Embed Size (px)
Citation preview

ShockShock
Year 4 TutorialsYear 4 Tutorials
A B A B C C D ED E

Objectives:Objectives:
What is shock?What is shock?
Types of shockTypes of shock
Management principlesManagement principles

Shock Definition:Shock Definition:
State of inadequate tissue perfusion and tissue State of inadequate tissue perfusion and tissue oxygenation as a result of a deficiency in the oxygenation as a result of a deficiency in the
circulationcirculation

Types of Shock:Types of Shock:
Distributive – SepticDistributive – Septic
AnaphylacticAnaphylactic
NeurogenicNeurogenic CardiogenicCardiogenic Obstructive –Obstructive – Tension pneumothorax Tension pneumothorax
Cardiac tamponadeCardiac tamponade HypovolaemicHypovolaemic

BP = CO x SVRBP = CO x SVR
HR x SVHR x SVNormal vascular tone
determined by sympathetic innervation
•Contractility•Preload (ventricle stretch)•Afterload
CARDIAC PHYSIOLOGY

Distributive - SepsisDistributive - Sepsis
SIRS = 2 of SIRS = 2 of RR > 20 breaths per minute RR > 20 breaths per minute WCC < 4 or > 12 WCC < 4 or > 12 Heart rate > 90 beats per minute Heart rate > 90 beats per minute Temperature: Fever > 38.0 °C or < 36.0 °CTemperature: Fever > 38.0 °C or < 36.0 °C
Sepsis = SIRS + Evidence of infectionSepsis = SIRS + Evidence of infection

Distributive - SepticDistributive - Septic
Massive vasodilationMassive vasodilation BP = CO x BP = CO x SVR ( )SVR ( )
Often dehydratedOften dehydrated
Fluids & antibiotics, Fluids & antibiotics,
Vasoconstrictors.Vasoconstrictors.

Distributive - AnaphylaxisDistributive - Anaphylaxis
Massive vasodilationMassive vasodilation
Type 1 hypersensitivityType 1 hypersensitivity
Treatment:Treatment: Fluids, adrenaline, Fluids, adrenaline,
chlorphenamine, steroidschlorphenamine, steroids ?Anaesthetist?Anaesthetist

Distributive - Neurogenic Distributive - Neurogenic
Massive vasodilationMassive vasodilation
Loss of sympathetic Loss of sympathetic vascular tone.vascular tone.
Fluids and Fluids and vasoconstrictors.vasoconstrictors.

Cardiogenic shockCardiogenic shock
PUMP failure!PUMP failure! Cannot empty pumpCannot empty pump
BP = BP = CO CO x SVRx SVR
CO = CO = HRHR x x SVSV ( contractility)( contractility)
Causes:Causes: Acute MIAcute MI
Large InfarctionLarge Infarction Papillary muscle rupturePapillary muscle rupture
Other ConditionsOther Conditions Septic shockSeptic shock MyocarditisMyocarditis Arrhythmias Arrhythmias Drugs – eg beta-blocker Drugs – eg beta-blocker
overdoseoverdose Myocardial contusionMyocardial contusion

Cardiogenic shockCardiogenic shock
Treat underlying Treat underlying cause if possiblecause if possible
Inotropes.Inotropes. Balloon pumpBalloon pump

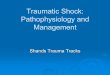
Obstructive –Tension PneumothoraxObstructive –Tension Pneumothorax
Accumulation of air Accumulation of air under pressure in the under pressure in the pleural space. pleural space.
1-way valve1-way valve
Mediastinal shift: Mediastinal shift: preload & afterload = preload & afterload = SV SV

Obstructive –Tension PneumothoraxObstructive –Tension Pneumothorax
Treatment:Treatment: Needle decompressionNeedle decompression Chest drainChest drain

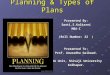
Obstructive – Cardiac Tamponade Obstructive – Cardiac Tamponade
Accumulation of fluid in Accumulation of fluid in the pericardial space, the pericardial space, resulting in reduced resulting in reduced ventricular fillingventricular filling
Rapid filling of only 150ml Rapid filling of only 150ml causes compromisecauses compromise

Obstructive – Cardiac Tamponade Obstructive – Cardiac Tamponade
Becks triad:Becks triad: increased jugular venous increased jugular venous
pressure, pressure, hypotension hypotension diminished heart sounds.diminished heart sounds.
Treatment: needle Treatment: needle pericardiocentesispericardiocentesis

Hypovolaemic ShockHypovolaemic Shock
The system is DRY.The system is DRY. Causes:Causes:
HaemorrhageHaemorrhage SepsisSepsis D&VD&V
BP = BP = COCO x SVR x SVR CO = HR x CO = HR x SVSV

Hypovolaemic / HaemorrhagicHypovolaemic / Haemorrhagic
Where is the Blood?Where is the Blood?
RevealedRevealed On the floor, at the sceneOn the floor, at the scene
ConcealedConcealed ChestChest Peritoneal/PelvisPeritoneal/Pelvis Long bonesLong bones RetroperitoneumRetroperitoneum

Hypvolaemic shock management:Hypvolaemic shock management:
Treat underlying cause Treat underlying cause haemorrhage control – 1haemorrhage control – 1stst aid, angio, theatre aid, angio, theatre
Venous access / fluidsVenous access / fluids
Fluid replacementFluid replacement

Vascular access:Vascular access:
TWO TWO large venflonslarge venflons
Where? Where? Anticubital fossaAnticubital fossa
Consider IOConsider IO Take samples – X-matchTake samples – X-match

Initial fluid therapy:Initial fluid therapy:
CrystalloidCrystalloid
ColloidColloid
Consider warmingConsider warming
Cross matchedCross matched
Type specificType specific
‘‘O’ negativeO’ negative
Massive transfusion Massive transfusion protocolprotocol

Response to fluid treatment:Response to fluid treatment:
General General
Urine - 30ml / hour (0.5mg/kg)Urine - 30ml / hour (0.5mg/kg)
Acid / Base balance (lactic acidosis)Acid / Base balance (lactic acidosis)

Shock summaryShock summary
Distributive – Distributive – vasodilation - reduced vasodilation - reduced
SVRSVR
Cardiogenic – Cardiogenic – reduced heart rate / reduced heart rate /
stroke volume - pump stroke volume - pump failurefailure
Obstructive – Obstructive – reduced stroke reduced stroke
volume – blood canvolume – blood can’’t t get in or outget in or out
Hypovolaemic –Hypovolaemic – reduced stroke reduced stroke
volume - lack of blood volume - lack of blood volumevolume
May be a combination

Shock summaryShock summary
ABCsABCs Assess degree and causeAssess degree and cause Intervene: Intervene:
Treat underlying causeTreat underlying cause Maintain CO and SVR - fluids, vasocostictors, Maintain CO and SVR - fluids, vasocostictors,
inotropesinotropes ReassessReassess Get HELPGet HELP

QuestionsQuestions
??A&E Department, Aberdeen Royal Infirmary
24