE,HanhamIWF. The etiology and prevention of func-tional instability of the foot. / Bone joint Surg Br. 1965;47:678-685.
11. Hubbard TJ, Kaminski TW. Kinesthesia is not affected by chronic ankle insta-bility status, / Athletic Train. 2002;37{4):481-486.
12. Hertel J. Functional anatomy, pathomechanics, and pathophysiology of lateralankle instability / Athletic Train. 2002;37(4):364-375.
13. Bosien WR, Staples OS, Russell SW. Residual disability following acute anklesprains. / Bone joint Surg Am. 1955;37:1237-1243.
14. Tropp H. Pronator weakness in functional instability of the ankle joint. Int }Sports Med. 1986;7:291-294.
15. Wilkerson GB, Pinerola JJ, Caturano RW. Invertor vs evertor peak torque andpower deficiencies associated with lateral ankle ligament injury. / Orthop SportsPhj/sT/jfr. 1997;26:78-86.
16. Uh BS, Beynnon BD, Helie BV, et al. The benefit of a single-leg strength train-ing program for the muscles around the untrained ankle. Am j Sports Med.2000;28:568-573.
17. Bernier JN, Perrin DH, Rijke A. Effect of unilateral functional instability of theankle on postural sway and inversion and eversion strength. / Athletic Train.1997;32:226-232.
18. Kaminski TW, Perrin DH, Gansneder BM. Eversion strength analysis ofuninjured and functionally unstable ankles. / Athletic Train. 1999;34:239-245.
19. Lentell GL, Katzman LL, Walters MR. The relationship between muscle func-tion and ankle stability / Orthop Sports Phys Ther. 1990;n:605-611.
20. Lephart S, Swanik CB, Fu F. Reestablishing neuromuseular control. In: PrenticeWE, ed. Rehahilitation Techniques In Sports Medicine. 3rd ed. St Louis, Mo: WCBMcGraw-Hill; 1999:88-106.
21. Mattacola CG, Dwyer MK. Rehabilitation of the ankle after acute sprain orchronic instability. / Athletic Train. 2002;37(4):413-429.
22. Gauffin H, Tropp H, Odenrick P. Effect of ankle disk training on postural con-trol in patients with functional instability of the ankle joint. Int} Sports Med.1988,9:141-144.
23. Pintsaar A, Brynhildsen J, Tropp H. Postural corrections after standardizedperturbations of single limb stance: effect of training and orthotic devices inpatients with ankle instability Br } Sports Med. 1996;30:151-155.
24. Tropp H, Odenrick P, Gillquist J. Stabilometry recordings in functionaland mechanical instability of the ankle joint. Int J Sports Med. 1985;6:180-182.
25. Isakov E, Mizrahi J. Is balance impaired by recurrent sprained ankle? Br j Sports. 1997;31:65-67.

Functional Ankle Instability 227
26. Lephart SM, Pincivero DM, Giroldo JL, et al. The role of proprioception in themanagement and rehabilitation of athletic injuries. Am } Sports Med. 1997;25:130-137.
27. Bernier JN, Perrin DH. Effect of coordination training on proprioception of thefunctionally unstable ankle. / Orthop Sports Phys Ther. 1998;27:264-275.
28. Matsusaka N, Yokoyama S, Tsunisaki T, et al. Effect of ankle disk training com-bined with tactile stimulation to the leg and foot on functional instability ofthe ankle. Am j Sports Med. 2001;29:25-30.
29. Rozzi SL, Lephart SM, Sterner R, Kuligowski L. Balance training for personswith functionally unstable ankles. / Orthop Sports Phys Ther. 1999;29:478-486.
30. Docherty CL, Moore JH, Arnold BL. Effects of strength training on strengthdevelopment and joint position sense in functionally unstable ankle. / AthleticTrain. 1998;33(4):310-314.
31. Blackbum T, Guskiewicz KM, Petschauer MA, et al. Balance and joint stabil-ity: the relative contributions of proprioception and muscular strength. / SportRehabiL 2000;9:315-328.
32. Vuillerme N, Danion F, Forestier N, Nougier V. Postural sway under musclevibration and muscle fatigue in humans. Neurosci Lett. 2002;333:131-135.
33. Yaggie JA, McGregor SJ. Effects of isokinetic ankle fatigue on the maintenanceof balance and postural limits. Arch Phys Med Rehabil. 2002;83:224-228.
34. Dimitrova NA, Dimitrov GV. Interpretation of EMG changes with fatigue: facts,pitfalls, and fallacies. / Electromyogr Kinesiol. 2003;13:13-36.
35. Tarata MT. Mechanomyography versus electromyography, in monitoring themuscular fatigue. Biomed Eng Online. 2003;2:3.
36. Gerdle B, Larsson B, Karlsson S. Criterion validation of surface EMG variablesas fatigue indicators using peak torque: a study of repetitive maximumisokinetic knee extensions. / Electromyogr Kinesiol. 2000;10:225-232.
37. Tomaszewski D. "T-Band Kicks" ankle proprioception program. / Athletic Train.1991 ;26(fall):216-217,219-227.
38. Tarantola J, Nardone A, Tacchini E, Schieppati M. Human stance stability im-proves with the repetition of the task: effect of foot position and visual condi-tion. Neurosci Lett. 1997;228:75-78.
39. Baker AG, Webright WG, Perrin DH. Effect of a "T-band" kick training proto-col on postural sway. / Sport Rehabil. 1998;7:122-127.
40. Cordova ML, Jutte LS, Hopkins JT. EMG comparison of selected ankle reha-bilitation exercises. / Sport Rehabil. 1999;8:209-218.
41. Patterson RM, Stegink Jansen CW, Hogan HA, et al. Material properties ofThera-Band tubing. Phys Ther. 2001;81:1437-1445.
42. Chong RKY, Ambrose A, Carzoli J, Hardison L, Jacobson B. Source of improve-ment in balance control after a training program for ankle proprioception. Per-cept Mot Skills. 2001;92:265-272.
43. Cox ED, Lephart SM, Irrgang JJ. Unilateral balance training of noninjured in-dividuals and the effects on postural sway. / Sport Rehabil. 1993;2:87-96.
44. Hess DM, Joyce CJ, Arnold BL, Gansneder BM. Effect of a 4-week agility-train-ing program on postural sway in the functionally unstable ankle. / Sport Rehabil.2001 ;10:24-35.
45. Hoffman M, Payne VG. The effects of proprioceptive ankle disk training onhealthy subjects. / Orthop Sports Phys Ther. 1995;21:90-93.
46. Sheth P, Yu B, Laskowski ER, et al. Ankle disk training influences reaction fimesof selected muscles in a simulated ankle sprain. Am } Sports Med. 1997;25:538-543.