Embed Size (px)
Citation preview

Shift from Rh-positive to Rh-negative phenotypecaused by a somatic mutation within the RHD genein a patient with chronic myelocytic leukaemia
BAYA CHERIF-ZAHAR,1 VIVIANE BO NY,1 RUDI ST EFFENSEN,2 PIE RRE GANE,1 VIRGINIE RAYNAL,1
DOMINIQUE GOOS ENS,1 JENS SKAANING LAURSE N,3 KIM VARMING,2 CASPER JERSIL D2
AND JEAN-PIERRE CARTRON1
1INSERM U76, Institut National de la Transfusion Sanguine, Paris, France, and 2Regional Centre for Blood Transfusionand Clinical Immunology, and 3Haematology Department, Aalborg Hospital, Aalborg, Denmark
Received 24 February 1998; accepted for publication 15 June 1998
Summary. We report a female patient whose Rh phenotypeshifted from RhD-positive to RhD-negative over a 3-yearperiod (1991–94), during which time she was treated withmastectomy (1992) and local irradiation for a low-graderecurrent breast cancer. She was diagnosed with chronicmyeloid leukaemia in 1994, and has since then receivedchemotherapy. The patient was repeatedly typed as O,RhD-positive between 1965 and 1991 and was repeatedlyfound RhD-negative after 1994. Bcr-Abl transcripts typicalof Ph1 chromosome were detected. Molecular analysisindicated that the patient was heterozygous at the RHlocus, carrying one haplotype in which the RHD geneexhibited a single nucleotide deletion (G600) resulting in a
frameshift and premature stop codon, and a normal RHCEgene (allele Ce). The second haplotype contained only theRHCE gene (allele ce) and was normal. Further analysiscarried out on total leucocytes, purified neutrophils, EBV-lymphoblastoid cell line and cultured erythroblasts indi-cated that the G600 deletion was restricted to the myeloidlineage. No modification of other blood group antigenscould be detected. These findings suggest a somaticmutation which most probably occurred in a stem cellcommon to the myeloid lineage.
Keywords: CML, RH locus, loss of D antigen, stem cellmutation, blood groups.
Abnormal expression of blood group antigens with diseasehas been recognized for a long time. The first examplereported concerned the ABH system and associated antigenchanges in haematological disorders such as leukaemia andmyeloproliferative disorders (for reviews see Salmon et al,1969; Garratty, 1977), and in solid tumours (Hakomori &Young, 1978; Hakomori, 1981; Hakomori & Kannagi,1983). Less frequently, Rh blood group changes, character-ized by the presence of two populations of red cells of differentRh phenotype (Rh mosaicism) in the blood from patientssuffering from acute and chronic myelogenous leukaemia(AML, CML), myeloid metaplasia, polycythaemia or myelo-fibrosis, have been described (Tovey et al, 1961; Leven et al,1964; Majsky, 1967; Mannoni et al, 1970; Callender et al,1971; Habibi et al, 1974; Fisher et al, 1984; van Brockstaeleet al, 1986). In a CML patient, both the RH and MNS lociwere affected (Bracey et al, 1983). On several occasions there
was a complete loss of Rh antigens (Marsh et al, 1974, 1980;Cooper et al, 1979; Garner et al, 1980; Mohandas et al, 1993;Mertens et al, 1997). Although in some cases there was anassociation of the Rh loss with chromosome aberrations(Marsh et al, 1974; Cooper et al, 1979; Mohandas et al,1993), no detectable abnormality of chromosome 1, wherethe RH locus is located (1p34-p36), was noticed in otherinstances. In these examples the Rh mosaicism mostprobably resulted in the expansion of an abnormal clone ofstem cells (somatic mutation, monosomy for RH?), whichoccasionally disappeared during clinical remission with areturn to a normal Rh phenotype (Bracey et al, 1983;Mohandas et al, 1993). However, it is not clear whether thesechanges in Rh blood group expression are caused by theleukaemic process itself. Rh mosaicism, was also found inapparently healthy individuals in whom chimaerism ordispermia could be eliminated as a possible explanation(Race & Sanger, 1975; Mertens et al, 1997; Salaru & Lay,1985). In one case a somatic mutation affecting only one ofthe monozygotic twins was suspected (Muller et al, 1978).
British Journal of Haematology, 1998, 102, 1263–1270
1263q 1998 Blackwell Science Ltd
Correspondence: Dr Jean-Pierre Cartron, INSERM U76, InstitutNational de la Transfusion Sanguine, 75739 Paris cedex 15, France.

In a healthy donor and a patient suffering from a non-haematological disease (prolapse of an invertebral disc),respectively, a mosaicism for the blood group RH and FYlocus (chromosome 1q) was noticed (Jenkins & Marsh,1965; Northoff et al, 1984).
The molecular changes of blood group ABH andassociated antigens were best investigated in carcinomas(Hakomori, 1995), but the alterations, if any, of the primarygene products, the glycosyltransferases, are still unknown.Similarly, there is currently no information availableregarding the molecular alterations causing Rh bloodgroup changes in malignant diseases, although the mole-cular basis of the RH genes has been largely determined (forreviews see Cartron & Agre, 1993; Anstee & Tanner, 1993;Cartron, 1994).
In this report we show that the loss of RhD antigen in apatient suffering a chronic myeloid leukaemia resulted froma somatic mutation within the RHD gene (single nucleotidedeletion) which affected the erythroid but not the lymphoidlineage.
METHODS
Blood samples. A blood sample from the patient was takenat the Aalborg Hospital (Denmark) and sent to Paris foranalysis in June 1994. After informed consent, a B-lymphoblastoid cell line was derived from the patient, aspreviously described (Goossens et al, 1987). Blood samplesfrom common RhD-positive (DCCee and DCcee) andRhD-negative (ddccee and ddCee) phenotypes were obtainedfrom the Institut National de la Transfusion Sanguine,Paris.
Flow cytometry. Immunostaining of intact red cells wascarried out as described (Tournamille et al, 1995), usingmurine monoclonal antibodies directed against CD47 (MAb
6H9, donated by Dr M. Telen, Durham, N.C.), LW (BS46,donated by Dr H. H. Sonneborn, Dreireich, Germany) and theRh50 glycoprotein (2D10, gift of Dr A. vom dem Borne,Amsterdam, The Netherlands). Fluorescein-conjugatedF(ab0)2 fragments of goat anti-mouse IgG (Immunotech,Marseille, France) were used and the mean fluorescenceintensity was determined with a FACScan flow cytometer(Becton Dickinson, San Jose, Calif.). Determination ofantigen site densities was carried out with QIFIKIT micro-beads coated with variable numbers of mouse Ig molecules(Biocytex, Marseille, France).
Southern blot analysis. Human genomic DNA extractedfrom peripheral leucocytes was digested with HindIIIrestriction enzyme (10 U/mg DNA), resolved by electro-phoresis in 0·8% agarose gel and transferred by Southerntechnique to a Zeta probe GT nylon membrane (Biorad,Richmond, Calif.), as previously described (Southern,1975). Hybridization with the RhIXb cDNA probe(Cherif-Zahar et al, 1990) (106 cpm/ml) was performedfor 16 h at 658C in 7% sodium dodecyl sulphate (SDS),0·5 M NaHPO4. Final washes were performed at 658C for45 min in 5% SDS, 40 mM NaHPO4 and for 30 min in 1%SDS, 40 mM NaHPO4.
Two-phase liquid culture of erythroid progenitors. Mono-nuclear cells of the peripheral blood from the patient wereseparated by Ficoll-Paque density gradient centrifugation(Pharmacia, Uppsala, Sweden) and cultured in a two-phaseliquid culture system as described (Fibach et al, 1989, 1991;Wada et al, 1990), with some modifications as follows. TheEpo-independent phase was performed at a density of 106
cells/ml in Iscove’s modified Dulbecco medium (IMDM,GIBCO BRL, Eragny, France) supplemented with 10% fetalcalf serum (FCS, GIBCO), 50 ng stem cell factor (PeproTech.Inc., Rock Hill, N.J.), 2 ng/ml recombinant IL-3 (PeproTech),and 1 mg/ml cyclosporin A for 6 d at 378C in a 5% CO2
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 1263–1270
1264 Baya Cherif-Zahar et al
Table I. Sequence and position of primers.
Primers Nucleotide sequence* Position (nt)† PCR products (bp)
cDNA amplificationD 1456
J (sense) 50-GCACAGAGACGGACACAG-30 ¹19 to ¹2P (antisense) 50-ATGGTGAGATTCTCCTC-30 1437 to 1421
CE 1400J (sense) 50-GCACAGAGACGGACACAG-30 ¹19 to ¹2N (antisense) 50-CTGACCTTGTTTCATTATAC-30 1381 to 1362
DNA amplification (D-specific)Exon 4 to exon 5 728
P6 (sense) 50-CATGAACATGATGCACA-30 498 to 514P7 (antisense) 50-CTTGCTGATCTTCCCTT-30 801 to 785
PCR-ASP (intron 3 to exon 4) 773p11 (sense) 50-AGCCTGAGCAACATAGCA-30 Intron 3P14 (antisense) 50-TGGGTATCGTTGCTGTC-30 616 to 600PIJ (antisense) 50-TGGGTATCGTTGCTGTTG-30
* D-specific positions are indicated in bold characters.† nt þ1 is the A of the ATG inititation codon of the cDNA.

1265RhD Loss in CML
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 1263–1270
atmosphere. The Epo-dependent phase was performed byreculture of non-phagocytic cells (0·5–1 × 106 cells/ml) inIMDM containing 30% FCS, 1% deionized BSA, 10·5 mol/lmercaptoethanol, 1·5 mmol/l glutamine, 300 mg/ml iron-saturated transferrin and 2 U/ml human recombinant Epo(INTS Paris, France) for 8–10 d at 378C in a 5% CO2 and 5%O2 atmosphere.
Erythroid maturation in the culture was monitored byflow cytometry (FacScan, Becton Dickinson) using aphycoerythrin-conjugated murine monoclonal antibody toglycophorin A (GPA) and thiazole orange (TO) staining(Retic-COUNT, Becton Dickinson). Dead cells and debris wereexcluded by setting a gate on a FSC v SSC dot plot. Threegates were set by analysis GPA v TO staining: GPAþTO¹
(mature red cells), GPAþTOþ (reticulocytes) and GPAþTOþþ
(nucleated cells).Reverse transcription coupled with PCR amplification. Reti-
culocyte RNA from 30 ml of peripheral blood was extractedby selectively lysing red cells with the Orskov reaction(Gossens & Kan, 1981). 1 mg RNA was reverse transcribed ina total volume of 33 ml using the First Strand cDNA synthesiskit (Pharmacia) following the manufacturer’s instructions.5 ml cDNA products were then subjected to PCR in 50 mM
KC1, 10 mM Tris (pH 8·3), 1·5 mM MgCl2, 0·01% gelatin,0·2 mM of the four dNTPs, 50 pmol of each primer and2·5 units of Taq polymerase (Perkin-Elmer-Cetus, Norwalk,U.S.A). Primers used are described in Table I. PCR conditionswere: denaturation 5 min at 948C (first cycle) and 1 min at948C, annealing 1 min at 558C, extension 1 min 30 s at728C, for 30 cycles. Relevant PCR fragments were purified ona 1% low melting point agarose gel followed by a WizardTM
PCR preps minicolumns (Promega, Madison, Wis.) andsubcloned into a PCRTMII vector using the TA cloning kit(Invitrogen, The Netherlands).
Genomic DNA analysis. PCR amplification was performedon genomic DNA extracted from total leucocytes or from apure neutrophil preparation isolated from peripheral blood,and from the cultures of erythroid progenitors of the patient.Initial analysis of RH genes was performed in Aalborg usingsequence specific primers for Rhc and RhD (Bennett et al,1993; Le Van Kim et al, 1994). A 728 bp fragment,encompassing exon 4 to exon 5 sequences of the RHDgene, was obtained using primers P6 and P7 (Table I) after30 cycles as follows: 1 min at 948C, 30 s at 508C and 30 s at728C. The PCR product was purified through a microconultrafiltration membrane (Amicon) and cloned into aPCRTMII vector.
DNA sequencing. Sequencing was carried out on anautomated ALF express sequencer (Pharmacia) using theThermo Sequence sequencing kit (Amersham International,Bucks., U.K.) following the manufacturer’s instructions.
Philadelphia chromosome analysis. This was performed inApril 1994 by Southern blot analysis using the specific probe(phl-bcr3) distributed by Oncogene Science Inc. (New York,U.S.A.). Briefly, BglII genomic fragments of 4·8, 2·3 and1·1 kb were detected in addition to one or two additionalbands, as seen in a large number of CML patients. Repeatanalysis for Philadelphia (Ph1) chromosome was performedin September 1997 by a multiplex PCR assay with cDNAs
reverse transcribed from peripheral blood leucocyte RNAsused as template, as described (Cross et al, 1994).
RESULTS
Case historyThe patient, a 69-year-old Caucasian woman, wasadmitted to her local hospital in 1979 for treatment ofcarcinoma of the right breast with mastectomy. The resultof routine blood group determination performed in Aalborgwas O, c þ, D þ, E¹ (RhD-positive). In 1989 a localrecurrence of the breast cancer was treated with surgery.In 1991 the patient was admitted to the out-patient clinic,Oncology Department, of Aalborg Hospital, where theblood group was determined to be O, RhD-positive. In 1992she was admitted to local hospital, when carcinoma of theleft breast was diagnosed and treated with mastectomy.Both tumours were evaluated to be low-grade malignantand the patient received local irradiation (4000 r). In 1994she was admitted to local hospital with a diagnosis of CMLo.p., and transferred to the Department of Haematology,Aalborg Hospital, for verification of diagnosis and treat-ment. Investigation of marrow aspirate and peripheralblood confirmed the diagnosis of CML. Blood groupdetermination showed the patient to be O, RhD-negative.Further serological Rh phenotyping showed red cellsreacting as follows: C þ, c þ, E¹, eþ. Chromosome analysiswas unsuccessful due to lack of detectable metaphases inPHA-stimulated bone marrow aspirate. A normal karyo-type: 46,XX was detected in peripheral blood leucocytes(PBL), but no prophases were analysed. Philadelphiachromosome abnormality was initially detected in April1994 by Southern blot and was confirmed in September1997 by multiplex PCR analysis of mRNA transcripts,which showed the presence of a b3a2 (p210) BCR-ABLtranscript, the most common chromosome abnormalityfound in CML patients. Treatment of CML was initiated inMarch 1994 with 1000 mg/d hydroxyurea and hascontinued at doses of 1500–2000 mg/d. In addition, thepatient has received antineoplastic treatment with oestro-gen inhibitors (Tamoxifen, 30 mg/d). The patient has neverreceived any transfusions. It was not possible to performmore extensive family studies: the patient has no childrenand both parents are deceased. One older brother wasunwilling to donate.
Cell surface expression of the proteins from the Rh membranecomplexA red cell sample from the patient was analysed by flowcytometry with MAbs specific for Rh (D, C, c, E and e) and LWantigens, as well as MAbs directed against Rh50 and CD47(Table II). The C, c and e antigens were normally expressed ascompared to the RhD-positive (DCCee) and RhD-negative(ddCcee) controls (Table II). There was no reactivity witheither the anti-E or anti-D antibodies, confirming theserological types obtained in Aalborg. The D antigen wasnot detectable by the antiglobulin test. However, a very weakpositive adsorption-elution of anti-D was found. Interestingly,the number of LW antigen sites on the patient’s red cells was

lower than those on RhD-positive cells and corresponded tothe amount normally found on RhD-negative cells (Table II).The Rh-related proteins Rh50 and CD47 were present insimilar amounts as compared to controls. Serological typingfor other blood group antigens showed the followingphenotype: MNSs, P1(þ), Lu(a¹b þ), K¹k þ, Kp(a¹bþ),Le(a¹b þ), Fy(a þb þ), Jk(a þ b þ), Vel(þ), Ge(þ). Strengthsof reactions were similar to the positive control cells, and nomixed field reactions were observed.
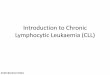
Southern blot analysis of the RH genesThe complete absence of RhD antigen expression on thepatient’s red cells may have resulted from some alteration ofthe RHD gene. To test this hypothesis, genomic DNAextracted from an EBV-lymphoblastoid cell line derivedfrom the patient was digested with HindIII and subjected toSouthern blot analysis with the RhIXb cDNA probe (Fig 1).DNA from RhD-positive and RhD-negative donors wereincluded as controls. The hybridization pattern of the patientsample was identical to that of common RhD-positivecontrols, as shown by the presence of bands at 7·5 and2·7 kb, which were absent from the RhD-negative samples.These findings indicate that the RH locus from the patientwas composed of the two RH genes, D and CE, as opposed tothat of Caucasian RhD-negative individuals which is made ofa single gene, CE (Colin et al, 1991).
These results also indicated that the loss of the D antigenwas not associated with either a gross deletion or arearrangement of the RHD gene. Moreover, the results (Fig1) showed a 1:2 gene dosage effect between some D and CEspecific restriction fragments (Cherif-Zahar et al, 1993),indicating that the patient was heterozygous (Dd) for the Dgene, with one chromosome carrying the D and CE genes (‘Dhaplotype’), and the other carrying only the CE gene (‘dhaplotype’). Similar results were obtained by Southernanalysis of BamHI and EcoRI digests (not shown). Theprobable genotype of the patient is DCe/dce, but this couldnot be confirmed by family studies (see above).
Rh transcripts analysisReticulocyte RNA isolated from the patient was reversetranscribed and the D and CE cDNAs were amplified using J-P
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 1263–1270
1266 Baya Cherif-Zahar et al
Fig 1. Southern blot analysis of the RH locus from the patient. DNAfrom the patient, RhD-positive (DDCCee and DdCcee), homozygousand heterozygous for the RHD gene, respectively, and RhD-negative(ddccee) donors was digested with HindIII restriction enzyme andanalysed on a Southern blot with the RhIXb cDNA probe. Genedosage effect was estimated by determination of the relative intensityof the 2·7/2·5 kb fragments corresponding to the exon 1 of the RHDand RHCE genes, respectively.
Table II. Basic characteristics of the patient sample.
Antigens and protein expression
Rh*
Sample D C c E e Rh50† CD47† LW†
Patient 8 203 218 7 95 135 38 1
ControlsDCCee 453 191 192 6 78 112 24 2·5ddCcee 6 254 211 5 99 116 24 1·1
* Mean fluorescence intensity (arbitrary values).† Molecules/cell × 10¹3.

1267RhD Loss in CML
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 1263–1270
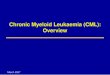
and J-N primer pairs, respectively (Table I). PCR products ofthe expected sizes (1456 and 1400 bp for D and CE,respectively) were cloned into PCRTMII plasmid andsequenced. Sequence analysis of the CE transcripts indicatedthe presence of the ce and Ce alleles, with no alteration. Incontrast, a single base deletion of a guanine (G) located at nt600 (hereafter called G600) was detected in the D cDNA (Fig2). This deletion introduced a frameshift after the glutaminecodon at position 200 and resulted in a premature stopcodon at nt 682–684 (Fig 2). The predicted size of the Dprotein from the patient, if translated, would be muchshorter (227 residues) as compared to the normal D proteinwhich comprises 417 residues.
Lymphocyte and erythroblast cells analysisThe region containing the G600 deletion is comprisedwithin exon 4 of the D gene. To confirm the presence of thismutation at the genomic level, we used a DNA preparationfrom the EBV-transformed lymphoblastoid cell line derivedfrom the patient. The fragment surrounding the G600deletion was amplified with the P6 (exon 4) and P7 (exon5) primers (Table I). A 728 bp amplified fragment,encompassing exon 4 to exon 5 of the RHD gene, wascloned and sequenced. Surprisingly, no mutation wasfound in the exon 4 sequence of the RHD gene. There was,therefore, a discordance in these results, since the G600deletion was present only in the D transcripts from
reticulocytes and not in the D gene from the lymphoidcell line. The possibility of a somatic mutation in themyeloid compartment was raised.
This issue was addressed by studying the genomic DNAfrom erythroid cells derived from the patient in a two-phaseliquid culture system supporting the proliferation anddifferentiation of erythroid progenitors present in theperipheral blood (see Methods). After 8 d of culture in thesecond phase (Epo-dependent), the cell population analysedfor GPA and TO staining consisted of 12% GPAþTOþþ
(erythroblasts), 12% GPAþTOþ cells (reticulocytes), 1%GPAþTO¹ cells (red cells) and 75% GPA¹ cells (non-erythroid). DNA and RNA were extracted from culturederythroblasts (see Methods) and the genomic fragmentsurrounding the G600 deletion was amplified with theP6–P7 primer pair (see above). A PCR product of 728 bp wasobtained, inserted into PCRTMII plasmid and sequenced. TheG600 deletion was present in three of the four clonesanalysed. Parallel analysis of the mRNA (see above) fromcultured erythroblasts confirmed the presence of the G600deletion in some D transcripts.
PCR amplification with allele-specific primers (PCR-ASP)To determine whether the G600 deletion was specific to theerythroid lineage, allele-specific PCR was performed usingthe D-specific primers P11 and P14 and primer PIJ, specificto the mutant allele from the patient (see Table I). PCR
Fig 2. Sequence analysis of the RhD transcripts from the patient. Nucleotide sequence surrounding position 600 and inferred amino acidsequence. Top: sequencing of the RhD cDNA revealed a G deletion (arrow) at position 600 in the patient as compared to control (C). Bottom: the Gnucleotide deletion in the patient caused a frameshift resulting in a new amino-acid extension (shown in bold). Star indicates a premature stopcodon.

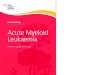
amplifications were carried out on DNA templates extractedfrom total leucocytes or from a purified neutrophil prepara-tion, as well as from erythroblast cultures and the EBV-transformed B lymphocytes from the patient (Fig 3).Genomic DNA extracted from peripheral blood leucocytesof RhD-positive and RhD-negative donors were used ascontrols. The wild-type D allele amplified with the primerpair P11–P14 (773 bp) was identified in the D-positive butnot the D-negative sample, as expected (Fig 3). A band of773 bp was also present in the patient’s blood and B cells. Inthe purified neutrophils only a very weak amplificationproduct was detected. In the cultured erythroblasts a band of773 bp was also detectable which presumably arose from thepresence of non-erythroid cells in the preparation (see above)or from some non-mutated erythroid cells. This wouldcorrelate with the weak positive absorption-elution of anti-Dfrom red cells of this patient (see above).
The mutant allele generated with the primer pair P11–PIJappeared as a strong band of 773 bp in the samples of bloodleucocytes, purified neutrophils and cultured erythroblastsfrom the patient but not in the RhD-positive and RhD-negative controls nor in the B-cell line sample from thepatient. This result substantiates that the G600 deletion wasspecific to the myeloid lineage.
DISCUSSION
We have studied a female patient whose Rh phenotypeshifted from RhD-positive to RhD-negative over a 3-yearperiod (1991–94), during which time she was treated withmastectomy (1992) and local irradiation for a low-graderecurrent breast cancer, and was then diagnosed as CML in1994 for which she received chemotherapy (hydroxyureaand tamoxifen), but was never transfused.
Total loss of RhD antigen in malignant haemopathies isextremely rare and molecular information on the bloodgroup changes of these patients is lacking. Southern blotanalysis using a Rh-specific probe showed that the patientwas heterozygous for the RHD gene and there was no grossrearrangement of the RH locus. Sequence analysis of the Rhtranscripts amplified from the patient’s reticulocytes revealeda single nucleotide deletion (G600), localized in a region
encoded by exon 4 of the RHD gene, whereas other transcriptswere normal. This mutation introduced a frameshift and ledto a premature stop codon at position 682–684. If translated,the truncated mutant protein would encode a polypeptide of227 residues, including a C-terminus with 27 new residues.However, since the D antigen is not detectable on native redcells, either the mutant transcript or the truncated proteinmight be degraded within the cells. Thus, the absence of theRhD polypeptide on red cells from this patient resulted in a‘Rh-negative’ phenotype, consistent with the serologicalresults (see above). Single nucleotide deletion in the RHDgene coding region is an extremely rare type of mutation sincethe only other example yet found concerned a family from aRhnull patient of the amorph type (Cherif-Zahar et al, 1998).However, after this study was completed, a healthy individualexpressing the Rh phenotype dCCee who carries an intactRHD gene with a nonsense mutation altering codon 41(Gln41→ter) identified only by sequencing reticulocyte Rhtranscripts was described (Avent et al, 1997). However,genomic analysis of other haemopoietic cell lines and offamily members of this donor were not carried out todetermine whether the mutation was inherited.
Further, we also demonstrated that the G600 deletionpresent in our patient most probably corresponded to asomatic mutation since it was found in erythroblastsgrown in liquid culture and pure neutrophils from theperipheral blood, but not in a B-lymphoid cell line derivedfrom the patient. This mutation most probably occurred in astem cell common to all myeloid lineages. However, we cannotexclude that this mutation could occur in immature BFU-E,which have a low self-renewal capacity and may still becommitted to other myeloid lineages to some extent (Fauser &Messner, 1978, 1979; Vainchencker et al, 1979). It is alsopossible that in our CML patient the bcr-abl translocationarose in a cell which had already undergone this somaticmutation. Expansion of such abnormal clones) would accountfor the spreading of the mutation in the erythroid compart-ment and the resultant change of the Rh phenotype from D-positive to D-negative. Whether this mutation conferred someproliferative advantage or was related to the leukaemicprocess itself or the treatment received by the patient is atpresent not known.
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 1263–1270
1268 Baya Cherif-Zahar et al
Fig 3. Detection of the mutated RH allele byPCR-ASP. PCR-ASP amplification for thenormal (wild type) RH allele and the mutatedRH allele (G600 deletion) in genomic DNAfrom control doners (C) and the patient.Amplifications with normal and mutatedprimers were performed on DNA extractedfrom the peripheral blood (blood), EBV-transformed B-lymphoblastoid cell line (Bcells), cultured erythroblasts (eryth.) andneutrophils (neutro.) purified from peripheralblood. Size marker (M) is a 100 bp ladder.

1269RhD Loss in CML
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 1263–1270
ACKNOWLEDGMENTS
We thank Giorgio Matassi (INSERM U76, Paris) for criticalreading of the manuscript. This work was supported in partby funds from the Aalborg Frivillige Bloddonorers Fond.
REFERENCES
Anstee, D.J. & Tanner, M.J.A. (1993) Biochemical aspects of theblood group Rh (Rhesus) antigens. Bailliere’s Clinical Haematology,6, 401–422.
Avent, N.D., Martin, P.G., Armstrong-Fisher, S.S., Liu, W., Finning,K.M., Maddocks, D. & Urbaniak, S.J. (1997) Evidence of geneticdiversity underlying Rh D¹, weak D (Du), and partial Dphenotypes as determined by multiplex polymerase chain reactionanalysis of the RHD gene. Blood, 89, 2568–2577.
Bennett, P., Le Van Kim, C., Colin, Y., Warwick, R.M., Cherif-Zahar,B., Fisk, N.M. & Cartron, J.P. (1993) Prenatal determination offetal RhD type by DNA amplification. New England Journal ofMedicine, 329, 607–610.
Bracey, A.W., McGinniss, M.H., Levine, R.M. & Whang-Peng, J.(1983) Rh mosaicism and aberrant MNSs antigen expression in apatient with chronic myelogenous leukemia. American Journal ofClinical Pathology, 79, 397–401.
Callender, S.T., Kay, H.E.M., Lawler, S.D., Millard, R.E., Sanger, R. &Tippett, P.A. (1971) Two populations of Rh groups together withchromosomally abnormal cell lines in the bone marrow. BritishMedical Journal, i, 31–33.
Cartron, J.P. (1994) Defining the Rh blood group antigens;biochemistry and molecular genetics. Blood Reviews, 8, 199–212.
Cartron, J.P. & Agre, P. (1993) Rh blood group antigens: protein andgene structure. Seminars in Hematology, 30, 193–208.
Cherif-Zahar, B., Bloy, C., Le Van Kim, C., Blanchard, D., Bailly, P.,Hermand, P., Salmon, C., Cartron, J.P. & Colin, Y. (1990)Molecular cloning and protein structure of a human bloodgroup Rh polypeptide. Proceedings of the National Academy ofSciences of the United States of America, 87, 6243–6247.
Cherif-Zahar, B., Matassi, G., Raynal, V., Gane, P., Mempel, W.,Perez, C. & Cartron, J.P. (1998) Molecular defects of the RHCEgene in Rh-deficient individuals of the amorph type. Blood, 92,639–646.
Cherif-Zahar, B., Raynal, V., Le Van Kim, C., D’Ambrosio, A.M.,Bailly, P., Cartron, J.P. & Colin, Y. (1993) Structure and expressionof the RH locus in the Rh-deficiency syndrome. Blood, 82, 656–662.
Colin, Y., Cherif-Zahar, B., Le Van Kim, C., Raynal, V., Van Huffel, V. &Cartron, J.P. (1991) Genetic basis of the RhD-positive and RhD-negative blood group polymorphism as determined by Southernblotting. Blood, 78, 2747–2752.
Cooper, B., Tishler, P.V., Atkins, L. & Breg, W.R. (1979) Loss of Rh antigenassociated with acquired Rh antibodies and chromosome transloca-tion in a patient with myeloid metaplasia. Blood, 54, 642–647.
Cross, N.C.P., Melo, J.V., Feng, L. & Goldman, J.M. (1994) Anoptimized multiplex polymerase chain reaction (PCR) for detectionof BCR-ABL fusion mRNAs in hematological disorders. Leukemia,8, 186–189.
Fauser, A.A. & Messner, H.A. (1978) Granulo-erythropoieticcolonies in human bone marrow, peripheral blood and cordblood. Blood, 52, 1243–1248.
Fauser, A.A. & Messner, H.A. (1979) Identification of megakaryo-cytes, macrophages and eosinophils in colonies of human bonemarrow containing neutrophilic granulocytes and erythroblasts.Blood, 53, 1023–1027.
Fibach, E., Manor, D., Oppenheim, A. & Rachmilewitz, E.A. (1989)
Proliferation and maturation of human erythroid progenitors inliquid culture. Blood, 73, 100–103.
Fibach, E., Manor, D., Treves, A. & Rachmilewitz, E.A. (1991)Growth of human normal erythroid progenitors in liquid culture:a comparison with colony growth in semisolid culture. Inter-national Journal of Cell Cloning, 9, 57–64.
Fisher, H.E., Lichtiger, B. & Trujillo, J.M. (1984) Change inexpression of Rho(D) antigen in the case of a secondarypreleukemia. (Abstract). Proceedings of the 18th Congress of theInternational Society of Blood Transfusion and 20th Congress of theInternational Society of Haematology, Munich, p. 162.
Garner, R.J., Rembe, A.M. & Landells, M. (1980) Loss of Rho(D)antigen. (Abstract). Transfusion, 20, 619.
Garratty, G. (1977) ABO blood groups and their relationship todisease. Cellular Antigens and Disease (ed. by G. Garratty), pp. 1–29. American Association of Blood Banks, Bethesda.
Goossens, D., Champomier, G., Rouger, P. & Salmon, C. (1987)Human monoclonal antibodies against blood group antigens.Journal of Immunological Methods, 101, 193–200.
Gossens, M. & Kan, Y.Y. (1981) DNA analysis in the diagnosis ofhemoglobin disorders. Methods in Enzymology, 76, 805–806.
Habibi, B., Lopez, M. & Salmon, C. (1974) Two new cases of Rhmosaicism: selective study of red cell populations. Vox Sanguinis,27, 232–242.
Hakomori, S.I. (1981) Glycosphingolipids in cellular interaction,differentiation, and oncogenesis. Annual Review of Biochemistry,50, 733–764.
Hakomori, S.I. (1995) Histo-blood group antigens as tumor-associated carbohydrate antigens and ligands for cell adhesion.Blood Cell Biochemistry, Vol. 6. Molecular Basis of Major HumanBlood Group Antigens (ed. by J. P. Cartron and P. Rouger), pp. 421–443. Plenum Press, New York.
Hakomori, S.I. & Kannagi, R. (1983) Glycosphingolipids as tumor-associated and differentiation markers. Journal of the NationalCancer Institute, 71, 231–251.
Hakomori, S.I. & Young, W.W. (1978) Tumor-associated glycolipidantigens and modified blood group antigens. Scandinavian Journalof Immunology, 7, 97–117.
Jenkins, W.J. & Marsh, W.L. (1965) Somatic mutation affecting theRhesus and Duffy blood group systems. Transfusion, 5, 6–10.
Levan, A., Nichols, W.W. & Hal, B. (1964) Mixture of Rh positive andRh negative erythrocytes and chromosomal abnormalities in acase of polycythemia. Hereditas, 52, 89–105.
Le Van Kim, C., Mouro, I., Brossard, Y., Chavine, J., Cartron, J.P. &Colin, Y. (1994) PCR-based determination of the Rhc and RhEstatus of fetuses at risk of Rhc and RhE haemolytic disease. BritishJournal of Haematology, 88, 193–195.
Majsky, A. (1967) Some cases of leukaemia with modifications of theD(Rho)-receptor. Neoplasma, 14, 335–344.
Mannoni, P., Brack, C., Yvart, J. & Salmon, C. (1970) Anomalie defonctionnement du locus Rh au cours d’une myelofibrose. NouvelleRevue Francaise d’Hematologie, 10, 381–388.
Marsh, W.L., Chaganti, R.S.K., Gardner, F.H., Mayer, K., Nowell, P.C.& German, J. (1974) Mapping human autosomes: evidencesupporting assignment of rhesus to the short arm of chromosomeno.1. Science, 183, 966–968.
Marsh, W.L., Johnson, C.L., DiNapoli, J., Oyen, R., Shraft, W.,Hiranandani, J., Jimenez, P. & Jimenez, M. (1980) Two cases ofacquired in vivo change in red cell Rh. (Abstract). Transfusion, 20,619–620.
Mertens, G., Gielis, M., Muylle, L. & de Raets, S. (1997) Loss of D andC expression in chronic myelomonocytic leukemia. Transfusion,37, 880–881.
Mohandas, K., Najfeld, V., Gilbert, H., Azar, P. & Tabrizi, D. (1993)

Loss and reappearance of Rh0(D) antigen in an individual withacute myelogenous leukemia. (Abstract). Transfusion, 33, S85.
Muller, A., Seger, J., Garretta, M., Habibi, B., Lopez, M., De Grouchy,J., Salmon, D. & Salmon, C. (1978) Mosaicisme Rh par mutationdans une gemellite monozygote. Revue Francaise de Transfusion etImmunohematologie, 21, 151–163.
Northoff, H., Goldman, S.F., Lattke, H. & Steinbach, P. (1984)A patient, mosaic for Rh and Fy antigens lacking other signsof chimerism or chromosome disorder. Vox Sanguinis, 47, 164–169.
Race, R.R. & Sanger, R. (1975) The Rh blood groups. Blood Groups inMan (ed. by R. R. Race and R. Sanger), 6th edn. pp. 178–260.Blackwell Scientific Publications, Oxford.
Salaru, N.N.R. & Lay, W.H. (1985) Rh blood group mosaicism in ahealthy elderly woman. Vox Sanguinis, 48, 362–365.
Salmon, C. (1969) A tentative approach to variations in ABH andassociated erythrocyte antigens. Seminars in Hematology, 2, 3–33.
Southern, E. (1975) Detection of specific sequences among DNA
fragments separated by gel electrophoresis. Journal of MolecularBiology, 98, 503–517.
Tournamille, C., Le Van Kim, C., Gane, P., Cartron, J.P. & Colin, Y.(1995) Molecular basis and PCR-DNA typing of the Fya/Fyb bloodgroup polymorphism. Human Genetics, 95, 407–410.
Tovey, G.H., Lockyer, J.W. & Tierney, R.B.H. (1961) Changes in Rhgrouping reactions in a case of leukaemia. Vox Sanguinis, 6, 628–631.
Vainchencker, W., Guichard, J. & Breton-Gorius, J. (1979) Growth ofhuman megakaryocytic colonies in culture from fetal, neonataland adult peripheral blood cells. Blood Cells, 5, 25–42.
Van Brockstaele, D.R., Berneman, Z.N., Muyelle, L., Cole-Dergent, J.& Peetermans, M.C. (1986) Flow cytometric analysis of erythro-cytic D antigen density profile. Vox Sanguinis, 51, 40–46.
Wada, H., Suda, T., Miura, Y., Kajii, E., Ikamoto, S. & Yamata, Y.(1990) Expression of major blood group antigens on humanerythroid cells in a two-phase liquid culture system. Blood, 75,505–511.
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 1263–1270
1270 Baya Cherif-Zahar et al