Embed Size (px)
Citation preview

SEXUAL FUNCTION AFTER HIGHLY SELECTIVE EMBOLIZATION OFCAVERNOUS ARTERY IN PATIENTS WITH HIGH FLOW PRIAPISM:
LONG-TERM FOLLOWUP
GIANFRANCO SAVOCA,* FRANCESCO PIETROPAOLO, FRANCESCO SCIERI,MICHELE BERTOLOTTO, FABIO POZZI MUCELLI AND EMANUELE BELGRANO
From the Departments of Urology (GS, FP, FS, EB) and Radiology (MB, FPM), School of Medicine, University of Trieste, Trieste, Italy
ABSTRACT
Purpose: We present 15 cases of high flow priapism treated by selective embolization andevaluate erectile function at long-term followup.
Materials and Methods: Between 1995 and 2001, 15 patients underwent highly selectiveembolization of the cavernous artery for high flow priapism. Trauma was reported by 12 of the15 patients, and no etiologic causes were evident in the other 3. The fistula was unilateral in 13patients and bilateral in 2. All patients underwent embolization during arteriography. Erectilefunction was determined using the International Index of Erectile Function (IIEF) at followupafter an average of 55 months (range 18 to 93).
Results: Postoperative color Doppler ultrasonography showed no recurrence in 11 patients(73%). Repeat pelvic angiography with selective embolization was required at 1 month postop-eratively in 3 patients (20%). In 1 case (7%) 3 consecutive embolizations were not conclusive anda surgical operation was required. The IIEF results showed that sexual function was in thenormal range in 80% of patients. Three patients (20%) reported a slight change in the quality oferection. Mean postoperative IIEF score was 26.3 (range 18 to 30).
Conclusions: Highly selective embolization of the fistula is an effective and safe treatmentoption for high flow priapism because it ensures a high level of preservation of pretreatmenterectile function.
KEY WORDS: priapism; fistula; therapy; penile erection; embolization, therapeutic
Arterial or high flow priapism is a fairly rare dysfunctionresulting from penile or perineal trauma.1–4 In rare cases theetiology remains unknown. A clinical suspicion of this patho-logical condition is usually based on medical history and theobjective findings of the penile examination. Diagnostic pro-cedures include blood gas analysis of the cavernous blood andcolor Doppler ultrasonography (CDUS) of the cavernous bod-ies.5, 6
Several treatment options, such as intracavernous injec-tions of �-adrenergic agonists7 or methylene blue,8 surgicalligation of the cavernous artery9 and embolization of thecavernous artery have been used.10–12 Selective embolizationof the artery, first described by Wear et al in 1997,11 allowsfor temporary occlusion of the cavernous artery, thus permit-ting cicatricial closure of the fistula and subsequent re-channeling of the embolized artery. Analysis of previousstudies on this subject shows that case histories are oftenlimited and that the treatment methods are still mostly con-troversial.13, 14 In particular, sexual function after treatmenthas been poorly investigated. We report on the managementand long-term erectile function of patients treated withhighly selective embolization at our clinic between 1995 and2001.
MATERIALS AND METHODS
Between 1995 and 2001, 16 patients with high flow pria-pism were observed at the urologic clinic of our university.The records of 15 patients treated with highly selective em-
bolization with long-term followup were examined. One pa-tient treated by surgery was not included in the study. Meanpatient age was 32 � 9.8 (range 18 to 51).
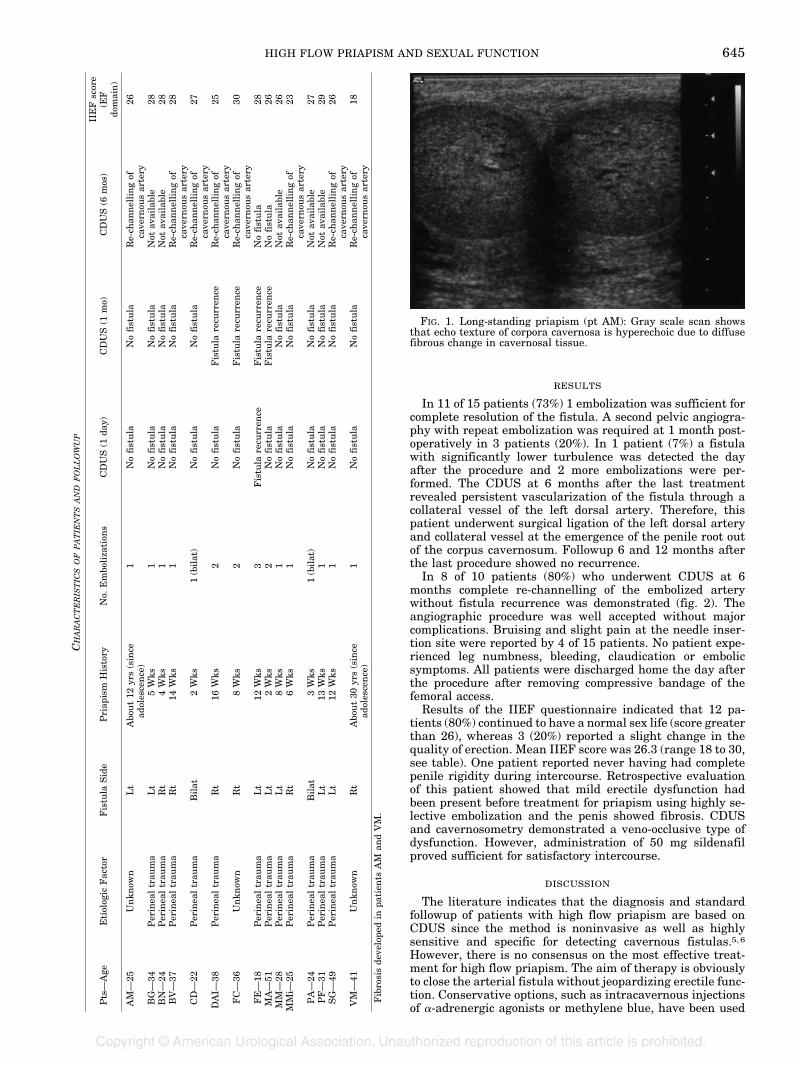
From the medical history significant trauma was apparentin 12 of the 15 patients, and 3 did not recall any penile orperineal trauma (see table). Nonetheless, the presence of acavernous fistula was detected by CDUS in all 15 patients.The fistula was unilateral in 13 patients and bilateral in 2.Symptoms of priapism developed within days of the trauma.In all cases examinations were performed at least 2 weeksafter the appearance of clinical symptoms (range 2 weeks toapproximately 30 years, see table). In 2 patients 25 and 41years old the diagnosis was made during andrology evalua-tion for varicocele and mild progressive erectile dysfunction,respectively. Both patients reported having had persistenttumescence since puberty. In both cases the physical exam-ination and CDUS showed diffuse penile fibrosis (fig. 1) as-sociated with a ventral curvature in 1.
After blood gas analysis of the cavernous blood and CDUS,all patients underwent pelvic angiography using a 5Fr cath-eter introduced into the common femoral artery. The proce-dure consisted of introducing a micro-guidewire and micro-catheter system coaxially and advancing it as proximally aspossible to the fistula to inject polyvinyl alcohol particles ofvariable size (350 to 500 �m) into the fistula. The procedurewas performed unilaterally in 13 patients and bilaterally in2. CDUS was performed 1 day and 1 month after the proce-dure. In 10 of the 15 patients repeat CDUS was done at 6months (see table). Sexual function was investigated usingthe International Index of Erectile Function (IIEF) question-naire administered to the patients in the office at meanfollowup of 55 months (range 18 to 93).
Accepted for publication March 26, 2004.* Correspondence: Clinica Urologica, Ospedale di Cattinara,
Strada di Fiume 447 34149, Trieste, Italy (telephone: �39 0403994734; FAX: �39 0403994895; e-mail: [email protected]).
0022-5347/04/1722-0644/0 Vol. 172, 644–647, August 2004THE JOURNAL OF UROLOGY® Printed in U.S.A.Copyright © 2004 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000132494.44596.33
644
RESULTS
In 11 of 15 patients (73%) 1 embolization was sufficient forcomplete resolution of the fistula. A second pelvic angiogra-phy with repeat embolization was required at 1 month post-operatively in 3 patients (20%). In 1 patient (7%) a fistulawith significantly lower turbulence was detected the dayafter the procedure and 2 more embolizations were per-formed. The CDUS at 6 months after the last treatmentrevealed persistent vascularization of the fistula through acollateral vessel of the left dorsal artery. Therefore, thispatient underwent surgical ligation of the left dorsal arteryand collateral vessel at the emergence of the penile root outof the corpus cavernosum. Followup 6 and 12 months afterthe last procedure showed no recurrence.
In 8 of 10 patients (80%) who underwent CDUS at 6months complete re-channelling of the embolized arterywithout fistula recurrence was demonstrated (fig. 2). Theangiographic procedure was well accepted without majorcomplications. Bruising and slight pain at the needle inser-tion site were reported by 4 of 15 patients. No patient expe-rienced leg numbness, bleeding, claudication or embolicsymptoms. All patients were discharged home the day afterthe procedure after removing compressive bandage of thefemoral access.
Results of the IIEF questionnaire indicated that 12 pa-tients (80%) continued to have a normal sex life (score greaterthan 26), whereas 3 (20%) reported a slight change in thequality of erection. Mean IIEF score was 26.3 (range 18 to 30,see table). One patient reported never having had completepenile rigidity during intercourse. Retrospective evaluationof this patient showed that mild erectile dysfunction hadbeen present before treatment for priapism using highly se-lective embolization and the penis showed fibrosis. CDUSand cavernosometry demonstrated a veno-occlusive type ofdysfunction. However, administration of 50 mg sildenafilproved sufficient for satisfactory intercourse.
DISCUSSION
The literature indicates that the diagnosis and standardfollowup of patients with high flow priapism are based onCDUS since the method is noninvasive as well as highlysensitive and specific for detecting cavernous fistulas.5, 6However, there is no consensus on the most effective treat-ment for high flow priapism. The aim of therapy is obviouslyto close the arterial fistula without jeopardizing erectile func-tion. Conservative options, such as intracavernous injectionsof �-adrenergic agonists or methylene blue, have been used
CHARACTERISTICSOFPATIENTSANDFOLLOWUP
Pts—
Age
Etiolog
icFac
tor
Fistu
laSide
Priap
ism
History
No.
Embo
liza
tion
sCDUS
(1da
y)CDUS
(1mo)
CDUS
(6mos
)IIEF
scor
e(E
Fdo
main)
AM
—25
Unkn
own
Lt
Abo
ut12
yrs(since
adoles
cence
)1
Nofistula
Nofistula
Re-ch
annellingof
cave
rnou
sar
tery
26
BG—
34Per
inea
ltrau
ma
Lt
5W
ks1
Nofistula
Nofistula
Not
available
28BN—
24Per
inea
ltrau
ma
Rt
4W
ks1
Nofistula
Nofistula
Not
available
28BV—
37Per
inea
ltrau
ma
Rt
14W
ks1
Nofistula
Nofistula
Re-ch
annellingof
cave
rnou
sar
tery
28
CD—
22Per
inea
ltrau
ma
Bilat
2W
ks1(bilat
)Nofistula
Nofistula
Re-ch
annellingof
cave
rnou
sar
tery
27
DAI—
38Per
inea
ltrau
ma
Rt
16W
ks2
Nofistula
Fistu
lare
curren
ceRe-ch
annellingof
cave
rnou
sar
tery
25
FC—
36Unkn
own
Rt
8W
ks2
Nofistula
Fistu
lare
curren
ceRe-ch
annellingof
cave
rnou
sar
tery
30
FE—
18Per
inea
ltrau
ma
Lt
12W
ks3
Fistu
lare
curren
ceFistu
lare
curren
ceNofistula
28M
A—
51Per
inea
ltrau
ma
Lt
2W
ks2
Nofistula
Fistu
lare
curren
ceNofistula
26M
M—
28Per
inea
ltrau
ma
Lt
8W
ks1
Nofistula
Nofistula
Not
available
26M
Mi—
25Per
inea
ltrau
ma
Rt
6W
ks1
Nofistula
Nofistula
Re-ch
annellingof
cave
rnou
sar
tery
23
PA—
24Per
inea
ltrau
ma
Bilat
3W
ks1(bilat
)Nofistula
Nofistula
Not
available
27PF—
31Per
inea
ltrau
ma
Lt
13W
ks1
Nofistula
Nofistula
Not
available
29SG—
49Per
inea
ltrau
ma
Lt
12W
ks1
Nofistula
Nofistula
Re-ch
annellingof
cave
rnou
sar
tery
26
VM
—41
Unkn
own
Rt
Abo
ut30
yrs(since
adoles
cence
)1
Nofistula
Nofistula
Re-ch
annellingof
cave
rnou
sar
tery
18
Fibro
sisde
velope
din
patien
tsAM
andVM
.
FIG. 1. Long-standing priapism (pt AM): Gray scale scan showsthat echo texture of corpora cavernosa is hyperechoic due to diffusefibrous change in cavernosal tissue.
HIGH FLOW PRIAPISM AND SEXUAL FUNCTION 645

with only temporary results.7, 8 Other treatments includeembolization and surgical ligation of the cavernous artery.9In many reports pelvic angiography followed by selectiveembolization of the cavernous artery with autologous clots orsynthetic substances proved to be satisfactory for high flowpriapism.10–19
The results of our experience confirm the effectiveness ofangiography with highly selective embolization in healinghigh flow priapism. In 3 of 15 cases the fistula recurred,requiring repeat embolization, which almost always provedconclusive. Only in 1 patient (7%) was surgical therapy re-quired. Moreover, the embolization procedure was well toler-ated by all patients, including those who underwent repeattreatment.
Surgical ligation as an alternative to angiography could beperformed by ligating the cavernous artery at the outlet fromAlcock’s canal9 or by performing exploratory corporotomyfollowed by microsurgical closure of the arterial fistula. Thefirst procedure resolves the priapism but the cavernous ar-tery is irreversibly closed. Considering the natural history ofthe disease and the young age of the patients, permanentocclusion should be avoided. The second method is, in ouropinion, complex. We performed exploratory corporotomywith microsurgical ligation of the fistula in 1 patient.15 Theprocedure proved difficult and postoperative erectile dysfunc-tion developed. This history suggests that dissection of thecorpora placed the patient at high risk of erectile dysfunctionbecause of scarring of the tunica albuginea and venous leak-age. A few weeks after formation of the fistula, a vascularpseudocapsule forms which can be detected on CDUS6 butintraoperative detection of the site of the fistula becomesdifficult and extensive exploration of the cavernous body maybe necessary. On the basis of these findings, we believe thatopen corporotomy should not be considered as the first linetherapy.
Erectile dysfunction following priapism treatment hasbeen reported in about 15% to 20% of patients.15–19 Theresults of our experience show the safety of highly selectiveembolization of the cavernous artery in preserving premorbiderectile function. Of our patients 80% experienced no changein the quality of sexual function after treatment, whereasonly 1 (7%) required a pharmacological aid for satisfactoryintercourse. These results are comparable to those of Bas-tuba et al who reported the complete restoration of premor-bid erectile function in 6 of 7 patients treated with selectiveembolization.13
Also in agreement with previous reports,13, 17 re-channelling the cavernous artery was demonstrated in mostpatients on CDUS (fig. 2). When cavernous artery re-channelling did not occur, vascularization of the cavernousbody was warranted by the contralateral cavernous arterythrough the communications of the septum. Re-channellingthe embolized arteries is especially important in patientswith bilateral fistulas. A review of the literature shows thatmost patients are treated bilaterally in a single session.17 In
our experience we also performed immediate embolization ofboth fistulas in 1 session. In these patients transient, partialand reversible erectile dysfunction occurred for at least 3weeks but erectile function was normal at followup. However,embolization of 1 side could be deferred because of the sup-posed risk of impotence.
Many authors propose a conservative management strat-egy for high flow priapism.1, 14 From the analysis of the casehistories reported in other studies and our experience, it isevident that most patients with high flow priapism enjoy anormal sex life for many years before treatment. Therefore,these patients could be followed conservatively for severalweeks with the hope that the fistula will close spontaneously.However, only a few cases of spontaneous resolution of thefistula have been published in the literature, and most ofthem were in children.20
The long-term effects of high flow priapism on erectiletissue remain to be clarified. Hakim et al reported on 5patients who underwent a period of watchful waiting duringthe treatment course.1 In none of these cases was spontane-ous closure of the fistula encountered. In 2 of the 5 cases thequality of erection had changed at long term followup. Al-though the authors were unable to explain the relationshipbetween the change in erectile function and the persistenterection, they postulated that persistent unregulated highoxygen levels associated with chronic erection for many yearslead to cavernous smooth muscle damage, and that shortcyclic episodes of corporeal blood oxygen levels (as exist innormal physiology) are required for normal regulation of theconnective tissue matrix. In our experience, only the 2 pa-tients with long-standing priapism had diffuse fibrosis. Inone of these patients erectile dysfunction occurred a fewmonths before our observation and approximately 30 yearsafter the onset of priapism. We cannot explain with certaintythe reasons for the erectile dysfunction in this case: thepatient could have had changes in erectile function as aresult of age (41 years), long-standing priapism or the initialinjury, which he did not recall. Nevertheless, we can statethat patients who were treated early, although most of themreported trauma, did not have fibrosis or changes in theerectile function at long-term followup.
Based on these results, we believe that an observationalperiod can be useful for small fistulas to await the possiblespontaneous closure which usually occurs within about 3weeks.20 If priapism does not resolve after a given period,still to be defined, highly selective embolisation should beperformed. Conversely, for large fistulas in which spontane-ous closure in unlikely, a long observational period could behazardous because we do not really know the long-term ef-fects of excessive arterial inflow on the structure of the cor-pus cavernosum. The results of our experience confirm thathighly selective embolization of the fistula is an effective andsafe treatment option for high flow priapism because it en-sures a high level of preservation of pretreatment erectilefunction.
FIG. 2. A, CDUS shows color blush in area of cavernosal tear and high velocity, turbulent flow. B, after embolization CDUS reveals absenceof turbulent flow in lacuna but normal arterial flow in cavernous artery just before lacuna. C, at 6-month followup CDUS demonstratespatency of cavernous artery with antegrade flow through lacuna without blood spread in area previously embolized.
HIGH FLOW PRIAPISM AND SEXUAL FUNCTION646
REFERENCES
1. Hakim, L. S., Kulaksizoglu, H., Mulligan, R., Greenfield, A. andGoldstein, I.: Evolving concepts in the diagnosis and treatmentof arterial high flow priapism. J Urol, 155: 541, 1996
2. Ricciardi, R. J., Jr., Bhatt, G. M., Cynamon, J., Bakal, C. W. andMelman, A.: Delayed high flow priapism: pathophysiology andmanagement. J Urol, 149: 119, 1993
3. Brock, G., Breza, J., Lue, T. F. and Tanagho, E. A.: High-flowpriapism: a spectrum of disease. J Urol, 150: 968, 1993
4. Witt, M. A., Goldstein, I., Saenz de Tejada, I., Greenfield, A. andKrane, R. K.: Traumatic laceration of intracavernosal arteries:the pathophysiology of nonischemic, high flow arterial pria-pism. J Urol, 143: 129, 1990
5. Feldstein, V. A.: Posttraumatic “high-flow” priapism evaluationwith color flow Doppler sonography. J Ultrasound Med, 12:589, 1993
6. Bertolotto, M., Quaia, E., Mucelli, F. P., Ciampalini, S., Forgacs,B. and Gattuccio, I.: Color Doppler imaging of posttraumaticpriapism before and after selective embolization. Radiograph-ics, 23: 495, 2003
7. Mizutani, M., Nakano, H., Sagami, K. and Nihira, H.: Treatmentof post-traumatic priapism by intracavernous injection ofalpha-stimulant. Urol Int, 41: 312, 1986
8. Steers, W. D. and Selby, J. B., Jr.: Use of methylene blue andselective embolization of the pudendal artery for high-flowpriapism refractory to medical and surgical treatments.J Urol, 146: 1361, 1991
9. Shapiro, R. H. and Berger, R.: Post-traumatic priapism treatedwith selective cavernosal artery ligation. Urology, 49: 638,1997
10. Bookstein, J. J.: Penile angiography: the last angiographic fron-tier. AJR Am J Roentgenol, 150: 47, 1988
11. Wear, J. B., Jr., Crummy, A. B. and Munson, B. O.: A new
approach to the treatment of priapism. J Urol, 117: 252, 199712. Walker, T. J., Grant, P. V., Goldstein, I., Krane, R. J. and
Greenfield, A. J.: “High-flow” priapism: treatment with super-selective transcatheter embolization. Radiology, 174: 1053,1990
13. Bastuba, M. D., Saenz de Tejada, I., Dinlenc, C. Z., Sarazen, A.,Krane, R. J. and Goldstein, I.: Arterial priapism: diagnosis,treatment and longterm followup. J Urol, 151: 1231, 1994
14. Hatzichristou, D., Salpiggidis, G., Hatzimouratidis, K.,Apostolidis, A., Tzortzis, V., Bekos, A. et al: Managementstrategy for arterial priapism: therapeutic dilemmas. J Urol,168: 2074, 2002
15. Ciampalini, S., Savoca, G., Buttazzi, L., Gattuccio, I., Mucelli,F. P., Bertolotto, M. et al: High-flow priapism: treatment andlong-term follow-up. Urology, 59: 110, 2002
16. Levine, F. J., Greenfield, A. J. and Goldstein, I.: Arteriographi-cally determined occlusive disease within the hypogastric-cavernous bed in impotent patients following blunt perinealtrauma. J Urol, 144: 1147, 1994
17. Langenhuijsen, J. F., Reisman, Y., Reekers, J. A. and de Reijke,Th M.: Highly selective embolization of bilateral cavernousarteries for post-traumatic penile arterial priapism. Int J Im-pot Res, 13: 354, 2001
18. Alvarez Gonzalez, E., Pamplona, M., Rodriguez, A.,Garcia-Hidalgo, E., Nunez, V. and Leiva, O.: High flow pria-pism after blunt perineal trauma: resolution with bucrylateembolization. J Urol, 151: 426, 1994
19. Ji, M.-X., He, N.-S., Wang, P. and Chen, G.: Use of selectiveembolization of the bilateral cavernous arteries for post-traumatic arterial priapism. J Urol, 151: 1641, 1994
20. Moscovici, J., Barret, E., Galinier, P., Liard, A., Juricic, M.,Mitrofanoff, P. et al: Post-traumatic arterial priapism in thechild: a study of four cases. Eur J Pediatr Surg, 10: 72, 2000
HIGH FLOW PRIAPISM AND SEXUAL FUNCTION 647












![Short circuit followup[1]](https://img.pdfslide.us/doc/110x75/556264fad8b42ae87d8b4ffa/short-circuit-followup1.jpg)