Embed Size (px)
Citation preview
Sex-Specific Attention Problems inLong-Term Survivors of PediatricAcute Lymphoblastic LeukemiaNeelam Jain, PhD1,2,3; Pim Brouwers, PhD4,5,6; M. Fatih Okcu, MD, MPH4,5; Paul T. Cirino, PhD1;
and Kevin R. Krull, PhD1,2,3,4
BACKGROUND: Neurocognitive problems are a frequent outcome of chemotherapy for pediatric leukemia,
although individual differences exist in patient outcome. Sex of the patient and age at diagnosis are 2 char-
acteristics that have been associated with differential outcomes. The relation between these patient char-
acteristics and specific attention deficits (ie, initiating, inhibiting, shifting, focusing, sustaining attention,
and working memory) has not been well researched. The purpose of this study was to evaluate the pattern
of attention problems in male and female long-term survivors of pediatric acute lymphoblastic leukemia
(ALL). METHODS: One hundred three long-term survivors (ie, �5 years from diagnosis; 51% boys, mean
age at diagnosis of 3.9 years, and mean time since diagnosis 7.5 years) completed standardized measures
of basic and complex attention skills related to anterior (ie, inhibition, shifting attention, working memory),
posterior (ie, focusing), and subcortical brain systems (ie, sustaining). RESULTS: Treatment intensity was
related to sustained attention, with those patients treated on high-risk protocols displaying significantly
lower performance. Girls performed worse than boys on measures related to the anterior attention system
(ie, shifting attention, P < .042) and the subcortical attention system (ie, sustained attention, P < .001),
whereas boys performed worse than girls on different measures of anterior control (ie, inhibition, P < .039;
working memory, P < .003). CONCLUSIONS: The results of this study suggest that children diagnosed with
and treated for pediatric ALL perform poorly on select measures of attention and executive control, and
that this performance is influenced by sex and treatment intensity. Cancer 2009;115:4238–45. VC 2009
American Cancer Society.
KEY WORDS: acute lymphoblastic leukemia, long-term survivors, attention problems, sex.
Survival rates for childhood acute lymphoblastic leukemia (ALL) have improved significantly duringthe past few decades, with 5-year rates now exceeding 80%.1 However, the intensive therapy required toreach these rates has been associated with increased neurocognitive late effects in several children, oftenonly becoming evident between 2 and 5 years after treatment completion.2,3 Deficits in attention and
Received: November 17, 2008; Revised: January 28, 2009; Accepted: January 30, 2009
Published online June 17, 2009 in Wiley InterScience (www.interscience.wiley.com)
DOI: 10.1002/cncr.24464, www.interscience.wiley.com
Corresponding author: Neelam Jain, PhD, Department of Epidemiology & Cancer Control, St. Jude Children’s Research Hospital, 262 Danny
Thomas Place, MS 735, Memphis, TN 38105-3678; Fax: (901) 595-5845; [email protected]
1Department of Psychology, University of Houston, Houston, Texas; 2Child Psychology, Texas Children’s Hospital, Houston, Texas; 3Department of
Epidemiology and Cancer Control, St Jude Children’s Research Hospital, Memphis, Tennessee; 4Department of Pediatrics, Baylor College of Medicine,
Houston, Texas; 5Texas Children’s Cancer Center, Houston, Texas; 6Division of AIDS & Health and Behavior Research, National Institute of Mental
Health, Rockville, Maryland
The views expressed in this article do not necessarily represent the views of the National Institute of Mental Health, National Institutes of Health,
Health and Human Services, or the US Government.
4238 Cancer September 15, 2009
Original Article

processing speed have consistently been noted as commonlate sequelae.4-6 However, significant individual variabili-ty in neurocognitive outcomes exist, with roughly 20% to40% of survivors demonstrating significant impairment.7
To date, few studies have examined attention problemsand individual variability in a comprehensive manner inchildren treated with chemotherapy only.
Recent studies have associated methotrexate inten-
sity (MTX) with poor neurocognitive outcome, particu-
larly attention problems.8-10 MTX treatment has also
been associated with acute leukoencephalopathy, and
related impact on white matter volume has been corre-
lated to sustained attention problems.11,12 In addition,
individual biologic differences in the pharmacokinetics or
pharmacodynamics of antifolate therapy (ie, MTX) have
been associated with variability in these outcomes. For
example, the presence of specific folate pathway genetic
polymorphisms has been associated with increased rates of
development of problems with inattention in childhood
leukemia survivors.13
Sex of the patient has been identified as a potential
moderator of late effects and neurocognitive outcomes.
Boys are reported to display worse event-free survival at 2
and 5 years after diagnosis, and higher rates of hemato-
logic relapse.14,15 Conversely, girls appear more sensitive
to the purine antimetabolite mercaptopurine, requiring
more frequent dosage decreases in comparison with
boys.16 Girls also appear to be at increased risk for adverse
neurocognitive outcomes after chemotherapy.5,17-19
Differences in neurocognitive outcome may be
related to varied sexual dimorphism in male and female
brains. Throughout maturation boys display more age-
related decreases in gray matter and increases in white
matter volume compared with girls.20 The result is that
girls have a higher percentage of gray matter, whereas boys
have a higher percentage of white matter.21 This differen-
tial neuroanatomical development may predispose girls to
neurocognitive deficits dependent on subcortical white
matter integrity, whereas boys may be more impacted by
disruption of cortical gray matter integrity.22
Previous neurocognitive outcome studies in long-
term survivors of pediatric ALL have examined only lim-
ited aspects of attention problems. The present study
focused on examining attention using a multidimensional
neurocognitive approach that would account for differen-
ces in the anterior and posterior cortical attention systems,
as well as subcortical attention systems. These compo-
nents are different, although overlapping and interde-
pendent, aspects of attention that differentially invoke
related neural substrates. The frontomedial and dorsolat-
eral cortical brain regions of the anterior attention system
account for the capacity to hold and manipulate informa-
tion in working memory, initiate and inhibit or control
goal-directed activities, and shift attention.23 Further-
more, the frontomedial brain regions are connected to
subcortical brain regions via abundant connections.24 The
posterior attention system, particularly the superior tem-
poral and inferior parietal regions, accounts for basic in-
formation processing including filtering and focusing on
incoming information.25 The subcortical attention sys-
tem, comprised of rostral midbrain structures, including
the mesopontine reticular formation and midline and
reticular thalamic nuclei, is involved in the maintenance
of attention or vigilance over time.26
The purpose of this study was to examine patterns of
attention problems in survivors of pediatric ALL as a func-
tion of sex. We hypothesized that girls would be more
likely to demonstrate impairment on measures reflective
of subcortical brain systems because of their relatively
lower ratio of white to gray matter volume in comparison
to boys. Conversely, boys were expected to demonstrate
impairment on measures reflective of anterior cortical
brain systems because of their relatively lower gray to
white matter volume in comparison to girls. Finally, we
expected the attention problems to be mediated by risk
stratification, as determined by factors such as age at diag-
nosis and intensity of treatment.
MATERIALS AND METHODS
Participants
Participants were long-term survivors of pediatric ALL,
routinely referred by their attending oncologist for a neu-
rocognitive evaluation as part of institutional standard of
care. These evaluations were conducted as part of routine
monitoring; thus, patients were a clinical sample of con-
venience. Detailed recruitment information was not
collected for this particular study. However, a similar neu-
rocognitive study conducted in the same clinic at about
the same time and using similar recruitment procedures,
for which detailed information was available, indicated an
Attention Problems in ALL/Jain et al
Cancer September 15, 2009 4239

82% recruitment rate.7 Approximately 15% of the eligible
patients had to be excluded because of lack of sufficient
mastery of the English language. Recruitment patterns are
expected to be comparable for the current investigation.
All participants in the current study had completed ther-
apy at least 2 years previously and were between the ages
of 6 and 16 at the time of the evaluation. For the purposes
of analyses, exclusionary criteria included the presence of
central nervous system disease at diagnosis, history of
relapse, history of bone marrow transplantation, a preex-
isting developmental disorder (eg, Down syndrome),
treatment with cranial radiation, and non-English speaker
status. A total of 103 long-term ALL survivors were iden-
tified as meeting established inclusion and exclusion
criteria.
Procedure
The procedures used in this study were reviewed and
approved by the institutional review board at the Baylor
College of Medicine, Texas Children’s Hospital, and the
University of Houston. Informed consent was obtained
from all parents/legal guardians, and assent for participa-
tion was obtained from the children.
Children participated in a neurocognitive evaluation
using standardized testing procedures. The neurocogni-
tive measures included clinical tests that individually
assessed a broad spectrum of attention constructs, includ-
ing the Digit Span subtest,27 the Gordon Diagnostic Sys-
tem (GDS),28 and the Trail Making Test Parts A and B.29
Shifting attention, inhibitory control, and working mem-
ory (ie, anterior attention system) were assessed through
performance on the Trail Making Test Part B, commis-
sion errors on the GDS, and the backward Digit Span
tests, respectively.30 Focused attention and attention span
(ie, posterior attention system) were assessed through per-
formance on the Trail Making Test Part A and forward
Digit Span tests, respectively.31 Sustained attention (ie,
subcortical attention system) was assessed through the
number of correctly identified targets on the GDS.32,33
Data Analysis
Chi-square tests of independence were used to analyze the
association between sex, risk, and race. Independent-
samples t tests were used to evaluate the association
between the amounts of MTX administered to standard
and high-risk groups. Pearson product-moment correla-
tions were used to assess the association between the
treatment variables and attention outcome measures. Mul-
tivariate analysis of variance (MANOVA) was used to
examine the impact of sex and risk stratification on the out-
come measures. The alpha level was set at .05 for all statisti-
cal tests, and Bonferroni correction was used when
appropriate to account for multiple comparisons. Effect
sizes, the measure of the strength of the relation between 2
variables, were reported as partial eta-square (partial g2)
values for analysis of variance, with a small effect concep-
tualized as 0.01, a moderate effect as 0.06, and a large effect
as 0.14, or Cohen d values for t tests, with a small effect
conceptualized as 0.2, a moderate effect as 0.5, and a large
effect as 0.8.34 Statistical assessments were carried out using
SPSS forWindows Version 15.0 (SPSS Inc., Chicago, Ill).
RESULTS
The sample included a similar number of girls and boys
(51% boys, n¼ 53). Caucasian (51.5%) and Hispanic
(35%) children were the predominant ethnic groups. Sex
was not significantly confounded with ethnicity or risk
stratification, although there were proportionately more
high-risk Hispanic children compared with the remainder
of the sample, chi-square (2, n¼ 103)¼ 6.23, P < .044.
Demographic information for the sample is reported in
Table 1.
A 1-way between-groups MANOVA was performed
to investigate the relation between sex and performance
on outcome measures, F6,96¼ 9.73, P < .001, partial
g2¼ 0.38. When the results for the dependent variables
Table 1. Demographic Data for Total Study Sample
Age atDiagnosisMean (SD)
Age atEvaluationMean (SD)
SexGirls, n550 3 y, 11 mo (2 y, 4 mo) 11 y, 8 mo (2 y, 7 mo)*
Boys, n553 3 y, 10 mo (1 y, 10 mo) 11 y, 2 mo (2 y, 7 mo)*
RiskHigh, n537 3 y, 4 mo (2 y, 4 mo) 11 y, 1 mo (2 y, 5 mo)*
Standard, n566 4 y, 2 mo (1 y, 11 mo) 11 y, 7 mo (2 y, 8 mo)*
SD indicates standard deviation.
* Independent-samples t test results for group differences were not signifi-
cant at P < .05.
Original Article
4240 Cancer September 15, 2009
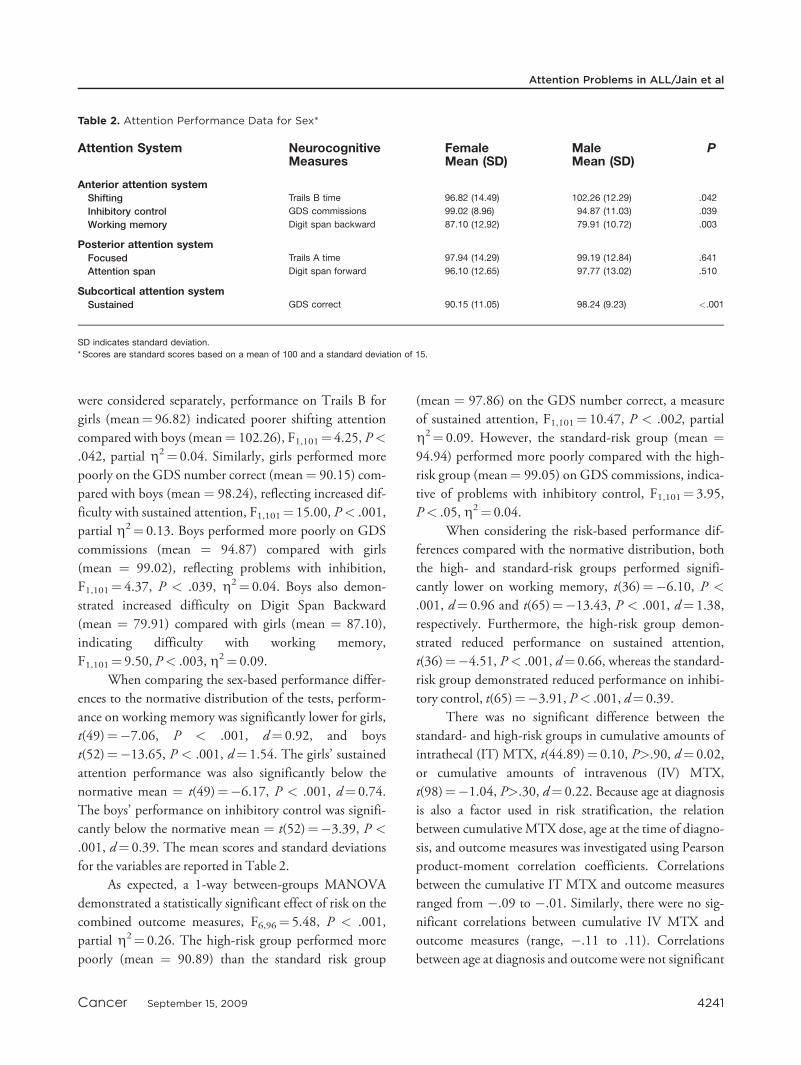
were considered separately, performance on Trails B for
girls (mean¼ 96.82) indicated poorer shifting attention
compared with boys (mean¼ 102.26), F1,101¼ 4.25, P<
.042, partial g2¼ 0.04. Similarly, girls performed more
poorly on the GDS number correct (mean¼ 90.15) com-
pared with boys (mean ¼ 98.24), reflecting increased dif-
ficulty with sustained attention, F1,101¼ 15.00, P< .001,
partial g2¼ 0.13. Boys performed more poorly on GDS
commissions (mean ¼ 94.87) compared with girls
(mean ¼ 99.02), reflecting problems with inhibition,
F1,101¼ 4.37, P < .039, g2¼ 0.04. Boys also demon-
strated increased difficulty on Digit Span Backward
(mean ¼ 79.91) compared with girls (mean ¼ 87.10),
indicating difficulty with working memory,
F1,101¼ 9.50, P< .003,g2¼ 0.09.
When comparing the sex-based performance differ-
ences to the normative distribution of the tests, perform-
ance on working memory was significantly lower for girls,
t(49)¼�7.06, P < .001, d¼ 0.92, and boys
t(52)¼�13.65, P < .001, d¼ 1.54. The girls’ sustained
attention performance was also significantly below the
normative mean ¼ t(49)¼�6.17, P < .001, d¼ 0.74.
The boys’ performance on inhibitory control was signifi-
cantly below the normative mean ¼ t(52)¼�3.39, P <
.001, d¼ 0.39. The mean scores and standard deviations
for the variables are reported in Table 2.
As expected, a 1-way between-groups MANOVA
demonstrated a statistically significant effect of risk on the
combined outcome measures, F6,96¼ 5.48, P < .001,
partial g2¼ 0.26. The high-risk group performed more
poorly (mean ¼ 90.89) than the standard risk group
(mean ¼ 97.86) on the GDS number correct, a measure
of sustained attention, F1,101¼ 10.47, P < .002, partial
g2¼ 0.09. However, the standard-risk group (mean ¼94.94) performed more poorly compared with the high-
risk group (mean¼ 99.05) on GDS commissions, indica-
tive of problems with inhibitory control, F1,101¼ 3.95,
P< .05,g2¼ 0.04.
When considering the risk-based performance dif-
ferences compared with the normative distribution, both
the high- and standard-risk groups performed signifi-
cantly lower on working memory, t(36)¼�6.10, P <
.001, d¼ 0.96 and t(65)¼�13.43, P < .001, d¼ 1.38,
respectively. Furthermore, the high-risk group demon-
strated reduced performance on sustained attention,
t(36)¼�4.51, P< .001, d¼ 0.66, whereas the standard-
risk group demonstrated reduced performance on inhibi-
tory control, t(65)¼�3.91, P< .001, d¼ 0.39.
There was no significant difference between the
standard- and high-risk groups in cumulative amounts of
intrathecal (IT) MTX, t(44.89)¼ 0.10, P>.90, d¼ 0.02,
or cumulative amounts of intravenous (IV) MTX,
t(98)¼�1.04, P>.30, d¼ 0.22. Because age at diagnosis
is also a factor used in risk stratification, the relation
between cumulative MTX dose, age at the time of diagno-
sis, and outcome measures was investigated using Pearson
product-moment correlation coefficients. Correlations
between the cumulative IT MTX and outcome measures
ranged from �.09 to �.01. Similarly, there were no sig-
nificant correlations between cumulative IV MTX and
outcome measures (range, �.11 to .11). Correlations
between age at diagnosis and outcome were not significant
Table 2. Attention Performance Data for Sex*
Attention System NeurocognitiveMeasures
FemaleMean (SD)
MaleMean (SD)
P
Anterior attention systemShifting Trails B time 96.82 (14.49) 102.26 (12.29) .042
Inhibitory control GDS commissions 99.02 (8.96) 94.87 (11.03) .039
Working memory Digit span backward 87.10 (12.92) 79.91 (10.72) .003
Posterior attention systemFocused Trails A time 97.94 (14.29) 99.19 (12.84) .641
Attention span Digit span forward 96.10 (12.65) 97.77 (13.02) .510
Subcortical attention systemSustained GDS correct 90.15 (11.05) 98.24 (9.23) <.001
SD indicates standard deviation.
* Scores are standard scores based on a mean of 100 and a standard deviation of 15.
Attention Problems in ALL/Jain et al
Cancer September 15, 2009 4241

and ranged from�.16 to .11. The mean scores and stand-
ard deviations for the variables are reported in Table 3.
The interaction between sex and risk stratification
on the outcome measures did not reach significance,
F6,94¼ 0.53, P> .78,g2¼ 0.03.
DISCUSSION
Sex of the participant was associated with the type of
attention deficit they experienced. Girls performed more
poorly than boys on tasks commonly associated with the
frontomedial anterior attention system and the subcortical
attention system. Specifically, they had difficulty with
shifting attention (ie, rapidly alternating between 2 sets of
information) and with sustaining attention over time (ie,
continuously differentiating rapidly presented target from
nontarget stimuli over a lengthy time course). Although
performances for both girls and boys remained within the
average range, and the associated statistically significant
difference was small, the performance of the girls is a
relative weakness, and previous research suggests that it
may indicate a decline from expected levels of function-
ing.35-37 Both the shifting attention and sustained atten-
tion tasks are speed dependent, and likely rely upon the
integrity of anterior white matter.38,39 Conversely, boys
performed more poorly than girls on tasks commonly
associated with the cortical anterior attention system. Spe-
cifically, boys had difficulty with working memory and
inhibitory control over responding. Both of these skills
involve cortical control over more basic processes and, as
such, are often referred to as executive functions. They are
typically considered to be dependent upon the integrity of
neocortical prefrontal brain areas (ie, those areas in the
dorsolateral prefrontal system that are dependent upon
gray matter integrity), and less dependent upon white
matter integrity.40,41
These differences between the performance of boys
and girls on the neurocognitive measures may be related
to sex-based differences in brain morphology and matura-
tion. As indicated earlier, the rates of myelination of vari-
ous brain regions differ between boys and girls during
early development, with boys displaying a larger increase
in white matter development during childhood.20 This
rapid increase in myelination in boys may buffer them
from processes that impact white matter development and
enhance subsequent performance on tasks dependent on
white matter integrity, as in the case of chemotherapeutic
treatment for ALL. Consistent with the findings of this
study, it would be expected that boys would evidence dif-
ficulties on tasks mediated by gray matter, as their rate of
gray matter development during childhood is slower than
that for girls. The converse is true for girls, who experience
a slower rate of white matter development, which subse-
quently would result in reduced performance on tasks
related to white matter functioning, a finding that is also
consistent with the current results.
There was a significant difference between high- and
standard-risk groups in performance on neurocognitive
measures of attention. Specifically, performance on the
measures of inhibitory control and sustained attention
differed between the groups, with effect sizes within the
small to moderate range.34 Children treated on high-risk
protocols performed worse on the measure of sustained
attention than children treated on standard-risk protocols.
Table 3. Attention Performance Data for Risk*
Attention System NeurocognitiveMeasures
High RiskMean (SD)
Standard RiskMean (SD)
P
Anterior attention systemShifting Trails B time 100.19 (13.44) 99.30 (13.67) .751
Inhibitory control GDS commissions 99.05 (9.23) 94.94 (10.52) .05
Working memory Digit span backward 86.22 (13.75) 81.79 (11.01) .077
Posterior attention systemFocused Trails A time 98.78 (12.45) 98.79 (14.16) .999
Attention span Digit span forward 99.86 (11.02) 95.30 (13.61) .085
Subcortical attention systemSustained GDS correct 90.89 (12.29) 97.86 (9.35) .002
SD indicates standard deviation.
* Scores are standard scores based on a mean of 100 and a standard deviation of 15.
Original Article
4242 Cancer September 15, 2009

However, children treated on high-risk protocols per-
formed better on the measures of inhibitory control.
Although at first glance this pattern seems contradictory,
the relation between these 2 outcome measures warrants
further consideration. By definition, individuals who
demonstrate reduced sustained attention in a task are not
as engaged and are, thus, less likely to engage in disinhib-
ited responding. In other words, to demonstrate poor in-
hibitory control, one must be engaged and sustaining
attention to the task to which one is disinhibited.
These results are consistent with previous literature
demonstrating treatment-related group differences in per-
formance on measures of attention. The performance of
the high-risk group on measures of sustained attention
suggests difficulty maintaining a high state of readiness to
respond to the demands of the task over an extended pe-
riod of time. This ability to sustain attention is directly
related to executive functioning skills, which are largely
mediated by the frontal and prefrontal cortices in the
brain.42 Children who received higher doses of chemo-
therapy are more susceptible to interruption of myelina-
tion development in the brain, which has been evidenced
by leukoencephalopathy in frontal white matter regions
during active treatment and acute recovery and in postero-
temporal/parietal and occipital white matter regions dur-
ing long-term recovery from treatment.12,43,44 These
anatomical interruptions to development are reportedly
related to problems with attention and processing speed.43
Disruption of myelination to the prefrontal, frontal, and
subcortical brain regions would make these children vul-
nerable to the associated deficits in the ability to sustain
attention.5
Overall, this study characterized the nature of atten-
tion problems in a large sample of children treated for
ALL with chemotherapy. The results confirm that long-
term survivors of ALL have a specific pattern of problems
with the anterior and subcortical attention systems after
chemotherapy treatment. Risk level, as traditionally
defined for medical management, does not fully account
for the pattern or degree of attention problems. Sex-based
attentional differences, which may be related to an inter-
action of disruption of myelination and neuroanatomical
sexual dimorphism, contribute to the pattern and degree
of attention problems.
Given that this sample was 1 of clinical convenience,
generalization to the rest of the population who are survi-
vors of pediatric leukemia may be limited. Another limita-
tion was that several treatment protocols were used, and as
a function thereof, the amounts of IV and IT MTX
administered were inconsistent across participants; this
could have resulted in increased type 2 error and conse-
quently failure to identify additional factors that may have
influenced the sex and outcome effect. It will be impor-
tant for future studies to be sensitive to the differences in
patient and treatment characteristics that are most likely
to result in attention difficulties and to comprehensively
assess attention to better define sex- and treatment-based
attentional difficulties. To further assess the attention
problems found in this population, future studies will
need to evaluate the specific nature of the myelination dis-
ruption in addition to performing neurocognitive testing.
Future research with this population should be prospec-
tive in design and should include neuroimaging so as to
capture concurrent measurements of white matter devel-
opment and attentional dysfunction in each participant in
an effort to further develop individualized and targeted
interventions. Such interventions may be differentiated by
sex and age and then further tailored to each individual
participant based on their particular attentional needs.
Despite the stated limitations, this study provides the basis
for refined research on attention through a systematic
approach to evaluating the moderating effect of sex and
risk after brain insult. Furthermore, the results illuminate
the specific types of attention-related problems experi-
enced by long-term survivors of ALL.
Conflict of Interest Disclosures
The authors made no disclosures.
References
1. Gurney JG, Bondy ML. Epidemiology of childhood cancer.In: Pizzo PA, Poplack DG, eds. Principles and Practice ofPediatric Oncology. 5th ed. Philadelphia, PA: Lippincott,Williams, & Wilkins; 2006:1-13.
2. Bhatia S. Late effects among survivors of leukemia duringchildhood and adolescence. Blood Cells Mol Dis. 2003;31:84-92.
3. Moleski M. Neuropsychological, neuroanatomical, and neu-rophysiological consequences of CNS chemotherapy foracute lymphoblastic leukemia. Arch Clin Neuropsychol. 2000;15:603-630.
Attention Problems in ALL/Jain et al
Cancer September 15, 2009 4243
4. Brown RT, Madan-Swain A, Walco GA, et al. Cognitiveand academic late effects among children previously treatedfor acute lymphocytic leukemia receiving chemotherapy asCNS prophylaxis. J Pediatr Psychol. 1998;23:333-340.
5. Buizer AI, de Sonneville LM, van den Heuvel-EibrinkMM, Veerman AJ. Chemotherapy and attentional dysfunc-tion in survivors of childhood acute lymphoblastic leuke-mia: effect of treatment intensity. Pediatr Blood Cancer.2005;45:281-290.
6. Mennes M, Stiers P, Vandenbussche E, et al. Attention andinformation processing in survivors of childhood acute lym-phoblastic leukemia treated with chemotherapy only.Pediatr Blood Cancer. 2005;44:478-486.
7. Krull KR, Okcu MF, Potter B, et al. Screening for neuro-cognitive impairment in pediatric cancer long-term survi-vors. J Clin Oncol. 2008;26:4138-4143.
8. Carey ME, Hockenberry MJ, Moore IM, et al. Brief report:effect of intravenous methotrexate dose and infusion rateon neuropsychological function 1 year after diagnosis ofacute lymphoblastic leukemia. J Pediatr Psychol. 2007;32:189-193.
9. Brown RT, Madan-Swain A, Pais R, Lambert RG, Sexson S,Ragab A. Chemotherapy for acute lymphocytic leukemia: cog-nitive and academic sequelae. J Pediatr. 1992;121:885-889.
10. Waber DP, Urion DK, Tarbell NJ, Niemeyer C, Gelber R,Sallan SE. Late effects of central nervous system treatmentof acute lymphoblastic leukemia in childhood are sex-dependent. Dev Med Child Neurol. 1990;32:238-248.
11. Reddick WE, Glass JO, Helton KJ, et al. Prevalence of leu-koencephalopathy in children treated for acute lymphoblas-tic leukemia with high-dose methotrexate. AJNR Am JNeuroradiol. 2005;26:1263-1269.
12. Reddick WE, Shan ZY, Glass JO, et al. Smaller white-mat-ter volumes are associated with larger deficits in attentionand learning among long-term survivors of acute lympho-blastic leukemia. Cancer. 2006;106:941-949.
13. Krull KR, Brouwers P, Jain N, et al. Folate pathway geneticpolymorphisms are related to attention disorders in child-hood leukemia survivors. J Pediatr. 2008;152:101-105.
14. Shuster JJ, Wacker P, Pullen J, et al. Prognostic significanceof sex in childhood B-precursor acute lymphoblastic leuke-mia: a Pediatric Oncology Group Study. J Clin Oncol.1998;16:2854-2863.
15. Margolin JF, Steuber CP, Poplack DG. Acute lymphoblas-tic leukemia. In: Pizzo PA, Poplack DG, eds. Principlesand Practice of Pediatric Oncology. 5th ed. Philadelphia,PA: Lippincott, Williams, & Wilkins; 2006:538-590.
16. Hale JP, Lilleyman JS. Importance of 6-mercaptopurinedose in lymphoblastic leukaemia. Arch Dis Child. 1991;66:462-466.
17. Jain N, Brouwers P, Krull KR, Law R, Bottomley S,Dreyer ZE. Treatment length and gender affect outcomefor childhood leukemia survivors. J Int Neuropsychol Soc.2003;91:261.
18. Langer T, Martus P, Ottensmeier H, Hertzberg H, Beck JD,Meier W. CNS late-effects after ALL therapy in childhood. PtIII: Neuropsychological performance in long-term survivorsof childhood ALL: impairments of concentration, attention,and memory.Med Pediatr Oncol. 2002;38:320-328.
19. Buizer AI, De Sonneville LM, van den Heuvel-EibrinkMM, Njiokiktjien C, Veerman AJ. Visuomotor control insurvivors of childhood acute lymphoblastic leukemia treatedwith chemotherapy only. J Int Neuropsychol Soc. 2005;11:554-565.
20. De Bellis MD, Keshavan MS, Beers SR, et al. Sex differen-ces in brain maturation during childhood and adolescence.Cereb Cortex. 2001;11:552-557.
21. Cosgrove KP, Mazure CM, Staley JK. Evolving knowledgeof sex differences in brain structure, function, and chemis-try. Biol Psychiatry. 2007;62:847-855.
22. Schmithorst VJ, Holland SK, Dardzinski BJ. Developmen-tal differences in white matter architecture between boysand girls. Hum Brain Mapp. 2008;29:696-710.
23. Cohen RA, Sparling-Cohen YA, O’Donnell BF. The Neu-ropsychology of Attention. 1st ed. Norwell, MA: KluwerAcademic Publishers;1993.
24. Tekin S, Cummings JL. Frontal-subcortical neuronal cir-cuits and clinical neuropsychiatry: an update. J PsychosomRes. 2002;53:647-654.
25. Mirsky AF. Disorders of attention: a neuropsychologicalperspective. In: Lyon GR, Krasnegor NA, eds. Attention,Memory, and Executive Function. Baltimore, MD: Paul H.Brookes Publishing Co.; 1996:71-96.
26. Posner MI, Raichle ME.Images of Mind. New York, NY:Scientific American Library; 1994.
27. Wechsler D. Wechsler Intelligence Scale for Children. 3rded. San Antonio, TX: Psychological Corporation; 1991.
28. Gordon M, McClure FD, Aylward GP.The Gordon Diag-nostic System. DeWitt, NY: Gordon Systems, Inc.; 1996.
29. Reitan R.The Halstead-Reitan neuropsychological test bat-tery: theory and clinical interpretation. 2nd ed. Tucson,AZ: Neuropsychology Press; 1993.
30. Davis EP, Bruce J, Gunnar MR. The anterior attentionnetwork: associations with temperament and neuroendo-crine activity in 6-year-old children. Dev Psychobiol.2002;40:43-56.
31. Serber SL, Kumar R, Woo MA, Macey PM, Fonarow GC,Harper RM. Cognitive test performance and brain pathol-ogy. Nurs Res. 2008;57:75-83.
32. Kinomura S, Larsson J, Gulyas B, Roland PE. Activationby attention of the human reticular formation and thalamicintralaminar nuclei. Science. 1996;271:512-515.
33. Greene CM, Braet W, Johnson KA, Bellgrove MA. Imag-ing the genetics of executive function. Biol Psychol. 2008;79:30-42.
34. Cohen J. Statistical Power Analysis for the Behavioral Sci-ence. Hillsdale, NJ: Erlbaum; 1988.
Original Article
4244 Cancer September 15, 2009

35. Nathan PC, Whitcomb T, Wolters PL, et al. Very high-dose methotrexate (33.6 g/m) as central nervous system pre-ventive therapy for childhood acute lymphoblastic leukemia:results of National Cancer Institute/Children’s CancerGroup trials CCG-191P, CCG-134P and CCG-144P.Leuk Lymphoma. 2006;47:2488-2504.
36. Jansen NC, Kingma A, Tellegen P, et al. Feasibility of neu-ropsychological assessment in leukaemia patients shortly af-ter diagnosis: directions for future prospective research.Arch Dis Child. 2005;90:301-304.
37. Janzen LA, Spiegler BJ. Neurodevelopmental sequelae ofpediatric acute lymphoblastic leukemia and its treatment.Dev Disabil Res Rev. 2008;14:185-195.
38. Warner TD, Behnke M, Eyler FD, et al. Diffusion tensorimaging of frontal white matter and executive functioning incocaine-exposed children. Pediatrics. 2006;118:2014-2024.
39. Sperling RA, Guttmann CR, Hohol MJ, et al. Regionalmagnetic resonance imaging lesion burden and cognitivefunction in multiple sclerosis: a longitudinal study. ArchNeurol. 2001;58:115-121.
40. Mahone EM, Martin R, Kates WR, Hay T, Horska A.Neuroimaging correlates of parent ratings of working mem-ory in typically developing children. J Int Neuropsychol Soc.2009;15:31-41.
41. Haldane M, Cunningham G, Androutsos C, Frangou S.Structural brain correlates of response inhibition in bipolardisorder I. J Psychopharmacol. 2008;22:138-143.
42. Arnsten AF. Fundamentals of attention-deficit/hyperactivitydisorder: circuits and pathways. J Clin Psychiatry. 2006;67(suppl 8):7-12.
43. Paakko E, Harila-Saari A, Vanionpaa L, Himanen S, Pyhti-nen J, Lanning M. White matter changes on MRI duringtreatment in children with acute lymphoblastic leukemia:correlation with neuropsychological findings. Med PediatrOncol. 2000;35:456-461.
44. Iuvone L, Mariotti P, Colosimo C, Guzzetta F, RuggieroA, Riccardi R. Long-term cognitive outcome, brain com-puted tomography scan, and magnetic resonance imagingin children cured for acute lymphoblastic leukemia. Cancer.2002;95:2562-2570.
Attention Problems in ALL/Jain et al
Cancer September 15, 2009 4245