Embed Size (px)
Citation preview
Cardiovascular Boot Camp April 2009
www.cardionursing.com 1
CNEACNEA 20092009 11
Pulmonary Pulmonary
Pathophysiology:Pathophysiology:
Presented by: Presented by:
Karen Marzlin BSN, RN, CCRN, CMC Karen Marzlin BSN, RN, CCRN, CMC
22
Cardiovascular Boot Camp April 2009
www.cardionursing.com 2
33
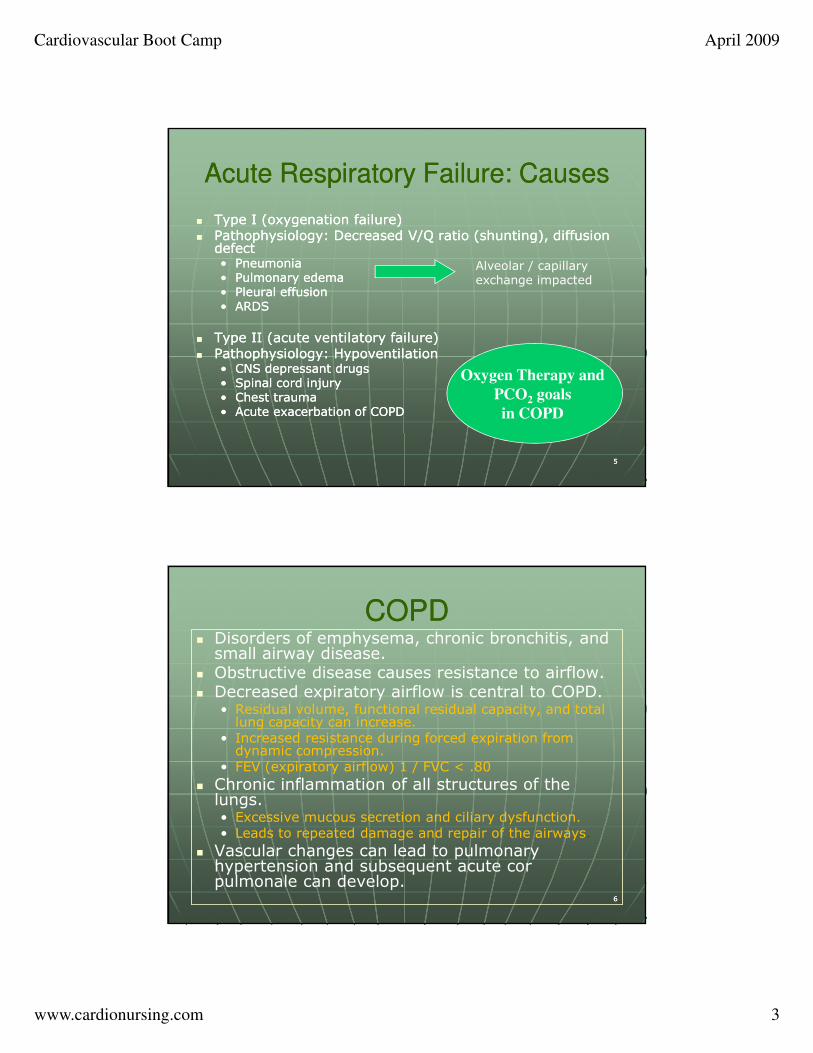
Acute Respiratory Failure Acute Respiratory Failure
Failure of the respiratory system to Failure of the respiratory system to provide for the exchange of oxygen provide for the exchange of oxygen and carbon dioxide between the and carbon dioxide between the environment and tissues in quantities environment and tissues in quantities sufficient to sustain life sufficient to sustain life
44
Acute Respiratory Failure Acute Respiratory Failure
�� Type I: Hypoxemic NormocapnicType I: Hypoxemic Normocapnic•• Low PaO2 Low PaO2
•• Normal PaCO2 Normal PaCO2
•• Widened AWidened A--a gradient a gradient
�� Type II: Hypoxemic Hypercapnic Type II: Hypoxemic Hypercapnic •• Low PaO2 Low PaO2
•• High PaCO2 High PaCO2
•• Normal ANormal A--a gradient a gradient
Ventilatory Failure
Oxygenation Failure
Cardiovascular Boot Camp April 2009
www.cardionursing.com 3
55
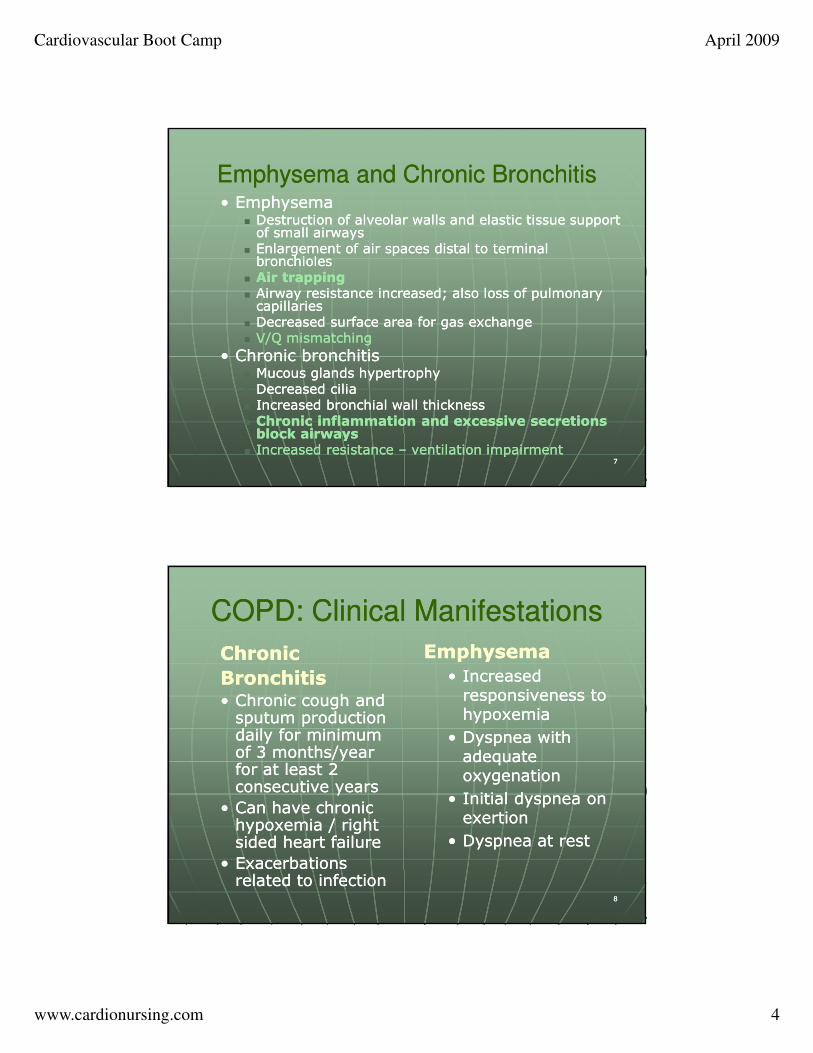
Acute Respiratory Failure: Causes Acute Respiratory Failure: Causes
�� Type I (oxygenation failure) Type I (oxygenation failure) �� Pathophysiology: Decreased V/Q ratio (shunting), diffusion Pathophysiology: Decreased V/Q ratio (shunting), diffusion
defect defect •• Pneumonia Pneumonia •• Pulmonary edema Pulmonary edema •• Pleural effusion Pleural effusion •• ARDS ARDS
�� Type II (acute ventilatory failure) Type II (acute ventilatory failure) �� Pathophysiology: Hypoventilation Pathophysiology: Hypoventilation
•• CNS depressant drugs CNS depressant drugs •• Spinal cord injury Spinal cord injury •• Chest trauma Chest trauma •• Acute exacerbation of COPDAcute exacerbation of COPD
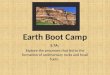
Oxygen Therapy and
PCO2 goals
in COPD
Alveolar / capillary exchange impacted
66
COPD COPD � Disorders of emphysema, chronic bronchitis, and small airway disease.
� Obstructive disease causes resistance to airflow. � Decreased expiratory airflow is central to COPD.
• Residual volume, functional residual capacity, and total lung capacity can increase.
• Increased resistance during forced expiration from dynamic compression.
• FEV (expiratory airflow) 1 / FVC < .80
� Chronic inflammation of all structures of the lungs. • Excessive mucous secretion and ciliary dysfunction.• Leads to repeated damage and repair of the airways.
� Vascular changes can lead to pulmonary hypertension and subsequent acute corpulmonale can develop.
Cardiovascular Boot Camp April 2009
www.cardionursing.com 4
77
Emphysema and Chronic BronchitisEmphysema and Chronic Bronchitis•• Emphysema Emphysema
�� Destruction of alveolar walls and elastic tissue support Destruction of alveolar walls and elastic tissue support of small airways of small airways
�� Enlargement of air spaces distal to terminal Enlargement of air spaces distal to terminal bronchioles bronchioles
�� Air trappingAir trapping�� Airway resistance increased; also loss of pulmonary Airway resistance increased; also loss of pulmonary capillaries capillaries
�� Decreased surface area for gas exchange Decreased surface area for gas exchange �� V/Q mismatchingV/Q mismatching
•• Chronic bronchitis Chronic bronchitis �� Mucous glands hypertrophy Mucous glands hypertrophy �� Decreased cilia Decreased cilia �� Increased bronchial wall thickness Increased bronchial wall thickness �� Chronic inflammation and excessive secretions Chronic inflammation and excessive secretions block airways block airways
�� Increased resistance Increased resistance –– ventilation impairmentventilation impairment
88
COPD: Clinical Manifestations COPD: Clinical Manifestations
ChronicChronic
BronchitisBronchitis•• Chronic cough and Chronic cough and sputum production sputum production daily for minimum daily for minimum of 3 months/year of 3 months/year for at least 2 for at least 2 consecutive years consecutive years
•• Can have chronic Can have chronic hypoxemia / right hypoxemia / right sided heart failure sided heart failure
•• Exacerbations Exacerbations related to infection related to infection
Emphysema Emphysema
•• Increased Increased responsiveness to responsiveness to hypoxemia hypoxemia
•• Dyspnea with Dyspnea with adequate adequate oxygenation oxygenation
•• Initial dyspnea on Initial dyspnea on exertion exertion
•• Dyspnea at rest Dyspnea at rest
Cardiovascular Boot Camp April 2009
www.cardionursing.com 5
99
COPD: Clinical Manifestations COPD: Clinical Manifestations
�� Blended symptoms Blended symptoms
�� Large lung volumes / diminished Large lung volumes / diminished breath sounds breath sounds
�� Ventilation / perfusion mismatchingVentilation / perfusion mismatching
�� High PaCOHigh PaCO22 / low PaO/ low PaO22
�� Increase erythropoietin for increased Increase erythropoietin for increased RBCs RBCs
�� Right sided heart failure Right sided heart failure
1010
COPD: Treatment COPD: Treatment � Smoking cessation
� Bronchodilators• Anticholinergics are the first-line medication in maintenance therapy.
� ipratropium (Atrovent).
• Beta-agonists can be added � Short acting
• racemic albuterol (Ventolin, Proventil, Accuneb).
• levalbuterol (Xopenex).
• metaproterenol (Alupent).
• pirbuterol (Exirel, Maxair).
� Long acting• salmeterol (Serevent).
• formoterol (Foradil, Oxeze).
• Theophylline is a long acting weak bronchodilator.
Cardiovascular Boot Camp April 2009
www.cardionursing.com 6
1111
COPD: Treatment COPD: Treatment � Antibiotics - acute exacerbations can be caused by bacterial infections.
� Corticosteroids: Remains controversial, but they are frequently used in treating exacerbations. Steroids are used as part of chronic treatment in some patients. Corticosteroids can also be combined with other medications.
• budesonide (Pulmicort)
• fluticasone and salmeterol (Advair)
� Expectorants/mucolytics.
1212
COPD: Treatment COPD: Treatment
� Oxygen (Can improve survival in patients who
are hypoxemic)
• Criteria
� Room air: PaO2 < 55 mm Hg with saturation < 85%. PaO2 56-59 and saturation 86-89%, with a qualifying secondary diagnosis.
� Goal of oxygen therapy is to obtain PaO2 of 65-80 mm Hg while awake and at rest.
• Typically delivered at 1-4 L/min, with an increase of 1 L during sleep and exercise.
• Should be given continuously at least 19 hours of each day.
� Pneumonia and influenza vaccines
Cardiovascular Boot Camp April 2009
www.cardionursing.com 7
1313
Case Example Case Example
�� Patient history: COPD (COPatient history: COPD (CO22) retainer ) retainer
�� Initial presentation: Tachypneic with Initial presentation: Tachypneic with SaOSaO22 of 78%of 78%
�� Cause of exacerbation ?Cause of exacerbation ?
�� Initial interventions? Initial interventions?
1414
Case Example Case Example
�� ABG ABG
•• 7.29 7.29
•• PaCO2 60 PaCO2 60
•• HCO3 30 HCO3 30
•• PaO2 48 PaO2 48
�� Treatment options? Treatment options?
�� Goals for ABG values?Goals for ABG values?
Cardiovascular Boot Camp April 2009
www.cardionursing.com 8
1515
Status Asthmaticus Status Asthmaticus
Exacerbation of acute asthma Exacerbation of acute asthma characterized by severe airflow characterized by severe airflow obstruction that is not relieved obstruction that is not relieved after 24 after 24 hours of maximal doses of traditional hours of maximal doses of traditional therapy therapy
Characterized by expiratory wheezingCharacterized by expiratory wheezing
1616
Status Asthmaticus: Etiology Status Asthmaticus: Etiology
�� Extrinsic (specific Extrinsic (specific allergy can be related allergy can be related to attack) to attack)
•• Pollen Pollen
•• Dust Dust
•• Pets Pets
•• Smoke Smoke
•• Food Food
•• Drugs Drugs
�� Intrinsic (attack is Intrinsic (attack is seemingly unrelated seemingly unrelated to an allergen) to an allergen)
•• InfectionInfection
•• Stress Stress
•• Exercise Exercise
•• AspirationAspiration
Cardiovascular Boot Camp April 2009
www.cardionursing.com 9
1717
Status Asthmaticus: Status Asthmaticus: Pathophysiology Pathophysiology
�� Trigger (extrinsic or intrinsic) Trigger (extrinsic or intrinsic)
�� Intrinsic trigger causes imbalance of sympathetic Intrinsic trigger causes imbalance of sympathetic and parasympathetic nervous systems and parasympathetic nervous systems
�� Extrinsic: IgE released Extrinsic: IgE released ►►histamine and slowhistamine and slow--reacting substance of anaphylaxis (SRSreacting substance of anaphylaxis (SRS--A) A)
�� Histamine Histamine ►►swelling and inflammation of smooth swelling and inflammation of smooth muscle of large bronchi (and mucous membrane muscle of large bronchi (and mucous membrane swelling) swelling)
�� Swelling of smooth muscle of small bronchi and Swelling of smooth muscle of small bronchi and release of prostaglandins (enhance histamine) release of prostaglandins (enhance histamine)
1818
Status Asthmaticus: Status Asthmaticus: Pathophysiology Pathophysiology
�� Histamine causes excessive secretion of Histamine causes excessive secretion of mucous mucous ►►narrows the airway lumen narrows the airway lumen
�� TachypneaTachypnea increases insensible water loss increases insensible water loss ►►thicker secretionsthicker secretions
�� Mucous in small airwaysMucous in small airways
�� Increased work of breathing Increased work of breathing (impaired (impaired ventilation)ventilation) (Note: (Note: ▲▲PaCO2 is late PaCO2 is late sign) sign)
Cardiovascular Boot Camp April 2009
www.cardionursing.com 10
1919
Status Asthmaticus: Treatment Status Asthmaticus: Treatment
�� Eliminate or treat cause Eliminate or treat cause
�� Steroids Steroids
�� Need to ventilate when PaCONeed to ventilate when PaCO22
becomes elevated becomes elevated
�� Additional similar treatment as Additional similar treatment as pneumonia pneumonia
2020
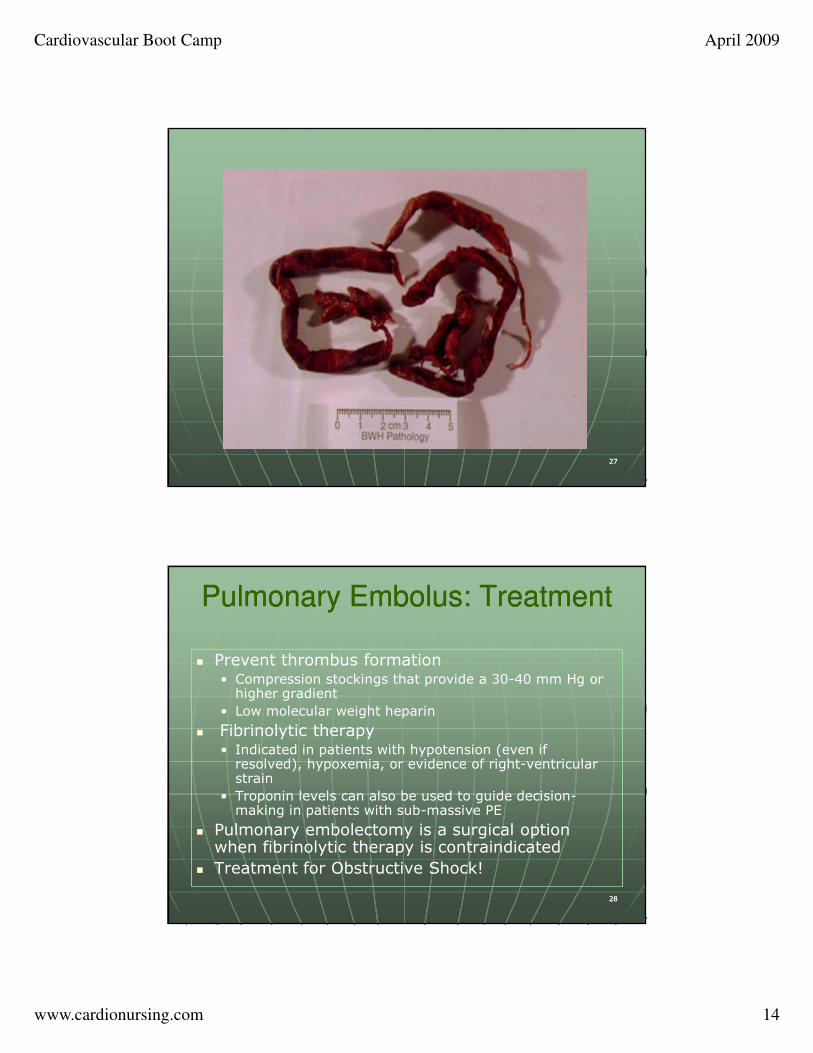
Pulmonary Embolism Pulmonary Embolism
�� Obstruction of blood flow to one or Obstruction of blood flow to one or more arteries of the lung by a more arteries of the lung by a thrombus (other emboli thrombus (other emboli –– fat, air, fat, air, amniotic fluid) lodged in a pulmonary amniotic fluid) lodged in a pulmonary vesselvessel
�� Lower lobes frequently affected due Lower lobes frequently affected due to increased perfusion to increased perfusion
Cardiovascular Boot Camp April 2009
www.cardionursing.com 11
2121
Risk Factors for PE Risk Factors for PE �� Stasis of blood
• Prolonged immobilization after surgical procedures• Plaster casts• Venous obstruction• Heart failure / Shock / Hypovolemia• Varicose veins• Obesity
�� Hypercoagulability• Polycythemia vera• Sickle cell disease• Malignancy• Pregnancy• Recent trauma• Oral contraceptives
� Injury to the vascular endothelium• Central venous and arterial catheters• Phlebitis
2222
Pulmonary Embolism: Pulmonary Embolism: Pathophysiology Pathophysiology
�� > 90% of thrombus develop in deep veins of
iliofemoral system• Can also originate in the right side of the heart, pelvic veins, and axillary or subclavian veins.
• Another source is around indwelling catheters.
� Thrombus formation leads to platelet adhesiveness and release of serotonin (vasoconstrictor).
� Dislodgement of thrombus• Intravascular pressure changes (standing, massaging legs, fluid challenge, valsalva maneuver).
• Natural clot dissolution (7-10 days after development).
Cardiovascular Boot Camp April 2009
www.cardionursing.com 12
2323
Pulmonary Embolism: Pulmonary Embolism: PathophysiologyPathophysiology
� Clot lodges in pulmonary vessels� Ventilation continues but perfusion decreases
• Increase in alveolar dead space• Alveolar CO2 decreases (alveolar shrinking). Allows for more inspired air into the perfused alveoli.
� Overperfusion of uninvolved lung results in a decreased V/Q ratio
� Decreased blood flow damages type II pneumocytes, which results in a decrease in surfactant production. (atelectasis)
� Pulmonary edema can develop as secondary complication � Hypoxemia can occur due to ventilation perfusion
mismatching.� Increased PVR can lead to pulmonary hypertension and
potential acute cor pulmonale.� Cardiogenic shock can occur as the result of right-ventricular
failure.
2424
Pulmonary Embolus: Pulmonary Embolus: Clinical Presentation Clinical Presentation
� Large to massive when 50% of pulmonary artery bed is occluded
• Impending doom
• Hypoxemia
• Syncope
• Sign and symptoms of right heart strain or right-ventricular failure
• Signs of right-ventricular strain on ECG.
• Sudden shock
• Pulseless electrical activity
�� Medium-sized emboli
• Dyspnea
• Substernal chest discomfort/pleuritic chest pain
• Many non-specific signs
• Tachypnea
• Tachycarida
• Rales
• Accentuated 2nd heart sound

Cardiovascular Boot Camp April 2009
www.cardionursing.com 13
2525
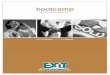
Pulmonary Infarction Pulmonary Infarction
� Pulmonary infarction is infrequent
� More common• Large embolus
• Pre-existing lung disease
� Results in alveoli filling with RBCs and inflammatory cells
� Complicated by infection • Abscess
�� Signs and Symptoms Signs and Symptoms • Pleuritic chest pain
• Dyspnea
• Hemoptysis
• Cough
• Pleural friction rub
2626
Cardiovascular Boot Camp April 2009
www.cardionursing.com 14
2727
2828
Pulmonary Embolus: Treatment Pulmonary Embolus: Treatment
� Prevent thrombus formation • Compression stockings that provide a 30-40 mm Hg or higher gradient
• Low molecular weight heparin
� Fibrinolytic therapy• Indicated in patients with hypotension (even if resolved), hypoxemia, or evidence of right-ventricular strain
• Troponin levels can also be used to guide decision-making in patients with sub-massive PE
� Pulmonary embolectomy is a surgical option when fibrinolytic therapy is contraindicated
� Treatment for Obstructive Shock!
Cardiovascular Boot Camp April 2009
www.cardionursing.com 15
2929
Pulmonary Embolus: TreatmentPulmonary Embolus: Treatment� Heparin is the treatment of choice for reducing mortality in
PE• Initiated prior to a confirmed diagnosis• Slows or prevents clot progression and decreases risk of further emboli
� Oxygen is indicated, even in the absence of hypoxemia � Pulmonary vasodilators to help reduce pulmonary vascular
resistance� Treat right-ventricular failure with fluids and inotropes� Warfarin
• 3 to 6 months if there is identifiable reversible risk factor• Minimum of 6 six months if there is no identifiable risk factor• Long term with recurrent PE or in patients with ongoing risk factors
� Surgical interruption of inferior vena cava with a filter• Patients with contraindication to anticoagulants.• Recurrent thromboembolism despite anticoagulant.• Survivor of massive PE
3030
Special Considerations Fat Emboli Special Considerations Fat Emboli
�� Risk Factors:Risk Factors:
•• Skeletal Trauma: femur and Skeletal Trauma: femur and pelvis)pelvis)
•• Major orthopedic surgery Major orthopedic surgery
•• 24 to 72 hours post insult24 to 72 hours post insult
�� Signs and Symptoms: Signs and Symptoms:
•• Vague chest pain Vague chest pain
•• Shortness of breath Shortness of breath
•• Sudden restlessness Sudden restlessness ––drowsiness drowsiness
•• Fever Fever
•• Petechiae (transient Petechiae (transient ––axillary or subconjunctival) axillary or subconjunctival)
�� Release of free Release of free fatty acids causes fatty acids causes endothelial injury endothelial injury and toxic and toxic vasculitis vasculitis
�� Hemorrhage into Hemorrhage into lungs lungs (decrease (decrease
H&H and platelets)H&H and platelets)
�� CXR pattern CXR pattern similar to ARDS similar to ARDS
�� Steroids Steroids
Cardiovascular Boot Camp April 2009
www.cardionursing.com 16
3131
Special Considerations Air Emboli Special Considerations Air Emboli
�� Large volume of air Large volume of air into venous systeminto venous system
�� Risk FactorsRisk Factors
•• Dialysis Dialysis
•• Pulmonary artery Pulmonary artery catheters catheters
•• Surgical procedures Surgical procedures
•• CABG CABG
�� Symptoms Symptoms
•• DyspneaDyspnea, chest pain, , chest pain, agitation, confusion, agitation, confusion, cough cough
�� Treatment Treatment
•• Prevent Prevent
•• 100% oxygen 100% oxygen
•• Hyperbaric oxygen Hyperbaric oxygen
•• Left lateral / Left lateral / trendelenburgtrendelenburg
•• Positive pressure Positive pressure ventilation ventilation
•• Aspiration of air Aspiration of air
3232
Pulmonary Edema Pulmonary Edema �� Extra vascular accumulation of fluid in the Extra vascular accumulation of fluid in the
lungs (cardiac or non cardiac) lungs (cardiac or non cardiac) •• Results in Results in impaired diffusionimpaired diffusion of oxygen due to of oxygen due to
increase in interstitial space increase in interstitial space
•• Results in Results in decreased V/Q ratiodecreased V/Q ratio due to poorly due to poorly ventilated fluid filled alveoli ventilated fluid filled alveoli
•• Fluid in alveoli also impacts compliance of lungs Fluid in alveoli also impacts compliance of lungs and therefore and therefore ventilation ventilation
�� Capillary endothelium more permeable to water Capillary endothelium more permeable to water and solute than alveolar endothelium and solute than alveolar endothelium
�� Edema accumulates in the interstitium before Edema accumulates in the interstitium before the alveolithe alveoli
Cardiovascular Boot Camp April 2009
www.cardionursing.com 17
3333
Pulmonary Edema Pulmonary Edema
�� Fluid in pulmonary interstitium is Fluid in pulmonary interstitium is removed by lymphatic drainage of removed by lymphatic drainage of the lung the lung
�� Volume of lymph flow from the lung Volume of lymph flow from the lung can increase ten fold in pathological can increase ten fold in pathological conditions conditions
�� Only when this large safety factor is Only when this large safety factor is taxed does pulmonary edema occur taxed does pulmonary edema occur
3434
Pulmonary Edema: Risk Factors Pulmonary Edema: Risk Factors and Treatment and Treatment
�� Loss of integrity of Loss of integrity of alveolar capillary alveolar capillary membrane membrane •• Infection Infection •• Inhaled toxins Inhaled toxins •• Oxygen toxicity Oxygen toxicity
�� Increase in pulmonary Increase in pulmonary capillary hydrostatic capillary hydrostatic pressure pressure •• Left sided heart failure Left sided heart failure •• Excessive fluid Excessive fluid administration administration
•• Occlusion of pulmonary Occlusion of pulmonary vein vein
Other: Blockage of Other: Blockage of lymphatic system lymphatic system
�� Cardiac pulmonary Cardiac pulmonary edema is treated edema is treated as acute as acute decompensated decompensated heart failure. heart failure.
�� Non cardiac Non cardiac pulmonary edema pulmonary edema is treated like is treated like ARDS. ARDS.
Cardiovascular Boot Camp April 2009
www.cardionursing.com 18
3535
Pneumonia Pneumonia
�� Acute infection of the lung parenchyma, Acute infection of the lung parenchyma, including alveolar spaces and interstitial including alveolar spaces and interstitial space space
�� Causes: Causes: •• Bacteria (Community acquired versus Hospital Bacteria (Community acquired versus Hospital acquired) acquired)
•• Virus Virus
•• Fungi Fungi
•• Parasites Parasites
•• MycoplasmaMycoplasma
3636
Risk Factors for Risk Factors for Bacterial Pneumonia Bacterial Pneumonia
�� Previous viral respiratory infection
� Gastro esophageal reflux disease (GERD)
� Chronic alcohol abuse
� Cigarette smoking
� Decreased level of consciousness
� Anesthesia
� Intubation
� Lung disease
�� Diabetes mellitus
� Use of corticorsteroids
� Elderly
Cardiovascular Boot Camp April 2009
www.cardionursing.com 19
3737
Pneumonia: Pathophysiology Pneumonia: Pathophysiology
� Causative agent is inhaled or enters pharynx via direct contact
� Alveoli become inflamed
� Alveolar spaces fill with exudate and consolidate
� Diffusion of O2 obstructed
• Hypoxemia.
� Goblet cells are stimulated to increase mucous
• Increased airway resistance and work of breathing
3838
Pneumonia: Causative Agents Pneumonia: Causative Agents � Common agents in community-acquired pneumonia (younger
and healthier population) • Streptococcus pneumoniae (most common agent in community acquired pneumonia).
• Mycoplasma pneumoniae.• Chlamydia pneumoniae• Viral.
� Haemophilus influenza common among smokers � Klebsiella pneumoniae in patients with chronic alcoholism� Agents in the older population commonly include gram
negative bacilli• Moraxella catarrhalis (particularly common in patients with chronic bronchitis).
• Staphylococcus aureus (in the setting of post viral influenza).
� Methicillin-resistant Staphylococcus aureus (MRSA) also as a cause of community-acquired pneumonia
Cardiovascular Boot Camp April 2009
www.cardionursing.com 20
3939
Hospital Acquired Pneumonia Hospital Acquired Pneumonia
Causative agents � Aerobic gram negative
rods• Klebsiella sp.• Psuedomonas sp.• Enterobacter sp.• Escherichia coli.• Proteus sp• Serratia sp.• Enterococci.
� Staphylococcus aureus (including methicillin-resistant Staphylococcus aureus [MRSA])
� Group B streptococci
� Nosocomial pneumonia is typically caused by bacterial agents that are more resistant to antibiotic therapy.
� Sources• Contamination of pharynx and perhaps stomach with bacteria
• Repeated small aspirations of oral pharyngeal secretions.
• Retrograde contamination from GI tract.
4040
Pneumonia: Clinical Presentation Pneumonia: Clinical Presentation
�� Flu-like symptoms.
� Pleuritic chest pain.
� Confusion in elderly.
� Tachycardia, tachypnea, fever.
� Crackles and wheezes.
� Productive cough.
� Clinical signs of dehydration.
The clinical presentation in the elderly may be more subtle including confusion, dehydration, and fever.
Cardiovascular Boot Camp April 2009
www.cardionursing.com 21
4141
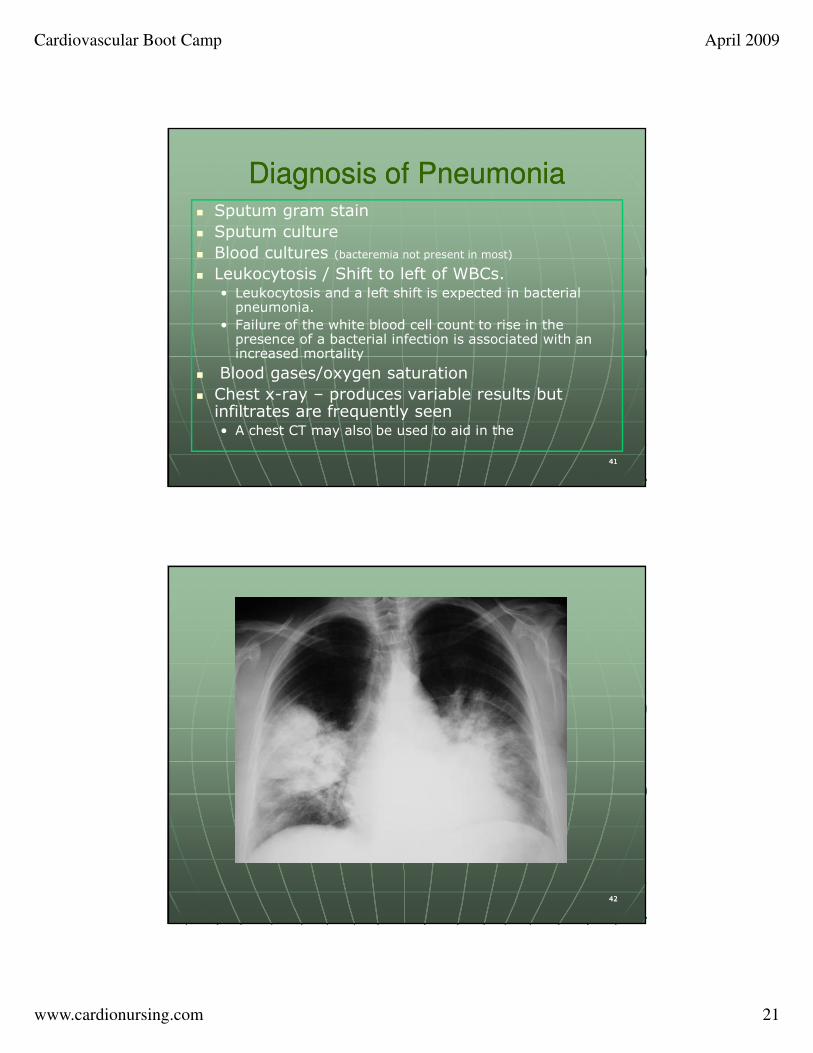
Diagnosis of Pneumonia Diagnosis of Pneumonia � Sputum gram stain
� Sputum culture
� Blood cultures (bacteremia not present in most)
� Leukocytosis / Shift to left of WBCs.• Leukocytosis and a left shift is expected in bacterial pneumonia.
• Failure of the white blood cell count to rise in the presence of a bacterial infection is associated with an increased mortality
� Blood gases/oxygen saturation
� Chest x-ray – produces variable results but infiltrates are frequently seen • A chest CT may also be used to aid in the
4242
Cardiovascular Boot Camp April 2009
www.cardionursing.com 22
4343
Complications of Pneumonia Complications of Pneumonia
� Abscesses may form and rupture into pleural space leading to pneumothorax and/or empyema• Video assisted thoracoscopy with debridement is a treatment option for empyema in the early organizing phase
• Full thoracotomy with decortication may be necessary in later organizing phases
� Pleural Effusion� Acute respiratory failure� ARDS� Sepsis
Mortality rates for nosocomial or hospital-acquired pneumonia are higher than those for community acquiredpneumonia (particularly in the elderly)
4444
Pneumonia: Treatment Pneumonia: Treatment
�� Prevent nosocomial infectionsPrevent nosocomial infections
�� Timely AntibioticsTimely Antibiotics
�� Hydration Hydration (Electrolyte Monitoring) (Electrolyte Monitoring)
�� Deep breathing / incentive spirometry Deep breathing / incentive spirometry
�� Bronchodilators, expectorants, mucolytics Bronchodilators, expectorants, mucolytics
�� Avoid: sedatives and antitussives Avoid: sedatives and antitussives
�� Early activity and mobility Early activity and mobility (DVT Prophylaxis) (DVT Prophylaxis)
Cardiovascular Boot Camp April 2009
www.cardionursing.com 23
4545
Aspiration Aspiration
�� Vomiting or regurgitation Vomiting or regurgitation
�� Large particles Large particles –– airway obstruction airway obstruction
�� pH of liquid determines injury pH of liquid determines injury
•• pH<2.5 or large volume pH<2.5 or large volume
•• Chemical burns destroy type II cells Chemical burns destroy type II cells
•• May induce bronchospasm May induce bronchospasm
•• Increase alveolar capillary membrane Increase alveolar capillary membrane permeability permeability
�� Decrease compliance Decrease compliance
�� Decrease V/Q ratioDecrease V/Q ratio
4646
Aspiration Aspiration
�� Non acidic aspiration Non acidic aspiration
•• More transient More transient
�� Food stuff / small particles Food stuff / small particles
•• Inflammatory reaction Inflammatory reaction
•• Hemorrhagic pneumonia within 6 hours Hemorrhagic pneumonia within 6 hours
�� Contaminated material with bacteria Contaminated material with bacteria can be fatal can be fatal
Cardiovascular Boot Camp April 2009
www.cardionursing.com 24
4747
Aspiration: Possible Prevention Aspiration: Possible Prevention Strategies Strategies
� Avoiding sedation.
� Resting prior to meal time.
� Eating slowly.
� Flexing the head slightly to the “chin down” position.
� Determining food viscosity best tolerated (thickening liquids will improve swallowing in some patients).
4848
Acute Respiratory Distress Acute Respiratory Distress Syndrome Syndrome
A syndrome of acute respiratory failure characterized by non-cardiac pulmonary edema and manifested by refractory hypoxemia. ARDS does not include mild or early acute lung injury, but rather
involves severe and diffused lung injury.
Cardiovascular Boot Camp April 2009
www.cardionursing.com 25
4949
Risk Factors in ARDSRisk Factors in ARDS
�� Sepsis (most common)
� Transfusion
� Aspiration
� Trauma
� Massive transfusion
� Pancreatitis
5050
Acute Respiratory Distress Acute Respiratory Distress Syndrome: Etiology Syndrome: Etiology
�� Direct lung injury Direct lung injury
•• Chest trauma Chest trauma
•• Near drowning Near drowning
•• Smoke inhalation Smoke inhalation
•• Pneumonia Pneumonia
•• Pulmonary Pulmonary embolism embolism
�� Indirect lung Indirect lung injury injury
•• Sepsis Sepsis
•• Shock Shock
•• Multi system Multi system traumatrauma
•• BurnsBurns
•• CABG CABG
•• Head injury Head injury Time from injury of alveolar capillary
membrane to onset of symptoms is 12-48 hours.
Cardiovascular Boot Camp April 2009
www.cardionursing.com 26
5151
ARDS: Pathophysiology ARDS: Pathophysiology � Stimulation of inflammatory and immune systems� Release of toxic substances, causing micro vascular injury� Pulmonary capillary membranes are damaged
• Increase in capillary permeability.
� Cells and fluids leak into interstitium and alveolar spaces• Pulmonary Edema
� Impaired production and dysfunction of surfactant• Alveolar collapse and massive atelectasis.
� Intrapulmonary shunting � Hypoxic vasoconstriction� Decreased the compliance of lung
• High-peak inspiratory pressures to ventilate the lungs.
� Potential development of pulmonary fibrosis in chronic phase.• Endothelium, epithelium, interstitial space expand.• Protein exudate inside the alveoli produces a hyaline membrane.
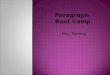
5252
Acute Respiratory Distress Acute Respiratory Distress Syndrome: Diagnosis Syndrome: Diagnosis
� Predisposing condition
� PaO2/FIO2 ratio < 200
� Chest x-ray: Diffuse bilateral infiltrates
(Chest CT may also be used)
� Decreased static compliance of lungs
� PAOP < 18 mm Hg or no evidence of
increased left-atrial pressure
� No evidence of COPD
� No other explanation for above
Cardiovascular Boot Camp April 2009
www.cardionursing.com 27
5353
ARDS: Treatment ARDS: Treatment
�� Optimal ventilation / oxygenation Optimal ventilation / oxygenation
�� Avoid over hydration Avoid over hydration
�� No routine use of steroids No routine use of steroids
�� Pulmonary vasodilators Pulmonary vasodilators
High Mortality High Mortality Persists so Persists so Prevention Prevention
Remains Key Remains Key
5454
Drugs Used to Decrease Drugs Used to Decrease
Right Sided Afterload / Treat Right Sided Afterload / Treat
Pulmonary HypertensionPulmonary Hypertension
•• OxygenOxygen
•• Pulmonary vasodilators Pulmonary vasodilators
�� IV IV
•• NTG NTG
•• Sodium Nitroprusside Sodium Nitroprusside
•• Prostaglandins (PGEProstaglandins (PGE11, PGI, PGI22) )
•• PDEPDE1 1 (phosphodiesterase enzyme) (phosphodiesterase enzyme)
�� Inhaled Inhaled
•• Any of the above Any of the above
•• Nitric Oxide Nitric Oxide
•• Prostacyclin (PGIProstacyclin (PGI22, Epoprostenol, Flolan) or derivative , Epoprostenol, Flolan) or derivative Iloprost Iloprost
Cardiovascular Boot Camp April 2009
www.cardionursing.com 28
5555
Mechanical Ventilator Mechanical Ventilator Management Strategies for ARDSManagement Strategies for ARDS
•• Lower tidal volume ventilation Lower tidal volume ventilation �� Permissive hypercapniaPermissive hypercapnia
•• Maintain plateau pressure < 30 mmHg Maintain plateau pressure < 30 mmHg
•• Uninterrupted PEEP Uninterrupted PEEP •• Avoidance of auto PEEP Avoidance of auto PEEP
•• Airway pressure release ventilation Airway pressure release ventilation •• High frequency ventilation (Oscillatory) High frequency ventilation (Oscillatory) •• Independent lung ventilation Independent lung ventilation •• ECMO ECMO
5656
Case Example Case Example
�� 65 year old female; 85 kg 65 year old female; 85 kg
�� Post witnessed cardiac arrest Post witnessed cardiac arrest
�� Initial PaOInitial PaO22 / FIO/ FIO22 ratio 102 ratio 102
�� Initial diagnosis? Initial diagnosis?
Cardiovascular Boot Camp April 2009
www.cardionursing.com 29
5757
Case ExampleCase Example
�� Ventilator settings:Ventilator settings:•• AC AC
•• Rate 12Rate 12
•• TV 700 ml TV 700 ml
•• FIO2 80% FIO2 80%
•• PEEP 5 cm PEEP 5 cm
�� 22ndnd ABG ABG •• pH pH –– 7.33 7.33
•• PaCO2 PaCO2 –– 40 mmHg 40 mmHg
•• HCO3 HCO3 –– 14 14
•• PaO2 PaO2 -- 9292
�� Ventilator adjustment? Ventilator adjustment?
�� Other treatment Other treatment considerations? considerations?
5858
Open Lung Strategies: Focus on Open Lung Strategies: Focus on Mean Airway Pressure Mean Airway Pressure
�� APRV APRV •• Similar to CPAP with Similar to CPAP with release release
•• Spontaneous breathing Spontaneous breathing allowed throughout cycle allowed throughout cycle
�� Can also be used with no Can also be used with no spontaneous effort spontaneous effort
•• Release time allows Release time allows removal of COremoval of CO22
•• P High P High (20 (20 --30 cmH30 cmH22O)O) and and P low P low (O)(O) (pressure)(pressure)
•• T high T high (4(4--6 seconds)6 seconds) and T and T low low (0.8 seconds)(0.8 seconds) (time) (time)
�� Facilitates oxygenation and Facilitates oxygenation and COCO2 2 clearance clearance
�� Time triggered Time triggered
�� Pressure limited Pressure limited
�� Time cycled Time cycled
AdvantagesAdvantages
�� Lower peak and plateau Lower peak and plateau pressures for given volume pressures for given volume
�� Decreased sedation / near Decreased sedation / near elimination of elimination of neuromuscular blockade neuromuscular blockade
Cardiovascular Boot Camp April 2009
www.cardionursing.com 30
5959
Open Lung Strategies: Focus on Open Lung Strategies: Focus on Mean Airway PressureMean Airway Pressure
�� High frequency oscillation High frequency oscillation
•• Not jet ventilation Not jet ventilation
•• Constant mean airway pressure Constant mean airway pressure
•• TV 1TV 1--3ml/kg3ml/kg
•• Delivers and removes gas: 1/3 time delivery in Delivers and removes gas: 1/3 time delivery in and 2/3 time delivery out and 2/3 time delivery out
•• Usually set starting at 5 to 6 HZ (60 Usually set starting at 5 to 6 HZ (60 oscillations / HZ)oscillations / HZ)
•• Chest wiggle Chest wiggle
•• JVD: Tamponade effect JVD: Tamponade effect
6060
Closed (Simple) Pneumothorax Closed (Simple) Pneumothorax �� Air enters the intra pleural space through the lung Air enters the intra pleural space through the lung causing partial or total collapse of the lung causing partial or total collapse of the lung •• Between visceral and parietal pleura Between visceral and parietal pleura
�� Possible etiologyPossible etiology•• Primary (no underlying lung disease) Primary (no underlying lung disease)
�� Blebs / bullae Blebs / bullae
�� Smoking Smoking
•• Secondary (underlying lung disease) Secondary (underlying lung disease) �� Air enters damaged aveoli Air enters damaged aveoli
�� COPDCOPD
•• Blunt trauma (lung laceration by rib fracture) Blunt trauma (lung laceration by rib fracture)
•• Positive pressure ventilation (rupture of weak alveoli, Positive pressure ventilation (rupture of weak alveoli, bleb or bullous) bleb or bullous)
•• Iatrogenic Iatrogenic –– from medical procedure from medical procedure
Cardiovascular Boot Camp April 2009
www.cardionursing.com 31
6161
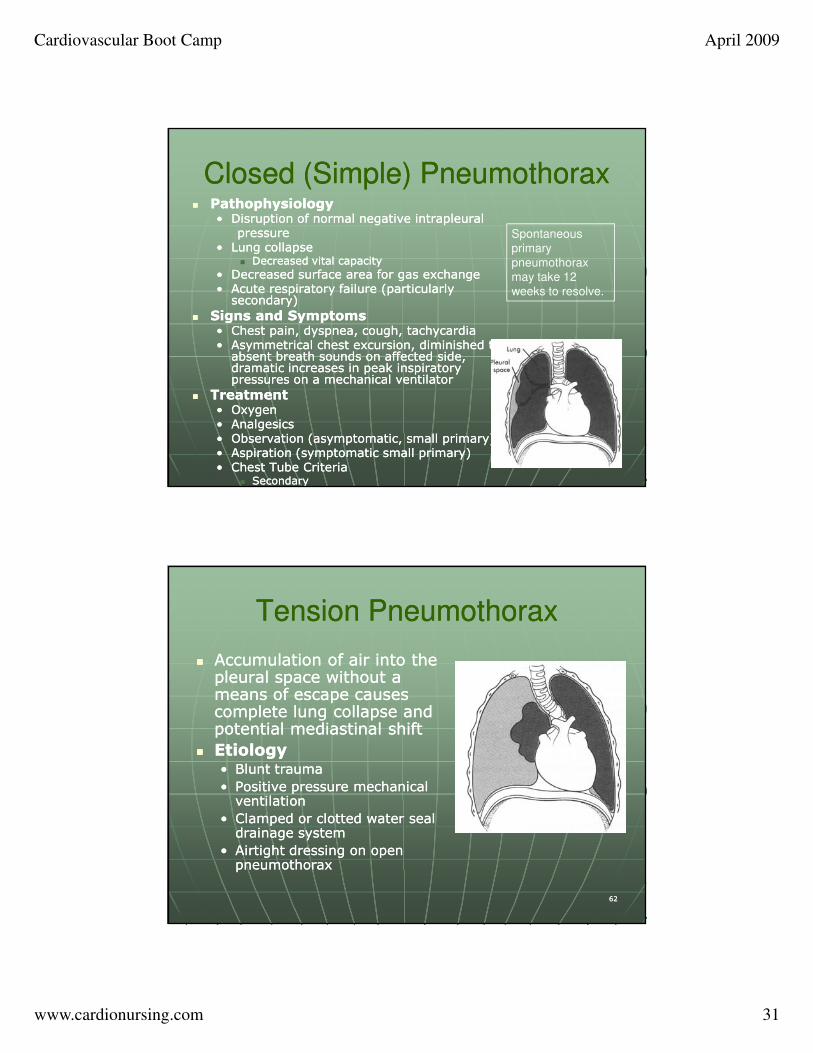
Closed (Simple) PneumothoraxClosed (Simple) Pneumothorax�� Pathophysiology Pathophysiology
•• Disruption of normal negative intrapleural Disruption of normal negative intrapleural pressure pressure
•• Lung collapse Lung collapse �� Decreased vital capacity Decreased vital capacity
•• Decreased surface area for gas exchange Decreased surface area for gas exchange •• Acute respiratory failure (particularly Acute respiratory failure (particularly secondary) secondary)
�� Signs and Symptoms Signs and Symptoms •• Chest pain, dyspnea, cough, tachycardia Chest pain, dyspnea, cough, tachycardia •• Asymmetrical chest excursion, diminished to Asymmetrical chest excursion, diminished to absent breath sounds on affected side, absent breath sounds on affected side, dramatic increases in peak inspiratory dramatic increases in peak inspiratory pressures on a mechanical ventilatorpressures on a mechanical ventilator
�� Treatment Treatment •• Oxygen Oxygen •• Analgesics Analgesics •• Observation (asymptomatic, small primary) Observation (asymptomatic, small primary) •• Aspiration (symptomatic small primary) Aspiration (symptomatic small primary) •• Chest Tube CriteriaChest Tube Criteria
�� Secondary Secondary
Spontaneous
primary
pneumothorax
may take 12
weeks to resolve.
6262
Tension Pneumothorax Tension Pneumothorax
�� Accumulation of air into the Accumulation of air into the pleural space without a pleural space without a means of escape causes means of escape causes complete lung collapse and complete lung collapse and potential mediastinal shift potential mediastinal shift
�� Etiology Etiology •• Blunt trauma Blunt trauma
•• Positive pressure mechanical Positive pressure mechanical ventilation ventilation
•• Clamped or clotted water seal Clamped or clotted water seal drainage system drainage system
•• Airtight dressing on open Airtight dressing on open pneumothorax pneumothorax
Cardiovascular Boot Camp April 2009
www.cardionursing.com 32
6363
Tension PneumothoraxTension Pneumothorax
�� Pathophysiology Pathophysiology
•• Air rushes inAir rushes in--cannot escape pleural space cannot escape pleural space
•• Creates positive pressure in pleural space Creates positive pressure in pleural space
•• Ipsalateral lung collapse Ipsalateral lung collapse
•• Mediastinal shift contralateral lung Mediastinal shift contralateral lung compression potential tearing compression potential tearing of thoracic aorta of thoracic aorta
•• Can also compress heart Can also compress heart decrease RV filling shock decrease RV filling shock
6464
Tension PneumothoraxTension Pneumothorax
�� Similar to closed Similar to closed pneumothorax pneumothorax
�� If mediastinal shift: If mediastinal shift:
•• Tracheal shift away Tracheal shift away from affected side from affected side
•• JVD JVD
•• Hypotension Hypotension
�� Oxygen (100%) Oxygen (100%)
�� Emergency Emergency decompression decompression
�� Chest Tube Chest Tube
�� Other as with Other as with closed pneumoclosed pneumo
Signs and Symptoms
Treatment
Cardiovascular Boot Camp April 2009
www.cardionursing.com 33
6565
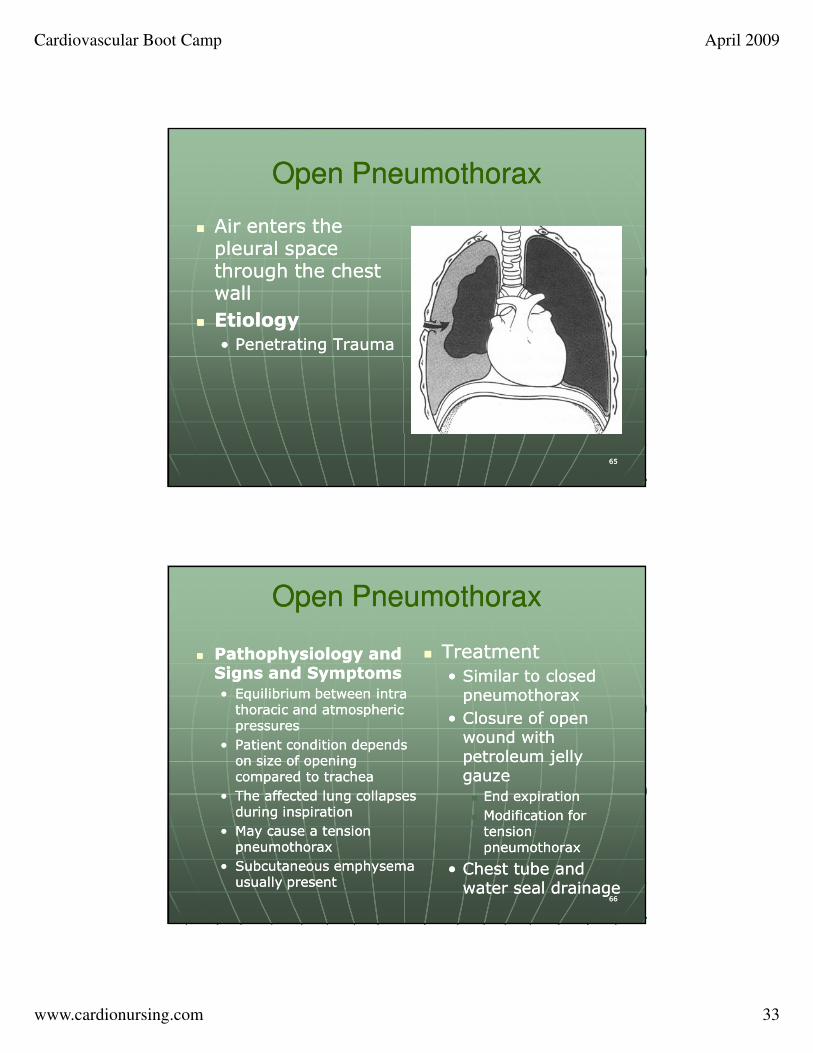
Open Pneumothorax Open Pneumothorax
�� Air enters the Air enters the pleural space pleural space through the chest through the chest wall wall
�� Etiology Etiology
•• Penetrating Trauma Penetrating Trauma
6666
Open PneumothoraxOpen Pneumothorax
�� Pathophysiology and Pathophysiology and Signs and SymptomsSigns and Symptoms
•• Equilibrium between intra Equilibrium between intra thoracic and atmospheric thoracic and atmospheric pressures pressures
•• Patient condition depends Patient condition depends on size of opening on size of opening compared to trachea compared to trachea
•• The affected lung collapses The affected lung collapses during inspiration during inspiration
•• May cause a tension May cause a tension pneumothorax pneumothorax
•• Subcutaneous emphysema Subcutaneous emphysema usually present usually present
�� Treatment Treatment
•• Similar to closed Similar to closed pneumothorax pneumothorax
•• Closure of open Closure of open wound with wound with petroleum jelly petroleum jelly gauze gauze
�� End expiration End expiration
�� Modification for Modification for tension tension pneumothorax pneumothorax
•• Chest tube and Chest tube and water seal drainage water seal drainage
Cardiovascular Boot Camp April 2009
www.cardionursing.com 34
6767
Thanks for Attending Thanks for Attending Cardiovascular Boot CampCardiovascular Boot Camp
You may contact us at You may contact us at www.cardionursing.comwww.cardionursing.com
6868