Embed Size (px)
Citation preview

American Journal of Industrial Medicine 19:205-213 (1991)
Silicosis Among Gemstone Workers in South Africa: Tiger’s-Eye Pneumoconiosis
Neil W. White, MD, FCP(SA), Runjan Chetty, FFPath(SA), and Eric D. Bateman, MD, FRCP
Six cases of silicosis in workers involved in the processing of semiprecious gem stones have been seen in our clinic since 1976. They had been employed as stone sculptors in lapidaries where they processed tiger’s-eye, rose quartz, amethyst, quartz crystal, and a variety of other locally occurring semiprecious stones. In five of the cases, exposure was in small and poorly regulated lapidaries without specific dust control measures. The sixth was detected during the course of a health and hygiene survey (including dust sampling) that was conducted in one of two lapidaries still operating in our area. Progressive massive fibrosis (PMF) or accelerated silicosis was noted in four of the six cases, three of whom had progression of their disease after cessation of exposure. With the development of PMF, the initial restrictive pulmonary function abnormalities were followed by steadily worsening airflow obstruction. Lung biopsies confirmed silicosis in three cases. Tuberculosis was confirmed in two cases and suspected and treated in a third. Workmen’s Compensation was awarded in five cases. The survey confirmed that in semiprecious gem stone processing, the risk of silicosis appears to be confined to stone sculptors. Tried and proven techniques of general and local exhaust ventilation combined with water or oil to control dust at source were capable of effectively reducing dust emission to acceptable levels.
Key words: accelerated silicosis, pulmonary function abnormality, tiger’s-eye, amethyst, rose quartz, lapidary work
INTRODUCTION
Silicosis has been described in relation to a variety of occupations, the common factor in these being the use of physical force (chiselling, drilling, abrasive use, etc.) in the generation of respirable silica particles. The semiprecious stones processed by sculpturing in our local lapidary industry are either crystalline or cryptocrystalline quartz (SiO,.nH,O) containing quantities of trace or other elements. The particular conditions under which they crystalize give them their special qualities [Read, 19701. The various stones include rose quartz, jasper, agate, amethyst, aventurine, and quartz crystal. The most important and prized of the semiprecious gem stones of
Respiratory Clinic, Department of Medicine, University of Cape Town and Groote Schuur Hospital, Cape Town, South Africa (N.W.W., E.D.B.). Department of Anatomical Pathology, University of Cape Town, Cape Town, South Africa (R.C.). Address reprint requests to Dr. Eric D. Bateman, Respiratory Clinic, Department of Medicine, University of Cape Town and Groote Schuur Hospital, Cape Town, South Africa, 7925. Accepted for publication July 13, 1990.
0 1991 Wiley-Liss, Inc.
206 White et al.
southern Africa is tiger’s-eye. This unique form of silicified crocidolite occurs almost exclusively in an area of the northern Cape Province of South Africa where it is associated with deposits of crocidolite asbestos. Significant quantities of mineral tiger’s-eye and other gemstones are exported for processing, particularly to East Asia.
Radiological and pulmonary function abnormalities have been described in relation to processing of gemstones such as jade and lapis lazuli, where silica flour is used as an abrasive [Ng et al., 19871. Similar findings have also been documented in relation to working the harder quartz gemstones occurring in Southern Africa [Chap- man and Tracey, 19891 but there is no detailed description of this pneumoconiosis in the classical [Morgan and Seaton, 1984; Parkes, 1982; ILO, 19831 or recent medical literature [Ziskind et al., 19761.
We describe a series of six sculptors of semiprecious gemstones whom we have seen, evaluated, and followed-up in our clinic since 1976. They presented with a variety of manifestations of silicosis. These were skilled workmen who hand-sculpted gemstones. The stone is worked by hand-holding carefully preselected pieces against a mechanical abrasive belt or disc (usually carborundum) and thereby gradually shaping it. There is obvious potential for liberating significant amounts of respirable dust.
The lapidary industry in the Western Cape is small, with enterprises employing a total of fewer than 100 persons. In the last 10 years, economic pressures have resulted in the closure of three of five of these lapidaries. Five of the six workers had been employed in factories that have ceased operation. The skilled workmen in these lapidaries knew one another and requested referral to our clinic once the risk of pneumoconiosis became known. From their descriptions and our inspections, it is apparent that the general ventilation in these lapidaries was poor [NIOSH, 19781. Minimal and ineffective steps were taken to control the dust at source and respirators were not provided. Only case 6 had the benefit of protection against dust in the form of continuous watering of the abrasive belt, combined with down-draft local venti- lation and reasonable general ventilation. We carried out an evaluation of the respi- ratory health of the workforce at one lapidary, combined with analysis of air quality. The results of this survey are presented.
CASE REPORTS Case 1
A 35 year-old man worked for 19 years as a gemstone sculptor. He presented to our clinic in 1976 with symptoms of dyspnea, intermittent wheezing, weight loss, and a nonproductive cough, including a single small hemoptysis. He smoked 20 cigarettes a day. Pulmonary function testing showed a modest nonobstructive reduc- tion in lung volumes with reduced carbon monoxide transfer factor (Table I). The chest radiograph was compatible with simple nodular silicosis (Table 11). Because of uncertainty about the diagnosis, he underwent open lung biopsy. The results are presented below.
He continued in his occupation until 198 1 and was followed-up regularly in our clinic. He continued to work despite advice to the contrary. Workmen’s Compensa- tion was applied for and awarded. Radiographs taken in 1978 showed changes com- patible with stage C progressive massive fibrosis (PMF). Nodules were present throughout both lungs, with large confluent areas in both upper lobes and in the apical
Tiger’s-Eye Pneumoconiosis 207
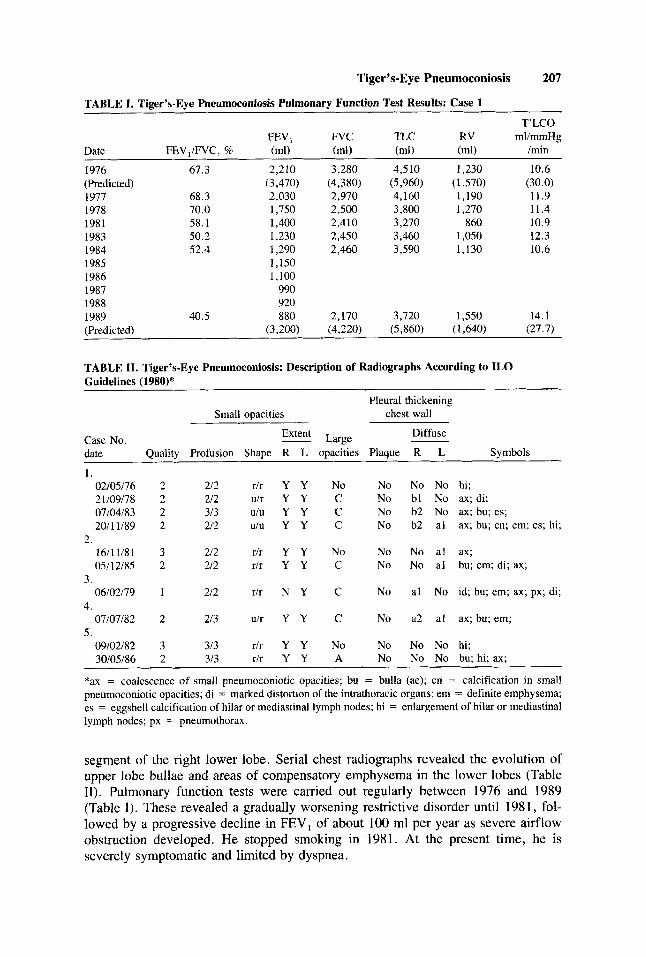
TABLE I. Tiger’s-Eye Pneumoconiosis Pulmonary Function Test Results: Case 1
T’LCO FEVl FVC TLC RV ml/mmHg
Date FEV,/FVC, % (ml) (ml) (ml) (ml) /min
1976 67.3 (Predicted) 1977 68.3 1978 70.0 1981 58.1 1983 50.2 1984 52.4 1985 1986 1987 1988
2,210 3,280 4,510 (3,470) (4,380) (5,960) ( 2,030 2,970 4,160 1,750 2,500 3,800 1,400 2,410 3,270 1,230 2,450 3,460 1,290 2,460 3,590 1,150 1,100
990 920
,230 10.6 ,570) (30.0) ,190 11.9 ,270 11.4 860 10.9
,050 12.3 .130 10.6
1989 40.5 880 2,170 3,720 1,550 14.1 (Predicted) (3,200) (4,220) (5,860) (1,640) (27.7)
TABLE 11. Tiger’s-Eye Pneumoconiosis: Description of Radiographs According to ILO Guidelines (1980)* ~
Pleural thickening Small opacities chest wall
Diffuse Case No. Extent Large date Quality Profusion Shape R L opacities Plaque R L Symbols
1. 02/05/76 2 1/09/78 07/04/83 2011 1/89
1611 1/81 05/12/85
06/02/79
07/07/82
09/02/82 30/05/86
2.
3.
4.
5.
2 2 2 2
3 2
1
2
3 2
212 r/r Y Y 212 u/r Y Y 313 UIU Y Y 212 ulu Y Y
212 rlr Y Y 212 rlr Y Y
212 r/r N Y
213 u/r Y Y
313 r/r Y Y 313 r/r Y Y
No No No No hi; C No bl No ax; di; C No b2 No ax; bu; es; C No b2 a1 ax; bu; cn; em; es; hi;
No No No a1 ax; c No No a1 bu; em; di; ax;
C No a1 No id; bu; em; ax; px; di;
C No a2 a1 ax; bu; em;
No No No No hi: A No No No bu; hi; ax;
*ax = coalescence of small pneumoconiotic opacities; bu = bulla (ae); cn = calcification in small pneumoconiotic opacities; di = marked distortion of the intrathoracic organs; em = definite emphysema; es = eggshell calcification of hilar or mediastinal lymph nodes; hi = enlargement of hilar or mediastinal lymph nodes; px = pneumothorax.
segment of the right lower lobe. Serial chest radiographs revealed the evolution of upper lobe bullae and areas of compensatory emphysema in the lower lobes (Table 11). Pulmonary function tests were carried out regularly between 1976 and 1989 (Table I). These revealed a gradually worsening restrictive disorder until 1981, fol- lowed by a progressive decline in FEV, of about 100 ml per year as severe airflow obstruction developed. He stopped smoking in 1981. At the present time, he is severely symptomatic and limited by dyspnea.

208 White et al.
TABLE 111. Tiger’s-Eve Pneumoconiosis Pulmonary Function Test Results: Case 2 -~
T’LCO FEV , FVC TLC RV ml/mmHig
Date FEV,/FVC, % (ml) (mu (ml) (ml) /min
1981 75 8 2,200 2,900 1985 50.2 1,280 2,125 3,475 1,280 14 8 (P red ictcd ) (3,200) (3,900) (5,460) (1,570) (28 6) 1986 52 3 1,100 2,100 1988 54 9 790 1,440 I990 49 1 390 795 (PrediLted) (3,030) (3,770)
Case 2
A 32 year-old man presented in 1981 with right sided pleuritic pain and was found to have a spontaneous pneumothorax and diffuse nodularity on chest radio- graph. He smokcd 5 cigarettes a day and had worked for 15 years in lapidaries, mostly as a sculptor. Hc was particularly experienccd in the working of tiger’s-eye. He initially refused further treatment but was seen again in November 1985 on the advice of his colleagucs and because the company was closing down for financial reasons. At the initial visit he was asymptomatic and his pulmonary functions showed mild nonobstructive reduction in spirometry . The chest radiograph showed the pres- ence of simple nodular silicosis with some minor pleural thickening (Table 11). During 1985 he startcd to develop dyspnea and a radiograph showed established progressive massive fibrosis with contracture of both upper lobes together with a diffuse nodular pattern in both lung fields. Workmen’s Compensation with 100% disability was succcssfully obtained. Subsequent follow-up documented a progressive decline in his pulmonary function and dcvelopment of severe airflow obstruction (Table 111). He began to have repeated admissions to hospital for the treatmcnt of respiratory tract infections. By 1989, he had deteriorated markedly with signs and symptoms of cor pulmonale. He received domiciliary oxygen but died in respiratory Failure in March 1990.
Case 3
This 41 year-old man was first secn in our clinic in 1979. He had first been diagnosed as having silicosis following evaluation and open lung biopsy at another hospital in 1977. He had worked as a gcmstone cuttcr, primarily with tiger’s-eyc and rosc quartL, for IS years. He had an estimated 40-pack-ycar smoking history. At presentation he was severcly dyspneic and unable to work. Observed (and predicted) [Schoenberg et al., 19781 pulmonary function test results were: TLC 4,370 ml (5,460), R V 3,150 ml (1,690). FEV, 520 ml (3,110), FVC, 120 ml (3,760), FEV,/ FVC = 46.4%, T’LCO 5.5 ml/mmHg/min (27.0), and KCO 3.0 ml/mmHg/min/liter (5.0). The chest radiograph showed the features of PMF and marked bullous change with compensatory emphysema. A small right apical pneumothorax was present. In vicw of the possibility of co-existent tuberculosis, he was subjected to fiberoptic bronchoscopy and transbronchial biopsy. In spite of negative findings, he was given a full course of antituberculous therapy, together with bronchodilators and cortico-
Tiger’s-Eye Pneumoconiosis 209
steroids. There was little subjective or objective response and the patient died from respiratory failure in early 1981.
Case 4
This 56 year-old man worked in lapidaries as a gemstone sculptor and foreman from 1947 until he was retrenched in 198 1. Pulmonary tuberculosis was diagnosed in 1981 on the basis of direct examination of a sputum specimen. The chest radiograph failed to improve with treatment and he was therefore referred to us for an evaluation. He felt improved from the treatment and was only mildly dyspneic. He had smoked 20 cigarettes per day for many years. His pulmonary function showed moderate obstruction with reduced carbon monoxide transfer factor: TLC 4,460 ml(5,870), RV 1,190 ml (1,980), FEV, 1,313 ml (3,010), FVC 3,215 ml (3,890), FEV,/FVC = 40.8%, T’LCO 12.6 ml/mmHg/min (24.4), and KCO 3.18 ml/mmHg/min/liter (4.4). The chest X-ray showed PMF with marked bilateral upper lobe destruction and contracture, worse on the right than on the left. There was a diffuse nodular infiltrate. Both lower zones appeared hyperlucent with compensatory emphysema. He was awarded Workmen’s Compensation. Subsequently we have been unable to recall him but he is known to have been alive in 1989.
Case 5
This 29 year-old man had worked in the same enterprise as cases 2 and 3 for 13 years but had spent only the last 3 years as a stone sculptor. He presented to us on the advice of his colleagues, asymptomatic and with pulmonary function within normal limits: TLC 5,600 ml (5,960), RV 940 ml (1,450), FEV, 3,940 ml (3,640), FVC 4,780 ml (4,510), FEV,/FVC = 82.4%, T’LCO 30.2 ml/mmHg/min (32.1), and KCO 5.6 ml/mmHg/min/liter (5.4). His chest X-ray showed diffuse nodular opacities with bilateral hilar adenopathy . A transbronchial biopsy was obtained by fiberoptic bronchoscopy. He remained well until 1986 when he presented with a cold abscess of the sternum. The chest radiograph showed some coalescence of nodules and upper lobe bullae. He received a full course of antituberculous therapy. When recalled in 1989 he was asymptomatic, the chest radiograph was unchanged, and the pulmonary function tests were normal.
Case 6
This 46 year-old man was detected in 1989 during the health and hygiene survey of the lapidary described below. He had an 18 year history of lapidary work, 8 of which had been spent as a sculptor with his current employer, the balance of time having been spent in a number of similar establishments. At the first consultation, he had symptoms of chronic bronchitis and dyspnea on moderate exertion. He was a smoker of 10 cigarettes a day. Pulmonary function testing showed severe obstruction with gas trapping and markedly decreased gas transfer: TLC 7,645 ml (4,690), RV 4,060 ml (1,460), FEV, 1,360 ml before bronchodilator and FEV, 1,560 ml (2,750) after, FVC 3,400 ml(3,230), FEV,/FVC = 40%, T’LCO 8.9 ml/mmHg/min (28.7), and KCO 1.9 mlimmHgiminiliter (4.8). The chest radiograph showed simple nodular silicosis.

210 White et al.
Fig. 1 . typical silicotic lesions hernatoxylin and eosin. X 100.
Tiger’s-eye pneumoconiosis. Section of a transbronchial biopsy taken from case 5 showing
Pathological Findings
Similar histological features were present in the three lung biopsies from pa- tients l , 3 , and 5 . The entire spectrum from early to late changes of silicosis was seen. The early lesions were typified by conccntrically layered fibroblasts and histiocytes. It was in these areas that silica particles were identified by means of a polarizing lens. The histiocytes were granular in appearance and were also found in the alveolar spaces. The late lesions were characterized by the laying down of collagen with progressive hyalinization. Individual nodules coalesced into larger ones with conse- quent distortion of small airways and dcstruction of vessels (Fig. 1). Although pre- dominantly nodular in configuration, stellate extensions of fibrous tissue into the surrounding septae were also evident. Micronodular scars were evident along the lymphatic pathways with accentuation around bronchovascular bundles. No evidence of tuberculosis or other pathology was found.
LAPIDARY HEALTH AND HYGIENE SURVEY
The management of one of the two lapidaries still operating in the Western Cape agreed to our studying the facility. The second refused. Twenty-one persons were employed in the process of producing stones ready for mounting into jewelry from

Tiger’s-Eye Pneumoconiosis 21 1
gemstones in their natural state. The process involves crushing and tumbling, fol- lowed by cutting or ultrasonic drilling. Crushing is carried out in the open air; tumbling is a wet, enclosed process; and cutting and drilling are enclosed processes carried out under diesel oil. Only two employees are engaged in stone sculpting. They carefully select virgin stones and hand shape these against a continuous wet carbo- rundum belt.
All 21 employees were evaluated. An ATS Respiratory Symptoms question- naire [Ferris, 19781 was administered by a trained nurse; a vitallograph dry wedge spirometer was used to measure pulmonary function according to ATS criteria [Gard- ner et al., 19871; chest X-rays were carried out according to ILO standards for the radiological detection of pneumoconiosis [ILO, 198 11; abnormalities were subse- quently evaluated by a physician.
Only one employee (case 6, one of the stone sculptors) had a chest radiograph suggestive of silicosis. The other sculptor was thought to be normal. Of the remaining employees, two were diagnosed as having pulmonary tuberculosis and were started on therapy; a third had an X-ray appearance suggestive of pulmonary tuberculosis but sputum was negative for AAFB and he refused further investigation. Two further employees, both cigarette smokers, were found to have significant chronic obstruc- tive airway disease. The mean age of those surveyed was 34.95 years (S.D. 11.33) and the mean length of service was 7.7 years (S.D. 6.53).
Dust exposure was estimated with a personal sampler using an MSA cyclone head calibrated to a flow rate of 2 limin, collecting on a matched weight Millipore filter (MAWP 0371pm). Eight hundred and thirty (830) liters of air was sampled over a working shift of the gemstone sculptor described as case 6 above. The respirable dust level was less than 0.0001 mg per cubic meter. Analysis of samples settled dust from the vicinity of sculpting operations by X-ray diffraction analysis confirmed that the free crystalline silica content of samples was 79-81% and that no fibers were present. No analysis of the proportion of dust that was respirable was carried out.
We concluded that sufficient measures had been taken in this lapidary, that the risk of silicosis was low, and that case 6 was likely to have developed silicosis in previous employment.
DISCUSSION
The close geological relationship of tiger’s-eye and crocidolite asbestos raised the possibility that this pneumoconiosis might be more akin to asbestosis than sili- cosis. The biopsy findings confirmed a silicotic type of pathology and dust analysis confirmed a high level of free crystalline silica with no fibers present.
Crystalline silica has long been held responsible for serious forms of pneumo- coniosis and predisposition to tuberculosis. The danger of accelerated silicosis re- sulting from intense exposure to high concentrations of free silica is well known from activities such as sandblasting and tunneling. Mechanical cutting and smoothing tools in the monumental masonry industry are known to increase risk of pneumoconiosis [Ziskind et al., 19761. Stone dressing and polishing in this industry is similar in many respects to lapidary work. Abrasives have also been implicated in pneumoconiosis. These include silica flour [Ng et al., 19871 and sandpaper which may contain flint and quartz [Ziskind et al., 19761 or carborundum [BCgin et al., 19891.
Accelerated silicosis shares all the major features of chronic silicosis but may

212 White et al.
produce dyspnea and have a progressive course over about 10 years [Ziskind et al., 19761. Radiological features of progressive massive fibrosis are well known and were amply illustrated in cases 1 to 4. Cases 1 and 2 progressed radiologically from simple silicosis to accelerated silicosis within 2 and 4 years respectively. Cases 2 and 3 progressed to respiratory failure, cor pulmonale, and death. There is a striking asso- ciation of accelerated silicosis with a history of exposure to very pure forms of newly fractured crystalline quartz in this industry. Ideally, workers should be withdrawn from exposure as soon as relevant radiologic abnormalities are detected. There is no legal requirement that this should happen in South Africa and it remains a matter of choice by the individual worker as to what he will do on being told that he has silicosis.
The frequency with which active pulmonary tuberculosis was diagnosed in this group of patients is also noteworthy. Notwithstanding the moderately high back- ground incidence of tuberculosis in our area, the frequency with which the disease occurred in these patients still appears excessive. Tubercle bacilli and their products have been implicated in the development of progressive massive fibrosis and silicotics are known to have an increased susceptibility to tuberculosis [Snider, 19781.
Our findings contrast with those of gemstone workers in Hong Kong and arc more in keeping with the findings among jewelry workers in Lesotho [Chapman and Tracey, 19891. In both situations, work was carried out in small, poorly ventilated work-rooms. In the Hong Kong study [Ng et al., 19871, 27% of 157 workers were found to have radiological pneumoconiosis, defined as opacities with median profu- sion 1/0 and above. The highest profusion observed was 1/2 and this occurred among gemstone polishers who were using silica flour as an abrasive. Silica flour could contribute to a quartz content of respirable dust exceeding 90%, whilst jade and lapis lazuli, the most commonly processed gemstones, are complex silicates or carbonates and seldom contribute quartz in excess of 5% in respirable dust. The spectrum of disease documented among workers in Hong Kong was therefore less severe than we have encountered. In a short report on a lapidary in Lesotho where tiger’s-eye is processed, there werc 24 stone-cutters with more than 1 year of exposure: 22 had radiological evidence of pneumoconiosis although it appears that radiological tech- niques were not standardized.
Silica dust exposure is known to be associated with restrictive, obstructive, and mixed patterns of ventilatory impairment. In South African gold mines, dust exposure may produce airflow obstruction independently of silicosis and cigarette smoking [Irwig and Rocks, 19781. Accelerated silicosis is often described as causing a severe restrictive disorder, particularly in advanced cases [Ziskind et al., 19761. However, it is acknowledged that we do not have adequate longitudinal studies of pulmonary function in accelerated silicosis. The pulmonary function abnormalities encountered in accelerated silicosis must depend on the stage of the disease at which measure- ments are made. A sequence of patterns was found in our first and best documented case. In 1976, simple nodular silicosis was associated with a moderate nonobstructive reduction in lung volumes. As progressive massive fibrosis developed, there was an initial worsening of the restrictive disorder to moderate severity with FEV, , FVC, TLC, and RV decreasing in a proportional manner over a 5 year period up to 1981. Between 1981 and 1989, there has been a continued dccline in FEV, (i 100 rnl/year) with a proportional increase in RV and the development of severe airflow obstruction. These measurements reflect the pathological process taking place in accelerated sil-

Tiger’s-Eye Pneumoconiosis 213
icosis with progressive contractural or compensatory emphysema, peribronchial fi- brosis, airway distortion, and consequently, worsening of airflow obstruction and functional impairment.
Our experience with pneumoconiosis among lapidary workers is illustrative of silicosis and a number of enduring basic principles in occupational health. Case 6 had a long history of exposure but relatively mild disease. We attribute this to the fact that he had been protected by the application of basic principles of dust control, namely, liberal local use of water or oil to dampen dust at source, combined with adequate local and general exhaust ventilation.
REFERENCES
BCgin R, Cantin A, and SCbastien P (1989): Carborundum pneumoconiosis. Chest 95:842-845. Chapman TT, Tracey D (1989): “Acute” pneumoconiosis in jewelry workers. Chest 96:267s. Ferris BG (1978): Epidemiological Standardisation Project. Am Rev Respir Dis 118:6. Gardner RM, Hankinson JL, Clausen JL, Crapo RO, Johnson RL, Epler GR (1987): ATS statement on
standardisation in spirometry. Am Rev Respir Dis 136:1285-1298. International Labour Office (198 1): “Guidelines for the Use of ILO International Classification of
Radiographs of Pneumoconiosis.” Occupational Safety and Health Series No. 22 (Rev.). Geneva: ILO .
International Labour Office (1983): “Encyclopedia of Occupational Health and Safety.” Geneva: ILO. Invig LM, Rocks P (1978): Lung function and respiratory symptoms in silicotic and nonsilicotic gold
Morgan WKC, Seaton A (1984): “Occupational Lung Diseases. ” Philadelphia: W.B. Saunders Com-
National Institute for Occupational Health and Safety (1978): ‘‘Ventilation Requirement for Grinding,
Ng TP, Tsin TW, O’Kelly FJ, Chan SL (1987): A survey of the respiratory health of gemstone workers
Parkes WR (1982): “Occupational Lung Disorders.” London: Buttenvorths. Read HH (1970): “Rutlet’s Elements of Mineralogy,” 26th ed. London: Thomas Durby & Co. Schoenberg JB, Beck GJ, Bouhuys A (1978): Growth and decay of pulmonary function in healthy blacks
Snider DE (1978): The relationship between tuberculosis and silicosis. Am Rev Respir Dis 118:455-460. Ziskind M, Jones RN, Weill H (1976): State of the Art: Silicosis. Am Rev Respir Dis 113:645-665.
miners. Am Rev Respir Dis I17:429-434.
pany.
Buffing and Polishing Operations. ” Cincinnati: DHEW Publication No. (NIOSH) pp 75-107.
in Hong Kong. Am Rev Respir Dis 135:1249-1254.
and whites. Respir Physiol 33:367-393.