CAVERNOUS SINUS
CAVERNOUS SINUSSurgical anatomy and Cavernous Sinus
ThrombosisDr. Mukhallat Qazi1st Year PostgraduateDepartment of
OMFSOVERVIEW Introduction Development AnatomyStructures
withinStructures aroundTributaries
2Cavernous Sinus Thrombosis Clinical Presentation Danger Area of
the Face Investigations Neuroradiology Complications Treatment
INTRODUCTION3The space or compartment commonly called the
cavernous sinus is a veritable anatomical jewel box containing more
significant structures than any other comparable space outside the
brain itself. (Parkinson 1990)
Cavernous+ SinusCavernous- Cavern: A large cave or chamber in a
cave specific type of cave, naturally formed in soluble rock with
the ability to grow speleothems
Sinus- Medieval Latin: A hollow curve or cavity in the
bodyCalled Circular sinus" by Ridley (1695)Wilson(1732)Named this
structure CAVERNOUS SINUS Due to its spongious structure which
seemed to be formed by numerous fibres and connective tissue
septae4
Dural SinusesLie between the endosteal and meningeal layers of
dura materAre lined by endothelium, firm collagenous tissueHave no
valvesWalls are devoid of muscular tissueNumerous lacunes and
trabeculae56
DEVELOPMENTPadget (1956)Cavernous sinus Plexiform extension of
prootic sinus and ventral myelencephalic veinSuperior ophthalmic v
Primitive maxillary v as it drains into the prootic sinus, and
develops into the superior ophthalmic vein which drains directly
into the cavernous sinus.778Knosp (1987)20% of fetal skull bases-
SMCV drains into the Cavernous Sinus60% of fetal skull bases- SPS
and Cavernous Sinus show a connectionHence developmental basis for
varied pattern of venous tributaries and drainage
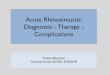
9Schematic drawings of the developmental anatomy of cavernous
and para-cavernous venous structures in the embryonic stage.
S. Tanoue et al. AJNR Am J Neuroradiol 2006;27:1083-10892006 by
American Society of NeuroradiologySchematic drawings of the
developmental anatomy of cavernous and para-cavernous venous
structures in the embryonic stage. SSS indicates superior sagittal
sinus; PTS, primitive tentorial sinus; PS, prootic sinus; PMS,
primitive maxillary sinus; and IPS, inferior petrosal sinus.A,
Lateral view; B, axial view. In an 8-week embryo, cerebral venous
structures develop from primitive dural plexuses surrounding
primitive cerebral vesicles. The plexuses fuse to form venous
sinuses and cortical veins. Two major primitive sinuses, the
primitive tentorial sinus and the prootic sinus, contribute to the
development of cavernous sinus and para-cavernous sinus veins. The
primitive SMCV is connected with the transverse sinus via the
primitive tentorial sinus.C, In a 12-week embryo, after several
weeks, the primitive SMCV is elongated and develops anteromedially
to form the SMCV as a development of the cerebral hemisphere. The
prootic sinus contributes to form the superior ophthalmic vein, the
cavernous sinus, and the foramen ovale venous plexus.D, Axial view;
E, lateral view. In a developed embryo, the SMCV makes further
anteromedial development in the prenatal stage; however, in many
patients, there is no direct connection between the SMCV and the
cavernous sinus. Secondary anastomosis after birth may form a
connection between the SMCV and the cavernous sinus, and the
connection to the primitive tentorial sinus subsequently
degenerates.ANATOMY11
Number 2, Paired Dimensions Length 20mm Width 09mmLocation
Middle Cranial Fossa Either side of body of sphenoid Extent From
Superior Orbital Fissure to the Petrous apex of Temporal bone Shape
Triangular in cross section, Boat shaped12
STRUCTURES WITHIN.. CONTENTS1314
Anatomical Relations1516
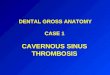
The CS in parasagittal views. A. Osteology. OF, optic foramen;
SOF, superior orbital fissure; FR, foramen rotundum; CC, carotid
canal; Se, sella turcica; Ac, anterior clinoid process; Pc,
posterior clinoid process. Note that the optic canal runs medial to
the Ac. B. Venous plexus. The plexus consists of large-caliber
fenestrated venous spaces that may communicate with the
contralateral CS through foramina in the medial bony wall. II,
optic nerve; PG, pituitary gland. C. The carotid siphon and
sympathetic plexus. The ophthalmic artery is given off as the first
major intracranial branch of the internal carotid artery just as it
exits the roof of the CS. Smaller meningeal branches are not shown.
The sympathetic nerve supply travels as a neural plexus (not shown)
around the carotid artery, entering the orbit with the ophthalmic
artery and through the superior orbital fissure. ICA, internal
carotid artery (carotid siphon); OA, ophthalmic artery. D. Cranial
nerve supply. All cranial nerves except the abducens travel through
the CS tightly adherent to the lateral dural wall. The abducens
nerve has an unpredictable course through the venous plexus but is
usually adherent at least in part to the carotid siphon. Note how
the abducens nerve travels vertically over the petrous ridge and
becomes tethered by Gruber's ligament just before entering the CS.
This tethering predisposes the abducens nerve to deceleration
injury in head trauma. The maxillary division is closely
associated, but outside, the CS. The parasympathetic nerve supply
to the globe travels within the oculomotor nerve. III, oculomotor
nerve; IV, trochlear nerve; V-1, ophthalmic division (trigeminal
nerve); V-2, maxillary division; V-3, mandibular division; VI,
abducens nerve. E. The lateral dural wall. (Modified from Zide BM,
Jelks GW: Surgical Anatomy of the Orbit, p 8. New York, Raven
Press, 1985) 16Osseous Relations171718
ANTERIOROptic strutAnterior clinoid processLesser wing of
sphenoidMEDIALCarotico-clinoid foramenMiddle clinoid
processPituitary fossaBody of sphenoidCarotid sulcusLATERALGreater
wing of sphenoidForamina (rotundum, ovale,
spinosum)POSTERIORPosterior Cliniod ProcessDorsum SellaPetrous
ApexTrigeminal Impression
1819
Ant Clin Process Carotid sulcus- Course of ICA Optic Strut-
Lateral and inferior wall of the optic canalThese three structures
almost encircle the ICA CLINICAL SIGNIFICANCE OF OSSEOUS
RELATIONS
In surgically exploring cavernous sinus, an initial step is to
unlock the contents of the sinus from the bony confines.This step
includes unroofing and mobilizing the optic nerve, and then
removing anterior clinoid process.This phase can be performed in an
extradural or intradural fashion.
DURAL RELATIONS
Floor formed by single periosteal layer of dura,
supero--medially it continues with dura of sella turcica.2122
ROOFAnterior extension of the Tentorium CerebelliLateral
extension of Diaphragma SellaRoofAnteriorDura lining the lower
margin of Ant Clin Process- Anterior Clinoidal FoldPosterior
Posterior Clinoidal FoldPatch of dura- Occulomotor triangle
2223
Posterior WallLower margin shared with basilar sinus, pierced by
Abducens nUpper edge- posterior petroclinoidal foldInferomedial
Triangles are seen2324
25Lateral wall
Dura propria of Uncus of the temporal lobe
26
27
Upper and lower dural rings
The segment of the internal carotid artery located between the
upper and lower dural rings, which is exposed by removing the
anterior clinoid process, is referred to as the clinoid segment.The
dura lining and extending medially from the upper surface of the
anteriorclinoid forms the lateral part of a dural ring, referred to
as the upper or distal ring, which defines the upper margin of the
carotids clinoid segment Further medially, the dura forming the
upper ring blends into the diaphragma sellae.27NEURAL
RELATIONSCranial nerves III to VI are closely related to cavernous
sinus.
Oculomotor Nerve29
30
Trochlear Nerve31Ophthalmic Nerve32
33
Abducens Nerve34
Exit through the SOF and supplies the Superior Oblique mClinical
SignificanceCranial nerve palsy is the most common manifestation of
pathologic processes involving the cavernous sinus.
Diplopia, Sixth nerve palsy with Horners Syndrome, impaired
visual acuity may suggest cavernous sinus lesions.
Most cavernous sinus explorations are for benign disease with
the goal of preserving and improving cranial nerve function.
Exploration of cavernous sinus usually follows mobilization of
lateral wall and entry through one or more of the various triangles
formed by these cranial nerves and dural folds.
35Horner syndrome (Horners syndrome) results from an
interruption of the sympathetic nerve supply to the eye and is
characterized by the classic triad of miosis (ie, constricted
pupil), partial ptosis, and loss of hemifacial sweating (ie,
anhidrosis)35Anatomic Triangles
Vascular Relations37Arterial RelationsInternal Carotid Artery
and its anatomically divided course-Petrous
CavernousIntracranialVenous RelationsAfferent TributariesEfferent
DrainageInternal carotid artery38
39
Petrous part40
ICA ascends to reach itsbifurcation into the middle and anterior
cerebralartery (MCA and ACA) to form the circle of Willis4041
42Veinous relationsTributaries (afferent veins): Superior
ophthalmic vein (SOV) Inferior ophthalmic vein (IOV)Central retinal
vein Superficial middle cerebral vein (SMCV) Uncal vein (UV)
Sphenoparietal sinus (SPPS) Meningeal veins43
Drainage (efferent veins):
Foramen ovale plexus (FOP)Vein of the foramen rotundumPterygoid
plexus (PP)Internal jugular vein (IJV)Facial vein (FV)Angular vein
(AV)Retromandibular veinSupraorbital veinFrontal vein (FrV)44
45
Basilar plexus (BP)Sphenoparietal sinus (SPPS)Sigmoid sinus (SS)
Superior petrosal sinus (SPS)Inferior petrosal sinus
(IPS)Intercavernous sinus (ICS)Jugular bulb (JB)Middle temporal
vein (MTV)46
COMMUNICATIONS OF CAVERNOUS SINUSVenous blood from the brain
flows via the superficial( cortical) and the deep cerebral veins
into the venous (dural) sinuses. There are numerous connections
between the cortical veins and dural sinuses. This facilitates the
spread of thrombus infection between these vessels. Also allows
opening of collateral draining vessels in the event of an
occlusion.Summary of communicationThe cavernous sinuses receive
blood from cerebral veins the ophthalmic veins (from the orbit)
emissary veins (from the pterygoid plexus of veins in the
infratemporal fossa). These connections provide pathways for
infections to pass from extracranial sites into intracranial
locations. In addition, because structures pass through the
cavernous sinuses and are located in the walls of these sinuses,
they are vulnerable to injury due to inflammation.
49
Clinical significance of Vascular RelationsLesion of surgical
importance affecting ICA range from aneurysm to carotid-cavernous
fistulae.After removal of anterior clinoid process, mobilization of
anterior loop of ICA can be done for clipping of aneurysm.Treatment
of aneurysm ranges from simple observation to balloon occlusion and
trapping of the lesion with or without bypass.Conditions affecting
Cavernous sinus and its contents Midbrain Infection Cavernous Sinus
Thrombosis Orbital FracturePetrous Bone Fracture (Temporal bone
Fracture ) Internal Carotid Artery Aneurysm MastoiditisIncreased
Intracranial Pressure
Clinical and applied aspects It is the only anatomic location in
the body in which an artery travels completely through a venous
structure. If the internal carotid artery ruptures within the
cavernous sinus, an atriovenous fistula is created.Cavernous sinus
syndrome may result from mass effect from a tumour or CST and cause
opthalmoplegia from compression of the oculomotor nerve, trochlear
nerve, and abducens nerve, ophthalmic sensory loss from compression
of the ophthalmic nerve, and maxillary sensory loss from
compression of the maxillary nerve.Cavernous sinus thrombosis is
the formation of a blood clot within the cavernous sinus. Emissary
Veins53Emissary Syn. ambassadorFrom skull veins to external
veinsImportance- to maintain intracranial and extracranial venous
pressure at an equilibrium, valve-less to ensure the same.May carry
Infected thrombus from extracranial to intracranial circulation
The emissary veins are valveless veins which normally drain from
the dural venous sinuses into veins that lie outside the skull
(external veins) Usually, the body takes the help of muscle
contraction to pump blood up the veins. So, when the muscles
contract, they squeeze blood up in the veins. When this happens,
there should be mechanism to prevent blood from going back. This is
where the valves come in to play. They prevent backward flow of
blood. Veins have valves because they contain blood that flows at a
low pressure while arteries do not have valves because they contain
blood that flows at high pressure. Valves prevent the back flow of
blood which would normally occur in the veins as a result of the
low pressure compared to arteries where the heart provides the
pressure needed to send blood through the system.
53CAVERNOUS SINUS THROMBOSISThrombosis of the cavernous sinus is
one of the most dramatic of neuro-ophthalmic conditions. Within a
short period, a swollen orbit, limited ocular motility and impaired
vision develop, and may progress to a life threatening
conditionRapid diagnosis and therapeutic action are required.
Morbidity is high, and outcome cannot be
certain.54EpidemiologyFrequency: In the US occurrence of CST has
always been low, with only a few hundred case reports in the
medical literature. The majority of these date from before the
modern antibiotic era. One review of the English language found
only 88 cases from 1940 -1988.Mortality/ morbidity: Prior to the
advent of affective antimicrobial agents, the mortality rate from
CST was effectively 100%. Typically death is due to sepsis or
central nervous system infection. With aggressive management the
mortality rate is now less than 30%. Morbidity however remains high
and complete recovery is rare. Roughly one sixth of patients are
left with some degree of visual impairment and one half have
cranial nerve deficits. Race : no predilection Sex: no predilection
Age : all ages are affected with a mean of 22 years
55Causes of cavernous sinus thrombosis56Danger area of the
face57
Odontogenic origin of CVTCST is one of the major complications
resulting from infection of teeth or surrounding structures in the
upper and lower jaws.Extraction of mandibular molars (Buccal Space)
and maxillary anterior teeth (Infraorbital Space) in the presence
of acute infection, usually staphylococcal, can cause this
condition.The infection can spread by Direct
Hematogenous(metastatic )
Infra Temporal Space Pterygoid plexus which receives tributaries
from transverse facial vein, which passes through buccal
space.Buccal space infections that erode the transverse facial vein
may cause ascending thrombophlebitis of pterygoid venous plexus
posterior routeEmissary veins connect pterygoid plexus to the
cavernous sinus through for. of vesalius, ovale and lacerumAngular
vein ascending thrombophlebitis as a result of infraorbital space
infection Ophthalmic vein Anterior route58Direct SpreadSpread by
direct extension via the infratemporal space through the cranial
wall By way of pterygoid plexus and emissary veins, against the
usual flow. This is possible because of the anatomic anomaly of the
absence of valves in the angular, facial and ophthalmic
veins.Staphylococcus aureus More often from upper teeth than lower
teeth.
Heamatogenous SpreadMore often from lower teeth than upper
teethReverse of direct spread.Streptococcus (haemolytic,
non-hemolytic, or viridans) usually associated
59Method of spread into cranial cavity
PtosisProptosisChemosisStarts as unilateral may prgress to
contralateralSystemicToxic appearance, headache nausea giddiness
vomiting and somnolenceFeverProgression- signs of meningitis, brain
abscess 6162
The clinical symptoms of CST vary depending upon the anatomical
structures involved. The most common symptoms are fever, proptosis,
chemosis, and external ophthalmoplegia. Ophthalmoplegia is
extraocular muscle weakness that results (in CST) when cranial
nerves III, IV, and/or VI are damaged due to their passage through
the cavernous sinus. Other symptoms of lethargy, headache,
periorbital swelling, papilledema, and venous engorgement occur in
50%-80% of patients. Decreased visual acuity, sluggish/dilated
pupil, periorbital sensory loss, and decreased corneal reflex are
less frequent symptoms that occur in