Embed Size (px)
DESCRIPTION
MED-341: Acute Leukaemia. Professor Abdulkareem Almomen, MD, FRCPC (March 2011). Acute Leukaemia: main subtypes. Acute Myeloid Leukemia (AML) Acute Lymphoblastic Leukemia (ALL) Biphenotypic Acute Leukemia (BAL): My + Ly. Proliferation + differentiation block / maturation arrest. - PowerPoint PPT Presentation
Citation preview

MED-341: Acute Leukaemia
Professor Abdulkareem Almomen, MD, FRCPC(March 2011)

– Acute Myeloid Leukemia (AML)
– Acute Lymphoblastic Leukemia (ALL)
– Biphenotypic Acute Leukemia (BAL): My + Ly
Acute Leukaemia: main subtypes

• Clonal expansion of myeloid blasts in blood marrow
(BM), peripheral blood (PB) or other tissue
• Minimum threshold of blast cells for defining AML (BM):– >20% blasts
AML: definition / concept
Proliferation + differentiation block / maturation arrest

Maturation arrest

Maturation arrest

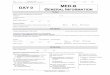
Normal Bone Marrow: Cell Heterogeneity

BM in AML: Monomorphous Cell Appearance

AML5a
AML4-eos

• Incidence: 2 - 3 pts /100.000 inhab - year
• Overall: 1.2% (US)
• Lineal increase with age:
<35: < 1 /100.000 inhab - year >65: >10 /100.000 inhab - year
• Median age: 60 - 70 year-old
• Not apparent increase during last years
AML: epidemiology

• Bone marrow failure – Anemia– Neutropenia– Thrombocytopenia
• Extramedullary involvement (skin, gums, CNS, other)
• Proliferative symptoms
• Coagulopathy
• Leukostasis
• Metabolic disorders (tumor lysis syndrome)
AML: clinical presentation

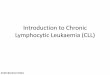
AML: skin infiltration (granulocytic sarcoma)

AML: gums (gingival) infiltration

Acute Myeloid Leukemia (AML)

• Cytology– PB – BM (BM aspirate ± BM biopsy)
• Cytochemistry– MPO (myeloperoxidase) & Sudan Black B (SBB) – Myeloid origin
– Non-specific esterase (NSE): -naphthyl acetate (ANA), -naphthyl butyrate (ANB) – Monocytic origin
• Inmunophenotype– Hematopoietic precursors: CD34, HLA-DR, CD45– My Ag: CD13, CD33, CD15, MPO, CD117– Megakaryoblastic Ag: CD41, CD61
• Cytogenetics• Molecular biology
– Fusion transcripts (RT-PCR): PML/RAR-, AML1/ETO, CBF-/MYH11, MLL/..., BCR/ABL, DEK/CAN)
– New mutations with prognostic impact: flt-3-ITD, CEBPalfa, NPM, …
AML - diagnosis:


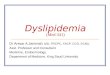
AML – Auer rod

MPO
Naphtol-As-D-acetate esterase -naphthyl acetate esterase
AML : Cytochemistry

CD
56 P
E
100 101 102 103 104
CD2 FITC
10
01
01
10
21
03
10
4
NG
2 P
E
100 101 102 103 104
CD34 FITC
10
01
01
10
21
03
10
4
CD
14 P
E
100 101 102 103 104
CD123 FITC
10
01
01
10
21
03
10
4
AML : Flow cytometry

AML: Cytogenetics

Acute Promyelocytic Leukemia (APL, M3)
bcr1 bcr3
RT-PCR PML/RAR-alpha
FISH: PML/RARA fusion signal
Anti-PGM3 pattern staining

• Minimally differentiated (M0)
• AML w/o maturation (M1)
• AML with maturation (M2)
• Promyelocytic (M3)
• Myelomonocytic (M4)
• Monoblastic (M5a)
• Monocytic (M5b)
• Erythroleukemia (M6)
• Acute megakaryoblastic (M7)
FAB classification for AML: lineage/differentiation- based
Granulocytic diff
Monocytic diff


I. AML with recurring genetic abnormalities– AML with t(8;21)(q22;q22) & (AML1/ETO) rearrangement– AML with abn BM eosinophils & inv(16)(p13q22)/t(16;16)(p13;q11) -
CBF/MYH11 rearrangement– Acute promyelocytic leukemia associated to t(15;17)(q22;q11-12) &
PML/RAR- rearr– AML with 11q23 (MLL) abn
II. AML with multilineage dysplasia
III. Therapy-related AML
IV. AML not otherwise categorized
WHO, 2001
WHO classification (AML): towards molecularly-based categories

– Favorable: t(15;17), t(8;21), inv(16)
– Intermediate risk: normal karyotype
– Unfavorable: abn 5 (del/-5), abn 7 (del/-7),
inv(3q)/t(3;3), complex karyotype (≥5 abn),
abn 11q, t(6;9), del(17p)
AML: main cytogenetic abnormalities

AML (non-APL): standard approach
Intensification CT Ara-C HD-based
Post-remission tx
AlloSCT AutoSCT CT
Induccion CT
Anthacycline + Ara-C /…
CR~75%
Long-term OS~35-40% (<60)
Salvage therapy
Refractory
Relapse

Acute Lymphoblastic Leukemia (ALL)

ALL: definition
– Clonal expansion of lymphoid (precursor
lymphoid cells) in blood marrow (BM),
peripheral blood (PB) or other tissue

ALL: main subtypes
– B-cell ALL / precursor B lymphoblastic leukemia
– T-cell ALL / precursor T lymphoblastic leukemia

• Incidence: 2/100.000 (inhab-year) • 3/4 in children
• B-ALL: – 80-85%– Predominance in children– 10% presenting without BM involvement (B-cell
lymphoblastic lymphoma)
• T-ALL:– 15% of children ALL– 25% of adult ALL– Predominance in adolescent / young male pts– Frequent presentation with exclusive extramedullary involvement (T-cell
lymphoblastic lymphoma)
ALL: epidemiology

• Extramedullary involvement– CNS– Mediastinal (T-ALL)– Other (lymph node, testicular, ...)
• B symptoms• Bone marrow failure
• Metabolic disorder
ALL: characteristic clinical features

T-ALL: mediastinal involvement

ALL – FAB1 subtype

ALL – FAB2 subtype

Common B-lineage antigens: HLA-DR, CD19, CD79a,CD22
• Pro-B (B-cell progenitor, B-I): Tdt+, CD10(-), cytIg(-), CD20(-)
• Common (early pre-B, B-II): TdT(+), CD10(+), cytIg(-)
• Pre-B (B-III): Tdt(+), cytIg(+)
• Mature B-ALL (B-IV): Tdt(-), sIg+, CD20(+)
B-ALL: immunological classification

T-ALL/Common Ag: Tdt, CD3cyt, CD7
– Early T-ALL: CD1(-),CD2(-),CD3s(-), CD5(-),CD4(-),
CD8(-)
– Thymic T-ALL: CD1a(+),CD2(+),CD5(+)
– Mature T-ALL: CD1a(-), CD2(+),CD5(+),CD3s(+)
T-ALL: immunological classification

– Favorable: t(12;21),
– Intermediate risk: normal karyotype, t(1;19)
– Unfavorable: t(9;22), 11q23 abn [t(4;11) & other],
hypoploid
ALL: main cytogenetic abnormalities

ALL: current therapeutic approach
Consolidation CT
Post-remission
AlloSCT AutoSCT CT (reinduction & maintenance)
CR: 83%
Induction Antr. / VCR / PDN
L-ASA, ARA-C, CFM
Surv*: 80% (children) 35% (adults)

Imatinib: molecular-targeted therapy for Ph-positive ALL
Goldman et al, Lancet 2000
Y = TyrosineP = Phosphate
Bcr-Abl
ATP
Substrate
PPP
P
Abl: a highly overexpressed tyrosine kinase protein in CML & Ph-pos ALL

Imatinib: molecular-targeted therapy for Ph-positive ALL
Goldman et al, Lancet 2000
Bcr-AblBcr-Abl
ATP
Substrate
PPP
P
Imatinib: blocks abl function by interfering with ATP binding
Y = TyrosineP = Phosphate

Outcome
– Response criteria
• Complete response
• Cytogenetics response
• Molecular response
– Failure: primary refractory, relapse
– …

NCI criteria (Cheson et al, 1999)
1. <5% blasts in BM
2. Absence of extramedullary leukemia
3. Recovery of PB counts (ANC >1 & platelet >100x109/L)
4. Minimum 4-week duration
Definition of CR

CR (morphologic assessment) <5% of BM blast cells
Low sensitivity
Universally applicable
Cytogenetic CR Absence of abnormal metaphases
Low sensitivity
Only in cases with cytogenetic abn
(i.e., Ph-pos)
Molecular response Clearance of molecular marker (bcr/abl, PML/RAR, AML1/ETO,...)
Only in AL with known molecular marker
High sensitivity (1 x 10-5)
Response assessment: types (degree) of response

Morphologic assessment of response
CR Non-CR