Embed Size (px)
Citation preview

1 3
Knee Surg Sports Traumatol ArthroscDOI 10.1007/s00167-016-3982-8
KNEE
Short-interval two-stage approach to primary total knee arthroplasty for acutely septic osteoarthritic knees
Bettina Hochreiter1 · Carol Strahm2 · Henrik Behrend1
Received: 5 August 2015 / Accepted: 5 January 2016 © European Society of Sports Traumatology, Knee Surgery, Arthroscopy (ESSKA) 2016
joint, accounting for 40–50 % of reported cases [4, 34]. Osteoarthritis as well as other previous joint pathologies are considered risk factors for bacterial seeding [19]. The pre-sent standard of care of an acutely infected knee consists of joint decompression, arthroscopic irrigation, debridement and systemic antibiotics, whereas open procedures are considered for chronic septic arthritis or persistent infec-tion after arthroscopic intervention [9, 19, 35, 37]. Treat-ment strategies for advanced knee osteoarthritis and coex-istent joint infection are not well established. Therapeutic approaches include debridement and administration of high concentrations of systemic and local antibiotics as the first stage before considering total knee arthroplasty (TKA) [12, 20, 21], as well as arthrodesis or amputation in cases where previous surgical attempts have failed [36]. Although in the situation of periprosthetic joint infection (PJI) the two-stage approach using antibiotic-loaded cement spacers, later followed by revision TKA has been studied exten-sively [10, 11, 14, 17, 26, 33, 38], only few case reports on two-stage TKA for arthritis with coexistent joint infection have been published [13, 20–23, 32]. Research presented thus far reports consistent infection eradication therefore suggesting that a two-stage approach is a viable option in these rare situations. However, isolated pathogens, spacers used, interval between stages, as well as peri- and postop-erative choice and length of antimicrobial treatment were diverse and often not specified (Table 1).
This paper reports on a method of implementing a two-stage TKA with intervening articulating cement spacers to treat two patients with acute Staphylococcus aureus knee joint infection and pre-existing end-stage osteoarthritis. In contrast to previous literature, this case report provides a detailed description of pre-, peri-, and postoperative intra-venous, oral and local antimicrobial management with a preoperatively known, homogenous and common pathogen
Abstract Treatment strategies for advanced knee osteo-arthritis with coexistent joint infection are not well estab-lished. While in periprosthetic joint infection the two-stage approach has been studied extensively, only few case reports on two-stage total knee arthroplasty (TKA) for knee osteoarthritis with coexistent joint infection have been published. The purpose of this paper was to report on our method of implementing a two-stage TKA with inter-vening antibiotic-loaded articulating cement spacers and a short interval between first- and second-stage procedures to treat two patients with Staphylococcus aureus-infected end-stage knee osteoarthritis. Consistent infection eradi-cation was found at a 1-year follow-up with postoperative range of motion and knee scores comparing favourably with those of other case series.
Level of evidence V.
Keywords Knee · TKR · Total knee replacement · Total knee arthroplasty · Short interval · Two-stage TKA · Septic osteoarthritis
Introduction
Septic arthritis remains a serious problem in orthopaedic surgery with the knee being the most commonly affected
* Henrik Behrend [email protected]
1 Department of Orthopaedic Surgery and Traumatology, Cantonal Hospital St. Gallen, 9007 St. Gallen, Switzerland
2 Department of Infectious Diseases and Infection Control, Cantonal Hospital St. Gallen, 9007 St. Gallen, Switzerland

K
nee Surg Sports Traumatol A
rthrosc
1 3
Table 1 Overview of current literature
Author No. patients
Preoperative organism isolated from bacterial culture
Spacer Antibiotics between stages
Time between stages
Peri- and Postoperative choice/length of antibi-otic administration
Follow-up Infection eradication
Nazarian et al. [23]
14 S. aureus (3)S. epidermidis (2)Streptococcus spp. (2)E. coli (1)None (6)
Non-articulatingPMMA(2,4 g TOB + 1 g
VAN per 40 g cement)
6 weeks IVcontinued p.o.
for remainder of explantation period
3.1 months 5 days IV6 months p.o. (6
patients for life)
4.5 years Yes
Shaikh et al. [32]
15 Candida spp. (2)P. aeruginosa (1)MRSA (2)MSSA (1)None (7)
ArticulatingPMMAIf pathogen unknown:4 g VAN + 2 g STR per
40 g cementIf pathogen known: anti-
biotics were modified to achieve organism-specific coverage
2 weeks IVcontinued p.o.
when possible duration not specified
5.6 months2 patients denied
TKA and kept spacer
14 days IV4–12 weeks p.o.
4 years Yes
Moyad [22] 1 C. pseudodiphteriticum ArticulatingPMMA(3 g TOB + 2 g VAN per
40 g cement)
6 weeks IV PCN 2.5 months NA 18 months Yes
Kirpalani et al. [13] 5 NA NA NA NA NA 3.2 years Yes
Mirza et al. [21] 2 First case—NA Non-articulating NA 2.5 and 3 months NA 5 and 6 years Yes
Second case— S. aureus
GEN beads and antibiotic-loaded PMMA “hamburger”
Matsumoto et al. [20]
1 MRSA HA blocks (4,5 g VAN) 2 weeks IV 3 months NA 3 years Yes
Immobilization/no weight bearing with fixateur externe
2 weeks oral not further specified
MRSA methicillin resistant S. aureus NA not available
MSSA methicillin-sensitive S. aureus PMMA polymethylmethacrylate
TOB tobramycin VAN vancomycin
GEN gentamicin STR streptomycin
HA hydroxyapatite PCN penicillin

Knee Surg Sports Traumatol Arthrosc
1 3
in both cases and use of a much shorter interval of three and 4 weeks respectively between the first- and second-stage procedures.
Case reports
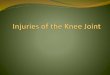
Between 2013 and 2014, two patients presenting with advanced knee osteoarthritis and coexistent acute joint infection were treated with the two-stage approach (Table 2). The diagnosis of a septic joint was based pri-marily on positive intraoperative cultures as well as clini-cal presentation, laboratory inflammatory markers (white blood cell count, thrombocytes, c-reactive protein), blood cultures and joint aspiration. Conventional X-rays were performed confirming pre-existing osteoarthritis (Fig. 1), and arthroscopy showed articular cartilage defects grade IV [25] in both cases.
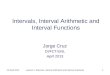
The first patient (61, male) presented with assumedly traumatic exacerbation of chronic posttraumatic osteoar-thritis. Three days later, he was referred to another hospital, where septic arthritis with methicillin-sensitive S. aureus (MSSA) was diagnosed. Two arthroscopic irrigations and debridement surgeries were performed. Four days later, the patient was admitted to our tertiary-care centre in a septic state with persistent joint infection and presumed endocar-ditis. Open arthrotomy was performed without delay. One week later, due to persistent infection, first-stage procedure with open medial parapatellar arthrotomy, radical synovec-tomy and complete debridement of infected and necrotic tissue was performed. Femoral and tibial bone cuts were made in preparation for primary TKA using extramedullary cutting guides and a soft tissue-tensioning device. An artic-ulating cement spacer was then constructed using Copal® G+V (Palacos R mixed with 2 g vancomycin and 0.5 g gentamicin per 40 g cement, Heraeus Medical, Zurich, Switzerland) adding 1 g vancomycin per 40 g of cement (Fig. 2). The cement was mixed without vacuum using a “poor mixing technique” to improve antibiotic elution [16]. The spacer was created manually and was applied onto non-dried bone surfaces after waiting 6 min for the cement to be more solidified to prevent complete bonding of the spacer and the bone. A polyethylene inlay was inserted between the femoral and the tibial spacer component.
Partial weight bearing was allowed and passive motion was guided by physiotherapists. Primary TKA was per-formed 4 weeks later when the laboratory inflammation markers had normalized and there was no further clinical evidence of infection (reddened and hyperthermic joint, drainage from the wound, unreasonable knee pain). Intra-operatively, thorough debridement and Jet-Lavage with Lavasept® (B. Braun Melsungen AG) were performed again, the cement spacer was retrieved and computer
navigated, and cemented TKA (ATTUNE® Primary Total Knee System, DePuy Synthes, Warsaw, IN) was implanted.
One of two blood cultures on admission and all seven (7/7) biopsies taken during the first open arthrotomy were positive for MSSA. On the fourth day of adequate antibi-otic treatment, blood cultures were sterile. Endocarditis was excluded by transesophageal echocardiography (TEE). Systemic antibiotic treatment consisted of flucloxacillin 6 × 2 g/day IV. Two out of five (2/5) biopsies taken dur-ing first-stage procedure showed growth of MSSA. For implantation of primary TKA, prophylaxis with vanco-mycin 1 g was applied [3]. Postoperatively vancomycin was continued and flucloxacillin was stopped. 7 days after TKA implantation, treatment was changed to flucloxacil-lin 4 × 2 g/day IV and rifampin 2 × 450 mg p.o. since biopsies (0/5) showed no growth and wounds were dry [1, 30]. Ten days after TKA implantation IV, treatment was stopped and a combination therapy with oral ciprofloxacin 2 × 750 mg/day and rifampin 2 × 450 mg/day was contin-ued for another 18 weeks [24]. Laboratory findings during hospitalization and follow-up period were followed closely. Clinical and radiological follow-ups were conducted at 8 weeks and 1 year postoperatively.
The second patient (74, male) presented with acute immobilizing knee pain and known severe posttraumatic osteoarthritis. Septic arthritis was confirmed by positive Gram stain. Arthroscopic irrigation and debridement were performed immediately and an empirical antimicrobial treatment with amoxicillin/clavulanic acid 3 × 2.2 g/day was started after biopsies were taken. Intraoperative cul-tures confirmed MSSA (6/6), and antibiotic therapy was changed to flucloxacillin 6 × 2 g/day IV. Two-stage arthro-plasty was indicated, and the first-stage procedure was per-formed 3 days later. Intra- and postoperative protocols were implemented as described in the first case.
Blood cultures taken 3 days after admission were nega-tive, a TEE was performed and endocarditis excluded. After 3 weeks of IV flucloxacillin, computer navigated TKA (LCS® Complete™ Knee System, DePuy Synthes, War-saw, IN) was performed. A preoperative prophylaxis with vancomycin 1 g was applied and treatment with flucloxacil-lin was continued perioperatively. When wounds were dry, rifampin 2 × 450 mg p.o. was added to the regimen [1, 30]. Biopsies showed no growth (0/5). After 10 days, a com-bination therapy with oral ciprofloxacin 2 × 750 mg/day and rifampin 2 × 450 mg/day was established for another 10 weeks [24, 27]. Otherwise, the same postoperative pro-tocol was applied.
ROM, WOMAC, VAS and EQ-5D were evaluated at follow-up (Table 3). In both cases, there were no clini-cal signs of recurrent infection, and radiographs showed a properly aligned TKA with no evidence of loosening at

K
nee Surg Sports Traumatol A
rthrosc
1 3
Table 2 Patient characterization and therapy
Age/sex Comorbidities Pathogen Previous knee surgeries
Antibiotics before first stage
Spacer Antibiotics between stages
Time between stages
Peri- and postoperative choice/length of antibi-otic admin.
1 61/M Prostate cancer MSSA 32 Arthroscopic1 Open arthrotomy
AMOX/CLAV IV 3 × 2.2 g/day
FLOX IV6 × 2 g/day
PMMA (3 g VAN and 0.5 g GEN per 40 g cement)
FLOX IV 6 × 2 g/day 4 weeks Prophylaxis with VANFollowed by VAN for
7 daysThen FLOX 4 × 2 g/
day IV and RIF 2 × 450 mg p.o. for 3 days
Then CIP 2 × 750 mg/day and RIF 2 × 450 mg/day p.o. for 18 weeks
2 74/M Diabetes mellitus MSSA 1Arthroscopic
AMOX/CLAV p.o. PMMA (3 g VAN and 0.5 g GEN per 40 g cement)
FLOX IV 6 × 2 g/day 3 weeks Prophylaxis with VANThen FLOX 6 × 2 g/day
IV for 5 daysThen FLOX 6 × 2 g and
RIF 2 × 450 mg p.o. for 5 day
Then CIP 2 × 750 mg/day and RIF 2 × 450 mg/day p.o. for 10 weeks
AMOX/CLAV amoxicillin and clavulanic acid MSSA methicillin-sensitive Staphylococcus aureus
GEN gentamicin VAN vancomycin (targeted trough levels 15–20 mg/l)
PMMA polymethyl methacrylate FLOX flucloxacillin
CIP ciprofloxacin RIF rifampin

Knee Surg Sports Traumatol Arthrosc
1 3
1-year follow-up. Informed consent was obtained from all individual participants included in the study.
Discussion
There are limited therapeutic options and few reports in the literature regarding the infected osteoarthritic knee joint
[12]. Due to the paucity of data, there are no specific guide-lines for this rare but challenging situation [23]. Two retro-spective studies with a reasonably sized patient group have been published [23, 32].
Nazarian et al. [23] reported a highly successful two-stage approach to primary TKA in a series of 14 patients with septic knee arthritis or chronic periarticular osteo-myelitis using a non-articulating antibiotic-loaded cement spacer with an average interval of 3.1 months between spacer implantation and TKA. However, while surgical management was standardized, the infectious etiologies were diverse and antibiotic management was not specified.
Shaikh et al. [32] reported infection control and good results in a proof-of-concept series of 13 patients with a two-stage approach using articulating antibiotic cement spacers and subsequent TKA with an average interval of 5.6 months. Again, antibiotic treatment was not further described. Besides the studies of Nazarian et al. and Shaikh et al., four case reports with consistent results have been published [13, 20–22].
The reported success rate of two-stage revision arthro-plasty for periprosthetic knee joint infections has been approximately 90 % in many series [28]. Outcomes of aforementioned case studies compare to those of two-stage revision surgery for other indications. However, previously published reports use an interval of 1.5 to 8.2 months, with some patients even declining to have definitive reconstruc-tion with TKA and retaining the spacer. On the contrary, if prosthesis cannot be retained [24, 42], latest findings support a trend towards short-interval two-stage exchange or even one-stage exchange in PJIs. In their recently pub-lished, comprehensive study, Zahar et al. [40] reported an infection control rate of 93 % and good clinical results in a retrospective series using a one-stage approach, combining aggressive debridement including the collateral ligaments and posterior capsule with a rotating hinge implant at a 10-year follow-up and very short systemic antimicrobial treatment.
These findings have encouraged us to use the two-stage approach with a much shorter interval for the arthritic knee with coexistent infection based on the treatment concept in PJI of Zimmerli et al. [42]. Consistent infection eradication was found with postoperative range of motion (ROM) and knee scores comparing favourably with those of other case series [13, 20–23, 32].
The optimal timeframe between explantation and reimplantation in PJI’s is not clearly defined and varies between 2 weeks and several months [29]. In short-interval exchanges, the prosthesis is implanted in a potentially non-sterile area. Therefore, prolonged postoperative antibiotic treatment against adherent bacteria is considered necessary [29]. In-vitro studies and experimental models of foreign body infection with staphylococci showed most antibiotics
Fig. 1 Preoperative X-ray of infected, osteoarthritic knee
Fig. 2 Articulating spacer

Knee Surg Sports Traumatol Arthrosc
1 3
were inefficient against adherent bacteria, whereas rifampin was consistently effective [41]. The importance of rifampin-based combination therapy was proven in a pro-spective study of PJI by Zimmerli et al. [43] and supported by further retrospective case studies with success rates over 70 % [5, 15].
According to Anagnostakos et al. [2], the release of very high therapeutically effective antibiotic concentrations is limited to a few days with PMMA cement. These results would seem to suggest that over long intervals, biofilm formation on a spacer might be possible and could lead to persistent infection or reinfection [18, 29]. Therefore, the purpose of a long-term interval may be questioned.
Furthermore, reducing the period of time in which the patient is hospitalized and antibiotics are administered cuts costs and reduces the development of resistances and com-plications associated with the therapy [31, 39].
Studies have shown the advantages of using an articu-lating spacer over a static spacer during the treatment of infected TKAs [6–8, 26]. We believe that a shorter inter-val in combination with using articulating spacers pro-vides better peri- and postoperative functional outcome and reduces the risk of arthrofibrosis.
However—despite the favourable outcome—our study has some limitations. These results are based on a small sample size, a retrospective study design and a short fol-low-up. The follow-up period was not long enough to iden-tify long-term issues such as recurrent or residual infection or failure of the prosthesis. Nonetheless we believe our case report offers valuable information for the clinician due to the provided detailed description of the antimicrobial treatment regimen used in two highly specific but similar cases and the general lack of guidelines in this situation. It is important to note that this approach was used for MSSA-infected end-stage osteoarthritis only and is not a substi-tute for open or arthroscopic debridement. It relies on the rifampin-based antimicrobial treatment regimen. Caution must be applied when transferring this treatment concept to
other pathogens or resistances and further studies need to be conducted.
Conclusion
These results show that a short-interval two-stage TKA in MSSA-infected end-stage osteoarthritic knees in combina-tion with rifampin-based antimicrobial treatment regimen appears to be an effective method to eradicate infection and maintain knee function.
References
1. Achermann Y, Eigenmann K, Ledergerber B, Derksen L, Rafeiner P, Clauss M, Nuesch R, Zellweger C, Vogt M, Zimmerli W (2013) Factors associated with rifampin resistance in staphy-lococcal periprosthetic joint infections (PJI): a matched case–control study. Infection 41(2):431–437
2. Anagnostakos K, Wilmes P, Schmitt E, Kelm J (2009) Elution of gentamicin and vancomycin from polymethylmethacrylate beads and hip spacers in vivo. Acta Orthop 80(2):193–197
3. Anderson DJ, Podgorny K, Berrios-Torres SI, Bratzler DW, Del-linger EP, Greene L, Nyquist AC, Saiman L, Yokoe DS, Maraga-kis LL, Kaye KS (2014) Strategies to prevent surgical site infec-tions in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol 35(Suppl 2):S66–S88
4. Dearborn JT, Jergesen HE (1996) The evaluation and initial man-agement of arthritis. Prim Care 23(2):215–240
5. El Helou OC, Berbari EF, Lahr BD, Eckel-Passow JE, Razonable RR, Sia IG, Virk A, Walker RC, Steckelberg JM, Wilson WR, Hanssen AD, Osmon DR (2010) Efficacy and safety of rifampin containing regimen for staphylococcal prosthetic joint infections treated with debridement and retention. Eur J Clin Microbiol Infect Dis 29(8):961–967
6. Emerson RH Jr, Muncie M, Tarbox TR, Higgins LL (2002) Comparison of a static with a mobile spacer in total knee infec-tion. Clin Orthop Relat Res 404:132–138
7. Fehring TK, Odum S, Calton TF, Mason JB (2000) Articulating versus static spacers in revision total knee arthroplasty for sepsis. the Ranawat Award. Clin Orthop Relat Res 380:9–16
8. Freeman MG, Fehring TK, Odum SM, Fehring K, Griffin WL, Mason JB (2007) Functional advantage of articulating versus static spacers in 2-stage revision for total knee arthroplasty infec-tion. J Arthroplasty 22(8):1116–1121
9. Goldenberg DL (1998) Septic arthritis. Lancet 351(9097):197–202
10. Jiranek WA, Waligora AC, Hess SR, Golladay GL (2015) Sur-gical treatment of prosthetic joint infections of the hip and knee: Changing paradigms? J Arthroplasty. doi:10.1016/j.arth.2015.03.014
11. Kaminski A, Citak M, Schildhauer TA, Fehmer T (2014) Suc-cess rates for initial eradication of peri-prosthetic knee infection treated with a two-stage procedure. Ortop Traumatol Rehabil 16(1):11–16
12. Katz LM, Lewis RJ, Borenstein DG (1987) Successful joint arthroplasty following Proteus morganii (Morganella morganii) septic arthritis: a four-year study. Arthritis Rheum 30(5):583–585
13. Kirpalani PA, In Y, Choi NY, Koh HS, Kim JM, Han CW (2005) Two-stage total knee arthroplasty for non-salvageable
Table 3 Range of motion and outcome scores at initial presentation and follow-up
Patient Initial 8 weeks 1 year
ROM 1 60/0/0° 110/0/0° 110/0/0°
2 50/0/0° 90/5/0° 105/0/0°
WOMAC 1 – 1.1 8.9
2 – 3.9 4.3
VAS 1 – 90 80
2 – 80 80
EQ-5D 1 – 1 1
2 – 0.9 0.9

Knee Surg Sports Traumatol Arthrosc
1 3
septic arthritis in diabetes mellitus patients. Acta Orthop Belg 71(3):315–320
14. Kuzyk PR, Dhotar HS, Sternheim A, Gross AE, Safir O, Back-stein D (2014) Two-stage revision arthroplasty for management of chronic periprosthetic hip and knee infection: techniques, con-troversies, and outcomes. J Am Acad Orthop Surg 22(3):153–164
15. Laffer RR, Graber P, Ochsner PE, Zimmerli W (2006) Out-come of prosthetic knee-associated infection: evaluation of 40 consecutive episodes at a single centre. Clin Microbiol Infect 12(5):433–439
16. Lewis G (2009) Properties of antibiotic-loaded acrylic bone cements for use in cemented arthroplasties: a state-of-the-art review. J Biomed Mater Res Part B Appl Biomater 89B(2):558–574
17. Mahmud T, Lyons MC, Naudie DD, Macdonald SJ, McCal-den RW (2012) Assessing the gold standard: a review of 253 two-stage revisions for infected TKA. Clin Orthop Relat Res 470(10):2730–2736
18. Mariconda M, Ascione T, Balato G, Rotondo R, Smeraglia F, Costa GG, Conte M (2013) Sonication of antibiotic-loaded cement spacers in a two-stage revision protocol for infected joint arthroplasty. BMC Musculoskelet Disord 14:193
19. Mathews CJ, Weston VC, Jones A, Field M, Coakley G (2010) Bacterial septic arthritis in adults. Lancet 375(9717):846–855
20. Matsumoto K, Itokazu M, Uemura S, Takigami I, Naganawa T, Shimizu K (2007) Successful joint arthroplasty after treatment of destructive MRSA arthritis of the knee using antibiotic-loaded hydroxyapatite blocks: a case report. Arch Orthop Trauma Surg 127(1):47–50
21. Mirza AH, Noble J, Teanby D (2000) Infected knee treated by total knee arthroplasty. Knee 7(3):171–174
22. Moyad TF (2013) Two-stage arthroplasty for the treatment of chronic osteomyelitis after routine arthroscopic knee surgery. Orthopedics 36(1):e109–e112
23. Nazarian DG, de Jesus D, McGuigan F, Booth RE Jr (2003) A two-stage approach to primary knee arthroplasty in the infected arthritic knee. J Arthroplasty 18(7 Suppl 1):16–21
24. Osmon DR, Berbari EF, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, Rao N, Hanssen A, Wilson WR, Infectious Dis-eases Society of A (2013) Executive summary: diagnosis and management of prosthetic joint infection: clinical practice guide-lines by the Infectious Diseases Society of America. Clin Infect Dis 56(1):1–10
25. Outerbridge RE (1961) The etiology of chondromalacia patellae. J Bone Joint Surg Br 43-B:752–757
26. Pelt CE, Grijalva R, Anderson L, Anderson MB, Erickson J, Peters CL (2014) Two-stage revision TKA is associated with high complication and failure rates. Adv Orthop 2014:659047
27. Puhto AP, Puhto T, Syrjala H (2012) Short-course antibiotics for prosthetic joint infections treated with prosthesis retention. Clin Microbiol Infect 18(11):1143–1148
28. Romano CL, Gala L, Logoluso N, Romano D, Drago L (2012) Two-stage revision of septic knee prosthesis with articulating
knee spacers yields better infection eradication rate than one-stage or two-stage revision with static spacers. Knee Surg Sports Traumatol Arthrosc 20(12):2445–2453
29. Sendi P, Zimmerli W (2011) Challenges in periprosthetic knee-joint infection. Int J Artif Organs 34(9):947–956
30. Sendi P, Zimmerli W (2012) Antimicrobial treatment concepts for orthopaedic device-related infection. Clin Microbiol Infect 18(12):1176–1184
31. Senthi S, Munro JT, Pitto RP (2011) Infection in total hip replacement: meta-analysis. Int Orthop 35(2):253–260
32. Shaikh AA, Ha CW, Park YG, Park YB (2014) Two-stage approach to primary TKA in infected arthritic knees using intra-operatively molded articulating cement spacers. Clin Orthop Relat Res 472(7):2201–2207
33. Shanmugasundaram S, Ricciardi BF, Briggs TW, Sussmann PS, Bostrom MP (2014) Evaluation and management of peripros-thetic joint infection-an international, Multicenter Study. HSS J 10(1):36–44
34. Smith JW, Piercy EA (1995) Infectious arthritis. Clin Infect Dis 20(2):225–230 (quiz 231)
35. Stutz G, Kuster MS, Kleinstuck F, Gachter A (2000) Arthro-scopic management of septic arthritis: stages of infection and results. Knee Surg Sports Traumatol Arthrosc 8(5):270–274
36. Waldman BJ, Mont MA, Payman KR, Freiberg AA, Windsor RE, Sculco TP, Hungerford DS (1999) Infected total knee arthro-plasty treated with arthrodesis using a modular nail. Clin Orthop Relat Res 367:230–237
37. Wang C, Lee YH, Siebold R (2014) Recommendations for the management of septic arthritis after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 22(9):2136–2144
38. Wang KH, Yu SW, Iorio R, Marcantonio AJ, Kain MS (2015) Long term treatment results for deep infections of total knee arthroplasty. J Arthroplasty. doi:10.1016/j.arth.2015.04.008
39. Whittaker JP, Warren RE, Jones RS, Gregson PA (2009) Is pro-longed systemic antibiotic treatment essential in two-stage revi-sion hip replacement for chronic Gram-positive infection? J Bone Joint Surg Br 91(1):44–51
40. Zahar A, Kendoff DO, Klatte TO, Gehrke TA (2015) Can Good Infection Control Be Obtained in One-stage Exchange of the Infected TKA to a Rotating Hinge Design? 10-year Results. Clin Orthop Relat Res 474(1):81–87
41. Zimmerli W, Frei R, Widmer AF, Rajacic Z (1994) Microbiologi-cal tests to predict treatment outcome in experimental device-related infections due to Staphylococcus aureus. J Antimicrob Chemother 33(5):959–967
42. Zimmerli W, Trampuz A, Ochsner PE (2004) Prosthetic-joint infections. N Engl J Med 351(16):1645–1654
43. Zimmerli W, Widmer AF, Blatter M, Frei R, Ochsner PE (1998) Role of rifampin for treatment of orthopedic implant-related staphylococcal infections: a randomized controlled trial. Foreign-Body Infection (FBI) Study Group. JAMA 279(19):1537–1541













![Interval Notation: ], not interval notationpgrant.weebly.com/uploads/2/3/2/7/23274454/6.3b_interval_notation.… · •Interval Notation: Uses different brackets to indicate an interval](https://img.pdfslide.us/doc/110x75/5f8344624904df613146ef90/interval-notation-not-interval-ainterval-notation-uses-different-brackets.jpg)