Embed Size (px)
Citation preview

Graefe's Arch Clin Exp Ophthalmol (1986) 224:55-59 Graefe's Archive for Clinical and Experimental
Ophthalmology © Springer-Verlag 1986
Silicone-oil injection during closed microsurgery for diabetic retinal detachment* David McLeod The Surgical Vitreoretinal Unit, Moorfields Eye Hospital, City Road, London ECIV 2PD, UK
Abstract. A beneficial visual outcome was achieved in 16 (38%) of 42 eyes into which silicone oil was injected after difficulties were encountered during closed microsurgery for severe diabetic retinal detachment. Without recourse to oil injection, most if not all of the eyes would have remained blind and many would have deteriorated into rubeotic glau- coma or phthisis. The main cause of failed surgery was rhegmatogenous retinal detachment associated with residu- al or reparative epiretinal fibrosis, and silicone oil appeared to be of value in preventing rubeosis iridis in such cases. Cataract was a significant problem in the successfully treated eyes.
Introduction
The rationale of silicone-oil injection for massive periretinal proliferation (MPP) is well established. Sequential injection of silicone oil in exchange for vitreal and subretinal fluid permits hydraulic reattachment of the retina, while viscode- lamination of the fibrocellular epiretinal membranes (ERMs) is achieved either directly by injection of oil behind the membranes (Cibis et al. 1962) or indirectly utilising the principle of differential stretching of the membranoretinal complex (Scott 1979). Alternatively, simultaneous exchange of silicone oil for infusion solution and subretinal fluid can be performed after vitrectomy and ERM peeling (Lean et al. 1982). Postoperatively, the surface tension and buoy- ancy of silicone oil provide internal tamponade (or plug- ging) of closeable retinal breaks within the area of oil-retina contact, and the presence of silicone oil as a clear vitreous substitute also provides excellent clarity of vision and facili- tates photocoagulation of untreated breaks.
In contrast to its use in the management of MPP, sili- cone oil has a very limited role as a viscodelaminating agent (or "membrane dissector") during surgery for diabetic trac- tion detachment owing to the multiple firm membranore- tinal adhesions established by outgrowths of new blood vessels into the fibrovascular ERMs. Thus, stretching or elevation of the membranoretinal complex by silicone oil is frequently complicated by tearing of the retina or haem- orrhage. Nevertheless during the past 4 years silicone oil has been injected into selected diabetic eyes after vitrectomy and membrane dissection in order to reattach the retina hydraulically and to provide permanent internal tamponade
* Presented at the 1984 meeting of the Club Jules Gonin in Lau- sanne, Switzerland
of retinal breaks. In addition, it was anticipated that the clear vitreous substitution would permit postoperative pho- tocoagulation of both breaks and reattached ischaemic reti- na, and that the silicone globule might constitute a barrier against the anterior diffusion of vasoproliferative factor, thus preventing postoperative rubeosis iridis (Scott 1981). Because of the recent resurgence of interest in the use of silicone oil, and since there is little information available concerning its role in severe diabetic eye disease, the out- come in a consecutive series of 42 diabetic retinal detach- ments is presented in this report.
Materials and methods
Forty-two eyes of 42 diabetic patients underwent closed in- traocular microsurgery combined with injection of silicone oil (1000 cSt) in the Surgical Vitreoretinal Unit at Moor- fields Eye Hospital between 1980 and 1984. These eyes rep- resent approximately 10% of the total series of diabetic vitrectomies performed during this period. In all the 35 "pr imary" silicone procedures, retinal detachment was as- sociated with over six disc areas of fibrovascular ERM and was further categorised as follows: combined traction and rhegmatogenous retinal detachment (19 eyes); table-top traction retinal detachment (11 eyes) and traction retinal detachment (5 eyes). In a further 7 patients, silicone oil was injected in "secondary" procedures, i.e. during repeat mi- crosurgery after unsuccessful diabetic vitrectomy with rheg- matogenous recurrence of retinal detachment associated with reparative epiretinal fibrosis. At the time of silicone-oil injection, 6 of the eyes were aphakic (4 aphakic preopera- tively and 2 rendered aphakic peroperatively).
The decision to inject silicone oil was made peroperati- vely after difficulties were encountered during vitrectomy and membrane dissection; the indications for silicone-oil injection invariably included the necessity for postoperative internal tamponade of breaks. Fluid/silicone oil exchange was preferred to fluid-gas exchange for one (or often sever- al) of the following reasons : (a) for breaks associated with persistent tangential traction; (b) for posterior breaks (ma- cular or peripapillary) especially if they could not be coagu- lated by xenon endophotocoagulation or cryopexy peroper- atively; (c) for multiple retinal breaks (pre-existing and/or iatrogenic) especially if they were situated in widely sepa- rated locations; (d)for suspected or " los t" retinal breaks e.g. breaks hidden by peroperative haemorrhage; (e) to fa- cilitate phakic internal drainage of subretinal fluid and hy- draulic retinal reattachment (prior to the availability of the
55

56
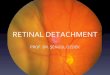
Fig. 1 a-e. Fundus photographs, a Table-top traction detachment (acuity hand motion), b Same eye 2 months after closed microsur- gery with silicone-oil injection because of multiple retinotomies and postoperative panretinal laser photocoagulation (acuity 6/36). e Same eye 3 years after closed microsurgery and 4 months after removal of cataract and silicone oil (acuity 6/18)
Landers infusion contact lens for biomicroscopic phakic gas exchange); (f) to provide permanent tamponade follow- ing deliberate retinal resection in areas o f tightly adherent and contracted ERMs; (g) to try and prevent the inevitable rubeotic phthisis of persistent diabetic detachment in three aphakic eyes in which the severe tractional configuration had proved impossible to relieve with the dissection tech- niques available at the time. In many cases, additional fac- tors influenced the decision to resort to silicone-oil injection (prior to the availability of endolaser photocoagulation), including: (a)very actively vascularised ERMs; (b)exten- sive untreated ischaemic retina; and (c) preoperative rubeo- sis iridis (as noted in 13 eyes).
Patients assumed an appropriate posture postoperative-
ly for 4-7 days in order to maximise the efficacy of silicone- oil tamponade of breaks. Argon laser photocoagulat ion was carried out as soon as practicable after surgery in the hope of sealing (or walling off) retinal breaks and to provide scatter photocoagulafion of reattached ischaemic retina; 20 eyes were so treated.
Further surgical procedures were carried out as follows: (a) lens extraction in five eyes (in four eyes for cataract
a n d in one for anteror dislocation of silicone oil around the lens); (b) buckling of open breaks in three eyes; (c) sili- cone oil top-up in one eye; (d) removal of oil in three eyes (in one in a forlorn attempt to prevent the development of cataract; in one because of anterior dislocation of sili- cone oil around the lens; and in one in conjunction with
56

57
"/,2
%
g.
i %0"
g o °
CF
HM
PL
DD
illl
/ / .
PL HM
o i
T °* i O J
/ Dm 0
0
CF "3/6o 6/60 PREOPERATIVE ACUITY
/
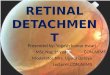
Fig. 2. Scattergram comparing preoperative acuity and final acuity in 22 eyes with anatomically successful results following closed mi- crosurgery and silicone-oil injection (together with cataract extrac- tion in 4 eyes). Each symbol or symbol-arrow-symbol sequence represents one eye; symbols above the oblique line represent eyes with improved vision, n=clear lens; o=aphakic; -,=cataract. PL=perception of light; HM=hand motion vision; CF=count fingers vision
cataract extraction); (e) glaucoma procedures in four eyes [trabeculectomy followed by cyclocryotherapy (one eye); insertion of a Malteno tube (two eyes); or broad iridectomy (one eye)]; and (f) corneal grafting for spontaneous corneal perforation and expulsion of silicone oil (one eye).
The minimum follow-up period for the eyes in this series
was 6 months. Notwithstanding the effects of retinal photo- coagulation, and ignoring transient rubeosis immediately after surgery, the ultimate degree of iris neovascularisation was compared that existing prior to surgery, and the change was documented as follows: (a) reversal of rubeosis; (b) no rubeosis (either preoperatively or finally); (c) persistence of rubeosis; and (d) development or progression of rubeosis.
Results
The retina remained completely attached at least 6 months after surgery in 15 eyes (in some of which minor retinal distortion was evident but not significantly affecting vision); in a further 7 eyes, the macula and most of the retina were reattached but an area of extramacular traction detachment or peripheral walled-off combined traction and rhegmatogenous detachment persisted. Of the 22 eyes thus deemed "anatomically successful", 16 eyes (all of which were maintained phakic during surgery) showed significant visual improvement over the preoperative acuity (Figs. 1, 2). In 11 of these 16 eyes, however, progressive lens opaci- ties have appeared and, in 4 eyes to date, cataract extraction has been performed. The causes of "visual failure" in the 6 otherwise "anatomically successful" cases were as fol- lows: irreversible macular damage i.e. failure of appropriate case selection (2 eyes); rubeotic glaucoma (2 eyes); closed- angle glaucoma, silicone-oil emulsification and cataract (1 eye); and aphakic silicone keratopathy with spontaneous corneal perforation (1 eye).
Anatomical failure was defined as a persisting retinal detachment whose distribution was either total or virtually total (in 15 eyes) or localised but including the macula (in 5 eyes). Many of these 20 eyes also showed complications such as cataract, but the primary cause of failed surgery was central retinal detachment. The anatomical failures could be further subdivided into two groups as follows:
Fig. 3a, b. Fundus photographs, a Severe traction retinal detachment, b Persistent detachment 3 months after closed microsurgery and silicone-oil injection owing to residual epiretinal proliferations and large retinotomy (arrowed) ; the silicone oil has limited the recruitment of subretinal fluid
57

58
Table 1. Outcome of vitrectomy and silicone-oil injection
CTRD TTTRD TRD REF Totals
Anatomical and 8 4 2 2 16 visual success
Anatomical success 4 1 0 1 6 and visual failure
Anatomical failure - early 4 1 2 4 11 (tamponade failure)
Anatomical failure - late 3 5 1 0 9 (reparative fibrosis)
Totals 19 11 5 7 42
Abbreviations: CTRD=combined traction and rhegmatogenous detachment; TTTRD=table-top traction retinal detachment; TRD = traction retinal detachment; REF = reparative epiretinal fi- brosis
Table 2. Change in rubeosis iridis after vitrectomy and silicone-oil injection
Phakic Aphakic Phakic Aphakic re- re- detached detached attached attached
Totals
Reversal of 2 2 1 2 7 rubeosis
No rubeosis 7 3 12 1 23
Persistence 3 1 0 1 5 of rubeosis
Development/ 3 1 3 0 7 progression of rubeosis
Totals 15 7 16 4 42
(a) °' early" failures (11 eyes), where retinal detachment was observed within 1 month postoperatively owing to inferior breaks or breaks associated with residual tangential traction (Fig. 3); and (b) "late" failures (9 eyes), in which retinal reattachment and visual improvement were documented during the first postoperative month, but in which redetach- ment of the retina subsequently occurred secondary to re- parative epiretinal fibrosis and the development or reopen- ing of retinal breaks.
The outcome of surgery in relation to the original cate- gory of diabetic detachment is presented in Table 1 ; no striking correlations are evident, though the "combined rhegmatogenous and traction detachment" group fared best. Changes in the degree of rubeosis iridis after vitrec- tomy and silicone-oil injection are presented in Table 2 in relation to the anatomical result of surgery (i.e. reattached or detached) and the ultimate phakic state of the eye. A majority of phakic and aphakic anatomical failures did not show development or progression of rubeosis, as might oth- erwise have been anticipated. By contrast, several anatomi- cal successes showed persistence (or even progression) of rubeosis. One phakic failure only developed rubeosis after anterior dislocation of silicone oil around the lens 4 months
postoperatively; one aphakic eye showed persistent rubeosis while reattached and reversal of rubeosis on subsequent redetachment.
Discussion
Most vitreoretinal surgeons subscribe to the view that sili- cone oil should be employed only as a last resort where conventional surgery (nowadays including vitrectomy and membrane dissection) has demonstrably failed in complex retinal detachments. The use of silicone oil in the repair of flapped-over giant retinal tears is a justified exception because of the ease of surgery and the excellent results thus attained (Leaver et al. 1984). Similarly, silicone-oil injection was only carried out during diabetic vitrectomy if alterna- tive measures (e.g. sulphahexafluoride gas tamponade) were felt to provide little or no prospect of a successful outcome. The limited success of silicone-oil injection in retrieving vision after complicated diabetic vitrectomy could no doubt be improved by extending the indications to less severe problems, but only at the risk of unjustified complications. Even in the visually successful group, the development of cataract and the persistence of intravitreal silicone oil in many eyes is a continuing cause for concern necessitating long-term follow-up and probably further surgery.
One important advantage of silicone-oil injection is that the transparent oil globule allows improved clinical obser- vation and identification of the means by which vitreore- tinal surgery fails, while also pointing to the limitations and problems associated with the use of this material. Over- filling of the preretinal space with silicone oil, for example, results in forward movement of the lens-iris diaphragm and angle-closure glaucoma, and even a "perfect" (100%) fill may result in creeping angle closure, as also seen with long- acting gases (Chang et al. 1984). However, it is difficult in practice to achieve a perfect oil fill (at a single surgical procedure) because of such factors as vitreous deturges- cence, temporary retinal and suprachoroidal oedema, in- complete peroperative reattachment etc. Where oil-filling is subtotal (for example, a 90% fill), the surface tension of silicone oil in aqueous fluid (50 dyne/cm) together with the limited buoyancy of silicone oil (specific gravity 0.97) produces a markedly curved oil meniscus and a limited area of oil-retina contact (as demonstrated by the distribution of residual vitreal fluid). Thus, unless the patient is postured prone, internal tamponade of breaks is essentially restricted to the hemisphere uppermost according to the orientation of the eye.
The amount of residual traction (e.g. from excessively adherent ERMs) which will nevertheless permit effective internal tamponade of breaks is very difficult to determine, not least peroperatively (although excessive residual trac- tion results in subretinal displacement of oil during attempt- ed hydraulic reattachment). With the benefit of hindsight, it is clear that further epiretinal dissection (or scleral buck- ling) might have prevented some of the early "tamponade failures", though the value of silicone oil in nevertheless limiting recruitment of subretinal fluid during rhegmato- genous recurrence of detachment (Lean et al. 1982) was frequently evident. Thus redetachment from breaks asso- ciated with relatively localised traction increased in extent until a 100% preretinal silicone fill was achieved. However, if traction was more generalised and progressive, as in some
58

59
cases of reparative epiretinal fibrosis, silicone oil was squeezed into the subretinal space through a rigid retinal break some weeks postoperatively.
Apart from restricting subretinal fluid recruitment and providing limited internal tamponade to breaks (some of which were associated with mild tangential traction), no evidence emerged that the silicone oil globule could exert other significant forces or beneficial influences upon the retina. On the contrary, reparative epiretinal fibrosis was disappointingly frequent, just as macular pucker often de- velops after silicone-oil injection for giant retinal tears (Leaver et al. 1984) and ERM proliferation and contraction is seen after intravitreal fibroblast injection in rabbits de- spite silicone-oil injection (Gonvers and Thresher 1983). In- deed, concern has been expressed elsewhere that, by main- taining a "fibrin-fibronectin sandwich" between retina and oil globule, silicone-oil injection during diabetic vitrectomy may even increase the tendency to reparative epiretinal fi- brosis (Barry et al. 1985).
A clear-cut influence of intravitreal silicone oil on post- operative rubeosis iridis was not apparent in this study. Rubeosis iridis reflects the production of vasoproliferative factor by ischaemic retina and this is thought to increase when the retina detaches. Furthermore, anterior diffusion of vasoproliferative factor is believed to be facilitated by vitrectomy (and especially by removal of the anterior hya- loid face) so that rubeosis invariably complicates extensive retinal detachment in an aphakic vitrectomised diabetic eye. Reversal of rubeosis may follow photocoagulation of at- tached ischaemic retina or retinal reattachment; further- more, the presence of an intravitreal silicone-oil globule might also be expected to retard anterior diffusion of vaso- proliferative factor. In the event, the changes in rubeosis documented in this series were sometimes contrary to those otherwise anticipated from the anatomical outcome of sur- gery. However, the unexpected results might be explained in part by the degree of silicone-oil filling. Thus, persisting or progressive rubeosis after successful retinal reattachment
appeared to reflect incomplete silicone-oil filling of the pre- retinal space, which allowed continuing anterior diffusion of vasoproliferative factor from uncoagulated ischaemic retina. By contrast, the 100% preretinal oil-fill resulting from rhegmatogenous retinal redetachment seemed to af- ford some protection against rubeosis. Thus, the role of silicone oil in preventing or reversing rubeosis was most evident after failed reattachment surgery.
Acknowledgements. I am indebted to Miss Heather Lucas for secre- tarial help, to Mr. K. Sehmi for the photographs and to Mr. P.K. Leaver for helpful criticism.
References
Barry PJ, Hiscott PS, Grierson I, Marshall J, McLeod D (1985) Reparative epiretinal fibrosis after diabetic vitrectomy. Trans Ophthalmol Soc UK 104:287-298
Chang S, Coleman D J, Lincoff H, Wilcox LM (1984) Perfluoropro- pane gas in the management of proliferative vitreoretinopathy. Am J Ophthalmol 98:180-188
Cibis PA, Becker B, Okun E, Canaan S (1962) The use of liquid silicone in retinal detachment surgery. Arch Ophthalmol 68 : 590-599
Gonvers M, Thresher R (1983) Temporary use of silicone oil in the treatment of proliferative vitreoretinopathy. Graefe's Arch Clin Exp Ophthalmol 221:46-53
Lean JS, Leaver PK, Cooling RJ, McLeod D (1982) Management of complex retinal detachments by vitrectomy and fluid/silicone exchange. Trans Ophthalmol Soc UK 102: 203-205
Leaver PK, Cooling RJ, Feretis EB, Lean JS, McLeod D (1984) Vitrectomy and fluid silicone oil exchange for giant retinal breaks: results at six months. Br J Ophthalmol 68:432-438
Scott JD (1979) A rationale for the use of liquid silicone in retinal detachment surgery. Acta XXIII Concilium Ophthalmol, part I, Kyoto 1978. Excerpta Medica, Amsterdam, pp 433-437
Scott JD (1981) Use of liquid silicone in vitrectomised eyes. Dev Ophthalmol 2:185 190
Accepted May 16, 1985
59