Embed Size (px)
Citation preview

Severe, Highly Active,or Aggressive MultipleSclerosis
Mark S. Freedman, MSc, MD, FAAN, FRCPC;Carolina A. Rush, MD, FRCPC
ABSTRACTPurpose of Review: Despite the efficacy of current therapies for relapsing forms ofmultiple sclerosis (MS), there remains a group of patients whose disease fails torespond and warrants a different approach to treatment. This article reviews this formof aggressive MS and proposes a definition and new treatment algorithm. Failingto recognize aggressive MS and initiate more effective therapy will result in a lostopportunity to effectively treat the disease.Recent Findings: Natural history studies, together with the results of contempo-rary clinical trials, help to identify and profile a subset of patients with relapsingMS who have a much poorer prognosis and for whom conventional treatmenttends to fail. Therapies that have shown success in the treatment of this patient groupwith aggressive MS are reviewed and discussed.Summary: It is imperative to recognize aggressive MS to effectively treat it beforepatients progress. Recognizing aggressive MS as early as possible is the key to suc-cessful implementation of a proposed algorithm.
Continuum (Minneap Minn) 2016;22(3):761–784.
INTRODUCTIONAlthough some controversy still exists,most believe that multiple sclerosis (MS)is a disease of the central nervous system(CNS) propagated by CNS-directed au-toimmunity that early on is character-ized by inflammation, demyelination,and axonal transection.1 As the diseaseevolves, so does the pathology, and amore diffuse and indolent inflammatorypathology is noted, characterizing theneurodegenerative phase of disease,which to date lacks effective treatment.2
A number of disease-modifying ther-apies have been approved for thetreatment of relapsing forms of MS withvariable success at controlling the earlytype of inflammatory events. However,no treatments exist that can stop orreverse the later type of pathology
characterizing the neurodegenerativephase or its clinical counterpart, pro-gressive MS (either primary or sec-ondary). Natural history studiesrepeatedly inform us that patients withgreater amounts of early disease ac-tivity are more likely to advance to theprogressive phase earlier and faster.3Y5
Conversely, studies have shown thatearly introduction of effective therapymay well stave off the progressivephase.6 It is therefore imperative thateffective early treatment be optimizedto take advantage of the window ofopportunity7 before it closes and pa-tients transition from relapsing to pro-gressive disease.
Before the development of disease-specific therapies for MS, treatmentwas confined to the use of immuno-suppressive agents, limited in dose
Address correspondence toDr Mark S. Freedman,501 Smyth Rd, Ottawa,ON K1H 8L6, Canada,[email protected] Disclosure:Dr Freedman has servedas a consultant for OpexaTherapeutics, Inc, and on theadvisory boards of ActelionPharmaceuticals Ltd; Biogen;Chugai Pharma USA, Inc;EMD Serono, Inc;F Hoffmann-La Roche Ltd;Novartis AG; Sanofi Genzyme;and Teva PharmaceuticalIndustries Ltd. Dr Freedmanserves on the editorial boardsof Multiple Sclerosis Journaland Journal of the NeurologicSciences. Dr Rush has servedas a consultant for SanofiGenzyme and has receivedpersonal compensation forspeaking engagements fromEMD Serono, Inc; the MultipleSclerosis Society of Canada;and Teva PharmaceuticalIndustries Ltd.
Unlabeled Use ofProducts/InvestigationalUse Disclosure:Drs Freedman and Rushdiscuss the unlabeled/investigational use ofocrelizumab, parenteralcladribine, rituximab, andstem cell transplantation forthe treatment of aggressivemultiple sclerosis.
* 2016 American Academyof Neurology.
761Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Review Article
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

and duration of treatment by theirinherent toxicities. At best, such treat-ment approaches seemed to “buy afew years” of time for patients beforethe return of disease activity, but ingeneral, and in part due to theirtoxicities, they were introduced ra-ther late in the course of disease.Today’s disease-specific therapies arenot hampered, for the most part,with lifetime limitations in dosage,allowing for a more continued ap-proach to treatment. Furthermore,many have fewer toxicities comparedwith older immunosuppressive treat-ments and can be introduced earlyin the disease course, when they arelikely to make the biggest difference.Based on the premise of controllingthe important early inflammation inMS, it is imperative that treatmentsget a foothold on the disease with-out sacrificing safety or tolerabilityin often young patients. Currentdisease-modifying therapies are con-centrated on controlling, segregating,blocking, or depleting disease-causingautoimmune cells, thus limiting theirability to enter and damage theCNS. They do so by various proposedmechanisms of action. Unfortunately,not a single one of today’s disease-modifying therapies has been shownto completely control disease activityin all patients, even within the nar-row window of a 2-year clinical trial.A subset of those patients is emerg-ing as having a more aggressive formof disease, warranting perhaps a dif-ferent approach.
Several treatment algorithms havebeen proposed for patients with re-lapsing forms of MS that focus on thetypical patient, starting with the mod-estly effective but safe first-line treat-ments and switching either laterally toan alternate first-line agent or movingto a second- or even third-line disease-modifying therapy if the responseto therapy is suboptimal.8Y10 This ap-
proach should be adequate for mostpatients today and maximizes thebenefit to risk of disease-modifyingtherapy, provided that patient moni-toring is adequate. However, for thesubgroup of patients with a more ag-gressive and rapidly deterioratingcourse marked by rapid accumulationof physical and cognitive deficits de-spite attempted treatment with oneor more disease-modifying therapies,such an approach is clearly subopti-mal. This subgroup of patients is oftenreferred to as having aggressive MS,but no consensus definition or ap-proach to treatment exists for thesepatients. Over the years, many havecome to recognize the existence of thissubgroup of aggressive MS, but defi-nitions have been either vague orambiguous. Common to all is thesomewhat unexpected appearance ofearly advancing disability, often withfrequent disabling relapses that haveincomplete resolution, and highly ac-tive MRI measures. Pragmatically, ag-gressive MS has been defined as MSthat is associated with repeated severeattacks with accelerated accrual of dis-ability or, more simply, rapidly progres-sive MS. The literature also harbors theterm malignant MS, but this definesa heterogeneous group of patients.Some use malignant to describe ful-minant forms of MS that deteriorateso rapidly and progressively from thebeginning that they are almost mono-phasic illnesses and can result in deathwithin a very short time (ie, the Marburgvariant of MS).11 This probably repre-sents the most extreme variant of theaggressive MS spectrum, but othersmay use the term malignant inter-changeably with what will be referredto here as aggressive MS. In its firstrendition, a report on defining theclinical phenotypes of MS included adefinition of malignant MS12 as a “dis-ease with a rapid progressive course,
KEY POINTS
h The window ofopportunity for effectiveearly treatment inmultiple sclerosis isunique for each patient.It most likely opens afterthe first attack inclinically isolatedsyndrome and closes attransition from relapsingmultiple sclerosis tosecondary progressivemultiple sclerosis or laterelapsing-remittingmultiple sclerosis inwhich the presence ofrelapses, MRI activity,and inflammation is nolonger evident.
h The perceptionthat currentdisease-modifyingtherapies are effectivein all patients withrelapsing multiplesclerosis needs to bedispelled. All studiesinclude patientswith considerablebreakthrough diseasethat warrant adifferent approach.
h The ideal monitoringschedule for relapsingmultiple sclerosis(both clinical and MRI)is not agreed upon; itdepends on the levelof concern for eachpatient, based onrelapses, MRI activity,changes in neurologicexamination, andavailability of resources.
762 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

leading to significant disability in mul-tiple neurologic systems or death in arelatively short time after disease on-set.” This committee, however, de-spite recent and increasing concern forearly detection and treatment of ag-gressive MS, did not update its origi-nal definition of malignant MS in itslatest version.13
More succinct attempts at definingaggressive MS have been made. Someresearchers described malignant MSas a subgroup of patients attainingan Expanded Disability Status Scale(EDSS) score of 6.0 within 5 years of MSonset.14 They found that only 12.11% oftheir 487 patients had malignant MS,which was further divided into transientmalignant and sustained malignantbased on whether it was relapse orprogression that was the main con-tributor to the EDSS score. Being older,male, or a smoker made patients morelikely to attain sustained malignantstatus. Conversely, younger patientswith brainstem relapses characterizedthe transient malignant subgroup,identifying specific clinical featuresfor which opportune interventionmight make a difference.
In a 2013 study from BritishColumbia, the definition of aggressiveMS was expanded by defining threesubgroups of criteria, used alone or incombination, based on EDSS scoreand time to progression to secondaryprogressive MS.15 Aggressive MS wasdefined using three slightly differentdefinitions depending on the rapidityof disability accumulation. AggressiveMS1 (AMS1) reached confirmed EDSSscore of 6.0 or more within 5 years fromthe onset of MS symptoms, aggressiveMS2 (AMS2) reached confirmed EDSSscore of 6.0 or more by age 40, and ag-gressive MS3 (AMS3) reached second-ary progressive MS within 3 years of arelapsing onset course. Out of a data-base of 5891 patients, 5.5% fulfilled
criteria for AMS1, 14.0% for AMS2, and4.0% for AMS3. Most important withrespect to treatment considerations,of the first two definitions, whichcould include primary progressive MS,74.5% of AMS1 and 92.8% of AMS2were, in fact, relapsing-onset patients.Thus, aggressive MS could be identi-fied in 4% to 14% of patients, depend-ing on the definition used; the majorityof these are relapsing forms of MS andtherefore amenable to treatments thatcan target early inflammation.
Another definition for aggressiveMS was used to identify eligible can-didates for a trial of immunoablativetherapy followed by autologous hema-topoietic stem cell rescue or transplan-tation. This international consortiumreferred to these patients as havinghighly active MS and at higher riskof poor prognosis. That definitioncombines the failure of conventionaltreatment to control disease with fre-quent severe (disabling) relapses andMRI activity (new T2 or gadolinium-enhancing lesion).16 In addition, how-ever, patients considered for this typeof treatment are also typically restrictedby age, EDSS score, and duration ofMS or time from first treatment.
Any definition for aggressive MSneeds to be both sensitive and specific,but sensitivity is probably more impor-tant. It is likely acceptable today toovertreat some patients who mightnot truly have aggressive MS in favorof not missing anyone warranting treat-ment to prevent the inexorable pro-gressive phase of disease. Previousdefinitions are probably too restric-tive, sacrificing sensitivity for specific-ity in too often failing to identify at-riskpatients who should be offered poten-tially helpful yet aggressive treatments.No consensus exists on how fast pro-gression should occur or a thresholdof disability attained, but probablymost consider that reaching an EDSS
KEY POINT
h To date, aggressivemultiple sclerosis has nouniform definition.
763Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

score of 6.0 represents an upper limitbeyond which the benefit to risk ofan aggressive treatment is likely notwarranted. Others have argued that at-taining even an EDSS score of 4.0 isalready a strong indicator of advancingdisease and that further relapses, evenif prevented, are unlikely to changethe course of progression.3 Therefore,no perfect definition exists, but in anattempt to reasonably describe a pop-ulation that could warrant a moreaggressive approach to therapy, it issuggested that aggressive MS be de-fined as a relapsing form of MS withone or more of the following features:
& EDSS score of 4.0 within 5 yearsof onset
& Poor response to at least 1 full yearof therapy with one or moredisease-modifying therapies, notbecause of intolerance
& Breakthrough disease over at least1 year of disease-modifyingtherapy consisting of:) Two or more disabling relapses
with incomplete resolution) Two ormoreMRI studies showing
new or enlarging T2 lesions orgadolinium-enhancing lesions
Studies now have identified a num-ber of poor prognostic factors thatundoubtedly will also characterizemany patients with aggressive MS.These include male gender; older ageat onset; multifocal attacks involvingmotor, cerebellar, or sphincter func-tion; and cognitive involvement. His-torical attack characteristics may alsoprovide additional prognostic infor-mation: multifocal versus monofocal,motor versus sensory, residual defi-cits unresponsive to steroids,17 andgreater effect on activities of dailyliving.18Y20 Certain MRI characteristicshave also been associated with a poorerprognosis, especially early in the courseof disease, such as T1 black holes at
presentation,21 T2 burden,22Y24 earlypresence of atrophy,25,26 or even loca-tion of the burden of lesions (eg,brainstem and spinal cord).27,28 Al-though useful, these MRI metricshave not yet been shown to particu-larly distinguish an aggressive patternof disease in the absence of concur-rent clinical information either at dis-ease onset or early in the course ofdisease (Table 4-1).
THE NEED FOR EARLY DISEASECONTROLIt is becoming clearer that active earlyMS, although seemingly controllable,takes its toll and leads to earlierprogression. A number of mechanismscontribute to this, such as the inabilityto repair early damage or the degree towhich an individual’s CNS can withstandinjury. However, one of the mostimportant factors may well be the lossof CNS reserve that gets tested as apatient begins to age. Studies haverepeatedly shown that uncontrolleddisabling relapses that occur in thefirst 2 years of disease hasten earlydisease progression, with diminishingcontribution from later relapses as thedisease progresses.17,29 Data derivedfrom patients followed long termfrom their first demyelinating eventas well as data from one of the pivotallong-term trial cohort studies suggestthat long-term outcomes can be pre-dicted based on factors present earlyin the disease. The time to an EDSSscore of 3.0 is a strong independentdeterminant of time to later EDSS scoresof 6.0, 8.0, and 10.0 (death due to MS).29
The inability to contain the early dam-age or heal to recovery is noted in pa-tients with high attack rates and shorterinterattack intervals who convert withina shorter time to secondary progressiveMS. The amount of silent disease, asmanifested by the first MRI at the time
KEY POINT
h Multiple sclerosis hasseveral well-knownclinical and MRI factorsfor poor prognosis.
764 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

TABLE 4-1 Factors Associated With a Poorer Prognosis inMultiple Sclerosis
b Demographics
Male
Older than 40 years at onset
African American, African Latin American
b Relapse Characteristics
Severity of relapse
Moderate/severe (Q1 point change on EDSS or Q2 point change on anyindividual KFS, or Q1 point change on any two KFS)
Steroid requirement
Hospital admission
Type of attack
Multifocal
Partial or incomplete recovery
Affecting motor, cerebellar, sphincteric, or cognitive functions
Frequency
Frequent relapses in the first 2Y5 years
Short interattack interval
b Disease Course
Rapid accrual of disability (EDSS of 3.0 within 5 years with superimposedrelapses)
Progressive from onset
b MRI Features
At onset
High T2 lesion burden
More than two gadolinium-enhancing lesions
Presence of T1-hypointense lesions (black holes)
Early discernable atrophy
Infratentorial versus supratentorial lesions
Follow-up MRI while on treatment
Presence of new T2 lesions
More than one gadolinium-enhancing lesion
EDSS = Expanded Disability Status Scale; KFS: Kurtzke Functional System; MRI = magneticresonance imaging.
765Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

of first presentation, correlates with thedegree of disability seen up to 20 yearsfrom that heralding first event.30 Inpatients converting from relapsing-remitting MS to secondary progressiveMS, the rate of lesion volume changewas 3 times higher than those who didnot convert.
If early inflammation eats up CNSreserve and current medications aremost effective at reducing this inflam-mation, then it makes sense to max-imize the treatment effect wheninflammation is at its peak. Therefore,a window of opportunity for optimiz-ing treatment opens once it is clearthat a patient has MS, likely followingthe first clear demyelinating event.31
One could equally argue that once thisinflammation subsides, it probably in-dicates that the window has closedand likely the patient has entered thesecondary progressive MS phase ofdisease. While the search for effectivetherapeutic strategies for secondaryprogressive MS continues, it is fairlyobvious that most agents demon-strated to be effective at controllingrelapsing MS are ineffective at slow-ing progression in secondary progres-sive MS, notwithstanding their abilityto reduce attack rates or limit MRI ac-tivity. Patients with aggressive MS willhave a narrower window that can closequickly and therefore warrant a differ-ent approach. Conventional treatmentparadigms developed for relapsingMS need to be reconsidered. The nor-mal move to escalate treatment onlyafter failure of a less effective disease-modifying therapy could lead to amissed opportunity to identify andtreat aggressive MS in a timely manner.Similarly, we must avoid the ineffec-tive use of more aggressive treatmentsthat offer “too little too late” in termsof efficacy once disease has evolvedbeyond the stage of relapsing MS,but whose risks may still be formi-
dable, thus presenting a poor risk-benefit ratio.
TREATING AGGRESSIVEMULTIPLE SCLEROSISWe have now an array of effectivetreatments for relapsing MS; however,choosing the best sequence for anindividual can be very challenging. Dowe simply start with the safest, butpossibly least effective, treatments andescalate only when breakthrough dis-ease is evident? Or is there some wayof identifying patients who may war-rant a more aggressive approach,starting with perhaps riskier but per-ceived more effective therapies andeither maintaining them or backingdown to the safer treatments once it isevident that disease is well controlled?Fortunately, for most relapsing MS, anescalation approach is effective, butfor aggressive MS, it clearly is not.Once identified, patients with aggres-sive MS warrant a sustained effort tocontrol disease activity in an attempt tostave off imminent disease progression.
By definition, patients with aggres-sive MS are identified by an early fail-ure to control disease activity withconventional first- or even second-line agents. If one can imagine a rogueforce of aberrant disease-causing in-flammatory immune cells whose mis-sion is to attack CNS myelin and whichcan self-renew ad infinitum, then partof the reason for failure of the usualrelapsing MS treatments is that theyfall short in reducing the size of thisforce. Even therapies that either im-pede the force of disease-causingcells from gaining access to the CNS(eg, natalizumab) or sequester theforce in lymph nodes (eg, fingolimod)will fail in patients with aggressive MS,most of whom will have been tried onone or both of these types of treat-ments. Treating aggressive MS requires
KEY POINTS
h Effectively treatingmultiple sclerosis earlypreserves centralnervous system reservefor aging later in life.
h The ideal sequence inwhich multiple sclerosistreatments should beused has not beenclearly explored. Thesequence maypredispose patients toincreased risk of toxicitydue to compoundedside effects and limitthe successive use ofcertain agents.
766 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

agents immediately capable of signifi-cantly depleting the force of disease-causing cells; these include agentssuch as alemtuzumab; chemothera-peutic treatments such as cladribine,cyclophosphamide, or mitoxantrone;and even a full-on assault using immu-noablation and autologous hemato-poietic stem cell transplantation.
Patients with aggressive MS are athigh risk of further imminent progres-sion and are rapidly running out oftime (ie, their window is closing). Theytherefore warrant a more definitivetreatment, not a temporary fix. First-line agents will have failed, and currentsecond-line agents, such as fingolimodor natalizumab, exert disease controlas long as they are maintained, butboth are associated with a return ofdisease activity if they are stopped. Agradual return of activity is seen withfingolimod discontinuation,32,33 but arapid, sometimes severe, rebound ofdisease activity is observed with stop-ping natalizumab, which can be fatal,especially in patients with aggressiveMS.34,35 The likelihood of achievingthe goals for treatment of aggressiveMS is low, with fingolimod providingthe only partial benefit observed forpatients with highly active relapsingMS seen in clinical trials.36 Similarly,although natalizumab has been usedanecdotally in some patients with ag-gressive MS,37 the propensity for harmin the development of progressivemultifocal leukoencephalopathy withextended use and the potential forsevere rebound should the drug bestopped suddenly are both limitingfactors. Fingolimod too is now associ-ated with the development of progres-sive multifocal leukoencephalopathy,although as yet no clear identifyingfactors have been found to offset therisk. Both therapies must therefore beviewed as unsustainable in the long term.
Drugs Considered for TreatingAggressive Multiple SclerosisThe following treatments (Table 4-238Y56)all share the ability to significantlydeplete disease-causing autoimmunecells. In many cases, they still do noteliminate all the cells; what differenti-ates them is the length of time re-quired before the cells come back anddisease activity returns. In some cases,it may be possible for retreatmentwith another course of the same ther-apy, but in other cases, especiallywhere cumulative dosing leads totoxicity, this may not be possible.Given the propensity for a return ofdisease activity, some feel that a first-line disease-modifying therapy maybe used following the initial treat-ment of aggressive MS with one ofthese agents to extend the initial ben-efit or even maintain it; but thus farlittle evidence exists to support thisstrategy beyond anecdotal reports.
Alemtuzumab. Alemtuzumab is ahumanized monoclonal antibody di-rected against CD52, a surface antigenpresent at high levels on T and Blymphocytes. Alemtuzumab rapidlydepletes lymphocytes, producing a sus-tained depression for up to 1 year.38,57
It is approved mainly for patients withrelapsing MS with breakthrough dis-ease but is proven ineffective for sec-ondary progressive MS.58 It is viewedas probably the most useful currenttherapy as an induction agent in thetreatment of aggressive MS, especiallyin Europe.59 Although trials attest toits benefit in both naıve and break-through patients, with an effect onslowing disease progression and actu-ally improving EDSS score, especiallyin breakthrough patients compareddirectly with a first-line high-dose inter-feron treatment,39 there is still littleexperience in aggressive MS. The big-gest concern with alemtuzumab is the
KEY POINTS
h Effective treatmentfor aggressive multiplesclerosis requiresthe depletion ofdisease-causingimmune cells.
h Aggressive multiplesclerosis warrantsaggressive treatment.These patients arerunning out ofbiological time andhave a narrowertherapeutic window.
767Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

TABLE 4-2 Drugs to Treat Aggressive Multiple Sclerosis
Drug Protocol
Adverse Effects NotDirectly Related toImmunosuppression Monitoring
Alemtuzumab38,39 12 mg/d infusion for5 days followed bysecond course of 12 mg/dfor 3 days at month12 from first course
Infusion-relatedreactions 93%
Mild tomoderate 990%
Serious 3%
Follow treatmentprotocol, symptomaticmanagement
Retreatment with a3-day course in the thirdor subsequent year asdictated by continueddisease activity
Infections 71%
Serious infections 2.7%
Nasopharyngitis
Upper airway tractinfections
Urinary tract infections
No specific recommendation,patient education
Superficial fungalinfections 12%
Oral candidiasis
Vaginal candidiasis
No specific recommendation,patient education
Herpesvirus infections 3%
Oral herpes simplex
Varicella-zosterinfections 0.3%
No specific recommendation,patient education
Cervical human papillomavirus infection 2%
Annual screening for humanpapilloma virus
Thyroid problems 36%
Hyperthyroidism
Hypothyroidism
Graves disease
Thyroidophthalmopathy
Thyroid cancer 0.3%
Thyroid-stimulating hormoneand free T4 every 3 monthsfor 48 months after thefinal infusion, monthlysymptom-monitoring survey
Hematologic problems 1%
Idiopathicthrombocytopenicpurpura
Other cytopenias(neutropenia,hemolytic anemia,pancytopenia)
Monthly blood cell countwith differential andplatelet counts,symptom-monitoring survey,patient education
Nephropathies 0.3%
AntiYglomerularmembrane
Membranousglomerulonephritis
Monthly serum creatinineand urinalysis withmicroscopy, monthlysymptom-monitoringsurvey, patient education
Continued on page 769
768 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

TABLE 4-2 Drugs to Treat Aggressive Multiple Sclerosis Continued from page 768
Drug Protocol
Adverse Effects NotDirectly Related toImmunosuppression Monitoring
Cladribine40,41 Scripps protocol:0.875 mg/kg/d IV for4 days every 6 monthsfor 2 years
Possible long-term riskof malignancy
Cancer screening, patientand primary physicianeducation
Retreatment with two6-month cycles in the thirdor subsequent year asdictated by continueddisease activity
Mitoxantrone Mitoxantrone In MultipleSclerosis Study Group (MIMS)protocol42: 12 mg/m2 IV every3 months for 24 months
Gonadal failure Symptomaticmanagement, patienteducation, fertilitypreservation techniquesprior to treatment
French British Study Protocol43:12Y20 mg/month IV +1 g/month methylprednisoloneIV for 6 months
Amenorrhea in22Y26%44,45
Symptomatic management,patient education, fertilitypreservation techniquesprior to treatment
Lifetime maximum: 140 mg/m2
Liver toxicity Liver functionmonitoring (aspartateaminotransferase andalanine transaminase)
Cardiotoxicity46
Systolic dysfunction12%
Cardiotoxicity 10%
Heart failure 0.4%
Echocardiogram ormultigated acquisitionscan (MUGA) annually for5 years posttreatment
Leukemia 1%46 Blood cell counts every6 months for 5 years
Cyclophosphamide47 Induction protocol48:600 mg/m2 IV for 5 days plus 1 gmethylprednisolone IV andbimonthly boosters
Hemorrhagic cystitis7Y15%49
Prevention with adequatepre- and post-IV hydration,mesna, and frequentvoiding or bladdercatheterization if needed
Pulse protocol50:800Y1000 mg/m2 (with orwithout methylprednisolone)IV monthly for 12Y24 months
Bladder cancer 5.7%51 Urinalysis and cytologyevery 6 months; if cytologyis abnormal, performcystoscopy annually
High-dose protocol52:120Y200 mg/kg/d IV for5 days
Infertility 33Y44.7%53 Symptomatic management,patient education, fertilitypreservation techniquesprior to treatmentLifetime maximum: 80Y100 g54
Brain atrophy55,56 Role for neurocognitiveassessment
IV = intravenous.
769Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

emergence of autoimmune disordersunrelated to MS (eg, thyroid disease,idiopathic thrombocytopenic purpura,or Goodpasture syndrome) that canarise remotely (up to 4 years from thelast exposure) regardless of whetherone or many treatment courses aregiven.60 Fortunately, all of these canbe easily detected with proper mon-itoring. A course of treatment withalemtuzumab entails 5 consecutivedays of treatment in the first year and3 consecutive days in the second year.Unlike the other agents with maximallifetime exposure limits, it appearsthat alemtuzumab can be used beyond2 years intermittently as neededshould the disease return, as a 3-dayannual treatment, as long as morethan 1 year has passed from the lasttreatment and the lymphocyte counthas returned to normal. Data fromextension studies of the phase 3 trials(Comparison of Alemtuzumab andRebif Efficacy in Multiple Sclerosis[CARE-MS] I and CARE-MS II) showedthat more than 80% of patients didnot require retreatment during thethird year, but these studies comprisedmostly patients without aggressive MS.
Cladribine. Cladribine is a syntheticpurine nucleoside and antimetabolitethat acts as an antineoplastic agent withimmunosuppressive effects. It selec-tively reduces lymphocyte subpopula-tions, especially CD4+ and CD8+because these subsets of T cells lackalternative degrading enzymes, leadingto cell-selective sequestration of thenucleoside. Animal data exist showingit is capable of crossing the blood-brain barrier.61
Parenteral cladribine was found tobe beneficial in early phase 2 studiesin relapsing-remitting MS,41,62 but notin secondary progressive MS.40 Oralc ladribine was studied in theCladribine Tablets Treating MS Orally
(CLARITY) study,63 which includedmore than 1000 patients and comparedtwo different doses over 96 weeks.Although both doses produced a sig-nificant reduction in clinical relapsesand MRI activity and slowed diseaseprogression, the higher dose showedno particular benefit, even in a sub-group of patients with highly activeMS. Oral cladribine was subsequentlystudied in a select group of patientswith more active MS who had break-through disease on interferon beta ina study called Oral Cladribine AddedON to Rebif New Formulation in Pa-tients With Active Relapsing Disease(ONWARD), in which patients takingcladribine together with interferon betahad fewer subsequent relapses andgadolinium-enhancing lesions com-pared to the arm taking interferon betaalone, despite the study not beingpowered for these outcomemeasures.The combination of cladribine andinterferon beta also showed a greaterreduction of relapse relative to place-bo following a first demyelinatingevent (clinically isolated syndrome)than any other treatment used at thisstage of disease.64
Although clinical development oforal cladribine has remained on hold,parenteral infusions can still be read-ily used. Most commonly, cladribine isgiven as an initial 2-year course, start-ing with an induction therapy over4 consecutive days and repeated every6 months. Patients can then be fol-lowed and a repeat 1-year course oftreatment offered should disease ac-tivity rekindle, as long as lymphocytelevels have recovered and it has beenmore than 6 months since the lasttreatment. Alternatively, cladribine canbe followed by a first-line treatment tosustain the benefits, although scant dataare available to support that option.
Cladribine remains an option fortreating aggressive MS but can be a
770 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

complicated treatment with signifi-cant toxicity, so it is best given in cen-ters where hematologic expertise andsupport is available. It has at leastsome advantage over other similaragents listed later because it does notnegatively affect fertility, but its long-term safety in MS is unknown.
Cyclophosphamide. Cyclophos-phamide is a broad-spectrum alkylatingcompound used in cancer and autoim-mune diseases. It is a cell cycle non-specific cytotoxic agent that exerts itseffects on both B cells and T cells,suppressing both humoral and cell-mediated immunity.48 It has been usedin various regimens to treat MS for thepast 40 years.
Early studies, mainly in patients withprogressive MS, produced conflictingresults at slowing disease progres-sion. Then a 2-year randomized trial of256 patients with relapsing MS usingdifferent regimens of cyclophospha-mide induction followed or not bymonthly infusions of cyclophospha-mide reported that treatment with thecyclophosphamide boosters was asso-ciated with better disease stabilization;especially in younger patients who hadonly recently converted to secondaryprogressive MS.65 Over the years, manysmall, often single-center, studies havedemonstrated a potential benefit ofcyclophosphamide in refractory, fulmi-nant, or rapidly progressing patientsin at least temporarily slowing downdisease progression or limiting furtherdisabling attacks for 12 or 24 months,depending on the study.47,50,52 Someinterest was given to a regimen termedHigh Cy, which professed to beimmunoablative (as opposed tomyeloablative; refer to the later dis-cussion of autologous hematopoieticstem cell transplantation),66,67 produc-ing clinical and radiologic stability thatcould last more than 3 years.68 A small
study of patients with aggressive MSrefractory to several previous therapiesreceived monthly cyclophosphamideinfusions and were shown to have adramatic reduction in gadolinium-enhancing and T2 lesion load.53 Thisresult was reiterated by a subsequentstudy where gadolinium-enhancing le-sions decreased by 81% over 2 years,69
along with other reports of combi-nation studies of cyclophosphamide(often in association with interferonbeta) that showed significant efficacyin reducing MRI activity.70,71
Cyclophosphamide has significanttoxicity with limitations on lifelong cu-mulative dose (around 80 g to 100 g).Increased risk of malignancy (in partic-ular bladder cancer), hemorrhagic cys-titis, and gonadotoxicity are the mostfeared side effects. The risk of blad-der cancer with cyclophosphamidehas been found to be similar to thegeneral population, contrasting witholder studies, perhaps because of theuse of parenteral cyclophosphamideinstead of the oral formulation used inthe past.72 Experience with the variousregimens dictates which one may beused, but no evidence exists that anyone is superior to another.
Despite the known downside ofcyclophosphamide, attestations to itsefficacy, low cost, extensive availability,and experience keep it on the list ofpotentially useful agents for treatingaggressive MS.
Mitoxantrone. Mitoxantrone is ananthracenedione similar to doxorubicin.It inhibits proliferation of B cells andT cells and suppresses TH1-mediatedcytokines (eg, tumor necrosis factor[TNF]-!, interleukin [IL]-12).73 Mostpatients benefiting from mitoxantronein the pivotal trials were young, hadfrequent relapses and lower EDSSscores, or had an early secondary pro-gressive MS or relapsing MS/aggressiveMS diagnosis.42,43
KEY POINT
h Cyclophosphamide hasbeen resurrected in thetreatment of multiplesclerosis and has avalid position in ourcurrent armamentariumas induction therapyin aggressivemultiple sclerosis.
771Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Mitoxantrone has a moderate effectat reducing disability progression andrelapses in patients with persistentinflammatory activity. The most com-monly used regimen is the inductionprotocol (three doses of 12 mg/m2
monthly followed by six monthlyinfusions of the same dose until amaximum of 110 mg/m2 to 120 mg/m2
has been reached). Cumulative lifetimedoses should not exceed 140 mg/m2.Gonadal dysfunction is a relevant tox-icity in young patients. A full course oftreatment can stabilize patients withaggressive MS for 5 years or more,74
but if maximal lifetime doses arereached, then patients might be betteroff following the treatment with main-tenance of a first-line agent such as in-terferon beta75 or glatiramer acetate.76,77
Despite its more common use foraggressive MS more than a decadeago, mitoxantrone has fallen consider-ably out of favor because of its dose-dependent cardiotoxicity and moreidiosyncratic tendency to leukemia,but it still remains an option shouldother modalities fail or if other op-tions are unavailable.
Rituximab. Rituximab is a partiallyhumanized monoclonal antibody tar-geting the CD20 antigen on B cellsproducing depletion of circulatingB cells.78 Although somewhat exten-sively used off-label in many parts ofthe world for refractory MS, it has onlybeen tested in small short-term studies,but a similar agent called ocrelizumab79
has completed two large randomizedstudies in relapsing MS. Some of thedata revealed that mostly naıve pa-tients in both studies showed an ex-cellent therapeutic effect of ocrelizumabtreatment on relapse rate reduction,slowing of disease progression, andsuppression of MRI activity comparedto active therapy with subcutaneousinterferon beta-1a 3 times a week over2 years, but there were no data on
subsets of patients that might bedeemed as having aggressive MS. Reg-ulatory bodies will review the studydata to determine whether this will bepositioned as first- or second-line ther-apy.80 Smaller studies with rituximabhave also been encouraging, demon-strating a powerful effect on MRIactivity.81,82 Based in part on a theorythat the presence of B-cell follicles inthe meninges83 contributes to diseaseprogression, rituximab was tested in alarge clinical trial in primary progres-sive MS and failed to slow progressionin the entire study group, although asubgroup of younger patients withenhancing lesions might have bene-fited.84 A similar study with ocrelizumabreported a successful overall delay indisease progression of patients withprimary progressive MS, but it is notknown whether this was all driven byyounger patients with continued evi-dence of inflammation as some 25%of patients had gadolinium-enhancinglesions at baseline.85 In other condi-tions, such as rheumatoid arthritis,periodic rituximab treatment could suc-cessfully control disease with or with-out using concurrent agents.86
Rituximab is discussed here be-cause it has been used anecdotally totreat aggressive MS in many parts of theworld, despite the lack of supportingdata. However, we are not advocatingfor its use, rather just acknowledgingthat some have used it rather than theother agents listed here.87 Without thelevel of evidence that can only be de-rived from properly conducted con-trolled trials, we would not consider itan alternative to the other proposedtreatment choices.
Immunoablation andAutologous HematopoieticStem Cell TransplantationIntensive myeloablative or immuno-ablative conditioning treatment with
KEY POINT
h Despite its morecommon use foraggressive multiplesclerosis more thana decade ago,mitoxantrone hasfallen considerably outof favor because of itsdose-dependentcardiotoxicity and moreidiosyncratic tendencyto leukemia, but it stillremains an optionshould other modalitiesfail or if other optionsare unavailable.
772 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

various regimens of chemotherapy fol-lowed by a rescue imparted by auto-logously derived hematopoietic stemcells has been used successfully forthe past 2 decades to treat severetreatment-refractory autoimmunediseases, including MS. More than800 patients with MS around theworld have been treated with autolo-gous hematopoietic stem cell transplan-tation using various regimens.88 Earlierstudies that selected patients whowere more severely disabled to estab-lish the safety of the procedure notsurprisingly showed little in the wayof efficacy, but a high morbidity andmortality (approximately 5%) was seen,probably owing to the poorer clinicalstate of these patients with advanceddisease. Mortality rates were approxi-mately 5% in the early transplant era.Other trials have focused more onpatients with highly active disease thatwas refractory to conventional disease-modifying therapy, and demonstratedmuch more encouraging safety data(mortality less than 1%).88 The ratio-nale for this severe approach rests inthe ability of this treatment to producea complete immune system reset, ef-fectively eradicating the disease-causingimmune cells using intense immuno-suppression and reestablishing a newimmune system derived from autolo-gous stem cells.89 The newly develop-ing immune system leads to immunetolerance, devoid of disease-causingautoreactive cells. Furthermore, themore definitive ablative regimens pro-duce long-lasting remissions withoutthe need for further treatment withdisease-modifying therapy.
The problem is that several trans-plant conditioning regimens are usedamong different transplantationgroups, and no consensus exists thatone protocol is superior. Although it isuncertain whether the intensity of theconditioning (ablative) protocol influ-
ences the outcome, nonmyeloablativeregimens trade reduced toxicity forreduced efficacy in halting MRI activityor stopping relapses,90 with one ofthe largest studies showing an 80%relapse-free survival over 4 years andsignificant improvement in EDSSscores in a majority of patients withthis regimen.91 The 3-year interimreport of the High-dose Immunosup-pression and Autologous Stem CellTransplantation for Multiple Sclerosis(HALT MS) study in North Americaused a medium-intensity conditioningprotocol and demonstrated that 86.6%of patients were relapse free with aprogression-free survival of 90.9% over3 years.92 The European study useda similar conditioning protocol, ran-domly assigning patients to autologoushematopoietic stem cell transplantationversus mitoxantrone, but recruitmentwas so dismal over the years that theychanged their primary outcome to MRImeasures and curtailed the study early.However, the study did show thesuperiority of autologous hemato-poietic stem cell transplantation versusmitoxantrone in reducing MRI activityand relapses.93 Our own experience,using a much higher myeloablativeconditioning regimen and a CD34+selected graft to treat aggressive MS,showed that 100% of patients followedfor more than 10 years from transplantwere free of relapses or new MRI ac-tivity. Many actually improved, butapproximately 30% progressed despitethe fact that no further inflammatoryactivity was detected.94
Increasing expertise and promisingresults have sparked multinational ef-forts and even a consensus on how tofurther investigate the role of autolo-gous hematopoietic stem cell transplan-tation in aggressive MS and to assesslong-term efficacy and safety.16 Still, thistype of treatment should be reserved
KEY POINTS
h Limited, but promising,evidence exists for useof autologoushematopoietic stemcell transplantation insevere neurologicconditions with immunebasis other than multiplesclerosis (eg, myastheniagravis, chronicinflammatorydemyelinatingpolyneuropathy, stiffperson syndrome,neuromyelitis optica,and autoimmuneencephalitis).
h It is possible tocompletely or almostcompletely remove anentire immune systemand replace it with anew one that may nolonger attack the centralnervous system.
773Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

for centers with established experi-ence in bone marrow transplantation.
Changing the TreatmentParadigm of AggressiveMultiple SclerosisClassically, the paradigmof starting withsafer agents in early phases of disease,then escalating to medications withpresumed greater efficacy but provengreater toxicity only after a subopti-mal response followed by either main-tenance or deescalation after a periodof stability is appropriate for mostpatients with relapsing MS. This con-servative approach prioritizes safetyover possibly greater efficacy and canbe quite effective provided that pa-tients are closely monitored to detectearly suboptimal response and thenpromptly escalated (Case 4-1). Suchan approach is, however, inadequatein patients with aggressive MS, whohave a much narrower treatment win-dow and may lose precious biologicaltime and opportunity to control theirdisease. In this context, it is impor-tant to tailor initial therapies to maxi-mize efficacy, trading off any highertreatment-related risks in exchange forrapid disease control.
An induction approach has beenconsidered and used for many years in
patients deemed to have more aggres-sive forms of MS, especially when firstseen (Case 4-2). This “hit hard andearly” approach involves more potentagents early on in the disease coursebut also has the potential for moreserious side effects.95 It could be usedin a temporary fashion for a limitedperiod of time (mitoxantrone, cladribine,or cyclophosphamide) or as a moredefinitive therapy (alemtuzumab or au-tologous hematopoietic stem cell trans-plantation). The duration of theinduction treatment is often dictatedby specific toxicities, in part becauseof cumulative doses, and the intendedchoice of an “exit strategy” (what todo following induction). Therapeuticresponse needs to bemonitored closelyin both treatment paradigms to cap-ture partial and nonresponders in atimely manner.
“No evidence of disease activity”(NEDA) is a new concept of diseasecontrol that should ultimately be thegoal of all disease-modifying therapy.96
It is also referred to as freedom fromdisease activity and is a composite offreedom from relapses and disabilityworsening as well as lack of MRI ac-tivity (new/enlarging T2 lesions orgadolinium-enhancing lesions). Severalcaveats exist concerning this concept,
KEY POINTS
h Autologoushematopoietic stem celltransplantation shouldbe performed only incenters with extensivehematologic andneurologic experience inthis treatment and themanagement ofpatients after bonemarrow transplantation,as specific issues andcomplications may beseen in multiple sclerosispatients undergoingthis procedure.
h ‘‘No evidence of diseaseactivity’’ (NEDA) is acomposite of absence ofclinical relapses, MRIactivity (new orenlarging T2 orgadolinium-enhancinglesions), anddisability progression.
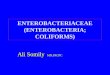
Case 4-1A 26-year-old man was diagnosed with relapsing-remitting multiple sclerosis when he presented3 years ago with diplopia and ataxia. He initially started interferon beta-1a but developed two mildattacks in 12 months (right optic neuritis and left hand numbness), each resolving on its own. Hisfollow-up MRI showed two new T2 lesions, and he was switched to fingolimod. In the past year,he had two additional relapses: a thoracic myelitis (T6 sensory level, mild spasticity, moderate leftankle dorsiflexor weakness, and loss of vibration in the left foot) and a brainstem attack (rightinternuclear ophthalmoplegia, facial myokymia, and vertigo). Both attacks were deemed moderatein severity and impacted his daily functioning; they were treated with steroids. He made a goodrecovery but had residual left leg fatigability and a neurogenic bladder. His Expanded Disability StatusScale (EDSS) score was 2.5. Repeat imaging 10 months after starting fingolimod demonstratedmultiple gadolinium-enhancing lesions both in the brain and cervical spine (Figure 4-1). His diseasewas deemed aggressive, so he was started on alemtuzumab.
Continued on page 775
774 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

but in relapsing MS, many early pa-tients achieve NEDA when given notreatment (ie, in the placebo groupof trials). This would not be the caseat all with aggressive MS, a patientgroup highly likely to demonstratedamaging disease activity in the ab-sence of definitive treatment. There-fore, achieving a result as close as
possible to NEDA would be evenmore relevant in aggressive MS andshould be a realistic goal for this pa-tient group.
Aggressive Multiple SclerosisTreatment AlgorithmTreatment algorithms for aggressiveMS do not currently exist. The authors
Comment. This case highlights the importance of close follow-up of both clinical and MRI statuswhile initiating a first-line treatment. The quick emergence of disease while on first-line treatmentis a telltale sign of active disease warranting treatment escalation. The continued activity with residualdeficits while on an escalated therapy put his disease into the aggressive level.
Continued from page 774
FIGURE 4-1 Follow-up brain and spinal cord MRI of the patient in Case 4-1showing multiple gadolinium-enhancing lesions. A, CoronalT1 postcontrast brain image; B, sagittal T1 postcontrast
cervical spine image; C, D, axial postcontrast T1 brain images atdifferent levels.
775Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Case 4-2A 29-year-old woman presented for a neurologic consultation because of a 5-year history of neurologicsymptoms. Five years previously, she developed right arm and handweakness with Lhermitte phenomenonand was diagnosed by her primary physician with a cervical radiculopathy, which was treated with physicaltherapy and resolved. However, 1 year later, she developed a tight and squeezing sensation in her chestradiating to her back at the bra line along with numbness in her feet and urinary urgency, but this wasattributed to anxiety. For the past year she has noted blurred vision in the right eye when overheatedor tired, as well as severe fatigue. One month prior to her visit, she developed dysarthria, vertigo, andataxia that was accompanied by a spastic paraparesis to the point of needing a cane to ambulate.
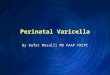
Her examination showed a visual acuity of 20/20 in the left eye and 20/40 in the right eye with aright afferent pupillary defect and a pale right optic disk. Her left corneal reflex was diminished,and she had left facial hypoesthesia in the V1 and V2 dermatomes. She had moderate leg spasticitywith bilateral clonus and diffuse hyperreflexia. Finger extensors, hip flexors, and knee flexors weregraded 4/5 bilaterally in strength, and she had moderate bilateral lower limb dysmetria. She had lossof vibration and graphesthesia in the left hand with severe sensory ataxia in the upper limbs. HerExpanded Disability Status Scale (EDSS) score was 6.0. MRI of the brain and spinal cord revealedevidence for widespread demyelination with lesions both supratentorially and infratentorially as wellas in her spinal cord at C2, C5, T4, and T11 (Figure 4-2).
Because of her delayed diagnosis and accrued disability, IV cladribine was given initially and thepossibility of autologous hematopoietic stem cell transplantation was discussed. She chose to completea 2-year course of IV cladribine, with disease stabilization and no complications and dramaticallyrecovered. Glatiramer acetate was initiated 6 months after finishing the cladribine induction as maintenancetreatment. Four years after the diagnosis of aggressive multiple sclerosis and 2.5 years after completingthe cladribine course, she remained relapse free, and her EDSS score had improved to 3.0.
Comment. This case is an example of recognizing aggressive disease from the beginning and movingto an induction approach for a naıve patient who had accumulated significant disability with anumber of severe early attacks. It was deemed that first- or even second-line agents available at the time(natalizumab or fingolimod) would have most likely been inadequate, with additional concernsregarding the possibility of severe rebound disease should they be discontinued abruptly. Her delayeddiagnosis, rapid accumulation of deficits, and MRI burden all indicated a rapidly advancing severecondition with a narrow therapeutic window of opportunity for treatment. Autologous hematopoieticstem cell transplantation would have also been an option in selected naıve cases in centers withexperience in autologous hematopoietic stem cell transplantation.
FIGURE 4-2 A high T2 lesion burden. A, Sagittal T2 brain MRI showing typical Dawson fingers and corpus callosuminvolvement; B, axial T2 brain MRI revealing multiple infratentorial lesions; C, axial T2 cervical spinal cordMRI with a large lesion involving most of the cord width.
776 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

propose a potential model specificallytailored for this type of patient; how-ever, no optimal strategy exists for thesequencing of these therapies. More-over, not all therapies will be con-sidered, depending on familiarity,availability, experience, and propersupport from colleagues in hematology/oncology who use these agents andtreatments regularly (Figure 4-397).Access, coverage, and regulatory guide-lines for different agents used in thetreatment of MS vary greatly aroundthe world and even regionally within acountry. Interestingly, infrastructure,local resources, expertise, and logis-tics of implementation of such drugscan also be very heterogeneous, man-
dating changes and adaptations toexisting protocols.
Alemtuzumab would be the authors’first choice in patients with aggressiveMS who continue to exhibit disease ac-tivity after at least 1 year of attemptedtreatment and failure with one or moreagents, because of its proven efficacyand manageable safety issues. In thisalgorithm, if alemtuzumab maintainsgood control over the 2 years of itstreatment course, then the authorswould recommend it be used inter-mittently thereafter (yearly treatmentcourse consisting of three doses sim-ilar to the year 2 therapy) should NEDAnot be attainable. Typically, one wouldconsider a course of alemtuzumab to
KEY POINT
h The availability,expertise, and logisticsof implementation fordifferent therapies usedfor multiple sclerosisvary around the world.
FIGURE 4-3 Proposed treatment algorithm for aggressive multiple sclerosis (MS). To meetthe authors’ definition of aggressive MS, patients will either not have respondedto one or more therapies for up to 1 year or present naıve to treatment with
many of the characteristics described in Table 4-1. Some of these patients might warrantinduction therapywith autologous hematopoietic stem cell transplantation (aHSCT), whereas othersare better suited to escalation using alemtuzumab or available immunosuppressive agents(cyclophosphamide, mitoxantrone, or cladribine). If disease activity returns after a period of successwith alemtuzumab or the immunosuppressants, these agents can be used again, assumingthat lifetime cumulative toxicity limits have not been reached (Table 4-2). Maintenance therapy withfirst-line agents (such as interferon beta) might also be beneficial. If MS remains refractory, werecommend moving quickly to aHSCT where possible. Patients should be assessed clinicallyevery 3 months and radiologically every 6 months, permitting only minimal evidence of continueddisease activity before considering further treatment escalation.
Modified with permission from Rush CA, et al, Nat Rev Neurol.97
B 2015 Rights Managed by Nature Publishing Group.www.nature.com/nrneurol/journal/v11/n7/full/nrneurol.2015.85.html.
777Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

be the 2-year treatment (eight doses);however, if alemtuzumab fails to ade-quately control aggressive diseasewithin the first year, then the authorswould suggest moving quickly toautologous hematopoietic stem celltransplantation, where expertise isavailable. It is uncertain if the use ofcladribine, cyclophosphamide, or mi-toxantrone after alemtuzumab failurewould be of additional benefit. In the-ory, they could be valid options in in-stances where autologous hematopoieticstem cell transplantation is not available.
In cases where alemtuzumab is notavailable, any of the immunosuppres-sive agents (cladribine, cyclophospha-mide, or mitoxantrone) would be thefirst logical alternative consideration inthe therapeutic algorithm. Patients mayeither stabilize or continue having sub-optimal response (lack of NEDA), and ifit is deemed to be refractory disease,further courses of immunosuppres-sion could be attempted, keeping inmind the limits for some of theseagents in terms of lifetime cumulativedoses and the risk of toxicity. It is im-portant to keep in mind that the safetyof immunosuppressant use followingmany of the current disease-modifyingtherapies, especially agents such asnatalizumab, has not been established.
Fortunately, stabilization occurs inmany patients after use of the immu-nosuppressant agents and in ap-proximately 70% of patients after onetreatment course of alemtuzumab.However, in most cases, the control isnot indefinite and maintenance treat-ment should be considered. Someevidence exists that patients respondwell to immunomodulating agentssuch as interferon beta or glatirameracetate in this postimmunosup-pression setting and there do not ap-pear to be any additive or sequentialtoxicities. The safety and efficacy ofmaintenance therapy using newer
agents postimmunosuppression isnot established.
For some agents, notably alemtuzumabor cladribine, an alternative optionexists instead of choosing a typicalfirst-line agent for maintenance. If, aftera period of clinical stability, diseaseactivity reappears, either alemtuzumabor cladribine could be used again (a3-day course of alemtuzumab or 4-daycycle of cladribine every 6 months for2 cycles) in a given year. If break-through disease occurs followingcyclophosphamide or mitoxantrone,assuming lifetime cumulative toxicitylimits have not been reached, theseagents could be used again. If limitshave been reached, the logical next stepwould be to proceed to alemtuzumab,cladribine, or even autologous hemato-poietic stem cell transplantation.
Severe disease seems to be unstop-pable in certain patients who continueto have relapses, MRI activity, and un-relenting progression and who ulti-mately fail more potent agents overthe years. For individuals who haveaccrued significant disability andtreatment-related toxicities with noevidence of further relapse or MRI le-sion development over at least 2 years,further immune suppression may notbe warranted.
However, for some young patientsor individuals who are still within theirpersonal “therapeutic window” (ie, evi-dence of active inflammatory disease),autologous hematopoietic stem celltransplantation may be an alternative incenters where autologous hemato-poietic stem cell transplantation exper-tise is available.
In assessing the response to treat-ment for aggressive MS, the authorsrecommend lowering the acceptablethreshold for continued disease activity.Diligent monitoring is critical to cap-ture suboptimal response in a timelymanner and intercede with a more
KEY POINT
h It is important to keepin mind that the safetyof immunosuppressantuse following manyof the currentdisease-modifyingtherapies, especiallyagents such asnatalizumab, has notbeen established.
778 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

effective strategy. Whereas some phy-sicians might be willing to accept min-imal evidence of disease activity, suchas a mild relapse or a couple of newMRI lesions in routine relapsing dis-ease, these would be unacceptable ina case of aggressive MS along with anyindication of EDSS score progression.Any evidence of continued diseaseactivity should be reason enough toworry about the success of the treat-ment chosen for aggressive MS.
Personalizing the Treatment forAggressive Multiple SclerosisIt is important to consider not onlythe factors that might predispose toa better response using the aggres-sive MS strategy the authors propose,but also other patient characteristics,including the desire for pregnancy,comorbidities, previous use of immu-nosuppressants, JC virus seropositivity,geographic parameters, health insur-ance coverage, and personal prefer-ence (of both patient and treatingneurologist), to determine the treat-ment selection. Risk tolerance differssignificantly between patients with MSand their neurologists. Some studieshave shown that patients with MS arewilling to take more risks than theirtreating neurologists; this may be re-lated to their worse perception of theirown disease.98,99 Risk-averse patientsare more likely to choose less effectivedrugs with a safer side effect profile,whereas risk-tolerant patients willaccept higher risks if the benefit ofhigher efficacy is warranted. It is im-portant to have a good discussion withpatients and their families in orderfor all to understand the gravity of thecondition (aggressive MS) and theplanned treatment strategy to betterensure proper follow-up, not only formonitoring the success of the plannedstrategy, but also to mitigate against
some of the potential risks due to thechoice of treatment.
CONCLUSIONEarly identification of patients with ag-gressive MS is critical since they are athigher risk of early progression andtend to have disease that is refractoryto control using conventional disease-modifying therapies. Opportune andtailored implementation of treatmentstrategies specific to this set of patientsmay have a positive impact on diseaseseverity and neurologic disability. Theuse of more aggressive treatment agentswill require ongoing safety surveillanceto mitigate possible known and un-known risks. So much could be gainedfrom an organized clinical trial fortreating aggressive MS, but such a studywould be ethically challenging since aplacebo cannot be used and mostdisease-modifying therapies are un-likely to be of benefit. Perhaps with amore uniform definition of aggressiveMS and the treatment approach theauthors propose here, data can becompiled from small single-centerstudies over time to determine whichtreatment regimen of those suggestedmight offer superior benefit and safety.
REFERENCES1. Trapp BD, Peterson J, Ransohoff RM, et al.
Axonal transection in the lesions ofmultiple sclerosis. N Engl J Med1998;338(5):278Y285. doi:10.1056/NEJM199801293380502.
2. Frischer JM, Bramow S, Dal-Bianco A, et al.The relation between inflammation andneurodegeneration in multiple sclerosisbrains. Brain 2009;132(pt 5):1175Y1189.doi:10.1093/brain/awp070.
3. Confavreux C, Vukusic S, Adeleine P. Earlyclinical predictors and progression ofirreversible disability in multiple sclerosis:an amnesic process. Brain 2003;126(pt 4):770Y782. doi:10.1093/brain/awg081.
4. Ebers GC. Prognostic factors for multiplesclerosis: the importance of natural historystudies. J Neurol 2005;252(suppl 3):iii15Yiii20.doi:10.1007/s00415-005-2012-4.
KEY POINTS
h Risk tolerance and riskaversion differ frompatient to patientand between patientsand treatingneurologists, dictatingthe degree of theaggressive or intensivetreatment plan.
h Early detection andtreatment of aggressivemultiple sclerosis iscrucial to preventirreversible damageand disability.
h Identification ofsuboptimal response isalso paramount toredirect treatment ifbreakthrough disease isongoing despite morepotent agents in viewof the complexity ofthe new agents andunknown long-termsafety profile.
779Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

5. Weinshenker BG, Bass B, Rice GP, et al.The natural history of multiple sclerosis: ageographically based study. 2. Predictivevalue of the early clinical course. Brain1989;112(pt 6):1419Y1428. doi:10.1093/brain/112.6.1419.
6. Trojano M, Pellegrini F, Fuiani A, et al.New natural history of interferon-beta-treatedrelapsing multiple sclerosis. Ann Neurol2007;61(4):300Y306. doi:10.1002/ana.21102.
7. Freedman MS. Multiple sclerosis therapeuticstrategies: use second-line agents asfirst-line agents when time is of the essence.Neurol Clin Pract 2011;1(1):66Y68.doi:10.1212/CPJ.0b013e31823cc2c2.
8. Freedman MS, Selchen D, Arnold DL, et al.Treatment optimization in MS: Canadian MSWorking Group updated recommendations.Can J Neurol Sci 2013;40(3):307Y323.doi:10.1017/S0317167100014244.
9. Karussis D, Biermann LD, Bohlega S, et al.A recommended treatment algorithm inrelapsing multiple sclerosis: report of aninternational consensus meeting. Eur JNeurol 2006;13(1):61Y71. doi:10.1111/j.1468-1331.2006.01147.x.
10. Wingerchuk DM, Carter JL. Multiple sclerosis:current and emerging disease-modifyingtherapies and treatment strategies. MayoClin Proc 2014;89(2):225Y240. doi:10.1016/j.mayocp.2013.11.002.
11. Nunes JC, Radbruch H, Walz R, et al. Themost fulminant course of the Marburgvariant of multiple sclerosis-autopsy findings.Mult Scler 2015;21(4):485Y487. doi:10.1177/1352458514537366.
12. Lublin FD, Reingold SC. Defining the clinicalcourse of multiple sclerosis: results of aninternational survey. National MultipleSclerosis Society (USA) Advisory Committeeon Clinical Trials of New Agents in MultipleSclerosis. Neurology 1996;46(4):907Y911.doi:10.1212/WNL.46.4.907.
13. Lublin FD, Reingold SC, Cohen JA, et al.Defining the clinical course of multiplesclerosis: the 2013 revisions. Neurology2014;83(3):278Y286. doi:10.1212/WNL.0000000000000560.
14. Gholipour T, Healy B, Baruch NF, et al.Demographic and clinical characteristics ofmalignant multiple sclerosis. Neurology2011;76(23):1996Y2001. doi:10.1212/WNL.0b013e31821e559d.
15. Menon S, Shirani A, Zhao Y, et al.Characterising aggressive multiple sclerosis.J Neurol Neurosurg Psychiatry2013;84(11):1192Y1198. doi:10.1136/jnnp-2013-304951.
16. Saccardi R, Freedman MS, Sormani MP, et al.A prospective, randomized, controlled trialof autologous haematopoietic stem celltransplantation for aggressive multiplesclerosis: a position paper. Mult Scler2012;18(6):825Y834. doi:10.1177/1352458512438454.
17. Scott TF, Schramke CJ. Poor recovery afterthe first two attacks of multiple sclerosis isassociated with poor outcome five yearslater. J Neurol Sci 2010;292(1Y2):52Y56.doi:10.1016/j.jns.2010.02.008.
18. Amato MP, Ponziani G, Bartolozzi ML,Siracusa G. A prospective study on thenatural history of multiple sclerosis: clues tothe conduct and interpretation of clinicaltrials. J Neurol Sci 1999;168(2):96Y106.doi:10.1016/S0022-510X(99)00143-4.
19. Bergamaschi R, Berzuini C, Romani A, Cosi V.Predicting secondary progression inrelapsing-remitting multiple sclerosis: aBayesian analysis. J Neurol Sci2001;189(1Y2):13Y21. doi:10.1016/S0022-510X(01)00572-X.
20. Wolfson C, Confavreux C. Improvements to asimple Markov model of the natural historyof multiple sclerosis. I. Short-term prognosis.Neuroepidemiology 1987;6(3):101Y115.
21. Tomassini V, Paolillo A, Russo P, et al.Predictors of long-term clinical response tointerferon beta therapy in relapsing multiplesclerosis. J Neurol 2006;253(3):287Y293.doi:10.1007/s00415-005-0979-5l.
22. Brex PA, Ciccarelli O, O’Riordan JI, et al. Alongitudinal study of abnormalities on MRIand disability from multiple sclerosis. N EnglJ Med 2002;346(3):158Y164. doi:10.1056/NEJMoa011341.
23. Filippi M, Horsfield MA, Morrissey SP, et al.Quantitative brain MRI lesion load predictsthe course of clinically isolated syndromessuggestive of multiple sclerosis. Neurology1994;44(4):635Y641. doi:10.1212/WNL.44.4.635.
24. Rudick RA, Lee JC, Simon J, Fisher E, et al.Significance of T2 lesions in multiple sclerosis:a 13-year longitudinal study. Ann Neurol2006;60(2):236Y242. doi:10.1002/ana.20883.
25. Lukas C, Minneboo A, de Groot V, et al.Early central atrophy rate predicts 5 yearclinical outcome in multiple sclerosis. J NeurolNeurosurg Psychiatry 2010;81(12):1351Y1356.doi:10.1136/jnnp.2009.199968.
26. Popescu V, Agosta F, Hulst HE, et al.Brain atrophy and lesion loadpredict long term disability in multiplesclerosis. J Neurol Neurosurg Psychiatry2013;84(10):1082Y1091. doi:10.1136/jnnp-2012-304094.
780 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

27. Sailer M, O’Riordan JI, Thompson AJ, et al.Quantitative MRI in patients with clinicallyisolated syndromes suggestiveof demyelination.Neurology 1999;52(3):599Y606. doi:10.1212/WNL.52.3.599.
28. Sastre-Garriga J, Tintore M. Multiplesclerosis: lesion location may predictdisability in multiple sclerosis. Nat RevNeurol 2010;6(12):648Y649. doi:10.1038/nrneurol.2010.161.
29. Scalfari A, Neuhaus A, Degenhardt A, et al.The natural history of multiple sclerosis: ageographically based study 10: relapses andlong-term disability. Brain 2010;133(pt 7):1914Y1929. doi:10.1093/brain/awq118.
30. Fisniku LK, Brex PA, Altmann DR, et al.Disability and T2 MRI lesions: a 20-yearfollow-up of patients with relapseonset of multiple sclerosis. Brain 2008;131(pt 3):808Y817. doi:10.1093/brain/awm329.
31. Freedman MS, Comi G, De Stefano N, et al.Moving toward earlier treatment ofmultiple sclerosis: findings from a decadeof clinical trials and implications forclinical practice. Mult Scler Relat Disord2014;3(2):147Y155. doi:10.1016/j.msard.2013.07.001.
32. Hakiki B, Portaccio E, Giannini M, et al.Withdrawal of fingolimod treatment forrelapsing-remitting multiple sclerosis: reportof six cases. Mult Scler 2012;18(11):1636Y1639. doi:10.1177/1352458512454773.
33. Havla JB, Pellkofer HL, Meinl I, et al. Reboundof disease activity after withdrawal offingolimod (FTY720) treatment. Arch Neurol2012;69(2):262Y264. doi:10.1001/archneurol.2011.1057.
34. Killestein J, Vennegoor A, Strijbis EM, et al.Natalizumab drug holiday in multiplesclerosis: poorly tolerated. Ann Neurol2010;68(3):392Y395. doi:10.1002/ana.22074.
35. O’Connor PW, Goodman A, Kappos L, et al.Disease activity return during natalizumabtreatment interruption in patients withmultiple sclerosis. Neurology 2011;76(22):1858Y1865. doi:10.1212/WNL.0b013e31821e7c8a.
36. Cohen JA, Barkhof F, Comi G, et al.Fingolimod versus intramuscular interferon inpatient subgroups from TRANSFORMS. JNeurol 2013;260(8):2023Y2032. doi:10.1007/s00415-013-6932-0.
37. Hutchinson M, Kappos L, Calabresi PA, et al.The efficacy of natalizumab in patientswith relapsing multiple sclerosis: subgroupanalyses of AFFIRM and SENTINEL. J Neurol2009;256(3):405Y415. doi:10.1007/s00415-009-0093-1.
38. Coles AJ. Alemtuzumab therapy for multiplesclerosis. Neurotherapeutics 2013;10(1):29Y33.doi:10.1007/s13311-012-0159-0.
39. Coles AJ, Twyman CL, Arnold DL, et al.Alemtuzumab for patients with relapsingmultiple sclerosis after disease-modifyingtherapy: a randomised controlled phase 3trial. Lancet 2012;380(9856):1829Y1839.doi:10.1016/S0140-6736(12)61768-1.
40. Rice GP, Filippi M, Comi G. Cladribine andprogressiveMS: clinical andMRI outcomes of amulticenter controlled trial. Cladribine MRIStudy Group. Neurology 2000;54(5):1145Y1155. doi:10.1212/WNL.54.5.1145.
41. Sipe JC, Romine JS, Koziol JA, et al.Cladribine in treatment of chronicprogressive multiple sclerosis.Lancet 1994;344(8914):9Y13.doi:10.1016/S0140-6736(94)91046-4.
42. Hartung HP, Gonsette R, Konig N, et al.Mitoxantrone in progressive multiplesclerosis: a placebo-controlled, double-blind,randomised, multicentre trial. Lancet2002;360(9350):2018Y2025. doi:10.1016/S0140-6736(02)12023-X.
43. Edan G, Miller D, Clanet M, et al. Therapeuticeffect of mitoxantrone combined withmethylprednisolone in multiple sclerosis: arandomised multicentre study of activedisease using MRI and clinical criteria. JNeurol Neurosurg Psychiatry1997;62(2):112Y118. doi:10.1136/jnnp.62.2.112.
44. Cocco E, Sardu C, Gallo P, et al. Frequencyand risk factors of mitoxantrone-inducedamenorrhea in multiple sclerosis: theFEMIMS study. Mult Scler 2008;14(9):1225Y1233. doi:10.1177/1352458508094882.
45. Rivera VM, Jeffery DR, Weinstock-Guttman B,et al. Results from the 5-year, phase IVRENEW (Registry to Evaluate NovantroneEffects in Worsening Multiple Sclerosis) study.BMC Neurol 2013;13:80. doi:10.1186/1471-2377-13-80.
46. Marriott JJ, Miyasaki JM, Gronseth G, et al.Evidence report: the efficacy and safetyof mitoxantrone (Novantrone) in thetreatment of multiple sclerosis: report of theTherapeutics and Technology AssessmentSubcommittee of the American Academyof Neurology. Neurology 2010;74(18):1463Y1470. doi:10.1212/WNL.0b013e3181dc1ae0.
47. Perini P, Gallo P. Cyclophosphamide iseffective in stabilizing rapidly deterioratingsecondary progressive multiple sclerosis.J Neurol 2003;250(7):834Y838. doi:10.1007/s00415-003-1089-x.
781Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

48. Awad A, Stuve O. Cyclophosphamide inmultiple sclerosis: scientific rationale, historyand novel treatment paradigms. Ther AdvNeurol Disord 2009;2(6):50Y61. doi:10.1177/1756285609344375.
49. Stillwell TJ, Benson RC Jr. Cyclophosphamide-induced hemorrhagic cystitis. A review of100 patients. Cancer 1988;61(3):451Y457.doi:10.1002/1097-0142(19880201)61:3G451::AID-CNCR282061030893.0.CO;2-G.
50. Hohol MJ, Olek MJ, Orav EJ, et al. Treatmentof progressive multiple sclerosis with pulsecyclophosphamide/methylprednisolone:response to therapy is linked to the durationof progressive disease. Mult Scler1999;5(6):403Y409. doi:10.1177/135245859900500i606.
51. De Ridder D, van Poppel H, Demonty L, et al.Bladder cancer in patients with multiplesclerosis treated with cyclophosphamide.J Urol 1998;159(6):1881Y1884. doi:10.1016/S0022-5347(01)63185-9.
52. Khan OA, Zvartau-Hind M, Caon C, et al.Effect of monthly intravenouscyclophosphamide in rapidly deterioratingmultiple sclerosis patients resistant toconventional therapy. Mult Scler 2001;7(3):185Y188. doi:10.1177/135245850100700309.
53. Patti F, Lo Fermo S. Lights and shadows ofcyclophosphamide in the treatment ofmultiple sclerosis. Autoimmune Dis 2011;2011:961702. doi:10.4061/2011/961702.
54. Gobbini MI, Smith ME, Richert ND, et al.Effect of open label pulse cyclophosphamidetherapy on MRI measures of disease activityin five patients with refractoryrelapsing-remitting multiple sclerosis. JNeuroimmunol 1999;99(1):142Y149.doi:10.1016/S0165-5728(99)00039-9.
55. Chen JT, Collins DL, Atkins HL, et al. Brainatrophy after immunoablation and stemcell transplantation in multiple sclerosis.Neurology 2006;66(12):1935Y1937.doi:10.1212/01.wnl.0000219816.44094.f8.
56. Roccatagliata L, Rocca M, Valsasina P, et al.The long-term effect of AHSCT on MRImeasures ofMS evolution: a five-year follow-upstudy. Mult Scler 2007;13(8):1068Y1070.doi:10.1177/1352458507076982.
57. Freedman MS, Kaplan JM, Markovic-Plese S.Insights into the mechanisms of thetherapeutic efficacy of alemtuzumab inmultiple sclerosis. J Clin Cell Immunol2013;4(4). doi:10.4172/2155-9899.1000152.
58. Coles AJ, Cox A, Le Page E, et al. Thewindow of therapeutic opportunity inmultiple sclerosis: evidence frommonoclonal antibody therapy. J Neurol
2006;253(1):98Y108. doi:10.1007/s00415-005-0934-5.
59. Edan G, Le Page E. Induction therapy forpatients with multiple sclerosis: why? When?How? CNS Drugs 2013;27(6):403Y409.doi:10.1007/s40263-013-0065-y.
60. Cossburn M, Pace AA, Jones J, et al.Autoimmune disease after alemtuzumabtreatment formultiple sclerosis in amulticentercohort. Neurology 2011;77(6):573Y579.doi:10.1212/WNL.0b013e318228bec5.
61. Liliemark J. The clinical pharmacokineticsof cladribine. Clin Pharmacokinet1997;32(2):120Y131.
62. Romine JS, Sipe JC, Koziol JA, et al. Adouble-blind, placebo-controlled, randomizedtrial of cladribine in relapsing-remittingmultiple sclerosis. Proc Assoc Am Physicians1999;111(1):35Y44. doi:10.1046/j.1525-1381.1999.09115.x.
63. Giovannoni G, Comi G, Cook S, et al. Aplacebo-controlled trial of oral cladribine forrelapsing multiple sclerosis. N Engl J Med2010;362(5):416Y426. doi:10.1056/NEJMoa0902533.
64. Leist TP, Comi G, Cree BA, et al. Effect of oralcladribine on time to conversion to clinicallydefinite multiple sclerosis in patients with afirst demyelinating event (ORACLE MS): aphase 3 randomised trial. Lancet Neurol2014;13(3):257Y267. doi:10.1016/S1474-4422(14)70005-5.
65. Weiner HL, Mackin GA, Orav EJ, et al.Intermittent cyclophosphamide pulse therapyin progressive multiple sclerosis: final reportof the Northeast Cooperative MultipleSclerosis Treatment Group. Neurology1993;43(5):910Y918. doi:10.1212/WNL.43.5.910.
66. de Bittencourt PR, Gomes-da-Silva MM.Multiple sclerosis: long-term remission aftera high dose of cyclophosphamide. ActaNeurol Scand 2005;111(3):195Y198.doi:10.1111/j.1600-0404.2005.00340.x.
67. Gladstone DE, Zamkoff KW, Krupp L, et al.High-dose cyclophosphamide for moderate tosevere refractory multiple sclerosis. ArchNeurol 2006;63(10):1388Y1393. doi:10.1001/archneur.63.10.noc60076.
68. Schwartzman RJ, Simpkins N, Alexander GM,et al. High-dose cyclophosphamide in thetreatment of multiple sclerosis. CNS NeurosciTher 2009;15(2):118Y127. doi:10.1111/j.1755-5949.2008.00072.x.
69. Krishnan C, Kaplin AI, Brodsky RA, et al.Reduction of disease activity and disabilitywith high-dose cyclophosphamide inpatients with aggressive multiple sclerosis.Arch Neurol 2008;65(8):1044Y1051.doi:10.1001/archneurol.65.8.noc80042.
782 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

70. Patti F, Amato MP, Filippi M, et al. A doubleblind, placebo-controlled, phase II, add-onstudy of cyclophosphamide (CTX) for 24months in patients affected by multiplesclerosis on a background therapy withinterferon-beta study denomination:CYCLIN. J Neurol Sci 2004;223(1):69Y71.doi:10.1016/j.jns.2004.04.023.
71. Smith DR, Weinstock-Guttman B, Cohen JA,et al. A randomized blinded trial ofcombination therapy with cyclophosphamidein patients-with active multiple sclerosison interferon beta. Mult Scler 2005;11(5):573Y582. doi:10.1191/1352458505ms1210oa.
72. Lebrun C, Debouverie M, Vermersch P, et al.Cancer risk and impact of disease-modifyingtreatments in patients with multiplesclerosis. Mult Scler 2008;14(3):399Y405.doi:10.1177/1352458507083625.
73. Goodin DS, Arnason BG, Coyle PK, et al. Theuse of mitoxantrone (Novantrone) for thetreatment of multiple sclerosis: report of theTherapeutics and Technology AssessmentSubcommittee of the American Academy ofNeurology. Neurology 2003;61(10):1332Y1338.doi:10.1212/01.WNL.0000095425.84407.39.
74. Le Page E, Leray E, Taurin G, et al.Mitoxantrone as induction treatment inaggressive relapsing remitting multiplesclerosis: treatment response factors in a5 year follow-up observational study of100 consecutive patients. J NeurolNeurosurg Psychiatry 2008;79(1):52Y56.doi:10.1136/jnnp.2007.124958.
75. Edan G, Comi G, Le Page E, et al. Mitoxantroneprior to interferon beta-1b in aggressiverelapsing multiple sclerosis: a 3-yearrandomised trial. J Neurol NeurosurgPsychiatry 2011;82(12):1344Y1350.doi:10.1136/jnnp.2010.229724.
76. Ramtahal J, Jacob A, Das K, Boggild M.Sequential maintenance treatment withglatiramer acetate after mitoxantroneis safe and can limit exposure toimmunosuppression in very active, relapsingremitting multiple sclerosis. J Neurol2006;253(9):1160Y1164. doi:10.1007/s00415-006-0178-z.
77. Vollmer T, Panitch H, Bar-Or A, et al.Glatiramer acetate after induction therapywith mitoxantrone in relapsing multiplesclerosis. Mult Scler 2008;14(5):663Y670.doi:10.1177/1352458507085759.
78. Barun B, Bar-Or A. Treatment of multiplesclerosis with anti-CD20 antibodies. ClinImmunol 2012;142(1):31Y37. doi:10.1016/j.clim.2011.04.005.
79. Kappos L, Li D, Calabresi PA, et al. Ocrelizumabin relapsing-remitting multiple sclerosis: aphase 2, randomised, placebo-controlled,multicentre trial. Lancet 2011;378(9805):1779Y1787. doi:10.1016/S0140-6736(11)61649-8.
80. Hauser SL, Comi GC, Hartung HP, et al.Efficacy and safety of ocrelizumab inrelapsing multiple sclerosis: results of theinterferon-beta-1a-controlled, double-blind,phase III OPERA I and II studies [Abstract 190].Mult Scler 2015;21(S11):61.
81. Hauser SL, Waubant E, Arnold DL, et al.B-cell depletion with rituximab inrelapsing-remitting multiple sclerosis.N Engl J Med 2008;358(7):676Y688.doi:10.1056/NEJMoa0706383.
82. Naismith RT, Piccio L, Lyons JA, et al.Rituximab add-on therapy for breakthroughrelapsing multiple sclerosis: a 52-weekphase II trial. Neurology 2010;74(23):1860Y1867.doi:10.1212/WNL.0b013e3181e24373.
83. Howell OW, Reeves CA, Nicholas R, et al.Meningeal inflammation is widespread andlinked to cortical pathology in multiplesclerosis. Brain 2011;134(pt 9):2755Y2771.doi:10.1093/brain/awr182.
84. Hawker K, O’Connor P, Freedman MS, et al.Rituximab in patients with primary progressivemultiple sclerosis: results of a randomizeddouble-blind placebo-controlled multicentertrial. Ann Neurol 2009;66(4):460Y471.doi:10.1002/ana.21867.
85. Montalban X, Hemmer B, Rammohan K,et al. Efficacy and safety of ocrelizumabin primary progressive multiple sclerosis:results of the placebo-controlled,double-blind, phase III ORATORIO study[Abstract 228]. Mult Scler 2015;21(S11):781Y782.
86. Mok CC. Rituximab for the treatment ofrheumatoid arthritis: an update. Drug DesDevel Ther 2013;8:87Y100. doi:10.2147/DDDT.S41645.
87. Derwenskus J, Lublin FD. Future treatmentapproaches to multiple sclerosis. Handb ClinNeurol 2014;122:563Y577. doi:10.1016/B978-0-444-52001-2.00024-8.
88. Mancardi G, Saccardi R. Autologoushaematopoietic stem-cell transplantationin multiple sclerosis. Lancet Neurol2008;7(7):626Y636. doi:10.1016/S1474-4422(08)70138<8.
89. Pfender N, Saccardi R, Martin R. Autologoushematopoietic stem cell transplantationas a treatment option for aggressivemultiple sclerosis. Curr Treat OptionsNeurol 2013;15(3):270Y280. doi:10.1007/s11940-013-0234-9.
783Continuum (Minneap Minn) 2016;22(3):761–784 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

90. Burt RK, Loh Y, Cohen B, et al. Autologousnon-myeloablative haemopoietic stemcell transplantation in relapsing-remittingmultiple sclerosis: a phase I/II study.Lancet Neurol 2009;8(3):244Y253.doi:10.1016/S1474-4422(09)70017-1.
91. Burt RK, BalabanovR, HanX, et al. Associationof nonmyeloablative hematopoietic stem celltransplantation with neurological disabilityin patients with relapsing-remitting multiplesclerosis. JAMA 2015;313(3):275Y284.doi:10.1001/jama.2014.17986.
92. Nash RA, Hutton GJ, Racke MK, et al.High-dose immunosuppressive therapyand autologous hematopoietic celltransplantation for relapsing-remittingmultiple sclerosis (HALT-MS): a 3-yearinterim report. JAMA Neurol2015;72(2):159Y169. doi:10.1001/jamaneurol.2014.3780.
93. Mancardi GL, Sormani MP, Gualandi F, et al.Autologous hematopoietic stem celltransplantation in multiple sclerosis: aphase II trial. Neurology 2015;84(10):981Y988.doi:10.1212/WNL.0000000000001329.
94. Darlington PJ, Touil T, Doucet JS, et al.Diminished Th17 (not Th1) responses
underlie multiple sclerosis disease abrogationafter hematopoietic stem cell transplantation.Ann Neurol 2013;73(3):341Y354. doi:10.1002/ana.23784.
95. Freedman MS. Induction vs. escalation oftherapy for relapsing multiple sclerosis:the evidence. Neurol Sci 2008;29(suppl 2):S250YS252. doi:10.1007/s10072-008-0953-y.
96. Bevan CJ, Cree BA. Disease activityfree status: a new end point for a newera in multiple sclerosis clinical research?JAMA Neurol 2014;71(3):269Y270.doi:10.1001/jamaneurol.2013.5486.
97. RushCA,MacLeanHJ, FreedmanMS. Aggressivemultiple sclerosis: proposed definition andtreatmentalgorithm.Nat RevNeurol 2015;11(7):379Y389. doi:10.1038/nrneurol.2015.85.
98. Heesen C, Kleiter I, Nguyen F, et al. Riskperception in natalizumab-treated multiplesclerosis patients and their neurologists.Mult Scler 2010;16(12):1507Y1512.doi:10.1177/1352458510379819.
99. Johnson FR, Van Houtven G, Ozdemir S, et al.Multiple sclerosis patients’ benefit-riskpreferences: serious adverse event risks versustreatment efficacy. J Neurol 2009;256(4):554Y562. doi:10.1007/s00415-009-0084-2.
784 www.ContinuumJournal.com June 2016
Aggressive Multiple Sclerosis
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.