Embed Size (px)
Citation preview
SERUM FERRITIN AS AN EARLY INDICATOR OF
SEVERITY OF DENGUE
DISSERTATION SUBMITTED FOR THE DEGREE OF
M.D BRANCH VII
(PAEDIATRIC MEDICINE)
REG. NO: 201717102
MAY 2020
MADURAI MEDICAL COLLEGE, MADURAI
THE TAMILNADU DR. M.G.R MEDICAL UNIVERSITY
CHENNAI, TAMIL NADU
CERTIFICATE
This is to certify that the dissertation entitled “SERUM
FERRITIN AS AN EARLY INDICATOR OF SEVERITY OF
DENGUE” is the bonafide work of Dr. V. MOHAN RAJ in partial
fulfilment of the university regulations of the Tamil Nadu Dr. M.G.R
Medical University, Chennai, for M.D Degree Branch VII –
PAEDIATRIC MEDICINE examination to be held in MAY 2020.
Dr. J. SANGUMANI, MD.,
Dean, Madurai Medical College,
Government Rajaji Hospital,
Madurai – 625020
BONAFIDE CERTIFICATE
This is to certify that the dissertation entitled “SERUM
FERRITIN AS AN EARLY INDICATOR OF SEVERITY OF
DENGUE” submitted by Dr. V MOHAN RAJ to the faculty of
Pediatrics, The Tamil Nadu Dr. M.G.R Medical University, Chennai
in partial fulfillment of the requirement for the award of M.D Degree
Branch VII (PAEDIATRIC MEDICINE) is a bonafide research
work carried out by him under our direct supervision and guidance.
Dr. S.BALASANKAR MD DCH
Director I/C & Professor of Paediatrics
Institute of Child Health & Research center,
Madurai Medical College,
Madurai.
DECLARATION
I, Dr. V MOHAN RAJ, solemnly declare that the dissertation
titled “SERUM FERRITIN AS AN EARLY INDICATOR OF
SEVERITY OF DENGUE” has been conducted by me at Institute
of Child Health and Research Centre, Madurai under the guidance and
supervision of Prof. Dr. S. BALASANKAR M.D., DCH.,
This is submitted in part of fulfillment of the regulations for the
award of M.D Degree Branch VII (Paediatric Medicine) for the
May 2020 examination to be held under The Tamil Nadu Dr. M.G.R
Medical University, Chennai. This has not been submitted previously
by me for any Degree or Diploma from any other University.
Place: Madurai Dr. V MOHAN RAJ
Date:
CERTIFICATE - II
This is to certify that this dissertation work titled “SERUM
FERRITIN AS AN EARLY INDICATOR OF SEVERITY OF
DENGUE” of the candidate Dr. V MOHAN RAJ with registration
Number 201717102 for the award of M.D., in the branch of
PAEDIATRICS personally verified the urkund.com website for the
purpose of plagiarism Check. I found that the uploaded thesis file
contains from introduction to conclusion pages and result shows 16%
percentage of plagiarism in the dissertation.
Guide & Supervisor sign with Seal.
ACKNOWLEDGEMENT
First, I would like to thank the almighty for giving me this
opportunity. My sincere thanks to Prof. Dr. J. SANGUMANI, M.D.,
Dean, Government Rajaji Hospital and Madurai Medical College for
permitting me to do this study and utilize the institutional facilities.
I express my sincere thanks and gratitude to
Prof. Dr. S. BALASANKAR M.D., DCH., Professor and Director I/C,
Institute of Child Health & Research Centre, Madurai, for his able
supervision, encouragement, valuable suggestions and support for this
study. I am also greatly thankful for his able guidance, critical review,
constant encouragement and full support rendered in every aspect of this
study.
I would extend my sincere thanks to Prof. Dr.M.S.
Rajarajeshwaran, M.D., DCH., Prof. Dr. M. Kulandaivel, M.D.,
DCH., Prof. Dr. S. Shanmugasundaram, M.D., DCH., and
Prof. Dr. Nandhini, M.D., DCH., Prof. Dr. M. Balasubramanian,
M.D., DCH., Prof Dr. D Raj Kumar, M.D., and
Prof. Dr. J Ashokaraja, M.D., DM., for their valuable advice and
encouragement at every stage of this study.
I wish to express my sincere thanks to my Assistant Professors of
Pediatrics, Dr.P.Ramasubramaniam, M.D., DCH., Dr. Vanitha, M.D.,
Dr.J.Balasubramanian, M.D., DCH., Dr.R.Suresh, M.D., for their
constant guidance, encouragement and support throughout my study. I also
extend my thanks to Dr. P. Murugalatha, M.D., Dr. P. Kannan, M.D.,
Dr. K. Ramya, M.D., Dr. P. Guna, M.D., DMRD.,
Dr. S. Murugesalakshmanan, M.D., Dr. Abu backer siddiq, M.D.,
DCH., Dr. Suganthi, M.D., Dr. A.N.Karthik, M.D.,
Dr. Venkataramanan, M.D., DCH., Dr. Sonia Rosalind Martina,
M.D., Dr. M. K. Lenin, M.D., for their guidance, supervision, valuable
suggestions and support throughout this study.
I thank the Institutional Ethical Committee for granting me
permission to conduct the study. I also express my gratitude to all my
fellow postgraduates for their kind cooperation in carrying out this study
and for their critical analysis.
I thank the Institute of Microbiology, Department of Biochemistry
and Department of Radiology of Government Rajaji hospital, Madurai for
their co-operation throughout my study.
Last but not the least, I submit my heartfelt thanks to the children
and their parents for extending full co–operation to complete my study
successfully.
CONTENTS
Sl.
No Title Page no
1. Introduction 1
2. Aims and Objectives 38
3. Review of literature 39
4. Materials and Methods 41
5. Observation and Results 46
6. Discussion 74
7. Conclusion 77
8. Limitations 78
Annexures :
• Bibliography
• Proforma
• Abbreviations
• Consent form
• Master Chart
1
INTRODUCTION
Dengue is a arthropod borne viral infection caused by flavi virus
which causes simple fever to severe complications like dengue shock
syndrome and dengue hemorrhagic syndrome. It is epidemic all over the
world and in recent upsurge.
Dengue epidemic has resulted in significant mortality. There is no
appropriate treatment and only supportive treatment can be given.
Most of the cases recover with no complications and only certain
number of cases can have complications and they require careful
monitoring and assessment. In order to predict the complications and to
find out which case requires monitoring, we need a parameter to assess.
In this study we aimed to predict the severity in early phase of the
disease, using Serum Ferritin.
SERUM FERRITN & DENGUE
In recent times a phenomenon called macrophage activation
syndrome (MAS) or hemophagocytic syndrome (HS) is being frequently
reported in patients with severe dengue. MAS is a severe systemic
inflammatory condition due to excessive activation and proliferation of T
cells and well differentiated macrophage that leads to hyperactivated but
dysregulated immune responses22,23,24. This results in an overwhelming
2
inflammatory response leading to non remitting high rise of temperature,
organomegaly (involving liver and spleen), hemorrhage,
lymphadenopathy, and central nervous system (CNS) dysfunction.
Hyperferritinemia (levels above 10000ug/L) is a flagship sign of MAS;
however hypoalbuminemia, cytopenia, coagulopathy, abnormal liver
function tests, hypertriglyceridemia, hemophagocytosis, and elevated
serum sCD25 and sCD16 levels also serve as adjunct markers of MAS.
Hemophagocytic syndrome (HS) is being increasingly reported in patients
with severe dengue with multiorgan complication and is observed in severe
dengue involving children.25-28
Another mechanism by which ferritin can be used as a predictor is
increased expression of acute phase reactants is observed in patients with
severe dengue infection when compared to non-severe cases. This serves
to prognosticate the dengue infected patients well ahead of the appearance
of clinical warning signs. One such acute phase reactant is ferritin which is
produced by reticuloendothelial cells in response to infection and
inflammation. Ferritin is highly elevated in dengue infected patients than
in patients with other febrile illnesses. Hyperferritinemia seen in these
patients exhibit two opposite functions; Early in the phase of clinical
illness, increased serum ferritin levels exert a protective effect by chelating
the toxic free iron radicals at the site of inflammation15. while in severe
3
cases, raised ferritin may assume a pathogenic role by activating immune
cells resulting in cytokine storm.
GEOGRAPHICAL DISTRIBUTION
Global
Dengue fever is known in the tropical Southeast Asia and Western
Pacific for more than a century. The haemorrhagic form was first
recognized in Philippines in 1953. Subsequently DHF was recognized in
Thailand, India, Singapore, malaysia and Vietnam. In 1978, a big outbreak
was reported from China resulting in 22,122 cases. In 1981, a large
epidemic occurred in Cuba resulting in nearly 0.35 million cases of dengue
fever. Out of these, 24,000 had DHF and 10,000 had DSS. Dengue has also
been noticed in temperate regions of North America, Africa, and
Mediterranean Europe1,2.
As per current estimates, more than 100 countries are endemic for
dengue fever and about 40% of the world populations (2.5 billion people)
are at risk in tropics and subtropics. In 2010, 1.6 million cases of dengue
were reported in the Americas alone, of which 49,000 cases were severe
dengue3,4. Recently, dengue has also been reported from Costa Rica,
France, Mexico, Croatia and Portugal. Incidence of dengue infections
annually has almost doubled from 50 million to 96 million (2010) in last
few years.
4
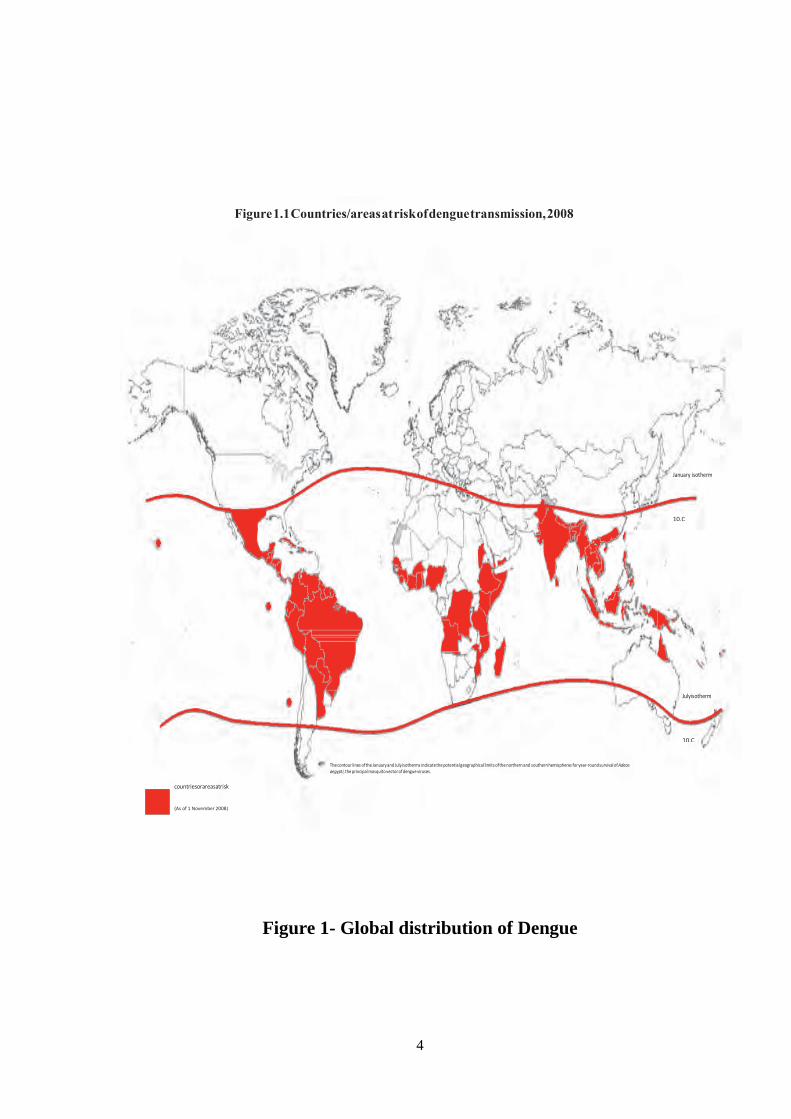
Figure 1- Global distribution of Dengue
Figure 1.1 Countries/areas at risk of dengue transmission, 2008
10.C
10.C
(As of 1 November 2008)
5
India
India alone accounted for almost 34% of global dengue burden by
2010. The National Dengue Day was observed on 16th May 2016. Disease
is prevalent throughout India in most of the metropolitan cities and towns
and is endemic in 18 out of 35 states. Outbreaks have also been reported
from rural areas of Haryana, Maharashtra, and Karnataka. Recent trends in
transmission have shown occurrence of larger and more frequent
outbreaks, geographic expansion of endemic transmission, spread of the
disease from urban to semiurban and rural areas and an increasing
proportion of severe cases and deaths. An increased propensity to
hyperendemic areas particularly in large urban areas, is also noted5.
During 1996, a severe outbreak of dengue or DHF occurred in Delhi
wherein about 10,252 cases and 423 deaths were reported. In 2006, India
witnessed another outbreak with 12,317 cases and 184 deaths in 21 states.
The initial epidemics in India were due to serotype 2 or 4. The dengue
serotype 1 was seen as predominant serotype in Delhi during 2007-2010.
Concurrent infection of chikungunya and dengue serotype 2 has been
reported from Delhi and vellore.
Cyclic epidemics are increasing in frequency and in-country
geographic expansion is reported in India due to deciduous dry and wet
climatic zone with circulation of multiple virus serotypes. Cyclic
6
epidemics occurs once in every few years, which is usually associated with
good monsoon rains. Sporadic case usually present throughout the year.
However, with improved case management, the case fatality has decreased
from 3.3% in 1996 to 0.4% in 2010.
DENGUE VIRUS
Dengue virus has at least four serotypes.
DENV-1
DENV-2
DENV-3
DENV-4
These are antigenically similar but do not offer a complete cross
protection after infection by any one of them to other serotypes. Infections
in human by a serotype will produce lifelong immunity against reinfection
only for that particular serotype but not aganist other serotype. Subsequent
infection (secondary infection) by another serotype causes severe dengue
along with increased mortality. The severity of epidemics mostly caused
by serotype 1 followed by types 2 and 3.
EPIDEMIOLOGY
Vector
Aedes aegypti is the vector for dengue virus. Female mosquito bites
the man mostly during daytime. After feeding on a person with viremia,
7
the female mosquito can transmit dengue virus immediately or after a
period of 10-14 days (extrinsic incubation period). The extrinsic incubation
period is a important factor in successful transmission of the disease. A
lower environmental temperature increases the extrinsic incubation period,
which in turn, decreases the transmission. Once the mosquito becomes
infective, it remains so till its death
Figure 2- Aedes mosquito
The flight range of an adult A. aegypti mosquito is usually around
25-50 metres in an urban environment. However, the vector can be
transported by water, land, and air travel contributing to the speedy
transmission for vast areas. For dengue transmission, the number of
infected female mosquitoes per house is important. Usually this number is
small, and for an Indian epidemic it was observed to be just 1 per household
(house index). The minimum vector density, below which the dengue
8
transmission ceases, is not known at present. The Aedes aegypti mosquito
breeding is not necessarily related to the ambient temperature. The
mosquito has been found at very high altitudes like 2,200 metres above the
sea level. Vectors must survive longer than the sum of the initial non-
feeding period after birth (usually 2 days) and the extrinsic incubation
period to be able to infect another human. Longevity under natural
conditions ranges from 8 days to 42 days. The eggs of Aedes aegypti can
survive without water for a year.
Host factor
People at all ages are susceptible to dengue. In Asians, disease is
more severe in children. This is in contrast to America where infection
mainly occurs in adults which is usually mild. Severe dengue occurs in
children who have experienced a previous dengue infection. Other factors
which are associated with increase host susceptibilities to severe dengue
include HIV infection, bronchial asthma, certain HLA types like HLA
1(A04, A2, B0, B46), HLA 2 (DQ, DR4, DR1), TNF alpha, TGF beta,
G6PD deficiency, mutation in mannose binding lectin 2 gene.
ENVIRONMENTAL FACTORS
In tropical countries, a positive association between rainfall or larval
density and dengue incidence has been documented. The vector survives at
hot and humid temperature (16-30 degree celsius & 60-80% humidity). But
9
dengue cases are also reported in areas with less rainfall also. The
transmission of disease occurs only, if the ambient temperature is above 16
degree Celsius. In winter season the transmission rate is very low. This is
due to prolongation of extrinsic incubation period beyond the longevity of
mosquito.
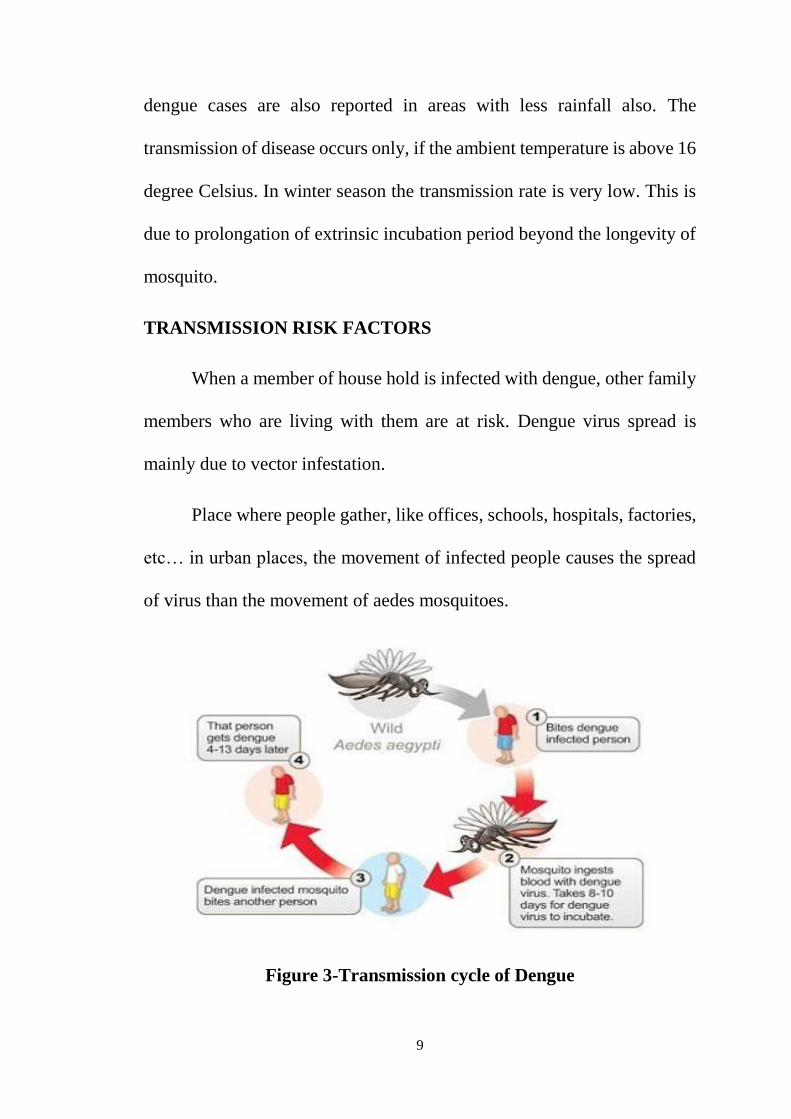
TRANSMISSION RISK FACTORS
When a member of house hold is infected with dengue, other family
members who are living with them are at risk. Dengue virus spread is
mainly due to vector infestation.
Place where people gather, like offices, schools, hospitals, factories,
etc… in urban places, the movement of infected people causes the spread
of virus than the movement of aedes mosquitoes.
Figure 3-Transmission cycle of Dengue
10
PATHOGENESIS
Dengue virus infects the peripheral blood mononuclear cells within
a few days of infective mosquito bite.
Two patterns of immune response follow:
(1) Primary and (2) secondary (anamnestic).
Persons never previously infected with a flavivirus, nor immunized
with a flavivirus vaccine (e.g. Yellow Fever, Japanese encephalitis), mount
a primary IgM antibody response when infected with dengue virus,
appearing within 2-3 days of defervescence and peaking at 2 weeks after
the onset of symptoms. Antidengue IgG appears afterwards. Individuals
with immunity due to previous flavivirus infection or immunization mount
a secondary anamnestic antibody response when infected with dengue
virus5,6. In secondary flavivirus infections, which account for most cases
of severe dengue, the dominant immunoglobulin is IgG; the levels of IgM
being much lower. A mechanism of immune enhancement or antibody
dependent enhancement (ADE) is observed in dengue due to heterologous
non-neutralizing antibodies. This is responsible for serious organ
dysfunction and haemorrhagic disturbances which can occur during
secondary infection by a different serotype. This mechanism promotes
binding of dengue virus to surface expressed Fc gamma receptors on
monocytes and macrophages, further promoting viral replication and
11
spread. Thus, sequential rather than simultaneous exposure of different
serotypes of dengue virus carry a higher chance of ADE resulting in serious
disease. Thus, antibody against a strain of dengue virus does not protect
from a different strain of virus. Rather, it may increase its capacity to
multiply in human monocytes. The infected monocytes result in activation
of cross-reactive CD4+ and CD8+ cytotoxic lymphocytes. Cytotoxic
lymphocytes mediate release of cytokines resulting in plasma leakage and
haemorrhage and are primarily responsible for host defense in dengue
mediated via interferon-gamma. Recent studies have highlighted the role
of HLA linked protective role of CD8 lymphocytes. Researchers have
found that certain phenotypes of HLA may cause hyporesponsiveness of
interferon -7 response, thereby weekening the host response.7

12
PATHOPHYSIOLOGY
Two main pathophysiological changes occur in dengue,
These are
(1) Increased vascular permeability, resulting in loss of plasma from
the vascular compartment to third space accumulation, hemoconcentration,
low pulse pressure, and other signs of shock8 and
(2) Disorder in the hemostasis involving thrombocytopenia,
coagulopathy and vascular changes.
Secondary dengue infection results in formation of immune
complexes and activation of complement system. TNF-alpha, interferon,
and interleukin-2 are elevated, and C1q, C3-C8, are depressed. As a result,
vasoactive amines are released from the platelets, These cause massive
release of water, electrolytes, and plasma proteins from the blood vessels
and lead to hypovolemic shock. Increased vascular permeability is
mediated through the nitric oxide pathway
Platelet defects are both quantitative and qualitative. Thus, a patient
with a normal platelet count may still have a prolonged bleeding time,
maculopapular and petechial rashes are present. In these lesions, dengue
antigen, IgM, and complement (C3) have been observed.

13
It may be noted that virus is usually not detectable in blood once
shock manifests, though viral replication occurs in various organs.
COURSE OF DENGUE FEVER
Figure 4- Course of Dengue illness
FEBRILE PHASE
Febrile phase lasts from 2-5 days. During the febrile phase child
presents with fever, headache, retro orbital pain, myalgia and vomiting.
14
It is difficult to distinguish dengue fever from non dengue illnesses
at this stage. Child may present with progressive decrease in leucocyte
count with tender hepatomegaly.
CRITICAL PHASE
Following the febrile phase, child may enter into the critical phase,
which usually lasts from 4 to 7 days. Patients with increased capillary
permeability may manifest with the warning signs, mostly as a result of
plasma leakage.
The warning signs are persistent vomiting and severe abdominal
pain which are the early indications of plasma leakage and become
increasingly worse and the patient progresses to the shock state.
The patient becomes increasingly lethargic but usually remains
mentally alert. These symptoms may persist into the shock stage.
Weakness, dizziness or postural hypotension, spontaneous mucosal
bleeding or bleeding at previous venepuncture sites are important
haemorrhagic manifestations. Increasing liver size and a tender liver is
frequently observed.
Appropriate management at this stage prevents the complication and
mortality.
15
RECOVERY PHASE
As the patient survives the critical period, enters into the recovery
phase, which occurs due to reabsorption of fluid from the extravascular
compartment. At this stage patient develops bradycardia, electrocardiac
abnormalities and pruritis.
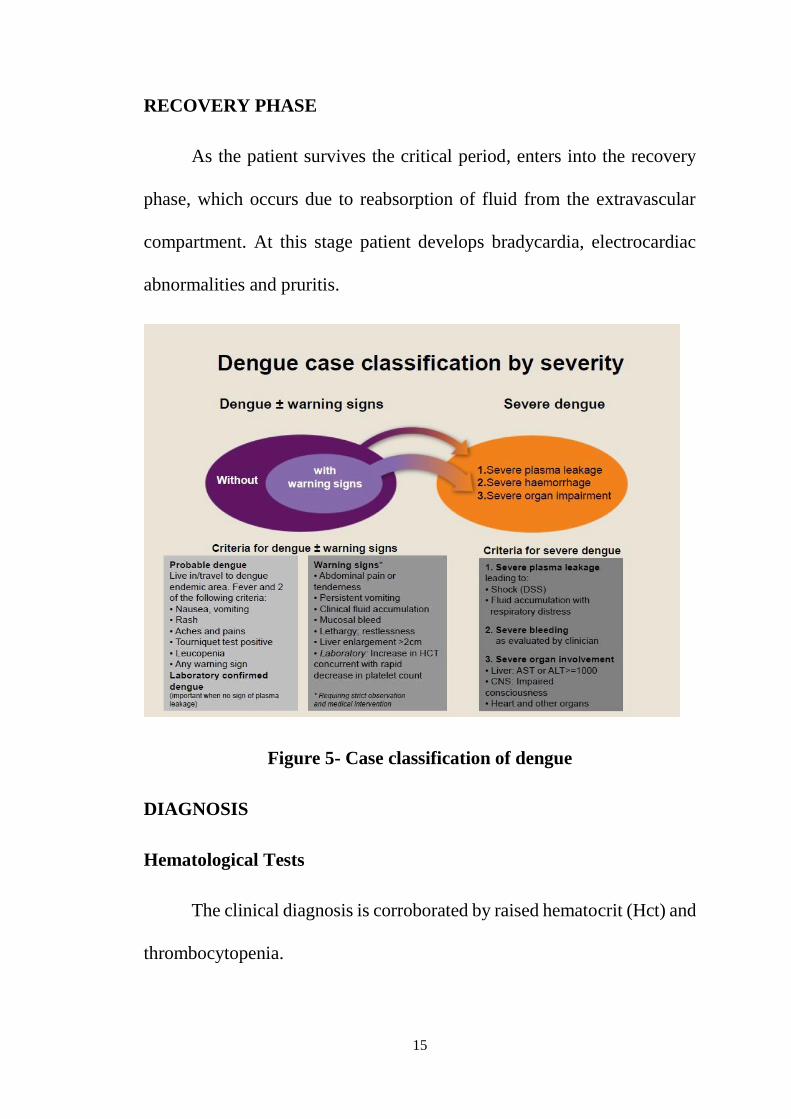
Figure 5- Case classification of dengue
DIAGNOSIS
Hematological Tests
The clinical diagnosis is corroborated by raised hematocrit (Hct) and
thrombocytopenia.
16
An Hct level rise of greater than 20% is a sign of hemo concentration
and precedes shock. The Hct level should be monitored at least every
24 h to facilitate early recognition of warning signs and every 3-4 h
in severe dengue.
Thrombocytopenia occurs in up to 50% of children with dengue.
Platelet counts of less than 100,000 cells/uL indicate onset of critical
phase and typically occur before defervescence and the onset of
shock. The platelet count should be monitored at least every 24 h
initially.
The white blood cell count can be normal or show leukocytosis
during initial phase. Leukopenia, often with lymphopenia, precedes
thrombocytopenia and is observed near the end of the febrile phase
of illness.
Electrolyte abnormalities are seen in critical phase. Metabolic
acidosis and elevated blood urea are observed in those with shock.
Serum glutamic pyruvic transaminase (SGPT) levels are elevated.
Low serum albumin levels are a sign of hemoconcentration10
17
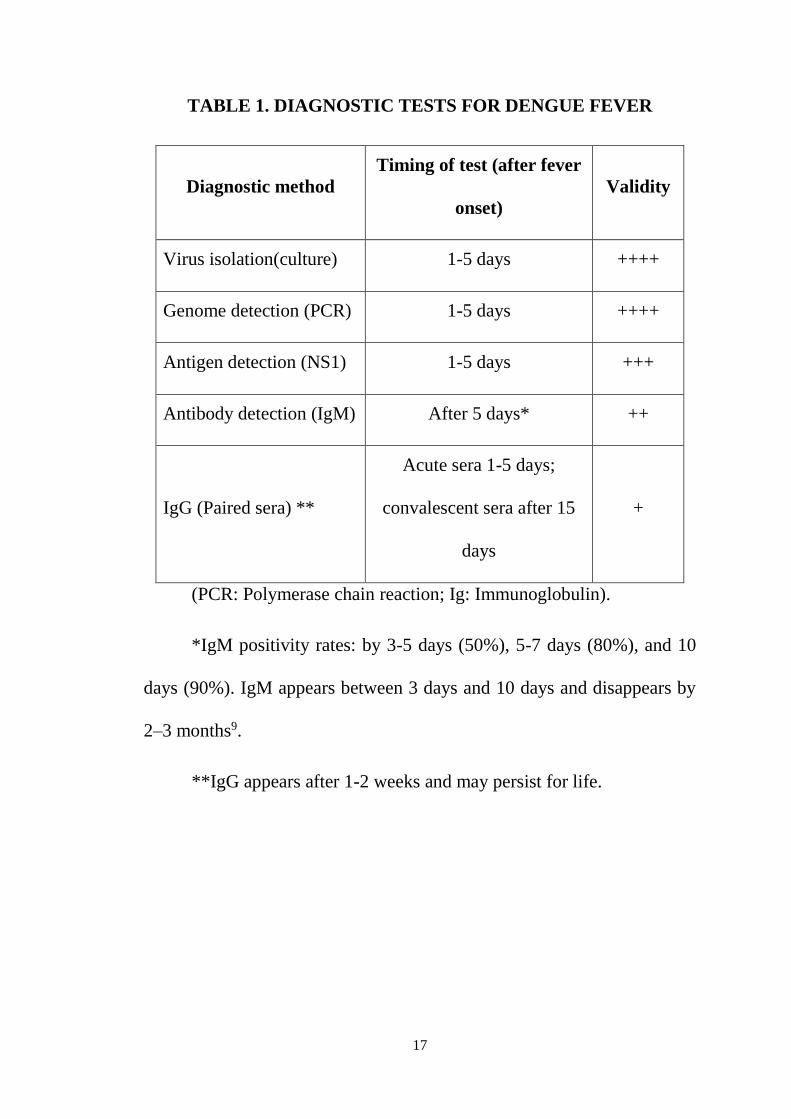
TABLE 1. DIAGNOSTIC TESTS FOR DENGUE FEVER
Diagnostic method
Timing of test (after fever
onset)
Validity
Virus isolation(culture) 1-5 days ++++
Genome detection (PCR) 1-5 days ++++
Antigen detection (NS1) 1-5 days +++
Antibody detection (IgM) After 5 days* ++
IgG (Paired sera) **
Acute sera 1-5 days;
convalescent sera after 15
days
+
(PCR: Polymerase chain reaction; Ig: Immunoglobulin).
*IgM positivity rates: by 3-5 days (50%), 5-7 days (80%), and 10
days (90%). IgM appears between 3 days and 10 days and disappears by
2–3 months9.
**IgG appears after 1-2 weeks and may persist for life.
18
Serodiagnosis
Serum specimens should be sent to the laboratory for serodiagnosis,
polymerase chain reaction (PCR), and viral isolation. Because the signs
and symptoms of dengue fever are nonspecific, attempting laboratory
confirmation of dengue infection is important.
Serodiagnosis is based on (1) detection of viral nonstructural protein
1 (NS1) during initial illness; (2) detection of IgM antibodies to dengue; or
(3) fourfold rise in dengue IgG in paired samples11. Table 1 outlines the
desired timing of these tests for confirming the diagnosis. Laboratory
criteria for definitive diagnosis include one or more of the following:
Isolation of the dengue virus from serum, plasma, leukocytes, or
autopsy samples
Demonstration of dengue virus antigen in serum samples via enzyme
immunoassay or in autopsy tissue via immunohistochemistry or
immunofluorescence can be done. NS1 is a glycoprotein produced by the
virus which can be detected early, between 1st to 4th day of illness. It is
specific and has a high sensitivity.
Demonstration of a fourfold or greater change in reciprocal IgG or
IgM antibody titers to one or more dengue virus antigens in paired serum
samples. IgM antibody appears early in disease course, requires single
sample and is less cross-reactive to other flaviviruses12.
19
Thus, measurement of raised IgM appears to be most prudent when
done after 5th day of illness. As per the NVBDCP, the laboratory test being
followed is the IgM antibody-capture enzyme-linked immunosorbent assay
(MAC-ELISA) for dengue virus, which captures the dengue specific IgM
by using anti-human IgM. There are quicker and cheaper rapid diagnostic
test (RDT) kits available which test the presence of anti-IgM or IgG or NS1
antigen. However, these kits carry a high false positive rate and are not
recommended by the WHO or under NVBDCP.
Detection of viral genomic sequences in autopsy tissue, serum, or
cerebral spinal fluid (CSF) samples via PCR.
Diagnostic kits for NS1 and MAC-ELISA can be procured from
National Institute of Virology, Pune under NVBDCP. The Government of
India has set up surveillance hospitals and apex referral laboratories for
improved disease surveillance.
Dengue diagnostics for clinicians
The objectives of dengue laboratory diagnosis are
(i) to confirm the clinical diagnosis and
(ii) to provide information for epidemiological surveillance.
Laboratory diagnosis is not necessary for clinical management except in
atypical cases or when carrying out differential diagnosis with other
infectious diseases.
20
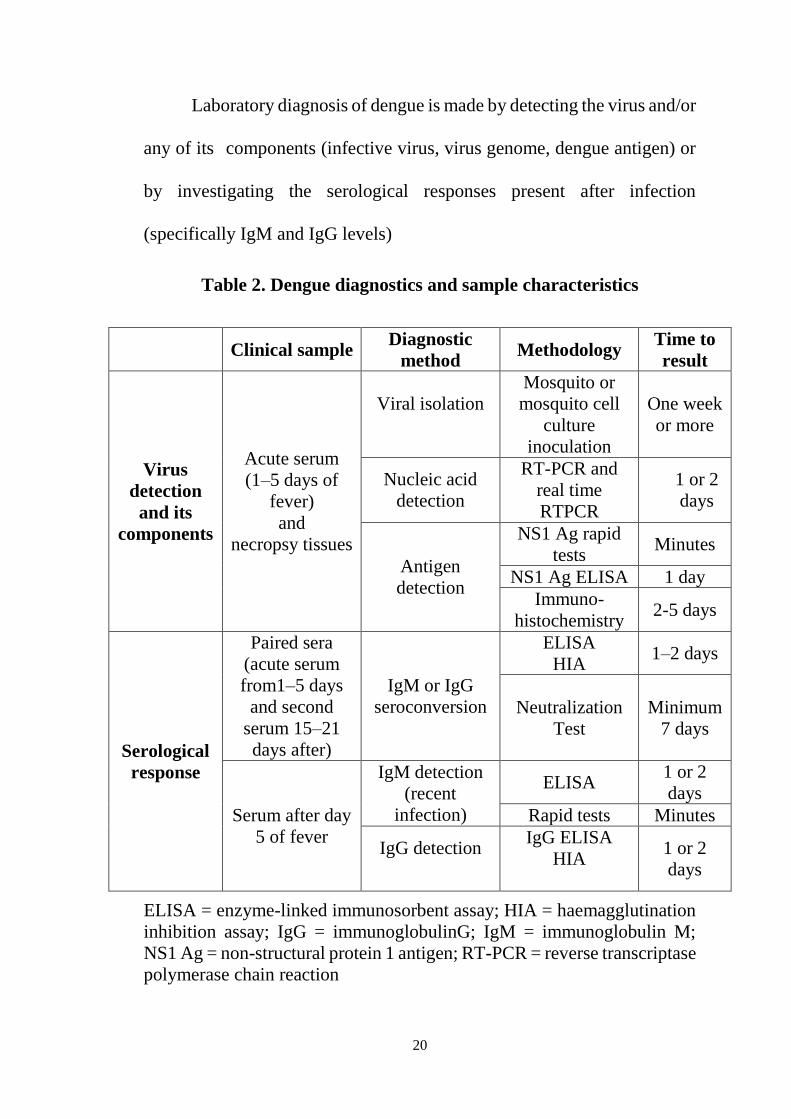
Laboratory diagnosis of dengue is made by detecting the virus and/or
any of its components (infective virus, virus genome, dengue antigen) or
by investigating the serological responses present after infection
(specifically IgM and IgG levels)
Table 2. Dengue diagnostics and sample characteristics
Clinical sample Diagnostic
method Methodology
Time to
result
Virus
detection
and its
components
Acute serum
(1–5 days of
fever)
and
necropsy tissues
Viral isolation
Mosquito or
mosquito cell
culture
inoculation
One week
or more
Nucleic acid
detection
RT-PCR and
real time
RTPCR
1 or 2
days
Antigen
detection
NS1 Ag rapid
tests Minutes
NS1 Ag ELISA 1 day
Immuno-
histochemistry 2-5 days
Serological
response
Paired sera
(acute serum
from1–5 days
and second
serum 15–21
days after)
IgM or IgG
seroconversion
ELISA
HIA 1–2 days
Neutralization
Test
Minimum
7 days
Serum after day
5 of fever
IgM detection
(recent
infection)
ELISA 1 or 2
days
Rapid tests Minutes
IgG detection
IgG ELISA
HIA
1 or 2
days
ELISA = enzyme-linked immunosorbent assay; HIA = haemagglutination
inhibition assay; IgG = immunoglobulinG; IgM = immunoglobulin M;
NS1 Ag = non-structural protein 1 antigen; RT-PCR = reverse transcriptase
polymerase chain reaction
21
Dengue viruses are RNA viruses belonging to the family
flaviviridae, genus flavivirus. The four dengue viruses (DEN-[1–4]) are
serologically related but antigenically and genetically distinctive 13.
Three main aspects should be considered for an adequate dengue
diagnosis:
● virological and serological markers in relation to the time of dengue
infection;
● type of diagnostic method in relation to clinical illness;
● characteristics of the clinical samples.
Virological and serological markers in relation to time of dengue
infection
An incubation period of 4–10 days occurs after the mosquito bites,
resulting in an asymptomatic or symptomatic dengue infection. During this
period the virus replicates and an antibody response is developed. In
general, viraemia is detectable in most dengue cases at the same time that
symptoms appear, and is no longer detectable at the time of defervescence.
The development of IgM antibody is coincident with the disappearance of
fever and viraemia. Virological and serological markers differ in time
evolution and titre response and according to whether the infection is
primary or secondary.
22
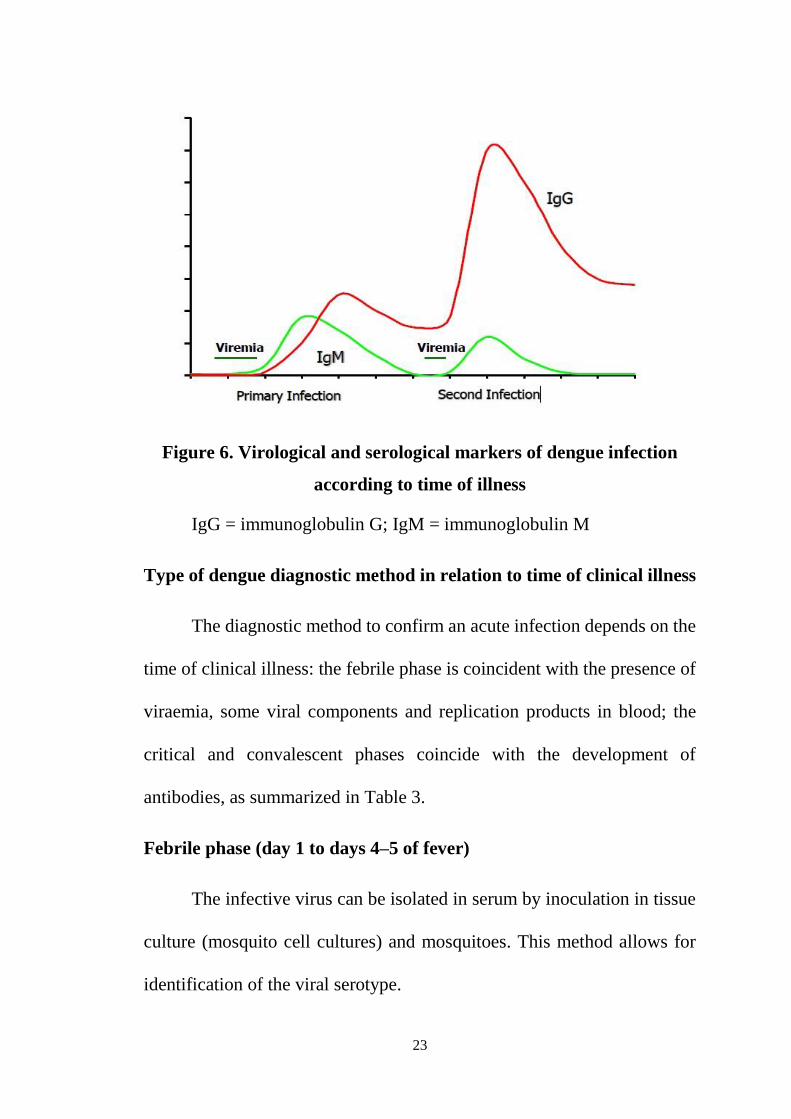
In a primary infection (i.e. when an individual is infected for the first
time with a flavivirus), viraemia develops from 1–2 days before the onset
of fever until 4–5 days after. Accordingly, anti-dengue IgM specific
antibodies can be detected 3−6 days after fever onset. On average, IgM is
detected in 50% of cases by days 3–5 after the onset of illness, this figure
increasing to 95–98% for days 6−10. Low levels of IgM are still detectable
around one to three months after fever. In addition, the primary infection
is characterized by slowly increasing but low levels of dengue-specific
IgG, becoming elevated at days 9−10. Low IgG levels persist for decades,
an indication of a past dengue infection. A totally different picture is
observed during a secondary infection, with a rapid and higher increase of
anti-dengue specific IgG antibodies and slower and lower levels of IgM.
High IgG levels remain for 30–40 days. A short-lasting but higher viraemia
level characterizes the secondary infection compared to the primary
infection.
23
Figure 6. Virological and serological markers of dengue infection
according to time of illness
IgG = immunoglobulin G; IgM = immunoglobulin M
Type of dengue diagnostic method in relation to time of clinical illness
The diagnostic method to confirm an acute infection depends on the
time of clinical illness: the febrile phase is coincident with the presence of
viraemia, some viral components and replication products in blood; the
critical and convalescent phases coincide with the development of
antibodies, as summarized in Table 3.
Febrile phase (day 1 to days 4–5 of fever)
The infective virus can be isolated in serum by inoculation in tissue
culture (mosquito cell cultures) and mosquitoes. This method allows for
identification of the viral serotype.
24
Virus genome detection using reverse transcriptase polymerase
chain reaction (RT-PCR) and real-time RT-PCR confirms an acute dengue
infection. Both methods have a high sensitivity and allow serotype
identification and quantification of genome copies. Some studies suggest
the presence of a higher number of copies in severe dengue cases.
NS1 Ag is a marker of acute dengue infection. Both enzyme-linked
immunosorbent assay (ELISA) and rapid commercial tests are available for
NS1 Ag detection. The sensitivity and specificity of commercial kits in
different serotype infections and days of illness are being evaluated.14
Critical and convalescent phases (after days 4–5 of illness)
Specific IgM is the best marker of a recent dengue infection. MAC-
ELISA and rapid tests are the most frequent methods for IgM detection;
however a recent evaluation of four rapid tests demonstrated a low
sensitivity. In addition to IgM, high levels of specific IgG in sera collected
early after fever onset as detected by ELISA and haemagglutination
inhibition assay (HIA) also suggest a recent dengue infection.
Primary infections are characterized by high levels of IgM and low
levels of IgG, while low levels of IgM with high levels of IgG characterize
secondary infections.
25
A single serum sample collected after day 5 of fever onset is useful
for IgM determination. Depending on the IgG level in the sample,
classification into primary or secondary infection can also be determined
using the IgM/IgG optical density ratio. Ratios greater than 1.2 (using the
patient’s sera at 1/100 serum dilution) or 1.4 (using serum dilution of 1/20)
suggest a primary infection. In addition, IgG titres higher than 1/1280 by
HIA or ELISA are also suggestive of a secondary infection.
As IgM antibodies persist for almost three months after fever onset,
the detection in samples collected late after the acute phase of illness
suggests a recent infection. In dengue endemic countries, acute clinical
cases with a positive IgM are classified as probable dengue cases.
The study of paired sera (acute and convalescent serum samples with
the second sample being collected 15–21 days after the first sample),
allows for serological confirmation of dengue infection. The diagnosis
depends upon the demonstration of rising titres of dengue antibodies
between acute and convalescent sera
A broad cross-reactivity of ELISA and HIA with other flaviviruses
has been observed. Neutralization Test is the method of choice for
determination of specific serotype15.
26
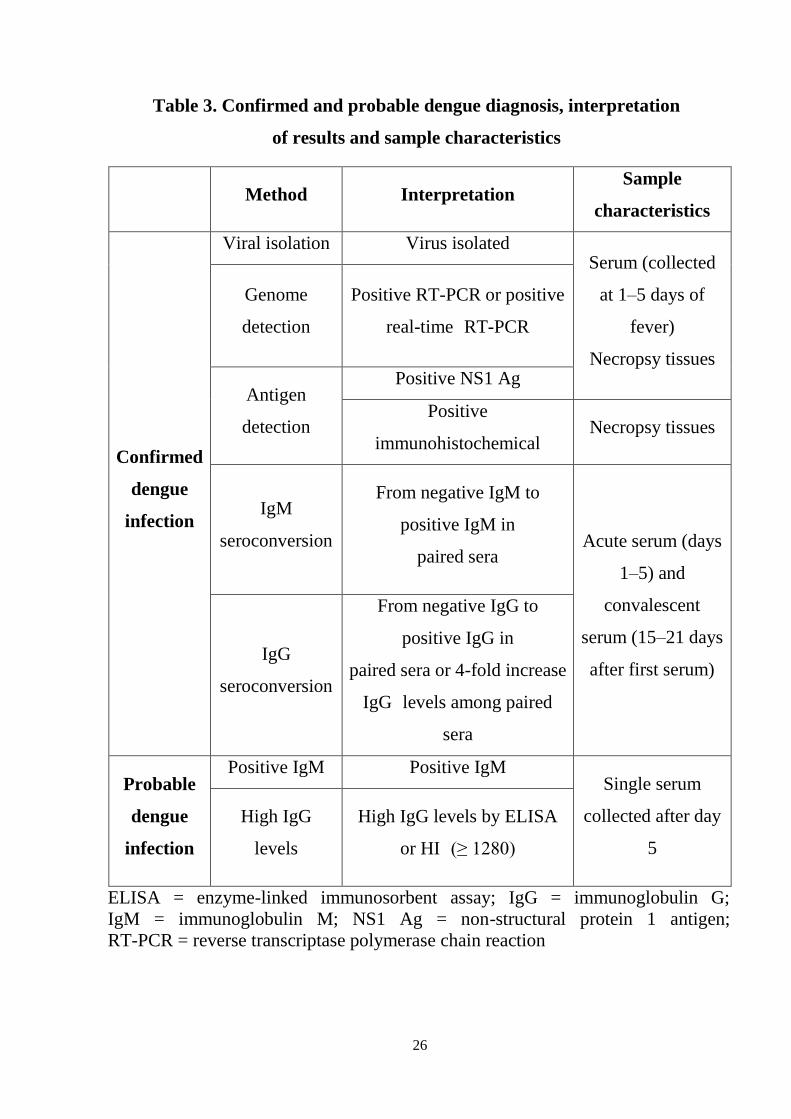
Table 3. Confirmed and probable dengue diagnosis, interpretation
of results and sample characteristics
Method Interpretation Sample
characteristics
Confirmed
dengue
infection
Viral isolation Virus isolated Serum (collected
at 1–5 days of
fever)
Necropsy tissues
Genome
detection
Positive RT-PCR or positive
real-time RT-PCR
Antigen
detection
Positive NS1 Ag
Positive
immunohistochemical Necropsy tissues
IgM
seroconversion
From negative IgM to
positive IgM in
paired sera Acute serum (days
1–5) and convalescent
serum (15–21 days
after first serum) IgG
seroconversion
From negative IgG to
positive IgG in
paired sera or 4-fold increase
IgG levels among paired
sera
Probable
dengue
infection
Positive IgM Positive IgM Single serum
collected after day
5
High IgG
levels
High IgG levels by ELISA
or HI (≥ 1280)
ELISA = enzyme-linked immunosorbent assay; IgG = immunoglobulin G; IgM = immunoglobulin M; NS1 Ag = non-structural protein 1 antigen; RT-PCR = reverse transcriptase polymerase chain reaction
27
TREATMENT OF DENGUE FEVER
Supportive therapy is the mainstay of treatment. Increased oral fluid
intake is recommended to prevent dehydration. Supplementation with IV
fluids may be necessary to prevent dehydration and significant hemo
concentration. But unnecessary iv fluid without dehydration may lead to
fluid overload. Fever is managed with paracetamol and tepid sponging.
Aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDS) should
be avoided as these drugs may worsen the bleeding tendency associated
with some of these infections. Shock is managed with isotonic fluids.
Packed cell (PRBC) transfusion is indicated in refractory shock or if there
is significant bleeding.
Patients with known or suspected dengue fever should have their
platelet count and hematocrit measured daily from the third day of illness
until 1-2 days after defervescence. Patients with a rising Hct level or falling
platelet count should be monitored more frequently.
Management of dengue illness can be discussed in three steps:
Step 1: Overall assessment of signs and symptoms
Step 2: Diagnosis and severity assessment
Step 3: Categorizing the patients into mild, moderate or severe
dengue and treating accordingly.
28
Overall Assessment
History and Examination
Emphasis on history should be on assessment of warning signs.
Physical examination should concentrate on hemodynamic assessment, to
determine the presence and extent of shock, confirming or finding the new
warning signs, and checking for bleeding and shock manifestations,
abdominal tenderness, mental state, and hydration. Tourniquet test should
be done compulsorily.
Investigations
Initial investigations should include Hematocrit, WBC count,
platelet count and tests to confirm the diagnosis, as described in the sec.
Laboratory diagnosis. In critical phase, additional tests need to be and
include liver function test, renal function test, chest X-ray, serum
electrolytes, ultrasound abdomen and neuroimaging as necessary.
Diagnosis and Severity Assessment
Determine the phase of disease (febrile, critical, and recovery) and
severity (non-severe, severe) of dengue, as per criteria explained earlier.
The child will need admission if any of the following criteria is fulfilled.
● Presence of any of warning signs
● Bleeding from any site.
29
● Signs and symptoms suggestive of hypotension
● Renal, hepatic, or/and central nervous system (CNS) involvement
● Pleural effusion or pericardial effusion, ascites
● Rising Hematocrit
● Platelet countless than 50,000/mm3
● High-risk age group-infants and old age
Categorize Patients in Mild, Moderate, and Severe Dengue (Table 2)
This step is aimed to place the patient in an appropriate Group (mild,
moderate and severe) to decide on future course of treatment, which is as
follows:
● Mild: Patients, who may be sent home with advised to come for
follow up.
● Moderate: Patients needing continuous monitoring and
hospitalization
● Severe: Patients requiring tertiary level care.
Mild Dengue: Home Management
All children who are tolerating oral fluids, passing urine at least once
in 6 hr, and not having any of the warning signs can be sent home.
Following managements need to be advised:
30
Encourage fluid intake; can give oral rehydration salt (ORS), fresh
fruit juice, tender coconut, etc. The parents should be advised to increase
the amount of oral fluids in any form to be given (e.g. 3-10 kg: 100 ml/kg
and 10-20 kg: 75 ml/kg) Paracetamol (15 mg/kg/dose) if the child is
uncomfortable because of fever once in six hours if required. Avoid aspirin,
ibuprofen, mefenamic acid, nimesulide and other NSAIDS.
Monitor at home for fluid intake, urine output, fever, obvious
bleeding, and altered sensorium. Bring back if any of the above is present
or the child develops any of the warning signs.
Parents of infants should be explained the danger signs before
sending them home. Tepid sponging for fever may be done as febrile
convulsions may occur commonly in this age group. Breastfeeding should
be encouraged and continued.
Moderate Dengue:
Close Monitoring and Hospital Management is needed. Any patient
who fulfill the admission criteria should be admitted and monitered (as
mentioned above). They may or may not have warning signs. A baseline
Hematocrit is measured and continuous monitoring is started. In cases
where no warning signs are there, patients should be started on
maintenance fluids with isotonic fluid. If patient shows signs of mild
dehydration, a correction of 50 mL/kg (<12 months) and 30 ml/kg (>12
31
months) is added to maintainence fluid. At all the times clinical parameters
are monitored closely and correlated with Hematocrit to guide further fluid
therapy. For those who present with warning signs, the following is
advised.
• Start isotonic IV fluids (normal saline or Ringer's lactate) at 6
ml/kg/hr for 1-2hr
• Reassess Hematocrit and clinical status:
• If improvement occurs, decrease to 3 ml/kg/hr for 2-4 h, and then
continue with 1.5 ml/kg/hr for 2-4 hr,
• If clinical status worsens or Hematocrit rises, increase rate of fluids
to 10ml/kg/hr for 1-2 hr
• Reassess clinical status, repeat Hematocrit, and review fluid
infusion rates, till the child is better
• If the child improves, maintain minimum IV fluids at 1 ml/kg/hr
for 24-48 hr. Stop fluids when child demands and accepts adequate oral
fluids, and food along with adequate urine output.
• Those who worsen or develop profound shock bleeding or
multisystem involvement manage as severe dengue.
32
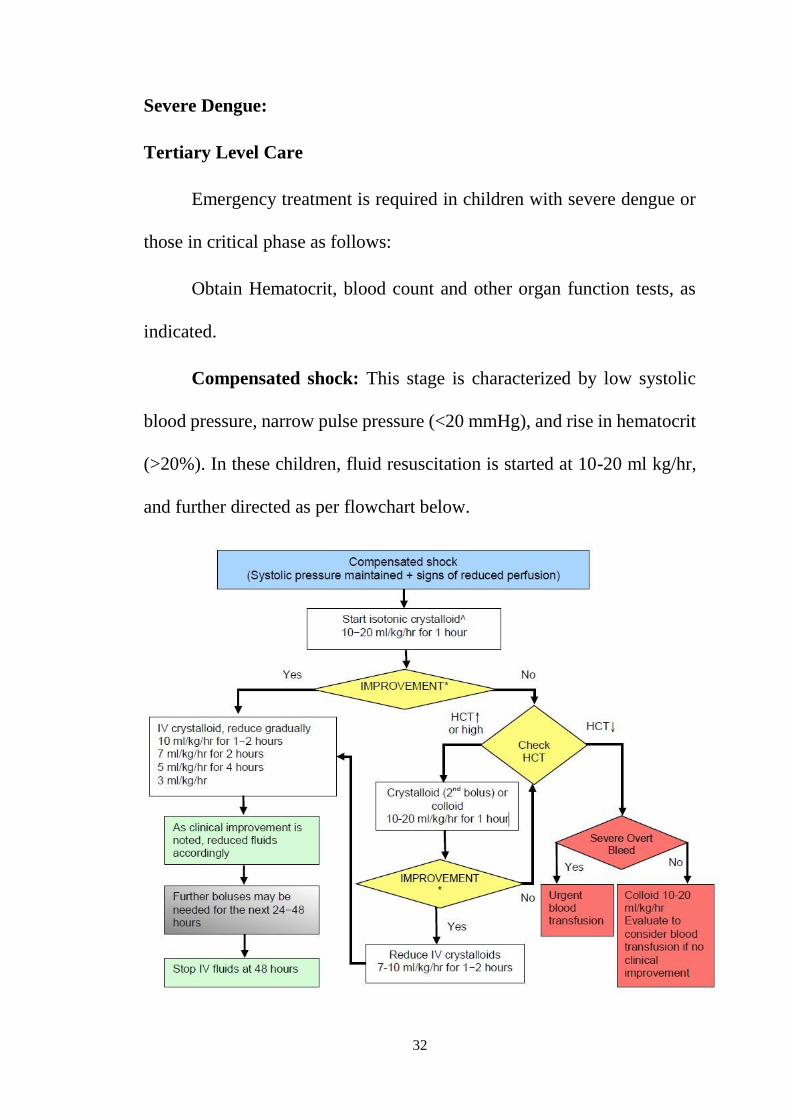
Severe Dengue:
Tertiary Level Care
Emergency treatment is required in children with severe dengue or
those in critical phase as follows:
Obtain Hematocrit, blood count and other organ function tests, as
indicated.
Compensated shock: This stage is characterized by low systolic
blood pressure, narrow pulse pressure (<20 mmHg), and rise in hematocrit
(>20%). In these children, fluid resuscitation is started at 10-20 ml kg/hr,
and further directed as per flowchart below.
33
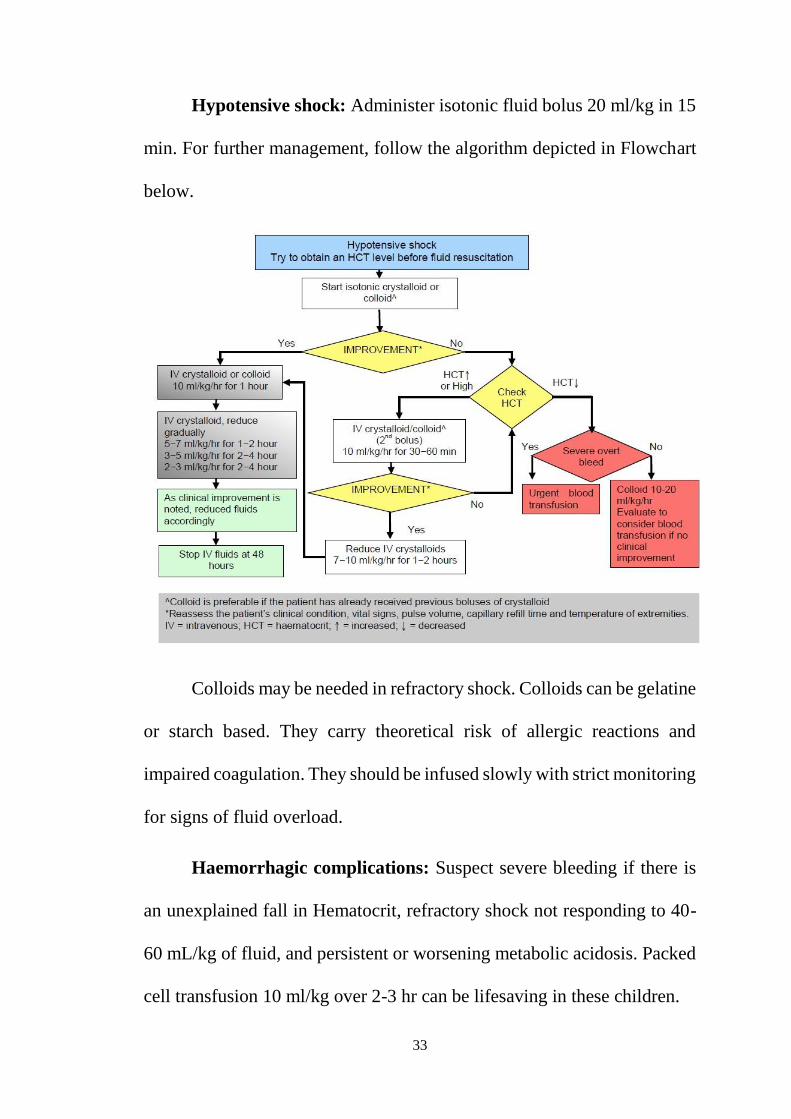
Hypotensive shock: Administer isotonic fluid bolus 20 ml/kg in 15
min. For further management, follow the algorithm depicted in Flowchart
below.
Colloids may be needed in refractory shock. Colloids can be gelatine
or starch based. They carry theoretical risk of allergic reactions and
impaired coagulation. They should be infused slowly with strict monitoring
for signs of fluid overload.
Haemorrhagic complications: Suspect severe bleeding if there is
an unexplained fall in Hematocrit, refractory shock not responding to 40-
60 mL/kg of fluid, and persistent or worsening metabolic acidosis. Packed
cell transfusion 10 ml/kg over 2-3 hr can be lifesaving in these children.
34
There is not much evidence for platelet transfusion or fresh frozen
plasma (FFP) for severe bleeding. Platelet transfusions should not be used
prophylactically. Its use has neither shown to prevent progression to severe
bleeding nor does it shorten the bleeding time, but may be associated with
severe side effects. Platelet transfusion should be restricted to cases with
severe bleeding or when platelet counts are below 10,000/mm3. Platelets
obtained by single donor apheresis are preferred as they raise the platelet
count by 30,000-50,000 as compared to random donor platelets which
result in rise by 5,000-10,000 per unit.
Monitoring: This essentially remains the basic prerequisite for
treating children with severe dengue, in an emergency setting
• Monitor vital signs and peripheral perfusion, urine output 1-4
hourly till patient is out of critical phase. Monitor Hematocrit before and
after fluid replacement, then 6-12 hourly.
• Monitor blood glucose and other organ dysfunction both clinically
and biochemically.
• A typical monitoring chart for dengue fever should record the
following: body temperature, heart rate, BP, pulse volume, capillary refill
time, abdominal pain, appetite, abdominal pain, vomiting, bleeding, and
sensorium.
35
Treatment of Fluid Overload
A child with dengue can have fluid overload due to excessive or
rapidly transfused IV fluids, use of hypotonic fluids, and inappropriate use
of fresh frozen plasma (FFP) or platelets. Another important reason is
continuation of IV fluids even during the phase of plasma reabsorption and
recovery phase.
These children may present with features of respiratory distress,
pulmonary edema or congestive heart failure.
Following management is suggested:
● Oxygen therapy
● Discontinuation of IV fluids
● Frusemide 0.1-0.5 mg/kg/dose once or twice daily
● Correction of electrolyte imbalance
● Look for occult hemorrhage and transfuse packed cells (PRBC)
Management of Other Complications
Encephalopathy in dengue may result due to dengue encephalitis,
intracranial bleeding, electrolyte disturbances, occlusion due to DIVC or
hepatic failure (hepatic encephalopathy). Appropriate diagnosis for cause
and specific management should be instituted. Cardiac involvement may

36
be seen during shock or during convalescence, which may manifest as
arrhythmias or heart failure.
Criteria for Discharge
Patient should be discharged only if he has been
Afebrile for at least 48 hours
Passing urine normally and adequately
Having improved appetite
And has no respiratory distress
Laboratory parameters should show a stable Hematocrit and platelet
count of more than 50,000/mm3 and in rising trend.
37
VACCINES FOR DENGUE
A live attenuated tetravalent dengue vaccine (CYD-TDV) has been
developed which contains four dengue virus with expression of dengue pre
membrane and envelope protein and non-structural and capsid protein of
yellow fever strain (YF-17D)
Dosage : 3 dose schedule against serotypes 1,3 and 4
The vaccine is still under multicentric phase III trials.
The Chimeri Vax TM system, originally developed to construct JE
vaccine, has now been applied to dengue viruses. This vaccine was shown
to be safe and immunogenic in a monkey study.
38
AIM AND OBJECTIVES
To find out whether Serum Ferritin level during the febrile phase of
dengue fever can be used as a predictor of complications.
39
REVIEW OF LITERATURE
Chaiyaratana w. et al (2008)16, 172 children with dengue infection
between 2002 to 2005 were included in their study. Their study showed
median duration of febrile period is 5 days. Their data showed that both
patients with DF and DHF had higher serum ferritin levels during the
febrile, toxic and convalescent stages than they did at follow-up. Patients
with DHF had higher levels of serum ferritin than those with DF
throughout the course of the illness. Those with DHF grades III and IV had
higher serum ferritin levels than those with DF and DHF grades I and II.
Cornelia A.M.Van de wag (2014), conducted a study on the
carribean island aruba, during the epidemic between sep 2011 to april 2012.
It stated that ferritin can be used as a clinical marker to discriminate
between dengue and other febrile illnesses. The occurrence of
hyperferritinaemia in dengue virus infected patients is indicative for highly
active disease resulting in immune activation and coagulation disturbances.
Therefore, they recommended that patients with hyperferritinaemia should
be monitered carefully, as there is a high risk for them to develop severe
disease.
R.Soundravally et al (2014)17, conducted a study on 96 patients
with dengue fever and other febrile illness. A steady increase in the level
of serum ferritin was recorded throughout the course of illness. The
40
elevated ferritin level could predict the disease severity with highest
sensitivity and specificity of 76.9 and 83.3 %, respectively, on the day of
admission and the same was found to be 90 and 91.6% around
defervescence. On the basis on its diagnostic efficiency, they proposed that
ferritin may serve as a potential biomarker for an early prediction of disease
severity.
Muhammed Nadeem et al (2016)18, conducted a study on 104
patients with dengue infection. In that study they concluded 1. Raised
serum ferritin levels are significantly associated with severe dengue. Mean
ferritin levels are also high in patients with severe dengue as compared to
dengue fever. 2. Serum ferritin levels on the day of admission may serve
as biomarker for an early prediction of disease severity in dengue virus
infection.
Soumyabatra Roy Chaudri et al (2017)19 conducted a study on 358
cases of serological proven cases and selected only 30 cases of confirmed
dengue and compared them with other febrile illness. Ferritin was
evaluated as an adjunct marker for the diagnosis of dengue which could
possibly aid their clinical judgment and prompt early fluid resuscitation
which in turn could be useful in avoiding undue complications. Ferritin, as
evaluated in the present study may serve as a significant marker for
differentiating between dengue fever and fever of other etiology, even in
the absence of a positive NS1 antigen or a positive IgM antibody for
dengue.
41
MATERIALS AND METHODS
STUDY POPULATION:
The study was conducted on 80 dengue patients admitted in
Institute of Child Health & Research Centre, Madurai during the study
period of 6 months from February 2019 to august 2019.
INCLUSION CRITERIA:
All fever cases which are dengue NS1 antigen positive or which
show classical signs and symptoms of dengue.
Children from 1 month to 12 years of age
EXCLUSION CRITERIA:
Patients who do not have serological evidence of NS1 positivity or
IgM antibody.
Patient with anemia (Hb <11g/dl) and transfusion dependent chronic
disease.
DATA COLLECTION:
A previously designed proforma was used to collect the
demographic and clinical details of the patients. All the patients
underwent detailed clinical evaluation and appropriate investigations
are noted.
42
STUDY PROTOCOL:
DESIGN OF STUDY:
Prospective study
PERIOD OF STUDY:
February 2019 to august 2019.
METHODOLOGY:
History was taken in detail and duration of fever and other
associated signs and symptoms noted. Necessary investigations were done.
Child was then followed throughout the clinical course of the disease.
LABORATORY INVESTIGATIONS:
Total count, Platelet count, serum ferritin, USG abdomen, LFT,
RFT, neuroimaging and other investigations if necessary.
SERUM FERRITIN ESTIMATION20
Ferritin is a globular protein found mainly in the liver, which can
store about 2250 iron (Fe3+) ions. The ferritin molecule consists of a
protein shell (Apoferritin) composed of heavy and light subunits, which
surrounds a crystalline core containing iron oxide and phosphate. Ferritin
is synthesized in the liver, spleen and numerous other body tissues, with
major concentrations found in the liver, spleen, bone marrow, and intestinal
mucosa. The ferritin levels measured have a direct correlation with the total
43
amount of iron stored in the body. If ferritin is high there is iron in excess,
which would be excreted in the stool. If ferritin is low there is a risk for
lack in iron, which sooner or later could lead to anaemia. In the setting of
anaemia, serum ferritin is the most sensitive lab test for iron deficiency
anaemia. In contrast, serum ferritin levels are normal or increased in
anemia associated with chronic disease. Elevated serum ferritin levels
have been observed in acute and chronic liver disease and lymphoid
malignancy (leukemia and Hodgkin lymphoma).
Ferritin is an acute-phase reactant, it is often elevated in the course
of disease.
In dengue serum ferritin is elevated because of macrophage
activation.
METHOD AND PRINCIPLE OF SERUM FERRITIN
ESTIMATION:
Immuno enzymatic colorimetric method for quantitative
determination of Ferritin concentration in human serum or plasma.
Ferritin ELISA test is based on simultaneous binding of human
Ferritin to two monoclonal antibodies, one immobilized on microwell
plates and the other conjugated with horseradish peroxidase (HRP). After
incubation the bound/free separation is performed by a simple solid-phase
washing. Then the enzyme HRP in the bound-fraction reacts with the
44
Substrate (H2O2) and the TMB Substrate and develops a blue colour that
changes into yellow when the Stop Solution (H2SO4) is added. The colour
intensity is proportional to the Ferritin concentration in the sample. The
Ferritin concentration in the sample is calculated based on a standard curve.
Typical reference interval
Children 1-9 years, 10-60 ng/ml
10-18 years male 10-300 ng/ml
10-18 years female 10-70 ng/ml
Men, 18 - 60 years: 30–400 ng/ml
Women, 18 - 60 years: 15‐150 ng/ml
Men and women, 60–90 years: 15–650 ng/ml
COLLABORATING DEPARTMENTS:
Department of Microbiology
Department of Biochemistry
Department of Radiology
ETHICAL CLEARANCE: Clearance obtained
CONSENT: Individual written and informed consent obtained from the
parents of their children who were included in this study.
45
STATISTICAL ANALYSIS:
All data were entered in Excel 2007 and statistical analysis was
performed using the statistical software SPSS 1.6.0. Data were
expressed as frequency (with percentages), median values (with range
(min, max). For continuous variables, Mann Whitney U-test was
performed to find the differences between two groups and for
categorical variables Pearson’s chi-square test was performed. Results
were defined as statistically significant when the P value (2-sided) was
less than 0.05.
46
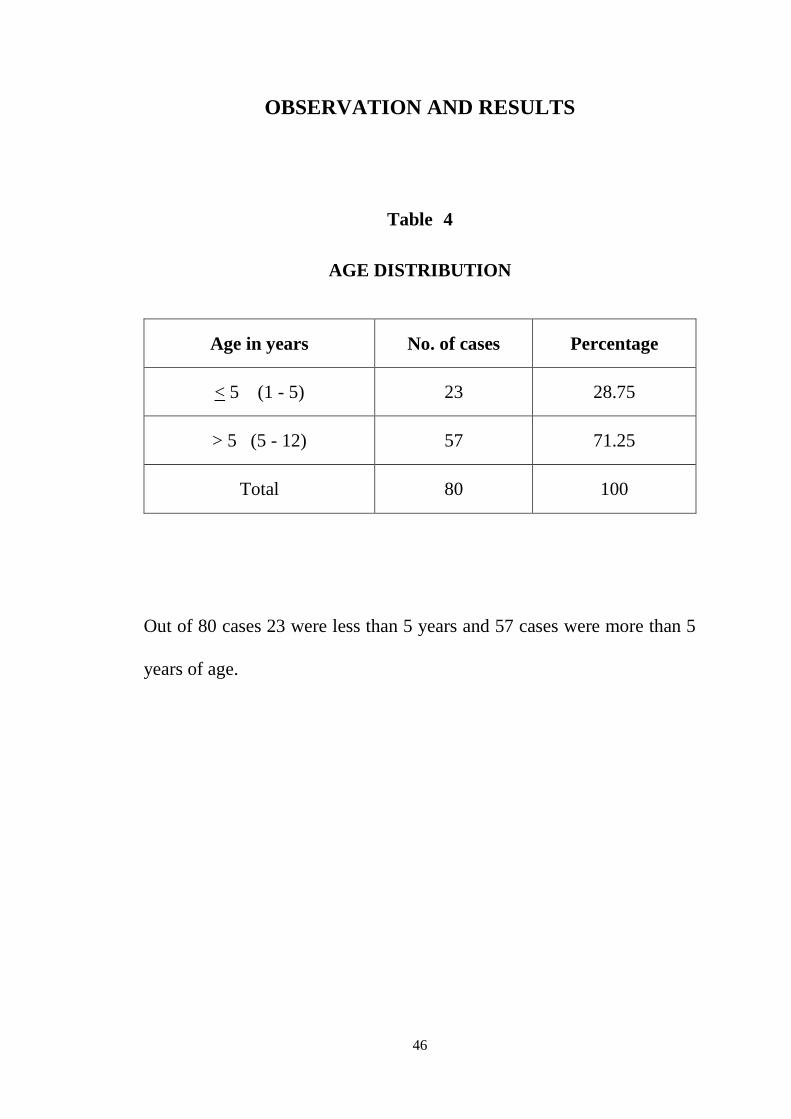
OBSERVATION AND RESULTS
Table 4
AGE DISTRIBUTION
Out of 80 cases 23 were less than 5 years and 57 cases were more than 5
years of age.
Age in years No. of cases Percentage
< 5 (1 - 5) 23 28.75
> 5 (5 - 12) 57 71.25
Total 80 100

47
Figure 7 - Age distribution
23
57
28.75
71.25
0
10
20
30
40
50
60
70
80
< 5 (1 - 5) > 5 (5.5 - 12)
AGE DISTRIBUTION
No.of cases Percentage
(5-12) 5
48
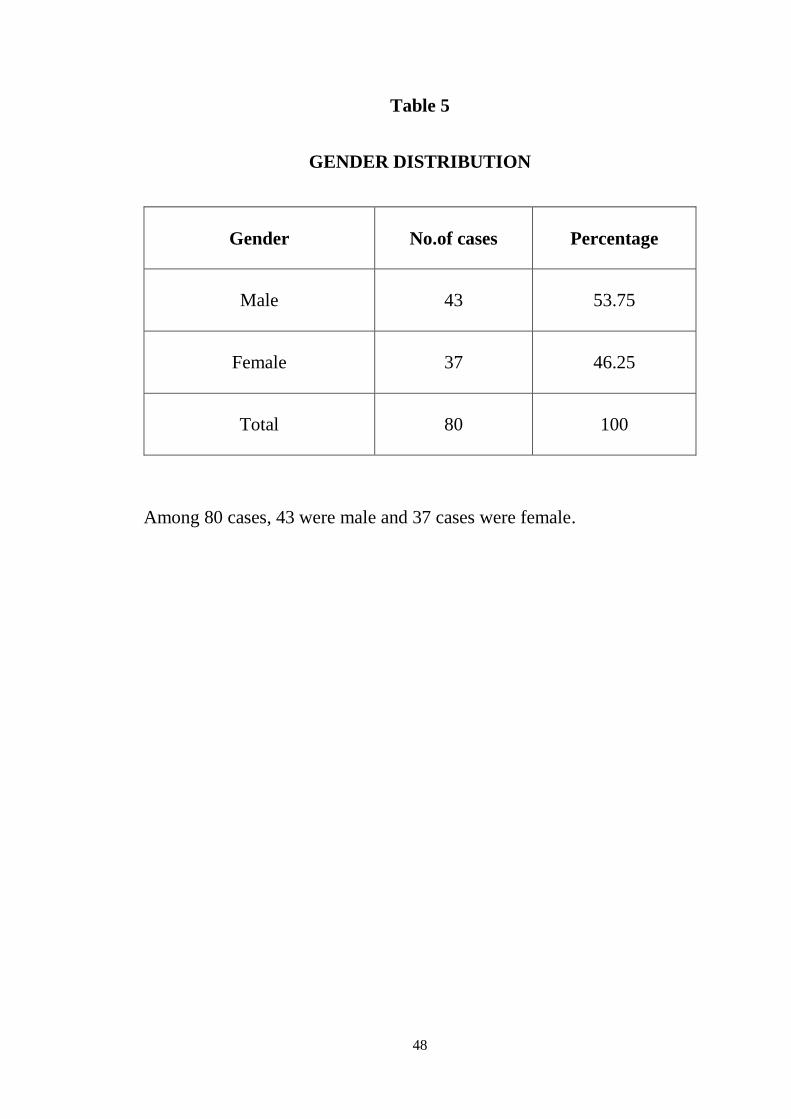
Table 5
GENDER DISTRIBUTION
Gender No.of cases Percentage
Male 43 53.75
Female 37 46.25
Total 80 100
Among 80 cases, 43 were male and 37 cases were female.
49
53.75
46.25
Figure 8 - Gender distribution
Male Female
50
Table 6
Age & Gender
Age in years Male Female
< 5 (1 - 5) 11 12
> 5 (5 - 12) 32 25
Total 43 37
51
0
5
10
15
20
25
30
35
< 5 (1 - 5) > 5 (5.5 - 12)
11
32
12
25
Figure 9 Age vs Gender
Male Female
(5-12) 5
52
Table 7
DENGUE CASE CLASSIFICATION
Out of 80 cases, 63 cases were non severe dengue and 17 were severe
dengue.
Dengue No. of cases Percentage
Non severe 63 78.75
Severe 17 21.25
Total 80 100
53
78.75
21.25
Figure 10 - Dengue Case Classification
Non severe Severe
54
Table 8
SEVERE DENGUE MANIFESTATIONS
Out of 17 severe dengue cases, 1 case had fluid accumulation with
respiratory distress, 11 cases had shock, 3 cases had bleeding, 2 cases had
organ involvement (1 case had liver involvement with elevated liver
enzymes and 1 other case had CNS involvement in the form of
encephalitis).
Complications No. of cases Percentage
Fluid Accumulation With
Respiratory Distress 1 1.25
Shock 11 13.75
Bleeding 3 3.75
Organ Involvement 2 2.5
55
0
2
4
6
8
10
12
FLUID
ACCUMULAT
ION WITH
RESPIRATOR
Y DISTRESS
SHOCK BLEEDING ORGAN
INVOLVEME
NT
No.of cases 1 11 3 2
1
11
3
2
Figure 11 - Severe Dengue Manifestations
No.of cases
56
Table 9
SERUM FERRITIN ON DAY 3 OF ILLNESS
Out of 80 cases, 5 cases had serum ferritin < 300, 54 cases had 301-600
cases, 8 cases had serum ferritin 601 - 800 and 13 cases had serum ferritin
levels >800.
Sr Ferritin Day 3
(ng/ml) No. of cases Percentage
< 300 5 6.25
301 - 600 54 67.5
601 - 800 8 10
> 800 13 16.25
Total 80 100
57
0
10
20
30
40
50
60
70
< 300 301 - 600 601 - 800 > 800
6.25
67.5
10
16.25
Figure 12 - SERUM FERRITIN - DAY 3
Percentage
(ng/ml)
58
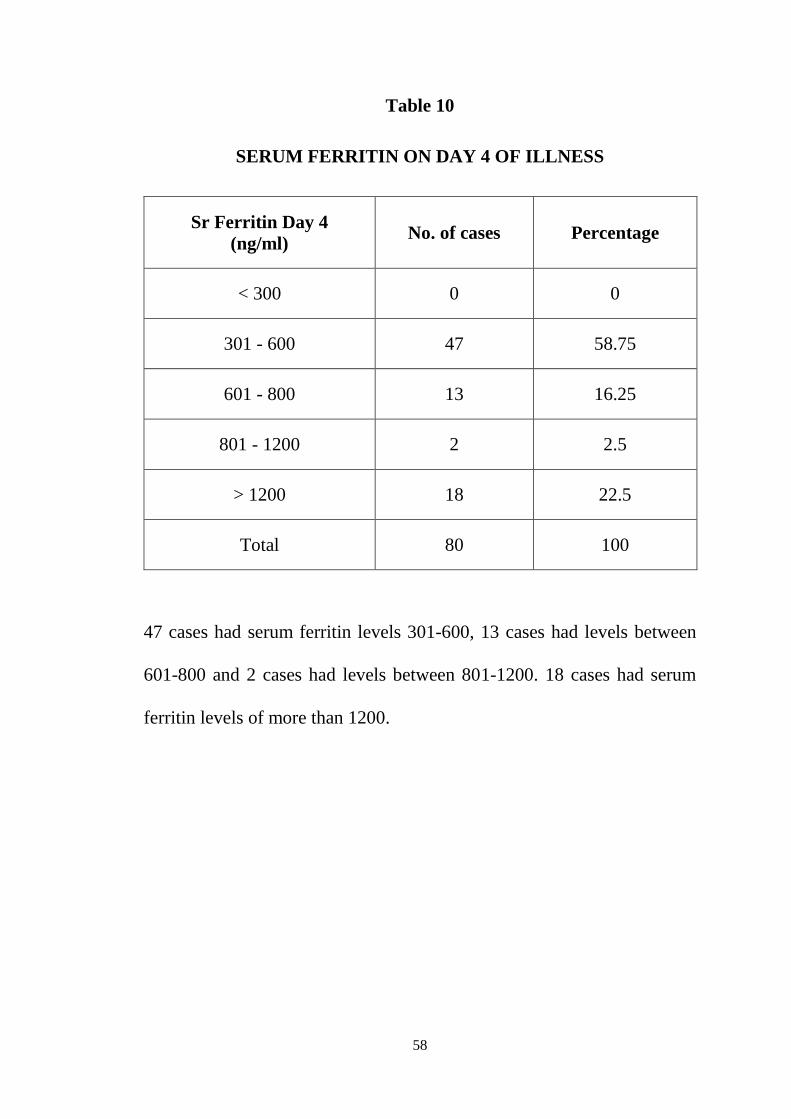
Table 10
SERUM FERRITIN ON DAY 4 OF ILLNESS
Sr Ferritin Day 4
(ng/ml) No. of cases Percentage
< 300 0 0
301 - 600 47 58.75
601 - 800 13 16.25
801 - 1200 2 2.5
> 1200 18 22.5
Total 80 100
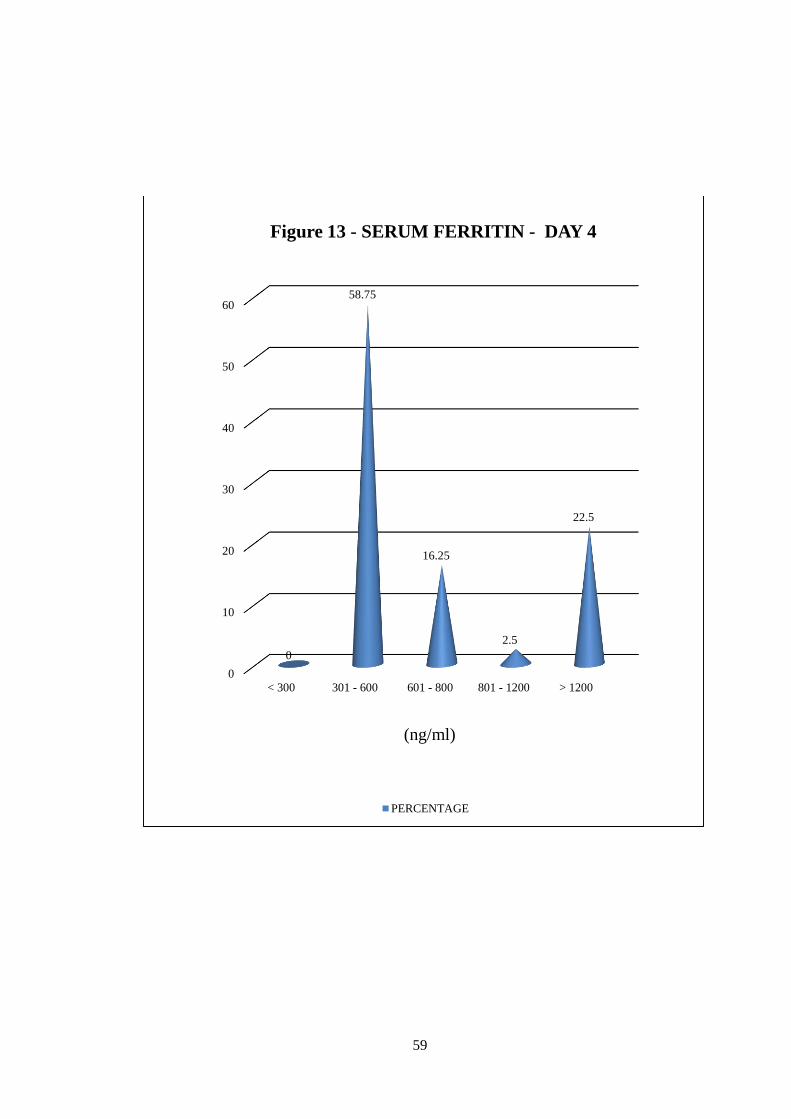
47 cases had serum ferritin levels 301-600, 13 cases had levels between
601-800 and 2 cases had levels between 801-1200. 18 cases had serum
ferritin levels of more than 1200.
59
0
10
20
30
40
50
60
< 300 301 - 600 601 - 800 801 - 1200 > 1200
0
58.75
16.25
2.5
22.5
Figure 13 - SERUM FERRITIN - DAY 4
PERCENTAGE
(ng/ml)
60
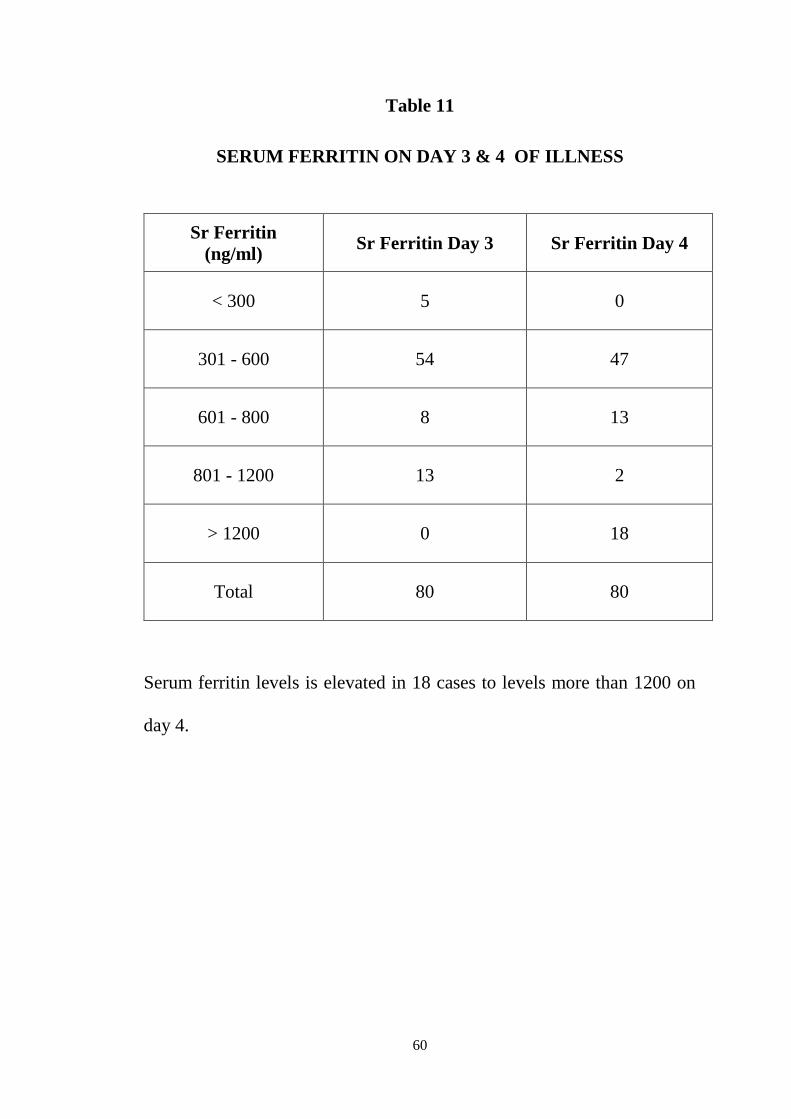
Table 11
SERUM FERRITIN ON DAY 3 & 4 OF ILLNESS
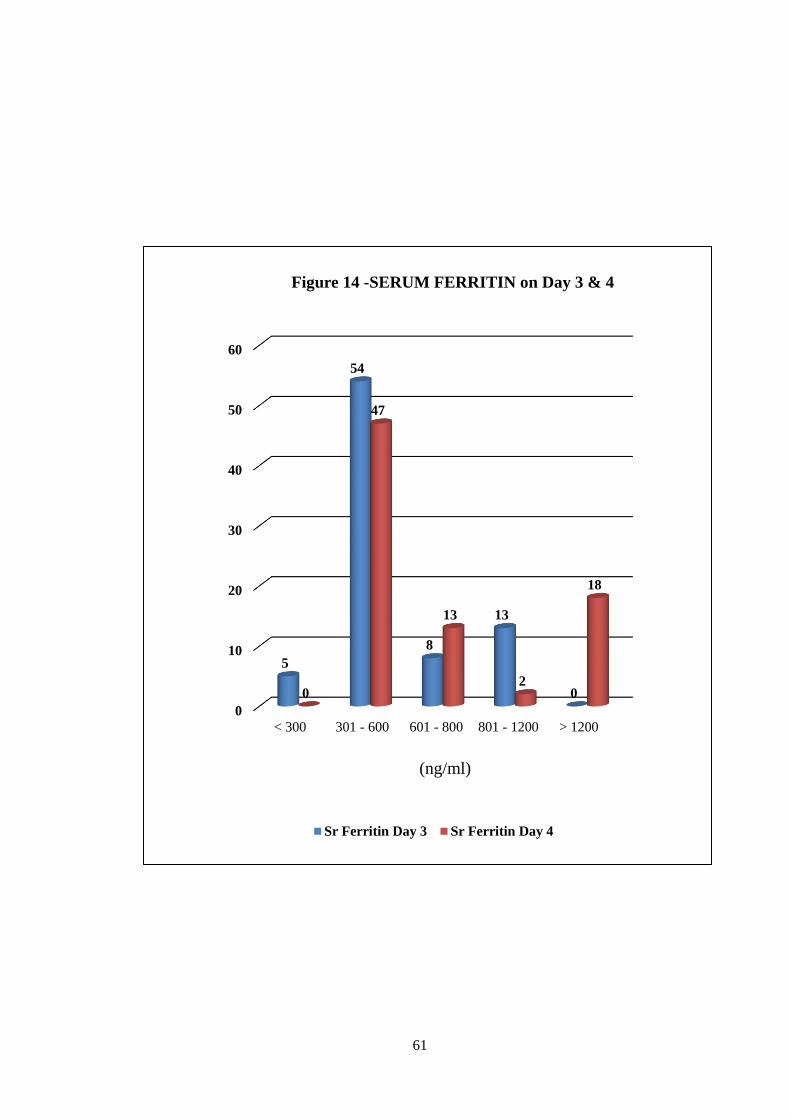
Serum ferritin levels is elevated in 18 cases to levels more than 1200 on
day 4.
Sr Ferritin
(ng/ml) Sr Ferritin Day 3 Sr Ferritin Day 4
< 300 5 0
301 - 600 54 47
601 - 800 8 13
801 - 1200 13 2
> 1200 0 18
Total 80 80
61
0
10
20
30
40
50
60
< 300 301 - 600 601 - 800 801 - 1200 > 1200
5
54
8
13
00
47
13
2
18
Figure 14 -SERUM FERRITIN on Day 3 & 4
Sr Ferritin Day 3 Sr Ferritin Day 4
(ng/ml)
62
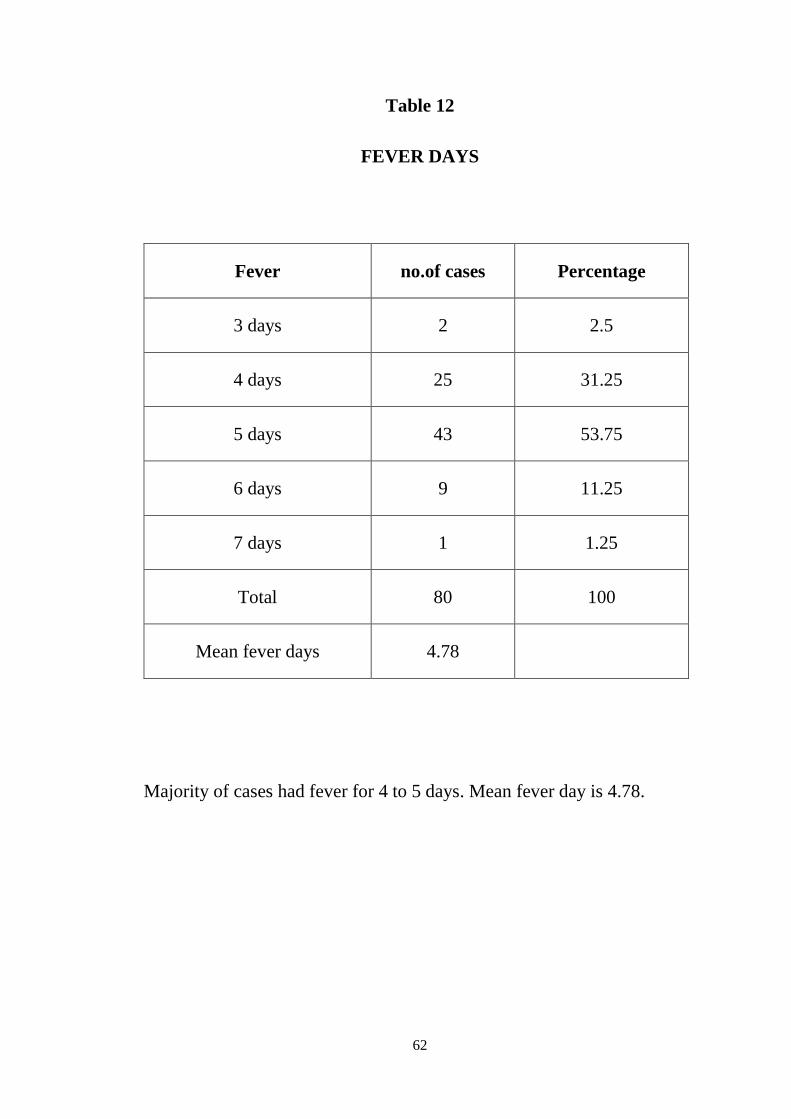
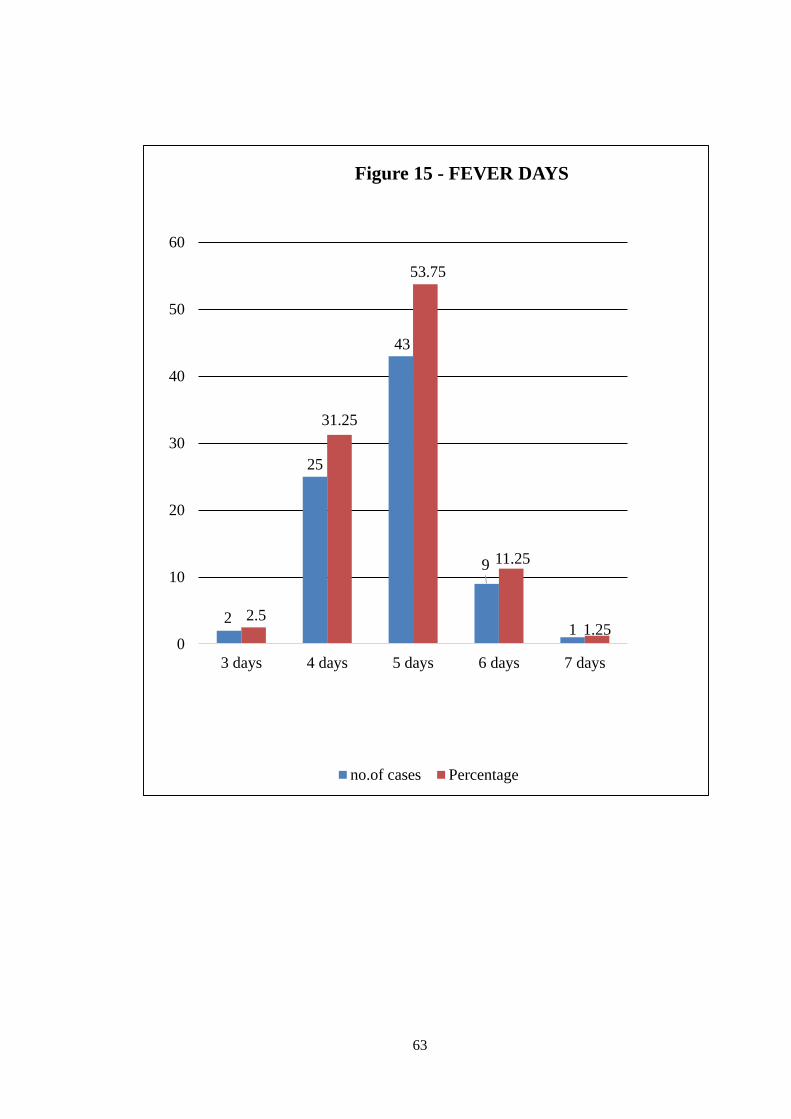
Table 12
FEVER DAYS
Majority of cases had fever for 4 to 5 days. Mean fever day is 4.78.
Fever no.of cases Percentage
3 days 2 2.5
4 days 25 31.25
5 days 43 53.75
6 days 9 11.25
7 days 1 1.25
Total 80 100
Mean fever days 4.78
63
2
25
43
9
12.5
31.25
53.75
11.25
1.250
10
20
30
40
50
60
3 days 4 days 5 days 6 days 7 days
Figure 15 - FEVER DAYS
no.of cases Percentage
64
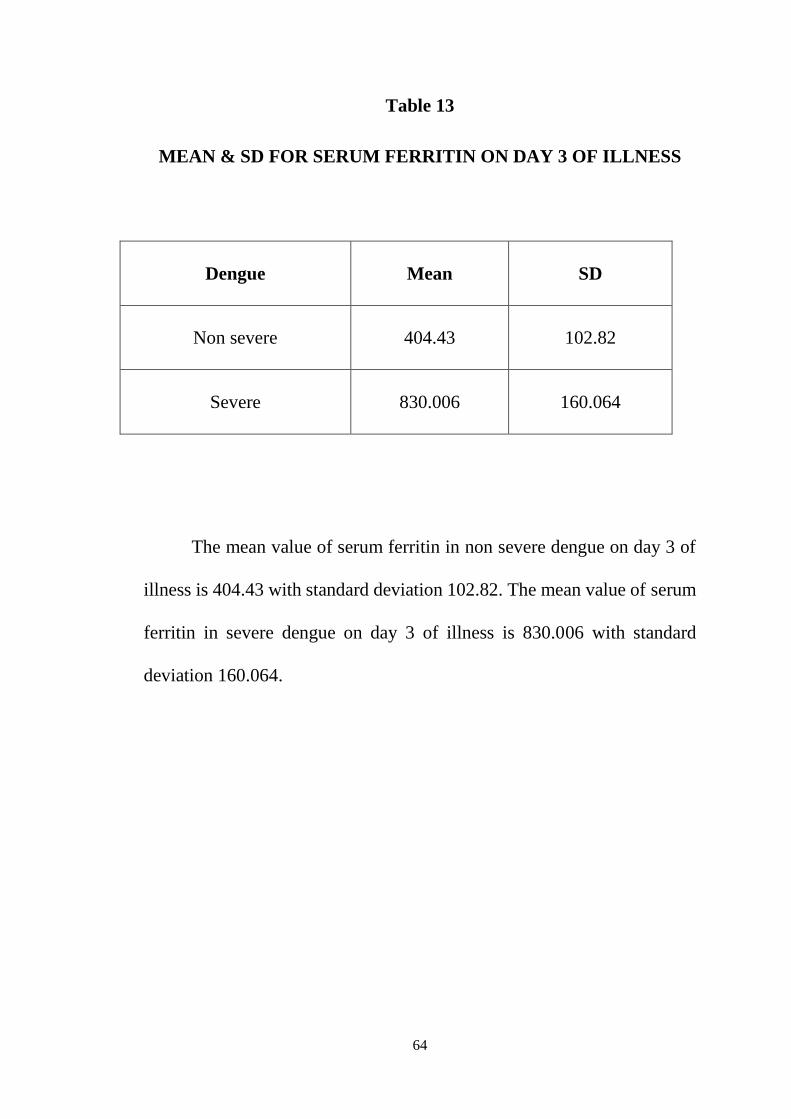
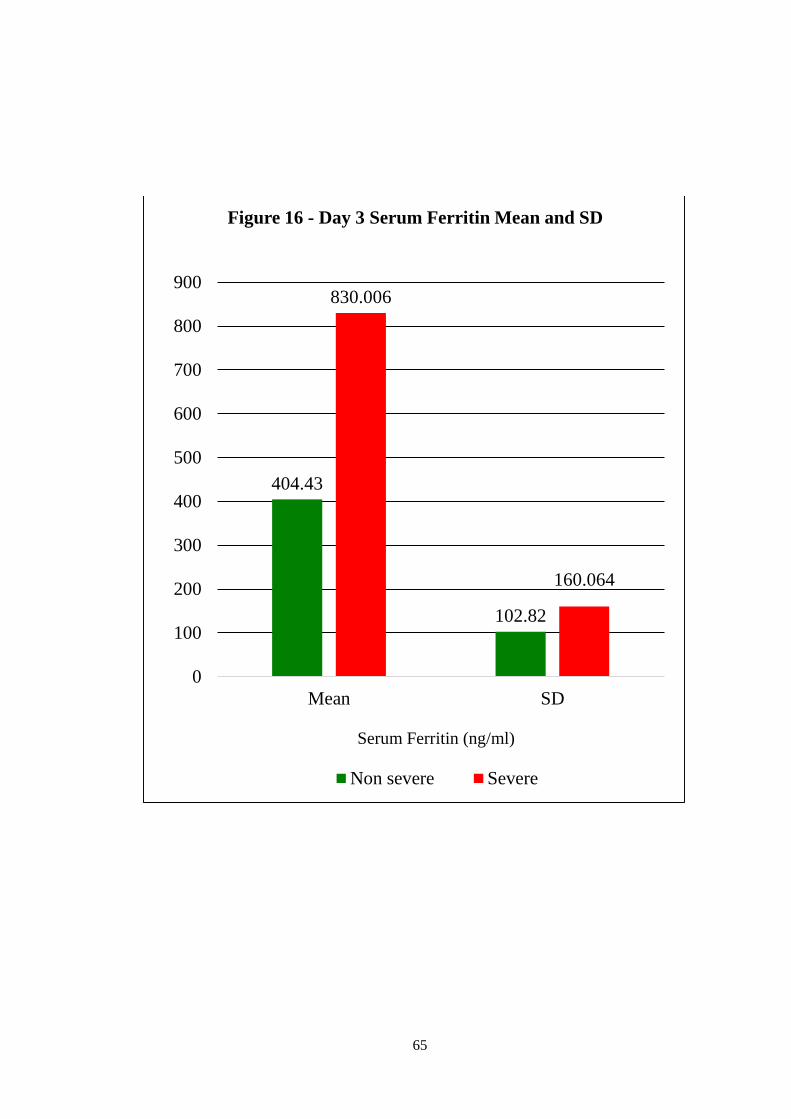
Table 13
MEAN & SD FOR SERUM FERRITIN ON DAY 3 OF ILLNESS
The mean value of serum ferritin in non severe dengue on day 3 of
illness is 404.43 with standard deviation 102.82. The mean value of serum
ferritin in severe dengue on day 3 of illness is 830.006 with standard
deviation 160.064.
Dengue Mean SD
Non severe 404.43 102.82
Severe 830.006 160.064
65
404.43
102.82
830.006
160.064
0
100
200
300
400
500
600
700
800
900
Mean SD
Figure 16 - Day 3 Serum Ferritin Mean and SD
Non severe Severe
Serum Ferritin (ng/ml)
66
Table 14
MEAN & SD FOR SERUM FERRITIN ON DAY 4 OF ILLNESS
Dengue Mean SD
Non severe 585.905 193.082
Severe 1259.824 192.461
The mean value of serum ferritin in non severe dengue on day 4 of illness
is 585.905 with standard deviation 193.082. The mean value of serum
ferritin in severe dengue on day 4 of illness is 1259.824 with standard
deviation 192.461.
67
585.905
193.082
1259.824
192.461
0
200
400
600
800
1000
1200
1400
Mean SD
Sr. Ferritin
Figure 17 - Day 4 Serum Ferritin Mean and SD
Non severe Severe
Serum Ferritin (ng/ml)
68
Table 15
CLINICAL DIAGNOSIS VS SERUM FERRITIN DAY 3
p value < 0.001 Significant
In severe dengue 12 cases out of 17 cases had serum ferritin levels of more
than 800 which is statistically significant compared to non severe cases
where only 1 had high ferritin levels.
Day 3 Ferritin > 800 (13)
(ng/ml)
Ferritin < 800 (67)
(ng/ml)
Severe dengue 12 5
Non severe dengue 1 62
69
12
5
1
62
0
10
20
30
40
50
60
70
Ferritin > 800 (13) Ferritin < 800 (67)
Figure 18 Clinical Diagnosis vs Serum Ferritin on Day 3
severe dengue non severe dengue
(ng/ml)
70
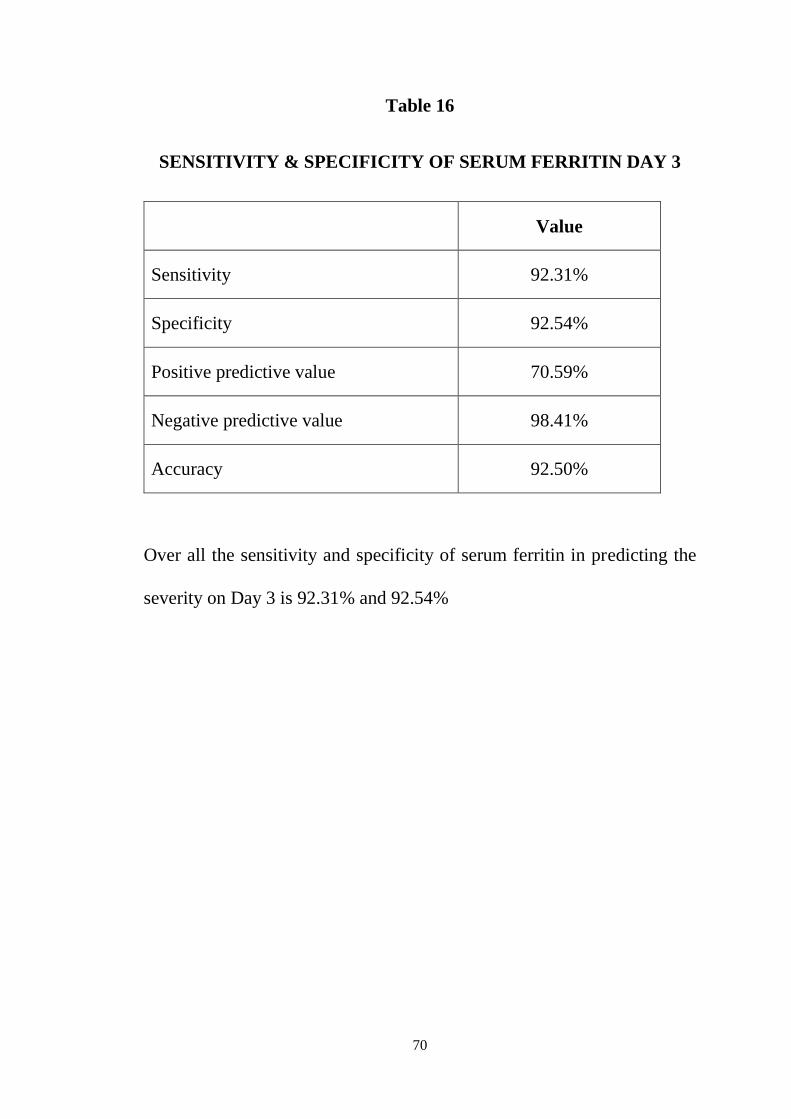
Table 16
SENSITIVITY & SPECIFICITY OF SERUM FERRITIN DAY 3
Value
Sensitivity 92.31%
Specificity 92.54%
Positive predictive value 70.59%
Negative predictive value 98.41%
Accuracy 92.50%
Over all the sensitivity and specificity of serum ferritin in predicting the
severity on Day 3 is 92.31% and 92.54%
71
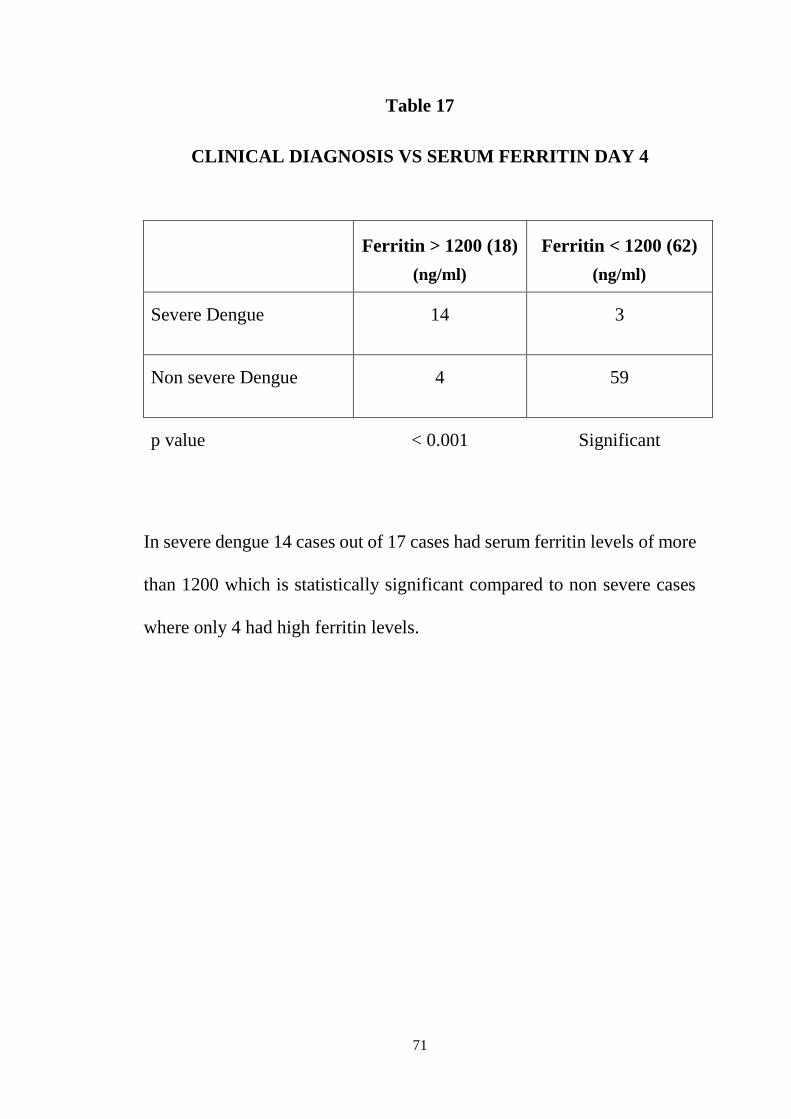
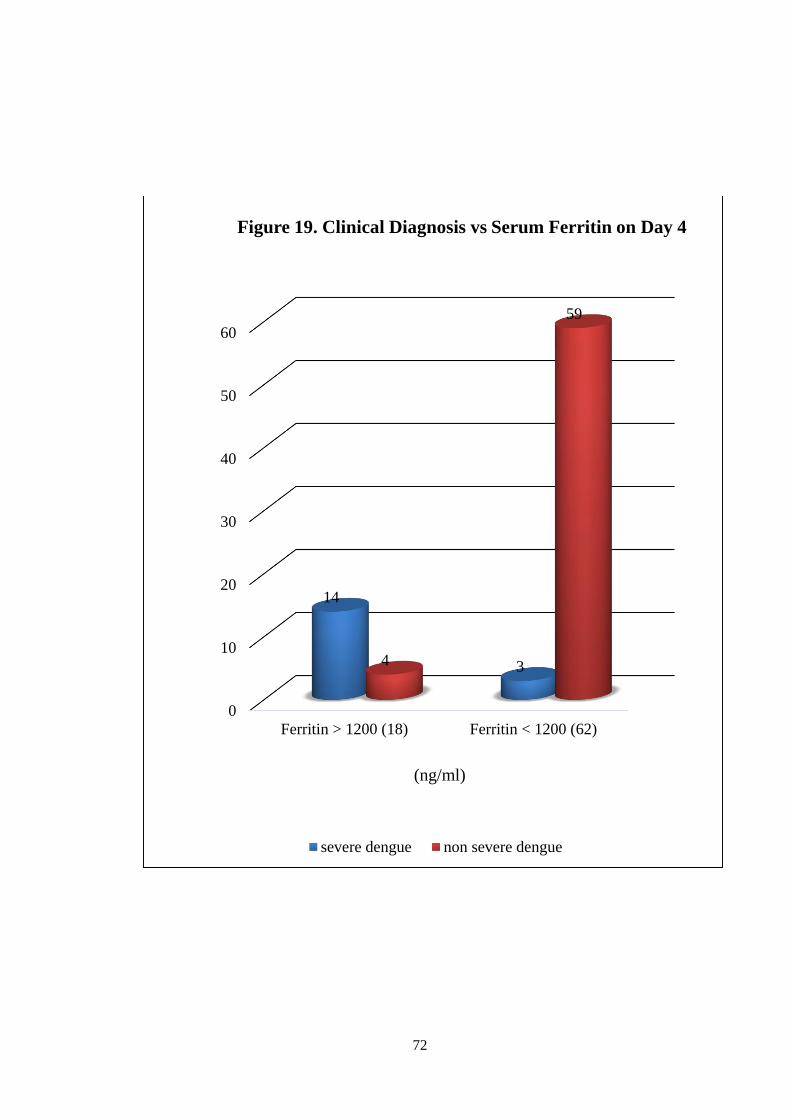
Table 17
CLINICAL DIAGNOSIS VS SERUM FERRITIN DAY 4
In severe dengue 14 cases out of 17 cases had serum ferritin levels of more
than 1200 which is statistically significant compared to non severe cases
where only 4 had high ferritin levels.
Ferritin > 1200 (18)
(ng/ml)
Ferritin < 1200 (62)
(ng/ml)
Severe Dengue 14 3
Non severe Dengue 4 59
p value < 0.001 Significant
72
0
10
20
30
40
50
60
Ferritin > 1200 (18) Ferritin < 1200 (62)
14
34
59
Figure 19. Clinical Diagnosis vs Serum Ferritin on Day 4
severe dengue non severe dengue
(ng/ml)
73
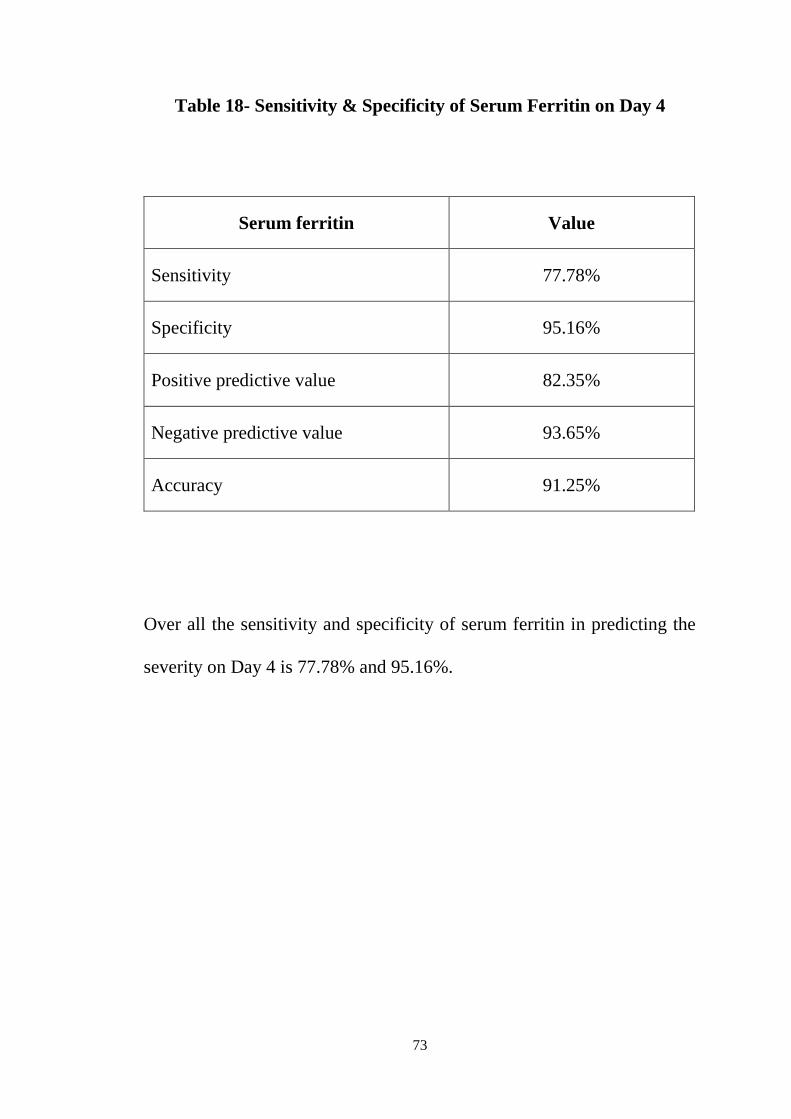
Table 18- Sensitivity & Specificity of Serum Ferritin on Day 4
Serum ferritin Value
Sensitivity 77.78%
Specificity 95.16%
Positive predictive value 82.35%
Negative predictive value 93.65%
Accuracy 91.25%
Over all the sensitivity and specificity of serum ferritin in predicting the
severity on Day 4 is 77.78% and 95.16%.
74
DISCUSSION
Dengue hemorrhagic fever (DHF) and dengue shock syndrome
(DSS) causes more mortality if not diagnosed earlier and treated promptly.
Many studies are available in adult patients to predict the severity but very
few studies are available in pediatric patients to predict the severity.
Our study was done to co-relate the elevation in serum ferritin in
dengue patients during febrile phase with severity of the disease during
critical period. By predicting the severity earlier, we can improve the
outcome and can decrease the mortality.
Among the 80 dengue cases, 43 cases were male children and 37
cases were female children. (Table 5)
In gender predilection, male children were affected mostly (Table
5), however it doesn’t affect the serum ferritin levels.
23 cases belong to the age group less than 5 years and 57 belong to
the age group between 5-12 years. (Table 6)
Duration of fever was counted and the mean febrile period was 4.78
days. (Table 12)
The mean value of serum ferritin on day 3 for non-severe dengue is
404.43 with standard deviation 102.82 and the mean value of serum ferritin
on day 3 for severe dengue is 830.006 with standard deviation 160.064.
(Table 13)
75
The mean value of serum ferritin on day 4 for non-severe dengue is
585.905 with standard deviation 193.082 and the mean value of serum
ferritin on day 4 for severe dengue is 1259.824 with standard deviation
192.461. (Table 14)
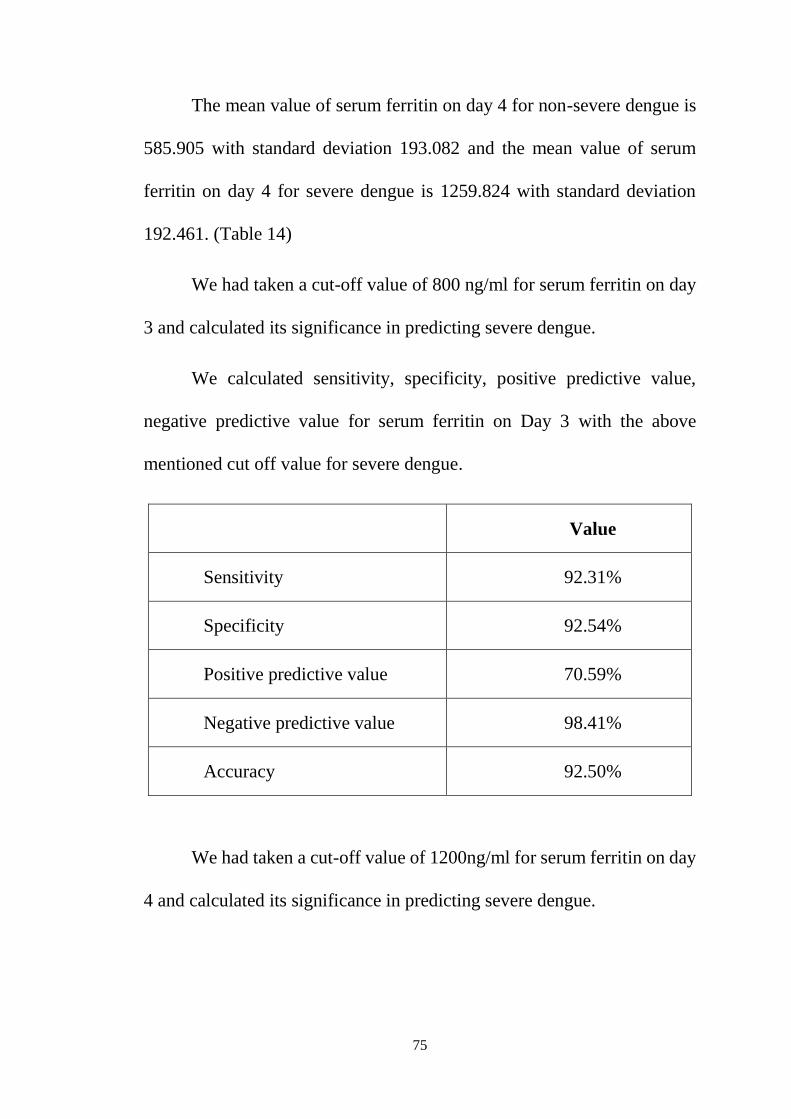
We had taken a cut-off value of 800 ng/ml for serum ferritin on day
3 and calculated its significance in predicting severe dengue.
We calculated sensitivity, specificity, positive predictive value,
negative predictive value for serum ferritin on Day 3 with the above
mentioned cut off value for severe dengue.
Value
Sensitivity 92.31%
Specificity 92.54%
Positive predictive value 70.59%
Negative predictive value 98.41%
Accuracy 92.50%
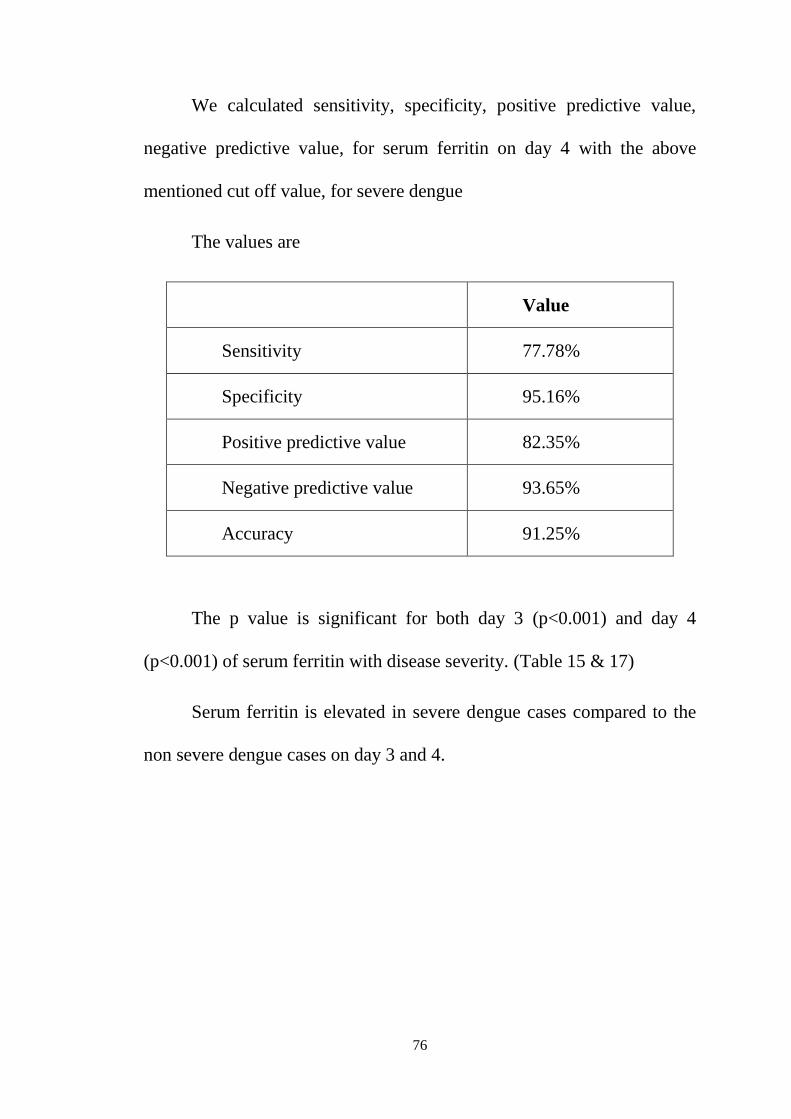
We had taken a cut-off value of 1200ng/ml for serum ferritin on day
4 and calculated its significance in predicting severe dengue.
76
We calculated sensitivity, specificity, positive predictive value,
negative predictive value, for serum ferritin on day 4 with the above
mentioned cut off value, for severe dengue
The values are
Value
Sensitivity 77.78%
Specificity 95.16%
Positive predictive value 82.35%
Negative predictive value 93.65%
Accuracy 91.25%
The p value is significant for both day 3 (p<0.001) and day 4
(p<0.001) of serum ferritin with disease severity. (Table 15 & 17)
Serum ferritin is elevated in severe dengue cases compared to the
non severe dengue cases on day 3 and 4.
77
CONCLUSION
Dengue is a serious infection which can range from mild illness to
severe life threatening complications like DSS/DHF. In this period of
dilemma in the clinicians’ front, ferritin was evaluated as an adjunct marker
for the diagnosis of dengue which could possibly aid their clinical
judgement and prompt early fluid resuscitation which in turn could be
useful in avoiding undue complications. Ferritin, as evaluated in the
present study may serve as a significant marker for differentiating between
non severe dengue cases and severe dengue cases.
78
LIMITATIONS
The spectrum of dengue infection is wide and this study only looked
at the hospitalized patients with severe dengue and also at admitted patients
with non severe dengue having warning signs positive.
However, a large set of patients with non severe dengue treated on
an OPD basis are not captured in this study.
A major limitation is that we have conducted the study with a
relatively small number of samples. However this data adds to the existing
data of medical literature and recommends extending our study during
future dengue outbreaks.
BIBLIOGRAPHY
1) Nelson textbook of pediatrics, 1st south Asian edition, vol 2, chapter
269, page 1629; scott B. halstead
2) Guzman MG, Halstead SB, Artsob H, Buchy P, Farrar J, et al. (2010)
Dengue: a continuing global threat. Nat Rev Microbiology 8: S7–
S16.
3) Maria G. Guzman, Scott B. Halstead, Harvey Artsob, Philippe
Buchy, Jeremy Farrar, Duane J. Gubler et al., Dengue: a continuing
global threat. Nat Rev Microbiology. 2010; 8: S7–S16.
4) PG Textbook of pediatrics; second edition; volume 2, Piyush gupta;
page no: 2384
5) Ghai essentials of pediatric medicine 9th edition; Tanu Singhal,
rakesh lodha, sunil k kabra; page 2196
6) L. Rothman and F. A. Ennis, “Immunopathogenesis of dengue
hemorrhagic fever,” Virology, vol.257, no.1, pp.1–6, 1999.
7) A. L. Rothman, “Immunity to dengue virus: a tale of original
antigenic sin and tropical cytokine storms,” Nature Reviews
Immunology, vol.11, no.8, pp.532–543, 2011.
8) Y.Sun,C.Jin, F.Zhanetal., “Hostcytokinestormis associated with
disease severity of severe fever with thrombocytopenia syndrome,”
Journal of Infectious Diseases, vol. 206, no. 7, pp. 1085–1094,2012.
9) Soundravally R, Hoti SL, Patil SA, Cleetus CC, Zachariah B,
Kadhiravan T, Narayanan P, Agiesh Kumar B. Association between
proinflammatory cytokines and lipid peroxidation in patients with
severe dengue disease around defervescence. Int J Inf dis. 2014;
18:68–72.
10) Kong YY, Thay CH, Tin TC, Devi S. Rapid detection, serotyping
and quantitation of dengue viruses by TaqMan real-time one-step
RT-PCR. J Virol Methods. 2006; 138: 123–30.
11) Wiwanitkit V. Accuracy and applicability of the revised WHO
classification (2009) of dengue. Infection. 2013; 41:1047. doi:10.
1007/s15010-013-0435-x. (Epub 2013 Mar 9. PubMed PMID:
23475504).
12) Wang SM, Sekaran SD. Early diagnosis of Dengue infection using
a commercial dengue Duo rapid test kit for the detection of NS1,
IgM, and IgG. Am J Trop Med Hyg 2010; 83: 690–95.
13) T. Pang, M. J. Cardosa, and M. G. Guzman, “Of cascades and perfect
storms: the immune pathogenesis of dengue haemorrhagic fever-
dengue shock syndrome (DHF/DSS),” Immunology and Cell
Biology, vol.85, no.1, pp.43–45, 2007.
14) G. N. Malavige, L.-C. Huang, M. Salimi, L. Gomes, S. D. Jayaratne,
and G. S. Ogg, “Cellular and cytokine correlates of severe dengue
infection,” PLoS ONE, vol. 7, no. 11, Article ID e50387, 2012.
15) Gregory CJ, Lorenzi OD, Colo ´n L, Sepu ´lveda Garcı ´a A,
Santiago LM, et al. Utility of the tourniquet test and the white blood
cell count to differentiate dengue among acute febrile illnesses in the
emergency room. PLoS Negl Trop Dis. 2011; 5:e1400.
16) Chaiyaratana W, Chuansumrit A, Atamasirikul K,
Tangnararatchakit K. Serum ferritin levels in children with dengue
infection. Southeast Asian J Trop Med Public Health. 2008; 39:832–
6. 29.
17) Ferritin levels predict severe dengue: R. Soundravally et al; springer;
October 2014
18) Serum Ferritin: An Indicator of Disease Severity in Patients with
Dengue Infection; Muhammad Nadeem1, Muhammad Mudassir
Shafiq; Journal of Rawalpindi Medical College (JRMC);
2016;20(3):165-167
19) Serum Ferritin: A Backstage Weapon in Diagnosis of Dengue Fever
20) SoumyabrataRoy Chaudhuri, Subhayan Bhattacharya;
Interdisciplinary Perspectives on Infectious Diseases; Volume
2017, Article ID 7463489, 6 pages
21) Can serum ferritin levels predict the severity of dengue early? an
observational study; velammal petchiappaj; international journal of
research in medical sciences; 2019 march;7(3);876-881
22) 3. Torti FM, Torti SV. Regulation of ferritin genes and protein.
Blood. 2002; 99: 3505–16.
23) Reif DW. Ferritin as a source of iron for oxidative damage. Free
Radic Biol Med. 1992; 12: 417–2
24) C. Ros´ario, G. Zandman-Goddard, E. G. Meyron-Holtz, D. P.
D’Cruz, and Y. Shoenfeld, “The hyperferritinemic syndrome:
macrophage activation syndrome, Still’s disease, septic shock and
catastrophic antiphospholipid syndrome,” BMC Medicine,
vol.11,no.1,article185,2013.
25) C.E.Allen, X.Yu, C.A.Kozinetz, and K.L.Mc Clain, “Highly
elevated ferritin levels and the diagnosis of hemophagocytic
lymphohistiocytosis,” Pediatric Blood & Cancer, vol. 50, no. 6,
pp.1227–1235, 2008.
26) T. Srichaikul, S. Punyagupta, T. Kanchanapoom, C. Chanokovat, K.
Likittanasombat, and A. Leelasiri, “Hemophagocytic syndrome in
dengue hemorrhagic fever with severe multiorgan complications,”
Journal of the Medical Association of Thailand, vol.91, no.1,
pp.104–109, 2008.
27) E.Rueda, A.Mendez, and G.Gonzalez, “Hemophagocyticsyndrome
associated with dengue hemorrhagic fever,” Biomedica, vol.22,
pp.160–166, 2002.
28) L. H. Tan, L. C. S. Lum, S. F. S. Omar, and F. K. Kan,
“Hemophagocytosis in dengue: comprehensive report of six cases,”
Journal of Clinical Virology, vol.55, no.1, pp.79–82, 2012.
29) A.Ab-Rahman, P.-F.Wong, H. Rahimetal., “Dengue death with
evidence of hemophagocytic syndrome and dengue virus infection
in the bonemarrow” Springer Plus, vol.4, no.1, article no.665, 2015.
PROFORMA
Name :
Age/ Sex :
Ip / Op no :
Address:
Symptoms:
Fever : yes / no duration :
Nausea and vomiting yes /no duration :
Aches and pain : yes /no
Abdominal pain : yes /no duration :
Persistent vomiting : yes/no duration :
Clinical fluid accumulation :yes/no
Mucousal bleed : yes/no
Lethargy /restlessness : yes/no
Past history :
Birth history :
Developmental history :
Immunization history :
General Examination :
Vitals :
PR : RR: BP:
TEMP : CRT : PERIPHERIES:
Anthropometry :
Height : Weight : MAC :
HC: AG:
Abdomen :
Cardio vascular system :
Respiratory system :
Central nervous system:
Diagnosis : Non severe dengue / Severe dengue
Severe dengue manifestations :
- Shock
- Bleeding
- Fluid Accumulation with respiratory distress
- Organ Involvement
Investigations :
Complete heamogram :
RFT :
LFT :
USG abdomen & pelvis :
IgM dengue / NS1 antigen:
SERUM FERRITIN : Day 3
Day 4
OTHER TESTS:
ABBREVATIONS
ALT - Alanine aminotransferase
ARDS - Acute respiratory distress syndrome
AST - Aspartate aminotransferase
BP - Blood Pressure
°C - Degree Celsius
CBC - Complete blood count
CNS - Central nervous system
CRT - Capillary refill time
DEN - Dengue
DEN-1 - Dengue virus serotype 1
DEN-2 - Dengue virus serotype 2
DEN-3 - Dengue virus serotype 3
DEN-4 - Dengue virus serotype 4
DF - Dengue fever
DHF - Dengue haemorrhagic fever
DIVC - Disseminated intravascular coagulopathy
DSS - Dengue shock syndrome
ECG - Electrocardiogram
ELISA - Enzyme-linked immunosorbent assay
FBC - Full blood count
FFP - Fresh frozen plasma
FWB - Fresh whole blood
GP - General practitioner
Hb - Haemoglobulin
HCO3 - Bicarbonate
HCT - Haematocrit
HF - Haemorrhagic fever
HELLP - Haemolysis, elevated liver enzymes and low
platelet count
HI - Haemagglutinin inhibition test
HIA - Haemagglutination inhibition assay
HIV - Human immunodeficiency virus
HR - Heart rate
IBW - Ideal body weight
ICU - Intensive care unit
IgM - Immunoglobulin M
IgG - Immunoglobulin G
IHA - Indirect haemagglutination
INR - International normalized ratio
JVP - Jugular venous pressure
NS1 Ag - Non-structural protein 1 antigen
NSAID - Non-steroidal anti-inflammatory agent
NT - Neutralization test
ORS - Oral rehydration solution
PaCO2 - Partial pressure of carbon dioxide
PCR - Polymerase chain reaction
PEEP - Positive end-expiratory pressure
PICU - Paediatric intensive care unit
PLT - Platelets
PR - Pulse rate
PT - Prothrombin time
PTT - Partial thromboplastin time
RBC - Red blood cell
RL - Ringer’s lactate
RR - Respiratory rate
RT-PCR - Reverse transcriptase polymerase chain reaction
SD - Standard deviation
SpO2 - Oxygen saturation
TWBC - Total white blood count
URTI - Upper respiratory tract infection
WBC - White blood cell
WHO - World Health Organization
CONSENT FORM
I hereby give consent to
participate in the study being conducted by Dr.V.MOHANRAJ
postgraduate in the Institute of Child Health & Research Centre, Madurai
medical college, Madurai and to use my personal clinical data and result of
investigations for the purpose of analysis and to study serum ferritin as a
predictor of dengue severity. I also give consent for further investigations.
Place:
Date:
Signature of the parents/guardian
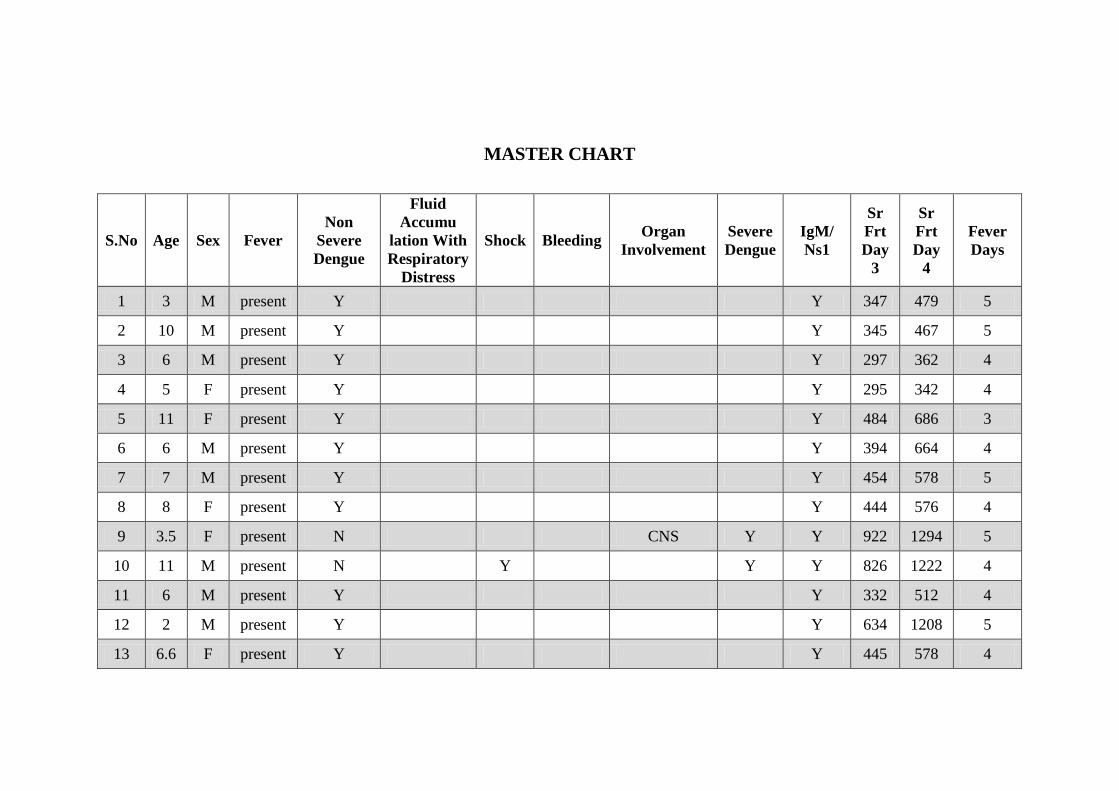
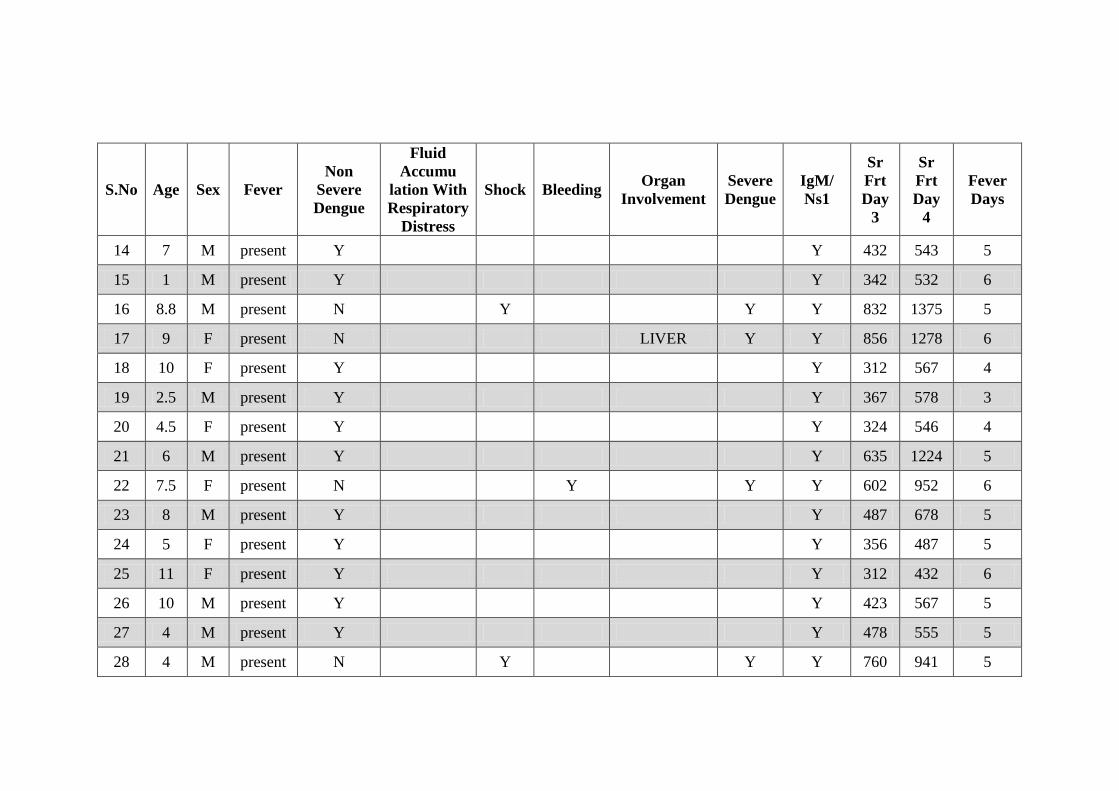
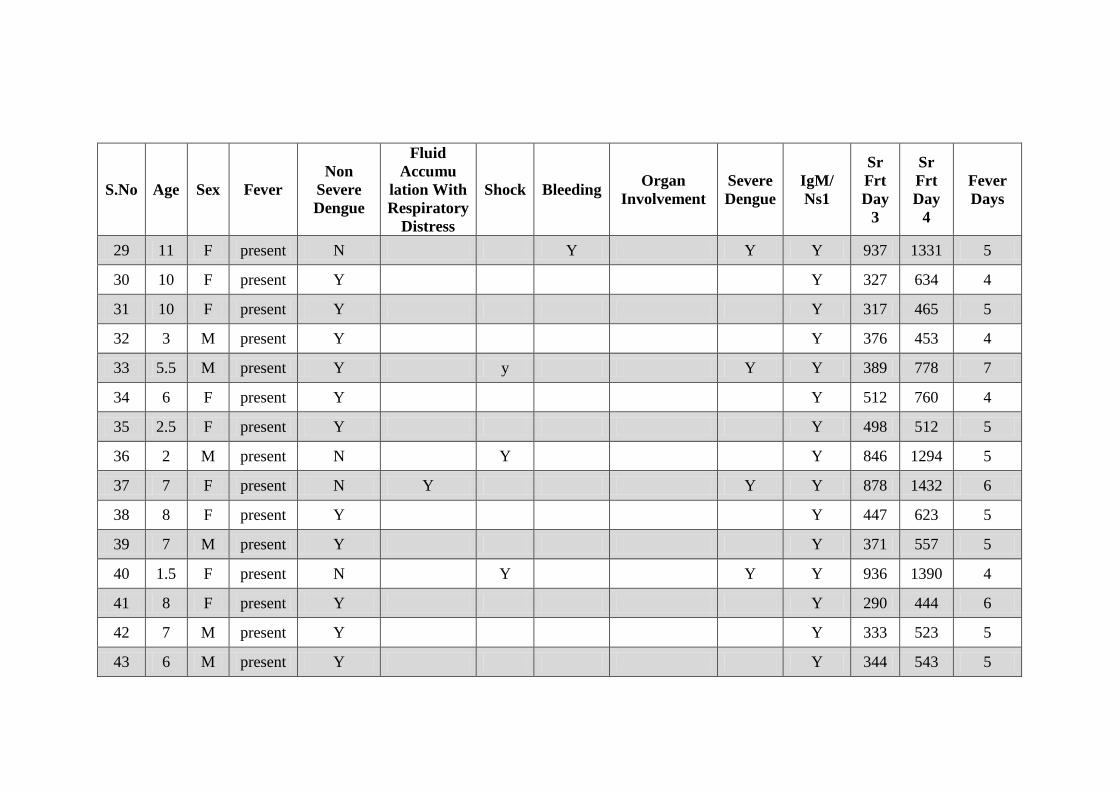
MASTER CHART
S.No Age Sex Fever
Non
Severe
Dengue
Fluid
Accumu
lation With
Respiratory
Distress
Shock Bleeding Organ
Involvement
Severe
Dengue
IgM/ Ns1
Sr
Frt
Day
3
Sr
Frt
Day
4
Fever
Days
1 3 M present Y Y 347 479 5
2 10 M present Y Y 345 467 5
3 6 M present Y Y 297 362 4
4 5 F present Y Y 295 342 4
5 11 F present Y Y 484 686 3
6 6 M present Y Y 394 664 4
7 7 M present Y Y 454 578 5
8 8 F present Y Y 444 576 4
9 3.5 F present N CNS Y Y 922 1294 5
10 11 M present N Y Y Y 826 1222 4
11 6 M present Y Y 332 512 4
12 2 M present Y Y 634 1208 5
13 6.6 F present Y Y 445 578 4
S.No Age Sex Fever
Non
Severe
Dengue
Fluid
Accumu
lation With
Respiratory
Distress
Shock Bleeding Organ
Involvement
Severe
Dengue
IgM/ Ns1
Sr
Frt
Day
3
Sr
Frt
Day
4
Fever
Days
14 7 M present Y Y 432 543 5
15 1 M present Y Y 342 532 6
16 8.8 M present N Y Y Y 832 1375 5
17 9 F present N LIVER Y Y 856 1278 6
18 10 F present Y Y 312 567 4
19 2.5 M present Y Y 367 578 3
20 4.5 F present Y Y 324 546 4
21 6 M present Y Y 635 1224 5
22 7.5 F present N Y Y Y 602 952 6
23 8 M present Y Y 487 678 5
24 5 F present Y Y 356 487 5
25 11 F present Y Y 312 432 6
26 10 M present Y Y 423 567 5
27 4 M present Y Y 478 555 5
28 4 M present N Y Y Y 760 941 5
S.No Age Sex Fever
Non
Severe
Dengue
Fluid
Accumu
lation With
Respiratory
Distress
Shock Bleeding Organ
Involvement
Severe
Dengue
IgM/ Ns1
Sr
Frt
Day
3
Sr
Frt
Day
4
Fever
Days
29 11 F present N Y Y Y 937 1331 5
30 10 F present Y Y 327 634 4
31 10 F present Y Y 317 465 5
32 3 M present Y Y 376 453 4
33 5.5 M present Y y Y Y 389 778 7
34 6 F present Y Y 512 760 4
35 2.5 F present Y Y 498 512 5
36 2 M present N Y Y 846 1294 5
37 7 F present N Y Y Y 878 1432 6
38 8 F present Y Y 447 623 5
39 7 M present Y Y 371 557 5
40 1.5 F present N Y Y Y 936 1390 4
41 8 F present Y Y 290 444 6
42 7 M present Y Y 333 523 5
43 6 M present Y Y 344 543 5

S.No Age Sex Fever
Non
Severe
Dengue
Fluid
Accumu
lation With
Respiratory
Distress
Shock Bleeding Organ
Involvement
Severe
Dengue
IgM/ Ns1
Sr
Frt
Day
3
Sr
Frt
Day
4
Fever
Days
44 11 M present Y Y 421 624 4
45 3 F present Y Y 465 613 5
46 11 F present Y Y 324 467 5
47 10 M present N Y Y Y 1015 1442 5
48 9 M present N Y Y Y 789 1378 4
49 9 F present Y Y 354 512 5
50 5 F present Y Y 355 423 4
51 9 F present Y Y 356 478 4
52 9 F present Y Y 323 534 4
53 8 M present Y Y 444 578 6
54 4 F present Y Y 412 632 5
55 6 M present Y Y 423 676 5
56 7 M present Y Y 434 569 5
57 6.5 F present Y Y 323 555 4
58 4.5 F present N Y Y Y 812 1267 5
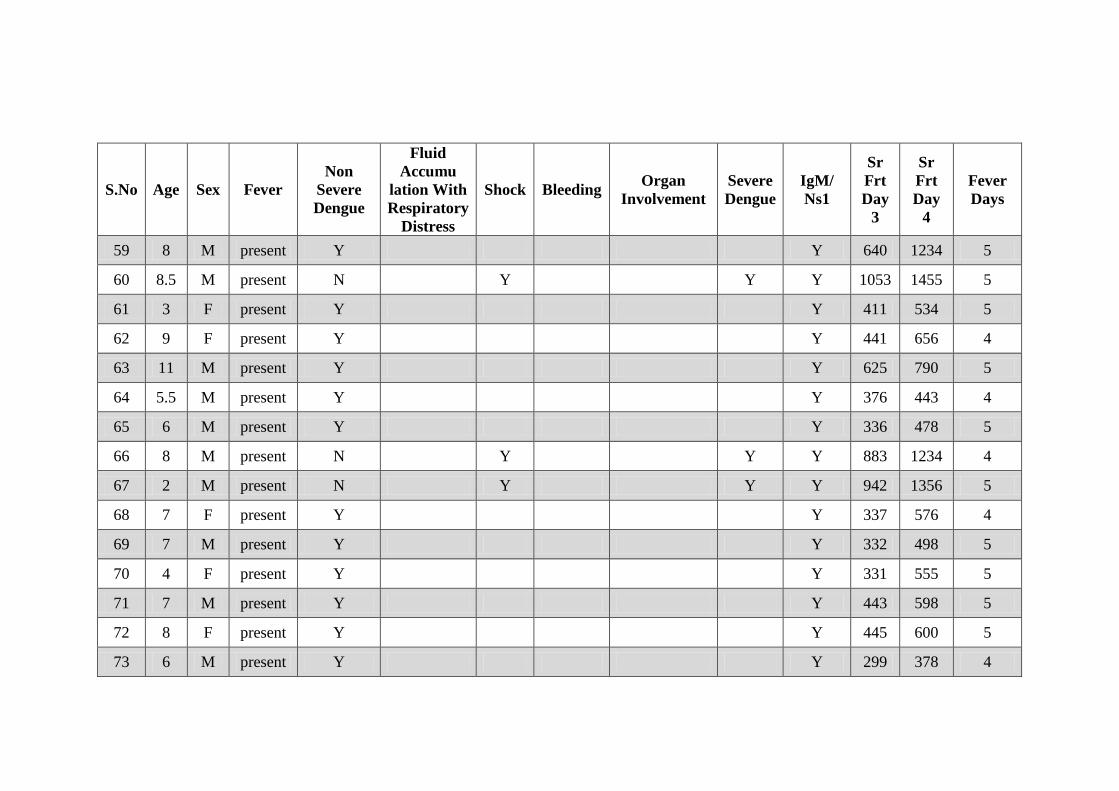
S.No Age Sex Fever
Non
Severe
Dengue
Fluid
Accumu
lation With
Respiratory
Distress
Shock Bleeding Organ
Involvement
Severe
Dengue
IgM/ Ns1
Sr
Frt
Day
3
Sr
Frt
Day
4
Fever
Days
59 8 M present Y Y 640 1234 5
60 8.5 M present N Y Y Y 1053 1455 5
61 3 F present Y Y 411 534 5
62 9 F present Y Y 441 656 4
63 11 M present Y Y 625 790 5
64 5.5 M present Y Y 376 443 4
65 6 M present Y Y 336 478 5
66 8 M present N Y Y Y 883 1234 4
67 2 M present N Y Y Y 942 1356 5
68 7 F present Y Y 337 576 4
69 7 M present Y Y 332 498 5
70 4 F present Y Y 331 555 5
71 7 M present Y Y 443 598 5
72 8 F present Y Y 445 600 5
73 6 M present Y Y 299 378 4
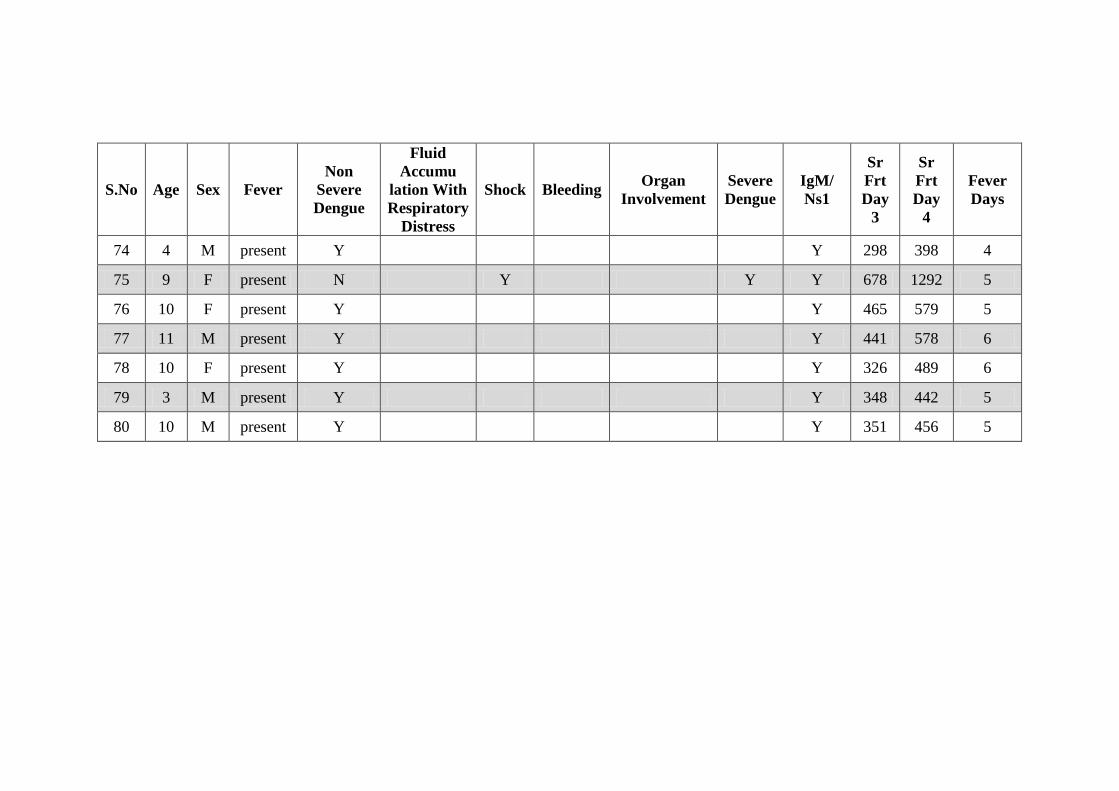
S.No Age Sex Fever
Non
Severe
Dengue
Fluid
Accumu
lation With
Respiratory
Distress
Shock Bleeding Organ
Involvement
Severe
Dengue
IgM/ Ns1
Sr
Frt
Day
3
Sr
Frt
Day
4
Fever
Days
74 4 M present Y Y 298 398 4
75 9 F present N Y Y Y 678 1292 5
76 10 F present Y Y 465 579 5
77 11 M present Y Y 441 578 6
78 10 F present Y Y 326 489 6
79 3 M present Y Y 348 442 5
80 10 M present Y Y 351 456 5