-
TRISOMY 21- DOWN SYNDROME
-
IncidenceApproximately one in 1000 live births.
-
GeneticsTrisomy 21 (47, +21), - 94 %, The frequency of trisomy
increases with increasing maternal age.Robertsonian translocation
involving chromosome 21- Approx. 3-4 %, not related to maternal
age.Trisomy 21 mosaicism 2 to 3 % cases
-
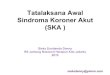
Clinical FeaturesHead and neckBrachycephalyUp-slanting palpebral
fissuresEpicanthal foldsBrushfield spotsFlat nasal bridgeFolded or
dysplastic earsOpen mouthProtruding tongueShort neck Excessive skin
at the nape of neckExtremitiesShort broad handsShort fifth
fingerIncurved fifth fingerTransverse palmer creaseSpace between
first and second toeHyper flexibility of joints
-
Neonatal featuresFlat facial profilePoor Moro reflexExcessive
skin at the nape of neckSlanted palpebral fissuresHypotonia Hyper
flexibility of jointsDysplasia of pelvisAnomalous earsDysplasia of
midphalanx of fifth fingerTransverse palmer crease
-
Mental RetardationAlmost all DS babies have MR.Mildly to
moderately retarded .Starts in the first year of life.Average age
of sitting(11 mon), and walking (26 mon) is twice the typical
age.First words at 18 months.IQ declines through the first 10 years
of age, reaching a plateau in adolescence that continues into
adulthood.
-
Heart Disease50 % of Down Syndrome pts have heart
diseaseAtrioventricular septal defectVSDSecundum ASDPDATetrology of
FallotMitral valve prolapseAR, MR
-
GI abnormalities5% of casesDuodenal atresia or stenosis,
sometimes assoc with annular pancreas in 2.5 % of casesImperforate
anusEsophageal atresia with TE fistula is less commonHirschsprungs
diseaseStrong assoc with celiac disease b/w 5 16 % , 5 16 fold
increase as compared to general population
-
GrowthBW, length and HC are less in DS Reduced growth
ratePrevalence of obesity is greater in DSWeight is less than
expected for length in infants with DS, and then increases
disproportion ally so that they are obese by age 3-4 yrs
-
Eye problems Most common disorders are Refractory error 35 to 76
percent Strabismus 25 to 57 percent Nystagmus 18 to 22 percent
Cataract occur in 5 % of newborns. Frequency increases with
age.
-
Hearing lossUnilateral or bilateralConductive, sensorineural or
mixedOtitis media is a frequent problem
-
Hematologic disordersThe risk of leukemia is 1 to 1.5
percent.65% of newborn have polycythemia resulting in
hypoglycemia.Risk of AML and ALL is also much higher than the
general population.Transient leukemia exclusively affects NB. - It
is asymptomatic with spontaneous resolution in 2-3 months. -
Vesiculopustular skin eruptions are common and resolve with
disorder.
-
Endocrine disorderThyroid disease Hypothyroidism occurs more
frequently than hyperthyroidism.Diabetes The risk of type 1
diabetes is three times greater than that of the general
population.
-
ReproductionWomen with DS are fertile and may become
pregnant.Nearly all males with DS are infertile. The mechanism is
impairment of spermatogenesis
-
Atlantoaxial instabilityExcessive mobility of atlas (C1) and the
axis (C2), may lead to subluxation of the cervical spine. Diagnosis
made by lateral neck radiograph.Patients are advised to avoid
contact sports.
-
Sleep apneaObstructive sleep apnea is more common.
-
Skin disorderPalmoplantar hyperkeratosisSeborreic
dermatitisFissured tongueCutis marmorataGeographical
tongueXerosis
-
DiagnosisPrenatal screeningIf no screening It is recognized from
the characteristic phenotypic features.Confirmed by Karyotype.
-
Management1. Growth Measurements should be plotted on the
appropriate growth chart for children with DS.This will help in
prevention of obesity and early diagnosis of celiac disease and
hypothyroidism.
2. Cardiac disease All newborns should be evaluated by cardiac
ECHO for CHD in consultation with pediatric cardiologist.
3. Hearing Screening to be done in the newborn period, every 6
months until 3 yrs of age and then annually.
-
Management (cont.)4. Eye disorders - An eye exam should be
performed in the newborn period or at least before 6 months of age
to detect strabismus, nystagmus, and cataracts.
5. Thyroid Function Should be done in newborn period and should
be repeated at six and 12 months , and then annually.
6. Celiac Disease Screening should begin at 2 yrs. Repeat
screening if signs/Sx develop.
-
Management ( cont)Hematology CBC with differential at birth to
evaluate for polycythemia as well as WBC.
Atlanto-axial instability X ray for evidence of AAI or
sub-luxation at 3 to 5 years of age.
Alzheimers disease Adult with a Down Syndrome has earlier onset
of symptoms. When diagnosis is considered, thyroid disease and
possible depression should be excluded.
-
MortalityMedian age of death has increased from 25 yrs in 1983
to 49 yrs in 1997, an average of 1.7 yrs increase per year.
Most likely cause of death is CHD, Dementia, Hypothyroidism and
Leukemia.
Improved survival is because of increased placements of infants
in homes andchanges in treatment for common causes of death.
Survival is better for males and blacks.
-
CounselingMay begin when a prenatal diagnosis is made.Discuss
the wide range of variability in manifestation and
prognosis.Medical and educational treatments and interventions
should be discussed.Initial referrals for early intervention,
informative publications, parent groups, and advocacy groups.