Embed Size (px)
Citation preview

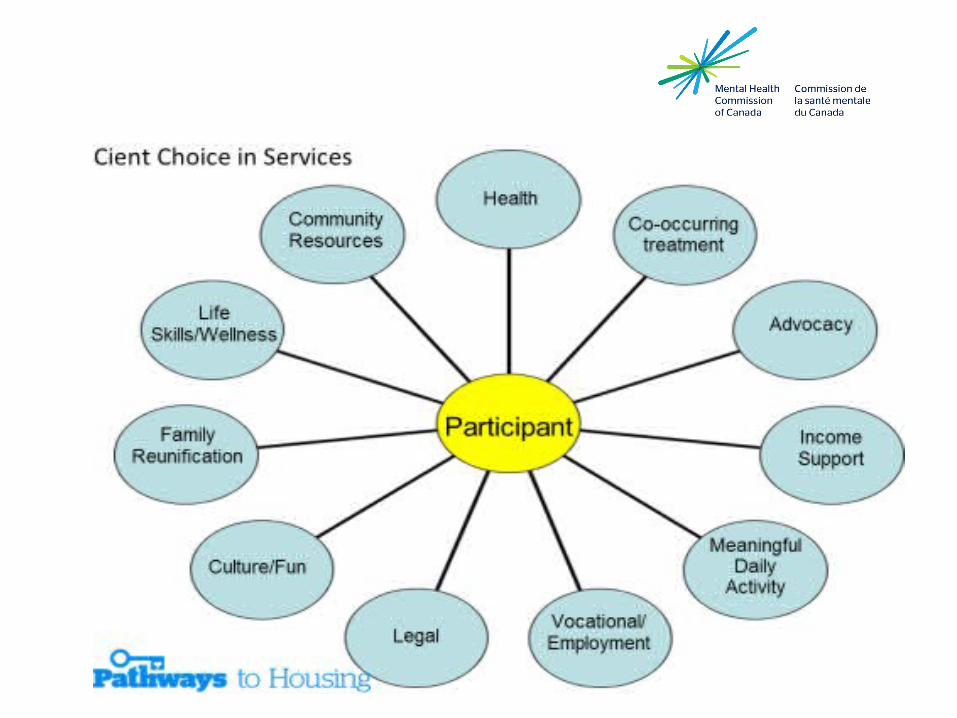
Service teams and home visit
Saint John, New Brunswick, March 12 & 13, 2015
Murielle Doucet, Housing First Trainer (Moncton)Nancy Keays, clinical nurse, Housing First Trainer (Montreal)
Topics today
Act team in a Housing first model
ICM team in a Housing first model
Training
Video « the visit » Pathways
Home visit (principles and chalenges)
At Home / ACT Team
• Intensive treatment and support in community
• Model where almost all services are provided by
team clinicians
• Client/staff ratio of 10:1 or less if higher needs
• 24 hour coverage 7 days a week
• 90% visits in the community
• Medication delivery program/injections
• Program staff are closely involved in hospital
admissions and discharges
At Home / Act Team Peer engagement specialists Psychiatrist & Physician Nursing (medical and mental health) Social worker Substance abuse counselors Supported employment specialist Counsellors, Home Economist, other outreach workers Housing specialist
All staff trained in client choice as a model of care
MHCC decided on adding evidence based interventions to the Housing First ACT teams standards.
• Minimum one peer worker as full team member
• Motivational interviewing
• Integrated Dual Diagnosis Treatment - harm reduction
• “IPS” Employment specialist
• “Illness Management and Recovery” programs
• Family psycho-education and support
Doing ACT
• Morning meeting
• Weekly clinical/planning meeting/complex cases
• Scheduling
• Flexibility all around to meet participant needs
• Challenges of trans-disciplinary care and staff burnout are
very big issues
• Team leader needs to keep eye on workload and team
cohesion
How to “do ACT” and Housing First
Follow Housing First Fidelity measures with your Team rather than standard ACT fidelity measures Yearly fidelity review Always maintain a Housing first philosophy Ask advice, talk to other folks doing Housing First Be Innovative and daring Try new things Avoid too many rules
Think outside the box
ICM teams (At home )
15-20:1 ratio of Staff
Services for people with moderate needs
7 days a week/ 12 hours a day
Outreach/ home visits primarily
Weekly team meetings
Non clinical staff, services brokered out
Challenges are developing linkages to health and mental health
and addiction services
Building a good team
Great team leader with skills, experience
Provide basic and ongoing trainings
Hire Peer Workers in fully integrated roles !!!
Staff need to be eternally Hopeful, Empathic and Flexible
Ability to work with challenging personalities and
behaviours
Innovative strategies are needed
Training - Team Skills
Recovery oriented Strengths based approach Harm reduction Motivational interviewing Trauma-informed practice Cultural competency Crisis Management/Suicide intervention & Assessment Self Medication Management Anger Management

Video « The visit » Pathways
https://www.youtube.com/watch?v=JOb8tX1MFGk

Home Visit
5 principles of Housing First
① Immediate access to housing with no readiness conditions② Personal choice and self –determination③ Recovery orientation④ Individualized person-driven supports⑤ Social and community integration
2 Conditions : 1) Visit once a week2) Pay 30 percent of income for rent
Choice based Goals
work towards the persons goals
Recovery/Care plans should be focused.
Doing a Recovery plan - way to get to know people - their
hopes and dreams
Use motivational interviewing techniques to make goals more
specific and focused
Strength-based approach
• Recovery is based on strengths
• Focus on the healthy part of the person and believe in the potential of recovery
• Recovery is a personal journey of healing and transformation
• An on-going process, takes time and is multi-dimensional
Recovery is the main focus
The person in recovery « owns » his or her recovery process. The person searches for…
• Hope for the future• A more positive sense of self• Positive social roles• A sense of belonging within the community• A sense of purpose• The sense that what he or she does and decides matters
How Housing First differs…From what’s wrong to what’s STRONGRather than focusing primarily on what is “wrong” with the person • symptoms• substance use concerns• skill and resource deficits
HF focuses foremost on what is “right” with people • Goals• Skills• Knowledge• Interests• Resources and supports• Motivation• What they are already doing that helps them manage their condition
Home Visit Philosophy
Respectful of the person’s : • Boundaries• Culture• Space and time• Their tolerance for degree of
contact (length and # of visits)
• Ongoing active engagement• Focus on Person’s Choices not
the programs goals

Opportunity for Engagement
Opportunity to develop a trusting relationship
Clues about tastes, interests and hopes
Learn who they are
Targeted Intervention
Purposeful and goal directed
Focus on person’s chosen goals (recovery plans)
Provides continuity of support and treatment
Opportunity for continuous engagement
Interventions extends from home to community settings
Assess Well-being
How is the person today?• Their greeting
• Clothing
• State of alertness
• Mood
• Changes from usual patterns
Why Home visits: “Achieving goals”
• Learning new skills best done in “real” environments• Budgeting and ADL’s• Recovery happens in the community, not the office• Friends, work and social inclusion happen in the community• Community Integration
Team operations/home visits
• Minimum once a week• Schedule in advance/avoid surprise
visits• Reminders, calendars, notes on fridges • Varies over time• Non-linear process• Need to be flexible and accommodate
the needs of the individual• Effi ciency is important• Distribute workload by specialty and
geographically
To look at the condition of the apartment
Organized to disorganized?
Do you look in every room?
Careful observation
Are there repairs that need
to be made?
Liaising with property
manager?
Looks like we have a guest! Who’s the guest?

Do you intervene?

What if you see this in a tenant’s fridge?
Are there dreams and hopes that you would not support?

What ever path the person chooses, just be there to listen and support. Walk beside them.



![[2003] 3 R.C.S. DOUCET-BOUDREAU c. NOUVELLE-ÉCOSSE 3[2003] 3 R.C.S. DOUCET-BOUDREAU c. NOUVELLE-ÉCOSSE 3 Glenda Doucet-Boudreau, Alice Boudreau, Jocelyn Bourbeau, Bernadette Cormier-Marchand,](https://img.pdfslide.us/doc/110x75/5e55f1919ac6771b5d14d0f6/2003-3-rcs-doucet-boudreau-c-nouvelle-cosse-3-2003-3-rcs-doucet-boudreau.jpg)