Embed Size (px)
Citation preview

Page 1 of 24
Module D
Sepsis, Septic
Shock, and DIC
NUR 203

Page 2 of 24
Shock
Patho: a response to poor tissue oxygenation
Etiology: Any problem that impairs oxygen delivery to tissues and organs
can start the syndrome of shock; if shock progresses the hypoxia can lead
to multiple organ dysfunction syndrome (MODS) and death
Key Features:
Respiratory Neuro Integumentary Kidney ↑ respiratory rate
Shallow depth of
respirations
↑ Paco2; ↓ PaO2
Cyanosis,
especially around
lips & nail beds
Anxiety
Restlessness
↑ Thirst
Cool to cold
Pale to mottled to
cyanotic
Moist, Clammy
Mouth dry; pastelike
coating present
↓ urine output
↑ specific gravity
Sugar & acetone
present in urine

Page 3 of 24
Shock Key Features Continued
Cardio GI Late ↓ CO
↑ Pulse Rate
Thready pulse
↓ BP
Narrowed Pulse Pressure
Postural Hypotension
Low CVP (central
venous pressure)
Flat neck & hand veins
in dependent positions
Slow Capillary Refill in
nail beds
Diminished peripheral
pulses
↓ Motility
Diminished or absent
bowel sounds
N & V
Constipation
↓ central nervous
system activity
(lethargy to coma)
Generalized muscle
weakness
Diminished or absent
deep tendon reflexes
Sluggish pupillary
response to light

Page 4 of 24
Tissue and organ perfusion is related to mean arterial pressure (MAP)
Factors that influence MAP
Total blood volume
Cardiac Output
Size of vascular bed
Sympathetic tone
Types of Shock
Hypovolemic shock – when too little circulating blood vol. causes a MAP ↓ → ↓ O2
Cardiogenic shock –when the actual heart muscle is unhealthy & pumping is impaired
Distributive shock – blood vol. not lost; distribut to interstitial tissues/cannot deliver O2
o Neural induced
o Chemical induced
Anaphylaxis
Sepsis
Capillary leak syndrome
Obstructive shock – caused by problems that impair ability heart muscle to pump
effectively

Page 5 of 24
Hypovolemic Shock
Pathophysiology: Loss of blood volume from the vascular space;
Decreased MAP; Loss of O2 carrying capacity from loss of circulating
RBC’s; Decrease in MAP of 5-10 mmHg below baseline is detected by
baroreceptors; Compensatory mechanisms can halt the progression; If
MAP continues to fall, cell damage can be so severe that the client cannot
survive

Page 6 of 24
Stages of Shock
Initial
(Early)
Nonprogressive
(Compensatory)
Progressive
(Intermediate)
Refractory
(Irreversible) MODS
Early shock;
baseline MAP is
decreased by less
than 10 mm Hg;
Compensatory
mechanisms are effective at
returning MAP to
normal perfusion to vital organs;
Lactic acid will
cause
compensation of
sympathetic system;
vasoconstriction
and increased heart rate;
Symptoms are so
mild it is hard to detect shock
When MAP ↓ 10 to
15 mm Hg from
baseline
Kidney and
baroreceptors sense
an ongoing decrease in MAP
and trigger the
release of renin, ADH, aldosterone,
epinephrine and
norepinephrine
Tissue hypoxia
occurs in nonvital organs and in the
kidney, it is not ↑
enough to cause permanent damage
Mild acidosis and
hyperkalemia; ↑ HR/R
Sustained decrease
in MAP of more
than 20 mm Hg
from baseline
Compensatory
mechanisms are functioning but no
longer deliver
sufficient oxygen, even to vital organs
Overall metabolism
is anaerobic:
moderate acidosis
and hyperkalemia; tissue ischemia
Life threatening
emergency; Cold
Severe tissue
hypoxia with
ischemia and
necrosis
Release of
myocardial depressant factor
from the pancreas
Buildup of toxic metabolites
MODS
Death
Sequence of cell
damage caused by
the massive release
of toxic
metabolites and
enzymes Metabolites trigger
small clots to form
Occurs first in the liver, heart, brain,
and kidney
Damage to the
heart muscle is
severe (one cause is the release of
MDF from
ischemic pancreas)

Page 7 of 24
Shock Assessment
• Assessment
• History
• PE/Clinical manifestations
• Cardiovascular changes
• Respiratory changes
• Kidney/Urinary changes
• Skin changes
• CNS changes
• Skeletal muscle changes

Page 8 of 24
Shock Psychosocial Assessment
Is it necessary to repeat questions to obtain response?
Does the response answer the question asked?
Does the client have difficulty making word choices?
Is the client irritated or upset by the questions?
Can the client concentrate on a question long enough to answer appropriately, or
is the attention span limited?
Laboratory Assessment
pH—decreased
PaO2—decreased
PaCO2—increased
Lactic acid—increased
Hct—increased with fluid shift and dehydration; decreased with hemorrhage
Hgb—as above
K+--increased

Page 9 of 24
Best Nursing Practice for Shock
Ensure airway
IV access
Administer supplemental oxygen
Elevate client’s feet
Examine client for overt bleeding
Apply direct pressure to overt bleeding
Administer medications as prescribed
Increase the rate of IV fluids
DO NOT LEAVE CLIENT

Page 10 of 24
Nursing Interventions for Shock
Nonsurgical management
o Oxygen
o IV therapy (Crystalloids and Colloids)
o Drug therapy: Vasoconstrictors (Dopamine,
Norepinephrine, Phenylephrine); Inotropic Agents
(Dobutamine, Milirinone – Primacor); Agents Enhancing
Myocardial Perfusin (Sodium Nitroprusside – Nitropress,
Nipride)
o Monitoring
Surgical management
Community-based care

Page 11 of 24
Sepsis and Septic Shock
Patho:
Infection
Sepsis/SIRS – sepsis is a condition in which infectious
microorganisms have entered the bloodstream. As the numbers of
organisms increase, an inflammatory response, known as systemic
inflammatory response syndrome (SIRS), is triggered as a result of
infection escaping local control.
Severe sepsis – the progression of sepsis w/an amplified
inflammatory response.
Septic shock – the stage of sepsis and SIRS when multiple organ
failure is evident and uncontrolled bleeding occurs. Even
w/appropriate intervention, the death rate among patients in this
stage of sepsis exceeds 50%.

Page 12 of 24
Risk Factors for Shock
(Nursing Focus on the Older Adult)
Hypovolemic Cardiogenic Distributive Obstructive Diuretic therapy;
Diminished thirst
reflex;
Immobility; Use
of ASA-
containing
products; Use of
complimentary
therapies such as
Ginkgo biloba;
Anticoagulant
therapy
Diabetes mellitus;
Presence of
cardiomyopathies
Diminished
immune response;
Reduced skin
integrity; Presence
of cancer;
Peripheral
neuropathy;
Strokes;
Institutionalization
(hospital or
extended –care
facility);
Malnutrition;
Anemia
Pulmonary HTN;
Presence of
cancer

Page 13 of 24
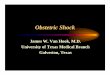
Changes in Selected Parameters during Sepsis and Septic Shock
Parameter Normal Early Sepsis Late Sepsis
Septic
Shock
Cardiac Output
Normal 3-5
L/min Decreased Increased
Greatly
Decreased
Stroke Volume
Normal 60-80
mL Decreased Increased
Greatly
Decreased
Serum Lactate
(Arterial) < 2 mmol/L
Normal to
slightly increased 2-4 mmol/L > 4 mmol/L
Blood Glucose <110 mg/dL 110-120 mg/dL 120-150 mg/dL >150 mg/dL
Oxygen
Saturation 95-100% <95% < 85% <80%
Serum
Creatinine
0.6-1.2 mg/dL
(men)
0.5 – 1.1 mg/dL
(women)
Normal to
slightly increased
> 2 mg/dL (men)
> 1.4 mg/dL
(women)
> 3.0 mg/dL
(either gender)
Segmented
Neutrophils
55% - 70% of
WBC count Increased Decreased < 10%
Band
Neutrophils
2%-5% of total
WBC count
Normal to
slightly increased > 10% > 20%

Page 14 of 24
Left Shift

Page 15 of 24
Interventions – Table 39-6
• Oxygen Therapy
• Drug Therapy
• Antibiotics
• Steroids
• Insulin
• Anticoagulants
• Activated Protein C
• Blood replacement therapy

Page 16 of 24
DIC (Disseiminated Intravascular Coagulation)
The body’s blood clotting mechanisms are activated throughout the body
instead of being localized to an area of injury
Small blood clots form throughout the body, and eventually the blood
clotting factors are used up and unavailable to form clots at sites of real
tissue injury – Bleeding cannot be stopped
Also called consumption coagulopathy

Page 17 of 24

Page 18 of 24

Page 19 of 24
Clients at Risk for DIC
Recent sepsis
Injury or trauma
Recent surgery or anesthesia
Complications of delivery (retained placenta)
Leukemia or disseminated cancer
Recent transfusion reaction
Severe liver disease

Page 20 of 24
Signs and symptoms of DIC
Bleeding from multiple body sites
Clot formation
Hypotension
Bruising and petechiae
Tests for DIC
Fibrin degradation products—increased
PT/PTT—increased
Platelet count—decreased
Serum fibrinogen—decreased
D-dimer—positive

Page 21 of 24
DIC Treatments
Treat the underlying cause
Improve oxygenation, replace fluids, correct electrolyte imbalances, administer
vasopressor medications
Cryoprecipitate
FFP
Heparin
Activated protein C
Nursing Care for DIC
Be aware of at risk clients
Assess clients thoroughly and frequently for signs and symptoms of DIC

Page 22 of 24
DIC Things to avoid
Procedures/activities that increase ICP
Medications that interfere with platelet function
Rectal probes/rectal medications
IM injections
High-pressure suctioning
Lemon-glycerin swabs and commercial mouthwash for oral care
Dislodging any clots, including those around IV sites

Page 23 of 24
DIC Things to DO
Monitor VS closely, including neuro checks, hemodynamics, abdominal
girth, and urine output
Monitor amount of external bleeding carefully—number of dressings
saturated, time to saturate a dressing, pad count in women with vaginal
bleeding
Low-pressure suctioning
Administer oral hygiene carefully—use sponge-tipped swabs with baking
soda rinses
Assess skin q.2h and reposition carefully
Use lamb’s wool between digits

Page 24 of 24
DIC Things to DO Continued
Auscultate breath sounds q.2h
Monitor edema
Monitor volume of IVF’s, blood products
Administer diuretics as prescribed
Monitor fibrinogen levels
Identify previous coping mechanisms
Explain all procedures in terms the client and family can understand