Embed Size (px)
Citation preview

Letter to the Editor
Shprintzen–Goldberg Syndrome With Osteopeniaand Progressive Hydrocephalus
We report on a boy with Shprintzen-Goldberg syndrome, the 12th patient de-scribed to date. In addition to the commonlydescribed anomalies of individuals withSGS, this patient also had cranial asymme-try, hypotonia, osteopenia, and hydroceph-alus. These manifestations should be in-cluded in the diagnosis and anticipatoryguidance of children with SGS. Am. J. Med.Genet. 70:450–453, 1997. © 1997 Wiley-Liss, Inc.
KEY WORDS: Shprintzen-Goldberg; osteo-penia; hydrocephalus; devel-opmental delay; arachnodac-tyly; abdominal hernias
INTRODUCTION
In 1982 Shprintzen and Goldberg reported on 2 un-related patients with a previously undescribed syn-drome comprising craniosynostosis, exophthalmos,maxillary and mandibular hypoplasia, low-set and ab-normal ears, arachnodactyly, camptodactyly, abdomi-nal hernias, infantile hypotonia, obstructive apnea,and intellectual deficit. The similarity to a patient re-ported by Sugarman and Vogel [1981] was noted. Itwas thought that these 3 unrelated patients compriseda newly described multiple malformation syndromethat has since been referred to as Shprintzen-Goldbergsyndrome (SGS).
In 1995, six additional patients were described, mostof them with the cardinal manifestations of craniosyn-ostosis or dolichocephaly, minor facial anomalies,arachnodactyly, camptodactyly, abdominal hernias,hypotonia, hydrocephalus, osteopenia, and intellectualdeficits.
We report on an additional patient with Shprintzen-Goldberg syndrome. Greater than half of reported pa-tients have been described during the past year, indi-cating that the SGS may be more common than previ-ously thought. As pediatricians and other health care
professionals become aware of the diagnostic criteria, itis likely that SGS will be diagnosed with increasingfrequency. Recommendations are made regardingevaluation and diagnosis based on the clinical findings.
CLINICAL REPORT
Our patient, the second son of nonconsanguineousparents, was born by vaginal delivery following induc-tion of labor at 40 weeks of gestation for pre-eclampsia.Birth weight was 3.37 kg (75th centile), length 50 cm(75th centile), and OFC 36 cm (>95th centile). The pa-tient was noted to have congenital anomalies, femurfracture, and respiratory distress, and was transportedto a tertiary care center.
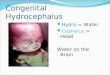
Physical examination showed plagiocephaly; down-slanting palpebral fissures; prominent eyes; small andlow-set, ‘‘cup shaped’’ ears (Fig. 1); high arched palate;normal male genitalia; arachnodactyly; camptodactyly;left femoral fracture; clubfeet; and poor suck. Primarydiagnoses considered at that time included congenitalMarfan syndrome, and Beals contractural arachnodac-tyly.
Neonatally, ophthalmologic, head ultrasonographic,renal ultrasonographic, and echocardiographic find-ings, and chromosomes were normal. A skeletal surveyshowed gracile bones, bilateral coxa valga, left femurfracture, dislocated hips with shallow acetabulae, andarachnodactyly. He was noted on two occasions to as-pirate on feeding, requiring intubation. A barium swal-low demonstrated GE reflux. An ENT evaluationshowed a deviated nasal septum. At age 21⁄2 months aNissen fundoplication, gastrostomy, and pyloroplastywere performed for poor feeding, reflux, and delayedgastric emptying. He also underwent bilateral inguinalhernia repair. Respiratory problems continued and fur-ther evaluation demonstrated a ‘‘large, floppy’’ epiglot-tis. A tracheostomy was performed at 4 months.
At age 31⁄2 half years, the patient was feeding en-tirely by mouth allowing removal of the gastrostomytube. The tracheostomy was also closed. A CT scan wasperformed following accidental head trauma whichidentified ventricles larger than demonstrated in theneonatal period. Vomiting and irritability were dispro-portionate to the small epidural hematoma beneath alinear skull fracture. Because of symptomatic, appar-ently progressive hydrocephalus, a VP shunt wasplaced.
*Correspondence to: S.J. Hassed, Section of Genetics, ArkansasChildren’s Hospital, 800 Marshall St., Little Rock, AR 72202.
Received 18 June 1996; Accepted 18 October 1996
American Journal of Medical Genetics 70:450–453 (1997)
© 1997 Wiley-Liss, Inc.

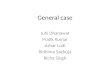
On reassessment at 4 years of age he had continuedasymmetry of skull and face, wide prominent forehead,marked midfacial hypoplasia, hypertelorism, down-slanting palpebral fissures, prominent eyes, flat nasalbridge with bulbous nose, prominent lips, mild micro-gnathia, high palate, and low-set ears with extensiveoverfolding and cupping (Fig. 2). He also had arachno-dactyly, long and finger-like thumbs, marked genuvalga, flat feet with shortness of the 4th and 5th meta-tarsals, and long and camptodactylous fifth toes. Hisstance was wide-based. The parents reported signifi-cantly improved developmental progress especiallywith regard to speech. An audiology evaluation dem-onstrated mild bilateral hearing loss, and developmen-tal assessment was consistent with a 12-month delay,largely in the area of speech. The diagnosis of Shprint-zen-Goldberg syndrome was made based on clinicalfindings as described above.
A skin sample was obtained during surgery at 21⁄2months and sent for fibrillin staining and fibroblastcultures. The result of immunofluorescent staining wasnot diagnostic for Marfan syndrome.
DISCUSSION
The Shprintzen-Goldberg syndrome was described in1982 and comprises craniosynostosis, exophthalmos,maxillary and mandibular hypoplasia, low-set and ab-normal ears, arachnodactyly, camptodactyly, abdomi-nal hernias, hypotonia, obstructive apnea, and intellec-tual deficits. Additional anomalies reported in somepatients included various skeletal abnormalities, osteo-penia, and hydrocephalus (Table I).
Nine of 12 patients had brain imaging studies, and 6were reported to have had hydrocephalus. Of the other3 patients, 2 survived infancy and both had normalpsychomotor development. The third patient had nor-
mal brain imaging at 20 days of life and died at age 5months without further brain imaging, therefore, pro-gressive hydrocephalus could not be ruled out. There isno mention of brain imaging studies in the remaining 3patients. Based on the literature and our patient, hy-drocephalus appears to be a common component ofShprintzen-Goldberg syndrome.
Eight of 9 patients studied had abnormal radio-graphic findings in addition to the previously describedpectus deformity, arachnodactyly, camptodactyly, andtalipes equinovarus (Table I). Five of those 9 patientsalso had osteopenia. Multiple skeletal abnormalitiesincluding osteopenia should be considered characteris-tic of this condition.
In 5 patients where respiratory status was reported,3 had respiratory distress or obstructive apnea and an-other had vocal cord paralysis. Our patient had ob-structive apnea during infancy which resolved. Thoughonly 6 of the patients described had respiratory statusreported, 5 of those had abnormalities which supportsthe inclusion of this trait.
In 1987 Furlong et al. described a patient with amarfanoid appearance and craniosynostosis. Findingsincluded dolichocephaly, bilateral proptosis, hypertel-orism, micrognathia, high narrow palate, low-setcupped ears, pectus carinatum, mitral valve prolapse
Fig. 1. The infant with plagiocephaly, prominent eyes, low nasalbridge, bulbous nose, and low-set anomalous ears.
Fig. 2. The patient at age 41⁄2 years, showing change of appearance.
Letter to the Editor 451

TA
BL
EI.
Su
mm
ary
ofM
anif
esta
tion
sO
bser
ved
inth
eP
atie
nt
and
Pre
viou
sly
Rep
orte
dC
ases
Man
ifes
tati
ons
No.
affe
cted
/to
tal
rep.
Ou
rpa
tien
tA
des
etal
.,pt
.1
Ade
set
al.,
pt.
2A
des
etal
.,pt
.3
Ade
set
al.,
pt.
4F
url
ong
etal
.L
acom
bean
dB
atti
nS
aal
etal
.
Sh
prin
tzen
Gol
dber
g,pt
.1
Sh
prin
tzen
Gol
dber
g,pt
.2
Su
garm
anan
dV
ogel
Kos
ztol
anyi
etal
.
Cra
nio
syn
osto
sis/
asym
met
ry8/
9+a
+a+a
++
++
+a−
Max
illa
ryh
ypop
lasi
a9/
9+
++
+P
roba
ble
++
++
Mic
rogn
ath
ia11
/11
+m
ild
++
++
mil
d+
++
++
+H
yper
telo
rism
11/1
2+
+b+
+P
roba
ble
+b−b
+b+b
++
+D
own
slan
tin
gpa
lp.
fiss
ure
s10
/10
++
++
Pro
babl
e+
++
++
Exo
phth
alm
us
10/1
1+
++
Pro
babl
e+
−+
++
++
Opt
icat
roph
y1/
3−
+−
Str
abis
mu
s4/
9−
−c−c
−c−c
++
++
Hig
har
ched
pala
te11
/12
++
++
Pro
babl
e+
−+
++
++
Low
-set
/po
st.
angu
late
dea
rs9/
9+
++
++
++
++
Sof
tau
ricl
es6/
6+d
+d+d
+d+
+C
ardi
acan
omal
ies
3/9
−T
VP
−−
+g+g
+−
−A
bdom
inal
her
nia
9/10
+e+f
+f?
+e,f
+e−
++
++
Pec
tus
defo
rmit
y8/
10−
++
+−
++
++
+A
rach
nod
acty
ly11
/12
++
++
Pro
babl
e−
++
++
++
Cam
ptod
acty
ly8/
9+
++
++
++
+−
Tal
ipes
equ
inov
aru
s5/
6+
++
−+
+H
ypot
onia
10/1
0+
++
+P
roba
ble
++
++
+In
tell
ectu
alde
fici
ts10
/12
++
++
+−
−+
++
++
Obs
tru
ctiv
eap
nea
4/6
+−
−h+
+R
esp.
dist
.R
adio
grap
hic
abn
orm
alit
ies
not
not
edab
ove
9/10
++
++
++
+−
++
Ost
eope
nia
5/6
++
++
+−
Hyd
roce
phal
us
6/9
++
++
+−
−+
−
aD
olic
hoc
eph
alic
.bP
tosi
s.c M
yopi
a.dO
verf
olde
dh
elic
es.
eIn
guin
alh
ern
ia.
f Um
bili
cal
her
nia
.gD
ilat
edao
rtic
root
.hV
ocal
cord
para
lysi
s.

with a dilated aortic root, bilateral inguinal hernia re-pair, long fingers with camptodactyly, various radio-graphic abnormalities, and normal development. Thispatient had many of the anomalies of SGS, thoughwithout neonatal hypotonia or hydrocephalus and withnormal development. Lacombe and Battin [1993] re-ported on a patient with findings of SGS, includingcraniosynostosis, micrognathia, downslanting palpe-bral fissures, strabismus, low-set ears, high arched pal-ate, dilated aortic root, arachnodactyly, camptodactyly,but without hydrocephalus, obstructive apnea, or intel-lectual deficits. The 6 patients described in 1995 [Saalet al.; Ades et al.; Kosztolanyi et al.] and our patient aretypical for SGS as originally described (Table I).
Dietz et al. [1995] postulate that SGS is allelic withMarfan syndrome. They describe two patients withSGS-like anomalies and mutations in EGF-like do-mains within the fibrillin-1 gene. The possibility of aconnective tissue abnormality in SGS is supported bythe fact that many of the findings in this condition aresimilar to those with a connective tissue component,i.e., multiple skeletal findings, cardiac defects, abdomi-nal hernias, and neonatal hypotonia. A causal effect forprogressive hydrocephalus and/or intellectual deficitshas not been determined. It will be necessary to deter-mine whether mutations in the gene responsible forSGS affect brain development in a way not encounteredin Marfan syndrome, or if the reported intellectual defi-cits are otherwise related to the progressive hydroceph-alus noted in SGS. It is also possible that the muta-tional defect is in actuality more extensive and mayinvolve contiguous genes.
ACKNOWLEDGMENTS
The authors thank Dr. Maurice Godfrey for hisevaluation of fibrillin in our patient.
REFERENCES
Ades LC, Morris LL, Power RG, Wilson M, Haan EA, Bateman JF,Milewicz DM, Sillence DO (1995): Distinct skeletal abnormalities infour girls with Shprintzen-Goldberg syndrome. Am J Med Genet 57:565–572.
Dietz HC, Sood S, McIntosh I (1995): The phenotypic continuum associatedwith FBN1 mutations includes the Shprintzen-Goldberg syndrome. AmJ Hum Genet 57(4) (suppl.):1214.
Furlong J, Kurczynski TW, Hennessy JR (1987): New marfanoid syndromewith craniosynostosis. Am J Med Genet 26:599–604.
Kosztolanyi G, Weisenbach J, Mehes K (1995): Syndrome of arachnodac-tyly, disturbance of cranial ossification, protruding eyes, feeding diffi-culties, and mental retardation. Am J med Genet 58:213–216.
Lacombe D, Battin J (1993): Marfanoid features and craniosynostosis: Re-port of one case and review. Clin Dys 2:220–224.
Saal HM, Bulas DI, Fonda Allen J, Vezina LG, Walton D, Rosenbaum KN(1995): Patient with craniosynostosis and marfanoid phenotype(Shprintzen-Goldberg syndrome) and cloverleaf skull. Am J Med Genet57:573–578.
Shprintzen RJ, Goldberg RB (1982): A recurrent pattern syndrome of cra-niosynostosis associated with arachnodactyly and abdominal hernias. JCraniofac Genet Dev Biol 2:65–74.
Sugarman G, Vogel MW (1981): Craniofacial and musculoskeletal abnor-malities—a questionable connective tissue disease. Synd Ident 7:16–17.
Susan Hassed*Kris ShewmakeCharles TeoMary CurtisUniversity of Arkansas for Medical Sciences andArkansas Children’s HospitalLittle Rock, Arkansas
Christopher CunniffDepartment of PediatricsUniversity of Arizona College of MedicineTucson, Arizona
Letter to the Editor 453