-
ShockandManagement ConceptHardi Darmawan, MD, MPH&TM,
FRSTMDept of Physiology ,Sriwijaya Medical SchoolRK Charitas
HospitalPalembang
-
What is shock?
-
SHOCK SYNDROMEShock is a condition in which the cardiovascular
system fails to perfuse tissues adequatelyAn impaired cardiac pump,
circulatory system, and/or volume can lead to compromised blood
flow to tissuesInadequate tissue perfusion can result
in:generalized cellular hypoxia (starvation)widespread impairment
of cellular metabolismtissue damage organ failuredeath
-
DefinitionInadequate peripheral perfusion leading to failure of
tissue oxygenation may lead to anaerobic metabolismShock is a major
critical illness that involves almost every organ system. It is not
simply a problem of decreased blood pressure. Rather, it is a
problem of inadequate tissue perfusion (Rice,1991)
-
DefinisiHipotensiTekanan Darah Sistolik < 90 mmHgTekanan
Darah Sistolik berkurang > 40 mmHgHipoperfusiPerubahan status
mentalOliguriaAsidosis laktat
-
Diagnosis of ShockMAP < 60 Clinical s/s of hypoperfusion of
vital organs
-
PATHOPHYSIOLOGY OF SHOCK SYNDROMEImpaired tissue perfusion
occurs when an imbalance develops between cellular oxygen supply
and cellular oxygen demand.
All types of shock eventually result in impaired tissue
perfusion & the development of acute circulatory failure or
shock syndrome.
-
Oxygen transport and utilization
-
CARDIAC OUTPUT = HR X SVSympathetic n. systemCatecholamine
releaseIncrease EDV via:VenoconstrictionArteriolar
constrictionRenal reabsorptionIncreased contractility
-
PATHOPHYSIOLOGY OF SHOCK SYNDROME
Cells switch from aerobic to anaerobic metabolism
lactic acid production
Cell function ceases & swells
membrane becomes more permeable
electrolytes & fluids seep in & out of cell
Na+/K+ pump impaired
mitochondria damage
cell death
-
COMPENSATORY MECHANISMS: Sympathetic Nervous System
(SNS)-Adrenal ResponseSNS - Neurohormonal response Stimulated by
baroreceptorsIncreased heart rateIncreased
contractilityVasoconstriction (SVR-Afterload)Increased Preload
-
COMPENSATORY MECHANISMS: Sympathetic Nervous System
(SNS)-Adrenal ResponseSNS - Hormonal: Renin-angiotension
systemDecrease renal perfusionReleases renin angiotension I
angiotension II potent vasoconstriction &releases aldosterone
adrenal cortexsodium & water retention
-
COMPENSATORY MECHANISMS: Sympathetic Nervous System
(SNS)-Adrenal ResponseSNS - Hormonal: Antidiuretic
HormoneOsmoreceptors in hypothalamus stimulatedADH released by
Posterior pituitary glandVasopressor effect to increase BPActs on
renal tubules to retain water
-
COMPENSATORY MECHANISMS: Sympathetic Nervous System
(SNS)-Adrenal ResponseSNS - Hormonal: Adrenal CortexAnterior
pituitary releases adrenocorticotropic hormone (ACTH)Stimulates
adrenal Cx to release glucorticoidsBlood sugar increases to meet
increased metabolic needs
-
Failure of Compensatory ResponseDecreased blood flow to the
tissues causes cellular hypoxia Anaerobic metabolism begins Cell
swelling, mitochondrial disruption, and eventual cell deathIf Low
Perfusion States persists:
IRREVERSIBLE DEATH IMMINENT!!
-
Hypovolaemia and Shockdecreased blood volumedecreased cardiac
outputdecreased oxygen deliveryimpaired
macrocirculationvasoconstrictionInadequate perfusionErythrocyte
aggregationimpaired micro circulationtissue ischemiaorgan
failurekidneybowelendotoxin releaseseptic shockDampak Syok
-
Perfusi normalPompa jantungVolume sirkulasiTahanan pembuluh
darah perifer
-
Pathophysiological causes of shock. After about an hour most
patients will demonstrate a dysfunction of all components and it
may be difficult to identify the original cause.
Reduced Cardiac Outputpump problem(Cardiogenic - Ischaemic)
Reduced Intravascular volumefluid problem(Hypovolaemic)
Reduced Vascular Resistancepipe problem(Neurogenic - Septic -
Anaphylactic)
-
CLASSIFICATIONS OF SHOCK
Cardiogenic Hypovolemic Distributivesepsis, anaphylaxis, and
neurogenic (spinal or epidural anaesthesia, and spinal cord
injury). Obstructivepulmonary embolism, dissecting aortic aneurysm,
pericardial tamponade and tension pneumothorax Combined
-
Dissecting ThrorecicAortic Aneurysm
-
Pulmonary Embolism
-
Pulmonary Emboli
-
Tamponade
-
Stages of ShockInitial stage - tissues are under perfused,
decreased CO, increased anaerobic metabolism, lactic acid is
building Compensatory stage - Reversible. SNS activated by low CO,
attempting to compensate for the decrease tissue perfusion.
Progressive stage - Failing compensatory mechanisms: profound
vasoconstriction from the SNS ISCHEMIA Lactic acid production is
high metabolic acidosisIrreversible or refractory stage - Cellular
necrosis and Multiple Organ Dysfunction Syndrome may occur DEATH IS
IMMINENT!!!!
-
Pathophysiology Systemic LevelNet results of cellular
shock:systemic lactic acidosisdecreased myocardial
contractilitydecreased vascular tonedecrease blood pressure,
preload, and cardiac output
-
Tanda dan gejala syokSistem KardiovaskulerGangguan
sirkulasiPucat, dingin, sianosisVena perifer kolapsNadi cepat dan
halusTekanan darah rendah kurang bisa jadi peganganVena jugularis
penting.CVP
-
Tanda dan gejala syokSistem RespirasiNafas cepat dan
dangkalSistem susunan saraf pusatPerubahan mental / kesadaranSistem
saluran cernaMual dan muntahSistem saluran kencingProduksi urin
< cc/kg/jam
-
Clinical Presentation: Generalized ShockMental status: (LOC)
restless, irritable, apprehensive unresponsive, painful stimuli
only
Decreased Urine output
-
Shock SyndromesHypovolemic Shockblood VOLUME problemCardiogenic
Shockblood PUMP problemDistributive Shock
[septic;anaphylactic;neurogenic]blood VESSEL problem
-
Hypovolemic ShockLoss of circulating volume Empty tank decrease
tissue perfusion general shock responseETIOLOGY: Internal or
External fluid lossIntracellular and extracellular compartmentsMost
common causes:HemorrhageDehydration
-
Hypovolemik Shock
-
A 25 year old woman was admitted in the ERShe had given birth 2
hours ago helped by dukun
-
Hypovolemic Shock: External loss of fluid
Fluid loss: Dehydration Nausea & vomiting, diarrhea, massive
diuresis, extensive burns
Blood loss: trauma: blunt and penetrating BLOOD YOU SEE BLOOD
YOU DONT SEE
-
BP 60, pulse just palpable, over 160 per minuteCold clammy skin,
unconscious
Multiple iv line were inserted and hemodilution started
-
Hypovolemic Shock: Internal fluid loss
Loss of Intravascular integrity
Increased capillary membrane permeability
Decreased Colloidal Osmotic Pressure (third spacing)
-
Pathophysiology of Hypovolemic ShockDecreased intravascular
volume leads to.Decreased venous return (Preload, RAP) leads
to...Decreased ventricular filling (Preload, PAWP) leads to.
Decreased stroke volume (HR, Preload, & Afterload) leads to
..Decreased CO leads to...(Compensatory mechanisms)Inadequate
tissue perfusion!!!!
-
Assessment & ManagementS/S vary depending on severity of
fluid loss:15%[750ml]- compensatory mechanism maintains CO15-30%
[750-1500ml- Hypoxemia, decreased BP & UOP30-40% [1500-2000ml]
-Impaired compensation & profound shock along with severe
acidosis40-50% - refactory stage: loss of volume= death
-
On arrivalAfter infusion
-
Guidelines for the clinical use of red cell transfusionsBritish
Journal of Hematology 2001, 113, p24-3115% loss (750
ml)crystalloids, no transfusion15-30% loss (800-1500
ml)crystalloids, colloids, no transfusions30-40% loss (1500-2000
ml)crystalloids, colloids, probably transfusion> 40% loss (>
2000 ml)crystalloids, colloids, requires transfusion
-
Clinical PresentationHypovolemic ShockTachycardia and
tachypneaWeak, thready pulsesHypotension Skin cool &
clammyMental status changesDecreased urine output: dark &
concentrated
-
Hypovolemic Shock: Hemodynamic Changes Correlate with volume
lossLow CO Decreased RAP ( Preload)Decreased PAD, PAWPIncreased SVR
(Afterload)
-
Initial Management Hypovolemic ShockManagement goal: Restore
circulating volume, tissue perfusion, & correct cause:Early
Recognition- Do not relay on BP! (30% fld loss)Control
hemorrhageRestore circulating volumeOptimize oxygen
deliveryVasoconstrictor if BP still low after volume loading
-
Penanganan Syok HipovolemikMengembalikan volume
intravaskulerTekanan DarahNadiPerfusi organPilihan
cairanKristaloidKoloidPRC
-
American Soc of Anesthesiologists 1996
-
21Hemorrhage
Loss of IVFPoor sluggish perfusionIncreasing pulse
rateDecreasing BP2. Partially compensated by ISF (transcapillary
refill)
-
21Crystalloids for hemorrhage
Rapid Infusion to normalize IVFAfter IVF stabilized, infusion is
intended for ISFVolume required thus 2-4x initially lost
IVF12Ringer LactateRinger AcetateNaCl 0.9%
-
Pulmonary Edema Neurogenic
-
Hb 3Hb 3edemaHb 8RL 7-8000 mlPlasma Subs1500-2000mlBP and pulse
normalize faster|shortershock time3.1.2.Hemorrhage2500 ml
-
TreatmentImpaired perfusion secondary to reduced volumerestore
volume Restoration of circulating volume can be achieved by the
infusion of 3 mL of balanced electrolyte solution for each
milliliter of blood lost.Fluids are infused through two large-bore
intravenous lines
-
TreatmentAdministration of supplemental oxygenControl
bleedingFoley catheter to monitor renal functionestablishment of
urine output at approximately 50 cc/hr for the adult
-
Penanganan Syok HipovolemikPasang jalur IV satu/lebih no. 18 /
16Infus cepat Kristaloid / kombinasi+ koloidBila perdarahan, ambil
contoh darahBila vena sudah terisi, peningkatan isi nadi dan
tekanan darah, infus lambatkanJangan kelebihan cairan
-
Cardiogenic Shock
DEFINISISimply stated, cardiogenic shock is lack of perfusion
from pump failure.Cardiogenic shock is related to the inability of
the myocardium to produce sufficient flow and/or pressure to
maintain adequate tissue perfusion.
-
Cardiogenic ShockThe impaired ability of the heart to pump
bloodPump failure of the right or left ventricleMost common cause
is LV MI (Anterior)Occurs when > 40% of ventricular mass
damageMortality rate of 80 % or >
-
Etiologies of Cardiogenic ShockI. Ischemic heart diseaseA. Acute
myocardial infarction, usually anteroseptalB. Ventricular septal
defect C. Papillary muscle ruptureD. Ventricular aneurysmII.
Valvular heart diseaseA. Acute mitral or aortic insufficiencyB.
Severe aortic stenosis
-
Etiologies of Cardiogenic ShockIII.
ArrhythmiasSupraventricularVentricularIV.TraumaTension
pneumothoraxPericardial tamponade, may include nontraumatic
causesCardiac contusion
-
Cardiogenic Shock: PathophysiologyImpaired pumping ability of LV
leads toDecreased stroke volume leads to..Decreased CO leads to
..Decreased BP leads to.. Compensatory mechanism which may lead to
Decreased tissue perfusion !!!!
-
Cardiogenic Shock: PathophysiologyImpaired pumping ability of LV
leads toInadequate systolic emptying leads to ... Left ventricular
filling pressures (preload) leads to... Left atrial pressures leads
to . Pulmonary capillary pressure leads to Pulmonary interstitial
& intraalveolar edema !!!!
-
Diagnosa Syok KardiogenikCardiac Output berkurangLV filling
pressure meningkatSVR meningkat
-
Clinical PresentationCardiogenic ShockSimilar catecholamine
compensation changes in generalized shock & hypovolemic
shockMay not show typical tachycardic response if on Beta blockers,
in heart block, or if bradycardic in response to nodal tissue
ischemiaMean arterial pressure below 70 mmHg compromises coronary
perfusion (MAP = SBP + (2) DBP/3)
-
Cardiogenic Shock: Clinical Presentation Abnormal heart
sounds
MurmursPathologic S3 (ventricular gallop)Pathologic S4 (atrial
gallop)
-
Clinical PresentationCardiogenic ShockPericardial
tamponademuffled heart tones, elevated neck veinsTension
pneumothoraxJVD, tracheal deviation, decreased or absent unilateral
breath sounds, and chest hyperresonance on affected side
-
CLINICAL ASSESSMENT Pulmonary & Peripheral Edema JVD CO
HypotensionTachypnea, Crackles
PaO2 UOP LOCHemodynamic changes: PCWP,PAP,RAP & SVR
-
COLLABORATIVE MANAGEMENTGoal of managementTreat Reversible
CausesProtect ischemic myocardiumImprove tissue perfusionTreatment
is aimed atEarly assessment & treatment!!!Optimizing pump
by:Increasing myocardial O2 deliveryMaximizing CODecreasing LV
workload (Afterload)
-
COLLABORATIVE MANAGEMENTLimiting/reducing myocardial damage
during Myocardial Infarction:Increased pumping action &
decrease workload of the heartInotropic agentsVasoactive
drugsIntra-aortic balloon pumpCautious administration of
fluidsTransplantationConsider thrombolytics, angioplasty in
specific cases
-
Management Cardiogenic ShockOPTIMIZING PUMP FUNCTION:Pulmonary
artery monitoring is a necessity !! Aggressive airway management:
Mechanical VentilationJudicious fluid managementVasoactive
agentsDobutamineDopamine
-
Management Cardiogenic ShockOPTIMIZING PUMP FUNCTION
(CONT.):Morphine as needed (Decreases preload, anxiety)Cautious use
of diuretics in CHFVasodilators as needed for afterload
reductionShort acting beta blocker, esmolol, for refractory
tachycardia
-
Hemodynamic Goals of Cardiogenic ShockOptimized Cardiac function
involves cautious use of combined fluids, diuretics, inotropes,
vasopressors, and vasodilators to :Maintain adequate filling
pressures (LVEDP 14 to 18 mmHg)Decrease Afterload (SVR
800-1400)Increase contractilityOptimize CO/CI
-
Treatment of Cardiogenic ShockDeterminants of MyocardialOxygen
ConsumptionHeart rateContractilityWall tension,
preloadAfterload
-
TreatmentCardiogenic shock cannot be managed appropriately
without the ability to measure right and left ventricular filling
pressures, cardiac index, and arterial blood pressure or the
ability to calculate oxygen delivery, oxygen consumption, and
pulmonary and systemic vascular resistance. The pulmonary artery
catheter,therefore, is mandatory.
-
TreatmentBroadly based on four methods(a) increasing
contractility (b) altering preload and afterload(c) providing
mechanical support(d) controlling arrhythmias.
-
TreatmentIncreasing ContractilityThe three drugs commonly used
to increase cardiac contractility are dobutamine, dopamine,
noradrenalin and isoproterenol.Reducing Preload and
AfterloadDiuretics may be used as an adjuvant in the treatment of
cardiogenic shock but not as a primary agent. vasodilator therapy
may be added to reduce preload and afterload, thereby enhancing
cardiac output and reducing myocardial oxygen needs
-
TreatmentMechanical Interventionstension pneumothorax, relief of
tension in the chest cavity pericardiocentesis in the case of
pericardial tamponadeintraaortic balloon pump
-
Treatment Common Drugs for ArrhythmiasSupraventricular
tachycardia Digitalis
VerapamilPropanololProcainamideQuinidineVentricular ectopy
LidocaineProcainamideBretyliumQuinidine
-
DISTRIBUTIVE SHOCKMaldistribution of blood to the tissues.Acute
vasodilation without concommitant increase in intravascular
volume.Inadequate tissue perfusion. This type of shock is seen in
:sepsis, anaphylaxis, and neurogenic (spinal or epidural
anaesthesia, and spinal cord injury).
-
Mechanism of distributive
shockhttp://content.nejm.org/cgi/reprint/345/8/588.pdf
-
Sepsis
-
Anaphylaxis
-
Neurogenic
-
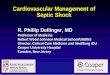
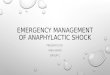
Septic Shock
DEFINISIResult of the systemic effects of infection, primarily
with bacterial or fungal organismsinadequate oxygen delivery
supernormal oxygen demand by the increased metabolism of septic
cells metabolic derangement of cellular metabolism such that cells
cannot utilize oxygen
-
PathophysiologyEarly Septic Shock (Warm Shock)low systolic blood
pressurea relative normal pulse pressure and stroke volume normal
or high cardiac outputBecause these patients tend to be vasodilated
and have a low systemic vascular resistance, the skin is usually
warm (or even flushed) and dry. (a "relative" hypovolemia)
-
PathophysiologyEarly Septic Shock (Warm Shock)Tachycardia and
tachypnea Arterial blood gases usually reveal a moderate
respiratory alkalosisLactate levels are usually normal or only
mildly increased initially
-
PathophysiologyLate Septic Shock (Cold Shock)Impaired organ
functionintravascular fluid retentiondepletion of the functional
extracellular fluid volumeCardiac index usually falls below normal
Lactate levels begin to rise rapidly bicarbonate levels fall
-
PathophysiologyLate Septic Shock (Cold Shock)pH becomes
increasingly acidoticThe skin becomes cold, clammy, mottled, and
cyanoticOliguria and depressed mental status are common
accompaniments of severe sepsis.
-
Diagnosa Syok DistributifCardiac Output normal atau meningkatLV
filling pressure normal atau rendahSVR berkurang
-
Gambaran Hemodinamik Syok
-
HipotensiBiasanya (tidak selalu) cardiac output berkurang,
kecuali Sepsis beratTidak selalu berarti syokHipertensi bisa CO
rendah dan hipoperfusi organ (Gagal Jantung)Penting pemeriksaan
fisik
-
PRINCIPLES OF MANAGEMENT identify cause establish adequate
ventilation and oxygenation restore optimum intravascular volume
maintain adequate cardiac output and renal perfusion maintain
optimum internal metabolic environment
-
Penanggulangan SyokPrinsip dasarMeningkatkan O2
deliveryCararesusitasi cairanmeningkatkan kontraktilitas
jantungmeningkatkan SVRMemperbaiki kelainan iramaOptimalisasi O2
content darahPasang kateter urinThe goal of all treatment is to
maintain adequate tissue perfusion and treat the underlying
cause
-
Penanganan Syok DistributifSyok SeptikCorrect primary
processAntibioticsDrainageResuscitationVentilatory support and 02,
as neededFluidsInotropesVasodilators or vasopressors
-
Resuscitationincrease vascular volumecrystalloid solutions are
preferred for raising intravascular volumesevere acidosis may
impair cardiac function if the arterial pH is < 7. 1,
bicarbonate may be required.Dopamine in doses of 5 to 15 ug/kg/min
seems ideal for improving myocardial contractility and cardiac
output in hypotensive vasodilated patients.
-
Syok AnafilaktikEpinephrine SQResusitasi cairanEpinephrine
IVPenanganan Syok Distributif
-
Terapi CairanMengganti volume intravaskulerMenentukan status
volume cairan pasienVena leherAuskultasi paruCVP
-
Resusitasi CairanKoreksi hipotensiTurunkan HRKoreksi
hipoperfusiOliguriaPerubahan status mentalAsidosis laktatPantau
perburukkan oksigenasi
-
Prioritas dalam Terapi CairanEMERJENSI : VOLUME
INTRAVASKULARCURAH JANTUNGPERFUSI ORGAN VITALSUB-EMERJENSI :
INTERSTITIALINTRASELTANDA-TANDA VITALPROD. URIN
-
Jenis CairanKristaloidRinger Asetat / Ringer LaktatNormal
SalineKoloidHetastarchAlbumin 5%PRCMeningkatkan kapasitas angkutan
O2Fresh-frozen plasmaTidak diindikasikan untuk mengganti volume
-
TERAPI CAIRANASERINGRINGER LAKTATNORMAL SALINE
RESUSITASI
KRISTALOID
KOLOID
ELEKTROLIT
NUTRISIMENGGANTIKAN KEHILANGAN AKUT CAIRANDEXTRAN- 40MEMENUHI
KEBUTUHAN HARIAN ELEKTROLIT DAN NUTRISIKA-EN 1B KA-EN 3AKA-EN
3BKA-EN 4AKA-EN 4B
AMIPARENAMINOVEL- 600PAN- AMIN GKA-EN MG 3Martos -10TRIPAREN
ITRIPAREN II
RUMATANKONSEP MEDIS
KOREKSI- NaCl 3 % - MgSO4 20 % - Mannitol 20 %
-
TREATMENT CONCEPT OF SHOCK
ENHANCING PERFUSION / OXYGEN DELIVERYOxygen delivery/DO2 = HR X
SV X Hb X S02 X 1.34 + Hb X paO2Cardiac outputArterial O2
contentDO2 = CO x CaO2
-
Cardiac Output x SVRPipe = VascularPump =HeartVolume
=BloodHypovolemic ShockCardiogenic ShockDistributive ShockInotropes
(Dob,Dop,Adr,Amr)Vasopressor ( NE,PE,ADR,Dop)FluidsObstructive
ShockRelease tamponade,etcBlood Pressure
-
John Collin Warren (1800s)
momentary pause in the act ofdeath.
-
Samuel D. Gross (late 19th century)rude unhinging of the
machinery of life.
-
Arthur C. Guyton
-
20