Embed Size (px)
Citation preview
Shawn K. Hatch, ACSW, LMSW, CCS, CAADCMarquette General Health System
Maximum east-west distance – 320 miles
Maximum north-south distance – 125 miles
1700 miles of continuous shoreline with the Great Lakes
4,300 inland lakes and 12,000 miles of streams
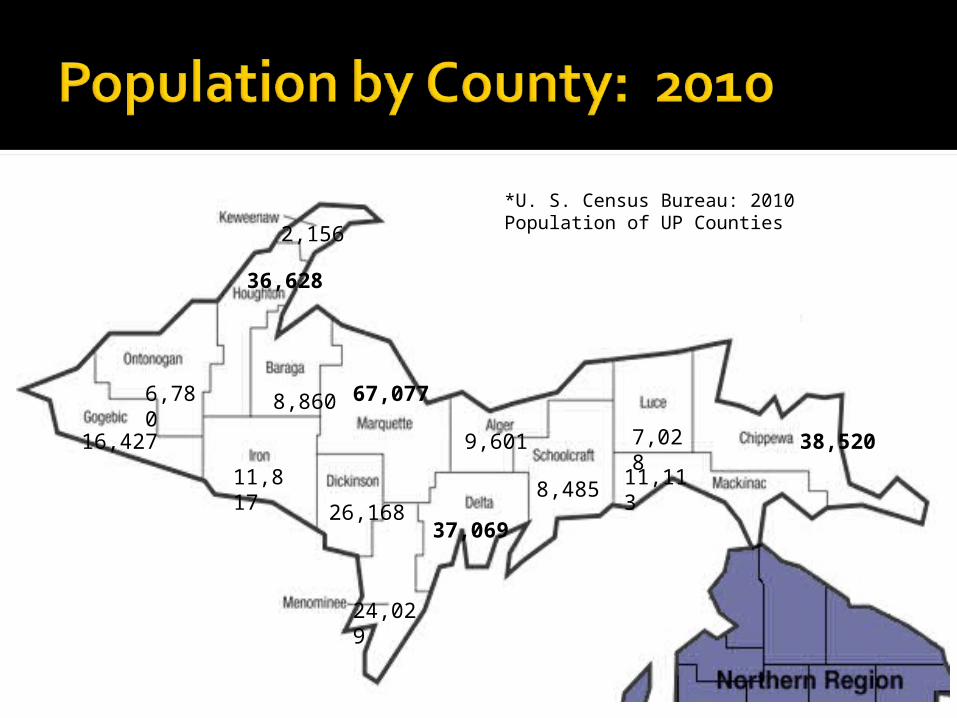
2,156
36,628
6,780
16,427
8,860
11,817
67,077
26,168
9,601
24,029
37,069
8,485
7,028
11,113
38,520
*U. S. Census Bureau: 2010 Population of UP Counties

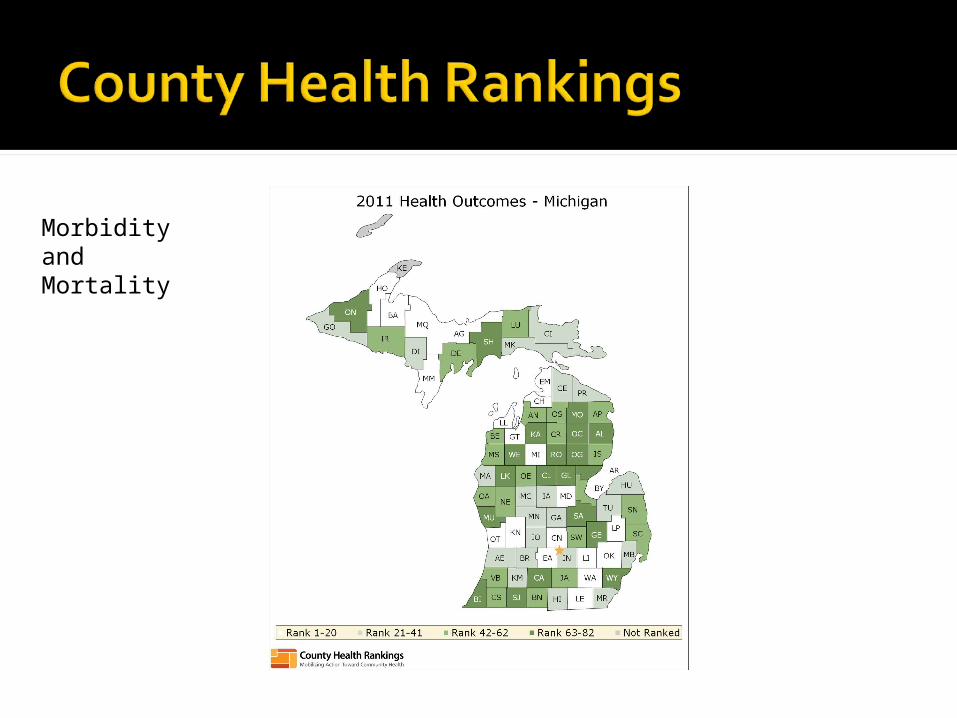
Morbidity and Mortality
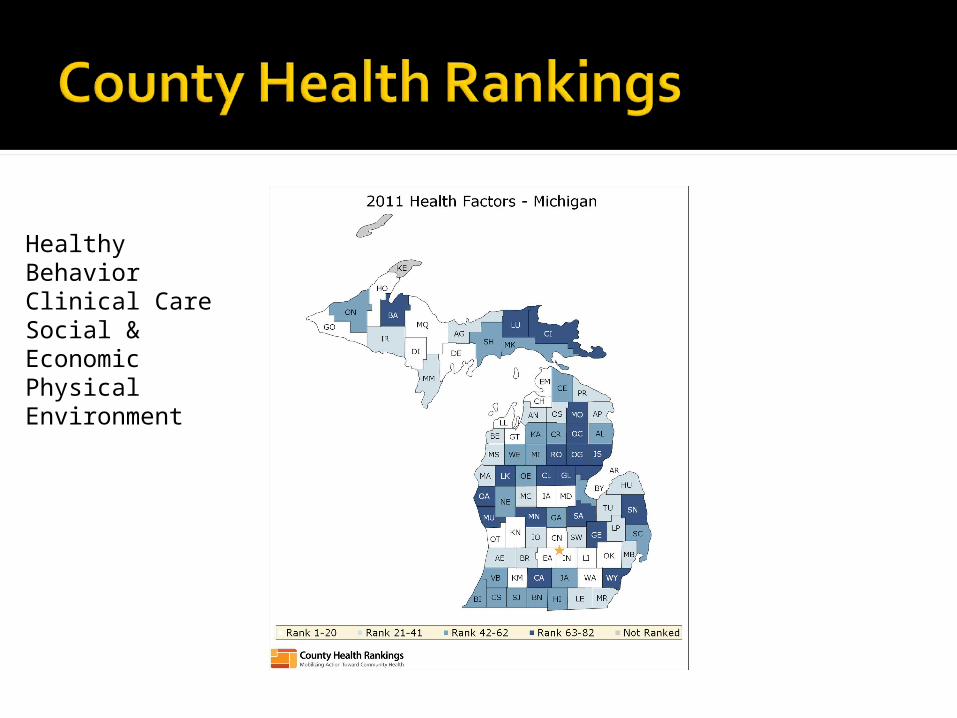
Healthy BehaviorClinical CareSocial & Economic Physical Environment
The UP has a growing problem with opiate and prescription drug abuse.
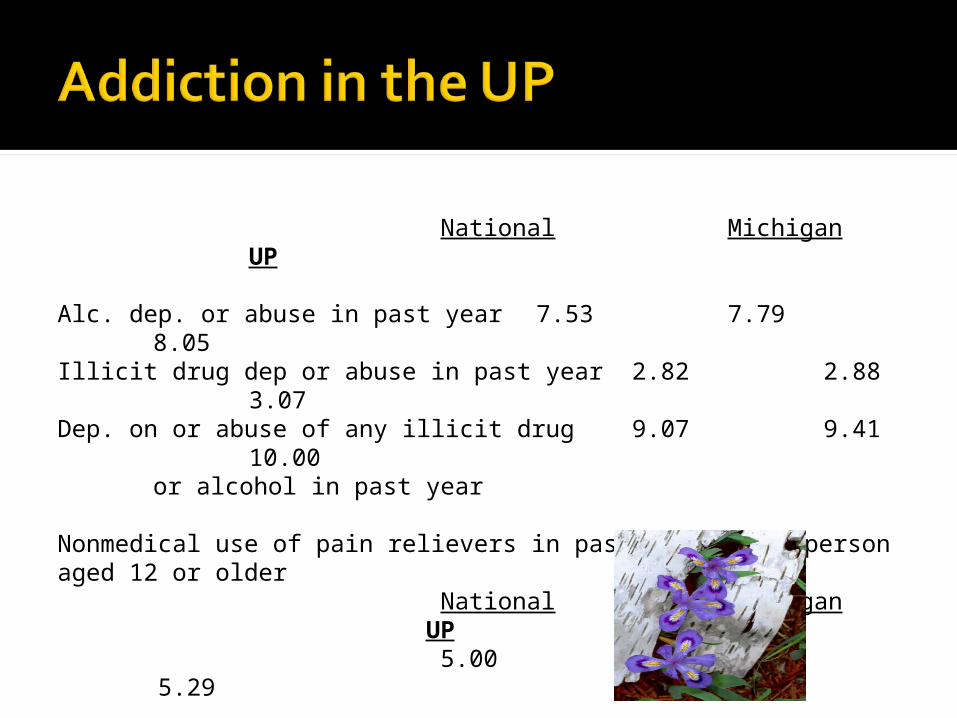
National MichiganUP
Alc. dep. or abuse in past year 7.53 7.79 8.05Illicit drug dep or abuse in past year 2.82 2.88
3.07Dep. on or abuse of any illicit drug 9.07 9.41
10.00or alcohol in past year
Nonmedical use of pain relievers in past year among person aged 12 or older
National Michigan UP
5.00 5.63 5.29
MDCH, Mental Health & Substance Abuse AdministrationBureau of Substance Abuse & Addiction ServicesState & Substate Estimates of Substance Use in Michigan
2006-2008 National Surveys on Drug Use and Health
Traditional outpatient and residential treatment programs
Methadone . . . not available in the UP Green Bay, WI – 175 miles Muskegon, MI – 440 miles
Buprenorphine 4 physicians accepting new patients
Medication approved for the OP treatment of opiate dependence in 2000 (Drug Abuse Treatment Act of 2000). Set physician qualifications for prescribing.
FDA approved Suboxone/Subutex in 2002.
Partial Opioid Agonist Ceiling effect
Withdrawal & Craving
Suboxone 8 mg buprenorphine/2 mg naloxone
Subutex 8 mg buprenorphine▪ Primarily for pregnancy
Multiple reports of addicts snorting or using IV.
Amount of naloxone may not be enough for some individuals.
This is an abusable drug – like most, can be used for good or evil.
Prescribers must go through special training and are issued a separate DEA number.
Prescribers are limited to 30 patients for the first year. Can apply for a waiver and treat up to 100
after the first year. Many prescribers want this population
out of their office . . . . Prescribers still have limited knowledge of
addiction.
Yes It isn’t the “drug of choice” but it is
(significantly) better than nothing▪ The “high” experience▪ Expectancy▪ Relief from sick to not sick
Great to have on hand in case addict can’t score▪ Selling/trading for full agonist
Methadone is currently the “standard of care” for the pregnant opiate addict.
ACOG: Buprenorphine Versus Methadone Treatment for Opiate Addiction in Pregnancy: An Evaluation of Neonatal Outcomes, 2010 Lower NAS scores for the Subutex babies▪ 10.69 versus 12.5
Shorter LOS▪ 8.4 versus 15.7
Less than 50% of Subutex babies requiring treatment versus 73% of methadone babies
2006 142007 232008 172009 232010 45
Yes . . . . and noMaking the leap
June of 2007 – MGHS accepts first patient
Brief phone screen Quickly overwhelmed
Swamped with phone calls High “hassle factor”▪ Reports of “lost” or “stolen” meds▪ Requests for early refills▪ Refill requests . . . from jail
High volume of drop-outs and non-compliance
April of 2008 – Discontinued admissions 10 months and 29 patients
No denying how desperately this service was needed.
At this point, only one other physician prescribing in the UP.
We had a handful of patients who were doing well for the first time in their lives.
This posed an interesting and challenging question: How do we expand this classification of patients?
Prescribing physician left our organization
Dr. John Lehtinen agrees to prescribe.
Road trip
How do we manage a limited resource?How do we make this service available
to the best treatment candidates?How do we manage the “hassle factor”
and prevent burning out our staff and physician?
How do we maintain our integrity and credibility with local agencies, treatment providers, law enforcement, and most importantly, our patients?
Slowing down the process and looking for the best matches for the medication.
Rationale for the application: Completing and mailing the application would
require effort. The application would allow us a better
opportunity to screen applicants and potentially fill the limited treatment slots with those in the best position to benefit from buprenorphine.
Items from criteria in TIP 40: Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Dependence: History of treatment completion/compliance Not currently abusing benzos, sedative-
hypnotics, or barbiturates Not currently abusing alcohol Supportive living environment Supports for recovery
Dependence is limited to opiatesEmployedNo medical contraindications Indicated agreement to abide by
rules and expectations.
Already being treated with Suboxone and successful
Active in substance abuse treatmentTreatment goal of abstinenceHas resources to pay for treatment
and medicationNot in collections with us“Clean” MAPSApplication is complete
Buprenorphine screening questionnaire
MGHS Personal Data form Releases of Information to the PCP and
current substance abuse professionals, as applicable
Treatment contract* Patient and family information about
buprenorphine Summary of substance use
Program Requirements: Attendance at all scheduled
appointments Attendance at a substance abuse
program ROI’s to all physicians and
counselors/therapists Abstinence from alcohol and drugs
Patient Responsibilities: Store medication properly Take as prescribed Pill counts Drug testing Notify office if medication lost or stolen Notify of relapse Payment for services
Application is sent to caller.Returned applications are “scored”Review by CommitteeHigher scoring applicants are
contacted to schedule appointment with physician and for induction; assuming no medical contraindications.
The score sheet – no magic number or total score for automatic admission
Receive letter with specific treatment recommendations and an invitation to meet with addiction physician in consideration of other treatment options.
Receive instructions regarding how to access services for his/her circumstances, i.e., location, treatment history, funding source, etc.
Encouraged to contact us for second review if treatment recommendations are followed through.
Prescribing PhysicianDirector of Clinical ServicesClinical SupervisorClinician
Provides forum to review program policy, discuss clinical challenges, and advocate for candidates.
Takes “heat” away from prescribing physician.
Between August of 2009 and March of 2011 more than 350 applications were distributed.
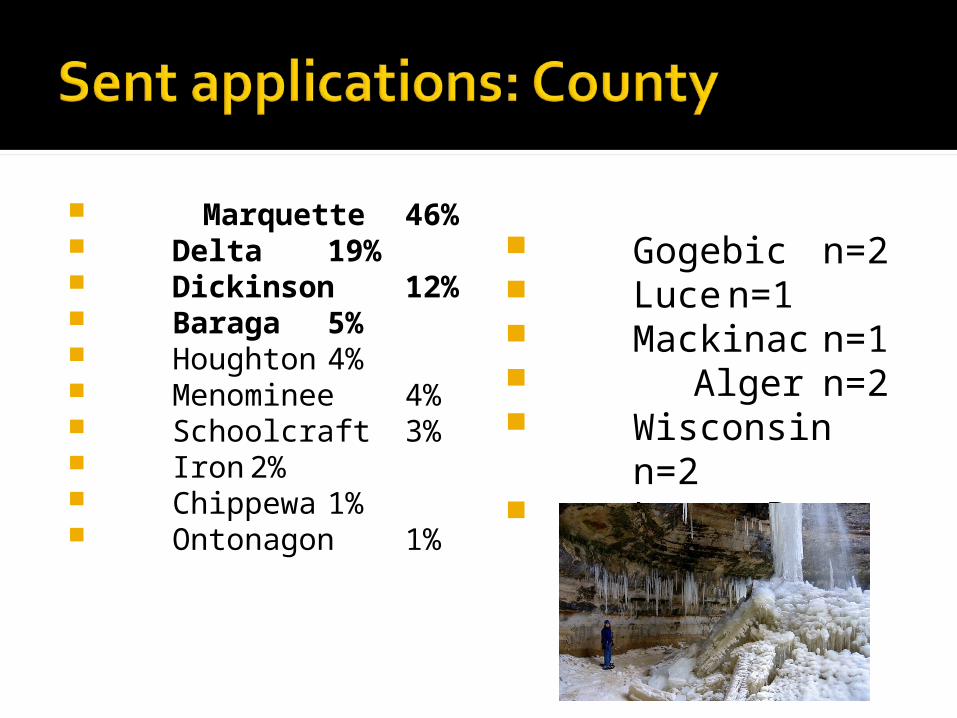
Marquette 46%
Delta19%
Dickinson12%
Baraga 5% Houghton 4% Menominee 4% Schoolcraft 3% Iron 2% Chippewa 1% Ontonagon 1%
Gogebic n=2 Luce n=1 Mackinac n=1 Alger n=2 Wisconsinn=2 Lower Pen.
n=1
50/50 split between males/femalesAverage distribution rate has been
18 per monthNearly half (170) of the 350
applications were completed and returned to the Review Committee
28% of those who have returned applications have been admitted for buprenorphine treatment.
Average age 29.8 Age:
17 1% 18-30 61% 31-40 28% 41-50 8% 51-65 1%
Race 91% Caucasian 9% Native American
Sex Male 46% Female 54%
June 2007 – April 2008 (10 months) 29 patients admitted 22 of original 29 were discharged 20 of the 22 were discharged by
October of 2009, however, nearly half were gone within the first 4 months of treatment 13 dropped out 7 discharged “at staff request” 2 completed
August 2009 – March 2011 (19 months) 48 patients admitted 7 discharges
5 dropped out 2 discharged “at staff request”
Retention rate went from 24% to 85% Significant reduction in the “hassle
factor” Able to more than double admissions
without additional staff resources Currently have 76 patients enrolled in
the program.
Pregnancy The only exception to the application
process The application process would delay
treatment Acknowledgement that our focus has
shifted to treat the pregnant addict and provide the best possible start for the baby.▪ Limited window to engage the patient in
treatment and recovery.
Non-compliance with counseling Late entry into pre-natal care and
treatment Shame Use of other drugs/continued drug use Poor support system Poverty Distance from physician (from all over
UP) “Hostage” until birth Case coordination between OB/NICU and
prescribing physician Pregnancy to access program.
High volume of pregnant addicts seeking treatment with buprenorphine 43 since December of 2010; 40 pregnant
at admission The return of the “hassle factor”
Incentive to comply▪ About 25% compliance but improving.
Better outcomes from NICU Shorter LOS and less severe withdrawal
How significant problem of opiate addiction is in the UP
Buprenorphine isn’t for everyoneThe application process is an
effective way to manage a valuable and limited treatment resource
Support group didn’t fly.How long should someone be on
buprenorphine? A controversial and individualized question.
Counseling need to start before the buprenorphine and the longer the better
We need to continually “take our own inventory” regarding attitudes, beliefs, biases, regarding buprenorphine treatment and patients.
We still have much to learn . . . . More challenging and stimulating
opportunities lie ahead . . . .
Shawn K. Hatch, ACSW, LMSW, CCS, CAADCDirector of Clinical Services, Behavioral HealthMarquette General Health [email protected](906) 225-3214