Embed Size (px)
Citation preview
Br Heartj (Supplement) 1994;71:15-19 1
Setting up a transoesophageal echocardiographyservice
S Saltissi, M A de Belder, P Nihoyannopoulos
Department ofCardiology, RoyalLiverpool UniversityHospital, LiverpoolS SaltissiRegionalCardiothoracicCentre, SouthCleveland Hospital,Middlesbrough,ClevelandM A de BelderDepartment ofCardiology,HammersmithHospital, LondonP NihoyannopoulosCorrespondence to:Dr S Saltissi, Department ofCardiology, Royal LiverpoolUniversity Hospital, PrescotStreet, Liverpool L7 8XP.
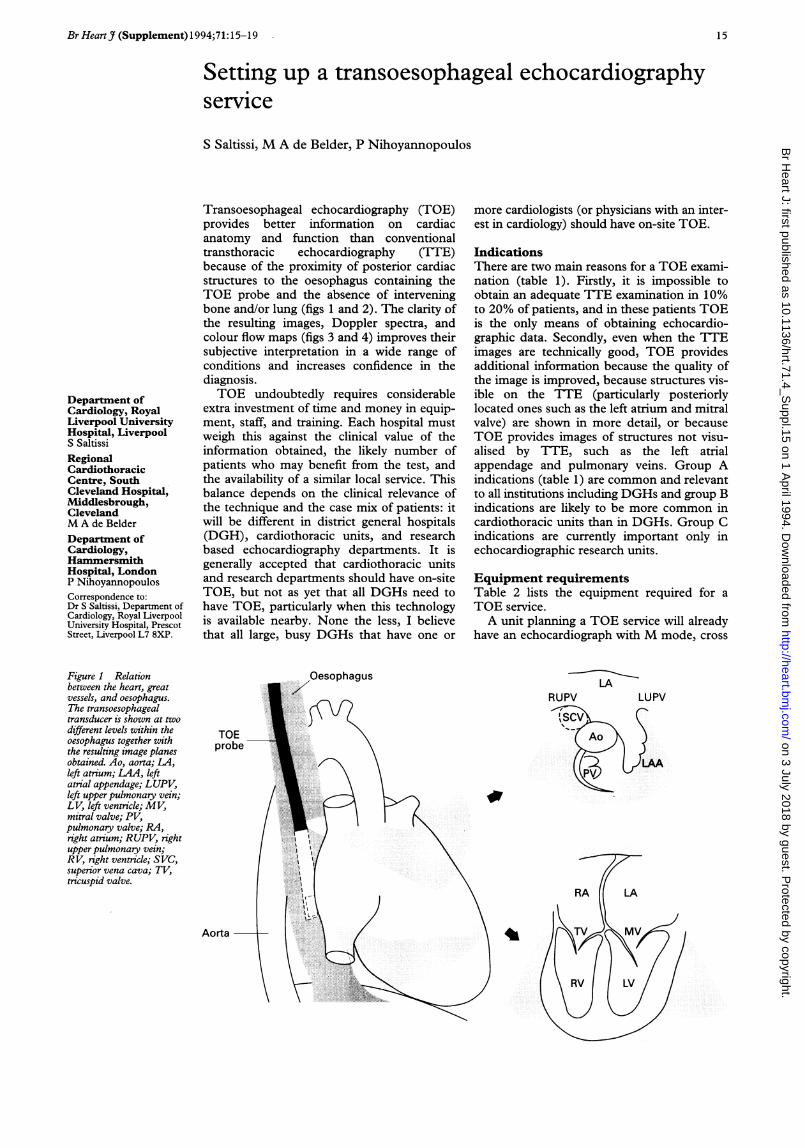
Transoesophageal echocardiography (TOE)provides better information on cardiacanatomy and function than conventionaltransthoracic echocardiography (TTE)because of the proximity of posterior cardiacstructures to the oesophagus containing theTOE probe and the absence of interveningbone and/or lung (figs 1 and 2). The clarity ofthe resulting images, Doppler spectra, andcolour flow maps (figs 3 and 4) improves theirsubjective interpretation in a wide range ofconditions and increases confidence in thediagnosis.TOE undoubtedly requires considerable
extra investment of time and money in equip-ment, staff, and training. Each hospital mustweigh this against the clinical value of theinformation obtained, the likely number ofpatients who may benefit from the test, andthe availability of a similar local service. Thisbalance depends on the clinical relevance ofthe technique and the case mix of patients: itwill be different in district general hospitals(DGH), cardiothoracic units, and researchbased echocardiography departments. It isgenerally accepted that cardiothoracic unitsand research departments should have on-siteTOE, but not as yet that all DGHs need tohave TOE, particularly when this technologyis available nearby. None the less, I believethat all large, busy DGHs that have one or
more cardiologists (or physicians with an inter-est in cardiology) should have on-site TOE.
IndicationsThere are two main reasons for a TOE exami-nation (table 1). Firstly, it is impossible toobtain an adequate TTE examination in 10%to 20% of patients, and in these patients TOEis the only means of obtaining echocardio-graphic data. Secondly, even when the TTEimages are technically good, TOE providesadditional information because the quality ofthe image is improved, because structures vis-ible on the TTE (particularly posteriorlylocated ones such as the left atrium and mitralvalve) are shown in more detail, or becauseTOE provides images of structures not visu-alised by TTE, such as the left atrialappendage and pulmonary veins. Group Aindications (table 1) are common and relevantto all institutions including DGHs and group Bindications are likely to be more common incardiothoracic units than in DGHs. Group Cindications are currently important only inechocardiographic research units.
Equipment requirementsTable 2 lists the equipment required for aTOE service.A unit planning a TOE service will already
have an echocardiograph with M mode, cross
Figure 1 Relationbetween the heart, greatvessels, and oesophagus.The transoesophagealtransducer is shown at twodifferent levels within theoesophagus together withthe resulting image planesobtained. Ao, aorta; LA,left atrium; LAA, leftatrial appendage; LUPV,left upper pulmonary vein;LV, left ventricle; MV,mitral valve; PV,pulmonary valve; RA,right atrium; RUPV, rightupper pulmonary vein;RV, right ventricle; SVC,superior vena cava; TV,tricuspid valve.
7Oesophagus LARUPV LUPV
15
on 3 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.71.4_S
uppl.15 on 1 April 1994. D
ownloaded from

16
Figure 2 Short axis view of mitral valve obtained with a multiplane transducer. Theanatomy of the prolapsing, floppy anterior and posterior mitral valve leaflets is very clearlyseen. ANT, anterior; POST, posterior; MVL, mitral valve leaflet. See legend tofig 1 forother abbreviations.
sectional, and Doppler facilities. Most manu-facturers of modem echocardiographic equip-ment produce or recommend one or morecompatible TOE probes. Until recently onlysingle (transverse) plane imaging probes wereavailable but now biplane probes-that isthose imaging in the longitudinal and trans-verse axes-and multiplane probes areincreasingly becoming available. Such probesallow structure to be seen from different ori-entations and so provide a better spatialappreciation in three dimensions of anyabnormality and of the relation of one struc-ture to another. This is useful in conditionssuch as congenital heart disease and aortic
Figure 3 Transoesophagealfour chamber view showing a large left atrial myxoma. A jetof mitral regurgitation is clearly seen on the colourflow map. MR, mitral regurgitation.See legend to fig 1 for other abbreviations.
Table 1 Indications for TOEInadequatelimpossible 7TE
Adverse patient characteristics-for example, gross obesity ormarked pectus excavatum. Coexisting disorder-for example,chronic obstructive pulmonary disease, chest trauma.Inconvenient patient location-for example, ITU, ventilation,haemodialysis unit.
Additional information requiredGroup A:
Infective endocarditis and its complicationsCardiac site for embolismClarification of intracardiac massesNative valve structure-for example, tears and prolapseThoracic aortic disease-for example, dissection,aneurysm, atheroma
Group B:Prosthetic valve structure and function-for example, leaks, thrombusAdult congenital heart disease-for example, ASDDuring cardiac surgery-for example, MV repair, HOCMDuring non-cardiac surgery, mainly for LV functionOn ITU, mainly for LV function
Group C:Diagnosis of IHD-pacing techniques3D image reconstructionTissue characteristics
ITU, intensive therapy unit; MV, mitral valve; ASD, atrialseptal defect; HOCM, hypertrophic obstructive cardiomyo-pathy; LV, left ventricular; IHD, ischaemic heart disease.
dissection and for the assessment of prostheticvalves.
Because the patient lies in the left lateralposition for up to 45 minutes a comfortablecouch or trolley is needed. Ideally this shouldhave lockable wheels, be of adjustable height,and have an adjustable head section. Morethan one couch/trolley will be needed if sev-eral studies are performed in the same session.TOE is a safe procedure but serious com-
plications can develop (see later). This meansthat equipment to monitor vital signs, includ-ing blood pressure and the electrocardiogramECG and very occasionally pulse oximetry foroxygen saturation, must be available. Fullresuscitation equipment including a "crash"trolley and defibrillator must also be immedi-ately available. Saliva and upper respiratorytract secretions need to be aspirated through asuction apparatus. Patients occasionally needoxygen and this can be supplied through anasal speculum from an oxygen cylindermounted on the trolley.
At the end of the procedure, the probemust be removed, rinsed, and cold sterilised(usually in 2% glutaraldehyde solution) eitherin a dedicated covered tank or in a cold
Table 2 Equipment neededfor TOE
Echo hardware:Cross sectional machine with video and hardcopy facilityTOE probeInstrument trolleyPatient couch/trolley
Safety equipment:Full resuscitation trolley with defibrillatorOxygen sourceDrugs and infusion fluidsSuction apparatusMonitors-for example, BP cuff, ECG machine, oximeter
Cleaning equipment and materials:Glutaraldehyde tank/cold steriliserProtective clothing for disinfection-for example, rubbergloves and goggles
Consumables:Gauze swabsLubricant gelGloves, aprons, patient gownsECG leadsBite guardsCleansing solutionsProtective rubber sheaths for probes (optional)
BP, blood pressure.
Saltissi
on 3 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.71.4_S
uppl.15 on 1 April 1994. D
ownloaded from

Seting up a transoesophageal echocardiography service
Figure 4 Transoesophageal images obtained with a single (transverse) plane transducer.The transthoracic images tn this patient presenting with a transient ischaemic attack wereofgood quality and entirely normal. Top: Four chamber view showing pronouncedspontaneous echo contrast in the left atrium. Bottom: Transverse axis image at the level ofthe left atrium. A large pedunculated thrombus is clearly shown in the left atrialappendage. PV, pulmonary vein; AO, aorta. See legend to fig I for other abbreviations.
steriliser according to manufacturer's direc-tions. The staff should be protected againstskin and eye sensitisation to glutaraldehyde"byrubber gloves, goggles, and gowns. At the endof the session the probe must be storedaccording to manufacturer's recommenda-tions either by hanging from a rack or in an
individual storage case.
LocationTOE equipment requires a large laboratory.The gastroenterology (GI) endoscopy suite orthe echocardiography laboratory are suitable
sites for TOE. The GI endoscopy suite hascleaning and storage facilities, medications,monitoring equipment, nurses trained inendoscopy, and endoscopists to help with diffi-cult intubations. Echocardiographic equip-ment, however, will have to be moved and afull GI programme will lead to an inflexibleschedule. The echocardiography laboratoryis convenient, has readily available echocardio-graphic equipment, and enables easy sched-uling, though additional equipment formonitoring, cleaning, storage, and suctionmay need to be bought. Either location isappropriate but in practice most units preferthe familiarity of the echocardiography labora-tory.
Whichever site is chosen, an adjacent area isneeded for cleaning, disinfecting, and storingthe transducer probe. To fulfil Health andSafety Executive regulations the dimensionsand ventilation of this room need to keep theatmospheric concentration of glutaraldehydebelow set limits during cleaning. Theserequirements must be discussed with the localdesignated health and safety representativewho may monitor concentrations.
Occasional urgent TOE investigations canbe performed almost anywhere includingaccident and emergency departments, inten-sive therapy units, coronary care units, or thecardiac catheter laboratory. These areas, how-ever, are not suitable as a permanent site forTOE facilities.
StaffingA physician, cardiac technician, and a nurse(or further technician) are required for TOE(table 3). The TOE operator will usually be acardiologist or physician with cardiac trainingwho is experienced in probe introduction andmanipulation and familiar with the controls onthe probe and echocardiograph. Before start-ing, however, the operator must ensure thatthe TOE investigation is both indicated andappropriate and that there are no contraindi-cations. Then he or she must fully explain theprocedure to the patient (even if an assistanthas already done so). This is to allay any fearsand to reassure the patient that the test is non-invasive. No drug is as anxiolytic as a calm,confident, informative, and competent opera-tor. Indeed, some units prefer not to sedatepatients because they believe that explanationand instruction are sufficient. Most units inthe United Kingdom, however, (includingmine) almost always give a small dose of seda-tive (usually midazolam) as much for itsamnesic properties as for its sedative effects.The operator must obtain written consent forthe investigation and any possible additionalprocedures (before sedation if used). A func-tioning intravenous line must be in place: Iadvise using a medium sized cannula in aproximal vein-for example, the antecubitalfossa-so that contrast can be injected if nec-essary.
Safe TOE examination requires two morehealth care workers in addition to the opera-tor. A cardiac ultrasound technician is neededto set up the echocardiogram and probe and toalter the gain controls, image depth, and
17 on 3 July 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.71.4_Suppl.15 on 1 A
pril 1994. Dow
nloaded from
Saltissi
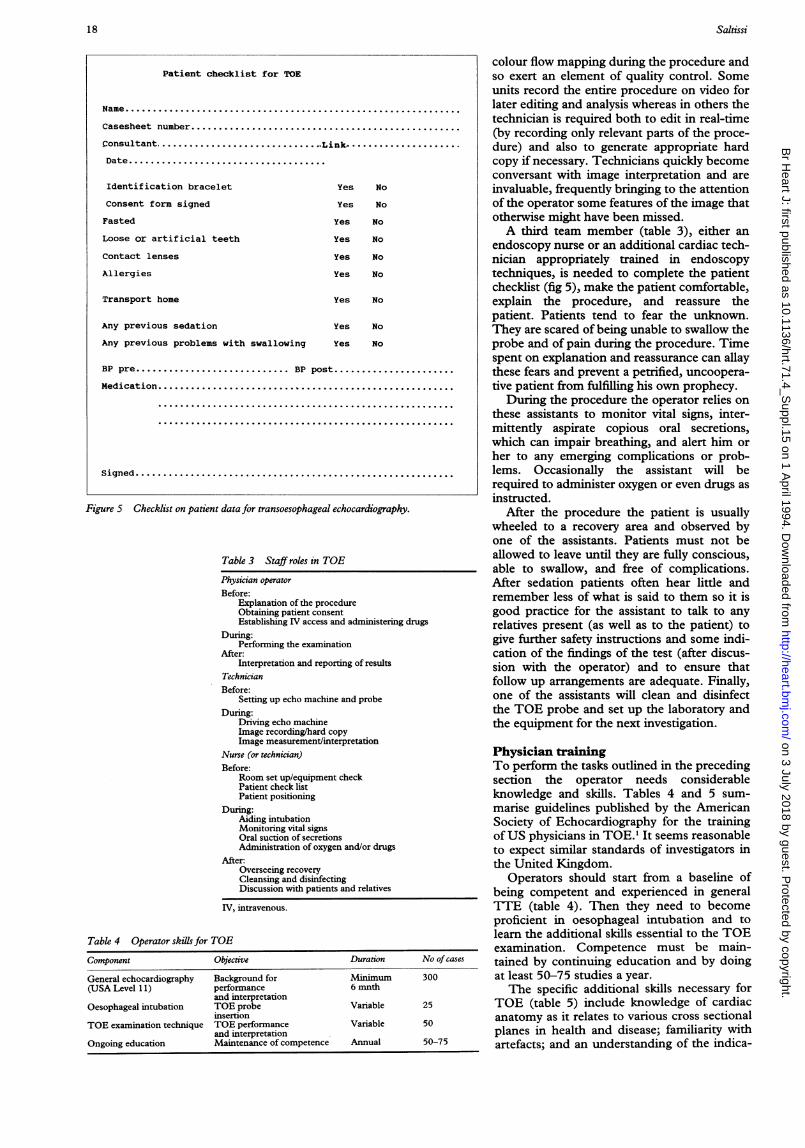
Figure 5 Checklist on patient data for transoesophageal echocardiography.
Table 3 Staff roles in TOE
Physician operator
Before:Explanation of the procedureObtaining patient consentEstablishing IV access and administering drugs
During:Performing the examination
After:Interpretation and reporting of results
TechnicianBefore:
Setting up echo machine and probeDuring:
Driving echo machineImage recording/hard copyImage measurement/interpretation
Nurse (or technician)Before:
Room set up/equipment checkPatient check listPatient positioning
During:Aiding intubationMonitoring vital signsOral suction of secretionsAdministration of oxygen and/or drugs
After:Overseeing recoveryCleansing and disinfectingDiscussion with patients and relatives
IV, intravenous.
Table 4 Operator skills for TOE
Component Objective Duration No of cases
General echocardiography Background for Minimum 300(USA Level 11) performance 6 mnth
and interpretationOesophageal intubation TOE probe Variable 25
insertionTOE examination technique TOE performance Variable 50
and interpretationOngoing education Maintenance of competence Annual 50-75
colour flow mapping during the procedure andso exert an element of quality control. Someunits record the entire procedure on video forlater editing and analysis whereas in others thetechnician is required both to edit in real-time(by recording only relevant parts of the proce-dure) and also to generate appropriate hardcopy if necessary. Technicians quickly becomeconversant with image interpretation and areinvaluable, frequently bringing to the attentionof the operator some features of the image thatotherwise might have been missed.A third team member (table 3), either an
endoscopy nurse or an additional cardiac tech-nician appropriately trained in endoscopytechniques, is needed to complete the patientchecklist (fig 5), make the patient comfortable,explain the procedure, and reassure thepatient. Patients tend to fear the unknown.They are scared of being unable to swallow theprobe and of pain during the procedure. Timespent on explanation and reassurance can allaythese fears and prevent a petrified, uncoopera-tive patient from fulfilling his own prophecy.
During the procedure the operator relies onthese assistants to monitor vital signs, inter-mittently aspirate copious oral secretions,which can impair breathing, and alert him orher to any emerging complications or prob-lems. Occasionally the assistant will berequired to administer oxygen or even drugs asinstructed.
After the procedure the patient is usuallywheeled to a recovery area and observed byone of the assistants. Patients must not beallowed to leave until they are fully conscious,able to swallow, and free of complications.After sedation patients often hear little andremember less of what is said to them so it isgood practice for the assistant to talk to anyrelatives present (as well as to the patient) togive further safety instructions and some indi-cation of the findings of the test (after discus-sion with the operator) and to ensure thatfollow up arrangements are adequate. Finally,one of the assistants will clean and disinfectthe TOE probe and set up the laboratory andthe equipment for the next investigation.
Physician trainingTo perform the tasks outlined in the precedingsection the operator needs considerableknowledge and skills. Tables 4 and 5 sum-marise guidelines published by the AmericanSociety of Echocardiography for the trainingof US physicians in TOE.' It seems reasonableto expect similar standards of investigators inthe United Kingdom.
Operators should start from a baseline ofbeing competent and experienced in generalTTE (table 4). Then they need to becomeproficient in oesophageal intubation and tolearn the additional skills essential to the TOEexamination. Competence must be main-tained by continuing education and by doingat least 50-75 studies a year.The specific additional skills necessary for
TOE (table 5) include knowledge of cardiacanatomy as it relates to various cross sectionalplanes in health and disease; familiarity withartefacts; and an understanding of the indica-
Patient checklist for TOE
Name.............................................................
Casesheet number.................................................
Consultant.......... Link.
Date....................................
Identification bracelet Yes No
Consent form signed Yes No
Fasted Yes No
Loose or artificial teeth Yes No
Contact lenses Yes No
Allergies Yes No
Transport home Yes No
Any previous sedation Yes No
Any previous problems with swallowing Yes No
BP pre......... BP post.
Medication...........
igne................................---*--... ss-........---.....-.*-.-... . . . . . . . . . . . . . . .
Signed..........................................................
18 on 3 July 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.71.4_Suppl.15 on 1 A
pril 1994. Dow
nloaded from

Setting up a transoesophageal echocardiography service
Table 5 Acquisition of operator skills for TOE
Skill Source
Cognitive:Indications/contraindications TextbooksRisks Journals/reviewsCross sectional anatomy VideosInterpretations of images Observations
PM roomPractical:
Probe introduction GI labProbe manipulation ObservationOptimisation of controls Direct supervision
Training coursesPractice
GI, gastrointestinal; PM, postmortem.
tions, contraindications, and risks of the pro-cedure. Practical skills, in addition to probeintroduction, include positioning and manipu-lation of the probe to obtain all the requiredviews and information and competence ininterpreting the results of studies.To date it has been fairly difficult to get
much formal TOE training in the UnitedKingdom but this is increasingly available(table 5) as the number of trained operatorsincreases, formal training courses emerge, andthe literature (including text books, reviews,journals, and videos) on the subject expands.Use of all these resources will speed acquisi-tion of skill.
Safety, risks, and complicationsTOE is safe when it is performed carefully bytrained staff. Nonetheless, complications canand do occur (table 6) and it is important notonly to know what they may be but also toknow how to avoid them.
In a recent large multicentre study of experi-ence in 15 European centres with 10 419 TOEexaminations insertion of the probe was unsuc-cessful in 1-9% and the procedure was inter-rupted despite successful insertion in 0-88%(usually because the patient could not toleratethe probe or because cardiopulmonary orbleeding complications developed).2 There wasone death (from gastrointestinal bleeding)(mortality 0 0098%). In addition, a diabeticwoman has died of cardiorespiratory arrest5-10 minutes after the procedure.3 As might beexpected, mortality and morbidity are slightlyhigher than for routine diagnostic endoscopy ofthe upper gastrointestinal tract (0 004% and0-13% respectively4).
In addition to mechanical injury TOE cancause pressure damage at the site of contact orthermal injury by local heat generation.
Table 6 Complications of TOE
Gastrointestinal:Sore throat (common)Salivary gland swelling (rare)Dysphagia (rare)Haematemesis (rare)Oesophageal mucosal tear (Mallory-Weiss) (rare)Oesophageal perforation (potential)
Respiratory:Oedema of uvula (occasional)Transient unilateral paralysis of vocal cord (rare)Laryngospasm (rare)Hypoxia (occasional)Aspiration pneumonia (rare)Drug-induced respiratory depression (occasional)
Cardiac:Unsustained arrhythmia (occasional)Sustained arrhythmia (rare)Infective endocarditis (potential)
General:Transient bacteraemia (common)Buckling of probe tip (rare)Unsuccessful intubation (rare)
However, in practice these complications arerare. Table 6 lists most known complications;some are worth mentioning here. The mostfeared (but as yet unreported) complication ofTOE is perforation of the oesophagus at itsjunction with the hypopharynx or at its lowerend and particularly where there is anoesophageal tumour. When there is a history ofdysphagia TOE should not be performed untilthe patient has been investigated fully.Insertion of the probe should never be forcedand should always be synchronised with swal-lowing.
Bacteraemia occurs after 7-16% of TOEintubations"6 and 4-13% of diagnostic endo-scopy examinations of the gastrointestinaltract.7 The organisms involved are the pre-dictable ones-Staphylococcus aureus, Staphylo-coccus epidermidis, and alpha haemolyticstreptococci. However, there has been only onereport of a case of streptococcal endocarditistemporally related to TOE8 and none causallyor directly linked to TOE. Therefore the rou-tine use of antimicrobial prophylaxis beforeTOE is not advised currently even in high riskpatients.
Significant sustained arrhythmias are rareand transient; and minor ones occur in lessthan 1% of cases. Changes in heart rate andblood pressure are generally small and well tol-erated. There is little evidence of myocardialischaemia during or after the procedure.
ConclusionTOE is a relatively non-invasive investigationthat can produce high quality images of greatdiagnostic value. It is valuable in a wide range ofindications and is an appropriate service inmost medical institutions including DGHs,where it will improve the diagnosis of condi-tions such as aortic dissection that are difficultto diagnose by other means and aid decisionmaking regarding the need for specialist refer-ral to a cardiac centre. The successful develop-ment of such a service requires considerationof several factors including equipment needs,location, staffing, training, policies and proce-dures, and education of patients. With appro-priate planning and attention to detail alaboratory can be set up and a high quality pro-gramme developed surprisingly quickly andefficiently.
1 Pearlman AS, Gardin JM, Martin RP, Parisi AF, Popp RL,Quinones MA, Stevenson JG, Schiller NB, Seward JB,Stewart WJ. Guidelines for physician training in trans-oesophageal echocardiography: Recommendations of theAmerican Society of Echocardiography Committee forPhysician Training in Echocardiography. Jf Am SocEchocardiogr 1992;5:187-94.
2 Daniel WG, Erbel R, Casper W, et al. Safety of trans-oesophageal echocardiography. A multicentre survey of10,419 examinations. Circulation 1991;83:817-21.
3 Ansari A. Transesophageal two dimensional echocardiogra-phy: Current perspectives. Prog Cardiovasc Dis 1993;35:349-97.
4 Silvis SE, Nebel 0, Rogers G, et al. Endoscopic complica-tions. Results of the 1974 American Society forGastrointestinal endoscopy survey. JAMA 1976;235:928-30.
5 Gorge G, Erbel R, Heinrichs KJ, et al. Positive blood cul-tures during transoesophageal echocardiography. AmJ Cardiol 1990;65: 1404-5.
6 Dennig K, Sedlmayr V, Selling B, et al. Bacteraemia withtransoesophageal echocardiography. Circulation 1989;80(suppl 2):473.
7 Botoman VA, Surawicz CM. Bacteraemia with gastroin-testinal endoscopic procedure. Gastrointest Endosc 1986;32:342-6.
8 Foster E, Kusumoto FM, Sobols M, et al. Streptococcalendocarditis temporally related to transesophagealechocardiography. JYAm Soc Echocardiogr 1990;3:424-7.
19 on 3 July 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.71.4_Suppl.15 on 1 A
pril 1994. Dow
nloaded from





























