Embed Size (px)
Citation preview

Simultaneous hearing problems: health conditions in tinnitus, sound sensitivity and both diagnoses
Josefin Nordin
VT 2014 Examensarbete, 30 hp Handledare: Steven Nordin och Eva Palmquist

2
SIMULTANEOUS HEARING PROBLEMS: HEALTH CONDITIONS IN TINNITUS, SOUND SENSITIVITY AND BOTH DIAGNOSES
Josefin Nordin
Little research has been conducted on simultaneous hearing problems. The aim of this study was to investigate health conditions (stress, sleep quality, depression, anxiety, and burnout) in individuals with 1) tinnitus, 2) sound sensitivity, and 3) both tinnitus and sound sensitivity, compared to a reference group without these diagnoses. Data from a Swedish population-based sample, stratified for age and gender, was collected through a mail survey. The participation rate was 40 %, and 3406 individuals participated. The results showed that the sample with sound sensitivity was in poorest health condition, raising the notion of different underlying mechanisms of the sound sensitivity in the samples with sound sensitivity versus double diagnoses. More research is needed to further explore the effects of living with simultaneous hearing problems, and subgroups within the phenomena of sensitivity to sound. Lite forskning har hittills undersökt simultana hörselproblem. Syftet med denna studie var att undersöka hälsotillstånd (stress, sömnkvalitet, depression, ångest och utbrändhet) hos individer med 1) tinnitus, 2) ljudkänslighet, och 3) tinnitus och ljudkänslighet, jämfört med en referensgrupp utan dessa diagnoser. Data från en svensk populationsbaserad grupp, stratifierat för ålder och kön, samlades in via en brevenkät. Deltagandet var 40 % och 3406 individer deltog. Resultatet visade att gruppen med ljudkänslighet var i sämst hälsotillstånd, vilket väcker funderingar om olika underliggande mekanismer för ljudkänsligheten i grupperna med ljudkänslighet jämfört med dubbeldiagnos. Mer forskning behövs för att vidare utforska följderna av att leva med simultana hörselproblem, och subgrupper inom fenomenet för ljudkänslighet.
Hearing problems are a-common complaints in the general population, and it is not unusual for individuals to suffer from more than one form of symptom (Canlon, Theorell, & Hasson, 2013). Reported by between 10 - 15 % of the population, tinnitus is the perceived sensation of sound in the absence of a corresponding external acoustic stimulus (Langguth, Kreuzer, Kleinjung, & De Ridder, 2013). The perceived phantom sound is usually of an unformed acoustic nature such as a ringing, hissing or buzzing (Henry, Dennis, & Schechter, 2005). Tinnitus displays as a heterogeneous condition with varying characteristics, etiology and accompanying symptoms. Tinnitus can be unilateral, bilateral or described as emerging from within the head. The condition is often divided into subjective and objective tinnitus. While subjective tinnitus only can be heard by the individual, objective tinnitus or somatosound, consisting of sound generated within the individual’s body, can be heard also by an examiner (Holmes & Padgham, 2009). Tinnitus can be intermittent or pulsatile in character, as well as temporary or chronic. The etiology of tinnitus is in many cases multifactorial, and the factors leading to tinnitus onset might differ from those related to its persistence (Ortmann, Muller, Schlee, & Weisz, 2011). Tinnitus can arise from pathological changes along the entire auditory pathway. The most common causes for developing tinnitus are initial cochlear lesions (e.g. sudden hearing loss, noise trauma or presbyacusis), which can result in an abnormal neuronal activity in central auditory pathways finally perceived as phantom sound (Langguth et al., 2013). Imaging data provide evidence for a widespread and dynamically changing tinnitus brain network involving both

3
auditory and non-auditory structures (e.g. cortical regions involved in perceptual, emotional, memory, attentional and salience functions; De Ridder, Elgoyhen, Romo, & Langguth, 2011; Langguth, Landgrebe, Kleinjung, Sand, & Hajak, 2011; Lanting, De Kleine, & Van Dijk, 2009). Abnormal changes to the auditory nerve (Langguth et al., 2013), stress (Hébert & Lupien, 2007), emotional factors (Canlon et al., 2013), and temporomandular joint disorder and neck injuries (Levine, 1999) are common factors associated with tinnitus onset. Objective tinnitus is often generated by vascular, muscular or respiratory abnormalities (Henry et al., 2005). In 1 - 2 % of the population tinnitus and accompanying symptoms cause a lowered quality of life, needing clinical treatment (Langguth et al., 2013). Many patients with tinnitus report symptoms such as frustration, annoyance, irritability, concentration difficulties and anxiety (Langguth, 2011). A Swedish longitudinal study (Hébert, Canlon, Hasson, Magnusson Hanson, et al., 2012) recently showed a direct and long-term association between depression and tinnitus severity, the extent to which the individual is bothered, upset, or worried by the condition. Furthermore, tinnitus severity seems to be exacerbated by stress and fatigue (Hébert, Canlon, & Hasson, 2012). In line with these results, tinnitus is associated with emotional exhaustion (Canlon et al., 2013), and insomnia (e.g. poor perceived quality of sleep or difficulty initiating and/or maintaining sleep; Izuhara et al., 2013; Lasisi & Gureje, 2011). Tinnitus may accompany almost any other form of hearing problems, and very often does (Andersson, Strömgren, Ström, & Lyttkens, 2002). Being the most common cause for developing the condition, many studies show a strong association between hearing loss and tinnitus prevalence (Canlon et al., 2013). However, discomfort loudness levels i.e., the level which a sound is judged as being too loud, has been found to be a stronger predictor than hearing loss of both tinnitus prevalence and severity (Hébert et al., 2012). An overlap of 40 % has been found between tinnitus and hyperacusis, defined as an exaggerated or inappropriate reaction to sound in levels that are not uncomfortably loud to the average person (Baguley, 2003). A recent study further showed an increased sensitivity to loud sounds in individuals with tinnitus compared with normal hearing individuals matched for hearing loss (Hébert, Fournier, & Noreña, 2013). Phonophobia, defined as an abnormal and unwarranted fear of specific sounds, is also associated with tinnitus (Langguth et al., 2013). These findings support an intimate relationship between tinnitus and different forms of sound sensitivity. While not closely defining the term, Andersson, Strömgren, Ström, and Lyttkens (2002) reported a 60 % overlap between tinnitus and sound sensitivity. Hyperacusis and phonophobia play their different parts in the more general sound phenomena of sensitivity to sound. Asha’ari, Zain, and Razali (2010) have discussed the differences between hyperacusis and phonophobia, while agreeing that most people with sensitivity to sound usually have both types of hearing problems in varying proportions. Sound sensitivity has been defined as an internal state that increases the individual’s degree of reactivity to noise in general (Job, 1999). With a prevalence of between 8 - 9 % in the general Swedish population (Andersson, Lindvall, Hursti, & Carlbring, 2002) sound sensitivity is a common public health

4
problem. Without closely defining the term, a population-based study in Poland additionally reported a 15 % prevalence of hyperacusis (Skarzynski, Rogowski, Bartnik, & Fabijanska, 2000). Sound sensitivity can be both central (e.g. William’s syndrome) and peripheral (e.g. Bell’s palsy) in origin, caused by sensory mechanisms resulting in elevated perceived sound intensity (Katzenell & Segal, 2001). It can also be caused by cognitive mechanisms, related to how sounds are perceived by the individual (e.g. involving abnormally strong reactions of the limbic and autonomic systems; Nordin, Körning Ljungberg, Claeson, & Neely, 2013). Higher sound sensitivity has previously been associated with higher levels of perceived stress (Nordin, Körning Ljungberg et al., 2013), anxiety (Baguley, 2003), depression (Marriage & Barnes, 1995), and other forms of environmental intolerances (e.g. sensitivity to certain buildings, chemicals and electromagnetic fields; Palmquist, Claeson, Neely, Stenberg, & Nordin, 2014). In summary, tinnitus and sound sensitivity are common and intimately connected hearing problems affecting the individual’s health condition and causing much suffering in the general population. To this date little research has been conducted on more than one facet of hearing problems at the time (Canlon et al., 2013). To increase current knowledge about simultaneous hearing problems the aim of this study was to investigate health conditions, with respect to stress, sleep quality, depression, anxiety, and burnout, in individuals with 1) tinnitus, 2) sound sensitivity, and 3) both tinnitus and sound sensitivity, compared to a reference group without these diagnoses.
Method Study population and sample The present study used data from the Västerbotten Environmental Health Study (VEHS), a questionnaire-based survey regarding various forms of environmental hypersensitivity in Sweden. The study population was recruited from the county of Västerbotten, which has an age and gender distribution very similar to that of Sweden in general (Palmquist et al., 2014). A random sample of 8600 adults aged 18 to 79 years were selected from the population registry and invited to participate. The sample was stratified for age and gender. Of the selected individuals 8520 could be reached, among whom 3406 (40 %) chose to participate. Age and gender distributions for the responders are given in Table 1. In the questionnaire participants were asked to self-report if they had ever been diagnosed by a physician with tinnitus or sound sensitivity. Two-hundred fifty six individuals reported a tinnitus diagnosis. To ensure that individuals with sound sensitivity had a present problem, a control question for inclusion was used together with the diagnosis: do you have a hard time tolerating every day sounds in your surrounding that most other people can tolerate. Excluding those who answered no on the control question, 66 individuals qualified as having sound sensitivity.

5
Twenty-nine individuals reported having been diagnosed with both conditions and answered positively on the question regarding presently having sound intolerance. These individuals were included in both the tinnitus group, and the sound sensitivity group, as well as making up the third sample with double diagnoses. The reference group consisted of 3113 participants reporting having neither tinnitus nor sound sensitivity diagnoses. Table 1. Number of responders (and response percentages) across age and gender strata.
Material To measure participant’s sensitivity to sound the 11-item Noise Sensitivity Scale (NSS-11; Nordin, Palmquist, & Claeson, 2013) was used. Formed from the 21-item Noise Sensitivity Scale (NSS; Weinstein, 1978), NSS-11 is a brief questionnaire instrument for quantifying affective reactions to and behavioural disruptions attributed to sounds, avoiding general inquiries about noise as an environmental problem. The scale ranges from 0 to 54 (high score representing high level of sensitivity to sound). NSS shows good test-retest reliability, internal consistency (Kuder-Richardson reliability 0.83) and concurrent validity (Nordin, Millqvist, Löwhagen, & Bende, 2003; Weinstein, 1978). Evaluation of NSS-11 further demonstrates satisfying internal consistency (Chronbach α ranging from 0.71 to 0.85) and concurrent validity (Nordin, Palmquist, & Claeson, 2013). The 10-item Perceived Stress Scale (PSS-10; Cohen & Williamson, 1988) was used to measure participants’ perception of stress, emphasizing the appraisal of stressful life situation. The original 14-item version of PSS was translated into Swedish by Eskin and Parr (1996). The scale ranges from 0 to 40 (high score representing high level of stress). The Swedish version of PSS-10 shows good internal consistency (Chronbach α 0.84), construct validity and generates approximately normally distributed data (Nordin & Nordin, 2013). To measure sleep quality the Karolinska Sleep Questionnaire (KSQ; Kecklund & Åkerstedt, 1992) was used. KSQ consists of 18 items answered on a 6-point scale ranging from 0 (Never) to 5 (Always), and measures four dimensions of subjective sleep and sleepiness (sleep quality, non-restorative sleep, sleepiness, and sleep apnea), of which sleep quality was used in the present study. The scale ranges from 0 to 5 (low score representing low sleep quality). KSQ exhibits good internal
Age
Women
Men
18-29 307 (32.7) 179 (17.7) 30-39 266 (40.9) 177 (25.2) 40-49 288 (40.7) 230 (31.3) 50-59 367 (51.0) 295 (39.7) 60-69 405 (58.6) 356 (50.7) 70-79 265 (53.8) 271 (63.9) 18-79 1898 (45.2) 1508 (34.9)

6
consistency (Chronbach α ranging from 0.71 to 0.87 for the different sleep dimensions) and construct validity (Nordin, Åkerstedt, & Nordin, 2013). The Swedish version of the Hospital Anxiety and Depression Scale (HADS; Sullivan et al., 1993) was used to measure symptoms of anxiety and depression. HADS was originally constructed by Zigmont and Snait (1983), consisting of two scales with seven items for measuring anxiety (HADS-A), and seven for depression (HADS-D). Each scale ranges from 0 to 21 (high score representing high anxiety and depression). HADS displays good internal consistency (Chronbach α ranging from 0.67 to 0.93 for each scale), as well as discriminant and concurrent validity (Bjelland, Dahl, Haug, & Neckelmann, 2002). Degree of burnout was measured with a Swedish translation of the Shirom Melamed Burnout Questionnaire (SMBQ; Grossi, Perski, Evengård, Blomkvist, & Orth-Gomér, 2003; Melamed, Kushnir, & Shirom, 1992). SMBQ consists of 22 items measuring both mental and physical exhaustion in life. The mean value of all items form a global scale ranging from 1 to 7 in score (high score indicating more exhaustion). SMBQ demonstrates good internal consistency (Chronbach α 0.78) and construct validity (Grossi et al., 2003). Procedure VEHS was approved by the Umeå Regional Ethics Board (Dnr 09-171M), and conducted between March and April 2010. The study addressed diagnoses, symptomatology, annoyance, environmental intolerance, physiological and psychological health, coping, and social support (Palmquist et al., 2014). The questionnaire was sent by mail together with written information regarding the purpose of the study, estimated time to complete the survey, confidentiality, and that participation was voluntary. Non-responders was sent a reminder after three weeks. An additional reminder and a new copy of the questionnaire were sent after another three weeks. Statistical analysis Descriptive statistics were computed using independent t-tests for continuous variables and chi2-tests for categorical variables. Independent t-tests were used to compare the level of stress, sleep quality, depression, anxiety, and burnout between each of the three samples and the reference group respectively. Due to multiple analyses, a relatively strict criterion for statistical significance was applied ( = 0.01). Participants’ test scores were transformed into z-scores. The difference in mean z-scores between the three samples and the reference group was used as a measure of effect size. SPSS Statistics 21 (IBM Corporation, New York) was used for the statistical analysis. Missing values were estimated with multiple imputation using fully conditional Markov Chain Monte Carlo methods (Liang, Liu & Carroll, 2010), with 10 maximum iterations by means of which five imputed datasets were created and analysed, and their estimated values averaged. The percentages of missing data were between 5.10 – 5.19 % for PSS-10, between 3.86 – 3.93 % for Sleep quality index, between

7
2.97 – 3.11 % for HADS, and between 11.36 – 11.52 % for SMBQ global index. The use of imputed data in SPSS may generate very large degrees of freedom for t-tests. The reason for this is that SPSS uses an approximation that is based on the assumption that the complete-data statistic, if no data were missing, is a z-test rather than a t-test. Table 2. Characteristics of samples with tinnitus, sound sensitivity, and double
diagnoses, and the reference group.
1Self-report of having been given a diagnosis by a physician
Tinnitus
Sound sensitivity
Double diagnoses
Reference group
N 256 66 29 3113 Age, m (sd) 59.98 (14.0) 57.83 (11.4) 58.38 (10.8) 50.43 (16.9) Women, n (%) 96 (37.5) 44 (66.7) 14 (48.3) 1772 (57.0) Level of education, n (%) Compulsory school Senior high school College/university Missing
100 (39.1) 81 (31.6) 73 (28.5) 2 (0.8)
19 (28.8) 19 (28.8) 28 (42.4) 0
7 (24.1) 10 (34.5) 12 (41.4) 0
711 (22.8) 1047 (33.6) 1316 (42.3) 39 (1.3)
General health status, n (%) Excellent/very good Good Somewhat good/poor Missing
56 (21.9) 91 (35.5) 106 (41.5) 3 (1.2)
11 (16.7) 22 (33.3) 32 (48.5) 1 (1.5)
5 (17.2) 9 (31.0) 15 (51.7) 0
1287 (41.3) 1048 (33.7) 745 (23.9) 33 (1.1)
NSS, m (sd) 30.4 (8.57) 40.2 (6.89) 40.6 (7.59) 26.8 (7.75) Other diagnosis1, n (%) Hearing impairment Head trauma Bells pares Migraine Depression GAD ADHD Panic disorder PTSD Burnout syndrome Chronic fatigue syndrome Fibromyalgia Irritable Bowel Syndrome (IBS)
164 (64.1) 2 (0.8) 1 (0.4) 19 (7.4) 19 (7.4) 7 (2.7) 3 (1.2) 8 (3.1) 6 (2.3) 21 (8.2) 9 (3.5) 14 (5.5) 9 (3.5)
39 (59.1) 2 (3.0) 0 8 (12.1) 15 (22.7) 7 (10.6) 2 (3.0) 2 (3.0) 8 (12.1) 12 (18.2) 7 (10.6) 7 (10.6) 6 (9.1)
23 (79.3) 0 0 5 (17.2) 4 (13.8) 1 (3.4) 2 (6.9) 1 (3.4) 3 (10.3) 5 (17.2) 4 (13.8) 2 (6.9) 3 (10.3)
327 (10.5) 18 (0.6) 12 (0.4) 129 (4.1) 140 (4.5) 19 (0.6) 14 (0.4) 41 (1.3) 16 (0.5) 116 (3.7) 11 (0.4) 56 (1.8) 68 (2.2)

8
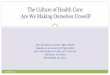
Results Sample characteristics Descriptive statistics for the three samples and reference group are presented in Table 2. There was a significant difference in age between each of the samples with tinnitus, t(319.31) = 10.31, p < .001, sound sensitivity, t(71.14) = 5.14 , p < .001, and double diagnoses, t(29.28)= 3.90, p < .001, compared to the reference group. Significant differences in gender, X2(1) = 36.12, p < .001, and level of education, X2(2) = 36.85, p < .001, were found between the tinnitus sample and the reference group. Health status Means, standard deviations and p-values for participants’ scores on the measures of stress, sleep quality, depression, anxiety, and burnout are reported in Table 3. There were significant differences between the sample with sound sensitivity and the reference group, concerning levels of stress, t(12239.45) = 2.60, sleep quality, t(91642.48) = 6.79, depression, t(98670.51) = 3.02, and burnout, t(734368.12) = 4.43. A significant difference in sleep quality was also found for the tinnitus sample, t(1248747.26) = 4.55, and the double diagnoses sample, t(175270.38) = 3.94, when compared to the reference group. The rest of the results did not reach significance, t < 2.48. Differences in mean z-scores, between each of the three samples compared to the reference group, are presented in Figure 1. Table 3. Means ± standard deviations and p-values from independent t-tests between
samples with tinnitus, sound sensitivity, and double diagnoses respectively compared
to the reference group.
Tinnitus
Sound sensitivity
Double diagnoses
Reference group
Stress
13.97±6.29 p=0.902
16.48±7.87 p=0.009
15.12±7.98 p=0.325
13.92±6.31
Sleep quality 1.88±1.14 p<0.001
2.57±0.15 p<0.001
2.54±1.35 p<0.001
1.55±0.99
Depression 3.28±2.90 p=0.391
4.67±4.17 p=0.003
3.83±3.80 p=0.212
3.10±3.09
Anxiety 4.34±3.51 p=0.552
5.98±4.88 p=0.013
5.03±4.79 p=0.438
4.49±3.73
Burnout 3.03±1.09 p=0.069
3.67±1.41 p<0.001
3.31±1.28 p=0.051
2.89±1.14

9
Health condition
Stress Sleep quality Depression Anxiety Burnout
Z-s
core
diff
eren
ce
0,0
0,2
0,4
0,6
0,8
1,0
Tinnitus
Sound sensitivity
Double diagnoses
Figure 1. Mean differences on health conditions turned into z-scores for samples with tinnitus, sound sensitivity, and double diagnoses respectively compared to the reference group.
Discussion
The aim of this study was to investigate health conditions, with respect to stress, sleep quality, depression, anxiety, and burnout, in individuals with 1) tinnitus, 2) sound sensitivity, and 3) both tinnitus and sound sensitivity, compared to a reference group without these diagnoses. The results show that the sample with sound sensitivity is in poorest health condition when compared to the reference group. The sample with sound sensitivity as a whole, reported significantly lower sleep quality, and higher levels of perceived stress, depression, and burnout. These results are in agreement with previous findings, associating sound sensitivity with higher levels of stress and depression (Marriage & Barnes, 1995; Nordin, Körning Ljungberg et al., 2013). Results are strengthened by participants’ lower rating of their general health status, and high rate of self-reported diagnoses of depression, GAD, PTSD, and burnout syndrome (see Table 2). Nevertheless, high occurrence of other medically unexplained syndromes, like migraine, chronic fatigue syndrome, fibromyalgia, and irritable bowel syndrome, may also have contributed to the sample’s poorer health condition. Contrary to previous findings (Baguley, 2003), there was no significant difference in anxiety between the sound sensitivity sample and the reference group when applying a strict criterion for the -level. However, the result suggest a strong tendency of higher level of anxiety in the sound sensitivity sample (p = 0.013). In line with previous findings (Izuhara et al., 2013; Lasisi & Gureje, 2011), the sample with tinnitus, and the sample with double diagnoses, reported significantly lower sleep quality in comparison with the reference group. No further differences

10
in health conditions between the two samples and the reference group were found. This supports Langguth et al.’s (2013) conclusion that most individuals with tinnitus cope quite sufficiently with their condition. Lower depression scores, as seen in both samples, have further been associated with low tinnitus severity (Hébert, Canlon, Hasson, Magnusson Hanson et al., 2012). However, due to participants being asked, in the VEHS questionnaire, if they have ever been diagnosed with tinnitus by a physician it is not certain that all individuals reporting a tinnitus diagnosis had a current hearing problem at the time of investigation. Hearing impairment was very common among the individuals in the three samples. The percentage of participants reporting being hearing impaired ranged from 59.1 % to 79.3 % for the three samples, compared to 10.5 % in the reference group. Hearing impairment may lead to individuals experiencing loudness recruitment, often consisting of a rapid growth of perceived loudness for those sounds located in the pitch region of a hearing loss (Marozeau & Florentine, 2007). Based on the current data it is not possible to dismiss loudness recruitment as a contributing underlying mechanism impersonating as sound sensitivity. However, recent findings have shown that tinnitus ears display significantly less loudness recruitment than non-tinnitus ears matched for hearing loss (Hébert, Fournier, & Noreña, 2013). Looking at Figure 1 there is an order in the results for the three samples that is visible to the naked eye. The sound sensitivity sample consequently showed the greatest mean differences in z-scores when compared to the reference group, followed by the double diagnoses sample, and last the tinnitus sample. Differences in z-score on all health conditions indicate medium to large effect sizes (ca 0.4 – 0.7) for the sound sensitivity sample, medium effect sizes (ca 0.2 – 0.4) for the double diagnoses sample, and small effect sizes (ca 0 – 0.1) for the tinnitus sample. For all three samples the effects were largest for sleep quality and burnout, indicating strongest associations between these health conditions and the three samples with hearing problems. Being a cross sectional study it is only possible to speculate about the overall directions between the variables. However, directions between different health conditions and hearing problems go both ways. Moreover, while stress, sleep quality, depression, anxiety, and burnout, are intimately associated with one another (Grossi et al., 2003), high scores on one health condition may contribute to an overall poorer wellbeing. Considering that the sound sensitivity sample, and the double diagnoses sample, seem to be fairly equal in their degree of sound sensitivity, looking at their similar mean scores on the NSS-11, it is an interesting result that the sound sensitivity sample differed from the reference group on three additional health conditions. The result may partly depend on the smaller sample size of the double diagnoses sample, limiting the statistical power. Nevertheless, it further indicates different underlying mechanisms of the sound sensitivity in individuals who have sound sensitivity, compared to those with both tinnitus and sound sensitivity. Higher levels of stress, depression, and burnout in the sample with sound sensitivity may be explained by their sound sensitivity being of a more cognitive origin, involving the limbic and

11
autonomic systems, as described by Nordin, Körning Ljungberg, et al. (2013). The sound sensitivity of the double diagnoses sample, displaying less affective symptoms, may in turn, to a greater extent, be caused by sensory mechanisms resulting in elevated perceived sound intensity (Katzenell & Segal, 2001). The mean score on burnout for the sound sensitivity sample is close to the cut off for high degree of burnout syndrome (≥3.75 on SMBQ; Grossi et al., 2003), indicating that several individuals in the sample may qualify as being burned out. From a clinical point of view this calls for practitioners to more closely investigate the level of burnout in their patients with sound sensitivity. Even if the sound sensitivity sample’s mean scores of anxiety and depression are below the most recommended cut off-values for HADS (≥8 for both anxiety and depression; Bjelland et al., 2002), the significant differences between the sample and the reference group may further indicate the occurrence of depressive symptoms among individuals in the sound sensitivity sample. With high detrition rates becoming more common for epidemiological studies (Galea & Tracy, 2007), the VEHS had a participation rate of 40 %. The lowest participation rate was found in the age and gender strata of men 18 - 29 years old (17.7 %). The average study participant was a woman (55.7 %) of age 60 to 69 years (22.3 %). Due to tinnitus increasing with age (Holmes & Padgham, 2009), these findings may be explained by research showing that women, and individuals with personal symptoms related to a study, show greater tendency to participate in research projects (Galea & Tracy, 2007). However, the prevalence of tinnitus (7.5 %), and sound sensitivity (1.9 %), among participants was lower than previously reported in the general population (Andersson et al., 2002; Langguth et al., 2013). This result may be due to differences in the criteria used. In line with previous research (Holmes, & Padgham, 2009), there was a significant difference in age between all samples with hearing problems and the reference group. Considering that being male is one of the greatest risk factors for requiring tinnitus (Hébert, Canlon, Hasson, Magnusson Hanson, et al., 2012), the tinnitus sample consisting of significantly more men was expectable. The tinnitus sample’s lower level of education may be understood by the increasing risk to develop tinnitus if exposed to a noisy environment, as for example by working with manual labour. As this study did not control for potential confounders it is not possible to say whether other variables contributed to the results. Previous studies have associated women with higher levels of burnout (Nordlund, Reuterwall, Höög, Lindahl, Janlert, & Slunga Birglander, 2010), as well as anxiety and depression (Faravelli, Scarpato, Castellini, & Lo Sauro, 2013). The higher male prevalence of the tinnitus sample may in this case have contributed to the sample not showing worse health condition than the reference group. Low education has further been associated with lower sleep quality (Arber, Bote, & Meadows, 2009). Note worthily, the calculations of degrees of freedom for the t-tests were based on the assumption that the complete-data statistic, if no data were missing, is a z-test

12
rather than a t-test. However, this assumption has been questioned (Barnard & Rubin, 1999), and may possibly have implications for the results. In conclusion the results suggests that sound sensitivity is associated with poor sleep quality, stress, depression, burnout, and possibly anxiety. In contrast results suggest that tinnitus and double diagnoses is associated only with poor sleep quality. Furthermore, results raise the notion of more sensory, versus cognitive, origin of sound sensitivity in individuals with, versus without, tinnitus. More research is needed on how individuals are affected by living with simultaneous hearing problems, and to further explore the existence of subgroups within the phenomena of sensitivity to sound.
Referenser Andersson, G., Lindvall, N., Hursti, T. & Carlbring, P. (2002). Hypersensitivity to sound (hyperacusis): A prevalence study conducted via the internet and post. International Journal of Audiology, 41(8), 545-554. Andersson, G., Strömgren, T., Ström, L. & Lyttkens, L. (2002). Randomized controlled trial of internet-based cognitive behavior therapy for distress associated with tinnitus. Psychosomatic Medicine, 64(5), 810-816. Arber, S., Bote, M. & Meadows, R. (2009). Gender and social-economic patterning of self-reported sleep problems in Britain. Social Science & Medicine, 68(2), 281-289. Asha’ari, Z. A., Zain, N. M. & Razali, A. (2010). Phonophobia and hyperacusis: Practical points from a case report. Malaysian Journal of Medical Sciences, 17(1), 49-51. Barnard, D. & Rubin, D. B. (1999). Small-sample degrees of freedom with multiple imputation. Biometrika, 86, 948-955. Baguley, D. M. (2003). Hyperacusis. Journal of the Royal Society of Medicin, 96(12), 582-585. Bjelland, I., Dahl, A. A., Haug, T. T. & Neckelmann, D. (2002). The validity of the Hospital Anxiety and Depression Scale: An updated literature review. Journal of Psychosomatic Research, 52(2), 69-77. Canlon, B., Theorell, T. & Hasson, D. (2013). Associations between stress and hearing problems in humans. Hearing Reasearch, 295(12), 9-15. Cohen, S. & Williamson, G. M. (1988). Perceived tress in a probability sample of the United States. In S. Spacapan & S. Oskam (Eds.). The social psychology of health: the Claremont Symposium on applied social psychology (pp. 31-67). Newbury Park, CA: Sage. De Ridder, D., Elgoyhen, A. B., Romo, R. & Langguth, B. (2011). Phantom percepts: tinnitus and pain as persisting aversive memory networks. Proceedings of the National Academy of Sciences of the United States of America, 108(20), 8075–8080. Eskin, M. & Parr, D. (1996). Introducing a Swedish version of an instrument measuring mental stress (Reports from the Department of Psychology, no. 813). Stockholm: Stockholm University, Department of Psychology. Faravelli, C., Scarpato, M. A., Castellini, G. & Lo Sauro, C. (2013). Gender differences in depression and anxiety: The role of age. Psychiatric Research, 210(3), 1301-1303.

13
Galea, S. & Tracy, M. (2007). Participation rates in epidemiological studies. AEP, 17(9), 643-653. Grossi, G., Perski, A., Evengård, B., Blomkvist, V. & Orth-Gomér, K. (2003). Physiological correlates of burnout among women. Journal of Psychosomatic Research, 55(4), 309-316. Hébert, S., Canlon, B. & Hasson, D. (2012). Emotional exhaustion as a predictor of tinnitus. Psychotherapy and Psychosomatics, 81(5), 324-326. Hébert, S., Canlon, B., Hasson, D., Magnusson Hanson, L. L., Westerlund, H. & Theorell, T. (2012). Tinnitus severity is reduced with reduction of depressive mood: A prospective population study in Sweden. PLoS ONE, 7(5), e37733. Hébert, F., Fournier, P. & Noreña, A. (2013). The auditory sensitivity is increased in tinnitus ears. The Journal of Neuroscience, 33(6), 2356-2364. Hébert, S. & Lupien, S. J. (2007). The sound of stress: blunted cortisol reactivity to psychosocial stress in tinnitus sufferers. Neuroscience Letters, 411(2), 138-142. Henry, J. A., Dennis, K. C. & Schechter, M. A. (2005). General review of tinnitus: prevalence, mechanisms, effects and management. Journal of Speech, language and Hearing Research, 48, 1204-1235. Holmes, S. & Padgham, N. D. (2009). Review paper: More than ringing in the ears: a review of tinnitus and its psychosocial impact. Journal of Clinical Nursing, 18(21), 2927-2937. Izuhara, K., Wada, K., Nakamura, K., Tamai, Y., Tsuji, M., Ito, Y. & Nagata, C. (2013). Association between tinnitus and sleep disorder in the general Japanese population. Annals of Otology, Rhinology & Laryngology, 122(11), 701-706. Job, R. F. (1999). Noise sensitivity as a factor influencing human reaction to noise. Noise & Health, 1(3), 57-68. Katzenell, U. & Segal, S. (2001). Hyperacusis: Review and clinical guidelines. Otology & Neurotology, 22(3), 321-327. Kecklund, G. & Åkerstedt, T. (1992). The psychometric properties of the Karolinska Sleep Questionnaire. Journal of Sleep Research, 1(Suppl. 1), 113. Langguth, B. A. (2011). Review of tinnitus symptoms beyond ‘ringing in the ears’: A call to action. Current Medical Research and Opinion, 27(8), 1635–1643. Langguth, B., Kreuzer, P. M., Kleinjung, T. & De Ridder, D. (2013). Tinnitus: Causes and clinical management. The Lancet Neurology, 12(9), 920-930. Langguth, B., Landgrebe, M., Kleinjung, T., Sand, G. P. & Hajak, G. (2011). Tinnitus and depression. The World Journal of Biological Psychiatry, 12(7), 489-500. Lanting, C. P., De Kleine, E. & Van Dijk, P. (2009). Neural activity underlying tinnitus generation: Results from PET and fMRI. Hearing Researsh, 255(1-2), 1–13. Lasisi, A. O. & Gureje, O. (2011). Insomnia and impact on quality of life among community elderly subjects with tinnitus. Annals of of Otology, Rhinology & Laryngology, 120(4), 226-230. Levine, R. A. (1999). Somatic (craniocervical) tinnitus and the dorsal cochlear nucleus hypothesis. American Journal of Otolaryngology, 20(6), 351–362.

14
Liang, F., Liu, C. & Carroll, R. J. (2010). Advanced Markov Chain Monte Carlo methods: Learning from past samples. New York: Wiley. Marozeau, J. & Florentine, M. (2007). Loudness growth in individual listeners with hearing losses: A review. The Journal of the Acoustical Society of America, 122(3), EL81-EL87. Marriage, J. &Barnes, N. M. (1995). Is central hyperacusis a symptom of 5-hydroxytryptamine (5-HT) dysfunction? The Journal of Laryngology and Otology. 109(10), 915-921. Melamed, S., Kushnir, T. & Shirom, A. (1992). Burnout and risk factors for cardiovascular diseases. Behavior Medicine, 18(2), 53-60. Nordin, M. & Nordin, S. (2013). Psychometric evaluation and normative data of the Swedish version of the 10-item perceived stress scale. Scandinavian Journal of Psychology, 54(6), 502-507. Nordin, M., Åkerstedt, T. & Nordin, S. (2013). Psychometric evaluation and normative data for the Karolinska Sleep Questionnaire. Sleep and Biological Rhythms, 11(4), 216-226. Nordin, S., Körning Ljungberg, J., Claeson, A-S. & Neely, G. (2013). Stress and odor sensitivity in persons with noise sensitivity. Noise and Health, 15(64), 173-177. Nordin, S., Millqvist, E., Löwhagen, O., & Bende, M. (2003). The Chemi¬cal Sensitivity Scale: Psychometric properties and comparison with the Noise Sensitivity Scale. Journal of Environmental Psychology, 23(4), 357–65. Nordin, S., Palmquist, E. & Claeson, A-S. (2013). Metric properties and normative data for brief noise and electromagnetic field sensitivity scales. Scandinavian Journal of Public Health, 41(3), 293-301. Nordin, S., Palmquist, E., Claeson, A-S. & Stenberg, B. (2013). The environmental hypersensitivity symptom inventory: Metric properties and normative data from a population-based study. Archives of Public Health, 71:18. Norlund, S., Reuterwall, C., Höög, J., Lindahl, B., Janlert, U. & Slunga Birgander, L. (2010). Burnout, working conditions and gender - results from the northern Sweden MONICA Study. BMC Public Health, 10:326. Ortmann, M., Muller, N., Schlee, W. & Weisz, N. (2011). Rapid increases of gamma power in the auditory cortex following noise trauma in humans. European Journal of Neuroscience, 33(3), 568–575. Palmquist, E., Claeson, A-S, Neely, G, Stenberg, B. & Nordin, S. (2014). Overlap in prevalence between various types of environmental intolerance. International Journal of Hygiene and Environmental Health, 217(4-5), 427-434. Skarzynski, H., Rogowski, M., Bartnik, G. & Fabijanska, A. (2000). Organization of tinnitus management in Poland. Acta Otolaryngol, 120(2), 225-226. Sullivan, M., Karlsson, J., Sjöström, L., Backman, L., Bengtsson, C, Bouchard, C, ... Wedel, H. (1993). Swedish obese subjects (SOS): An intervention study of obesity: Baseline evaluation of health and psychosocial functioning in the first 1743 subjects examined. International Journal of Obesity, 17(9), 503-512. Zigmond, A. S. & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67(6), 361-370. Weinstein, N. D. (1978). Individual differences in reactions to noise: A longitudinal study in a college dormitory. Journal of Applied Psychology, 63(4), 458–66.