Embed Size (px)
DESCRIPTION
SIR RFS Case Series: January 2015 (1 of 2)
Citation preview

AN UNCOMMON CAUSE OF ARTERIAL OCCLUSION
Resident(s): J. Allen Swanson Jr., M.D.
Attending(s): Dr. Haraldur Bjarnason, Dr. James Andrews
Program/Dept(s): Mayo Clinic, Rochester, MN
Originally Posted: January 01, 2015
CHIEF COMPLAINT & HPI
Chief Complaint Right hand pain, paresthesias, and discoloration for the past 1 week
History of Present Illness • 20-year old right-hand dominant female college volleyball player transferred from
outside hospital with increasing right hand pain, paresthesias, and discoloration for the past 1 week.
• Outside ultrasound is unavailable, but by report demonstrated echogenic material in the right radial artery.

RELEVANT HISTORY
Past Medical and Surgical History No relevant past medical or surgical history
Medications None
Allergies None
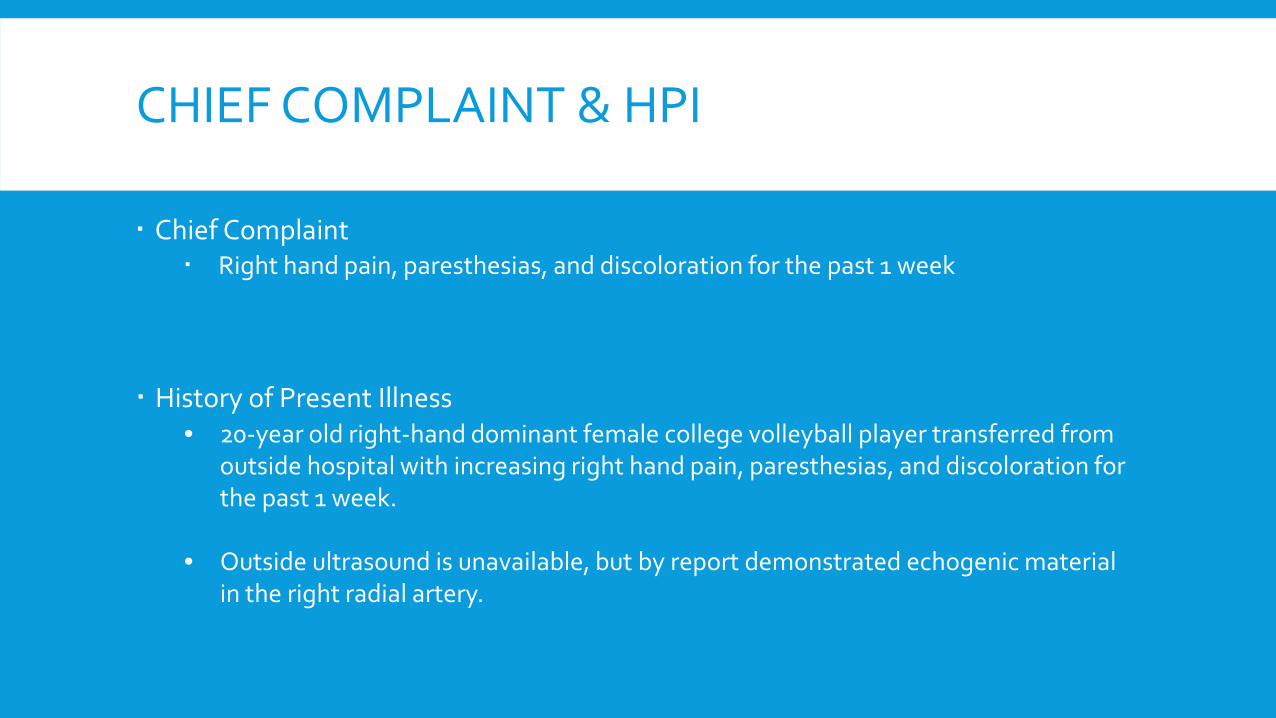
DIAGNOSTIC WORKUP
Non-Invasive Imaging CT angiography: Multifocal occlusion of the right ulnar artery with distal reconstitution
Long-segment occlusion of the mid-distal right radial artery
No evidence of thoracic outlet arterial compression or aneurysm (Images not shown)
Brachial A. Radial A.
Occluded Ulnar A. Reconstituted Ulnar A.
Occluded Radial A.
Reconstituted Ulnar A. Occluded
Radial A.

DIAGNOSTIC WORKUP
Non-Invasive Imaging Trans-esophageal echocardiogram: No intracardiac mass or thrombus No evidence of patent foramen ovale

DIAGNOSIS
Multifocal embolic disease involving the right upper extremity, without identifiable etiology.

INTERVENTION
Radial A.
UlnarA.
Common Interosseous A.
Right Upper Extremity Angiography: Abrupt occlusion of the mid-distal right
radial artery Multiple occlusions in the proximal and
mid right ulnar and common interosseous arteries Multiple occlusions of the right princeps
pollicis and digital arteries
Princeps Pollicis A.

INTERVENTION
Right and Left Upper Extremity Angiography: Normal, patent right subclavian and right axillary arteries. No evidence of thoracic outlet compression.
Abrupt occlusion of the right posterior humeral circumflex artery.
Normal left posterior circumflex artery.
Overall, findings likely represent right upper extremity embolic disease secondary to quadrilateral space syndrome.
L. Posterior Circumflex Humeral A.
Occluded R. Posterior Circumflex Humeral A.

QUESTION
Which letter corresponds to the quadrilateral (quadrangular) space? Click on one of the following answers.
A. A
B. B
C. C
D. D
A
B C D

CORRECT!
Which letter corresponds to the quadrilateral (quadrangular) space? Click on one of the following answers.
A. A
B. B. The quadrilateral space is bordered by the long head of the triceps, teres minor and teres major muscles, and the humerus. This space contains the axillary nerve and posterior circumflex humeral artery.
C. C
D. D
A
B C D
CONTINUE WITH CASE

SORRY, THAT’S INCORRECT.
Which letter corresponds to the quadrilateral (quadrangular) space? Click on one of the following answers.
A. A
B. B. The quadrilateral space is bordered by the long head of the triceps, teres minor and teres major muscles, and the humerus. This space contains the axillary nerve and posterior circumflex humeral artery.
C. C
D. D
A
B C D
CONTINUE WITH CASE
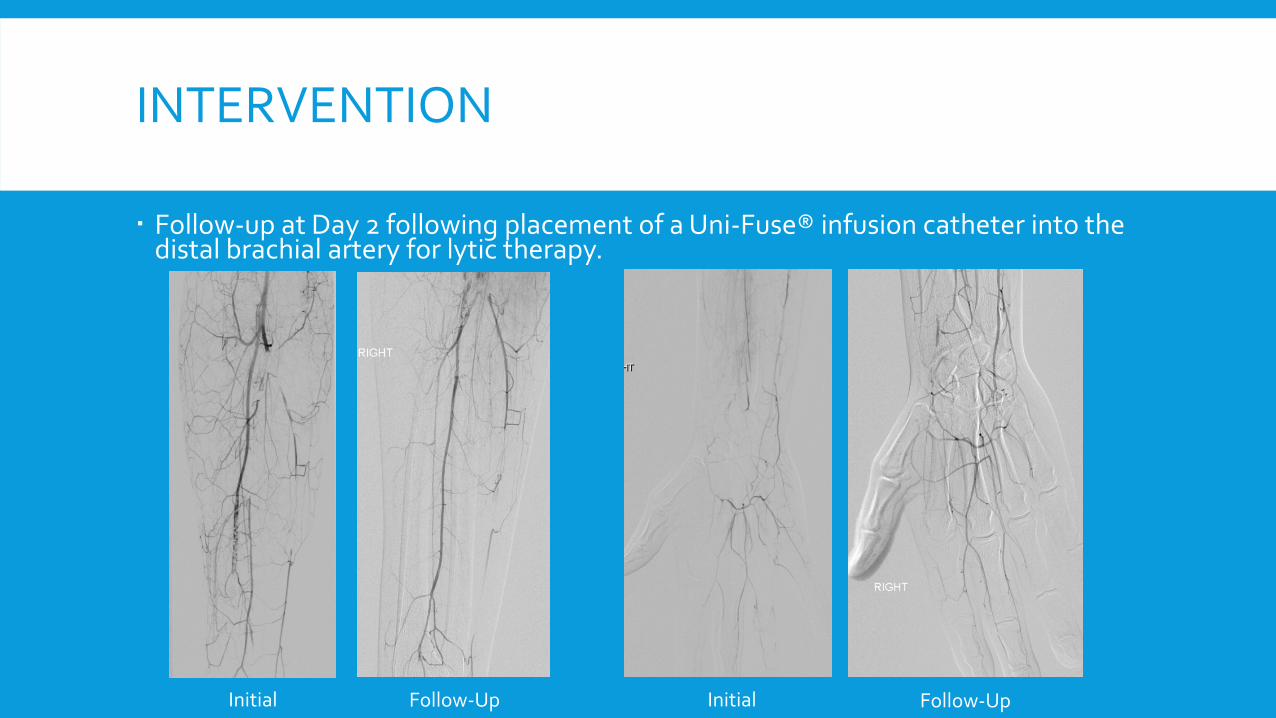
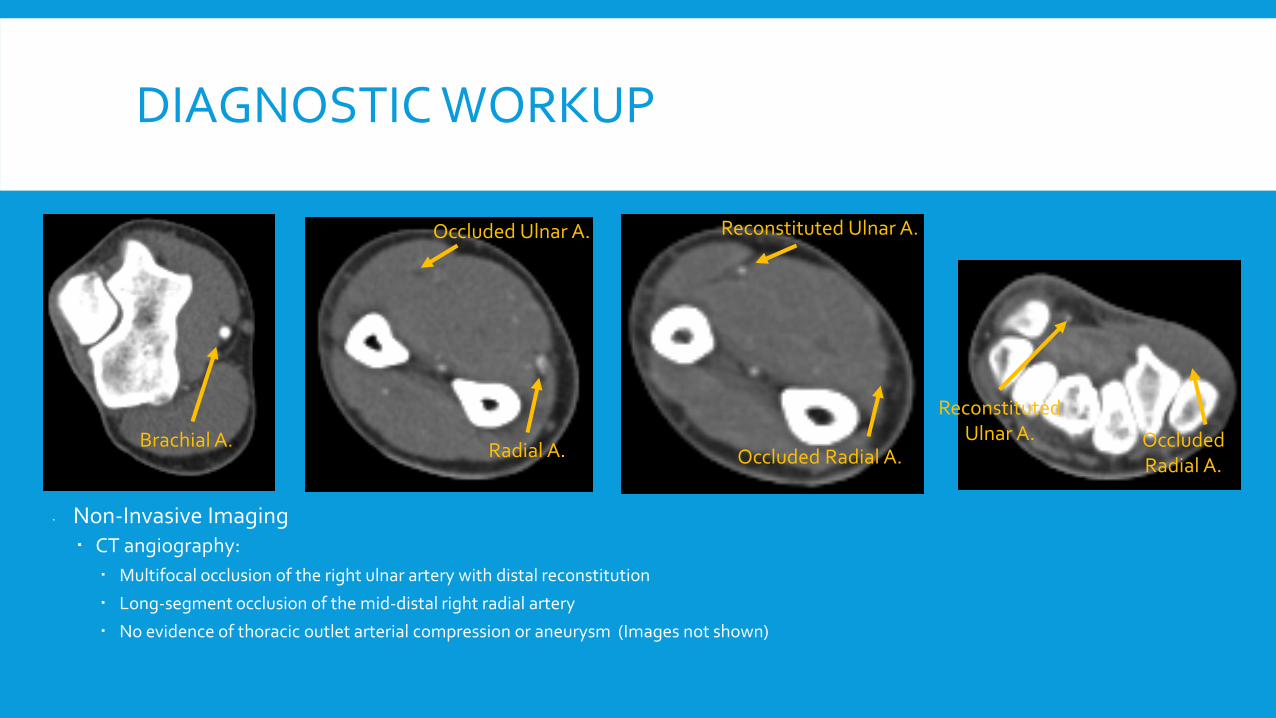
INTERVENTION
Follow-up at Day 2 following placement of a Uni-Fuse® infusion catheter into the distal brachial artery for lytic therapy.
Initial Follow-Up Follow-Up Initial

SUMMARY & TEACHING POINTS
Final diagnosis: Quadrilateral space syndrome resulting in thrombus formation in the posterior circumflex humeral artery, which is “squeezed” retrograde into the brachial artery, leading to embolic disease to the right upper extremity . While uncommon, it is an important potential source for embolic disease.
Sources of arterial emboli: Cardiac: Arrhythmias, endocarditis, valvular disease, paradoxical embolism Arterial: Aneurysm, atherosclerosis Thrombosis: Grafts, hypercoagulability, atherosclerosis, entrapment Trauma
Patient’s Outcome: Moderate improvement of clot burden in the right radial, ulnar, and interosseous arteries following intra-arterial lytic infusion. Patient subsequently underwent ligation of the right posterior circumflex humeral artery with thrombectomies of the involved arteries.

QUESTION
Which of the following upper extremity maneuvers exacerbate shoulder pain associated with quadrilateral space syndrome? Click on one of the following answers.
A. Abduction and internal rotation
B. Adduction and internal rotation
C. Abduction and external rotation
D. Adduction and external rotation

CORRECT!
Which of the following upper extremity maneuvers exacerbate shoulder pain associated with quadrilateral space syndrome? Click on one of the following answers.
A. Abduction and internal rotation
B. Adduction and internal rotation
C. Abduction and external rotation
D. Adduction and external rotation
CONTINUE WITH CASE
SORRY, THAT’S INCORRECT.
Which of the following upper extremity maneuvers exacerbate shoulder pain associated with quadrilateral space syndrome? Click on one of the following answers.
A. Abduction and internal rotation
B. Adduction and internal rotation
C. Abduction and external rotation
D. Adduction and external rotation
CONTINUE WITH CASE

SUMMARY & TEACHING POINTS
Anatomy: The quadrilateral space is formed by teres minor, teres major, long head of the triceps, and humerus. The axillary nerve and posterior circumflex humeral artery pass through this space.
Pathophysiology: Any source of compression of the contents within the quadrilateral space. Etiologies include muscle hypertrophy, osseous lesions, ganglia, and fibrous bands. Compression may be static or dynamic (may be present/increased with abduction and external rotation of the upper extremity).
Symptoms: Classic presentation is shoulder pain, which is worse with abduction and external rotation of the upper extremity.

SUMMARY & TEACHING POINTS
Best methods for diagnosis of quadrilateral space syndrome are: Angiography, MRA, CTA Performing exam with the arm in abduction/external rotation may improve
sensitivity, though this is debatable
Treatment options: Conservative management initially, especially if secondary to muscle
hypertrophy Surgical decompression for space occupying lesions Ligation of the posterior circumflex humeral artery to prevent further emboli

REFERENCES
1. Van de Pol D, Kuijer PP, Langenhorst T, Maas M. High Prevalence of Self-Reported Symptoms of Digital Ischemia in Elite Male Volleyball Players in the Netherlands: A Cross-Sectional National Survey. Am J Sports Med. 2012;40:2296. doi:10.1177/0363546512456973.
2. Zurkiya, O, Walker TG. Quadrilateral Space Syndrome. J Vasc Interv Radiol. 2014;25(2):229. doi:10.1016/j.jvir.2013.10.016.