-
SHOULD ALL OBSTRUCTIVE SLEEP APNEA PATIENTS BE TREATED?
YES!
Yksel PekerMD*, PhD**
*Sleep Medicine Unit, Skaraborg Hospital, Skvde &
**University of Gothenburg, Sweden
-
OSA (Asymptomatic OSA; Non-sleepy sleep apnoeics)
OSAS (Symptomatic OSA; Sleepy sleep-apnoeics)
-
Wisconsin Sleep Cohort (age 30-60 yrs)Men Women OSA 24 %9 %
OSAS4 %2 % Young et al, N Engl J Med 1993; 328: 1230-1235
Majority of the OSA patients do not report daytime
sleepiness
-
Eight-year follow-up AHI versus baseline AHI in the Wisconsin
Sleep Cohort Study (n= 282) Young T et al, AJRCCM 2002OSA increases
by age
-
Bixler et al, AJRCCM 1998%OSAS decreases after age of 64?Do
theybecome asymptomatic? die?
-
OSA
Immediate changes
Long-term effects
-
Modified from Grote L, Schneider H, 1997
-
Acute Blood Pressure Changes in OSA - Mechanisms -
Part
SaO2
EMG
EEG
EOG
Flow
Effort
30 sec
-
REM-sleepapneatachycardiacomplete AV blockarousalmodified from
Becker et al, AJRCCM 1995
-
Cardiovascular mechanisms (I)
Repeated nocturnal hypoxemiaCoccogna G et al, 1972; Podszus T et
al, 1986
Sympathetic nervous activity Fletcher EC et al, 1987; Hedner J
et al, 1988; Narkiewicz K & Somers VK 2003 Vascular endothelial
dysfunction Carlson J et al, 1996; Remsburg S et al, 1999; Kraiczi
H et al, 2000
-
Cardiovascular mechanisms (II)
Enhanced release of superoxide from polymorphonuclear
neutrophils in OSA. Impact of CPAP. Schulz R et al, AJRCCM 2000
Plasma vascular endothelial growth factor in OSAS: Effects of
CPAP. Lavie L et al, AJRCCM 2002 Elevated levels of C-reactive
protein and interleukin-6 in patients with OSAS are decreased by
CPAP. Yokoe T et al, Circulation 2003
-
OSA & CVD
Immediate changes
Long-term effects
-
Hypnogram
00:0002:0004:0006:0008:00S4S3S2S1REMWakeMTLights
Out00:0001:0002:0003:0004:0005:0006:0007:00S4S3S2S1REMWakeMTLights
OutNormalOSA
-
Long-term complications
Cognitive dysfunctionDaytime sleepiness
Cardiovascular dysfunction
-
DAYTIME SLEEPINESS
-
Sleepy OSA patients should be treated!
No doubt!
Evidence based data on impact of treatment regarding daytime
sleepiness, quality of life!
Ballester E, et al, AJRCCM 1999Farre R, et al, Lancet 1999Benson
K, Hartz AJ. N Engl J Med 2000
-
How to treat?
-
CVD OSAObesity
-
Treatment of sleep apnea
Weight reductionGastric by-passCPAPPalatal surgeryOral
devicesTracheostomyDrugs?
-
Why to treat all OSA patients regardless daytime sleepiness?
-
Clinical and epidemiological aspects
Obstructive sleep apnea is associated withHypertensionCoronary
heart diseaseCardiac arrhythmias Heart failureStrokeDiabetes and
Insulin ResistanceMortality
-
MORTALITY
-
%Mortality in severe OSAS patients at 5 to 7-yr follow-up(AHI
5527, age 5310 yrs, BMI 325 kg/m2 at baseline)modified from Marti S
et al, ERJ 2002
-
Long-term cardiovascular outcomes in men with OSA with or
without treatment with CPAP: an observational study
Marin JM et al Lancet 2005; 365:1046-53
-
Long-term cardiovascular outcomes in men with OSA with or
without CPAP
Sleep clinic (1992-1994), PSG 1465 Simple snorers (n=377) OSA
(n=1071) CPAP recommended (n=667) CPAP accepted (n=426) Untreated
severe OSA (AHI>30, n=235)
Healthy controls (n=264) individually matched with the severe
untreated OSA for age and BMI (AHI
-
Variables HealthySnorersMild Severe CPAP men OSA OSA treated at
baseline (AHI 5-30) (AHI>30)
Patients (n) 264 377 403 235 372
AHI* n/h 1 4 18 43 42 Age yrs 49 50 50 50 50BMI* kg/m2 30 26 28
30 31Hypertens.* (%) 15 18 25 35 35Diabetes (%) 7 7 7 8 8Smokers
(%) 23 23 24 25 25
Marin JM et al, Lancet 2005
-
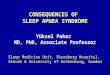
%Cardiovascular events in men during 10 yearsmodified from Marin
JM et al, Lancet 2005******
-
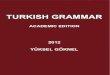
Fully adjusted Odds Ratios for cardiovascular death associated
with clinical variables
OR (95% CI)p
Age, yrs1.09 (1.04-1.12)0.001Snoring1.03 (0.31-1.84)0.88Mild
OSA1.15 (0.34-2.69)0.71Severe OSA2.87 (1.17-7.51)0.025CPAP1.05
(0.39-2.21)0.74Cardiovascular disease2.54 (1.31-4.99)0.005Marin JM
et al, Lancet 2005
-
OVERALL CARDIOVASCULAR DISEASE
-
Peker et al, AJRCCM 2002; 166: 159-65
FOURVARIABLES
6.56.756.8
4.16.727
3.3021.6
1.6016.2
Non OSA (n=122)
Efficiently treated OSA (n=15)
Incompletely treated OSA (n=37)
%
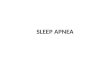
Incidence of cardiovascular disease during a 7-year follow-upin
otherwise healthy middle-aged men at baseline
Blad1
OSA (ineffectively treated)OSA (effectively treated)Non OSA
Coronary Artery Disease804
Hypertension1015
Cardiovascular Disease2118
Non OSA (n=122)Efficiently treated OSA (n=15)Incompletely
treated OSA (n=37)
Cardiovascular disease6.56.756.8
Hypertension4.16.727.0
Coronary artery disease3.3021.6
Cardiovascular event1.6016.2
-
HYPERTENSION
-
OSA as an independent risk factor for hypertension (sleep-clinic
population, n=599)
Grote et al., AJRCCM, 1999
Chart1
11.522.072.154.15
BMI (kg/m2)123.24.96
Age (years)11.831.982.98
GenderGender11.1Gender
= 40Systolic and diastolic hypertension72.654.833.919.44.8
% hypertensive patients41.660.369.170.386.2
% controlled hypertensives28.814.724.613.9811.96
< 55 -< 1010 - < 2020 - < 40> = 40
% hypertensive patients20.533.738.53553.4
< 55 -< 1010 - < 2020 - < 40> = 40
% controlled hypertensives28.814.724.613.9811.96
5 = 405 = 40
% hypertensive patients on treatment25.545.654.470.4%
hypertensive patients (total 798)41.666.770.386.2
% controlled hypertension on treatment28.820.913.9811.96%
hypertensive patients on treatment (total 599)25.545.654.470.4
% controlled hypertension on treatment (total 100 out of
599)33.825.82117.7
Sheet3
-
Control of Hypertension in OSA
Grote et al., J. Hypertension, 2000
Chart3
130.1
132.9
137.3
146.2
Systolic Blood Pressure
Age
mmHg
Systolic Blood Pressure and age in patients referred to the
Marburg Sleep Disorders Centre (n=591 patients, no antihypertensive
medication)
Chart4
83.6
86.2
88
85.1
Diastolic Blood Pressure
Age
mmHg
Diastolic Blood Pressure and age in patients referred to the
Marburg Sleep Disorders Centre (n=591, no antihypertensive
medication)
Chart5
69.8
71.2
72.6
72.5
Heart Rate
Age
bpmin-1
Heart Rate and age in patients referred to the Marburg Sleep
Disorders Centre (n=591, no antihypertensive medication)
Chart6
46.5
46.8
49.4
57.1
Pulse Pressure
age
mmHg
Pulse Pressure and age in patients referred to the Marburg Sleep
Disorders Centre (n=591, no antihypertensive medication)
Chart7
13.9
19.5
20.7
22.1
RDI
age
events/hour of sleep
OSA activity (RDI) and age in patients referred to the Marburg
Sleep Disorders Centre (n=591, no antihypertensive mediaction)
Chart8
130.183.669.8
132.986.271.2
137.38872.6
146.285.172.5
&A
Page &P
Systolic Blood Pressure
Diastolic Blood Pressure
Heart Rate
Age
mmHg/bpmin-1
Blood Pressure and Heart Rate in patients referred to the
Marburg Sleep Disorders Centre (n=591, no antihypertensive
medication)
Chart9
21.527.715.410.824.6
20.611.82517.625
25.417.516.717.522.8
14.719.619.621.724.5
1114.416.724.933
RDI-Classes
sys bp = 170
% patients
Control of systolic blood pressure in prediagnosed hypertensive
patients in relation to OSA activity (n=599)
Chart10
15.423.19.227.724.6
10.313.210.329.436.8
14.921.99.627.226.3
718.913.329.431.5
7.714.81024.443.1
dia bp < 90
dia bp 90-94
dia bp 95-99
dia bp 100-104
dia bp >= 105
RDI-Classes
% patients
Control of diastolic blood pressure in prediagnosed hypertensive
patients in relation to OSA activity (n=599)
Chart11
10.833.8
5.920.6
9.628.9
4.221
4.817.7
controlled hypertension < 140/90
controlled hypertension < 160/95
RDI Classes
% patients
Control of hypertension in relation to OSA activity (n=599)
Chart1
51.212.70.613.921.7
37.613.9216.829.7
32.814.70.921.630.2
30.8102.521.735
34.16.83.411.444.3
normotension
borderline isolated systolic hpt
isolated systolic hpt
diastolic hpt
systolic and diastolic hpt
RDI-Classes
% patients
Type of Hypertension and OSA Activity Patients referred to the
Marburg Sleep Disorders Centrewith no previous history of
hypertension (n=591)
Chart2
51.24161.8
37.643.616.82
32.853.410.32.6
30.850.815.82.5
34.134.1255.7
normotension
stage 1 hypertension
stage 2 hypertension
stage 3 hypertension
RDI Classes
% patients
Stage of Hypertension and OSA Activity Patients referred to the
Marburg Sleep Disorders Centre with no previous history of
hypertension (n=591)
Chart18
21.527.715.410.824.6
23.615.419.817.623.6
14.719.619.621.724.5
1114.416.724.933
sys bp = 170
RDI-Classes
% Patients
Chart23
15.423.19.227.724.6
13.218.79.92830.2
718.913.329.431.5
7.714.81024.443.1
dia bp < 90
dia bp 90-94
dia bp 95-99
dia bp 100-104
dia bp >= 105
RDI-Classes
% patients
Chart24
10.833.8
8.225.8
4.221
4.817.7
controlled hypertension < 140/90
controlled hypertension < 160/95
RDI-Classes
% patients
Chart25
51.212.70.613.921.7
32.814.70.921.630.2
30.8102.521.735
34.16.83.411.444.3
normotension
borderline isolated systolic hpt
isolated systolic hpt
diastolic hpt
systolic and diastolic hpt
DI-Classes
% patients
Type of Hypertension and OSA ActivityPatients referred to the
Marburg Sleep Disorders Centre with no previous history of
hypertension (n=591)
Chart26
51.24161.8
3548.813.42.3
30.850.815.82.5
34.134.1255.7
normotension
stage 1 hypertension
stage 2 hypertension
stage 3 hypertension
RDI-Classes
% patients
Stage of Hyperetnsion and OSA Activity Patients from the Marurg
Sleep Disorders Clinic with no previous history of hypertension
(n=591)
Chart28
12.70.613.921.7
14.70.921.630.2
102.521.735
6.83.411.444.3
borderline isolated systolic hpt
isolated systolic hpt
diastolic hpt
systolic and diastolic hpt
RDI Classes
% patients
Type of Hypertension and OSA Activity Newly diagnosed
hypertensive Patients referred to the Marburg Sleep Disorders
Centre (n=363)
Chart29
4161.8
48.813.42.3
50.815.82.5
34.1255.7
stage 1 hypertension
stage 2 hypertension
stage 3 hypertension
RDI-Classes
% patients
Stage of Hypertension and OSA Activity Newly diagnosed
hypertensive patients referred to the Marburg Sleep Disorders
Centre (n=363)
Sheet1
-
Stage of Hypertension and OSA
Grote et al., J Hypertens. 2001
Chart3
130.1
132.9
137.3
146.2
Systolic Blood Pressure
Age
mmHg
Systolic Blood Pressure and age in patients referred to the
Marburg Sleep Disorders Centre (n=591 patients, no antihypertensive
medication)
Chart4
83.6
86.2
88
85.1
Diastolic Blood Pressure
Age
mmHg
Diastolic Blood Pressure and age in patients referred to the
Marburg Sleep Disorders Centre (n=591, no antihypertensive
medication)
Chart5
69.8
71.2
72.6
72.5
Heart Rate
Age
bpmin-1
Heart Rate and age in patients referred to the Marburg Sleep
Disorders Centre (n=591, no antihypertensive medication)
Chart6
46.5
46.8
49.4
57.1
Pulse Pressure
age
mmHg
Pulse Pressure and age in patients referred to the Marburg Sleep
Disorders Centre (n=591, no antihypertensive medication)
Chart7
13.9
19.5
20.7
22.1
RDI
age
events/hour of sleep
OSA activity (RDI) and age in patients referred to the Marburg
Sleep Disorders Centre (n=591, no antihypertensive mediaction)
Chart8
130.183.669.8
132.986.271.2
137.38872.6
146.285.172.5
&A
Page &P
Systolic Blood Pressure
Diastolic Blood Pressure
Heart Rate
Age
mmHg/bpmin-1
Blood Pressure and Heart Rate in patients referred to the
Marburg Sleep Disorders Centre (n=591, no antihypertensive
medication)
Chart9
21.527.715.410.824.6
20.611.82517.625
25.417.516.717.522.8
14.719.619.621.724.5
1114.416.724.933
RDI-Classes
sys bp = 170
% patients
Control of systolic blood pressure in prediagnosed hypertensive
patients in relation to OSA activity (n=599)
Chart10
15.423.19.227.724.6
10.313.210.329.436.8
14.921.99.627.226.3
718.913.329.431.5
7.714.81024.443.1
dia bp < 90
dia bp 90-94
dia bp 95-99
dia bp 100-104
dia bp >= 105
RDI-Classes
% patients
Control of diastolic blood pressure in prediagnosed hypertensive
patients in relation to OSA activity (n=599)
Chart11
10.833.8
5.920.6
9.628.9
4.221
4.817.7
controlled hypertension < 140/90
controlled hypertension < 160/95
RDI Classes
% patients
Control of hypertension in relation to OSA activity (n=599)
Chart1
51.212.70.613.921.7
37.613.9216.829.7
32.814.70.921.630.2
30.8102.521.735
34.16.83.411.444.3
normotension
borderline isolated systolic hpt
isolated systolic hpt
diastolic hpt
systolic and diastolic hpt
RDI-Classes
% patients
Type of Hypertension and OSA Activity Patients referred to the
Marburg Sleep Disorders Centrewith no previous history of
hypertension (n=591)
Chart2
51.24161.8
37.643.616.82
32.853.410.32.6
30.850.815.82.5
34.134.1255.7
normotension
stage 1 hypertension
stage 2 hypertension
stage 3 hypertension
RDI Classes
% patients
Stage of Hypertension and OSA Activity Patients referred to the
Marburg Sleep Disorders Centre with no previous history of
hypertension (n=591)
Chart18
21.527.715.410.824.6
23.615.419.817.623.6
14.719.619.621.724.5
1114.416.724.933
sys bp = 170
RDI-Classes
% Patients
Chart23
15.423.19.227.724.6
13.218.79.92830.2
718.913.329.431.5
7.714.81024.443.1
dia bp < 90
dia bp 90-94
dia bp 95-99
dia bp 100-104
dia bp >= 105
RDI-Classes
% Patients
Chart24
10.833.8
8.225.8
4.221
4.817.7
controlled hypertension < 140/90
controlled hypertension < 160/95
RDI-Classes
% patients
Chart25
51.212.70.613.921.7
32.814.70.921.630.2
30.8102.521.735
34.16.83.411.444.3
normotension
borderline isolated systolic hpt
isolated systolic hpt
diastolic hpt
systolic and diastolic hpt
DI-Classes
% patients
Type of Hypertension and OSA ActivityPatients referred to the
Marburg Sleep Disorders Centre with no previous history of
hypertension (n=591)
Chart26
51.24161.8
3548.813.42.3
30.850.815.82.5
34.134.1255.7
normotension
stage 1 hypertension
stage 2 hypertension
stage 3 hypertension
RDI-Classes
% patients
Stage of Hyperetnsion and OSA Activity Patients from the Marurg
Sleep Disorders Clinic with no previous history of hypertension
(n=591)
Chart28
12.70.613.921.7
14.70.921.630.2
102.521.735
6.83.411.444.3
borderline isolated systolic hpt
isolated systolic hpt
diastolic hpt
combined systolic and diastolic hpt
RDI-Classes
% patients
Chart29
4161.8
48.813.42.3
50.815.82.5
34.1255.7
grade 1 hypertension
grade 2 hypertension
grade 3 hypertension
RDI-Classes
% patients
Sheet1
-
Lavie P et al; BMJ 2000;320:479-482OSA as a risk factor for
hypertension (sleep-clinic population, n=2677)
-
OR FOR HYPERTENSION
Odds ratio
Wald 95% CI
3.5
3.0
2.5
2.0
1.5
1.0
5
10
15
20
30
40
50
60
70
APN-HYPOPNINDEX (per hour)
Samband mellan hypertoni och apn-hypopn index hos 2452
oselekterade patienter remitterade till ett smnlaboratorium under
en 10-rs period. Odds ratio och Wald 95% KI fr hypertension
associerad med AHI niver av 5,15,30,40,50,60,och 70predikterade
genom bst anpassad multipel logistisk modell: T=e.012apn-hypopn
index+.081lder+.161manligt kn+.067BMI . Omarbetad frn Lavie et al.
BMJ 2000; 320:479-82.
-
OSA & HT in a general population
Sleep Heart Health Study Cross-sectional analysis (n=6,132)
Adjusted OR for HT 1.37 (95% CI 1.03-1.83) (AHI>30 versus
AHI
-
Incidence of HT in a general population
Wisconsin Sleep Cohort Prospective 4-yr follow-up (n=893)
AHI Adj. OR95% CI0 10.1-4.9 1.41.1-1.85.0-14.9 2.01.3-3.2>=15
2.91.5-5.6
Peppard PE et al, N Engl J Med 2000;342:1378-1384
-
Pepperell J et al, LANCET 2001; 359: 204-210Ambulatory BP after
therapeutic and subtherapeutic CPAP for OSA: a randomised parallel
trial
Normotensive & HypertensiveOSAS (n=118)More BP-reduction in
hypertensivesMore BP-reduction in severe OSAS
-
CORONARY ARTERY DISEASE
-
OSA & CAD in a general population
Sleep Heart Health Study Cross-sectional analysis (n=6,132)
Adjusted OR for CAD 1.27 (95% CI 0.99-1.62) (AHI>11 versus
AHI
-
Peker et al, Eur Resp J 1999; 14: 179-84Prevalence of risk
factors (%) OSA & Coronary Artery Disease
-
Explanatory variables associated with CAD (multivariate
analysis)
______________________________________________________________ Odds
Ratio 95 % CI p values
______________________________________________________________Current
smoking9.82.6-36.50.001Diabetes mellitus4.21.1-17.10.045Obstructive
sleep
apnea3.11.2-8.30.025______________________________________________________________
Peker et al, Eur Resp J 1999; 14: 179-84
-
Prevalence of OSA in CAD
First author; publ yrnAHI>10controlsDe Olazabal; 1982 Andreas
S; 1996Mooe T; 1996Mooe T; 1996Koehler U; 1996Peker Y; 1999Moruzzi
P; 1999Sanner BM;
200117501421027462224976%50%37%30%35%31%9%27%nonoyesyesnoyesnono
Total51837%
-
Peker et al, AJRCCM 2000; 162:81-86
-
Peker et al, AJRCCM 2000; 162:81-86
-
Hazard function of death estimated by use of Poisson modelPeker
et al, AJRCCM 2000; 162:81-86
-
Eur Resp J, in press
-
Eur Resp J, in press
-
CAD incidence in a sleep-clinic cohort at a 7-yr
follow-up***%Eur Resp J, in press
-
Probability of CAD incidence estimated by Poisson model
(Start age 49 yrs, Systolic BP 133 mmHg and Sat. min 86%)
Eur Resp J, in press.
-
Eur Resp J, in press
-
Eur Resp J, in press
-
CONCLUSIONS (I)
Recurrent obstructive events during sleep, independently or in
concert with other recognized risk factors, have harmful effects on
vascular structure and function.
CVD development and proneness to CVD complications are likely to
depend on genotypic and phenotypic factors.
Not only may OSA induce a CVD but also the events in themselves
may aggravate an already existing CVD.
-
CONCLUSIONS (II)
OSA should be included among factors considered in the primary
and secondary prevention models of CVD.
OSA should be treated not only to eliminate daytime sleepiness.
Treatment may also have a beneficial prognostic impact by reducing
cardiovascular morbidity in OSA.
-
SHOULD ALL OBSTRUCTIVE SLEEP APNEA PATIENTS BE TREATED?
YES!
*********************