Embed Size (px)
DESCRIPTION
critical care
Citation preview
Chapter 157Shock: An OverviewMichael L. CheathamErnest F.J. BlockHoward G. SmithMatthew W. LubeJohn T. PromesShock is one of the most complex conditions encountered in the critically ill patient. The term “shock” encompasses a broad range of pathologic processes that may require diametrically opposed methods of treatment. The underlying cause may be quite evident, as in traumatic hemorrhage, or occult, as in severe sepsis due to infection. Delayed shock resuscitation is associated with significant morbidity and mortality. Therapy must commonly be initiated before all clinical information and diagnostic studies are available. As a result, the intensivist must possess a solid understanding of the common shock states, their clinical presentation, and the necessary therapeutic interventions. Although mortality remains high, increasing application of early goal-directed resuscitation to achieve defined physiologic endpoints has significantly improved patient outcome from shock [1,2,3].Over the centuries, shock has been defined in various ways. In 1534, Ambrose Pare wrote that shock was caused by “toxins in the blood” and recommended phlebotomy as the treatment, a practice that persisted until the early 1800s. By that time, shock-associated hypotension was well recognized as was the detrimental impact of bloodletting on systemic perfusion [4]. Although subsequent early definitions of shock lack scientific terminology, they compensate for this in their simplicity. John Collins Warren described shock as “a momentary pause in the act of death,” whereas Samuel David Gross defined shock as “a rude unhinging of the machinery of life” [5]. In the 1930s, Alfred Blalock published his classic series of investigations into shock confirming that hypotension was due to loss of blood and plasma into the tissues (so called “third-space losses” due to increased capillary permeability) [6]. Blalock found that the hypotension and high mortality of shock were reversible through the infusion of crystalloid solutions to replace lost intravascular and interstitial fluid, and that simple reinfusion of lost blood was not sufficient. Shock was thus identified as a systemic disorder caused by increased vascular permeability, interstitial edema, and intravascular volume depletion with the classic signs of hypotension, decreased urinary output, and multiple organ failure.The importance of regional end-organ perfusion, rather than simply systemic blood flow alone, is the singular concept for recognizing and improving patient outcome from shock. Perfusion may be decreased either systemically (as in hemorrhagic or cardiogenic shock) or only regionally (as in septic shock) with global perfusion being normal or even elevated. Regardless of cause or severity, all forms of shock have the commonality of perfusion inadequate to meet metabolic demands at the cellular level. Decreased organ perfusion leads to tissue hypoxia, anaerobic metabolism, activation of the inflammatory cascade, and eventually organ dysfunction. The ultimate consequences of shock depend on the degree and duration of hypoperfusion, the number of organs affected, and the presence of prior organ dysfunction. The challenges to the intensivist are identifying the hypoperfused state, diagnosing its cause, and rapidly restoring cellular perfusion.PhysiologySignificant progress has been made in elucidating the cellular basis for shock. Although low blood pressure and other vital sign derangements were previously thought to be sufficient to cause shock, they are now recognized as being signs of a complex physiologic cascade of events. The delivery and consumption of oxygen at the mitochondrial level, as well as the adequate removal of cellular waste products, is of paramount importance to survival. Cellular hypoxia leads to local vasoconstriction, thrombosis, anaerobic glycolysis, release of superoxide radicals, accumulation of pyruvate and lactate, and intracellular acidosis. The severity of a patient's acidemia, demonstrated by elevated base deficit or lactate levels, correlates with the lethality of shock [7].
In patients who experience such an anaerobic insult, injured tissues and damaged cells release a variety of intracellular mediators which initiate the proinflammatory cascade. Cytokines are small polypeptides and glycoproteins produced by a variety of immunologic cells that are responsible for many of the sequelae seen during shock. Tumor necrosis factor alpha (TNF-α) is one of the earliest cytokines released and is a product of monocytes, macrophages, and T-cells. TNF-α levels rise after a variety of cellular insults and cause hypotension, procoagulant activity, muscle breakdown, catabolism and cachexia. TNF-α levels have been seen to correlate with mortality in animal models of hemorrhagic shock [8]. Produced by macrophages and endothelial cells, interleukin-1 (IL-1) has similar effects, producing fever and anorexia. Activated T-cells produce interleukin-2 which augments cell mediated immunity. Interleukin-6, together with IL-1, mediates the acute phase response to injury and may have a role in the development of acute lung injury. Interleukin-8 is chemotactic for neutrophils and interleukin-12 has a role in cell-mediated immunity by promoting the differentiation of T-helper 1 cells. A variety of “anti-inflammatory” cytokines such as growth hormone interleukin-4, interleukin-10, interleukin-13, soluble TNF receptors (sTNFR), and IL-1 receptor antagonists (IL-1ra) are simultaneously released in an attempt to counterbalance the proinflammatory cascade.These proinflammatory and counter-regulatory substances may lead to processes that may not be in the best interest of the patient in shock. The body's (mal)adaptive response to the primary injury or inciting event may cause secondary injury to previously unaffected cells and organs leading to impaired perfusion, cellular death, and organ dysfunction. This systemic inflammatory response syndrome, if left unabated, may result in the multiple organ dysfunction syndrome, a common cause of shock-related morbidity and mortality.IL-1 also activates the patient's hypothalamopituitary axis (HPA) as well as the neuroendocrine response to critical illness. HPA activation releases adrenocorticotrophic hormone (ACTH) that acts on the adrenal gland to stimulate P.1645
glucocorticoid (cortisol) production. Appropriate adrenocortical response to shock is essential for patient survival. Relative adrenal insufficiency during critical illness is a commonly underappreciated reason for a patient's failure to respond to resuscitative interventions [9]. Vasopressin (antidiuretic hormone [ADH]) is cosecreted from the posterior pituitary and potentiates the effect of ACTH. In addition to its primary osmoregulatory role in resorption of water from the nephron's collecting duct, ADH is also a potent vasoconstrictor, improving systemic perfusion, and promoting gluconeogenesis and glycolysis to provide much needed metabolic substrates.The neuroendocrine response to shock involves many counter-regulatory substances. Epinephrine and norepinephrine are produced from the adrenal medulla and synapses of the sympathetic nervous system respectively. β-Adrenergic stimulation results in increased heart rate and contractility, and α-adrenergic stimulation increases systemic vascular resistance and blood pressure through peripheral vasoconstriction. Blood is thus shunted from less essential organs preserving flow to the heart and brain. Sympathetic stimulation also causes venoconstriction accelerating venous return to the central circulation. Through their metabolic effects, catecholamine secretion contributes to stress induced hyperglycemia, a common problem during critical illness. The renin angiotensin system is activated resulting in the release of angiotensin-II (AT-II), another potent vasoconstrictor and stimulus for aldosterone secretion. Aldosterone promotes salt and water conservation at the level of the distal renal tubule in an attempt to preserve intravascular volume. It also regulates acid-base and potassium homeostasis. Glucagon is produced by the pancreatic alpha islet cells and, unlike insulin, has a catabolic role. Release of many of these substances also leads to decreased levels of circulating insulin. The resultant catabolic state characterized by insulin resistance, hyperglycemia, lipolysis, free fatty acid formation, ketogenesis, erosion of lean body mass and negative nitrogen balance may last for weeks to months.Classification
Shubin and Weil's classic paper distinguished the various forms of shock with respect to cardiovascular parameters [10]. Four categories of inadequate systemic perfusion were described: (a) hypovolemic, (b) obstructive, (c) cardiogenic, and (d) distributive. Although new etiologies of shock (e.g., adrenal insufficiency of critical illness) have recently received significant attention, they are easily placed into one of these physiologic descriptions.
Table 157.1 Classification of Shocka Class I Class II Class III Class IVBlood loss (mL) Up to 750 750–1,500 1,500–2,000 ≥2,000Blood loss (% blood volume)
Up to 15 15–30 30–40 ≥40
Pulse rate < 100 > 100 > 120 ≥140Blood pressure Normal Normal Decreased DecreasedPulse pressure Normal/increased Decreased Decreased DecreasedCapillary refill Normal Decreased Decreased DecreasedRespiratory rate 14–20 20–30 30–40 > 35Urinary output (mL/h) 30 or more 20–30 5–15 NegligibleCentral nervous system Slightly anxious Anxious Anxious, confused Confused, lethargicFluid replacement Crystalloid Crystalloid Crystalloid + blood Crystalloid + bloodaEstimates based on a 70-kg male.Modified from Committee on Trauma of the American College of Surgeons: Advanced Trauma Life Support for Doctors. Chicago, American College of Surgeons, 2008, p 61.Hypovolemic ShockHypovolemic shock is the most common form of shock. Almost all forms include some component of hypovolemia as a result of decreased intravascular volume or “preload.” The sympathetic response to reduced preload is arterial vasoconstriction, diverting blood from the splanchnic viscera, skin, and skeletal muscle. Physical findings include cold clammy skin, tachypnea, tachycardia, and low urinary output, all a result of either hypovolemia or compensatory mechanisms.Hypovolemic shock is stratified into four classes based on the degree of circulating volume loss (Table 157.1). It is important to recognize that significant blood volume may be lost in the absence of any clinical signs. Compensatory mechanisms allow systemic blood pressure to be maintained and a well-compensated patient may display tachycardia as the only objective clinical abnormality, even with a blood volume loss of up to 30%. Hypovolemic shock may be further subclassified as either hemorrhagic or nonhemorrhagic. Hemorrhagic shock may be visibly apparent (external blood loss from traumatic injury) or occult (chronic gastrointestinal hemorrhage). Emphasis on hemorrhage control rather than simply volume replacement is an essential difference in the management of hemorrhagic shock [11,12]. Nonhemorrhagic hypovolemic shock is seen in a number of pathologic states and may be caused by absolute loss of total body fluid volume and/or migration of acellular fluid from the intravascular to the interstitial compartment (third spacing). Third spacing of fluid occurs predictably in severe illnesses such as pancreatitis, small bowel obstruction, and burns. Volume depletion may also occur as a consequence of uncompensated gastrointestinal, urinary, or evaporative losses. It is imperative that the intensivists focus on resuscitation of the patient's intravascular volume as opposed to total body volume. Failure to do so will uniformly result in under-resuscitation and poor patient outcome.Obstructive ShockObstructive forms of shock are those in which the underlying pathology is a mechanical obstruction to normal cardiac output (CO) with a resulting diminution in systemic perfusion. Cardiac tamponade is an example of obstructive shock. A small amount of fluid (usually less than 200 mL) within a noncompliant pericardium may produce significant myocardial compression [13]. Clinical signs of tamponade include jugular venous distention and a central venous pressure (CVP) waveform P.1646
demonstrating a rapid “x” descent and a blunted “y” descent due to inability of the heart to fill during diastole. Pulsus paradoxus, an exaggerated fluctuation in arterial pressure caused by changes in intrathoracic pressure during respiration, may be present. Formal echocardiography is helpful in making the diagnosis although recent advances in the use of bedside ultrasonography by noncardiologists have demonstrated excellent sensitivity and rapid performance of the examination [14].Pulmonary venous thromboembolism is another example of obstructive shock and may present as profound circulatory collapse. CO is restricted either by mechanical obstruction of the pulmonary arterial tree or by pulmonary hypertension induced by release of secondary mediators. Additional findings include elevated CVP and pulmonary hypertension, but normal pulmonary artery occlusion pressure (PAOP). Through similar mechanisms, venous air embolism can completely obstruct pulmonary arterial blood flow, with ensuing cardiac arrest. Central hemodynamics mimic those of pulmonary embolism. Although numerous causes exist, of greatest concern are the placement and removal of central venous catheters and surgical procedures in which the operative site is more than 5 cm above the right atrium [15]. Venous air embolism is diagnosed by auscultation of the classic “mill wheel” heart murmur. Immediate placement of the patient in a head-down, left lateral decubitus position is advocated, as are attempts to aspirate air from the right ventricle through a central venous catheter.Finally, tension pneumothorax may cause shock through obstruction of venous return. Elevated intrapleural pressure collapses intrathoracic veins resulting in inadequate venous filling. Tension pneumothorax should be diagnosed by physical examination and not by radiography. Needle decompression often restores venous filling sufficiently until a thoracostomy tube can be placed.Cardiogenic ShockIn cardiogenic shock, the underlying defect is primary ventricular pump failure, the most common cause of coronary artery disease related mortality. The foundations of ventricular failure include (a) myocardial infarction with loss of myocardium, (b) reduced contractility (cardiomyopathy), (c) ventricular outflow obstruction (aortic stenosis or dissection), (d) ventricular filling anomalies (atrial myxoma, mitral stenosis), (e) acute valvular failure (aortic or mitral regurgitation), (f) cardiac dysrhythmias, and (g) ventriculoseptal defects. Most often, cardiogenic shock is a direct or indirect consequence of acute myocardial infarction.Cardiogenic shock due to left ventricular infarction suggests that more than 40% of the left ventricle is involved [16]. On physical examination, signs of peripheral vasoconstriction are evident and oliguria is common. The typical hemodynamic profile includes systemic hypotension with decreased CO and elevated PAOP. Physical examination findings of pulmonary and peripheral edema as well as hepatomegaly may suggest volume overload, but are commonly due to third spacing of fluid due to shock with relative intravascular volume depletion being present. In such situations, hemodynamic monitoring using echocardiography or a volumetric pulmonary artery catheter may provide additional diagnostic information clarifying the patient's true volume status.Right ventricular dysfunction as a consequence of inferior wall myocardial infarction carries a better prognosis than left-sided failure. Diagnosis may be suggested by elevated right ventricular diastolic pressure with decreased pulmonary artery pressure [17]. Hypotension caused by right-sided heart failure must be distinguished from left-sided failure because of the significant differences in their management. Shock from right-sided failure is corrected by volume resuscitation to maintain right ventricular preload while left-sided failure is treated by volume restriction to reduce myocardial work. If inotropes are indicated, agents that do not increase pulmonary vascular resistance should be chosen [18].Dysrhythmias are another source of cardiogenic shock. In addition to malignant dysrhythmias, such as ventricular fibrillation, atrial dysrhythmias such as atrial fibrillation or flutter as well as supraventricular tachycardia are common in the critically ill and may result in shortened diastolic filling time with a profound decrease in CO.Distributive Shock

The classic hemodynamic profile of septic shock (high CO and systemic hypotension) has prompted some clinicians to institute antimicrobial therapy and search for an infectious source in any patient who exhibits these cardiac parameters. Such hyperdynamic patterns, however, are seen in non-infectious conditions as well including anaphylaxis, spinal cord injury, and severe liver dysfunction. The term distributive shock, rather than septic shock, is therefore used to account for these dissimilar diseases with a common hemodynamic picture.The management of septic shock remains a major challenge to the intensivist [1,2,3]. A milieu of inflammatory cytokines, bacterial factors, and complement and coagulation activation combine to induce the complex hemodynamic pattern characteristic of septic shock. In most forms of shock, illness leads to a low CO state with elevated systemic vascular resistance (SVR) and reduced mixed venous oxygen saturation (SvO2). Early septic shock, however, is manifested by normal-to-low
cardiac filling pressures, increased CO, decreased SVR, and increased SvO2 [19]. Despite elevated
systemic blood flow and oxygen delivery (DO2), abnormalities exist in tissue oxygen extraction at
the cellular level, perhaps through disruption of normal mitochondrial metabolic pathways [20,21]. Sepsis-induced myocardial depression may be demonstrated through decreased ejection fraction, right ventricular dysfunction, and left ventricular dilation. In the later stages of septic shock, cardiac function deteriorates with the patient's hemodynamic status mimicking that of cardiogenic shock with decreased CO and increased SVR [22].Anaphylaxis represents another form of distributive shock in which histamine-mediated vasodilatation occurs. The most common causes are medications, insect envenomations, blood products, radiographic contrast media, and food allergies [23]. Reactions severe enough to result in shock occur shortly after exposure to the offending agent. Physical findings include a dermatologic reaction (erythema, urticaria) and obstructive respiratory processes. Occasionally, the reaction is severe enough to produce shock through myocardial depression.Neurogenic shock, another form of distributive shock, occurs as a result of upper thoracic spinal cord injury with hypotension, bradycardia, and warm, dry skin due to loss of sympathetic vascular tone. Although euvolemic, patients demonstrate relative hypovolemia due to vasodilatation of the intravascular space. If hypotension does not respond to volume resuscitation, it may be treated with vasopressors and any bradycardia may be corrected with atropine. In the trauma patient, hemorrhage should always be excluded before attributing shock to a neurogenic source [24].Over the last decade, endocrine insufficiency as a result of critical illness has been recognized as an underappreciated cause of distributive shock. This relative adrenal insufficiency may worsen the impact of the various shock states as the patient is unable to respond appropriately to the stress of their critical illness [25,26]. Corticosteroid supplementation in such P.1647
patients can significantly improve systemic perfusion as well as reduce the patient's requirement for vasopressor support.Physiologic MonitoringVital sign derangements are typically the first indication that a shock state is present. Normalization of such parameters signifies that the patient is appropriately responding to resuscitative therapy. Physiologic monitoring is thus essential to both the diagnosis and management of shock. Such monitoring typically begins with the use of routine vital signs, but may progress to the application of invasive monitoring techniques.Vital SignsThe diagnosis of shock was originally based on abnormalities in a patient's vital signs. Until the late 1960s, the presence of tachycardia and hypotension was considered synonymous with shock. Over time, it became apparent that normalization of heart rate, blood pressure, temperature, and urinary output was not necessarily sufficient to reverse a patient's shock state. Critically ill patients continued to have a high incidence of multiple organ failure and mortality despite seemingly adequate resuscitation based on restoration of vital signs to “normal.” Shock is therefore defined by the adequacy of end-organ perfusion rather than derangements in vital signs alone. Nevertheless,
these physiologic parameters remain the foundation for the initial recognition that shock is present.Heart RateAlterations in heart rate are common during shock. Tachycardia is most common and is usually a direct effect of intravascular volume loss in where heart rate increases to maintain adequate CO and DO2 to tissues. These increases may become pathologic if inadequate diastolic filling time results in
decreased stroke volume. Tachycardia can be used to predict the presence of intravascular volume depletion and its resolution to suggest volume resuscitation adequacy [27]. Decreased heart rate, in response to a volume challenge, can be a simple and useful test for diagnosing hypovolemia.Bradycardia is usually representative of severe physiologic derangement and impending cardiovascular collapse. Its presence in a critically ill patient demands immediate attention. Patients receiving beta-blocker therapy or with high spinal cord injuries or pacemakers may not be able to increase their heart rate and compensate for their shock. Patients with an inappropriately low heart rate and inadequate CO will benefit from increasing heart rate by withholding beta-blocker therapy, use of chronotropic medications, or reprogramming their pacemakers to a higher rate.Blood PressureHypertension is an uncommon finding in shock. Patients are typically hypotensive due to the presence of hypovolemia, decreased cardiac contractility, or systemic vasodilatation. Normotension should be restored as quickly as possible to improve tissue perfusion and oxygen delivery at the cellular level. Blood pressure may be measured either noninvasively or invasively. Both techniques are subject to certain mechanical and physiologic measurement errors, or “dynamic response artifacts,” that can result in inappropriate therapy if unrecognized by the clinician [28]. Because of these intrinsic monitoring errors, systolic blood pressure (SBP) and diastolic blood pressure (DBP) measurements may vary widely from one measurement technique to another. The mean arterial pressure (MAP), however, will remain fairly consistent regardless of the measurement method and any artifact present. As a result, MAP should be used to titrate resuscitative therapies rather than SBP or DBP. MAP is calculated as
TemperaturePatient temperature, although not indicative of either the presence or absence of shock, may help define the cause and can have significant prognostic value [29,30]. The presence of hypothermia (core body temperature less than 96.8°F or 36.0°C) suggests severe physiologic derangement and has a significant impact on patient survival [31]. Hypothermia places the patient at risk for cardiac dysrhythmias, acute renal failure, and refractory coagulopathy [32]. Although hypothermia reduces metabolic activity of the body, rewarming significantly increases global metabolic demands and oxygen consumption ([V with dot above]O2). Such demands may exceed the patient's capacity to
deliver oxygen to the cells, resulting in an oxygen transport imbalance. Care must be taken to ensure adequate DO2 and tissue perfusion during rewarming. Because of its significant morbidity
and mortality, nontherapeutic hypothermia should be avoided or rapidly corrected in most critically ill patients [29,30].Urine OutputInadequate renal blood flow results in decreased urinary output. Oliguria is one of the earliest signs of inadequate perfusion at the tissue level. Worsening renal function is an important indicator of the presence of shock. Decreases in urine output as a result of hypovolemia are seen before changes in heart rate or blood pressure (Table 157.1). Improvements in urine volume in response to fluid loading can guide shock resuscitation as long as confounding factors are not present (e.g., diabetes insipidus, diabetic ketoacidosis, and diuretic therapy).Pulse OximetryTechnologic advances in the 1970s and 1980s led to the widespread introduction of pulse oximetry as the “fifth” vital sign [33]. Pulse oximetry is now routinely used in the critically ill as a noninvasive method of continuously monitoring arterial oxygen saturation. This addition to the traditional four vital signs serves two purposes. First, it provides an early warning of hypoxemia, allowing corrective interventions to be made. Second, it can be used as an endpoint in the

resuscitation of patients and in the assessment of oxygen transport balance.Hemodynamic MonitoringIn 1970, Swan and Ganz introduced the flow-directed pulmonary artery catheter, allowing clinicians to measure pulmonary artery pressures at the bedside [34]. In 1972, addition of a temperature thermistor provided the ability to calculate CO. These advancements provided clinicians with the ability to assess a variety of new hemodynamic parameters evaluating patient preload, contractility, and afterload. In the 1980s, continuous mixed venous oximetry was added as the importance of DO2, [V with dot above]O2, and oxygen transport balance in the diagnosis and management of the
shock states became clear. By the early 1990s, catheters capable of calculating right ventricular volumes became available, further improving preload assessment. Current pulmonary artery catheters continuously assess hemodynamic and oxygen transport variables providing the clinician with minute-by-minute assessments of cardiopulmonary function by which to guide resuscitation. Although pulmonary artery catheterization is performed with much less frequency than in years past, it remains an important P.1648
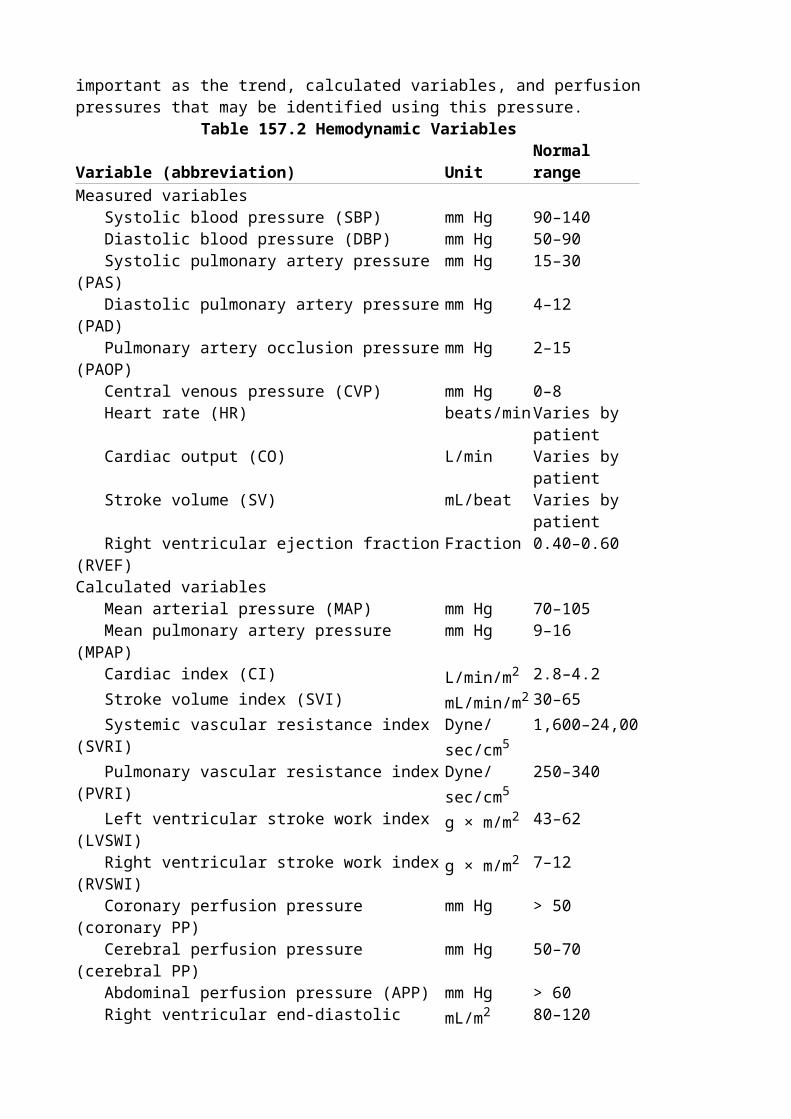
monitoring technology for the most critically ill patients with shock and has recently been demonstrated to improve patient outcome when used in a goal-directed fashion [35,36]. A variety of other hemodynamic monitoring techniques have been developed including arterial pressure wave contour analysis, esophageal Doppler, and transesophageal echocardiography among others. Regardless of the method by which hemodynamic data is obtained, a thorough understanding of the available hemodynamic and oxygenation variables is essential if resuscitative therapy is to improve patient outcome from shock (Tables 157.2 and 157.3) [37].Pressure and Pressure-Derived VariablesPressure variables form the foundation for physiologic monitoring in shock assessment. It is important to recognize, however, that the absolute value of any single pressure variable is not as important as the trend, calculated variables, and perfusion pressures that may be identified using this pressure.
Table 157.2 Hemodynamic VariablesVariable (abbreviation) Unit Normal rangeMeasured variables Systolic blood pressure (SBP) mm Hg 90–140 Diastolic blood pressure (DBP) mm Hg 50–90 Systolic pulmonary artery pressure (PAS) mm Hg 15–30 Diastolic pulmonary artery pressure (PAD) mm Hg 4–12 Pulmonary artery occlusion pressure (PAOP) mm Hg 2–15 Central venous pressure (CVP) mm Hg 0–8 Heart rate (HR) beats/min Varies by
patient Cardiac output (CO) L/min Varies by
patient Stroke volume (SV) mL/beat Varies by
patient Right ventricular ejection fraction (RVEF) Fraction 0.40–0.60Calculated variables Mean arterial pressure (MAP) mm Hg 70–105 Mean pulmonary artery pressure (MPAP) mm Hg 9–16 Cardiac index (CI) L/min/m2 2.8–4.2 Stroke volume index (SVI) mL/min/m2 30–65 Systemic vascular resistance index (SVRI) Dyne/sec/
cm51,600–24,00
Pulmonary vascular resistance index (PVRI) Dyne/sec/cm5
250–340
Left ventricular stroke work index (LVSWI) g × m/m2 43–62 Right ventricular stroke work index (RVSWI) g × m/m2 7–12 Coronary perfusion pressure (coronary PP) mm Hg > 50 Cerebral perfusion pressure (cerebral PP) mm Hg 50–70 Abdominal perfusion pressure (APP) mm Hg > 60 Right ventricular end-diastolic volume index (RVEDVI)
mL/m2 80–120
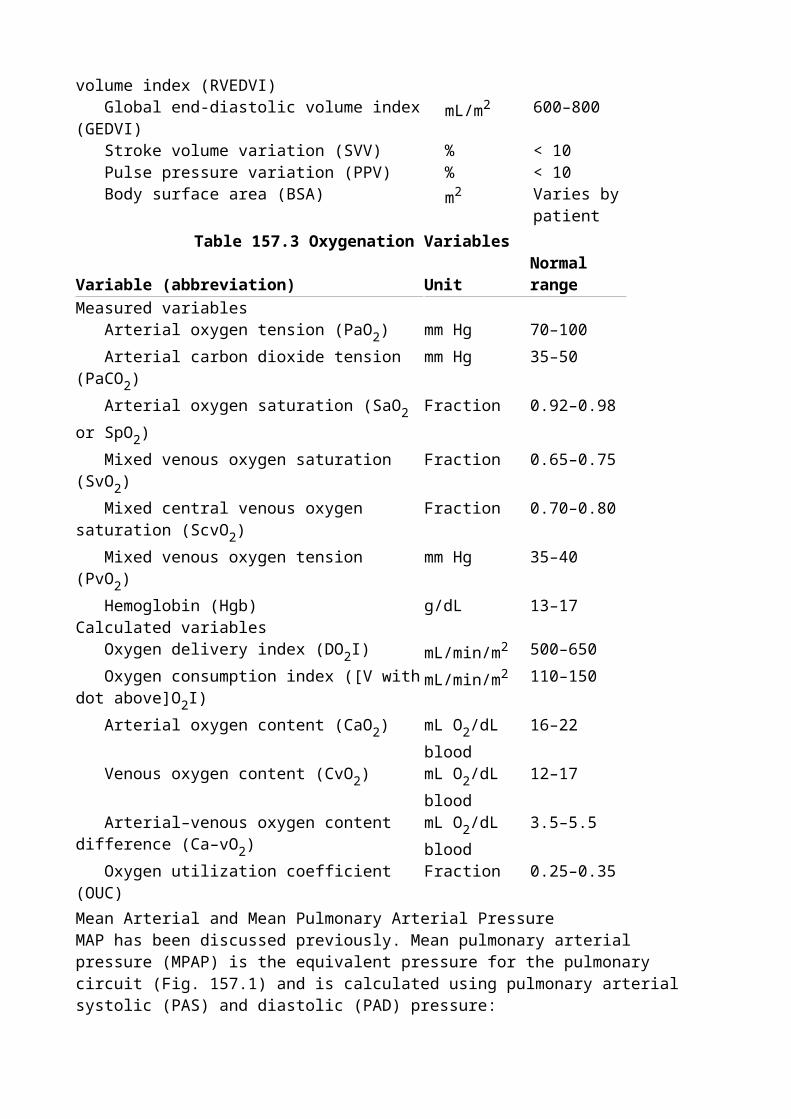
Global end-diastolic volume index (GEDVI) mL/m2 600–800 Stroke volume variation (SVV) % < 10 Pulse pressure variation (PPV) % < 10 Body surface area (BSA) m2 Varies by
patientTable 157.3 Oxygenation Variables
Variable (abbreviation) Unit Normal rangeMeasured variables Arterial oxygen tension (PaO2) mm Hg 70–100
Arterial carbon dioxide tension (PaCO2) mm Hg 35–50
Arterial oxygen saturation (SaO2 or SpO2) Fraction 0.92–0.98
Mixed venous oxygen saturation (SvO2) Fraction 0.65–0.75
Mixed central venous oxygen saturation (ScvO2) Fraction 0.70–0.80
Mixed venous oxygen tension (PvO2) mm Hg 35–40
Hemoglobin (Hgb) g/dL 13–17Calculated variables Oxygen delivery index (DO2I) mL/min/m2 500–650
Oxygen consumption index ([V with dot above]O2I)mL/min/m2 110–150
Arterial oxygen content (CaO2) mL O2/dL blood16–22
Venous oxygen content (CvO2) mL O2/dL blood12–17
Arterial–venous oxygen content difference (Ca–vO2)
mL O2/dL blood3.5–5.5
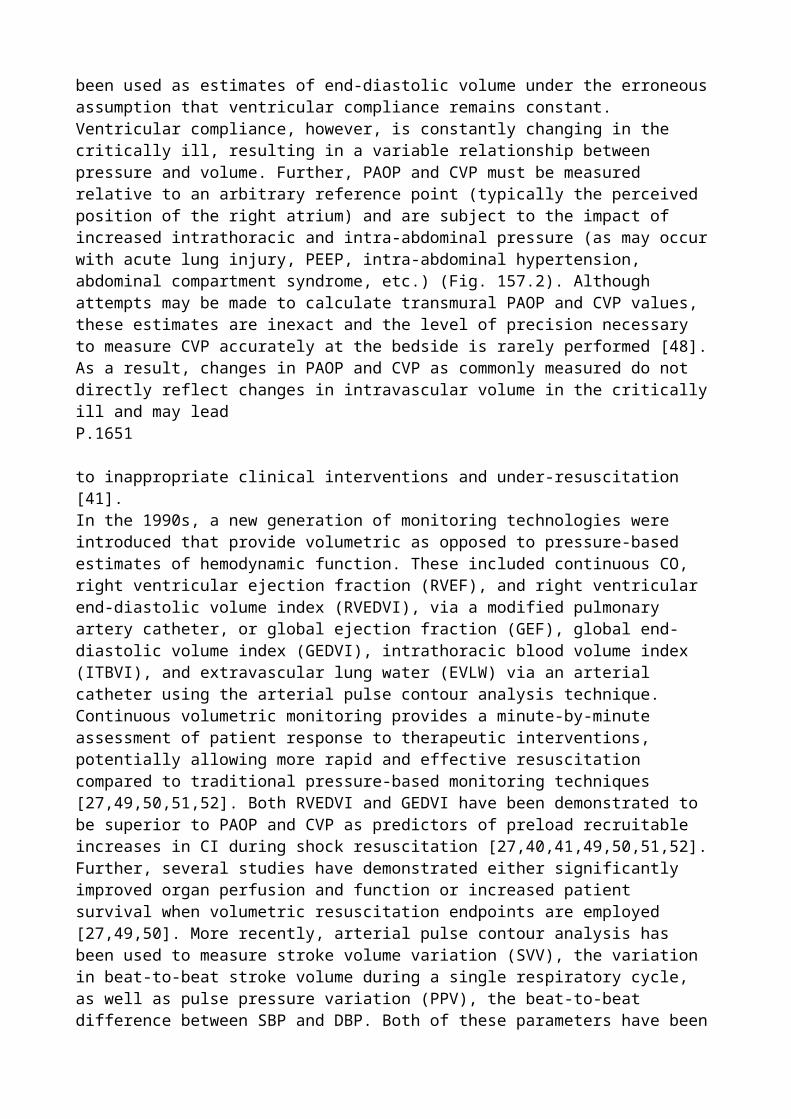
Oxygen utilization coefficient (OUC) Fraction 0.25–0.35Mean Arterial and Mean Pulmonary Arterial PressureMAP has been discussed previously. Mean pulmonary arterial pressure (MPAP) is the equivalent pressure for the pulmonary circuit (Fig. 157.1) and is calculated using pulmonary arterial systolic (PAS) and diastolic (PAD) pressure:
Mean pressures should be used to guide decision making and resuscitative therapy whenever possible as they are less P.1649
subject to monitoring artifacts. They are also essential components to calculate vascular resistance and cardiac work.
Figure 157.1. Hemodynamic calculations. PAOP, pulmonary artery occlusion pressure; CVP, central venous pressure; MAP, mean arterial pressure; MPAP, mean pulmonary artery pressure; SVRI, systemic vascular resistance index; PVRI, pulmonary vascular resistance index; LVSWI, left ventricular stroke work index; RVSWI, right ventricular stroke work index.
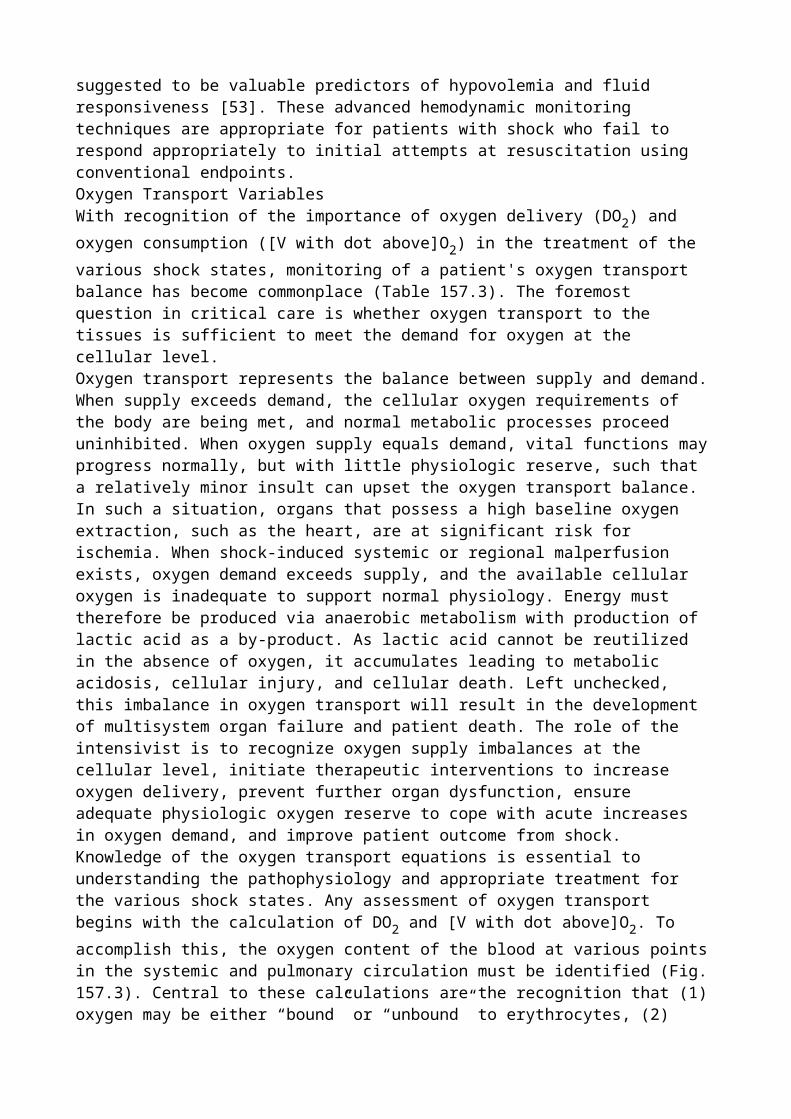
Figure 157.2. The “PAOP assumption”: Why intracardiac filling pressures do not accurately estimate preload status? LVEDV, left ventricular end-diastolic volume; LVEDP, left ventricular end-diastolic pressure; LAP, left atrial pressure; PAOP, pulmonary artery occlusion pressure. [Adapted from Cheatham ML: Right ventricular end-diastolic measurements in the resuscitation of trauma victims. Int J Crit Care 7:165–176, 2000, with permission.]Pulmonary Artery Occlusion and Central Venous PressureFluid administration is an essential element in the initial resuscitation of almost all forms of shock. Intracardiac-filling pressure measurements such as PAOP or “wedge” and CVP are commonly used to estimate intravascular volume or “preload.” Preload, by the Frank–Starling Law, is defined in terms of myocardial fibril length at end-diastole. Because this is clinically immeasurable, several assumptions are made to use PAOP to clinically assess the preload status of the left ventricle (Fig. 157.2). These assumptions are frequently invalid in critically ill patients due to changing ventricular compliance caused by a variety of factors. As a result, PAOP measurements should be carefully considered as estimates of intravascular volume status in the patient with shock [38,39,40]. In fact, reliance on PAOP measurements for preload assessment in critically ill patients may lead to inappropriate interventions in more than 50% of patients [41]. The trend rather than the absolute value of such measurements in response to therapeutic interventions is of greater value. The optimal PAOP is that value which, through careful evaluation of the patient's hemodynamic status, is determined to optimize systemic perfusion (CO) and cellular oxygenation (DO2, [V with dot
above]O2). For similar reasons, absolute CVP measurements do not accurately portray left
ventricular volume status or ventricular function [38,39,40,41]. As with PAOP, the trend of CVP measurements in response to therapeutic measures may be of value.Perfusion VariablesThe importance of adequate end-organ perfusion in correcting the shock state cannot be overemphasized. The following perfusion variables are easily calculated and represent important resuscitation endpoints in the critically ill.Coronary Perfusion PressureMaintaining adequate coronary perfusion pressure (PP) should be a primary goal in the resuscitation of any patient in shock. Patients with preexisting coronary artery disease may have marginal myocardial blood flow, which is only worsened by inadequate systemic perfusion during shock. Coronary PP is calculated as the pressure change across the coronary artery during maximal blood flow:
The goal should be to maintain coronary PP greater than 50 mm Hg. Failure to maintain this level of perfusion increases the risk for myocardial ischemia and infarction. Note that DBP and not SBP is the critical determinant of coronary perfusion as maximal myocardial blood flow occurs during diastole. PAOP estimates myocardial wall tension and resistance to perfusion by approximating end-diastolic pressure in the left ventricle.Cerebral Perfusion PressureMonitoring cerebral perfusion pressure is important in the head-injured patient with increased intracranial pressure (ICP) [42]. Because the brain is enclosed within the skull with little room for expansion, increases in ICP and development of cerebral edema can have significant and detrimental effects on cerebral blood flow and oxygenation. Monitoring of ICP is an important component of the hemodynamic monitoring of patients with brain injury and shock. Cerebral PP is calculated as the pressure change across the brain:
The goal should be to maintain a cerebral PP of 50 to 70 mm Hg [42]. This may be accomplished by either increasing MAP (using a vasopressor such as norepinephrine) or decreasing intracerebral volume (through the use of mannitol or hypertonic fluids), thereby decreasing ICP. Maintenance of a cerebral PP > 70 mm Hg does not appear to provide a survival benefit and may lead to potentially detrimental over-resuscitation.Abdominal Perfusion Pressure
Analogous to coronary and cerebral PP, abdominal perfusion pressure (APP) has been identified as a valuable parameter in the resuscitation of patients with elevated intra-abdominal pressure (IAP), a condition present in over half of all ICU patients [43,44]. IAP is most commonly determined as intravesicular or “bladder” pressure by transducing the patient's indwelling urinary catheter [45,46]. APP is calculated as the pressure change across the abdominal organs:
Failure to maintain APP ≥ 60 mm Hg has been found to discriminate between survivors and nonsurvivors [43]. Maintenance of adequate APP through a balance of judicious fluid resuscitation and application of vasoactive medications has been demonstrated to reduce the incidence of acute renal failure [47].Blood Flow and Flow-Derived VariablesCritically ill patients with shock and systemic malperfusion frequently benefit from calculation of blood flow-related variables such as CO and stroke volume (SV). Flow-related variables are used with pressure variables to calculate vascular resistance and estimate the work performed by the left and right ventricles. Such advanced hemodynamic monitoring should be implemented whenever a patient fails to respond to resuscitation as expected.Interpatient variability makes it difficult to assign a normal range to flow-derived variables. What might be an adequate CO for a 50-kg woman is inadequate for a 150-kg man. To normalize these measurements and allow comparison from patient to patient, flow-derived variables are indexed to body surface area (BSA), obtained from a nomogram. Indexed variables, such as cardiac index (CI) and stroke volume index (SVI), are more meaningful because normal ranges aid in interpretation. P.1650
All flow-derived hemodynamics should be indexed to facilitate comparison with accepted normal ranges.Cardiac Index and Stroke Volume IndexCI is the total blood flow from the heart (in liters per minute) divided by BSA. SVI is the volume of blood ejected from the heart per beat, divided by BSA:
Most shock states have a decreased CI as a result of intravascular volume depletion, poor underlying cardiac pump function, increased vascular resistance, or a combination of these factors. To maintain CI, tachycardia is the usual response to inadequate preload and a low SVI. Appropriate therapy is to restore intravascular volume and increase SVI, thus improving CI. An increased CI may be seen in early septic shock, but may also be seen with other nonshock hyperdynamic states, such as cirrhosis, pregnancy, and high-performance athletes.Systemic Vascular Resistance Index/Pulmonary Vascular Resistance IndexAccording to Ohm's law, the resistance of an electrical circuit is equal to the voltage difference across the circuit divided by the current. A simplified view of the circulatory system can be likened to an electrical circuit in which the resistance across the systemic or pulmonary vascular beds is calculated using Ohm's law (Fig. 157.1):
The constant, 79.9, is used to convert mm Hg · L per minute to the more physiologic units of dynes per seconds per · cm5.Increased SVRI is commonly seen in obstructive, hypovolemic, late septic, and cardiogenic shock. Systemic resistance may also rise in nonshock states such as pheochromocytoma (secondary to increased endogenous catecholamine output). Decreased SVRI is common in distributive shock states (neurogenic, early septic, endocrine shock). Vasodilators such as sodium nitroprusside, nitroglycerin, and other antihypertensives reduce SVRI.Increased PVRI is indicative of pulmonary hypertension and may be classified as being either primary or secondary. Primary pulmonary hypertension is an intrinsic lung disease developing over many years and typically refractory to treatment. Secondary pulmonary hypertension may develop as a result of acute respiratory distress syndrome, application of positive end-expiratory pressure
(PEEP), or development of mitral or aortic stenosis. Treatment of pulmonary hypertension begins with institution of increased inspired oxygen fractions due to oxygen's effect as a potent pulmonary vasodilator. Nitroglycerin and morphine sulfate also are helpful in the acute treatment of pulmonary hypertension. Decreased PVRI occurs in the setting of various shock states. Treatment is rarely instituted to specifically increase PVRI alone.Perfusion pressure and vascular resistance determine total blood flow to an organ, but absolute values of these determining factors do not define the shock state. For example, a high vascular resistance is commonly compensatory for reduced systemic perfusion pressure. The same numeric value of high resistance may contribute to organ dysfunction when it is so high that perfusion pressure cannot overcome it. When organ blood flow is maldistributed, as in septic shock or abdominal compartment syndrome, multiple organ dysfunction may occur despite normal systemic perfusion pressures. It is also important to recognize that vascular resistance numbers are calculated and are inversely proportional to CI. Therefore, therapy should usually be directed at enhancing CI in addition to reducing vascular resistance as simply reducing vascular resistance may reduce perfusion pressure.Ventricular Stroke Work IndicesThe ventricular stroke work indices describe how much work the ventricles perform and can identify patients with poor cardiac function. They may also be useful to construct ventricular function curves to assess a patient's response to therapy. As with vascular resistance, the work performed by the heart can also be calculated using the laws of physics. Work is calculated as the force generated multiplied by the distance over which the work is performed. Clinically, the force generated (per area) by each side of the heart is the change in pressure it creates across the ventricle. The distance (per area) is the volume of blood ejected with each beat (SVI) normalized for patient size. Therefore,
Increased LVSWI/RVSWI is relatively uncommon, but may be encountered in patients with ventricular hypertrophy, pulmonary hypertension, or in athletes. Decreased LVSWI/RVSWI is much more common and may be seen in various shock states; heart failure; aortic or mitral stenosis; myocardial depression, ischemia, or infarction; or advanced age. When evaluating decreased ventricular stroke work, it is important to keep in mind that the decreased function may be due to decreased intravascular volume (decreased SVI), changes in vascular resistance (increased MAP or MPAP), or decreased contractility. If preload and afterload remain constant, decreases in stroke work indicate decreases in ventricular contractility.Volumetric VariablesThe clinical accuracy of pressure-based monitoring techniques is limited by a variety of factors including proper catheter positioning, pressure transducer calibration, and pressure waveform interpretation. By the Frank–Starling principle, ventricular preload is defined as myocardial muscle fiber length at end-diastole with the appropriate clinical correlate being end-diastolic volume. As ventricular chamber volume cannot be directly measured, intracardiac filling pressures such as PAOP and CVP have been used as estimates of end-diastolic volume under the erroneous assumption that ventricular compliance remains constant. Ventricular compliance, however, is constantly changing in the critically ill, resulting in a variable relationship between pressure and volume. Further, PAOP and CVP must be measured relative to an arbitrary reference point (typically the perceived position of the right atrium) and are subject to the impact of increased intrathoracic and intra-abdominal pressure (as may occur with acute lung injury, PEEP, intra-abdominal hypertension, abdominal compartment syndrome, etc.) (Fig. 157.2). Although attempts
may be made to calculate transmural PAOP and CVP values, these estimates are inexact and the level of precision necessary to measure CVP accurately at the bedside is rarely performed [48]. As a result, changes in PAOP and CVP as commonly measured do not directly reflect changes in intravascular volume in the critically ill and may lead P.1651
to inappropriate clinical interventions and under-resuscitation [41].In the 1990s, a new generation of monitoring technologies were introduced that provide volumetric as opposed to pressure-based estimates of hemodynamic function. These included continuous CO, right ventricular ejection fraction (RVEF), and right ventricular end-diastolic volume index (RVEDVI), via a modified pulmonary artery catheter, or global ejection fraction (GEF), global end-diastolic volume index (GEDVI), intrathoracic blood volume index (ITBVI), and extravascular lung water (EVLW) via an arterial catheter using the arterial pulse contour analysis technique. Continuous volumetric monitoring provides a minute-by-minute assessment of patient response to therapeutic interventions, potentially allowing more rapid and effective resuscitation compared to traditional pressure-based monitoring techniques [27,49,50,51,52]. Both RVEDVI and GEDVI have been demonstrated to be superior to PAOP and CVP as predictors of preload recruitable increases in CI during shock resuscitation [27,40,41,49,50,51,52]. Further, several studies have demonstrated either significantly improved organ perfusion and function or increased patient survival when volumetric resuscitation endpoints are employed [27,49,50]. More recently, arterial pulse contour analysis has been used to measure stroke volume variation (SVV), the variation in beat-to-beat stroke volume during a single respiratory cycle, as well as pulse pressure variation (PPV), the beat-to-beat difference between SBP and DBP. Both of these parameters have been suggested to be valuable predictors of hypovolemia and fluid responsiveness [53]. These advanced hemodynamic monitoring techniques are appropriate for patients with shock who fail to respond appropriately to initial attempts at resuscitation using conventional endpoints.Oxygen Transport VariablesWith recognition of the importance of oxygen delivery (DO2) and oxygen consumption ([V with dot
above]O2) in the treatment of the various shock states, monitoring of a patient's oxygen transport
balance has become commonplace (Table 157.3). The foremost question in critical care is whether oxygen transport to the tissues is sufficient to meet the demand for oxygen at the cellular level.Oxygen transport represents the balance between supply and demand. When supply exceeds demand, the cellular oxygen requirements of the body are being met, and normal metabolic processes proceed uninhibited. When oxygen supply equals demand, vital functions may progress normally, but with little physiologic reserve, such that a relatively minor insult can upset the oxygen transport balance. In such a situation, organs that possess a high baseline oxygen extraction, such as the heart, are at significant risk for ischemia. When shock-induced systemic or regional malperfusion exists, oxygen demand exceeds supply, and the available cellular oxygen is inadequate to support normal physiology. Energy must therefore be produced via anaerobic metabolism with production of lactic acid as a by-product. As lactic acid cannot be reutilized in the absence of oxygen, it accumulates leading to metabolic acidosis, cellular injury, and cellular death. Left unchecked, this imbalance in oxygen transport will result in the development of multisystem organ failure and patient death. The role of the intensivist is to recognize oxygen supply imbalances at the cellular level, initiate therapeutic interventions to increase oxygen delivery, prevent further organ dysfunction, ensure adequate physiologic oxygen reserve to cope with acute increases in oxygen demand, and improve patient outcome from shock.Knowledge of the oxygen transport equations is essential to understanding the pathophysiology and appropriate treatment for the various shock states. Any assessment of oxygen transport begins with the calculation of DO2 and [V with dot above]O2. To accomplish this, the oxygen content of the
blood at various points in the systemic and pulmonary circulation must be identified (Fig. 157.3). Central to these calculations are the recognition that (1) oxygen may be either “bound” or “unbound” to erythrocytes, (2) each gram of hemoglobin (Hgb) can carry up to 1.34 mL of oxygen,
(3) the solubility of oxygen in blood is 0.0031 mL per dL, and (4) the amount of oxygen carried by Hgb depends upon its saturation.
Figure 157.3. Oxygenation calculations. CaO2, arterial oxygen content; PaO2, arterial oxygen
tension; SaO2, arterial oxygen saturation; CvO2, venous oxygen content; PvO2, venous oxygen
tension; SvO2, mixed venous oxygen saturation; Ca–vO2, arterial–venous oxygen content
difference; OUC, oxygen-utilization coefficient.The oxygen content of arterial blood as it leaves the heart may be calculated as:
In a similar fashion, the oxygen content of venous blood as it returns to the heart may be calculated as:
The partial pressure of oxygen in venous blood (PvO2) is typically 35 to 40 Torr. As a result, for
most purposes, the contribution of dissolved oxygen in venous blood is so small as to be clinically insignificant and is often disregarded. The arterial–venous oxygen content difference (Ca–vO2)
therefore represents the amount of oxygen extracted by the tissues and organs of the body. It is frequently elevated in shock, due to the increased oxygen demands of injured tissue, and represents an important resuscitation endpoint. The Ca–vO2 is calculated as:
Ca–vO2 is an important indicator of the relative balance between CI and [V with dot above]O2. A
Ca–vO2 in excess of 5.5 mL per dL of oxygen suggests that CI is inadequate to meet cellular
oxygen demands and that anaerobic metabolism and lactic acidosis may result. Maneuvers to improve CI and DO2 should be performed to meet the patient's cellular oxygen demand and reduce
Ca–vO2 to a normal range.
The volume of oxygen delivered from the left ventricle (DO2) and the amount of oxygen consumed
by the organs ([V with dot above]O2) provide the clinician with vital information by which to assess
the patient's overall oxygen transport balance. DO2 is determined by two factors: the volume of
oxygen in blood P.1652
(CaO2) and the blood flow delivered (CI). Values indexed to BSA allow comparison across patients
of differing body habitus, so that
[V with dot above]O2 is calculated similarly, using Ca–vO2 to account for the oxygen consumed by
the body:
One of the most important determinants of tissue DO2I is Hgb concentration. The optimal Hgb
concentration during shock resuscitation remains a topic of significant debate. Although previous clinical trials concluded that a Hgb concentration of 7 g per dL is sufficient and that transfusion to higher levels provides no survival benefit, it must be remembered that hemodynamically unstable patients, including hemorrhagic shock victims, were excluded from the study [54]. Further, patients with recent acute myocardial infarction or unstable angina were felt to require a higher Hgb concentration to ensure adequate DO2I. More recent studies in hemorrhagic shock patients,
however, have demonstrated significantly improved survival among patients resuscitated to a Hgb > 11 g per dL [55]. Recent evidence-based medicine guidelines have advocated higher Hgb levels in patients with myocardial ischemia, severe hypoxemia, acute hemorrhage, cyanotic heart disease, lactic acidosis, or closed head injury [2]. Although a subject of continued controversy, the optimal Hgb concentration can appropriately be considered the level that restores a patient's oxygen
transport balance while minimizing the potentially detrimental infectious and immunosuppressive effects of allogeneic blood.Shock Resuscitation AdequacyResuscitation of the critically ill patient who has developed one of the shock states is an ongoing process. It requires constant assessment of the patient's response to resuscitative therapy. In the patient whose shock state and oxygen transport balance fail to improve, the administered therapies must be reconsidered and adjusted as necessary to achieve the desired outcome. To guide this dynamic resuscitation, “resuscitation adequacy” endpoints may be employed.Mixed Venous OximetryContinuously measured SvO2 correlates well with calculated oxygen extraction ratios and
represents a valuable endpoint for assessing the adequacy of shock resuscitation [56]. The four factors affecting SvO2 are (1) SaO2, (2) Hgb concentration, (3) CO, and (4) [V with dot above]O2.
Increases in any of the three variables affecting DO2 (SaO2, Hgb concentration, and CO) result in
an increase in SvO2, whereas uncompensated increases in [V with dot above]O2 result in a decrease
in SvO2. The SvO2 measured in the proximal pulmonary artery is a global flow-weighted average of
the effluent blood from all perfused vascular beds. SvO2 does not reflect the oxygenation of
nonperfused tissues; thus, a normal SvO2 does not mean that all organs are adequately oxygenated.
In the absence of a pulmonary artery catheter, the mixed central venous oxygen saturation (ScvO2)
may be measured either intermittently using a venous blood gas drawn from a central venous catheter whose tip is located in the superior vena cava or continuously via a special oximetric central venous catheter [1]. It should be recognized that SvO2 and ScvO2 are not equivalent
measurements with normal ScvO2 values being 0.05 to 0.1 higher than SvO2.
A low SvO2 (less than 0.65) virtually always indicates an unfavorable disturbance in the normal
balance between DO2 and [V with dot above]O2. Normal or high values of SvO2 are more difficult
to interpret. A normal SvO2 in a patient with otherwise normal hemodynamics generally indicates a
stable condition with a satisfactory oxygen transport balance. A high SvO2 (greater than 0.75) is
difficult to interpret and implies a either a maldistribution of peripheral blood flow, providing some vascular beds with DO2 in excess of consumption, or the presence of “shunting” in which
oxygenated blood is returned to the heart without releasing its bound oxygen. This state of vaso-deregulation is often associated with high-flow states such as cirrhosis, sepsis, pregnancy, and inflammation.Arterial LactateAs discussed previously, shock is hypoperfusion resulting in inadequate DO2 to meet tissue oxygen
demand at the cellular level. The resulting oxygen debt forces cells to switch to anaerobic metabolism to make adenosine triphosphate by the inefficient method of glycolysis. The by-products of glycolysis are hydrogen ion, pyruvate, and lactate. If aerobic metabolism is restored through resuscitation and improved tissue DO2, the excess hydrogen ion is buffered, and both
pyruvate and lactate are metabolized to yield adenosine triphosphate. Under continued anaerobic conditions, however, hydrogen ion and lactate accumulate within the cell, resulting in acidosis, injury, and cellular death. Serum lactate levels therefore provide the clinician with an excellent laboratory marker of the presence of anaerobic metabolism as well as resuscitation adequacy.Elevated serum lactate levels indicate that the patient has sustained a period of inadequate perfusion and oxygenation within the past 6 to 12 hours with the severity of lactic acidosis directly correlating with the severity of the shock insult. If such levels are rising, anaerobic metabolism remains ongoing and the magnitude of resuscitative therapy should be increased. A decreasing lactate level suggests that resuscitation has been adequate and anaerobic metabolism has resolved. Although serum lactate levels identify the presence of anaerobic metabolism, they are not specific in identifying the location of abnormal regional perfusion. Further, profound hypoperfusion can exist
despite normal lactate levels when there is inadequate blood flow to ischemic tissues. Some septic patients have increased lactate levels in the absence of hypoperfusion as a result of increased aerobic glycolysis. In this situation, the elevated lactate continues to be significant despite resuscitation and is an indicator of a potentially severe pathologic process. Patients with significant hepatic dysfunction do not clear lactate normally, and will therefore manifest higher lactate levels in the absence of anaerobic metabolism [57].Elevated lactate concentrations predict an increased mortality rate. The magnitude and duration of the elevation correlate with mortality and reversal of hyperlactatemia suggests a better prognosis. Mortality rates of 24% to 86% are seen if lactate has not normalized by 48 hours [57,58,59,60,61].Base DeficitThe presence of an elevated base deficit correlates directly with the presence and severity of shock [61,62,63]. It predicts fluid resuscitation requirements and is a rapidly obtainable monitor of resuscitation adequacy [62]. Further, base deficit normalizes rapidly with restoration of aerobic metabolism, making it a useful physiologic marker by which to guide resuscitation. Base deficit must be interpreted with caution in the patient who has P.1653
received exogenous sodium bicarbonate as it will no longer be useful as a predictor of resuscitation adequacy.Rutherford et al. identified that patients younger than 55 years of age without a head injury who demonstrate a base deficit of -15 mmol per L have a 25% mortality rate [63]. Patients with a head injury or patients older than 55 years without a head injury have a 25% mortality at a base deficit of -8 mmol per L. These authors suggested that base deficit could be used to identify patients in severe shock who might benefit from having operative procedures terminated early (so-called “damage control laparotomy”).Treatment PrinciplesPatient morbidity and mortality after development of one of the shock syndromes correlates directly with the duration and severity of malperfusion. The intensivist must therefore rapidly diagnose the presence and cause of shock, restore systemic and regional perfusion to prevent ongoing cellular injury, and prevent the development of end-organ failure. The intensivist must command a strong understanding of the various therapeutic options for each of the shock states. Using the hemodynamic variables and calculations previously described, shock resuscitation should focus on assessment of preload, contractility, afterload, and oxygen transport balance with the intent to optimize the patient's end-organ perfusion and cellular oxygenation. In addition, the etiology for the shock state should be investigated to treat and/or correct the underlying cause. This may be simple, as in needle decompression for a tension pneumothorax, or may be complex, as in the treatment of sepsis.PreloadIn almost all shock states, a component of diminished preload, either relative or absolute, exists. Therefore, the initial therapeutic intervention for almost all patients in shock should be a crystalloid bolus of 20 mL per kg with subsequent resuscitation guided by signs of improved organ perfusion: reduction in tachycardia, restoration of normotension, maintenance of adequate urinary output, return of normal mentation, improvement in systemic oxygenation, and/or correction of abnormalities in serum lactate or base deficit. In patients with preexisting cardiopulmonary disease or those who do not respond to resuscitation as expected, invasive hemodynamic monitoring may be of value in achieving these goals.Over-resuscitation with intravenous fluids should be avoided and can cause acute lung injury, intra-abdominal hypertension, and abdominal compartment syndrome. Although some authors have suggested the use of colloid-based resuscitation to avoid such complications, large-scale clinical trials and meta-analyses have failed to demonstrate a survival advantage to such an approach [64,65]. A subset analysis of the SAFE trial demonstrated an increased mortality in head injured patients who received colloid-based resuscitation [66]. A balanced resuscitation using a combination
of crystalloid and colloid reduces the required resuscitation volume and appears to be associated with decreased organ dysfunction and failure [65].In patients with hemorrhagic shock, blood product transfusions should be considered early in the volume resuscitation phase as increasing evidence from the battlefield has demonstrated improved survival with early, aggressive blood, plasma, and platelet transfusions to restore adequate hemoglobin concentration and normal coagulation [55]. Current evidence suggests that a 1:1:1 ratio of packed red blood cells/plasma/platelets reduces the morbidity and mortality of hemorrhagic shock [67,68].ContractilityResuscitative therapy should optimize the patient's heart rate. Although tachycardia may partially compensate for low perfusion, further increases in heart rate may only decrease diastolic filling of the heart and reduce CO. Treatment of pain and anxiety as well as control of supraventricular tachyarrhythmias in the volume-resuscitated patient can improve CO. In bradycardia from neurogenic shock, atropine-induced blockage of parasympathetic stimulation may help ameliorate the hypoperfusion by raising heart rate and CO. Patients taking beta-blockers who have inappropriately low heart rates may benefit from administration of both calcium and glucagon. Those with pacemakers who are unable to raise their own heart rates in response to shock will frequently benefit from resetting their pacemakers to a more physiologically appropriate higher rate.Contractility agents should be considered only after adequate attempts to improve preload have been made. Dopamine, a naturally occurring catecholamine that is the immediate precursor of norepinephrine, is a widely used agent with a variable dose response. Classically, low rate (0 to 3 μg per kg per minute) or so-called “renal dose” dopamine was advocated to increase glomerular filtration rate, renal blood flow, and urinary output. The clinical benefit of such therapy, however, has been disproven and dopamine's use in this fashion has largely been abandoned [69]. In moderate doses (5 to 10 μg per kg per minute), cardiac contractility and heart rate are increased through stimulation of cardiac beta-receptors. High-dose dopamine therapy (10 μg per kg per minute and higher) results in stimulation of α-adrenergic receptors, elevating systemic blood pressure. Although a valuable tool in improving cardiac performance, dopamine should be used with caution in patients with coronary artery stenosis because of the potential risk of tachycardia and increased myocardial oxygen demand.Dobutamine is a synthetic catecholamine that also acts on β1-receptors, but, unlike dopamine, does
not directly release norepinephrine. Dobutamine has both chronotropic and systemic vasodilatory effects, reducing afterload and increasing CO in the weakened heart. However, it should be used with caution in hypovolemic, vasodilated states, as it may decrease blood pressure and increase heart rate, leading to reduced systemic perfusion [70].Norepinephrine is a naturally occurring catecholamine with both α- and β-adrenergic activity. As a potent vasoconstrictor, there is some reluctance to use this agent because of its possible effects on mesenteric and renal blood flow. However, in the setting of an appropriately volume-repleted patient who remains hypotensive, norepinephrine has been shown to be effective and safe and may have beneficial effects on renal function [71]. It should be considered the vasopressor of choice of all but the cardiogenic shock states [2].Amrinone is a noncatecholamine intravenous inotrope that, like dobutamine, has vasodilatory effects. Its mechanism of action is as a phosphodiesterase-III inhibitor, raising intracellular cyclic adenosine monophosphate levels. In patients with shock due to congestive heart failure, amrinone increases stroke volume without an effect on heart rate. In some patients with hypovolemic shock, its vasodilatory properties preclude its use because of dramatic hypotension.AfterloadIf preload is optimized and hemodynamic goals have still not been met, afterload should be assessed and corrected as needed. The persistently hypotensive patient should not be considered a candidate for afterload reduction. In patients with hypertension or even normotension, however, afterload reduction may allow for improved CO and, hence, improved resuscitation especially in patients with decreased contractility.
Sodium nitroprusside is a commonly used agent with the advantages of rapid onset and short duration, making it ideal P.1654
for titration in the hemodynamically labile patient. Nitroprusside acts as both a venous and arterial vasodilator, in essentially equal amounts. However, it should be used with caution in patients with coronary artery disease when concerns of coronary steal and myocardial ischemia exist. Alternatively, intravenous nitroglycerin may be used. Although primarily affecting venous capacitance, nitroglycerin also decreases arterial resistance and may improve CO. Angiotensin-converting enzyme–inhibiting agents may also be of significant value in reducing afterload in the normovolemic patient with poor cardiac function.Afterload may also be reduced mechanically, using a percutaneously placed intra-aortic balloon counterpulsation pump (IABP). IABP is most commonly used in myocardial infarction and in the immediate postoperative period following coronary artery bypass. IABP provides mechanical afterload reduction and improves coronary artery perfusion. IABP demonstrates survival benefit primarily in myocardial infarction patients who have reversible pathology and has been used successfully in high-risk patients undergoing noncardiac surgery [72].Although afterload reduction may be beneficial in improving cardiac performance, the patient with aortic stenosis leading to shock may be harmed by use of these agents. In this disease, left ventricular wall tension remains high, and afterload reduction only serves to reduce coronary perfusion by reducing coronary perfusion pressure.In septic and neurogenic shock, it will often be necessary to counteract the vasodilatory effects of the underlying disease process. Recent studies suggest that norepinephrine should be used as the first-line agent and vasopressin in low doses (0.01 to 0.04 U per minute) should be added when patients fail to respond to norepinephrine. Vasopressin should be used with caution in patients with poor cardiac function [2]. Studies in Europe with terlipressin, a synthetic vasopressin analogue with theoretical advantages over arginine vasopressin, are ongoing [73].Oxygen TransportThe goal of shock resuscitation is to improve tissue oxygenation so that oxygen delivery meets the demand of cells to function aerobically. Beginning in 1977, Shoemaker et al. suggested in a series of clinical trials that resuscitation to achieve “supranormal” CI (> 4.5 L per minute per m2), DO2I
(> 600 mL per minute per m2), and [V with dot above]O2I (> 170 mL per minute per m2) levels was
associated with improved high-risk patient survival following operative procedures [74,75]. Subsequent trials, however, identified that it is a patient's ability to spontaneously reach such supranormal levels of oxygen transport that is predictive of survival and not the applied intervention itself [74,75,76,77,78,79]. In fact, Balogh et al. have demonstrated that supranormal resuscitation is associated with a higher incidence of over-resuscitation, intestinal malperfusion, abdominal compartment syndrome, multiple system organ failure, and death [80]. They concluded that traumatic shock patients should be resuscitated to achieve a DO2I of 500 mL per minute per m2
during the first 24 hours of resuscitation and that maintaining such a level beyond 24 hours is rarely beneficial unless evidence of ongoing shock is present. The potential benefits of adequate sedation and analgesia as a method to reduce oxygen demand must always be considered in any patient who presents with shock.Systematic Approach to the Treatment of ShockPerhaps most noteworthy in the recent literature on the treatment of shock are multiple studies demonstrating that a proactive, systematic, evidence-based approach to shock resuscitation improves patient outcome (Table 157.4) [1,2,3]. The Surviving Sepsis Campaign is a multimodality approach to timely resuscitation of the septic patient encompassing diagnosis, source control, fluid resuscitation, vasoactive medications, appropriate antimicrobial therapy, correction of oxygen transport inequalities, low-dose steroid administration for relative adrenal insufficiency, selective use of recombinant human activated protein C, targeted blood product administration, mechanical
ventilation strategies geared at reducing barotrauma, sedation, and neuromuscular blocking protocols that include daily interruption, glycemic control, deep venous thrombosis prophylaxis, and stress ulcer prophylaxis [2,3]. This comprehensive approach to the critically ill patient has also been applied with marked success outside the ICU setting using the “rapid response team” concept to treat nonseptic shock patients as well [81]. Many of these same tenets of shock resuscitation are also applicable to the other shock states that may be encountered.
Table 157.4 Summary of Advances in Managing Shock Based on Randomized Controlled Clinical Trials
Patients with hypotension or evidence of anaerobic metabolism should receive immediate early goal-directed resuscitation to restore systemic perfusion and oxygenation within six hours [1,2]
Fluid resuscitation using either 0.9% normal saline or 4% albumin may be considered equivalent with similar outcomes in 28-day mortality [64].
Patients in shock should be resuscitated to maintain a mean arterial pressure ≥ 65 mm Hg [2,3]
Centrally administered norepinephrine or dopamine should be considered the vasopressors of choice for noncardiogenic shock resuscitation [2]
Dobutamine is the inotropic agent of choice for cardiogenic shock [2] Low-dose dopamine infusions should not be used for renal protection [69] Resuscitation to achieve supranormal levels of oxygen delivery or consumption do not
improve patient outcome [78,80] Recombinant human activated Protein C should not be administered to septic patients with
an APACHE-II < 25 [2] Corticosteroids should not be used to treat septic shock unless the patient demonstrates
evidence of symptomatic adrenal insufficiency [2] Transfuse packed red blood cells when hemoglobin decreases to < 7.0 gm/dL. A higher
hemoglobin level is appropriate in patients with myocardial ischemia, severe hypoxemia, acute hemorrhage, cyanotic heart disease, lactic acidosis, or closed head injury [2,54].
A 1:1:1 red blood cell/plasma/platelet transfusion strategy should be utilized in patients with massive hemorrhagic shock (≥4 units of packed red blood cells over 1 h or ≥ 10 units over 24 h [more than one total blood volume]) [67].
Hypothermia should be rapidly corrected in any patient with shock [30]. Patients resuscitated to elevated levels of preload have significantly improved visceral
perfusion than those resuscitated to normal preload with additional inotropes. Elevated preload levels do not affect pulmonary function [49].
Shock resuscitation continues to evolve as new research identifies the pathophysiology of the various shock states. Numerous treatments for shock are currently being evaluated P.1655
including nitric oxide therapy, levosimendan, intravenous immunoglobulin, continuous hemodiafiltration, factor VIIa, and statin therapy among others [82,83,84,85,86]. Time will determine whether these therapies provide a survival benefit to the patient with shock.SummaryShock is a common and highly lethal condition that is commonly encountered in the critically ill patient. Its cause is varied and complex. It may present in a spectrum from subclinical laboratory abnormalities to complete cardiovascular collapse. A high degree of clinical suspicion and thorough evaluation are essential to both making the diagnosis and initiating timely resuscitative therapy. Inadequate tissue perfusion that is unresponsive to initial treatment should lead to early, goal-directed therapy. Correction of abnormalities in ventricular preload, contractility, afterload, and oxygen transport are the first steps to breaking the cycle of cellular injury and microcirculatory failure. Correction of the precipitating, underlying condition is essential for patient survival. Early
treatment to predefined physiologic endpoints reduces the potentially devastating complication of end-organ dysfunction and failure.
Chapter 158Resuscitation from Shock Following InjuryDonald H. JenkinsJohn B. HolcombPhillip A. LetourneauDustin L. SmootStephen L. BarnesAfter the initial evaluation and operative management of the surgical/trauma patient, many patients require further resuscitation, support, and care in an intensive care unit (ICU) setting. This chapter provides a brief outline of considerations, priorities, treatment algorithms, and the newest innovations that may assist any intensivist tasked with managing such critically ill surgical patients.Statement of the ProblemSurgical patients die from shock abruptly through lack of oxygen delivery to the heart and brain, or subacutely through development of multiple organ dysfunction from late recognition of shock or inadequate resuscitation. Unlike the typical nonsurgical critically ill patient, exsanguination is often the cause of death in the surgical/trauma patient, second only to central nervous system injuries as the cause of death of trauma victims in the United States [1,2,3]. The control of hemorrhage has been identified as a priority in modern trauma patient care, second in importance only to adequate ventilation [4]. Advanced Trauma Life Support teaches a schema that incorporates the vital signs, skin color, capillary refill, and mentation to alert the physician to how severely injured the patient may be and help to quantify how much blood the patient may have lost [4]. By the time the blood pressure falls, the patient has lost 30% to 40% of his or her blood volume, or approximately 2,000 mL. This situation demands rapid action, but action should not wait until this point has been reached.P.1657
One classification system defines four types of shock: Hypovolemic (such as dehydration, diarrhea, and hemorrhage, the most common form of shock following major trauma), distributive (such as septic shock, the most common form of shock in the late phase of recovery—5 days or more—after major surgery/trauma), cardiogenic (such as from massive myocardial infarction or arrhythmia), and obstructive (such as from tension pneumothorax, pulmonary embolus, or pericardial tamponade). By far, hemorrhagic shock is the most common form following major surgery/trauma and the major focus of this chapter (although the astute physician should always keep tension pneumothorax in the differential diagnosis). Therefore, in most instances, the ICU physician faced with a surgical patient in shock should direct initial efforts toward correction of hypovolemia.Without obvious external bleeding, vital signs and evidence of organ hypoperfusion are assessed to evaluate the patient for significant or ongoing hemorrhage. A falling hematocrit may be a sign, but as hemorrhage causes loss of cells and fluid in equal proportion, an isolated normal hematocrit should not be reassuring to the clinician. With very rapid hemorrhage, a patient can die with a normal hematocrit. A fall in central venous oxygen saturation when the cardiac output remains the same may be one of the earliest signs of hemorrhage in the ICU setting as the body begins to extract more oxygen from the remaining blood.Physiology of Effects of HemorrhageThe physiologic responses to hemorrhage can be broken into three categories: Hemostasis, oxygen delivery, and immunology.HemostasisIf bleeding does not stop, then no intervention can prevent death. It is this concept that has led to some of the most heated debates in the resuscitation literature: “Does resuscitation promote tissue perfusion and cellular metabolism, thus increasing survival, or does the increase in blood pressure destroy clot, promote rebleeding, and decrease survival?” [5]. The astute physician recognizes that both concepts are true. Cellular metabolism must be ensured, without overwhelming the clotting mechanism.After injury, the body attempts to stop hemorrhage by clotting at the site of vascular injury. This is accomplished by the interaction of circulating clotting factors, platelets, and tissue factors from the injured cells. These factors work primarily to form a “plug” initiated by the physical presence of the platelets and augmented by the cross-linking of fibrin to form a more permanent seal. The tissue injury factors released may also lead to constriction of the local blood vessels to decrease the blood flow to the leaking area concurrently with platelet plug formation and is mediated both locally by tissue factors as well as centrally. Finally, when the blood loss leads to a fall in the blood pressure, the clotting efforts are aided by a smaller vessel diameter, decreased wall tension, and lower pressure head.Oxygen DeliveryIn 1872, Gross called shock a “rude unhinging of the machinery of life.” Although this definition is accurate, it is not precise. It is at the level of cellular oxygen delivery and utilization that the understanding of shock is defined. Without oxygen, the cells may survive briefly using anaerobic metabolism. Many of the physiologic defense mechanisms work to augment this delivery and depend on oxygen-carrying capacity, cardiac output, and oxygen delivery to and utilization by the cell.The oxygen-carrying capacity of blood depends on the amount of circulating hemoglobin, which diminishes continually during hemorrhage. Although erythropoietin stimulates the production of new red blood cells (RBCs) and eventually restores hemoglobin over weeks, this response does not acutely restore oxygen-carrying capacity [6]. As hemorrhage proceeds, the body becomes incapable of supporting metabolic need. The primary defense, however, is the extra capacity inherent in the human system: only approximately 25% to 30% of the transported oxygen is normally used, leaving central venous or mixed venous oxygen saturations in the range of 70%. When fully stressed, extraction improves as anaerobic metabolism leads to lactic acidosis, which shifts the oxygen dissociation curve to favor release of oxygen at the tissue level. This allows much more oxygen to be removed from the hemoglobin, and much lower central venous oxygen saturations.
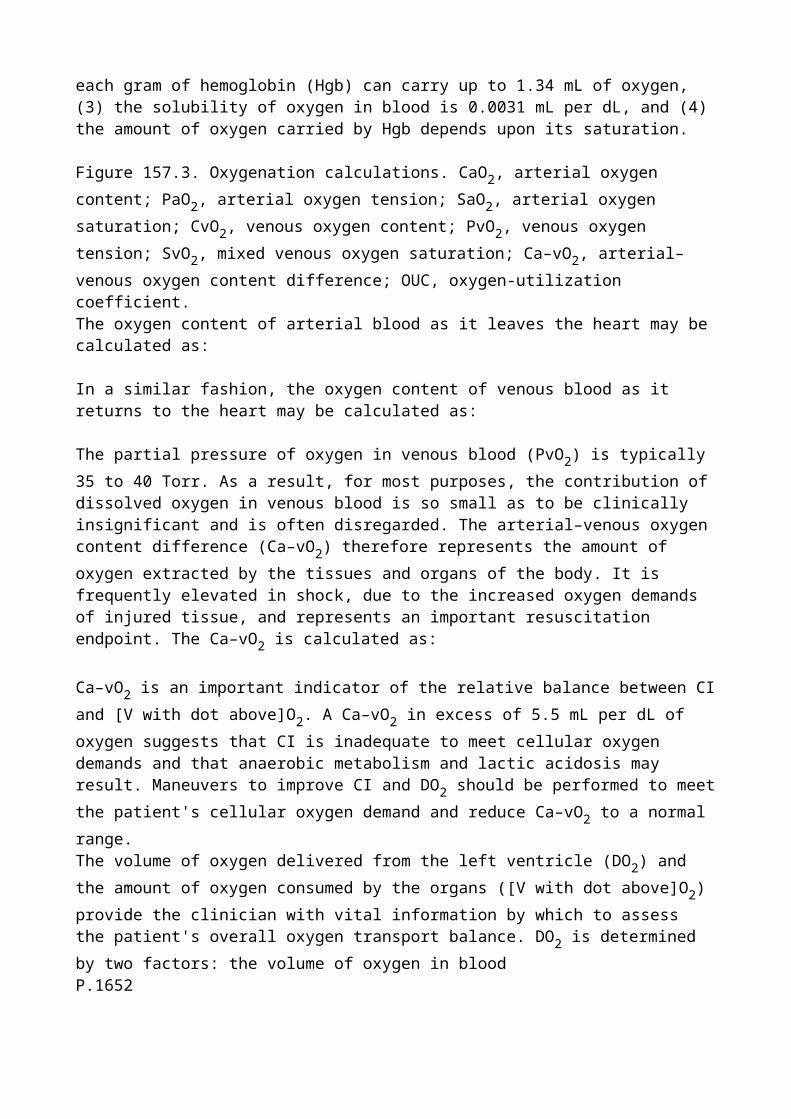
Cardiac output is the product of heart rate and stroke volume. There is reserve built into the heart rate, in that most people use only approximately two-thirds of their maximal heart rate. Pain, fear, and a variety of baroreceptors release catecholamines and other factors in response to hemorrhage. These lead to an increased heart rate, and thus increased cardiac output and oxygen delivery. With a few exceptions, in the elderly or those with heart disease, this response is maximally achieved by the body, in an unaided fashion.The stroke volume can be increased by increased contractility through the direct effects of many of the same substances that increase heart rate. In hemorrhage, however, the primary component of cardiac output is the volume of blood coming into the heart (preload). During hemorrhage, the preload falls. As the blood pressure falls, oncotic forces predominate and fluid begins to shift into the vascular space. This “borrowing” of fluid from the interstitial, and ultimately from the intracellular, space is gradual, with a gradual restoration of the blood pressure—often not to normal—which allows time for the clotting mechanisms to stop the bleeding and stabilize the clot.Other factors that restore the preload include the prevention of further fluid loss via the kidney. A lower blood pressure leads to less filtration and less fluid removed in urine. In addition, antidiuretic hormone and the renin–angiotensin systems act to augment this response. Catecholamines and large proteins circulate as part of the defense signaling systems. These augment the oncotic pull. The glucose that increases with the release of corticosteroids also acts to pull fluid into the vascular space. Finally, the body is willing to shunt blood away from most areas of the body to support cardiac preload and the brain. This shunting is very evident in the pale clammy skin of hemorrhagic shock. Initially it is less evident in the relative ischemia that occurs in every other organ of the body.Oxygen delivery (DO2) to the tissues includes the variables of cardiac output, arterial oxygen
content (CaO2, the total amount of oxygen in the blood), which includes the amount of hemoglobin
that is present. During hemorrhage, these components are altered, and oxygen delivery may be decreased. Cardiac output can be indexed to body surface area and expressed as cardiac index, which when multiplied by CaO2 yields an oxygen delivery index (DO2I). Normal DO2I is roughly
450 mL per minute per m2 and it may increase by as much as 30% in response to injury. The primary goal of shock resuscitation is the early establishment of “adequate” oxygen delivery (DO2)
to vital organs; however, adequate is subject to ongoing debate.The complications of a “successful” resuscitation that should be watched for are related to ischemia and reperfusion injury. These may manifest as multiple organ dysfunction syndrome or individual organ dysfunction. Hepatic dysfunction P.1658
may present as jaundice and coagulopathy. Pulmonary dysfunction and acute respiratory distress syndrome may be seen as renal failure, with rising blood urea nitrogen and creatinine. Compromise of intestinal mucosa may lead to sepsis, bleeding, or perforation.ImmunologyHemorrhagic shock alone, without tissue injury, was once thought to have minimal consequences [7]. Hemorrhagic shock alone has been shown to result in a multitude of responses, however, especially in the immune system. The immune system is intended to protect the body from infectious invaders and remove aberrant cells to prevent cancer. During shock, cells produce messengers or mediators that signal for the help of this system [8]. During reperfusion, these mediators are released widely into the systemic circulation.Currently, a focus in hemorrhagic shock research is the effect of resuscitation on the immune and coagulation system. Extensive research in the last decade has shown that hemorrhagic shock from trauma activates both the inflammatory and coagulation system, resulting in profound perturbations in both. This is often manifested by a spectrum of clinical problems starting from acute lung injury, progressing to acute respiratory distress syndrome, systemic inflammatory response syndrome, hypo- or hypercoagulation, bleeding or diffuse thrombosis, and even multiple organ dysfunction syndrome [9]. One of the major areas of study involves the activated immune response that results
in enhanced activation and increased adhesion of leukocytes. During this activated stage, neutrophils can release harmful reactive oxygen species, which are thought to play a major role in loss of capillary integrity. This leads to edema and the sequestration of fluid in the tissues outside the vascular space.Although it has been clear that the immune response occurs in response to shock and reperfusion, it now seems that some of the resuscitation fluids used to treat the shock may trigger this altered immune and coagulation response. The immunologic response to various resuscitation fluids is now an area of intense research [10,11].Hemorrhagic Shock ManagementThe first goal in hemorrhagic shock, following assessment of the ABCs (airway, breathing, and circulation), is to stop ongoing bleeding. In the surgical/trauma patient reaching the ICU, this has generally been accomplished in the emergency department (ED), interventional suite, and/or operating room. During the ICU phase, resuscitation is continued, and can last 24 to 48 hours. The goal of resuscitation is to restore normal perfusion to all body organ systems, using the components of oxygen delivery: hemoglobin, cardiac output, and oxygenation. In hemorrhagic shock, this primarily involves hemorrhage control, reversal of coagulopathy, and then administration of sufficient volumes of blood products and crystalloid fluid volume to restore normal aerobic metabolism.Confirmation of a hypoperfusion state (shock) is obtained through simple examination and a single blood test. Shock is diagnosed by the effect of hypoperfusion on the body's organ systems: low blood pressure, tachycardia, oliguria, tachypnea, decreased mental status or agitation, skin cyanosis, pallor, decreased pulse character, or mottling. Equivocal cases can be confirmed by obtaining an arterial blood gas and looking for a base deficit exceeding 6 or a serum lactate assay (more than 2 mmol per L). Hypoperfusion implies inadequate delivery of oxygen to the body's cells. Oxygen delivery is a function of cardiac performance, arterial hemoglobin content, and arterial oxygen saturation. All attempts to correct shock involve optimizing these three variables. Hypotension is not synonymous with shock, which can be present in a normotensive patient. Conversely, not all hypotensive patients are in shock. Hypotension, like many other physical findings, is but one sign helpful in the overall clinical picture of shock diagnosis. As detailed below, reestablishment of normal heart rate, blood pressure and urine output does not equate to resolution of shock; resolution of tissue hypoperfusion as manifested by lactate clearance does.Resuscitation of the patient in shock should be approached in two phases, based on the end points of the resuscitative effort. In the first phase, the patient should be resuscitated to a systolic blood pressure of 80 to 100 mm Hg or mean arterial pressure of 55 to 65 mm Hg, a urine output of 0.5 mL per kg per hour, and an arterial oxygen saturation of 93% or higher. These end points are pursued to prevent imminent death from hypoperfusion to the heart and brain, and should be achieved optimally within 1 hour.In the second phase, resuscitation is continued with fluid, as well as inotropic and vasopressor agents, as needed, to the goal of eliminating the base deficit of metabolic acidosis, or, if available, restoring the serum lactate or base deficit to a normal level. This end point is important in reversing systemic anaerobic metabolism, which, if unrelieved, leads inexorably to multiple organ failure (MOF). This goal should be accomplished within 12 to 24 hours.Lessons Learned from WarThe modern-day trauma system owes a large debt to combat casualty care. Techniques from system development to operating room procedures have their roots in battlefield medicine. Resuscitation as well, is no stranger to advancement during wartime. To understand the advancements made and differences that exist with modern combat resuscitation strategies it is important to understand the history of combat resuscitation.A modern ATLS resuscitation strategy of 2 L of crystalloid owes its roots to strategies developed during the Vietnam War. Based on research by Shires [12,13], Dillon [14], and others, the need for volume resuscitation was brought to the forefront to replace an interstitial volume debt secondary to intravascular movement in hemorrhagic shock. High volume crystalloid resuscitation strategies
were used to replace volume loss encountered by the bleeding soldier in ratios of 3:1 to as high as 8:1. The physiology was sound, but disappointingly when outcomes were examined, clinical efficacy in the way of improved survival was not seen over previous war efforts with Killed in Action rates of 16% for the US Civil War, 19.6% for World War I, 19.8% for World War II, and 20.2% for the Vietnam War [15]. In fact, the adopted strategy of IV fluid administration would spawn its own set of complications, most notably the emergence of Da Nang lung known more widely now as acute respiratory distress syndrome. Initially felt to be the result of the volume of resuscitation, eventually its mechanisms linked to immunologic effects would come to be understood by Ashbaugh et al. in their case series of 12 patients (seven with trauma) published in the Lancet in 1967 [16].High-volume crystalloid resuscitation strategies were further supported by Shoemakers early prospective study of 67 patients with greater than 2,000 mL of blood loss. Supranormal endpoints of resuscitation, defined as a cardiac index > 4.52 L per minute per m2, oxygen delivery ≥ 670 mL per minute per m2, and oxygen consumption ≥ 166 mL per minute per m2 were assessed against “standard” therapy. Survival was nearly double in the supranormal group as well as statistically significant decreases in length of ICU stay, mean number of organ P.1659
failures, and days of ventilation [17]. Despite these promising results, several other groups failed to achieve similar findings. More importantly with an ever increasing understanding of the immunology of intravenous fluids and resulting proinflammatory properties the complications of high-volume crystalloid resuscitation for combat casualties came into question.If aggressive crystalloid resuscitation was not the answer, then what would the optimal resuscitation strategy be? A report by the Institute of Medicine in 1999 as well as two consensus conferences held by Office of Naval Research, the US Army Medical Research and Material Command and the Uniformed Services University of Health Sciences in 2001 and 2002 tried to answer the question.The IOM report was the first to recognize the several inadequacies of the then standard fluid therapy. First noted was the paucity of good Level I and II data to support the then standard of care. Second, the immunologic activity of common intravenous fluids used and deleterious effects of high-volume resuscitation was better defined as it related to complications [17]. This report would mark a significant paradigm shift. Initial recommendations were to remove the racemic mixture of D and L Lactated Ringers (still clinically available) in favor of L-isomer only. Replacement of lactate with ketones was advocated. Finally, the report supported the initial battlefield use of low volume hypertonic saline (HTS) resuscitation [18]. A 250-mL bolus of HTS was chosen based on research showing decreased neutrophil activation as well as increased oncotic properties as well as the battlefield logistics of less fluid to carry for frontline medics.The 2001 consensus conference took it one step further by defining what the endpoints of resuscitation would be on the battlefield [19]. Triggers for fluid resuscitation would be systolic blood pressure less than 80 mm Hg or absence of palpable radial pulse, decreasing blood pressure, or altered mental status with no confounding brain injury [19]. This protocol allowed for “permissive hypotension” during resuscitation until definitive hemorrhage control. The goal was not to return blood pressure to normal, but rather to target clinical goals of mentation and palpable pulse. These protocols were developed with several civilian trauma studies in mind.The first by Bickel and Mattox done at the Ben Taub in which 598 adult patients sustaining penetrating torso trauma with a systolic blood pressure less than 90 were assigned to either standard fluid therapy with Lactated Ringers or IV cannulation with no fluid infusion. Although controversies with study design and protocol surround the results, a significant survival benefit 70% versus 62% was seen for the delayed resuscitation arm [20].Second were several studies that suggested early aggressive fluid resuscitation before hemorrhage control may have a deleterious effect. As early as 1964, Shaftan et al. published data showing the effects of aggressive volume correction slowed spontaneous control of arterial bleeding [21]. This was followed by military research data done in swine by Bickell et al. Adult swine had their
infrarenal aorta cannulated with a stainless steel wire. The wire was pulled creating a 5-mm aortotomy and free intraperitoneal hemorrhage. Eight pigs received 80 mL per kg of Lactated Ringers where the control group received nothing. Hemorrhage was significantly higher in the intravenous fluid group (2,142 ± 178 mL vs. 783 ± 85 mL, p < 0.05) as well as mortality (8 of 8 vs. 0 of 8, p < 0.05) [22]. This ultimately culminated in a complete 180-degree shift from the high volume crystalloid resuscitation seen in the Vietnam War.If awake, alert, and having a palpable pulse, a soldier sustaining a penetrating wound should have an IV placed, but no fluids would be infused. PO fluids would be encouraged and evacuation undertaken to the next level of care. If resuscitation had to be undertaken, again recognizing a low-volume strategy the recommendation of the panel was for 500 mL hetastarch (Hespan or Hextend) as FDA approval for HTS was lacking. The hetastarch bolus could be repeated at which point a reassessment was done and if no response the possibility of futility was entertained [23].Expanding on this the 2002 consensus conference held in conjunction with the Canadian Defense and Civil Institute for Environmental Medicine reexamined prehospital requirements for fluid therapy. The “hypotensive” strategy was again approved, but the recommendation for initial battlefield fluid was changed to hypertonic saline dextran (HTS-D) based on then current research showing a favorable volume expansion profile of the dextran with the inflammatory inhibition of the HTS component [24,25].Current strategies in the Iraq and Afghanistan wars are very similar. First and foremost, the problem had to be defined with the unique set of circumstances that are present in live fire situations. The first point of care would be the battlefield medic. It was recognized that logistical problems exist in bringing care to the wounded at the point of injury. Hemorrhage control still remains the first priority in resuscitating the injured patient, for if quick, effective hemostasis cannot be achieved fluid therapy has no hope of working in austere environments where definitive therapy may be hours away [23]. This has led to the reintroduction of vascular tourniquets, the use of Battlefield hemostatic dressings, and newer therapies such as Factor VII to arrest hemorrhage so that resuscitation efforts can be effective, a discussion of which is beyond the scope of this chapter.As recognized in the previous consensus conferences, if medics are to be mobile and effective on the battlefield they need the ability to carry their supplies with them [18,19,23,24]. This makes low-volume intravascular expansion much more attractive. For this reason, colloid solutions, specifically Hespan or Hextend, continue to be the fluid of choice for military applications [23]. HTS-D has fallen out of favor due to more current civilian prehospital data that has shown an increase in mortality in trauma patients during interim analysis of the recent ROC trial [26].With the choice of fluids now made (Hespan or Hextend), the next decision point is how to get those fluids into an injured soldier. Trauma providers know the key tenet of ATLS “two large-bore IVs in the antecubital fossa.” This principle becomes increasingly difficult in combat conditions. To this end, the US military takes a different approach. If awake, alert and having a palpable radial pulse, a wounded soldier with a palpable radial pulse have a single 18-gauge peripheral IV placed (chosen for ease of cannulation versus a larger bore IV) and PO fluids encouraged [23]. If IV access cannot be obtained or conditions will not allow access, a sternal intraosseous device is placed. Sternum was chosen as the reproducible target as extremity injuries prevail in current warfare and the trunk remains relatively protected with modern armor. The sternal IO can be placed with reproducible landmarks quickly and in low- or no-light conditions making it extremely beneficial in modern combat [23].Resuscitation then continues as appropriate with evacuation to the next level of care. It is at this level that the paradigm has shifted dramatically. The emphasis now is on damage control. This pertains not only to the way in which the operations are done (quick procedures leaving abdominal wounds open, temporary packing for hemorrhage control, and temporary vascular shunts) but also to the way in which resuscitation is continued. The use of early blood and coagulation component therapy as well as fresh whole blood (FWB) is emphasized. Again logistics dictate limited storage capabilities in far forward treatment centers. This continues to promote a walking blood bank using fellow combat troops as donors, a luxury not afforded by the civilian trauma provider.
Clinically, FWB has been demonstrated to reverse dilutional coagulopathy, with evidence that a single unit of FWB has a P.1660
hemostatic effect similar to 10 units of platelets [27,28,29,30,31,32,33,34]. In a retrospective study of the results of the FWB procedures for one U.S. Combat Support Hospital in 2004, 87 patients received 545 units. In that experience the FWB drive was called for only after the patient had received a massive transfusion, yet the transfusion of FWB resulted in significant improvements in both hemoglobin concentration and coagulation parameters [32].The nature of military medical logistics frequently limits the availability of FFP, platelets, and cryoprecipitate for transfusion in theaters, giving the battlefield physician few options in the treatment of traumatic coagulopathy. However, the use of FWB in massively transfused patients may circumvent the problem of dilutional coagulopathy. Consider the usual mixture of one packed RBC unit (335 mL) with a hematocrit of 55%, one unit of platelet concentrate (50 mL) with 5.5 × 1010 platelets, and one unit of FFP (275 mL) with 80% coagulation factor activity. This combination results in 660 mL of fluid with a hematocrit of 29%, 88,000 platelets per μL, and 65% coagulation factor activity. By definition, transfusion of these standard components will only serve to further dilute critical factors in a bleeding casualty. In contrast, FWB is replete with functional platelets as well as fully functional clotting factors. A 500-mL unit of FWB has a hematocrit of 38% to 50%, 150,000 to 400,000 platelets per μL, and 100% activity of clotting factors diluted only by the 70 mL of anticoagulant [35]. In addition, the viability and flow characteristics of fresh RBC are better than their stored counterparts that have undergone metabolic depletion and membrane loss.Initial retrospective studies by Holcomb found higher 24-hour (96% vs. 88%, p = 0.018) and 30-day (95% vs. 82%, p = 0.020) survival in a group of combat casualties when FWB was used [36]. The immunology and pathophysiology of improved clinical outcomes continues to be an active area of research. Also reported from military and civilian evidence is that higher ratio FFP to PRBC improves outcomes [37,38,39]. The exact ratio is still part of ongoing research, with some evidence suggesting that there may be a survival bias in those patients receiving higher ratios. Despite these controversies, the early and aggressive use of blood and coagulation factors forms the cornerstone of damage control resuscitation.
Damage Control ResuscitationThe concept of damage control resuscitation or hemostatic resuscitation has rapidly evolved on the modern battlefield. This concept is philosophically derived from the widely practiced damage control surgery approach to severely injured patients. Understanding the epidemiology of combat casualties is paramount to devising a logical resuscitation strategy. Most deaths (80%) in combat operations are not preventable [40,41]. Of the remaining 20% of potentially preventable deaths in combat casualties, two-thirds are from hemorrhage. Furthermore, the killed in action rate is lower than at any time in history, while the died of wounds rate has increased, largely due to improved body armor, rapid evacuation, improved extremity hemorrhage control, and medic training [40]. With the recent widespread use of tourniquets and hemostatic dressings for compressible hemorrhage control, the current unmet need is for rapid, effective interventions for noncompressible hemorrhage from the neck, axilla, thorax, abdomen, groin, and pelvis.Fortunately, most casualties receive at most one to four units of packed RBCs after injury and are not at high risk of presenting or developing a coagulopathy and subsequently dying [42]. Only 5% to 10% of all combat casualties require massive transfusion (10 or more units of packed RBCs) and this group constitutes those at risk for hemorrhagic death [43]. These same patients are those who will benefit from early use of recombinant activated factor VII (rFVIIa), as described in the Clinical Practice Guideline (Table 158.1).The 5% to 10% of all combat casualties that require massive transfusion fall into two broad categories. Group 1 patients are the wounded who are clearly in profound shock, arrive moribund, and are resuscitated with heroic efforts. These casualties do not pose a diagnostic dilemma; rather,
they require immediate hemorrhage control and very rapid resuscitation with the optimal ratio of all available products. Surgically, the only question is what cavity to enter first, as they usually have multiple significant injuries. Frequently, these casualties have severely injured extremities, requiring life-saving tourniquets and delayed completion amputations after successful truncal hemorrhage control. These casualties, if surviving the initial 10 to 15 minutes resuscitation in the ED, require the full massive transfusion protocol and surgical intervention described in the following sections.Group 2 patients are more difficult to recognize. They are typically the young soldier with incredible physiologic reserve who arrive “talking and looking good,” who are actually in shock, have had significant blood loss, and soon progress to cardiovascular collapse. This classic presentation occurs once a week at a busy combat hospital. The challenge is rapidly separating these critical casualties from those who are really hemodynamically stable. These casualties require rapid and accurate diagnosis of their hemorrhagic injury. This group needs immediate hemorrhage control, as fast as group 1; however, they are much more difficult to initially diagnose. Traditional reliance on mental status, blood pressure and pulse rate is notoriously inaccurate for individual risk stratification [44,45,46,47].Fortunately, there are five risk factors that are easily identified very early in the hospital course of severely injured casualties, each of which independently predicts the need for massive transfusion and/or increased risk of death. These simple variables are now available within 2 to 5 minutes after presentation in every ED and each of these variables is independently associated with massive transfusion or death after trauma; any one of them should prompt activation of the massive transfusion protocol (discussed later).First, an initial international normalized ratio (INR) of 1.5 or more reliably predicts those military casualties who will require massive transfusion [48,49,50] Patients who have a significant injury present with a coagulopathy as a marker of severe injury. Severity of injury and mortality is linearly associated with the degree of the initial coagulopathy [35,47,48,49,50]. Second, a base deficit of 6 or more is strongly associated with the need for massive transfusion and mortality in both civilian and military trauma. Patients have an elevated base deficit before their blood pressure drops to classic “hypotension” levels [51,52,53]. Third, a temperature of 96°F or less is associated with an increase in mortality. Trauma patients who are hypothermic are in shock, not perfusing their mitochondria, and are not generating heat fast enough to keep up with their ongoing heat loss [52,53,54]Fourth, a hemoglobin of 11 mg per dL or less on presentation to the ED is associated with massive transfusion and a mortality rate of 39% [43]. Otherwise, young healthy soldiers who present with a low hemoglobin have only one reason for their anemia, namely, acute blood loss [43,55]. Lastly, a systolic blood pressure of 90 mm Hg or less is indicative casualties who have lost more than 40% of their blood volume (2,000 mL in an adult), are experiencing impending cardiovascular collapse, and have a significantly increased mortality [56,57].The current resuscitation protocol for combat casualties not only has an affect on current military outcomes (initial reports show Case Fatality Rates dropping from a historic 20% to close to 10%), but has provided exciting tools for civilian trauma providers [40,58].P.1661
Table 158.1 U.S. Central Command Clinical Practice Guideline for Use of Recombinant Factor VIIA (RFVIIA) and Thawed Plasma
1. Background: The most critically injured casualties present hypothermic (T ≤ 96°F) acidemic (BD ≤ 6), with a coagulopathy (INR ≥ 1.5), hypotensive (SBP ≤ 90 mm Hg) or with a Hgb ≤ 11). Interventions aimed at reversing the coagulopathy starting as soon after arrival as possible may improve survival.
2. Recombinant factor VIIa is FDA-approved for use during critical bleeding or surgery in hemophilic patients with inhibitors to factor VIII or IX. rFVIIa has been shown to be safe and decreases transfusion requirements in humans with life-threatening hemorrhage,

including patients with hypothermia (30°C–33°C, pH > 7.1). In a total of seven prospective randomized surgical trials, the drug causes no increase in any complication.
3. Plasma used in a 1:1 ratio with PRBCs has been shown to improve survival in combat casualties.
4. In the combat surgical setting, rFVIIa and plasma should be used in patients who area. Hypotensive from blood loss (SBP ≤ 90 mm Hg) b. Have a base deficit ≥ 6 c. Hypothermic (T ≤ 96°F) d. Coagulopathic (clinically or an INR ≥ 1.5) e. Have a Hgb ≤ 11 f. Have weak or absent radial pulse character g. Have more than one major amputation h. Have major truncal injury with a positive FAST examination i. Abnormal mental status from trauma or CT scan with intracranial injury j. Have > 1,000 mL immediately out of a chest tube or > 200 mL/h k. Anticipated and actual transfusion of > four units of PRBCs l. Require damage control maneuvers m. Require fresh whole blood
5. Guidelines for administrationa. Protocol for use
i. Infuse rFVIIa at dose of three vials (2.4 mg) or 90–120 μg/kg IV push. ii. If coagulopathic bleeding continues 20 min after infusion
1. Administer two additional units fresh whole blood or four units FFP, 10 packs of cryoprecipitate and 6 packs of platelets
2. Redose rFVIa 90–120 μg/kg rFVIIa IV push. b. Administration limits
i. Four doses (typically 12 vials) within a 6-h period. ii. If bleeding persists after four doses, there should be attention to conservation
of resources. Consult the senior surgeon before administering more rFVIIa.
BD, base deficit; CT, computed tomography; FAST, focused abdominal sonogram for trauma; FDA, Food and Drug Administration; Hgb, hemoglobin; INR, international normalized ratio; PRBC, packed red blood cell; SBP, systolic blood pressure; T, temperature.Emphasis on early hemorrhage control and damage control resuscitation through aggressive replacement of blood component and coagulation factors still needs further study, but remains one of the positive hallmarks of modern combat medicine. From the point of injury on the battlefield to the arrival at definitive care facilities the current combat casualty enters into a well thought out system of multiphasic resuscitation with specific goals to be achieved at each level; early hemorrhage control, limited intravascular replacement until definitive control is available, and the early use of blood and coagulation factors in a damage control resuscitative strategy.Civilian ExperienceDamage control resuscitation defines a new philosophy of acute traumatic resuscitation. Its tenants define a number of important maneuvers during the resuscitation. First is permissive relative hypotension, with a goal systolic blood pressure slightly below normal. Next is prevention and treatment of hypothermia, acidosis, and hypocalcemia, while avoiding hemodilution with crystalloid fluids. Early surgical control of bleeding is also tantamount to damage control resuscitation. Lastly, hemostatic resuscitation with blood products in high ratios of fresh frozen plasma (FFP) and platelets to packed red blood cells, with appropriate use of adjuvants like factor VIIa, and fibrinogen containing compounds, is considered fundamental to this approach to the hemorrhaging patient [59].There has been ongoing controversy in the surgical literature concerning the optimal use of resuscitative fluids. Questions of type, amount, and timing dominate the ongoing discussion. In
addition, some authors maintain that the differences between civilian and military mechanisms of injury limit the applicability of military data to the civilian practice patterns. There is some belief that combat-related injuries result in a distinct patient population, and that lessons learned there may not be translatable to the civilian population [60,61]. However, multiple civilian studies in Europe and in the United States demonstrate similar results to wartime casualties and the benefits to aggressively resuscitating these patients with plasma and platelets versus excessive crystalloid. The evidence in these studies is all retrospective, and is subject to survivor bias and multiple other confounding variables. Unfortunately, no prospective randomized trials have been conducted examining any resuscitation strategy, including damage control resuscitation.P.1662
The early coagulopathy of trauma, identified by as early as 1969 by Simmons and Borowiecki, and highlighted separately by Brohi and MacLeod is a common and dangerous condition that many patients manifest upon admission to the emergency department [50]. Brohi defines coagulopathy as prothrombin time (PT) over 18 seconds, activated partial thromboplastin time (aPTT) over 60 seconds, or thrombin time over 15 seconds. This London study found a significant coagulopathy in 24.4% of patients admitted to their ED. This coagulopathic cohort had a much greater mortality (46% vs. 10.9%, p < 0.001) compared with those with normal coagulation studies. Contradicting previous suspicions about the contribution of fluids to coagulopathy, Brohi found that the early coagulopathy of trauma was not linked to amount of IV fluids (crystalloid and colloid) administered [49].Adding to this observation, Gonzalez et al. demonstrated that patients that arrived to the emergency department in a coagulopathic state (INR = 1.8 ± 0.2) and received primarily PRBCs and crystalloid fluids were persistently coagulopathic on admission to the ICU (INR = 1.6 ± 0.1). Ninety-one patients were identified who received > 10 units of PRBCs in the first 24 hours of admission. According to the massive transfusion protocol at that time, FFP was not transfused until the patients received six units of PRBCs. Once admitted to the ICU, patients received a ratio of FFP/PRBC 1:1. Using univariate logistic regression analysis, the authors concluded that risk of mortality was increased with higher initial ICU INR. This study highlighted the potential importance of earlier administration of FFP and its possible benefits in the form of improved patient survival [34].Recent civilian studies have demonstrated benefits in survival with high FFP to PRBC ratios, as well as platelets to PRBCs. A study by Holcomb et al. included 466 massively transfused (≥ 10 units PRBCs in 24 hours). This retrospective multicenter study demonstrated that patients who received a high ratio of FFP to PRBCs (≥ 1:2) had increased survival (59.6%) compared with those who received a low ratio (< 1:2) of FFP to PRBCs (40.4%, p = < 0.01). This effect was also seen in patients who received a high ratio (≥ 1:2) of platelets to PRBCs. Those patients had 59.9% survival compared with those in the low (< 1:2) platelet to PRBCs group, who demonstrated only 40.1% survival at 30 days (p = < 0.01) [37]. Another paper with the same cohort of patients highlighted the importance of early (within 6 hours) administration of high FFP ratios. This study showed that a transfusion ratio of ≥ 1:1 FFP/PRBCs in the first 6 hours of admission decreased mortality at 6 hours (2% vs. 15.2% and 37.3% for ratios ≥ 1:1, 1:4 to 1:1, and < 1:4, p = < 0.001) and in hospital mortality (25% vs. 41.1% and 54.9% for the same groups, p = < 0.04). Patients receiving high platelet/PRBC ratios also had improved survival [62].Another large single-center retrospective study examined 383 patients that received greater than 10 units of PRBCs in the first 24 hours of admission. This group, from Los Angeles, demonstrated survival benefit with higher ratios of FFP to PRBCs. Patients that received ≤ 1:3 FFP to RBC had 25% mortality, whereas those that received > 1:3 had 49% mortality. Further analysis demonstrated that the mean FFP/PRBC ratio for survivors was 1:2.1. Nonsurvivors received 1:3.7 FFP/PRBC (p < 0.001). They concluded that higher FFP/PRBC ratios improve survival, but unlike the Holcomb study, no benefit was shown when ratios were more aggressive than 1:3 [63].Two recent studies from New Orleans also examine FFP/PRBC ratios and survival. Both are retrospective single center-studies. The first study reports that 135 patients, suffering 72%
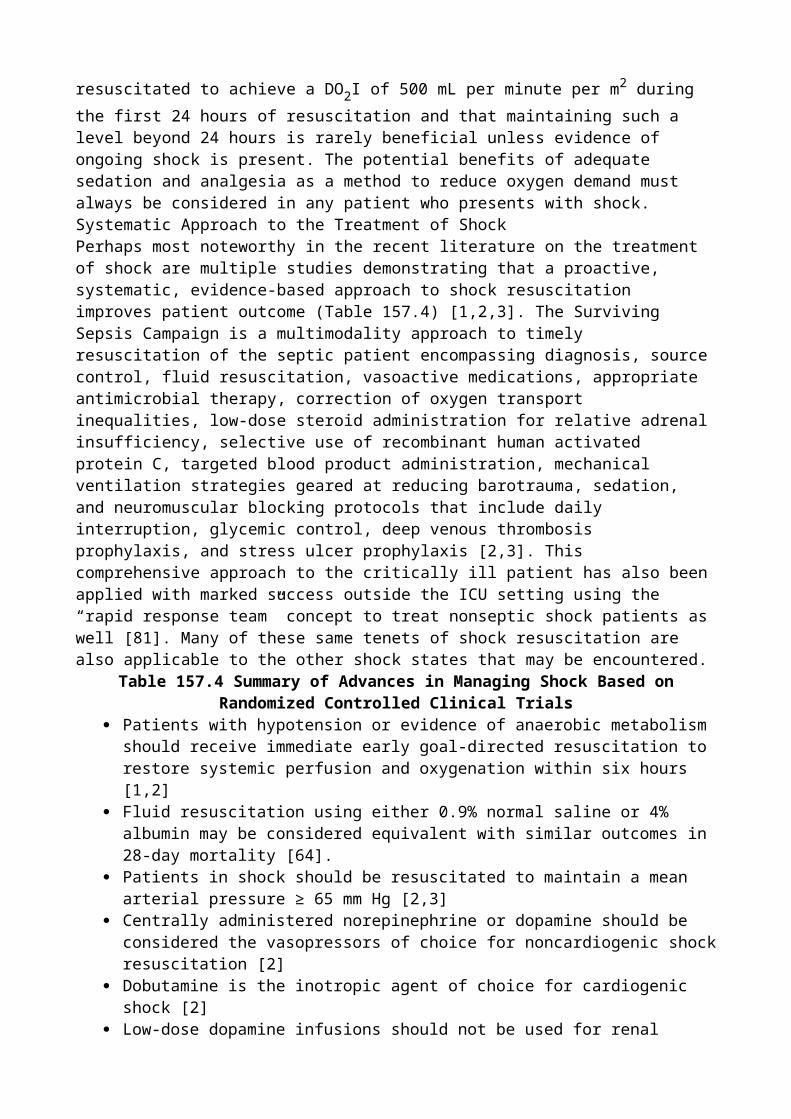
penetrating injuries, received > 10 units of PRBCs during the first 24 hours of treatment. All of these patients received surgical intervention. In this population they report a dramatic improvement in survival for patients that received > 1:2 FFP to PRBC compared with those who received 1:4, 26% versus 87.5% (p = 0.0001) [37]. The second study also examines patients who underwent emergency surgery for trauma and received > 10 units of PRBCs. The population of 135 patients were coagulopathic, as defined by INR > 1.2, PT > 16 seconds, and partial thromboplastin time > 50 seconds. A statistically significant improvement in survival was demonstrated in patients receiving 1:1 ratio of FFP to PRBCs compared with those who received 1:4, 28% compared with 51% (p = 0.03). This study also demonstrated an improvement in ICU days (10 vs. 23, p = < 0.01) in the 1:1 group versus 1:4 [64].Other studies have demonstrated improved survival with aggressive use of FFP associated with massive transfusion protocols. One study, from Nashville, is a retrospective study with a historical control before implementation of a massive transfusion protocol that specified a ratio of 2:3 FFP to PRBC and 1:5 platelets to PRBCs. The study included 264 total patients, with 125 in the protocol group and 141 in the historical group. The authors demonstrated an improvement in survival from 37.6% to 56.8% (p = 0.001) after implementation of the protocol. The transfusion protocol cohort also protected against MOF in univariate and logistic regression analysis. The authors attribute the protection from multiorgan failure to the overall decrease in number of blood product units that patients received as a result of enrollment into the transfusion protocol [65].Two recent European studies also demonstrate benefits to early plasma transfusion both in trauma patients and in other surgical patients. Maegele et al. demonstrate survival benefit for trauma patients at < 6 hours, 24 hours, and 30 days in groups that received high (1:1 and < 0.9) ratios of FFP/PRBC. This study included a multicenter retrospective review of 713 patients who received > 10 units PRBCs in 24 hours. Patients who received > 1:1 FFP to PRBCs had 6-hour mortality equal to 24.6%, 24-hour mortality at 32.6%, and 30-day morality at 45.5%. The mortality rates for 1:1 ratio were 9.6%, 16.7%, and 35.1% at the same time points (p < 0.005 for all values). However, these increases in survival came with the cost of increase septic-related complications. The incidence of multiorgan failure in the 1:1 FFP/PRBC group was the greatest at 67% [66].A group of investigators in Denmark have assessed the principles of damage control resuscitation outside of trauma. A review of 832 surgical patients, including abdominal surgery, cardiovascular, orthopedic surgery, and trauma patients, demonstrated improved survival for patients receiving a ratio of FFP/PRBC equal to 1:1.3 compared with those who received 1:1.6. Mortality at 30 days was 20.4% for the high ratio group compared with 31.5% (p = 0.0002). Higher FFP/PRBC ratios did increase ICU days and hospital stay [67]. This study suggests that aggressive use of plasma may be indicated in all bleeding patients, regardless of traumatic etiology.One recent multicenter study from the Glue grant project demonstrates a lower risk of mortality with a high FFP/PRBC ratio, but also highlights risks associated with transfusion. This study, by Sperry et al., included 415 patients and did not show a crude improvement in mortality, but did reveal a significant difference in 24-hour mortality (high FFP/PRBC 3.9% vs. low FFP/PRBC 12.8%, p = 0.012). Their high ratio group received ≥ 1:1.5 FFP to PRBCs. On Cox regression analysis, the group demonstrated a 52% reduced risk in mortality if patients received the higher FFP/PRBC ratio (p = 0.002). Although there was no increase in multiorgan failure or infection, the high FFP/PRBC group did have an increased (2×) risk of acute respiratory distress syndrome (p = 0.004) [68].Watson et al. demonstrate an association between plasma and MOF in an examination of 1,175 patients in a prospective multicenter study. Using Cox proportional hazard regression, the researchers found a 2.1% increased risk of MOF with every unit of FFP transfused. The risk of ARDS increased 2.5% with P.1663
each unit of FFP. However, the group also reported that each unit of FFP decreased the risk of mortality by 2.9% [69].
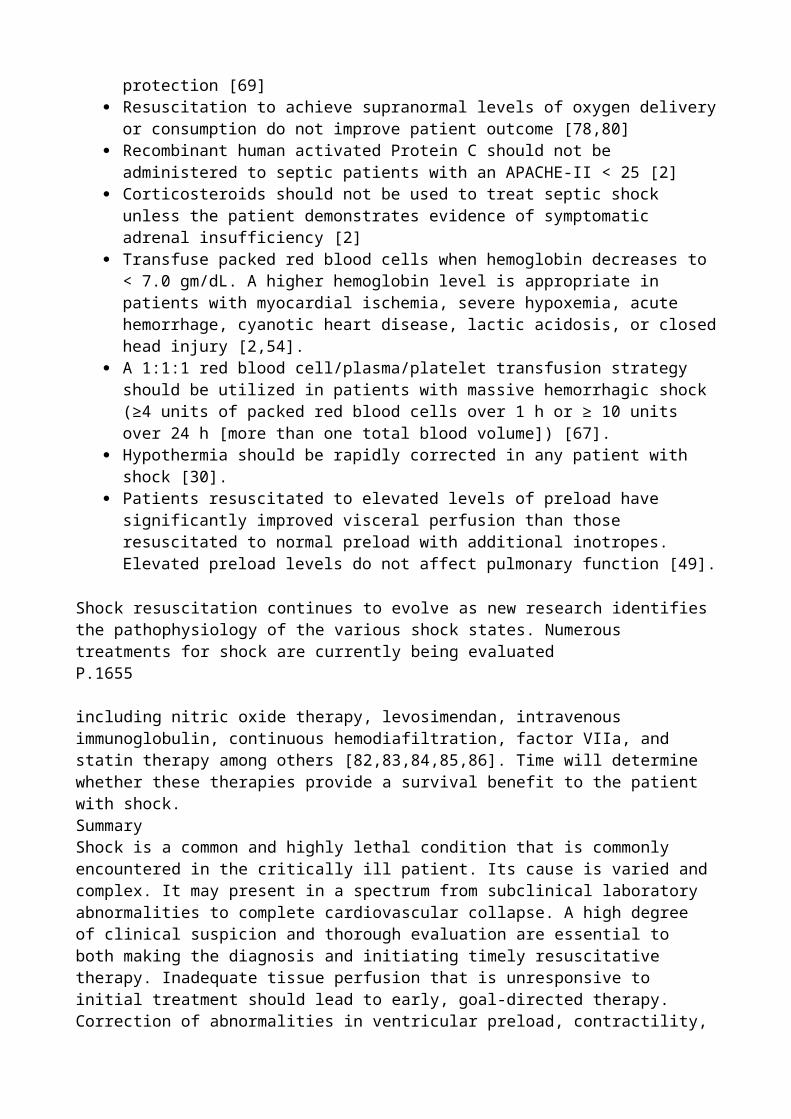
Other civilian studies that do not find a survival benefit to high FFP/PRBC ratios. Kashuk et al., report a single-center retrospective study that examined 133 patients who received > 10 units of PRBCs in the first 6 hours. This study presented data that patients receiving FFP/PRBC ratios of 1:2 to 1:3 had the lowest predicted probability of mortality. However, the study did note improvement in coagulopathy with higher ratios of FFP/PRBC. However, because of small study size, this was not statistically significant. Also, of important note, the number of patients receiving FFP/PRBC at a 1:1 ratio was only 11 [61]. Another paper, from Baltimore, also fails to demonstrate a survival benefit from high (1:1) FFP/PRBC ratios. However, their massive transfusion subgroup was underpowered, at 81 patients, to demonstrate a survival benefit [60]. A previous study from the same group also highlighted the increased risk of infection and mortality associated with transfusion of PRBCs and FFP [70].In summary, much like the recent military experience, the preponderance of civilian experience suggest that early and increased use of FFP and platelets in trauma resuscitation results in an overall reduction in early and late mortality. By decreasing early hemorrhagic death, there may be an association with increased risk of infection, ARDS, and multiorgan failure, but patients will survive to suffer these events.Resuscitative FluidsIn hemorrhagic shock, the choice of intravenous fluid has been long debated and is beyond the scope of this chapter. Historically, a crystalloid solution such as normal saline or lactated Ringer's solution was used in the initial resuscitation. Recent evidence suggests that a more aggressive use of blood and blood products, a so-called damage control resuscitation encompassing “hemostatic resuscitation” may be more beneficial (see Damage Control Resuscitation section). Traditional regimens call for using crystalloids while awaiting blood products from the blood bank, with a rate of infusion of 500 mL to 1,000 mL bolus during 15 to 20 minutes and repeated as necessary. Certainly by the time 2 L of crystalloid have been used for resuscitation, blood product replacement should be given at similar rates of infusion. All fluids should be infused via a warming device to alleviate or prevent hypothermia. Unfortunately, this approach may worsen the coagulopathy present in the most severely injured trauma patients.Our current recommendations are to minimize the amount of crystalloid a patient receives. Physicians in the ED have little control over what fluids a patient may receive before arrival to the hospital. Blood is the fluid of choice to resuscitate the surgical patient from hemorrhage. Although hemorrhage as the cause of shock had been debated for many years, the treatment of hemorrhage by returning blood to the body seemed logical. The first successful animal transfusion was by Richard Lower in 1665. In 1667, he transfused the blood of a lamb into a human to treat melancholy [71]. Because of transfusion reactions, blood transfusions were infrequently used before the 1900s. During this period, however, the use of autotransfusion emerged. The first American use of autotransfusion was in 1916 after a splenectomy. World War I saw the widespread use of blood banks. Brown, in 1931, was the first to autotransfuse the blood obtained from a hemothorax [72]. World War II demonstrated that truly massive use of blood across multiple theaters of war was possible. With the advent of cardiac surgery in the 1950s, autotransfusion became more common [73]. Its usefulness for the trauma victim was firmly established in the late 1960s and the early 1970s [74,75,76,77,78]. Complications from autotransfusion such as thrombocytopenia, disseminated intravascular coagulopathy (DIC), hypofibrinogenemia, infection, and air embolism have been well documented [78]. Improvement of delivery systems with filters and air monitors, as well as a limit to the amount of blood autotransfused, has kept these problems to a minimum. Because autotransfusion has restrictions on its use, autotransfusion alone will never be adequate for resuscitation, but the value of its use should not be overlooked.Whole blood contains all of the factors lost by the bleeding patient; this includes plasma proteins, clotting factors, platelets, and white blood cells, as well as erythrocytes. Although FWB is a superb resuscitation fluid, it has a short storage life [36]. Infectious disease testing and blood banking inventory management issues have made FWB largely unavailable in civilian trauma centers. However, whole blood is used in many centers and clinical studies on whole blood are planned for
civilian trauma patients. Prospective data collected in these studies may present an impetus for change in blood banking and provide access to this resuscitative fluid.Usually, oxygen-carrying capacity is gained by giving RBCs. These should be typed and cross-matched to the patient to avoid transfusion reactions. In severe hemorrhage, time may not be available for cross-matching, so type-specific or even O-negative blood should be administered. PRBCs can be stored for 42 days according to current FDA standards. However, detrimental effects of stored PRBCs can be related to their age. Hyperkalemia is a well-known problem with red cell storage. Potassium is lost into the PRBC supernatant at a rate of 1 mEq a day [79]. Cardiac events have been attributed to PRBCs stored for less than a week [80]. Also multiple studies have documented increased infection risk, multiorgan failure and decreased survival associated with older RBCs [81,82,83,84,85]. Despite safeguards, clerical errors lead to mismatched blood administrations, with a rate of fatal major ABO blood group reactions of between 1 in 500,000 and 1 in 2 million. Currently, the risk of infection from a transfused unit is 1 in 30,000 to 1 in 150,000 for hepatitis C, and 1 in 200,000 to 1 in 2,000,000 for human immunodeficiency virus [86].Thawed plasma is FFP that is stored for up to 5 days at 1°C to 6°C. This storage timeline is based on similar red blood cell storage guidelines and preservation of factors V and VIII, however clinical data is lacking [59,87]. It is unknown what the biologic effect is of storing thousands of proteins at 4°C for 5 days and then administrating them to patients who are in shock. As more centers are using earlier and increased amounts of plasma, thawed plasma is now routinely available at many trauma centers, and increasingly stored in emergency departments. Type AB plasma, the universal donor for plasma, is chosen initially before cross-matched product is available. Having thawed plasma available in the ED allows for identification of severely injured patients requiring massive transfusion and initiation of a protocol driven high ratio of FFP to PRBCs. Primary risks associated with plasma are transfusion-related lung injury (TRALI), infection, and multiorgan failure [69,70]. As described earlier, the risk of infection and MOF was increased 2.1% with each unit of plasma [69]. However, these observations have been made in the context of higher survival in patients that received high ratios of FFP, suggesting that those patients survived with the potential cost of developing sepsis and multiorgan failure.Platelets are transfused in two different formulations. Pooled whole blood-derived platelets are generally transfused in six unit increments from five to six different blood donors. Apheresis platelet units are derived from a single donor and are transfused in volumes approximately equal to five to six units of pooled whole blood-derived platelets. Both types of platelets are stored at room temperature for up to 5 days. Bacterial contamination from skin flora remains the greatest risk of platelet transfusion. However, apheresis platelet units have been shown P.1664
to have lower risk of infection in the United States. This risk is derived from a decreased number of venipunctures of donors. European studies have failed to demonstrate a similar benefit [88].Cryoprecipitate is a product of FFP that contains factor VIII, von Willebrand factor, fibrinogen, fibronectin, factor XIII, and platelet microparticles. Cryoprecipitate is made after centrifuging thawed plasma and removing the supernatant. It has a shelf life of one year when frozen at - 20°C [89]. The American Association of Blood Banks mandates a minimum of 150 mg of fibrinogen per unit. Cryoprecipitate is customarily transfused in 10 unit bags, although this is highly variable. As a result of this practice, patients generally receive 2.5 g of cryoprecipitate per transfusion. Its indications for use and benefits derived from it are controversial. Two studies from the military demonstrate improved survival in patients who received relatively high doses of cryoprecipitate [90,91]. Fibrinogen concentrate, a product licensed for use in many European countries, has also been investigated. Fries et al., in Austria, have demonstrated that blood loss is decreased after administration of fibrinogen in coagulopathic swine with a liver injury [92]. Ex vivo experiments also demonstrated improved clot characteristics after administration of fibrinogen concentrate [93,94]. However, the data for this product are limited and this is a potential area of clinical investigation.
HTS is any sodium chloride solution that is more concentrated than normal saline. Solutions of 3.0%, 5%, and 7.5% are commercially available. However, 7.5% HS is not approved for use in the United States. High concentrations of sodium chloride in the vascular system favor the flux of water from the interstitial space and from the cells to augment the blood volume. This results in a rapid restoration of intravascular volume. Infusions of small amounts of these solutions lead to hemodynamic responses equivalent to much larger volumes of crystalloid solutions. This is advantageous because of the rapidity of the response. In some military and wilderness environments, the smaller and much lighter volume of fluid is a significant advantage logistically. Recent work suggests that these fluids decrease the activation of neutrophils, so they may offer an advantage in preventing multiple organ dysfunction syndrome [95]. The proponents of these fluids believe that the smaller volumes lead to less tissue edema and associated potential complications. Once fluid is drawn into the vascular space, the sodium chloride is diluted, so it then equilibrates across the fluid spaces of the body. As this happens, the effect of the HTS is gradually lost. Increases in mean arterial pressure are short-lived, with hemodynamic effects lasting only 15 to 75 minutes [96]. The largest potential danger with hypertonic solutions is hypernatremia. This may be accentuated in the previously dehydrated patient without additional extravascular fluid to donate to the vascular system. Although some rapid and transient hypernatremia seems to be tolerated, caution in administration and careful monitoring of sodium levels are important in the safe use of these solutions [97].Vasopressor agents can be useful for achieving a minimal acceptable blood pressure, but typically only after adequate resuscitation. Phenylephrine, dopamine, norepinephrine, and vasopressin are the preferred agents, starting in the lower dose range. If blood pressure and intravascular volume status are acceptable but there is evidence of ongoing hypoperfusion (elevated lactate or base deficit), an inotropic agent such as dobutamine or dopamine can be used. Recent work suggests that adrenal insufficiency is much more common than previously thought, especially in conjunction with etomidate use, and responds well to 2 to 3 days of steroids and vasopressin [98].In general, the intensivist should approach cardiovascular support in the surgical and trauma patient using the four parameters of hemodynamic performance: (a) preload (best index: pulmonary artery occlusion pressure, “wedge”), (b) afterload (best index: calculated systemic vascular resistance = (mean arterial pressure - central venous pressure [CVP])/cardiac output × 80), (c) cardiac contractility (best index: stroke volume = cardiac output/heart rate), and (d) heart rate. All but heart rate traditionally require invasive monitoring with a pulmonary artery catheter for accurate measurement.For intravascular volume depletion, hypovolemia, and cardiovascular instability due to sepsis, this manipulation of variables should proceed in the order listed, assuring adequate preload (wedge of 15 to 18 mm Hg) by volume repletion before adjusting other variables (such as adding inotropes for diminished cardiac output). There is, however, a certain cohort of surgical patients who are “nonresponders” to ongoing volume resuscitation. These patients do not vasodilate with initial volume loading. Additional volume loading in the setting of persistent high systemic vascular resistance sets the stage for a problematic tissue edema entity called secondary abdominal compartment syndrome (ACS) wherein intra-abdominal pressure reaches deleterious levels due to “third-spacing” of resuscitation fluid in the abdomen. This occurs in patients without intra-abdominal injuries who require massive resuscitation for injuries in which hemorrhage control is difficult or delayed (e.g., pelvic fractures, mangled extremities). These are the patients who receive 10 to 20 L of crystalloid. In contrast, primary ACS occurs in patients with abdominal injury and the ACS is directly attributed to hemorrhage and tissue response within the abdomen to the primary trauma. Formation of secondary ACS in this group of nonresponders led Balogh and colleagues [99] to decrease DO2 goal from 600 or more to 500 mL per minute per m2. The cardiac index and SvO2
response to this ICU resuscitation protocol and clearance of metabolic acidosis were similar to historic matched controls. The DO2 600 or more cohort received significantly more crystalloid, had
greater incidence of intra-abdominal pressure more than 20 mm Hg (42%* vs. 20%; *p < 0.05), ACS (16%* vs. 8%), MOF (22%* vs. 9%), and death (27%* vs. 11%). The use of plasma has also

been linked to avoiding ACS. Cotton et al. demonstrate a significant decrease (from 9.9% to 0%, p < 0.001) in the incidence of ACS after implementation of a massive transfusion protocol [65].Management of CoagulopathyIdeally decisions regarding management of coagulopathy in trauma, the operating room, or the ICU ideally should be based on laboratory data. Unfortunately, this ideal situation is rarely achieved. Although point-of-care coagulation testing is commercially available via devices designed for home use monitoring of INR, most EDs and ICUs do not have this capability, and they have not been validated in critically injured patients. Patients who have received large amounts of crystalloids, colloids, and/or packed RBCs or other blood components should have a coagulation panel performed that includes PT, activated partial thromboplastin time, INR, and platelet count. When suspicion of consumption and/or dilutional coagulopathy exists, a more complete coagulopathy panel should be performed to include fibrinogen, D-dimer, and fibrin split products. The bleeding patient with thrombocytopenia, hypofibrinogenemia, elevated fibrin split products, and D-dimer should be considered to have a dilutional coagulopathy. We have recently added thromboelastography (TEG) to our coagulation panel.A recent study by Hess et al. describes the relationship of abnormal coagulation studies and mortality. This paper highlights the connection between injury severity score and coagulopathy, with a linear correlation between the two values. The authors find that an abnormal INR increases the risk of death P.1665
from 4.2% to 26.4%. Abnormal aPTT increases the risk from 4.0% to 43.2%. These laboratory values are therefore cheap and reliable indicators of mortality risk, and suggest that early and aggressive treatment of coagulopathy may impact survival [100].TEG, a simple test developed in 1948 and used primarily in cardiac and transplant surgery, provides a rapid and comprehensive analysis of coagulation status and can likely be used in place of a DIC panel [101,102,103,104]. Use of the thrombelastography test is occurring more frequently in trauma patients. In swine TEG has been shown to be a more sensitive test than PT and aPTT, and may be a better test than traditional laboratory tests [105]. TEG has been shown to be better in certain circumstances as it allows testing of blood in its in vivo state temperature rather than warming it up in the laboratory. Watts et al. [106] showed enzyme slowing and decreased platelet function each individually contribute to hypothermic coagulopathy in trauma patients, particularly at body temperatures < 34°C, whereas such changes were not evident on standard coagulation testing. TEG will likely become more widely used as clinicians become more aware of its usefulness and limitations.Because prolonged hypotension is a known predisposing factor for the development of coagulopathy after trauma, aggressive resuscitation is the most critical factor in prevention of coagulopathy in the injured patient [107]. Platelets and coagulation factors are consumed with ongoing bleeding. In addition, intravascular volume replacement with crystalloid, colloid, or packed RBCs results in dilution of coagulation factors and platelets, with dilutional thrombocytopenia being the most frequent coagulopathy in trauma patients [108,109]. DCR concepts describe replacing lost intravascular volume with plasma and platelet proteins and minimizing ongoing dilution with excessive crystalloids. Various formulas exist regarding whether to begin with platelets, cryoprecipitate, or FFP when correcting dilutional coagulopathies and regarding when to begin this replacement (e.g., after n units of packed RBCs).Recent studies have investigated the role of activated protein C in traumatic coagulopathy. Brohi et al. describe indirect evidence for consumption of activated protein C as a result of hypoperfusion [110]. Another study by Brohi correlates D-dimer levels, as a corollary of fibrinolysis, with degree of shock and hypoperfusion. This relationship between shock and the anticoagulant and fibrinolytic pathways suggests the need to decrease the severity and duration of shock as a method to manage coagulopathy [111].
If laboratory data are available, they can be used to guide therapy. However in most rapidly bleeding patient's laboratory data returns far too slowly to make intelligent decisions for optimal care. It is this reason that ratio driven transfusion is likely optimal while the patient is bleeding. Once bleeding is controlled, transfusion therapy can convert to laboratory driven parameters. Platelet counts can be obtained to assess need for platelet transfusion (see later discussion), PT/activated partial thromboplastin time to assess need for FFP (if PT or activated partial thromboplastin time are greater than 1.5 times normal), and fibrinogen levels to assess need for FFP (below normal fibrinogen level) and/or cryoprecipitate (fibrinogen levels less than 100 mg per dL). A panel of the aforementioned tests plus fibrin split products and D-dimer demonstrate whether dilutional coagulopathy or fibrinolysis is present. [112]. Conversely, if TEG is available (especially rapid TEG), it likely can be used to drive optimal use of blood products, although these guidelines have not been prospectively validated [113].Acute hemolytic transfusion reactions, although rare, remain a cause of coagulopathy (from compatibility mismatch). The physician must consider this as a possible inciting cause for DIC, especially when no other cause is apparent. The physician must also be familiar with other less common coagulopathies in the trauma patient (and treatment) such as primary fibrinolysis (epsilon–aminocaproic acid), uremia (desmopressin/1-deamino-8-D-arginine vasopressin), and primary liver disease (FFP and vitamin K). With wider spread of the use of TEG early in trauma resuscitation, the incidence of fibrinolysis is likely to increase.Platelet counts of less than 20,000 per μL should always be corrected in any bleeding trauma patient being resuscitated, whether or not a life-threatening injury has been identified. If the patient has a known history of aspirin use within the preceding 7 days, ibuprofen or other nonsteroidal anti-inflammatory drug use within the last 2 to 3 days, or an unknown history, it may be necessary to transfuse platelets despite a platelet count greater than 50,000 per μL, particularly in those patients with head injury or those being managed nonoperatively for significant liver or other solid organ injury. Platelet counts of less than 100,000 per μL are a relative indication for platelet transfusion in the head-injured patient with evidence of intracranial hemorrhage, whether as a single-system injury or as part of multisystem injuries. Each unit of platelets transfused can be expected to raise the platelet count by at least 5,000. It is possible that we have been overly restrictive in the use of platelet transfusions, as recent data suggests that increased and early use improves survival, and that keeping platelet counts > 100,000 are associated with improved outcomes [66,89].Recombinant factor VIIa (rFVIIa) has emerged as an adjuvant to plasma and platelets in the military and has also been extensively studied in civilian trauma centers. However, there exists controversy on timing, appropriate doses, and indications for the use of recombinant factor VIIa [114]. One Level I study on rFVIIa has been published. The primary endpoint for this randomized double-blind clinical trial was blood product use. In blunt trauma patients, a decreased need for RBC transfusion was seen in patients who received rFVIIa (14% vs. 33% required > 20 units of PRBCs, p = 0.02). In penetrating trauma, a similar trend was demonstrated, but it did not decrease statistical significance. There were no differences in thrombotic complications between groups and mortality differences were not seen [115]. One military study did demonstrate a survival benefit in patients who received rFVIIa compared to those that did not (14% vs. 35%, p = 0.01). Other retrospective studies have demonstrated decreased transfusion requirements with rFVIIa use and no increase in thromboembolic events when matched to controls [116]. Timing of administration has also been studied. The dose of rFVIIa seems to be most effective when given early in a massive transfusion protocol [117]. The use of rFVIIa remains controversial and may be considered as an adjuvant to massive transfusion, based on individual physician preference, although no improvement in survival has been seen.The early use of plasma and platelets has been demonstrated to improve coagulopathy, although it is unclear why this happens. It seems simplistic to think a minimally improved INR could account for changes in survival or be based on replacing a small percentage of lost coagulation factors. Dente et al. demonstrated an improvement in PT and INR (15.1 ± 0.26 and 1.31 ± 0.29 compared with 17.5 ± 1.1 and 1.72 ± 0.17, p = 0.04) with their massive transfusion protocol compared with a historical

control group. These benefits were demonstrated on admission to the ICU [118]. Subjectively, using the concepts of DCR has decreased the incidence of coagulopathic bleeding, allowing easier control of surgical bleeding [119]. By identifying patients with coagulopathy secondary to injury, early implementation of an evidenced-based massive transfusion protocol should decrease coagulopathy and improve the possibility of survival. Our recommendation marries the use of a massive transfusion protocol to the tenants of damage control resuscitation. This approach to the severely injured trauma patient will improve survival, but also may present more risk to infection and multi-organ failure. Patients will, however, suffer those complications with the benefit of survival. Critics P.1666
of this approach have wisely and appropriately noted the pitfalls of retrospective studies and the potential for survivorship bias. To address these concerns, prospective observational trials are ongoing and randomized control trials are being planned.Practicing Damage Control ResuscitationDamage control resuscitation consists of two components: Hypotensive resuscitation and hemostatic resuscitation [120,121]. Hypotensive resuscitation is a military concept that dates from World Wars I and II, and was resurrected in the early 1990s in Houston. The key is to maximize the resuscitation benefit to the mitochondria while at the same time minimizing rebleeding by not “popping the clot,” a strategy that is supported by a significant body of scientific data. This not only preserves the resuscitation fluid within the vascular system but is also logistically sound by preventing needless waste of blood and fluids [20,46,122,123,124,125,126,127].Hemostatic resuscitation is a concept centered on the surgical judgment inherent in damage control surgery, namely, “staying out of trouble rather than getting out of trouble” [120,121,128]. By focusing on restoring normal physiology, rather than normal anatomy, this surgical approach has decreased mortality in severely injured trauma patients and has become standard surgical teaching. From a resuscitation viewpoint, the damage control philosophy can be extended to resuscitation, focusing on restoring normal coagulation and minimizing crystalloid and even initial packed RBC resuscitation in the severely injured casualty. Both traditional resuscitation products further dilute the already deficient coagulation factors and can increase MOF [129,130,131,132,133,134,135,136,137,138,139]. The aggressive hemostatic resuscitation techniques described herein should be performed in parallel with equally aggressive and definitive control of bleeding.Process of Damage Control ResuscitationThe first element of damage control resuscitation is the rapid diagnosis and surgical control of named vessels and gauze packing (standard damage control surgery) in the operating room. Damage control surgery has improved outcomes in severely injured trauma patients [125,128].Thawed plasma is used as a primary resuscitative fluid, and is started in the ED. This product is shelf-stable for 5 days and thus is available on casualty arrival. This approach not only addresses the metabolic abnormality of shock, but also reverses the coagulopathy present on arrival in the ED. Storing plasma for 5 days does not significantly impair the labile factors (V and VIII), and allows this product to be immediately available for transfusion [140]. The Office of the U.S. Army Surgeon General Blood Bank consultant has recommended use of thawed plasma in theaters and the only two Level 1 trauma centers in the Department of Defense have this product available for their trauma patients [47,120,121].The packed RBC to plasma ratio of 1:1, early transfusion of platelets, and cryoprecipitate are indicated [141,142]. Coagulopathy is not only present on presentation to the ED but is exacerbated by the “bloody vicious cycle” of hemorrhage leading to crystalloid resuscitation, then hemodilution and hypothermia, followed by further hemorrhage, and so on [48,49,52]. Furthermore, transfusion of large amounts of preserved RBCs contributes to a dilutional coagulopathy, which is primarily the result of thrombocytopenia and poor platelet function [129,130,131]. In addition, compared to fresh blood cells, stored platelets demonstrate decreased thrombotic function, primarily due to a decrease in expression of high-affinity thrombin receptors during platelet storage [143].
End Points of ResuscitationThe search has been to find this “holy grail” of resuscitation: a better end point of adequate resuscitation than heart rate, blood pressure, or urine output. Cardiac output, venous return, low perfusion, and acidosis were all observed in Cannon's original shock experiments [122,144]. Urine output is often used as a surrogate marker of adequate resuscitation of an end organ, but has several drawbacks as a lone marker of adequacy of resuscitation. Resuscitation to normal levels of oxygen delivery and oxygen consumption were seen as possible goals of resuscitation, but even using these parameters, a significant number of patients proceeded to organ failure and death.Lactate that accumulates with a lack of tissue oxygenation correlates with base deficit in hemorrhagic shock. Correction of an elevated serum lactate or base deficit is viewed as a better, if not the best, end point for resuscitation of hemorrhagic shock [145]. One criticism of using the base deficit is that its recovery lags behind resuscitation, it is complicated by excess chloride, and its continued pursuit of a normal value leads to overresuscitation. Serum lactate elevation has also been criticized as being too broad a test, and it does not portray what goes on at the cellular level.Therefore, other techniques that include subcutaneous or intraluminal oxygen tension probes and gastric or luminal wall pH probes have all been described to show end-organ resuscitation [146,147,148]. Most recently, the use of near-infrared spectroscopy has shown promise in identifying patients in shock, but it remains to be seen if these indices can be used to judge adequacy of resuscitation from shock [149,150]. They all have their benefits, but they are variously invasive and expensive in relation to serum base deficit and lactate. At this time, their impracticality precludes their generalized use [151].ConclusionsThe thoughtful intensivist balances all needs of the patient when using blood products, fluids, and drugs in the resuscitation of patients in shock. Volume replacement is given for lost volume. Oxygen-carrying capacity replaces lost RBCs, and coagulopathy is reversed with hemostatic replenishment. Judicious use of steroids, pressors, and metabolic control are P.1667
the order of the day. The effect of each treatment is carefully monitored for its impact on the patient in a stepwise fashion, all the while monitoring indicators of tissue perfusion. Interventions are crisply applied and then removed on the basis of critically and serially evaluated data.
Table 158.2 Summary of Advances in Managing Resuscitation Based on Randomized Controlled Clinical Trials
A restrictive transfusion strategy is at least as effective and possibly superior to a liberal transfusion strategy in critically ill patients, with the possible exception of acute myocardial infarction and unstable angina patients [5].
Factor VIIa decreased transfusions with trends toward decreased mortality and critical complications [115].
Gastric mucosal pH may be an important marker of resuscitation and may provide an early warning for systemic complications in the postresuscitative period [148].
Etomidate use results in temporary and reversible adrenal insufficiency, responsive to vasopressin and steroids [98].
Research must continue to focus on rapid surgical control of hemorrhage and the use of hemostatic adjuncts. Research should also consider the immunologic and coagulation response of the body when creating a better fluid for initial resuscitation, such as an oxygen-carrying product, and the identification of accurate measurements of adequate resuscitation. The overarching metabolic milieu, including adrenal function, glucose control, and response to vasoactive medications, must also be carefully studied for best practices and best combination therapies, including dose–response effects. Finally, identifying the best marker or, better yet, combination of markers to prove adequacy of resuscitation deserve thorough study. The risks and benefits of given therapies must be thoughtfully balanced, given the needs of the patient in a particular situation.
Advances in managing resuscitation, based on randomized controlled trials or meta-analyses of such trials, are summarized in Table 158.2.
Chapter 159The Management of SepsisPaul E. MarikSepsis is among the most common reasons for admission to medical ICUs throughout the world. Over the last two decades, the incidence of sepsis in the United States has trebled and is now the 10th leading cause of death [1,2]. Advances in medical technologies, the increasing use of immunosuppressive agents, and the aging of the population have contributed to the exponential increase in the incidence of sepsis. In the United States alone, approximately 750,000 cases of sepsis occur each year, at least 225,000 of which are fatal [1,2]. Septic patients are generally hospitalized for extended periods, rarely leaving the ICU before 2 to 3 weeks. Despite the use of antimicrobial agents and advanced life support, the case fatality rate for patients with sepsis has remained between 20% and 30% over the last two decades [1,2]. This chapter provides an overview of this vast topic with particular emphasis on the management of severe sepsis and septic shock.DefinitionsSepsis originally meant “putrefaction,” a decomposition of organic matter by bacteria and fungi. Since then, a wide variety P.1670
of definitions have been applied to sepsis, including sepsis syndrome, severe sepsis, septicemia, and septic shock [3]. In 1991, the American College of Chest Physicians/Society of Critical Care Medicine developed a new set of terms and definitions to define “sepsis” in a more precise manner [4]. The definitions take into account the findings that sepsis may result from a multitude of infectious agents and microbial mediators and may not be associated with actual bloodstream infection. Although the use of these criteria has been criticized and a “newer” diagnostic schema has been suggested (PIRO, which stands for predisposition, insult infection, response, organ
dysfunction), these criteria still provide a useful framework to approach patients with infectious diseases [5]. The term “systemic inflammatory response syndrome” (SIRS) was coined to describe the common systemic response to a wide variety of insults. It is characterized by two or more of the following clinical manifestations: (a) a body temperature of > 38°C or < 36°C; (b) a heart rate greater than 90 beats per minute; (c) tachypnea, as manifested by a respiratory rate of greater than 20 breaths per minute; (d) an alteration of the WBC count of greater than 12,000 cells per mm3, less than 4,000 cells per mm3or the presence of greater than 10% immature neutrophils. When the SIRS is the result of a confirmed infectious process, it is termed “sepsis.” Severe sepsis is defined as sepsis plus either organ dysfunction or evidence of hypoperfusion or hypotension. Septic shock is best defined as systolic pressure less than 90 mm Hg (or a fall in systolic pressure of > 40 mm Hg) or a mean arterial pressure less than 65 mm Hg after a crystalloid fluid challenge of 30 mL per kg body weight (approximately 2,000 mL) in patients with sepsis and in the absence of other causes for hypotension [6]. In a patient previously known to have a low baseline blood pressure, septic shock is defined as a 30% or greater drop in the mean arterial pressure.Three stages in the hierarchy of the host's response to infection was therefore recognized, namely, sepsis, severe sepsis and septic shock, with sepsis having the best prognosis and septic shock the worst. Data from recently published trials support this postulate, with the mortality from sepsis ranging from 10% to 15%, severe sepsis from 17% to 20% and septic shock from 43 to 54% [6]. The distinction between severe sepsis and septic shock is critically important as it stratifies patients into groups with a low and high risk of dying respectively. It also suggests that a more aggressive treatment strategy may be indicated in patients with septic shock (see Fig. 159.1).In patients with shock, the serum lactate has long been recognized to be a marker of disease severity and to be useful for disease stratification [7,8]. Septic patients with a lactate above 4 mmol per L are at an increased risk of death and warrant a more aggressive approach to resuscitation [9,10,11]. In addition the rate of lactate clearance has been demonstrated to be a good prognostic marker [12].Sites of Infection and BacteriologyThe microbiology and primary sources of infection have undergone a remarkable transition over the past 30 years. The predominant pathogens responsible for sepsis in the 1960s and 1970s were Gram-negative bacilli; however, over the last few decades there has been a progressive increase in the incidence of sepsis caused by Gram-positive and opportunistic fungal pathogens [1]. Data from the large sepsis trials published during the last decade indicate that Gram-positive and Gram-negative pathogens are responsible for about 25% of infections each, with a further 15% due to mixed Gram-positive, Gram-negative organisms, with fungal pathogens accounting for between 5% and 10% of cases. This evolution in the spectrum of pathogens has been associated with an increase in the incidence of multiresistant organisms. Although the abdomen was the major source of infection from 1970 to 1990, in the last two decades pulmonary infections have emerged as the most frequent site of infection.Pathogenesis of SepsisThe pathogenesis of sepsis is exceeding complex and involves an interaction between multiple microbial and hosts factors. Indeed, after exposure to both Gram-negative and Gram-positive bacteria, macrophages upregulate the expression of over 1,000 genes (and proteins) and downregulate an excess of 300 genes, the net result depending on the complex interrelated interaction of these factors [13]. With advances in molecular biology many of the mysteries of sepsis are being unraveled; however, we have only just embarked on our journey along the “sepsis superhighway.” The reader is referred to many excellent reviews on this topic [14,15,16,17,18,19]. Essentially as noted by William Osler in 1921 “except on a few occasions the patient appears to die from the body's response to infection rather than from it” [20]. Sepsis can be viewed as an excessively exuberant proinflammatory response with increased production of proinflammatory mediators with activation of leukocytes, mononuclear cells, and the coagulation cascade. The end result is widespread microvascular and cellular injury. The cellular injury results in alteration of cellular and subcellular membranes and receptors, activation of intracellular enzymes, increased apoptosis, mitochondrial dysfunction, and sepsis-related immunosuppression. The excessive
proinflammatory responses together with activation of the coagulation cascade are believed to be fundamental events resulting in a systemic microvascular injury. The systemic microvascular injury is a defining characteristic of sepsis and is believed to play a major pathophysiologic role in the progressive organ dysfunction of sepsis.Organ System Involvement in SepsisThe Hemodynamic Derangements of SepsisSepsis is characterized by a complex combination of cardiovascular derangements, including vasodilation, hypovolemia, myocardial depression, and altered microvascular flow. In volume resuscitated patients with septic shock, systemic vascular resistance is usually low, contractility and biventricular ejection fractions are reduced while ventricular dimensions and heart rate are increased. Despite these changes, volume resuscitated patients typically have a hyperdynamic circulation with a high cardiac output. However, recent data suggest that up to 60% of patients with septic shock may have a hypodynamic circulation with a deceased ejection fraction (< 45%) and global left ventricular (LV) hypokinesia [21]. Furthermore, increasing evidence suggests that patients with sepsis develop structural injury to the contractile apparatus of the heart that may contribute to the myocardial dysfunction in sepsis. This is evident by elevated levels of troponin and B-type natriuretic peptide in patients with sepsis [22,23,24]. Estimates of LV ejection fraction correlate negatively with increased levels of cardiac troponin in patients with septic shock. These data suggest that all patients with sepsis should undergo serial echocardiography to characterize the hemodynamic pattern, as this impacts on the approach to the use of vasopressor and inotropic agents [21]. In addition, cardiac troponin should be measured to assess the degree of myocardial injury.P.1671
Figure 159.1. Suggested approach to the management of patients with severe sepsis and septic shock. CBC, complete blood cell count; CI, cardiac index; CXR, chest x-ray; ER, emergency room; IBW, ideal body weight; ICU, intensive care unit; IV, intravenous; LFTs, liver function tests; LR, lactated Ringer's solution; LV, left ventricle; MAP, mean arterial pressure; NS, normal saline; PPV, pulse pressure variation; PT, prothrombin time; SBP, systolic blood pressure; SI, stroke index; SIRS, systemic inflammatory response syndrome; PTT, partial thromboplastin time; WBC, white blood cell.Coagulation ActivationActivation of the coagulation cascade with the generation of fibrin is a pathologic and physiologic hallmark of sepsis that occurs in both the intravascular and extravascular compartments [25]. Intravascular coagulation is characterized by diffuse microvascular thrombosis that contributes to widespread ischemic organ damage. Activation of coagulation during sepsis is primarily driven by the tissue factor pathway. Fibrin formation in sepsis likely results from both increased fibrin generation and impaired fibrin degradation. Inhibition of fibrinolysis P.1672
is primarily due to increases in plasminogen activator inhibitor-1 (PAI-1). Downregulation of the anticoagulant Protein C pathway also plays an important role in the modulation of coagulation and inflammation in sepsis. Because activation of the coagulation cascade almost all septic patients are thrombocytopenic (or have a falling platelet count), and indeed a normal platelet count makes the diagnosis of sepsis unlikely. An elevated D-dimer, thrombin–antithrombin complexes and a prolonged prothrombin time are found in the majority of patients with severe sepsis while antithrombin, protein C, and protein S levels are significantly decreased. Replacement of coagulation factors with fresh frozen plasma ([FFP] and cryoprecipitate if the fibrinogen is less than 100 mg per dL) is only indicated in patients with clinical evidence of bleeding. Although it had previously been assumed that such therapy “fuels the fire of DIC,” there is no evidence that the infusion of plasma products stimulates the ongoing activation of coagulation [26].
PulmonarySepsis is by far the most common cause of the acute respiratory distress syndrome (ARDS) [27,28,29]. The mortality rate for patients with sepsis complicated by ARDS has been reported to be as high as 60%. The pathophysiology and management of patients with ARDS has been extensively reviewed in the literature.RenalAcute renal failure is a serious complication in patients with sepsis. Despite improvements in the support of these patients, the mortality rate remains consistently above 50%. It is, therefore, essential that all patients with sepsis be aggressively resuscitated in an attempt to prevent this complication. The pathogenetic mechanisms leading to ARF in patients with sepsis are unclear; however, mediator-induced cytotoxicity, alterations in renal perfusion and apoptosis have been suggested [30,31].GastrointestinalThe most important gastrointestinal complications occurring in patients with sepsis include gastric stress ulceration, a diffuse splanchnic mucosal injury with increased intestinal permeability and intrahepatic cholestasis.Nervous and MusculoskeletalSeptic encephalopathy is an acute, reversible, generalized disturbance in cerebral function [32,33]. Septic encephalopathy is essentially a diagnosis by exclusion as many factors such as sedative drugs, encephalitis, liver or renal failure, hypoperfusion, fever, adrenal insufficiency, cerebral vascular accidents, and drug fever either alone or in combination may result in disturbed cerebral function. Electroencephalography is useful in confirming the diagnosis of septic encephalopathy and allows assessment of the severity of the encephalopathy. Treatment is essentially supportive.Critical illness polyneuropathy (CIP), as initially described by Bolton et al. in 1984, is a sensorimotor polyneuropathy that is often a complication of sepsis and multiorgan failure, occurring in 70% of such patients [34,35,36]. Postmortem examination of peripheral nerve specimens from patients with CIP has shown primary degeneration of motor and sensory nerves that supply the limbs and respiratory system. Although this denervation is more widespread and severe in the distal muscle groups, the phrenic nerve, diaphragm, and intercostals muscles are also involved. Classically, CIP is associated with a symmetric predominantly distal paresis, with legs involved worse than arms, along with impaired sensory testing in the feet and hyporeflexia. CIP is difficult to diagnose clinically and is often suspected when critically ill patients are otherwise improving yet continue to have difficulty in weaning from mechanical ventilation.In addition to neuropathy, weakness in critically ill septic patients may stem from disturbances in the structure or function of muscle per se. According to biopsy and neurophysiologic studies, myopathies occur much more frequently during critical illness than was previously recognized. Myopathic changes have been demonstrated by electromyographic examination and biopsy in many septic ICU patients. The changes are often mild and usually accompany CIP. In other patients however, myopathy is the predominant finding. This myopathy has been called critical illness myopathy.Sepsis and Multisystem Organ DysfunctionThe ultimate cause of death in patients with sepsis is multiple organ failure. Typically, patients will first develop a single organ failure and then, if the disease remains unchecked, will progressively develop failure/dysfunction of other organ systems. There is a close relationship between the severity of organ dysfunction on admission to an ICU and the probability of survival. The pathogenesis of organ dysfunction is multifactorial and incompletely understood. Tissue hypoperfusion and hypoxia are dominant factors. Multisystem organ dysfunction has an extraordinarily high mortality and, for many patients, the support of this syndrome does not improve survival but rather prolongs the dying process.Clinical Features and Diagnosis of SepsisSepsis is a systemic process with a variety of clinical manifestations. The initial symptoms of sepsis are nonspecific and include malaise, tachycardia, tachypnea, fever, and sometimes hypothermia.
Although most patients with sepsis have an elevated white cell count, some patients present with a low white cell count, which in general, is a poor prognostic sign. A band count in excess of 10% has been reported to have a high specificity (92%) but low sensitivity for the diagnosis of sepsis (43%) [37]. Other clinical manifestations include altered mental status, hypotension, respiratory alkalosis, metabolic acidosis, hypoxemia with acute lung injury, thrombocytopenia, consumptive coagulopathy, proteinuria, acute tubular necrosis, intrahepatic cholestasis, elevated transaminases, hyperglycemia, and hypoglycemia. Patients may present with clinical features of a localized site of infection, such as cough, tachypnea and sputum production due to pneumonia; flank pain and dysuria with urinary tract infection and abdominal pain with intra-abdominal infection.The manifestations of sepsis can sometimes be quite subtle, particularly in the very young, the elderly, and those patients with chronic debilitating or immunosuppressing conditions. These patients may present with normothermia or hypothermia. The failure to generate a temperature greater than 99.6°F (37.5°C) in the first 24 hours of clinical illness, has been associated with an increased mortality rate. An altered mental state or an otherwise unexplained respiratory alkalosis may be the presenting feature of sepsis.The signs and symptoms of systemic inflammation are not useful in distinguishing infectious from noninfectious causes of SIRS. Furthermore, a bacterial pathogen is not isolated in P.1673
all patients with sepsis. Consequently, a number of biomarkers have been evaluated as more specific indicators of infection, including procalcitonin (PCT) and triggering receptor expressed on myeloid cells (TREM-1). PCT, a propeptide of calcitonin, is normally produced in the C-cells of the thyroid. In healthy individuals, PCT levels are very low (< 0.1 ng per mL). In patients with sepsis, however, PCT levels increase dramatically, sometimes to more than several hundred nanograms per milliliter. The exact site of PCT production during sepsis is uncertain; however, mononuclear leukocytes and the liver seem to be the major sources of PCT. TREM-1 is a monocyte receptor that is upregulated by bacterial and fungal pathogens [38]. The ligand for TREM-1 is unknown. A soluble form of TREM-1 (sTREM-1) is released from activated phagocytes and can be found in body fluids. The use of these biomarkers has not gained widespread acceptance presumable due to the cost of the tests and the uncertain diagnostic accuracy.Blood cultures are considered to provide the clinical gold standard for the diagnosis of bacterial infections. However, blood cultures are only positive in between 20% and 30% of patients with sepsis; moreover, it takes 2 to 3 days before the results become available. Molecular methods based on polymerase chain reaction (PCR) technology have been developed for infection diagnosis and pathogen identification. These methods offer a new approach based on detection and recognition of pathogen DNA in the blood, or indeed other clinical samples, with the potential to obtain results in a much shorter time frame (hours) than is possible with conventional culture. PCR based pathogen detection depends on the ability of the reaction to selectively amplify specific regions of DNA, allowing even minute amounts of pathogen DNA in clinical samples to be detected and analyzed. This technique holds great promise and may revolutionize our approach to the diagnosis of bacterial, fungal, and viral infections.Management of SepsisThe management of patients with severe sepsis and septic shock is complex requiring multiple concurrent interventions with close monitoring and frequent re-evaluations. These patients are best managed in intensive care units by physicians experienced in the management of critically ill septic patients. The reader is referred to the “Surviving Sepsis Campaign guidelines for the management of severe sepsis and septic shock”; these guidelines were developed by a number of international critical care organizations and should serve as the framework for the management of patients with sepsis [10].The current strategy for the management of patients with sepsis is largely based on treating or eliminating the source of infection, timely and appropriate usage of antimicrobial agents, hemodynamic optimization, and other physiologic organ supportive measures (see Table 159.1).
Attempts at downregulating the proinflammatory response with novel agents directed at specific proinflammatory mediators has uniformly met with failure. However, both activated protein C (APC) and glucocorticoids (low dose) are immunomodulators that have been demonstrated to improve the outcome of patients at high risk of death.Table 159.1 Suggested Fluid Resuscitation Algorithm for Hemodynamic Instability of Severe
Sepsis and Septic Shock1 L Normal Saline 15–20 minutes1 L 30 minutesStart Norepinephrine if MAP ≤70 mm Hg1 L 500 cc 5% albumin over 30–40 minutes1 L Ringers 30–40 minutes1 L 500 cc 5% albumin over 30–40 minutesRingers lactate 200 cc/hBolus 500 cc 5% albumin or Ringers LactateIt has become increasingly apparent that in many patients there is a long delay in both the recognition of sepsis and the initiation of appropriate therapy. This has been demonstrated to translate into an increased incidence of progressive organ failure and a higher mortality. Kumar et al. investigated the relationship between the duration of hypotension prior to antimicrobial administration in 2600 patients with sepsis induced hypotension [39]. They reported that the risk of dying increased progressively with time to receipt of the first dose of antibiotic. Furthermore, there was a 5% to 15% decrease in survival with every hour delay over the first 6 hours. In the ENHANCE study, the mortality was 33% if drotrecogin alpha-activated (APC) was given within the first 24 hours of admission as compared to 52% if it was given on day 3 of hospitalization [40].Levy et al. retrospectively analyzed the Sequential Organ Failure Assessment scores during the first 48 hours in 1,036 severely septic patients [41]. From baseline to day 1, the direction of change in cardiovascular, renal, respiratory, hematologic, and hepatic functions independently predicted 28-day mortality. The implications of this study is that if organ dysfunction is not improving during the first day of severe sepsis, the mortality risk is significantly increased, underscoring the importance of early recognition and therapeutic intervention to prevent sequential organ dysfunction [42]. Similarly, Rivers et al. demonstrated that early (within 6 hours) clearance of lactate is associated with improved outcome in severe sepsis and septic shock [12].The concept that early aggressive treatment (within the first 6 hours of admission to hospital) of patients with severe sepsis and sepsis shock reduces sequential organ failure and improves survival has been demonstrated in the “landmark” study by Rivers et al. [43]. In this study, early aggressive therapy that optimized cardiac preload, afterload, and contractility in patients with severe sepsis and septic shock improved survival. The patients in the early-therapy group received, on average, approximately 1,500 mL more in total fluids in the first 6 hours of treatment than did the standard-therapy group and had a significantly higher mean arterial pressure (mean [±SD], 95 ± 19 vs. 81 ± 18 mm Hg; p < 0.001). Mortality was 30.5% in the group receiving early goal-directed treatment, as compared with 46.5% in the control group (p = 0.009). This strategy for managing patients with severe sepsis and septic shock has been called “early goal-directed therapy (EGDT).”While the concept of early, as opposed to delayed, volume resuscitation and the timely initiation of appropriate antibiotics in patients suffering from severe sepsis and septic shock is a scientifically sound concept, the author believes that the major pillars on which EGDT is based (central venous pressure [CVP] > 8 mm Hg, ScvO2 > 70% and blood transfusion) may be flawed (see later) [44]. A
more evidence-based approach is provided in Figure 159.1.Identification and Eradication of the Source of InfectionOne of the most challenging features of the sepsis syndrome is that of identifying and eradicating, as early as possible, the source of infection. The majority of patients presenting with severe sepsis usually have a pulmonary, genitourinary, primary blood stream, intra-abdominal, or intravenous catheter as a source of infection. Recent studies have demonstrated that in approximately 75% of
patients with presumed sepsis, an P.1674
etiological agent can be isolated, these being equally divided amongst Gram-positive and Gram-negative organisms. It has been known for centuries that, unless the source of the infection is controlled, the patient cannot be cured of his or her infective process and that death will eventually ensue. Surgical control or percutaneous drainage of the infective process is therefore essential in most patients with severe intra-abdominal infections; recovery will not occur without them. Infected central venous catheters must be removed from patients with catheter related sepsis [45].Antimicrobial AgentsAntimicrobial therapy remains the cornerstone of treatment in patients with sepsis. Empiric intravenous antibiotic therapy should be started within the first hour of recognition of severe sepsis, after appropriate cultures have been obtained. The choice of antibiotics is largely determined by the source or focus of infection, the patient's immunologic status, whether the infection is nosocomial or community acquired as well as knowledge of the local microbiology and sensitivity pattern. Initial empirical anti-infective therapy should include one or more drugs that have activity against the likely pathogens (bacterial or fungal) and that penetrate into the presumed source of sepsis. Because the identity of the infecting pathogen(s) and its sensitivity pattern(s) are unknown at the time of initiation of antibiotics, patients with severe sepsis and septic shock the initial regimen should include two or more antibiotics or an extended spectrum β-lactam antibiotic. A number of studies have demonstrated that appropriate initial antimicrobial therapy, defined as the use of at least one antibiotic active in vitro against the causative bacteria reduced mortality when compared with patients receiving inappropriate therapy [45,46]. Once a pathogen is isolated, monotherapy is adequate for most infections; this strategy of initiating broad-spectrum cover with two or more antibiotics and then narrowing the spectrum to a single agent when a pathogen is identified is known as “antimicrobial de-escalation.” The indications for continuation of double-antimicrobial therapy include enterococcal infections and severe intra-abdominal infections. The role of double-antimicrobial therapy with a β-lactam antibiotic and aminoglycoside in patients with suspected or proven Pseudomonas aeruginosa infections is unclear; however, double coverage is prudent in immunocompromised patients [47,48]. In patients with culture-negative sepsis, continuation of the initial empiric combination is warranted. Additional antibiotics or a change in antibiotics may be required in patients with culture-negative sepsis who do not appear to be responding to the initial empiric regimen.Although monotherapy is considered standard for community-acquired pneumonia, a survival benefit of a combination β-lactam and macrolide has been suggested. Waterer et al. found that patients with bacteremic pneumococcal disease who receive at least two effective antibiotic agents within the first 24 hours after presentation to hospital had a significantly lower mortality than patients who received only one effective antibiotic agent [49]. The most common combination was a third-generation cephalosporin with a macrolide or quinolone. Using a large hospital database, Brown et al. demonstrated a lower mortality, shorter length of stay and lower hospital charges for patients with community-acquired pneumonia treated with dual therapy using macrolides as the second agent [50].To rapidly achieve adequate blood and tissue concentrations, antibiotics should be given intravenously, at least initially. Dosing regimens should take into account whether the antibiotic “kills” by time-dependent kinetics (e.g., β-lactam antibiotics, vancomycin) or concentration-dependent kinetics (e.g., aminoglycoside) [51,52]. The clinical effectiveness of β-lactam antibiotics and vancomycin is optimal when the concentration of the antimicrobial agent in the serum exceeds the minimum inhibitory concentration of the infecting organism for at least 40% of the dosing interval. In addition, antibiotic dosing should also take into account the patient's hepatic and renal function.Chastre et al. performed a study in which patients with ventilator associated pneumonia were randomized to receive either 8 or 15 days of antibiotics [53]. Those treated for 8 days had neither
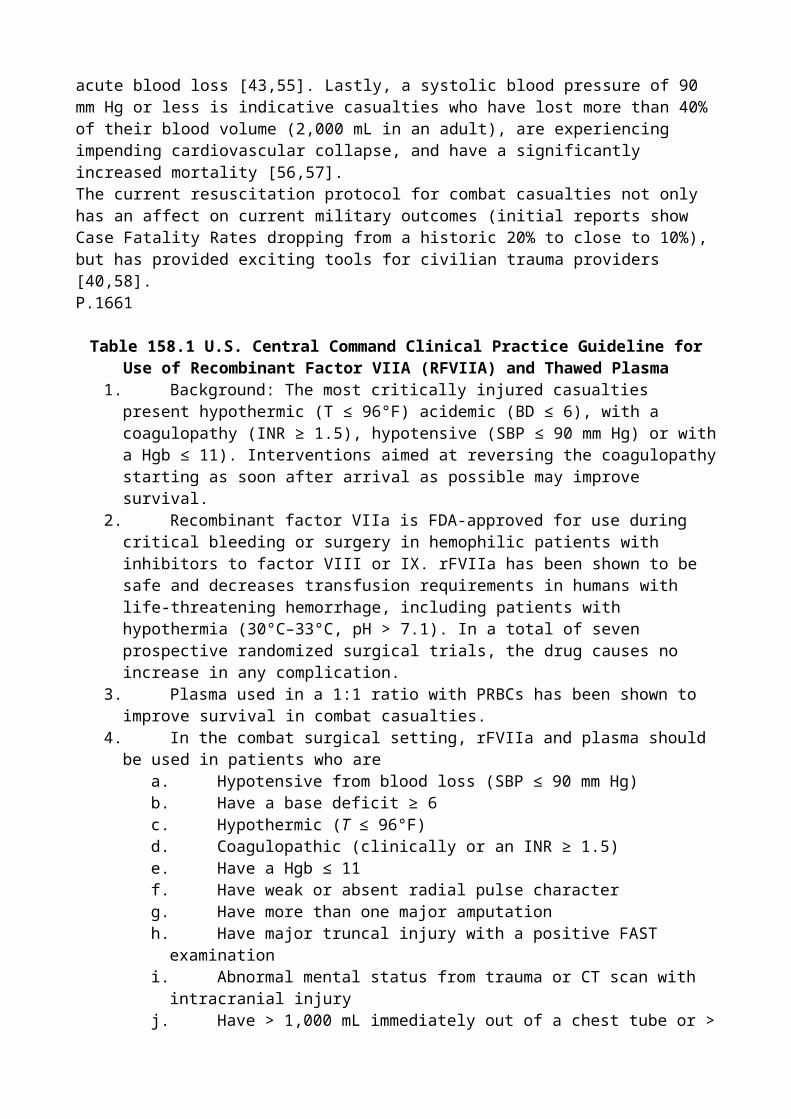
excess mortality nor more recurrent infections, although those with nonfermenting Gram-negative bacilli did have a higher pulmonary infection recurrence rate. Antibiotics should therefore be continued until clinical improvement is noted and ordinarily should not be continued for more than 10 days (14 days for P. aeruginosa and Acinetobacter species), except in cases of osteomyelitis and endocarditis.Hemodynamic SupportFluid Resuscitation: Initial Versus LateIn the first hours of severe sepsis, venodilatation, transudation of fluid from the vascular space into the tissues, reduced oral intake and increased insensible loss combine to produce hypovolemia. Along with ventricular dysfunction, and arteriolar dilation volume depletion contributes to impaired global perfusion and organ function. Treating hypovolemia is the most important component of the early management of severe sepsis. However, once the patient has received an adequate fluid challenge (3 to 5 L) further fluid challenges may not increase cardiac output and global perfusion. Additional fluid may increase interstitial edema and further comprise the microvascular dysfunction that characterizes severe sepsis. The current paradigm of fluid management in patients with sepsis is one of adequate initial fluid resuscitation followed by conservative late fluid management. Conservative late fluid management is defined as even-to-negative fluid balance measured on at least two consecutive days during the first 7 day after septic shock onset. In a retrospective cohort study, Murphy et al. demonstrated that an approach that combines both adequate initial fluid resuscitation followed by conservative late fluid management was associated with improved survival [54]. Additional studies have demonstrated that those patients who have a smaller cumulative fluid balance have improved clinical outcomes [55,56,57].Although the type of fluid used in the resuscitation of patients with sepsis has not been definitively shown to affect outcome, subgroup analysis of the SAFE study suggested a trend towards a more favorable outcome in patients who received albumin [58]. This finding is supported by experimental studies [59] and patients with malaria (similar pathophysiology to Gram-negative sepsis) [60]. Albumin has a number of properties that may be advantageous in patients with sepsis including the maintenance of the endothelial glycocalyx and endothelial function as well as having antioxidant and anti-inflammatory properties that may translate into less “third” space fluid loss. Hydroxyethyl starch solutions were previously recommended in patients with sepsis; however, these synthetic colloids have recently been demonstrated to be associated with an increased risk of renal failure (and death) and should therefore be avoided in patients with sepsis [61]. Despite differences in composition, normal saline (NS) and Lactated Ringer's solution (LR) are frequently considered equivalent and lumped under the term “balanced salt solution.” However, both experimental and clinical data have demonstrated that these fluids are not equivalent. Studies have demonstrated the development of a hyperchloremic metabolic acidosis in human volunteers and patients P.1675
resuscitated with normal saline [62,63,64,65]. Although the clinical implications of this finding are unclear, the additional loss (renal) of HCO3 in the setting of reduced buffering capacity only adds to
the acid–base burden characteristic of hypoperfused states [63]. Furthermore, resuscitation with normal saline may produce a “dilutional acidosis.” Many erroneously believe that LR may worsen or cause a “lactic acidosis.” This is impossible as lactate (the base) has already donated H+ ions; indeed, LR is converted to glucose (mainly in the liver). This reaction consumes hydrogen ions, thereby generating HCO3 [66]. Although, the lactate concentration (base) may increase with LR,
this increase is associated with an increase in HCO3 and an increase in pH (even with liver disease).
This observation was elegantly demonstrated by Phillips et al. in a swine hemorrhagic shock model; the results demonstrated a significantly higher pH (7.41 vs. 7.17) in animals resuscitated with LR as compared to normal saline [67]. In addition to its effects on acid–base balance, solutions high in chloride have been shown both experimentally and clinically to reduce the glomerular filtration rate (GFR) (due to tubuloglomerular feedback) [68]. The effects of normal saline on acid–base balance and renal function may be dose related. These data suggest that in patients with sepsis (except those
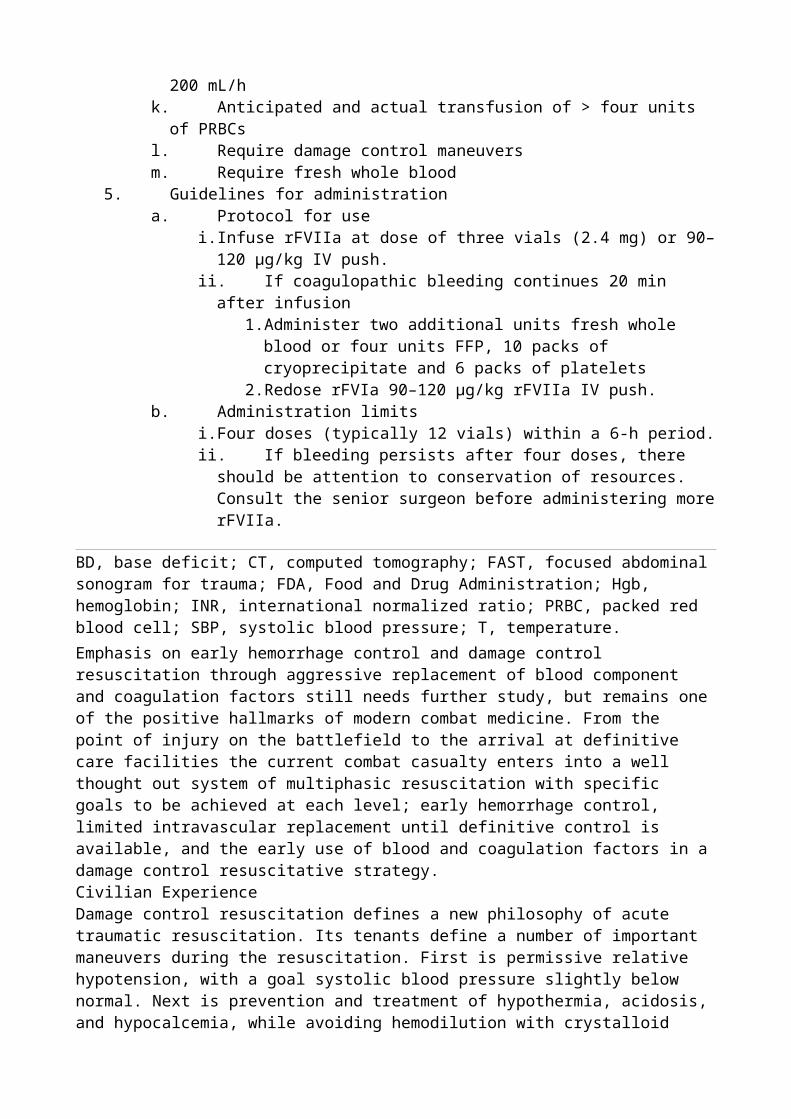
with hyperkalemia), LR may be preferable to normal saline. There is however, no outcome data to support this recommendation. Furthermore, it should be noted LR solution is a racemic mixture containing both the L- and D-isomer of lactate. Small animal hemorrhagic shock models have suggested that the D-isomer is proinflammatory and increases apoptotic cell death [69,70,71]. The clinical implications of these findings are unclear.On the synthesis of these data, we recommend initial resuscitation with NS (30 mL per kg). Normal saline is preferred until renal function tests and potassium are known. Patients who respond poorly to this initial bolus (±2 L) may best be fluid resuscitated with alternating boluses (500 mL) of albumin and LR until the hemodynamic goals are achieved (see “The Endpoints of Resuscitation” section and Fig. 159.1). The goal of this approach is to maintain normal acid–base balance, achieve adequate intravascular volume, and yet limit the total amount of fluid given.Vasopressors, Inotropes, and Cardiac FunctionThe optimal time to initiate vasopressor agents has not been rigorously studied. Many patients with severe sepsis will respond to a 2-L fluid challenge and require little additional hemodynamic support. Others will remain hypotensive despite 10 L of fluid (fluid does not increase vascular tone!). The goal of fluid resuscitation is the rapid early restoration of intravascular volume followed by a conservative fluid strategy. We have therefore recommended that a vasopressor agent (norepinephrine) be started once the patient has received 2 L of crystalloid [6,72]. At this point, the norepinephrine (starting at 0.01 μg per kg per minute) should be titrated upwards while fluid resuscitation continues (albumin and LR). Ongoing fluid resuscitation should be guided by mean arterial pressure, pulse pressure variation, urine output, oxygenation as well as cardiac output (determined noninvasively), and extravascular lung water measurement [73,74]. Bedside echocardiography is very useful to determine LV size and function. The CVP neither intravascular volume nor does it predict fluid responsiveness and therefore has no place in the resuscitation of patients with sepsis [75].Although there are little data to suggest that one vasopressor results in better outcomes than another (norepinephrine, epinephrine, vasopressin) [76,77,78], we favor norepinephrine as the first-line agent followed by dobutamine or epinephrine in patients with poor LV function and vasopressin (fixed dose of 0.03 U per minute) in patients with “preserved” LV function and a low systemic vascular resistance (see Fig. 159.1). In patients with sepsis, norepinephrine increases blood pressure, as well as cardiac output, renal, splanchnic, cerebral blood flow, and microvascular blood flow while minimally increasing heart rate [79,80]. Norepinephrine would therefore appear to be the ideal fist-line agent for the management of septic shock; additional agents should be considered in patients who remain hypotensive or display evidence of inadequate tissue or organ perfusion despite doses of norepinephrine up to 0.2 μg per kg per minute. The second/third-line agents should be chosen based on the patient's hemodynamic profile as determined by ECHO and noninvasive assessment of cardiac output.Dopamine has a number of theoretical disadvantages in patients with sepsis. It tends to increase heart rate that increases myocardial oxygen demand and is associated with splanchnic mucosal ischemia. In addition, dopamine inhibits T and B lymphocytes and decreases secretion of prolactin, growth hormone, and TSH. The SOAP study suggested that septic patients who received dopamine had an increased mortality when compared with other vasopressors [81]. This drug should therefore be avoided in patients with sepsis. Similarly phenylephrine is not recommended, as in experimental models it decreases cardiac output as well as renal and splanchnic blood flow [82]. Furthermore, these agents have not been rigorously tested in randomized controlled studies.
The Endpoints of ResuscitationThe optimal “hemodynamic” endpoint of resuscitation in patients with sepsis is unknown. Similarly, the target mean arterial pressure (MAP) is controversial. Traditional teaching suggests that we should achieve a MAP above 60 mm Hg. However, this pressure is below the autoregulatory range of a number of organs, particularly in elderly patients with atherosclerotic disease. The Surviving Sepsis Campaign Guidelines suggest targeting a MAP above 65 mm Hg [10]. In a dose escalation
study, Jhanji et al. incrementally increased the dose of norepinephrine to achieve a MAP of 60, then 70, then 80, and lastly 90 mm Hg [80]. In this study, global oxygen delivery, cutaneous microvascular flow, and tissue oxygenation increased with each sequential increase in MAP. However, LeDoux et al. demonstrated that increasing the MAP from 65 to 85 mm Hg with norepinephrine did not significantly affect systemic oxygen metabolism, skin microcirculatory blood flow, urine output, or splanchnic perfusion [83]. Dubin demonstrated that increasing mean arterial pressure from 65 to 75 and 85 mm Hg did not improve microcirculatory blood flow [84]. Similarly, Bourgoin et al. demonstrated that increasing MAP from 65 to 85 mm Hg with norepinephrine neither affected metabolic variables nor improved renal function [85]. However, Derudre et al. demonstrated that in patients with septic shock when the MAP was increased from 65 to 75 mm Hg, urinary output increased significantly while the renal resistive index significantly decreased [86]. These data suggest that although the endpoint of resuscitation should be individualized, a MAP of 65 to 70 mm Hg may be a reasonable initial target.Central venous oxygen saturation (ScvO2) is used as the endpoint of resuscitation in the EGDT
algorithm [43]. This is problematic for a number of reasons. Septic patients usually have a normal or increased ScvO2 due to reduced oxygen extraction [87,88]. A normal ScvO2 therefore does not
exclude tissue hypoxia [89]. A low ScvO2 is an important sign of inadequate oxygen delivery to
meet systemic oxygen demands. However, it provides no information for the reason for this inadequacy, nor does it provide guidance as to the optimal therapeutic approach. It is noteworthy that in the Rivers study the mean ScvO2 was 49% with 65% of patients having a ScvO2 less than
70%. To our knowledge, no other sepsis study has reproduced this finding, with the mean ScvO2
(on presentation) P.1676
in most sepsis studies being approximately 70% [89,90,91]. This suggests that other factors may have been in play to account for the low ScvO2 in the Rivers study [92,93]. These factors include
the delayed presentation to hospital (possibly due to socioeconomic factors), greater number of patients with comorbid medical conditions and a high incidence of alcohol use [93]. Thus the combination of significant comorbidities (including heart disease) and a more delayed arrival of patients to the Emergency Department in the River's study may have led to a low cardiac output state, and in turn, to the very low ScvO2 values.
Adjunctive TherapiesWhile antibiotics, fluid resuscitation, vasopressors/inotropic agents and source control form the basic elements of the management of severe sepsis/septic shock, a number of adjunctive agents have been demonstrated to improve outcome or hold promise in improving the outcome of patients with sepsis. These agents should be considered in patients with severe sepsis/septic shock. The benefit of these agents is, however, time dependent and should be started as soon as possible and always within the first 24 hours of ICU admissionCorticosteroidsWhile the role of hydrocortisone in patients with septic shock is controversial, hydrocortisone should be considered in patients who require in excess of 0.2 μg per kg per minute of norepinephrine [94,95]. Adrenal function testing is not required in these patients. Evolving data suggest that increased levels of inflammatory mediators persist long after clinical resolution of sepsis [96,97]. Furthermore, abruptly stopping steroids results in a rebound phenomenon with worsening lung inflammation and hypotension These data suggest that the duration of therapy should be guided by the length of the immune dysregulation and should then be followed by a slow taper. Furthermore, the risk/benefit ratio of treatment with glucocorticoids is tightly linked to the dosage used. Although high doses of glucocorticoids blunt all arms of the immune system, stress-doses (200 to 300 mg hydrocortisone Eq per day) inhibit systemic inflammation; yet, maintain innate and Th1 immune responsiveness and prevent an overwhelming compensatory anti-inflammatory response [98,99]. Similarly, although myopathy is common in patients treated with
high-dose corticosteroids, this complication is uncommon with stress-doses of corticosteroids. On the basis of these data, we suggest treatment with hydrocortisone in a dose of 50 mg every 6 hourly or a 100 mg bolus followed by an infusion at 10 mg per hour for 10 to 14 days followed by a slow taper.Activated Protein CThe PROWESS study demonstrated a significant reduction in mortality in patients with severe sepsis and septic shock who were treated with activated protein C (APC) within 24 hours of hospital admission [100]. APC should be considered in patients with septic shock and those with sepsis and at least one organ failure, who are at a high risk of death, particularly patients with severe community-acquired pneumonia [101]. The use of APC in patients with sepsis has, however, become a very controversial and charged issue. This is largely driven by the high rate of serious bleeding that has been reported in retrospective cohort studies [102]. APC should be avoided in patients at high risk of bleeding, including patients with a platelet count of < 30,000 per mL3. Although APC increases the partial thromboplastin time (PTT) in vitro, the PROWESS study demonstrated an increased risk of bleeding when the PTT increased above 75 seconds. On the basis of these data, we monitor the PTT in patients on APC and hold the infusion (for a few hours) and transfuse FFP when the PTT exceeds 80 seconds (anecdotal experience only). Disseminated intravascular coagulation (DIC) is not a contraindication to APC; indeed in PROWESS the risk reduction was greater in patients with overt DIC than those without DIC (RR of 0.6 vs. 0.85) [103].Patients with purpura fulminans and multiorgan failure due to meningococcal infection have significantly higher plasma PAI-1 levels as well as lower protein C levels than patients with meningococcal infection, but without purpura or organ failure [104]. In view of the low protein C levels in purpura fulminans, numerous case reports as well as open label studies have been published suggesting a benefit of treatment with APC [104,105,106]. Many of these patients concomitantly received FFP, fibrinogen, and platelets. APC has also been used for the treatment of purpura fulminans associated with Streptococcal and Staphylococcal infections [107].Enteral Nutrition Supplemented with Omega-3 Fatty AcidsThree randomized controlled trials have demonstrated that in patients with sepsis and ARDS an enteral nutritional formula high in omega-3 fatty acids was associated with an increase in ventilator-free days, a shorter ICU stay, and a lower morality than patients fed a diet with a low omega-3 to omega-6 fatty acid ratio [108]. On the basis of these data, an enteral nutritional formula high in omega-3 fatty acids should be initiated within 24 hours of admission to the ICU. Patients are best fed gastrically via an oral or nasogastric tube. The use of vasopressors agents is not a contraindication to the use of enteral nutrition; indeed, enteral nutrition reduces the risk of gastric stress ulceration and bowel ischemia [109,110].Polyclonal ImmunoglobulinsTwo meta-analyses have demonstrated that polyclonal immunoglobulins particularly those preparations enriched with IgA and IgM (IgGAM) reduce the mortality in patients with septic shock [111,112]. It is not clear which patient subgroups would benefit from this therapy; clearly asplenic patients should receive IgGAM as well as those patients at high risk of death.Adjunctive Therapies of Possible BenefitStatinsHMG-CoA reductase inhibitors (statins) are a group of drugs with anti-inflammatory, immunomodulating, antioxidant, antiproliferative, antiapoptotic, antithrombotic, and endothelial stabilizing effects. Statins increase expression of endothelial nitric oxide (eNOS) while downregulating inducible nitric oxide (iNOS) [113]. Furthermore, statins interfere with leucocyte–endothelial interactions by decreasing expression of adhesion molecules and have antithrombotic effects. Experimental P.1677
sepsis studies have demonstrated improved outcome with the use of statins and clinical studies have demonstrated that patients taking statins have a better outcome when they become septic
[113,114,115]. We recommend the use of high-dose statins (e.g., atorvastatin/simvastatin 80 mg daily) in patients with severe sepsis; statins should however be avoided in patients taking azole antifungal as well as calcineurin inhibitors. The clinician should monitor for rhabdomyolysis.SeleniumSepsis is associated with an increase in reactive oxygen species and low endogenous antioxidative capacity. The selenium dependent glutathione-peroxidases (GPx) as well as thioredoxin reductases are important compounds responsible for the maintenance of the redox system in all cells including the immune-competent cells. The activity of these enzymes is mainly regulated by the availability of selenium. The selenium in intensive care (SIC) study demonstrated that high-dose intravenous selenium improved the outcome of patients with severe SIRS, sepsis, and septic shock [116]. Selenium supplementation should be considered in patients with severe sepsis and septic shock. Although the optimal dose and route remain to be established, we recommend a dose of 400 to 600 μg PO daily.ZincZinc is required for normal function of both the innate and acquired immune systems. Zinc deficiency results in marked abnormalities of immune function with zinc supplementation restoring natural killer cell activity, lymphocyte production, mitogen responses, wound healing, and resistance to infection. Stress, trauma, and sepsis have been associated with very low serum zinc levels [117,118]. In an experimental sepsis model, mortality was significantly increased with zinc deficiency, while zinc supplementation normalized the inflammatory response, diminished tissue damage and reduced mortality [119]. The benefit of zinc supplementation in patients with sepsis has yet to be determined.ConclusionThe last two decades has seen a remarkable growth in our understanding of sepsis and the complex interconnection of multiple biological pathways involved in the septic process. This increased knowledge has opened the door to new therapeutic approaches to sepsis, and it is likely that these new approaches will lead to a reduction in the morbidity and mortality of patients with sepsis.
Chapter 160Multiple Organ Dysfunction SyndromeAndrew C. BernardTimothy A. PrittsCare of the critically ill has advanced substantially in the past 50 years to the point that patients who previously succumbed to illness or injury may now survive their initial insult. Unfortunately, this places them at risk for multiple organ dysfunction syndrome (MODS), with subsequent failure of organ systems and increased mortality [1]. A thorough understanding of the pathophysiology and treatment of MODS is necessary to attempt to mitigate associated secondary morbidity and mortality.MODS can be defined as “the inability of one or more organs to support its activities spontaneously without intervention” [2]. Initial recognition of MODS came from combat casualty care during
World War II as resuscitation strategies advanced sufficiently to allow casualties to survive the initial hemorrhagic shock insult, but rendered them vulnerable to subsequent acute renal failure [3]. Improved intensive care and resuscitation strategies subsequently led to the recognition of pulmonary failure in the form of ARDS during the Vietnam conflict [4]. Basic science and clinical research has increased our insight into the role of cellular hypoxia in the development of organ dysfunction and failure. Although advances in support for failing organs, including continuous dialysis and advanced ventilator care, have potentially increased survival, MODS remains a common cause of death in the intensive care unit.Diagnostic Criteria and Scoring SystemsMODS severity determines mortality [5]. Organ failure severity scoring was initially described by Knaus in 1985 [6]. Modern scoring systems consider grade and severity and are intended to serve as predictors of outcome. Among the most commonly used scoring systems are the multiple organ dysfunction score (MODS), sequential organ failure assessment (SOFA) and logistic organ dysfunction score (LODS) [7,8,9]. All include clinical and laboratory data for six organs: respiratory, cardiovascular, hematologic, hepatic, renal, and central nervous system (Table 160.1) [10]. The Denver Multiple Organ Failure (MOF) score is a simpler 4-point scale that has similar or superior specificity [11]. A “cellular injury score” based on measures of cellular dysfunction has also been described [12]. No single scoring system has been proven superior but all predict outcome more accurately than health care resource utilization [11,13]. The acute physiology and chronic health evaluation (APACHE), originally described by Knaus in 1985, is a scoring system that considers patient factors unrelated to the acute illness as well as acute illness severity [14]. APACHE considers many variables and is therefore not as easily calculable at P.1680
the bedside as MODS, SOFA, LODS, or Denver, but it reliably predicts both outcome and resource utilization, has been refined to its current version, APACHE IV, and may be useful for benchmarking ICU performance [15].
Table 160.1 Criteria Used in Common Organ Dysfunction Scoring Systems
Organ VariableDenver MOF [11] SOFA [8] LODS [9] MODS [7]
Respiratory PaO2/FIO2 Yes Yes Yes Yes
MV Yes Hematology Platelets Yes Yes Yes WBC Yes Hepatic Bilirubin Yes Yes Yes Yes Prothrombin time Yes Cardiovascular MAP Yes SBP Yes Heart rate Yes PAR [(HR*CVP)/MAP] Yes Dopamine Yes Dobutamine Yes Epinephrine Yes Norepinephrine Yes Any inotrope Yes CNS GCS Yes Yes YesRenal Creatinine Yes Yes Yes Yes BUN Yes Urine output Yes Yes Denver MOF, Denver multiple organ failure score; SOFA, sequential organ failure assessment; LODS, logistic organ dysfunction score; MODS, multiple organ dysfunction score; PaO2, blood
partial pressure of oxygen; FIO2, fraction of inspired gas which is oxygen; MV, mechanical
ventilation requirement; WBC, elevated white blood count; PAR, pressure adjusted heart rate; HR, heart rate; CVP, central venous pressure; MAP, mean arterial pressure; SBP, systolic blood pressure; CNS, central nervous system; GCS, Glasgow Coma Scale score; BUN, blood urea nitrogen.Modified from Mizock BA: The multiple organ dysfunction syndrome. Dis Mon 55(8):476–526, 2009.EpidemiologyIncidence of MODS varies based on primary diagnosis and the scoring system used to determine organ dysfunction. Seventy-one percent of ICU patients have some organ dysfunction [16] and about half have MODS [17], depending on the criteria used. For example, in one adult trauma ICU 47% had MODS, defined by SOFA ≤ 3 in two or more systems [18]. Septic patients are more likely to have organ dysfunction and more organ failures than nonseptic patients and mortality is higher if sepsis is present (31% vs. 21%) [16].EtiologyMODS is most often the result of shock, sepsis, and trauma but there are many causes (Table 160.2) [19]. Forty-one percent of those patients with organ dysfunction have sepsis [16]. Sepsis most commonly originates in the lung (68%) and abdomen (22%) but there are many causes of sepsis-induced MODS [16].Mechanisms of Multiorgan Dysfunction SyndromeThe systemic inflammatory response syndrome (SIRS) is frequently viewed as a predecessor to MODS and these syndromes represent a continuum of dysfunction. Components of the SIRS response are seen in virtually all patients following operation or injury. This response is usually self-regulating and rarely progresses to MODS. MODS may be viewed as a result of an ongoing and dysregulated SIRS response with progressive organ system derangement.Despite extensive efforts, the pathophysiology of MODS is not fully understood and remains an area of intensive investigation [20]. Several mechanisms for the onset and propagation of MODS have been proposed, including an initial insult leading immediately to organ failure, a “two hit” model, where an initial stimulus primes the immune system to respond to a subsequent insult with an exuberant reaction, and the concept that a continuous ongoing insult contributes to MODS [20]. In clinical practice, each of these scenarios may result in MODS.A common theme in the onset and propagation of MODS is the presence of a disordered immune response. It is likely that ongoing tissue hypoxia leads to activation of the acute inflammatory response and to dysregulation of the immune system [21]. Although the inflammatory response is an important component of normal recovery from injury and illness, organ failure appears to result from a loss of the balance between the pro- and anti-inflammatory cascades [22]. The proinflammatory response to a stimulus predominates initially, with increased release of proinflammatory mediators, increased capillary permeability, macrophage and neutrophil activation with tissue invasion and damage, disordered apoptosis, and microvascular thrombosis [23]. This initial response is normally tempered by the anti-inflammatory response, but this relationship may become dysfunctional. Together, these processes lead to early onset of MODS. If the organism survives the initial insult and onset of MODS, a period of immunosuppression follows. During this period, the patient becomes highly susceptible to nosocomial infection, with a normally survivable event such as pneumonia representing a life-threatening “second hit” [24].P.1681
Table 160.2 Risk Factors for ModsInfection Peritonitis and intra-abdominal infection Pneumonia Necrotizing soft tissue infections Tropical infections (e.g., falciparum malaria, typhoid fever, dengue fever)Inflammation
PancreatitisIschemia Ruptured aortic aneurysm Hemorrhagic shock Mesenteric ischemiaImmune reactions Autoimmune disease Reactive hemophagocytic syndrome Antiphospholipid antibody syndrome Transplant rejection Graft versus host diseaseIatrogenic causes Delayed or missed injury Blood transfusion Injurious mechanical ventilation Treatment associated increased intra-abdominal pressureIntoxication Drug reactions (anticonvulsants, carboplatin, antiretrovirals, colchicines, propofol, amiodarone, monoclonal antibodies) Arsenic Drug intoxication (ecstasy, cocaine, salicylates, acetaminophen)Endocrine Adrenal crisis Pheochromocytoma Thyroid storm Myxedema comaReproduced from Mizock BA: The multiple organ dysfunction syndrome. Dis Mon 55(8):476–526, 2009.
Table 160.3 Advances in Management of Multiple Organ Dysfunction Syndrome Based on Randomized Controlled Clinical Trials
Advance ReferenceRemarksEarly goal-directed therapy using venous oxygen saturation as a target.
[35] Included as one of the Surviving Sepsis Guidelines.
Digestive tract or oropharynx decontamination with antimicrobials reduces 28-day mortality in ICU patients
[40] Not widely practiced in the United States, as it conflicts with principles of antimicrobial stewardship
Lung protective ventilation strategies are associated with reduced mortality and increased ventilator-free days
[43] Lung protective strategies are commonly utilized in ICU settings
Aggressive enteral nutrition is associated with improved immune function and less mortality in burned children
[49] Landmark study suggested that protein repletion is essential in critically ill patients
Adjuvant treatment of patients with severe sepsis and septic shock with selenium is associated with decreased mortality
[53] Mechanism of effect is unknown
Extensive research continues to examine the potential role of the intestine in the onset and propagation of SIRS and MODS. From this work, it is hypothesized that acute injury damages the intestinal mucosa, leading to increased cytokine production from the intestinal epithelium and lamina propria with resultant systemic inflammatory response, and organ injury [25,26]. Under these circumstances, the intestinal barrier fails, leading to organ dysfunction. More recent studies have begun to examine the gut as a source of mediators that directly lead to organ damage [27]. These studies suggest that substances in the gut-derived mesenteric lymph directly lead to
pulmonary dysfunction during shock states [28]. Full characterization of these mediators remains elusive.Current Management StrategiesCourse of MODSOutcome in MODS partly depends upon host factors including genetics. Some patients are genetically predisposed to enhanced immune reactivity [29]. In most patients, MODS progression follows a typical sequence first described by Don Fry in 1980, beginning with lung failure, followed by the liver, gastric mucosa, and kidney [30]. Lung dysfunction was recently reaffirmed as the initial manifestation of MODS in the majority of patients [31]. Although a typical sequence of organ dysfunction usually occurs, the timing and rate of progression vary. MODS follows a bimodal onset with early and late MODS characterized by different patient characteristics and mechanisms of death [32]. An important distinction must also be made with early organ dysfunction during resuscitation, which is often reversible, and not necessarily the same as early MODS [33].Respiratory organ dysfunction is the most common early manifestation of MODS but is often not associated with death [34]. Renal, central nervous and hematologic system impairments characterize MODS progression and are more strongly associated with mortality. Treatment of MODS therefore is focused on early recognition of those at risk, removing the source, and preventing MODS progression [35]. Clinicians should move briskly to optimize cardiorespiratory function, remove catabolic foci, and provide nutrition while using antimicrobials selectively and avoiding transfusion. Key advances in the treatment of patients with severe critical illness and MODS based on randomized controlled trials are summarized in Table 160.3.P.1682
ResuscitationThe Surviving Sepsis Guidelines summarize current best practice regarding resuscitation as of 2008 [36]. One major strategy to reduce MODS is to ensure optimal initial resuscitation. Resuscitation should target adequate oxygen delivery evidenced by oxygen saturation in mixed venous blood (SvO2-saturation in mixed venous blood obtained from a pulmonary artery catheter or ScvO2-
saturation in central venous blood obtained from a central venous catheter in superior vena cava). Rivers et al. showed that by using oxygen delivery as a target for resuscitation with fluid, blood, and inotropes, lactic acidemia was less severe and outcomes were improved [37]. Inadequate initial resuscitation contributes to MODS [38]. For a comprehensive discussion of this topic, see Chapter 159.Preventing MODS ProgressionSource control is critical to prevent perpetuation of the inflammatory response [36]. Antimicrobials should be used as above, with tailored therapy and de-escalation [13]. On the basis of the possible role of the gut and enteric bacteria as a “motor” for MODS, several groups have proposed cleansing the bowel of bacteria to disrupt this relationship, but studies have yielded conflicting results and this practice remains controversial [27,28,29,39]. Although a recent European study supports parenteral and topical oropharyngeal antibiotics in reducing mortality, this is not widely accepted in the United States because it seemingly goes against the principle of antimicrobial stewardship [40]. Transfusion is a risk factor for MODS, suggesting that a conservative approach to blood transfusion is appropriate [41].Mechanical ventilation contributes to distant organ dysfunction in acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) [42]. In the ARDSNet trial, the “lung protective strategy” of plateau ≤ 30 cm H2O and tidal volumes ≤ 6 mL per kg body weight was associated with a reduction
in all cause mortality of 9% compared with conventional ventilation with plateau pressures ≤ 50 cm H2O and tidal volumes ≤ 12 mL per kg body weight [43]. A European study affirmed that use of a
ventilation strategy with volumes greater than ARDSNet (> 7.4 mL tidal volume per kg body weight) increased mortality [44]. For a comprehensive discussion of this topic, see Chapters 47 and 58.
Although Van den Berghe initially reported reduced mortality with intensive insulin therapy and the mortality reduction was in septic MODS [45], unacceptably high rates of hypoglycemia have since been reported [46] without a mortality benefit.Steroid therapy in patients with sepsis and MODS may be used for select indications. For a comprehensive discussion of this topic, see Chapter 159.NutritionThere are data to suggest that early initiation of enteral nutrition improves outcome in patients with severe trauma, surgery, sepsis, and MODS. MODS is attenuated in patients receiving enteral nutrition within 24 hours as opposed to initiation later [47,48]. Recent retrospective data support early enteral feeding to reduce ICU and hospital mortality [49]. Both the American and European Societies of Parenteral and Enteral Nutrition (ASPEN and ESPEN) recommend enteral nutrition in ventilated patients if hemodynamics are adequate and gastrointestinal function is present and the gut works [50,51]. Arginine has been shown to be beneficial in surgical and trauma patients but cannot be recommended in septic medical patients because of immunoinflammatory characteristics [50]. However, omega fatty acids do appear beneficial in shortening length of stay, ventilator days, and mortality in septic patients. Serum selenium is depleted in trauma and surgical patients and some evidence suggests that selenium depletion contributes to MODS. Selenium repletion reduced MODS in a multi-institutional prospective randomized trial [52]. For a comprehensive discussion of this topic, see Chapters 159 and 192.Recombinant human activated protein C was initially shown to reduce mortality in septic patients though its benefit has been questioned in recent studies [13]. rhAPC remains indicated in adults with high risk of death [36]. For a comprehensive discussion of this topic, see Chapter 159.Continuous renal replacement therapy has been associated with reduction of MODS severity, theoretically due to modulation of elevated pro- and anti-inflammatory cytokines [53], but no large studies currently support its use for this purpose. Other novel therapies include pharmacologic manipulation of the microcirculation or augmentation of mitochondrial oxidative metabolism to enhance oxygen delivery [13].Prognosis and ICU Length of StayUp to 20% of patients admitted to intensive care units develop aspects of MODS, with significantly increased morbidity and mortality [54]. MODS severity is decreasing but ICU mortality remains stable, perhaps because overall acuity is increasing [35,55]. In an epidemiologic study of sepsis in 2001, Angus determined that dysfunction of one, two, or three organ systems conveys 1%, 4.7%, and 20.7% mortality, respectively [19]. Four-organ dysfunction was associated with 65% to 74% mortality [16,19]. A more recent study examining the outcomes of critically ill patients reported ICU mortality of 10% for failure of three systems or less, increasing to 25% and 50% for four- and five-organ system failure, respectively. Mortality of seven-system failure was 100% [56]. In addition to mortality, MODS also affects long-term functional outcome [18].MODS is the most common reason for prolonged stays in the intensive care unit, exceeding single organ system failure and simply the need for ventilatory support [54]. The onset of MODS is associated with a markedly increased length of ICU stay and risk of mortality [17]. Determining prognosis for individual patients with MODS remains challenging. Severity of organ dysfunction at the time of ICU admission or during the ICU stay correlates well with mortality, with the highest scores suggestive of a nonsurvivable situation, but does not allow accurate bedside prediction of an individual patient's outcome [7]. The strongest independent risk factors for death appear to be CNS failure (RR = 16.06) and cardiovascular failure (RR = 11.83) [56].ConclusionsMODS is largely a result of medical progress and modern ICU care. A common denominator in the pathogenesis of MODS appears to be cellular hypoperfusion, leading to an imbalanced immune response, with resultant organ damage and failure. Treatment of patients at risk for MODS is supportive, ensuring adequate resuscitation, nutrition, source control, and support of individual organ systems as they fail. Despite modern critical care, MODS remains a common cause of death in critically ill patients.
Chapter 55Shock: GeneralS. Rob ToddKrista L. TurnerFrederick A. MooreHistoryDespite significant technologic advances and the improved understanding of shock, it remains a diagnosis associated with significant morbidity and mortality. Hippocrates and Galen were the first to describe a “posttraumatic syndrome.” Then in 1737, LeDran, a French surgeon, used the term choc to characterize a severe impact or jolt (1). However, it was not until 1867 that Edwin Morris popularized the term (2). He defined shock as “a peculiar effect on the animal system, produced by
violent injuries from any cause, or from violent mental emotions.”In the late 1800s, Fischer and Maphoter further delineated the pathophysiology of shock (3,4). Fischer proposed a generalized “vasomotor paralysis” resulting in splanchnic blood pooling as the underlying mechanism of shock, while Maphoter suggested that the clinical manifestations appreciated in shock were the result of the extravascular leakage of fluids. A variation of Fischer's theory was supported by Crile in 1899 (5).In the early 1900s, Walter B. Cannon proposed a toxin as the source of this altered capillary permeability and intravascular volume loss (6). Blalock challenged this theory in 1930 (7). He charged that significant hemorrhage alone could account for insufficient cardiac output in shock states and that it wasn't the result of circulating toxins. Then in the 1940s, Carl Wiggers demonstrated that following prolonged shock, irreversible circulatory failure could occur (8). At that time, hypotension was synonymous with shock, and blood pressure was the primary end point of resuscitation in shock. As such, volume resuscitation was the primary management strategy.It wasn't until the turn of the 19th century that sources other than trauma were thought to cause shock. Sepsis was first depicted as causing shock during the Spanish American War (9). This was followed in 1906 with the description of anaphylactic shock. And subsequently in 1935, Tennant and Wiggers documented decreased myocardial contractility following coronary perfusion deprivation (10).Definition of ShockThe definition of shock has historically been a moving target. Initially equated with hypotension, this is no longer the case (11,12). Shock is defined as an acute clinical syndrome resulting when cellular dysoxia occurs, ultimately leading to organ dysfunction and failure (13). Cellular dysoxia or inadequate tissue perfusion is critical in diagnosing shock, as there are many other causes of organ dysfunction and failure that are not resultant from shock.Note the emphasis on shock as a syndrome, as this constellation of signs and symptoms predictably follows a well-described series of pathophysiologic events (14). Its clinical presentation varies widely based on the underlying etiology, the degree of organ perfusion, and prior organ dysfunction.Classification of ShockThe incidence and prevalence of shock are poorly characterized for a multitude of reasons. First and foremost, the definition of shock continues to lack consensus. As such, the screening for shock tends to be inadequate, and thus it is underreported. Additionally, patients presumably die in the prehospital setting. Taking these facts into account, one can readily appreciate why the reported incidence and mortality of shock varies widely.In 1937, Blalock classified shock (15). He defined four categories: hematogenic or oligemic (hypovolemic), cardiogenic, neurogenic, and vasogenic. Subsequently, Weil and Shubin characterized shock based on cardiovascular parameters (16). The categories included hypovolemic, cardiogenic, extracardiac obstructive, and distributive. Table 55.1 represents an adaptation of this system (17). It is important to appreciate that most shock states incorporate different components of each of the aforementioned shock categories.Hypovolemic ShockHypovolemic shock represents a state of decreased intravascular volume. Inciting events include internal or external hemorrhage, significant fluid losses from the gastrointestinal tract (emesis, high-output fistulae, or diarrhea) or urinary tract (hyperosmolar states), and “third spacing” (“capillary leakage” into the interstitial tissues or the corporeal cavities) (Table 55.1). Additional etiologies include malnutrition and large open wounds (burns and the open abdomen) (16,18).The pathophysiology of shock is dependent upon its classification. Hypovolemic shock is characterized by a decrease in intravascular volume with resultant decreases in pulmonary capillary wedge pressure and cardiac output (Table 55.2). There is a subsequent increased sympathetic drive in an attempt to increase peripheral vasculature tone, cardiac contractility, and heart rate. These initially beneficial measures ultimately turn detrimental, as their resultant hypermetabolic state predisposes tissues to localized hypoxia (14). Furthermore, the aforementioned increased peripheral vascular tone may result in tissue ischemia via an inconsistent microcirculatory flow. In cases of

P.814severe hypovolemic shock, a significant inflammatory component coexists.
Table 55.1 Shock classificationsHYPOVOLEMICHemorrhagic-Trauma, gastrointestinal, retroperitonealNonhemorrhagic-Dehydration, emesis, diarrhea, fistulae, burns, polyuria, “third spacing,” malnutrition, large open woundsCARDIOGENICMyocardial-Infarction, contusion, myocarditis, cardiomyopathies, pharmacologicMechanical-Valvular failure, ventricular septal defect, ventricular wall defectsArrhythmiasOBSTRUCTIVEImpairment of diastolic filling-Intrathoracic obstructive tumors, tension pneumothorax, positive-pressure mechanical ventilation, constrictive pericarditis, pericardial tamponadeImpairment of systolic contraction-Pulmonary embolism, acute pulmonary hypertension, air embolism, tumors, aortic dissection, aortic coarctationDISTRIBUTIVE-Septic, anaphylactic, neurogenic, pharmacologic, endocrinologicFrom Jimenez EJ. Shock. In: Civetta JM, Taylor RW, Kirby RR, eds. Critical Care 3rd ed. Philadelphia: Lippincott-Raven Publishers; 1997:359; and Kumar A, Parrillo JE. Shock: classification, pathophysiology, and approach to management. In: Parrillo JE, Dellinger RP, eds. Critical Care Medicine 2nd ed. St. Louis: Mosby, Inc.; 2002:371.Cardiogenic ShockCardiogenic shock is defined as inadequate tissue perfusion due to primary ventricular failure. Its incidence has remained fairly stable, and ranges from 6% to 8% (19,20,21,22,23). In the United States, it is the most common cause of mortality from coronary artery disease (19). Despite medical advances, it remains the number one cause of in-hospital mortality in patients experiencing a transmural myocardial infarction, with rates ranging between 70% and 90% (21,24). Other causes include myocarditis, cardiomyopathies, valvular diseases, and arrhythmias (Table 55.1).The most common inciting event in cardiogenic shock is an acute myocardial infarction. Historically, once 40% of the myocardium has been irreversibly damaged, cardiogenic shock may result. From a mechanical perspective, decreased cardiac contractility diminishes both stroke volume and cardiac output (Table 55.2). These lead to increased ventricular filling pressures, cardiac chamber dilatation, and ultimately univentricular or biventricular failure with resultant systemic hypotension. This further reduces myocardial perfusion and exacerbates ongoing ischemia. The end result is a vicious cycle with severe cardiovascular decompensation. Similar to hypovolemic shock, a significant systemic inflammatory response has been implicated in the pathophysiology of cardiogenic shock.Obstructive ShockIn obstructive shock, external forces compress the thin-walled chambers of the heart, the great vessels, or any combination thereof. These forces impair either the diastolic filling or the systolic contraction of the heart (Table 55.1). Large obstructive intrathoracic tumors, tension pneumothoraces, pericardial P.815tamponade, and constrictive pericarditis limit ventricular filling, while pulmonary emboli and aortic dissection impede cardiac contractility.
Table 55.2 Shock hemodynamic parameters
CVP PCWP CO SVR
S[v with bar above]O2
Hypovolemic ↓↓ ↓↓ ↓↓ ↑ ↓Cardiogenic Left ventricular myocardial infarction
Nl or ↑ ↑ ↓↓ ↑ ↓
Right ventricular myocardial infarction
↑↑ Nl or ↑ ↓↓ ↑ ↓
Obstructive Pericardial tamponade ↑↑ ↑↑ ↓ or ↓↓ ↑ ↓ Massive pulmonary embolism ↑↑ Nl or ↓ ↓↓ ↑ ↓Distributive Early Nl or ↑ Nl ↓ or Nl or
↑↑ or Nl or ↓
Nl or ↓
Early after fluid administration Nl or ↑ Nl or ↑ ↑ ↓ ↑ or Nl or ↓ Late Nl Nl ↓ ↑ ↑ or ↓CVP, central venous pressure; PCWP, pulmonary capillary wedge pressure; CO, cardiac output; SVR, systemic vascular resistance; S[v with bar above]O2, mixed venous oxygen saturation; Nl,
normal.From Jimenez EJ. Shock. In: Civetta JM, Taylor RW, Kirby RR, eds. Critical Care. 3rd ed. Philadelphia: Lippincott–Raven Publishers; 1997:359; and Kumar A, Parrillo JE. Shock: classification, pathophysiology, and approach to management. In: Parrillo JE, Dellinger RP, eds. Critical Care Medicine. 2nd ed. St. Louis: Mosby, Inc.; 2002:371.The hemodynamic parameters witnessed in obstructive shock include increases in central venous pressure and systemic vascular resistance and decreases in cardiac output and mixed venous oxygen saturation (Table 55.2). The pulmonary capillary wedge pressure and other hemodynamic indices are dependent on the obstructive cause. In pericardial tamponade, there is equalization of the right and left ventricular diastolic pressures, the central venous pressure, and the pulmonary capillary wedge pressure (increased). However, following a massive pulmonary embolus, right ventricular failure leads to increased right heart pressures and a normal or decreased pulmonary capillary wedge pressure.Distributive ShockDistributive shock is characterized by a decrease in peripheral vascular tone. Septic shock is the most common form. Additionally, distributive shock includes the other oft-quoted classes of shock including anaphylactic, neurogenic, and adrenal shock (Table 55.1).Physiologically, all forms of distributive shock exhibit a decreased systemic vascular resistance (Table 55.2). Subsequently, these patients experience a relative hypovolemia as evidenced by a decreased (or normal) central venous pressure and pulmonary capillary wedge pressure. The cardiac output is initially diminished; however, following appropriate volume loading, the cardiac output is increased.Cellular AlterationsAll forms of shock, especially hemorrhagic and septic, induce a host response that is characterized by local and systemic release of proinflammatory cytokines, arachidonic acid metabolites, and activation of complement factors, kinins, and coagulation as well as hormonal mediators. Clinically, this is the systemic inflammatory response syndrome. Paralleling the systemic inflammatory response syndrome is an anti-inflammatory response referred to as the compensatory anti-inflammatory response syndrome. An imbalance between these responses appears to be responsible for increased susceptibility to infection and organ dysfunction (25,26,27,28,29).Systemic Inflammatory Response Syndrome
In 1991, a consensus conference of the American College of Chest Physicians and the American Society of Critical Care Medicine defined systemic inflammatory response syndrome (SIRS) as a generalized inflammatory response triggered by a variety of infectious and noninfectious events (30). They arbitrarily established clinical parameters through a process of consensus. Table 55.3 summarizes the diagnostic criteria for systemic inflammatory response syndrome. At least two of the four criteria must be present to fulfill the diagnosis of systemic inflammatory response syndrome. Note, this definition emphasizes the inflammatory process regardless of its etiology. Subsequent studies have validated these criteria as predictive of increased intensive care unit mortality, and indicated that this risk increases concurrent with the number of criteria present.The systemic inflammatory response syndrome is characterized by the local and systemic production and release of multiple mediators, including proinflammatory cytokines, complement factors, proteins of the contact phase and coagulation system, acute phase proteins, neuroendocrine mediators, and an accumulation of immunocompetent cells at the local site of tissue damage (31).
Table 55.3 Clinical parameters of the systemic inflammatory response syndrome1. Heart rate >90 beats/min 2. Respiratory rate >20 breaths/min, or PaCO2 <32 mm Hg
3. T emperature >38°C or <36°C 4. Leukocytes >12,000/mm3 or <4,000/mm3 or ≥10% juvenile neutrophil
granulocytes
PaCO2, arterial CO2 partial pressure.
Compensatory Anti-inflammatory Response SyndromeShock stimulates not only the release of proinflammatory mediators, but also the parallel release of anti-inflammatory mediators (26). This compensatory anti-inflammatory response is present concurrently with systemic inflammatory response syndrome (Fig. 55.1) (32). When these two opposing responses are appropriately balanced, the patient is able to effectively recover without incurring secondary injury from the autoimmune inflammatory response (25). However, overwhelming compensatory anti-inflammatory response syndrome appears responsible for postshock immunosuppression, which leads to increased susceptibility to infections and sepsis (26,31,33). With time, the systemic inflammatory response syndrome ceases to exist and the compensatory anti-inflammatory response syndrome is the predominant force.Cytokine ResponseProinflammatory cytokines, tumor necrosis factor-α (TNF-α), and interleukin-1β (IL-1β) are key to the resultant inflammation (34,35). Secondary proinflammatory cytokines are released in a subacute fashion and include IL-2, IL-6, IL-8, platelet-activating factor (PAF), interferon-γ, endothelin-1, leukotrienes, thromboxanes, prostaglandins, and the complement cascade (34,36).Interleukin-6 also acts as an immunoregulatory cytokine by stimulating the release of anti-inflammatory mediators such as IL-1 receptor antagonists and TNF receptors, which bind circulating proinflammatory cytokines (35). IL-6 also triggers the release of prostaglandin E2
(PGE2) from macrophages (35). Prostaglandin E2 is potentially the most potent endogenous
immunosuppressant (35). Not only does it suppress T-cell and macrophage responsiveness, but it also induces the release of P.816IL-10, a potent anti-inflammatory cytokine that deactivates monocytes (35). A listing of pro- and anti-inflammatory mediators may be found in Tables 55.4 and 55.5.
Figure 55.1. Postinjury multiple organ failure occurs as a result of a dysfunctional inflammatory response. SIRS, systemic inflammatory response syndrome; MOF, multiple organ failure; CARS, compensatory anti-inflammatory response syndrome.Cell-mediated Response

Shock alters the ability of splenic, peritoneal, and alveolar macrophages to release IL-1, IL-6, and TNF-α, leading to P.817decreased levels of these proinflammatory cytokines (35). Kupffer cells, however, have an enhanced capacity for production of proinflammatory cytokines. Cell-mediated immunity requires not only functional macrophage and T cells, but also intact macrophage–T-cell interaction (35). Following injury, human leukocyte antigen (HLA-DR) receptor expression is decreased, leading to a loss of antigen-presenting capacity and decreased TNF-α production. Prostaglandin E2, IL-10, and
TGF-β all contribute to this “immunoparalysis” (25,35).Table 55.4 Proinflammatory mediators
MediatorActionIL-1 IL-1 is pleiotropic. Locally, it stimulates cytokine and cytokine receptor production by T
cells as well as stimulating B-cell proliferation. Systemically, IL-1 modulates endocrine responses and induces the acute phase response.
IL-6 IL-6 induces acute phase reactants in hepatocytes and plays an essential role in the final differentiation of B cells into Ig-secreting cells. Additionally, IL-6 has anti-inflammatory properties.
IL-8 IL-8 is one of the major mediators of the inflammatory response. It functions as a chemoattractant and is also a potent angiogenic factor.
IL-12 IL-12 regulates the differentiation of naive T cells into TH1 cells. It stimulates the growth
and function of T cells and alters the normal cycle of apoptotic cell death.TNF-α TNF-α is pleiotropic. TNF-α and IL-1 act alone or together to induce systemic
inflammation as above. TNF-α is also chemotactic for neutrophils and monocytes, as well as increasing neutrophil activity.
MIF MIF forms a crucial link between the immune and neuroendocrine systems. It acts systemically to enhance the secretion of IL-1 and TNF-α.
IL, interleukin; Ig, immunoglobulin; TNF, tumor necrosis factor; MIF, migration inhibitory factor.Table 55.5 Anti-inflammatory mediators
MediatorActionIL-4 IL-4, IL-3, IL-5, IL-13, and CSF2 form a cytokine gene cluster on chromosome 5q, with
this gene particularly close to IL-13.IL-10 IL-10 has pleiotropic effects in immunoregulation and inflammation. It down-regulates
the expression of TH1 cytokines, MHC class II antigens, and costimulatory molecules on
macrophages. It also enhances B-cell survival, proliferation, and antibody production. In addition, it can block NF-κB activity, and is involved in the regulation of the JAK-STAT signaling pathway.
IL-11 IL-11 stimulates the T-cell–dependent development of immunoglobulin-producing B cells. It is also found to support the proliferation of hematopoietic stem cells and megakaryocyte progenitor cells.
IL-13 IL-13 is involved in several stages of B-cell maturation and differentiation. It up-regulates CD23 and MHC class II expression, and promotes IgE isotype switching of B cells. It down-regulates macrophage activity, thereby inhibiting the production of proinflammatory cytokines and chemokines.
IFN-α IFN-α enhances and modifies the immune response.TGF-β TGF-β regulates the proliferation and differentiation of cells, wound healing, and
angiogenesis.α-MSH α-MSH modulates inflammation by way of three mechanisms: direct action on peripheral
inflammatory cells; actions on brain inflammatory cells to modulate local reactions; and indirect activation of descending neural anti-inflammatory pathways that control peripheral tissue inflammation.
IL, interleukin; CSF, colony-stimulating factor; TH, T helper; MHC, major histocompatibility
complex; Ig, immunoglobulin; IFN, interferon; TGF, transforming growth factor; MSH, melanocytestimulating hormone.T helper cells differentiate into either TH1 or TH2 lymphocytes. TH1 cells promote the
proinflammatory cascade through the release of IL-2, interferon-γ (IFN-γ), and TNF-β, while TH2
cells produce anti-inflammatory mediators (25,35). Monocytes/macrophages, through the release of IL-12, stimulate the differentiation of T-helper cells into TH1 cells (35). Because IL-12 production
is depressed following trauma, there is a shift toward TH2, which has been associated with an
adverse clinical outcome (25,35).Adherence of the leukocyte to endothelial cells is mediated through the up-regulation of adhesion molecules. Selectins such as leukocyte adhesion molecule-1 (LAM-1), endothelial leukocyte adhesion molecule-1 (ELAM-1), and P-selectin are responsible for polymorphonuclear leukocytes (PMNLs) “rolling” (25,37). Up-regulation of integrins such as the CD11/18 complexes or intercellular adhesion molecule-1 (ICAM-1) is responsible for PMNL attachment to the endothelium (25). Migration, accumulation, and activation of the PMNLs are mediated by chemoattractants such as chemokines and complement anaphylotoxins (25). Colony-stimulating factors (CSFs) likewise stimulate monocyte- or granulocytopoiesis and reduce apoptosis of PMNLs during SIRS. Neutrophil apoptosis is further reduced by other proinflammatory mediators, thus resulting in PMNL accumulation at the site of local tissue destruction (25).Leukocyte RecruitmentProinflammatory cytokines enhance PMNL recruitment, phagocytic activity, and the release of proteases and oxygen-free radicals by PMNLs. This recruitment of leukocytes represents a key element for host defense following trauma, although it allows for the development of secondary tissue damage (38,39,40,41). It involves a complex cascade of events culminating in transmigration of the leukocyte, whereby the cell exerts its effects (42). The first step is capture and tethering, mediated via constitutively expressed leukocyte selectin denoted L selectin. L selectin functions by identifying glycoprotein ligands on leukocytes and those up-regulated on cytokine-activated endothelium (42).Following capture and tethering, endothelial E selectin and P selectin assist in leukocyte rolling or slowing (37,43,44,45,46,47,48). P selectin is found in the membranes of endothelial storage granules (Weibel-Palade bodies) (45). Following granule secretion, P selectin binds to carbohydrates presented by P selectin glycoprotein ligand (PSGL-1) on the leukocytes (25). In contrast, E selectin is not stored, yet it is synthesized de novo in the presence of inflammatory cytokines (43,44). These selectins cause the leukocytes to roll along the activated endothelium, whereby secondary capturing of leukocytes occurs via homotypic interactions.The third step in leukocyte recruitment is firm adhesion, which is mediated by membrane-expressed β1- and β2-integrins (49,50,51). The integrins bind to ICAM, resulting in cell–cell interactions and
ultimately signal transduction. This step is critical to the formation of stable shear-resistant adhesion, which stabilizes the leukocyte for transmigration (49,50,51).Transmigration is the final step in leukocyte recruitment following the formation of bonds between the aforementioned integrins and immunoglobulin (Ig)-superfamily members (42). The arrested leukocytes cross the endothelial layer via bicellular and tricellular endothelial junctions in a process coined diapedesis (52). This is mediated by platelet-endothelial cell adhesion molecules (PECAMs), proteins expressed on both the leukocytes and intercellular junctions of endothelial cells (42).Proteases and Reactive Oxygen SpeciesPolymorphonuclear lymphocytes and macrophages are not only responsible for phagocytosis of micro-organisms and cellular debris, but can also cause secondary tissue and organ damage through degranulation and release of extracellular proteases and formation of reactive oxygen species or respiratory burst (25,39,40,41,53,54,55). Elastases and metalloproteinases, which degrade both structural and extracellular matrix proteins, are present in increased concentrations following trauma (25). Neutrophil elastases also induce the release of proinflammatory cytokines (25).
Reactive oxygen species are generated by membrane-associated nicotinamide adenine dinucleotide phosphate (NADPH)-oxidase, which is activated by proinflammatory cytokines, arachidonic acid metabolites, complement factors, and bacterial products (56,57). Superoxide anions are reduced in the Haber-Weiss reaction to hydrogen peroxide by superoxide dismutase located in the cytosol, mitochondria, and cell membrane (25). Hydrochloric acid is formed from H2O2 by
myeloperoxidase, while the Fenton reaction transforms H2O2 into hydroxyl ions (25). These free
reactive oxygen species cause lipid peroxidation, cell membrane disintegration, and DNA damage of endothelial and parenchymal cells (58,59,60). Oxygen radicals also induce PMNLs to release proteases and collagenase as well as inactivating protease inhibitors (61).Reactive nitrogen species cause additional tissue damage following trauma (62). Nitric oxide (NO) is generated from L-arginine by inducible nitric oxide synthase (iNOS) in PMNLs or vascular muscle cells and by endothelial nitric oxide synthase in endothelial cells (62). Nitric oxide induces vasodilatation (25). Inducible nitric oxide synthase is stimulated by cytokines and toxins, whereas endothelial nitric oxide synthase (eNOS) is stimulated by mechanical shearing forces (62,63). Damage by reactive oxygen and nitrogen species leads to generalized edema and the capillary leak syndrome (62).Complement, Kinins, and CoagulationThe complement cascade, kallikrein-kinin system, and coagulation cascade are intimately involved in the immune response to shock. They are activated through proinflammatory mediators, endogenous endotoxins, and tissue damage. The classic pathway of complement is normally activated by antigen–antibody complexes (Ig M or G) or activated coagulation P.818factor XII (FXII), while the alternative pathway is activated by bacterial products such as lipopolysaccharide (64,65,66). Complement activation following trauma is most likely from the release of proteolytic enzymes, disruption of the endothelial lining, and tissue ischemia. The degree of complement activation correlates with the severity of injury. The cleavage of C3 and C5 by their respective convertases results in the formation of opsonins, anaphylotoxins, and the membrane attack complex (MAC) (64,65,66). The opsonins C3b and C4b enhance phagocytosis of cell debris and bacteria by means of opsonization (64,65). The anaphylotoxins C3a and C5a support inflammation via the recruitment and activation of phagocytic cells (i.e., monocytes, polymorphonuclear cells, and macrophages), enhancement of the hepatic acute phase reaction, and release of vasoactive mediators (i.e., histamine) (52,65). They also enhance the adhesion of leukocytes to endothelial cells, which results in increased vascular permeability and edema. C5a induces apoptosis and cell lysis through the interaction of its receptor and the MAC (52,65,66). Additionally, C3a and C5a activate reparative mechanisms (65). C1 inhibitor inactivates C1s and C1r, thereby regulating the classic complement pathway. However, during inflammation, serum levels of C1 inhibitor are decreased via its degradation by PMNL elastases (65).The plasma kallikrein-kinin system is a contact system of plasma proteases related to the complement and coagulation cascades. It consists of the plasma proteins FXII, prekallikrein, kininogen, and factor XI (FXI) (67). The activation of FXII and prekallikrein is via contact activation when endothelial damage occurs exposing the basement membrane (67). Factor XII activation forms factor XIIa (FXIIa), which initiates the complement cascade through the classic pathway, whereas prekallikrein activation forms kallikrein, which stimulates fibrinolysis through the conversion of plasminogen to plasmin or the activation of urokinaselike plasminogen activator (uPA) (67). Tissue plasminogen activator (tPA) functions as a cofactor. Additionally, kallikrein supports the conversion of kininogen to bradykinin (67). The formation of bradykinin also occurs through the activation of the tissue kallikrein-kinin system, most likely through organ damage as the tissue kallikrein-kinin system is found in many organs and tissues including the pancreas, kidney, intestine, and salivary glands. The kinins are potent vasodilators. They also increase vascular permeability and inhibit the function of platelets (67).The intrinsic coagulation cascade is linked to the contact activation system via the formation of factor IXa (FIXa) from factor XIa (FXIa). Its formation leads to the consumption of FXII,

prekallikrein, and FXI while plasma levels of enzyme–inhibitor complexes are increased (25). These include FXIIa-C1 inhibitor and kallikrein-C1 inhibitor. C1 inhibitor and α1-protease inhibitor are both inhibitors of the intrinsic coagulation pathway (68,69).Although the intrinsic pathway provides a stimulus for activation of the coagulation cascade, the major activation following trauma is via the extrinsic pathway. Increased expression of tissue factor (TF) on endothelial cells and monocytes is induced by the proinflammatory cytokines TNF-α and IL-1β (69,70,71). The factor VII (FVII)–TF complex stimulates the formation of factor Xa (FXa) and ultimately thrombin (FIIa) (25). Thrombin-activated factor V (FV), factor VIII (FVIII), and FXI result in enhanced thrombin formation (25). Following cleavage of fibrinogen by thrombin, the fibrin monomers polymerize to form stable fibrin clots. The consumption of coagulation factors is controlled by the hepatocytic formation of antithrombin (AT) III (25). The thrombin–antithrombin complex inhibits thrombin, FIXa, FXa, FXIa, and FXIIa (72). Other inhibitors include TF pathway inhibitor (TFPI) and activated protein C in combination with free protein S (72). Free protein S is decreased during inflammation due to its binding with the C4b binding protein (68,72).Disseminated intravascular coagulation (DIC) may occur following shock. After the initial phase, intra- and extravascular fibrin clots are observed. Hypoxia-induced cellular damage is the ultimate result of intravascular fibrin clots. Likewise, there is an increase in the interactions between endothelial cells and leukocytes (68,69,70,73). Clinically, coagulation factor consumption and platelet dysfunction are responsible for the diffuse hemorrhage (68,71). Consumption of coagulation factors is further enhanced via the proteolysis of fibrin clots to fibrin fragments (68,71). The consumption of coagulation factors is further enhanced through the proteolysis of fibrin clots to fibrin fragments by the protease plasmin (25,69,74).Acute Phase ReactionThe acute phase reaction describes the early systemic response following shock and other insult states. During this phase, the biosynthetic profile of the liver is significantly altered. Under normal circumstances, the liver synthesizes a range of plasma proteins at steady-state concentrations. However, during the acute phase reaction, hepatocytes increase the synthesis of positive acute phase proteins (i.e., C-reactive protein [CRP], serum amyloid A [SAA], complement proteins, coagulation proteins, proteinase inhibitors, metal-binding proteins, and other proteins) essential to the inflammatory process at the expense of the negative acute phase proteins. The list of acute phase proteins is in Table 55.6 (75,76).The acute phase response is initiated by hepatic Kupffer cells and the systemic release of proinflammatory cytokines (76). IL-1, IL-6, IL-8, and TNF-α act as inciting cytokines (77,78). The acute phase reaction typically lasts for 24 to 48 hours prior to its down-regulation (35). IL-4, IL-10, glucocorticoids, and various other hormonal stimuli function to down-regulate the proinflammatory mediators of the acute phase response (35). This modulation is critical. In instances of chronic or recurring inflammation, an aberrant acute phase response may result in exacerbated tissue damage (35).The major acute phase proteins include CRP and SAA, the activities of which are both poorly understood (79,80). C-reactive protein was so named secondary to its ability to bind the C-polysaccharide of Pneumococcus. During inflammation, CRP levels may increase by up to 1,000-fold over several hours depending on the insult and its severity (35). It acts as an opsonin for bacteria, parasites, and immune complexes; activates complement via the classic pathway; and binds chromatin (35). Binding chromatin may minimize autoimmune responses by disposing of nuclear antigens from sites of tissue debris (35). Clinically, CRP levels are relatively nonspecific and not predictive of posttraumatic complications. Despite this fact, serial measurements are helpful in trending a patient's clinical course (35).Serum amyloid A interacts with the third fraction of high-density lipoprotein (HDL3), thus becoming the dominant P.819apolipoprotein during acute inflammation (81). This association enhances the binding of HDL3 to macrophages, which may engulf cholesterol and lipid debris. Excess cholesterol is then utilized in
tissue repair or excreted (35). Additionally, SAA inhibits thrombin-induced platelet activation and the oxidative burst of neutrophils, potentially preventing oxidative tissue destruction (35).
Table 55.6 Acute phase proteinsGroup Individual proteinsPOSITIVE ACUTE PHASE PROTEINS
Major acute phase proteins
C-reactive protein, serum amyloid A
Complement proteins C2, C3, C4, C5, C9, B, C1 inhibitor, C4 binding proteinCoagulation proteins Fibrinogen, prothrombin, von Willebrand factorProteinase proteins α1-Antitrypsin, α1-antichymotrypsin, α2-antiplasmin, heparin cofactor II,
plasminogen activator inhibitor IMetal-binding proteins
Haptoglobin, hemopexin, ceruloplasmin, manganese superoxide dismutase
Other proteins α1-Acid glycoprotein, heme oxygenase, mannose-binding protein, leukocyte
protein I, lipoprotein (a), lipopolysaccharide-binding proteinNEGATIVE ACUTE PHASE PROTEINS
Albumin, prealbumin, transferrin, apolipoprotein AI, apolipoprotein AII, α2-
Heremans-Schmid glycoprotein, inter-α-trypsin inhibitor, histidine-rich glycoprotein, protein C, protein S, antithrombin III, high-density lipoprotein
Positive acute phase proteins increase production during an acute phase response. Negative acute phase proteins are those that have decreased production during an acute phase response.Diagnosis of ShockEarly diagnosis of shock affords the patient the best possible outcome. The patient in overt shock with hypotension and tachycardia is relatively easy to diagnose. However, more often than not, shock presents in more insidious forms, whereby underrecognition and delay in treatment can lead to a poor outcome. Moreover, the concurrent presence of mixed shock states can confuse the picture. Diagnosis of shock relies on both basic history and physical examination skills, as well as more advanced technology available to the clinician.Numerous clues in a patient's history may help alert the physician to the possibility of impending shock. Large fluid losses via traumatic or gastrointestinal hemorrhage, third spacing from intra-abdominal surgery or pancreatitis, prolonged dehydration from vomiting or diarrhea, or insensible losses from burns may very easily tip the patient into hypovolemic shock. A history of infection, presence of indwelling catheters, or recent surgery may be implicated in septic shock. Neurogenic shock occurs almost exclusively after trauma, although limited forms are seen with spinal anesthesia. History of prolonged steroid use, particularly in the elderly, may indicate adrenal shock in the patient with hypotension postoperatively. Exposures to drugs, transfusions, or other allergens should be sought to rule out anaphylactic shock. Recent myocardial infarction or cardiac intervention can lead to pump failure and cardiogenic shock. A detailed history is especially important for obstructive forms of shock, in which any intervention involving the chest can lead to either immediate or delayed compromise via cardiac tamponade or tension pneumothorax. Likewise, a history of deep venous thrombosis (DVT) or risk factors for thrombosis should alert the physician to the possibility of acute massive pulmonary embolism in the hypotensive patient.Physical examination can provide more clues than just basic blood pressure measurements. As noted previously, hypotension alone is neither exclusive to shock nor absolute for a diagnosis, and therefore is only a small component of the physical examination. Certain findings may vary based on the type and timing of shock. The end result of any form of shock, however, is diminished end-organ perfusion. Therefore, any signs or symptoms of organ dysfunction should be considered as possible indicators of shock (Table 55.7). Often, the first sign of shock manifests as mental status changes, whether excitatory or somnolent in nature. The patient may appear diaphoretic and clammy in cardiogenic shock or warm and dry in early distributive shock. Heart rate may also be variable, with tachycardia compensating for diminished cardiac output in the patient with intact
sympathetic drive. Vasoplegic shock such as neurogenic or adrenal (or in the β-blocked patient) may not have the compensatory increase in heart rate normally seen, and may itself provide a clue as to the type of shock. Tachypnea is almost universally seen, as the body tries to buffer the lactate produced in a state of tissue hypoxia. The kidneys provide a sensitive measure of adequate end-organ perfusion, as manifested by low urinary output. Cardiogenic shock has its own specific physical findings including increased venous jugular distension, acute pulmonary edema, and new murmurs or arrhythmias.
Table 55.7 Clinical recognition of shockOrgan system Symptoms or signs CausesCNS Mental status changes ↓ Cerebral perfusionCirculatory Cardiac Systemic
TachycardiaOther dysrhythmiasHypotensionNew murmursHypotension↓ JVPs↑ JVPsDisparate peripheral pulses
Adrenergic stimulation, depressed contractilityCoronary ischemiaDepressed contractility secondary to ischemia or MDFs, right ventricular failureValvular dysfunction, VSD↓ SVR, ↓ venous returnHypovolemia, ↓ venous returnRight heart failureAortic dissection
Respiratory TachypneaCyanosis
Pulmonary edema, respiratory muscle fatigue, sepsis, acidosisHypoxemia
Renal Oliguria ↓ Perfusion, afferent arteriolar vasoconstrictionSkin Cool, clammy Vasoconstriction, sympathetic stimulationOther Lactic acidosis
FeverAnaerobic metabolism, hepatic dysfunctionInfection
CNS, central nervous system; MDFs, myocardial depressant factors; VSD, ventricular septal defect; SVR, systemic vascular resistance; JVPs, jugular venous pulsations.From Jimenez EJ. Shock. In: Civetta JM, Taylor RW, Kirby RR, eds. Critical Care. 3rd ed. Philadelphia: Lippincott–Raven Publishers; 1997:359.P.820Various modalities for evaluating shock may be used either alone or in combination. Pooling data from multiple sources, however, is often required to get an adequate picture of shock resuscitation. Basic laboratory studies such as lactate level, base deficit, hemoglobin, creatinine, and cortisol may help provide evidence of or reason for shock. Likewise, a more advanced evaluation of shock may include echocardiogram, central venous pressure monitoring, tissue oxygenation and capnography, or advanced methods of determining cardiac output. Advantages and disadvantages of these more advanced modalities will be discussed later within the context of shock monitoring.Management of ShockOptimal management of shock depends first and foremost on early recognition of the syndrome and correct determination of its etiology. Ongoing assessment of interventions is likewise paramount, as adjustments can be made in type and degree of specific therapies. The underlying goal of shock management is to improve tissue oxygen perfusion. This may be accomplished by manipulating one or multiple physiologic parameters involved in oxygen delivery and extraction.Forms of obstructive shock require the most prompt diagnosis, as continued mechanical impairment can be rapidly fatal. Conversely, adequate treatment of these etiologies can be just as rapid. Performing needle decompression for a tension pneumothorax or pericardiocentesis for cardiac tamponade can be all that is required for these forms of shock. Pharmacologic and fluid support can be used as an adjunct while relief of mechanical obstruction is ongoing.Management of distributive and hypovolemic forms of shock likewise involves attempted source control early in the diagnosis. This may be in the form of hemorrhage control, removal of infected tissue, or avoidance of sources of anaphylaxis. Once the inflammatory cascade has set in,
vasoactive medications are often used in addition to fluid provision to increase perfusion.Treatment of cardiogenic shock in particular warrants keen understanding of the physiologic process. Currently, initial therapy of cardiogenic shock consists of volume optimization, control of arrhythmias, use of the intra-aortic balloon pump, addition of vasopressors, and early revascularization in primary myocardial ischemia, with addition of inotropes only when these measures fail (82).Classically, all forms of shock are treated in some capacity with a combination of fluids and vasoactive agents. Deliberation is ongoing regarding the dosing and selection of these modalities for resuscitation, and will be examined in greater detail.Fluid ResuscitationThe initial treatment for all forms of shock is fluid administration. Provision of fluid helps restore perfusion and replace volume lost via hemorrhage, capillary leak, or redistribution. Historically, Blalock demonstrated reversal of shock state induced by tissue injury by using vigorous resuscitation of intravascular volume (83). As such, the use of fluids for shock management has become a cornerstone of therapy. Intravenous fluid is readily available, inexpensive, and easy to administer, P.821and has low intrinsic morbidity. The etiology of shock and response to fluid will further dictate continued use of volume as primary therapy; however, all forms of shock potentially benefit from an initial fluid challenge (84). There are endless means of administering fluid given a particular clinical setting. General guidelines can be followed; however, considerable debate exists regarding the nuances of this most basic therapy. Deliberation should be given to the method of delivery, timing of administration, type of fluid, and volume of administration. Complications of fluid resuscitation, as well as emerging research in this area, should also be considered.Route of AdministrationThe setting of shock dictates administration of fluid primarily via the intravenous route. Factors such as endotracheal intubation, mental status, adynamic or mechanical ileus, rapidity of response, and questionable absorption from the gastrointestinal tract preclude the enteric route as a primary vessel for fluid resuscitation in most cases. Intravenous access may be in the form of a peripheral or central venous catheter. Although the type of shock may guide the choice of catheter (i.e., an introducer catheter for a rapid infusion system or anticipated pulmonary artery catheter placement in cardiogenic shock, or a triple lumen for anticipated vasopressor therapy), the dictum of “two large-bore peripheral IVs” cannot be overstated (85). As per Poiseuille's Law, width and length of the catheter dictates flow; therefore, a long, narrow, peripherally inserted central catheter will be of little utility when infusing a large bolus of fluid quickly. In the severely volume depleted patient with collapsed veins, obtaining percutaneous venous access can prove difficult. Saphenous vein cut-downs or interosseus access, particularly in the trauma patient, can provide means of fluid administration until more permanent intravenous access can be obtained.Timing of AdministrationAs stated previously, fluid is the initial therapy in all forms of shock. For forms of hypovolemic shock in particular, the concept of early restoration of intravascular volume to prevent circulatory collapse has long been recognized. In the hemorrhagic patient, aggressive volume resuscitation combined with source control may limit or prevent a state of irreversible shock, or the more currently described “lethal triad” of hypothermia, coagulopathy, and acidosis (86,87). The importance of the timing of volume loading is also being recognized in other forms of shock, particularly in sepsis (88). Amplification of the previously described immune response can potentially be avoided if perfusion is restored early in the pathophysiologic process (89). Often the resuscitation process begins in the prehospital phase, with ambulance personnel administering combinations of crystalloid and colloids en route. In this setting, timing of fluid resuscitation is given due attention. Delayed aggressive fluid resuscitation once the patient is already in the intensive care unit, and therefore later in the course of shock, as well as excessive doses of dobutamine (5–200 µg/kg/minute) can be detrimental (90).
Continued administration of fluid alone, however, should be based on the patient's underlying pathology. While vigorous fluid provision may be life sustaining in certain patients, an equal measure could prove counterproductive in others. Ongoing replacement of fluid should be based on both direct and insensible losses, keeping in mind the huge potential third-spacing loss into the interstitium. Again, the idea of pushing fluid beyond the initial phases of ischemia may propagate reperfusion injury, emphasizing early recognition and treatment of shock.Volume of ResuscitationAlthough there is general consensus regarding the timing of administration of fluids, there is little information to support the optimum volume to be given. Guidelines reference various quantities for crystalloid administration, including 500 mL, 1,000 mL, or the more universal 20 mL/kg bolus. The speed of the bolus likewise varies, although common sense dictates that rapid administration is preferred in the setting of hypotension.Continued fluid administration beyond an initial bolus relies more on patient response than on arbitrary numbers. Physical examination characteristics such as jugular venous distension, skin turgor, and basic vital signs may give clues to volume state, but are notoriously subject to interpretation. The examiner is often misled by the appearance of gross edema, insomuch that it has no bearing on effective extracellular fluid volume in the patient with capillary leak. Efforts to measure intravascular volume status should be made, but these values should be interpreted in the context of cardiac output and ongoing therapy. Tools used to measure volume status include central venous pressure, pulmonary artery occlusion pressure, esophageal Doppler, and echocardiography, each with its own strengths and weaknesses (91,92,93,94). There is renewed interest in the actual measurement of blood volume rather than relying on surrogate markers (see Blood Volume chapter).The amount of fluid required to achieve these goals will vary with patient size, cardiac status, type of fluid given, and timing and type of shock. Prominent guidelines direct the clinician to volume load to a central venous pressure of 8 to 10 mm Hg or a pulmonary capillary wedge pressure of >12 mm Hg prior to initiating vasopressor therapy for shock (95,96). Ideal volumes for shock resuscitation continue to be debated. In fact, restrictive fluid therapies for resuscitation have emerged in an effort to reduce the cardiac, wound healing, and pulmonary complications associated with large crystalloid infusions (97).Fluid therapy in excess may lead to numerous complications. The coagulation profile may be altered secondary to dilution with excessive crystalloid infusion (98). Red blood cell mass is also diluted, and while this may not have a net effect on oxygen delivery, it may complicate interpretation of bleeding states. Tissue edema is also a consequence of volume resuscitation, and of these, the pulmonary component is most visible to the practitioner. Lung edema will manifest most readily with crystalloid therapy in the setting of hypoproteinemia—a common state in the shock patient (99). While some degree of pulmonary edema can be tolerated, critical hypoxia often threatens the recovery of patients who survive via massive volume resuscitation. The added mechanical impairment of ventilation induced by abdominal compartment syndrome, also seen with large volume resuscitation, further exacerbates the situation (100).Types of FluidConsiderable debate abounds regarding the types of fluid to be administered for shock resuscitation. The physiologic makeup of the human body allows for movement of fluids and solutes across compartments, specifically between the interstitium and intravascular space. Hydrostatic and oncotic forces dictate this P.822movement at the capillary level, as explained by the Starling equation:Jv = Kf{(Pc - Pi) - σ(πc - πi)}
where Jv is the net fluid flux (mL/minute). (Pc - Pi) is hydrostatic pressure difference between
capillary (c) and interstitium (i), and (πc - πi) is the oncotic pressure difference between the capillary
and interstitium, Kf is the filtration coefficient for that membrane (mL/minute per mm Hg), and is
the product of capillary surface area and capillary hydraulic conductance. σ is the permeability factor (i.e. reflection coefficient) with one being impermeable, and zero being completely permeable. Imbalance in the forces—whether decreased oncotic pressure from hypoalbuminemia, increased hydrostatic pressure from heart failure, or decreased protein reflection coefficient with sepsis—occurs often with shock states. The choice of fluid type therefore requires appropriate knowledge of the characteristics of the fluid, as well as the pathophysiology of the shock state.CrystalloidsInvariably, the workhorse of shock resuscitation is isotonic crystalloid. Composed of varying amounts of electrolytes and sugar, crystalloids are inexpensive, require no special tubing or preparation, and pose little to no allergy or transfusion risk. Almost every patient receives some form of intravenous crystalloid upon entering a hospital with little consequence as to the type given due to the low volumes given on average.Crystalloids used in shock resuscitation are generally categorized as isotonic or hypertonic, describing the in vivo tonicity of the fluid. Typical isotonic crystalloids used are normal saline, lactated Ringer solution, or other commercially available combinations of electrolytes with sodium as the primary ion. Lacking protein components, the isotonic crystalloids readily distribute to the extracellular fluid compartment and will require larger volumes of infusion to maintain intravascular filling. Traditional philosophy dictates that a threefold volume of crystalloid to colloid is required for intravascular expansion. This ratio has recently been debated, however, and may actually be closer to a ratio of 1.5:1 when comparing crystalloid to 5% albumin (101).Normal saline and lactated Ringer solution compromise the majority of isotonic crystalloid used for shock. Normal saline simply provides sodium with an equal amount of chloride for buffer. Hypernatremia and hyperchloremic metabolic acidosis are therefore potential consequences of continued normal saline administration (102). While the tonicity is essentially the same, the electrolyte composition of lactated Ringer is considered more physiologic, with inclusion of potassium and calcium, and reduction in chloride concentrations. Conversion of the lactate in lactated Ringer to bicarbonate in theory provides a buffer to metabolic acidosis in the patient with adequate liver function. Current compositions of lactated Ringer contain a racemic mixture of D- and L-lactate in solution. The presence of this D-isomer has been implicated as a potentiator of neutrophil activation in large volume infusions (103). Likewise, the presence of a large lactate load has been implicated in promoting respiratory acidosis in the spontaneously breathing patient (104).Hypertonic CrystalloidCombining the convenience of crystalloid with the tonicity of colloids, hypertonic saline has emerged as an important tool in shock resuscitation. Hypertonicity of the sodium concentration promotes influx of fluid from the interstitial space. As such, hypertonic saline is advantageous for rapid, low-volume resuscitation for hypovolemic shock, particularly in situations where resources may be scarce. Hypertonic solutions also favorably impact immune modulatory function. Studies particularly investigating hemorrhagic shock have found a decrease in neutrophil activation, and up-regulation of anti-inflammatory cytokine production with use of hypertonic saline (105,106).While relatively safe compared to colloid infusion, the administration of high concentrations of sodium for volume resuscitation carries the concern for hypernatremia and hyperosmolarity. The neurologic consequences of rapid sodium flux are well known; however, these have not been described in the hypertonic saline resuscitation population. Compromise of renal function is likewise feared with high sodium and osmolar loads. While some patient populations exhibit increases in creatinine without clinical renal dysfunction, studies in the burn population support this trepidation regarding hypertonic saline (107,108). Reports of hypokalemia, metabolic acidosis, and impaired platelet aggregation have also been documented with hypertonic saline use (109).ColloidsPertaining to volume resuscitation, colloids generally consist of fluids that have a higher molecular weight based on composition consisting of protein, starches, or cells. These components increase the cost of colloids, make them susceptible to shortage, and mandate specialized tubing for delivery. Possibility for transfusion reaction is increased as some of these compounds are derived from blood
products. Likewise, allergic reactions can be noted with some of the synthetic formulations.Conceptually, colloids more rapidly expand intravascular volume owing to their higher oncotic pressure. This effect may not necessarily persist beyond a few hours, especially in the critically ill patient in which capillary permeability is altered (110). In addition to more rapid volume expansion with less fluid infusion, this same increase in intravascular oncotic pressure has prompted the employment of colloids with the intent to reduce or prevent secondary edema. This mechanism does not hold in critical illness, particularly for lung edema in which dysfunction is unrelated to capillary oncotic pressure in shock (111).Despite these findings, colloids are an important component of shock resuscitation. Integration of colloids into most protocols usually follows initial infusion of crystalloids or while awaiting blood product transfusion (112).AlbuminFirst used for fluid resuscitation during World War II, albumin is a colloid derived from pooled human plasma and diluted with sodium. Preparations consist of 5% or 25% solution in quantities of 250 to 500 mL or 50 mL, respectively. As a blood product derivative, albumin is subject to disadvantages faced by other donated products—namely periodic shortages, high acquisition costs, and refusal based on religious grounds. While transmission of viruses or other blood-borne diseases is theoretically a risk, only a few cases have been reported. Like any resuscitation fluid, patients are subject to sequelae of volume overload if infusion amounts are not monitored.While indications for albumin use are broad, proven benefit to particular therapies is increasingly narrow. Numerous studies detailing poor prognosis with low serum albumin levels in critically ill patients prompted attempts to improve survival with intravenous supplementation (113,114,115). Compared with P.823other colloid administration, albumin itself has no benefit in this patient population (116,117).Albumin as a resuscitation fluid likewise has come under scrutiny. Previously, studies investigating albumin as a volume expander have been underpowered, prompting meta-analysis as the primary statistical measure of its worth. An initial Cochrane review comparing albumin to crystalloid examined 24 studies and found a 6% increase in absolute risk of death with albumin infusion (118). To confuse matters, subsequent meta-analysis of 55 studies bore out no difference in mortality between albumin and crystalloid for resuscitation (119). In 2004, the Saline versus Albumin Fluid Evaluation (SAFE) trial prospectively compared albumin to isotonic crystalloid for fluid resuscitation in a mixed intensive care unit population (101). Results showed no difference in morbidity or mortality overall with albumin use. Advocates for albumin hail this study as an indicator that its use poses no harm as previously indicated. Opponents likewise cite the study, but as an indicator that there is no advantage to using albumin for volume resuscitation. A revised Cochrane analysis following the SAFE study again reported no advantage to albumin infusion for hypovolemic patients (120). Results must be interpreted in light of the heavy weight thus given to the SAFE trial in this review.StarchesIn an attempt to retain the oncotic properties of albumin while decreasing cost and transfusion risk, synthetic colloid polymers have been developed for use in volume resuscitation. As one of the primary synthetic colloids, starches, of which hydroxyethyl starch is most popular, consist of polymers of amylopectin. Like other colloids, hydroxyethyl starch owes its main advantage to providing appropriate volume expansion with less infusion than that of crystalloids. Initial formulations of hydroxyl ethyl starch (HES) included high-molecular-weight moieties, accounting for an increased risk of coagulation and renal disturbances associated with their use (121,122,123). Lower-molecular-weight HES solutions have since been developed, with resultant fewer negative effects on bleeding (124).Of particular interest in colloid resuscitation, hydroxyethyl starch has favorable effects both on vascular permeability and inflammatory properties in animal models. Reduced pulmonary capillary leakage has been described with hydroxyethyl starch use in comparison to crystalloid and gelatin

resuscitation (125,126). While numerous studies have illustrated down-regulation of proinflammatory cytokines with hydroxyethyl starch use, some of these results may be an effect of the efficiency of volume resuscitation, and not necessarily the fluid itself (127,128,129). How this anti-inflammatory effect is translated into clinical outcomes is the subject of ongoing research.DextranAmong the lower-molecular-weight colloids, dextran consists of large glucose polymers of varying sizes. As a colloid, it does expand intravascular volume; however, the smaller-sized molecules redistribute quickly, giving it a short half-life. It improves microcirculation by decreasing blood viscosity and therefore primarily is used in situations where platelet adherence and red blood cell aggregation is discouraged, such as postcarotid endarterectomy. As such, the risk of bleeding limits their use as a primary resuscitation fluid. The combination of dextran with other fluids, most notably hypertonic saline, limits the adverse effects of dextran alone. Conceptually, the combination of the two would increase the amount and duration of oncotic pressure in the intravascular space compared with either alone. In animal models, the use of hypertonic saline plus dextran-70 is associated with improved hypovolemic resuscitation when compared to hypertonic saline alone. This effect has not translated well into human clinical studies, in which the combination shows no benefit over hypertonic saline alone in prehospital resuscitation (130,131). The administration of dextran plus hypertonic saline is considered safe, however, resulting in fewer complications than crystalloid in trauma resuscitation (132). Additional studies are needed to establish appropriate use of dextrans as they apply to shock resuscitation.GelatinsGelatins consist of moderate-size molecular weight colloids derived from porcine sources. A perceived high level of antigenicity limits their use, particularly in the United States where they are not Food and Drug Administration (FDA) approved. The absolute incidence of anaphylaxis, however, is only 0.066% (133). Modified fluid gelatin is the most common colloid used worldwide, owing to its otherwise favorable side effect profile and inexpensive production costs. In comparison to crystalloids for shock resuscitation, gelatins provide superior volume expansion without additionally noted adverse effects of bleeding or pulmonary dysfunction (134,135,136). As gelatins gain approval throughout worldwide markets, further research is emerging to investigate their utility in shock resuscitation.Blood ProductsProvision of blood products as either a primary or adjunctive resuscitation fluid should be considered carefully. The risk of infection, immunosuppression, and transfusion reaction are well known (137,138). The cost of preparation, as well as short supply, also limits their use.Blood products do provide an effective source of colloid for increasing oncotic pressure, but should only be used when secondary properties of the specific product are sought. Transfusing packed red blood cells, while increasing oxygen-carrying capacity, does not necessarily translate into improved survival in all situations. Targeting a specific hemoglobin concentration in critically ill patients may only benefit those with active coronary artery disease; otherwise, a restrictive transfusion policy to a hemoglobin level of 7.0 g/dL is safe (139). Specifically, in septic shock, the administration of red blood cells may benefit a subset of patients who have a low mixed venous oxygenation and low hemoglobin level after volume resuscitation with crystalloids (88). Measurement of red cell volume may be a better guide to blood transfusion rather than hemoglobin or hematocrit since the hemoglobin/hematocrit reflect red cell volume in relationship to plasma volume.Fresh frozen plasma, cryoprecipitate, and platelets also have utility as colloids based on the coagulation profile. Each has the same adverse transfusion profile as administering red blood cells, however, and should only be used in combination with packed red blood cells for hemorrhagic shock, or in the setting of the coagulopathic patient requiring fluid resuscitation. Standard teaching of administering 1 unit of plasma for every 3 units of red blood cells has recently been challenged. More advanced hemorrhagic shock resuscitation requires a one-to-one ratio of plasma to red blood cell administration, with addition of platelets and cryoprecipitate based on laboratory evaluation (140).
Fluid Choices for Different Classifications of ShockDebate abounds regarding appropriate use of crystalloids versus colloids in various shock states as illustrated by the P.824numerous meta-analyses found in the literature. Differences in mortality are illustrated when subgroup analysis is performed; therefore, fluids for shock resuscitation can be examined based on underlying pathophysiology of the shock state. The two most studied categories are trauma-induced hemorrhagic shock and septic shock.Hemorrhagic Shock ResuscitationCurrent guidelines for hemorrhagic shock emphasize mixed crystalloid and colloid provision until blood products (either type specific or O negative) are available. Aggressive use of crystalloids during the Vietnam conflict resulted in improved mortality and reduction in renal failure, but also led to the emergence of acute lung injury and acute respiratory distress syndrome in the trauma population. Extensive use of crystalloids for trauma followed, with the popular concept of pushing fluids beyond supranormal resuscitation goals (141). Meta-analyses at the time provided further encouragement for this practice, with mortality favoring crystalloids over colloids in the trauma population (142). The advancement of damage control surgery led to improved outcomes while compensating for the accepted postoperative edema by leaving the abdomen open. Consequences of this large-volume approach are becoming more evident, with adverse cardiac, pulmonary, coagulation, and immunologic effects documented with massive crystalloid infusion (143).The advent of synthetic colloids, as well as further research regarding hypertonic saline use, renewed interest in the concept of small-volume resuscitation, particularly on the battlefield. Hypertonic saline, dextran, and hydroxyethyl starch have the advantages of long shelf life, convenient preparation, and small aliquot volumes for equal resuscitation. This is particularly important in combat situations, where low-bolus 7.5% hypertonic saline is now the standard for initial resuscitation (144). Current battlefield practice has translated to civilian trauma, with the use of these compounds in the prehospital setting (132).Hypotensive resuscitation in the hemorrhagic patient is an additional emerging concept. This strategy may be applied to the patient in whom mechanical control of bleeding has not been achieved—whether in traumatic injury, aortic aneurysm rupture, or gastrointestinal bleed (145,146,147). Measures to raise blood pressure, particularly with fluid administration, may be counterproductive. In the penetrating thoracic trauma patient, early administration of large volumes of crystalloid has been shown to increase bleeding and subsequent mortality (148). This is a very specific patient population, however, and further examination of fluid administration by a recent Cochrane review provided insufficient evidence for or against the use of early, large-volume resuscitation in hemorrhagic shock (149).Septic Shock ResuscitationResuscitation for septic shock is currently a highly investigated topic, with numerous guidelines and protocols taking the forefront in hospital initiatives. While a large number of investigations seek the optimal pharmacologic therapy, fluid management is still a source of debate. The inflammatory process and resulting capillary leak inherent to sepsis creates an additional variable when considering which fluids to administer. The logical choice would therefore be a colloid with the idea of maintaining higher intravascular oncotic pressure. When comparing filling pressures and oxygen delivery, however, there is no appreciable difference between colloids and crystalloids, except in amount of fluid required. Despite delivering two to three times more fluid with crystalloid, patient outcomes are the same (150). With the exception of small subgroup analyses indicating a trend toward improved outcome with albumin resuscitation (SAFE), there are insufficient data to definitively support colloids over crystalloids for septic shock resuscitation. As such, large practice guidelines such as the Surviving Sepsis Campaign either incorporate a combination of fluids or simply leave this choice to the practitioner (95).Pharmacotherapy in Shock
When incorporating pharmacotherapy for treatment of shock, catecholamines classically come to mind. Sympathomimetics are still the standard for raising the mean arterial pressure (MAP) in the hypotensive patient who is not responding to fluids. Shock is not hypotension alone, however, and other agents can be used to compensate for the diminished tissue perfusion defined by this syndrome. Drugs used for shock will be examined here by the classifications of vasopressor, inotrope, and miscellaneous, although these categories may overlap to a degree. An overview of the more common sympathomimetics is listed in Table 55.8.VasopressorsEnd-organ arterial autoregulation generally compensates for decreased MAP within a certain range. Local vasoconstriction and vasodilatation may be unable to overcome extremes of perfusion. Administering vasopressors may help improve MAP and therefore improve tissue perfusion by redistributing cardiac output. The venous compartment also benefits from vasopressor therapy by decreasing compliance and therefore improving effective volume.Vasopressors are generally given after an initial fluid bolus has failed or had marginal effect. Within the context of avoiding the consequences of excessive fluid administration, vasopressors may help limit volumes of fluid given; however, peripheral and end-organ vasoconstriction have their own adverse effects. Striking the balance between volume and pressors in the context of timing and type of shock is therefore a key component to resuscitation. With early recognition of shock, vasopressors can often be avoided by restoration of volume.Classifications of vasopressors consist of natural and synthetic versions of catecholamines (Table 55.8). Each pressor has its own advantage and disadvantage, although practitioners generally use only a few common agents in their armamentarium. The limited number of randomized controlled trials for in vivo use of pressors makes selection often one of familiarity, availability, and current trends (151). Often, surrogate end points serve as the basis for judging responsiveness to a drug agent, a strategy that may or may not manifest in improved patient outcome. There are some general recommendations, however, for certain drug regimens in particular types of shock.NorepinephrineA naturally occurring vasopressor, norepinephrine is released by the postganglionic adrenergic nerves in response to stress. It has potent α-adrenergic effects, with less potent β1 stimulation. The
α-adrenergic effects lead to increased systolic and diastolic pressure, with the addition of increased venous return via decreasing venous capacitance. This subsequently leads to increased cardiac filling pressure. Effect P.825on the coronary arterial flow is enhanced via the increase in diastolic blood pressure. The β-adrenergic effects lead to increased chronotropic function, although this is limited by the baroreflex of vasoconstriction, resulting in zero net change in heart rate. Enhanced inotrope stimulation and stroke volume are likewise negated by an increase in left ventricular afterload, leading to a limited increase in cardiac output.
Table 55.8 Sympathomimetic drugs
Adrenergic
effects
Drug Usual IV dose α β DopaArrhythmogenic potential Setting
Dopamine 1–2 µg/kg/mina
2–10 µg/kg/min10–30 µg/kg/min
1+2+3+
1+2+2+
3+3+3+
1+2+3+
Oliguria despite “normal” blood pressureInitial emergency treatment of hypotension (any cause)Alternative treatment for bradycardia
Dobutamine 2–30 µg/kg/min
1+ 3+ 0 2+ Cardiac shockPulmonary edema with marginal blood pressure
Norepinephrine0.5–80 µg/min 3+ 2+ 0 2+ Initial emergency treatment of hypotension (any cause, especially sepsis)
Epinephrine 0.5–1 mgb (1:10,000)1–200 µg/min0.3–0.5 mg SQ (1:1,000)c
1+2+
2+3+
00
3+3+
Cardiac arrestSevere hypotension and bradycardiaAnaphylaxis
Phenylephrine 20–200 µg/min
3+ 0 0 0 Distributive shock when no cardiac effect is desired
Isoproterenol 2–10 µg/min 0 3+ 0 3+ Refractory bradycardiaDenervated hearts
Milrinoned Load: 50 µg/kg over 10 minThen: 0.375–0.75 µg/kg/min
0 0 0 2+ Cardiogenic shock
Dopa, dopamine.aIncreases renal and splanchnic blood flow.bMilligram doses are in bold to differentiate from micrograms.cSQ: Subcutaneous dosing, may be repeated every 15–20 min.dPhosphodiesterase inhibitors; require loading dose.From Jimenez EJ. Shock. In: Civetta JM, Taylor RW, Kirby RR, eds. Critical Care. 3rd ed. Philadelphia: Lippincott–Raven Publishers; 1997:359.Historically, the exaggerated peripheral vasoconstrictive properties of the drug have promoted a level of distrust leading to the often quoted “Leave 'em Dead.” These fears are largely unfounded at indicated dosing ranges, and use of the drug may actually enhance renal function (152). The drug is safe and easily titratable, and lacks the tachyarrhythmic properties of other frequently used agents for shock. A resurgence in the use of norepinephrine has occurred with the recognition of its beneficial properties, and is now recommended as the first-line vasopressor in the treatment of septic shock (95). Norepinephrine is also useful for other forms of distributive shock and as a temporizing agent in cardiogenic shock.EpinephrineEpinephrine is the major physiologic adrenergic hormone of the adrenal medulla and represents the maximum in catecholamine stimulation. The agent potently stimulates α1 receptors with resultant
marked venous and arterial vasoconstriction. These changes may lead to detrimental effects on regional blood flow, particularly on mesenteric and renal vascular beds. β effects lead to increased heart rate and inotropism. Due to counter effects of β2 vasodilation, the diastolic blood pressure is
only slightly affected, with a lesser degree of increase in MAP than norepinephrine. Stimulation of β2 receptors and blunting of mast cell response also makes epinephrine highly effective for
anaphylaxis. Epinephrine has dose-dependent effects, with very low doses stimulating primarily β receptors. This property makes epinephrine attractive as a primary inotrope; however, the range of that particular low dose varies with each patient and titration may prove dangerous. In general, the use of epinephrine is considered a drug of last choice or in extreme situations such as cardiac arrest.DopamineDopamine has long been the workhorse in shock resuscitation, although the preponderance of its use has slowed with increasing evidence of deleterious effects (153). As the hormone precursor of norepinephrine and epinephrine, dopamine stimulates α, β, and dopaminergic receptors in a dose-dependent fashion. This results in mixed vasoconstrictive, inotropic, chronotropic, and vasodilatory
effects.Classically, “renal-dose” dopamine ranges from 0 to 5 µg/kg/minute and results in vasodilation of renal and P.826mesenteric vascular beds via dopamine receptors. Although this stimulation results in diuresis, the overall effect on renal function and need for renal replacement therapy is unchanged and may actually be worsened (154). Conversely, at high doses of 10 to 20 µg/kg/minute, α effects predominate, resulting in almost pure vasoconstriction. β-Receptor stimulation at middle doses of 5 to 10 µg/kg/minute results in increased inotropic and chronotropic function leading to increased MAP similar to norepinephrine. However, without simultaneous activation of α receptors at this dose, vasodilatation by dopamine receptors is unopposed and reflex tachycardia may predominate. These dose-related effects are simply a guideline, as responsiveness to titration varies patient to patient, particularly in critical illness.In the past, dopamine has been postulated as the first inotrope of choice in cardiogenic failure with hypotension (155). More recent recommendations, however, identify sympathetic inotropes such as dopamine as increasing mortality when used for primary left heart failure (156). Likewise, in septic shock, norepinephrine has a more reliable dosing profile and has demonstrated more beneficial outcomes compared to dopamine (157).PhenylephrinePhenylephrine is a rapidly acting vasopressor with a short duration of action and pure α1
stimulation. As such, it increases MAP primarily by increasing systemic vascular resistance. Reflex bradycardia may develop; therefore, it is occasionally used for distributive shock in the face of tachyarrhythmias. This same unopposed increase in vascular resistance also impairs cardiac output in the patient with impaired pump function. The use of phenylephrine has since fallen out of favor, and is generally reserved for the pregnant patient with shock for whom other vasopressors may be detrimental.InotropesAs a group, inotropic agents augment cardiac output by increasing contractility. Sources of left ventricular failure are many, including exacerbation of congestive heart failure, acute infarction, or sepsis-related cardiomyopathy. Although improvement of pump function in these situations seems logical as a primary therapy, no literature supports any positive benefit on mortality when inotropes are used. This may be particularly true when the agents are used in a long-term fashion. As with other forms of pharmacotherapy for shock, inotropes should be used only in a short-term situation until underlying pathology can be corrected. Prolonged use can increase myocardial work and exacerbate ischemia.The classic paradigm of cardiogenic shock with resulting reflexive increase in afterload has been recently challenged, with recognition of an inflammatory component to acute infarction. This inflammatory state results in vasodilation, making particular inotropes less useful for restoration of tissue perfusion (158). Likewise, the concept of pushing oxygen delivery to supranormal levels with excessive amounts of dobutamine (5–200 µg/kg/minute) to enhanced cardiac output has been largely abandoned, as it may worsen outcome (90).DobutamineDobutamine is a synthetic adrenergic agent derived from dopamine. Current formulation of the drug is as a racemic mixture, with the L-isomer stimulating α1 and the D-isomer stimulating β1 and β2
receptors. This combined stimulation results in a net increase in inotropic and chronotropic parameters. In theory, vasodilatory (β2) effects are limited, making dobutamine useful in increasing
pump function without lowering blood pressure. In practice, some degree of vasodilation is encountered, resulting in decreased blood pressure and tachycardia acutely. With increase in cardiac output, however, the blood pressure generally corrects to normal. For this reason, adequate volume loading prior to initiation of dobutamine is emphasized. Likewise, the lack of increase in blood pressure makes dobutamine a poor selection as monotherapy in primary cardiogenic shock. Currently, dobutamine is the standard inotrope used in noncardiogenic shock (such as sepsis) when
cardiac contractility is compromised (159).DopexamineAnother of the synthetic catecholamines, dopexamine uniquely stimulates β2 and dopaminergic
receptors with no α-adrenergic effects and minimal β1 stimulation. Resultant effects therefore
include vasodilation and positive inotropy via increased stroke volume. The agent may also exert indirect vasoactive changes via inhibition of norepinephrine reuptake at the postganglionic synapse (160). Dopexamine is often compared to dobutamine in trials, with the possible benefit of improved splanchnic perfusion (161).IsoproterenolWith practically no α-adrenergic stimulation, isoproterenol functions as a pure β agonist. β1
stimulation results in increased stroke volume and heart rate, while β2 stimulation induces
vasodilatation. The net result is that of enhanced cardiac output without the benefit of distribution of blood flow. Increased myocardial oxygen consumption exacerbated by lack of coronary perfusion due to decreased diastolic pressures may lead to cardiac ischemia. Use of isoproterenol is generally limited to β-blocker overdose or in the atropine-resistant transplanted heart.MilrinoneA novel agent in vasoactive treatment, milrinone is a synthetic phosphodiesterase III inhibitor. Reduction in this enzyme results in an increase in cyclic adenosine monophosphate (cAMP), a modulator of myocardial contractility. Additional increase in cAMP results in vasodilation, with the net effect of increasing cardiac output and tachycardia at higher doses. This vasodilatory effect may decrease effective left ventricular preload, but may also benefit afterload reduction, reducing cardiac work. In the hypotensive patient, this vasodilation may not be tolerated acutely. While not recommended in vasodilatory shock for this reason, milrinone may be used in specific situations for cardiogenic shock. These include advanced heart failure in patients awaiting heart transplant, in acute decompensation of congestive heart failure (CHF) on standard medications, and in patients in cardiogenic shock with long-term β-blocker use (162).LevosimendanLevosimendan is the singular drug in a new class of inotropic agents. Primary mechanism of action is by increasing the sensitivity of troponin C for calcium without enhancing influx of calcium itself. The advantage of this physiology would be increased contractility without risk of arrhythmias. The drug shows promise as a new agent and is currently undergoing further investigation (163).Miscellaneous Pharmacologic TherapyNumerous other noncatecholamine agents have been used for various shock states. These may work by treating the P.827symptoms, such as increasing vascular tone, or by treating the source depending on the type of shock. Examples of drug therapy for source treatment include antibiotics for septic shock, histamine blockers for anaphylactic shock, or somatostatin analogues for gastrointestinal hemorrhagic shock (164,165,166). Septic shock, in particular, is a syndrome for which the “magic bullet” is constantly sought. Numerous drugs under investigation seek to manipulate the inflammatory cascade at multiple levels. The agents reviewed here are more commonly incorporated into shock management.VasopressinVasopressin is an attractive hormone for use in shock states not only for its vasoconstrictive properties, but also for its antidiuretic effects. As a noncatecholamine vasopressor, it acts via V1 receptors to restore vascular tone. Catecholamine responsiveness may decrease over time during severe sepsis, possibly due to an increase in nitric oxide–induced vasodilatation. This alternate mode of action makes vasopressin a logical treatment for catecholamine-resistant shock. Studies of hemorrhagic and vasodilatory shock have demonstrated a relative deficiency of vasopressin. For this reason, vasopressin is often used at a low dose without titration, in the manner of hormone replacement. Potentiation of adrenergic agents makes vasopressin particularly useful in combination
with norepinephrine, and has been recommended for the treatment of septic shock (167). Addition of vasopressin allows for reduced dosing of more harmful catecholamines in this situation. The ongoing Vasopressin and Septic Shock Trial (VASST) will help to define the role of vasopressin compared to norepinephrine in sepsis (168).TerlipressinTerlipressin is an analogue of vasopressin that is used in countries in which vasopressin is not available. It is employed in a similar fashion, usually for the treatment of catecholamine-resistant shock. Early studies are favorable, showing an increase in MAP and a decrease in the need for catecholamine vasopressors (169). Splanchnic circulation is spared excessive vasoconstrictive effects, as demonstrated by an increase in gastric mucosal perfusion (170). Terlipressin is used as a single bolus in these studies due to its long half-life (6 hours). This long duration of action may be disadvantageous as the effects are not easily discontinued if necessary, as with a vasopressin drip.SteroidsThe use of steroids in critical care has long been the topic of debate and refinement. For the purposes of shock, however, more definitive literature is emerging to help clarify their role. The role of “stress-dose steroids” perioperatively to prevent hypotension in the adrenal-insufficient patient has been supported for many years. The concept of relative adrenal insufficiency complicating shock states is now established as a recognizable and treatable entity. A recent meta-analysis reviewed the use of 200 to 300 mg of hydrocortisone daily for patients with septic shock. Administration for 5 days or more reduced duration of shock and mortality without increasing associated side effects of infection (171). Use of steroids should be limited to patients with shock refractory to fluids and vasopressors, and with a chemical diagnosis of adrenal insufficiency. Fludrocortisone at a dose of 50 mg/day orally may be added to the hydrocortisone regimen (172).Drotrecogin AlfaAmong the newer immunomodulatory agents, drotrecogin alfa has received the most attention. The agent is a recombinant form of activated protein C, which acts to down-regulate the proinflammatory state, anticoagulate, and enhance fibrinolysis to enhance reopening of the microcirculation. As such, it is used for severe sepsis rather than shock per se. Due to its effect on the coagulation profile, the drug has limitations in patients with a risk of bleeding. When used as a drip (24 g/kg/hour for 96 hours), the drug provided a 6% reduction in 28-day mortality for patients with severe sepsis. The drug is expensive, and treatment should be limited to the patient with septic shock requiring renal or respiratory support, as outlined in the PROWESS trial (173).End Points of ResuscitationThe primary goal in the management of shock is a return to normal tissue perfusion. If shock is recognized promptly and timely appropriate treatment strategies are implemented, reversal of its clinical signs may be appreciated. These include improvement in mental status, normalization of vital signs, and restoration of urine output. However, despite these findings, many patients remain in a state of occult hypoperfusion and ongoing tissue acidosis with resultant multiple organ failure and death (12,174). This has been termed “compensated shock.” Consequently, better end points of resuscitation are needed to guide resuscitation efforts.The ideal end point should be operator independent, noninvasive, readily available, safe, and inexpensive. Unfortunately, no single parameter has proven superior in its ability to drive resuscitation efforts. This being said, numerous parameters have been proposed and/or utilized including basic hemodynamic monitoring, invasive hemodynamic monitoring, oxygen delivery, oxygen consumption, mixed venous oxygen saturation, lung water, arterial base deficit, arterial lactate, capnometry, tissue oxygen and carbon dioxide electrodes, and near infrared spectroscopy. We will discuss several of these in more depth in the following paragraphs.Basic Hemodynamic MonitoringBasic monitoring in patients with shock includes noninvasive vital sign measurements, cardiac rhythm, and urinary output. During this timeframe, an accurate blood pressure reading is essential. There are several states that underestimate blood pressure measurements including tachycardia in instances of a narrow pulse pressure, arrhythmias, and peripheral vascular disease, all of which are
not uncommon in this population (175). The utilization of Doppler is helpful in such instances; however, it does not always rectify the problem (176). When more detailed information is desired, invasive hemodynamic monitoring is indicated.Invasive Hemodynamic MonitoringThe hemodynamic profiles of shock are depicted in Table 55.2. It is these parameters that often guide the management of shock. As such, meticulous equipment calibration and documentation are essential (177,178). These measurements are subject to many potential artifacts as seen in Table 55.9 (14). P.828P.829Therefore, it is critical for the clinician to evaluate these variables in concert with the patient's clinical picture.
Table 55.9 Common artifacts in hemodynamic measurementsVariable Artifact Causes Comments/corrective actionVascular pressures (including PCWP)
Preload overestimation
Technical:Improper leveling of transducerImproper calibrationImproper system frequency response
Avoid with rigid nursing protocols
Respiratory: Not recording pressures at
end-expiration during mechanical ventilation
Avoid digital readoutsUse analog tracings
Active expiratory effortPositive end-expiratory pressure
Suspect with respiratory distress; consider muscle paralysisUsually not significant with <10 cm H2O PEEP
Improper positioning of catheter tip
Suspect if tip in upper lobes on chest radiograph or PAD < PCWP
Cardiac: Mitral regurgitation Read PCWP as post–A wave Mitral stenosis Interpret with caution as preload
estimate Acute changes in left
ventricle complianceSuspect in presence of myocardial ischemia
Preload underestimation
Technical: (as above)Respiratory:
Not recording pressures at end-expiration during spontaneous breathing
Cardiac output Inaccuracies Technical: Incorrect injectable volume;
thermistor contact with vessel wall; incorrect computational constant
Inspect temperature curves; suspect if pulmonary artery waveform is dampened; follow rigid nursing protocol
Cardiac: Tricuspid regurgitation Do not use in presence of
significant tricuspid regurgitation
Wide variation Technical: (as above) Delete measurements with >20% variation from the mean
Respiratory: Variable respiratory rate
during mechanical ventilation
Average measurements throughout respiratory cycle
Mixed venous oxygen saturation
Inaccuracies Technical:Light reflecting against vessel wall, catheter kinking
Note computer error messages
Presence of significant HgbCO
Measure HgbCO directly at least once
Misinterpretation Shifts in oxygen dissociation curve
Correlate with PvO2
measurements Dependence on oxygen
deliveryCorrelate with oxygen delivery measurements
Extravascular lung water
Inaccuracies Inaccurate measurement of cardiac output (as above)
Correlate cardiac output with regular thermodilution measurements
Underestimation Presence of significant areas of nonperfused lung
Measurements suspect in presence of significant regional disease (i.e., lobar pneumonia) or known vascular obstruction
Systemic vascular resistance
Inaccuracies Inaccurate measurement of cardiac output (as above)
Inaccurate measurement of blood pressure
Measure directly (see above)
PCWP, pulmonary capillary wedge pressure; PEEP, positive end-expiratory pressure; PAD, pulmonary artery diastolic; HgbCO, carboxyhemoglobin; PvO2, mixed venous oxygen partial
pressure.From Jimenez EJ. Shock. In: Civetta JM, Taylor RW, Kirby RR, eds. Critical Care. 3rd ed. Philadelphia: Lippincott–Raven Publishers; 1997:359.Central venous catheters are commonly used in this patient population. As such, central venous pressure measurements are readily available, and often serve as a rough guideline in the resuscitation of shock. The problem is the lack of a well-defined goal for central venous pressure. Similarly, with pulmonary artery catheters, numerous additional hemodynamic parameters become available; however, it is not clear that the appropriate end point is the normalization of these values, nor is it clear how these end points should be achieved (179,180,181,182).In fact, observational studies have suggested that pulmonary artery catheters may actually increase mortality, intensive care unit length of stay, hospital costs, and resource utilization (183). In 2005, Shah et al. performed a meta-analysis of 13 randomized clinical trials evaluating the use of pulmonary artery catheters (184). They documented no improvement in overall mortality or hospital length of stay. An even more recent randomized controlled trial by the National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network found no survival benefit and increased catheter-associated complications when comparing pulmonary artery catheters to central venous catheters in the management of patients with acute lung injury when utilized relatively late (within 48 hours), which is the time when resuscitation should already be completed (185). The only positive trial involving pulmonary artery catheters was in older trauma patients who were in severe shock (186). In this subset, Friese et al. documented a survival benefit when patients were managed with a pulmonary artery catheter. This was, however, a retrospective review of the National Trauma Data Bank.Oxygen Delivery
Oxygen delivery (DO2) is a function of cardiac index (CI), hemoglobin (Hb), and oxygen saturation
(SaO2) as seen in the Fick equation:
DO2 (mL/minute/m2) = (CI)
× (1.34 mL O2 carried by 1 g of Hb if 100% saturated)
× (Hb)(SaO2)
The use of oxygen delivery as a resuscitation end point has had varying results. In the 1970s, Shoemaker et al. reviewed the physiologic patterns in surviving and nonsurviving shock patients (187,188). They observed that survivors had significantly increased oxygen delivery, oxygen consumption, and cardiac index values (oxygen delivery ≥600 mL/minute/m2, oxygen consumption ≥170 mL/minute/m2, and cardiac index ≥4.5 L/minute/m2). In a subsequent prospective study, they documented decreased complications, lengths of stay, and hospital costs when employing these parameters as goals of resuscitation in high-risk surgical patients (189). Further work by Shoemaker's group and others have shown that utilization of this “supranormal resuscitation” strategy decreases morbidity and mortality in critically ill patients (180,190,191,192).Others have been unable to demonstrate any benefit to supranormal oxygen delivery (193,194,195). Moreover, supranormal resuscitation has been associated with significant morbidity (i.e., ongoing tissue ischemia, abdominal compartment syndrome, coagulopathy, and congestive heart failure) and mortality (196). In 2000, Velmahos et al. documented improved survival in patients who achieved supranormal oxygen delivery; however, they concluded that “this was not a function of the supranormal resuscitation, but rather the patient's own ability to achieve these parameters” (197,198). More recently, Kern and Shoemaker reviewed all randomized clinical trials of hemodynamic optimization (199). They determined that a survival benefit was only appreciable in those studies with interventions prior to the onset of organ failure and mortality of >20% in the control group (200). As demonstrated here, the utilization of oxygen delivery and more specifically “supranormal resuscitation” in the management of shock has had varying degrees of success.Mixed Venous Oxygen SaturationAnother end point previously examined was mixed venous oxygen saturation. In critically ill patients, Gattinoni resuscitated patients to one of three hemodynamic goals (193). These included a cardiac index between 2.5 and 3.5 L/minute/m2, cardiac index >4.5 L/minute/m2, and SvO2 ≥70%.
There were no differences in multiple organ failure or mortality between the groups. This is in contrast to Rivers' study of severe sepsis/septic shock patients where reaching SvO2 ≥70% within 6
hours of resuscitation improved survival (88).Base DeficitBase deficit is defined as the amount of base in millimoles required to increase 1 liter of whole blood to the predicted pH based on the PaCO2 (161). It may be calculated using the arterial blood
gas as follows (201):Base Deficit = -[(HCO3) - 24.8 + (16.2)(pH - 7.4)]
In shock states, the base deficit may serve as a surrogate marker for anaerobic metabolism and subsequent lactic acidosis if metabolic acidosis is the primary disorder and not a compensatory response (202). In this sense, it is superior to pH secondary to the many compensatory mechanisms in place to normalize pH (203).Secondary to its availability and rapidity, base deficit has been extensively studied as an end point of resuscitation. In a retrospective review, Davis et al. demonstrated that an increasing base deficit correlated directly with admission hypotension and increasing fluid requirements within the first 24 hours of admission (204). Furthermore, they determined that failure to normalize the base deficit was associated with increased mortality. Others have documented correlations between base deficit and blood product requirements, lengths of stay, acute lung injury, acute respiratory distress syndrome, renal failure, coagulopathy, multiple organ failure, and mortality (205,206,207,208,209,210,211,212,213,214,215,216,217,218,219).
In the clinical arena, base deficit levels have numerous confounders. These include alcohol intoxication, hyperchloremic metabolic acidosis secondary to aggressive normal saline or lactated Ringer resuscitation, and sodium bicarbonate administration (220,221). Base deficit may also be a normal compensatory response to respiratory alkalosis. As such, base deficit may be useful in trending resuscitation efforts; however, it is not a definitive stand-alone end point.P.830LactateSerum lactate levels are used extensively in monitoring shock resuscitation. In patients suffering from noncardiogenic shock, Vincent et al. documented a correlation between initial serum lactate levels and patient outcomes (222). However, in shock resuscitation it is the lactate trend that is most predictive of mortality. In trauma patients managed with “supranormal resuscitation,” Abramson et al. determined that the time to lactate normalization was an important predictor of mortality (223). Patients whose lactate levels normalized (serum levels below 2 mmol/L) within 24 hours had a <10% mortality, those who normalized between 24 and 48 hours had a 25% mortality, while those who did not normalize by 48 hours had a >80% mortality. This trend was corroborated by McNelis et al. in postoperative surgical patients (224). In the trauma population, Manikas et al. further demonstrated that initial and peak lactate levels correlated with multiple organ failure (225). Although the serum lactate level signifies shock and ongoing tissue ischemia, its utilization as an end point in the resuscitation of shock has yet to be validated.BicarbonateDuring anaerobic metabolism, bicarbonate serves as a buffer for released hydrogen ions. Serum bicarbonate levels decrease as the acidosis worsens, and in essence act as a surrogate for metabolic acidosis. In recent studies, serum bicarbonate levels have been determined to better predict metabolic acidosis and mortality than pH, anion gap, or lactate (226,227). Unfortunately, bicarbonate suffers from the same limitations as base deficit; therefore, its use as an end point of resuscitation is unclear at this time.CapnometryDuring periods of shock and ongoing tissue hypoperfusion, blood flow to the most vulnerable organs (brain and heart) is preserved at the expense of other organs (kidneys, intestinal tract, and musculoskeletal system) (200). In theory, the expended organs will manifest this state with an increase in tissue PCO2 and a subsequent decrease in tissue pH. The splanchnic and oral mucosa are
especially sensitive to such hypoxemic states; therefore, buccal, sublingual, and gastric capnometry would seem invaluable in monitoring shock resuscitation. Gastric capnometry is limited by gastric enteral nutrition, endogenous gastric acid secretion, and H2 blockers (228,229).
Buccal and sublingual capnography have been shown to directly correspond with blood pressure, cardiac output, and tissue perfusion in animal models (230,231). Furthermore, they are more accurate in predicting mortality than blood pressure is. Povoas et al. documented a correlation between sublingual and duodenal PCO2 and mesenteric blood flow during hemorrhagic shock in
swine (232). In acutely ill humans, Weil et al. demonstrated a correlation between sublingual PCO2
and lactate levels, the presence of shock, and survival (233,234). Additional studies have shown a correlation between sublingual PCO2 and changes in regional microcirculatory blood flow and
ongoing bleeding (235,236). Unfortunately, PCO2 levels vary widely in the population, making
standardization quite difficult (198). Monitoring device for sublingual capnography was recalled in 2004 for infectious complications and may be reinstated in the future.Near-infrared SpectroscopyNear-infrared spectroscopy is the measurement of the wavelength and intensity of the absorption of near-infrared light by a sample. In medicine, it uses chromophores such as hemoglobin to do so and allows for the measurement of tissue oxygenation, PO2, PCO2, and pH (237). Taylor et al.
documented a close correlation between tissue oxygenation measurements and hemodynamic parameters in a hemorrhagic shock model (238). In this study, near-infrared spectroscopy was also better able to differentiate “responder” from “nonresponder” animals in comparison to lactate levels
or global oxygen delivery. McKinley et al. studied near-infrared spectroscopy in critically injured trauma patients (239). They determined that the oxygen saturation of hemoglobin in tissue (StO2)
correlated well with systemic oxygen delivery, base deficit, and lactate. This modality is increasing in popularity with trials currently ongoing.In shock resuscitation, the treatment strategy is to return normal tissue perfusion. Resuscitation end points are critical in this management. The ideal end point should be operator independent, noninvasive, readily available, safe, and inexpensive. Currently, no single parameter has proven superior in its ability to drive resuscitation efforts.SummaryShock is likely the most common life-threatening diagnosis made in the intensive care unit. Despite technologic advances, it remains a significant source of morbidity and mortality. Its etiology is vast. As such, the diagnosis of shock and its inciting source can be difficult to identify if not elusive. Aggressive diagnostic testing is required to avoid irreversible cellular injury, multiple organ failure, and potentially death. The primary goal in the management of shock is a return to normal tissue perfusion. This is attained via various volume resuscitation modalities, pharmacologic agents, and resuscitation end points. Past and current research efforts continue in hopes of optimizing the diagnosis and management of shock with the ultimate goal of improving patient outcomes.
Chapter 56Cardiogenic ShockMarc A. SimonMichael R. PinskyThis work is supported in part by NIH grants HL007820, HL067181, and HL073198, and the NIH Roadmap Multidisciplinary Clinical Research Career Development Award Grant (K12 RR023267) from the National Institutes of Health.Immediate ConcernsDefinitionCardiogenic shock is a major and frequently fatal complication of a variety of acute and chronic disorders that results in a primary impairment of the ability of the heart to maintain adequate tissue perfusion despite sufficient intravascular volume.Essential Diagnostic Tests and Procedures
Bedside clinical criteria that provide evidence of reduced organ perfusion include oliguria, confusion, peripheral cyanosis, and evidence of peripheral vasoconstriction.
An accurate definition of cardiogenic shock also requires persistence of the shock state after correction of extracardiac conditions, such as hypovolemia or a variety of metabolic
abnormalities including significant disturbances in acid-base metabolism, electrolyte abnormalities, or arrhythmias.
The pulmonary artery occlusion pressure (PAOP) is frequently in excess of 18 mm Hg, and the cardiac index (CI) is usually less than 2.2 L/minute/m2.
Initial Therapy
Cardiogenic shock in the setting of acute myocardial infarction warrants pharmacologic intervention to limit infarct size and includes using heparin, aspirin, nitrates, β-blockers, calcium channel blockers, or a combination thereof. Primary coronary artery stenting is now recommended for patients with ST elevation or left bundle branch block who develop shock within 36 hours of acute myocardial infarction and are suitable for revascularization that can be performed within 18 hours of shock onset (1). Thrombolytic therapy may be used if early revascularization is not available (2).
Hemodynamic management includes optimization of preload and afterload and augmentation of contractility, when appropriate, with agents such as dobutamine, dopamine, norepinephrine, digitalis preparations, or phosphodiesterase inhibitors.
Surgical intervention in myocardial infarction has been used to limit infarct size by direct revascularization or correction of mechanical defects of an acute ischemic event such as ventricular septal defects (VSDs), acute mitral insufficiency, free wall rupture, or left ventricular aneurysm.
Mechanical assist devices such as the intra-aortic balloon pump (IABP) are used as temporizing measures to optimize blood pressure, cardiac output, and tissue perfusion in patients with cardiogenic shock while further diagnostic procedures and disease staging are performed. Newer percutaneous ventricular assist devices (VADs) providing 2 to 5 L/minute blood flow are now available and hold promise for rapid restoration of peripheral perfusion.
ClassificationA variety of classification schemes have been proposed for the division of circulatory shock according to etiology and underlying hemodynamic mechanisms. Circulatory shock can be subdivided into four distinct classes on the basis of underlying mechanism plus hemodynamics; these classes should be considered and excluded before establishing a definite diagnosis of cardiogenic shock.Hypovolemic ShockHypovolemic shock results from volume loss caused by conditions such as gastrointestinal bleeding or extravasation of plasma.Obstructive ShockObstructive shock results from impedance of the circulatory channels by an intrinsic or extrinsic obstruction. Pulmonary embolism, dissecting aneurysm, and pericardial tamponade result in obstructive shock.Distributive ShockDistributive shock is caused by conditions such as direct arteriovenous shunting and is characterized by decreased resistance or increased venous capacity from the vasomotor dysfunction.Cardiogenic ShockCardiogenic shock is characterized by primary myocardial dysfunction resulting in the inability of the heart to maintain an adequate cardiac output with subsequent compromising of metabolic requirements (Fig. 56.1). The most common P.836etiologies are myocardial infarction and cardiomyopathy with a superimposed hemodynamic stress.
Figure 56.1. Neurohumoral and mechanical events that lead to death in patients with cardiogenic shock. ANP, atrial natriuretic peptide. (Used with permission from Pasternak RC, Braunwald E. Acute myocardial infarction. In: Wilson JD, Braunwald E, Isselbacher KJ, eds. Harrison's Principles
of Internal Medicine. 12th ed. Vol. 1. New York: McGraw-Hill; 1991:953–964; and Francis GS. Neuroendocrine manifestations of congestive heart failure. Am J Cardiol. 1988;62[Suppl]:9A–13A.)EtiologyIn order to understand the therapeutic approaches used to support left ventricular (LV) ejection and aid acutely decompensated hearts, it is important to understand the mechanisms underpinning LV systole. Systolic ventricular function is determined by preload, afterload, and contractility. Preload is the wall stress on the left ventricle prior to ejection. Operationally, we use LV end-diastolic volume to reflect this wall stress. Since measures of volumes can be difficult at the bedside, LV end-diastolic pressure, left atrial pressure, or pulmonary artery occlusion pressure are often used as surrogates for LV end-diastolic volume. Afterload is the maximal LV wall stress during ejection. By LaPlace's law, wall stress is proportional to the product of LV radius of curvature and transmural pressure. Under normal conditions, maximal LV afterload occurs at the instant of aortic value opening. Contractility is a more difficult term to define and quantify. A reasonable definition is the amount of force capable of being produced by the contracting myocardium (3). On a cellular level, contractility is related to the integrity of the actin–myocin coupling, intracellular calcium (Ca2+) flux rate, and quantity. Functionally, one measures contractility by varying preload and afterload. Numerous measures have been attempted to quantify contractility with varying degrees of success depending upon the degree of true independence they have from preload or afterload. Measures of contractility include the maximal rate of isovolumic pressure development (dP/dtmax), the Frank-
Starling law relating peak systolic activity (defined as either maximal developed pressure, volume ejected, or the product of the two) directly to end-diastolic volume (4), and left ventricular end-systolic pressure–volume relation (ESPVR) derived from pressure–volume loops. Systolic performance is the ability of the left ventricle to empty. This is a function of end-systolic volume; a commonly used calculation is the LV ejection fraction (effective ejection fraction in the case of valvular regurgitation).The most common etiology of cardiogenic shock is acute myocardial infarction (MI) with a resultant loss of approximately 40% of functioning myocardium. Following myocardial infarction, the final infarct size has been shown to correlate with the degree of LV dysfunction (5). Loss of myocardial function may occur in one massive MI or may result in a cumulative loss of pump function caused by serial smaller infarcts. Cardiogenic shock more commonly results from infarction of the left ventricle, although recent clarification of the potential role of the right ventricle in the precipitation of the shock state P.837has been recognized. Additionally, acute mechanical complications of myocardial infarction such as mitral insufficiency, free wall rupture, and acute VSD may result in cardiogenic shock during the peri-infarct period, as does the late development of left ventricular aneurysm (Table 56.1). Other causes of cardiogenic shock include end-stage or fulminant cardiomyopathy, myocarditis, acute chordal rupture causing valvular regurgitation, obstruction to left ventricular ejection (severe aortic stenosis or hypertrophic cardiomyopathy) or left ventricular filling (mitral stenosis or left atrial myxoma), or severe septic shock with myocardial depression.
Table 56.1 Contributing factors to the development of cardiogenic shock in myocardial infarction
1. Loss of left ventricular functionCumulative loss of myocardial tissue exceeding 40% ofventricular mass, particularly anterior infarctsMyocardial infarction associated with bradyarrhythmiasor tachyarrhythmiasHypovolemia or hypervolemia
2. Right ventricular infarction 3. Mechanical defects
Papillary muscle dysfunction or rupture causing acuteregurgitationVentricular septal defectVentricular pseudoaneurysm
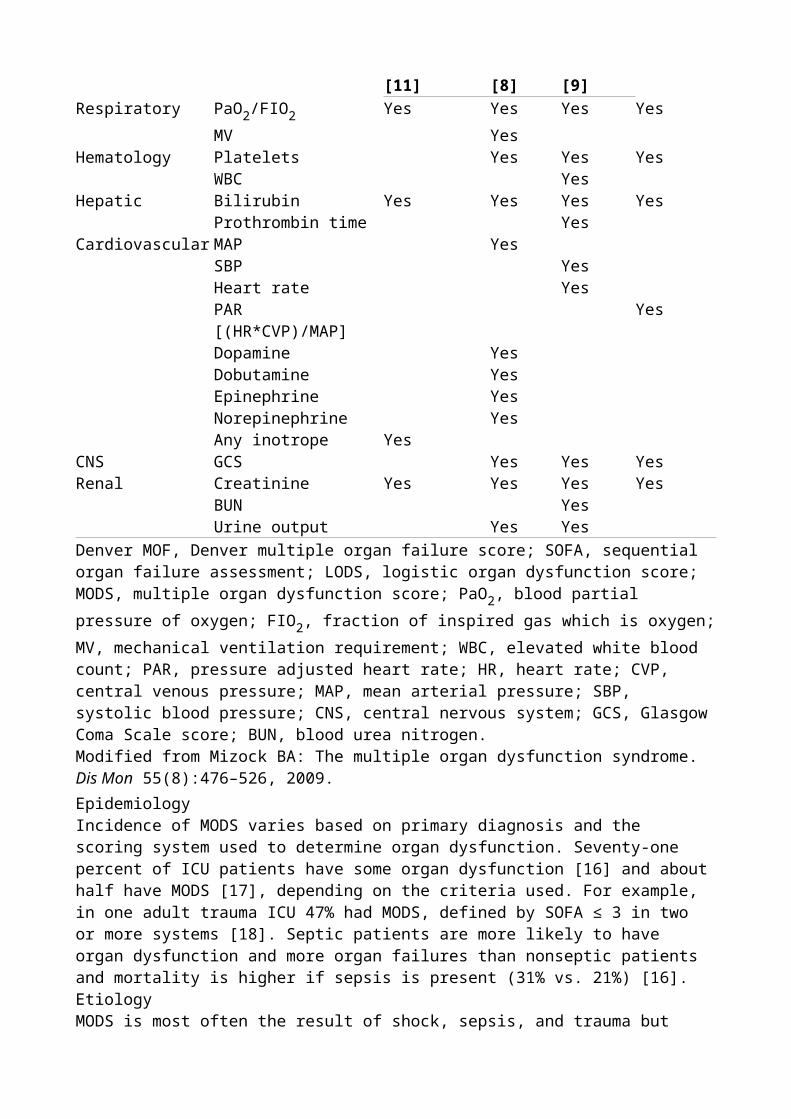
Free wall rupture and/or cardiac tamponade
Left Ventricular Acute Myocardial InfarctionReduction in left ventricular performance is one of the major complications of ischemic heart disease. Several classifications that attempt to standardize the clinical and hemodynamic presentation of myocardial infarction have been proposed to aid in determining prognosis and the therapeutic approaches in patients with established cardiogenic shock or those who have the potential to progress to the shock state.The Killip classification uses pure clinical bedside evaluation of the patient to establish prognostic indicators to predict the mortality associated with an acute myocardial infarction using the physical findings of congestive heart failure (6).
Class I patients developed no overt signs of congestive heart failure, and these individuals had a low in-hospital mortality rate. This subgroup represented approximately 40% to 50% of all patients who presented with an acute MI. The in-hospital fatality rate was approximately 6%.
Class II patients demonstrated evidence of impaired ventricular function as manifest by persistent bibasilar rales and an audible third heart sound. This subset of patients accounted for approximately 30% to 40% of patients with acute MI. The in-hospital mortality rate of 17% was triple relative to class I patients.
Class III patients were characterized by the development of acute pulmonary edema, which was seen in approximately 10% to 15% of patients admitted to the hospital. A significant mortality rate of 38% was seen in this group treated conservatively before the thrombolytic era.
Table 56.2 Hemodynamic subsets and mortality in myocardial infarctionSwan-Forrester class Mortality rate (%)I: CI >2.2; PAOP <18 <3II: CI >2.2; PAOP >18 9III: CI <2.2; PAOP <18 23IV: CI <2.2; PAOP >18 51PAOP, pulmonary artery occlusion pressure; CI, cardiac index in liters per minute per square meter.
Class IV patients had established cardiogenic shock with hypotension and signs of organ hypoperfusion. Cardiogenic shock occurred in 5% to 10% of infarct patients in this series but was associated with a high in-hospital mortality rate of 80%, which was a function of both severity of the underlying illness plus the limited availability of definitive treatment at the time this classification was proposed.
The group at Cedars Sinai Medical Center, Los Angeles, also developed a clinical classification of heart failure associated with acute MI, which was subsequently refined by the availability of invasive hemodynamic monitoring using pulmonary artery catheters (PACs) (7) (Table 56.2). The Cedars Sinai classification also subdivided patients with acute myocardial into four subsets based on the measurement of the PAOP, CI, and clinical assessment.Class I patients had no clinical evidence of pulmonary congestion or tissue hypoperfusion. Hemodynamic parameters measured in these subjects revealed the PAOP to be less than 18 mm Hg and the CI to be in excess of 2.2 L/minute/m2. The advent and widespread use of pulmonary artery catheters clarified the concept of the ideal wedge that established the impact of diastolic dysfunction secondary to acute ischemia, with resultant impaired relaxation and elevated filling pressures being required to maintain adequate cardiac output.Class I patients accounted for 25% of subjects admitted to the coronary care unit, and there was a low in-hospital mortality rate of 1%. Patients who on clinical grounds demonstrated no evidence of hypoperfusion or pulmonary congestion would not be expected to benefit from invasive cardiac
monitoring. Frequent clinical reassessments and close attention paid to blood pressure and evidence of organ perfusion would represent adequate care.Class II patients demonstrated pulmonary congestion as manifest by only an elevated PAOP greater than 18 mm Hg with an associated normal cardiac index. Class II patients accounted for approximately 25% of patients admitted to the coronary care unit, but an 11% mortality rate was associated with this group. Mild pulmonary congestion is transiently seen in a significant percentage of patients admitted to the coronary care unit and has a multifactorial etiology. Diastolic dysfunction induced by ischemia with retrograde transmission of elevated filling pressures into the pulmonary venous circuit results in extravasation of fluid into the pulmonary bed when hydrostatic pressure exceeds oncotic pressure. Ischemic papillary muscle dysfunction with mild degrees of mitral insufficiency is also P.838a potential cause of pulmonary congestion in this subgroup. Physical examination of these patients reveals mild to moderate rales and potentially an audible third heart sound associated with radiographic evidence of pulmonary venous hypertension. Dyspnea and orthopnea are the main symptoms superimposed on the clinical presentation of myocardial ischemia. Treatment in this group is centered on reduction of filling pressures to a level that relieves pulmonary venous congestion but does not result in an overzealous reduction of filling pressures below the ideal wedge as the reduced cardiac contractility will require some increased filling volume and pressure to maintain adequate stroke volume and perfusion pressure (Starling mechanism). Excessive diuresis should be assiduously avoided, especially in patients who were euvolemic before the onset of their infarct. Despite signs of pulmonary congestion, patients presenting with acute pulmonary congestion frequently are not intravascularly volume overloaded, and diuretic therapy may reduce filling pressures to a level that would impair cardiac output. It is often difficult to ascertain at the bedside which patients are actually euvolemic and which are hypervolemic. Afterload reduction therapy will benefit both groups of patients and may allow time to assess total effective circulating blood volume by indirect measures, such as the existence of hyponatremia, peripheral edema, and S4 gallop. Inotropic agents should be considered in such a situation so that pulmonary congestion
can be relieved by diuresis if afterload reduction is not immediately effective since the increased inotropic state mitigates against a reduction in cardiac output induced by any reduction in cardiac filling pressures. Oxygenation should be maintained with adequate arterial saturation that may be monitored by oximetry. Vasodilator therapies in the form of nitroglycerin or inotropic agents with vasodilating capacity such as dobutamine are effective to return the hemodynamic parameters to normal. The usefulness and risk–benefit ratio of invasive hemodynamic monitoring in this subgroup of patients are controversial, although these patients frequently may be managed on clinical grounds.Class III patients are characterized predominantly by clinical evidence of hypoperfusion. Hemodynamic monitoring reveals a PAOP less than 18 mm Hg and a cardiac index of less than 2.2 L/minute/m2. The class III subgroup accounted for approximately 15% of patients with acute MI and was associated with a 23% mortality rate. Patients in this subgroup may be extremely difficult to manage on clinical grounds, and treatment can be facilitated by invasive hemodynamic monitoring to establish the volume status. Relative hypovolemia is determined by measuring the pulmonary artery occlusion pressure, which falls below that of the ideal wedge as predicted in ischemic states. Excessive diuresis is extremely problematic in this group of patients and may excessively decrease cardiac output because of the pre-existent relative hypovolemia. Class III patients require restoration of intravascular volume to increase filling pressures to a degree that ensures adequate cardiac output and organ perfusion.Class IV patients demonstrated elevated PAOP in excess of 18 mm Hg and a depressed cardiac index of less than 2.2 L/minute/m2 and frequently manifested signs of cardiogenic shock with clinical evidence of organ hypoperfusion and dysfunction. This subgroup accounted for approximately 35% of patients with MI and was associated with an in-hospital mortality rate of approximately 50%. Class IV patients may have a mechanical defect such as acute mitral
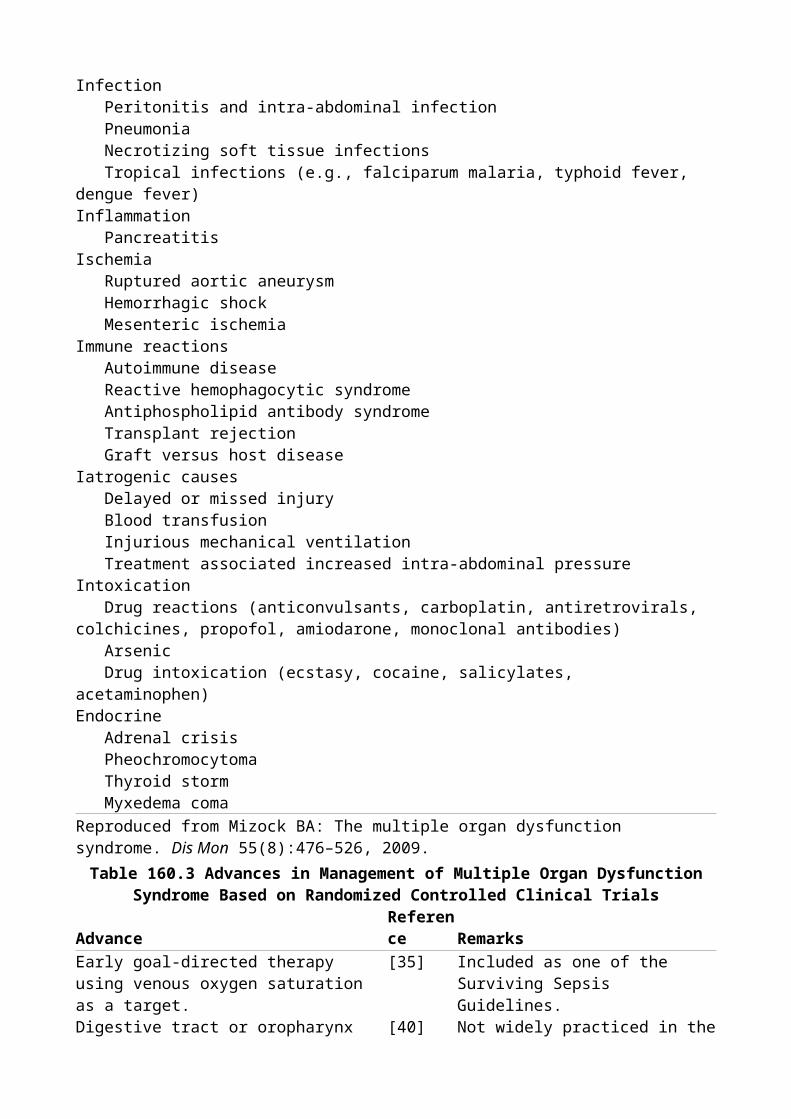
insufficiency, free wall rupture, or VSD underlying the acute myocardial infarction; these are discussed separately. Oxygenation with the potential assisted ventilation in addition to inotropic and judicious use of vasodilator support is the recommended therapy in these subgroups.Right Ventricular InfarctionAlthough isolated right ventricular (RV) infarction is rare, evidence of RV infarction and RV dysfunction is found in up to half of all infarcts and is clinically significant in nearly half of all inferior infarcts (8,9). The clinical diagnosis of RV infarction should be considered when elevated jugular venous pressure is accompanied by hypotension while the lung fields are clear. But the diagnosis may be difficult to establish clinically unless hemodynamic measurements, special electrocardiographic leads, echocardiography, or nuclear imaging are performed (10). Right-sided precordial leads obtained by electrocardiography that demonstrates at least 1-mm ST elevation is approximately 70% sensitive in the diagnosis of RV infarction and confers a particularly poor prognosis (11). Echocardiography is an easily obtainable noninvasive study that demonstrates RV dilation and impairment of wall motion of the right ventricle. Radionuclide angiography currently is considered to be the most sensitive means to diagnose RV infarction, although more recent data suggest that magnetic resonance imaging is comparable (12,13). A decrease in RV ejection fraction that is associated with wall motion abnormalities is more than 90% sensitive in the diagnosis of an RV infarction. Hemodynamic studies that are supportive of significant ischemic involvement of the right ventricle are manifest by increases in right atrial pressures plus demonstration of resistance to diastolic filling, as shown by blunting of the y-descent that follows tricuspid valve opening. A “square root” sign or “dip and plateau” pattern in the diastolic pressure curve is commonly demonstrated in RV infarctions but is not specific and may be associated with pericardial tamponade or restrictive cardiomyopathy (14).The Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock (SHOCK) trial registry reported on the clinical characteristics of patients presenting with isolated RV shock (15). Patients with RV shock compared to LV shock were younger and had a lower prevalence of previous MI (25.5% vs. 40.1%), a lower prevalence of anterior MI (11% vs. 59%), and less multivessel disease (34.8% vs. 77.8%). As expected, the infarct-related vessel involved the right coronary artery more in RV shock (96% of cases) versus LV shock (27% of cases). These patients had a shorter median time between myocardial infarction and the diagnosis of shock (2.9 vs. 6.2 hours) compared to patients with left ventricular shock. Right atrial pressure was a highly significant distinguishing factor of right from left ventricular shock (mean pressure 23.0 ± 9.9 vs. 14.2 ± 7.4, p = 0.0001), while all other hemodynamic measures were similar. Interestingly, in-hospital mortality was not significantly different between RV and LV shock (53.1% vs. 60.8%). Improvement in survival due to revascularization was similar between groups and multivariate analysis revealed that RV shock was not an independent predictor of lower in-hospital mortality (odds ratio 1.07, 95% confidence interval 0.54–2.13). This similarity in survival was despite patients with RV shock being younger; thus, RV shock may carry a worse prognosis.Cardiogenic shock in patients with RV infarction frequently represents a substantial loss of functioning myocardium and P.839carries a poor prognosis. RV infarction accompanied by cardiogenic shock is frequently associated with a variety of conduction abnormalities, including a high-grade atrioventricular block or significant rhythm disturbances. The treatment of RV infarction complicated by cardiogenic shock centers around maintaining RV filling pressures and assurance of adequate volume. Hemodynamic measurements may facilitate the estimate of volume loading required. Nitrates, diuretics, and other predominantly vasodilating compounds should be avoided. Atrial fibrillation is frequently poorly tolerated by these patients and may require immediate electrical cardioversion. The use of digitalis in acute RV infarction, even in the presence of atrial fibrillation, is controversial. Adequate inotropic support with vasodilating inotropic agents such as dobutamine is used if cardiac output fails to optimize after adequate volume loading. Percutaneous revascularization should be considered as it has been shown to improve outcomes (16).
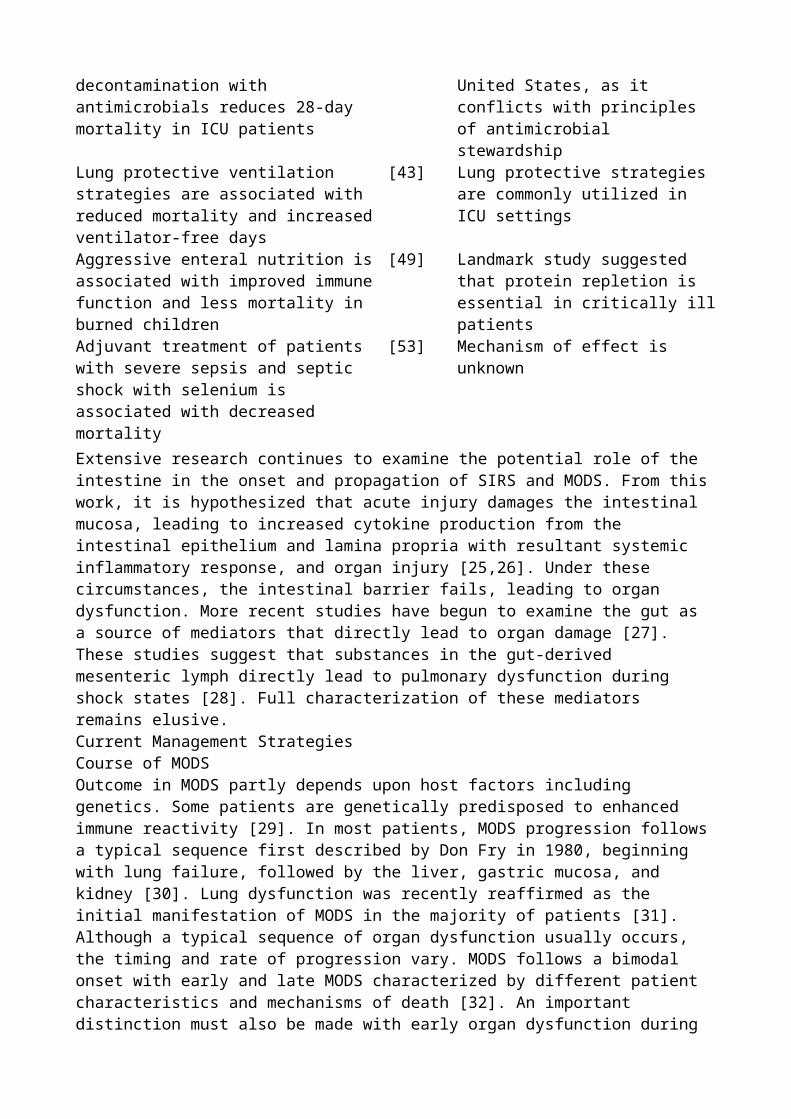
Mechanical DefectsA variety of mechanical defects may be associated with cardiogenic shock in the peri-infarction stage (Table 56.3). Myocardial infarction resulting in cardiogenic shock from the appearance of mechanical defects such as acute mitral insufficiency, VSD, or free wall rupture represents a major complication and requires aggressive diagnostic and therapeutic interventions if the patient is expected to survive. Despite improvements in imaging techniques plus mechanical assist devices and emergency surgery, the mortality from these complications remains extremely high.Acute Mitral InsufficiencyThe mitral valve is a complicated apparatus and consists of the valvular annulus, leaflets, chorda tendineae, and papillary muscles plus potential functional alterations from involvement of the adjacent myocardium. Abnormalities affecting any of the components of the mitral valve may result in acute or chronic mitral insufficiency. The mitral valve annulus may be dilated and contribute to mitral insufficiency, although this complication is primarily associated with cardiomyopathies or connective tissue diseases such as Marfan syndrome rather than an acute myocardial infarction. Calcification of the mitral valve annulus is common in the elderly and may alter coaptation of the mitral valve leaflets and result in mitral incompetence.
Table 56.3 Complications of myocardial infarction
CharacteristicVentricular septal rupture
Papillary muscle rupture Papillary muscle dysfunction
Incidence Unusual Rare CommonMurmur Type Pansystolic Early to pansystolic Variable Location Left sternal border
(95%)Apex → axilla (50%)Apex
Thrill >50% Rare NoClinical presentationLeft and right
ventricular failureProfound pulmonary edema
None to moderate left ventricular failure
Catheterization O2 step-up in right
ventricle
Large left atrial V wave
Mild to moderate elevation of left atrial pressure
With permission from Crawford MH, O'Rourke RA. The bedside diagnosis of the complications of myocardial infarction. In: Eliot RS, ed. Cardiac Emergencies. Mount Kisco, NY: Futura; 1962.Acute mitral insufficiency caused by involvement of the valvular leaflets is associated with infective endocarditis from necrotizing organisms such as Staphylococcus aureus or Enterococcus, resulting in destruction of the valvular apparatus. Traumatic penetrating injuries that involve the valve itself are rare. Rupture of the chorda tendineae may also be seen in endocarditis or a variety of connective tissue diseases, including myxomatous degeneration or Marfan syndrome.Chordal rupture that results in severe impairment of left ventricular function depends on the number of involved structures and the rapidity with which the rupture occurs. Mitral insufficiency in the peri-infarction state may result from involvement of the surrounding myocardium or papillary muscles. Papillary muscles located adjacent to the infarction zone may simply become dysfunctional because of alteration of synchrony of contraction related to ischemia or frank rupture from ischemic necrosis.The degree of mitral insufficiency is a function of the degree of involvement and anatomic competence. The two papillary muscles (posteromedial and anterolateral papillary muscles) have different ischemic vulnerabilities because of the blood supply from the coronary arteries. The anatomic vascular supply represents end arteries that are solely supplied by terminal portions of the coronaries, thus rendering the papillary muscles vulnerable to ischemic involvement during an acute myocardial infarction. Papillary muscle dysfunction may result from intermittent ischemia during unstable angina or myocardial infarction with involvement of the adjacent myocardium (17). Papillary muscle dysfunction is characterized by mild flow murmurs, which may be grade I or grade II by auscultation. The anterolateral papillary muscle has a dual blood supply, which provides partial protection during ischemia. The diagonal branches of the left anterior descending and
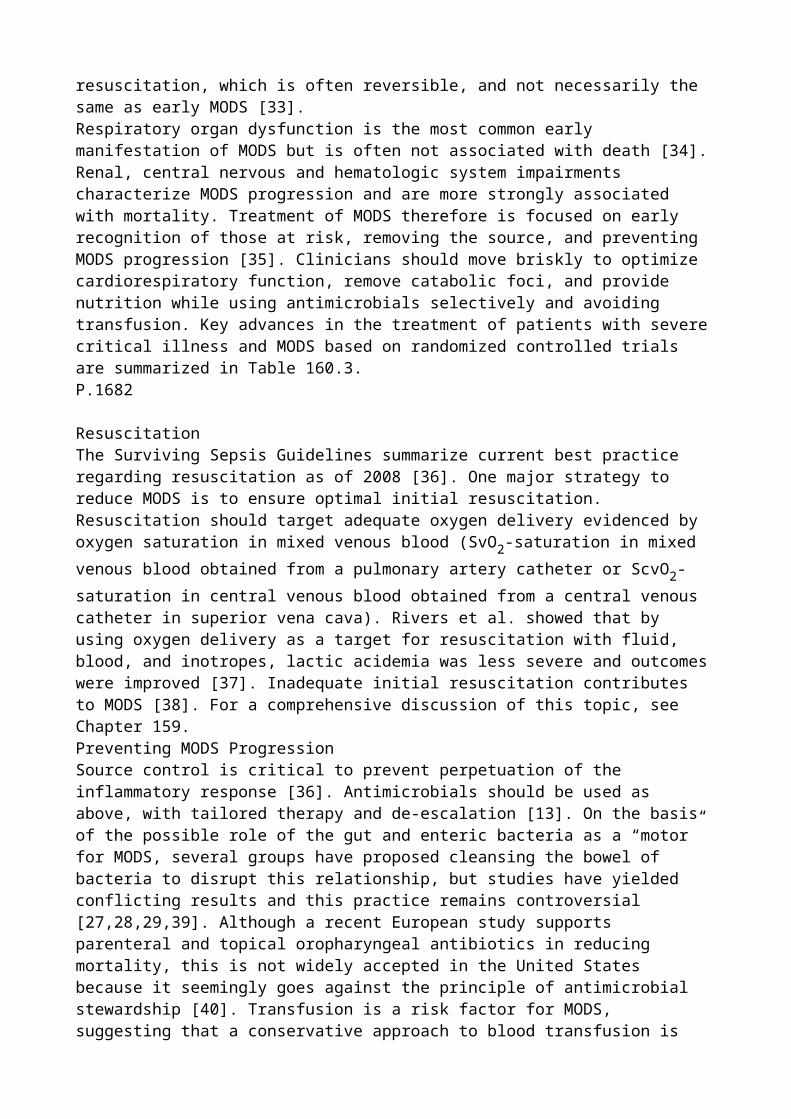
marginal branches from the circumflex supply blood to the anterolateral papillary muscle. The posteromedial papillary muscle is generally supplied solely from the posterior descending branch of the right coronary artery, increasing its vulnerability to ischemic-related dysfunction.P.840Significant ischemia involving the papillary muscle that results in complete rupture with fulminant mitral insufficiency is generally fatal because of the marked volume load ejected retrograde into the left atria and pulmonary venous bed (18). However, if the major ischemic-related necrosis is distal and only involves rupture of the head of the papillary muscle, the resultant mitral insufficiency may be tolerated hemodynamically long enough to allow recognition, proper diagnosis, and surgical intervention. Mild ischemic involvement of the papillary muscle may be increased in hemodynamic significance in the presence of pre-existing left ventricular dilation, which alters the ability of the mitral leaflets to coapt. Severe ischemic-related mitral insufficiency is more frequently a result of posteromedial papillary muscle necrosis resulting from inferior or posterior myocardial infarctions, although one third of cases may result from anterior infarction (19,20). Less than half of cases present with electrocardiographic evidence of ST elevation or Q waves (20). Right ventricular papillary muscle rupture may occur but is uncommon. Involvement of papillary muscles in the right ventricle results in tricuspid insufficiency, which if severe may result in right ventricular failure.Papillary muscle rupture is a relatively uncommon complication and occurs in approximately 1% of patients having an acute ischemic event. The incidence has decreased in the thrombolytic era (21). After acute MI with cardiogenic shock, the incidence of acute severe mitral regurgitation is 6.9% (22). The peak incidence of papillary muscle rupture is within the first week, with the majority occurring between days 3 and 5 after an acute MI. The diagnosis of papillary muscle rupture may be suspected on physical examination and has been facilitated with the advent of hemodynamic monitoring and echocardiography.The physical examination in acute mitral insufficiency secondary to papillary muscle rupture differs from the findings associated with chronic valvular regurgitation. In the acute setting a palpable thrill is uncommon and the radiation of the murmur differs from chronic conditions. The systolic murmur is soft, is decrescendo, generally ends before the second heart sound, and is best audible at the base of the heart as opposed to the apex with radiation to the neck or the top of the head.Echocardiography and Doppler ultrasound has been a major advance in the diagnosis of acute mitral insufficiency and its clinical separation from other mechanical lesions associated with a new murmur (23). The left atrium and left ventricle are generally of normal size, and the ejection fraction is increased and frequently hyperdynamic. The mitral leaflet flails and may prolapse into the left atrium. Doppler ultrasound with color flow study determines the presence and severity of mitral insufficiency and presence of an intracardiac shunt and quantifies the degree of mitral regurgitation. Data from the Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock (SHOCK) trial, which randomized patients with cardiogenic shock within 36 hours of an acute myocardial infarction, has shown that the severity of mitral regurgitation quantified by Doppler echocardiography is an independent predictor of survival (24).Pulmonary artery catheter placement with measurement of PAOP and cardiac output is useful in mitral insufficiency. The presence of a regurgitant wave in the PAOP tracing may be visible in acute mitral regurgitant lesions, especially when there is no evidence of a step-up in oxygen concentration in the right atria or right ventricle. Pulmonary artery catheterization is not necessary for diagnosis, but the use of invasive monitoring allows optimization of cardiac output, filling pressures, and adjustment of inotropic, vasodilator, and diuretic therapy on the basis of induced changes in pressures.Ventricular Septal DefectRupture of the interventricular septum may present in a similar clinical manner as mitral insufficiency with the abrupt onset of congestive heart failure plus a new murmur, making the two conditions difficult to separate on clinical grounds. Rupture of the interventricular septum also occurs in the first week after the acute ischemic event with a peak incidence occurring between days 3 and 5. The prevalence rate of acute VSDs after an infarction is difficult to accurately determine
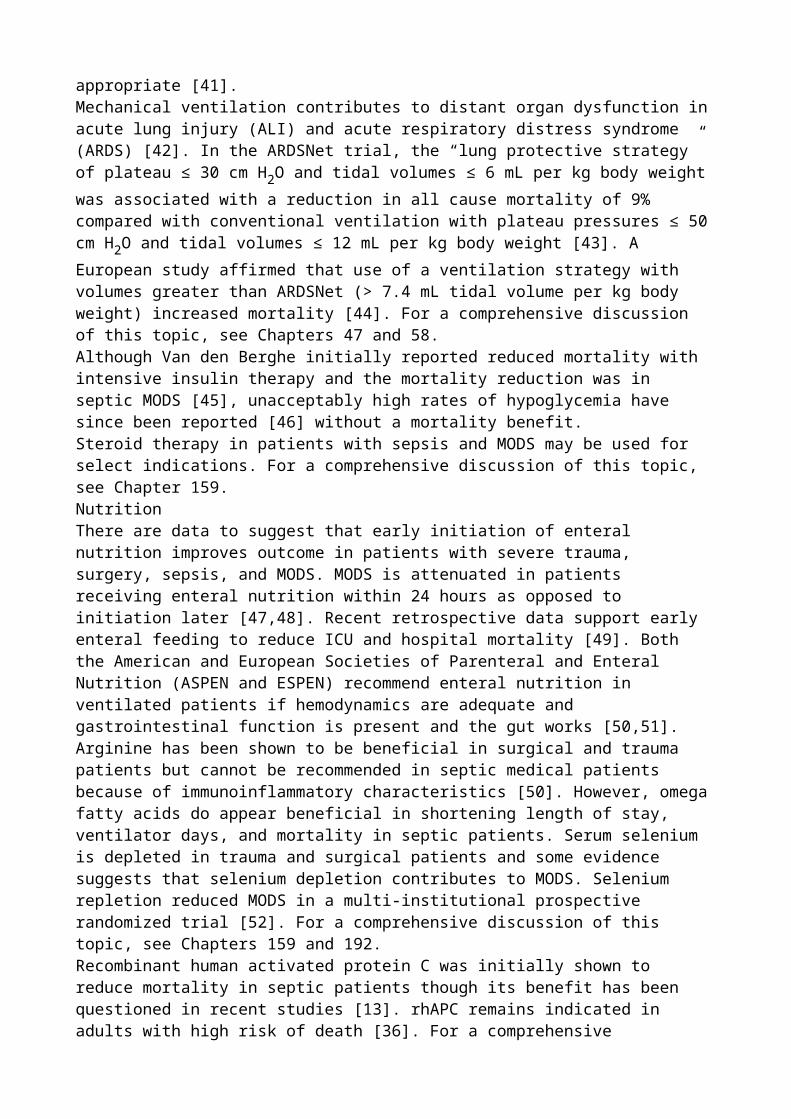
but occurs within the range of 0.5% to 2.0% and is the cause of death in approximately 5% of all fatal MIs. Incidence of VSD as a cause of cardiogenic shock after acute myocardial infarction in the SHOCK trial registry was 3.9% (22). Blood supply to the septum is supplied by septal perforating branches of the left anterior descending vessel and acute VSD is more common in anterior myocardial infarctions. These patients frequently have multivessel disease and are older patients experiencing an initial myocardial infarction (25).The diagnosis of acute VSD may be inferred on clinical grounds but frequently requires more sophisticated evaluation to accurately diagnose and quantify the defect, which is located in the muscular septum and may be multiple. The physical examination in acute VSD depends on the magnitude of the shunt, which is, in turn, a function of the size of the ventricular defect, right ventricular compliance, pulmonary artery pressures, and inotropic state. A significant VSD is associated with the characteristic findings of shock in addition to a new holosystolic murmur associated with a precordial thrill. A precordial thrill may be palpated in approximately 50% of patients with an acute VSD and is a function of the magnitude of pressure gradient between the two chambers.The diagnosis of VSD and its separation from acute mitral insufficiency has been facilitated by the advent of noninvasive and invasive diagnostic procedures. Two-dimensional echocardiography combined with Doppler flow study generally identifies a significant defect (26). Contrast echocardiography using microbubble techniques also may aid in the diagnosis of acute VSD and establish the presence of an intracardiac shunt. Pulmonary artery catheterization demonstrates the absence of a V wave in the pulmonary wedge tracing and an increase in oxygen saturation by ~10% in the right ventricle compared with the right atrium. The mortality rate for septal defects is significant, with approximately 25% of patients dying within the first 24 hours and a 50% mortality rate at 1 week. Less than 10% survive 1 year when treated solely with medical therapy (27). When occurring in the setting of cardiogenic shock, in-hospital mortality has been reported as high as 87% (22).Free Wall Rupture and TamponadeFree wall rupture is a major complication of myocardial infarction and is difficult to diagnose premortem. The prevalence of this complication is unknown but may occur in up to 8% of all myocardial infarctions with approximately one third occurring in the first 24 hours after the onset of the ischemic event and the peak incidence between days 5 and 7 (28). The SHOCK trial registry reported a 1.4% incidence of free wall rupture as a cause of cardiogenic shock after acute MI (22). P.841Rupture of the free wall is a major cause of mortality in acute ischemic events and is associated with large transmural infarcts with inadequate collateral circulation. This serious complication occurs more commonly in elderly hypertensive patients. Involvement of the left ventricle is the rule, although free wall rupture involving the right ventricle has been reported. Rupture of the free wall is frequently associated with the ventricular remodeling process in which a segmental infarction results in elevated left ventricular and diastolic pressure with expansion of the infarcted area. Expansion involves thinning of the affected area with regional hypertrophy in the adjacent region surrounding the infarct. A disproportionate dilatation occurs in the infarcted area and the risk of free wall rupture is enhanced with high shearing forces and elevated pressures. Free wall rupture generally occurs in the border zone between the infarcted area and the normal surrounding myocardium. The advent of thrombolytic therapy has been postulated to potentially increase the risk of free wall rupture, although this has not been definitely confirmed. Thrombolytic therapy may actually minimize the extent of myocardial necrosis and decrease free wall rupture. The use of agents such as corticosteroids, previously used to blunt inflammatory response and infarct size, has been associated with increased risk of free wall rupture.Cardiac rupture is a catastrophic event resulting in sudden cardiac death unless a pseudoaneurysm forms. Hemopericardium with cardiac tamponade is difficult to diagnose early enough to institute definitive therapy. Cardiac tamponade after acute myocardial infarction also may be secondary to hemorrhagic pericarditis, but massive hemopericardium is usually due to cardiac rupture with rapid
development of electromechanical dissociation and death. The diagnosis of free wall rupture is difficult but should be suspected with sudden hypotension, elevated jugular venous pressures, muffled heart sounds, and a pulsus paradoxus. Echocardiography can document the presence of pericardial fluid and occasionally demonstrates the perforated free wall (29,30). The classic signs of tamponade are present on echocardiography and are caused by the rising intrapericardial pressure compressing the right atrium and right ventricle, resulting in equalization of pressures and right ventricular diastolic collapse. Definitive therapy involves pericardiocentesis plus volume and pressure support with early surgical intervention being necessary for salvage. Untreated free wall rupture is universally fatal, although isolated instances of successful aggressive intervention with surgical therapy have been reported (31).Left Ventricular AneurysmLeft ventricular aneurysm is a relatively common complication of MI and may occur in up to 15% of survivors (32). A true aneurysm has a wide base with the ventricular walls composed entirely of myocardium, compared with a pseudoaneurysm, which generally has a narrow base with the walls consisting of pericardium and thrombotic debris. True aneurysms have a relatively low risk of free wall rupture but are associated with increased mortality due to sudden death from ventricular arrhythmias, emboli from mural thrombus, and progressive loss of left ventricular function (33). Aneurysms may develop early in the postinfarction period and can be asymptomatic or present with significant deterioration of left ventricular function. The presence of left ventricular aneurysm may be inferred by persistent ST elevation in the absence of chest pain or enzyme leakage (34).Echocardiography demonstrating dyskinesis is a valuable tool in diagnosing aneurysms, as is left ventricular angiography. Left ventricular angiography demonstrates paradoxic systolic distention during ventricular contraction. Successful treatment of the aneurysm may be achieved with resection of the involved myocardium, frequently in combination with saphenous vein or mammary artery bypass grafting because of the high associated prevalence of multivessel coronary artery disease. Surgical resection has been advocated in the presence of arrhythmias to eliminate the substrate for ventricular tachycardia, but electrophysiologic mapping techniques are necessary to demonstrate that the origin of the arrhythmia arises from the left ventricular aneurysm.Clinical ManifestationsThe clinical manifestations of cardiogenic shock are a function of the underlying cause, and mechanical defects must be aggressively sought because of the need for definitive therapy. Clinical recognition of the shock syndrome frequently requires prompt and aggressive stabilization procedures to be instituted before the definitive diagnosis of the underlying etiology (Fig. 56.2). A history and physical examination should be obtained with special attention to mental status, jugular venous pulsations, quality and intensity of heart sounds, presence and localization of a murmur, and presence of oliguria. Diagnostic tests such as electrocardiogram, portable chest radiograph, arterial blood gases, and echocardiography frequently provide adequate clinical information to make a diagnosis and initiate stabilization therapy. A quarter of patients presenting with cardiogenic shock secondary to predominant left ventricular dysfunction do not have evidence of pulmonary congestion (35).TherapyPercutaneous RevascularizationPrior to 1999, interventions for the management of cardiogenic shock complicating acute MI were not systematically studied. The landmark SHOCK trial demonstrated that a strategy of early revascularization by angioplasty or surgery reduced mortality from 63% to 50% at 6 months (36). This finding has resulted in a major paradigm shift in the management of cardiogenic shock. The first branch-point in the decision algorithm is whether or not shock is present in the setting of an acute MI. If shock is present, patients should undergo immediate coronary angiography with percutaneous intervention if feasible.The SHOCK trial studied patients with onset of shock within 36 hours of an MI and randomized the patients to immediate revascularization versus initial medical stabilization. Almost all patients required inotropes or vasopressors. Treatment in the revascularization group (64% of patients) was
angioplasty or stenting (stents were not available at the beginning of the trial in 1993, but were actively used by the end of the trial in 1998) and coronary artery bypass graft surgery in 36%. In a subgroup analysis, survival was similar between percutaneous and surgically revascularized patients (55.6% vs. 57.4% at 30 days and 51.9% vs. 46.8% at 1 year, respectively) despite a higher incidence of diabetes and multivessel disease in those patients surgically revascularized (37).P.842Thrombolytic therapy was used in 49% of patients in the revascularization group and in 63% of the medical therapy group. There was no difference in survival at 30 days (53.3% in the revascularization group vs. 44.0% in the medical therapy group), likely a result of improved medical therapy. Age older than 75 years was associated with significantly higher 30-day mortality. Follow-up reports have shown persistent benefit to early revascularization with survival rates of 47% versus 34% at 1 year and 33% versus 20% at 6 years (38,39). Of the patients surviving to hospital discharge (143/302), 6-year survival was 62% versus 44% (39).
Figure 56.2. Management algorithm for cardiogenic shock. ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; PA, pulmonary artery.An exciting aspect of the SHOCK trial was the registry that was created from patients screened for enrollment but not randomized, whose data was reported separately in a dedicated supplement to the Journal of the American College of Cardiology in September 2000. This registry described 1,190 patients and is the largest prospectively collected database for cardiogenic shock (22). Etiology of shock from the registry was left ventricular failure (78.5%), acute severe mitral regurgitation (6.9%), ventricular septal rupture (3.9%), isolated right ventricular shock (2.8%), and tamponade from free wall rupture (1.4%). Electrocardiographic site of infarction was anterior (55%), inferior (46%), posterior (19%), lateral (32%), and apical (11%), with multiple sites present in half of the cases. There was ST elevation, Q waves, or new left bundle branch block in 79% of cases. Systolic blood pressure averaged 88 mm Hg with a mean heart rate of 96 beats per minute. Of the subset of patients with invasive hemodynamics measured, PAOP was 23 mm Hg, cardiac index was 2.08 L/minute/m2, and left ventricular ejection fraction was 33%. In-hospital mortality averaged 60% and ranged from 55% for acute severe mitral regurgitation, isolated right ventricular shock, and tamponade to 87% for ventricular septal rupture. Of the 717 patients who underwent coronary angiography, 15.5% had significant left main stenosis and 53.4% had three-vessel disease. Coronary artery disease severity also correlated with in-hospital mortality: No or single-vessel disease was associated with a 35% mortality rate as compared with three-vessel disease with a mortality rate of 50.8% (40).Since the SHOCK trial, stenting has replaced angioplasty alone as the primary treatment for ischemic coronary artery disease due to its reduced incidence of restenosis. One recent case series has shown that stenting for cardiogenic shock decreased mortality compared to angioplasty alone (from 68% to 43%) (41). Primary coronary artery stenting is now recommended for patients with ST elevation or left bundle branch block who develop shock within 36 hours of acute myocardial infarction and are suitable for revascularization that can be performed within 18 hours of shock onset (1). Thrombolytic therapy may be used if early revascularization is not available (2).While drug-eluting stents, which slowly elute a pharmacologic agent (currently either sirolimus or paclitaxel), are now widely used instead of bare metal stents due to their proven efficacy in reducing the incidence of restenosis, to date they have not been studied in the setting of cardiogenic shock (42,43).Pharmacologic Limitation of Infarct SizeSeveral pharmacologic interventions have been used during acute myocardial infarction to minimize the extent of irreversible ischemic damage and decrease the likelihood of subsequent development of cardiogenic shock. Quantitative measurements of the extent of myocardial damage by electrocardiographic mapping and creatine kinase (CK) release are imprecise and frequently limit quantitative assessment of the potential therapeutic impact of pharmacologic interventions. Calcium channel blockers, β-blockers, and nitrates have been

P.843the main agents that have undergone clinical analysis to minimize myocardial damage, whereas a variety of experimental or uncommonly used therapies have been evaluated in small-scale clinical trials. Nitrates are complex pharmacologic agents with arterial and venodilating activity in addition to other potential beneficial effects, such as alteration of prostacyclin metabolism. Nitrates, when administered as topical, oral, or sublingual agents, are predominately venodilators with subsequent venous pooling, decreased venous return, and lowering of PAOP. Reduction in venous return and optimization of PAOP decrease left ventricular volume and improve subendocardial perfusion, thus reducing wall stress with the potential for minimizing infarct extent. Nitrates also have effects on systemic vascular resistance and epicardial coronary arteries, with resultant reduction of impedance to left ventricular ejection and increase in coronary blood flow.Intravenously administered nitroglycerin has a more balanced arterial and venodilating effect. Clinical trials demonstrate that intravenous nitroglycerin administered at a level to decrease mean aortic pressure by 10% (44) results in a decrease in extension of MI and improves left ventricular ejection fraction and survival (45). Intravenous nitrates minimize the magnitude of infarct size as monitored by CK, and alter infarct expansion with reduction in the subsequent remodeling process and progression to congestive heart failure. Intravenous nitrates are potent vasodilators and require careful blood pressure monitoring to prevent significant hypotension and paradoxical bradycardia. Nitrates may result in a beneficial redistribution of coronary flow to the subendocardium without the coronary steal syndrome, a major detriment of other potent intravenous vasodilators such as nitroprusside.Calcium channel blockers are important agents in managing patients with classic and vasospastic angina. The calcium channel blocking agents decrease systemic vascular resistance, decrease oxygen demand, and increase coronary flow, improving the balance between supply and demand. At pharmacologic doses, these agents also may have other potentially beneficial effects including antiplatelet activity.Despite the documented beneficial effect of these agents in hypertension and angina, calcium channel blockers have not been proven to be beneficial in the treatment of MI and do not definitely limit infarct size. Studies using nifedipine have been unable to demonstrate benefit in patients with acute MI. Diltiazem has been advantageous in non–Q-wave infarction in the Diltiazem Reinfarction study (46). However, the Multicenter Diltiazem Postinfarction trial was not able to document a benefit to the administration of diltiazem in the postinfarction state when compared with placebo (47). Subgroup analysis demonstrated a mortality benefit with diltiazem therapy when no pulmonary congestion was present. However, mortality was increased when diltiazem was administered to subjects whose infarction was complicated by pulmonary congestion, implying that this agent should not be used in patients with cardiogenic shock. Studies performed in Denmark using intravenous verapamil followed by oral administration did not demonstrate a benefit. Later studies using only oral verapamil demonstrated a mortality reduction, although these trials have not been reconfirmed (48). Currently, the evidence for using calcium channel blockers for the treatment of acute MI to limit infarct size and progression to cardiogenic shock is limited.β-Adrenergic blocking agents have been used in treating hypertension, atrial fibrillation, and a variety of ischemic conditions. β-Blockers act predominantly by decreasing myocardial oxygen demand caused by the negative chronotropic and inotropic activities of these agents. β-Blockers may have several other potentially beneficial effects including antiplatelet activity, regression of left ventricular hypertrophy, and reduction in sudden cardiac death. Clinical trials using β-blockade in acute MI have yielded conflicting results. The Goteborg trial administered metoprolol or placebo to subjects having an acute myocardial infarction and demonstrated a significant reduction in mortality at 90 days in the group randomly assigned to β-blocker therapy (49). Early administration of metoprolol was associated with a reduction in estimated infarct size, which presumably has an effect on early and long-term survival. Despite the fact that β-blockers are not commonly used as antiarrhythmic agents, there was a documented decrease in sudden cardiac death in the β-blocker group, which has been shown to be secondary to an increase in the ventricular fibrillatory threshold.
The Metoprolol in Acute Myocardial Infarction trial was able to demonstrate that the early administration of intravenous metoprolol followed by oral maintenance dose in acute MI was associated with a decrease in mortality in a high-risk subgroup of infarct patients (50). A subgroup study of the Goteborg Metoprolol trial found that early treatment with metoprolol in patients with suspected acute MI and signs of heart failure resulted in significantly reduced mortality at 3 months (10% vs. 19%), which persisted to 1 year (14% vs. 27%), compared to those who did not receive metoprolol (51). Propranolol, a noncardioselective β-blocker, has not uniformly been demonstrated to decrease mortality or limit infarct size when administered early in acute MI patients. However, the Beta-Blocker Heart Attack trial demonstrated reduced mortality when propranolol was administered after the acute phase of the infarction had subsided (52). Intravenous atenolol was studied in the First International Study of Infarct Survival Trial and demonstrated a 15% reduction in the early mortality of infarct patients who were given oral atenolol after the intravenous loading doses (53). β-Blockers also have been combined with thrombolytic therapy to limit infarct size. The Thrombolysis in Myocardial Infarction trial (TIMI II-B) studied the impact of three 5-mg boluses of metoprolol administered at 5-minute intervals followed by oral metoprolol compared with thrombolysis plus oral metoprolol. The TIMI II-B trial demonstrated a decrease in nonfatal reinfarctions and recurrent ischemic episodes in the group who received immediate intravenous metoprolol followed by oral therapy compared with the delayed subgroup. More recently, the CAPRICORN (Carvedilol Post Infarct Survival Control in Left Ventricular Dysfunction) trial studied carvedilol (6.25–25 twice per day in addition to standard therapy of aspirin, angiotensin converting enzyme [ACE] inhibition, and thrombolysis) versus placebo in a high-risk group of acute MI patients (n = 1,959) with an LV ejection fraction of ≤40%. Patients were treated for a mean of 1.3 years. All-cause mortality was lower in the carvedilol group than in the placebo group (54). Patients who had echocardiography demonstrated a significantly higher LV ejection fraction and decreased LV end-systolic volume in the carvedilol group at 6 months (55). Another post hoc analysis of the CAPRICORN study found that carvedilol suppressed atrial arrhythmias (2.3% vs. 5.4%) as well as ventricular arrhythmias (0.9% vs. 3.9%) compared to the control group (56). The beneficial effect on ventricular remodeling, in P.844addition to the antiarrhythmic effect, may be one of the mechanisms by which carvedilol decreased mortality after acute MI in patients treated with ACE inhibitors. Use of β-blockers in acute myocardial infarction, while now standard of care, must be undertaken with caution because of the potential of precipitating atrioventricular block, reactive airways disease, and hypotension (57).ACE inhibitors have been administered orally and intravenously in clinical trials to halt progression to congestive heart failure in the SAVE (Survival and Ventricular Enlargement) and Consensus-II (Cooperative New Scandinavian Enalapril Survival Study) trials. The SAVE study used captopril in over 2,000 patients who had an acute anterior MI when enrolled during the period from 3 to 16 days after the acute myocardial event (58). All patients with ejection fractions <40% were randomized to receive oral captopril or a placebo. Patients receiving captopril demonstrated less congestive heart failure, fewer recurrent MIs, fewer hospitalizations, and improved mortality over a 42-month period. The Consensus-II trial used intravenous enalapril in the early phase of infarction followed by oral enalapril, but there was no mortality benefit when compared with placebo (59). A review of the major post-MI heart failure trials such as SAVE, AIRE (Acute Infarction Ramipril Efficacy), and TRACE (Trandolapril Cardiac Evaluation), between 1992 and 1995, calculated that ACE inhibitors produced a relative risk reduction of 16% while β-blockade in addition to ACE inhibition in the CAPRICORN trial demonstrated an additional relative risk reduction of 23% (60). Oral ACE inhibitors are attractive agents because of their effects on hemodynamics, microcirculation, and angiotensin-mediated vasoconstriction and should be administered especially in anterior infarcts with significant reductions in ejection fraction unless there are contraindications (hyperkalemia, known drug sensitivity).Selective aldosterone blockade with eplerenone for patients with LV ejection fraction of ≤40% after acute MI has been studied in one large, placebo-controlled trial, EPHESUS (Eplerenone Post-Acute
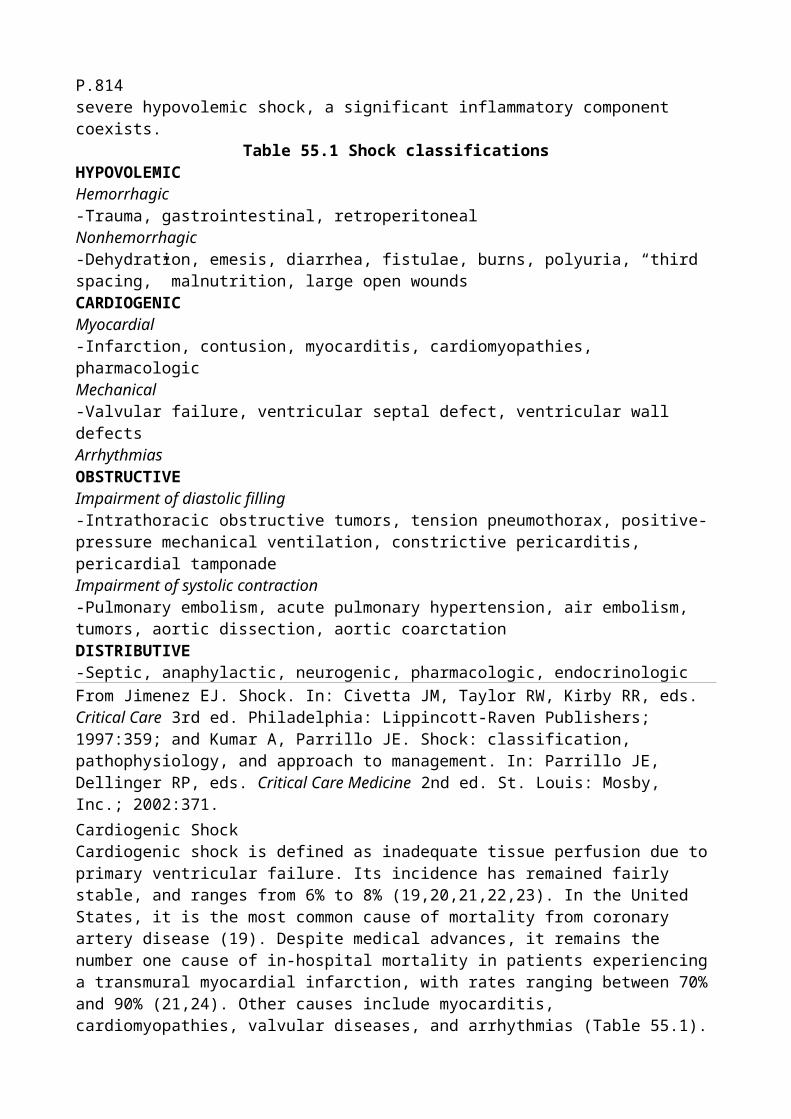
Myocardial Infarction Heart Failure Efficacy and Survival Study). Eplerenone (in addition to treatment with β-blockers and ACE inhibitors) reduced all-cause mortality by 15%, cardiovascular mortality by 17%, heart failure hospitalizations by 23%, and sudden cardiac death by 21% (61). These outcomes were even more marked in the subgroup of patients with LV ejection fraction of ≤30%. In this group, all-cause mortality was reduced by 21%, cardiovascular mortality by 23%, sudden cardiac death by 33%, and heart failure mortality or hospitalization by 25% (62).Angiotensin receptor blockade for LV ejection fraction of ≤40% after acute MI has been studied in the VALIANT (Valsartan in Acute Myocardial Infarction Trial) study (63). This was a multicenter, double-blind, randomized, active-controlled, parallel-group study comparing the efficacy and safety of long-term treatment with valsartan, captopril, and their combination in high-risk patients after MI. This compared three treatment groups consisting of patients receiving standard therapy plus valsartan (n = 4,909), valsartan plus captopril (n = 4,885), or captopril alone (n = 4,909). Valsartan treatment alone resulted in similar outcomes as captopril treatment alone and thus these agents can be used interchangeably. The combination of valsartan plus captopril increased the rate of adverse events (hypotension and renal dysfunction more commonly with valsartan; cough, rash, and taste disturbance more commonly with captopril) with no change in survival.Adjunctive antiplatelet therapy with the glycoprotein IIb/IIIa inhibitor abciximab during emergent coronary artery stenting for cardiogenic shock has been shown to reduce mortality from 43% to 33% in one case series (41). The glycoprotein IIb/IIIa inhibitor eptifibatide used for non–ST-elevation myocardial infarction or unstable angina in the PURSUIT (Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression in Using Integrelin Therapy) study has been shown to reduce 30-day mortality in the subset of patients developing cardiogenic shock (64). Clopidogrel in addition to aspirin is now standard of care after percutaneous coronary intervention and has been shown to decrease 1-year mortality in the setting of ST-elevation myocardial infarction (65). However, clopidogrel significantly increases the risk of postoperative bleeding in patients requiring surgical intervention.Several agents have been used in small studies as adjunctive therapy in acute MI but have not reached widespread clinical use. Myocardial damage may be potentiated by the presence of reactive oxygen radicals, and free radical scavengers such as superoxide dismutase or catalase may provide potential benefit. Free radical scavengers have been shown to be effective when administered before the onset of experimental infarcts and definitive clinical studies are currently ongoing.Glucose insulin potassium infusions (polarizing solution) have been used for several years to reduce infarct size by altering free fatty acid metabolism (66). Polarizing solution consists of 300 g of glucose, 50 units of regular insulin, and 80 mmol of potassium in 1 L of water delivered at 1.5 mL/kg/hour. Ejection fraction and wall motion abnormalities have been noted to improve after administering this solution, resulting in decreased mortality. Polarizing solution has not been studied extensively in double-blind, placebo-controlled trials and routine administration of this solution has not reached clinical acceptance.Hyaluronidase may have anti-inflammatory activity and modulate the immune response postulated to play some role in the extent of infarct size. Hyaluronidase has been administered in small clinical studies and was associated with improved mortality and decreased development of Q waves implying myocardial salvage. There are no large-scale clinical trials available (67).ThrombolysisThrombolysis induced by pharmacologic agents or direct angioplasty is an attractive treatment for re-establishing coronary perfusion to minimize the extent of myocardial infarction and progression to cardiogenic shock. The open artery hypothesis postulates that clinical outcome is dependent on maintaining adequate coronary perfusion to minimize ischemic damage mediated by vascular occlusion secondary to an intravascular thrombus. Recent trials of coronary thrombolysis, GISSI (Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto Miocardio), ISIS (International Study of Infarct Size), and GUSTO (Global Utilization of Strategies to Open Occluded Coronary Arteries), demonstrate the prevalence of cardiogenic shock in approximately 2% to 3% of acute MIs on arrival to the hospital with an additional 3% to 4% subsequently developing cardiogenic shock
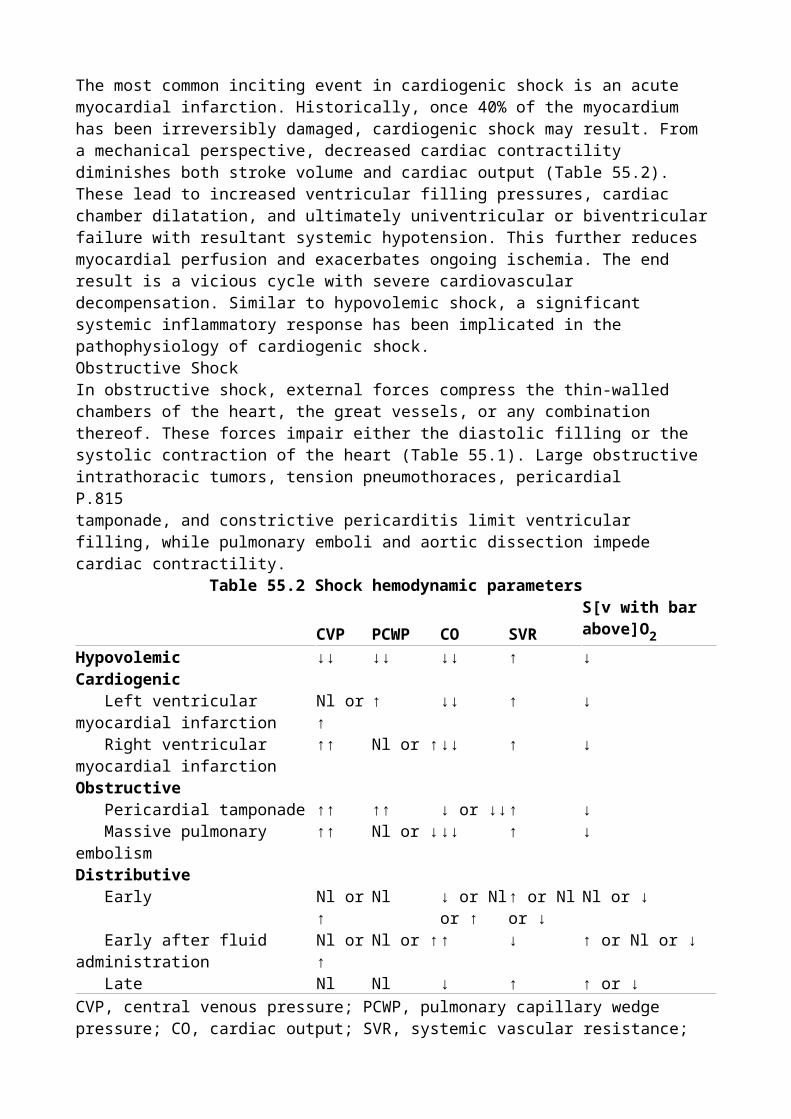
for a combined P.845total of 7% (68,69). Early progression to cardiogenic shock is characterized demographically by elderly patients and the presence of anterior infarctions, low ejection fractions, diabetes, and previous MIs. Despite the theoretical attractiveness of administering recombinant tissue plasminogen activators or streptokinase in patients with established or impending cardiogenic shock, the mortality associated with cardiogenic shock remains high despite thrombolytic therapy, with the survival rate being only 35% as reported in the GISSI-I and GISSI-II trials (70). Prompt administration of thrombolytic agents within the first hour of acute MI may result in improved survival rates if reperfusion of the infarct-related artery can be sustained. Low coronary perfusion pressures in cardiogenic shock may play a potential role in the poor clinical outcome of these patients after thrombolytic therapy.In vitro experimental infarct studies with reduced perfusion pressure have shown decreased diffusion of thrombolytic agents into clots with resultant impaired fibrinolysis (71). Enhanced pressure increases the rate of dissolution of an intravascular thrombus, implying that in cardiogenic shock with systemic hypotension, a reduced transcoronary pressure gradient may decrease efficacy of thrombolytic agents. The metabolic abnormalities associated with cardiogenic shock including lactic acidosis also may alter the conversion of plasminogen to plasmin and limit the efficacy of these drugs in clot lysis. Failure from lytic agents to sustain vascular patency in patients with cardiogenic shock is an indication for early cardiac catheterization and direct angioplasty if no contraindications exist. Persistent hypotension, nonevolving ST elevation, continuing clinical evidence of myocardial ischemia, CK elevations, and clinical instability are potential indications for rescue coronary angioplasty, which may result in increased survival (72). Rescue angioplasty has not been systematically studied in randomized controlled trials comparing it to thrombolytic therapy. If thrombolytic therapy does not result in establishment of coronary perfusion, angioplasty should be considered as a therapeutic option. The SHOCK trial reported that 49% of patients in the revascularization group received thrombolytic therapy and the early intervention group had a survival benefit (see section above) (36). Additionally, the SHOCK trial reported a survival benefit due to thrombolytic therapy (in-hospital mortality of 54% vs. 64%) (73). Cardiogenic shock secondary to mechanical defects such as papillary muscle dysfunction also has been treated successfully with percutaneous transluminal coronary angioplasty (PTCA), resulting in improved mitral regurgitation with resolution of cardiogenic shock (74).Thrombolytic agents should be administered to all patients with acute MI who demonstrate evidence of the shock state if there are no contraindications and availability of a cardiac catheterization laboratory is >90 minutes. Failure of evidence of reperfusion is an indicator for rescue angioplasty.Pharmacologic AgentsInotropic AgentsThe effectiveness of various inotropic agents in cardiogenic shock depends on the cause and underlying pathophysiologic mechanism of the shock state. With systemic hypotension, adequate perfusion of the coronary arteries must be maintained (Fig. 56.3).DopamineDopamine is an endogenous catecholamine with positive inotropic properties secondary to stimulation of α- and β-receptors plus dopamine receptors, which have been divided into two subtypes: DA1 and DA2 (75,76). DA1 receptors are postsynaptic and induce dilation of the
coronary, renal, and mesenteric vasculature. DA2 receptors are located in autonomic ganglia and in
the postganglionic sympathetic nervous system. Stimulation of DA2 receptors blocks the release of
endogenous catecholamines from intraneuronal storage sites. The effect of dopamine on α and β activity is dose related. Low infusion dosages of dopamine (2–5 µg/kg/minute) result in positive inotropic activity secondary to stimulation of the β1 receptors. α-Receptor stimulation occurs at
dosages above 10 µg/kg/minute and results in a secondary increase in systemic vascular resistance
caused by peripheral vasoconstriction. In addition to the inotropic effect, dopamine results in increased atrioventricular conduction from adrenergic stimulation. The effects of dopamine are thus dose dependent, and pharmacologic activity is a function of the amount of dopamine infused corrected for body weight. The individual response may be variable and unless the clinical situation warrants large pressor doses to maintain blood pressure, dopamine infusion should begin at a low rate (1 µg/kg/minute) and gradually be increased to clinical responsiveness. Cardiogenic shock with low tissue perfusion accompanied by hypotension may be treated in a more aggressive manner with progressively increasing doses of dopamine at 5-minute intervals.Low-dose dopamine infusion results in stimulation of DA2 receptors and minimal or no changes in
heart rate, cardiac output, or blood pressure. Stimulation of DA2 receptors results in renal
vasodilation and increases glomerular filtration rate, renal blood flow, and sodium excretion. Reduction in cardiac output in shock frequently results in shunting of blood away from the renal vasculature and induction of a prerenal state with elevated blood urea nitrogen–to–creatinine ratios and sodium retention. Dopamine reverses the redistribution of cardiac output and increases the amount of sodium presented to the loop of Henle, which allows increased efficacy of diuretics such as furosemide or bumetanide.Medium dosing ranges of dopamine (5–10 µg/kg/minute) result in an increase in cardiac output, which may also improve volume status by increasing renal blood flow. The cardiac effects of dopamine in this dosing range are secondary to stimulation of the β1-adrenergic receptors caused by
a secondary release of norepinephrine. The effect of dopamine is indirect and depends on a pre-existent adequate storage level of endogenous catecholamines. Long-standing congestive heart failure is frequently associated with reduction in sympathetic receptors in the myocardium and the efficacy of dopamine may be limited if prolonged congestive heart failure was present before the shock syndrome. Dopamine infusion at this dose generally does not result in alterations of venous return secondary to venodilation, and right atrial and PAOP may not decrease. Dopamine may be combined with either direct vasodilating compounds or other inotropic agents such as dobutamine, which combine inotropism with vasodilation. Medium dosing range infusions of dopamine are generally safe and effective in maintaining blood pressure. Acid-base status and electrolyte levels should be optimized to avoid potential induction of arrhythmias with resultant malignant ventricular arrhythmias or marked sinus or supraventricular tachycardias, which would increase myocardial oxygen demand.
Figure 56.3. Mechanisms of action of inotropic drugs. (Used with permission from Garcia Gonzalez MJ, Dominguez Rodriguez A. Pharmacologic treatment of heart failure due to ventricular dysfunction by myocardial stunning: potential role of levosimendan. Am J Cardiovasc Drugs. 2006;6[2]:69–75.) β1AR, β1-adrenergic receptor; β2AR, β2-adrenergic receptor; AC, adenyl cyclase;
AMP, adenosine monophosphate; ATP, adenosine triphosphate; Ca2+, calcium; CaMK, calmodulin-activated kinase; cAMP, cyclic AMP; Gi, inhibitory G protein with α, β, and γ subunits; Gs, stimulatory G protein with α, β, and γ subunits; P, phosphorus; PDEc, cytosolic phosphodiesterases; PDEp-III, particulate, SR-associated PDE III; PHLMBN, phospholamban; PKA, cAMP-dependent protein kinase A; SR, sarcoplasmic reticulum.P.846High-range dopamine infusions (>10 µg/kg/minute) result in activation of α-adrenergic receptors and a secondary norepinephrine release with vasoconstriction and increased systemic vascular resistance. Patients in cardiogenic shock may need much higher doses of dopamine and ranges up to 50 µg/kg/minute have been used. Strict attention to volume status and repeated examinations for signs of excessive vasoconstriction are necessary. A central venous line is used for higher dopamine doses due to tissue necrosis should the solution extravasate. Dopamine may interact with certain coadministered drugs. Tricyclic antidepressants may increase the pressor response of direct-acting sympathomimetics and decrease the sensitivity to indirect-acting sympathomimetics. Because dopamine has direct and indirect effects on the vasculature, this agent should be used with caution,
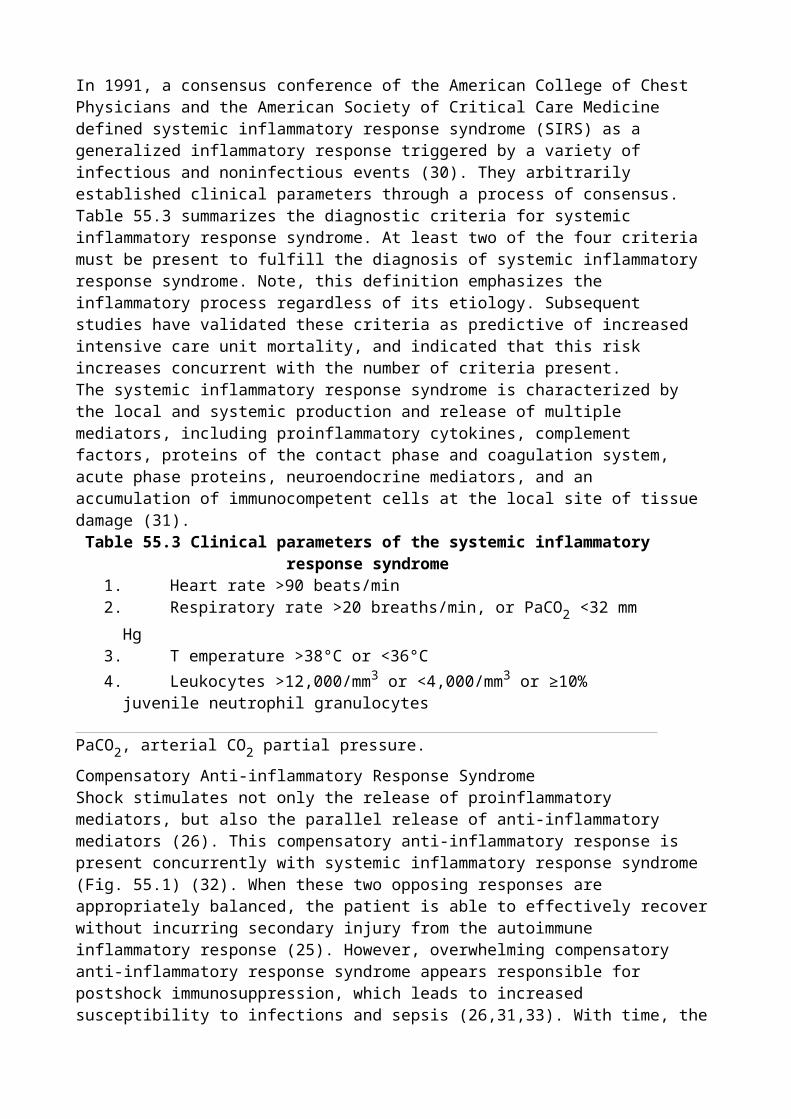
especially with overdoses of the tricyclic drugs (77). Although not commonly used, the rauwolfia alkaloids may potentiate the pressor response of direct-acting sympathomimetics resulting in hypertension. Monoamine oxidase inhibitors may increase pressor response of dopamine (78). Dopamine is an endogenous catecholamine that is degraded by catechol-o-methyltransferase and is not effective when administered in oral doses.DobutamineAs opposed to dopamine, which is an endogenous catechol and immediate precursor of norepinephrine and epinephrine, dobutamine is a synthetic agent that stimulates predominantly β1-
adrenoreceptors (79) (Table 56.4). Dobutamine is a direct-acting agent, unlike dopamine, and does not require the presence or release of intramyocardial norepinephrine to modulate its effects. Mild activation of β2 and α receptors may be seen with this agent, but significantly less when compared
with β1 receptors. Administration of dobutamine results in a direct inotropic stimulation plus a
secondary reflex vasodilation with reduction of systemic vascular resistance and an increase in cardiac output.The pharmacologic mechanism of dobutamine is complicated because of its asymmetric structure and racemic mixture. The positive and negative isomers have been evaluated as to their relative activities in in vitro studies, and it seems that the positive isomer is predominantly responsible for the activation of the β receptors. The administration of dobutamine alters stimulation of β receptors in a differential manner with an increased binding affinity for the predominantly cardiac β1-
adrenergic receptors with a direct inotropic effect. The inotropic effects of this agent are not coupled with an increased P.847rate of arrhythmias when compared with epinephrine and norepinephrine and there seems to be fewer adverse electrophysiologic effects when compared with dopamine. Although a mild vasodilator, there are no major effects on arterial blood pressure due to an increase in cardiac output and stroke volume. The increase in cardiac output results in improved renal blood flow and enhanced ability to excrete sodium and water. Dobutamine is effective in cardiogenic shock, assuming that the underlying etiology is not caused by valvular or subvalvular stenosis and the pharmacologic infusion does not result in significant hypotension, and this agent may be combined with dopamine to maintain blood pressure.
Table 56.4 DobutamineAdrenergic receptor Site Actionβ1 Myocardium Increases atrial and ventricular
contractility Sinoatrial node Increases heart rate Atrioventricular conduction system Enhances atrioventricular
conductionsβ2 Arterioles Vasodilation
Lungs Bronchodilationα Peripheral arterioles VasoconstrictionDA1 Postsynaptic Dilation of coronary, renal, and
mesenteric vasculatureDA2 Autonomic ganglia and postganglionic
sympathetic nervous systemDecreased release of endogenous catechols
NorepinephrineNorepinephrine is a powerful α-adrenergic agonist that results in significant peripheral vasoconstriction when administered within the usual dosage range of 2 to 8 µg/minute. Norepinephrine is generally instituted in the treatment of cardiogenic shock after failure of volume correction and dopamine to maintain adequate cardiac output and blood pressure (80). Norepinephrine is a naturally occurring catecholamine that has both α- and β1-adrenergic activity.
Although generally associated with an increase in cardiac output, increases in systemic vascular resistance and mean aortic blood pressure may affect cardiac output adversely. The pressure work of the left ventricle and oxygen consumption are increased and blood may be shunted away from various organ beds because of volume redistribution secondary to catecholamine sensitivity. Oliguria and azotemia from impaired renal blood flow may be worsened secondary to the norepinephrine-mediated vasoconstriction. Norepinephrine has been associated with increased irritability of the ventricle with an increased electrical instability and potential adverse rhythm disorders. Clinical response will vary depending on the advantageous effects of increased perfusion pressure and cardiac output weighed against the detrimental effects of increased myocardial oxygen consumption and shunting from visceral organs.Digitalis PreparationsThe use of digitalis in general and cardiogenic shock specifically has been controversial because of theoretical objections involving the use of this agent and the lack of controlled clinical trials documenting a beneficial impact on mortality (81). Digitalis glycosides have complex mechanisms of action whose inotropic activity is modulated by increasing the availability of intracellular calcium secondary to inhibition of sodium–potassium ATPase. Inhibition of this ubiquitous enzyme, which is found not only in cardiac tissue but also in the central nervous system, gastrointestinal tract, and kidney, results in calcium influx by the activation of the sodium–calcium exchange mechanism. The level of free cytosolic calcium regulates the activity of tropomyosin with increased interactions between actin and myosin filaments and increased contractility. Alterations in contraction are caused by variations in levels of cytosolic calcium, which can be moved in and out of the sarcoplasmic reticulum.The increase in cardiac output after administration of digitalis is modest when compared with the more powerful intravenous inotropes such as dobutamine, dopamine, and norepinephrine. Digitalis increases the refractory period at the atrioventricular node and decreases conduction velocity, resulting in a negative chronotropic effect in patients with atrial fibrillation. An advantage is that digitalis lacks the negative inotropic activity of other agents that have been used to slow the rate in atrial fibrillation, including β-blockers and calcium channel blockers such as diltiazem and verapamil (82). Digitalis increases vagal tone, decreases levels of norepinephrine in chronic heart failure possibly from decreased activity of the peripheral sympathetic nervous system, resets baroreceptor sensitivity, and may enhance natriuresis from increased cardiac output.Digitalis withdrawal has been associated with worsening heart failure in a randomized, double-blind, placebo-controlled study of digitalis withdrawal in patients also treated with ACE inhibitors. However, the role of digitalis in cardiogenic shock is limited due to a modest increase in cardiac output, although the autonomic effects of this agent with decreases in the heart rate in atrial fibrillation are clinically beneficial.IsoproterenolIsoproterenol has both β1- and β2-adrenergic properties with increased myocardial contractility,
heart rate, P.848and cardiac output without vasoconstriction. The powerful chronotropic and inotropic activities of this agent increase myocardial work and oxygen. Isoproterenol is infrequently used in heart failure or cardiogenic shock unless the shock state is associated with bradyarrhythmias that do not respond to other therapies or with acute valvular insufficiency if blood pressure and volume status are maintained. Isoproterenol thus has a limited role in the acute management of cardiogenic shock.Phosphodiesterase InhibitorsAmrinone and milrinone are bipyridine derivatives that inhibit cellular levels of phosphodiesterase (83). Inhibition of this key enzyme results in increased levels of cyclic adenosine monophosphate (AMP) in cardiac muscle with resultant enhancement of protein phosphorylation by protein kinase with increased inotropic and chronotropic activities. The methylxanthines were known to nonspecifically inhibit phosphodiesterase activity and result in mild enhancement of the inotropic state. Both amrinone and milrinone have been shown in experimental and clinical studies to
increase cardiac output in patients with severe congestive heart failure or cardiogenic shock (84).Administering these agents results in reduction of central filling pressures and increases in stroke volume and cardiac output. The chronotropic effects of amrinone and milrinone are modest, but a mild increase in heart rate may be observed. Large doses may result in severe peripheral vasodilation, hypotension, and tachycardia. The phosphodiesterase inhibitors have been studied in patients with pump failure after myocardial infarctions, and at a dose of 200 µg/kg/hour, have been shown to improve cardiac function. Comparison in clinical trials of amrinone to other vasodilating inotropes such as dobutamine documented a greater decrease in systemic and pulmonary venous pressures in the group that received amrinone (85). The vasodilating activity of the phosphodiesterase inhibitors, while increasing cardiac output, may result in significant hypotension, requiring concomitant administration of sympathomimetic amines with at least partial α activity such as norepinephrine. The side effect profile of the phosphodiesterase inhibitors relates mainly to hematologic and gastrointestinal effects. Nausea, vomiting, and diarrhea occur in many patients. Thrombocytopenia is common with amrinone (approximately 15%), although the marked decreases in platelet counts to levels under 50,000 seems to be relatively rare and may require dose reduction. Milrinone is more potent on a milligram basis when compared with amrinone and also has effects on the inotropic state and ventricular relaxation. Incidence of thrombocytopenia seems less (<5%) than with amrinone. Enoximone is an imidazole derivative that also results in phosphodiesterase inhibition and increases levels of cyclic AMP and contractile force in isolated muscle preparations (86). Intravenous enoximone results in an increase in cardiac index with a decrease in right-sided filling pressures with minimal impacts on systemic vascular resistance and heart rate. Enoximone is currently undergoing a variety of controlled trials and seems to have a relatively mild side effect profile, and thrombocytopenia is uncommon with the use of this agent.GlucagonGlucagon is uncommonly used in cardiogenic shock but has a potential advantage in that it has a different mechanism of action from other sympathomimetic amines and does not require β-receptor stimulation to exert its inotropic effects (87,88). Glucagon is administered in a dosing range of 4 to 6 mg intravenously, which may be followed by a constant infusion of 4 to 12 mg/hour. Glucagon administration increases cardiac output by approximately 20%, which is associated with a decrease in peripheral vascular resistance with less myocardial oxygen demand when compared with norepinephrine. The indications for glucagon have not been delineated, although it seems justifiable to administer this agent to patients with cardiogenic shock who do not respond to conventional therapy or cannot tolerate other agents because of the development of significant arrhythmias or hematologic toxicity.LevosimendanLevosimendan is the first of a new class of inotropic agents called calcium sensitizers. Its mechanism of action involves increasing calcium sensitivity by binding to troponin C and stabilizing it in the calcium-induced conformation. This augments the effect of calcium binding to troponin C. Additionally, at high concentrations levosimendan inhibits phosphodiesterase 3, which also results in increased intracellular calcium concentration. These effects result in increased myocardial contraction associated with increased intracellular calcium transients (89). It improves myocardial contractility without increasing oxygen requirements and induces peripheral and coronary vasodilation with a potential antistunning, anti-ischemic effect (90). Given its vasodilatory properties, it is not primarily for cardiogenic shock but more for low-output heart failure. In addition to calcium sensitization, levosimendan also stimulates adenosine triphosphate (ATP)-sensitive potassium ion channels that are suppressed by intracellular ATP and acts synergistically with nucleotide diphosphates. This mechanism may contribute to the vasodilator action and may protect cardiomyocytes against ischemic damage (91). A loading dose of 6 to 24 mg/kg over 10 minutes followed by an infusion of 0.1 mg/kg/minute for 50 minutes, increased to 0.2 mg/kg/minute for an additional 23 hours, has been well tolerated (90). Initial clinical experience suggests that levosimendan causes dose-dependent increases in stroke volume and cardiac index, with minimum increase in heart rate (92). There are dose-dependent decreases in PAOP and right atrial, pulmonary
arterial, and mean arterial pressures. The hemodynamic effects of levosimendan appear to be more pronounced than those seen with dobutamine (93) and sustained up to 24 hours after discontinuation of infusion due to an active metabolite (94). An initial clinical trial found no significant adverse events (92). Data from two published clinical trials indicate that levosimendan is associated with improved 6-month survival compared with dobutamine or placebo, although the studies were not powered to look at this outcome (93,95,96). There are several other trials not yet published but presented at national meetings that report a survival benefit of levosimendan compared with dobutamine or placebo. However, a 24-hour infusion of levosimendan had no effect on 6-month survival compared with dobutamine for patients with acutely decompensated heart failure in the Survival of Patients with Acute Heart Failure in need of Intravenous Inotropic Support (SURVIVE) trial reported at the American Heart Association Scientific Sessions in 2005 but not yet published (93). The European Society of Cardiology's 2005 guidelines on the diagnosis and treatment of acute heart failure include the use of levosimendan in patients with symptomatic low cardiac output secondary to systolic dysfunction without severe hypotension (97). This drug is not yet approved by the Food and Drug Administration (FDA), although it is available in some European countries.P.849Surgical InterventionSurgical intervention in myocardial infarction has been used to limit infarct size by direct revascularization or to correct the mechanical defects of an acute ischemic event such as VSD, acute mitral insufficiency, free wall rupture, or left ventricular aneurysm. Surgical intervention for revascularization in acute myocardial infarction had been contraindicated on theoretic grounds because of the presumed high morbidity and mortality rates from cardiac catheterization and operative interventions during the unstable period of acute myocardial infarction. A variety of clinical studies determined that coronary bypass surgery could be performed in an expeditious manner with low mortality. Bypass surgery has been used as primary therapy in acute myocardial infarction with an overall operative rate of approximately 5% for transmural infarctions and a highly acceptable long-term mortality rate (98,99). Evidence is accumulating that early revascularization (<6 hours) by direct PTCA, intravenous or intracoronary thrombolytic agents, or bypass surgery in selected patients represents the treatment of choice. Congestive heart failure that occurs in the postmyocardial state may be amenable to revascularization by surgical interventions, although large-scale, controlled, randomized studies are lacking. However, several surgical series have reported on early and long-term survival of patients with an acute MI complicated by cardiogenic shock receiving coronary artery bypass surgery (98,99,100,101,102). Surgical intervention in cardiogenic shock is fraught with considerable clinical problems and requires the presence of surgically accessible and potentially viable myocardium. Surgical intervention has the advantage of re-establishing flow not only in the infarct-related artery, but also in vessels not involved in the acute ischemic process but significantly obstructed. Viability of the myocardium in the peri-infarction state may be difficult to determine secondary to problems with the acute delineation of stunned, hibernating, or irreversibly damaged myocardium. Nitroglycerin or dobutamine enhancement of ejection fraction is an indirect method of determining viability but is time consuming in a period where early revascularization is of prime importance.Indications for surgical intervention in cardiogenic shock have not been completely delineated but should be considered in patients who fail to respond to volume correction and inotropic therapy. Failure of conventional medical interventions for cardiogenic shock should result in consideration of intra-aortic balloon counterpulsation, a temporizing measure before revascularization. Historically, emergent coronary artery bypass surgery preceded by placement of intra-aortic balloon pump has demonstrated improved survival rates in cardiogenic shock to approximately 75%. The SHOCK trial registry reported a 28% in-hospital mortality for the 290 patients undergoing coronary artery bypass surgery, which is comparable to other reported series (22,100). In a subgroup analysis of the SHOCK trial, survival was similar between percutaneous and surgically revascularized patients (55.6% vs. 57.4% at 30 days and 51.9% vs. 46.8%, respectively, at 1 year) despite a higher incidence of diabetes and multivessel disease in those patients surgically revascularized (37). Thus,
surgical revascularization has an important role in patients with more extensive coronary artery disease.Surgery for acute mitral insufficiency associated with cardiogenic shock in the postinfarction state is the only available definitive therapy. The impact of acute mitral insufficiency on left ventricular performance may be underestimated by studying the ejection fraction since the left ventricle ejects retrograde into the low-compliance left atrial and pulmonary venous system. Medical therapy with inotropic support and systemic peripheral vasodilation improves regurgitant flow as calculated by the regurgitant fraction. Severe mitral insufficiency is associated with a variety of adverse pathophysiologic changes that result in a poor survival after surgical intervention, but the results are significantly better than medical treatment that results in essentially 100% mortality if marked mitral insufficiency is associated with cardiogenic shock.Surgical intervention is generally required for acute VSDs, which occur in the muscular portion of the interventricular septum and may be multiple. Two anatomic types of acute VSDs have been described. A VSD resulting from occlusion of a posterior descending coronary artery that arises from the right coronary is associated with a defect located in the inferobasilar region of the septum. Anteroseptal myocardial infarctions, which are associated with thrombotic occlusion of the left anterior descending, are associated with midapical to anterior defects in the septum. The physiologic impact of a left-to-right shunt is a function of the quantitative amount of involved myocardium plus associated left ventricular dysfunction, pulmonary artery pressures, and right ventricular compliance. A significant left-to-right shunt markedly decreases forward flow with poor peripheral perfusion and the clinical characteristics of cardiogenic shock. If the left ventricular end-diastolic pressure is markedly elevated, left-to-right shunting will also occur during diastole and is associated with an extremely high 24-hour mortality rate of approximately 25% (101,102). Medical treatment alone is associated with a 20% survival beyond 60 days and 1-year survival of less than 10%.Surgical intervention in acute VSDs requires early and aggressive diagnostic and therapeutic interventions. Despite IABP and optimization with medical management, refinements in surgical technique have improved 1-year survival to 32% without coronary artery bypass. Evaluation of clinical trials that attempt to postpone therapy to improve the healing process have been questioned because this eliminates the most severely ill patients from definitive therapy and introduces a selection bias into the implications of therapy. Early surgical intervention with direct patch grafts plus coronary artery bypass may result in survival rates of up to 75%.Free wall rupture of the left ventricle is a surgical disease even with a clotted hemopericardium tamponading further extravasation of blood into the pericardial space. The diagnosis of free wall rupture may be extraordinarily difficult on clinical grounds, and signs of pericardial tamponade should be actively sought. Pericardiocentesis with decompression of the pericardial space may be lifesaving in the short term but represents only a temporizing procedure. Cardiac rupture is essentially fatal, but surgical intervention may be successful with direct oversewing of the defect if recognized and managed in a timely fashion (103,104).Left ventricular aneurysm as a cause of cardiogenic shock may require surgical intervention as a definitive therapy. The remodeling process, which begins after an acute ischemic event with regional thinning and expansion of the infarct zone, may result in progressive decrease in left ventricular performance and cardiogenic shock. If the aneurysmal dilation of the left ventricle involves more than 20% of the left ventricular mass, P.850severe impairment of pumping ability ensues and potentially requires surgical intervention if there is a poor response to medical management including intra-aortic balloon pumping. Surgical intervention for aneurysms should be optimized in timing with adequate healing and fibrosis.Mechanical Circulatory SupportThe intra-aortic balloon pump has been in clinical use for over 20 years to increase diastolic coronary arterial perfusion and to decrease left ventricular afterload (105). The intra-aortic balloon pump is a temporizing measure that does not increase myocardial oxygen demand and results in
reduction of ventricular diastolic volume and reduces pulmonary congestion with an increase in cardiac output. The intra-aortic balloon pump is the most widely used circulatory assist device in patients with cardiogenic shock because of the ease of insertion either percutaneously or surgically. Effective counterpulsation results in stabilization and potential reversal of the shock state with improvement in peripheral perfusion but does require an adequate systemic pressure and left ventricular performance to maximize its use. Profoundly hypotensive patients respond poorly to intra-aortic counterpulsation and the IABP has limited efficacy.Balloon pumping in selected patients allows optimization of blood pressure, cardiac output, and tissue perfusion in patients with cardiogenic shock while further diagnostic procedures are performed. Hemodynamic effects of the IABP include the following (in percent change): Peak aortic systolic pressure (10%–15%), diastolic intra-aortic pressure (70%), arterial end-diastolic pressure (10%), peak ventricular pressure (10%), LV end-diastolic pressure (10%), dp/dt (10%), systemic vascular resistance (no change), mean arterial pressure (no change), cardiac index (10%–15%), and pulmonary capillary resistance (10%–15%). The intra-aortic balloon pump may be used prophylactically in patients with mechanical defects such as acute mitral insufficiency or VSD to increase coronary perfusion, allow time for healing, and restore cardiac output toward normal. The impact of intra-aortic balloon pumping on long-term survival is controversial and depends on the indications for insertion, hemodynamic status, and etiology of the cardiogenic shock. Patient selection is a key issue and early insertion of the intra-aortic balloon may result in increased clinical benefit rather than procrastination until overt low flow state has developed. The addition of the IABP to thrombolytic therapy for acute MI complicated by cardiogenic shock has been studied in a randomized clinical trial. There was no overall mortality benefit, but the subgroup of patients with Killip class III or IV benefitted with a 6-month mortality rate of 39% for combined therapy versus 80% for fibrinolysis alone (106). The SHOCK trial registry also reported a survival benefit with intra-aortic balloon pumping in addition to thrombolytic therapy (47% vs. 63% in-hospital mortality), but these results were heavily affected by higher revascularization rates in the group receiving the intra-aortic balloon pump (68% vs. 20%) (73).Patients who are not expected to significantly benefit from an intra-aortic balloon pump are elderly patients, those with severe peripheral vascular disease, and those with large MIs exceeding 40% of the left ventricular myocardium. The overall survival rate of patients with cardiogenic shock treated with the intra-aortic balloon pump is approximately 40%. For subjects who required balloon insertion for large myocardial infarctions without a significant mechanical obstruction, the survival rate was only 27%. Complications may be documented in up to 30% of patients who undergo intra-aortic balloon pumping and relate mainly to local vascular problems, including surgical trauma, emboli, infection, and hemolysis.Left ventricular assist devices (LVADs) function as prosthetic ventricles but require a sternotomy for insertion. Assist devices may be used to support left ventricular performance, right ventricular performance, or a combination, depending on the underlying condition. The indications for insertion of an LVAD are controversial, and traditionally have been reserved for medical and intra-aortic balloon pump failure and in the presence of the potentially salvageable myocardium and particularly as a bridge to cardiac transplantation. The Thoratec extracorporeal left ventricular assist device (Thoratec, Pleasanton, CA) has been used as a bridge to cardiac transplantation. Insertion of the Thoratec device in patients with severe left ventricular dysfunction allowed survival to transplant in approximately 75% of 29 patients (107). Similarly, in the Heartmate LVAD (Thoratec, Pleasanton, CA), survival to cardiac transplantation has been reported as 76% out of 97 patients (108). The REMATCH (Randomized Evaluation of Mechanical Assistance in the Treatment of Congestive Heart Failure) trial demonstrated improved outcomes in chronically ill patients too sick for cardiac transplantation as an alternative (destination therapy) to routine medical care (109). Hemodynamic unloading and myocardial rest after ventricular assist device (VAD) placement may lead to recovery of native cardiac function, allowing for removal of the device without cardiac transplantation (110,111,112,113,114,115,116). Ventricular assist device support is also associated with decreases in neurohormonal activation, alterations in myocyte calcium handling, and
improvement in the proinflammatory cytokine milieu (117,118,119,120,121,122,123,124,125). Histologic analysis of the explanted heart at the time of transplantation demonstrated decreased fibrosis and myocyte size after VAD placement (121,126,127). Despite these salutatory changes as a result of VAD support, the frequency of bridge to recovery (BTR) in chronically supported subjects remains low, in the range of 3% to 10% in various series (111,114,115,128).The Heartmate LVAD is approved for life-long support in patients deemed too ill for cardiac transplantation with several other devices undergoing clinical trials. There is retrospective data that early mechanical support as a bridge to transplantation after acute MI complicated by cardiogenic shock improves survival compared with a strategy of early revascularization (129). The technology has now advanced to include several other continuous flow pumps that offer the potential advantage of greater mechanical longevity, thus making them truly a lifelong option. Complications include hemolysis, thromboembolism, and infection, which have been decreased with increasing experience.The Nimbus hemopump (Nimbus Medical, Inc., Rancho Cordova, CA) circumvented the problem associated with median sternotomy and allows a percutaneous placement of a cannula across the aortic valve, which is coupled to an extracorporeal power source. The Nimbus hemopump uses an Archimedes spiral screw valve that rotates at approximately 25,000 revolutions per minute without significant hemolysis (130). Although this pump is no longer available, there are several other percutaneous continuous rotary flow VADs, including the TandemHeart (Cardiac Assist, Pittsburgh, PA), P.851Cancion (Orqis Medical, Lake Forest, CA), and Impella (Abiomed, Danvers, MA). The TandemHeart is currently FDA approved, while the Impella is approved in Europe and in clinical trial in the United States. The Cancion system is also in clinical trial in the United States.Future and Adjunctive TherapiesAutologous Stem CellsStem cells offer the hope of biologically rebuilding damaged myocardium due to their ability to differentiate into cardiomyocytes. There has been a substantial amount of research into the biology of various stem cells and now several clinical trials have been reported, with mixed results. Most trials have looked at stem cells' delivery percutaneously by intracoronary catheter after acute myocardial infarction in numbers ranging from 30 to 100 patients. The BOOST (Bone Marrow Transfer to Enhance ST-elevation Infarct Regeneration) trial found 6% improvement in ejection fraction compared to control but no significant difference at 18 months (131,132). The ASTAMI (Autologous Stem Cell Transplantation in Acute MI) trial found no difference in ejection fraction at 4 and 6 months, although Janssens et al. reported improved regional wall motion and decreased infarct size (133,134). The TOPCARE-CHD (Transcoronary Transplant of Progenitor Cells after MI with Chronic Ischemic Heart Disease) trial found 2.9% improvement in ejection fraction at 3 months, while the REPAIR-AMI (Intracoronary Administration of Bone Marrow-derived Progenitor Cells in Acute Myocardial Infarction) trial reported a 2.5% improvement in ejection fraction at 4 months (135,136). Multiple studies are currently under way including evaluating the safety and efficacy of stem cells implanted during surgery for VAD installation as well as coronary artery bypass surgery with depressed ventricular function and percutaneously for chronic angina. While this is a very promising therapy, considerable issues remain, including the risk of generating an arrhythmic focus, the best cell type, the amount of local myocardial blood flow necessary, the best method to deliver the cells to the myocardium, and the number of cells necessary.ClenbuterolClenbuterol is a β2-adrenergic receptor agonist that induces skeletal muscle hypertrophy and
improves contraction. It also has been found to cause cardiomyocyte hypertrophy without apoptosis (137). In a recently reported single-center study, 15 patients requiring LVAD support were treated with clenbuterol in addition to lisinopril, carvedilol, spironolactone, and losartan (138). There was sufficient myocardial recovery to explant the LVAD in 11 of 15 patients, in whom 4-year survival was 89%, quality-of-life scores were almost normal, and mean left ventricular ejection fraction was
64%. These patients all had heart failure due to nonischemic cardiomyopathy without histologic evidence of active myocarditis. A multicenter trial in the United States is being planned.Tissue-engineered PatchesPatches made from decellularized extracellular matrix may be another useful solution to biologic regeneration of myocardium. The patch retains biologically active substances such as growth factors providing paracrine as well as mechanical support for regrowth of cardiomyocytes. These devices are still in preclinical testing but have shown improvements in regional function in a myocardial infarction model (139).ConclusionsDespite rapid advancement in pharmacologic thrombolytic therapy, mechanical revascularization techniques, and development of mechanical ventricular assist devices, cardiogenic shock remains a major clinical challenge with an associated high mortality. Improved survival in cardiogenic shock may be seen with an aggressive approach to diagnosis and management of the problem, with emphasis on early recognition and treatment of mechanical defects such as VSD, acute mitral insufficiency, and free wall rupture. Limitation of infarct size by minimizing the extent of infarcted tissue is the key component in all therapeutic strategies with the goal to maximize perfusion, limit irreversible cell death, and decrease potential for a secondary mechanical event.Pearls
Clinical criteria used to establish the diagnosis of cardiogenic shock include absolute or relative hypotension, which is defined as a systolic blood pressure less than 90 mm Hg or a blood pressure that has fallen to at least 30 mm Hg less than the individual's baseline blood pressure.
Cardiogenic shock thus may be a complication in patients with chronic hypertension who have an acute cardiac event that results in a decrease in blood pressure, but not to the 90 mm Hg systolic level.
If signs of organ dysfunction and tissue hypoperfusion accompany this condition, the individual qualifies for the diagnosis of cardiogenic shock.
The exact incidence of cardiogenic shock is difficult to ascertain because of variability in diagnostic criteria and survival rates in the early phase of acute MI. The Multicenter Investigation of Limitation of Infarct Size trial (140) documented an incidence rate of cardiogenic shock in 7.5% of subjects who were admitted to the hospital after having an acute myocardial infarction, a constant value from 1975 to 1997 (141). The Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Arteries (GUSTO-I) trial, the GUSTO-III trial, and other thrombolytic trials have reported incidences of 5% to 10% (68,142).
The mortality rate for cardiogenic shock in the setting of acute MI is exceedingly high despite significant improvements due to a strategy of early revascularization as reported in the SHOCK (Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock) trial. Historically, mortality rates were 81% as originally reported by Killip in 1967 (6). Early revascularization by angioplasty or surgery has been shown to reduce mortality from 63% to 50% at 6 months in the SHOCK trial (36).
Chapter 57Sepsis and Septic ShockAnand KumarAseem KumarSeptic shock (shock due to infection) and sepsis-associated multiple organ failure are the dominant cause of death in intensive care units of the industrialized world. As many as 800,000 cases of sepsis are admitted every year to American hospitals (comparable to the incidence of first myocardial infarctions), with half of those developing septic shock (1). Historically, the mortality associated with sepsis and septic shock has been approximately 50% to 75% (2,3,4). The major advance in the therapy of septic shock was the development of antibiotic therapy 50 years ago, which resulted in a reduction in sepsis-associated mortality in the 30% to 50% range (2,3). However, the past 40 years have seen a gradual year-to-year increase in the incidence of sepsis (5). As a result, total deaths in the United States have increased even though the overall mortality rate has fallen from 27.8% to 17.9% during that period (5). At present, the total death toll from sepsis is comparable to that from myocardial infarction and far exceeds the impact of illnesses such as acquired immune deficiency syndrome (AIDS) or breast cancer (1,6).The total number of cases continues to gradually increase due to a burgeoning population of patients with a chronic and high degree of susceptibility to infection (age, AIDS, organ failure with transplant, and other chronic illness); an increased use of invasive medical devices; and increased use of cytotoxic agents for autoimmune disease, transplants, and malignancy for patients at high risk for sepsis. Current estimates suggest a doubling of total United States cases by 2050 but with only a projected increase in population of 33% (1). Until recently, despite major advances in technology and constant refinement of our understanding of sepsis pathophysiology, numerous clinical trials have failed to produce any new drugs with consistent beneficial effects on this patient population. Nonetheless, the last 50 years have seen a gradual improvement in mortality, perhaps related to improvements in supportive care (5,7).DefinitionsDerived from the Greek word “sepo,” meaning “I rot,” the first introduction of the term sepsis occurs in the poems of Homer (circa eighth century B.C.) (8). Over the intervening 2,700 years, through Homer, Hippocrates, Aristotle, and Galen to current-day physicians, the term has continued to be used virtually unchanged in meaning. Hugo Schottmüller modernized the term with his 1914 definition, “Septicemia is a state of microbial invasion from a portal of entry into the blood stream which causes signs of illness” (9). From the time of Schottmüller's definition of septicemia until recent years, terms such as septicemia, sepsis, toxemia, and bacteremia were all used interchangeably to indicate patients exhibiting systemic responses to infection.A significant problem with the term septicemia (as defined by Schottmüller) is that most patients with a septic response cannot be documented to have bacteremia/fungemia, and many with bacteremia/fungemia (e.g., endocarditis, catheter-related infection) do not exhibit overt sepsis. Recognizing that future large-scale clinical trials of novel sepsis therapies will require more consistent and precise definitions of the septic response, consensus definitions were developed in 1991 (10). These criteria were developed primarily as a tool to enhance the ability to perform clinical sepsis research. However, the terminology soon entered the clinical lexicon. These
consensus definitions were revised in 2001 to accommodate the clinician's perspective (11). Current and previous definitions follow.Infection:A microbial phenomenon characterized by an inflammatory response to the presence of micro-organisms or the invasion of normally sterile host tissue by these organisms.Bacteremia:The presence of viable bacteria in the blood. The presence of other organisms in the blood should be described in like manner—viremia, fungemia, and so on. Bacteremia can either be transient, sustained, or intermittent.Systemic Inflammatory Response Syndrome (SIRS):The systemic inflammatory response to various severe clinical insults, including but not limited to infection. Various other clinical insults include pancreatitis, ischemia, multiple trauma and tissue injury, hemorrhagic shock, immune-mediated organ injury, and exogenous administration of inflammatory mediators such as tumor necrosis factor or other cytokines. Previous criteria for SIRS are enumerated in Table 57.1. The more recent revision to sepsis definitions removed these SIRS criteria while retaining the concept. However, some understanding of these criteria remains crucial for the intensivist/clinical researcher, as most trials in the last 15 years have been predicated on patients having three or more of these criteria.Sepsis:The systemic response to infection. This response is similar to SIRS, except that it is considered to result from an infection. The previously accepted definition required at least two of the four SIRS criteria in the presence of documented or suspected infection. The recent revision of the criteria enumerates multiple potential diagnostic criteria for sepsis (Table 57.2) and no longer specifically requires the discarded elements of the SIRS criteria.Severe Sepsis:Sepsis associated with organ dysfunction, perfusion abnormalities, or hypotension. Organ system dysfunction can be described by organ failure scoring systems (12,13).Septic Shock:Sepsis with hypotension despite adequate fluid resuscitation, in conjunction with perfusion abnormalities. P.856Standard abnormalities in an adult include mean arterial pressure (MAP) <60 mm Hg, systolic blood pressure <90 mm Hg, or a drop in systolic blood pressure >40 mm Hg from baseline.
Table 57.1 Definition of Systemic Inflammatory Response Syndrome (SIRS)Systemic inflammatory response syndrome (SIRS): The systemic inflammatory response to a wide variety of severe clinical insults manifests by two or more of the following conditions:
Temperature greater than 38°C or less than 36°C Heart rate greater than 90 beats per minute (bpm) Respiratory rate greater than 20 breaths per minute or PaCO2 less than 32 mm Hg
White blood cell count greater than 12,000/µL, less than 4,000/µL, or 10% immature (band) forms
From Bone R. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20:864–874.Multiorgan Dysfunction Syndrome (MODS):The presence of altered organ function in an acutely ill patient, such that homeostasis cannot be maintained without intervention. Primary MODS is the direct result of a well-defined insult in which organ dysfunction occurs early and can be directly attributable to the insult itself. Secondary MODS develops as a consequence of a host response and is identified within the context of SIRS.
The relationship of many of these conditions to each other is demonstrated in Figure 57.1. An understanding of sepsis definitions has become increasingly important since most clinical trials in the last two decades have used the modified version of the 1991 sepsis definitions (usually requiring three rather than two SIRS criteria) in their entry criteria. The concept of a compensatory anti-inflammatory response has also been introduced after the demonstration that traditional anti-inflammatory mediators were also elevated during sepsis (14).EpidemiologyAlthough the sepsis syndromes (from sepsis to septic shock) have been a major burden on human health in both the developed and undeveloped world, there has been a surprising dearth of epidemiologic information. In North America, this has been caused by the earlier lack of consensus definitions of these syndromes and, more recently, the absence of syndrome-specific diagnostic codes for sepsis within the International Classification of Disease (ICD) coding system. In the last 20 years, the development of consensus definitions and application of computerized hospital and government administrative databases has allowed substantial insight into the problem.Martin et al. (5) have estimated 660,000 annual cases of sepsis in the United States during 2000 (adjusted rate 240/100,000 population) using an analysis of ICD-9 codes associated with National Hospital Discharge Survey data. With the exception of a single major study with much higher values (1), estimates for severe sepsis from sites across North America and Europe have been fairly consistent at 50 to 80/100,000 population (15,16,17,18,19). These cases account for approximately 10% to 15% of all intensive care unit (ICU) admissions (16,17,19,20,21). Approximately 25% of cases of sepsis (22) and 50% to 75% of cases of severe sepsis progress to septic shock (20). Septic P.857shock represents between 5% and 8% of all ICU admissions (21,23). In the United States, the cost of sepsis and severe sepsis ranges from $22,000 to $60,000 per episode at a total cost of approximately $17 billion annually (1,24). Sepsis and related conditions are the tenth leading cause of death in the United States (6).
Table 57.2 Revised Diagnostic Criteria for SepsisInfection,a documented or suspected, and some of the following:General variables Fever (core temerpature >38.3°C) Hypothermia (core temperature <36°C) Heart rate >90 min or >2 SD above the normal value for age Tachypnea Altered mental status Significant edema or positive fluid balance (>20 mL/kg over 24 h) Hyperglycemia (plasma glucose >120 mg/dL or 7.7 mmol/L) in the absence of diabetesInflammatory variables Leukocytosis (WBC count >12,000 µL) Leukopenia (WBC count <4,000 µL) Normal WBC count with >10% immature forms Plasma C-reactive protein >2 SD above the normal value Plasma procalcitonin >2 SD above the normal valueHemodynamic variables Arterial hypotensiona (SBP <90 mm Hg, MAP <70, or an SBP decrease >40 mm Hg in adults or <2 SD below normal for age) SvO2 >70%a
Cardiac index >3.5 L/min/m2b
Organ dysfunction variables Arterial hypoxemia (PaO2/FiO2 <300)
Acute oliguria (urine output <0.5 mL/kg/h or 45 mmol/L for ≥2 h) Creatinine increase >0.5 mg/dL
Coagulation abnormalities (INR >1.5 or aPTT >60 s) Ileus (absent bowel sounds) Thrombocytopenia (platelet count <100,000 µL) Hyperbilirubinemia (plasma total bilirubin >4 mg/dL or 70 mmol/L)Tissue perfusion variables Hyperlactatemia (>1 mmol/L) Decreased capillary refill or mottlingWBC, white blood cell; SBP, systolic blood pressure; MAP, mean arterial blood pressure; S[v with bar above]O2, mixed venous oxygen saturation; INR, international normalized ratio; aPTT,
activated partial thromboplastin time.aInfection defined as a pathologic process induced by a micro-organism.bS[v with bar above]O2 sat >70% is normal in children (normally, 75%–80%), and CI 3.5–5.5 is
normal in children; therefore, neither should be used as signs of sepsis in newborns or children.From Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31(4):1250–1256.
Figure 57.1. Venn diagram showing the relationship between infection and other sepsis-associated terms. The intersection of systemic inflammatory response syndrome (SIRS) and infection defines sepsis. Severe sepsis is a subset of sepsis defined by the presence of organ failure. Septic shock is a subset of severe sepsis in which the organ failure is cardiovascular (i.e., shock). Patients with certain inflammatory conditions (e.g., extensive burn injury, pancreatitis, major trauma, postpump syndrome, and so on) may demonstrate a “septic” appearance (i.e. SIRS) without the presence of infection required for a diagnosis of sepsis. (Adapted from Bone R. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20:864–874.)The incidence of sepsis appears to be increasing at a rate of about 9% per year in the United States (5) (Fig. 57.2). Reasons for this increase include the following: (a) An aging population with increased predisposition to illness; (b) increased proportion and longevity of the subpopulation with conditions that predispose to systemic infection including chronic organ failure (e.g., cirrhosis, renal failure, cardiomyopathy, chronic obstructive pulmonary disease [COPD]), and other conditions (e.g., diabetes, cancer, AIDS, etc.); (c) extensive use of invasive diagnostic and therapeutic modalities (indwelling catheters and devices), which lead to breakdown of native resistance to infection; and (d) widespread use of immunosuppressive chemotherapies for a wide range of diseases (asthma, inflammatory bowel disease, rheumatoid arthritis, systemic lupus erythematosus, and other autoimmune diseases).
Figure 57.2. Incidence of sepsis in the United States stratified by organism group. The incidence of sepsis increased approximately 9% per year between 1979 and 2001 with the greatest relative increase in fungal infections. In addition, as of the late 1980s, Gram-positive pathogens became numerically dominant over Gram-negative organisms. (From Martin GS, Mannino DM, Eaton S, et al. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546–1554. Copyright © 2003 Massachusetts Medical Society. All rights reserved.)Age is a substantial risk factor for sepsis, severe sepsis, and septic shock (1,5,25). Patients older than the age of 65 years are approximately 13-fold more likely to develop sepsis compared to others (5). Similarly, septic shock is 18 times more likely in the >80-year age group compared to those in the 20- to 29-year age group (23). Given that the average age of the North American population is increasing, and that the incidence of all the sepsis-related syndromes is markedly elevated in the elderly (23), the fact that the average age of patients with sepsis has climbed over the last few decades can be no surprise (1,5). That septic shock is substantially a geriatric illness is reflected in the median age of 67 years (25). The persistent 60:40 male:female preponderance in sepsis, severe
sepsis, and septic shock may have its origins in men's increased predisposition to smoking-associated cases of pneumonia and peptic ulcer disease/gastrointestinal malignancy-associated gastric and bowel perforation (1,5,17,20,22,23). Nonwhite racial groups are also at substantially increased risk, particularly African Americans (5). However, low socioeconomic status is a substantial risk factor for septic shock (a fourfold increased risk in the lowest quintile of income compared to any other quintile) (23). In this context, it is unclear whether race may be relevant only as a marker of socioeconomic status. Comorbidities are common in patients with sepsis, as might be expected given an average age of 55 to 65 years for sepsis and perhaps higher for septic shock (5,19,25,26,27,28,29). Diabetes, COPD, renal failure, congestive heart failure, and malignancy can each be found in 10% to 20% of patients with sepsis or septic shock. At least 50% of patients with severe sepsis have at least one major medical comorbidity (5). Patients with septic shock have an even higher incidence (>90%) of major comorbidities. Alcoholism and substance abuse also substantially increases the risk of sepsis, as well as death from sepsis and septic shock (30).As might be expected, mortality increases with the severity of the septic syndrome. Mortality is <15% for sepsis, 25% to 50% for severe sepsis, and >50% for septic shock (1,5,15,16,17,20,21,22,25,31). This mortality rate for septic shock, while staggering, nevertheless represents an improvement in survival P.858from 35 years ago when mortality rates frequently exceeded 80% (32,33). Early septic mortality (<3 days) appears to be associated most closely with shock with other deaths within the first week due to multiple organ failure. Later deaths tend to be most closely associated with pre-existing comorbidities (34). Of those succumbing to septic shock, approximately 75% are early deaths (within 1 week of shock), primarily due to hyperdynamic circulatory failure (35).Throughout recorded history, there has been an evolution of the organisms that cause infectious diseases and the associated clinical syndromes. This phenomenon has become particularly pronounced since the advent of antibiotics in the last half of the previous century. By the 1960s and 70s, Gram-negative organisms had become the dominant pathogens over Staphylococcus aureus and streptococci. During the 1980s, resistant Gram-positive organisms (methicillin-resistant S. aureus, coagulase-negative staphylococci, penicillin-resistant S. pneumoniae, and enterococci) again re-emerged as major pathogens. Gram-positive cocci account for approximately 40% to 50% of single isolates (excluding fungi) in sepsis and septic shock (20,25,31,36,37,38).Most recently, yeast and other fungi have demonstrated a remarkable increase in their contribution to sepsis (5% of total) and septic shock (8.2% of total), with an increase of about 10% per year (5,25,37,38). Candida albicans remains numerically dominant (about 60% of total fungal infections), but fluconazole-resistant yeasts are the most rapidly increasing species (39,40,41). Other major concerns in recent years include the emergence of vancomycin-resistant enterococci (42), extended spectrum β-lactamase (ESBL) resistance in Gram-negative organisms (reliably sensitive only to carbapenems) (43), and an endemic strain of virulent, methicillin-resistant S. aureus in the community (44). In addition, concerns regarding sporadic cases of vancomycin-resistant S. aureus (VRSA) are growing (45).Pathogenesis of Sepsis, Severe Sepsis, and Septic ShockSepsis and septic shock or sepsis-associated multiple organ failure typically begin with a nidus of infection within the body (e.g., pneumonia, peritonitis, urinary tract infection, abscess). Within that nidus, the organism replicates. Eventually, the infection at the inciting focus releases sufficient microbial antigens to elicit a systemic inflammatory response designed to eliminate the invading microbes (Fig. 57.3). Many constitutive and/or inducible elements of invasive microorganisms are capable of inciting the systemic inflammatory responses that result in sepsis and septic shock (Fig. 57.3, Table 57.3). Beyond endotoxin (lipopolysaccharide; LPS) of Gram-negative bacteria, other major triggers of the systemic inflammatory response characteristic of sepsis include various exotoxins (bacteria), peptidoglycans (streptococci), and teichoic acid (S. aureus); lipoarabinomannan of mycobacteria; and mannoproteins and β-glucan of fungi (46). Bacterial DNA may possess sufficient antigenic properties (based on unique CG repetitions and lack of
deoxyribonucleic acid [DNA] methylation) to initiate a substantial inflammatory response independent of other bacterial elements (47,48,49). Bacterial ribonucleic acid (RNA) may be able to do the same (50). Recent investigations suggest a surprising commonality of signaling mechanisms in septic shock via Toll-like receptors from a broad range of etiologic agents (48,51,52,53,54).Despite the large number of potential elements of pathogenic microorganisms that can drive the septic response, endotoxin of Gram-negative bacteria remains the prototype of such factors and the model for subsequent research. This antigen is thought to be central in initiating the powerful host response to infection with these organisms (55). LPS and other antigens interact with immune cells (particularly macrophages), resulting in the induction of proinflammatory cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-1β (IL-1β) secreted by monocytes, macrophages, and other cells (Fig. 57.3) (56). These cytokines initiate a complex signaling sequence involving the release of secondary mediators (platelet-activating factor, leukotrienes, prostaglandins) and monocytes, as well as endothelial tissue factor expression, inducible nitric oxide synthetase induction, microvascular coagulation, cell-adhesion molecule up-regulation, and apoptosis (57,58,59,60). To maintain homeostasis (and likely as part of a feedback mechanism), several anti-inflammatory mediators are also released, including interleukin-10 (IL-10), transforming growth factor-β (TGFβ), and interleukin-1 receptor antagonist (IL-1ra). If homeostasis cannot be maintained, progressive and sequential dysfunction of various organ systems (i.e., MODS) may occur. If the inflammatory stimulus is particularly intense, or if there is limited cardiovascular reserve, effects on the cardiovascular system as manifested by septic shock may dominate the clinical presentation.Microbial Antigen SignalingAs the prototypical and best-studied microbial antigen, an understanding of the signaling cascade of endotoxin is instructive. Endotoxin is an amphiphilic macromolecule located on the outer cell wall membrane of Gram-negative bacteria. It is composed of lipid A (a diglucosamine-based acylated phospholipid), and a polysaccharide side chain (61,62) (Fig. 57.4). The polysaccharide chain is composed of a short, highly conserved, proximal section (core polysaccharide) and a highly variable, longer distal oligosaccharide side chain. The core polysaccharide and lipid A are sometimes referred to as the core glycolipid. The highly conserved lipid A moiety is the toxic element of endotoxin and can reproduce the manifestations of endotoxic shock when administered alone (62,63,64,65,66,67). As a circulating form in the plasma, endotoxin exists in a multimeric aggregate form.Lipopolysaccharide-binding protein (LBP) is an acute phase reactant protein present in plasma (61,68,69). The levels increase with inflammatory stimulation. LBP catalyzes the transfer of endotoxin from serum aggregates to either serum lipoproteins, such as high-density lipoprotein (HDL), leading to endotoxin neutralization or to CD14 receptors (either membrane-bound [mCD14] or soluble [sCD14]), the putative primary LPS receptor (Fig. 57.5). The degree to which endotoxin is shunted through either pathway appears to play a significant role in the phenotypic physiologic response (46). LBP, by forming a complex with endotoxin monomers, appears to enhance the ability of endotoxin to bind CD14 and allows cellular activation at relatively low endotoxin concentrations (61,69). P.859P.860Although LBP appears to be a specific carrier molecule for endotoxin, available data suggest that other microorganism toxins associated with sepsis may use similar carrier proteins (70,71).
Figure 57.3. Pathogenesis of sepsis and septic shock. ATIII, antithrombin III; DNA, deoxyribonucleic acid; HMGB1, high mobility group box 1 protein; LPS, lipopolysaccharide; MIF, macrophage migration inhibitory factor; TFPI, tissue factor pathway inhibitor; TGF, transforming growth factor; Toxin A, Pseudomonas toxin A; TSST-1, toxic shock syndrome toxin 1. (Adapted from Parrillo JE. Pathogenic mechanisms of septic shock. N Engl J Med. 1993;328:1471–1477.)
Table 57.3 Elements of Microorganisms Capable of Inducing a Septic Response
Microorganism ComponentGram-negative bacteria Lipopolysaccharide Peptidoglycan Porins Lipoproteins Lipopeptides Lipid A–associated proteins Pili Exotoxins DNA/RNAGram-positive bacteria Exotoxins Peptidoglycan Lipoteichoic and teichoic acids DNA/RNAMycobacteria Lipoarabinomannan Lipomannan Mycolylarabinogalactan-peptidoglycanFungi Mannoproteins β-glucanAdapted from Heumann D, Glauser MP, Calandra T. Molecular basis of host-pathogen interaction in septic shock. Curr Opin Microbiol. 1998; 1(1):49–55.CD14, a glycoprotein receptor, is found primarily in the cells of the myelomonocytic lineage (monocytes, macrophages, polymorphonuclear leukocytes) (72). Although there appear to be several other membrane-associated LPS receptors, membrane-associated CD14 (mCD14) represents the only receptor that is clearly involved in LPS binding and activation of cellular inflammatory responses. In contrast to the low endotoxin concentrations required to activate CD14 (an effect mediated by the LBP-LPS interaction [73]), other receptors such as CD18 appear to require exceptionally high concentrations of LPS to elicit a cellular effect, suggesting a lack of physiologic relevance (74).
Figure 57.4. Endotoxin (lipopolysaccharide). Endotoxin is a component of the cell wall of Gram-negative bacilli. (From Young LS, Martin WJ, Meyer RD, et al. Gram-negative rod bacteremia: microbiologic, immunologic, and therapeutic considerations. Ann Intern Med. 1977;86:456–471, with permission.)Recent data suggest that CD14, far from being uniquely a receptor for LPS, may also bind ligands from various pathogens, including peptidoglycan and lipoteichoic acid of Gram-positive bacteria, lipoarabinomannan of mycobacteria, and chitin of fungi (Table 57.4) (46,75). In several of these, binding is serum dependent, suggesting the possibility of serum carrier/binding proteins similar to LBP (70). This convergence of receptor-signaling mechanisms may explain why downstream intracellular signaling events (activation of NF-κB, MAP kinases, etc.) and cellular responses (cytotoxicity, cytokine generation, etc.) appear to be so highly conserved in sepsis due to different etiologic agents. Although elements of different microorganisms bind and activate CD14, limited data suggest that the precise binding sites vary.Despite the importance of CD14, the receptor lacks the ability to initiate intracellular signaling on its own because of the lack of an intracytoplasmic-signaling domain. CD14 signaling requires the involvement of the most recently discovered (and most central) element of microbial antigen-mediated signal transduction, the Toll-like receptors (TLRs) (52,76,77,78,79). The original Toll receptor was initially described as an essential component of embryogenesis of Drosophila (80). In mammals, various TLRs have been shown to play a crucial role in the recognition of microbial antigens and initiation of the immune response. TLR4, and to a lesser extent TLR2, have been implicated in signaling associated with endotoxin (53,77,78,79,81). TLR4 appears to be coexpressed and forms a plasma membrane complex with mCD14. mCD14 appears to bind with the
LPS/LBP complex to enable transfer to TLR4 and an accessory protein, MD-2 (82). mCD14, acting as a receptor for other non-LPS microbial antigens, also appears to have a role in TLR2 signaling (83). The exact nature of the CD14-TLR interaction is as yet undetermined. However, interaction of CD14 and TLR4 stimulates downstream activity of the intracellular domain of TLR to generate NF-kB and other intracellular mediators that drive the response to LPS (Fig. 57.5). Notably, the intracellular domain of the TLRs is shared with the IL-1 receptor. Several other TLR receptors are known to be involved in microbial antigen signaling from various pathogens, including Gram-positive and Gram-negative bacteria, fungi, mycobacteria, and viruses (Table 57.5).
Figure 57.5. Endotoxin signaling pathway related to CD14 and TLR4 (Toll-like receptor 4). IκB, inhibitory κB; IKK, IκB kinase; IRAK, IL-1R–associated kinase; LBP, lipopolysaccharide-binding protein; LPS, lipopolysaccharide; MYD88, myeloid differentiation factor; NFκB, nuclear factor-κB; NIK, nuclear factor κB–inducing kinase; TRAF 6, tumor necrosis factor receptor associated factor.P.861Besides the Toll-like receptor pathways, other important routes of microbial antigen signaling exist. In particular, some Gram-positive organisms produce potent exotoxins that are implicated in the pathogenesis of toxic shock syndromes. These include the toxic shock syndrome toxin-1 associated with staphylococcal toxic shock and pyrogenic toxins predominantly associated with group A streptococci. These exotoxins appear to be superantigens in that they are able to activate broad polyclonal groups of lymphocytes, resulting in massive cytokine generation and toxic shock (84,85).CytokinesThe concept of a systemic inflammatory response syndrome (SIRS) has already been discussed in the context of sepsis. The notion of an innate anti-inflammatory response, termed compensatory anti-inflammatory response syndrome (CARS), during sepsis also exists (14). This model suggests that a clinical insult (such as infection or injury) initiates a proinflammatory response that is countered by an endogenous anti-inflammatory reaction. The aggregate responses produce endogenous circulating mediators (cytokines, soluble receptors, adhesion molecules, growth factors, eicosanoids, etc.), generating systemic phenomena such as septic shock or immunosuppression. Clinical manifestations and patient outcome are dependent on the balance between proinflammatory and anti-inflammatory elements. The predominance of the inflammatory response corresponds to SIRS and may lead to cardiovascular compromise, shock, and organ dysfunction. However, a predominance of anti-inflammatory mediators produces a state of immune paralysis associated with a propensity to infection and inability to fight infection. Both may ultimately lead to death. In patients with sepsis, the duration of monocyte inactivation (a potential manifestation of CARS) correlates with mortality (86). If the counterinflammatory response is able to balance the inflammatory stimuli (while the infecting micro-organism is effectively cleared), homeostasis is achieved and clinical recovery will occur. In this model, sepsis has a dynamic nature based on the development and balance of the above-described responses (Fig. 57.6). This interplay is influenced by the nature of the inflammatory injury and the genetically determined variability of the host immune response (87,88).Table 57.4 CD14 Binding-Capable Microbial ProductsLigands OriginLipopolysaccharide Gram-negative bacteriaPeptidoglycan Gram-positive bacteriaLipoteichoic acid Gram-positive bacteriaLipoarabinomannan Mycobacterium tuberculosisRhamnose-glucose polymersStreptococcus speciesPolyuronic acids BacteriaAcylpolygalactoside Klebsiella pneumoniaeChitin YeastAmphiphilic molecules Staphylococcus aureus
Proinflammatory cytokines have multiple effects, including the stimulation of production and release of other proinflammatory mediators. TNF-α, interleukin-1β (IL-1β), and interleukin-6 (IL-6) are the best known proinflammatory cytokines and have overlapping and synergistic effects in stimulating the inflammatory cascade. The next phase in the cytokine response to infection is the endogenous counterinflammatory cascade in response to the systemic activity of proinflammatory cytokines. Cytokine inhibitors (e.g., IL-1 receptor antagonist [IL-1ra], soluble TNF receptor) and anti-inflammatory cytokines (e.g., TGFβ, IL-4, IL-10, and IL-13) are involved in this phase of the response. Other cytokines like HMGB1 may be involved even later in the syndrome. Thus, the cytokine network in sepsis involves proinflammatory cytokines, P.862anti-inflammatory cytokines, and cytokine inhibitors (Table 57.6). It is the balance between these cytokines at different time points that determine the clinical manifestations and outcome of sepsis.
Table 57.5 Microbial Ligands of the Toll-like Receptors (TLRs)Receptor Microbial ligands OriginTLR1 Triacyl lipopeptides
Soluble factorsMycobacteria, bacteriaN. meningitidis
TLR2 Peptidoglycan and LTA Gram-positive bacteria Lipoprotein/lipopeptide Gram-positive bacteria Atypical LPS Leptospira interrogans and
Porphyromonas gingivalis Lipoarabinomannan, cell wall and
lipoproteins/lipopeptidesMycobacteria
Lipoproteins/lipopeptides Borrelia burgdorferi Glycolipids and lipoproteins/lipopeptides Treponema spp. Lipoproteins and lipopeptides Mycoplasma spp. Phenol-soluble modulin S. aureus Cell wall S. pneumoniae Soluble factor Group B streptococci Porins Neisseria meningitidis Zymosan Yeast Heat shock protein Human proteinTLR3 dsRNA VirusTLR4 LPS Gram-negative bacteria LTA Gram-positive bacteria Heat-sensitive compound Mycobacteria Heat shock protein Chlamydia pneumoniae Fusion protein Respiratory syncytial virus Glycolipids Treponema brennaborense Heat shock protein Human protein Heat shock protein Human proteinTLR5 Flagellin Bacteria with flagellaTLR6 Diacyl lipopeptides Mycoplasma Lipoteichoic acid Gram-positive bacteria Zymosan FungiTLR7 ssRNA VirusTLR8 ssRNA VirusTLR9 CpG DNA BacteriaTLR10 Unknown UnknownTLR11 Unknown UnknownLTA, lipoteichoic acid; LPS, lipopolysaccharide; dsRNA, double-stranded RNA; ssRNA, single-stranded RNA.Adapted from Leaver SK, Finney SJ, Burke-Gaffney A, et al. Sepsis since the discovery of Toll-like
receptors: disease concepts and therapeutic opportunities. Crit Care Med. 2007;35(5):1404–1410; and Van Amersfoort ES, Van Berkel TJ, Kuiper J, et al. Receptors, mediators, and mechanisms involved in bacterial sepsis and septic shock. Clin Micro Rev. 2003;16(3):379–414.Nitric OxideAnother important mediator, nitric oxide (NO), has a vital role in normal intracellular signal transduction (89). NO is synthesized by a family of enzymes called NO synthases (NOS) that incorporate nitrogen from one of the guanidine terminals of L-arginine with molecular oxygen to form NO and L-citrulline. Three distinct nitric oxide synthases have been purified, cloned, and characterized: (i) Neuronal NOS or nNOS, (ii) inducible NOS or iNOS, and (iii) endothelial NOS or eNOS, reflecting the cell types from which they were originally identified.NO has several important roles in infection, sepsis, and septic shock. The iNOS gene is induced in immunoactivated cells. NO formed by these cells plays a role in host defense against bacterial, viral, and protozoan infections. Of particular importance in relation to septic shock, nitric oxide is the mediator through which endothelial cells normally cause relaxation of adjacent smooth muscle (89). Endothelial cells, through eNOS, P.863produce picomolar quantities of nitric oxide in response to several vasodilatory stimuli such as shear stress, acetylcholine, and bradykinin. This nitric oxide diffuses to adjacent smooth muscle and activates guanylate cyclase to produce cyclic GMP, which effects vascular relaxation. Activity of endothelial NOS is regulated and is calcium and calmodulin dependent.
Figure 57.6. The dynamic cytokine inflammatory response. Sepsis is associated with an early transient dominance of proinflammatory cytokines corresponding to the systemic inflammatory response syndrome (SIRS) and the onset of organ damage. After this initial phase, the anti-inflammatory pathways of CARS (compensatory anti-inflammatory response syndrome) become active with the development of a refractory state characterized by a decreased capacity of mononuclear cells to produce proinflammatory cytokines. Recovery occurs if homeostasis is re-established. (Adapted from van der Poll T, van Deventer SJ. Cytokines and anticytokines in the pathogenesis of sepsis. Infect Dis Clin North Am. 1999;13(2):413–426.).During septic shock, an iNOS capable of producing nanomolar quantities of nitric oxide is generated in endothelium and vascular smooth muscle (89,90). Following this generation, the activity of this iNOS is unregulated and constant. Nitric oxide–mediated generation of cyclic guanosine monophosphate (cGMP) explains the profound loss of arterial vascular tone and venodilatation seen in septic shock (90,91) and may, in part, explain the irreversible vascular collapse seen late in hemorrhagic shock (92) (Fig. 57.7). A potential role for NO in inflammation-associated edema and third-spacing during shock has also been suggested (93). The in vitro myocardial depressant effects of TNF-α, IL-1β, and serum from septic humans may be mediated by a similar NO- and cGMP-dependent pathway (94,95). TNF-α, IL-1β, and IFN-γ have been identified as key mediators of iNOS activation. An alternative pathway by which NO may play a role in the cardiovascular pathophysiology of shock and sepsis involves the production of peroxynitrite (ONOO-), a highly reactive oxidant, from the interaction of superoxide (OH-) and nitric oxide (NO-) (96).Table 57.6 Major Proinflammatory and Anti-inflammatory Cytokines and Receptors in Sepsis
Proinflammatory CytokinesAnti-Inflammatory Cytokines Cytokine Inhibitors
Tumor necrosis factor-α (TNF-α) Transforming growth factor (TGF-β)
Soluble TNF receptors
- Type I - Type IIInterleukin-1β (IL-1β) Interleukin-4 (IL-4) Interleukin-1 receptor
antagonist (IL-1ra)Interleukin-2 (IL-2) Interleukin-6 (IL-6)
Interleukin-6 (IL-6) Interleukin-8 (IL-8) Interleukin-12 (IL-12) Interleukin-9 (IL-9) Interferon-γ (IFN-γ) Interleukin-10 (IL-10) Macrophage migration inhibitory factor (MIF)
Interleukin-11 (IL-11)
High mobility group 1 protein (HMG-1)
Interleukin-13 (IL-13)
HemostasisThe coagulation cascade represents a highly conserved antimicrobial defense mechanism common to even the most primitive complex organisms, such as the Limulus horseshoe crab. The hemolymph of the horseshoe crab, one of the oldest complex organisms still in existence, clots rapidly in response to minute quantities of endotoxin or beta-(1,3) glucan, a component of fungi. Pathogens are immobilized in the clot, allowing subsequent elimination (97,98). This commonality of purpose and function of the coagulation and inflammatory systems in eliminating invading microbes has persisted in evolution to present-day mammals including humans (99). These systems, in sharing common activation pathways, are inextricably linked.Although both these systems are normally highly adaptive in nature, excessive activity of the coagulation and inflammation pathways can result in vascular injury, aberrant tissue blood flow, tissue damage, and, ultimately, organ dysfunction. Recent clinical and laboratory investigations have established that, in conjunction with the cytokine cascade, the coagulation system plays a key role in inflammatory states such as sepsis (100,101,102) (Fig. 57.8). A critical process in sepsis-induced coagulopathy is the activation of the extrinsic pathway (100).During the normal hemostatic response, exposure of blood to nonvascular cell-bound tissue factor in the subendothelial layer initiates the extrinsic pathway through the binding of tissue factor to activated factor VII. The resulting enzyme complex, in turn, activates factor IX of the intrinsic pathway and factor X of the common pathway. With factor V as a cofactor, P.864activated factor X cleaves prothrombin to form thrombin. Thrombin then converts fibrinogen to fibrin, which results in clot formation (103).
Figure 57.7. Physiologic and pathophysiologic vasodilatory factors relevant in sepsis and septic shock. cGMP, cyclic GMP; eNOS, endothelial nitric oxide synthetase; IL-1, interleukin-1β; iNOS, inducible nitric oxide synthetase; NO, nitric oxide; ONOO-, peroxynitrite; PAF, platelet-activating factor; PGE2, prostaglandin E2; PGI1, prostacyclin; TNF, tumor necrosis factor-α. (Adapted from
Kumar A, Parrillo JE. Shock: pathophysiology, classification and approach to management. In: Parrillo JE, Dellinger RP, eds. Critical Care Medicine: Principles of Diagnosis and Management in the Adult. 3rd ed. St. Louis, MO: Mosby; 2007:379–422.)In sepsis, however, the expression of tissue factor is either directly or indirectly induced by inflammatory cytokines. Overexpression of proinflammatory cytokines, such as TNF-α, IL-1β, and interleukin-8, are thought to upset the balance toward a procoagulant state (60,101,104) (Fig. 57.8). TNF-α and IL-1β, for example, can induce the expression of tissue factor in circulating monocytes and endothelial cells (101). The vascular endothelial injury resulting from inflammation can also further expose tissue factor in subendothelial tissue and perivascular cells. Endothelial injury also inhibits the production and activity of anticoagulants such as proteins C and S, the heparin–antithrombin complex, and thrombomodulin. Loss of native anticoagulant function is indicated by decreased activity and circulating levels of protein C (105,106), antithrombin III, (ATIII) (101,106), and tissue factor pathway inhibitor (TFPI) (107,108) in patients with severe sepsis and septic shock.Current evidence suggests that the pathogenesis of sepsis is associated with (a) systemic activation of coagulation resulting in consumption of coagulant factors, (b) suppression of the anticoagulant system by the same proinflammatory mediators that activate coagulation, and (c) early activation followed by later suppression of fibrinolysis (60,101) (Fig. 57.8). Whereas the coagulation cascade is clearly activated in sepsis, the specific inciting events and the molecular linkages between

inflammation and coagulation remain to be elucidated (60,101,102,103). Given observational studies demonstrating the depletion of anticoagulant factors (decreased activity levels of protein C [60,102], ATIII [101,103], and TFPI [28]) in patients with severe sepsis and septic shock, such markers may be useful to indicate the presence or severity of sepsis in the future.
Figure 57.8. Cytokines induce the endothelial cell to shift from an antithrombotic to a prothrombotic phenotype. Expression of tissue factor by monocytes, and perhaps a subset of endothelial cells, initiates coagulation through the extrinsic system in patients with severe sepsis and septic shock. At the same time, fibrinolysis is inhibited through the release of thrombin-activatable fibrinolysis inhibitor (TAFI) and plasminogen activator inhibitor-1 (PAI-1). IL-1, interleukin-1β; IL-6, interleukin-6; TNF-α, tumor necrosis factor-α. (Copyright © 2002 Eli Lilly and Company. All rights reserved. Printed with permission. Permission to reproduce the copyrighted material must be obtained from Lilly prior to reproducing or using the image.)Host Genetic FactorsAlthough the characteristics of the pathogen have much to do with the occurrence of clinical infection and progression to sepsis and septic shock, a growing body of data suggests that genomic variations between patients are equally important. These genomic variations in microbial and cell signaling, innate immunity, and coagulation and inflammatory stress cytokine responses appear to explain individual variations in susceptibility to infection, sepsis/septic shock, and septic death. They likely explain why identical organisms cause fulminant disease P.865with septic shock in some but only minimal clinical illness in others. The importance of inheritable elements in susceptibility and mortality risk of life-threatening infections is demonstrated by adopted twin studies which demonstrated remarkable convergence in the causes of death (including sepsis/infection) of such individuals (109).Table 57.7 Human Genetic Markers Associated with Risk of Infection and Sepsis/Septic ShockGene product group/Gene product Infection/sepsis associationPattern Recognition ReceptorsTLR2 •Tuberculosis •Life-threatening bacterial infections •S. aureus infectionsTLR4 •Gram-negative infection •Septic shockTLR5 •Legionella infectionCD14 •Septic shock and septic shock mortality •Isolation of pathogenic bacteria in infectionMannose-binding lectin •Bacterial infections •Isolation of pathogenic bacteria in infectionIntracellular Proteins IRAK4 •Recurrent Gram-positive infectionsCytokines TNF-α •Sepsis, septic shock, septic mortality •Meningococcal mortalityTNF-β •Sepsis and septic mortalityIL-6 •Septic mortalityIL-10 •Sepsis and septic mortality •CAP severity and mortality •Pneumococcal septic shockIFNγ •InfectionMIF •Sepsis and sepsis-induced acute lung injuryIL-1Ra •Sepsis and septic mortalityCoagulation Factors
PAI-1 •Meningococcal sepsis, septic shock, septic mortality, vascular complications
•Septic mortalityProtein C •Septic organ dysfunction and mortalityTAFI •Meningococcal and septic mortalityFibrinogen-β •Septic mortalityFactor 5 (Leiden) •Septic mortality, pressor use, purpura fulminansCD, cluster differentiation; IFN, interferon; IL, interleukin; IL-1Ra, IL-1 receptor antagonist; IRAK, interleukin-1 receptor-associated kinase; MIF, macrophage inhibitor factor; PAI, plasminogen activator inhibitor; TAFI, thrombin activatable fibrinolysis inhibitor; TLR, toll-like receptor; TNF, tumor necrosis factor.Adapted from Arcaroli J, Fessler MB, Abraham E, et al. Genetic polymorphisms and sepsis. Shock. 2005;24(4):300–312; Lin MT, Albertson TE, Lin MT, et al. Genomic polymorphisms in sepsis. Crit Care Med. 2004;32(2):569–579; Texereau J, Pene F, Chiche JD, et al. Importance of hemostatic gene polymorphisms for susceptibility to and outcome of severe sepsis. Crit Care Med. 2004;32(5 Suppl):S313–S319; and Papathanassoglou ED, Giannakopoulou MD, Bozas E, et al. Genomic variations and susceptibility to sepsis. AACN Adv Crit Care. 2006;17(4):394–422.The advent of complete gene mapping via high throughput analysis techniques (e.g., microarray gene chips, etc.) have resulted in a rapid expansion of the list of human genetic markers associated with risk of infection, sepsis/septic shock, and death. These markers fall into several broad groups, including those involved with microbial ligand binding, intracellular signaling, cytokine generation, and coagulation factor generation/activity as described in Table 57.7. It should be noted that some genetic polymorphisms may be linked to other genetic loci. An association between a given polymorphism and susceptibility to infection, sepsis, septic shock, or septic death does not always imply a direct causal relationship.Bioenergetic FailureThe underlying metabolic defect in sepsis and septic shock has been the source of substantial controversy over the last 30 years. Most forms of shock are associated with low cardiac output (CO) and tissue hypoperfusion leading to overt tissue P.866ischemia. This results in anaerobic glycolysis with intracellular acidosis, increased lactate, and high-energy phosphate depletion in the affected tissues. Blood oxygen extraction ratio (the ratio of oxygen consumed divided by the oxygen delivered) is increased as tissues maximize oxygen extraction in order to maintain oxygen consumption. During septic shock, the same tissue metabolic phenomenon of intracellular acidosis and increased lactate production is noted. However, cardiac output and total tissue perfusion is typically increased, and the oxygen extraction ratio falls. The explanation for tissue acidosis and lactate production in septic shock in the presence of tissue hyperperfusion is unknown.
Figure 57.9. Microanatomic shunting in sepsis and septic shock. One explanation of the increased lactatic acidosis and MvO2 found in septic shock is the potential presence of opening of nonnutrient
blood vessels between the arterial and venous vascular beds. MvO2, mixed venous oxygen
saturation.Loss of vascular autoregulatory control may explain some of the typical metabolic findings of sepsis and septic shock. An early theory postulated the existence of microanatomic shunts between the arterial and venous circulations (110) (Fig. 57.9). During sepsis, these shunts were said to result in decreased systemic vascular resistance (SVR) and increased mixed venous oxygen saturation (MvO2) (111). The resultant decrease in perfusion to tissue beds with normal or even increased
metabolic demand could generate tissue ischemia and lactic acid. However, whereas microanatomic shunting has been noted in localized areas of inflammation, systemic evidence of this phenomenon in sepsis and septic shock is lacking (111,112,113,114,115). Another theory involving “functional”
shunting due to defects of microcirculatory regulation in sepsis has also been proposed (Fig. 57.10) (116,117). Overperfusion of tissues with low metabolic requirements would result in increased MvO2
P.867and narrowing of the arteriovenous oxygen content difference. The relative vasoconstriction of vessels supplying more metabolically active tissues would result in tissue hypoxia and lactate production due to anaerobic metabolism. Observations that some capillary beds may be occluded by platelet microaggregates, leukocytes, fibrin deposits, and endothelial damage support this theory (112,116,118). Additional support comes from studies that demonstrate evidence of supply-dependent oxygen consumption in sepsis (119,120,121,122,123). Both of these theories of the metabolic defect of energy metabolism in sepsis and septic shock fall within the category of “stagnant” hypoxia as described by Barcroft in 1920 (124).
Figure 57.10. Functional shunting in sepsis and septic shock. Loss of ability to appropriately regulate microvascular flow according to tissue metabolic demand can lead to overperfusion of low-metabolic-demand tissue beds resulting in increased MvO2 (mixed venous oxygen saturation).
Underperfusion of high-metabolic-demand beds can result in tissue ischemia, anaerobic metabolism, and lactic acidosis.A third theory of the metabolic presentation of sepsis and septic shock suggests that circulating mediators cause an intracellular metabolic defect involving substrate use. This results in bioenergetic failure with high-energy phosphate (adenosine triphosphate [ATP] and phosphocreatine) depletion and lactate production (125,126,127). Increased mixed venous oxygen saturation could then be explained by perfusion, which is maintained in excess of tissue oxygen use capability. This phenomenon has been termed histotoxic (124) or cytopathic (127) hypoxia. Potential mechanisms to explain this form of hypoxia include impairment/ inactivation of pyruvate dehydrogenase; nitric oxide or peroxynitrite-mediated inhibition of mitochondrial respiration; uncoupling of oxidative phosphorylation or activation of poly-(ADP-ribosyl)-polymerase (PARP) (127). Observations demonstrating preservation of tissue PO2 (128), absence of tissue hypoxia
(129), and impairment of mitochondrial function (127,130,131,132) during sepsis and septic shock support this possibility.In particular, near-infrared spectroscopy (NIRS) has been used to examine mitochondrial function in a primate model of septic shock using live Escherichia coli infusion. NIRS demonstrated the presence of mitochondrial dysfunction in skeletal muscle in animals with experimentally induced sepsis. This was manifested by the impairment of oxidation of cytochrome a,a3 with reperfusion after transient ischemia in septic animals compared to controls (131). Another primate study demonstrated early disturbance of mitochondrial redox state in skeletal muscle and brain in the presence of live E. coli bacteremia. Of note, these changes occurred before the onset of overt hemodynamic alterations (133). In a limited observational study, uncoupling of tissue oxyhemoglobin levels and mitochondrial oxygen consumption, as indicated by cytochrome a,a3 redox state (indicating mitochondrial oxidative stress), predicted the development of multiple organ failure in patients with major trauma (134). These data particularly support the possibility of a decreased ability of mitochondria to use oxygen as a potential cause of decreased tissue high-energy phosphate in sepsis.All these theories of septic bioenergetic metabolism would be expected to result in a deficit of tissue high-energy phosphates during septic shock. A series of studies using biochemical analysis of harvested tissues and nuclear magnetic resonance (NMR) spectroscopy of septic animals have suggested that high-energy phosphate reserves are decreased in animal models of septic or endotoxic shock (125,135,136). It can be argued that in many of these studies, animals were inadequately fluid resuscitated, which resulted in tissue hypoperfusion. However, animals in at least one study (125) were clearly adequately resuscitated (cardiac output and tissue oxygen tension were maintained comparable to shams) and demonstrated similar evidence of high-energy phosphate depletion (skeletal muscle biopsy) along with an increased lactate/pyruvate ratio during rat

peritonitis induced by cecal ligation and perforation (125). Little human data exist. In one study of critically ill patients (most of whom were septic), the acetoacetate/β-hydroxybutyrate ratio (a marker of mitochondrial redox state) rose significantly in nonsurvivors compared to survivors (137). Evidence of increased acetoacetate/β-hydroxybutyrate ratio, along with an increase in ATP degradation products in critically ill patients with sepsis, also exists (138,139). In addition, independent studies using skeletal muscle biopsies in patients with sepsis/septic shock observed decreased ATP and phosphocreatine but variable changes in lactate levels (140,141).In contrast, other animal studies using NMR spectroscopy demonstrate that high-energy phosphates are not depleted in septic animals as would be expected in these theories of septic bioenergetic failure (142,143,144). According to these and other studies, cellular ischemia is not the dominant factor in metabolic dysfunction in sepsis (129,142,143,144,145,146,147). Rather, circulating mediators may result in cellular dysfunction, aerobic glycolysis, and lactate production in the absence of global ischemia (143). This position is weakened by data suggesting that increased lactate in septic shock is also associated with decreased pH (which would not be expected in aerobic glycolysis) (143). Nonetheless, ongoing controversy of this issue remains.Cardiac and Vascular ResponsesPrior to the introduction of the balloon-tipped pulmonary artery catheter (PAC) and echocardiography to assess cardiovascular performance, much of our understanding of septic hemodynamics was based on clinical findings. Two distinct clinical presentations of septic shock were proposed: Warm shock characterized with high CO, warm dry skin, bounding pulses and hypotension; and cold shock characterized with low CO, cold clammy skin, and diminished pulses (148). These two presentations were thought to represent a progressive continuum, starting with warm shock (in the initial hemodynamically well-compensated phase) and progressing to cold shock (indicating decompensation), culminating in death. This notion was supported by studies showing a correlation between survival and a high cardiac index (CI) (148,149). A major problem with this interpretation was that these studies used central venous pressure (CVP) as a reflection of left ventricular end-diastolic volume (LVEDV) and adequacy of fluid resuscitation. The central role of adequacy of intravascular volume status to CI and survival was suggested in a handful of studies at that time (150,151). Based on evidence collected over the past four decades, CVP is now accepted to be a poor measure of preload in critically ill patients, particularly those with sepsis and septic shock (152). Studies in recent years have clearly shown that adequately resuscitated septic shock patients typically exhibit a persistent hyperdynamic state, high CO, and low SVR (153,154). In nonsurvivors, this hyperdynamic state usually persists until death (Fig. 57.11) (35,155).More than any other form of shock, distributive and, particularly, septic shock involves substantial elements of the hemodynamic characteristics of other shock categories. All forms of distributive shock involve decreased mean peripheral vascular resistance. Before fluid resuscitation, distributive shock also P.868involves a hypovolemic component with decreased central venous and pulmonary artery occlusion pressures. The primary cause of this relative hypovolemia is an increase of the vascular capacitance due to venodilatation. This phenomenon has been directly supported in animal models of sepsis (156,157,158,159,160) and is reinforced by the fact that clinical hypodynamic septic shock (low CO) can usually be converted to hyperdynamic shock (high CO) with adequate fluid resuscitation (35,148,161). Relaxation of vascular smooth muscle is attributed to several of the mediators known to circulate during sepsis. These same mediators also contribute to the second cause of hypovolemia in sepsis: Third-spacing of fluid to the interstitium due to loss of endothelial integrity. Further, decreased oral fluid and salt intake during the course of the illness may play a role. As a consequence, CO and central/mixed venous oxygen saturation in unresuscitated and poorly resuscitated septic shock patients is usually decreased (161,162). Septic shock also involves a cardiogenic element. Myocardial depression is common in human sepsis and septic shock (163,164). Circulating substances such as TNF-α, IL-1β, platelet-activating factor (PAF), leukotrienes, and most recently, IL-6 and macrophage migration inhibitory factor have been
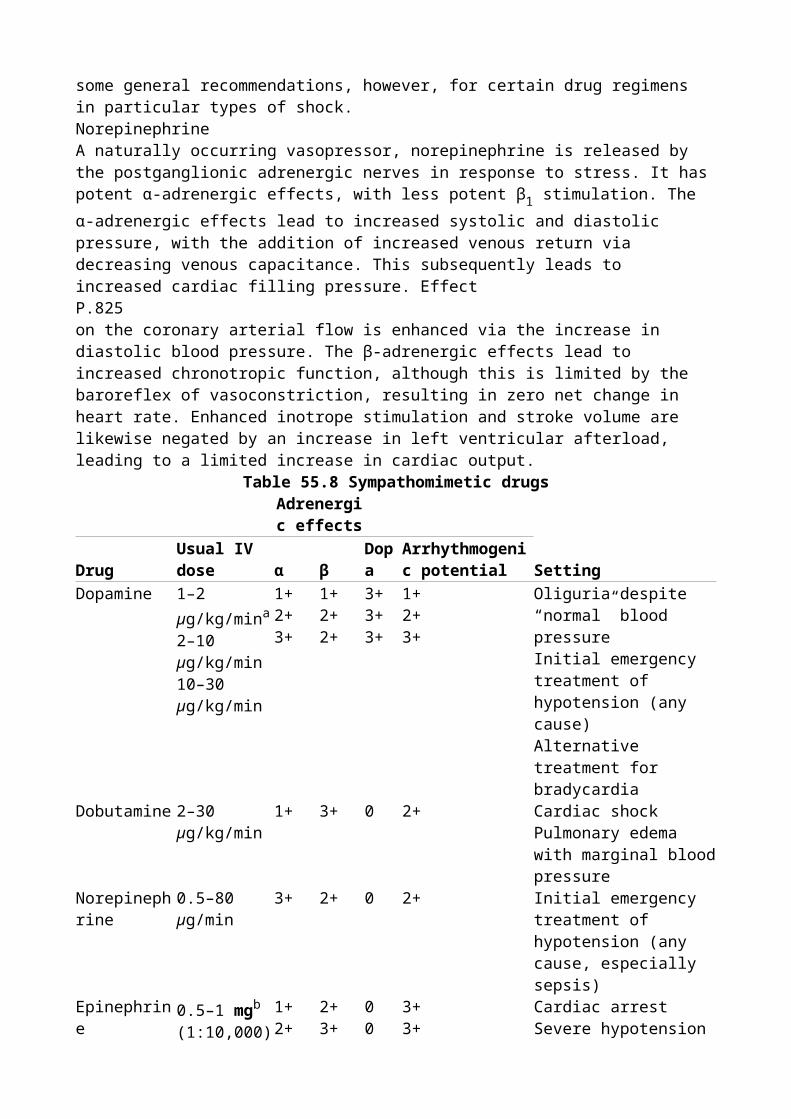
implicated in this process (95,165,166,167,168,169,170,171,172).
Figure 57.11. Cardiac index in resuscitated septic shock. The mean (standard error of the mean [SEM]) cardiac index plotted against time for all patients, survivors, and nonsurvivors. The hatched areas show the normal range. All groups maintained an elevated cardiac index throughout the study period. The difference between the survivors and nonsurvivors was not statistically significant. Open circles, survivors; closed circles, nonsurvivors. (Adapted from Parker MM, Shelhamer JH, Bacharach SL, et al. Profound but reversible myocardial depression in patients with septic shock. Ann Intern Med. 1984;100:483–490.)Organ System Dysfunction Due To Sepsis And Septic ShockTable 57.8 summarizes organ system dysfunction in sepsis and septic shock.Central Nervous SystemSeptic encephalopathy is the most common neurologic manifestation of sepsis and septic shock, encompassing between 8% and 80% of patients with sepsis (173,174,175,176). The likely reason for the divergent frequencies of the syndrome in studies is the difficulty of identifying the condition in patients with superimposed hypotension, sedation, hypoxemia, acidosis, electrolyte disturbances, hypoglycemia/hyperglycemia, hypothermia/hyperthermia, and/or concurrent hepatic/renal failure/encephalopathy. The diagnosis, requiring the presence of altered mentation with an extracranial source of infection, is often one of exclusion. Although deficits can range from impairment of higher cognitive functions to delirium or coma, asterixis, myoclonus, and seizure activity are highly atypical (173,176). The diagnosis is best made by electroencephalography (EEG) (177). The occurrence and severity of septic encephalopathy (graded by EEG or Glasgow coma scale) appears to be associated with increased mortality (as high as 70%) (173,178).Table 57.8 Organ System Dysfunction in Sepsis and Septic ShockCNS Septic encephalopathy Critical illness polyneuropathy/ myopathyHeart Tachycardia Supraventricular tachycardia Ventricular ectopy Myocardial depressionPulmonary Acute respiratory failure Adult respiratory distress syndromeKidney Prerenal failure Acute tubular necrosisGI Ileus Erosive gastritis Pancreatitis Acalculous cholecystitis Colonic submucosal hemorrhage Transluminal translocation of bacteria/antigensLiver Intrahepatic cholestasisHematologic Disseminated intravascular coagulation ThrombocytopeniaMetabolic Hyperglycemia Glycogenolysis Gluconeogenesis HypertriglyceridemiaImmune System
Neutrophil dysfunction
Cellular immune (T-cell/macrophage) depression
Humoral immune depression
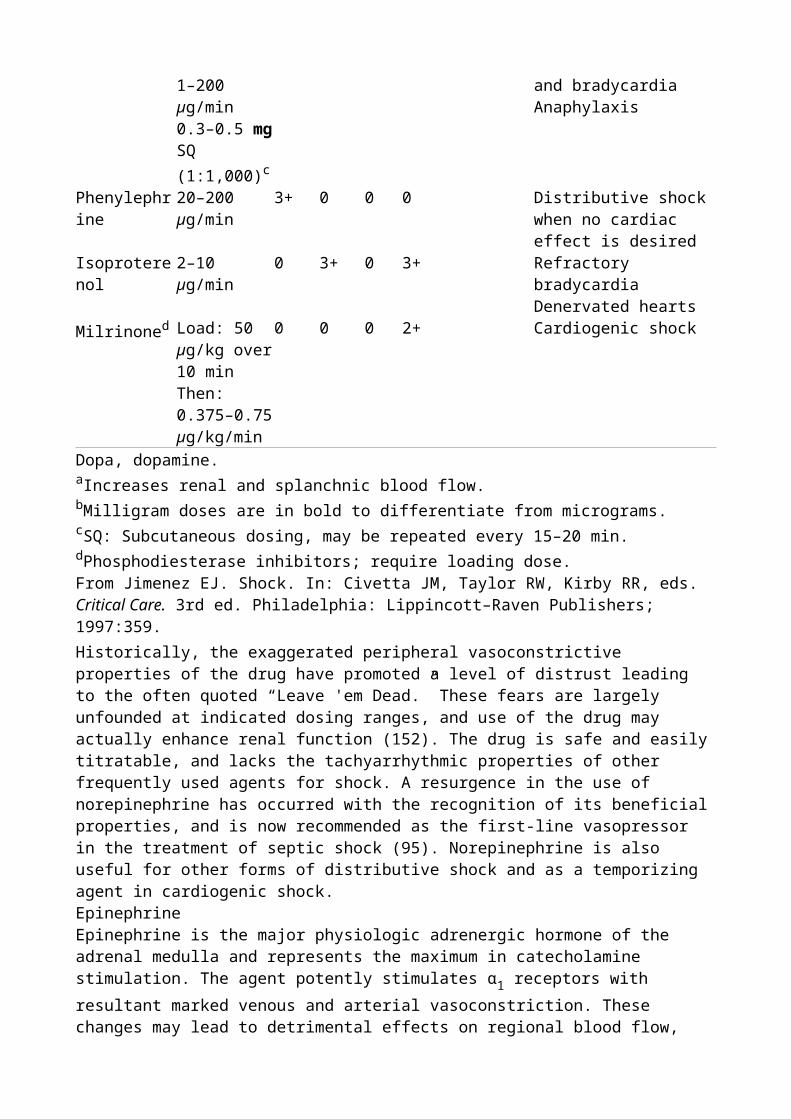
CNS, central nervous system; GI, gastrointestinal.Critical illness-associated neuromuscular syndromes (inclusive of critical illness polyneuropathy and myopathy) are the most common cause of neuromuscular problems in the ICU (179). The primary clinical manifestation of this condition is muscle weakness. Since many patients who are in the ICU with sepsis and septic shock require ventilatory support, the initial overt manifestation may be either respiratory failure or failure to wean from ventilation. Studies have suggested an incidence between 35% and 50% based on clinical criteria and 40% to 80% based on electromyography (EMG)/nerve conduction studies (180,181,182). Although the disorder is commonly P.869noted later in the recovery phase of sepsis and septic shock, EMG/nerve conduction data suggest that the onset is much earlier (concurrent or within days of the onset of septic shock) (183,184). The condition is a predominantly peripheral motor neuropathy in association with the presence of the systemic inflammatory response. Physical findings may include difficulty in weaning from the ventilator, symmetric paresis greater in the lower extremities, reduced deep tendon reflexes, and ataxia (180). A distal sensory neuropathy is also common. Approximately 25% of patients who are awake after a week on mechanical ventilation have significant weakness that lasts at least a week (185). The condition is considered to be an element of and is closely associated with the occurrence of MODS.Cardiovascular SystemThe major clinically apparent manifestations of shock on the heart are due to sympathoadrenal stimulation. Heart rate is almost universally increased in the absence of disturbances of cardiac conduction; the degree of increase is predictive of outcome (35). In addition, catecholamine-driven supraventricular tachycardias and ventricular ectopy with ischemic electrocardiography (ECG) changes, particularly in patients predisposed to myocardial ischemia, may be found.Like the brain, the blood supply to the heart is autoregulated, rendering it resistant to sympathetically driven vasoconstriction and shock-related hypoperfusion. Perfusion of the heart is unchanged or even increased during sepsis and septic shock (186,187). The occurrence of septic myocardial depression has already been addressed. Circulating myocardial depressant substances contribute to myocardial depression in sepsis and septic shock (188,189). This has been linked to decreased beta-adrenoreceptor affinity and density (190,191,192), as well as potential defects of intracellular signal transduction involving nitric oxide, G proteins, cyclic adenosine monophosphate (cAMP), and cGMP (95,193,194,195,196,197).Although septic myocardial depression is a transient phenomenon in survivors, myocardial cell injury as evidenced by increased troponin levels does occur (198,199). Serum troponin is elevated in almost half of patients with septic shock (without myocardial creatine kinase [CK-MB] elevation or ischemic ECG changes) (200). A correlation between left ventricular (LV) dysfunction and troponin I (TnI) positivity has been shown (199). Serum TnI correlated with left ventricular dysfunction and was an independent predictor of the need for inotropic/vasopressor support, adverse outcome, and mortality in septic shock patients (200). Whether the clinically inapparent myocardial cell injury that is the source of elevated troponin contributes to, or is a consequence of, septic shock is yet to be determined. Although troponin is used as a marker of myocardial injury (particularly in the context of myocardial ischemia), it does not specifically suggest myocardial infarction in other contexts.Respiratory SystemEarly respiratory responses to sepsis include tachypnea and hyperventilation. Gas exchange may be mildly abnormal. Later in the course of sepsis, patients may develop diffuse alveolar damage consistent with the acute lung injury (ALI) or adult respiratory distress syndrome (ARDS). Infections account for about one half of all cases of ARDS. These infections can involve local pneumonia or distant foci of infection associated with sepsis or septic shock. The risk of ARDS in association with sepsis increases with the severity of the syndrome (sepsis to septic shock) (201). From 40% to 60% of patients with Gram-negative septic shock develop ARDS. Sepsis is the single condition most closely associated with progression to acute lung injury or ARDS, with an incidence
of 40% (202). Several comorbid factors increase the risk of ARDS, including chronic alcohol abuse, chronic lung disease, and severe acidemia (202). Most patients with septic ARDS also have other organ failure, i.e., MODS. Death is more commonly due to MODS or the underlying sepsis, although the impact of low tidal volume ventilation in ARDS studies suggest that the lung injury may still play a significant role (perhaps as a source of persistent inflammatory stimulation) (202,203,204). The mortality of ARDS/MODS is approximately 40%, although some recent reports suggest that it may be decreasing (202,205). Failure to improve in the first week is associated with progression of the syndrome and poor prognosis, as are MODS, chronic liver disease, and age; interestingly, indices of oxygenation and ventilation are not predictive (202).RenalAcute renal failure (ARF) is a major complication of sepsis and septic shock and occurs with increasing frequency in relation to the severity of the syndrome, from 16% to 19% with sepsis to 51% with septic shock (31,201,206). Sepsis has been the leading cause of acute tubular necrosis (ATN) in some ICU studies, accounting for almost 50% of cases (207,208,209). Sepsis-associated acute renal failure is associated with a substantially higher mortality risk (75%) than nonseptic ARF (45%); within this group, septic shock mortality is higher (80%) than in those with severe sepsis (70%) (201,208). Compared with nonsepsis-associated ARF, sepsis-related ARF patients are significantly older, sicker, require mechanical ventilation more often, and present later in the hospital course more frequently (208).GastrointestinalThe gut is relatively sensitive to circulatory failure due to the responsiveness of the splanchnic vasculature to vasoconstrictive stimulation by extrinsic factors. In addition, gut tissues may have increased sensitivity to proinflammatory cytokine-driven inflammatory injury. Typical clinical gut manifestations of hypoperfusion, sympathetic stimulation, and inflammatory injury associated with sepsis and septic shock include ileus, erosive gastritis, pancreatitis, acalculous cholecystitis, and colonic submucosal hemorrhage (210). In addition, enteric ischemia produced by circulatory shock and free radical injury with resuscitation may breach gut barrier integrity (211,212). Some theories propose that enteric bacteria and antigens (notably endotoxin) may translocate from the gut lumen to the systemic circulation during gut ischemia, resulting in irreversible shock (213) and MODS (214).P.870HepatobiliaryTwo major forms of organ injury can be seen in the liver with sepsis and septic shock (215,216). “Shock liver” (ischemic hepatitis) is associated with massive ischemic necrosis and major elevations of transaminases, which can occur with septic shock and is atypical in the absence of extensive hepatocellular disease (217). When it does occur, it can contribute substantially to lactic acidosis since the liver accounts for most serum lactate clearance. Hypoglycemia may also be seen. Centrilobular injury with mild increases of transaminases and lactate dehydrogenase is much more common. Transaminases usually peak within 1 to 3 days of the insult and resolve over 3 to 10 days. In both cases, there are only mild increases in bilirubin and alkaline phosphatase in the early phase. Despite the production of acute-phase reactants in early sepsis and septic shock, synthetic functions may be impaired, with decreased generation of prealbumin, albumin, and hepatic coagulation factors (increased prothrombin time [PT]). After, or independent of, the occurrence of septic shock, evidence of biliary stasis with increased bilirubin and alkaline phosphatase may be present (216). Increases in transaminases are modest.HematologicSepsis and septic shock are associated with a range of hematologic disorders including overt disseminated intravascular coagulation (DIC), thrombocytopenia, and coagulopathy. Thrombocytopenia and coagulopathy are multifactorial in nature. Bone marrow suppression, consumption, and medications can contribute to thrombocytopenia, whereas consumption and decreased liver production of coagulant factors, as well as malnutrition (leading to depleted vitamin K stores), contribute to coagulopathy. Nonetheless, whenever these findings are present, early
disseminated intravascular coagulation (DIC) is possible.Septic shock is the single most common cause of DIC, characterized by microangiopathic hemolysis, consumptive thrombocytopenia, consumptive coagulopathy, and microthrombi with tissue injury. Overt DIC occurs in one quarter to one half of cases of Gram-negative sepsis (218). Although Gram-positive sepsis has been thought to be less closely associated with DIC, the frequency of occurrence is quite similar (218,219). The occurrence of DIC in sepsis is associated with a doubling of projected mortality (218,220). DIC may also represent both a driver and manifestation of MODS. The deposition of microvascular thrombi can cause significant endothelial injury and inflammatory responses, leading to ischemic and inflammatory tissue injury, the basis of MODS.A prolonged prothrombin time and partial thromboplastin time, hypofibrinogenemia, elevated level of fibrin split products, and the presence of the D-dimer herald the onset of disseminated intravascular coagulation. Since it is due to simultaneous systemic activation of coagulation and fibrinolysis cascades, it can be differentiated from the coagulopathy of liver failure by determination of endothelial cell-produced factor 8 (normal or increased with hepatic dysfunction). The pathogenesis of this disorder is linked to activation of tissue factor on endothelial cells and macrophages, probably by proinflammatory cytokines induced by exogenous bacterial toxins (220,221).MetabolicSpecific, predictable, and overlapping metabolic alterations occur in both sepsis and shock. Foremost among these is hyperglycemia. There are two reasons for hyperglycemia in sepsis and states of shock. Early in sepsis, when hemodynamic stress initiates compensatory responses, endogenous catecholamines are released as a consequence of enhanced sympathoadrenal stimulation. In addition, increased release of adrenocorticotropic hormone (ACTH), glucocorticoids, and glucagon with a concomitant decreased release of insulin results in glycogenolysis and gluconeogenesis (222,223). Increased epinephrine also results in skeletal muscle insulin resistance, sparing glucose for use by glucose-dependent organs such as the heart and brain (224). In addition, proinflammatory, stress-related cytokines such as TNF-α, IL-1β, and IL-6 contribute to insulin resistance in peripheral tissues (225). Pharmacologic therapies of sepsis and shock, including catecholamine vasopressors/inotropes, steroids, and total parenteral nutrition, can add to these effects. It is notable that, despite insulin resistance, the increased metabolic demands of sepsis also result in increased overall glucose uptake and utilization (226).With the evolution of sepsis to septic shock, metabolic responses progress. Late in shock, hypoglycemia may develop, possibly due to glycogen depletion or failure of hepatic glucose synthesis (227). Fatty acids are increased early in sepsis but fall later with hypoperfusion of adipose-containing peripheral tissue (226,228). Hypertriglyceridemia is often seen during shock as a consequence of catecholamine stimulation and reduced lipoprotein lipase expression induced by circulating TNF-α (223,226,229). Increased catecholamines, glucocorticoids, and glucagon also increase protein catabolism, resulting in a negative nitrogen balance (223,228).EndocrineEndocrine abnormalities are frequently underappreciated in sepsis and septic shock. Notable alterations in levels of pituitary, adrenal, thyroid, growth, and sex hormones are known to occur (225,230,231,232,233,234,235,236). In recent years, “relative” adrenal insufficiency in septic shock has received substantial attention. Few septic patients exhibit overt adrenal insufficiency. Relative bradycardia and a nontoxic appearance in a patient with septic shock is suggestive of this possibility. These are often elderly patients who have survived an initial episode of septic shock and either fail to fully recover or suffer a relapse. However, a considerable body of literature suggests that a suboptimal cortisol response (within the normal range) to sepsis and septic shock can have deleterious effects, including prolonged pressor dependence and increased mortality. Estimates of the frequency of adrenal insufficiency in septic shock vary wildly from 0% to 95% (237,238). In great part, this is due to the use of varying definitions based on baseline or cosyntropin-stimulated cortisol levels or changes in levels from baseline in response to cosyntropin. Common definitions in

septic shock patients include random cortisol of <700 nmol/L (25 µg/dL), peak postcosyntropin level of <500 to 550 nmol/L (1–20 µg/dL), or postcosyntropin change in cortisol of <200 to 250 nmol/L (7–9 µg/dL) (230,237,239,240). Interestingly, pituitary dysfunction may play a role in many
P.871patients with adrenal insufficiency, as 85% of critically ill patients have decreased levels of adrenocorticotropic hormone (ACTH) (241).Abnormalities of thyroid hormones are also present in sepsis and septic shock, although the clinical significance is less certain. In humans, serum T4 and T3 levels fall shortly after the onset of severe
clinical infection. Euthyroid sick syndrome is manifested by low serum levels of thyroid hormones in clinically euthyroid patients with severe nonthyroidal systemic illness. Decreased T3 levels are
most common. Patients with more severe or prolonged illness also have decreased T4 levels. Serum
reverse T3 (rT3) is increased. Patients are clinically euthyroid and do not have clinically significant
thyroid-stimulating hormone (TSH) elevations.Sepsis and septic shock are clearly associated with perturbations of various hormones including insulin, growth hormone, TSH, thyroxin, ACTH, cortisol, growth hormone (242), and sex hormones. Perturbations of hormones of the posterior pituitary should be expected. In addition to abnormal prolactin levels (243), sepsis and septic shock are accompanied by relative deficiencies of vasopressin/antidiuretic hormone (ADH) levels. Vasopressin, produced in the hypothalamus and stored in the posterior pituitary gland, is released in response to hyperosmolarity. Hypotension as seen in shock states is an even more powerful stimulus for release. Recent human studies have suggested a relative deficit of circulating vasopressin in patients with septic shock (relative to those with cardiogenic or hypovolemic shock). This deficiency may be related to depletion of neurohypophyseal stores combined with NO-mediated inhibition of production (225,235). Clinically, vasopressin exerts powerful vasopressor effects in hypotensive patients, particularly those with septic shock. To some extent, this effect appears to be mediated through reestablishment of reduced sensitivity to catecholamine (244).Diagnosis Of SepsisUnder ideal circumstances, each patient with evidence of sepsis would undergo a thorough evaluation at presentation prior to the initiation of therapy. In the context of sepsis and septic shock, circumstances are rarely ideal, so an abbreviated initial assessment focusing on critical diagnostic and management planning elements is frequently necessary.To ensure maximally rapid implementation of effective therapy, an initial presumptive diagnosis of severe sepsis and septic shock is mandated. The criteria for this presumptive diagnosis should be highly inclusive and based primarily on clinical criteria.The initial presumptive diagnosis of sepsis with organ dysfunction (severe sepsis) may be made in the presence of the following elements:
Suspected infection based on a minimal clinical constellation of localizing (e.g., dyspnea, cough, purulent sputum production, dysuria, pyuria, focal pain, local erythema, etc.) and systemic signs and/or symptoms of infection and sepsis (Table 57.9)
Clinical evidence of organ dysfunction (e.g., hypotension with peripheral hypoperfusion, oliguria, hypoxemia, obtundation, etc.)
Table 57.9 Clinical Symptoms/Signs for Presumptive Diagnosis of Severe Sepsis/Septic ShockFever or hypothermiaChills, rigorsTachycardiaWidened pulse pressureTachypnea or hyperpneaConfusion, decreased level of consciousness or delirium
Decreased urine outputHypotensionSimilarly, an initial diagnosis of septic shock is established in the presence of suspected infection with sustained hypotension without a definitive alternate explanation.The initial presumptive diagnosis of severe sepsis or septic shock is based on clinical criteria and does not require microbiologic, radiographic, or other laboratory evidence of specific infection or organ injury. Only clinical evidence of infection and organ failure is necessary. For the most part, available laboratory tests or imaging studies represent supportive, not diagnostic, elements. This clinical approach allows a parallel, rapid initiation of empiric antimicrobials and supportive measures.Although a suggestive clinical examination is sufficient for the presumptive diagnosis of severe sepsis and septic shock, more authoritative investigations (both laboratory and radiologic) are generally required for confirmation. For this reason, the definitive diagnosis of severe sepsis and septic shock involves a broader range of clinical and laboratory evidence of sepsis (Table 57.10) and organ dysfunction (arterial hypotension, lactic acidosis, or any organ dysfunction variables in Table 57.2). Establishment of a definitive diagnosis can help to more specifically target antimicrobial therapy and trigger specific therapies such as surgical source control and activated protein C.
Table 57.10 Supportive/Confirmatory Findings for Severe Sepsis/Septic ShockLeukocytosis, leukopenia, increased immature white blood cell (WBC) forms, toxic granulation, Dohle bodiesThrombocytopenia ± increased INR or prothrombin time (PT)Increased D-dimer or fibrin split productsIncreased serum bilirubin, AST/ALT, C-reactive proteinSerum procalcitonin elevationMetabolic acidosis with anion gapSerum lactate elevationRespiratory alkalosis or acidosisMixed venous saturation >70%Diagnostic imaging findingsPositive microbiologic or pathologic samples for abnormal presence of microorganisms, leukocytes, or tissue necrosisINR, international normalized ratio; AST/ALT, aspartate aminotransferase/alanine aminotransferase.P.872HistoryThe initial history should focus on two major areas: The key symptoms with respect to diagnosis of sepsis and of the specific site of infection, and key factors that would modify initial empiric therapies such as antimicrobials, fluid resuscitation, and possibly, vasopressors/inotropes.With respect to symptoms, constitutional complaints are entirely nonspecific. The classic pattern of fever, rigors, and chills is common but far from universal. Fatigue, malaise, anxiety, or confusion may be observed, particularly in the elderly. Occasionally, the elderly, the immunocompromised (nonspecific immune dysfunction due to chronic organ failure), and the immunosuppressed (specific immune defects) may present without classic signs and symptoms.Fever is a common feature of infection and/or sepsis. Fever is caused by a direct effect of inflammatory mediators, such as IL-1β, on the hypothalamus. The fever response may be suppressed in septic shock and may be absent in the elderly, immunocompromised, or immunosuppressed patient. Hypothermia in septic shock is associated with reduced cardiac output and portends a poor prognosis (245). Septic encephalopathy manifested by disorientation or confusion is especially common in elderly individuals. Apprehension, anxiety, and agitation may all occur early in the course. With severe disease (i.e., septic shock) or progression of sepsis, overt encephalopathy with a decreased level of consciousness and coma can occur. Hyperventilation with respiratory alkalosis can manifest even before the onset of metabolic acidosis as a consequence of

cytokine-mediated stimulation of the respiratory center in the medulla.Localizing symptoms as described in Table 57.11 may be more helpful in determining the septic cause of the constitutional manifestations of sepsis. The key historical factors used to modify initial therapies include antimicrobial sensitivities/allergies, recent infections/antimicrobial use, the locale of infection acquisition (i.e., nosocomial vs. community), and major comorbidities. The existence of comorbidities (e.g., AIDS; chemotherapy; hematologic malignancy; neutropenia resulting in immunosuppression or chronic renal, heart, liver, or other organ failure; COPD; dementia; inflammatory bowel diseases; diabetes; or via invasive catheters/devices) resulting in immunocompromise mandate the use of extended-spectrum antimicrobial therapy. Chronic renal, liver, or heart failure may also influence the choice and volume/dose of antimicrobials, resuscitation fluids, and vasopressors. Recent antimicrobial use and nosocomial or institutional acquisition of infection may also mandate consideration of extended-spectrum antimicrobial therapy to adequately cover nosocomial pathogens.
Table 57.11 Localizing Clinical Symptoms and Signs in Severe Infections History Physical examCentral nervous system
Headache, neck stiffness, photophobia
Meningismus (neck stiffness), focal neurologic signs (weakness, paralysis, paresthesia)
Head and neck Earache, sore throat, sinus pain, or swollen lymph glands
Inflamed or swollen tympanic membranes or ear canal, sinus tenderness, pharyngeal erythema and exudates, inspiratory stridor, and cervical lymphadenopathy
Pulmonary Cough (especially if productive), pleuritic chest pain, and dyspnea
Dullness on percussion, bronchial breath sounds, and localized crackles
Cardiovascular Palpitations, syncope New regurgitant valvular murmurIntra-abdominal Abdominal pain, nausea,
vomiting, diarrhea, purulent discharge
Abdominal distention, localized tenderness, guarding or rebound tenderness, and rectal tenderness or swelling
Pelvic/genitourinary
Pelvic or flank pain, vaginal or urethral discharge, and urinary frequency and urgency
Costovertebral angle tenderness, pelvic tenderness, pain on cervical motion, and adnexal tenderness
Skin/soft tissue/joint
Localized limb pain or tenderness, focal erythema, edema, and swollen joint
Focal erythema or purple discoloration (subcutaneous necrosis), edema, tenderness, crepitus in necrotizing infections (Clostridia and Gram-negative infections), petechiae, purpura, erythema, ulceration, and bullous formation and joint effusion
Adapted from Sharma S, Mink S. Septic shock. http://www.emedicine.com/MED/topic2101.htm. 2007. Accessed Dec. 1, 2007.Physical ExaminationThe physical examination should focus on ensuring that the patient is stable and on rapid localization of the site of infection. The physical examination should first ensure that the airway is patent, the patient is breathing satisfactorily, and vital signs and peripheral perfusion are acceptable.Tachypnea and tachycardia are almost universal. Normothermia and fever are consistent with sepsis, but hypothermia should be of concern due to its association with shock/hypoperfusion. All patients with sepsis should be observed for signs of hypoperfusion (mottling, pallor, diaphoresis, impaired capillary refill in nail beds). An acutely ill, flushed, and toxic appearance is common in the septic patient, particularly early in the course. In the early stages of sepsis, CO is well maintained or even increased, skin and extremities are warm, P.873and capillary refill is normal. As sepsis progresses, venodilation results in reduced central venous pressure and venous return. Hypovolemic manifestations with hypotension, reduced stroke volume, and CO with signs of tissue hypoperfusion develop. As patients are aggressively fluid resuscitated, a
hyperdynamic circulatory state (albeit with distributive shock) again dominates the clinical picture and will usually persist until recovery or death.The most common sites of infection causing sepsis and septic shock in order of frequency are respiratory, abdominal, urinary, and soft tissue. Abdominal infections are more closely associated with septic shock whereas urinary infections are more common in sepsis. Intravascular catheters are a frequently overlooked source of infection and sepsis. A recent study suggested that central venous catheters might account for as much as 3.7% of cases of septic shock (25). Similarly, cases of Clostridium difficile–related septic shock are often overlooked in the absence of overt toxic megacolon. Adding to the difficulty of managing the ICU patient with sepsis and/or septic shock is that many patients have simultaneous infection at more than one site.Laboratory StudiesPatients with sepsis require urgent lab testing to help make a firm diagnosis and to evaluate the severity of the illness. Sepsis and septic shock typically present with somewhat different, though naturally overlapping, laboratory parameters (see Table 57.12). Lab tests usually start with a complete blood count (CBC). Hemoglobin is often decreased, although this is usually due to the presence of chronic disease. Hemoglobin can occasionally be increased in patients with substantial interstitial third-spacing and relative hypovolemia. The white cell count is increased in sepsis but may transiently normalize or even drop below normal range, with progression to septic shock. Although this phenomenon has been linked to Gram-negative septic shock, it can be seen in septic shock due to any pathogen. Leukopenia in this setting has been linked to poor outcome. Toxic granulation and the presence of Dohle bodies are also seen more frequently, with progression to more severe disease. Similarly, a marked left shift with increasing immature forms (bands) is more common in septic shock. Platelets often respond as an acute-phase reactant, with increases early in infection/sepsis. However, platelet counts drop, with septic shock reaching a nadir around day 5 in survivors.
Table 57.12 Key Laboratory Values in Infection/Sepsis versus Septic Shock Sepsis Septic shockHb N or ↓ (chronic
disease)↑ (hemoconcentration)
WBC ↑ + left shift ↑, N or ↓ -marked left shift with metamyelocytes, toxic
granulation, and/or Dohle bodiesplatelets N or ↑ N or ↓PT/INR N or ↑ (malnutrition) ↑↑fibrinogen N or ↑ N or ↓Fibrin split products/ D-dimer activity
↑ ↑↑
Glucose N or ↑ ↑↑Cr/BUN N or ↑ ↑↑Bilirubin N, late ↑ ↑, late ↑↑AST/ALT N ↑-↑↑Albumin N or ↓ (malnutrition) ↓↓ (endothelial leakage/interstitial redistribution)ABG respiratory alkalosis metabolic acidosisHCO3
- N ↓
lactate N ↑-↑↑C-reactive protein ↑ ↑↑procalcitonin ↑ ↑↑Blood culture positivity 5%–10% 30%–40%↑ increase, ↑↑ marked increase, ↓ decrease, ↓↓ marked decrease, N normal. Hb, hemoglobin; WBC, white blood cell count; PT, prothrombin time; INR, international normalized ratio; Cr/BUN, serum creatine and blood urea nitrogen; AST/ALT, serum aspartate transaminase and alanine transaminase;
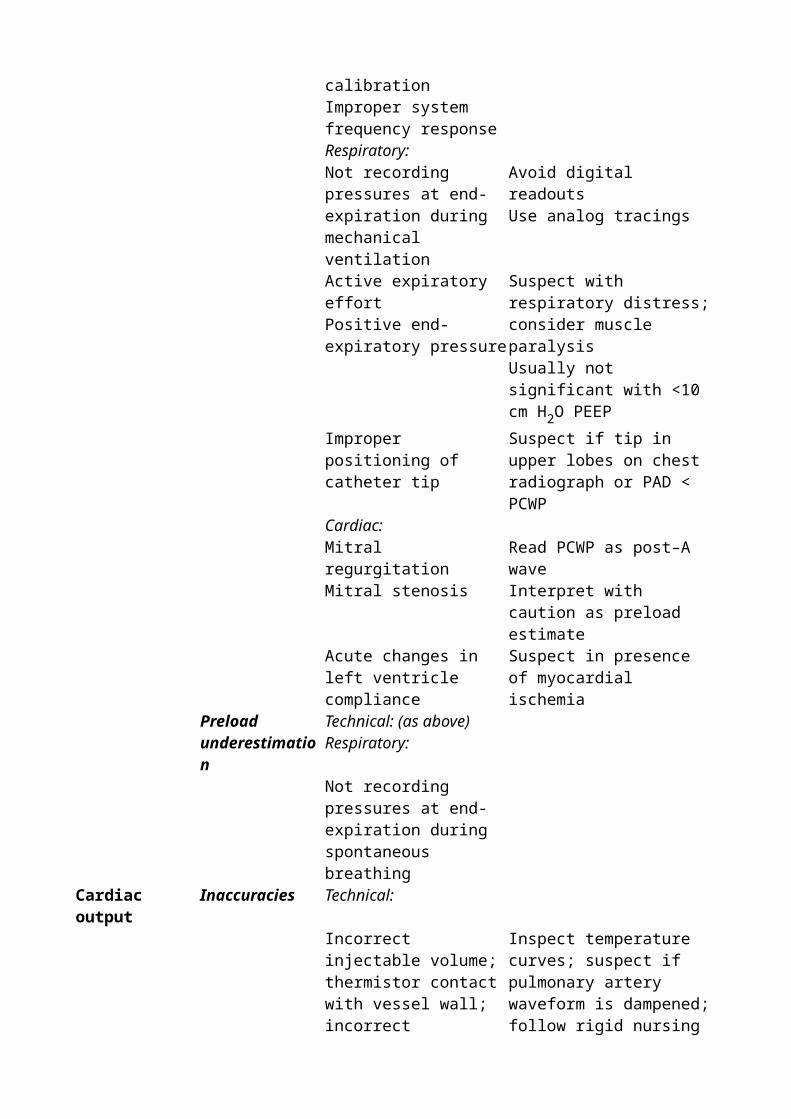
ABG, arterial blood gas; HCO3-, serum bicarbonate concentration.
In contrast, the international normalized ratio (INR) may be mildly abnormal at the onset of sepsis (due to malnourishment) and is usually most abnormal at onset of septic shock. Fibrinogen is an acute-phase reactant and is usually elevated with onset of infection/sepsis. However, levels will drop with septic shock, especially if DIC intervenes. Fibrin split products and D-dimers are very sensitive markers of progression of sepsis and are almost universally elevated with septic shock.Serum creatinine and blood urea nitrogen (BUN) may actually be decreased due to increased renal blood flow in the early hyperdynamic phase of sepsis but will increase with the onset of septic shock. An increase in serum creatinine denotes an increased mortality risk even within a few hours of the onset of septic shock. Similarly, elevated serum lactate is closely correlated with increased mortality risk in septic shock.P.874Septic patients should have both site-specific and blood cultures drawn prior to initiation of antimicrobial therapy. In the case of septic shock, however, antimicrobial therapy should never be delayed to accommodate these cultures because of the antimicrobial delay-dependent increase in mortality risk (25). Gram stain should be performed on all site samples. Although there are some data to suggest that Gram stain is not useful in the initial management of certain infections (nosocomial pneumonia, peritonitis due to bowel perforation), a good specimen, appropriately interpreted, can provide invaluable information.Imaging StudiesAlthough in most cases the clinical examination will localize the source of infection with a reasonable degree of confidence, basic radiographic imaging can be very useful in cases where an obvious site of infection is not apparent. Advanced imaging studies (computerized axial tomography [CAT], magnetic resonance imaging [MRI], ultrasound) rarely yield information regarding localization of the infection that has not been provided by the clinical examination and basic imaging studies. However, these techniques may be highly useful when definitive or precise localization and/or delineation of extent of disease are required.A chest radiograph should be obtained in most patients admitted to the hospital with sepsis. Elderly, immunocompromised, and immunosuppressed patients with occult sepsis will often be found to have a pulmonary source on radiographic examination. Supine and upright or lateral decubitus abdominal films are useful if bowel perforation is of concern. In the appropriate clinical context of crepitus, bullae, hemorrhage, or foul-smelling exudate with intense local pain, evidence of gas in soft tissues on plain extremity radiographs is almost pathognomonic of necrotizing soft tissue infection with clostridia or facultatively anaerobic Gram-negative bacilli.CT scan with contrast is the preferred imaging modality to rule out intra-abdominal, intracranial, epidural, perinephric, and soft tissue abscesses, as well as retroperitoneal abscess or mediastinal infection. They can also be useful for localizing bowel wall injury and assessing necrotizing soft tissue infections (although MRI is preferred for the latter). Ultrasound is the initial imaging modality of choice for biliary sepsis and obstructive uropathy, although CT scan is also sensitive and specific.Management of Severe Sepsis and Septic Shock (i.e., The Sepsis Six-Pack)To optimize outcome in sepsis with organ dysfunction (severe sepsis), the initiating triggers, amplification cascade, and downstream organ dysfunction must be addressed; this requires monitoring and therapeutic elements. With respect to the initiating triggers, antimicrobials and, where possible, surgical and nonsurgical source control are mandated. With respect to the amplification cascade, one new agent (activated protein C) has been developed that directly dampens septic response by exerting both anti-inflammatory and antithrombotic effects, such that mortality is improved. Organ dysfunction is addressed through direct supportive measures. The most immediate of these—fluid and vasopressor/inotropic resuscitation—support the circulatory system. However, mechanical ventilation and dialysis have also been shown to improve outcome in severe sepsis and septic shock.
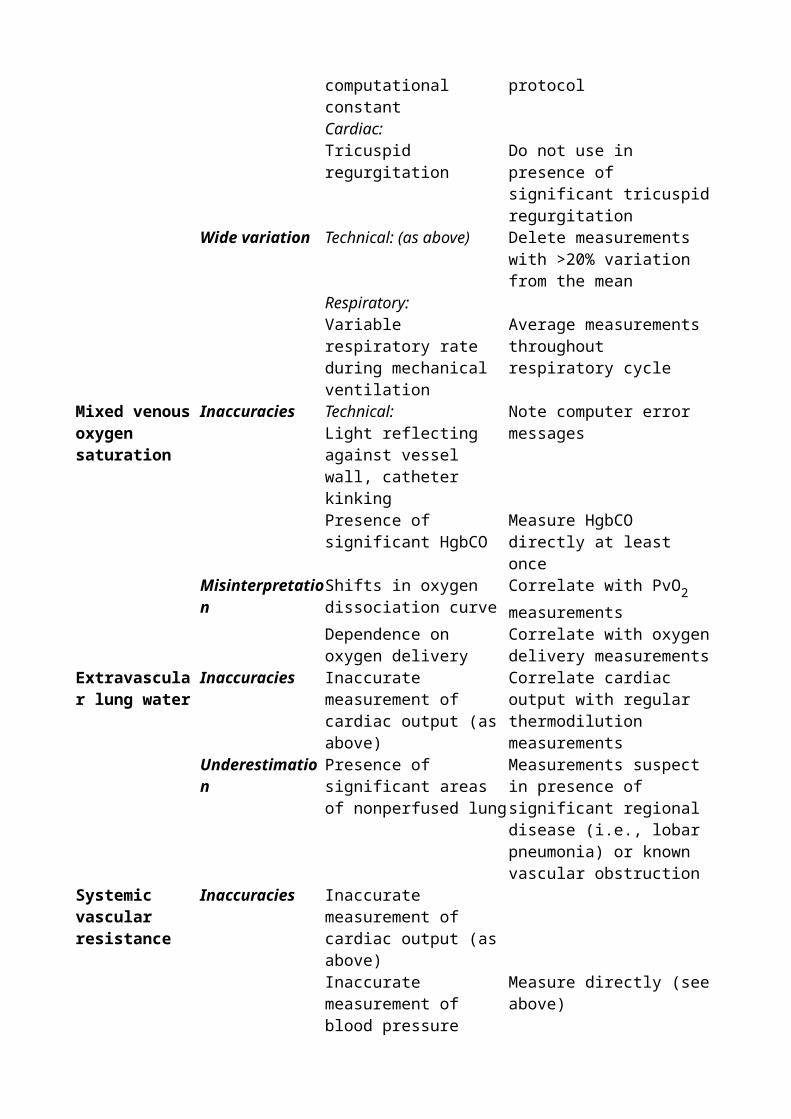
Six major areas in the evaluation and treatment of severe sepsis can be identified. These include the following:
Fluid resuscitation Antimicrobial therapy Vasopressors and inotropes Invasive and noninvasive monitoring Specific therapy Miscellaneous supportive therapy
Fluid ResuscitationThe development of shock in patients with sepsis involves disturbances of global and regional perfusion. Initially, ventricular filling pressures as reflected by CVP and pulmonary wedge pressure (PWP) are decreased. As a consequence, venous return falls, resulting in limitation of CO. Although an increase in insensible losses and decreased fluid intake may contribute to this effect, nitric oxide–mediated venular dilatation and loss of endothelial barrier integrity (resulting in a drop in colloid oncotic pressure from loss of albumin into the interstitium) probably play a dominant role (246,247). A significant degree of hypovolemia is almost universal in early, untreated severe sepsis or septic shock. Available data suggest that initial isotonic fluid deficits can exceed 10 L (248).Management of sepsis requires consideration of both global and regional perfusion defects, making the establishment of goals for therapy more complex than for other forms of shock. Support of global perfusion takes initial precedence. Since hypovolemia is a major factor in the hypotension and hypoperfusion of early septic shock, foremost among the appropriate initial therapeutic considerations is infusion of intravascular fluids. Fluid infusion should be implemented rapidly by large-bore peripheral intravenous catheters. Infusion of fluids can improve global perfusion indices (blood pressure, CO, and MvO2/central venous oxygen saturation [ScvO2]) and may reveal the
presence of regional perfusion disturbances and/or myocardial depression that may require therapy with vasopressors/inotropes.The three issues to consider in optimizing fluid resuscitation are the type of fluid used, the rapidity of infusion, and the amount of fluid administered.Initial resuscitation of septic patients should be aimed at rapid intravascular volume expansionThe view that intravascular fluid depletion plays a central role in the pathogenesis of early septic shock has been recognized since the past midcentury. Several studies suggested that septic shock is associated with reduced total circulating blood volume (149,150). Since almost all untreated patients with severe sepsis or septic shock have a significant element of hypovolemia, a hypodynamic circulation with decreased cardiac output is typical prior to fluid resuscitation. This hypovolemia is probably the basis of early observations that death in sepsis is associated with decreased cardiac output. The patients in those studies were clearly inadequately P.875resuscitated by current standards (149,150). Additional support for the central importance of functional hypovolemia in early septic shock comes from a more recent demonstration that the venous oxygen saturation is decreased in early preresuscitation septic shock (consistent with the findings in other forms of hypodynamic shock) (161).Aggressive fluid loading is the standard early therapy of septic shock and results in the generation of a hyperdynamic circulatory state in over 90% of patients (249). Rapid fluid resuscitation may reveal severe sepsis without shock in a significant subset of patients with apparent septic shock (248). Increased total blood volume has been associated with higher cardiac output and increased survival in human septic shock (150). Intravascular volume dependence of the hyperdynamic circulatory state in sepsis has been confirmed in animal models (158). Although the demonstration that resuscitation from hypovolemia improves outcome in traumatic shock dates back to the early work of Cannon (250) and Cournand et al. (251), clear evidence that early aggressive fluid resuscitation improves outcome in septic shock is limited to a small series of pediatric septic shock (252) and a recent randomized study of goal-directed resuscitation (253).
Initial fluid resuscitation should be titrated to specific clinical end pointsAggressive fluid loading in patients with septic shock can increase total blood volume, cardiac output, oxygen delivery, and consumption while reducing lactic acidosis (119). Older studies have suggested that an increased blood volume associated with normalization of cardiac output is associated with improved survival (149,150).In the absence of early invasive or echocardiographic monitoring, clinical end points can be used for titration of fluid resuscitation. Since both initial heart rate and blood pressure have been shown to be associated with outcome in septic shock as well as hypovolemic shock (35,254,255,256), standard goals may include the following:
Heart rate ≤100 beats/minute Systolic blood pressure (≥90 mm Hg) Mean arterial pressure (≥60–65 mm Hg) Urine output (≥0.5 mL/kg/hour)
It should be noted that these clinical parameters can underestimate initial resuscitative requirements in critically ill subjects including those with septic shock (257,258,259).Mortality in both septic and other forms of shock has also been associated with increased arterial lactate and base deficit levels (260). Normalization of these parameters can be used to augment clinical end points for titration of fluid resuscitation (261). However, both parameters represent relatively late responses to cellular stress, and resolution may similarly lag following the implementation of effective resuscitation (262).Initial fluid resuscitation should be achieved using isotonic crystalloid solutionsEffective fluid resuscitation can be delivered with either isotonic crystalloid (e.g., normal saline, lactated Ringer solution) or colloid solutions (e.g., hydroxyethyl starch, human albumin). All of these solutions are equally effective if titrated to the same clinical end points. Given the difference in distribution of such compounds, it typically requires approximately four times more crystalloid to achieve the same hemodynamic effect as a given amount of colloid (263). Several animal and human studies have pointed out theoretical advantages to colloids in limiting interstitial fluid accumulation (which may benefit ARDS) in sepsis and septic shock (264,265,266). However, no clinical study has suggested improved clinical outcomes (morbidity or mortality) with colloid solutions (267,268). Although the severe sepsis subset of one recent randomized controlled trial (RCT) trended toward a more favorable outcome with albumin resuscitation (269), another (meta-analytic) study suggested an opposite trend toward increased mortality with albumin use (268,270). In addition, colloids are substantially more expensive than crystalloid solutions. For these reasons, isotonic crystalloids are recommended as the initial resuscitative solution for severe sepsis and septic shock. The development of a hyperchloremic acidosis can be anticipated with use of large volumes of normal saline. Use of lactated Ringer solution may limit this effect. Hypertonic saline is not recommended for the routine resuscitation of septic shock.Rapid volume expansion (500 mL isotonic crystalloid every 10–30 minutes) should be continued until clinical and physiologic treatment targets are met. Vasopressor/inotropic support is required if fluid infusion alone fails to achieve physiologic response targetsEarly aggressive resuscitation to achieve physiologically normal hemodynamic goals reduces subsequent morbidity and mortality in patients with septic shock. In a pediatric population with septic shock, rapid fluid resuscitation in the first hour of presentation to hospital improved survival (252). In an adult study, the effect of early goal-directed resuscitation to normal physiologic values in patients presenting to an emergency department with severe sepsis or septic shock was examined (253). All patients (both conventional and goal-directed therapy groups) were resuscitated in the emergency room for the first 6 hours to standard hemodynamic end points of CVP ≥8 mm Hg, MAP ≥65 mm Hg, and urine output ≥0.5 mL/kg per hour. The experimental early goal-directed therapy group, in addition, was managed using an experimental protocol to achieve both the standard goals and a central venous oxygen saturation ≥70% (as measured by an oximetric central venous catheter). During the 6 hours of their protocolized emergency room support, the experimental group
received 1.5 L more fluid than the control group, and a substantially larger fraction of the patients in the experimental group achieved the physiologic resuscitative goals (99.2% vs. 86.1%). Overall mortality was significantly lower in the early goal-directed therapy group.Antimicrobial Therapy and Source ControlHistorically, critically ill patients with overwhelming infection have not been considered a unique subgroup comparable to neutropenic patients for purposes of selection of antimicrobial therapy. However, critically ill patients with severe sepsis and septic shock, similar to neutropenic patients, are characterized by distinct differences from the typical infected patient that impact on the optimal management strategy. These differences include the following:
Marked alterations in antibiotic pharmacokinetics Increased frequency of hepatic and renal dysfunction High prevalence of unrecognized immune dysfunction Predisposition to infection with resistant organisms Marked increase in frequency of adverse outcome if there is a failure of rapid initiation of
effective antibiotic therapy
P.876Critical management decisions in this patient group must often be made emergently in the absence of definitive data regarding the infecting organism and its sensitivity pattern, patient immune status, and organ function. Since outcomes in severe sepsis and septic shock are strongly influenced by the rapidity of administration of an appropriate antimicrobial regimen at first presentation, a particularly thoughtful and judicious approach to initial empiric antimicrobial therapy is required (271,272,273).Empiric antibiotic regimens should approach 100% coverage of pathogens for the suspected source of infectionInitial administration of inappropriate antimicrobials increases morbidity in a wide range of infections. The occurrence of initiation of inadequate antimicrobial therapy may occur as frequently as 17.1% in community-acquired and 34.3% in nosocomial bacteremia in patients admitted to the ICU (273). Similarly, 18.8% and 28.4% of septic shock cases were initially treated with inadequate antimicrobial therapy in another large study (274). Retrospective studies have shown that the risk of death increases from 30% to 60% in ICU bacteremia (4,272) to 70% to 100% in Gram-negative shock (4) when the initial empiric regimen fails to cover the inciting pathogen. More recent data suggest that the survival of septic shock with inappropriate initial antimicrobial therapy is reduced approximately 5-fold (range 2.5 to 10-fold in selected subgroups) to about 10% (274). These findings of a sharply increased mortality risk with initial inadequate antimicrobial therapy apply to serious infections caused by Gram-negative and Gram-positive bacteria as well as Candida species (4,274,275,276,277,278).As a consequence, empiric regimens should err on the side of overinclusiveness. The most common cause of initiation of inappropriate antimicrobial therapy is a failure of the clinician to appreciate the risk of infection with antibiotic-resistant organisms (either uncommon organisms with increased native resistance or antibiotic-resistant isolates of common organisms). Selection of an optimal antimicrobial regimen requires knowledge of the probable anatomic site of infection; the patient's immune status, risk factors, and physical environment; and the local microbiologic flora and organism resistance patterns. Risk factors for infection with resistant organisms include a prolonged hospital stay, prior hospitalization, and prior colonization or infection with multiresistant organisms.
Table 57.13 Indication for Extended Empiric Antibiotic Therapy of Severe Sepsis/Septic Shock
↑ Gram-negative coverage Nosocomial infection Neutropenic or immunosuppressed Immunocompromised due to chronic organ failure
(liver, renal, lung, heart, etc.)
↑ Gram-positive coverage (vancomycin)
High-level endemic MRSA (community or nosocomial)
Neutropenic patient Intravascular catheter infection Nosocomial pneumonia
Fungal/yeast coverage (triazole, echinocandin, amphotericin B)
Neutropenic fever or other immunosuppressed patient unresponsive to standard antibiotic therapy
Prolonged broad-spectrum antibiotic therapy Positive relevant fungal cultures Consider empiric therapy if high-risk patient with
severe shock
MRSA, methicillin-resistant Staphylococcus aureus.Superior empiric coverage can be obtained through the use of a local antibiogram or via consultation with an infectious disease specialist (279). Although not routinely required, extended-spectrum Gram-negative regimens, vancomycin, and/or antifungal therapy may be appropriate in specific high-risk cases with severe sepsis (Table 57.13). In addition, given that 90% to 95% of patients with septic shock have comorbidities or other factors that make them high risk for resistant organisms, it may be appropriate to initially treat all patients with septic shock using a combination of antimicrobials that result in a broadly expanded spectrum of coverage for the first few days. This approach should improve the adequacy of antimicrobial coverage initially, while ensuring that high-risk patients are not inappropriately categorized as low risk.Intravenous administration of broad-spectrum antimicrobials should be initiated immediately (preferably <30 minutes) following the clinical diagnosis of septic shockAppropriate intravenous, empiric broad-spectrum therapy should be initiated as rapidly as possible in response to clinical suspicion of infection in the presence of hypotension, i.e., presumptive septic shock. An assumption that hypotension is caused by anything other than sepsis in the setting of documented or suspected infection should be avoided, unless there is very strong data indicating a specific alternate cause. Retrospective studies of human bacteremia, pneumonia, and meningitis with sepsis suggest that mortality in sepsis increases with delays in antimicrobial administration (271,278,280,281,282). One major retrospective analysis of septic shock has suggested that a delay in the initial administration of effective antimicrobial therapy is the single strongest predictor of survival (25). Initiation of effective antimicrobial therapy within the first hour following the onset of septic shock-related hypotension was associated with 79.9% survival to hospital discharge. For every additional hour to effective antimicrobial initiation in the first 6 hours post onset of hypotension, survival dropped an average of 7.6%. With effective antimicrobial initiation between the first and second P.877hour post hypotension onset, survival had already dropped to 70.5%. With effective antimicrobial therapy delay to 5 to 6 hours after hypotension onset, survival was just 42.0%, and by 9 to 12 hours, 25.4%. The adjusted odds ratio of death was already significantly increased by the second hour post hypotension onset, and the ratio continued to climb with longer delays.Substantial delays before initiation of effective therapy have been shown in several studies of serious infections (271,282,283,284). In septic shock, the median time to delivery of effective antimicrobial therapy following initial onset of recurrent/persistent hypotension was 6 hours (25).A potential survival advantage may exist if a pathogenic organism can be isolated in severe infections, including septic shock. Every effort should be made to obtain appropriate site-specific cultures to allow identification and susceptibility testing of the pathogenic organism; however, such efforts should not delay antimicrobial therapy.Antimicrobial therapy should be initiated with dosing at the high end of the therapeutic range in all patients with life-threatening infection
Early optimization of antimicrobial pharmacokinetics can improve the outcome of patients with severe infection, including septic shock. This is most easily achieved by initiating antibiotic therapy with high-end dosing regimens.Early in sepsis, before the onset of hepatic or renal dysfunction, cardiac output is increased in many patients. In association with increased free drug levels due to decreased albumin levels, drug clearance can be transiently increased (285). As the illness progresses, ICU patients with sepsis or septic shock exhibit substantially increased volumes of distribution and decreased clearance rates. Consequently, suboptimal dosing of antibiotics is common in these conditions (286,287,288,289,290,291). Data is most well developed in reference to aminoglycosides but also exists for fluoroquinolones, β-lactams, and carbapenems (286,287,288,289,290,291). Failure to achieve targets on initial dosing has been associated with clinical failure with aminoglycosides (292,293). Similarly, clinical success rate for treatment of serious infections tracks with higher peak blood levels of fluoroquinolones (nosocomial pneumonia and other serious infections) (294,295,296) and aminoglycosides (Gram-negative nosocomial pneumonia and other serious infections) (297,298). Although there are extensive data in experimental animals and less serious human infections, data for optimization of outcomes using β-lactams in critically ill, infected patients is relatively limited (299,300). A single recent paper has shown improved survival in patients with Pseudomonas bacteremia when treated with extended infusions rather than standard intermittent dosing of piperacillin/tazobactam (301).Achievement of optimal serum concentrations of aminoglycosides (peak antibiotic serum concentration:pathogen minimal inhibitory concentration [MIC] ratio of ≥12) and longer periods of bactericidal β-lactam and carbapenem serum concentrations (minimum time above MIC in serum of 60% of dosing interval) are appropriate goals (294,302,303). This can most easily be attained with once-daily dosing of aminoglycosides (304). For β-lactams and related antibiotics, increased frequency of dosing (given identical total daily dose) is recommended. For example, piperacillin/tazobactam can be dosed at either 4.5 g every 8 hours or 3.375 g every 6 hours for serious infections; all things being equal, the latter would achieve a higher time above MIC and should be the preferred dosing option. A similar dosing approach should be used for other β-lactams in critically ill patients with life-threatening infections. Limited data suggest that continuous infusion of β-lactams and related drugs may be even more effective, particularly for relatively resistant organisms (305,306,307,308,309).Multidrug antimicrobial therapy is preferred for the initial empiric therapy of septic shockProbable pathogens should be covered by at least two antimicrobials with different bactericidal mechanisms. Given that highly resistant organisms are endemic in the critical care environment, multidrug antimicrobial therapy will reduce the probability of failure to cover these organisms. In addition, most patients with septic shock (even those without specific pre-existing immune defects) exhibit significant deficits of neutrophil and monocyte function during the course of their illness (310,311,312,313,314,315,316). Furthermore, malnutrition and organ dysfunction (e.g., renal or hepatic failure), which are common in ICU patients, suppress cell-mediated immunity. Based on these data, septic shock patients likely have a reduced ability to clear infection and may be best managed with multidrug therapy similar to that recommended for patients with neutropenic sepsis (317,318).No prospective controlled study has specifically compared multiple versus single antimicrobial therapy in a broad range of severe sepsis or septic shock patients. Most infectious diseases physicians and other experts suggest no advantage to multidrug therapy in serious infections, including bacteremia (319,320). However, a subgroup analysis of the sickest subset of patients with Gram-negative bacteremia, with or without shock, has tended to suggest improved survival with the use of two or more antibiotics to which the causative organism is sensitive (321,322,323,324). Similarly, at least two retrospective and one prospective analyses of the most severe, critically ill patients with bacteremic pneumococcal pneumonia suggested improvement in outcome if two or more effective agents were used (325,326,327). This occurred even as patients with pneumococcal bacteremia with a lower severity of illness demonstrated no such benefit (325). A recent secondary
analysis of a prospective study of community-acquired pneumonia has shown benefit with multidrug therapy compared to monotherapy but only in the subset of septic shock (328).Empiric antimicrobial therapy should be adjusted to a narrower regimen within 48 to 72 hours if a plausible pathogen is identified or if the patient stabilizes clinically (i.e., resolution of shock)Although several retrospective studies have demonstrated that inappropriate therapy of bacteremic septic shock yields increased mortality (4,272,276,277,278), none have suggested that early narrowing of antibiotic therapy is detrimental if the organism is identified or if the patient is responding well clinically. This approach will maximize appropriate antibiotic coverage of inciting pathogens in septic shock while minimizing selection pressure toward resistant organisms. Although it is tempting to continue a broad-spectrum regimen in the 15% of improving patients who are culture-negative for a potential pathogen, intensivists must recognize that a strategy of broad-spectrum initial antimicrobial therapy will be sustainable only if overuse of these agents can be avoided. Aggressive de-escalation of antimicrobial therapy within 48 to 72 hours after initiation is required.P.878Where possible, early source control should be implemented in patients with severe sepsis, septic shock, and other life-threatening infectionsSource control is a critical issue in the management of infection associated with severe sepsis. Infections found in ICU patients frequently require source control for optimal management. The need for such source control may initially be overlooked in many infections commonly found in the ICU (e.g., pneumonia-associated bacterial empyema, decubitus ulcers, C. difficile colitis). Causes of septic shock where source control may be required are noted in Table 57.14.Table 57.14 Common Sources of Severe Sepsis/Septic Shock Requiring Urgent Source ControlToxic megacolon or C. difficile colitis with shockIschemic bowelPerforated viscusIntra-abdominal abscessAscending cholangitisGangrenous cholecystitisNecrotizing pancreatitis with infectionBacterial empyemaMediastinitisPurulent tunnel infectionsPurulent foreign body infectionsObstructive uropathyComplicated pyelonephritis/perinephric abscessNecrotizing soft tissue infections (necrotizing fasciitis)Clostridial myonecrosisSource control may include removal of implanted or tunneled devices, open surgical/percutaneous drainage of infected fluids or abscesses, and surgical resection of infected tissues. In a broader sense, it is inclusive of elimination of inciting chemotherapies (e.g., antibiotics driving C. difficile colitis or chemotherapy causing gut injury). Efforts to identify infections requiring invasive forms of source control frequently require rapid (<2 hours) radiographic imaging (often CT scan) or, if clinical status and findings are supportive, direct and immediate surgical intervention without an imaging effort. With rare exceptions, surgical source control should follow aggressive resuscitative efforts to minimize intraoperative morbidity and mortality. In some cases (e.g., rapidly progressive necrotizing soft tissue infections, bowel infarction), optimal management mandates simultaneous aggressive resuscitation and surgical intervention. Subgroup analysis in at least one large prospective, severe sepsis study has suggested that failure to implement adequate source control is associated with increased mortality (329). Earlier surgical intervention has been shown to have a significant impact on outcome in certain rapidly progressive infections such as necrotizing fasciitis
(330,331). In a large retrospective study of septic shock, time from hypotension to implementation of source control was found to be highly correlated with outcome (332).The necessity for or efficacy of source control efforts should be reassessed within 12 to 36 hours following admission and/or source control efforts should be based on clinical response.Vasopressors and InotropesFollowing fluid resuscitation, patients with severe sepsis or septic shock may demonstrate persistent vasomotor dysfunction characterized by regional perfusion deficits with or without systemic hypotension despite normal or increased CO. Clinical manifestations may include lactic acidosis and ongoing progression of organ failure.Until recently, the only available approach to correction of regional perfusion defects was vasopressor therapy. Unfortunately, vasopressors do not represent a specific therapy for this problem. Their primary use is to increase systemic arterial pressure to a range that potentially sustains the ability of the vasculature to autoregulate flow on a tissue and organ level (333,334). This allows vital organ perfusion to be supported (potentially at the expense of peripheral perfusion) until definitive therapy (infection source control and antibiotics) can be implemented.The aim of vasopressor/inotropic therapy in septic shock is simply the optimization of critical organ and tissue perfusion. However, the specific global and/or regional perfusion goals required to achieve this result are complex and controversial. Although specific targets can be suggested, therapy for each patient must be highly individualized and dynamic. Appropriate goals will change over time and should be re-evaluated on a continuing basis.If hypotension and/or clinical evidence of tissue hypoperfusion persist after adequate fluid resuscitation of septic shock, vasopressor therapy is indicated. Norepinephrine and dopamine are both effective as initial therapyInitiation of vasopressor support is dependent on the patient's clinical status following fluid resuscitation. If systemic hypotension in association with evidence of tissue/organ hypoperfusion (oliguria, obtundation, lactic acidosis) persists, vasopressor support is indicated. Selection of a vasopressor agent is based on an individualized assessment of the patient's needs. The patient's hemodynamic presentation, the anticipated cardiovascular effect of each vasoactive agent (based on the distribution of receptor activity), and the physician's experience and comfort with each drug should be considered. As a consequence of the variety of factors that may play a role in vasopressor selection, septic shock patients with a predominantly distributive hemodynamic pattern can be appropriately and effectively managed with one of several vasopressors including dopamine, norepinephrine, or phenylephrine.Ideally, patients should have achieved the targeted intravascular volume status prior to initiation of vasopressors. Although vasopressors can be used to maintain blood pressure for brief periods while intravascular volume is repleted, the infusion of high-dose vasopressors to volume-depleted patients may substantially aggravate ischemic organ injury.Studies suggesting that norepinephrine is superior to dopamine are less than definitive (335,336,337,338,339,340). No controlled study has directly assessed norepinephrine and dopamine in terms of survival, and few have compared the two agents with respect to markers of organ dysfunction. Studies assessing the effects of these agents on renal and splanchnic perfusion have been mixed, with neither agent demonstrating conclusive superiority (336,337,340,341,342,343,344,345,346,347). Norepinephrine may have more powerful vasopressor activity than dopamine (348). In addition, its inotropic effects are mediated by direct activity on myocardial β-adrenoreceptors. Dopamine pressor effects are weaker than those of norepinephrine, and inotropic effects are substantially indirect (through stimulation of release of myocardial catecholamine stores); excessive tachycardia may be P.879more common. In addition, dopamine may exert significant immunosuppressive effects through suppression of prolactin production from the hypothalamus (349). Phenylephrine, a relatively pure β-adrenergic agonist, has minimal or absent inotropic effects and tends to cause reflex bradycardia. For that reason, it can be very useful in the context of excessive tachycardia or concurrent
tachyarrhythmias. However, phenylephrine consistently decreases cardiac output and has an increased propensity to cause ischemic complications. Despite potent inotropic and vasopressor activity, epinephrine is not commonly used as the initial pressor therapy in septic shock because it can generate profound tachycardia, tissue ischemia, and metabolic disturbances.Dobutamine is indicated for patients with low cardiac index or other evidence of hypoperfusion following achievement of adequate blood pressure. Milrinone can be used as an alternate agent if the response to dobutamine is suboptimalIn some cases of septic shock, clinical or laboratory evidence of hypoperfusion (e.g., oliguria, altered mentation, decreased mixed venous oxygen saturation, increased lactic acidosis) persists despite an adequate blood pressure. In this circumstance, the patient may require a higher blood pressure or assessment of cardiac output (via PAC or echocardiography) to determine the need for inotropic support. In the small proportion of septic shock patients who manifest overt myocardial depression following fluid resuscitation, dobutamine or milrinone may be indicated. Dobutamine can increase cardiac index in septic shock, although the inotropic response is frequently blunted relative to normal subjects (350,351). If catecholamine responsiveness is inadequate, low-dose milrinone may be effective since its inotropic activity is mediated through an alternate mechanism (352). When using either agent, patients must be adequately fluid resuscitated. Severe hypotension can result if intravascular volume is deficient when either dobutamine or milrinone is initiated (350,352).Although the aim of inotropic therapy in severe sepsis/septic shock is to improve cardiac output and tissue perfusion, specific goals for cardiac index have been controversial; the currently recommended target is a CO within the normal range (approximately 2.5–4 L/minute per m2). The utility of MvO2/ScvO2 as global indices of tissue perfusion adequacy in severe sepsis and septic
shock is also uncertain. Limited studies suggest that an MvO2/ScvO2 below the normal range
(65%–70%) may indicate inadequacy of resuscitation and/or total perfusion in early septic shock (161). If other hemodynamic targets have been achieved, an MvO2 below 65% may represent an
appropriate indication to increase oxygen delivery by starting inotropic agents. Recommendations to increase MvO2 are based on mixed evidence. No benefit was noted in a randomized trial of goal-
directed therapy using MvO2 in critically ill patients after the onset of organ dysfunction (353,354).
On the other hand, early goal-directed therapy targeting a ScvO2 of ≥70% was associated with
improved outcome in another study (253).Supranormal hemodynamic goals are not indicated in the management of septic shock. Observational studies of medical and surgical critical care patients have demonstrated lower values of physiologic variables such as oxygen consumption (VO2), oxygen delivery (DO2), and CI in
nonsurvivors relative to survivors of septic shock (355,356). These observations formed the basis of efforts to implement goal-directed therapy in septic shock to achieve supranormal physiologic parameters consistent with levels observed in survivors (i.e., CI ≥4.5 L/min/m2, DO2 ≥600
mL/minute per m2, and VO2 ≥170 mL/minute per m2). Although a single clinical trial and at least
one meta-analysis have suggested some promise with this approach (357,358), several large randomized trials have failed to demonstrate an overall significant benefit of supranormal oxygen delivery in patients with severe sepsis and septic shock (353,354,359,360,361). One has suggested increased mortality when supranormal oxygen delivery was generated with dobutamine (354). The absence of a beneficial effect with supranormal oxygen delivery in patients with severe sepsis and septic shock has been supported in recent meta-analytic reviews (362).Continuous infusion of vasopressin (0.01–0.04 U/minute) exerts a strong pressor effect and may be beneficial in catecholamine-resistant septic shock following adequate volume resuscitationRecently, vasopressin levels in septic shock patients have been shown to be decreased (363). Further studies have demonstrated that intravenous infusion of vasopressin in patients with septic shock results in a profound pressor response (236,364,365), an effect that is absent with even larger amounts of vasopressin in normotensive patients (235). A randomized, controlled, double-blind trial
of 4-hour infusion of norepinephrine and vasopressin in high-dose, pressor-dependent shock has demonstrated significant improvement in urine output and creatinine clearance, along with a concomitant reduction in conventional vasopressor requirements in the vasopressin group (365). Another RCT has recently demonstrated that, while vasopressin can spare the need for high doses of sympathomimetic agents, outcome is not affected (366).Because of the limited experience with this compound and the relatively prolonged pharmacologic effect of the drug, vasopressin should be used only after hemodynamic stabilization with standard agents (catecholamines) has been attempted.At high dose (>0.04 U/minute), vasopressin may produce increased blood pressure, bradycardia, arrhythmias (premature atrial contractions, heart block), severe peripheral vasoconstriction, decreased cardiac output, myocardial ischemia, myocardial infarction, and cardiac arrest. In patients with vascular disease, even relatively modest doses can precipitate peripheral vascular insufficiency, mesenteric ischemia, or myocardial infarction. Given these potential side effects, the minimal amount of vasopressin required should be used to achieve the desired blood pressure goals. In addition, since vasopressin appears to be a pure vasopressor in the context of vasodilatory shock, cardiac output will usually decline. Consideration of placement of an intra-arterial and pulmonary artery catheter (PAC) should be given to all patients receiving vasopressin for shock.Administration of low- or renal-dose dopamine (1–4 µg/kg per minute) to maintain renal or mesenteric blood flow in sepsis and septic shock is not recommendedAlthough concurrent infusion of low-dose dopamine during human septic shock does mitigate a decrease in renal perfusion that can occur as a consequence of norepinephrine infusion, the clinical benefit of this therapy is questionable (367,368). Low-dose dopamine infusions can cause a mild transient diuresis in the absence of other vasopressors in nonoliguric critically ill patients (369,370). However, low-dose dopamine does not prevent the development of renal dysfunction in these patients, including those with sepsis and septic shock (371,372).P.880Invasive and Noninvasive MonitoringControversy exists regarding the most appropriate monitoring methods for determining the adequacy of resuscitation in patients with severe sepsis and septic shock. The range of monitoring that must be considered in each patient begins with observation by specially trained nursing personnel, to routine noninvasive devices (e.g., continuous electrocardiographic monitors, intermittent mechanical sphygmomanometry, end-tidal carbon dioxide sensors, percutaneous oximetry), to commonly used invasive techniques (arterial, central venous, and pulmonary artery catheters). Prior to the advent of basic hemodynamic monitoring in the 1950s and early 1960s, clinical examination and manual sphygmomanometry were the only available methods for assessment of cardiovascular status. Clinical judgment correctly predicts the hemodynamic profile (including CO and central venous/pulmonary wedge pressures) of critically ill patients only about half of the time (373,374).CVP has been considered a useful measure of intravascular volume since the early studies of hypovolemic shock in young men following battlefield trauma (250,251). However, CVP may be much less reliable as a reflection of left ventricular preload in older patients with various cardiopulmonary disorders as are typically found in a modern-day ICU (152,375). Although low filling pressures may reliably indicate hypovolemia in most patients, the presence of a normal or even elevated central venous pressure can be misleading in patients in whom right ventricular afterload is elevated or right ventricular contractility is impaired (376).The PWP obtained by using a PAC has been considered to reflect intravascular volume more reliably than CVP. In addition, the device allows thermodilution-based derivation of CO (373,374,377). Although the PAC has gained widespread acceptance, significant questions about its use have been raised. Several studies have questioned the relationship of PAC-derived, pressure-based estimates of ventricular preload in specific groups of critically ill patients (375) and, more recently, even in normal subjects (378). In addition, the lack of randomized trials demonstrating benefit and the association of PAC with excess mortality in two observational cohort studies have
led to concerns regarding the clinical utility and safety of PACs (379,380). Despite these concerns, the PAC remains the most commonly used modality for hemodynamic monitoring of unstable critically ill patients.Patients with established septic shock should have continuous monitoring of blood pressure, oxygen saturation, electrocardiogram (ECG), and urine output in a closed ICU staffed with full-time dedicated intensivists and critical care–trained nursesSeveral studies have demonstrated that a reduced mortality with decreased length of stay and overall cost for a wide range of individual conditions are obtained when critically ill patients are cared for in closed ICUs staffed with full-time dedicated intensivists and nurses (381,382,383,384,385). Similar improvements in outcome of sepsis and septic shock have been documented with the use of dedicated intensivists in closed ICUs (386). Among the practice differences associated with the use of full-time intensivists is a greater use of invasive monitoring (384).Patients requiring vasopressor agents for a prolonged period or at high dose should be strongly considered for insertion of an arterial pressure catheter for continuous blood pressure monitoring, as well as to facilitate frequent measurements of arterial blood gases and chemistryAccurate, continuous monitoring of blood pressure is required for optimal assessment of severity of shock, response to fluid resuscitation, and titration of vasopressors and inotropes. However, intense peripheral vasoconstriction may occur during shock as a consequence of the vascular compensatory response to hypotension or due to administration of vasopressors. Clinical ausculatory and noninvasive mechanical methods can be highly inaccurate in this setting (387,388). Patients with sustained shock, particularly those requiring vasopressor support, should be assessed for placement of an intra-arterial catheter for continuous blood pressure monitoring. However, such catheters should be preferentially placed in peripheral sites in non-end arteries (radial, dorsalis pedis), and should be used with caution in patients at high risk for vascular disease.If volume resuscitation requirements exceed 2 L, placement of a central venous catheter for monitoring of CVP and for vasopressor/inotrope infusion should be considered. An initial target CVP of ≥8 mm Hg is recommendedFluid deficits during septic shock in adults typically range from 5 to 10 L (248). In the absence of significant cardiopulmonary dysfunction, central venous pressure should accurately assess intravascular volume status. However, cardiopulmonary dysfunction is not uncommon in patients with septic shock either as an underlying predisposition to critical illness/sepsis or as a consequence of the injury (ARDS/acute lung injury [ALI], myocardial depression). Low central venous pressures remain indicative of hypovolemia; elevated or normal central venous pressures in this patient group may not necessarily indicate euvolemia. CVP monitoring should be entertained if substantial amounts of fluid resuscitation are required to ensure that overt hypovolemia is adequately addressed. The initial target CVP should be ≥8 mm Hg, with additional increases indicated by the effect of fluid boluses on cardiac output and clinical perfusion. The overall goal is to provide adequate cardiac output and tissue perfusion using the lowest necessary cardiac filling pressures.Initiation of invasive cardiac monitoring using a pulmonary artery catheter should be considered if there has been an inadequate response to fluid resuscitation (3–5 L or CVP 8–12 mm Hg), if there is clinical suspicion of intravascular fluid volume overload, or if the patient has impaired cardiac function. An initial target of PWP of 12–15 mm Hg will ensure that hypovolemia is absent in most patients, but higher pressures may be required in certain subgroupsAlthough the maintenance of a blood pressure adequate for autoregulation of blood flow to vital organs and tissues is the first objective in the resuscitation of septic shock, support of global perfusion is also critical. Adequacy of global perfusion cannot always be reliably inferred from the clinical examination or CVP/arterial pressure monitoring (373,377,389). Patients who respond poorly to fluid resuscitation or are at high risk for fluid resuscitation–related complications may benefit from pulmonary artery catheterization. A substantial degree of variability in the relationship between PWP and end-diastolic volumes makes it difficult to specify target PWP goals that ensure adequate cardiac output and tissue perfusion (378,390,391). In general, a PWP titrated to at least 12
to 15 cm H2O will optimize cardiac function (152). If hypotension persists, a higher PWP may be
beneficial as P.881assessed by measuring the effect of additional fluids on cardiac index. An elevated PWP may risk the development or aggravation of ALI and ARDS (392,393). Specific groups that may require higher PWP include those with congestive heart failure, left ventricular hypertrophy, restrictive or constrictive heart disease, or increased intrathoracic pressures, including those on high levels of positive end-expiratory pressure (PEEP).In patients with vasopressor-requiring shock who develop progressive organ failure or hypoxemic respiratory failure, pulmonary artery catheterization may be a useful clinical management toolThe information available from a PAC can be used to help determine the cause of shock and provide a guide for interventions to maintain an appropriate cardiac output and intravascular volume to limit the risk of further progression of organ dysfunction/failure. If PACs are beneficial in patients with sepsis, the most likely candidates may be those in whom resuscitation by clinical assessment or CVP fails to reverse the progression of organ failure.Invasive monitoring using a pulmonary artery catheter is not recommended for routine use in all patients with severe sepsisAt least one major prospective, nonrandomized multicenter study has suggested increased length of stay, costs, and mortality in a cohort of risk-matched patients receiving a PAC in the first 24 hours after ICU admission (394). A recent multicenter randomized controlled trial involving 676 subjects with shock (primarily septic), ARDS, or both has demonstrated no difference in organ failure–free days, renal support needs, vasopressor requirements, mechanical ventilation, ICU/hospital length of stay (14 and 90 day), or mortality between subjects randomized to pulmonary artery catheterization or controls (395). A second, smaller randomized trial of 200 patients (about 100 with sepsis) also demonstrated no mortality difference with or without the use of PAC (396). Other smaller studies, including one randomized trial in high-risk operative patients, failed to demonstrate any difference in mortality with PAC use (397,398). In contrast, one meta-analysis of RCTs demonstrated a reduced mortality risk in surgical ICU patients treated with PAC but no effect on mortality in medical or mixed ICU patients (399). On the basis of the total data available, routine use of PAC in patients with sepsis or other critical illness cannot be recommended.Specific TherapyAs discussed, patients with severe sepsis and septic shock must first be treated using the following: (i) Appropriate resuscitation, (ii) broad spectrum antimicrobials, (iii) source control, and (iv) physiologic support of organ function in the intensive care unit. Immunomodulatory therapy has been evaluated only in association with adequate treatment based on these four elements.In the last few decades, the dominant hypotheses regarding the pathogenesis of septic shock and septic organ dysfunction focused on inflammatory mediators including TNF α, IL-1β, interleukin-6, and platelet-activating factor. Several clinical trials have been performed evaluating both nonspecific inhibitors of inflammation such as nonsteroidal anti-inflammatory drugs and high-dose glucocorticoids and specific immunomodulatory agents such as monoclonal antibody against TNF α and IL-1 receptor antagonist (400,401). Despite an expenditure of over 1 billion dollars, these studies have failed to demonstrate a survival benefit. No primary immunomodulatory experimental agent has received regulatory approval.Recently accepted models of the pathogenesis of sepsis have emphasized a central role for altered hemostatic/coagulant function. Three coagulation modulators have been assessed in large randomized controlled clinical trials: Tissue factor pathway inhibitor, antithrombin III, and drotrecogin alfa (activated) (recombinant human activated protein C). Drotrecogin alfa (activated) is the first and, to date, only specific therapy that has been shown to improve survival in patients with severe sepsis and septic shock.Recombinant human-activated protein C should be administered in patients with suspected sepsis with organ dysfunction. Acceptable criteria include, but are not necessarily limited to, a minimum of one organ dysfunction with an Acute Physiology and Chronic Health Evaluation (APACHE) II
score ≥25; or if an accurate APACHE II score is unavailable, the presence of two or more organ dysfunctionsAlthough clinical trials of modulation of the coagulation cascade for treatment of sepsis have been performed with several agents (e.g., antithrombin III [27], tissue factor pathway inhibitor [28]), only drotrecogin alfa (activated) has been shown to improve mortality (26). The pivotal study was an international multicenter RCT that compared drotrecogin alfa (activated) to placebo used in conjunction with standard treatment (antibiotics, physiologic support, and surgical source control) (26). Patients were entered into the study if they exhibited acute organ dysfunction due to a suspected infection (severe sepsis) within a 24-hour window. The study was stopped at a planned interim analysis because of definitive statistical evidence that supported a beneficial treatment effect. Using an intention-to-treat analysis, the study demonstrated an absolute mortality reduction of 6.5% from 31.3% in the placebo group to 24.8% in the drotrecogin alfa (activated) group, yielding a highly significant 21% relative risk reduction. Subsequent open-label studies of drotrecogin alfa (activated) using the same criteria as in the pivotal study have demonstrated a consistent mortality rate between 25.1% and 26.1% (402,403). A retrospective analysis of an open-label study suggests that earlier initiation of treatment (<24 hours after diagnosis of severe sepsis) yields superior outcomes (404).The original study demonstrated a differential treatment effect based on either APACHE II scores or the number of acute organ dysfunctions present at the time of enrollment into the study. The absolute reduction in mortality was 1.7% among patients with a single dysfunctional organ and 7.4% among those with two or more dysfunctional organs (402,405). Similarly, there was no overall reduction in absolute mortality in the first 2 quartiles of APACHE score (score <25), whereas there was a 13% reduction in the last 2 quartiles (score ≥25) (405). A more recent RCT (prematurely terminated for futility) has underlined concerns regarding the utility of drotrecogin alfa (activated) in relatively low-risk (generally APACHE<25 or single organ failure) adult patients with a slight trend toward increased mortality risk in the treatment arm (29). Similarly, a study of drotrecogin alfa (activated) in pediatric septic shock with respiratory failure was also prematurely terminated due to its futility, along with evidence of an increased central nervous system (CNS) bleeding risk in neonates (406).P.882Drotrecogin alfa (activated) remains approved for management of high-risk patients with severe sepsis/septic shock, but new studies are ongoing to validate the continued use of this agent.Intravenous immune globulin should be considered for patients suffering from streptococcal toxic shock syndromeThe potential utility of polyclonal immune globulin preparations for severe sepsis and septic shock in general is uncertain at present. One meta-analysis has suggested that sepsis-related mortality is significantly reduced when intravenous immunoglobulin (IVIG) is used in the management of such patients (407). A small randomized controlled trial of trauma patients has also demonstrated a reduced incidence of septic complications including pneumonia and other infections (other than catheter-related infections), although ICU length of stay and mortality were not reduced (408). Evidence favoring the use of polyclonal immunoglobulin for defined invasive streptococcal infections, including streptococcal septic shock, is more definitive. A case-matching study has demonstrated an improved 30-day survival in patients treated with intravenous polyclonal immune globulin, while a randomized controlled trial (aborted prematurely due to low enrollment) has shown decreased early sepsis-related organ failure with a trend toward improved survival (409).Immunosuppressive doses of corticosteroids are contraindicated in the management of sepsis and septic shockIn the past, high-dose steroids had been advocated for sepsis with organ failure to dampen inflammatory responses and minimize organ dysfunction (410). Several large multicenter randomized controlled trials have definitively demonstrated that administration of high dose (15–30 mg/kg methylprednisolone equivalent) corticosteroids fail to improve outcome in adult septic shock (411,412,413,414). In some of these studies, mortality in specific subgroups appeared to be
increased with steroid treatment (412).Supportive TherapyAlthough specific therapies for septic shock continue to be developed, general supportive care, in conjunction with antibiotics, remains the standard of care. Fluid and vasopressor/inotropic support have been addressed in this chapter. In addition, there has been an explosion of data in recent years regarding the efficacy of other elements of supportive care including ventilatory strategies, intensity of dialysis, endocrine support, and glycemic management. In other key areas (e.g., nutritional support), definitive data are lacking. Nonetheless, it is likely that an aggressive approach to optimization of supportive care, in combination with anti-infective therapy and resuscitative efforts, can improve morbidity and mortality. For that reason, application of appropriate support modalities in a timely manner should be the standard of care of septic patients in all ICUs.Intensive renal replacement therapy (daily intermittent dialysis or continuous renal replacement therapy) is indicated for severe sepsis or septic shock with renal failureIndications for acute dialysis in the ICU population are not dissimilar to those for other patients. These indications include volume overload, electrolyte imbalance, acid-base disturbances, elevated blood urea nitrogen, uremic pericarditis, or uremic encephalopathy. Unfortunately, ICU patients, especially those with acute renal failure, may have altered hemodialysis kinetics such that standard intermittent dialysis may offer suboptimal urea clearance kinetics despite apparently equivalent doses. Compared to standard intermittent dialysis, daily hemodialysis has been shown to yield higher urea clearance and improved mortality in ICU patients with acute renal failure (415). Similarly, another study has demonstrated that higher urea clearance with continuous venovenous hemodialysis yields reduced mortality (416). Whether these data can be extrapolated to include septic patients with a background of chronic renal failure is unknown. Peritoneal dialysis is not appropriate since even high-frequency exchanges yield relatively low urea clearance kinetics. A recent study of infection-related acute renal failure that included cases of sepsis demonstrated increased mortality among those treated with peritoneal dialysis compared to those treated with hemodialysis (417).Intensive insulin therapy maintaining a blood glucose of 4.4 to 6.1 mmol/L (80–110 mg/dL) may be beneficial in critically ill ICU patients with severe sepsisHyperglycemia is a recognized risk factor for increased mortality in the critically ill independent of the APACHE II score (418). One single-center randomized, controlled, nonblinded trial has indicated that tight glycemic control in surgical ICU patients undergoing mechanical ventilation (mostly post–coronary artery bypass graft or other cardiovascular surgery) reduces the incidence of severe sepsis and decreases mortality, primarily because of a decreased incidence of multiple organ failure with septic foci (419). These data are consistent with other clinical and experimental studies suggesting the presence of granulocyte dysfunction and increased risk of infection in postoperative surgical patients with persistent hyperglycemia (420). However, another RCT by the same group has failed to demonstrate similar improvements in critically ill medical patients (421). A retrospective subgroup analysis, however, suggested mortality improvement in those patients admitted with an ICU length of stay of greater than 3 days. In addition, there was a decreased incidence of renal dysfunction and critical illness polyneuropathy, with fewer days on ventilator support and shorter ICU and hospital length of stay (421,422). No definitive data exist regarding the question of whether a tight control strategy is useful in patients who are already septic. In addition, these data should be interpreted with caution pending replication of these results in other centers.Stress dose steroids may be administered at presentation to selected patients with septic shock pending the result of an ACTH stimulation testSeveral previous large randomized, double-blind, multicenter trials have definitively demonstrated that administration of immunosuppressive (15–30 mg/kg methylprednisolone equivalent) corticosteroids fail to improve outcome in adult septic shock (411,412,413,414). However, some evidence suggests that low “stress-dose” corticosteroids may be beneficial. A relative adrenal insufficiency has been suggested to exist in a substantial subset of patients with septic shock (239,423). Among other deleterious effects, adrenal insufficiency can result in impairment of
catecholamine sensitivity P.883(423,424,425). Administration of stress-dose steroids (150–300 mg hydrocortisone daily equivalent) to patients with septic shock can decrease pressor requirements while suppressing inflammatory markers (424,426,427). One recent RCT has demonstrated that 7 days of therapy with hydrocortisone, 50 mg IV every 6 hours, and fludrocortisone, 50 µg orally once daily, generates a significant reduction in mortality in patients with relative adrenal insufficiency (428). Subgroup analysis demonstrated that this improvement was restricted to those who fail to respond to an ACTH challenge (about 75% of septic shock patients), with an increase in serum cortisol of at least 250 nmol/L (9 µg/dL). In the recent past, these data were interpreted as suggesting that patients with pressor-dependent septic shock should undergo ACTH challenge on admission, followed immediately by initiation of stress-dose steroid therapy. If the ACTH stimulation test was within normal limits, corticosteroids were discontinued. If the test results indicated relative adrenal insufficiency, hydrocortisone and fludrocortisone were often continued for 7 days or as otherwise clinically indicated.The major uncertainty with regard to stress-dose steroid therapy had been the appropriate test and value of serum cortisol to indicate adrenal insufficiency. Various studies supported using random cortisol levels between 275 and 950 nmol/L (10–35 µg/dL) during the acute stress, or increments of cortisol of 250 nmol/L (9 µg/dL) within the first hour following ACTH stimulation (239,423,428). Although no definitive data existed as to which cutoff value was best, many clinicians considered a random value of less than 400 nmol/L (15 µg/dL) to be sufficiently suggestive of relative adrenal insufficiency during the shock state to initiate and continue stress-dose therapy. Similarly, a value greater than 950 nmol/L (35 µg/dL) during shock has been thought to be sufficiently normal to discontinue stress-dose therapy without further assessment. Values between those two extremes were often interpreted to be an indication for ACTH challenge with a response of less than 250 nmol/L (9 µg/dL) supporting the need, for steroid therapy. Unfortunately, a recent study has challenged these accepted cutoffs in the critically ill by questioning the scientific validity of using total as opposed to free serum concentrations of serum cortisol in such patients (429).Of most concern, a major multicenter, placebo-controlled, double-blind RCT of septic shock has failed to confirm an improvement in survival regardless of ACTH responsiveness (430). The steroid group did exhibit a reduction in pressor days but also had a higher incidence of superinfections and associated sepsis/septic shock events. Confounding these results, the steroid regimen (hydrocortisone alone) differed from the regimen used in the previous positive study and could also be implemented as late as 72 hours following onset of septic shock. Based on these data, stress-dose or low-dose steroid therapy should not be considered part of the routine management of septic shock pending further definitive trials.Low-volume (6–8 mL/kg ideal body weight), pressure-limited ventilation is indicated in patients with sepsis-associated acute lung injury or acute respiratory distress syndromeAnimal and human studies have suggested that high levels of PEEP and large tidal volumes are associated with increased pulmonary generation of proinflammatory cytokines (431,432) and ventilation-induced lung injury (433). ALI and ARDS represent a manifestation of MODS that may occur in conjunction with severe sepsis and septic shock. Septic patients with bilateral persistent opacities, in association with an acute and persistent defect of oxygenation (PaO2/FiO2 ratio of
≤200 for ARDS and ≤300 for ALI) and no clinical evidence of left atrial hypertension or a pulmonary wedge pressure of ≥18 mm Hg, fit the criteria for this syndrome (434). Small randomized studies have supported the possibility that a lung-protective strategy using low tidal volumes and limited airway pressures may decrease pulmonary injury and decrease mortality (435). A single large multicenter, randomized controlled trial has demonstrated that ventilation of critically ill patients with ARDS with a low tidal volume (tidal volume of 6–8 mL/kg ideal body weight) reduces all-cause absolute mortality by 10% (from 40% to 30%; 25% relative risk reduction) (436). Patients with severe sepsis or septic shock who meet criteria for ALI or ARDS should be ventilated with a low-volume, pressure-limited strategy. Available evidence suggests that ventilation of
patients at risk for ALI/ARDS with this strategy does not prevent the development of this pulmonary syndrome (437).Endotracheal intubation and mechanical ventilation should be considered early in the management of all patients with sepsis and organ failureAirway intubation is indicated for all patients with impaired airway protection reflexes (e.g., as a consequence of cerebral hypoperfusion or septic encephalopathy), refractory hypoxemia, respiratory acidosis, or respiratory distress associated with ongoing hypotension/hypoperfusion. Though not yet addressed by systematic studies, clinical experience suggests that respiratory arrest is a significant risk in such patients. These observations are consistent with observations of respiratory muscle compromise and respiratory failure in animal models of septic shock (438,439).Enteral feeding should be considered within 24 hours of admission to the ICU for most patients with sepsis and septic shock. Parenteral feeding should be used only if enteral feeding is not possible despite best effortsRecent meta-analyses suggest that early enteral feeding lowers the risk of infection and improves survival compared to delayed feeding in the critically ill (440). These findings are consistent with animal studies demonstrating that enteral nutrition maintains gut mucosal integrity, decreases bacterial translocation, and limits the systemic inflammatory response to bacterial toxins (441). Diminished bowel sounds should not prevent a trial of enteral feeding. Most patients will tolerate enteral feeding if a small bowel tube is used. Studies of parenteral feeding in the ICU have, in general, failed to demonstrate an improvement in mortality in critically ill patients (442). Other studies demonstrate the superiority of enteral over parenteral feeding in critically ill patients with respect to costs and complications, including risk of infection (441,443).Intravenous administration of sodium bicarbonate is not indicated for sepsis-associated metabolic acidosis with a pH ≥7.15Human investigations demonstrate that intravenous administration of sodium bicarbonate for lactic acidosis (pH ≥7.15) associated with septic shock does not improve cardiac performance or reduce vasopressor requirements compared to administration of an equimolar amount of normal saline (444,445). No human data exist in regard to the effect of intravenous bicarbonate administration for more severe degrees of metabolic acidosis.
Table 57.15 Time Line of Implementation of Recommended Diagnostic and Therapeutic Interventions
ResuscitationAntimicrobialsVasopressors/Inotropes Monitoring
Specific Therapy
Supportive Therapy
First hour
•Initiate crystalloid fluid resuscitation (500 mL every 10–15 min), titrating to HR <100, MAP ≥65 mm Hg, and urine output ≥0.5 mL/h
•Initiate empiric, broadspectrum, high-dose antimicrobial therapy with two or more cidal drugs where possible
•Implement continuous monitoring of ECG, arterial saturation, blood pressure and UO
•Supplemental oxygen•Consider intubation and mechanical ventilation prior to overt respiratory distress
1–8 hours
•Titrate fluid resuscitation to elimination of base deficit and normalization of serum
•Initiate radiographic investigation for localization and delineation of infection•Implement
•Initiate vasopressor therapy if circulatory shock persists following adequate fluid
•ICU transfer with full monitoring support•Arterial catheter assessment•If shock persists with >2 L crystalloid resuscitation, venous
•Consider low-dose steroid therapy ± ACTH stimulation test
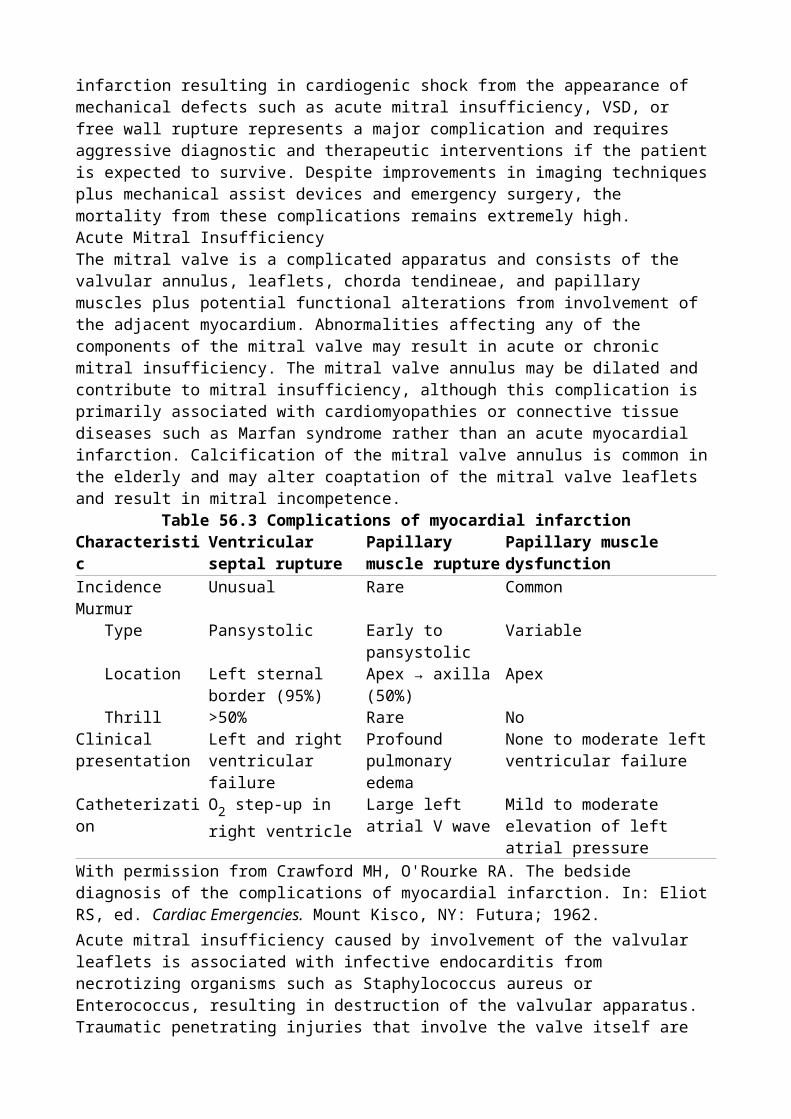
lactate source control if necessary
resuscitation•Initiate inotropes if CI or S[v with bar above]O2
are persistently decreased
catheter assessment ± placement (goal CVP ≥8 mm Hg)
8–24 hours
•Dynamic evaluation of resuscitative goals (based on clinical and invasive monitoring end points)
•Consider vasopressin if shock refractory to first-line vasopressors persists
•If persistently pressor dependent after 3–5 L crystalloid infusion, CVP ≥8 achieved, suspicion of intravascular volume depletion or limited cardiovascular reserve, PAC placement (initial goal PWP 12–15 mm Hg) •May be inserted earlier if clinically indicated
•Consider initiation of drotrecogin-alfa (activated) if single organ failure with APACHE II ≥25, two or more organ failures in absence of APACHE score
•Initiate enteral feeding•Consider intensive insulin therapy
>24 hours
•Narrow antimicrobial regimen depending on isolation of pathogenic organisms and/or clinical improvement•Reassess necessity for or efficacy of source control
•Consider PAC in vasopressor-dependent patients with progressive respiratory, renal, or multiple organ dysfunction
•Intensive hemodialysis therapy for renal failure•Low-pressure, volume-limited ventilation for ARDS
HR, heart rate; MAP, mean arterial blood pressure; ECG, electroencephalograph; UO, urine output; Cl, chlorine; S[v with bar above]O2, mixed venous oxygen saturation; CVP, central venous pressure; ACTH,
adrenocorticotropin hormone; PAC, pulmonary artery catheter; PWP, pulmonary wedge pressure; APACHE, Acute Physiology and Chronic Health Evaluation; ARDS, acute respiratory distress syndrome.P.884P.885SummarySevere sepsis and septic shock continue to be a major cause of mortality and morbidity among patients requiring ICU support. In recent years, both basic and clinical research in the field have accelerated substantially. This has led to the publication of several studies with major implications regarding the appropriate management of patients with these conditions. Many of these new studies relate to optimization of supportive care. Although controversial, a single specific therapy, drotrecogin alfa (activated), has been shown to improve mortality in severe sepsis and septic shock. Few major studies in the areas of fluid resuscitation, vasopressors/inotropes, invasive and noninvasive monitoring, or antimicrobial therapy have been published in recent years. Nonetheless, outcome can most likely be improved by taking a systematic approach to therapy as described in Table 57.15. Although significant improvements in outcome have been made possible by new pharmacologic therapies, recent studies focusing on antimicrobial and supportive elements clearly

demonstrate that close attention to established therapies can have a substantial impact on survival in severe sepsis and septic shock.
Chapter 58Hemorrhagic ShockMarianne E. CinatDavid B. HoytThe definition of shock describes the final common pathway of many disease states: ineffective tissue perfusion, resulting in severe dysfunction of organs vital to survival. The most commonly used classification system for shock includes four categories based on hemodynamic characteristics (1):
Hypovolemic shock resulting from a decreased circulating blood volume in relation to the total vascular capacity and characterized by a reduction of diastolic filling pressures and volumes
Cardiogenic shock related to cardiac pump failure caused by loss of myocardial contractility/functional myocardium or structural/mechanical failure of the cardiac anatomy characterized by elevations of diastolic filling pressures and volumes
Extracardiac obstructive shock involving obstruction to flow in the cardiovascular circuit and characterized by either impairment of diastolic filling or excessive afterload
Distributive shock caused by loss of vasomotor control, resulting in arteriolar and venular dilation and characterized by increased cardiac output and decreased systemic vascular
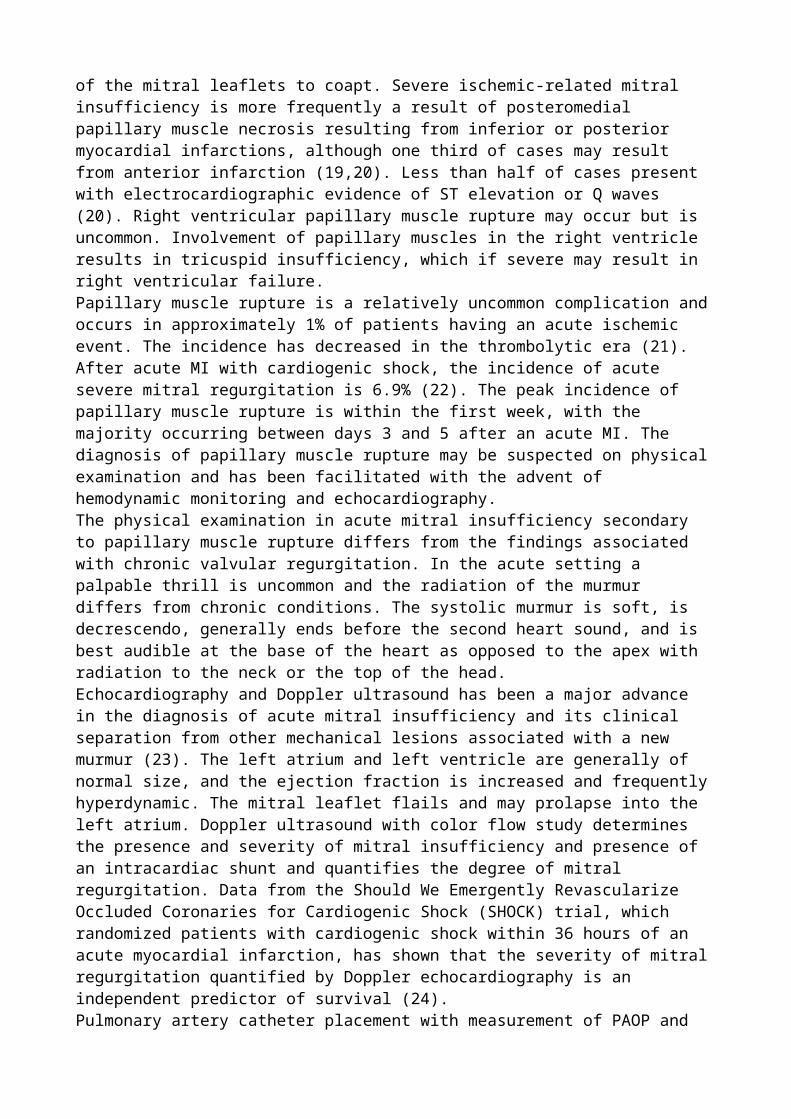
resistance after fluid resuscitation.
Although the hemodynamic characteristics of the various forms of shock may vary, the final common pathway—inadequate cellular perfusion—must be addressed early to prevent long-term sequelae and death (Fig. 58.1).Hemorrhagic shock is a form of hypovolemic shock. It is a common, yet complicated, clinical condition that physicians are frequently called upon to evaluate and treat. Etiologies include trauma, postoperative bleeding, medical conditions, and iatrogenic causes. Diagnosis must be accurate and expedient. Therapy must be direct, efficient, and multifactorial in order to avoid the potential multisystem sequelae.The purpose of this chapter is to address the immediate concerns for patients with hemorrhagic shock, as well as the etiology and epidemiology of this clinical condition, and to describe the pathophysiology, clinical features, and diagnostic and therapeutic approach to hemorrhagic shock. New and experimental therapies will also be introduced.Immediate ConcernsThe key steps in the approach to patients with hemorrhagic shock are listed in Table 58.1.
Early recognition. Early recognition requires astute clinical acumen to identify early systemic signs of hemorrhage and hypovolemic shock. Signs and symptoms include restlessness, anxiety, altered level of consciousness, shortness of breath, tachypnea, pallor, tachycardia, and oliguria. A decreased pulse pressure may also be observed along with decreased capillary refill due to peripheral vasoconstriction. Hypotension indicates significant volume depletion and may be a late clinical manifestation.
Important aspects in the patient history. An accurate history should be obtained expediently. For patients with traumatic injury, a thorough understanding of the mechanism of injury should be obtained, including the magnitude of blunt force trauma and/or the trajectory of the missile or object in penetrating trauma. In postoperative or postprocedural patients, the exact nature of the surgical procedure should be defined and potential sites of hemorrhage identified. In patients without recent surgery, risk factors for nonpostoperative, nontraumatic etiologies should also be sought (gastritis, peptic ulcer disease, atherosclerosis with aneurysmal disease). Significant comorbidities should also be delineated including coagulation disorders (von Willebrand, hemophilia), medical conditions associated with altered coagulation (cirrhosis, renal failure, iatrogenic vitamin K deficiency from parenteral nutrition or antimicrobials), or use of medications such as antiplatelet therapy and anticoagulants (Coumadin, heparin, low-molecular-weight heparin, or antimicrobials).
Initial action and intervention. The initial action taken in each case of hemorrhagic shock, regardless of etiology, should be directed at restoring circulating volume to ensure adequate tissue perfusion. Once the airway is secured and adequate ventilation is ensured, two peripheral large-bore intravenous catheters should be placed and fluid resuscitation begun. A blood sample should also be sent immediately for type and cross-match per institutional protocol. Initial resuscitation can include crystalloid, but should quickly be changed to blood products if signs of hypovolemia and ongoing hemorrhage persist. If a patient is in extremis and cross-matched blood products are not immediately available, type O blood (universal donor) should be immediately requested and transfused. For massive hemorrhage, clotting factors such as fresh frozen plasma, platelets, and cryoprecipitate should be prepared. The value of massive transfusion protocols to include predetermined ratios of clotting factors will be discussed later in this chapter.
Directed physical examination. Physical examination should be directed at obvious sources of external bleeding such as lacerations, extremity fractures, or surgical incisions. If identified, these should be immediately controlled. Physical signs of underlying liver disease should also be identified such as petechia, jaundice, ascites, angiomas, or testicular atrophy. Previous cardiac or carotid surgical incisions may hint toward concurrent antiplatelet or anticoagulant therapy. Evidence of retroperitoneal bleeding in patients with pancreatitis is
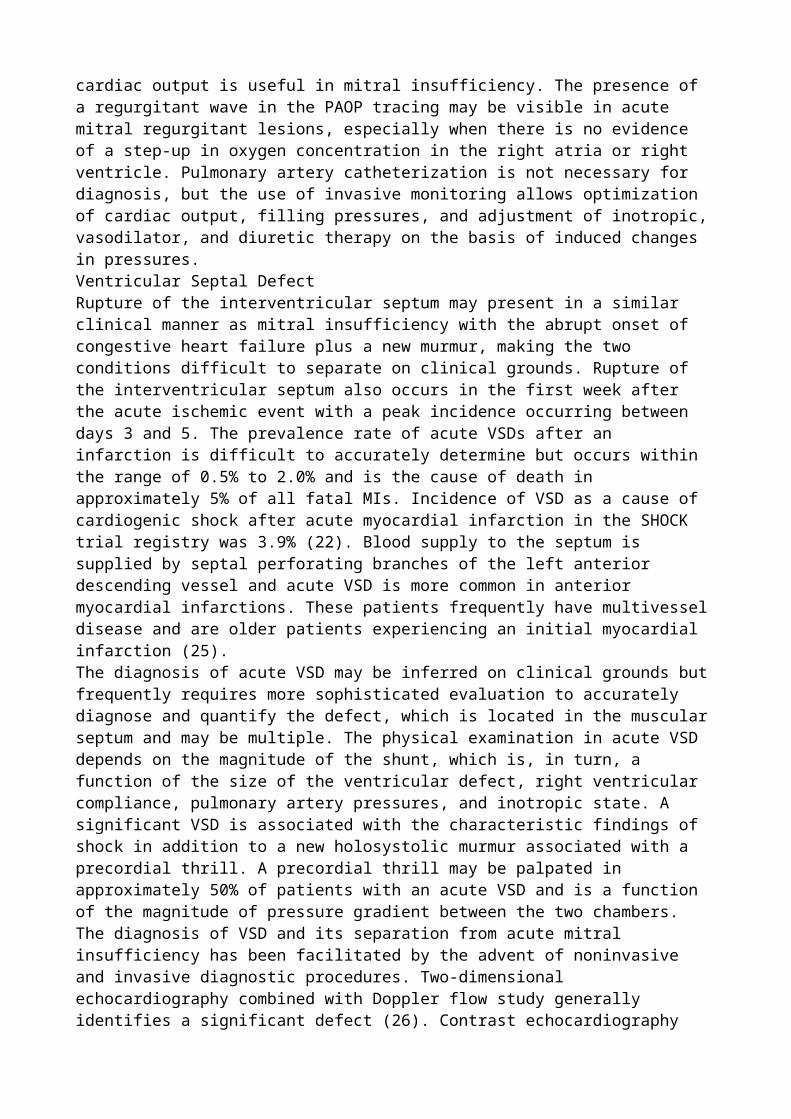
marked by flank or periumbilical contusions.P.894
Identify occult source of hemorrhage. If no obvious source of external bleeding is identified, a rapid evaluation should be performed to identify likely occult sources of bleeding. In the trauma patient, significant internal hemorrhage can occur in four defined regions: the thoracic cavity, the peritoneal cavity, the retroperitoneum, and extremity fractures. These areas can be rapidly assessed by chest radiograph, pelvic radiograph, a focused abdominal sonographic examination for trauma (FAST), and physical examination of extremities along with appropriate radiographs. In nontrauma patients without clear evidence of bleeding, the gastrointestinal tract should be rapidly evaluated via nasogastric tube, rectal examination, and endoscopy where appropriate. Additional diagnostic tests can be obtained based on clinical history, patient background, and condition. Abdominal aortic aneurysms can be identified on physical examination, by ultrasound, or by calcifications on abdominal radiograph. In rare selected instances, angiography may be used to identify and treat sources of hemorrhage not otherwise apparent (pelvic fractures, pancreatitis, lower gastrointestinal bleeding). This should only be instituted when a specific source of hemorrhage is highly likely and therapeutic intervention is sought. Computed tomography should never be sought in hemodynamically unstable patients with hemorrhage.
Figure 58.1. Final common pathway of shock. Hemorrhagic shock results in acute changes in circulating blood volume that culminates in a final common pathway shared by all classifications of shock.
Expedite treatment. Once a source of bleeding is identified, a swift and directed treatment plan should be formulated and implemented without delay. Prolonged untreated hemorrhagic shock can lead to rapid decompensation and death if not appropriately identified and treated. Rapid intervention with surgical, angiographic, or endoscopic control of the hemorrhage is indicated, along with rapid correction of the underlying coagulopathy.
Epidemiology and EtiologyHypovolemic shock can be due to hemorrhagic and nonhemorrhagic sources. Hemorrhage is the most frequent cause of hypovolemic shock and is most commonly due to blood loss after trauma or major surgery (Table 58.2). Following trauma, obvious external signs of injury and hemorrhage should be rapidly identified and controlled. As described above, the thoracic cavity, peritoneal cavity, and retroperitoneum should all be evaluated for occult hemorrhage.
Table 58.1 Key steps in the approach to a patient with hemorrhagic shock1. Early recognition
0. Signs and symptoms may be subtle. a. Astute clinical acumen is necessary to identify hemorrhage prior to hemodynamic
collapse. 2. Obtain an accurate patient history
0. Trauma a. Recent surgical procedures b. Medical history
0. Gastrointestinal disease (peptic ulcer disease, varices, etc.) i. Atherosclerosis (aneurysmal disease) ii. Coagulation disorders
c. Medication use0. Antiplatelet therapy i. Anticoagulants
2. Initiate intervention0. “ABCs”—airway, breathing, circulation a. Initiate resuscitation
0. Crystalloid
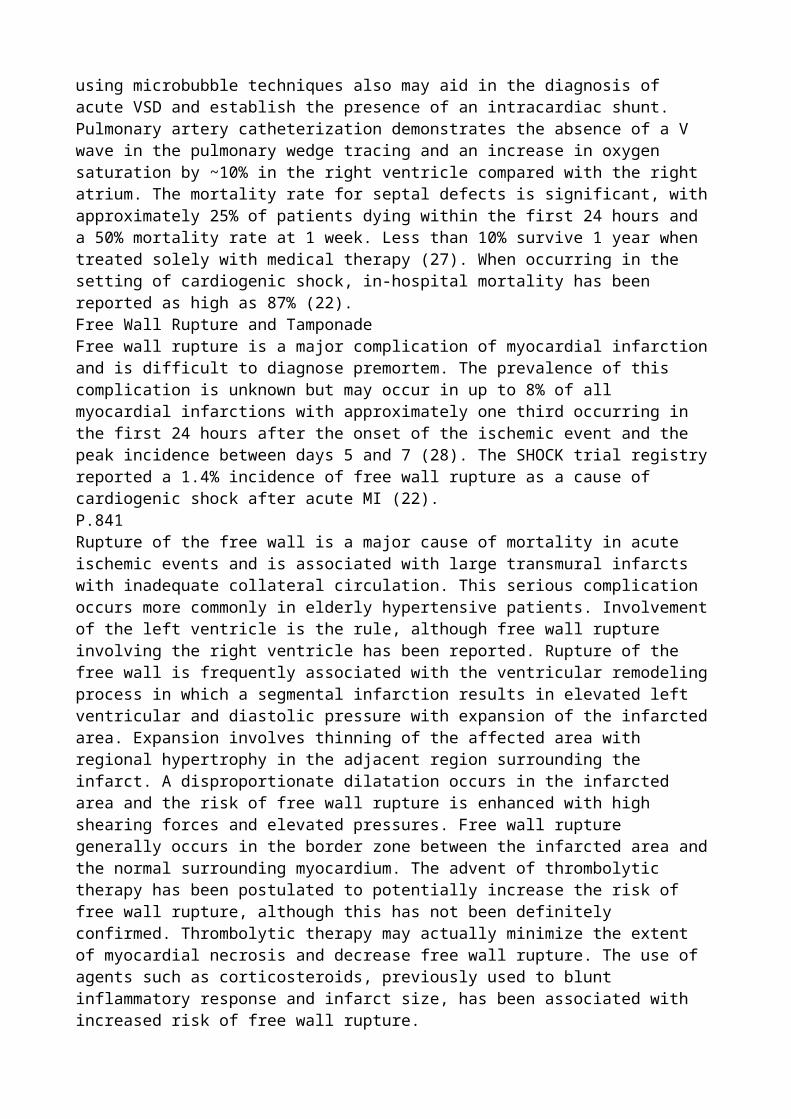
i. Blood products1. Type O uncross-matched blood if in extremis 2. Cross-matched blood when available 3. Clotting factors
2. Directed physical examination0. External sources of bleeding a. Internal sources of bleeding
2. Expedite definitive treatment0. Surgical control a. Endoscopic control b. Angiographic control
2. Correct coagulopathy
Table 58.2 Major etiologies of hemorrhagic shock0. Trauma (blunt or penetrating)
Intrathoracic Intraperitoneal Retroperitoneal Soft tissue or fractures
I. Gastrointestinal Upper gastrointestinal tract
Peptic ulcer disease, reflux esophagitis, variceal bleeding, erosive gastritis, aortoduodenal fistula
Lower gastrointestinal tract Hemorrhoids, tumor, arteriovenous malformation, diverticulitis, ulcerative
colitis, Crohn disease, ischemia Hemobilia
Biliary tumor, iatrogenic injury or manipulation, penetrating trauma Pancreatic
Pancreatitis, iatrogenic injury or manipulation II. Retroperitoneal (nontrauma)
Abdominal aortic aneurysm
P.895Causes of hemorrhagic shock not due to trauma include a ruptured abdominal aortic aneurysm and gastrointestinal bleeding. Gastrointestinal bleeding can be caused by peptic ulcer disease, reflux esophagitis, variceal bleeding, erosive gastritis (stress ulcers), or an aortoduodenal fistula after vascular surgery. Prior manipulation by endoscopy or sphincterotomy can also lead to upper gastrointestinal bleeding. Lower gastrointestinal bleeding can result from diverticular disease, carcinoma, polyps, arteriovenous malformations, ischemia, or colitis. Pulmonary sources of hemorrhage can occur from tumor, tuberculosis, fungal infection, bronchiectasis, or tracheoinnominate fistula following tracheostomy. Hematuria from a tumor, trauma, or polycystic kidney disease is rare but can lead to hemorrhagic shock.Nonhemorrhagic sources of hypovolemic shock can also occur. Although not the focus of this chapter, these are due to external fluid losses such as dehydration, vomiting, diarrhea, polyuria, uncontrolled diabetes mellitus leading to osmotic diuresis, and acute adrenocortical insufficiency. Disorders that lead to interstitial fluid redistribution such as thermal injury, trauma, and anaphylaxis can also lead to hypovolemic shock. Finally, disorders that cause increased vascular capacitance (venodilation) can lead to a relative hypovolemia and include sepsis, anaphylaxis, and the release of toxins/drugs leading to vasodilation.Classification of Hemorrhagic Shock
Early diagnosis of hemorrhagic shock is imperative to avoid delay in treatment. However, clinical signs are relatively insensitive for small amounts of blood loss (2). There is a progressive hemodynamic deterioration with ongoing blood loss. This classic progression is delineated in Table 58.3. Total blood volume is estimated at approximately 70 mL/kg in the average adult, or nearly 5 L for a 70-kg person.Class IClass I hemorrhage is marked by a less than 750 mL estimated blood loss, or less than 15% of total circulating blood volume. There are minimal physical signs associated with this volume of blood loss. The patient may not have tachycardia, with a heart rate remaining less than 100 beats per minute; the systolic blood pressure and pulse pressure remain normal; the respiratory rate remains at 14 to 20 breaths per minute; and urine output remains adequate (>30 mL/hour). Only subtle physical signs such as delayed capillary refill and slight anxiety may exist.Class IIClass II hemorrhage is marked by an estimated blood loss of 750 to 1,500 mL (or 15% to 30% of the total circulating blood volume). Physical signs begin to manifest during this stage of hemorrhage. Although the systolic blood pressure may be maintained, the patient usually becomes tachycardic (heart rate greater than 100 beats per minute), the pulse pressure begins to decrease, and capillary refill is delayed. The respiratory rate begins to increase (20–30 breaths per minute), urine output P.896becomes diminished (20–30 mL/hour), and the patient becomes very anxious.
Table 58.3 Clinical classes of hemorrhagic shock Class I Class II Class III Class IVBlood loss <750 mL 750–1,500
mL>1,500–2,000 mL
>2,000 mL
<15% 15%–30% >30%–40% >40%Heart rate (beats per minute) <100 >100 >120 >140Systolic blood pressure Normal Normal Decreased DecreasedPulse pressure Normal Decreased Decreased DecreasedCapillary refill Delayed Delayed Delayed DelayedRespiratory rate (breaths per minute)
14–20 20–30 30–40 >35
Urine output (mL/h) >30 20–30 5–15 MinimalMental status Slightly
anxiousAnxious Confused Confused and
lethargicClass IIIClass III hemorrhage is marked by an estimated blood loss of >1,500 to 2,000 mL (or >30%–40% of total circulating blood volume). During this phase, significant hemodynamic compromise becomes apparent. Heart rate increases to >120 beats per minute, systolic blood pressure decreases, pulse pressure decreases, capillary refill decreases, tachypnea worsens with a respiratory rate of 30 to 40 breaths per minute, urine output drops to 5 to 15 mL/hour, and the patient becomes confused, showing further evidence of decreased perfusion of the central nervous system.Class IVClass IV hemorrhage is marked by an estimated blood loss of >2,000 mL (or >40% of total circulating blood volume). During this phase, most compensatory cardiovascular mechanisms have been maximized and total hemodynamic collapse is imminent. Signs of class IV hemorrhage include severe tachycardia with a heart rate >140 beats per minute, a decreased systolic blood pressure, a decreased pulse pressure, delayed capillary refill, significant tachypnea with a respiratory rate of >35 breaths per minute, minimal to no urine output, and severely altered mental status as marked by confusion and/or lethargy.Potential Pitfalls
Despite these guidelines, several potential pitfalls exist that can make the diagnosis more difficult. Concurrent medication, such as β-blockers, may attenuate the physiologic response to hemorrhage. In the presence of β-blockade, tachycardia may be blunted or may not occur at all. Prior hydration status and use of diuretics can also alter the rate at which these signs present. Pregnant patients have a significantly increased total blood volume, and thus can lose up to 1,000 mL of blood before presenting with any clinical signs of hemorrhage. Blood is diverted from the placenta via vasoconstriction; the mother's total blood circulation is maintained at the expense of the fetus. Elderly patients may have atrial arrhythmias leading to a high ventricular response, making tachycardia less sensitive in this patient population. Concurrent use of antiplatelet or anticoagulant medication can cause relatively small injuries to bleed excessively, and identification and intervention may be delayed. Although unloading of the baroreceptors and activation of the sympathetic nervous system usually lead to tachycardia, some patients may respond to traumatic hemorrhage with bradycardia as a result of a vagal nerve–mediated transient sympathoinhibition due to acute and sudden blood loss (3,4,5,6,7,8,9). Finally, a significant reduction in skin blood flow (i.e., cool, clammy skin) is an early ominous sign of shock in view of selective cutaneous vasoconstriction (10). Intervention and resuscitation must be imminent upon presentation of these signs and symptoms.PathophysiologyCirculatory ChangesHemorrhage results in a predictable pattern of events that begins with acute changes in circulating blood volume and culminates in a final common pathway shared by all classifications of shock (Fig. 58.1). Hemodynamically, hypovolemic shock is characterized by a fall in ventricular preload, resulting in decreased ventricular diastolic filling pressures and volumes. This in turn leads to a decrease in cardiac output and stroke volume (3,4,5,11,12,13,14,15). Following unloading of the cardiac baroreceptors and activation of the sympathetic nervous system, tachycardia ensues in an attempt to compensate for the decrease in cardiac output and stroke volume (12). The sympathetic output also results in vasoconstriction, leading to a decrease in pulse pressure. Greater variations in blood pressure will occur with the respiratory cycle due to an increased sensitivity of the underfilled heart to changes in venous return with varying intrathoracic pressure (16,17,18). The increased sympathetic tone may prevent a severe drop in arterial blood pressure initially. However, continued blood loss will ultimately result in hypotension and shock (3). Due to compensatory vasoconstriction, systemic vascular resistance rises early after the development of hypovolemic shock, but may fall in later stages, potentially heralding irreversibility and death (3,19,20).The response to blood loss is a dynamic process that involves competing adaptive (compensatory) and maladaptive P.897responses at each stage of development. Although intravascular volume replacement is always a necessary component of resuscitation in hypovolemic shock, the complex biologic response to the insult may progress to a point at which such resuscitation is insufficient to reverse the progression of the shock syndrome. For instance, patients who have sustained greater than a 40% loss of blood volume for 2 hours or more may not be able to be effectively resuscitated. Severe hemorrhage leads to a series of inflammatory mediator, cardiovascular, and organ responses that supersede the injury itself and ultimately drive recovery or death (3,19,20,21,22,23,24,25).Oxygen BalanceShock is characterized by an oxygen deficit in tissues and cells. The significance of the deficit and the extent of cellular injury can be quantified as a function of both the severity and the duration of the deficit—the greater the severity, the longer the duration, the worse the outcome of shock.Oxygen delivery to tissues is determined by cardiac output and the oxygen content in arterial blood. Oxygen content refers to the number of milliliters of oxygen contained in 100 mL of blood (mL/dL) and is a function of the hemoglobin concentration, the oxygen saturation of hemoglobin, and the amount of oxygen dissolved in plasma (the calculation is [Hgb × 1.34 × O2 saturation] + [PaO2 ×
0.0003]). During hemorrhage, as the cardiac output falls, oxygen delivery to the tissues also falls.
Initially, the body will maintain sufficient uptake of oxygen by extracting more from the arterial blood. This will result in a fall in the mixed venous oxygen saturation (SvO2) with an increase in
the arteriovenous oxygen content gradient (CaO2 – CvO2). Eventually, this compensatory
mechanism also fails, and tissue hypoxia with lactic acidosis ensues. Cerebral and cardiac functions are maintained by diversion of blood flow from other organs (skin, muscle, and kidneys) (26). However, when these compensatory mechanisms are maximized, cardiac function and tissue oxygen delivery deteriorates further, and irreversible shock may develop (27).Critical oxygen delivery is a function of cellular needs for oxygen and the ability of cells to extract oxygen from the arterial blood. Many factors contribute to this equation. During hemorrhage, tissue oxygen needs may increase due to increased respiratory muscle activity and increased catecholamine circulation (28). However, some evidence suggests that catecholamines down-regulate the metabolic needs of cells during hypovolemic shock (4,5,28,29,30). Regional blood flow is modified during hypovolemic shock in an attempt to maintain oxygen delivery to critical tissues (26,31). In addition, the individual needs of various tissues may vary during hemorrhagic shock. For instance, the oxygen needs of the kidney may decline during hemorrhage because a fall in renal perfusion leads to a fall in glomerular filtration and a decrease in energy-consuming tubular absorption (26). In contrast, the gut may experience an increased oxygen debt early due to the high oxygen need of the mucosa, along with redistribution of blood away from the gut to more critical tissues. This is the physiologic basis for gastric tonometry as a means of measuring the adequacy of resuscitation early following hemorrhage (32,33).Oxygen extraction in tissues is influenced by the position of the oxyhemoglobin dissociation curve (34,35,36,37). Factors that improve the ability of tissues to extract oxygen from hemoglobin (i.e., shift the curve to the right) include acidosis, hypercarbia, hyperthermia, and decreased blood viscosity. However, in any extreme, each of these factors can be overcome by inadequate oxygen delivery and cardiovascular collapse. Interestingly, the oxyhemoglobin curve has been shown to shift to the left in critically ill patients (38). The presence of 2,3-diphosphoglycerate (DPG) in transfused blood has also been associated with a left shift of the oxyhemoglobin dissociation curve (39). Thus, although transfusions may increase the hemoglobin level, theoretically improving oxygen delivery, they may negatively affect the ability of tissues to extract oxygen from the hemoglobin.The severity of oxygen debt during hypovolemic shock has been shown to be a major determinant of survival in animals and in patients following trauma, hemorrhage, and major surgery (20,27,40,41). A large oxygen debt has been associated with the development of acute respiratory distress syndrome (ARDS) and multiple organ dysfunction syndrome (MODS) (33,40,41,42,43,44). Conversely, a high oxygen delivery and uptake during resuscitation has been associated with improved survival (27,41,42,43,44,45,46). Whether increasing oxygen delivery to supranormal levels ultimately improves survival during resuscitation in critical illness remains controversial, and the medical literature has produced mixed results (27,33,43,44,47,48,49,50).Cellular ResponseDuring hypovolemic shock, the oxygen deficit in the tissues causes a fall in the mitochondrial production and concentration of high-energy phosphates because of greater breakdown than production (51,52,53,54,55,56,57). This led many researchers to evaluate the utility of adenosine triphosphate (ATP) in the resuscitation of hemorrhagic shock (58,59). In the presence of sufficient oxygen, aerobic combustion of 1 mol of glucose yields 38 mol of energy-rich ATP. However, in the absence of sufficient oxygen, glucose taken up by the cells cannot be combusted because of insufficient uptake of pyruvate into the mitochondrial tricarboxylic acid cycle. Pyruvate is then converted to lactate within the cytoplasm. Anaerobic glycolysis yields only 2 mol of ATP, which is then hydrolyzed into hydrogen ion, ultimately leading to intracellular and extracellular metabolic acidosis (51,52,60,61,62) (Fig. 58.2). This process is ultimately a function of the severity and duration of regional hypoperfusion relative to oxygen demand and is more pronounced in some tissues (diaphragm, liver, kidney, gut) than in others (heart, skeletal muscle). Ultimately, a significant fall in the high-energy phosphates for a prolonged duration will lead to irreversible
cellular injury and death.The sequelae of low ATP production are profound. About 60% of the energy produced by respiring cellular mitochondria is needed to fuel the sodium-potassium (Na+-K+) pump of the cell. This pump controls the gradient in electrolyte concentrations and electric potential over the cell membrane. In the absence of sufficient ATP, the Na+-K+ pump is inhibited, resulting in an influx of sodium into the cell and efflux of potassium out of the cell. This in turn leads to cellular fluid uptake (51,53,63,64,65,66). Hyperkalemia may result due to potassium exchange between cells, the interstitial fluid, and vascular space.Independent of the Na+-K+ pump, there may be a selective increase in cell membrane permeability for ions during hemorrhagic shock. Hypovolemic shock has been shown to lead to a P.898rapid decrease in the transmembrane potential (with a less negative inner membrane potential), resulting in rapid electrolyte and fluid shifts across the membrane. Circulating heat shock proteins may also contribute to these changes independent of energy deficit (66,67,68,69,70,71).
Figure 58.2. Cellular mechanisms during anaerobic and aerobic glycolysis. In anaerobic conditions, pyruvic acid cannot enter the citric acid cycle within the mitochondria and is instead shunted to the production of lactate. This process produces only two molecules of adenosine triphosphate (ATP), as opposed to the 36 molecules of ATP produced from glucose in the mitochondria during aerobic glycolysis. Hydrolysis of ATP molecules in anaerobic conditions results in the production of hydrogen ions that cannot be cleared, leading to intracellular acidosis. (Adapted from Mizock BA, Falk JL. Lactic acidosis in critical illness. Crit Care Med. 1992;20[1]:80.)Finally, calcium (Ca2+) influx into cells and their mitochondria inhibits cellular respiration and ultimately contributes to cellular damage and swelling. Plasma levels of free Ca2+ may also fall. This may have profound consequences on the function of several organs during shock including the liver, kidney, heart, and vascular smooth muscle (64,65,72,73,74,75,76,77,78,79,80,81,82). Intracellular lysosomes lose their integrity, and proteolytic enzymes are released and contribute to cellular dysfunction and cell death.The sum of the intracellular changes and alterations in signaling transduction pathways described above ultimately leads to the development of cellular dysfunction and multiple organ dysfunction syndrome, which may be irreversible (82). Laboratory investigations are aimed at novel resuscitation techniques involving substances that attenuate abnormalities of cellular signaling following hemorrhagic shock (58,59,77,78,79,80,81,82).Neurohumoral ResponseIn response to hemorrhage and hypovolemia, a complex neurohumoral response is initiated in an attempt to maintain blood pressure and retain fluid. Decreased intravascular volume stimulates baroreceptors in the carotid body and aortic arch, along with mechanoreceptors in the right atrium. This stimulation leads to several neurohumoral responses (Fig. 58.3). Circulating catecholamines are liberated by activation of the sympathetic nervous system and the adrenal medulla. Direct sympathetic stimulation of the vessel wall leads to vasoconstriction. Angiotensin II is liberated via the renin–angiotensin–aldosterone system. Vasopressin (antidiuretic hormone [ADH]) is released by the pituitary in hypovolemic shock and leads to vasoconstriction. Finally, decreased cardiac filling pressures reduce cardiac secretion of α-atrial natriuretic peptide (ANP), thereby reducing the vasodilatory and diuretic effects of ANP.MacrocirculationDuring loss of circulating blood volume, mechanisms are initiated to counteract the fall in cardiac output and oxygen delivery by facilitating a redistribution of peripheral blood flow (26). Regional autoregulation takes place via a delicate balance of endogenous vasodilators and vasoconstrictors. Endothelial cells produce potent vasodilators such as endothelium-derived relaxing factor (nitric oxide [NO]), heme oxygenation–derived carbon monoxide (CO), and metabolic byproducts in tissues, including carbon dioxide (CO2), potassium, and adenosine (25,83,84,85,86,87,88,89). Some
authors describe that inhibition of NO early following hemorrhage ameliorates early hypotension and improves mortality (90,91,92,93,94). Conversely, other authors describe endothelial dysfunction in organs with diminished NO production (95,96). Endothelin is a potent endothelial cell–derived vasoconstrictor that is released upon catecholamine stimulation or hypoxia (97). The overall increase in systemic peripheral vascular resistance is distributed differently among various organs in the body (31). Vasoconstriction also occurs in the venous vasculature, increasing return of available blood to the heart (14,98). The complex interplay of these mechanisms for vasodilation and vasoconstriction ultimately determines the regional redistribution of blood flow to organs following hemorrhagic shock. The redistribution of blood flow results in a greater share of oxygen delivery to organs with high obligatory metabolic demands (heart and brain), and a lesser share to those with fewer demands including the skin, skeletal muscle, kidney, intestine, and pancreas (5,31,86,99,100,101).MicrocirculationOne of the most important determinants of tissue perfusion during shock is the response and function of the microvasculature, which is defined as vessels less than 100 to 150 µm in diameter. Although arteries and medium-sized arterioles constrict in response to the extrinsic control mechanisms described above, terminal arterioles, venules, and capillaries remain unaffected and are more controlled by local metabolic factors.
Figure 58.3. Neurohormonal response to hemorrhage. Hemorrhage results in a decrease in the circulating intravascular volume, which initiates a complex cascade of compensatory events. CNS, central nervous system; ACTH, adrenocorticotropic hormone; ADH, antidiuretic hormone.P.899Alterations in microvascular function and flow are effected through precapillary and postcapillary sphincters, which are sensitive to both extrinsic and intrinsic control mechanisms. Exchange of metabolites and compartmental regulation of fluids occurs at the capillary level. Therefore, alteration of tone of the pre- and postcapillary sphincters can have significant effects on microcirculatory function (102,103,104). Failure to dilate sphincters supplying metabolically active tissues may result in ischemia and anaerobic metabolism with lactate production. Increased precapillary tone, as seen with sympathetic stimulation, results in increased blood pressure systemically and decreased hydrostatic pressure locally. In fact, the microvascular arterioles may even dilate in response to the above vasoconstriction due to release of metabolic byproducts of underperfusion (carbon dioxide, hydrogen ion, etc.). The decrease in hydrostatic pressure locally then leads to redistribution of fluid from the interstitium to the circulation. Conversely, increased postcapillary tone (relative to precapillary tone) results in vascular pooling of blood and loss of fluid to the interstitium (as a result of increased hydrostatic pressure). This increased hydrostatic pressure may become accentuated in response to crystalloid resuscitation, leading to interstitial edema (104). Finally, hemorrhage and shock have also been shown to induce increased permeability of capillaries, leading to interstitial fluid leak during resuscitation (105,106).Hypovolemic shock and hemorrhage also induce the expression of endothelial adhesion molecules on neutrophils and endothelium (63,107). This results in neutrophil adherence and “rolling” of cells within the capillary bed (108,109,110,111,112,113). Capillary flow then diminishes and may also impair red blood cell flow. While this decrease in transit time may augment the ability of tissue to extract oxygen, it may also lead to microvascular thrombosis and further tissue ischemia (114,115).Metabolic and Hormonal ResponseThe early hyperglycemic response to trauma/hemorrhage is the combined result of enhanced glycogenolysis, caused by the hormonal response to stress including elevated epinephrine, cortisol, and glucagon levels; increased gluconeogenesis in the liver, partly mediated by glucagon; and peripheral resistance to the action of insulin (51,116). Increased gluconeogenesis in the liver, and to a lesser extent in the kidneys, follows increased efflux of amino acids, such as alanine and glutamine from the muscle to the liver, due to a breakdown of muscle protein. The P.900
latter is evidenced by increased urinary losses of nitrogen and a negative nitrogen balance. Lactate produced in muscle can also be converted to glucose in the liver (117). Increased epinephrine also results in skeletal muscle insulin resistance, sparing glucose for use by glucose-dependent organs such as the heart and brain. Later in shock, hypoglycemia may ensue, possibly because of glycogen depletion or hepatic ischemia (51,117,118). Fatty acids are increased early in shock, but later levels fall (116). Without energy for glycolysis, the cell depends on lipolysis and the autodigestion of intracellular protein for energy. Initially, ketone bodies and the branched-chain amino acids are used as alternative fuel sources. Without oxygen, these sources become inefficient, leading to hypertriglyceridemia, increased β-hydroxybutyric acid and acetoacetate levels, and changes in the amino acid concentration pattern. As these metabolic changes occur, set in motion by cellular hypoxia and promoted by systemic hormonal changes, structural changes occur within individual cells (119).Organ Perfusion and Function during HemorrhageHeartThe heart is a critical organ in the pathophysiology of shock. At baseline, myocardial oxygen extraction is almost maximal; therefore, increased cardiac work must be met by increased coronary blood flow. When coronary perfusion is compromised, as it is during systemic hypotension, cardiac function suffers. In the presence of sympathetic stimulation, blood flow from the endocardium is redistributed toward the epicardium, impairing cardiac performance (120). Underlying coronary artery disease, arrhythmias, hypoxemia, and acidosis can add to cardiac dysfunction. In the absence of coronary stenosis, myocardial necrosis/infarction is unusual in hypovolemic shock. Rather, the heart plays a participatory role in which it is unable to compensate fully for arterial hypotension caused by hypovolemia, vasodilation, and other factors.Under basal aerobic conditions, 60% of energy comes from fat (free fatty acids and triacylglycerides), 35% from carbohydrates, and 5% from amino acids and ketone bodies. However, during anaerobic conditions imposed by hypoxemia or ischemia, the myocardium shifts to glycolysis. Anaerobic glycolysis, however, is insufficient to meet cardiac work demands for any length of time because the myocardial glycogen stores, as an alternative fuel source, are minimal and rapidly depleted.BrainLike the heart, the brain almost exclusively depends on perfusion, rather than changes in extraction, to meet its oxidative metabolic needs. Protective mechanisms, collectively referred to as autoregulation, have evolved to guard perfusion. Pressure autoregulation refers to the ability of the brain to maintain total and regional cerebral blood flow (CBF) nearly constant despite large changes in systemic arterial blood pressure (Fig. 58.4) (121). Cerebral function seems to be maintained until the mean arterial pressure drops below 50 to 60 mm Hg (122). The factors that control cerebral autoregulation are not completely understood, but seem to include local carbon dioxide and oxygen tension, and the so-called Bayliss effect (i.e., contraction or dilation of arteriolar smooth muscle in the presence of increased or decreased intravascular pressure).
Figure 58.4. Autoregulation. Cerebral pressure autoregulation refers to the ability of the brain to maintain total cerebral blood flow (CBF) nearly constant between a broad range of mean arterial pressures (MAPs). Cerebral function seems to be maintained until the mean arterial pressure drops below 50 mm Hg. However, in the presence of traumatic brain injury, autoregulation may become impaired, and the brain may be more susceptible to changes in mean arterial pressure.In the presence of neurotrauma, autoregulation is impaired and the brain is exquisitely sensitive to secondary insults, such as hypoxia and hypotension. Hemorrhagic shock and resuscitation may also impair autoregulation because of endothelial cell dysfunction and diminished NO-dependent vasodilator reactivity, so that the brain may experience an oxygen deficit along with metabolic and functional deterioration (52,87). However, the vulnerability of the brain to anoxic injury is uncertain and appears variable. The adequacy and the method of resuscitation can critically influence postischemic recovery. These observations have motivated investigation of specific brain
resuscitation regimens (123,124,125,126). However, there are no conclusive data that one modality provides improved outcomes.LungsHypovolemic shock is associated with a rise in minute ventilation marked by tachypnea, hyperventilation, and a fall in arterial PCO2 (28,30,127,128,129,130). These changes are usually
due to a decrease in pulmonary perfusion, leading to an increase in dead space ventilation. Thus, a higher minute ventilation is necessary for a given CO2 production (28,30,127). In addition, minute
ventilation may need to increase further in order to compensate for a metabolic acidosis following accumulation of lactic acid in the blood. The imbalance between the increased demands of the diaphragm and reduced blood flow in shock may finally lead to respiratory muscle fatigue and respiratory failure, requiring intubation (28). Therefore, early airway control is imperative in patients with severe hemorrhagic shock.Hemorrhagic shock requiring massive transfusion also increases the risk of acute respiratory distress syndrome (129,130,131,132). Contributing factors include release of P.901proinflammatory mediators; activation of neutrophils in the lungs and other organs after reperfusion; contusion and/or ischemia-reperfusion of the lung; pulmonary microemboli of neutrophils, platelets, and fat particles from long bone fractures; and induction of transfusion-related acute lung injury (TRALI), which is discussed later in this chapter.KidneyOliguria, as defined by a urinary output of less than 0.5 mL/kg/hour, is a cardinal manifestation of shock. However, the pathogenesis of shock-related oliguria is more complex than mere renal hypoperfusion (133,134,135). Blood flow to the kidney is rarely reduced below 40% to 50% of normal levels, even in the face of more severe reductions in overall cardiac output. Thus, the decreased glomerular filtration rate results from additional mechanisms. Sympathetic stimulation, circulating catecholamines, angiotensin, and locally produced prostaglandins contribute to afferent arteriolar vasoconstriction. These compounds promote the redistribution of blood flow away from cortical glomeruli toward the renal medulla (65). Vasodilation of the efferent arteriole may amplify these changes. The net effect is a decreased glomerular filtration rate and a decrease in the energy needs of the kidney. Additional fluid (and salt) conservation is promoted by the effects of aldosterone and antidiuretic hormone.If renal hypoperfusion persists, the cortical kidney will become ischemic. Three pathologic changes are observed: (a) tubular necrosis with back-diffusion of glomerular infiltrate, (b) tubular obstruction by casts or other cellular debris, and (c) tubular epithelial damage with consequent interstitial edema and tubular collapse. Following hypovolemia and renal ischemia, these pathologic changes may be secondary events (i.e., reperfusion injury) that can amplify but rarely initiate acute renal failure. The presence of these pathologic changes partially explains why restoration of normal hemodynamic function does not often lead to an immediate improvement in renal function. Although irreversible renal failure from shock alone is rare, fluid and electrolyte balance are often supported by dialysis although normal perfusion has been restored.IntestineDuring hypovolemic shock, blood flow from intestine is redistributed to other organs. The decrease in blood flow to the gut is relatively greater than the decrease in cardiac output due to the local vasoconstriction caused by catecholamines, vasopressin, and angiotensin II (4,5,26,136,137,138,139). Ischemic injury to the gut is manifested primarily by interstitial fluid sequestration and hemorrhage or necrosis of the mucosal lining, and is most prominent in the stomach (139). Ulcer formation (140) with exsanguinating hemorrhage can occur several days after normal hemodynamic function has been restored (141). Breakdown of the gut epithelium creates a port of entry for translocation of bacteria or deleterious bacterial products (endotoxin) (142,143). These factors may be important in the pathogenesis of irreversible shock (144) by releasing mediators to the systemic circulation. The determination of mucosal pH via tonometry has been described as a potential indicator of the therapeutic response and a marker of MODS (145,146).
LiverHepatic perfusion declines during hypovolemic shock because of diminished portal and hepatic arterial blood flow, roughly in proportion to the fall in cardiac output (57,61,109,147,148,149,150). Clinical manifestations of ischemic liver injury are not usually apparent in the early stages of hemorrhagic shock, as the organ participates in the release of acute-phase reactants. As hepatic cells die, they release characteristic enzymes (i.e., aspartate aminotransferase, alanine aminotransferase) (151). Occasionally, an obstructive picture with elevated bilirubin and alkaline phosphatase predominates. Later, the synthesis of coagulation factors, albumin, and prealbumin may deteriorate (152,153). Less clinically obvious is the impairment in the reticuloendothelial system function. Impaired hepatic clearance functions and reticuloendothelial system failure contribute to continued circulation of vasoactive substances that can perpetuate shock. Hepatic ischemia may result in a diminished capacity for metabolism of drugs and for gluconeogenesis from lactate and amino acids, contributing to hypoglycemia in the late stages of hypovolemic shock. The capacity to clear gut-derived endotoxin and lactate may also decrease, and the ischemic liver produces lactate (154). The appearance of “shock liver” with massive hepatocellular necrosis is unusual and presents mainly in patients with pre-existing liver conditions (155).SpleenThe spleen contracts during hypovolemic shock, probably due to an increased sympathetic tone, which results in the release of red blood cells into the circulation (5,26). Changes in hematocrit during the early phase of bleeding probably underestimate the severity of plasma losses. The spleen also releases stored platelets.PancreasThe importance of the pancreas in the clinical picture in hemorrhagic shock has not been fully established. Older studies have demonstrated that the pancreas becomes severely ischemic during hypovolemic shock (156). Recently, much work has been done to better elucidate the role of the pancreas following hemorrhage and reperfusion. Preliminary data suggest that following hemorrhage, the mucosal barrier of the intestine becomes ischemic and therefore has increased permeability to pancreatic enzymes. These digestive enzymes then gain access to the wall of the intestine, initiating self-digestion of submucosal extracellular matrix proteins and interstitial cells. This initiates the generation and release of a host of strong inflammatory mediators, which may contribute to the multiorgan dysfunction syndrome. Recent investigations are focusing on protease inhibition in the intestinal lumen as a means of attenuating the inflammatory response following hemorrhage (157,158,159,160,161,162,163).Inflammatory Response and Tissue InjuryA detailed discussion of the inflammatory and immune response to trauma and hemorrhage is beyond the scope of this P.902chapter. However, several general concepts can be introduced. Following hemorrhage and resuscitation, macrophages, including lung macrophages and Kupffer cells in the liver, may release proinflammatory cytokines including tumor necrosis factor (TNF)-α and interleukin (IL)-1, -6, and -8. During reperfusion, cytokines may induce and amplify the inflammatory response to ischemia and may further induce local and remote organ damage (148,164,165,166,167,168,169,170,171,172,173,174). The reperfused gut, for example, may, together with the liver, be a source of systemically circulating cytokines, and possibly endotoxin. Release of mediators into the mesenteric lymph, portal, or systemic circulations during reperfusion may have deleterious effects on remote organs, such as the lungs, due to neutrophil activation and adherence, leading to pulmonary vascular injury with increased permeability (165,168,169). Circulating levels of proinflammatory cytokines may thus be of predictive value for remote organ damage, including ARDS, after trauma and hemorrhage in patients (167,170).Arachidonic acid makes up 20% of cell membranes and is released from these membranes in response to a multitude of stimuli that activate phospholipase A2 and C, and is then metabolized via
one of two major enzyme systems. The cyclo-oxygenase pathway results in the production of
thromboxanes and prostaglandins, while the lipoxygenase pathway produces leukotrienes. Thromboxane has potent vasoconstricting properties on both the pulmonary and splanchnic circulation, promotes aggregation of thrombocytes and neutrophils, causes bronchoconstriction, and can lead to increased vascular permeability. The prostaglandins have varied effects. Prostacyclin (prostaglandin I2 [PGI2]) has potent vasodilating properties and inhibits thrombocyte and neutrophil
aggregation (175). PGE2 and PGD2 also have vasodilating properties, while other prostaglandins
(PGF2α) are potent vasoconstrictors. Leukotrienes, which are produced by the lipoxygenase
pathway, cause vasoconstriction and increased capillary permeability and attract neutrophils (175). Thromboxane, prostaglandins, and leukotrienes interact with other mediators in a complex fashion (175,176,177,178,179). Vasoconstricting prostaglandins may be involved in the tissue damage during ischemia/reperfusion. Vasodilating prostaglandins may be involved in the vasodilated state of terminal hypovolemic shock (3,175,176,177,178,179).Platelet-activating factor (PAF) is a nonprotein phospholipid, which is secreted by many cells including platelets, endothelial cells, and inflammatory cells. It is a major mediator of the pulmonary and hemodynamic effects of endotoxin. The major systemic effects of PAF are vasodilatation, cardiac depression, and enhancement of capillary leak. Its complex interactions with other mediators are still poorly understood (180).Antigen–antibody complexes activate the complement cascade, and complement fragments thus generated can interact with other cytokines to promulgate the inflammatory response. Complement activation can yield potent vasodilating and leukoattractant substances (175,177,181,182).Oxygen radicals, such as hydrogen peroxide and superoxide anion, are released by activated neutrophils in response to a variety of stimuli. They are also released when xanthine oxidase is activated after reperfusion in ischemia-reperfusion models. These highly reactive products lead to cell membrane dysfunction, increased vascular permeability, and release of eicosanoids (183,184,185,186).This inflammatory process results in the local accumulation of activated inflammatory cells, which release various local toxins such as oxygen radicals, proteases, eicosanoids, platelet-activating factor, and other substances. When unregulated, such accumulations can cause tissue injury. The initial attachment of neutrophils to the vascular endothelium at an inflammatory site is facilitated by the interaction of adherence molecules on the neutrophil and endothelial cell surfaces (108,187,188,189,190,191,192).Immune Function following Hemorrhage and ResuscitationDespite the initiation of the inflammatory cascade, hypovolemic shock and resuscitation depress the immune system by suppressing the function of lymphocytes, macrophages, and neutrophils, depressing both humoral and cellular immune responses, decreasing antigen presentation and delayed hypersensitivity to skin-test antigens, and increasing susceptibility to sepsis (63,166,193,194,195,196,197,198). The immune consequences of hemorrhage and resuscitation differ among cell populations, however, with some cells expressing enhanced (199,200,201) and others diminished inflammatory responses (202,203). Hormone may also influence immune response (204,205). The immunosuppression after hypovolemic shock may also be potentiated by the release of anti-inflammatory cytokines (IL-10) (206,207,208) and soluble cytokine receptors (receptor antagonists) for the proinflammatory cytokines (203,209,210).Management of Hemorrhagic ShockTrauma is by far the most common etiology for hemorrhagic shock. While other causes do exist, management priorities are similar regardless of the source of bleeding. Diagnosis, evaluation, and management must often occur simultaneously. A methodical approach is necessary to optimize outcome. Unique to hemorrhagic shock, as opposed to other forms of shock, is that definitive management frequently requires surgical or procedural intervention to cease bleeding. The diagnostic pathway and interventions pursued become part of the resuscitation pathway. What follows is a summary of the interventions, diagnostic studies, monitoring strategies, and resuscitation techniques for hemorrhagic shock.Immediate Management
Airway and BreathingWhen approaching any patient in shock, the sequence of events should be to address the issues of airway, breathing, and circulation—also known as the “ABCs” (211). Most patients with fully developed shock require tracheal intubation and mechanical ventilation, even if acute respiratory failure has not yet developed. Studies have shown that during shock, the respiratory muscles require a disproportionate percent of the cardiac output (28). Failure to mount a hyperventilatory response to a metabolic acidosis is a significant predictor of the need for P.903subsequent intubation in trauma patients (212). Mechanical ventilation allows flow to be redistributed, lessens the work of breathing, may help reverse lactic acidosis, and supports the patient's airway until other therapeutic measures can be effective. Tracheal intubation is also required if there is evidence of mental status changes, such that airway protection is questionable. Evidence of hypoxemia and/or hypoventilation is also an absolute requirement for early intubation.Perhaps most complex is the patient with evidence of compensated hemorrhagic shock whose mental status is still intact. In this type of patient, clinical acumen is imperative. If the initial response to resuscitation is sustained (i.e., “a responder”—see below), then close observation of the airway may be appropriate while additional workup and treatment are pursued. However, in a patient who is not responsive or has a transient response (see below) to fluid resuscitation, control of the airway early is necessary prior to respiratory collapse (212). In addition, if diagnostic and therapeutic interventions, such as angiography and embolization, are required during resuscitation to control hemorrhage, early airway control should be obtained.Once the airway is secured, it is important to closely monitor techniques of ventilation. Studies have shown that there is a tendency of rescue and medical personnel to hyperventilate patients during resuscitation (213,214). Hyperventilated patients have been shown to have an increased mortality when compared to nonhyperventilated patients in the setting of severe traumatic brain injury (214). Animal studies have supported this information, showing that cardiac output increases with hypoventilation and decreases with hyperventilation and positive end-expiratory pressure (PEEP) (215,216). Thus, adequate appropriate ventilator strategies are imperative early in hemorrhagic shock to optimize tissue perfusion and outcome.CirculationThe management steps to restore adequate circulation are threefold:
Secure access to the bloodstream in order to initiate infusion of fluids and blood products Control obvious sources of hemorrhage and prevent ongoing hemorrhage Assess extent of shock and hemorrhage
Intravenous AccessAccess to the bloodstream should be obtained expediently. Two peripheral large-bore intravenous catheters (18 gauge or larger) are necessary. If cannulation of a peripheral vein is difficult due to collapse, then central venous access should be secured. In the presence of trauma to the torso, venous access above and below the diaphragm is preferable. When obtaining intravenous access, it is important to note that the maximal rate of infusion via a catheter is directly proportional to the diameter of the catheter and indirectly proportional to the length. Therefore, a 9 French percutaneous introducer sheath will infuse fluids more rapidly than a 7 French triple-lumen catheter. A large-bore peripheral intravenous catheter will also infuse fluids more rapidly than a 7 French triple lumen catheter due to a shorter length and less resistance. In pediatric patients, an intraosseous access may be necessary. This is only recommended for children under the age of 6 and should only be used until an alternative source of venous access is obtained.Control Obvious Hemorrhage ImmediatelyResuscitation of the bleeding patient requires early identification of potential bleeding sources followed by prompt action to minimize blood loss, restore tissue perfusion, and achieve hemodynamic stability. This is particularly important in the trauma patient where multiple sources may be involved. Wound compression is the initial maneuver to control an exsanguinating wound.
For massive soft tissue injuries, placing a tourniquet proximally may decrease hemorrhage and allow resuscitation prior to definitive control. Fractures should be splinted or placed in traction. Evidence of pelvic instability or hemorrhage may be temporized by a sheet, a pelvic binder, an external fixator, or a pelvic C-clamp (217,218,219,220). In the presence of massive trauma, patients may present with coagulopathy in the emergency department and this should be preemptively addressed. The same principles should be applied to nontraumatic hemorrhagic shock, such as gastrointestinal bleeding and ruptured aortic aneurysms: rapidly identify and attenuate the obvious sources of hemorrhage.Initiate Resuscitation and Assess Extent of Bleeding: Responders and NonrespondersThe traditional classification of hemorrhagic shock was discussed earlier (Table 58.3). While this is a useful guideline for determining the extent of blood loss for a given patient, perhaps more important in determining an appropriate treatment algorithm is the patient's response to resuscitation. Following hemorrhage, resuscitation should be initiated with 2 L of lactated Ringer solution or isotonic crystalloid solution. The response to this initial fluid bolus will provide critical insight as to the presence of ongoing hemorrhage and need for surgical intervention (Table 58.4) (221).Rapid responders become hemodynamically normal and remain this way following the initial fluid bolus. This group of patients has likely lost <20% of their total circulating blood volume, and ongoing aggressive resuscitation is not necessary. Intravenous fluids can be lowered to maintenance rates while additional workup proceeds. Blood should still be sent for type and cross-match and should be made available. Retrospective studies have shown that patients with field hypotension who become normotensive on arrival to the emergency department have increased morbidity, mortality, need for operation, and admission rate to the intensive care unit (ICU) (222,223,224). Approximately 15% of these patients will need transfusion, with 37% requiring therapeutic surgery (224). Hence, even a brief episode of hypotension can be a marker for significant underlying injury.Transient responders represent a group of patients who initially respond to a 2-L bolus of crystalloid, but then begin to show signs of deterioration when intravenous fluid infusion is lowered to maintenance levels. These patients have likely lost 20% to 40% of their circulating blood volume, and either have ongoing blood loss or inadequate resuscitation. Continued fluid resuscitation and initiation of blood transfusion are indicated. A transient response to blood infusion indicates ongoing hemorrhage. Rapid surgical intervention or angioembolization (225,226,227,228) to control hemorrhage is immediately indicated.Nonresponders represent patients who fail to respond to crystalloid and blood administration in the emergency department. These patients have likely lost >40% of their circulation blood volume and have ongoing hemorrhage. Immediate control of hemorrhage is necessary via surgical intervention P.904or angioembolization in the face of significant pelvic fractures (225,226,227,228). On rare occasions, failure to respond to fluid administration may be due to pump failure as a result of blunt cardiac injury, cardiac tamponade, tension pneumothorax, or myocardial infarction. Central venous pressure monitoring and cardiac ultrasonography may help differentiate between various etiologies in this setting.
Table 58.4 Response to initial fluid resuscitation and patient management Rapid response Transient response No responseVital signs Return to normal Transient response, recurrent
hypotension, and/or tachycardiaRemains abnormal
Estimated blood loss
Minimal (10%–20%) Moderate (20%–40%) Severe (>40%)
Additional crystalloid
Unlikely Yes Yes
Need for blood transfusion
Unlikely Moderate to high Immediate
Blood preparation Type and cross-match Type-specific (10–20 min) Emergency blood
(30–60 min) release(immediate type O Rh-negative blood)
Operative intervention
Possible Likely Highly likely
Early presence of surgeon
Yes Yes Yes
Adapted from American College of Surgeons Committee on Trauma. Shock. In: Advanced Trauma Life Support. 7th ed. American College of Surgeons Chicago, IL; 2004:79.Emergency Department Resuscitative ThoracotomyResuscitative thoracotomy is occasionally indicated for exsanguinating hemorrhage. In trauma, indications for resuscitative thoracotomy include (a) patients with penetrating thoracic injuries who arrive pulseless, but with myocardial electrical activity, and (b) blunt trauma patients who have vital signs on arrival but then sustain a witnessed arrest or onset of pulseless electrical activity. Specific recommendations are listed in Table 58.5. Therapeutic maneuvers that can be attained with a resuscitative thoracotomy include (a) evacuation of pericardial blood causing tamponade, (b) direct control of exsanguinating thoracic or cardiac hemorrhage, (c) open cardiac massage, and (d) cross-clamping of the descending aorta to slow blood loss below the diaphragm and improve perfusion to the heart and brain.Depending on the cause of injury, the overall mortality rate in these situations is extremely high (229,230,231). The highest survival rates are found in patients with isolated cardiac injury without loss of vital signs (approximately 35%). Some reports of thoracic aortic cross-clamping for exsanguinating intra-abdominal hemorrhage have reported survival rates of nearly one third (231,232), but this is mainly in the setting of penetrating abdominal trauma. Survival rates following resuscitative thoracotomy in blunt trauma are dismal, ranging from 0% to 5%. Aortic cross-clamping should be viewed as an adjunct to other initial hemorrhage control measures. It has not been established whether thoracic aortic clamping should be performed before or after the abdominal incision, or whether thoracic or intra-abdominal aortic cross-clamping is more effective (233). However, when aortic cross-clamping is deemed necessary for continuous bleeding or low blood pressure, the prognosis is generally poor (234). No clinical data exist for the use of emergency room thoracotomy in nontrauma infradiaphragmatic bleeding.Adjunctive MeasuresHistorical teachings have been that tilting a patient into head-down position (i.e., Trendelenburg) diverts blood volume into the central circulation and improves venous return, thereby improving stroke volume and cardiac output in hypovolemic shock. However, recent studies do not show any significant redistribution of blood volume centrally (235). In fact, the head-down position can worsen gas exchange and cardiac function. Therefore, the Trendelenburg position is no longer recommended as a resuscitative technique. If this type of measure is deemed desirable, raising the legs above the level of the heart should be adequate (13).
Table 58.5 Indications and contraindications for emergency department resuscitative thoracotomy
INDICATIONSSalvageable postinjury cardiac arrest
Patients sustaining witnessed penetrating trauma with <15 min of prehospital cardiopulmonary resuscitation (CPR)
Patients sustaining witnessed blunt trauma with <5 min of prehospital CPR
Persistent severe postinjury hypotension (systolic blood pressure ≤60 mm Hg) due to:
Cardiac tamponade Hemorrhage—intrathoracic, intra-abdominal, extremity, cervical
Air embolism
CONTRAINDICATIONS•Penetrating trauma: CPR >15 min, anda
•Blunt trauma: CPR >5 min, and No signs of lifea or asystoleaNo signs of life = no pupillary response, respiratory effort, or motor activity.Adapted from Cothren CC, Moore EE. Emergency department thoracotomy for the critically injured patient: objectives, indications, and outcomes. World J Emerg Surg. 2006;1:4.P.905The use of pneumatic antishock garments (PASGs, previously military antishock trousers [MAST]) currently has a limited role in the management of hypotensive trauma patients. Although their use was almost universal for hemorrhage control in the late 1970s and 1980s, recent studies have demonstrated that they have no effect on patients with thoracic injury. In fact, some evidence suggests that mortality is higher when PASGs are applied (236,237). No survival advantage has been demonstrated in the pediatric population, although there may be a small survival benefit in children with a systolic blood pressure of less than 50 mm Hg (238). The main utility of PASGs currently is as a temporizing agent to stabilize pelvic fractures.Fluid ResuscitationCareful attention to fluid resuscitation is necessary during management of hemorrhagic shock to optimize outcome. It is still unclear which type of fluid should be employed in the initial treatment of the bleeding patient.Colloids versus CrystalloidsSeveral meta-analyses have shown an increased risk of death in patients resuscitated with colloids as compared with crystalloids (239,240,241,242,243) during hemorrhagic shock. While three of these studies suggested that the effect was particularly significant in the trauma population (239,242,243), the results of a recent meta-analysis showed no significant difference (244). A recent trial evaluating 4% albumin versus 0.9% normal saline in nearly 7,000 ICU patients showed that albumin administration was not associated with worse outcome. There was a trend, however, toward higher mortality in the trauma subgroup that received albumin (p = 0.06) (245). The difficulty with interpreting these meta-analyses and the individual studies is that they are very heterogenous. Each evaluates different patient populations and resuscitation strategies, and mortality may not always be a primary end point. However, given these results, crystalloid resuscitation is currently the accepted standard as initial therapy for hemorrhagic shock.Many synthetic colloid solutions such as hetastarch and dextran have also been associated with coagulopathy. Recent research suggests that hetastarch solutions with a high mean molecular weight and a high C2/C6 ratio suppress coagulation more than solutions with rapidly degradable low-molecular-weight colloids (246,247,248). This coagulopathy may be produced by one of several potential mechanisms including a reduction in von Willebrand factor, platelet dysfunction, reduced factor VII levels, and an interaction with fibrinogen (249,250).Crystalloid solutions are not without side effects. Resuscitation with fluids that contain supraphysiologic concentrations of chloride can lead to hyperchloremic acidosis. This can be significant in patients where lactic acidosis may already be present. Lactated Ringer solution contains a more physiologic concentration of chloride (109 mEq/L) than normal saline (NS 154 mEq/L), and therefore may be the preferred choice. Animal studies have also shown that resuscitation with normal saline can lead to more coagulopathy and increased blood loss than resuscitation with lactated Ringer solution (251).Massive resuscitation with crystalloid fluids alone can lead to several significant complications including cardiac and pulmonary complications, gastrointestinal dysmotility, coagulation abnormalities, and immunologic dysfunction (252). Reports of lactated Ringer solution and normal saline increasing reperfusion injury and leukocyte adhesion suggest that crystalloid resuscitation may worsen acidosis and coagulopathy in severely injured patients and possibly increases the risk of ARDS, systemic inflammatory response syndrome (SIRS), and multiorgan failure (MOF)
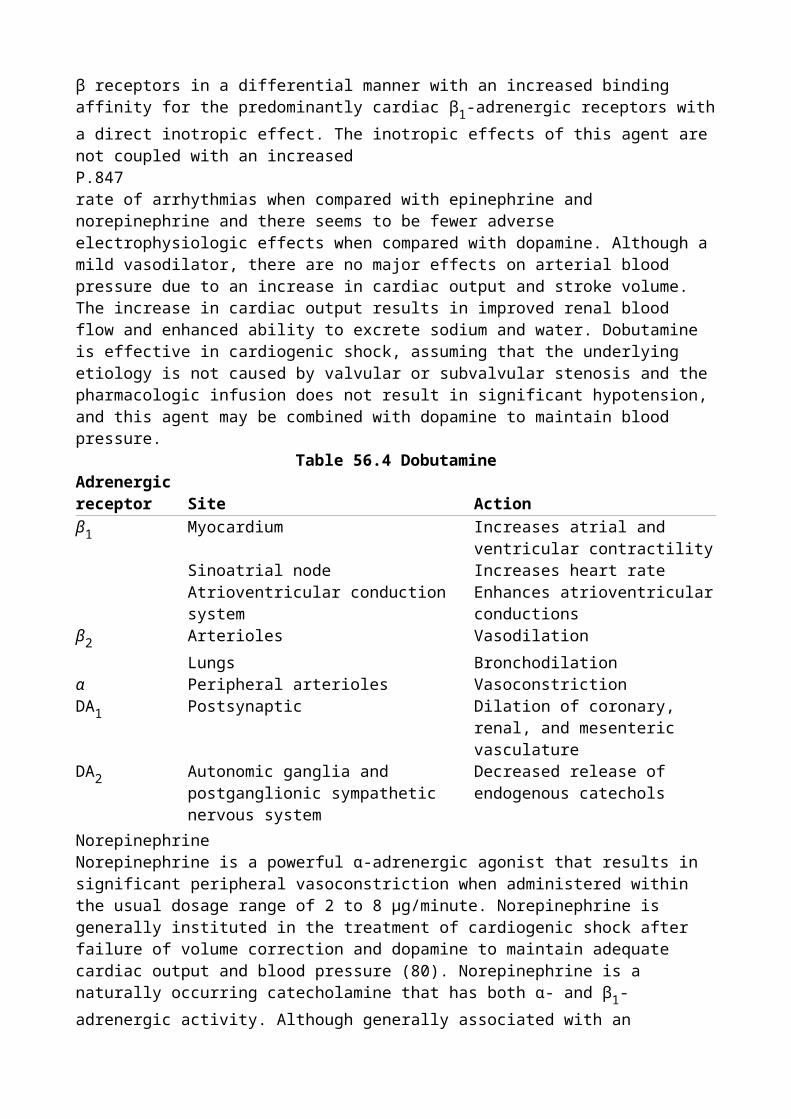
(252,253,254,255,256). Abdominal compartment syndrome has been clearly associated with excessive use of crystalloid resuscitation (50,257,258,259,260,261). Recently, there has been increased focus on early use of blood products in order to minimize crystalloid use in the resuscitation of hemorrhagic shock (262). Finally, resuscitation strategies that focus on early aggressive fluid resuscitation to normalize blood pressure before bleeding is controlled may result in increased hemorrhage and increased mortality. This has led some authors to suggest that “hypotensive resuscitation” should be the goal until the source of hemorrhage is controlled (263,264,265). However, the exact goals for mean arterial pressure and trigger points for bleeding have not been established. The potential adverse sequelae when used in patients with associated injuries or comorbidities (i.e., severe closed head injury) have not been clearly established (266).In light of these potential sequelae of resuscitation, future research should focus on improvement in fluid composition and adjuncts to the administration of large volumes of fluid (266). Current strategies should focus on the type of fluid delivered, the rate of delivery, the timing of delivery, and the prevention of sequelae from large-volume resuscitation.Preventing HypothermiaAll fluids during resuscitation from hemorrhagic shock should be warmed to prevent hypothermia. Equipment is now available that allows the rapid infusion of blood and/or crystalloids at warmed temperatures (i.e., up to 750 mL fluid per minute warmed to over 37°C). This newer equipment is more effective and efficient and results in fewer complications associated with earlier models (such as air embolism and bacterial contamination) (267). Other techniques during resuscitation that can be used to prevent hypothermia in the acutely hemorrhaging patient include warming the circuit on the ventilator in ventilated patients, ensuring the patient is covered with warm blankets at all times following exposure and thorough examination, warming the resuscitation and operating rooms, using external warming blankets such as the Baer hugger during resuscitation and in the operating room, and using warm water blankets on the operating room table during exploratory operations. Hypothermia is clearly associated with increased mortality following resuscitation from hemorrhagic shock (268), and every attempt to prevent or minimize its occurrence and severity should be employed.Diagnostic ApproachIf no obvious source of external bleeding is identified, a rapid evaluation should be performed to identify likely occult sources of bleeding. In the trauma patient, significant internal hemorrhage can occur in four defined regions: the thoracic cavity, the peritoneal cavity, the retroperitoneum, and extremity fractures. These areas can be rapidly assessed via chest radiograph, a pelvic radiograph, FAST, and physical examination of extremities along with appropriate radiographs. In-depth coverage of the diagnosis of abdominal trauma is provided in a later P.906chapter of this book. In nontrauma patients without clear evidence of bleeding, the gastrointestinal tract should be rapidly evaluated via nasogastric tube, rectal examination, and endoscopy where appropriate. Additional diagnostic tests can be obtained based on clinical history, patient background, and condition. Abdominal aortic aneurysms can be identified on physical examination, by ultrasound, or by calcifications on abdominal radiograph. In selected instances, angiography may be used to identify and treat sources of hemorrhage not otherwise apparent (pelvic fractures, pancreatitis, lower gastrointestinal bleeding) (225,226,227,228,269,270,271,272,273,274,275,276,277). This should only be instituted when a specific source of hemorrhage is highly likely and therapeutic intervention is sought. Computed tomography should never be sought in hemodynamically unstable patients with hemorrhage.Laboratory Testing and Monitoring of ResuscitationMeasurement of BleedingHematocrit/HemoglobinHemoglobin and hematocrit measurements have long been part of the basic diagnostic workup of patients with hemorrhage and/or trauma. However, in patients with rapid bleeding, a single hematocrit measurement on presentation to the emergency department may not reflect the degree of

hemorrhage. In a short transport or presentation time, prior to initiation of resuscitation, the body's compensatory mechanisms for fluid retention and resorption into the vascular space have not taken place, and initial hematocrit levels may remain stable despite significant blood loss. A retrospective study of 524 trauma patients (278) determined that the initial hematocrit had a sensitivity of only 0.50 for detecting patients with an extent of traumatic hemorrhage requiring surgery. The diagnostic value is further confounded by the administration of intravenous fluids and red cell concentrates during resuscitation (278,279,280,281).Two prospective observational studies determined the sensitivity of serial hematocrit measurements for detecting patients with severe injury (282,283). In the first study (282), the authors compared values of hematocrit at admission and 15 minutes and 30 minutes following arrival to the emergency department. A normal hematocrit on admission did not preclude significant injury. The mean change in hematocrit levels between arrival and 15 minutes, and 15 minutes and 30 minutes was not significantly different in patients with or without serious injuries. However, a decrease of hematocrit by >6.5% at 15 and 30 minutes had a high specificity for injury (0.93–1.0), but a low sensitivity (0.13–0.16).Another prospective observational study examined the utility of serial hematocrit measurements during the initial 4 hours following admission (283). A significant limitation to this study is that they removed patients who required a blood transfusion in order to eliminate confounding variables. In the remaining 494 patients, a decrease in hematocrit of more than 10% between admission and 4 hours was highly specific for severe injury (0.92–0.96), but again, it was not sensitive (0.09–0.27).Overall, decreasing hematocrit levels over time may reflect continued bleeding. However, patients with significant bleeding may maintain their hematocrit level, especially in the absence of resuscitation. Conversely, hematocrit levels may also be confounded by aggressive fluid resuscitation early during resuscitation (278,279,280,281). An initial hematocrit level will help to identify patients who present with pre-existing anemia who may have a lower threshold for hemorrhage. The hematocrit level should be used in conjunction with other measures of perfusion in order to determine the presence of occult hemorrhage.Measurements of PerfusionLactateLactate was initially suggested as a diagnostic parameter and prognostic indicator of hemorrhagic shock in the 1960s (284). Substantial data exist that lactate levels as a marker of tissue oxygen debt can predict outcome in various forms of shock (60,285,286,287,288). In 1983, Vincent et al. performed a prospective study on 27 patients with circulatory shock and concluded that changes in lactate concentrations provided an early and objective evaluation of a patient's response to therapy (289). However, its overall utility has been questioned by some because it is felt to be a late marker of tissue hypoperfusion, can be affected by hepatic function, and can be influenced by glycolysis and alkalosis (290,291,292,293).Despite these concerns, data do exist showing that the amount of lactate produced by anaerobic glycolysis is an accurate indirect marker of oxygen debt, tissue hypoperfusion, and the severity of hemorrhagic shock (294,295,296,297,298,299,300,301,302,303,304,305). In many forms of shock, arterial lactate levels above 2 mEq/L have been associated with increased mortality (286,287,300,305). However, during hemorrhage, not only is the initial lactate level important, but also the rate of clearance (298,299). Two prospective studies confirm this. In one prospective observational study (298), 76 patients with multiple trauma were analyzed with respect to clearance of lactate between survivors and nonsurvivors over 48 hours. If lactate normalized within 24 hours, survival was 100%. Survival decreased to 77.8% if normalization occurred within 48 hours, and to 13.6% in those in whom lactate levels remained elevated above 2 mEq/L for more than 48 hours. This was confirmed in another prospective study of 129 trauma patients (299) in which initial lactate levels were higher in nonsurvivors. A prolonged time to normalization (>24 hours) was associated with the development of posttraumatic organ failure. Finally, venous lactate has been shown to be an excellent approximation for arterial lactate in acute trauma patients and is a useful marker for significant injury (306).
Taken together, these studies suggest that both the initial lactate level and the rate of clearance are reliable indicators of morbidity and mortality following trauma. However, whether lactate should be used as an end point of resuscitation or is merely a marker of tissue ischemia has not been clearly established.Base DeficitBase deficit values derived from arterial blood gas analysis have also been shown to provide an indirect estimation of tissue acidosis due to impaired perfusion (294,296,297,300,301,302,303). However, base deficit can be affected by resuscitation fluids (hyperchloremic metabolic acidosis) and exogenous administration of sodium bicarbonate. Despite these potential drawbacks, initial base deficit has been shown in several retrospective studies to correlate with transfusion requirements, organ dysfunction, morbidity, and mortality following trauma (307,308,309,310,311,312,313). The magnitude and severity of the base deficit also correlates to outcome, and is useful in both pediatric and elderly patients (307,310,311,312). Base deficit has been shown to P.907be a better predictor of outcome than pH alone following traumatic injury (309). Recently, serum bicarbonate levels have been shown to be an appropriate surrogate for arterial base deficit in the ICU (314,315).Lactate versus Base DeficitAlthough many studies have shown that both base deficit and serum lactate levels correlate with outcome following trauma and hemorrhage, these two parameters do not always correlate with each other (304,316). In fact, lactate has been found to be a superior predictor of mortality as compared to base deficit in a recent study of patients in the intensive care unit following trauma (304). Both base deficit and lactate have been shown to correlate to outcome in nontraumatic etiologies of hemorrhagic shock (268,317). Given that there are confounding variables following trauma that can affect measured levels of both lactate and base deficit, independent assessment of both parameters along with the patient's clinical condition is recommended for the evaluation of shock in trauma patients.Measurement of CoagulopathyStandard Coagulation StudiesCoagulopathy associated with hemorrhagic shock may be due to one of several etiologies: (a) iatrogenic, in which a dilutional coagulopathy develops due to inadequate resuscitation with clotting factors and blood products; (b) premorbid, in which some patients may have a pre-existing coagulopathy due to underlying disease (such as cirrhosis, hemophilia, von Willebrand, renal failure, etc.); and (c) acute traumatic coagulopathy, in which coagulopathy after trauma is common. Traditional teachings have been that this coagulopathy is not inherent, but rather iatrogenic, due to dilution from intravenous fluid therapy, massive blood transfusions, progressive hypothermia, and acidosis. Recent literature has now determined that an inherent acute traumatic coagulopathy is present in up to 30% of patients who present to the emergency department immediately following trauma and is an independent predictor of morbidity and mortality (318,319,320,321). Therefore, acute measurement of coagulation parameters during resuscitation from hemorrhagic shock is indicated.
Table 58.6 Transfusion guidelines for patients with coagulopathy and hemorrhage or traumatic injury
GOALS RECOMMENDED THERAPYHematologic/coagulation parameters Blood productsHemoglobin/hematocrit
Hgb >7.0 g/dL Hemodynamic stability
Packed red blood cells
Prothrombin time <1.5 times normal Fresh frozen plasma
Prothrombin complex concentrate
Activated partial prothrombin time <1.5 times normal Fresh frozen plasmaFibrinogen >100 g/dL CryoprecipitatePlatelets >50 × 109 per liter (stable, nonbleeding patient)Platelets >100 × 109 per liter (acute, bleeding patient)
Platelet transfusion
Traditional studies of coagulation include prothrombin time (PT), activated partial thromboplastin time (aPTT), fibrinogen level, and platelet count. Although no tightly controlled trials have been performed, current recommendations for therapeutic end points in hemorrhagic shock include maintaining PT and aPTT at less than 1.5 times the normal value, maintaining a platelet count of >100 in patients with active bleeding or traumatic brain injury, and maintaining a fibrinogen level of >1 g/L (229,322,323) (Table 58.6).While these laboratory studies are standard, they do present several drawbacks. To begin, in vivo coagulation depends on the interaction between platelets and coagulation factor enzymes. Laboratory values of PT and aPTT are performed on platelet-poor plasma and fail to evaluate the cellular interactions of clotting. PT and aPTT measurements also do not take into account hypothermia-induced coagulopathy because samples are warmed prior to measurement. Platelet and fibrinogen assays give numerical values, but fail to assess function. Finally, each of these tests takes time, up to 30 to 45 minutes. This lag time makes these studies clinically inefficient because when the results become available, they may not truly reflect the patient's clinical condition. During resuscitation, actively bleeding patients are in a constant state of flux. Alternative point-of-care testing such as the iSTAT handheld analyzer can provide rapid bedside results, but is currently limited to activated clotting time (ACT) and PT/international normalized ratio (INR) (250). The clinical implications of acute trauma coagulopathy and clinical testing are discussed further later in this chapter.Thromboelastograph AnalyzerThe thromboelastograph (TEG) analyzer is a bedside machine that provides a functional evaluation of overall coagulation on whole blood at the same temperature as the patient. The TEG has been shown to be a more sensitive measure of coagulation disorders than standard coagulation measures (324). The thromboelastograph assay provides a tracing that measures clotting (R value), clot formation (α angle), clot strength (maximum amplitude [MA]), and clot lysis (LY 30) (Fig. 58.5). Elongation of the R value represents a deficiency in coagulation factors. The α angle P.908represents the rate of fibrin accumulation and cross-linking, which can be affected by fibrinogen function and, to a lesser degree, platelet function. The MA is a measure of clot strength and is affected primarily by platelets and, to a lesser degree, fibrinogen. A study investigating the utility of the TEG in trauma patients found that 65% of patients were hypercoagulable and 10% were hypocoagulable. Of the seven hypocoagulable patients, only one had an elevated PT and PTT, but six of seven required blood transfusion (325). Only the Injury Severity Score (ISS) and TEG were predictive of early transfusion.
Figure 58.5. Thromboelastogram. The thromboelastograph (TEG) analyzer is a bedside machine that provides a functional evaluation of overall coagulation on whole blood at the same temperature as the patient. The thromboelastograph assay provides a tracing that measures time to clot formation (R value), speed to a certain clot strength (K value), rate of clot formation (α angle), overall clot strength (maximum amplitude [MA]) and clot lysis (LY 30).A large volume of literature exists describing the use of the TEG in various settings including trauma, transplant, and cardiac surgery (250,325,326,327,328,329,330). However, despite its many advantages, the TEG has not become the standard of care for measurement of coagulopathy. Using the TEG, whole blood samples must be run within 3 to 4 minutes of collection, necessitating the presence of multiple machines in critical areas of the hospital. Quality control of each of these
machines is work intensive. Differences due to age, gender, blood collection sites, and sample stability have been raised (331,332,333,334,335,336). Finally, accurate readings require appropriate processing, and intensive ongoing education of hospital staff would be necessary to ensure accurate results. Although the real-time functional results of routine TEG analysis would be clinically useful, the current processing and maintenance requirements make it impractical for routine use.Rapid Definitive Control of BleedingMultiple studies have confirmed that patients in need of emergency surgery for ongoing hemorrhage have a better survival if the elapsed time to definitive care is minimized (337,338,339,340,341,342,343,344,345,346,347). Those patients with unnecessary delays in diagnosis and definitive treatment will have increased morbidity and mortality (344). Although there are no prospective randomized trials confirming this, multiple retrospective studies provide ample data to confirm the validity of this strategy. In trauma, early surgical control of hemorrhage has been associated with improved survival in penetrating vascular injuries (337), duodenal injuries (338), and polytrauma patients in extremis (339). A multicenter retrospective review of over 500 deaths in the operating room concluded that delayed transfer to the operating room was a cause of death that could be avoided by shortening the time to diagnosis and resuscitation (348). Similar results have been documented in the treatment of patients with ruptured abdominal aortic aneurysms who are hemodynamically unstable (345,346,347). The benefit for rapid transport time to the operating room is not as dramatic for patients who are hemodynamically stable following ruptured abdominal aortic aneurysm (AAA), implying that ongoing hemorrhage has been arrested in this group of patients.The development of trauma systems has significantly contributed to improved trauma outcomes by triaging more severely injured patients to hospitals that have systems in place to rapidly diagnose, resuscitate, and definitively treat patients with hemorrhagic shock (340,341,342,343). The implementation of trauma systems has resulted in improved outcomes in severely injured patients, decreased time to operating room in hypotensive patients, decreased complications, decreased hospital length of stay, and decreased mortality, especially in patients with severe injury as measured by an ISS of >15 (343). Definitive prompt care is critical to optimize outcomes in patients with trauma and hemorrhage.Lethal Triad of Resuscitation: Hypothermia, Acidosis, and CoagulopathyPatients with severe hemorrhagic shock requiring massive resuscitation are at risk for exhaustion of their physiologic reserves, leading to irreversible shock and the inability to recover despite ongoing resuscitation. The common denominator in these patients is the development of the “lethal triad,” “bloody vicious cycle,” or “spiral of death”—terms used to describe the combination of profound acidosis, hypothermia, and coagulopathy (Fig. 58.6). Each of these factors has been independently associated with increased risk of death P.909(268,303,319,349,350,351,352,353,354). There also seems to be a cumulative synergistic effect for each of these risk factors in patients with hemorrhagic shock. In one retrospective study of 39 patients with abdominal packing for surgically uncontrollable bleeding (351), five risk factors for death were identified: pH <7.18, temperature ≤33°C, PT ≥16, PTT ≥50, and transfusion greater than 10 units of blood. Patients with zero to one risk factor had an 18% mortality, two to three risk factors 83% mortality, and four to five risk factors 100% mortality. Similar findings were reported by Cosgriff et al., who identified risk factors for the development of life-threatening coagulopathy (352). Patients with an ISS of >25, pH <7.1, temperature less than 34°C, and systolic blood pressure ≤70 mm Hg had a 98% chance of developing life-threatening coagulopathy, whereas patients with none of these risk factors had a 1% chance of developing coagulopathy.
Figure 58.6. Lethal triad of hemorrhagic shock. The development of acidosis, hypothermia, and coagulopathy during resuscitation from hemorrhagic shock is described as the “lethal triad,” “bloody vicious cycle,” or “spiral of death.” Each of these factors has been independently associated with mortality. There is a cumulative synergistic effect for each of these variables, such
that irreversible shock may develop if all factors are present.The development of profound acidosis, hypothermia, and coagulopathy is a lethal combination in patients during the resuscitation from hemorrhagic shock. Resuscitation strategies should be designed at limiting the development of these complications.Damage Control LaparotomyDamage control laparotomy (355) is a concept that was initially introduced by Pringle in 1908 when he described the use of hepatic sutures over packs to control bleeding. In 1913, Halsted detailed the procedure and modified its techniques. During World War II, damage control laparotomy fell out of favor and was not reintroduced until 1955 when Madding et al. reported the use of packs to temporize intraoperative bleeding, but felt that they needed to be removed prior to abdominal closure. In the 1970s, Ledgerwood had successful case reports using abdominal packing to control bleeding following trauma. However, the modern era of damage control laparotomy is attributed to Stone et al. who, in 1983, described the techniques of abbreviated laparotomy, packing to control hemorrhage, and deferred definitive surgical repair of injuries until coagulation had been established (356). Since then, a number of authors have described the beneficial effects of damage control laparotomy (357,358,359,360,361,362,363,364,365,366). Although retrospective, studies have documented a nearly 50% decrease in operative times for the most severely injured patients treated by this approach and salvage rates of 20% to 60% in patients who would have formerly died in the operating room (351,353,358,367).The principle of damage control surgery is to obtain rapid control of hemorrhage and contamination, with early completion of the operation, with a goal to restore normal physiology as opposed to normal anatomy (Table 58.7). The ultimate goal is to prevent patients from exhausting their physiologic reserves by developing the “lethal triad of death,” or profound hypothermia, acidosis, and coagulopathy. Damage control surgery has three basic components. First, an abbreviated laparotomy for control of bleeding, control of contamination, and restitution of blood flow are necessary. The goal is to achieve these end points as quickly as possible without spending unnecessary time on traditional organ repairs that can be performed at a later time. The abdomen is packed and a temporary abdominal closure is performed (Fig. 58.7). The second component involves treatment in the intensive care unit that is focused on core rewarming, correction of acidosis, and reversal of coagulopathy, as well as optimizing ventilation and P.910hemodynamic status. This phase will typically last for 24 to 48 hours. The third component is definitive surgical repair that is performed only when target parameters have been achieved. This sequence may require several operative interventions to attain definitive repair, each with a goal of preserving the physiologic reserve of the patient.
Table 58.7 Damage control laparotomy and damage control resuscitationDAMAGE CONTROL LAPAROTOMY
1. Abbreviated laparotomy (initial procedure) Control of bleeding Control of contamination Restitution of blood flow
2. Resuscitation in the intensive care unit (24–48 h) Core rewarming Correction of acidosis Reversal of coagulopathy Optimization of ventilation and hemodynamics
3. Definitive surgical repair (days to weeks) Restoration of continuity Completion of resection Removal of packs Closure of abdomen
DAMAGE CONTROL RESUSCITATION
Hypotensive resuscitationa Hemostatic resuscitation
aHypotensive resuscitation is still considered experimental and requires experienced physician oversight and careful patient selection.
Figure 58.7. Open abdomen with temporary abdominal closure. A key component to damage control laparotomy is to perform an abbreviated laparotomy for control of bleeding, control of contamination, and restitution of blood flow. The goal is to achieve these end points as quickly as possible to avoid the development of irreversible shock and the lethal triad of acidosis, hypothermia, and coagulopathy. Frequently, the abdomen is temporarily closed and the fascia left open to prevent the development of abdominal compartment syndrome during resuscitation. Re-exploration usually takes place 24 to 48 hours later, and every few days thereafter until the fascia is closed. Occasionally, the fascia cannot be reapproximated due to loss of domain. In this circumstance, a ventral hernia remains, which can be repaired at a later date (usually 6–12 months postinjury).Damage Control ResuscitationDamage control resuscitation (DCR) is a term that has recently been coined to describe a specific strategy during the resuscitation phase of trauma care (250,368,369). It should be initiated within minutes of presentation and is meant to preemptively address issues associated with resuscitating critically injured patients: prevention of hypothermia, acidosis, and coagulopathy. Damage control resuscitation involves two components: hypotensive resuscitation and hemostatic resuscitation (Table 58.7).Hypotensive ResuscitationHypotensive resuscitation refers to the concept that fluid should be administered at a rate that returns the systolic blood pressure to a safe but lower than normal pressure until operative control of bleeding can be established. The traditional treatment of hemorrhaging patients has used early and aggressive fluid administration to restore blood volume. However, this approach may increase hydrostatic pressure on the wound or injured vessel, leading to dislodgement of blood clots, a dilution of coagulation factors, and undesirable cooling of the patient. Low-volume fluid resuscitation, or “permissive hypotension,” may avoid the adverse effects of early aggressive resuscitation while maintaining a level of tissue perfusion adequate for short periods. This strategy has been suggested historically for the management of ruptured abdominal aortic aneurysm patients (370), and has recently regained attention in the trauma population (263,264,265,266,371,372,373,374,375). It has shown promise in animal and human trials (263,265), but has yet to be confirmed in large-scale prospective randomized human clinical trials. Overall, data have been mixed (264). A recent animal trial suggests that increases in blood pressure are well tolerated without exacerbating hemorrhage when they are achieved gradually and with a significant delay following the injury (376). Finally, a recent Cochrane Database review found that there was not conclusive evidence from randomized controlled trials for or against early or larger volumes of intravenous fluid resuscitation in uncontrolled hemorrhage (377).Although the concept of permissive hypotension seems promising in some circumstances, further work needs to be done. In addition, it requires extraordinarily tight control by an experienced physician who is guiding fluid resuscitation moment to moment. Hypotensive resuscitation should not be considered in patients with traumatic brain injury and spinal cord injury where adequate cerebral perfusion pressure is crucial to ensure tissue oxygenation (229,375). It should also be carefully considered in elderly patients and may be contraindicated in patients with a history of chronic hypertension (229). At the present time, it is considered experimental, and should be employed only in specific circumstances with experienced physicians.Hemostatic Resuscitation
Conventional resuscitation practice for damage control has focused on rapid reversal of acidosis and prevention of hypothermia. Surgical techniques are aimed at controlling hemorrhage and contamination rapidly, with definitive repair occurring following hemodynamic stabilization. However, direct treatment of coagulopathy early has been relatively neglected, and has been viewed as a byproduct of resuscitation, hemodilution, and hypothermia. Delay in availability of blood products due to current blood banking techniques has also hindered the ability to employ immediate resuscitation with clotting factors.It has now been demonstrated that acute traumatic coagulopathy is present in 25% to 30% of critically injured patients on arrival to the emergency department (318,319,320,321). The presence of coagulopathy may be even higher in patients with severe closed head injury, with an incidence of 21% to 79% when stratified by ISS (378). It has also been shown that the presence of early coagulopathy is an independent predictor of mortality following trauma (319). Early acute traumatic coagulopathy appears to be due to alterations in the thrombomodulin–protein C pathway rather than consumption of coagulation factors (321); however, additional work needs to be done to clarify these mechanisms.Hemostatic resuscitation employs blood components early in the resuscitation process to restore both perfusion and normal coagulation function while minimizing crystalloid use. Lactated Ringer solution and normal saline resuscitation have been shown to increase reperfusion injury and leukocyte adhesion (252,253,254,255,256,379). As such, standard crystalloid resuscitation may worsen, presenting acidosis and coagulopathy in severely injured patients. Several retrospective studies in trauma have shown that survival is associated with an increased use of clotting factors (352,367). Many other studies have recommended more aggressive use of clotting factors to treat and correct underlying coagulopathy (380,381,382,383,384,385,386,387,388).Although additional prospective studies need to be completed, there seems to be increased literature supporting early aggressive resuscitation with clotting factors while minimizing crystalloid use during massive resuscitation. Current military experience has moved to using thawed plasma as the primary resuscitation fluid in at least a 1:1 or 1:2 ratio with packed red blood cells (368,387,388,389). Continued resuscitation occurs with a massive transfusion protocol at a ratio of 6 units of plasma, 6 units of packed red blood cells, 6 units of platelets, and 10 units of cryoprecipitate. Recombinant factor VIIa is occasionally used along with early red cell transfusion to promote early hemostasis (368,389).Massive TransfusionDefinitionIn the 1970s, massive transfusion was defined as greater than 10 units of blood transfused in a 24-hour period of time, and survival rates were dismal (6.6%) (390). Over the last two decades, however, survival rates have improved, and the criteria to define massive transfusion have evolved (367,383,384,391,392,393,394,395,396). Recent reports use variable end points, increasing the number of transfusions to greater than 20 units in 24 hours (383) or defining transfusions during the entire hospital stay P.911(392). Most recently, investigators have reported outcomes on patients receiving over 50 units of blood in 48 hours (367).
Table 58.8 Survival following massive transfusion No. of Transfusion volumeOverallStudy/year patients(avg. units) survival (%)Wilson et al., 1971 (390) 45 >25 7Phillips et al., 1987 (383) 56 35 39Kivioja et al., 1991 (391) 29 56 38Wudel et al., 1991 (392) 92 33 52Harvey et al., 1995 (384) 43 19 60Velmahos et al., 1998 (393) 141 31 31Cinat et al., 1999 (367) 46 63 45
Hakala et al., 1999 (394) 23 79 69Vaslef et al., 2002 (395) 44 75 43Huber-Wagner et al., 2007 (396)
148 41 40
SurvivalAs technology and blood banking procedures have improved, patient outcomes following massive transfusion have also improved (397). Although early survival rates were dismal, recent reviews report survival rates as high as 60% in patients requiring over 50 units of blood in the early resuscitation period (Table 58.8). Moreover, many of these patients can ultimately return to work (75% of survivors), and survival in elderly patients has also been reported in several studies (367,392,394,395). This dramatic improvement in survival over the past several decades can be attributed to many factors including an improved understanding of the consequences of massive resuscitation (268,349,352), improved technology for massive resuscitation (i.e., rapid transfusion with warmed fluids) (267), increased use of damage control techniques (353,367), improved trauma systems (343), improved transfusion practices during resuscitation (367), and improved blood banking techniques (367). Based on these results, massive transfusion in trauma patients receiving over 50 units of blood in the acute period following injury is justified, with acceptable survival and functional capacity following discharge (367,383,384,391,392,393,394,395,396,397).Transfusion ProtocolsHistorically, massive transfusion protocols have been developed to assist clinicians in the resuscitation of hemorrhaging patients. However, a recent review of massive transfusion protocols globally revealed wide variation in practice (389). Most protocols recommend empiric strategies of 1 unit of fresh frozen plasma (FFP) for every 4 to 10 units of packed red blood cells (PRBCs) and 1 plateletpheresis for every 10 to 20 units of PRBCs (380). Organizational guidelines recommended transfusing to laboratory end points (322). However, recent literature suggests that a more aggressive approach is warranted (368,380,387,388). During ongoing hemorrhage, the clinical situation of the patient changes too rapidly to depend on laboratory values sent 20 to 45 minutes prior. Thus, empiric strategies to correct or avoid coagulopathy need to be employed. These strategies need to be modified for two clinical conditions: (a) ongoing hemorrhage and (b) coagulopathy following hemorrhage control.Resuscitation during Ongoing HemorrhageRecent data have established that a significant number of patients have an acute traumatic coagulopathy on presentation to the emergency department immediately following injury. Moreover, it appears that traditional strategies for resuscitation have been inadequate and unable to reverse this coagulopathy early following trauma (387). Several retrospective clinical studies suggest that aggressive early transfusion of clotting factors (fresh frozen plasma, platelets, and cryoprecipitate) is associated with increased survival (352,367,380,385,388).Randomized prospective controlled trials evaluating therapy for massive hemorrhage are challenging. However, recently two studies utilizing computer modeling have suggested that more aggressive resuscitation is necessary to correct coagulopathy. In the first study, the optimal replacement ratios were 2:3 of FFP to PRBCs and 8:10 of platelets to PRBCs (398). Interestingly, a second computer model found similar results, suggesting a transfusion rate of 1:1 for FFP per unit of blood transfused if there is no pre-existing coagulopathy, and a ratio of 1.5 units of FFP per unit of PRBCs if coagulopathy exists on presentation (399). Moreover, both of these mathematical models underestimate the potential need for clotting factor replacement because only dilutional coagulopathy is taken into account; there is no assessment for the relative contributions of consumption, acidosis, and hypothermia, which are frequently seen in the acute trauma patient.Based on these data, old transfusion strategies appear to be fundamentally flawed in the acutely hemorrhaging patient. Current recommendations suggest that, in patients with ongoing hemorrhage, empiric transfusion should occur in the ratio of 1:1:1 (1 unit of fresh frozen plasma to 1 unit of packed red blood cells to 1 unit of platelets) (Table 58.9) (368,380,387,388). Since platelets are usually supplied pooled as 6 to 10 units or as a plateletpheresis, which is equivalent to 6 to 10 units,

patients should receive a platelet transfusion for every 6 to 10 units of PRBCs. When blood products are available, crystalloids should be avoided in the acutely hemorrhaging patients as they can worsen coagulopathy.It is important to note that while this is the recommended transfusion protocol for patients with traumatic injury and hemorrhage, it is unclear if the same blood products and clotting factors are necessary in nontrauma patients with acute hemorrhage (i.e., intra-operative, gastrointestinal, ruptured aneurysm) (322,400,401,402,403). In blood loss during elective P.912surgery, the situation is more controlled and resuscitation can be initiated immediately. A premorbid coagulopathy may or may not exist. Goals in resuscitation in this circumstance are similar: maintain adequate tissue perfusion to avoid acidosis, correct coagulopathy, and prevent hypothermia.Table 58.9 Recommended empiric massive transfusion protocol for acute ongoing hemorrhageCURRENT SUGGESTED PROTOCOL FOR TRAUMATIC HEMORRHAGE
6 units packed red blood cells 6 units of fresh frozen plasma 1 plateletpheresis (or 6–10 units of platelets) Cryoprecipitate as indicated
TRADITIONAL PROTOCOL–INADEQUATE FOR TRAUMA
10–20 units packed red blood cells 1–4 units fresh frozen plasma 1 plateletpheresis Cryoprecipitate as indicated
Resuscitation Once Hemorrhage Is ControlledOnce hemorrhage is controlled, goal-directed transfusion can be pursued based on laboratory data and clinical variables. Many clinicians will work to achieve normal coagulation parameters for 24 hours post injury and control of hemorrhage (PT INR <1.5, platelet count >100 × 109 per liter) (387). In a patient who no longer shows evidence of medical or surgical bleeding, traditional guidelines for transfusion therapy can be employed (322). These include using red blood cell transfusion for symptomatic anemia or a hemoglobin concentration of less than 7 g/dL; FFP or prothrombin complex concentrate for a prothrombin time >1.5 times normal; fresh frozen plasma for an activated partial thromboplastin time >1.5 times normal; cryoprecipitate for a fibrinogen level <80 to 100 mg/dL; and platelet transfusion for a platelet count <50 × 109 per liter (Table 58.6).Complications of Massive TransfusionDespite acceptable survival rates, there are several known complications to massive transfusion (Tables 58.10 and 58.11) (397,404,405,406,407,408,409). Physicians caring for patients who require massive transfusion must anticipate, identify, and rapidly treat these potential complications in order to optimize outcome.Disordered hemostasis following massive transfusion is a known complication of massive blood transfusion (397,400,401). Stored blood is lacking in factors V and VIII. These factors degrade over time in stored blood, and thus become deficient in the massively transfused patient. This can contribute to the coagulopathy seen following massive transfusion. Dilutional thrombocytopenia also occurs during massive transfusion, and is more common after 1.5 times the normal blood volume is transfused. However, thrombocytopenia can occur earlier, especially if there is disseminated intravascular coagulation, pre-existing thrombocytopenia, or a consumptive coagulopathy. As discussed previously, resuscitation of hemorrhagic shock must include clotting factors and platelets to avoid ongoing coagulopathy.Table 58.10 Noninfectious transfusion-associated complicationsACUTE (WITHIN 24 H OF TRANSFUSION)
Hemolytic reactionsFebrile nonhemolytic reactionsAllergic reactionsTransfusion-related acute lung injury (TRALI)HypothermiaHypocalcemiaHypo- or hyperkalemiaAcid-base derangementsDELAYED (MORE THAN 24 H AFTER TRANSFUSION)AlloimmunizationImmunosuppressionPosttransfusion purpuraGraft vs. host diseaseMultiple organ dysfunction syndromeOxygen delivery to tissues is also affected by blood transfusion. Transfused blood tends to have a higher affinity for oxygen, thus leading to decreased oxygen delivery to tissues. Longer storage periods for blood lead to a reduction in red cell deformability, altered red cell adhesiveness, and other red cell storage lesions. These changes reduce red blood cell viability after transfusion, reduce tissue oxygen availability, and promote the inflammatory response, specifically neutrophil priming and pulmonary endothelial cell activation.Systemic inflammation and potential tissue injury may also be induced by the transfusion of aged blood. Transfusion of aged blood (>14 days of storage) in the first 6 hours of resuscitation has been shown to be an independent risk factor for postinjury multiorgan failure (410) and is associated with
P.913delayed apoptosis of neutrophils (411), increased infection rates (412), and a longer ICU stay (413). This may be particularly significant in large trauma centers and transplantation centers where older blood is preferentially distributed because of their high-volume use.
Table 58.11 Infectious transfusion-associated complicationsType of infectious Incidence per allcomplication transfused componentsBacterial contamination (PRBCs + platelets) 1 per 2,000Hepatitis B transmission 1 per 205,000PRBC-related bacterial sepsis 1 per 500,000–786,000Hepatitis A transmission 1 per 1,000,000Hepatitis C transmission 1 per 1,600,000HIV transmission 1 per 2,135,000PRBC, packed red blood cell; HIV, human immunodeficiency virus. Adapted with data from Silliman CC, Moore EE, Johnson JL, et al. Transfusion of the injured patient: proceed with caution. Shock. 2004;21(4):291; McIntyre LA, Hebert PC. Can we safely restrict transfusion in trauma patients? Curr Opin Crit Care. 2006;12:575; Dodd RY, Notari EP, Stramer SL. Current prevalence and incidence of infectious disease markers and estimated window-period risk in the American Red Cross donor population. Transfusion. 2002;42:975; and Kleinman S, Chan P, Robillard P. Risks associated with transfusion of cellular blood components in Canada. Transfus Med Rev. 2003;17:120.Alloimmunization can occur when an immunocompetent host develops an immune response to donor antigens. The antigens most often involved include the human leukocyte antigen (HLA) class I and II on platelets and leukocytes, granulocyte-specific antigens, platelet-specific antigens, and red blood cell–specific antigens. Consequences of alloimmunization include a refractory response to platelet transfusion, posttransfusion purpura, neonatal alloimmune thrombocytopenia, acute intravascular hemolytic transfusion reaction, hemolytic disease in newborns, and febrile nonhemolytic reactions against granulocytes. Clinical manifestations can be minor, such as fever,
leading to active bleeding and hemolysis, which can be fatal. Workup and treatment vary, depending on the severity of the reaction (414,415).Metabolic and electrolyte disturbances can also occur following massive transfusion (397). Citrate toxicity can occur in patients with abnormal liver function or in whom the administration of blood is very rapid. The healthy adult liver will metabolize 3 g of citrate every 5 minutes. Each unit of blood contains approximately 3 g of citrate. Therefore, transfusion rates higher than 1 unit every 5 minutes can exceed the liver's capacity to handle this overload. Citrate then binds to calcium and can lead to clinical hypocalcemia. Patients may exhibit temporary tetany and hypotension. Calcium replacement should occur concurrently during massive transfusion.Electrolyte disturbances such as hyperkalemia or hypokalemia can occur with massive transfusion. The longer the shelf life, the higher the potassium concentration; sometimes concentrations may even exceed 30 mmol/L. Unless very large amounts of blood are transfused, hyperkalemia is generally not a problem. On the other hand, as red cells begin active metabolism, intracellular uptake of potassium begins, and hypokalemia may result.Acid-base disturbances can also occur with massive blood transfusions. Stored blood contains lactate at levels up to 30 to 40 mmol/L. In addition, citric acid is present and may be metabolized to bicarbonate, resulting in severe metabolic alkalosis. Conversely, the patient's overall condition and tissue hypoperfusion may actually lead to metabolic acidosis.Although rare, blood transfusion can also result in the induction of acquired inhibitors of coagulation. The most common antibodies are directed against coagulation factor VIII. This can result in massive bleeding, which is difficult and costly to treat. The main goals of treatment are to stop hemorrhage and remove the inhibitor. Factor VIII concentrate is used only for life-threatening circumstances. Successful elimination of the anti-VIII antibody has been accomplished with the use of oral immunosuppressants such as cyclophosphamide and prednisone (416).Transfusion-related acute lung injuryTRALI is a devastating complication of transfusion that consists of a syndrome that includes dyspnea, hypotension, bilateral pulmonary edema, and fever. Its incidence is reported to be between 0.04% and 0.06% (or approximately 1 in 2,000). Clinically, it resembles acute respiratory distress syndrome. Criteria for the diagnosis of TRALI include:
Acute lung injury (ALI) as defined by acute onset, hypoxemia (PaO2: FiO2 ratio ≤300),
bilateral infiltrates on frontal chest radiograph, and no evidence of left atrial hypertension or circulatory overload
No pre-existing ALI before transfusion Occurs during or within 6 hours of transfusion No temporal relationship to an alternative risk factor for ALI (i.e., burns, aspiration, multiple
trauma, cardiopulmonary bypass, sepsis, etc.)
If an additional risk factor exists, then possible TRALI is diagnosed (Table 58.12) (417,418,419,420).The pathogenesis can be either immune (antibody) mediated or nonimmune mediated (Table 58.13) (418,419,420,421,422). Immune-mediated TRALI is most common and is due to the presence of leukocyte antibodies in the donor transfusion (421,422). These antibodies form immune complexes that are deposited in the pulmonary vascular bed, leading to release of vasoactive substances, leakage of fluid into alveolar spaces, activation of complement, leukostasis, and activation of polymorphonuclear neutrophils. Immune-mediated TRALI occurs more commonly with fresh frozen plasma than with platelet concentrates, is associated with multiparous female donors (423), can occur in healthy recipients, and is usually severe, requiring mechanical ventilation in 70% of individuals. Non–immune-mediated TRALI is thought to be due to the presence of biologically active lipids in the donor transfusion (418,419,420). It occurs with stored platelet concentrates more commonly than stored red cells, occurs predominantly in critically ill patients with a primed immune system, and is usually mild and transient, requiring only supplemental oxygen support. Treatment of TRALI is generally supportive and includes ventilatory and hemodynamic assistance.

There are no data to support the use of corticosteroids, and additional blood component therapy should be given only if transfusion needs exist. The diagnosis of TRALI in the patients requiring massive transfusion is P.914difficult because of the many other etiologies also present that can lead to acute lung injury (424,425).
Table 58.12 Criteria for transfusion-related acute lung injury (TRALI)CRITERIA FOR TRALI
Acute lung injury (ALI) Acute onset Hypoxemia
PaO2: FiO2 ratio ≤300
SpO2 <90% on room air
No pre-existing ALI before transfusion Occurs during or within 6 h of transfusion No temporal relationship to an alternative risk factor for ALI
CRITERIA FOR POSSIBLE TRALI
ALI No pre-existing ALI before transfusion Occurs during or within 6 h of transfusion A clear temporal relationship to an alternative risk factor for ALI
Adapted from Kleinman S, Caulfield T, Chan P, et al. Toward an understanding of transfusion-related acute lung injury: statement of a consensus panel. Transfusion. 2004;44:1774.Table 58.13 Characteristics of immune and nonimmune transfusion-related acute lung injury
(TRALI) Immune TRALI Nonimmune TRALITrigger Leukocyte antibodies Biologically active lipidsBlood components implicated
Fresh frozen plasma > platelet concentrates
Stored platelet concentrates > stored red blood cells
Host Healthy or critically ill Predominantly in critically illClinical course Severe, often life threatening
Mechanical ventilationMild, self-limitingSupplemental oxygen
Adapted from Bux J. Transfusion-related acute lung injury (TRALI): a serious adverse event of blood transfusion. Vox Sang. 2005;89:1.Recombinant Factor VIIA in Massive Transfusion and HemorrhageNew developments in transfusion therapy include the discovery and use of recombinant coagulation factor VIIa (rFVIIa). Recombinant factor VIIa is a synthesized analog of human factor VII that has been used effectively in the treatment of patients with hemophilia as well as other congenital and acquired coagulopathies. Recently, there have been reports of the successful use of rFVIIa in treating coagulopathic trauma patients (426). In this study, patients with active hemorrhage and clinical coagulopathy from diverse causes such as traumatic hemorrhage, traumatic brain injury, warfarin use, congenital factor VII deficiency, and other acquired hematologic defects were administered rFVIIa as a last resort. Coagulopathy was reversed in 75% of patients, with an associated decrease in prothrombin time. Forty-two percent of patients survived to discharge.Recently, two randomized, prospective, placebo-controlled, double-blind clinical trials were conducted simultaneously to evaluate the efficacy and safety of recombinant factor VIIa as adjunctive therapy for the control of bleeding in patients with severe blunt (N = 143) or penetrating
(N = 134) trauma (427). In blunt trauma, the red blood cell transfusion requirement was significantly reduced by 2.6 units (p = 0.02) and the need for massive transfusion (>20 units of packed red blood cells) was reduced (14% vs. 33%, p = 0.03). In patients with penetrating trauma, the trends were similar, but not significant (reduction in red cell transfusion 1.0 unit, p = 0.10; massive transfusion 7% vs. 19%, p = 0.08). Trends toward reduction in mortality and critical complications were also observed. A subgroup analysis from this trial found particular benefit in those patients who were coagulopathic on presentation to the emergency department, with a significant decrease in transfusion of packed red blood cells, fresh frozen plasma, platelets, and need for massive transfusion. In addition, treatment with rFVIIa was also associated with a significant reduction in multiorgan failure and/or acute respiratory distress syndrome (3% vs. 20%, p = 0.004), without an increase in thromboembolic events (428).Recombinant factor VIIa, however, must be used responsibly. Recent studies have shown that early administration following trauma is more effective than late administration (429,430). Furthermore, the presence of profound acidosis, coagulopathy, and signs of irreversible hemorrhagic shock predict failure of rFVIIa therapy (431). Current recommendations suggest that optimal preconditions should be present prior to administration of rFVIIa, which include a fibrinogen concentration of >50 mg/dL, a platelet count of >50 × 109 per liter, and a pH ≥7.2 (432,433). Although early results in traumatic hemorrhage appear promising, rFVIIa should still be considered experimental and further investigation is warranted. Recombinant factor VIIa has shown promise for perioperative bleeding during liver transplantation (434) and in patients undergoing cardiac surgery (435,436). Investigations for its utility in perioperative bleeding for other surgical procedures have been mixed (437,438,439,440,441,442).A prospective randomized trial investigating the use of rFVIIa in patients with cirrhosis and upper gastrointestinal bleeding who were treated with standard endoscopic therapy and pharmacologic interventions showed that the administration of rFVIIa was not more effective than placebo with respect to the primary end point of failure to control bleeding within 24 hours and failure to prevent rebleeding or death within 5 days (443). However, subgroup analysis of patients with more severe cirrhosis showed that rFVIIa showed a reduction in the composite primary end point (8% vs. 23%, p = 0.03). None of the rFVIIa patients had rebleeding within the first 24 hours, whereas rebleeding occurred in 11% of the placebo group (p = 0.01) (443).As with any hemostatic agent, there are concerns over the potential thrombogenicity of rFVIIa (444). Although preliminary evidence shows a favorable safety profile (445,446), thrombogenic effects are being followed closely in ongoing clinical trials.Prevention of Hemorrhagic ShockAntifibrinolytic TherapyAntifibrinolytic therapy has been shown to significantly reduce the risk of bleeding following cardiac surgery in several P.915randomized controlled trials. Aprotinin has been studied most extensively (447,448,449,450,451), followed by tranexamic acid, then aminocaproic acid. However, recent information raises concern for the risk of renal failure following use of aprotinin with cardiac surgery (448,449) and a potential for increased mortality at 5 years following use of aprotinin (450). Although clearly the risk of postoperative bleeding following cardiac surgery is reduced, further investigation into these potential side effects is warranted.A recent systematic review of randomized controlled trials of antifibrinolytic agents (mainly aprotinin or tranexamic acid) in elective surgical procedures identified 89 trials including 8,580 randomized patients (74 cardiac, eight orthopedic, four liver, three vascular). Results demonstrated that these treatments reduced the number of patients needing transfusion by one third, reduced the volume needed per patient by 1 unit, and halved the need for further surgery to control bleeding. These differences were all statistically significant. There was also a trend toward a reduction in the risk of death (risk ratio = 0.85; 95% confidence interval, 0.63–1.14), although this was not statistically significant (452).
To date, there are limited data on the use of antifibrinolytic agents in other clinical scenarios (453). However, at this time, the CRASH-2 trial (Clinical Randomization of an Anti-fibrinolytic in Significant Hemorrhage) is ongoing in Europe and is designed to evaluate the utility of antifibrinolytic agents in the management of acute traumatic injury (454).Experimental TherapyRed Cell SubstitutesAlthough the blood supply in the United States is safe and currently has sufficient capacity to meet most patient needs, there is room for considerable improvement. The current system is dependent on blood donors on a regular basis, and the blood supply is subject to seasonal shortages due to holidays and convenience. The gap between the donor pool and the increasing transfusion requirements of an aging population is narrowing, and shortages are becoming more frequent. The risk of transmission of known infectious diseases still exists (Table 58.11), while the threat of new and emerging infections such as West Nile virus and Creutzfeldt-Jakob disease underscore the risk of a tainted blood supply (455).The ideal red cell substitute should have several characteristics including an ability to deliver (and potentially enhance) oxygen delivery, no risk of disease transmission, no immunosuppressive effects, available in abundant supply, universally compatible, prolonged shelf life, similar in vivo half-life to the red blood cell, available at a reasonable cost, easy to administer, able to access all areas of the human body (including ischemic tissues), and effective at room air or ambient conditions (455,456,457). There have been many attempts to develop red cell substitutes since 1934 when Amberson first reported the successful use of a bovine hemolysate for exchange transfusions in cats and dogs (455). However, this work could not be replicated.The two main types of oxygen carriers that are used as red blood cell substitutes are hemoglobin-based oxygen carriers (HBOCs) and perfluorocarbons (PFCs). Based on previous clinical trials, many obstacles still need to be overcome. Adverse effects associated with HBOCs include (a) severe vasoconstriction due to binding of nitric oxide and dysregulation of endothelin; (b) nephrotoxicity; (c) interference of macrophage function; (d) antigenicity; (e) oxidation on storage; (f) activation of complement, kinin, and coagulation; (g) iron deposition with concerns of hemochromatosis and iron overload; (h) gastrointestinal distress; (i) neurotoxicity; (j) free radical generation; and (k) interference with diagnosis of transfusion reaction. Adverse effects of PFCs include (a) limited shelf life, (b) flulike symptoms during infusion, (d) complement and phagocytic activation, and (d) short circulation time (456).Despite much research, no product to date has been able to fulfill all of the previously mentioned criteria or meet the U.S. Food and Drug Administration's requirements of purity, potency, and safety. At the time of this publication, three HBOC products continue in advanced clinical trials (455).Hypertonic SalineHypertonic saline (7.5% saline ± 6% dextan-70) has been investigated as an alternative resuscitation strategy in critically injured patients (458,459,460,461,462,463,464). Hypertonic resuscitation evokes an increase in serum osmolarity, which results in the redistribution of fluid from the interstitial and intracellular space to the intravascular space. This leads to a rapid restoration of circulating intravascular volume with a small amount resuscitation fluid. Hypertonic saline has also been shown to decrease intracranial pressure via its osmotic effects (125,126). This is particularly beneficial in patients with hypovolemic shock and closed head injury due to the ability of hypertonic saline resuscitation to concurrently restore circulating blood volume, improve tissue (including cerebral) perfusion, and lower intracranial pressure (126,465,466).Hypertonic saline resuscitation has also been shown to have significant immunomodulatory effects that could mitigate the dysfunctional inflammatory response seen after traumatic injury (108,109,111,150,253,467,468,469,470,471,472). The hypertonicity associated with hypertonic saline resuscitation is associated with significant effects on the innate and adaptive immune systems. There is suppression of the neutrophil oxidative burst, potentially leading to an attenuation of inflammatory organ injury (150,473).
Several clinical trials and meta-analyses have suggested improved outcome in patients resuscitated with hypertonic saline (474,475,476,477). Despite these results, hypertonic saline resuscitation has not gained widespread acceptance in North America. However, in 1999, the U.S. Navy, through the Office of Naval Research, requested that the Institute of Medicine (IOM) recommend that hypertonic saline be used as the initial resuscitation fluid for combat casualty (256,478). The rapid restoration of intravascular volume and possible immunomodulatory effects associated with hypertonic saline resuscitation make it an attractive alternative for the resuscitation of severe hemorrhagic shock. However, it is still considered experimental and prospective randomized trials are needed to confirm its utility.SummaryHemorrhagic shock is a common, yet complicated, clinical condition that physicians are frequently called upon to evaluate and treat. Diagnosis must be accurate and expedient. Therapy must be direct, efficient, and multifactorial in order to avoid P.916the potential multisystem sequelae. Metabolism and function of all organs are altered during hemorrhagic shock. A better understanding of the pathophysiology of hemorrhagic shock has led to improved resuscitation techniques and improved survival over recent years. Damage control laparotomy and damage control resuscitation have changed the approach to management in patients with multisystem trauma and hemorrhagic shock. Staged resuscitation and operative intervention to avoid irreversible shock are now the mainstays of care. Recognition of acute traumatic coagulopathy has improved the composition of massive transfusion protocols to include increased use of clotting factors early during resuscitation. New experimental therapies for resuscitation are being evaluated and appear promising. Overall, survival following hemorrhagic shock has improved. Early diagnosis, definitive cessation of bleeding, and comprehensive hemostatic resuscitation are the key elements to successful outcome.
Chapter 59Neurogenic ShockSusanne MuehlschlegelDavid M. GreerNeurologically injured patients, regardless of the nature of the injury, frequently experience hypotension and shock. Neurogenic shock refers to a neurologically mediated form of circulatory system failure that can occur with acute brain, spinal cord, or even peripheral nerve injuries. In this chapter, we will explain the epidemiology, pathophysiology, clinical presentation, and management strategies for this special form of shock.Contrary to common belief, neurogenic shock is not a single entity due to one single pathologic mechanism. The term is sometimes used in nonneuroscience intensive care units to explain hypotension occurring in any brain-injured patient, but neurogenic shock should be considered only after systemic causes of shock have been carefully ruled out. Just like other critically ill patients, neurologically ill patients are prone to developing systemic conditions, such as dehydration, congestive heart failure, acute blood loss, sepsis, pericardial tamponade, or massive pulmonary embolism.Subtypes of Neurogenic ShockOnce other systemic reasons for shock have been ruled out, neurogenic shock should be considered. Three mechanisms can lead to neurogenic shock (Fig. 59.1):
Vasodilatory (distributive) shock from autonomic disturbance with interruption of sympathetic pathways, with associated parasympathetic excitation, which causes profound vasodilatation and bradycardia, as seen in spinal cord injury or diseases of the peripheral nervous system (Guillain-Barré syndrome)
Cardiogenic shock, as frequently seen in subarachnoid hemorrhage (SAH) with stunned myocardium after a catecholamine surge or ischemic stroke, especially those involving the right insula
Hypopituitarism/adrenal insufficiency.
Although some subtypes of neurogenic shock occur more frequently with certain disease entities—for example, cardiogenic neurogenic shock after SAH, vasodilatory neurogenic shock with spinal cord injury—significant overlap exists between different disease entities (intracerebral hemorrhage [ICH], SAH, traumatic brain injury [TBI], ischemic stroke), and one cannot establish a firm rule by which neurogenic shock occurs. Interestingly, only some patients with neurologic injuries experience true neurogenic shock, and it remains difficult to predict in whom this will be seen.Incidence of Neurogenic ShockDue to the small number of prospective epidemiologic studies, it is difficult to establish the natural incidence of neurogenic shock. In a retrospective review of cervical spinal cord injuries, Bilello et al. (1) reported a 31% incidence of neurogenic shock with hypotension and bradycardia after high cervical spinal cord injury (C1–C5) and 24% after low cervical spinal cord injury (C6–C7).Cardiogenic neurogenic shock has been studied foremost in SAH and ischemic stroke. Banki et al. (2) prospectively studied the incidence of left ventricular (LV) dysfunction with transthoracic echocardiography (TTE) in the first 7-day period after SAH in 173 patients. Thirteen percent had a normal ejection fraction (EF) but had regional wall motion abnormalities that did not correlate with coronary artery territories, and 15% had an LVEF of less than 50%. Others report a 9% incidence of LV wall motion abnormalities, resulting in hypotension requiring vasopressor therapy, as well as pulmonary edema in most (80%) of these patients (3). The spectrum of injury can range from mild to severe systolic dysfunction—the latter defined as an EF less than 30%. Polick et al. (4) observed LV abnormalities on TTE in 4 of 13 patients (31%) studied within 48 hours of SAH. Resolution of these neurologically mediated wall motion abnormalities is usually seen (2,3,5).
The third subtype of neurogenic shock, adrenal insufficiency, has been studied primarily in traumatic brain injury. In the largest study to date, adrenal insufficiency occurred in about 50% of patients and led to hypotension in 26% (6). Although it has been documented in other cases of acute brain injury, the exact incidence and relationship to outcome is not clear (7).Pathophysiology of Neurogenic ShockVasodilatory Neurogenic ShockThis variation of neurogenic shock is commonly seen with spinal cord injuries and Guillain-Barré syndrome (acute demyelinating peripheral neuropathy) but also with traumatic brain injuries, large hemispheric ischemic strokes, and intracerebral hemorrhages. The hallmark of vasodilatory neurogenic shock is the combination of bradycardia with fluctuating blood pressures and heart rate variability due to interruption of sympathetic output and excitation of parasympathetic fibers.The sympathetic fibers originate in the hypothalamus, giving rise to neurons projecting to autonomic centers in the P.926brainstem—the periaqueductal gray matter in the midbrain, the parabrachial regions in the pons, and the intermediate reticular formation located in the ventrolateral medulla. From here, neurons project to nuclei in the spinal cord. The sympathetic preganglionic neurons originate in the intermediolateral cell column within the spinal cord gray matter between T1 and L2 and are therefore called the thoracolumbar branches. From here, they exit the spinal cord and project to 22 pairs of paravertebral sympathetic trunk ganglia next to the vertebral column. The main ganglia within the sympathetic trunk are the cervical and stellate ganglia. The adrenal medulla receives preganglionic fibers and thus is equivalent to a sympathetic ganglion. Blood pressure control depends on tonic activation of the sympathetic preganglionic neurons by descending input from the supraspinal structures (8).
Figure 59.1. Neurogenic shock consists of three pathomechanisms. CNS, central nervous system; CO, cardiac output; CVP, central venous pressure; PCWP, pulmonary capillary wedge pressure; SAH, subarachnoid hemorrhage; TBI, traumatic brain injury.The parasympathetic nervous system consists of cranial and sacral aspects. The cranial subdivision originates from the parasympathetic brainstem nuclei of cranial nerves III, VII, IX, X, and XI. The cranial parasympathetic neurons travel along the cranial nerves until they synapse in the parasympathetic ganglia in close proximity to the target organ. The sacral subdivision originates in the sacral spinal cord (S2–S4), forming the lateral intermediate gray zone where preganglionic neurons travel with the pelvic nerves to the inferior hypogastric plexus and synapse on parasympathetic ganglia within the target organs.Following a spinal cord injury, the sympathetic pathways are interrupted with dissociation of the sympathetic supply from higher control below the level of transection (9,10). Parasympathetic fibers are usually spared. This results in autonomic hyperreflexia with associated hypertension or hypotension with bradycardia, all observed in human studies as well as in animal models (10,11,12,13). Loss of supraspinal control of the sympathetic nervous system leads to unopposed vagal tone with relaxation of vascular smooth muscles below the level of the cord injury, resulting in decreased venous return, decreased cardiac output, hypotension, loss of diurnal fluctuations of blood pressure, reflex bradycardia, and peripheral adrenoreceptor hyperresponsiveness (14). The latter accounts for the excessive vasopressor response repeatedly seen in this clinical scenario. The acute phase, also known as spinal shock, more frequently consists of periods of hypotension. After the acute phase, starting about 2 months after the injury, autonomic dysreflexia occurs in patients with lesions above T5 (15). This state is characterized by sympathetically mediated vasoconstriction in muscular, skin, renal, and presumably gastrointestinal vascular beds, induced by afferent peripheral stimulation below the level of the lesion. For example, stimuli such as urinary catheterization, dressing changes, or surgical stimulation can lead to severe blood pressure spikes out of proportion to the stimulus. In Guillain-Barré syndrome, the autonomic dysregulation is likely caused by acute demyelination not only of sensory and motor fibers, but also of autonomic fibers.
Injury to the brain can also lead to vasodilatory neurogenic shock. Certain cerebral structures, such as the insular cortex, amygdala, lateral hypothalamus, and medulla, have great influence on the autonomic nervous system. Cortical asymmetry is present and is reflected in a higher incidence of tachycardia, ventricular arrhythmias, and hypertension with lesions of the right insula—resulting in loss of parasympathetic input and thus sympathetic predominance—and a higher incidence of bradycardia and hypotension with injuries to the left insula—resulting in a loss of sympathetic input and subsequent parasympathetic predominance (16,17,18) (Fig. 59.2).Cardiogenic Neurogenic ShockThis form of neurogenic shock is primarily encountered in SAH and TBI but is also seen in ischemic stroke and intracerebral hemorrhage. Cardiac dysfunction is a well-known complication of ischemic and hemorrhagic stroke, first described over 50 years ago (19). It is most often recognized on the electrocardiogram (ECG) as arrhythmias, QRS, ST-segment, and P.927T-wave abnormalities (20,21). Studies of SAH and cardiac injury have shown that the severity of SAH is an independent predictor of cardiac injury, supporting the hypothesis that cardiac neurogenic shock is a neurally mediated process (22). Based on the similarities observed between pheochromocytoma crisis and SAH, the cardiovascular changes have been linked to a catecholamine surge.
Figure 59.2. Example of a right ischemic stroke resulting in ventricular arrhythmias and cardiogenic shock. A 61-year-old man presents with sudden onset of left hemiparesis affecting his face and arm, left-sided neglect, and a left hemianopia. He presented outside of any acute treatment window and did not undergo thrombolysis. He was admitted to the neurointensive care unit (NICU) for close monitoring of his cardiac and respiratory function. The noncontrast head CT shows a right middle cerebral artery stroke and incidental hemorrhagic conversion. Electrocardiogram on admission showed diffuse T-wave inversion in all leads. Telemetry monitoring revealed frequent premature ventricular complexes and intermittent nonsustained ventricular tachycardia of 4 to 8 beats for the first 72 hours after stroke onset. His systolic blood pressure on admission was elevated at 190 mm Hg but then dropped to 85 mm Hg several hours after admission to the NICU, requiring vasopressor support for 2 days. Troponin T levels were elevated in the emergency room and peaked at 12 hours after stroke onset. Echocardiogram showed global hypokinesis and no regional wall motion abnormalities. No other causes for shock were found, so that the stroke involving the right insula was the most likely cause. The shock slowly resolved over 72 hours, and vasopressor infusion was weaned off successfully. A repeat echocardiogram 2 weeks later showed resolution of the abnormalities.This hypothesis has been confirmed by many studies. Patients with SAH can have a threefold increase in norepinephrine levels that are sustained for 10 days or longer after SAH but that normalize after the acute phase of injury (23). In an animal model, an increase in plasma catecholamines after experimental SAH causes specific lesions on electron microscopy within 4 hours of SAH (24). Selective myocardial cell necrosis, also known as contraction band necrosis, is the hallmark of catecholamine exposure (25,26,27). The same lesions can be found in patients with pheochromocytoma (28) and SAH (29), underlining the pathologic mechanism of cardiac injury in SAH or other neurologic injuries (Fig. 59.3). The cardiac dysfunction is not related to coronary atherosclerosis, as normal coronary arteries have been documented in these patients studied at autopsy or by coronary angiography (5,29,30,31). In fact, it appears that pre-existing heart disease, such as hypertensive heart disease, might even be protective of this form of neurogenic shock (32). In a case series of 54 consecutive SAH deaths, 42 had myocardial lesions consisting of foci of necrotic muscle fibers, hemorrhages, and inflammatory cells, none of which were found in the control group. Patients with a wider range of heart rate and blood pressure fluctuations were more likely to have myocardial lesions. Pre-existing hypertensive heart disease led to significantly fewer myocardial lesions, possibly reflecting a decreased sensitivity of these patients to the catecholamine surge (32).
Figure 59.3. Contraction band necrosis. Histologic examination of the myocardium, showing contraction band necrosis, see arrow. (Courtesy of Dr. James R. Stone, M.D., Ph.D., Department of Pathology, Massachusetts General Hospital, Boston, MA.)Pathologic studies link the central catecholamine release to the posterior hypothalamus. Postmortem studies have found microscopic hypothalamic lesions consisting of small hemorrhages and infarctions in those patients with typical myocardial lesions as noted above (29,32,33,34). However, it appears that raised intracranial pressure (ICP) is not responsible for these hypothalamic changes, as the control group with elevated ICP did not have any hypothalamic injury (32).Overall, by the described pathomechanism, the catecholamine surge results in direct myocardial injury resulting in decreased inotropy, and in addition an increase in cardiac preload due to venous constriction and increased cardiac afterload by peripheral arterial constriction. As a consequence, stroke volume diminishes, which cannot be compensated for by reflex tachycardia, thus resulting in decreased cardiac output and shock. This transient LV dysfunction with loss of myocardial compliance (stunning of the myocardium) is reflected by a characteristic shape of the cardiac silhouette on a ventriculogram and on chest radiograph, which has given this disease P.928entity its other name, Takotsubo cardiomyopathy, derived from the Japanese word for the Japanese octopus fishing pot, tako-tsubo (35,36,37) (Fig. 59.4).
Figure 59.4. Takotsubo cardiomyopathy. A: Japanese octopus fishing pot. B: CT brain of a 47-year-old woman with subarachnoid hemorrhage (SAH). C: Chest x-ray view of the same patient with typical cardiac silhouette of Takotsubo cardiomyopathy. An echocardiogram revealed an ejection fraction of 29 degrees with apical ballooning, global hypokinesis, and sparing of the apex. The chest radiograph and echocardiogram became normal within 1 week after her SAH.Pulmonary edema with concomitant hypoxia is frequently encountered in this context and may result from cardiac congestion but can occur independently from the cardiac dysfunction as its own entity: neurogenic pulmonary edema. Massive increases in pulmonary capillary pressures lead to pulmonary edema and hypoxia, which in turn decreases the uptake of oxygen in a high demand state, contributing to hemodynamic instability. The Vietnam war era head injury series (38) reported the rapid onset of acute pulmonary edema after severe head injury. In addition, experimental models as well as multiple human case reports of TBI and SAH have shown massive P.929sympathetic discharges as the primary cause of neurogenic pulmonary edema (39,40,41). Figure 59.5 summarizes the pathophysiology of cardiogenic neurogenic shock.
Figure 59.5. Summary of the pathophysiology of the cardiogenic type of neurogenic shock. ICH, intracerebral hemorrhage; LVEF, left ventricular ejection fraction; SAH, subarachnoid hemorrhage; TBI, traumatic brain injury.Overall, cardiac neurogenic shock, with or without neurogenic pulmonary edema, is usually transient, with resolution within several days to 2 weeks (2,3,4). Prevention of secondary brain injury from hypoxia and decreased cerebral perfusion pressures should be the focus of care in the management of this neurally mediated complication.Neuroendocrine Neurogenic ShockInsufficiency of the hypothalamic-pituitary-adrenal axis has been recognized as an important cause for shock. Inappropriately reduced release of cortisol in stress situations can lead to decreased systemic vascular resistance, reduced cardiac contractility, hypovolemic shock, or hyperdynamic shock that can mimic septic shock. Secondary adrenal insufficiency due to injury to the hypothalamic-hypopituitary feedback loop can cause neuroendocrine neurogenic shock. Acute brain injury, particularly TBI and SAH, can commonly lead to injury of the hypothalamus, pituitary gland, or the connecting structures (42). Cohan et al. (6) revealed that adrenal insufficiency after traumatic brain injury occurred in about half of all patients and led to a significantly higher rate of
hypotension in these patients. Most cases of adrenal insufficiency developed within 4 days of injury. Importantly, the authors defined adrenal insufficiency using a low random serum cortisol value and highlight the fact that an increase in the cortisol level after a stimulation test does not rule out the presence of adrenal insufficiency. This issue is particularly relevant in TBI patients, in whom the hypothalamus and the pituitary gland are the likely affected organs, and the adrenal glands might well be expected to mount an appropriate response when stimulated. When recognized, primary and secondary adrenal insufficiency can easily be treated.In septic shock, a low-dose vasopressin infusion has been shown to successfully restore blood pressure in hypotension refractory to standard catecholamine therapy (43,44). Recent studies in SAH have shown that endogenous vasopressin serum levels are elevated during the first 2 days after SAH but decrease to subnormal levels after 4 days (45,46,47). Arginine vasopressin supplementation in SAH at low dose (0.01–0.04 units/min) has been studied in only one single retrospective study (48). The role of vasopressin in the setting of neurogenic shock remains to be studied in a prospective manner, but the changes in endogenous vasopressin levels might indicate neuroendocrine changes in neurogenic shock and potential new treatment options in SAH.Clinical ManifestationsFigure 59.6 illustrates the clinical manifestations and symptoms seen in neurogenic shock. Acutely, vasodilatory neurogenic shock presents with a “warm and dry” hemodynamic profile. The patient is hypotensive and frequently bradycardic; however, the peripheral vessels are dilated, leading to warm limbs and a normal capillary refill time. Central venous pressure (CVP) is normal or low, and systemic venous resistance (SVR) is always low. Stroke volume and cardiac output are low due to the unopposed vagal tone. When a spinal cord injury is present, a difference in smooth muscle and vasculature tone can be observed between the body parts above and below the level of the injury. For example, in an injury at thoracic level 7 (T7), normal upper limb perfusion might be observed, while vasodilatation below T7 leads to warm and dry lower extremities. Orthostatic hypotension without reflex tachycardia on changing from a supine to an upright position—by standing P.930or with reverse Trendelenburg position—is common. When treating this form of neurogenic shock with a vasopressor infusion (such as phenylephrine or other pressors), extreme caution should be applied, as vasopressor hypersensitivity can lead to severe rebound hypertension, which can be difficult to control.
Figure 59.6. Clinical manifestations of the different types of neurogenic shock. CO, carbon monoxide; CVP, central venous pressure; EDVI, end-diastolic volume index; PCWP, pulmonary capillary wedge pressure; SV, stroke volume; SVR, systemic vascular resistance.Cardiogenic neurogenic shock manifests as hypotension and tachycardia, with bradycardia seen rarely. Peripheral vessels are often vasoconstricted, leading to a high SVR and cold and wet skin. Vascular filling, as measured by CVP, pulmonary capillary wedge pressure (PCWP), and end-diastolic volume index (EDVI), is normal or high, with low stroke volumes and cardiac output due to global myocardial dysfunction. Leaking of cardiac enzymes—troponin, creatine kinase (CK), CK-MB—may be seen, but frequently the peak levels are not as high as one would find in myocardial infarction. It is difficult to establish a cutoff value that differentiates stunned myocardium from myocardial infarction with atherosclerotic coronary artery disease. A retrospective study in SAH measuring troponin-I levels has reported an appropriate cutoff value to be 2.8 ng/mL (49), whereas CK-MB did not help differentiate between the two kinds of myocardial injury. Higher levels of troponin should raise the suspicion of true myocardial infarction, and ECG and echocardiography correlation is important.Neuroendocrine neurogenic shock presents with hypotension that does not respond well to vasopressor infusion. Hemodynamic signs of this category of neurogenic shock are low CVP, SVR, stroke volume, and cardiac output. Low baseline cortisol levels are the hallmark. A cosyntropin stimulation test frequently leads to an appropriate increase in the cortisol level, which does not rule out the presence of neuroendocrine neurogenic shock, as the adrenal gland is usually not the
primarily affected organ (6). For this reason, we do not find any clinical utility in this test when neuroendocrine neurogenic shock is suspected. Resolution of the hypotension with the use of hydrocortisone clinically confirms the presence of this shock form.Diagnostic ConsiderationsIn any case of hypotension and shock in the neurointensive care unit, systemic causes for shock must be ruled out first. Especially in the paralyzed patient (for example, one with a high spinal cord injury), recognition of other life-threatening injuries can be quite difficult. Signs of hypovolemic shock may be absent, even in a patient with profound internal bleeding, because of the absence of sympathetic tone below the level of injury. The usual pallor from vasoconstriction and reflex tachycardia might also be absent. The patient may even be bradycardic while continuing to bleed. For the same reason, signs of peritoneal irritation may be absent in patients with abdominal injuries. The reported incidence of pulmonary embolism (PE) varies tremendously in the neurocritical care patient population—ranging from 0.5% to 20% in ischemic stroke (50,51), to 1% in intracranial hemorrhage (52), to 8.4% in brain tumors (53)—and there are only limited data during the acute phase of subarachnoid hemorrhage, traumatic brain injury, and spinal cord injury (51). Interestingly, according to the study by Skaf et al. (50) using the National Hospital Discharge Survey, the incidence of PE did not change in patients with ischemic and hemorrhagic stroke between 1979 and 2003. However, the death rate from PE in the subgroup with ischemic stroke decreased, likely due to an increased use of antithrombotic prophylaxis over the last 20 years (54). Additionally, over the last two decades, the methods of PE detection have improved immensely—for example, pulmonary CT-angiogram versus nucleotide scan—and autopsy studies report additional asymptomatic cases. In our opinion, the true incidence of PE is underestimated. Pulmonary embolism should always be considered in cases of refractory shock. If profound hypotension is present, or hypotension becomes progressive, reasons other than neurogenic shock should be suspected and thoroughly ruled out.P.931Every patient should undergo serial ECGs, serial cardiac enzyme measurements, and a chest radiograph. As previously mentioned, pulmonary edema and neurocardiogenic injury may occur together or separately, making chest x-ray films important diagnostic tools. In particular, one should look for pulmonary vascular congestion and evaluate the size and shape of the cardiac silhouette. Hemodynamic monitoring with continuous blood pressure and central venous pressure (CVP) monitoring with an arterial line and central venous line (CVL) should be undertaken. Blood pressure measurements should be done continuously with an arterial line. Arteriosclerosis of the upper extremities is common and should be kept in mind either when there is a large discrepancy between right- and left-sided pressures or when the clinical appearance of the patient does not match the readings from the arterial line. Central venous access is key for determining CVP and for the administration of fluids and medications, especially vasopressors. The site of the placement of the central venous line (CVL) may play an important role in the management of shock in a neurologically injured patient. Subclavian vein catheters are the preferred site in patients with elevated intracranial pressure (ICP), as there is a theoretical risk of venous stasis within the internal jugular vein with venous congestion and higher risk for venous sinus thrombosis, which could result in increased ICP (55). In addition, trauma patients frequently have cervical spine injuries and require cervical collars, making the internal jugular vein accessible only with difficulty.In patients with cardiogenic neurogenic shock, more extensive hemodynamic monitoring may be necessary with either noninvasive cardiac monitoring devices or a pulmonary artery catheter (PAC). Echocardiography is very important to understanding the etiology of shock. In most cases, a transthoracic echocardiogram is sufficient. The typical echocardiographic appearance is that of apical ballooning, which results from global hypokinesis sparing the apex (56). This part of the heart is devoid of sympathetic nerve terminals, supporting the hypothesis that cardiac injury in SAH is neurally mediated by a sympathetic storm. Segmental wall motion abnormalities not conforming to distinct coronary artery territories is another characteristic echocardiographic finding. However, myocardial infarction from ischemic coronary disease is frequently seen in brain-injured patients, just as in any critically ill patient, and should always be ruled out first as a cause of shock. In the
setting of fever and shock, blood cultures must be obtained and the patient appropriately covered with antibiotics until the cultures yield results. However, older and immunosuppressed patients may not mount an appropriate febrile response, and thus sepsis should still be considered in these patients even when they are afebrile, especially in the setting of a rising white blood cell (WBC) count. Cerebral spinal fluid cultures are very important in the neurointensive care unit, with antibiotic coverage of potential central nervous system CNS infections, especially in patients after head trauma with skull fracture or sinus disease, after instrumentation of the head or spinal canal, or in immunocompromised patients. Placement of intracranial pressure measurement devices do not contribute to the diagnostic workup of shock, but they are important tools in the management of neurogenic shock, such as when the goal mean arterial pressure (MAP) is being titrated to the cerebral perfusion pressure. Finally, adrenal insufficiency should always be considered. Random serum cortisol levels should be obtained in the early stages of shock, keeping in mind that in some forms of brain injury, low random serum cortisol levels, and thus adrenal insufficiency, may be encountered for several days after injury (6).Many neurologically injured patients, especially those with spinal cord injuries, receive steroids while in the neurointensive care unit. The doses administered may be high enough to alter the result of a random serum cortisol level, but often the dose is not enough to treat true adrenal insufficiency appropriately. In these cases, one could either empirically treat with higher doses of steroids that also treat adrenal insufficiency—hydrocortisone, with or without fludrocortisone—or, keeping the potential adverse effects of steroids in acute injury in mind, one could withhold the administration of steroids for 12 hours, then obtain a random cortisol level and resume steroid treatment right after the blood draw. However, hypotension is frequently severe enough that immediate treatment is warranted, and withholding steroids often is not an option. Dexamethasone, which is frequently used in the neurointensive care unit, is the steroid that interferes the least with the cortisol assay after a corticotropin stimulation test and therefore allows for such a test. In cases of high suspicion, a random cortisol level is often preferred because of its simplicity. The cortisol level should be drawn immediately before the steroid dose. However, given the lack of mineralocorticoid activity of dexamethasone, changing to hydrocortisone with or without fludrocortisone is recommended when adrenal insufficiency is suspected.ManagementTwo important reasons for early and proactive treatment of patients in neurogenic shock are as follows:
Prevention of secondary brain injury from hypoxia and hypotension The fact that neurogenic shock, especially cardiogenic and neuroendocrine forms, is easily
treatable and transient, with potentially good outcomes despite the moribund appearance of the patient in the acute phase.
Identifying patients at risk has been very difficult, but at least in SAH it appears that poor neurologic grade, age older than 30 years, and ventricular repolarization abnormalities are risk factors for neurogenic shock (57).Once the diagnosis of neurogenic shock has been established and the pathophysiology (subtype) has been understood, treatment tailored to the specific subtype is initiated. In all cases, euvolemia is of utmost importance and must be achieved before any other treatment can be successful. In general, vasopressor treatment as a continuous infusion is initiated and titrated to a goal MAP and cerebral perfusion pressure (CPP). As an important management tool, an intracranial pressure measurement device is very helpful, allowing the indirect measurement of CPP. We recommend a goal CPP of greater than or equal to 65 mm Hg. The optimal CPP is not known. Data regarding the minimum tolerable CPP comes from TBI patients, in whom the ICP is often elevated. Several studies have suggested an improved outcome when CPP is maintained at greater than 70 mm Hg (58,59). Other studies using physiologic measurements, such as cerebral blood flow and brain tissue PO2 (PbtO2),
indicate that adverse changes do not occur unless the CPP is below 50 to 60 mm Hg (60,61).
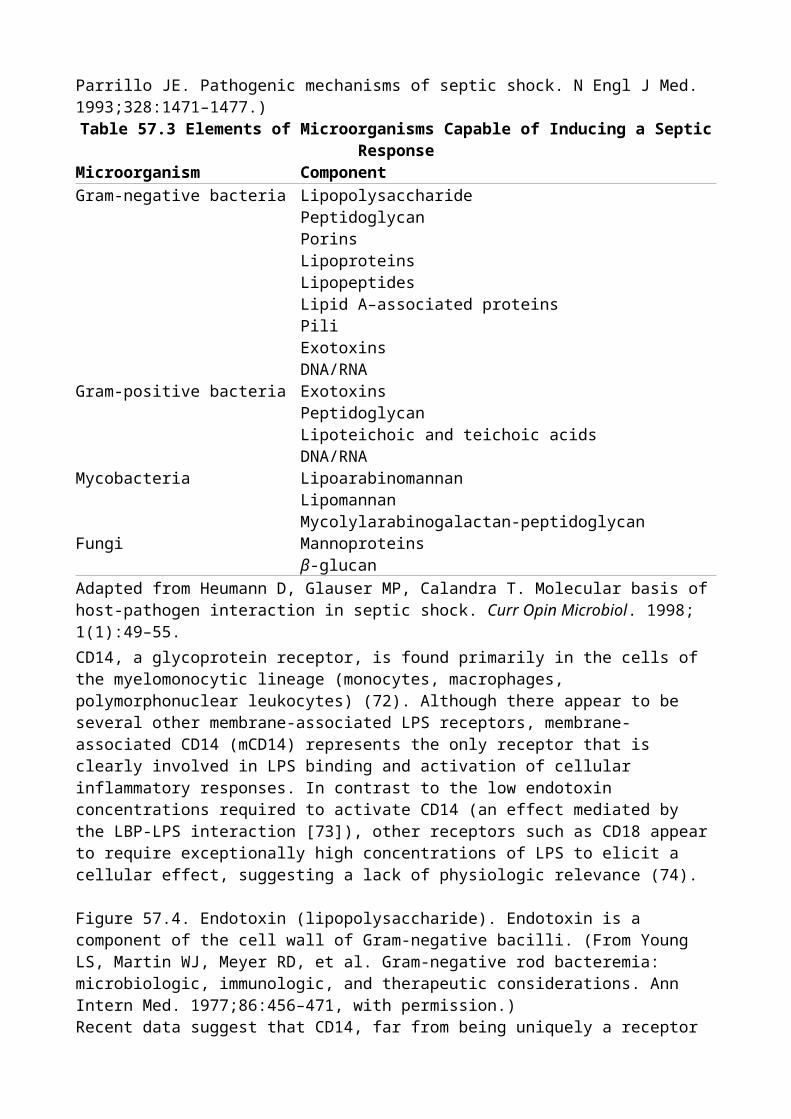
Vasodilatory neurogenic shock can be difficult to treat. In general, vagal tone predominates; however, in this state, P.932patients frequently have peripheral α-adrenoceptor hyperresponsiveness, limiting the use of norepinephrine, epinephrine, ephedrine, and phenylephrine. In fact, sympathomimetics should be avoided as they can lead to severe blood pressure fluctuations. Since arginine vasopressin (AVP) does not affect α- or β-adrenergic receptors, but acts on V1 receptors, AVP may have an advantage over catecholamines or phenylephrine in this form of neurogenic shock. It has not been studied in neurogenic shock, however, and it remains unclear whether AVP may have adverse effects on neurologically ill patients. This concern is based on animal studies indicating that vasopressin may promote the development of vasospasm in SAH, and indirect experimental studies showing a reduction in brain edema with vasopressin antagonists. No prospective human study has been undertaken to confirm or dismiss this concern, and the only retrospective study on the use of vasopressin in SAH did not show any of these potentially adverse effects (48). In addition to vasopressors, a temporary demand pacemaker and/or atropine may be required in cases of refractory bradycardia and hypotension.In cardiogenic neurogenic shock, some form of inotropic support may be necessary, either in the form of a dobutamine, milrinone, or norepinephrine infusion. Dopamine is generally avoided because of its proarrhythmic properties. Dobutamine and milrinone also have vasodilatory effects, frequently leading to more hypotension, requiring additional therapy with an α-receptor agonist, such as phenylephrine or norepinephrine. Afterload increases in the former, and tachycardia in the latter, might be limiting factors and need careful monitoring. Cardiac output monitoring may be undertaken with the guidance of a PAC. Beta-blockade is usually not recommended. In neurogenic cardiogenic shock, coronary artery disease is typically not present, and compensatory tachycardia is necessary to maintain cardiac output. Afterload reduction with cautious use of angiotensin-converting enzyme (ACE) inhibitors should be attempted, but further hypotension must be avoided to maintain tenuous cerebral perfusion pressures. Short-acting agents should be used whenever possible. Repeating an echocardiogram several days after the initial one is recommended to monitor the progression/resolution of cardiac dysfunction. The need for an intra-aortic balloon pump to mechanically reduce afterload and improve coronary perfusion pressure may be considered, albeit rarely used.Once diagnosed, neuroendocrine neurogenic shock from primary, or more often secondary, adrenal insufficiency is treated with steroid replacement therapy. We use the same dosing as in adrenal insufficiency in septic shock: hydrocortisone, 50 mg intravenously every 6 hours. As previously discussed, a cortisol stimulation test is usually not helpful, and empiric treatment after a random cortisol level should be initiated.SummaryNeurogenic shock is not a single entity, but rather is composed of three subtypes and pathophysiologies: vasodilatory, cardiac, and neuroendocrine. Other causes of hypotension should be ruled out first, prior to making the diagnosis of neurogenic shock. In most cases, neurogenic shock is transient and reversible, making this entity very treatable. Diagnosis and treatment should be tailored to the subtype of neurogenic shock. Maintenance of cerebral perfusion pressures is the key principle of management to prevent secondary brain injury and improve outcome.
Chapter 60Anaphylactic ShockMeghavi S. KosbothEric S. SobelAnaphylaxis is severe, has a rapid onset, and is potentially fatal—a systemic allergic reaction that occurs after contact with an allergy-causing substance (1,2). Activation of mast cell and basophil populations by either IgE-dependent (i.e., anaphylactic reactions) or IgE-independent (i.e., anaphylactoid reactions) mechanisms results in the release of multiple mediators capable of altering vascular permeability and vascular and bronchial smooth muscle tone, as well as recruiting and activating inflammatory cell cascades. Because the clinical presentations of anaphylactic and anaphylactoid reactions are indistinguishable, they will be referred to as anaphylaxis for the purposes of this chapter. Initial sequelae, which occur within minutes to an hour after exposure to an inciting stimulus, include generalized hives, tachycardia, flushing, pruritus, faintness, and a sensation of impending doom. Dermatologic (i.e., urticaria and angioedema), respiratory (i.e., dyspnea, wheeze, stridor, bronchospasm, and hypoxemia), and gastrointestinal (i.e., abdominal distension, nausea, emesis, and diarrhea) manifestations are common. Involvement of the cardiovascular and respiratory systems may result in potentially life-threatening manifestations, such as cardiovascular collapse caused by vasodilation and capillary leak, myocardial depression, myocardial ischemia and infarction, and atrial fibrillation (3). Prompt recognition and effective intervention are essential to prevent the fatal manifestations of anaphylactic and anaphylactoid reactions.P.934IncidenceThe incidence of anaphylaxis is difficult to determine accurately due to underdiagnosis and underreporting. In the United States, fatal anaphylaxis causes 500 to 1,000 fatalities per year and accounts for 1% of emergency department visits (1,4,5). The anaphylaxis rate was found to be 21 per 100,000 person-years in a study of nonhospitalized individuals in Olmsted County, Minnesota, between 1983 and 1987 (6). A subsequent analysis of the General Practice database in the United Kingdom noted the incidence to be 8.4 per 100,000 person-years (7). An epidemiologic study involving 481,752 individuals suggested that hospitalized patients are at increased risk of anaphylaxis, but these reactions are rarely fatal (8).EtiologyThe most common causes of anaphylaxis include insect stings, foods, drugs, and physical factors/exercise. Idiopathic anaphylaxis (where no causative agent is identified) accounts for up to two thirds of patients referred to allergy/immunology specialty clinics (9,10). Foods such as shellfish, eggs, nuts, and milk account for one third of food-induced anaphylactic episodes (10,11,12,13) (Tables 60.1 and 60.2). There is a syndrome of food-dependent, exercise-induced anaphylaxis (FDEIA) that develops only if food is ingested prior to exercise or exertion (14). Seafood, nuts, celery, wheat, and grains have been implicated as allergens in this syndrome. It is important to note that these foods are tolerated by the patient in the absence of exertion (14,15).Anaphylactic reactions to stings or bites of various insects, such as members of the order Hymenoptera (yellow jackets, bees, wasps, hornets, and saw flies) are commonly reported. A positive venom skin test along with a systemic reaction to the insect sting predicts a 50% to 60% risk of reaction to future stings (16). Medications can cause anaphylactic (IgE-mediated) and anaphylactoid (non–IgE-mediated) reactions. Previous exposure to drugs is required for IgE production and anaphylactic reactions, but anaphylactoid reactions can occur upon first administration. Penicillin is one of the most common causes of anaphylaxis, with 1 to 5 per 10,000 courses with penicillin resulting in allergic reactions and 1 in 50,000 to 1 in 100,000 courses with a
fatal outcome (17,18,19). Nonsteroidal anti-inflammatory drugs (NSAIDs) and aspirin are the second most common class of drugs implicated in anaphylaxis (20). Some hypersensitivity reactions will occur with different NSAID agents, while others are specific to a single drug (21).With widespread adoption of universal precautions against infections, latex allergy has become a significant problem. The development of low-protein, powder-free gloves has been associated with reduction in occupational-contact urticaria caused by latex rubber gloves (22). Despite this, latex allergy is still a concern since latex is found in gloves, catheters, and tubing (23,24,25). Iodinated radiocontrast media can cause anaphylaxis; however, life-threatening reactions are rare (26). A history of a previous reaction to radiocontrast media, asthma or atopic disease, treatment with β-blockers, and cardiovascular disease are risk factors for developing anaphylaxis to radiocontrast media (27,28,29).Clinical ManifestationsThe clinical syndromes associated with systemic anaphylactic and anaphylactoid reactions represent medical emergencies, as they are associated with a rapid, critical destabilization of vital organ systems. These syndromes, which are, again, clinically indistinguishable, may become rapidly fatal if appropriate therapy is not instituted immediately. Initial symptoms can appear within seconds to minutes but may be delayed by as much as 1 (or rarely more) hour after exposure to an inciting agent (30), and are often nonspecific (31). These symptoms include tachycardia, faintness, cutaneous flushing, urticaria, diffuse or palmar pruritus, and a sensation of impending doom (32). Of these, generalized urticaria is the most common, occurring in approximately 90% of patients (Table 60.3) (33,34). Subsequent manifestations indicate involvement of the cutaneous, gastrointestinal, respiratory, and cardiovascular systems. Involvement of the cardiovascular and respiratory systems is responsible for the fatal P.935complications of anaphylactic/anaphylactoid reactions. An unsettling sensation—including hoarseness, dysphonia, or dyspnea—may precede acute upper airway obstruction secondary to laryngeal edema. Other pulmonary manifestations include acute bronchospasm, intra-alveolar pulmonary hemorrhage, bronchorrhea, and a noncardiogenic, high permeability–type pulmonary edema (17,35). Tachycardia and syncope may precede the development of hypotension and frank cardiovascular collapse (36,37). Anaphylactic shock occurs as a consequence of diminished venous return secondary to systemic vasodilation and intravascular volume contraction caused by capillary leak. Although transient increases in cardiac output may occur at the onset of anaphylaxis, hemodynamic parameters later reveal decreases in cardiac output, systemic vascular resistance, stroke volume, pulmonary artery occlusion, and central venous pressures (38,39,40,41,42,43,44). In addition, the acute onset of a lactic acidosis and diminished oxygen consumption have been noticed after an anaphylactoid reaction (45). Other potentially serious cardiovascular manifestations are myocardial ischemia and acute myocardial infarction, atrioventricular and intraventricular conduction abnormalities such as prolonged PR interval, transient left bundle branch block, and supraventricular arrhythmias such as atrial fibrillation. Severe, but reversible, myocardial depression also has been reported (37). Hematologic manifestations, such as disseminated intravascular coagulation and hemoconcentration secondary to volume contraction, also may complicate anaphylactic and anaphylactoid reactions (32). Gastrointestinal manifestations include nausea, bloating, abdominal cramps, and diarrhea.
Table 60.1 Etiologic agents for anaphylaxis (IgE-mediated)HAPTENSβ-Lactam antibioticsSulfonamidesNitrofurantoinDemethylchlortetracyclineStreptomycinVancomycinLocal anesthetics
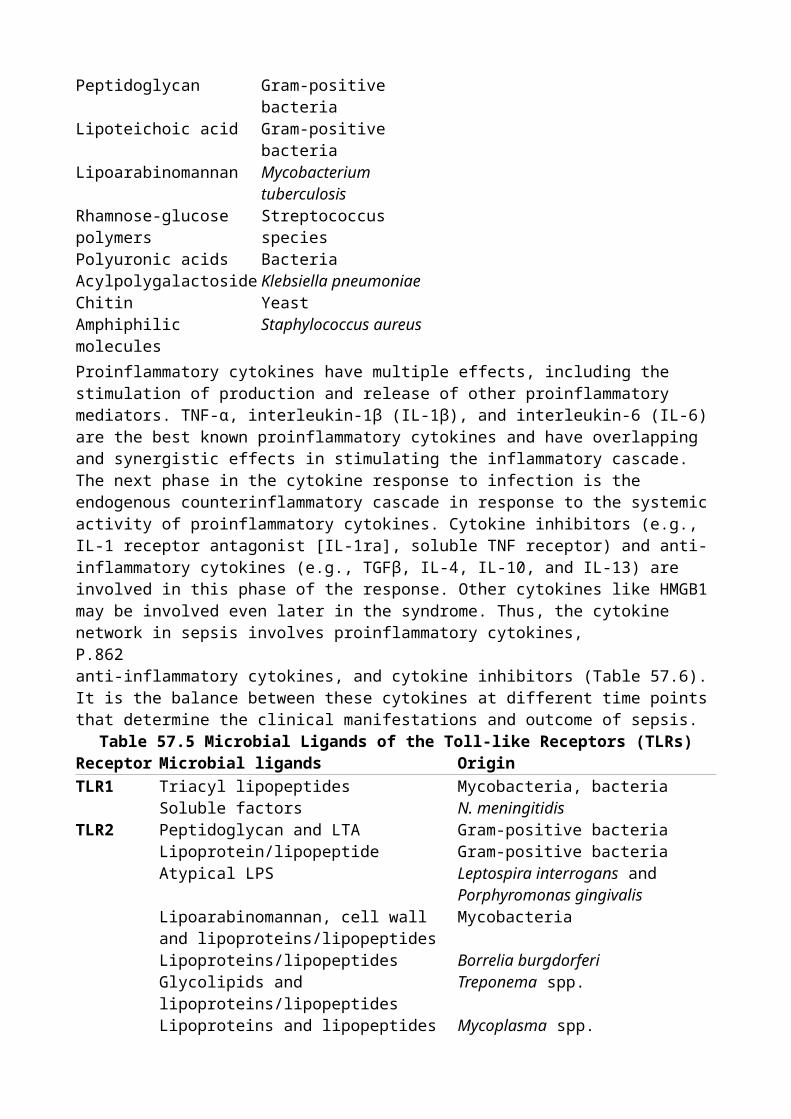
OthersSERUM PRODUCTSγ-GlobulinImmunotherapy for allergic diseasesHeterologous serumFOODSNuts (peanuts, brazil nuts, hazelnuts, cashews, pistachios, almonds, soy nuts)ShellfishBuckwheatEgg whiteCottonseedCow's milkCornPotatoRiceLegumesCitrus fruitsChocolateOthersVENOMStinging insects, particularly Hymenoptera, fire ants, deer flies, jelly fish, kissing bugs (triatoma), and rattlesnakesHORMONESInsulinAdrenocorticotropic hormoneThyroid-stimulating hormoneENZYMESChymopapainL-AsparaginaseMISCELLANEOUSSeminal fluidOthersBoldface: Relatively common causesModified from Austen KF. Systemic anaphylaxis in man. JAMA. 1965;192:108; and Kaliner M. Anaphylaxis. NER Allergy Proc. 1984;5:324.
Table 60.2 Etiologic agents for anaphylactoid reactionsCOMPLEMENT-MEDIATED REACTIONS ARACHIDONIC ACID MODULATORSBlood Nonsteroidal anti-inflammatory drugsSerum Tartrazine (possible)Plasma Plasmate (but not albumin) IDIOPATHICImmunoglobins Most common conclusion after thorough
evaluationNONIMMUNOLOGIC MAST CELL ACTIVATORS
UNKNOWN
Opiates and narcotics SulfitesRadiocontrast media OthersDextrans Neuromuscular blocking agents THERMOREGULATORY MECHANISM Cold temperature, exerciseBoldface: Relatively common causes.Adapted from Kaliner M. Anaphylaxis. NER Allergy Proc. 1984;5:324.
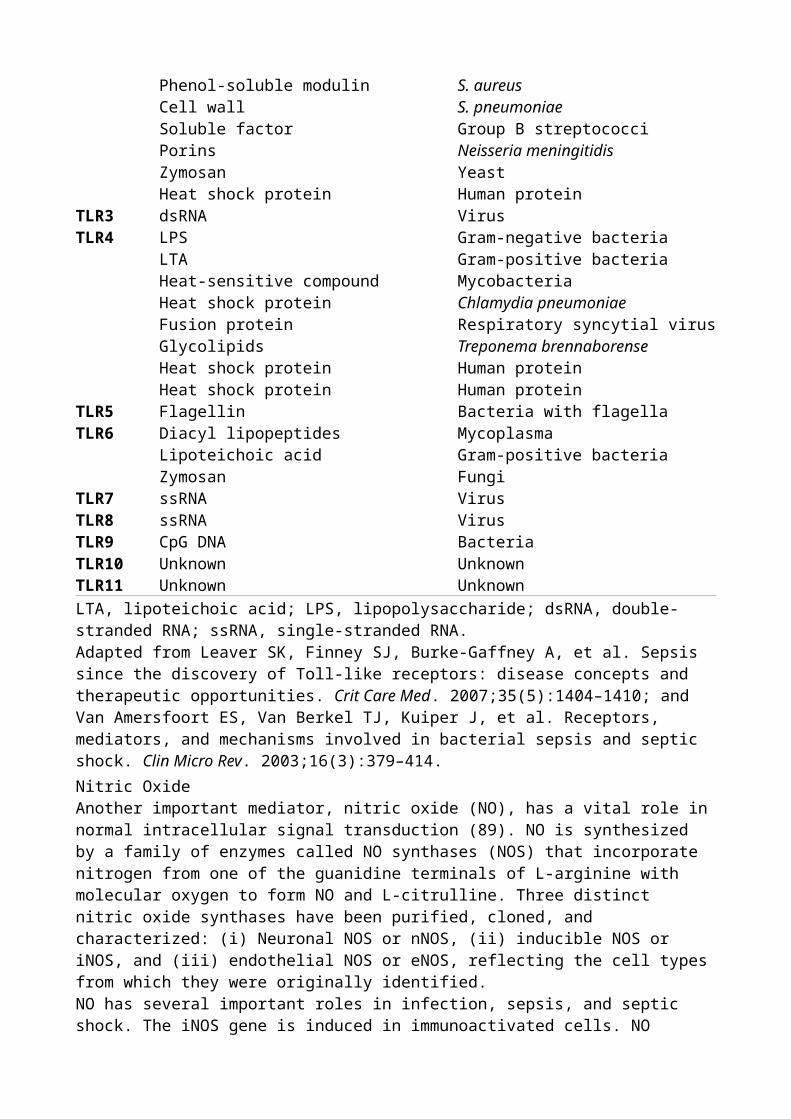
Table 60.3 Clinical manifestations of anaphylactic and anaphylactoid reactionsSystem Symptom FrequencySign/clinical manifestationRESPIRATORY 60%–80% Upper Dyspnea, dysphonia,
cough, “lump in throat”
Upper airway obstruction caused by laryngeal edema and spasm; bronchorrhea
Lower Dyspnea, cyanosis Noncardiogenic pulmonary edema, bronchospasm, acute hyperinflation, alveolar hemorrhage
CARDIOVASCULAR Palpitations, faintness, weakness
20% Shock, tachycardia, capillary leak, syncope, supraventricular arrhythmias, conduction disturbances, myocardial ischemia and infarction
CUTANEOUS Flushing, pruritus, rash 90% Urticaria, angioedema, diaphoresisGASTROINTESTINALAbdominal pain,
bloating, cramps, nausea
30% Emesis, diarrhea, hepatosplenic congestion; rarely hematemesis and bloody diarrhea
NEUROLOGIC Dizziness, disorientation, hallucinations, headache, feeling of impending doom
5%–10% Syncope, lethargy, seizures
NASAL Pruritus, sneezing 16%–20% Rhinorrhea, nasal congestionOCULAR Conjunctival pruritus,
periorbital edema10%–15% Conjunctival suffusion, lacrimation
HEMATOLOGIC Hemoconcentration, DICDIC, disseminated intravascular coagulation.In 1% to 20% of patients, there is a recurrence of symptoms after a period of recovery, termed biphasic anaphylaxis (46). In most cases, the symptoms recurred 1 to 8 hours after the initial P.936presentation, although there have been reports of recurrence up to 72 hours later. There were no features of the primary response that predicted the occurrence of a secondary response (47).DiagnosisThe diagnosis of anaphylaxis is established on the basis of clinical grounds alone because expedient institution of appropriate therapy is mandatory. These diagnoses should be considered when typical multisystem manifestations occur in a direct temporal relationship with exposure to an inciting agent. Recently, the National Institute of Allergy and Infectious Diseases (NIAID) and the Food Allergy and Anaphylaxis Network (FAAN) proposed clinical criteria for the diagnosis of anaphylaxis (Fig. 60.1) (1). Because of the multisystem nature of anaphylactic and anaphylactoid reactions, the list of differential diagnoses that must be considered is extensive. Diagnostic possibilities include cardiac dysrhythmias, myocardial infarction, distributive or hypovolemic shock, vasovagal syncope, asthma, pulmonary embolism, upper airway obstruction secondary to ingestion of a foreign body, hypoglycemia, and the carcinoid syndrome (Table 60.4).Demonstration of acute elevations of markers specific to mast cell activation such as histamine and tryptase have been proposed to help confirm the diagnosis of anaphylaxis (48,49). However, in a series of 97 patients presenting to an emergency department and given the diagnosis of anaphylaxis, only 42% were found to have elevated plasma histamine levels, and 24% had increased plasma tryptase levels (50). Skin testing or serum antibody tests can help demonstrate the presence of IgE against a specific allergen. Skin testing should be delayed for up to 4 weeks to allow the dermal mast cells to replenish intracellular mediators (51).Pathophysiology
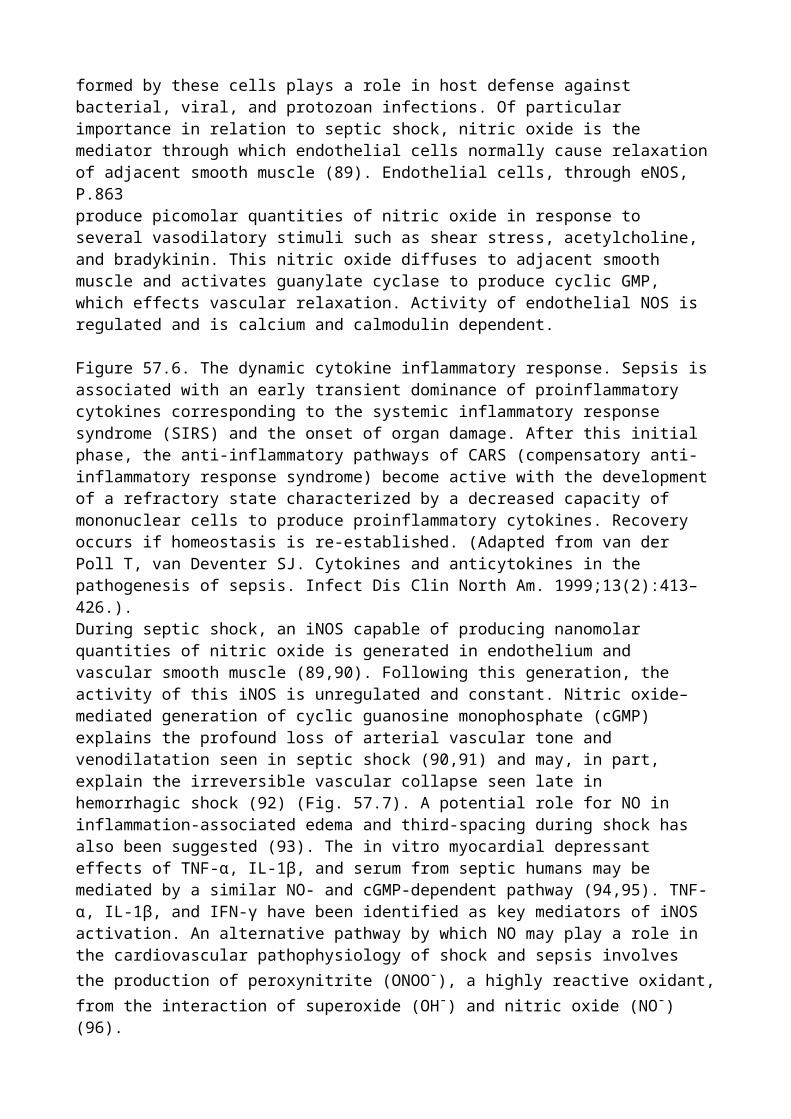
The systemic manifestations of anaphylactic and anaphylactoid reactions represent sequelae that result from the release of inflammatory mediators by mast cells and basophils. The classic anaphylactic response occurs through allergen-induced crosslinking of IgE tightly bound to the high-affinity FcεR1 receptor constitutively expressed by mast cells (52). Release of histamine from preformed mast cell granules seems to be the primary pathophysiologic mediator, resulting in systemic vasodilation, increased vascular permeability, bronchoconstriction, pruritus, and increased mucus production. However, a number of other preformed mediators are released, including heparin, serotonin, and mast cell proteases such as chymase and tryptase (53). In addition, other important mediators of anaphylaxis are generated by the metabolism of membrane phospholipids. Activation of the 5-lipoxygenase pathway results in synthesis of leukotrienes, including leukotrienes C4, D4, E4 (termed the slow-reacting substance of anaphylaxis), and B4. Leukotrienes
C4, D4, and E4, along with the intermediary products 5-hydroxyeicosatetraenoic acid and 5-
hydroperoxyeicosatetraenoic acid, elicit increases in vascular permeability and bronchoconstriction, whereas leukotriene B4 possesses eosinophil and neutrophil chemotactic properties. Activation of
the cyclooxygenase pathway leads to the production of prostaglandin D2, which produces
bronchoconstriction. Platelet-activating factor is also newly synthesized by activated mast cells and can result in bronchoconstriction, increased vascular permeability, platelet aggregation, and neutrophil chemotaxis. It also leads to further production of platelet-activating factor through stimulation of nuclear factor (NF)-κB, a positive feedback mechanism involving the cytokines interleukin-1 (IL-1) and tumor necrosis factor (TNF)-α, and contributes to a biphasic pattern seen in some patients (54). Combined, these primary mediators then facilitate the production of a diverse number of secondary mediators by platelets, neutrophils, eosinophils, and other cells, resulting in activation of the complement, coagulation, and fibrinolytic pathways (55).
Figure 60.1. Clinical criteria for diagnosing anaphylaxis. Fewer signs are required for diagnosis as the history of allergen exposure becomes more certain. Signs or symptoms of skin involvement: Generalized hives, pruritus, or flushing. Signs of mucosal involvement: Swollen lips, tongue, and/or uvula. Signs of respiratory compromise: Dyspnea, wheeze, bronchospasm, stridor, reduced peak expiratory flow, and/or hypoxemia. Definition of reduced blood pressure (BP): Adults—systolic BP less than 90 mm Hg or greater than 30% decrease from that person's baseline; children—systolic BP less than 70 mm Hg from 1 month to 1 year, less than (70 mm Hg + [2 × age]) from 1 to 10 years, and less than 90 mm Hg from 11 to 17 years or associated signs: Hypotonia, syncope, incontinence. Persistent gastrointestinal symptoms: Crampy abdominal pain and vomiting.Many of these mediators have complicated effects, and their relative roles in mediating anaphylaxis in vivo have been difficult to evaluate. Mouse models of anaphylaxis using strains with targeted deletions of specific mediators have been useful in elucidating the importance of different effector molecules, such as the leukotrienes (56,57,58), and in identifying regulatory P.937pathways, such as IL-10 (59), but have also provided some surprises that may lead to clinically useful information. For example, mice with targeted deletions of either the high-affinity FcεR1 receptor or IgE, not surprisingly, had a markedly decreased susceptibility to IgE-mediated anaphylaxis (53,60). This pathway can also be blocked with targeted deletion of histamine receptor 1 and, to a lesser extent, platelet-activating factor (52,53). However, such mice also revealed the presence of an alternate IgE-independent pathway of anaphylaxis (61). This pathway was mediated largely through platelet-activating factor, which was triggered by the binding of IgG to FcγRIII receptors present on macrophages (52,62). Like the classic IgE-mediated pathway, this alternative pathway required prior exposure to antigen, but differed in that much higher concentrations of antigen were required. The importance of this pathway in humans is as yet unclear (52). However, the administration of biologic agents, such as the anti-TNF antibody infliximab, has been reported to cause an IgE-independent anaphylactic response (63), and may be an example of this alternative pathway. The use of these biologic agents is expected to continue to increase.
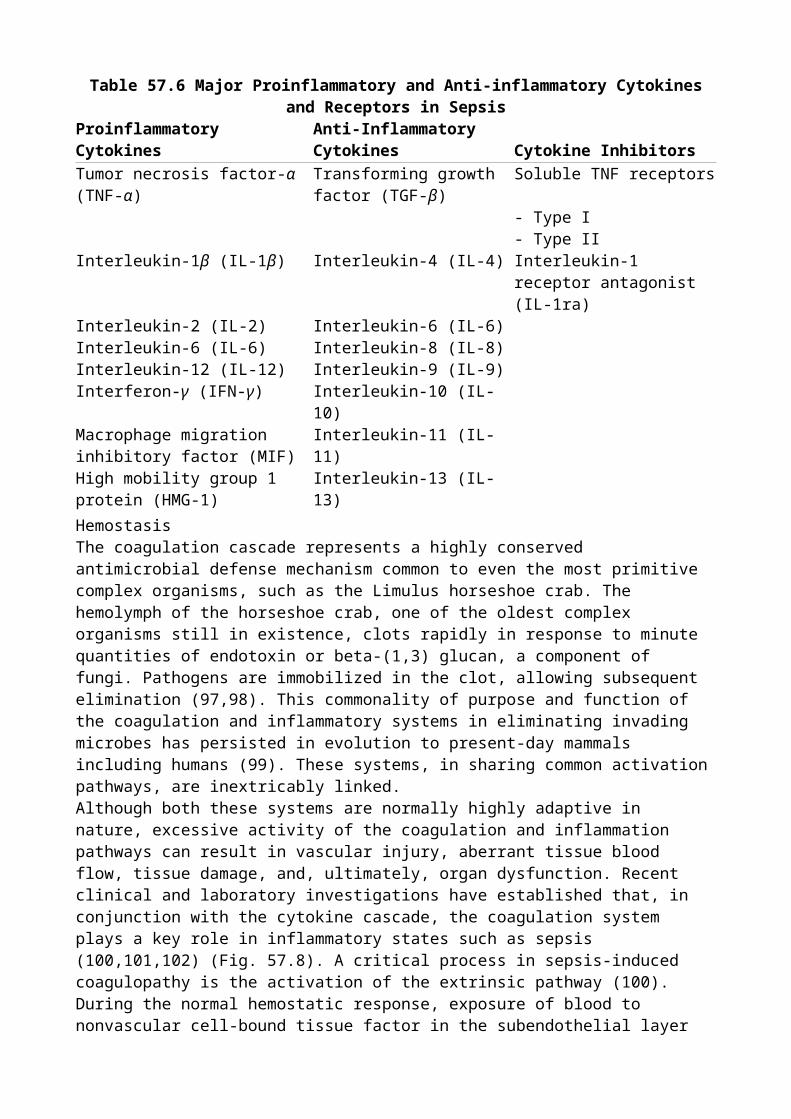
Table 60.4 Differential diagnosis of anaphylaxisFLUSH SYNDROME POSTPRANDIAL COLLAPSECarcinoid Airway foreign bodyPheochromocytoma Monosodium glutamate ingestionPeri-postmenopausal hot flushes SulfiteMedullary carcinoma of thyroid Scombroid fish poisoningRed man syndrome (vancomycin) MISCELLANEOUSHYPOTENSION Panic attacksSeptic shock Systemic mastocytosisHemorrhagic shock Basophilic leukemiaCardiogenic shock Hereditary angioedemaHypovolemic shock Hyper-IgE syndromeVasovagal reaction RESPIRATORY DISTRESS Status asthmaticus Airway foreign body Epiglottitis Pulmonary embolism Asthma and COPD exacerbation Vocal cord dysfunction IgE, immunoglobulin E; COPD, chronic obstructive pulmonary disorder.ManagementThe clinician must have a high index of suspicion for anaphylactic and anaphylactoid reactions because they require a prompt clinical diagnosis and a rapid therapeutic response. Because anaphylactic and anaphylactoid reactions both represent sequelae of mast cell and basophil degranulation, the therapeutic approaches to these disorders are identical. Initial attention should be given to assessment and stabilization of the pulmonary and cardiovascular manifestations of anaphylaxis, because these are the major causes of death.Epinephrine is the mainstay of initial management and should be administered immediately. It decreases mediator synthesis and release by increasing intracellular concentrations of cyclic adenosine monophosphate (cAMP) and antagonizes many of the adverse actions of the mediators of anaphylaxis (41). Aqueous epinephrine, 0.01 mg/kg (maximum dose 0.5 mg) administered intramuscularly every 5 to 15 minutes as necessary to control symptoms and maintain blood pressure, is recommended (41,64). The participants of the NIAID/FAAN symposium concluded that the intramuscular administration of epinephrine in the anterior lateral thigh is preferred over subcutaneous injection (1,2). In cases of severe laryngospasm or frank cardiovascular collapse, or when there is an inadequate response to subcutaneous epinephrine administration and fluid resuscitation, intravenous epinephrine is an option. There is no established dosage regimen for intravenous epinephrine in anaphylaxis, but suggested dosages are 5 to 10 µg bolus (0.2 µg/kg) for hypotension and 0.1 to 0.5 mg in the setting of cardiovascular collapse (1,2,65). When epinephrine is administered IV, the clinician should be aware of the potential adverse consequences of severe tachycardia, myocardial ischemia, hypertension, severe vasospasm, and gangrene—the latter when infused by peripheral venous access (66).Blood pressure measurements should be obtained frequently, and an indwelling arterial catheter should be inserted in cases of moderate to severe anaphylaxis. High-flow oxygen given via endotracheal tube or a nonrebreather mask should be administered to patients experiencing hypoxemia, respiratory distress, or hemodynamic instability (1,2). Orotracheal intubation may be attempted if the airway obstruction compromises effective ventilation despite pharmacologic intervention; however, attempts may be unsuccessful if laryngeal edema is severe. If endotracheal intubation is unsuccessful, then either needle-catheter cricothyroid ventilation, cricothyrotomy,
P.938or surgical tracheostomy is required to maintain an adequate airway. Clinicians must be familiar with at least one of these techniques in the event that endotracheal intubation cannot be accomplished. It has been suggested that inhaled β2-agonists such as albuterol may be useful for
bronchospasm refractory to epinephrine (1,2,67). Patients should be placed in the recumbent position, with lower extremities elevated to increase fluid return centrally, thereby increasing cardiac output (68). Airway protection should be ensured in the event of vomiting.Antihistamines (H1 and H2 antagonists) are considered second-line treatment for anaphylaxis (1,2).
They are useful in the treatment of symptomatic urticaria-angioedema and pruritus. Recent studies suggest that treatment with a combination of H1 and H2 antagonists is more effective in attenuating
the cutaneous manifestations of anaphylaxis than H1 antagonists alone (50,69). Diphenhydramine
hydrochloride (25 to 50 mg IV or IM for adults and 1 mg/kg, up to 50 mg, for children) and ranitidine (50 mg IV over 5 minutes) are commonly used in this setting. If hypotension persists despite administration of epinephrine and H1 and H2 blockers, aggressive volume resuscitation
should be instituted. Up to 35% of the blood volume may extravasated in the first 10 minutes of a severe reaction, with subsequent reduction in blood volume due to vasodilatation, causing distributive shock (70). Persistent hypotension may require multiple fluid boluses (10 to 20 mL/kg under pressure) as well as colloid and crystalloid infusions (1,2). Vasopressors such as norepinephrine, vasopressin, Neo-Synephrine, or even metaraminol may be useful in persistent hypotension (31).There have been no placebo-controlled trials evaluating the efficacy of corticosteroids in anaphylaxis, but their contribution in other allergic diseases has led to their inclusion in anaphylactic management. Due to their slow onset of action, they are not useful in acute management. However, it has been suggested that they may prevent protracted or biphasic reactions (67,71). The usual dose is 100 to 250 mg of hydrocortisone IV every 6 hours (39).The management of anaphylaxis in a patient receiving β-antagonist medications, such as β blockers, represents a special circumstance in which the manifestations of anaphylaxis may be exceptionally severe (72). β Blockade increases mediator synthesis and release, as well as end-organ sensitivity. In addition, β-blockade antagonizes the beneficial β-mediated effects of epinephrine therapy, thereby resulting in unopposed α-adrenergic and reflex vagotonic effects: vasoconstriction, bronchoconstriction, and bradycardia. Therapy of anaphylaxis occurring in patients receiving β-antagonist drugs, however, is similar to that of other patients. In addition, atropine may be useful for heart block and refractory bronchospasm, whereas glucagons—which increase cAMP levels through a β-receptor–independent mechanism—have been reported to reverse the cardiovascular manifestations of anaphylaxis in patients receiving β-antagonists (72). Glucagon can be administered as a 1- to 5-mg (20–30 µg/kg with maximum dose of 1 mg in children) intravenous infusion over 5 minutes, followed by an infusion of 5 to 15 µg/minute titrated to a clinical response (1,2). Furthermore, these patients may require extended periods of observation because of the long duration of action of many β-antagonist medications.An emergent evaluation for the inciting etiologic agent must accompany initial therapeutic interventions. After the etiologic agent is identified, the clinician should attempt to prevent further access to the circulation or limit further absorption. Infusions of possible etiologic agents should be stopped and the contents saved for analysis. If a Hymenoptera sting is responsible, the stinger should be removed. Small amounts of local epinephrine—0.1 to 0.2 mL of a 1:1,000 solution—should be injected next to a subcutaneous or intramuscular injection site that is dispersing the inciting agent. A tourniquet also should be placed proximal to the injection site and pressure applied to occlude venous return. After successful pharmacologic therapy, the tourniquet may be cautiously removed and the patient carefully observed for recurrent adverse sequelae. In cases where the offending agent was ingested, consideration may be given to insertion of a nasogastric tube to perform gastric lavage and gastric instillation of activated charcoal.Therapeutic Pearls

Rapidly assess and maintain the airway, breathing, and circulation. If airway obstruction is imminent, perform endotracheal intubation; if unsuccessful, consider needle-catheter cricothyroid ventilation, cricothyrotomy, or tracheostomy. Patients in anaphylactic shock should be placed in a recumbent position with the lower extremities elevated, unless precluded by shortness of breath or vomiting.
Remove the inciting agent (i.e., remove Hymenoptera stinger) and follow with an intramuscular epinephrine injection in the anterior lateral thigh. Consider gastric lavage and administration of activated charcoal if the inciting agent was ingested.
Administer aqueous epinephrine, 0.01 mg/kg (maximum dose, 0.5 mg) intramuscularly every 5 to 15 minutes as necessary for controlling symptoms and maintaining blood pressure.
Establish intravenous access for hydration and provide supplemental oxygen. Administer histamine antagonists to block vasodilation, capillary leak, and shock (H1
blockade, 25–50 mg of diphenhydramine IV or IM for adults, and 1 mg/kg—up to 50 mg—for children; H2 blockade, 50 mg of ranitidine IV).
Administer vasopressors for persistent hypotension and titrate to a mean arterial pressure of 60 mm Hg.
Consider aggressive fluid resuscitation with multiple fluid boluses (10–20 mL/kg under pressure), including colloid as well as crystalloid, in patients who remain hypotensive despite epinephrine.
Administer inhaled β2-agonists such as albuterol for bronchospasm refractory to epinephrine
(73). Consider corticosteroid therapy for protracted anaphylaxis or to prevent biphasic
anaphylaxis (1.0–2.0 mg/kg methylprednisolone IV every 6 hours). Oral prednisone at 1.0 mg/kg, up to 50 mg, may be used for milder attacks. Corticosteroids are not effective therapy for the acute manifestations of anaphylaxis.
Consider glucagon administration (1–5 mg IV over 1 minute, then 1–5 mg/hour in a continuous infusion) in the setting of prior β-blockade because of its positive inotropic and chronotropic effects mediated by a β-receptor–independent mechanism.P.939
Prevent recurrent episodes by avoidance of the inciting agent, desensitization, or premedication with corticosteroids and H1 and H2 blockade.
Admission to the intensive care unit is warranted for invasive monitoring with arterial and pulmonary artery catheters, electrocardiography, pulse oximetry, and frequent arterial blood gas measurements.
ObservationAn observation period should be considered for all patients following treatment of an anaphylactic reaction. On the basis of clinical data available to date, the NIAID/FAAN symposium recommends that observation periods be individualized on the basis of severity of initial reaction, reliability of the patient, and access to care. A reasonable time would be 4 to 6 hours for most patients, with prolonged observation or hospital admission for severe or refractory symptoms and patients with reactive airway disease (1,2).Follow-up, Management, and PreventionThe ideal method for managing severe systemic anaphylactic and anaphylactoid reactions is by preventing their occurrence. Persons with a known sensitivity should avoid re-exposure to the inciting etiologic agents. Patients who have experienced respiratory or cardiovascular symptoms of anaphylaxis should receive self-injectable epinephrine for use if anaphylaxis develops. These patients should also have an emergency action plan detailing its use and follow-up management (1,2). If a precipitating allergen is known or identified, patients should receive information about avoiding it in the future, prior to their discharge from the emergency facility. They should be encouraged to obtain prompt follow-up with their primary care physician as well as an allergist
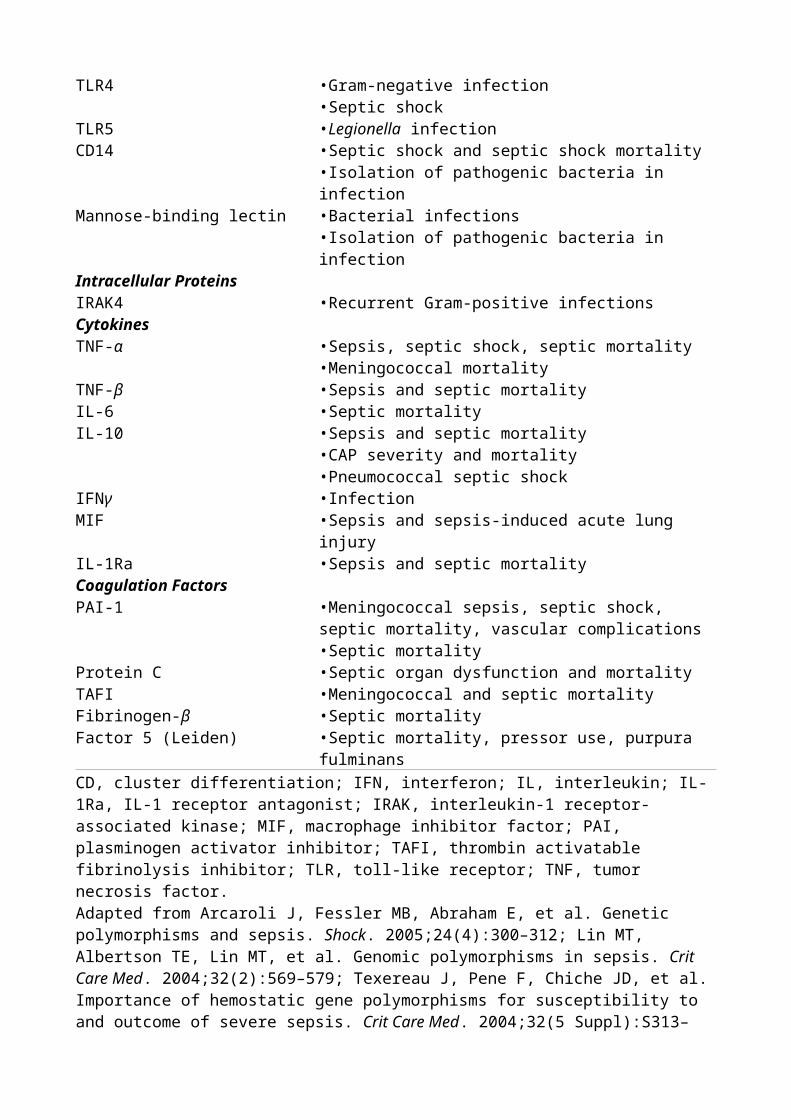
(1,2).Implications and OutcomeAnaphylactic/anaphylactoid reactions represent important, potentially reversible, acute respiratory and cardiovascular emergencies. Although the optimal management method is that of prevention, prompt diagnosis and institution of therapy are crucial after these reactions have been initiated in order to prevent the fatal cardiovascular and pulmonary manifestations. Factors associated with improved survival include the sensitivity of the person to the inciting agent, the duration between the exposure and the onset of symptoms (short latency periods are associated with more severe manifestations), the route and dose of the offending agent (larger doses and parenteral administration are associated with more severe manifestations), and the interval between onset of symptoms and subsequent diagnosis and institution of appropriate therapy (74). Optimal management of acute systemic reactions includes appropriate pharmacologic intervention, support of pulmonary and cardiovascular function, and removal of the offending agent. Expeditious institution of these measures helps to reduce the morbidity and mortality associated with these potentially life-threatening syndromes.Summary
Anaphylactic reactions represent type I immune responses mediated by IgE bound to mast cells or basophils. Common inciting agents include β-lactam antibiotics and Hymenoptera stings. Other common causes include foods, local anesthetics, and serum products.
Anaphylactoid reactions represent IgE-independent activation of mast cells or basophils, with resultant degranulation and mediator release. Common inciting agents include iodinated radiocontrast media, neuromuscular depolarizing agents, and opiates, all of which induce direct mast cell activation; nonsteroidal anti-inflammatory agents acting through cyclooxygenase inhibition; and blood products acting through complement activation.
A history of a previous reaction to radiocontrast media, asthma or atopic disease, treatment with β-blockers, and cardiovascular disease are risk factors for developing anaphylaxis to radiocontrast media (27,28,29).
The differential diagnosis of anaphylactic and anaphylactoid reactions includes cardiac arrhythmias, myocardial infarction and cardiogenic shock, distributive or hypovolemic shock, vasovagal syncope, asthma, pulmonary embolism, upper airway obstruction secondary to a foreign body, vocal chord dysfunction, hypoglycemia, carcinoid syndrome, systemic mastocytosis, hereditary angioedema, and leukemia with excess histamine production.
Epinephrine is the initial drug of choice for the management of anaphylactic or anaphylactoid reactions. H1- and H2-blocking agents also should be administered.
Corticosteroids are not effective for the acute management of anaphylactic or anaphylactoid reactions, but may prevent biphasic anaphylaxis or attenuate prolonged reactions. Glucagon may be used for persistent hypotension in patients taking β-blockers.
Chapter 61Splanchnic Flow and ResuscitationJohn W. MahOrlando C. KirtonIschemia signifies failure to satisfy the metabolic needs of the cell secondary to either impaired oxygen delivery or the impairment of cellular oxygen extraction and utilization. Incomplete splanchnic cellular resuscitation has been associated with the development of multiple organ system failure and increased mortality in the critically ill patient (1,2). For many years, the merits of augmenting systemic oxygen delivery and consumption and attainment of supranormal levels have been examined and debated as primary treatment goals (3,4,5,6). There is convincing evidence that systemic hemodynamic and oxygen transport variables fail to accurately portray the complex interaction between energy requirements and the energy supply at the tissue level (7,8,9), and that achieving supranormal cardiovascular oxygen transport and utilization indices does not reliably confer improved outcome (i.e., decreased mortality rates and diminished multiple organ system failure) in several clinical conditions (e.g., sepsis, acute respiratory distress syndrome [ARDS]) (10,11,12,13). These findings have led to the search for monitoring techniques that directly measure changes in regional tissue bioenergetics.Intestinal tonometry has been proposed as a relatively noninvasive index of the adequacy of aerobic metabolism in organs whose superficial mucosal lining is extremely vulnerable to low flow and hypoxemia, and in which blood flow is sacrificed first in both shock and the cytokine milieu of the systemic inflammatory response (1,14,15). The gastrointestinal tract, therefore, acts like the “canary,” displaying early metabolic changes before other indices of adequate oxygen utilization (16). This chapter reviews the fundamental and clinical underpinnings of splanchnic ischemia and resuscitation, intestinal and subsequently sublingual tonometry, the potential applications and limitations of this technology, its use as a prognostic and treatment end point, and, finally, a consideration of potential future directions.The Intestinal MicrocirculationThe gastrointestinal tract has three major functions: motility, secretion, and absorption. Blood flow is important for each of these functions, being highest in the small intestines and lowest in the colon. The splanchnic circulation contains approximately 30% of the circulating blood volume at any given moment with the bulk of this volume held in the postcapillary venous capacitance vessels (17). Resting blood flow in the intestine is ten times higher than in skeletal muscle. Most of the blood flow is delivered to the mucosa and submucosa, reflecting the varying demands for oxygen within the intestinal wall, being highest in the mucosal layer. The arterial supply emanates from an extensive arterial plexus in the submucosa. A countercurrent blood flow exchange system exists within the superficial mucosal layer between the arterial and venous circulation, rendering this tissue particularly sensitive to neuronal and systemic vasoconstrictors (18). The arterioles, which run in parallel with the venules in the stalk of the intestinal villus, allow diffusion of oxygen from the arterioles down a concentration gradient to the venules, bypassing the capillary bed at the villus tip; thus, the mucosa at the villus tip is rendered vulnerable to changes in oxygen content. Water also diffuses from arterioles to venules because of an osmotic gradient caused by the absorption of sodium in the capillary bed at the villus tip. Therefore, the sodium concentration is higher in the venules. Plasma water content is then lowered at the villus tip compared with the base of the stalk, predisposing this area to low or absent flow in states of compensated or uncompensated shock when splanchnic circulation is compromised.Mesenteric vasoconstriction is mediated by α-adrenergic postganglionic sympathetic fibers, but, even more dramatically, by the effects of circulating hormones and peptides (Table 61.1). Endogenous vasoconstrictors known to be released in major injury, sepsis, and other physiologically
stressful circumstances include catecholamines, angiotensin, vasopressin, myocardial depressant factor, leukotriene D4, thromboxane A2, and serotonin. The high concentration of receptors for these
systemically released vasoconstrictors, which affect the splanchnic circulation more than any other tissue beds, has a substantial effect on peripheral (systemic) vascular resistance and, hence, on systemic blood pressure by redistributing blood from the splanchnic organs (as well as the peripheral circulation) to the central circulation (i.e., heart and brain). This effect may be compounded by tissue edema and atheroma in the splanchnic arteries. The peptides, angiotensin II and vasopressin, are the most potent splanchnic vasoconstrictors (14). The splanchnic vasoconstriction induced by these two peptides alone accounts for most of the increase in total vascular resistance recorded in animal models of cardiogenic and hemorrhagic shock. The adequacy of gut mucosal oxygenation cannot be reliably inferred from measurements of tissue oxygenation in the skin or of subcutaneous tissue because of their different response to endogenous P.942vasoconstrictors.Table 61.1 Endogenous vasoconstrictors known to be released in stressful circumstances and
their actions on different tissue bedsVasoconstrictor Gut Renal Brain Coronary Pulmonary Muscle SkinCatecholamines + + 0 + ± ± +Angiotensin II + + 0 0 0 0 0Vasopressin + + ?0 + ? ? +Myocardial depressant factor+ 0 0 0 0 0 0Leukotriene D4 + + 0 + ? 0 0
Thromboxane A2 + + + + + + +
Serotonin + + ? ? + – ±+, vasoconstriction; –, vasodilatation; 0, no effect; ±, effect varies; ?, undefined.From Fiddian-Green RG. Studies in splanchnic ischemia and multiple organ failure. In: Marston A, Bulkley GR, Fiddian-Green RG, et al., eds. Splanchnic Ischemia and Multiple Organ Failure. London: Edward Arnold/St. Louis: CV Mosby; 1989:349.Pathophysiology of Mesenteric Ischemia and ReperfusionTissues with a high perfusion-to-extraction (demand) ratio, such as skeletal muscle, have high capillary densities that act as a microvascular reserve to produce an increase in local blood flow. These organs, in situations of low flow, use a disproportionate share of the cardiac output as increased capillary recruitment lowers local vascular resistance. These tissues are characterized by low oxygen extraction ratios and high mixed venous oxygen saturations. Less “fortunate” tissues, which include the intestinal tract, possess a lower capillary density and are unable to recruit capillaries to augment local blood flow to match increases in metabolic needs. This results in low perfusion-to-oxygen demand ratios and subsequent tissue hypoxia (the “trickle down economy” of systemic oxygenation) (15). The gastrointestinal tract is characterized by a high oxygen extraction ratio, lactate release, and low mixed venous oxygen saturation; it can tolerate severe hypoxemia without a decrease in oxygen consumption but is limited in its ability to respond to decreased blood flow.Intestinal tissue injury can be induced by the initial ischemia (either from inadequate oxygen content or inadequate flow) or by the generation of oxygen-derived free radicals during reperfusion (1,7). Ischemic injury may be progressive, spanning a spectrum from mild injury characterized by increased capillary permeability with no microscopic changes to transmural infarction, depending on the severity and duration of the ischemia (1,2,19,20). Inadequate oxygen supply results in anaerobic glycolysis and systemic lactic acidosis. In the anoxic cell, uncompensated adenosine triphosphate (ATP) hydrolysis is associated with the intracellular accumulation of adenosine diphosphate (ADP), inorganic phosphate, and hydrogen ions with resultant intracellular acidosis (7,21). These hydrogen ions lead to tissue acidosis as well, with unbound hydrogen ions combining with interstitial bicarbonate to form the weak acid, carbonic acid, that disassociates to produce
carbon dioxide (CO2) plus water.
Hypoxia renders the superficial gastrointestinal mucosa susceptible to the cytolytic effects of gastric acid, proteolytic enzymes, and bacteria already present in the intestine by impairing cellular mucus and bicarbonate secretion. Disruption of the mucosal barrier is associated with the generation of myocardial depressant factors that cause a low cardiac output syndrome in animals (14,22,23). Commonly, in low flow and hypoxic states, tissue oxygen consumption ([V with dot above]O2) is
maintained by adaptive mechanisms that are activated when oxygen delivery ([D with dot above]O2) falls below a critical level and oxygen consumption becomes delivery dependent.
Intracellular acidosis impairs cellular function by one of several mechanisms: (a) the loss of adenosine nucleotides from mitochondria by the inhibition of the ATP–magnesium/inorganic phosphate carrier; (b) inhibition of sodium–calcium exchange, resulting in the intracellular sequestration of calcium ions; (c) increases in the activity of cyclic adenosine monophosphate (AMP) deaminase and loss of adenine nucleotide precursors from the cell; (d) decreases in the nicotinamide adenine nucleotide pool by the acid-catalyzed destruction of nicotinamide adenine dinucleotide (NAD); and (e) the conversion of intracellular inorganic phosphate to its inhibitory deproteinated form (7).Hypoxia also results in intracellular calcium overload by inhibiting ATP-driven membrane transport pumps and sodium–calcium exchange. Increases in intracellular calcium are a pivotal event in cellular dysfunction during hypoxia, because calcium-activated proteases can destroy the sarcolemma and the cellular cytoskeleton (7). Cellular membrane degradation seems to be related to calcium influx. Calcium stimulates phospholipase A2 (PLA2) and phospholipase C, which are
known to degrade membrane phospholipids (24,25). The resultant imbalance between the rate of membrane synthesis and the rate of membrane breakdown results in the accumulation of arachidonic acid, the precursor of thromboxane, prostaglandins, and leukotrienes, substances that produce further cellular damage and profound alterations in microvascular control.P.943The Splanchnic Model of Multiple Organ FailureMultiple system organ failure (MSOF) (defined as failure of two or more vital organs or systems, in sequence or simultaneously, irrespective of the primary disease) and sepsis are distressingly familiar to surgeons who perform major elective cases, as well as to those involved in transplantation and trauma (26). Uncompensated or compensated shock leading to progressive oxygen debt, ischemia/reperfusion injury, and cellular dysfunction is the underlying unifying pathophysiologic mechanism (1). Throughout the world, MSOF has become the most common cause of death in the intensive care unit: The reported mortality rates vary from 30% to 100% with a mean of 50%, depending on the number of organ systems involved; the patients' intensive care unit (ICU) stay lasts for 6 weeks to many months and, in prior studies, these patients have used nearly 40% of the available ICU days (26,27,28,29,30). Many hypotheses link the noxious event, whether surgery or trauma, to the development of MSOF and sepsis. There have also been many attempts to use single agents (e.g., antibiotics, monoclonal antibodies against cytokines and endotoxin) or combinations of these agents to affect the process; unfortunately, no significant progress has been made with these approaches. This may result from the many redundancies in the initiation and promulgation of MSOF, so that attacking a single pathway is ineffective or, perhaps, efforts have been started too late in the sequence of events. Bacterial endotoxin in the gut may translocate across the semipermeable mucosa as a result of ischemia/reperfusion. Besides endotoxins, the products of the damaged mucosa also may contribute to the systemic inflammatory response and subsequent MSOF and death of the ICU patient. The translocation of enteric bacteria across the ischemic gut seems to be an important cause of nosocomial infection in the critically ill (14,26). However, reducing the number of nosocomial infections from enteric organisms by selective decontamination does not seem to have a dramatic effect on outcome; that is, “again, the horse is already out of the barn” (31).While representing an oversimplification, we believe the current hypotheses can be combined. Most current thinking can be categorized as the gut starter hypothesis popularized by Moore et al. (32)
and the gut motor hypothesis as described by Deitch (27) and Marshall et al. (28,29).In the gut starter hypothesis, the noxious stimulus leads to a neurohumoral response. High levels of catecholamines cause splanchnic vasoconstriction and a decrease in splanchnic flow. This leads to gut ischemia and, depending on the length of ischemic time, allows various reactions that prime tissue to develop a reperfusion injury once flow is restored. During reperfusion, PLA2 is activated,
which in turn activates platelet-activating factor (PAF). PAF attracts and primes polymorphonuclear leukocytes (PMNs) in the gut; thereafter, they are released into the systemic circulation, where they undergo activation (the two-hit model) and cause end-organ injury (32). Therefore, the PMN is implicated as the major effector of cellular damage attributed to ischemia/reperfusion through its respiratory burst and activation of cytokines and arachidonic acid metabolites.In the gut motor hypothesis, the steps leading to ischemia are the same. During reperfusion, gut mucosal injury results from the accumulation of intracellular calcium, activation of PLA2, and
generation of free oxygen radicals. This leads to bacterial translocation and initial production and amplification of numerous systemic cytokines (33,34). The end result again is MSOF. It is likely that these hypotheses are correct, although they are still incomplete explanations.Systemic Oxygen Delivery, Utilization, and MonitoringThe determinants of arterial oxygenation include hemoglobin content, inspired oxygen tension, alveolar oxygen tension, pH, temperature, mixed venous oxygen tension, ventilation/perfusion ([V with dot above]/[Q with dot above]) mismatch, physiologic shunting, and cellular–interstitial diffusion abnormalities. Indices of adequacy of systemic perfusion include the following: (a) global systemic parameters, such as blood pressure, heart rate, central venous pressure measurements, and urine output; (b) tissue markers, including arterial pH (pHa), base excess, and serum lactate level; and (c) pulmonary artery catheter measurements and derivations, such as cardiac output, oxygen delivery, oxygen consumption, and oxygen extraction. In fact, Rivers et al. demonstrated that goal-directed resuscitation using certain systemic measures (mean arterial pressure [MAP], urine output [UOP], central venous pressure [CVP]) including improving oxygen delivery to an ScVO2 >70%
can improve mortality in patients in severe sepsis and septic shock (35). Nonetheless, the interpretation of oxygen delivery and oxygen consumption measurements is challenging because (a) these parameters are global markers and do not provide any direct information regarding the oxygen requirements of specific tissues, (b) the distribution of oxygen delivery is impacted by local microvascular and neurogenic responses, (c) the effect of cytokines and endogenous peptides is unpredictable, and (d) the disease process may affect cellular metabolism directly (i.e., sepsis and ARDS) (36,37,38). Several prospective studies suggest that failure to achieve supranormal oxygen delivery and utilization parameters in the acute phase of major injury or physiologic stress is associated with increased mortality and shock-related complications, including multiple organ system dysfunction syndrome. The failure to reverse pathologic flow dependency, tissue hypoxia, and oxygen debt has been inferred as the cause of these adverse outcomes (3,4,5,6,39,40). In these prospective studies, both responders and nonresponders achieved normal or hyperdynamic cardiovascular function; however, more cardiovascular interventions were often used in patients who died, so, ultimately, failure of patient response to achieve therapeutic objectives could be considered as the cause of the observed increased mortality and morbidity. Several reports failed to identify either an optimal or a critical value of oxygen delivery or consumption to distinguish survivors from nonsurvivors in critically ill patients (10,11,12,13,23). Adequate or supranormal oxygen delivery may not be tantamount to effective tissue oxygen utilization.“Critical oxygen delivery” purportedly marks the transition from aerobic to anaerobic metabolism; however, the relationship between oxygen delivery and consumption obtained in critically ill patients with ARDS, sepsis, and heart failure has been linear (23). The lack of a clearly defined inflection point in a linear [D with dot above]O2–[V with dot above]O2 function makes it
impossible to determine P.944a critical level of oxygen delivery that aerobically satisfies cellular energy requirements.
Regional Oxygen Delivery, Utilization, and MonitoringA Historical Review of Gastric TonometryA tonometer is composed of a semipermeable silicone balloon, which is filled with either air or fluid and allowed to equilibrate with the surrounding tissue. The fluid/air is then accessed and the pressure of CO2 can be directly measured. Tonometry was first used by Bergofsky (41) and Dawson
et al. (42) in 1964 to demonstrate that the gas tension within a hollow viscus approximates that within the mucosa of the viscus. Grum et al. (21) extended this concept to the intestinal tract of adults. Antonsson et al. (43) and Hartmann et al. (44) performed validation studies demonstrating that both the stomach and small intestine could be used as suitable sites to measure intraluminal PCO2. They confirmed that intraluminal PCO2 equaled that measured within the intestinal mucosa
as well as approximated hepatic vein PCO2. Moreover, it has been validated that the intramucosal
PCO2 rises and falls in parallel with changes in PCO2 in arterial blood (45). This indirect method of
measuring the pH within the intestinal mucosa (pHi) is based on the fact that CO2 is a highly
permeable gas and on the assumption that this generated CO2 is the end result of ATP hydrolysis,
with neutralization of generated hydrogen ions by intestinal interstitial bicarbonate (46).The measurement of pHi depends also on the assumption that the bicarbonate concentration in the wall of the organ is the same as that which is delivered to it by arterial blood, and that the dissociation constant (pK) is the same as that in the plasma. Using the Henderson-Hasselbalch equation, pHi is calculated as follows:pHi = 6.1 + log(HCO3
-/0.03 × PCO2)
pKa is 6.1, and 0.03 is the solubility coefficient for CO2. The pK in plasma is not the same as that in
the cytosol, but the value 6.1 is the best approximation of the pK within the intestinal fluid of the superficial layers of the mucosa (14,47,48).Doglio et al. (49) demonstrated that gastric pHi was a predictor of ICU mortality at the time of admission to the ICU and at 12 hours later. Patients admitted with a pHi <7.36 had a greater ICU mortality rate, 65% versus 44% (p <0.04). Furthermore, patients with persistently low pHi at 12 hours after ICU admission had the highest mortality rate (87%). Maynard et al. (50) repeated the study in patients with acute circulatory failure and found remarkably similar outcomes. In addition, there were significant differences in mean gastric pHi values between survivors and nonsurvivors on admission (7.40 vs. 7.28) and at 24 hours (7.40 vs. 7.24), respectively (p <0.001). There was no difference in cardiac index, oxygen delivery, and oxygen uptake, suggesting that pHi is a more specific marker of resuscitation than our common global parameters.We also confirmed that failure of splanchnic resuscitation correlated with MSOF and increased length of ICU stay in the hemodynamically unstable trauma patient (51). The relative risk of death in patients whose pHi was less than 7.32 was 4.5-fold higher and the relative risk of developing multiple organ system failure was 5.4 times higher compared with those having a pHi of 7.32 or more. Global parameters of oxygen transport utilization did not distinguish survivors from nonsurvivors nor those patients who developed MSOF from those who did not.Chang et al. (52) then conducted a prospective study of 20 critically ill patients and were able to demonstrate that correction of an abnormal admission pHi correlated with better outcomes. Patients with pHi less than 7.32 on admission, who did not correct within the initial 24 hours, had a higher mortality (50% vs. 0%; p = 0.03) and more frequent MSOF (2.6 vs. 0.62 organs/patient; p = 0.02) than those whose pHi corrected.Ivatury et al. (53) compared correction of pHi versus supranormal oxygen delivery (as defined by Shoemaker et al. [3] in 27 critically ill trauma patients). Seventy-five percent of the patients who developed MSOF had pHi less than 7.3. Interestingly, four of the five patients who died in the supranormal oxygen group achieved supranormal oxygen delivery and consumption goals, but had a pHi less than 7.3 at 24 hours. Moreover, they observed that a late fall in pHi was often associated with a physiologic catastrophe (e.g., intestinal leak, gangrene, bacteremia).
There have been only two prospective controlled interventional studies in which therapy was instituted because the pHi was low. Neither of these studies, however, attempted to normalize the pHi, but rather focused on increasing oxygen delivery and utilization. Gutierrez et al. (54) observed that the hospital mortality rate was significantly greater in control patients whose pHi was normal on admission (pHi ≥7.35) and then became abnormal during their ICU stay compared with those whose abnormal pHi prompted interventions to increase oxygen delivery. Unfortunately, if admission pHi was low, the mortality rates were the same in both treatment and control groups. The authors chose to increase oxygen delivery rather than restore pHi to normal values.We also specifically studied ICU patients with persistent uncorrected gastric pHi who had pulmonary artery catheters to guide resuscitation (55). We observed a significant reduction in the incidence of MSOF per patient (1.9 ± 0.4 to 0.9 ± 0.2; p = 0.02), length of ICU stay (35 ± 9 to 18 ± 4 days; p = 0.03), and total hospital stay (51 ± 12 to 29 ± 5 days; p = 0.03) in patients with persistent gastric intramucosal acidosis who were administered agents that increased splanchnic perfusion and that were intended to prevent free radical damage during reperfusion. We conclude that efforts to correct gastrointestinal intramucosal acidosis related to splanchnic hypoperfusion are warranted because MSOF and mortality were increased in those patients whose pHi never corrected (i.e., pHi <7.25).Despite the potential benefits of regional monitoring, gastric tonometry has fallen out of favor for multiple reasons. The monitoring itself is labor intensive and time consuming, often requiring multiple attempts to ensure proper positioning and frequent catheter adjustments, lengthy equilibration times, and need for frequent troubleshooting of abnormal results. Gastric acid must be neutralized (pH >4.5), requiring pH litmus paper analysis and adjustments to the peptic ulcer prophylaxis regimen in the ICU patient. Tube feedings also must be held. In addition, one must use a dedicated blood gas analyzer for all pHi determinations. Periodic calibration of the analyzer with 10 to 20 ampules at three different PCO2 levels must be done. The saline sample must be
transported immediately on ice because of rapid loss of CO2 from the sample and overestimation of
the pHi.P.945Sublingual TonometryResearchers moved more proximally in the gastrointestinal tract in search of a more reliable and efficient place to measure tissue PCO2, evaluating first the esophagus and finally the sublingual
space (56). Weil et al. suggested that the sublingual space would respond similarly to the splanchnic circulation (57). Marik also demonstrated good correlation of sublingual tonometry with gastric tonometry and more importantly that it was the difference between the sublingual PCO2 (slPCO2)
and arterial PCO2 (PCO2 gap) that was more predictive of survival (58). Since then, sublingual
capnometry (SLC) has generated much interest as a potential splanchnic tissue monitor, overcoming the shortcomings and obstacles of the more invasive and burdensome intestinal tonometers. The device uses a disposable sensor that detects CO2 and sends the information back to the handheld
instrument. The sensor is placed directly under the sublingual space and is kept in place for approximately 60 to 90 seconds. Recent investigations have suggested use of SLC in the triage of patients with penetrating traumatic injuries showing statistical differences in severe to moderate (>1,500 mL) or minimal to moderate (<1,500 mL) amount of blood loss on admission (59). Our research supports Marik's findings that the PCO2 gap and to a lesser degree the absolute SLC value
correlates with outcome (60). Our observations show a significant difference in development of MSOF and mortality in 83 critically ill surgical patients subjected to a standard resuscitation protocol. Patients whose PCO2 gap was not corrected to 9 mm Hg or less at 24 hours after
admission were three times more likely to experience MSOF and more than ten times as likely to die during their hospital stay. Sublingual capnometry is a quick and simple method to directly measure tissue perfusion and is a potential tool for the clinician to help guide goal-directed therapy. The product has been recalled due to infectious complications but may be reinstated in the future.
Monitoring PlanIntramucosal PCO2 provides an intermittent direct measure of the ability of tissues to resynthesize
high-energy phosphate compounds utilizing aerobic metabolism. In dysoxic states, protons accumulate and pHi falls, indicative of inadequate oxidative metabolism. If this is recognized early and can be reversed, the clinician may be able to prevent or limit the duration of compensated shock. Global measurements of oxygen delivery, oxygen consumption, oxygen extraction ratio, and mixed venous blood hemoglobin oxygen saturation (S[v with bar above]O2) are unsatisfactory for
this purpose (47,61). The calculation of pHi can provide clinicians with a metabolic end point that may be used to determine whether the milieu is likely to create a reperfusion injury if resuscitation is successful or whether subclinical maldistribution of blood flow persists—a reflection of a still-active neurohumoral response to stress.Monitoring all patients likely to have had activation of the neurohumoral response and decreased splanchnic blood flow is probably beneficial because they are at risk for a reperfusion injury, MSOF, and a higher mortality rate (47). Outcome can be improved by recognizing compensated shock, preventing ischemia/reperfusion injury, and ensuring that intramucosal acidosis is promptly reversed. Recognize that the window of opportunity for effective therapy is early (61). Both a preemptive intervention to block and modify the ischemia/reperfusion injury and restoration of splanchnic perfusion must be incorporated into a resuscitation algorithm to reduce the incidence of bacterial translocation and systemic white cell priming before the ensuing systemic inflammatory response (1). Because early abnormalities in the gastrointestinal intramucosa act as a marker of mortality and morbidity, efforts to correct them may improve outcome and should diminish resource utilization (62,63). If pHi falls, or if slPCO2 or the PCO2 gap rises unexpectedly (the canary), look
for intra-abdominal catastrophes, intra-abdominal hypertension, sepsis, tissue necrosis, line sepsis, nosocomial infection, unappreciated excess patient ventilatory work, hypovolemia, and hypoxemia (53,62,64,65,66).Concepts in Splanchnic ResuscitationThe limited success thus far that has attended attempts to elevate an already depressed pHi and an understanding of the importance of the ischemia/reperfusion injury as a fundamental part of both the gut starter and gut motor hypotheses suggest that a new perspective is needed. Two separate elements must be combined: a preemptive intervention to prevent the ischemia/reperfusion injury in high-risk patients, and restoration of oxidative high-energy phosphate synthesis as judged by a normalizing pHi. As an approach to preventing intramucosal acidosis and ischemic gut mucosal injury, we suggest the following goals: (a) increase global oxygen delivery, (b) increase splanchnic flow, (c) affect ischemia/reperfusion injury and stop the cytokine cascade before it starts, and (d) judge reversal of ischemia and anaerobic metabolism by restoration of normal pHi or PCO2 gap
(9,19,32,33,34,67,68,69).To increase global oxygen delivery, ensure adequate volume resuscitation with isotonic fluids, albumin solutions, and red blood cells. Avoid α agents, which cause splanchnic vasoconstriction. This also means “tolerating” a lower mean arterial pressure, perhaps 60 mm Hg if there is satisfactory end-organ perfusion. Use splanchnic sparing inotropes like dobutamine and isoproterenol and vasodilators such as nicardipine, nitroglycerin, nitroprusside, prostaglandin E, or prostacyclin to increase splanchnic flow (38,70,71,72,73). Reperfusion injury can be attenuated by blocking free radical generation with folate or allopurinol and administering free radical scavengers such as albumin, mannitol, vitamin C, vitamin A, and vitamin E (74,75,76). Injury related to PLA2
activity may be ameliorated by quinacrine, lidocaine, allopurinol, and steroids (34,77,78,79). Moreover, vitamin C, and vitamin E stabilize cell membranes and prevent increased capillary permeability.Glutamine has been implicated as sustaining mucosal architecture and function by scavenging free radicals and preventing lipid peroxidation. In addition, glutamine combines with acetyl cystine to form glutathione (80). In the reaction catalyzed by the selenium-containing enzyme glutathione peroxidase, glutathione is transformed to oxidized glutathione. This then combines with hydrogen
peroxide and degrades it to water, preventing hydrogen peroxide from reacting with superoxide to produce a hydroxyl radical. N-acetyl cystine has been reported to favorably affect indirect indicators of tissue oxygenation (81), perhaps because it is a precursor of glutathione.P.946Hydrocortisone has been implicated in decreasing cytokine release from primed macrophages. Occasionally patients have an inadequate steroid response to stress and an appropriate daily stress dose of glucocorticoid (e.g., 300 mg of hydrocortisone) should be administered. Annane et al. showed a significant reduction in mortality from 73% to 63% in patients with septic shock and adrenal insufficiency who were given low-dose hydrocortisone and fludrocortisone (82). Polymyxin B avidly binds endotoxin; in fact, it is used in industry to clear endotoxin during production of various medical devices. Finally, albumin is another free radical scavenger and may have a place in trauma resuscitation if prior therapy can prevent increased capillary permeability. A solution of 5% albumin would then be an effective plasma volume expander while binding free radicals. Albumin has recently been shown to be as safe as saline in a large heterogeneous ICU population (6,997 patients), and other investigators have demonstrated improvement in organ function in specific patient populations such as hypoalbuminemic patients and patients with acute lung injury or ARDS (83,84,85). The iron-dependent reactions can be blocked by deferoxamine, a chelating agent; however, unless it forms a complex with hydroxyethyl starch, its duration of action is too short and its incidence of hypotension has been too great to justify use in patients (34,86,87). Activated protein C (APC) has also been proposed to reduce absolute mortality by 6.1% in severely ill patients in septic shock in an attempt to stop parts of the inflammatory cascade before it starts. APC exerts its effect by modulating the systemic inflammatory response, inhibiting production of TNF-α, interleukin-1, and interleukin-6 (88).Future InvestigationsInvestigators have considered serum lactate levels to be a cellular marker of oxygen debt in patients with sepsis. Serum lactate, however, may not be a reliable marker of hypoxia because it represents the net effect of production and elimination. Its level may be elevated in conditions associated with either increased lactate production or decreased clearance (i.e., sepsis associated with liver failure). Furthermore, the serum lactate level represents a global index and may not be an optimal measure of the adequacy of regional or microvascular perfusion and may transiently rise during therapeutic maneuvers because of a regional washout phenomenon (89,90). Other metabolic markers include the ATP:ADP ratio and direct plasma measurements of the metabolites resulting from the degradation of adenine nucleotides (e.g., inosine, hypoxanthine, xanthine, and uric acid) (21,91). Direct measurements of tissue pH can be made with pH microprobes placed in the intestinal mucosa. This technique is invasive and is limited by local tissue artifact, electrode artifact, and an inability to recalibrate the electrode in vivo, and, therefore, is not applicable clinically (46,91).Although results of gastric tonometry have been promising and suggestive of improved outcomes in critically ill patients, its practicality in today's ICU remains poor. Sublingual capnometry (when made available again after the recall in 2004) has good potential as an efficient and effective monitor of “splanchnic” tissue. Although pHi and PCO2 monitoring has been tested in several
clinical applications, several fundamental questions remain: Is the PCO2 gap a better predictor than
slPCO2 for development of MSOF and mortality? What are the normal and abnormal values?
Should slPCO2 be used to initiate therapy, represent an end point, or possibly both? The available
data suggest that intervention to prevent the ischemia/reperfusion injury should not wait for an abnormal pHi. Restoration of a normal pHi could be valuable as a marker for the restoration of oxidative metabolism. It is likely that sublingual capnometry will be used to assess organ preservation and function, as an early prognostic sign for shock states, or for the timely detection of catastrophic complications like pancreatic necrosis, anastomotic leaks, or ischemic bowel and will offer accurate information when the normal markers of resuscitation become unreliable. Sublingual capnometry may be helpful in decisions to both initiate therapy and halt resuscitation at a more appropriate end point. In addition, as the existing technology improves, continuous sublingual
monitoring may also become feasible, offering real-time monitoring of “splanchnic” tissue perfusion. In addition, much work is also needed to further determine the expansion of replacement steroids in septic shock to other critically ill patients. Duration of therapy, optimal dosage, and its role in the setting of hypoalbuminemia have yet to be determined.


























![SHOCK[1] - Hypovolemic Shock](https://img.pdfslide.us/doc/110x75/58edc1bc1a28abae538b4711/shock1-hypovolemic-shock.jpg)
