Embed Size (px)
Citation preview

Brief Bio: Rose D. Sheats� D.M.D., M.P.H. � Diplomate – American Board of Orthodontics� University of North Carolina Graduate Orthodontic Program Director (retired 2013)
� American Academy of Dental Sleep Medicine� Board of Directors� Associate editor – Journal of Dental Sleep Medicine
Rose D. Sheats, DMD, MPHUniversity of North Carolina (Retired)
Chapel Hill, NC
Topics� Impact of positive airway pressure to manage sleep disordered breathing (SDB) on craniofacial growth
� Orthodontic procedures to manage pediatric SDB� Rapid maxillary expansion� Mandibular advancement devices
� Controversy regarding orthodontic premolar extractions and development of SDB
Positive Airway Pressure (PAP)and Craniofacial GrowthCase reports and small case series of CPAP suggest adverse impact on craniofacial growth in children
BaroneCM et al. (1994). Cleft Palate Craniofac J 31(1): 74-‐77.FaurouxB et al. (2005). Intensive Care Med 31(7):965-‐9.

16 yr 11 mos maleBiPap x 10 yrs• Medical history:
Achondroplasia• Age 6 yr:
adenotonsillectomyfor OSA
• BiPAP initiated for residual OSA
• Pressure increased over time until titrated to max of 28 cm H2O (age 16 yrs)
• Severe maxillary retrusion
Positive Airway Pressure (PAP) and Pediatric Craniofacial Growth� 2014: SD Roberts, University of Washington orthodontic residency thesis
� N = 100 children, Seattle Children’s Hospital Craniofacial Center and Sleep Disorders Center
� nPAP > 2.5 yrs� Compliant(>20 hrs/week, > 6 mos): n = 50, mean age = 10.4 yrs
� Non-‐compliant: n = 50, mean age = 8.5 yrs
Roberts SD et al. (2016). J Clin Sleep Med 12 (4): 469-475.
PAP and Craniofacial Growth & DevelopmentNon-‐compliant PAP Compliant PAP
T1 (dark), T2 (light)Roberts SD et al.(2016). J Clin Sleep Med 12(4): 469-475.
Positive Airway Pressure and Pediatric Craniofacial Growth: Summary� SDB children compliant with PAP demonstrate impaired craniofacial growth, notably deficient maxillary development
� Sleep physicians who prescribe PAP are encouraged to collaborate with orthodontists to monitor growth and development� Discuss alternative treatment options� Have frank discussions about jaw surgery in future
RME & Pediatric Obstructive Sleep Apnea (OSA)• 31 children (8.7 yr) with OSA and crossbite
• AHI* Pre-‐tx = 12.2 (severe)
• Rapid maxillary expansion for 3 weeks
• At 4 months: AHI < 1 (normal) in 100% of patients
• No long-‐term outcomes
*Apnea-‐hypopnea index
Pirelli P, et al. (2004). Sleep 27(4):761-6, Fig 2.
Maxillary AnatomyMidpalatal Suture Maxillary Bone
Bartleby.com: Gray 's Anatomy, Plates 160 and 190. Licensed under Public Domain via Wikimedia Commons -
https://commons.wikimedia.org/wiki/File:Gray160.png#/media/File:Gray160.png
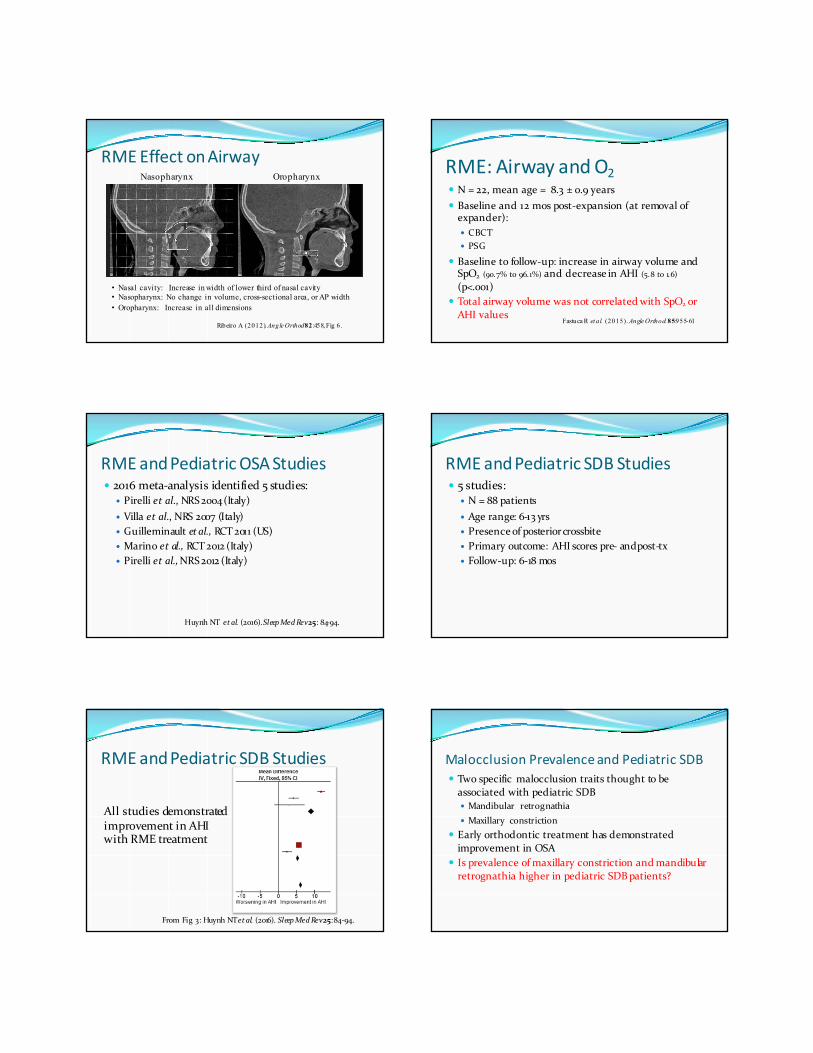
RME Effect on Airway
Ribeiro A (2012). Angle Orthod82 :458, Fig 6.
Nasopharynx Oropharynx
• Nasal cavity: Increase in width of lower third of nasal cavity• Nasopharynx: No change in volume, cross-sectional area, or AP width• Oropharynx: Increase in all dimensions
RME: Airway and O2� N = 22, mean age = 8.3 ± 0.9 years� Baseline and 12 mos post-‐expansion (at removal of expander):� CBCT� PSG
� Baseline to follow-‐up: increase in airway volume and SpO2 (90.7% to 96.1%) and decrease in AHI (5.8 to 1.6) (p<.001)
� Total airway volume was not correlated with SpO2 or AHI values
Fastuca R et al. (2015). Angle Orthod.85:955-61
RME and Pediatric OSA Studies� 2016 meta-‐analysis identified 5 studies:
� Pirelli et al., NRS 2004 (Italy)� Villa et al., NRS 2007 (Italy)� Guilleminault et al., RCT 2011 (US)� Marino et al., RCT 2012 (Italy)� Pirelli et al., NRS 2012 (Italy)
Huynh NT et al. (2016). Sleep Med Rev 25: 84-‐94.
RME and Pediatric SDB Studies� 5 studies:
� N = 88 patients� Age range: 6-‐13 yrs� Presenceof posteriorcrossbite� Primary outcome: AHI scores pre-‐ and post-‐tx� Follow-‐up: 6-‐18 mos
RME and Pediatric SDB Studies
All studies demonstrated improvement in AHI with RME treatment
From Fig 3: Huynh NT et al. (2016). Sleep Med Rev 25: 84-‐94.
Malocclusion Prevalence and Pediatric SDB� Two specific malocclusion traits thought to be associated with pediatric SDB� Mandibular retrognathia� Maxillary constriction
� Early orthodontic treatment has demonstrated improvement in OSA
� Is prevalence of maxillary constriction and mandibular retrognathia higher in pediatric SDB patients?

Pliska B et al. (2017).J Dent Sleep Med 4(2): 41-‐44.� Cohort of children consecutively referred to sleep center for SDB
� N = 90 (5-‐10 yrs old; mean age = 6.8 yrs)� Otolaryngology to assess airway� Orthodontics to identify need for early treatment� Parent report of SDB signs and symptoms
Findings (Total Sample = 90)n (%)
Age in yr (SD) 6.8 (1.29)Female 46 (51%)Parent report
Witnessed apneas 42 (47%)Mouthbreathing 42 (47%)Bruxism 22 (24%)
Class II Canines (n=63) 20 (32%)Overjet > 7 mm(n=63) 3 (5%)Anterior crossbite 5 (6%)Posterior crossbite 14 (16%)
� In pediatric SDB sample, prevalence of mandibular retrognathia and maxillary constriction similar to that of a typical orthodontic population of 6-‐9 year olds
� Referral to orthodontist for early treatment may not be beneficial for majority of pediatric SDB patients evaluated in regional sleep center
Data derived from Pliska B (2017). J Dent Sleep Med 4(2): 41-44, Table 1.
Study Limitations� SDB not confirmed by PSG� Criteria for early orthodontic treatment may have been too restrictive:� OJ > 7 mm� Presence of posterior crossbite
BimaxillaryExpansion (BE) for SDB� Retrospective study (2001-‐2011)� N=45 children (age: 3-‐14 yrs)� Inclusion criteria:
� PSG confirmed OSA pre-‐BE� Treated with maxillary and mandibular expansion� Complete records (including lateral cephs and PSGs)� No other co-‐therapy� Post-‐BE PSG (3-‐6 mos)
� Exclusion criteria:� Previous adenotonsillectomy� Syndromic craniofacial anomalies
Quo SD et al. (2017). Sleep Medicine 30: 45-‐51.
Bimaxillary ExpansionMaxilla: Skeletal Expansion (Rapid maxillary expansion)
Mandible:Dentoalveolar Expansion
Quo SD et al. (2017). Sleep Medicine 30 : 45-51 (left: Fig 3; right: Fig 2).
Bimaxillary ExpansionAHI Mild OSA
AHI < 5 (n=12)
Moderate5 < AHI < 10
(n=17)
SevereAHI > 10 (n=16)
Pre-‐BE 2.9 7.1 22.0Post-‐BE 6.1 6.1 10.3p-‐value 0.03 0.25 0.001
• AHI increased in 15/45 patients• No cephalometric findings associated with BE response• Favorable BE response significantly associated with OSA
severity• OSA was not eliminated in any case
Data derived from Quo 2017 and presented as median values (Min – Max AHI)
Quo SD et al. (2017). Sleep Medicine 30 : 45-51.

RME and Vomer� Beware of intervening with rapid maxillary expansion in children < 8 yrs old
� Anecdotal reports of nasal distortion
� Caused by “vomer drop”?� 10-‐20 lbs force
Fig 14-‐11 B & C. Proffit WR. Contemporary Orthodontics. St. Louis, Mo: Elsevier/Mosby, 2013.
VomerAnatomy� Paired bone in utero� Fuses prior to birth� Articulates with crest of maxilla and crest of palatine bone
Gray's Anatomy plates. (2015, April 13). Wikimedia Commons, the free media repository.Retrieved 02:46, October 20, 2015 from
https://commons.wikimedia.org/w/index.php?title=Gray%27s_Anatomy_plates&oldid=156953426.
VomerAnatomy
Gray's Anatomy plates. (2015, Apr il 13). Wikimedia Commons, the free media repository.
Retr ieved 02:46, October 20, 2015 from https://commons.wikimed ia.org/w/in dex.p hp? tit le=
Gray%27s_Anatomy_plates&oldid=15 6953426 .
"Vomer" by Anatomist90 -‐ Own work. Licensed under CC BY-‐SA 3.0 via Commons
https://commons.wikimed ia.org/wik i/File:Vomer .jpg#/media/File:Vomer .jpg
� Rapid maxillary expansion in children < 8 yrs may lead to drop in vomer, causing nasal deformities
� No studies have examined behavior of vomer or nose during maxillary expansionProffit WR. Contemporary Orthodontics.
St. Louis, Mo: Elsevier/Mosby, 2013. Fig 07-‐08
RME and Vomer “Drop”
RME for Pediatric SDB: Summary� Physician colleagues need to be educated on limitations
of RME� RME is promising tool in select orthodontic cases but
insufficient data exist to recommend its use more generally at this time as a treatment option for pediatric sleep disordered breathing
� Research efforts are underway to investigate this treatment modality in young children
� Slow expansion in management of pediatric SDB has not been described to date
Mandibular Advancement DevicesMethods� “Quasi-‐randomized” controlled
clinical trial� N=32, mean age: 7.2 yrs� Treatment: Mono-‐bloc
removable mandibular advancement device to correct Class II malocclusion x 6 mo(n=19)
� Controls: no tx (n=13)� Daytime and nighttime symptom
questionnaires in all subjects� Pre-‐ and post-‐PSG in treated
children only
Results
Villa MP et al. (2002). Am J Respir CritCare Med 165 (1):123-7.
• 9 dropouts (5 tx/4 control)• AHI significantly improved from
7.1 to 2.6 (p<.001) in tx group• Questionnaire results suggest
decrease in symptoms in treated group
Mandibular Advancement Devices (MAD)2002-‐2013: systematic review of MAD for pediatric SDB� Only 4 (of 1759) studies met criteria for inclusion
� Randomized or non-‐randomized, prospective or retrospective clinical trials
� Children and adolescents (< 16 yrs)� Dx = SDB, Treated with MAD� Treatment and control groups or pre-‐ and post-‐treatment outcomes (AHI)
� Available evidence is scarce and of poor quality
Nazarali N et al. (2015). EurJ Orthod 37:618-‐26.
Mandibular Advancement Devices (MAD)� 2016 Cochrane Review:
� 686 trials initially identified� one met inclusion criteria (RCT or quasi-‐RCT, with control group) – Villa et al. (2002) Am J RespirCritCare Med
� Small sample (N=23), low quality of evidence� Suggests promise of oral appliance therapy for pediatric SDB, but evidence is thus far lacking to demonstrate effectiveness
Fernando R Carvalho et al. Cochrane Database of Systematic Reviews 2016, Issue 10. Art. No.: CD005520. DOI: 10.1002/14651858.CD005520.pub3.
Mandibular Advancement Devices: Summary� Currently insufficient research to judge feasibility and effectiveness of oral appliance therapy (OAT) for pediatric OSA
� Practical considerations have limited use of OAT in children
� Long-‐term outcomes have not been assessed� Respiratory� Behavioral� Cognitive� Cardiovascular
To Extract or Not to Extract?� Zhang J, Chen G, Li W, Xu T, Gao X. Upper Airway Changes after Orthodontic
Extraction Treatment in Adults: A Preliminary Study using Cone Beam Computed Tomography. Cray J, ed. PLOS ONE. 2015;10(11):e0143233. doi:10.1371/journal.pone.0143233.
� Germec-‐Cakan D, TanerT, Akan S. Uvulo-‐glossopharyngeal dimensions in non-‐extraction, extraction with minimum anchorage, and extraction with maximum anchorage. EurJ Orthod 2011 Oct;33(5):515-‐20. Epub 2010 Nov 30. PubMed PMID: 21118911.
� Valiathan M, El H, Hans MG, PalomoMJ. Effects of extraction versus non-‐extraction treatment on oropharyngeal airway volume. Angle Orthod 2010 Nov;80(6):1068-‐74. PubMed PMID: 20677956.
� Chen Y, Hong L, Wang C, Zhang S, Cao C, Wei F, Lv F, Zhang F, and Liu D. Effect of large incisor retraction on upper airway morphology in adult bimaxillary protrusion patients. Angle Orthod 2012; 82: 964-‐970.
� Wang Q; Jia P; Anderson N; Wang L; Lin J. Changes of pharyngeal airway size and hyoid bone position following orthodontic treatment of Class I bimaxillaryprotrusion. Angle Orthod 2012;82:115–121.
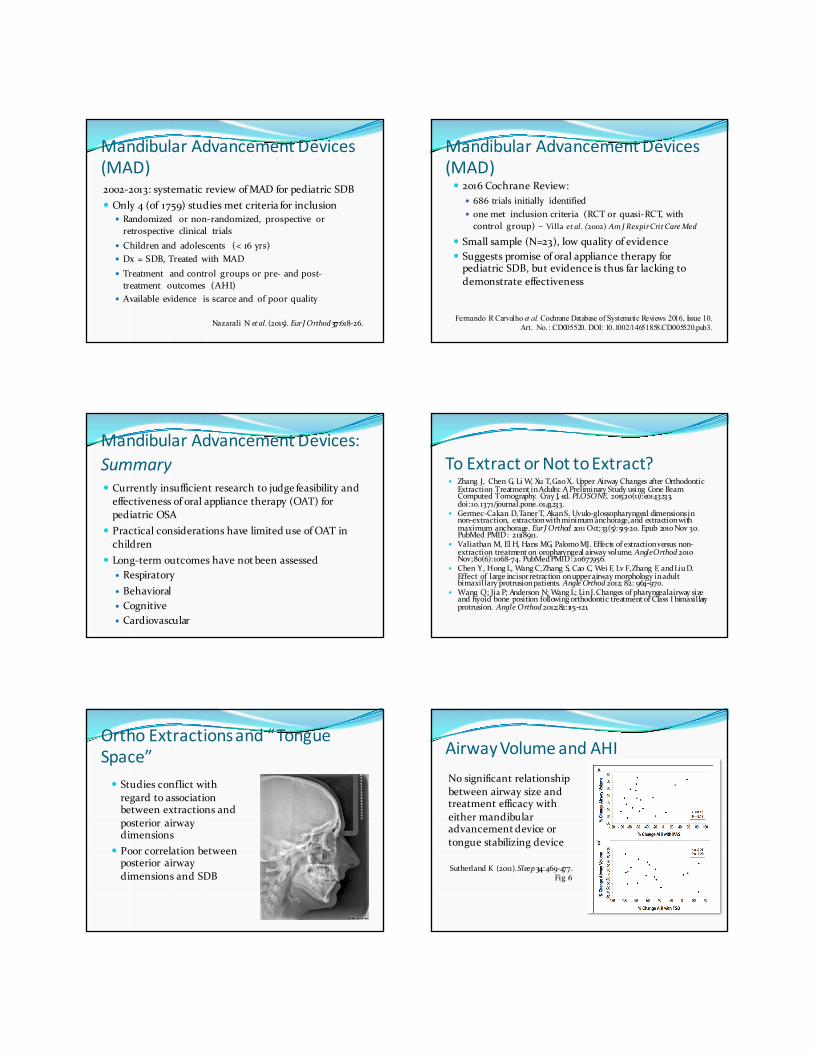
Ortho Extractions and “Tongue Space”� Studies conflict with regard to association between extractions and posterior airway dimensions
� Poor correlation between posterior airway dimensions and SDB
Airway Volume and AHINo significant relationship between airway size and treatment efficacy with either mandibular advancement device or tongue stabilizing device
Sutherland K (2011). Sleep 34:469-‐477. Fig 6

Missing Link� Assessment of airway size after treatment not most useful outcome
� Need data on association between premolar extractions and SDB confirmed by PSG
Premolar Extractions & OSA� Review of electronic medical and dental health records of HealthPartners in MN
� N=5,584� Cases: 50% (2,792) -‐ missing one premolar/quadrant� Controls: 50% -‐ no missing premolars� Matched 1:1 on age, gender, BMI categories (normal, overweight, obese, unknown)
� Age groups: 40-‐49 yrs, 50-‐59 yrs, 60-‐70 yrs� Outcome: prevalence of OSA (confirmed by PSG)
Larsen AJ et al. (2016). J ClinSleep Med 11(12): 1443-‐1448.
Premolar Extractions & OSAAssumptions:� If missing one premolar/quadrant and no more than one other missing tooth (except for 3rd molars) àorthodontic treatment
� Likelihood of being referred for PSG to rule out OSA same in both case and contol groups
Larsen AJ et al. (2016). J ClinSleep Med 11(12): 1443-‐1448.
Premolar Extractions & OSA: Results%
Female 35%Age Group
40-‐49 yrs50-‐59 yrs60-‐70 yrs
43%40%17%
BMI category (kg/m2)< 2525 -‐ <3030+Unknown
26%26%23%25%
� Prevalence of OSA� Controls: 9.56%� Cases: 10.71%
� Prevalence of OSA not significantly different between groups (OR = 1.14, p = .144)
Larsen AJ et al. (2016). J Clin Sleep Med 11(12): 1443-1448.)
Due to 1:1 matching, subject characteristics identical between Cases and Controls
Premolar Extractions & OSA: Conclusion
Extraction of premolars is not a risk factor in development of OSA
Conclusions� Orthodontic treatment modalities have been described to manage pediatric SDB
� Much research is still needed to clarify� Appropriate procedures� Optimal age� Outcomes: Cognitive, behavioral, cardiovascular, effect on airway and craniofacial growth and development
� Treatment protocols need to be established
AAO Donated Orthodontic Services (DOS) Program
All that is missing is You!
• Introduced in 2009, the DOS program provides access to care for children in need. Access to quality orthodontic care is missing in many children’s lives. The AAO DOS program mission is to serve indigent children without insurance coverage or that do not qualify for other assistance in their state of residence.
• The program has expanded and offers care to children nationwide in addition to the recognized state programs in Illinois, Indiana, Kansas, Michigan, New Jersey, North Carolina, Rhode Island, Tennessee, Texas and Virginia.
• In order to expand further, we need you to help us by volunteering to serve as a provider orthodontist or help identify orthodontists willing to lead efforts to establish a DOS chapter in your state.
• Stop by the DOS booth here in San Diego to learn more about the program or contact Ann Sebaugh at [email protected] with questions.
The AAO Foundation, the charitable arm of the American Association of
Orthodontists, provides support to orthodontic education programs and orthodontic research
If Your Passion is Orthodontics…
Then pledge, or increase your pledge, to the AAO Foundation
Ensure the future of orthodontics
� As a practicing orthodontic specialist, you are passionate about every aspect of your professional life. From day-‐to-‐day clinical experience to community relations to keeping abreast of the latest in innovative treatment options, orthodontics is your life.
� Qualified teachers, scholars and researchers have been the backbone of our specialty. The AAOF is committed to promoting education for our profession and ensuring the continuance of our specialty.
� You can help to improve the picture for orthodontics today by pledging or renewing your pledge to the AAOF.
� There is no better way to communicate your professional dedication while ensuring the ongoing vitality of our specialty.
� To contribute or discuss giving options, please call Mr. Robert W. Hazel at 800-‐424-‐2841, ext. 246 at the AAOF offices in St. Louis.
� Share the passion and give back to the profession that has given so much to you.