Embed Size (px)
Citation preview

SERUM 25(OH)D CONCENTRATION & CARDIOVASCULAR DISEASE RISK
ASSCOCIATIONS AMONG OLDER PUERTO RICANS
Dissertation Presented
By
Aziza A. Jamal-Allial, M.S.
To
The Bouvé Graduate School of Health Sciences
in Partial Fulfillment of the Requirements for or Doctor of Philosophy in Pharmaceutical
Sciences with specialization in
Statistics & Epidemiology
NORTHEASTERN UNIVERSITY
BOSTON, MASSACHUSETTS
August, 2013
© 2013 Aziza A. Jamal-Allial

2
TABLE OF CONTENTS
ABSTRACT .................................................................................................................... 6
ACKNOWLEDGMENTS ............................................................................................... 9
DEDICATION .............................................................................................................. 11
LIST OF TABLES ........................................................................................................ 12
LIST OF FIGURES ....................................................................................................... 14
CHAPTER ONE ........................................................................................................... 15
INTRODUCTION ......................................................................................................... 15
STATEMENT OF THE PROBLEM ............................................................................ 17
REVIEW OF THE LITERATURE ............................................................................... 19
The Epidemiology of Cardiovascular Disease and Atherosclerosis ............................. 19
The Progression of Atherosclerosis ........................................................................... 20
VITAMIN D METABOLISM ...................................................................................... 23
Overview of Synthesis and Metabolism .................................................................... 23
Vitamin D Receptor: .................................................................................................. 24
The Association between Vitamin D Deficiency and CVD Risk Factors ................. 26
Proposed Mechanisms of Anti-Inflammatory Actions of Vitamin D ........................ 27
PRELIMINARY STUDIES .......................................................................................... 30
RESEARCH DESIGN AND METHOOLOGY ........................................................... 41
Study Population and Data Collection....................................................................... 41
Data Collection .......................................................................................................... 42
Covariates Assessments and Definition .................................................................... 43
Laboratory Assays ..................................................................................................... 44
Potential Covariates: .................................................................................................. 45
Data Entry and Quality Control ................................................................................. 46
STATISTICAL ANALYTICAL PLAN ....................................................................... 47
The Specific Aims ..................................................................................................... 49
BIBLIOGRAPHY ......................................................................................................... 51
CHAPTER TWO........................................................................................................... 60

3
Longitudinal Association of serum 25(OH)D concentration and Dyslipidemia among
Older Puerto Ricans: ..................................................................................................... 60
ABSTRACT .................................................................................................................. 61
INTRODUCTION ......................................................................................................... 63
MATERIALS AND METHODS .................................................................................. 65
Study Population and Data Collection....................................................................... 65
Covariates Assessments and Definition .................................................................... 66
Laboratory assays ...................................................................................................... 67
Statistical analyses: .................................................................................................... 68
RESULTS...................................................................................................................... 70
DISCUSSION ............................................................................................................... 72
BIBLIOGRAPHY ......................................................................................................... 77
CHAPTER THREE ....................................................................................................... 92
An Inverse Association of Vitamin D Serum Concentration and Inflammatory Markers
....................................................................................................................................... 92
ABSTRACT .................................................................................................................. 93
INTRODUCTION ......................................................................................................... 95
MATERIALS AND METHODS .................................................................................. 96
Study Population and Data Collection....................................................................... 96
Covariates and Exposure Assessments ...................................................................... 97
Laboratory assays ...................................................................................................... 99
Statistical analyses: .................................................................................................... 99
RESULTS.................................................................................................................... 101
DISCUSSION ............................................................................................................. 102
BIBLIOGRAPHY ....................................................................................................... 105
Poster Presentation: ................................................................................................. 116
PDF of the presentation of Chapter Two data at Experimental Biology 2013 ........... 116
CHAPTER FOUR ....................................................................................................... 117
Longitudinal Association of Vitamin D Serum Concentration & Adiposity Phenotypes
..................................................................................................................................... 117
ABSTRACT ................................................................................................................ 118

4
INTRODUCTION ....................................................................................................... 120
MATERIALS AND METHODS ................................................................................ 121
Study Population and Data Collection..................................................................... 121
Covariates Assessments and Definition .................................................................. 122
Laboratory assays .................................................................................................... 123
Statistical analyses: .................................................................................................. 124
RESULTS.................................................................................................................... 125
DISSCUSION ............................................................................................................. 127
BIBLIOGRAPHY ....................................................................................................... 130
Poster Presentation .................................................................................................. 138
CHAPTER FIVE ......................................................................................................... 139
The Association of Total and Regional Adiposity with Serum 25-hydroxyvitamin D
Concentration .............................................................................................................. 139
ABSTRACT ................................................................................................................ 140
INTRODUCTION ....................................................................................................... 142
MATERIALS AND METHODS ................................................................................ 144
Study Population and Data Collection..................................................................... 144
Covariates Assessments and Definition .................................................................. 145
Exposure Assessment: ............................................................................................. 146
Laboratory assays .................................................................................................... 146
Statistical analyses: .................................................................................................. 147
RESULTS.................................................................................................................... 148
DISCUSSION ............................................................................................................. 149
BIBLIOGRAPHY ....................................................................................................... 152
CHAPTER SIX ........................................................................................................... 164
DISCUSSION AND SUMMARY .............................................................................. 164
BIBLIOGRAPHY ....................................................................................................... 177
APPENDIX ................................................................................................................. 184
Serum Vitamin D Concentration, Dietary Sources, and its relation to BMI among
Puerto Ricans Living in the Greater Boston Area ....................................................... 185

5
ABSTRACT ................................................................................................................ 186
INTRODUCTION ....................................................................................................... 187
MATERIALS AND METHODS ................................................................................ 188
Study Population...................................................................................................... 188
Field data collection ................................................................................................. 189
Laboratory assays .................................................................................................... 190
Statistical analyses ................................................................................................... 191
RESULTS.................................................................................................................... 191
DISCUSSION ............................................................................................................. 194
BIBLIOGRAPHY ....................................................................................................... 197

6
ABSTRACT
Cardiovascular disease (CVD) is the number one single cause of mortality and
morbidity, accounting for approximately 30% of deaths worldwide. Numerous risk
factors for CVD are well established, but novel ones continue to emerge. Several reports
have suggested that there is an association between plasma 25-hydroxyvitamin D
concentration (25(OH)D) and CVD. Vitamin D deficiency is prevalent, especially among
ethnic minorities.
The objective of this dissertation was to investigate, cross-sectionally and
longitudinally, the relation between serum 25(OH)D concentration and CVD risk factors
in 970 Puerto Rican adults, 270 men and 700 women, aged 45-75 years: (1) to
investigate, longitudinally, the relation between serum 25(OH)D concentration and lipid
profile, specifically, high-density lipoprotein (HDL-C), low-density lipoprotein (LDL-C),
total cholesterol (TC) and triglycerides (TG). (2) to investigate, cross-sectionally, the
relation between serum 25(OH)D concentration and serum inflammatory markers,
specifically, tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and high-
sensitivity C-reactive protein (hsCRP). (3) to investigate the longitudinal effect of body
mass index (BMI), and waist circumference (WC) as measures of adiposity on serum
25(OH)D concentration. (4) to investigate, cross-sectionally, the association of regional
and total adiposity, specifically, total body fat (TBF), percent body fat (%TBF), android
fat-mass (AFM) and gynoid fat-mass (GFM), using dual-energy x-ray absorptiometry
(DXA), on serum 25(OH)D concentration.
The cross sectional analyses from the two year time point showed that among all
participants, HDL-C had a significant positive association with plasma 25(OH)D

7
(P<0.01) while TG had significant negative association; but not LDL-C, or TC. The
longitudinal analyses showed that when predicting 2.5-year change in plasma HDL-C,
baseline-25(OH)D had a significant inverse association (β = -0.045 ± 0.02, P =0.007)
controlling for age, sex, baseline-HDL-C concentration, BMI, and follow-up time.
Similarly, after controlling for potential confounders, the baseline-25(OH)D was a
significantly positive predictor of the change in plasma TG concentration over time (β =
0.40 ± 0.02, P =0.03). With regard to inflammatory markers, after adjusting for age, sex,
and seasonality, the multivariate regression analyses showed that serum 25(OH)D had a
significantly negative association with TNF-α and IL-6, (P<0.01 and P<0.04),
respectively, but not with hsCRP. Further adjustment for numerous identified
confounders did not alter the significant associations between serum 25(OH)D
concentration with TNF-α and IL-6. The adiposity analyses showed that BMI and WC
were both negatively correlated, at both time points, with serum 25(OH)D concentration
(r = -0.1, P =0.02) and (r = -0.1, P =0.009), respectively. The multivariate analysis
showed that when predicting the change of serum 25(OH)D concentration, only baseline-
BMI had significantly inverse association (β = - 0.22, P =0.01) controlling for age, sex,
and baseline-BMI. This association remained significant after adjusting for numerous
recognized confounders, while baseline-WC was not significantly associated with serum
25(OH)D concentration. When investigating regional adiposity, our analyses showed that
neither TBF in grams nor %TBF were significantly associated with serum 25(OH)D.
However, AFM seems to have an inverse significant association with serum 25(OH)D,
whereas GFM showed a positive significant association with serum 25(OH)D.

8
In conclusion, even though 25(OH)D serum concentration was positively
associated with HDL-C in our cross-sectional analyses, the longitudinal analyses
showed that higher 25(OH)D serum concentration did not translate into an increase of the
atheroprotective HDL-C, nor a decrease in the not-atheroprotective plasma TG in this
population, which seems contradictory to the some of the literature . When we
investigated the association of serum 25(OH)D and inflammation, lower serum 25(OH)D
concentration was significantly associated with higher inflammatory concentration in this
population. The third major finding of the present dissertation work is that obesity has an
opposing effect on serum 25(OH)D concentration in this population of older Puerto Rican
adults living in the Boston area, which might accelerate vitamin D deficiency status.
Longitudinal studies are needed to clarify causal pathways.

9
ACKNOWLEDGMENTS
No words neither sentences can fully express my ample gratitude to everyone who was
there for me. I would like to extend my warmest appreciation and thankfulness to my committee
members, Dr. Mansoor Amiji, Dr. Katherine L. Tucker, Dr, John L. Griffith, Dr. S. John Gatley
and last but not least Dr. David R. Janero. This dissertation work would have not been achievable
without the endless support, encouragement, mentorship, and expertise I have endured from each
and every member of my committee.
My special appreciation is to Dr. Tucker for the tremendous and amazing opportunity she
gave me through these six years. Katy was there for me not only during the happy times, but as
well through the most difficult times with endless believe in my ability to achieve my dreams.
She understood that I am a mother first, and student second. Katy taught me how to be an
independent thinker and use my intellectual freedom as well as have a broad knowledge. I hope I
can carry a fraction of that knowledge I gained while working with her to the next chapter in my
career.
When I arrived at Northeastern I needed a home, and Dr. Amiji’s group was my home. I
cannot thank Dr. Amiji and his team enough for their generosity. His lab not only offered me
home, but also allowed me to broaden my knowledge and look at vitamin D from a different
perspective. My special thanks to Dr. Amit Singh, Dr. Srinivas Ganta, Dipti Deshpande, Shardool
Jain and Vanessa Nascimento among others who were there to mentor and answer my questions.
This study would not be possible without the tremendous mentorship of Dr, John L. Griffith. I
appreciate that every Tuesday at 1:00 pm, I know this is my blocked hour to ask, discuss and
converse with him about statistical modeling. I am better statistician because of his dedications. I
thank Dr. Gatley for all of these wisdom talks we had, it made me a better researcher. Finally, Dr.
Janero was always there to edit my writing, it made me a better writer.

10
This dissertation work would not be possible without the staff and the participants of the
Boston Puerto Rican Health Study. Without their dedication to the study, it would not be
possible. Much gratitude to the faculty and staff of the Pharmaceutical Science department and
Northeastern University, they have generously given their time and expertise to make us better
researchers. Every single interaction with them has been an amazing experience and I am truly
honored.
My deep gratitude to Dr. Mohamed Aleissa, the Cultural attaché at the Culture Mission of
Saudi Arabia, and Dr. Abudlaziz Aleisa, my advisor, among all the employee of SACM, for their
supports and encouragement. SCAM not only provided financial support but emotional
reassurance.
My friends were there for me all along, not only when laughing, but rather crying,
celebrating and even when it was hurtful, my special gratitude to Shilpa Bhuapathiraju, PhD.
Latrice Landry, PhD, Carlota Dao, PhD, Grace Bennett, PhD, Dr. Ons Khadra and Abeer Radady
M.D. In addition, special thanks to my amazing friend Stephanie Peterson for her editorial work
as well as to Shilpa Saklani for her amazing SAS macros.
Finally, I came to the most personal source of appreciation and gratefulness, my family.
My parents are the reason I have come to what I am today, they raised my siblings and I to
achieve and reach high in the sky. To my siblings, Mohammed, Olaa and May, who continued to
support and inspire me at every step of my life. Finally, to the most enduring source of strength
and motivation of my success, to my husband, Ashhal Jastania and my children, Hamza and
Mawada, this work is dedicated to you; you have given me endless love and support and without
you in my life, this was not possible. LOVE YOU!!

11
DEDICATION
To my lifelong partner, my husband Ashhal, and my rock and amazing children, Hamza
and Mawada, for the love, the devotion, the support, the persistence and the
encouragement needed to keep me going,
to my family, my friends, to everyone for truly believing in me.
This dissertation is dedicated to you!!

12
LIST OF TABLES
Table 1 List of studies of calcitriol and atherosclerosis using Apoe-/- mice....................29
Table 2 Descriptive characteristics of the BPRHS participants........................................35
Table 3 Selected dietary data of the participants of the BPRHS.....................................36
Table 4 Major Dietary Sources of Vitamin D intake among Puerto Rican adults…….37
Table 5 The Age-adjusted means for all variables……………………………………..38
Table 6 Multiple linear regression stratified by sex…………………………………...40
Table 7 Summary of calculated outcome measures and covariates……………………49
Table 1.1 Descriptive characteristic of men and women in the BPRHS & BPROS….....82
Table 1.2 Pearson partial linear correlation of serum 25(OH)D concentration and
adiposity phenotype at baseline and 2-year…………………………………………..…84
Table 1.3 Regression coefficients from longitudinal linear regression analysis of lipid
profile components and baseline serum 25(OH)D concentration………………………85
Table 1.4 Regression coefficients from longitudinal linear regression analysis of lipid
profile components and baseline serum 25(OH)D concentration………………………87
Table 2.1 Descriptive characteristic of the men and women of BPROS………………108
Table 2.2 Pearson partial linear correlation of serum 25(OH)D concentration and
inflammatory markers………………………………………………………………….110
Table 2.3: Regression coefficients from multivariate regression analysis of inflammatory
markers and 25(OH)D concentration. …………………………………………………111
TABLE 2.4: Regression coefficients from multivariate regression analysis of hsCRP and
serum 25(OH)D concentration. ………………………………………………………..112
Table 3.1 Descriptive characteristic of men and women of BPRHS & BPROS…........133
Table 3.2 Pearson partial linear correlation of serum 25(OH)D concentration and
adiposity phenotype at baseline and 2-year……………………………………………134
Table 3.3 Regression coefficients from longitudinal linear regression analysis of
adiposity phenotypes on plasma 25(OH)D concentration………………………..……135
Table 4.1 Descriptive characteristics of men and women of BPROS……………….....159
Table 4.2 Pearson partial linear correlation of serum 25(OH)D concentration and
adiposity phenotype at 2-year……………………………………………..……………161
Table 4.3 Regression coefficients from cross-sectional regression analysis of TBF and
%TBF on plasma 25(OH)D concentration….…………………………….……………162

13
Table 4.4 Regression coefficients from cross-sectional regression analysis of AFM and
GFM on plasma 25(OH)D concentration……………………………….…………...…163
Table 6.1 Descriptive characteristics of men and women in the BPRHS………..…….211
Table 6.2 Age-adjusted means of serum 25(OH)D stratified by sex for different
characteristics among BPRHS participants……….………………..…….……….……212
Table 6.3 Correlates of serum 25(OH)D concentration among Puerto Rican adults
stratified by sex. ……………………………………………………………….……….214
Table 6.4 The least-square means of serum 25(OH)D concentration for the effect of
vitamin D supplements categories by sex………………………………………………215
Table 6.5 The least-square means of serum 25(OH)D concentration and seasons
categories by age groups…………………………………………………………..……216
Table 6.6 Major Dietary Sources of Vitamin D intake among Puerto Rican adults…..217

14
LIST OF FIGURES
Figure 1 Ergocalciferol structure D2………………………………………………….....23
Figure 2 Cholecalciferol structure D3…………………………………………………...23
Figure 3 Calcidiol Structure 25(OH)D………………………………………………….23
Figure 4 Calcitriol structure 1α-25(OH)2D……………………………………………..24
Figure 5 The percent of BPRHS women and men serum 25(OH)D concentration…….31
Figure 6 The association between vitamin D intakes from food & supplement………..32
Figure 7 The association between vitamin D intakes from food only sources…………32
Figure 8 Diagram illustrates the relationship between serum 25(OH)D and the various
CVD risk factors ………………………………………….……………………….…….50
Figure 1.1 Prevalence of low serum 25(OH)D concentration among PR………………89
Figure 1.2 The association between serum (25)OH at baseline and the change in HDL
over time modified by smoking………………………………………………………… 90
Figure 1.3 The association between serum (25)OH at baseline and the change in LDL
over time modified by smoking………………………………………………………… 91
Figure 2.1 Adjusted means of IL-6 concentration by tertiles of adjusted serum
25(OH)D………………………………………………………………………………..113
Figure 2.2 Adjusted means of TNF-α concentration by tertiles of adjusted serum
25(OH)D……………………………………………………………………………..…114
Figure 2.1 Adjusted means of hsCRP concentration by tertiles of adjusted serum
25(OH)D……………………………………………………………………………..…115
Figure 3.1 The monthly distribution of serum 25(OH)D for the participants of BPRHS at both time points……………………………………………………………………….136 Figure 3.2 The adjusted means of serum 25(OH)D within the categories of class III obesity…………………………………………………………………………….…….137 Figure 4.1 The illustrations of android region and gynoid region………………….….157 Figure 4.2 the association between serum 25(OH)D concentration with gynoid and
android fat among………………………………………………………………………158
Figure 5.1 Diagram illustrates the relationship between serum 25(OH)D and the various
CVD risk factors among the participants of the BPRHS…………………………….…177
Figure 6.1 Prevalence of low serum 25-hydroxyvitamin D concentration among Puerto
Rican men and women……………………………………………………………….....218
Figure 6.2 Association between the median intake of total vitamin D (defined by the
RDA) and serum 25(OH)D for BPRHS participants…………………………………...219
Figure 6.3 Association between vitamin D intake from food only sources and serum
25(OH)D among non-supplement users of the BPRHS participants…………………..220
Figure 6.4 Mean serum 25(OH)D concentration by BMI categories of Puerto Rican
women…………………………………………..………………………………………221

15
CHAPTER ONE
INTRODUCTION
Cardiovascular disease (CVD) is the number one single cause of mortality and
morbidity, accounting for approximately 30% of deaths worldwide in 2008. Numerous
risk factors for CVD are well established, but novel ones continue to emerge.
Atherosclerosis underlies various adverse vascular events that contribute to the
development of CVD. It is considered a chronic inflammatory disease of the muscular
arterial walls that is characterized by the accumulation of lipoproteins, immune response
activation, and increased expression of growth factors, all of which leads to endothelial
dysfunction and induces proliferation and migration of smooth muscle cells within the
arterial wall. Despite substantial advances in drug discovery and development for
treatment of cardiovascular disease over the last decade, the use of regimens such as
lipid-lowering agents, anti-platelet drugs, and anti-inflammatory drugs has not solved the
complex, multifactorial interplay of the pathophysiological drivers of CVD.
We proposed an interdisciplinary study of the association of various CVD risk
factors and serum 25-hydroxyvitamin D [25(OH)D] concentration of the participants of
Boston Puerto Rican Health Study (BPRHS) and the Boston Puerto Rican Osteoporosis
Study (BPROS). We examined the association between serum 25(OH)D concentration
and pro-inflammatory markers such interleukin-6 (IL-6), tumor necrosis factor-α (TNF-
α), and high-sensitivity C-reactive protein (hsCRP); plasma lipid profile, including total

16
cholesterol (TC), low-density lipoproteins (LDL-C), high-density lipoproteins (HDL-C),
and triglycerides (TG); and adiposity measures including: body mass index (BMI), waist
circumference (WC), and total body fat (TBF). The Boston Puerto Rican Health Project
is an ongoing longitudinal study with two time-points and a sample size of 1502
participants.

17
STATEMENT OF THE PROBLEM
Cardiovascular disease (CVD) is a major public health concern worldwide [1].
The list of traditional risk factors for CVD published by the American Heart Association
(AHA) includes family history, age, sex, behavioral/lifestyle, smoking, obesity, diabetes,
hyperlipidemia and hypertension [2]. Atherosclerosis is one of major causes of CVD and
it is characterized by lipid accumulation and systematic inflammation, and endothelial
dysfunction. The expression of inflammatory cytokines is a critical factor influencing
CVD progression [3]. Vitamin D (vitamin D) deficiency is now believed to be associated
with CVD and immune response: vitamin D appears to have a regulatory influence on the
inflammatory cytokines involved in the progression of systematic inflammation and
endothelial dysfunction [4].
The aims of our study: Puerto Rican men and women, aged 45-75 years, will be
evaluated both cross-sectionally and longitudinally, at baseline and at 2 years.
Aim One: To evaluate longitudinal associations between serum 25(OH)D concentration
and plasma lipid profile, precisely, high-density lipoproteins (HDL-C), low-density
lipoproteins (LDL-C), and total cholesterol (TC) and triglycerides (TG).
Aim Two: To evaluate cross-sectional associations between serum 25(OH)D
concentration and inflammatory markers, precisely, interleukin-6 (IL-6), tumor necrosis
factor-α (TNF-α), and high sensitivity C-reactive protein (hsCRP).
Aim Three: To evaluate the longitudinal associations between serum 25(OH)D
concentration and adiposity phenotype, specifically, body mass index (BMI) and waist
circumference (WC) among 970 participants of the BPRHS and BPROS studies

18
Aim Four: To evaluate cross-sectional associations between serum 25(OH)D
concentration and adiposity measures, specifically, total body fat mass (TBF) measured
by dual-energy x-ray absorptiometry (DEXA).
The relationship between serum vitamin D concentration and CVD risk factors in
general, and atherosclerosis, in particular, is well documented [5, 6]. The continued high
incidence of CVD-related mortality and morbidity emphasizes the need to distinguish not
only the contributors to CVD risk, but also to identify new therapeutic modalities for the
treatment of atherosclerosis as a primary cause of CVD. We believe that the proposed
work will contribute to the current knowledge of vitamin D and CVD risk. We know of
no studies that have reported on associations between serum vitamin D concentration and
CVD risk factors among older Puerto Ricans. Thus, results from our cohort project will
be the first to assess this association, longitudinally, within this particular ethnicity.

19
REVIEW OF THE LITERATURE
The Epidemiology of Cardiovascular Disease and Atherosclerosis
Despite significant progress in scientific research of CVD, it remains the leading
cause of morbidity and mortality worldwide [1, 7, 8]. According to the World Health
Organization (WHO), in 2010, CVD accounted for 17.3 million deaths, which is about
29% of all global deaths; it is projected that CVD will be responsible for ~24 million
deaths annually by the year 2030 [1]. In the USA, the mortality data for 2007 showed that
CVD remained the primary cause of death in the USA; approximately 34% of deaths
were CVD related [7, 9]. CVD risk factors are diverse, ranging from traditional factors
such as age, sex, smoking, inactivity, obesity, family history, hypertension, and
hyperlipidemia [10, 11]. However, traditional factors cannot fully explain the increase in
CVD incidence, and the emergence of more novel pathophysiological factors such as
inflammation, oxidative stress and adipocyte dysfunction might provide more insights on
the development of CVD [9]. Atherosclerosis is a pathological condition that underlies
various adverse vascular events that contribute to CVD development [12]. It is
characterized by accelerated accumulation macrophages and oxidized LDL (oxLDL)
within arterial blood vessels [3, 13]. The early stages of atherosclerosis are characterized
by endothelial dysfunction—impairment of endothelium-dependent vasodilatation, which
can be measured by brachial artery flow-mediated dilation (FMD) [14, 15].

20
The Progression of Atherosclerosis
The walls of large musular arteries consist of three distinct, well-differentiated
layers. The outermost layer relative to the vessel lumen is the tunica adventitia, which is
composed of connective tissue; inside this is the tunica media, which consists of smooth
muscle cells and elastic tissue; and the innermost layer, called the intima, consists of the
internal elastic lamina and a monolayer of endothelial cells, which is continuously and
directly exposed to blood and its constituents, along with the hemodynamic shear forces
associated with the flowing blood [3, 13]. The endothelial layer of the intima is a critical
controller of vascular homeostasis and functions as an anti-thrombotic vessel lining [16].
Vascular endothelial cells synthesize and release a wide array of mediators that act in
autocrine and/or paracrine modes to modulate the structure of the artery, smooth muscle
quiescence, endothelial passivity as well as blood constituents, vessel tone, and
hemodynamic reactivity.
The development of atherosclerosis involves early endothelial activation generally
believed to be triggered by various local factors such as oxidative stress and increased
expression of pro-inflammatory mediators, all of which lead to increases of the
adhesiveness of leukocytes or platelets through the increased expression of intracellular
adhesion molecule (ICAM). Another hallmark of endothelial activation is the increased
permeability of lipoproteins such as LDL-C and TG [3, 12, 13] and a defect in the
production of nitric oxide (NO) from L-arginine by endothelial NO synthase (eNOS)
[14].

21
NO is the most potent vasodilator yet identified and further acts to inhibit platelet
activity and smooth-muscle cell proliferation. In addition to mediating endothelium-
dependent vasodilatation, NO is critical for preventing platelet and leukocyte aggregation
as well as leukocyte adhesion and infiltration [12, 14]. Further, trapped LDL-C undergoes
modification including oxidation, lipolysis, and proteolysis, generating oxLDL-C, which
has the ability to inhibit the production of NO as well as to stimulate the endothelium to
produce pro-inflammatory molecules including adhesion molecules and growth factors.
Subsequently, monocytes and lymphocytes migrate across the endothelial layer into the
intima, where they proliferate and differentiate into macrophages. This migration is
triggered by the accumulation of oxLDL-C. Moreover, increased expression of ICAM
induces the adhesion of these monocytes along with LDL-C. Later, the extensive
modification of the oxLDL-C allows their recognition by the scavenger receptors within
the macrophage, and, hence, their uptake leads to foam-cell formation. Such receptor
expression is mediated by TNF-α and interferon-γ (IFN-γ) cytokines. The progressive
accumulation of foam cells, oxLDL-C, and monocytes leads to fatty streak formation.
As fatty streaks progress to advanced lesions, smooth muscle cells (SMC) migrate
to the intima along with T cells, subsequently leading to the development of a necrotic
core. This advanced lesion is characterized by dead foam cells, accelerated lipoprotein
and SMC macrophage accumulation, and enhanced inflammatory response, all of which
are covered by a fibrous cap that extends into the lumen. Rupture of the fibrous cap
exposes the content of the necrotic core to the blood, leading to coagulation and
recruitment of platelets, resulting in thrombosis [3, 12, 13].

22
Inflammation plays a pivotal role in all stages of atherogenesis, from foam cell to
plaque formation, and all the way to rupture and ultimately to thrombosis [17, 18]. In
fact, atherosclerotic lesions are characterized by the release of various pro-inflammatory
cytokines, such as hsCRP, IL-1β, IL-6 and TNF-α. The binding of LDL-C to the
endothelium is mediated by both IL-1β and TNF-α. Inflammatory cytokines such as IFN-
γ activate the macrophages to undergo programmed cell death, apoptosis, causing a mass
of extracellular lipids and debris. Thus, this cycle that starts with inflammation,
modification of lipoprotein systems and further inflammation is an illustration of how the
inflammatory response has a profound effect not only the development of atherosclerosis,
but in some cases it is considered a healing and repair response.
Emerging evidence suggests that serum vitamin D concentration are associated
with a wide spectrum of CVD risk factors, generally, and with atherosclerosis
development, specifically [19-25]. It has been hypothesized that higher serum vitamin
D concentration may play a major role in the attenuation of atherosclerosis
development and improvement of endothelial function. However, due to the complexity
of CVD, with its wide range of risk factors as well as its clinical biomarkers, and
complexity of vitamin D with its limited dietary sources vs. synthesis from sunlight, the
supporting evidence is mixed.

23
VITAMIN D METABOLISM
Overview of Synthesis and Metabolism
Vitamin D is a secosteriod compound with 27 carbons,
there are two forms of vitamin D, D2 or ergocalciferol (Figure 1),
and D3 cholecalciferol (Figure 2). It is an essential nutrient, but is
unlike most other nutrients in terms of its limited food sources
[26]. Only a few food sources, such as fatty fish and cod liver oil,
naturally contain vitamin D, making it difficult to achieve optimal
vitamin D concentration through food intake alone. Since the
1930s, dietary fortification with vitamin D has been established in
a number of different products, including milk, soymilk, orange
juice and selected cereal grains [27, 28]. In most cases, achieving
optimum vitamin D only with dietary intake is not feasible [26, 29-
31]; rather, a relatively efficient way of obtaining vitamin D is
endogenously, via the ultraviolet-β activation of 7-
dehydrocholestrol to pro-vitamin D3, within the epidermal basal
layer, which then undergoes isomerization producing the D3 form,
cholecalciferol (Figure 2). Afterward, cholecalciferol binds to the vitamin D-binding
protein (VDBP) and is transported to the liver, where it gets its first hydroxylation at the
25 position by 25-hydorxylase, producing calcidiol or 25(OH)D (Figure 3) [32].
Afterward, cholecalciferol binds to the vitamin D-binding protein (VDBP) and is
Figure 1: Ergocalciferol structure (D2)
Figure 2: Cholecalciferol
structure (D3)
Figure 3: Calcidiol
Structure (25(OH)D)

24
transported to the liver, where it gets its first hydroxylation at the 25 position by 25-
hydorxylase, producing calcidiol or 25(OH)D (Figure 3) [32].
Several cytochrome-P450 enzymes (CYP-450s), such as
CYP2J2, and CYP3A4, also exhibit hydroxylase activity, which
metabolizes the less potent D2 form (Figure 1) [33]. 25(OH)D is
the blood biomarker for determining the status of vitamin D: it is
characterized by a relatively long half-life of about 3 weeks.
Mainly in the kidney, a second hydroxylation occurs at the 1-α
position by CYP27B1, a 1α-hydorxylase, converting 25(OH)D to 1α,25(OH)2D, calcitriol
(Figure 4), which is the active metabolite, but which has a very short half-life, up to only
12-15 hours [32, 34-36]. This pathway is exquisitely regulated by parathyroid hormone
(PTH), serum calcium concentration(Ca+), and phosphate (Pi) concentration, and also by
negative feedback inhibition from 1α,25(OH)2D concentration [37]. CYP-P450 regulates
the catabolism of vitamin D through the actions of CYP24A1, 24-hydroxylase, which
hydroxylates both 25(OH)D and 1α,25(OH)2D at the 24 position, leading to the inactive
hydrophilic metabolites 24,25(OH)2D and 1α,24,25(OH)3D, which are readily excreted
in the urine; consequently, this catabolic pathway is a limiting step [34].
Vitamin D Receptor:
Vitamin D and its analogs exert their differential effects on target cells through
two main pathways: genomic and non-genomic pathways. The genomic pathway is
mediated through the binding of 1α,25(OH)2D and/or its analogs to the nuclear vitamin D
Figure 4: Calcitriol
structure (1α-25(OH)2D)

25
receptor (VDR) to exert transcriptional activation and gene expression repression. VDR
is classified as a nuclear hormone receptor and is expressed and localized in various
tissues where vitamin D has regulatory the pancreatic β cells, monocytes, dendritic cells,
and peripheral T cells. The binding of 1α,25(OH)2D to VDR requires a specific ligand,
retinoid-X receptor (RXR). Thus, this later compound binds to response elements
(VDREs) in the promoter region of targeted genes, which is followed by a cascade of
binding of transcription factors, co-activators, and co-repressors to increase the
transcription and/or suppress of target genes. The non-genomic pathway is through the
binding of 1α,25(OH)2D and/or its analogs to cytosolic and membrane VDR, which
initiates a phosphorylation cascade of mitogen-activated protein kinases (MAPK) and
extracellular signal-regulated kinase (ERK), which might participate in a cross-talk with
the genomic pathway to modulate gene expression [37-39]. In conclusion, VDR is
considered a ligand-induced receptor that controls the expression of more than a thousand
genes, many of whom are involved in cell division, differentiation, and growth.
The literature is rich with considerable data for the role for vitamin D in bone and
mineral homeostasis [40, 41], however; in the late 1970’s, the discovery of VDR among
various types of tissues, other than bone and small intestine, has provided new insights to
the non-traditional roles of vitamin D in the immune system regulation [42], cancer [43-
45], CVD [46, 47] and diabetes [48, 49]. Moreover, the cloning of CYP27B1 in various
tissues has provided more evidence that vitamin D activation is not only limited to the
functions including: intestine, bone tissues and kidneys, as well as some immune cells,
namely, kidney, but rather 1α-hydroxylase is locally expressed where vitamin D is
needed including: (1) regulating the proliferation of normal cells such as the

26
keratinocytes; (2) regulating hormone secretion such as PTH, insulin, and growth
hormone; (3) regulating both adaptive and innate immunity [50].
The Association between Vitamin D Deficiency and CVD Risk Factors
Vitamin D deficiency is considered a global epidemic. It has been estimated that
more than one billion people have vitamin D concentration that are considered,
minimally, insufficient [26, 29, 51-53]. Thus far, there is no agreement within the medical
and/or scientific area on defining optimal levels of 25(OH)D. However, most scientists
define sufficient serum 25(OH)D concentration as above 75 nmol/L; insufficient as 50-75
nmol/L; deficient as below 50 nmol/L; and severely deficient as below 25 nmol/L [26, 54-
56]. In the US, 48% of young white girls in Maine and 52% of Hispanic adolescents in
Boston were found to be vitamin D deficient [57, 58]. Another report indicated that
among Hispanics, Puerto Ricans had the highest prevalence of vitamin D deficiency, 26%
[59]. Interestingly, another report investigated the levels of vitamin D concentration
among Puerto Ricans in Puerto Rico and found that about 55% of their sample had
vitamin D concentration >70 nmol/L, 31% had levels between 50 and 70 nmol/L, and
14% had levels below 50 nmol/L [60]. In the Middle East, vitamin D deficiency ranges
between 30 to 50% among adults [26]. A recent report from Scotland indicated that high
percentages of healthy adults were vitamin D deficient, 29%, or severely deficient, 34.5%
[61].
Aside from increased risk of osteoporosis and lower bone mineral density [40],
vitamin D deficiency has been associated with increased risk of several illness including
CVD and hypertension [20, 23, 62]; cancer, including breast and prostate [45, 63];

27
obesity and related metabolic disorders such as type-2-diabetes [48, 64]; sarcopenia and
muscle weakness [65, 66]; and multiple sclerosis [67]. In the last decade, a wide range of
scientific evidence has linked vitamin D deficiency to increased risk of CVD. First, a
number of large, nonrandomized, prospective studies have documented that vitamin D
deficiency was associated with CVD morbidity and mortality. The Framingham
Offspring Study showed that the incidence of CVD was higher among individuals whose
serum 25(OH)D concentration was below 37 nmol/L [68]. The Luric study showed that
participants whose 25(OH)D concentration was in the lowest quartile (median=19
nmol/L) or the second lowest (median=33 nmol/L) had high adjusted risk for CVD
mortality, relative to those in the highest quartile (median=71 nmol/L), 122% and 82%
risk, respectively [69]. A meta-analysis showed that vitamin D supplementation, ranging
between 300 and 2000 IU/day, was associated with lower total mortality, relative risk
(RR) = 0.93 (95% CI:0.87-0.99) [70].
Proposed Mechanisms of Anti-Inflammatory Actions of Vitamin D
Several studies have documented that vitamin D exerts anti-proliferative and pro-
differentiating effects on many types of normal and malignant cells [71, 72]. One of the
proposed mechanisms for the association of calcitriol with atherosclerosis is through the
increased expression of MAP kinase phosphatase-5 (MKP5) which, in turn,
dephosphorylates and, thereby, inactivates MAPKs, such as p38 and the stress-activated
protein kinase Jun-N-terminal kinase (JNK). This action leads to a decrease in the
production of pro-inflammatory cytokines such as IL-6 [4]. Another proposed mechanism

28
is through inhibition of nuclear-factor-κB (NF-κB) activation and signaling, which is a
major modulator of inflammatory and immune response, through increasing the
expression of IκB protein and activating IKB kinase (IKKB) [73]. The activation of
NFκB is accompanied with increased expression of a wide range of inflammatory
cytokines, such as IL-6, IL-8, and TNFα [73, 74]. One recent study, by Talmor and
collaborators, showed that in vitro calcitriol lowered the activity of NF-κB and p38, and
the expression of ICAM and IL-6 [75]. Table 1 illustrates several in vivo experimental
murine studies using ApoE-/- mice that investigated the effects of different vitamin D
analogs on atherosclerosis.
The association between vitamin D and adiposity, in general, and body fat, in
particular, was explained by Lumb and colleagues in 1971. They were the first to
introduce the hypothesis of vitamin D sequestration in adipose tissue and muscle [76].
Later, they were able to substantiate that prior hypothesis and confirm the link between
adiposity and vitamin D [77]. Subsequently, Wortsman and colleague confirmed the
aforementioned premise, stating that due to vitamin D deposition within adipose tissue,
the bioavailability of serum 25(OH)D and 1,25(OH)2D is lowered, leading to vitamin D
insufficiency/deficiency and higher PTH. They showed that obese people evidence, lower
[48].

29
Table 1: List of studies of calcitriol and analogs on atherosclerosis using ApoE-/- mice
Author Hypothesis Treatme
nt Animals
Treatmen
t Dose
Becker et, al. 2011 [78]
aortic wall *19-nor *1,25D3
ApoE-/- (n=16/trmt)
IP5x /wk for 10 wks
*19-norc�0.1 ug/kg
*1,25D3 �0.03 µg/kg
Husain et, al. 2010 [79]
atherosclerosis *9-nor
*Enalapril
ApoE-/- females
n=12/trmt
IP 3x/wk for 16 wks
*19-norc�200 ng
*Enlp�30mg/kg
Takeda et, al. 2010 [80]
atherosclerosis 1,25D3
only ApoE-/- n=6-9/trmt
Oral 2x/wk for
12 wks
20 ng 200 ng (10 ug/kg)
Wang et, al, 2011
Oxidative stress and proinflamm
cytokines 1αD2
NON mice (males)
n=12/trmt
IP for 28 wks
1αD2 �125 ng/kg
Wang et, al, 2011 [81]
Oxidative stress and proinflamm
cytokines 1αD2
NON mice males
n=12/trmt
IP for 28 wks
1αD2 �125 ng/kg

30
PRELIMINARY STUDIES
The BPRHS is an ongoing longitudinal study that follows 1505 older Puerto
Ricans in the Greater Boston Area. For the analyses we are presenting here, we used the
baseline and 2-year data time points. Complete baseline serum 25(OH)D concentration
and dietary vitamin D intake assessments were available for 1432 participants, 1004
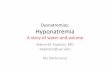
women (mean age =57.3 years) and 428 men (mean age = 56.6 years). Figure 13 shows
the prevalence of serum 25(OH)D concentration among the participants of BPRHS. The
majority of these Puerto Rican men and women (~75%) were considered vitamin D
deficient, with concentration below 50 nmol/L, whereas only 4.2-3% had sufficient serum
25(OH)D concentration of vitamin D, with levels above 75 nmol/L.
Women had significantly lower scores for serum albumin, serum creatinine,
systolic and diastolic blood pressure, HCY, VLDL-C, TG, and physical activity, but
significantly higher scores for BMI, HDL-C, TC, LDL-C, and poverty rate. Compared to
men, more women are taking supplements with a higher content of vitamin D -above 200
international units (IU) as well higher dietary intake of energy-adjusted total vitamin D
relative to men. No differences were observed between men and women for glycosylated
hemoglobin, fasting glucose, waist circumferences or Homa-IR (Table 2).
Analysis of dietary data shows that Puerto Rican women have significantly higher
carbohydrate intake, with more of their calories deriving from carbohydrates compared to
Puerto Rican men. On the other hand, the women tend to have significantly lower total
energy and dietary cholesterol intakes than do Puerto Rican men; also, a lower portion of
the women’s energy derives from fat sources compared to that for Puerto Rican men.

31
However, no significant differences were found by sex when dietary fiber and total fat
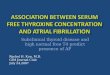
were compared (Table. 3). Figures 6 and 7 show the baseline association between serum
concentration and deciles of median intake of vitamin D from food and supplements
among all participants (n=1416). There was a wide range of vitamin D intake, 201 to 599
IU/day, when vitamin D supplements are included with food sources (Figure 6). On the
other hand, the range was very narrow when considering only the food sources of vitamin
D, 208 to 217 IU/day (Figure 7). Food products made from whole milk, 2% milk, and 1%
milk constituted 34% of vitamin D sources due to fortification with vitamin D. Fish
ranked second, constituting 16.2% of the vitamin D source. Eggs and ready-to-eat cereal
were fourth and fifth respectively, contributing about 4.5% and 4.3% of dietary vitamin D
intake (Table 3).
Figure 5: The percent of BPRHS women and men in two age groups, with serum 25(OH)D concentration (n=1495): deficient (<50 nmol/L), insufficient (50-75 nmol/L) or sufficient (>75 nmol/L).
0
10
20
30
40
50
60
70
80
40-60 yrs 60-75 yrs 40-60 yrs 60-75 yrs
Women Men
Per
cen
tage
Deficient
Insufficient
Sufficient

32
Table 4 shows the breakdown of age-adjusted means of serum 25(OH)D
concentration by different population factors. In general, the use of vitamin D-containing
supplements was associated with higher overall serum 25(OH)D concentration: our
results show that both Puerto Rican men and women who consume minimal daily
supplements (200 IU) vitamin D had significantly greater serum 25(OH)D concentration
compared to non-users: 50.1 and 47.0 nmol/L, respectively (P for trend <0.0001). We
observed a significant decreasing trend concentration across the four seasons, starting
from the summer toward spring season (P for trend <0.0001). Puerto Rican women aged
60-75 years had significantly higher serum 25(OH)D concentration compared to those
aged 45-59 yr: 45 and 42.1 nmol/L, respectively (P-value 0.009). On the other hand,
women with higher BMI had significantly lower serum 25(OH)D concentration (P for
trend 0.05). In addition, past and current female smokers had significantly lower
25(OH)D concentration (P for trend 0.04) compared to those who have never smoked.
30
35
40
45
50
55
20
8.5
20
9.5
21
0
21
0.5
21
1
21
1.5
21
2
21
3
21
4
21
7
Se
rum
25
(OH
)D n
mo
l/L
Median Vitamin D intake IU/day by deciles
from food sources only
Figure 6 & 7: The association between vitamin D intake from food & supplement (left) and food only sources (right) and serum 25(OH)D concentration from baseline (n=1416) BPRHS participants. The LS-means adjusted for age, sex, and seasonality are plotted against the median for each decile group of energy-adjusted vitamin D intake.
30
35
40
45
50
55
20
9
21
0
21
1
21
1.5
21
3
21
5
21
9.5
39
9.5
40
3
59
9.5
Se
rum
25
(OH
)D n
mo
l/L
Median Vitamin D intake IU/day by
deciles from food & supplement sources

33
Moreover, women, but not men, showed a significant increasing trend in serum 25(OH)D
concentration with increased physical activity score (P for trend 0.02). Among men,
lower concentration of serum albumin was associated with significantly lower serum
25(OH)D concentration: 32 and 44 nmol/L, respectively (P-value 0.05). Although higher
alcohol intake appeared to correlate with lower serum 25(OH)D among men as well as
women, this did not reach statistical significance. Finally, there was no significant
relationship between serum 25 (OH) D concentration, and activities of daily living (ADL)
for either men or women.
Known and potential factors that influence serum 25(OH)D concentration were
used to construct linear regression models (Table 5). The multiplicative interaction of sex
with age was highly significant (P<0.0001), thus models are presented separately for men
and women. In the fully adjusted model for women, serum 25(OH)D concentration was
significantly lower, by 0.15 nmol/L, for each year of age (P = 0.03). Lower concentration
were observed in winter and spring, -5.0 and -8.4 nmol/L, respectively (P= 0.0006 and <
0.0001) relative to summer. Higher BMI was associated with significantly lower
concentration, - 0.21 nmol/L (P< 0.0001 for each BMI unit). Serum 25(OH)D
concentration was 0.8 nmol/L greater for each IU difference in dietary vitamin D
(P<0.0001). Use of vitamin D-containing supplements was independently associated with
higher serum concentration (P<0.0001). Supplements containing vitamin D in the range
of 200-400 IU/day or > 400 IU/day, were associated with significant higher serum
25(OH)D concentration—to 5.0 and 11.1 nmol/L respectively—vs. no supplement use
(P<0.0001). Serum albumin was also associated with higher serum vitamin D
concentration (P= 0.008). Women who never smoked had significantly higher serum

34
concentration, 3.4 nmol/L compared to currently smoking women (P =0.01). Serum
creatinine, physical activity score, and alcohol intake were not significantly associated
with serum 25(OH)D concentration in women..
For men, seasonality was associated with similar decreasing serum 25(OH)D
concentration as seasons moved away from the summer season, but the reduction was
more pronounced than in women: the winter and spring levels were -11.6 and -12.3
nmol/L lower, respectively, (P< 0.0001 for each difference). Supplements with 200-400
IU/day of vitamin D (but not those >400 IU/day) were associated with serum 25(OH)D
concentration 9.0 nmol/L higher than non-users concentration (P<0.0001). In addition, as
reported above for women, serum albumin was independently associated with higher
serum 25(OH)D concentration (P= 0.003). In men, age, BMI, dietary intake of vitamin
D, and smoking did not contribute to serum 25(OH)D concentration, unlike changes seen
in women; nor was there any associations with the serum creatinine, physical activity
score, or alcohol intake.

35
TABLE 2 Descriptive characteristics of the BPRHS participants a
Covariates Women
(n=1048)
Men
(n=447) P-valueb
Age (years) 57.3 ± 7.5 56.6 ± 8.0 0.08b
Education (below 8th grade %) 48.0 44.0 0.1 c
Poverty (%) 62.0 51.0 0.0002 c
BMI (kg/m2) 33.0 ± 7.0 29.6 ± 5.2 <0.0001b
Waist (cm) 102.0 101.5 0.7
Serum Albumin c (g/L) 42.5 ± 7.0 43.2 ± 3.6 <0.0001b
Serum Creatinine c (nmol/L) 68.0 ± 27.5 87.5 ± 45.1 <0.0001b
Number of Walking Miles/day b 1.0 ± 1.4 1.3 ± 1.6 <0.0001b
Serum 25-(OH)Dc (nmol/L) 43.1 ± 16.0 43.5 ± 16.5 0.6b
Vitamin D Supplement use (> 200 IU %) 30.0 24.0 0.02c
Dietary vitamin D e.f (IU/day) 212 ± 3.0 212 ± 3.4 0.5b
Total vitamin D e,f (IU/day) 285 ± 4.5 285 ± 4.3 0.01b
Glycosylated Hemoglobin (%) 0.07 ± 2 0.07 ± 2 0.8
Fasting Glucose (mg/dL) 120± 53.0 121 ± 52.5 0.7
Homa-IR 6.03 ± 17 6.0 ± 10.2 0.004 b
LDL-C (mg/dL) 110.4 ± 34 101.0 ± 35.2 <.0001b
HDL-C (mg/dL) 47.02 ± 12.1 40.5 ± 12.4 <.0001b
VLDL-C (mg/dL) 29.3 ± 15.0 32.0 ± 19 0.007b
TG (mg/dL) 157.0 ± 99 174.0 ± 140 0.007b
Total Cholesterol (mg/dL) 188.2 ± 41 174.2 ± 43 <.0001b
Homocysteine (µmol/L) 8.45 ± 3.7 10.37 ± 5.7 <.0001b
Systolic blood pressure (mm Hg) 134.1 ± 19.2 137.1 ± 19 <.0001b
Diastolic blood pressure (mm Hg) 80.11 ± 10.4 83.0 ± 11.2 <.0001b
a Values are presented as mean ± SD unless indicated b
P-value are based on T-test, c P-value are based on chi-square test
d Range = 38.3 Total vitamin D= vitamin D from supplement + vitamin D from diet. e The recommended dietary allowance (RDA) for vitamin D for both men and women aged 19-50 years, and 51-70 years = 600 IU (15 ug /day) [82] f Adjusted for total energy

36
TABLE 3: Selected dietary intake data for the participants of the BPRHS
aMean ± standard error adjusted for age and total energy. bSignificant differences by sex (t-tests)
Women (n=1048)
Men (n=447)
P-valueb
Total Energy (kcal) 2021± 32 2367 ± 52 < 0.001b Carbohydrate (g) 273 ± 2 264 ± 3 < 0.01b
Dietary fiber (g) 18.5 ± 0.2 18.3 ± 0.3 0.06
Total Fat (g) 75.9 ± 0.5 77.0 ± 0.8 0.09
Saturated fat (g) 22.9 ± 0.2 23.1 ± 0.4 0.07
Monounsaturated fat (g) 26.2 ± 0.2 26.6 ± 0.3 0.5
Polyunsaturated fat (g) 17.7 ± 0.2 18.1 ± 0.3 0.07
Protein (g) 91.8 ± 0.7 91.2 ± 1.2 0.7
Cholesterol (mg) 298± 5 334 ± 7 < 0.001b
% Energy from Carbohydrate 52.2 ± 0.3 50.1 ± 0.5 < 0.001b
% Energy from Total Fat 32.0 ± 0.2 32.8 ± 0.3 < 0.05b
% Energy from Protein 17.4 ± 0.1 17.2 ± 0.2 0.07

37
TABLE 4: Major Dietary Sources of Vitamin D intake among Puerto Rican adultsa
Rank Food Groups % of dietary vitamin D
intake
1 Milk (whole, 2% &1% milk products)
32.4
2 Supplements 28.7 3 Fish 16.2 4 Eggs 4.5 5 Cereal, Ready-to-eat, Cold 4.3 6 Beef 2.3
7 Processed Meat, Sausage, Frank 2.1 8 Chicken/Turkey 2.0 9 Pork 1.3 10 Ice cream, Sherbet, Frozen Yogurt 1.2 11 Yogurt 1.1
12 Cheese 0.9 a Only food groups that contributed more than 0.8% of dietary vitamin D intake

38
TABLE 5 Age-adjusted means for all variables
Variables Women Men
n (%)* LSM SEM P value n (%) LSM SEM P
value
Age (y)
45-59 651 (61.5%)
42.0 0.64 281 (63.0%)
44.4 1.00
60-75 407 (38.5%) 45.0 0.81 0.007 164 (37.0%)
42.0 1.33 0.1
Vitamin D Supplement IU/day) † †‡
≤ 200 738 (70.0%) 41.1 0.6 338 (77.3%)
41.5 0.8
200 - 400 224 (21.5%) 46.5 1.1 <.0001 90 (20.5%)
51.0 1.6 <0.0001
≥400 77 (8.5%) 53.1 2.0 <.0001 9 (2.1 %) 39.2 5.36 0.9
<.0001|| <0.0001
||
Season of measurement†
Summer (July-Sept)
356 (34.5%) 44.5 0.9 137 (32.0%)
46.5 1.4
Fall (October- Dec)
264 (26.0%) 46.0 0.8 0.4 124 (29.0%)
48.7 1.4 0.6
Winter (Jan-March)
184 (18.0%) 41.1 1.2 0.05 78 (18.0%)
37.5 1.8 <0.0001
Spring (April-June)
224 (21.5%) 38.2 1.1 <.0001 91 (21.3%)
37.0 1.6 <0.0001
<.0001|| <0.0001
||
Body Mass Index (kg/m2) †
≤ 25 114 (11.0%) 44.0 1.5 80 (18.5%)
43.5 2.0
25-30 282 (27.3%) 45.5 0.9 0.8 164 (37.5%)
44.0 1.3 0.9
30-35 307 (29.3%) 44.5 0.9 0.9 130 (30.2%)
43.0 1.5 0.9
≥ 35 307 (29.3%) 44.5 0.9 0.08 130 (30.2%)
43.0 1.5 0.9
0.001 || 0.9
||
Smoking Status†

39
No 832 (79.5%) 44.0 1.1 291 (66.0%)
44.0 1.0
Yes 217 (20.5%) 41.0 0.5 0.01 149 (34.0%)
43.0 1.4 0.6
Alcohol Intake†
No 675 (64.5%) 43.0 0.7 211 (49.0%)
44.5 1.2
Yes 376 (35.5%) 44.0 0.8 0.4 228 (51.0%)
43.0 1.1 0.2
Serum Albumin† (g/L)
< 38 49 (5%) 42.0 2.2 16 (4.0%)
35.0 4.0
≥ 38 964 (95%) 43.1 0.5 0.5 410 (96.0%)
44.0 0.8 0.03
Serum Creatinine (nmol/L) †•
35.5 - 61.0 280 (27.5%) 41.5 1.0 19 (4.5%)
34.5 4.0
62.0 -70.0 298 (29.0%) 42.5 1.0 0.6 46 (11.0%)
40.0 2.4 0.3
71.0 -79.5 223 (22.0%) 45.3 1.1 0.009 92 (21.5%)
42.0 2.0 0.1
80.0 - 698 221 (22.0%) 44.1 1.1 0.1 270 (63.0%)
45.3 1.0 0.01
0.02 || 0.009
||
Miles Walked/day†
0 mile/day 263 (25.0%) 41.3 1.1 52 (12.0%)
40.5 2.4
0- 0.5 mile/day 395 (38.0%) 42.5 0.8 0.5 140 (32.0%)
44.0 1.4 0.3
> 0.5 mile/day 367 (37.0%) 45.0 1.0 0.01 247 (56.3%)
44.0 1.1 0.3
0.01 || 0.4
||
1P-value for individual comparisons to the referent group that is based on Dunnett
multiple testing. 2 P-value for Trend.*Quintiles; **Quartiles
3 Reference group, P-values are calculated with Dunnett adjustment for multiple comparisons.

40
TABLE 6 Multiple linear regression, stratified by sex (n= 1542)
Variable Women (n=966) Men (n=404)
β SE P-value β SE P-value
Age 0.15 0.07 0.03 -0.13 0.1 0.2
Seasons (Fall vs. summer) -1.6 1.3 0.1 -3.0 2.0 0.1
(Winter vs. Summer) -5.0 1.4 0.0006 -11.6 2.3 <0.0001
(Spring vs. Summer) -8.40 1.3 <0.0001 -12.3 2.2 <0.0001
BMI -0.21 0.07 0.006 0.02 0.15 0.8
vitamin D supplement use
(200-400 IU vs. None)
5.0 1.1 <0.0001 9.0 2.0 <0.0001
(> 400 IU vs. None) 11.1 2.0 <0.0001 -1.0 5.2 0.8
Energy-adjusted dietary vitamin D
(IU/day)
0.8 0.2 <0.0001 0.25 0.2 0.2
Serum Creatinine (nmol/L) 0.01 0.01 0.5 0.01 0.01 0.4
Serum Albumin (g/L) 0.4 0.1 0.008 0.64 0.2 0.003
Physical activity score 0.15 0.12 0.2 -0.10 0.13 0.4
Smoking (Never vs. Current) 3.4 1.3 0.01 -0.5 2.0 0.7
(Past vs. Current) 2.2 1.5 0.1 0.15 2.0 0.9
Alcohol (Never vs. Heavy) 3.8 2.5 0.1 3.6 2.3 0.1
(Moderate vs. Heavy) 4.6 2.5 0.07 3.2 2.4 0.1

41
RESEARCH DESIGN AND METHOOLOGY
The work presented in this dissertation involves collaboration among
investigators with expertise in nutritional epidemiology and biochemistry, and statistical
methodologies for clinical research. Using epidemiologic methods, we aimed to
understand the association of between vitamin D status and CVD risk factors among
Puerto Rican adults in Boston.
The parent study for the epidemiologic analyses is the Boston Puerto Rican
Health Study, an ongoing longitudinal study to examine the associations among social
and psychological stress, nutrition, allostatic load, and measures of depression, cognitive
function, and physical disability in a cohort of older Puerto Ricans, aged 45-75 years,
living in the Greater Boston, MA. Consenting participants returned to the Human
Nutrition Research Center on Aging (HNRCA) at Tufts University at the end of 2 years
for measurements of bone and body composition. For this analysis there were 1505
observations from baseline, 1276 observations from a 2-year time point, and 970 bone
and body composition measurements.
Study Population and Data Collection
Participants were identified from areas of high Hispanic density in the Boston
metropolitan area, as specified in the year 2000 Census. Blocks with 10 or more Hispanic
persons aged 45 and older were selected for enumeration from census tracks that contain
at least 25 Puerto Rican adults in the specified age range. After complete block
enumeration (blocks were visited up to 5 or 6 times, and on weekends and evenings to

42
maximize identification of all relevant households), households with at least one Puerto
Rican adult between the ages of 45-75 years were identified; one qualified individual was
randomly selected from each household, and invited to participate. Only those
participants who were unable to answer questions due to serious health conditions or who
were not able to provide reliable information for other reasons such as dementia or
alcoholism, were excluded from participation [83].
Data Collection
Baseline and 2-year visit: Informed consent was obtained during the baseline
interview, and neuropsychological tests were conducted to identify participants who
might require assistance (e.g., from a proxy); participants were excluded if their mini
mental state examination score was <10. Enrolled participants completed additional
questionnaires to capture information on general background and socioeconomic status,
dietary intake, food security, health history, health behaviors, health insurance, medical
conditions and use of medication, activities of daily living instrument, migration status,
stress, depressive symptomology, and cognitive function. Moreover, anthropometric and
blood pressure measures, and physical function tests, were completed. Participants were
provided with urine collection containers, two saliva tubes with procedures for collection,
and instructions for the next day’s 12-hour-fasting blood draw. The next day, a
phlebotomist collected 12-hour fasting blood, urine, and saliva samples. Samples were
analyzed at the Nutrition Evaluation Laboratory (NEL) at Tufts University; blood
samples were immediately cooled to 4oC and plasma separated within 4 hours in a
refrigerated centrifuge.

43
Bone visit protocol: During the 2-year follow-up visit, an appointment was made
for participants to visit the HNRCA to obtain bone density and body composition
measurements and an additional blood draw, and to complete additional questionnaires
on sun exposure, family history of osteoporosis, and history of fracture. Participants were
provided with written instructions for the urine collection, taking PABA tablets, and for
fasting. Two days before their scheduled visit, participants received a reminder phone call
and reinforced instructions for urine collection and overnight fasting. They were asked to
complete the 24-hour urine collection in two containers, one for each 12 hours. All
laboratory measurements for this study were performed by the NEL.
Covariates Assessments and Definition
Serum 25(OH)D concentration was measured with an 125I radioimmunoassay kit
(DiaSorin Inc, Stillwater, MN 55082) as specified by the manufacturer (68100E). Overall
adiposity was assessed from whole-body DXA scans (DXA; Lunar Prodigy; GE
Healthcare, Madison, WI) measured during the bone visit. Regional body composition
measures (android fat mass (grams and %), gynoid fat mass (grams and %), and
android/gynoid fat mass ratio were assessed with use of ENCORE software, version 12.2.
Weight, and waist and hip circumferences were measured in duplicate. Weight was
measured using a clinical scale (Toledo Weight Plate, Model I5S, Bay State, and Systems
Inc. Burlington, MA). Knee height was measured with a Harpenden pocket stadiometer
(also used for standing height). Knee height was used to estimate standing height for
participants who could not stand, or who had a spinal curvature. Body mass index (BMI)
was calculated as weight (kg) divided by height (m) squared [84, 85].

44
Laboratory Assays
Serum high sensitivity C-reactive protein (hsCRP) was measured with a solid-
phase, enzyme-labeled chemiluminescentimmunometric assay (Immulite 1000,
Diagnostic Products Corporation (DCP) Los Angeles, CA 90045-5597), as specified by
the manufacturer (PILKCR-7, 2003-11-25). The intra- and inter-assay CV% were 6.0%
and 7.3% respectively.
Serum TNF-α & IL-6 were each measured by non-cross-reacting enzyme-linked
immunoassays (ELISA), with use of monoclonal and polyclonal antibodies for the
analysis of specific cytokine antigens (Quantikine ELISA, R&D Systems, Minneapolis,
MN, USA). At the NEL, for IL-6, the intra-assay CV% is (1.6-4.2%) and the inter-assay
CV% is (3.3-6.4%). For TNF-α, the intra-assay CV% is 5.3-8.8% and the inter-assay
CV% is (10.8-16.7%). Plasma cholesterol was measured with EDTA plasma using an
enzymatic endpoint reaction in a Cobas Mira Analyzer with Roche Diagnostics Item
#44307. Ciba Corning Normal and Abnormal assayed control serum (Items #9702 and
#9705) and Sigma Diagnostics elevated lipid control (Item #L1008) were used as controls
[86]. HDL-C (mg/dL) was analyzed using EDTA plasma with the enzymatic endpoint
reaction in a Cobas Mira Analyzer with Roche Diagnostics (Item #44120), and was
calibrated with a Roche Diagnostics Cobas Calibrator with Roche Diagnostic Cholesterol
Reagent (Item#44307) Dextran Sulfate-Magnesium Precipitating Reagent. The standard
was Roche Diagnostics Cobas Calibrator Serum, (Item #44157), and the controls were
Sigma Assayed Bi-Level HDL-C Cholesterol Controls, (Items #H4009 and #H5009)
(Allan, Poon et al. 1974; Warnick, Benderson et al. 1982). LDL-C was calculated with
use of the Friedewald formula, except in the cases when triglyceride (TG) concentration

45
exceed 400 mg/dL [87]. TG was analyzed with an enzymatic endpoint reaction on the
Olympus AU400e with Olympus Triglyceride Reagents (OSR6033) (Olympus America
Inc., Melville, NY).
Potential Covariates:
Potential covariates include age (continuous), sex (categorical), socio-
demographic parameters such as education (categorical), income (continuous), smoking
status (categorical), alcohol intake (categorical), total energy intake (continuous),
physical activity (continuous /categorical). Information was obtained from all participants
on the following variables: age, education, and household income. This questionnaire was
designed based on questions from NHANES III [88], HHANES [89], the National Health
Interview Survey Supplement on Aging [90], and refined during our previous field
experience. Health-related behaviors: Information about current and past use of alcohol
and smoking and about physical activity were obtained. Seasonality was defined as
follows: July to September was coded as summer, October to December as fall, January
to March as winter, and April to June as spring.
Diabetes was considered present if fasting blood glucose exceeded 125 mg/dL or
if the participant was being treated with insulin or oral hypoglycemic agents. Serum
glucose was measured at baseline and 2 years, using an enzymatic, kinetic reaction on the
Olympus AU400e with Olympus Glucose Reagents (Olympus America Inc., Melville,
NY) at the NEL.

46
Data Entry and Quality Control
Participants were coded with a subject identification number. All data were
entered and managed at the BPRHS center at Northeastern University on password-
protected computers. Data entry reports were generated periodically to detect and
minimize missing data and data entry errors. When missing data were identified in
questionnaires, participants were contacted by phone within two weeks to retrieve the
information. Data were backed up each day and stored on our central server using unique
subject identification numbers.
Power and sample size:
The BPRHS study is ongoing and currently has baseline and 2 year-data through
home visits on 1502 and 1276, participants, respectively. In addition, we have bone and
body composition measurements on 970 subjects. The proposed sample size estimates
were selected to assure that we have at least 90% power to detect expected associations
that are reliable but consistent with published studies. We derived our sample size
estimates and the estimated power from the standard normal approximation to the Fisher
logarithmic transformation for linear correlations, which are likely conservative given
that multiple linear regression models generally provide greater precision, smaller
standard errors, and greater power.

47
STATISTICAL ANALYTICAL PLAN
Analyses were conducted with SAS© version 9.3 (SAS Institute Inc., Cary, NC).
Formal hypothesis testing was two-sided, with a nominal type I error of 0.05. We
assessed the modeling assumptions of non-linearity, and potential outliers and influential
data were considered. Plots and graphs were used to summarize the distributions of
primary analytic variables and other descriptive data. For all aims, results were
summarized using regression estimates, p-values, and 95% CI. Geometric means are
reported for log-transformed variables. Analyses were adjusted for covariates, including
sex, age, seasonality, etc. Potential confounding and effect modifiers were checked for by
including interaction term into the regression model. For continuous data, independent
sample t-tests were employed; for categorical data, chi-square test for differences in
proportions was employed. Only participants who met the eligibility criteria for the
intervention and with complete data for the primary analytical variables were included in
this analysis. Table 7 lists variables included in our statistical models.

48
TABLE 7 Summary of calculated outcome measures and covariates
Variables Measurement
Factor
Technique
Predictor variable
Exposure Serum 25(OH)D concentration (nmol/L)
Continuous /categorical
ELISA
Outcome variables
Pro-inflammatory cytokines
IL-6 (mg/L) TNF-α hsCRP
continuous 10 20 20
ELISA
Adiposity BMI WC TBF
continuous 10 20 20
Measurement tools DXA
Lipid profile
HDL-C (mg/dL) TC LDL-C TG
continuous
10 20 20 20
Lipid concentration
Covariates
Other blood measure
Albumin (g/L) Creatinine (µmol/L) Parathyroid hormone White blood cell counts Seasonality (blood drawn)
Continuous/ categorical
Kinetics
Demographics
Age Sex education poverty
categorical/ continuous
Designated questionnaire & measurement tools
Health and Life Style Factors
Smoking (y/n) Alcohol (gm/day) physical activity level # Blocks walking/day
categorical/ continuous
CVD
Systolic BP Diastolic BP Heart disease CVD medications
continuous categorical
Vitamin D intake Vitamin D dietary Vitamin D supplement
continuous FFQ

49
The Specific Aims
Specific Aim One: To evaluate the association between baseline serum 25(OH)D
concentration (nmol/L) and lipid profile constituent concentration (mg/dL), namely,
HDL-C, LDL-C, TG, and TC over time.
Primary Hypothesis One: lower serum 25(OH)D concentration is associated with 2.5
year change in HDL-C concentration.
Specific Aim Two: To evaluate the association between serum 25(OH)D concentration
with IL-6, TNF-α, and hsCRP.
Primary Hypothesis Two: lower serum 25(OH)D concentration is associated with higher
circulating levels of inflammatory markers.
Specific Aim Three: to evaluate the association between serum 25(OH)D concentration
and adiposity.
Primary Hypothesis Three: lower serum 25(OH)D concentration is associated with
higher adiposity as measured by BMI, and as a secondary aim, by waist circumference
(WC).
Specific Aim Four: to evaluate the cross-sectional association between serum 25(OH)D
concentration with total and regional adiposity
Primary Hypothesis Four: lower serum 25(OH)D concentration is associated with
higher total and regional adiposity measures as measured by dual-energy x-ray
absorptiometry (DXA), including total body fat (TBF).

50
FIGURE 8 Diagram illustrates the relationship between serum 25(OH)D and the various
CVD risk factors

51
BIBLIOGRAPHY
1. Organization, W.H., Cardiovascular diseases (CVDs), in Fact sheet N°3172011,
WHO: Geneva.
2. Balagopal, P., et al., Nontraditional Risk Factors and Biomarkers for
Cardiovascular Disease: Mechanistic, Research, and Clinical Considerations for
Youth. Circulation, 2011. 123(23): p. 2749-2769.
3. Lusis, A.J., Atherosclerosis. Nature, 2000. 407(6801): p. 233-241.
4. Krishnan, A.V. and D. Feldman, Mechanisms of the anti-cancer and anti-
inflammatory actions of vitamin D. Annual review of pharmacology and
toxicology, 2011. 51: p. 311-36.
5. Tomaschitz, A., et al., Independent association between 1,25-dihydroxyvitamin D,
25-hydroxyvitamin D and the renin–angiotensin system: The Ludwigshafen Risk
and Cardiovascular Health (LURIC) study. Clinica Chimica Acta, 2010. 411(17–
18): p. 1354-1360.
6. Vacek, J.L., et al., Vitamin D Deficiency and Supplementation and Relation to
Cardiovascular Health. The American Journal of Cardiology, 2012. 109(3): p.
359-363.
7. Sherry L. Murphy, B.S.J.X., M.D.; and Kenneth D. Kochanek, M.A., Deaths:
Preliminary Data for 2010, in National Vital Statisictis Report2012, CDC:
Division of Vital Statistics.
8. Writing Group, M., et al., Heart disease and stroke statistics--2010 update: a
report from the American Heart Association. Circulation, 2010. 121(7): p. e46-
e215.
9. Members, W.G., et al., Executive Summary: Heart Disease and Stroke Statistics—
2011 Update. Circulation, 2011. 123(4): p. 459-463.
10. Wilson, P.W. and B.F. Culleton, Epidemiology of cardiovascular disease in the
United States. American Journal of Kidney Diseases, 1998. 32(5 Suppl 3).
11. Lloyd-Jones, D.M., et al., Lifetime risk for developing congestive heart failure:
the Framingham Heart Study. Circulation, 2002. 106(24): p. 3068-72.

52
12. Tedgui, A. and Z. Mallat, Cytokines in Atherosclerosis: Pathogenic and
Regulatory Pathways. Physiological Reviews, 2006. 86(2): p. 515-581.
13. Ross, R., Atherosclerosis is an inflammatory disease. Am Heart J, 1999. 138: p.
S419-20.
14. Davignon, J. and P. Ganz, Role of Endothelial Dysfunction in Atherosclerosis.
Circulation, 2004. 109(23 suppl 1): p. III-27-III-32.
15. Lind, L., Lipids and endothelium-dependent vasodilation—A review. Lipids,
2002. 37(1): p. 1-15.
16. Almirall, J., et al., Association of low serum 25-hydroxyvitamin D levels and high
arterial blood pressure in the elderly. Nephrology Dialysis Transplantation, 2010.
25(2): p. 503-9.
17. Ameri, P., et al., High prevalence of vitamin D deficiency and its association with
left ventricular dilation: an echocardiography study in elderly patients with
chronic heart failure. Nutrition Metabolism & Cardiovascular Diseases, 2010.
20(9): p. 633-40.
18. Baz-Hecht, M. and A.B. Goldfine, The impact of vitamin D deficiency on diabetes
and cardiovascular risk. Current Opinion in Endocrinology, Diabetes & Obesity,
2010. 17(2): p. 113-9.
19. Bostick, R.M., et al., Relation of calcium, vitamin D, and dairy food intake to
ischemic heart disease mortality among postmenopausal women. American
Journal of Epidemiology, 1999. 149(2): p. 151-61.
20. Giovannucci, E., et al., 25-hydroxyvitamin D and risk of myocardial infarction in
men: a prospective study. Archives of Internal Medicine, 2008. 168(11): p. 1174-
80.
21. Oh, J., et al., 1,25(OH)2 Vitamin D Inhibits Foam Cell Formation and Suppresses
Macrophage Cholesterol Uptake in Patients With Type 2 Diabetes Mellitus.
Circulation, 2009. 120(8): p. 687-698.
22. Sugden, J.A., et al., Vitamin D improves endothelial function in patients with Type
2 diabetes mellitus and low vitamin D levels. Diabet Med, 2008. 25(3): p. 320-5.

53
23. Deshpande, D.D., D.R. Janero, and M.M. Amiji, Therapeutic strategies for
endothelial dysfunction. Expert opinion on biological therapy, 2011. 11(12): p.
1637-54.
24. Ridker, P.M., Clinical application of C-reactive protein for cardiovascular
disease detection and prevention. Circulation, 2003. 107(3): p. 363-9.
25. Shishehbor, M.H. and D.L. Bhatt, Inflammation and atherosclerosis. Current
Atherosclerosis Reports, 2004. 6(2): p. 131-9.
26. Holick, M.F., Vitamin D deficiency. N Engl J Med, 2007. 357(3): p. 266-81.
27. Armas, L.A., B.W. Hollis, and R.P. Heaney, Vitamin D2 is much less effective
than vitamin D3 in humans. Journal of Clinical Endocrinology & Metabolism,
2004. 89(11): p. 5387-91.
28. Holick, M.F., et al., The vitamin D content of fortified milk and infant formula. N
Engl J Med, 1992. 326(18): p. 1178-81.
29. Holick, M.F., High prevalence of vitamin D inadequacy and implications for
health. Mayo Clin Proc, 2006. 81(3): p. 353-73.
30. Holick, M.F., Resurrection of vitamin D deficiency and rickets. J Clin Invest,
2006. 116(8): p. 2062-72.
31. Holick, M.F., Deficiency of sunlight and vitamin D. Bmj, 2008. 336(7657): p.
1318-9.
32. Ramos-Lopez, E., et al., CYP2R1 (vitamin D 25-hydroxylase) gene is associated
with susceptibility to type 1 diabetes and vitamin D levels in Germans.
Diabetes/Metabolism Research and Reviews, 2007. 23(8): p. 631-636.
33. Rhieu, S.Y., et al., A new insight into the role of rat cytochrome P450 24A1 in
metabolism of selective analogs of 1alpha,25-dihydroxyvitamin D. Archives of
biochemistry and biophysics, 2011. 509(1): p. 33-43.
34. Prosser, D.E. and G. Jones, Enzymes involved in the activation and inactivation of
vitamin D. Trends in biochemical sciences, 2004. 29(12): p. 664-73.
35. Cheng, J.B., et al., Genetic evidence that the human CYP2R1 enzyme is a key
vitamin D 25-hydroxylase. Proceedings of the National Academy of Sciences of
the United States of America, 2004. 101(20): p. 7711-5.

54
36. Jones, G., Pharmacokinetics of vitamin D toxicity. The American Journal of
Clinical Nutrition, 2008. 88(2): p. 582S-586S.
37. Deeb, K.K., D.L. Trump, and C.S. Johnson, Vitamin D signalling pathways in
cancer: potential for anticancer therapeutics. Nature reviews. Cancer, 2007. 7(9):
p. 684-700.
38. Plum, L.A. and H.F. DeLuca, Vitamin D, disease and therapeutic opportunities.
Nat Rev Drug Discov, 2010. 9(12): p. 941-55.
39. POLLY, P., et al., VDR-Alien: a novel, DNA-selective vitamin D3 receptor-
corepressor partnership. The FASEB Journal, 2000. 14(10): p. 1455-1463.
40. Holick, M.F., Evolution and function of vitamin D. Recent Results Cancer Res,
2003. 164: p. 3-28.
41. Holick, M.F., The influence of vitamin D on bone health across the life cycle. J
Nutr, 2005. 135(11): p. 2726S-7S.
42. Etten, E.v. and C. Mathieu, Immunoregulation by 1,25-dihydroxyvitamin D3:
Basic concepts. The Journal of Steroid Biochemistry and Molecular Biology,
2005. 97(1–2): p. 93-101.
43. Bertone-Johnson, E.R., et al., Plasma 25-hydroxyvitamin D and 1,25-
dihydroxyvitamin D and risk of breast cancer. Cancer Epidemiol Biomarkers
Prev, 2005. 14(8): p. 1991-7.
44. Chen, T.C., et al., Prostatic 25-hydroxyvitamin D-1alpha-hydroxylase and its
implication in prostate cancer. J Cell Biochem, 2003. 88(2): p. 315-22.
45. Chen, T.C. and M.F. Holick, Vitamin D and prostate cancer prevention and
treatment. Trends Endocrinol Metab, 2003. 14(9): p. 423-30.
46. Judd, S.E. and V. Tangpricha, Vitamin D deficiency and risk for cardiovascular
disease. American Journal of the Medical Sciences, 2009. 338(1): p. 40-4.
47. Kim, D.H., et al., Prevalence of hypovitaminosis D in cardiovascular diseases
(from the National Health and Nutrition Examination Survey 2001 to 2004).
American Journal of Cardiology, 2008. 102(11): p. 1540-4.
48. Wortsman, J., et al., Decreased bioavailability of vitamin D in obesity. The
American Journal of Clinical Nutrition, 2000. 72(3): p. 690-693.

55
49. Liel, Y., et al., Low circulating vitamin D in obesity. Calcified tissue international,
1988. 43(4): p. 199-201.
50. Michael F, H.P.D., M.D., ed. Vitamin D. Physiology, Molecular Biology, and
clinical applications. Second ed. NUTRITION AND HEALTH, ed. P. Adrianne
Bendich2010, Springer Humana Press. 1155.
51. Bischoff-Ferrari, H.A., et al., Estimation of optimal serum concentrations of 25-
hydroxyvitamin D for multiple health outcomes. American Journal of Clinical
Nutrition, 2006. 84(1): p. 18-28.
52. Chapuy, M.C., et al., Prevalence of vitamin D insufficiency in an adult normal
population. Osteoporos Int, 1997. 7(5): p. 439-43.
53. Malabanan, A., I.E. Veronikis, and M.F. Holick, Redefining vitamin D
insufficiency. Lancet, 1998. 351(9105): p. 805-6.
54. Dawson-Hughes, B., et al., Estimates of optimal vitamin D status. Osteoporos Int,
2005. 16(7): p. 713-6.
55. Holick, M.F., Vitamin D status: measurement, interpretation, and clinical
application. Ann Epidemiol, 2009. 19(2): p. 73-8.
56. Holick, M.F. and T.C. Chen, Vitamin D deficiency: a worldwide problem with
health consequences. Am J Clin Nutr, 2008. 87(4): p. 1080S-6S.
57. Gordon, C.M., et al., Prevalence of vitamin D deficiency among healthy
adolescents. Arch Pediatr Adolesc Med, 2004. 158(6): p. 531-7.
58. Sullivan, S.S., et al., Adolescent girls in Maine are at risk for vitamin D
insufficiency. J Am Diet Assoc, 2005. 105(6): p. 971-4.
59. Araujo, A., et al., Serum 25-hydroxyvitamin D and bone mineral density among
Hispanic men. Osteoporosis International, 2009. 20(2): p. 245-255.
60. Palacios, C., et al., Determinants of vitamin D status among overweight and obese
Puerto Rican adults. Ann Nutr Metab, 2012. 60(1): p. 35-43.
61. Zgaga, L., et al., Diet, environmental factors, and lifestyle underlie the high
prevalence of vitamin D deficiency in healthy adults in Scotland, and
supplementation reduces the proportion that are severely deficient. Journal of
Nutrition, 2011. 141(8): p. 1535-42.

56
62. Michos, E.D., et al., 25-Hydroxyvitamin D deficiency is associated with fatal
stroke among whites but not blacks: The NHANES-III linked mortality files.
Nutrition, (0).
63. Freedman, D.M., et al., Serum Levels of Vitamin D Metabolites and Breast
Cancer Risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening
Trial. Cancer Epidemiology Biomarkers & Prevention, 2008. 17(4): p. 889-894.
64. Botella-Carretero, J.I., et al., Vitamin D deficiency is associated with the
metabolic syndrome in morbid obesity. Clinical Nutrition, 2007. 26(5): p. 573-80.
65. Oh, J.H., et al., The level of vitamin D in the serum correlates with fatty
degeneration of the muscles of the rotator cuff. Journal of Bone & Joint Surgery -
British Volume, 2009. 91(12): p. 1587-93.
66. Visser, M., et al., Low vitamin D and high parathyroid hormone levels as
determinants of loss of muscle strength and muscle mass (sarcopenia): the
Longitudinal Aging Study Amsterdam. Journal of Clinical Endocrinology &
Metabolism, 2003. 88(12): p. 5766-72.
67. Kragt, J., et al., Higher levels of 25-hydroxyvitamin D are associated with a lower
incidence of multiple sclerosis only in women. Multiple Sclerosis, 2009. 15(1): p.
9-15.
68. Wang, T.J., et al., Vitamin D deficiency and risk of cardiovascular disease.
Circulation, 2008. 117(4): p. 503-11.
69. Pilz, S., et al., Association of Vitamin D Deficiency with Heart Failure and
Sudden Cardiac Death in a Large Cross-Sectional Study of Patients Referred for
Coronary Angiography. Journal of Clinical Endocrinology & Metabolism, 2008.
93(10): p. 3927-3935.
70. Autier, P. and S. Gandini, Vitamin D supplementation and total mortality: a meta-
analysis of randomized controlled trials. Archives of Internal Medicine, 2007.
167(16): p. 1730-7.
71. Chung, I., et al., Anti-proliferative effects of calcitriol on endothelial cells derived
from two different microenvironments. The Journal of Steroid Biochemistry and
Molecular Biology, 2007. 103(3–5): p. 768-770.

57
72. Jacques M, L., Immunomodulatory actions of 1,25-Dihydroxyvitamin D3. The
Journal of Steroid Biochemistry and Molecular Biology, 1995. 53(1–6): p. 599-
602.
73. Berk, B.C., et al., Endothelial Atheroprotective and Anti-inflammatory
Mechanisms. Annals of the New York Academy of Sciences, 2001. 947(1): p. 93-
111.
74. de Vries-van der Weij, J., et al., Anti-inflammatory salicylate beneficially
modulates pre-existing atherosclerosis through quenching of NF-κB activity and
lowering of cholesterol. Atherosclerosis, 2010. 213(1): p. 241-246.
75. Talmor, Y., et al., Calcitriol blunts pro-atherosclerotic parameters through
NFkappaB and p38 in vitro. Eur J Clin Invest, 2008. 38(8): p. 548-54.
76. Becker, L.E., et al., Effect of paricalcitol and calcitriol on aortic wall remodeling
in uninephrectomized ApoE knockout mice. American Journal of Physiology -
Renal Physiology, 2011. 300(3): p. F772-F782.
77. Husain, K., et al., Effects of Paricalcitol and Enalapril on Atherosclerotic Injury
in Mouse Aortas. American Journal of Nephrology, 2010. 32(4): p. 296-304.
78. Takeda, M., et al., Oral Administration of an Active Form of Vitamin D3
(Calcitriol) Decreases Atherosclerosis in Mice by Inducing Regulatory T Cells
and Immature Dendritic Cells With Tolerogenic Functions. Arteriosclerosis,
Thrombosis, and Vascular Biology, 2010. 30(12): p. 2495-2503.
79. Bodyak, N., et al., Activated vitamin D attenuates left ventricular abnormalities
induced by dietary sodium in Dahl salt-sensitive animals. Proceedings of the
National Academy of Sciences of the United States of America, 2007. 104(43): p.
16810-5.
80. Wang, X.X., et al., Vitamin D receptor agonist doxercalciferol modulates dietary
fat-induced renal disease and renal lipid metabolism. American Journal of
Physiology - Renal Physiology, 2011. 300(3): p. F801-F810.
81. Lumb, G.A., E.B. Mawer, and S.W. Stanbury, The apparent vitamin D resistance
of chronic renal failure: A study of the physiology of vitamin D in man. The
American Journal of Medicine, 1971. 50(4): p. 421-441.

58
82. Mawer, E.B., et al., The distribution and storage of vitamin D and its metabolites
in human tissues. Clin Sci, 1972. 43(3): p. 413-31.
83. Dietary Reference Intakes for Calcium and Vitamin D. Committee to Review
Dietary Reference Intakes for Vitamin D and Calcium. , in 2010, Institute of
Medicine: Washington, DC: National Academy of Sciences.
84. Tucker, K., et al., The Boston Puerto Rican Health Study, a longitudinal cohort
study on health disparities in Puerto Rican adults: challenges and opportunities.
BMC Public Health, 2010. 10(1): p. 107.
85. Bermudez, O.I., E.K. Becker, and K.L. Tucker, Development of sex-specific
equations for estimating stature of frail elderly Hispanics living in the
northeastern United States. American Journal of Clinical Nutrition, 1999. 69(5):
p. 992-8.
86. Chumlea, W., et al., Stature prediction equations for elderly non-Hispanic white,
non-Hispanic black, and Mexican-American persons developed from NHANES III
data. J Am Diet Assoc, 1998. 98: p. 137 - 142.
87. Daughaday, W.H. and P. Rotwein, Insulin-like growth factors I and II. Peptide,
messenger ribonucleic acid and gene structures, serum, and tissue
concentrations. Endocr Rev, 1989. 10(1): p. 68-91.
88. Allain, C.C., et al., Enzymatic determination of total serum cholesterol. Clin
Chem, 1974. 20(4): p. 470-5.
89. Friedewald, W.T., R.I. Levy, and D.S. Fredrickson, Estimation of the
concentration of low-density lipoprotein cholesterol in plasma, without use of the
preparative ultracentrifuge. Clin Chem, 1972. 18(6): p. 499-502.
90. Dreon, D., et al., Use of NHANES Data to Assign Nutrient Densities to Food
Groups in a Multiethnic Diet History Questionnaire. Nutrition and Cancer, 1993.
20: p. 223 - 230.
91. Delgado, J.L., et al., Hispanic Health and Nutrition Examination Survey:
methodological considerations. Am J Public Health, 1990. 80 Suppl: p. 6-10.

59
92. Block, G. and A.F. Subar, Estimates of nutrient intake from a food frequency
questionnaire: the 1987 National Health Interview Survey. J Am Diet Assoc,
1992. 92(8): p. 969-77.
93. Tucker, K., et al., Adaptation of a food frequency questionnaire to assess diets of
Puerto Rican and non-Hispanic adults. American Journal of Epidemiology, 1998.
148(5): p. 507 - 518.
94. Brecher, G., M. Schneiderman, and G.Z. Williams, Evaluation of electronic red
blood cell counter. Am J Clin Pathol, 1956. 26(12): p. 1439-49.
95. Thomas, G.N., et al., Vitamin D Levels Predict All-Cause and Cardiovascular
Disease Mortality in Subjects With the Metabolic Syndrome. Diabetes Care, 2012.
35(5): p. 1158-1164.
96. McGill, A.T., et al., Relationships of low serum vitamin D3 with anthropometry
and markers of the metabolic syndrome and diabetes in overweight and obesity.
Nutr J, 2008. 7: p. 4.

60
CHAPTER TWO
Longitudinal Association of serum 25(OH)D concentration and Dyslipidemia
among Older Puerto Ricans:
The Boston Puerto Rican Health Study & Boston Puerto Rican Osteoporosis Study
Aziza Jamal-Allial1, John L. Griffith2,3, Katherine L. Tucker 3
1Department of Pharmaceutical Science. 3Department of Health Sciences, 2Bouvé
College of Health Sciences. Northeastern University.
Boston, MA, USA 02115
Presented at Experimental Biology 2013 (Oral Presentation)

61
ABSTRACT
Vitamin D deficiency is highly prevalent. Several reports suggest an association
between plasma 25-hydroxyvitamin D concentration (25(OH)D) and cardiovascular
disease (CVD). We examined, cross-sectionally and longitudinally, the relation between
serum 25(OH)D concentration and lipid profile of 970 Puerto Rican adults, 270 men and
700 women, aged 45-75 years. Cross sectional analyses at the two year time point
showed that high-density lipoprotein cholesterol (HDL-C) was significantly associated
with plasma 25(OH)D (P<0.01); but not low-density lipoprotein cholesterol (LDL-C),
triglycerides (TG), or total cholesterol (TC).
In longitudinal analyses, baseline-25(OH)D was significantly associated with
subsequent 2.5-year change in plasma HDL-C (β = -0.045 ± 0.02, P =0.007) controlling
for age, sex, baseline-HDL-C concentration, BMI, follow-up time, physical activity, total
energy, alcohol, smoking, seasonality, poverty, and education. This relationship remained
significant after adjustment for CVD medications and heart disease status. After
controlling for potential confounders, baseline-25(OH)D was a significantly positive
predictor of the change in plasma TG concentration over time (β = 0.40 ± 0.02, P =0.03).
In conclusion, even though 25(OH)D serum concentration was positively
associated with HDL-C in our cross-sectional analyses, the longitudinal analyses showed
that higher 25(OH)D serum concentration did not translate into an increase of the
atheroprotective HDL-C, nor a decrease in the not-atheroprotective plasma TG in this
population of older Puerto Rican adults living in the Boston area.

62
Abbreviations:
25-hydroxyvitamin D (25(OH)D); cardiovascular disease (CVD); confidence interval
(CI); United States (USA); food-frequency questionnaire (FFQ); high-density lipoprotein
(HDL-C); low-density lipoprotein (LDL-C); triglycerides (TG); total cholesterol (TC);
vitamin D receptor (VDR); cytochrome-P450 enzymes (CYP-450s).

63
INTRODUCTION
Vitamin D receptor (VDR) is found not only in not only in bone metabolism
tissues, but in a variety of tissues, making it likely that vitamin D actions extend beyond
maintaining calcium homeostasis and skeletal integrity [93, 94]. Achieving optimum
vitamin D status with only dietary sources is not generally feasible [26, 29-31]; rather,
endogenous synthesis is the most efficient way. This occurs via the ultraviolet-β
activation of 7-dehydrocholestrol producing the D3 form, cholecalciferol [32]. This later
binds to the vitamin D-binding protein (VDBP) and is transported to the liver, where it
gets its first hydroxylation at the 25 position by 25-hydorxylase, producing 25-
hydroxyvitamin D (25(OH)D). The second hydroxylation occurs at the 1-α position by
the actions of one of the cytochrome-P450 enzymes (CYP-450s), namely, CYP27B1, a
1α-hydorxylase, converting 25(OH)D to 1α,25(OH)2D, calcitriol. 25(OH)D is the blood
biomarker that determines the status of vitamin D; it is characterized by a relatively long
half-life of about 3 weeks. 1α,25(OH)2D is the active metabolite that binds to VDR, yet it
has very short half-life, up to only 12-15 hours [32, 34-36]. Vitamin D pathways are
exquisitely regulated by parathyroid hormone (iPTH), serum calcium (Ca+) and
phosphate (Pi) concentration, as well as by the negative feedback inhibition by
1α,25(OH)2D concentration [37, 95]. iPTH under the influence of low serum calcium
increases the second hydroxylation, thus, increasing 1α,25(OH)2D [95].
Notwithstanding increased risk of osteoporosis and lower bone mineral density
[40], vitamin D deficiency has been associated with increased risk of mortality [96] as
well as several chronic illnesses, including: CVD, hypertension [20, 23, 62], cancer [45,
63], obesity, type-2-diabetes [48, 64] and inflammatory disorders [67, 97, 98]. In the last

64
decade, a wide range of scientific evidence has linked vitamin D deficiency to an
increased risk of cardiovascular disease (CVD) [6, 25, 99, 100]. Dyslipidemia, which is
characterized by either low plasma HDL-C, high LDL-C and/or high TG concentration, is
a major risk factor for CVD concentration [101, 102]. Several epidemiological and
ecological studies have shown that lower 25(OH)D concentration is associated with an
unfavorable lipid profile [103-107]. However, divergent results were observed when
intervention studies investigated the effect of vitamin D supplementation on a number of
CVD risk factors that included the lipid profile [108].
Ethnic minorities, largely, and Puerto Ricans, explicitly, are reported to have a
greater burden of health disparities compared to non-Hispanic whites, thus increasing the
risk of developing chronic illness [109-111]. In their systematic review, Renzaho and
colleagures showed that ethnic minorities are substantially predisposed to a greater risk of
vitamin D deficiency among all age groups. They further conclude that a number of
indications link vitamin D deficiency to obesity-related chronic diseases [112].
The aim of this study is to determine the longitudinal association between serum
25(OH)D concentration and lipid profile components, namely, HDL-C, LDL-C, TC, and
TG (mg/dL), among participants of the Boston Puerto Rican Health Study (BPRHS) and
the Boston Puerto Rican Osteoporosis Study (BPROS), living in the Greater Boston Area.

65
MATERIALS AND METHODS
Study Population and Data Collection
Description of the recruitment and methods of the BPRHS [83] and its ancillary
study, the BPROS [113], are described in detail elsewhere. Concisely, at both time
points, a bilingual interviewer conducted home visits and administrated detailed
questionnaires on general background, socioeconomic status, education, household
income, health and health behaviors that include medical diagnosis, detailed use of
medication(s), depression and a psychological acculturation scale. They also
administered questionnaires on dietary intake, food security, activities of daily living,
migration status, stress, depressive symptomology, and cognitive function. Moreover, the
interviewer collected information about anthropometrics, physical performance measures
and blood pressure. The following day, the study phlebotomist collected 24-hr urine, 12-
hr fasting blood and saliva. By December 2010, 1504 participants completed baseline
visits. Once the 2-yr follow up was completed, participants were re-consented for the
BPROS. By May 2013, 1257 participants completed 2year follow-up visits and 970 of
these completed the BPROS study. All study protocols were approved by the Institutional
Review Boards at Tufts Medical Center and Northeastern University, and each
participant provided written informed consent.
There were no significant differences in socio-demographic characteristics
between those with complete or incomplete information. The present study includes
complete longitudinal data for 700 Puerto Rican women and 270 Puerto Rican men.

66
Covariates Assessments and Definition
At each time point, in addition to the designed questionnaires, physical function
tests were completed and anthropometric measures were taken. Blood pressure measures
were obtained at three times during the interview. Weight, and waist and hip
circumferences were measured in duplicate. Weight was measured using a clinical scale
(Toledo Weight Plate, Model I5S, Bay State, and Systems Inc. Burlington, MA). Body
mass index (BMI) was calculated as weight (kg) divided by height (m) squared [27, 28];
BMI was categorized into: recommended (BMI<25), overweight (25-30), and obese
(≥30) [114]. For the purpose of this analysis, vitamin D deficiency was defined as serum
25(OH)D concentration <50 nmol/L, insufficiency between 50-75 nmol/L, and
sufficiency as >75 nmol/L [54, 115]. Seasonality was defined as summer, July to
September; fall, October to December; winter, January to March; and spring, April to
June. Smoking status was categorized into yes or no for the current behavior. Vitamin D
from supplements was defined as: minimal 0-10 µg/day (200-400 IU/day); and high ≥ 10
µg/day (≥ 400 IU/day). Participant’s education was measured at baseline and defined by
the cutoff point of 8th grade, while poverty was measured at each time point and defined
by the U.S. Department of Health and Human Services federal poverty levels. Dietary
Vitamin D intake was estimated from a semi-quantitative food-frequency questionnaire
(FFQ) specifically designed for this population [91]. This FFQ has been validated against
serum carotenoids [116], and vitamin B12 [117] in a Hispanic population aged ≥ 60
years. Those with energy intakes < 600 or > 4800 kilocalories and/or > 10 questions
blank on the FFQ were excluded from the analyses. Nutrient intakes were calculated with
the Nutrition Data System for Research (NDS-R) software version 2007 (Nutrition

67
Coordinating Center, University of Minnesota, Minneapolis, MN, Food and Nutrient
Database 2007, released 2007). Alcohol intake (gm) was captured by the FFQ. Heart
disease status was self-reported. Medication classifications were based primarily on
AHFS Drug Information® (AHFS DI®) pharmacologic and therapeutic classification
2005. We only used cardiovascular pharmacologic medications based on the prefix 24.
Cardiovascular medication classification included: cardiac drugs, including glycoside
such as digoxin; antilipemic agents-HMG CoA reductase- such as Lipitor; omega-3 and -
6 supplements; hypotensive agents such as Thiazide; vasodilating-agents- including
nitrates, Viagra and Dypyridamole; alpha, beta and calcium channel blockers; ACE
inhibitors; angiotensin II inhibitors; and any hypertension medication [118].
Laboratory assays
Fasting blood samples (12-h) were drawn by a certified phlebotomist at the
participant’s home on the morning after the home interview, or as soon thereafter as
possible and kept at 4°C. Plasma was separated within 4 hours and was used for the
analysis of plasma lipid concentration. Aliquots of the isolated serum were saved and
stored at -80°C until processed. Serum 25(OH)D concentration was measured by
extraction followed by 25I radioimmunoassay Packard COBRA II Gamma Counter
(DiaSorin Inc., Stillwater, MN 55082 catalog # 68100E); intra- and inter-assay CV%
10.8% and 9.4%, respectively. Serum creatinine was assessed with a colorimetric, kinetic
reaction using the Olympus AU400e with Olympus Creatinine Reagents (OSR6178)
(Olympus America Inc., Melville, NY); intra-and inter-assay CV% were 2.0%, and 4.0%,
respectively. Plasma TC, HDL-C and TG were measured enzymatically on the Olympus

68
AU400. For TC, Olympus reagents (OSR6116) were used; intra- and inter-assay CV%
were 1.8%, and 2.2%, respectively. For HDL-C, Olympus reagents (OSR6156) were
used. For TG, Olympus reagents (OSR6033) were used; intra- and inter-assay CV% were
2.8%, and 2.7%, respectively. LDL-C and VLDL-C were calculated based on the
Friedewald equation from TC, HDL-C and TG i.e. VLDL=TG/5 and LDL-C =TC –
(VLDL + HDL-C) [119].
Statistical analyses:
All statistical analyses were conducted with SAS 9.1.3 (SAS Institute Inc., Cary,
NC); and all tests were 2-sided with P <0.05 to be considered statistically significant.
Dependent skewed variables were natural log-transformed to normalize their distributions
before the analysis. Demographic and clinical characteristics were compared using
Student’s t-test for continuous variables and the chi square tests for categorical variables.
Characteristics were compared by sex using two-tailed t-tests for two independent
samples, and χ2 test for differences in proportion. Paired t-tests were used to compare
characteristics across time points. Pearson partial linear correlation analysis was used to
examine relationships between serum 25(OH)D concentration with lipid profile at each
time point, adjusting for age and sex. Additionally, we constructed multivariate
regression analysis using general linear models to examine change in the plasma
concentration of the lipid profile components, with baseline serum 25(OH)D
concentration. A Risk factor model (RF-model) included: adjustment for age (y),
baseline-25(OH)D (nmol/L), BMI, baseline-lipid component, follow-up time (mos), and
sex in the full model. The Life-Style model (LS-model) included: physical activity, total

69
energy (kcal/day), current smoking status (y/n), alcohol (g/day), seasonality, poverty
level, and education in addition to the RF-model covariates. To control for confounding
by indications, the CVD model was used to adjust for the use of any cardiovascular
medication (y/n) as well as the prevalence of heart disease (y/n) [120]. For all
multivariate regression models, we checked assumptions of linearity and homogeneity by
examining outcome residuals against the exposure. For all final models, we performed
influence diagnostics tests to check for outliers and influential points. We also tested all
of our models for any potential effect modification by sex, with covariates in our models,
such as smoking, by including an interaction term with the exposure variable. Because
the lipid profile might be sex-specific, we constructed sex-stratified analyses in addition
to the full model. The baseline concentration of each lipid profile component was
included as a covariate to all of our models to control for regression to the mean [121].
To reduce bias and augment precision, we conducted multiple imputation analysis to
consider the uncertainty that missing values might convey within our dataset. We created
a total of five imputed data sets with (seed= 32, 37854) using procedure (PROC MI); we
included all covariates that are considered risk factors and being used in any of our
models. We used (PROC MIANALYZE) to combine all the five imputed data sets, thus,
producing valid statistical inferences that accounts for within and between imputation
variation [122]. We found that these missing values produced no significant impact on
our analysis.

70
RESULTS
Complete serum 25(OH)D concentration was available for 650 women and 255
men at both baseline and 2-yr. The mean ages of men and women were 59.5 ± 8.0 and
60.5 ± 8.0, respectively (Table 1). The mean follow-up time was 33.3± 12 months for
women and 30.5 ± 49 months for men. At baseline, the mean serum 25(OH)D of women
and men were, 44.0 ± 17.5 and 43.0 ± 16.1 nmol/L, respectively, while the 2-year values
were 50.1 ± 19.0 and 47.0 ± 17.5 nmol/L, respectively. The mean 25(OH)D at 2-yr was
5.5 nmol/L higher compared to baseline (P<0.0001) (Figure 1.1). Compared to men,
women had significantly higher plasma HDL-C, LDL-C and TC (mg/dL) at both time
points; while men had consistently higher plasma TG (mg/dL) and serum creatinine
(µmol/L). All lipid profile components increased significantly over time (P<0.0001). The
prevalence of reported heart disease status went up by 9 and 12% among men and
women, respectively. In addition, use of cardiovascular medication increased by 12% and
10.5% and of lipid lowering medication by 14% and 17%, for men and women,
respectively. While the mean BMI values did not differ across, the two time points,
women consistently had significantly higher mean BMI than men, (P<0.0001). In
contrast, waist circumference did not differ by sex, but was significantly higher at 2-yr
compared to baseline (P<0.0001).
There was no significant change over time in dietary vitamin D intake. However,
women had higher dietary vitamin D intake (IU/day) and higher vitamin D-containing
supplement use than men; while men had higher energy intake (kcal/day) than women at
both time points. There was a significant reduction in total energy consumed (P < 0.001)
over the 2.5 years for both men and women. The men walked significantly more

71
miles/day, i.e. 2 miles/day, compared to 1.4 miles/day (P<0.0001) for the women; men
also had higher physical activity scores and reported more current smoking and alcohol
consumption than women.
Among the lipid profile components, only HDL-C at 2-yr was significantly
correlated with serum 25(OH)D (r = 0.1, P =0.01) (Table 1.2). In longitudinal analysis
(Tables 1.3 and 1.4) baseline-25(OH)D was not associated with change in plasma HDL-C
concentration controlling for age, sex, BMI and follow-up time. However, in the CVD
model adjusting for physical activity, total energy (kcal/day), alcohol (gm/day), smoking
(y/n), seasonality, poverty level, education, heart disease (y/n) and taking CVD
medications (y/n), a significant association between baseline-25(OH)D and change in
plasma HDL-C concentration emerged (β = -0.04 ± 0.02, P =0.01), but in an unexpected
negative direction. Consistently, all three models explained about 62.5% of the variation
in the 2.5-year change in plasma HDL-C. Similarly, after differences in confounders were
controlled in LS-model, baseline-25(OH)D was significantly associated with change in
plasma TG, but in the unexpected positive direction (β = 0.40 ± 0.02, P =0.03). This
model explained only 30% of the variation in 2.5-year change in plasma TG. However,
when controlling for the CVD related covariates, the significant association was
attenuated (β = 0.34, P =0.05). Changes in plasma LDL-C and TC also tended to be
positively associated with baseline 25(OH)D , but these did not reach significance level
(P >0.05).
Smoking status was found to be an effect modifier of the association between
baseline-25(OH)D and HDL-C. The interaction between baseline-25(OH)D and smoking
status (P =0.04) was significant, thus, we stratified the analysis by smoking status for all

72
of the lipid profile components. Interestingly, baseline-25(OH)D was inversely yet
significantly associated with the change in plasma HDL-C concentration over time (β = -
0.06, P =0.002) only among non-smokers, when controlling for age, sex, BMI and
follow-up time. This association was strengthened after controlling for all life style
covariates (β = -0.06, P =0.0002) and CVD covariates (β = -0.07, P =0.0003). The
stratified models explained approximately 63 to 65% of the variation in 2.5-year change
in plasma HDL-C among non-smokers. On the other hand, null associations were found
among current smokers (Figure 1.2). Additionally, even though the interaction term
between baseline-25(OH)D and smoking status within the LDL-C models were not
significant, the stratified analysis showed that among currently smoking participants,
baseline-25(OH)D was inversely associated with the change in plasma LDL-C
concentration over time (β = -0.25, P =0.02), explaining roughly 42.3% of the model
variation. The addition of lifestyle covariates did not attenuate the coefficient, but the
significant association disappeared (β = -0.23, P =0.05) (Figure 1.3). Smoking status was
not an effect modifier of the association with baseline-25(OH)D and either plasma TG or
TC.
DISCUSSION
Although serum 25(OH)D concentration was positively associated with plasma
HDL-C cross-sectionally, longitudinal analyses showed inverse associations. Baseline-
25(OH)D demonstrated significant, negative association with 2.5-year change in plasma
HDL-C concentration (β = -0. 04, P =0.01), independent of important confounders

73
including age, sex, BMI, total energy intake, physical activity score, smoking, alcohol,
seasonality, poverty and education. This negative association remained after adjustment
for CVD-related variables. Similar relationships were seen with plasma TG, but not with
LDL-C and TC.
Our report is in contrast to several reports that indicate serum 25(OH)D
concentration is positively associated with plasma HDL-C, and negatively associated
with plasma LDL-C and TG [106, 107, 123-127]. In the prospective Health Professionals
Follow-up Study (HPFS), Giovannucci and colleagues demonstrated a positive linear
trend of LDL-C, HDL-C and TC, as well as a negative trend with plasma TG across
serum 25(OH)D quartiles among 900 US men, ages 64 and older [125]. Another study
showed that increasing serum 25(OH)D tertiles were independently associated with
higher HDL-C and lower TG; but not TC [107]. Interestingly, some the earlier studies
reported that both HDL-C and LDL-C were positively associated with serum 25(OH)D
concentration, thus, both increasing plasma concentration. It is well known that
increasing HDL-C and lowering LDL-C is desirable to improve CVD risk [2, 128]. A
cross-sectional analysis of the Third National Health and Nutrition Examination Survey
(NHANES III), found that serum 25(OH)D concentration was significantly inversely
associated with TC, in 13,331 US men and women ages 20 years and older [96]. The
study did not find an association between plasma HDL-C and serum 25(OH)D [96]. One
longitudinal study, with a 14 year follow-up in 1762 participants, found that serum
25(OH)D and plasma TG were inversely associated [104]. Most prior studies were cross-
sectional and no proof of a causal relationship can be inferred. In our longitudinal results,
with control for numerous confounders, we saw different results.

74
Our results are in accordance with a few reports that found that serum 25(OH)D
concentration may not be associated with an atheroprotective lipid profile [96, 104, 105,
123, 127]. One study found that TC was significantly associated with higher serum
25(OH)D concentration among 8,018 Norwegian men and women, aged 43-70 years
[104]. Two other studies also found that plasma TG were positively associated with
serum 25(OH)D; however, these latter studies were in children [123, 127].
Intervention studies in the form of placebo-controlled randomized trials (RCT) are
most informative for causal relationships. Very few RCT have been conducted to assess
the effect of vitamin D on lipid concentration, and most reported a null effect of vitamin
D supplementation on lipid profile [108, 129-131]. One study showed that daily vitamin
D supplementation (3320 IU/day) for one year significantly improved plasma TG: the
supplemented group lowered plasma TG compared to placebo, -13.5% and +3% (P
=0.001) correspondingly. However, the supplemented group also exhibited a significant
increase in plasma LDL-C [129]. Conversely, another study did not show that a year of
vitamin D supplementation, at 40, 000 IU/week, changed plasma lipids in 438
overweight/obese participants [108]. Yet another study showed that vitamin D
supplementation may not be atheroprotective in postmenopausal women [130]. Most of
these RCT can be criticized for low sample size, which may have contributed to the null
results.
Through stratification, we observed two distinct phenomena in the relationship
between plasma HDL-C, in particular, and serum 25(OH)D concentration. First, only
women retained the significant inverse association between serum 25(OH)D and the
change in plasma HDL-C concentration during follow up, thus, mirroring the association

75
of the combined data. The other explanation is that due to lack of power, we could not
detect a significant association of serum 25(OH)D and the change in plasma HDL-C
concentration among men. The significant association of serum 25(OH)D on HDL-C
among non-smokers was surprising, although similar results were reported previously
[132]. Among participants of the Tromsø study, smokers had 15-20% higher serum
25(OH)D concentration than non-smokers. The pathophysiological mechanism by which
smoking may impact serum 25(OH)D concentration or the metabolism of 1,25(OH)2D
has not been investigated. However, it has been suggested that smoking might influence
25-hydroxylase (CYP2R1) thus, lowering serum 25(OH)D concentration [133]. Another
point that might explain this paradox is that, smoking contains nicotine, which exerts
anti-inflammatory properties [134, 135].
Our results disagree with several epidemiologic and ecological studies regarding
the role of serum 25(OH)D on lipid profile as a major risk factor for CVD. One
explanation for our unexpected finding is that vitamin D induces the intestinal absorption
of dietary calcium, thus lowering calcium fecal excretion [37, 95]. This might affect the
amount of fatty acids in the feces, due to a reduction in the formation of insoluble fatty
soaps [136]. This could lead to an increased rate of the absorption of fatty acids, thus
higher plasma LDL-C and TG concentration, in particular, and TC in general [137]. In
addition, higher vitamin D could decrease cholesterol excretion because of the lower
availability of calcium within the intestine, and hence lower binding to bile acids, with
lower conversion of cholesterol to bile acids [138]. One study suggested that higher
calcium intake may lower LDL-C by increasing vitamin D A 15 week weight loss trial
showed that, among 63 healthy, overweight/obese women, the daily supplementation of

76
600 mg of calcium and 200 IU of vitamin D significantly improved LDL-C as well as
LDL: HDL-C ratio, while improvements in HDL-C and TG approached significance
[139].
Our findings should be interpreted within the context of a few limitations. First,
our population is Puerto Rican, therefore our findings could be very specific to this
particular admixture population, with genetic variation interacting not only with the
environment, but social factors as well [140-143]. This may limit generalizability.
Secondly, although we have controlled for many known potential covariates, residual
confounding is still be a possibility.
In conclusion, our longitudinal analysis showed that higher 25(OH)D serum
concentration did not translate into an increase of the atheroprotective plasma HDL-C,
nor a decrease of plasma TG in in this population of older Puerto Rican adults living in
the Boston area. Moreover, our results showed that smoking may be an effect modifier of
the longitudinal association of serum 25(OH)D and HDL-C, as well as LDL-C. The
conflicting information in the literature suggests that more studies are needed to clarify
the role of vitamin D on lipid profiles.

77
BIBLIOGRAPHY
1. Holick, M.F., The vitamin D deficiency pandemic and consequences for
nonskeletal health: mechanisms of action. Mol Aspects Med, 2008. 29(6): p. 361-8.
2. Holick, M.F., Vitamin D: extraskeletal health. Endocrinology and metabolism clinics of North America, 2010. 39(2): p. 381-400, table of contents.
3. Holick, M.F., High prevalence of vitamin D inadequacy and implications for
health. Mayo Clin Proc, 2006. 81(3): p. 353-73. 4. Holick, M.F., Resurrection of vitamin D deficiency and rickets. J Clin Invest,
2006. 116(8): p. 2062-72. 5. Holick, M.F., Vitamin D deficiency. N Engl J Med, 2007. 357(3): p. 266-81. 6. Holick, M.F., Deficiency of sunlight and vitamin D. Bmj, 2008. 336(7657): p.
1318-9. 7. Ramos-Lopez, E., et al., CYP2R1 (vitamin D 25-hydroxylase) gene is associated
with susceptibility to type 1 diabetes and vitamin D levels in Germans. Diabetes/Metabolism Research and Reviews, 2007. 23(8): p. 631-636.
8. Prosser, D.E. and G. Jones, Enzymes involved in the activation and inactivation of
vitamin D. Trends in biochemical sciences, 2004. 29(12): p. 664-73. 9. Cheng, J.B., et al., Genetic evidence that the human CYP2R1 enzyme is a key
vitamin D 25-hydroxylase. Proceedings of the National Academy of Sciences of the United States of America, 2004. 101(20): p. 7711-5.
10. Jones, G., Pharmacokinetics of vitamin D toxicity. The American Journal of Clinical Nutrition, 2008. 88(2): p. 582S-586S.
11. Deeb, K.K., D.L. Trump, and C.S. Johnson, Vitamin D signalling pathways in
cancer: potential for anticancer therapeutics. Nature reviews. Cancer, 2007. 7(9): p. 684-700.
12. Lacour, B., et al., Parathyroid function and lipid metabolism in the rat. Miner Electrolyte Metab, 1982. 7(3): p. 157-65.
13. Holick, M.F., Evolution and function of vitamin D. Recent Results Cancer Res, 2003. 164: p. 3-28.
14. Melamed, M.L., et al., 25-hydroxyvitamin d levels and the risk of mortality in the
general population. Archives of Internal Medicine, 2008. 168(15): p. 1629-1637. 15. Giovannucci, E., et al., 25-hydroxyvitamin D and risk of myocardial infarction in
men: a prospective study. Archives of Internal Medicine, 2008. 168(11): p. 1174-80.
16. Michos, E.D., et al., 25-Hydroxyvitamin D deficiency is associated with fatal
stroke among whites but not blacks: The NHANES-III linked mortality files. Nutrition, (0).
17. Ameri, P., et al., High prevalence of vitamin D deficiency and its association with
left ventricular dilation: an echocardiography study in elderly patients with
chronic heart failure. Nutrition Metabolism & Cardiovascular Diseases, 2010. 20(9): p. 633-40.

78
18. Freedman, D.M., et al., Serum Levels of Vitamin D Metabolites and Breast
Cancer Risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening
Trial. Cancer Epidemiology Biomarkers & Prevention, 2008. 17(4): p. 889-894. 19. Chen, T.C. and M.F. Holick, Vitamin D and prostate cancer prevention and
treatment. Trends Endocrinol Metab, 2003. 14(9): p. 423-30. 20. Wortsman, J., et al., Decreased bioavailability of vitamin D in obesity. The
American Journal of Clinical Nutrition, 2000. 72(3): p. 690-693. 21. Botella-Carretero, J.I., et al., Vitamin D deficiency is associated with the
metabolic syndrome in morbid obesity. Clinical Nutrition, 2007. 26(5): p. 573-80. 22. Kragt, J., et al., Higher levels of 25-hydroxyvitamin D are associated with a lower
incidence of multiple sclerosis only in women. Multiple Sclerosis, 2009. 15(1): p. 9-15.
23. Alvarez-Rodriguez, L., et al., Age and low levels of circulating vitamin D are
associated with impaired innate immune function. Journal of Leukocyte Biology, 2012. 91(5): p. 829-838.
24. Bellia, A., et al., Serum 25-hydroxyvitamin D levels are inversely associated with
systemic inflammation in severe obese subjects. Internal and Emergency Medicine, 2013. 8(1): p. 33-40.
25. Vacek, J.L., et al., Vitamin D Deficiency and Supplementation and Relation to
Cardiovascular Health. The American Journal of Cardiology, 2012. 109(3): p. 359-363.
26. Pittas, A.G., et al., Systematic Review: Vitamin D and Cardiometabolic
Outcomes. Annals of Internal Medicine, 2010. 152(5): p. 307-314. 27. Sugden, J.A., et al., Vitamin D improves endothelial function in patients with Type
2 diabetes mellitus and low vitamin D levels. Diabet Med, 2008. 25(3): p. 320-5. 28. Zittermann, A., et al., Vitamin D supplementation enhances the beneficial effects
of weight loss on cardiovascular disease risk markers. American Journal of Clinical Nutrition, 2009. 89(5): p. 1321-7.
29. Kannel, W.B., et al., Serum Cholesterol, Lipoproteins, and the Risk of Coronary
Heart DiseaseThe Framingham Study. Annals of Internal Medicine, 1971. 74(1): p. 1-12.
30. Gordon, T., et al., High density lipoprotein as a protective factor against
coronary heart disease: The Framingham study. The American Journal of Medicine, 1977. 62(5): p. 707-714.
31. Hypponen, E., et al., 25-hydroxyvitamin D, IGF-1, and metabolic syndrome at 45
years of age: a cross-sectional study in the 1958 British Birth Cohort. Diabetes, 2008. 57(2): p. 298-305.
32. Jorde, R., et al., High serum 25-hydroxyvitamin D concentrations are associated
with a favorable serum lipid profile. European Journal of Clinical Nutrition, 2010. 64(12): p. 1457-64.
33. Karhapää, P., et al., Diverse associations of 25-hydroxyvitamin D and 1,25-
dihydroxy-vitamin D with dyslipidaemias. Journal of Internal Medicine, 2010. 268(6): p. 604-610.

79
34. Kazlauskaite, R., et al., Vitamin D is associated with atheroprotective high-
density lipoprotein profile in postmenopausal women. Journal of Clinical Lipidology, 2010. 4(2): p. 113-119.
35. Maki, K.C., et al., Serum 25-hydroxyvitamin D is independently associated with
high-density lipoprotein cholesterol and the metabolic syndrome in men and
women. Journal of Clinical Lipidology, 2009. 3(4): p. 289-296. 36. Jorde, R., et al., No improvement in cardiovascular risk factors in overweight and
obese subjects after supplementation with vitamin D3 for 1 year. Journal of Internal Medicine, 2010. 267(5): p. 462-472.
37. Mattei, J., et al., Allostatic load is associated with chronic conditions in the
Boston Puerto Rican Health Study. Social Science & Medicine, 2010. 70(12): p. 1988-96.
38. Tucker, K.L., et al., Self-reported prevalence and health correlates of functional
limitation among Massachusetts elderly Puerto Ricans, Dominicans, and non-
Hispanic white neighborhood comparison group. J Gerontol A Biol Sci Med Sci, 2000. 55(2): p. M90-7.
39. Tucker, K.L., O.I. Bermudez, and C. Castaneda, Type 2 diabetes is prevalent and
poorly controlled among Hispanic elders of Caribbean origin. Am J Public Health, 2000. 90(8): p. 1288-93.
40. Renzaho, A.M., J.A. Halliday, and C. Nowson, Vitamin D, obesity, and obesity-
related chronic disease among ethnic minorities: a systematic review. Nutrition, 2011. 27(9): p. 868-79.
41. Tucker, K., et al., The Boston Puerto Rican Health Study, a longitudinal cohort
study on health disparities in Puerto Rican adults: challenges and opportunities. BMC Public Health, 2010. 10(1): p. 107.
42. Bhupathiraju, S.N., et al., Centrally located body fat is associated with lower bone
mineral density in older Puerto Rican adults. The American Journal of Clinical Nutrition, 2011. 94(4): p. 1063-1070.
43. Flegal, K.M., et al., Overweight and obesity in the United States: prevalence and
trends, 1960-1994. International journal of obesity and related metabolic disorders : journal of the International Association for the Study of Obesity, 1998. 22(1): p. 39-47.
44. Holick, M.F., et al., Evaluation, Treatment, and Prevention of Vitamin D
Deficiency: an Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism, 2011. 96(7): p. 1911-1930.
45. Dawson-Hughes, B., et al., Estimates of optimal vitamin D status. Osteoporos Int, 2005. 16(7): p. 713-6.
46. Tucker, K., et al., Adaptation of a food frequency questionnaire to assess diets of
Puerto Rican and non-Hispanic adults. American Journal of Epidemiology, 1998. 148(5): p. 507 - 518.
47. Bermudez, O., et al., Hispanic and non-Hispanic white elders from Massachusetts
have different patterns of carotenoid intake and plasma concentrations. Journal of Nutrition, 2005. 135(6): p. 1496 - 1502.
48. Kwan, L.L., O.I. Bermudez, and K.L. Tucker, Low vitamin B-12 intake and status
are more prevalent in Hispanic older adults of Caribbean origin than in

80
neighborhood-matched non-Hispanic whites. Journal of Nutrition, 2002. 132(7): p. 2059-64.
49. Pharmacists, A.S.o.H.-S., AHFS Pharmacologic-Therapeutic Classification 2008, American Society of Health-System Pharmacists.
50. Friedewald, W.T., R.I. Levy, and D.S. Fredrickson, Estimation of the
Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of
the Preparative Ultracentrifuge. Clinical Chemistry, 1972. 18(6): p. 499-502. 51. Signorello, L.B., et al., Confounding by indication in epidemiologic studies of
commonly used analgesics. American Journal of Therapeutics, 2002. 9(3): p. 199-205.
52. Barnett, A.G., J.C. van der Pols, and A.J. Dobson, Regression to the mean: what it
is and how to deal with it. International Journal of Epidemiology, 2005. 34(1): p. 215-220.
53. Sterne, J.A.C., et al., Multiple imputation for missing data in epidemiological and
clinical research: potential and pitfalls. BMJ, 2009. 338. 54. Delvin, E.E., et al., Vitamin D Status Is Modestly Associated with Glycemia and
Indicators of Lipid Metabolism in French-Canadian Children and Adolescents. The Journal of Nutrition, 2010. 140(5): p. 987-991.
55. Forouhi, N.G., et al., Baseline Serum 25-Hydroxy Vitamin D Is Predictive of
Future Glycemic Status and Insulin Resistance: The Medical Research Council
Ely Prospective Study 1990–2000. Diabetes, 2008. 57(10): p. 2619-2625. 56. Giovannucci, E., et al., 25-hydroxyvitamin d and risk of myocardial infarction in
men: A prospective study. Archives of Internal Medicine, 2008. 168(11): p. 1174-1180.
57. Pilz, S., et al., Vitamin D and mortality in older men and women. Clinical Endocrinology, 2009. 71(5): p. 666-672.
58. Williams, D.M., A. Fraser, and D.A. Lawlor, Associations of vitamin D,
parathyroid hormone and calcium with cardiovascular risk factors in US
adolescents. Heart, 2011. 97(4): p. 315-320. 59. Bonow, R.O., Primary Prevention of Cardiovascular Disease. Circulation, 2002.
106(25): p. 3140-3141. 60. Balagopal, P., et al., Nontraditional Risk Factors and Biomarkers for
Cardiovascular Disease: Mechanistic, Research, and Clinical Considerations for
Youth. Circulation, 2011. 123(23): p. 2749-2769. 61. Zittermann, A., et al., Vitamin D supplementation enhances the beneficial effects
of weight loss on cardiovascular disease risk markers. The American Journal of Clinical Nutrition, 2009. 89(5): p. 1321-1327.
62. Heikkinen, A., et al., Long-term vitamin D3 supplementation may have adverse
effects on serum lipids during postmenopausal hormone replacement therapy. European Journal of Endocrinology, 1997. 137(5): p. 495-502.
63. Nagpal, J., J.N. Pande, and A. Bhartia, A double-blind, randomized, placebo-
controlled trial of the short-term effect of vitamin D3 supplementation on insulin
sensitivity in apparently healthy, middle-aged, centrally obese men. Diabetic Medicine, 2009. 26(1): p. 19-27.

81
64. Jorde, R., et al., Cross-sectional and longitudinal relation between serum 25-
hydroxyvitamin D and body mass index: the Tromsø study. European Journal of Nutrition, 2010. 49(7): p. 401-407.
65. Yoon, V., N.M. Maalouf, and K. Sakhaee, The effects of smoking on bone
metabolism. Osteoporosis International, 2012. 23(8): p. 2081-2092. 66. Reid, I.R., Effects of calcium supplementation on circulating lipids: potential
pharmacoeconomic implications. Drugs Aging, 2004. 21(1): p. 7-17. 67. Hu, F.B., J.E. Manson, and W.C. Willett, Types of Dietary Fat and Risk of
Coronary Heart Disease: A Critical Review. Journal of the American College of Nutrition, 2001. 20(1): p. 5-19.
68. Van der Meer, R., et al., Effects of supplemental dietary calcium on the intestinal
association of calcium, phosphate, and bile acids. Gastroenterology, 1990. 99(6): p. 1653-9.
69. Major, G.C., et al., Supplementation with calcium + vitamin D enhances the
beneficial effect of weight loss on plasma lipid and lipoprotein concentrations. American Journal of Clinical Nutrition, 2007. 85(1): p. 54-9.
70. Junyent, M., et al., The effects of ABCG5/G8 polymorphisms on plasma HDL
cholesterol concentrations depend on smoking habit in the Boston Puerto Rican
Health Study. Journal of Lipid Research, 2009. 50(3): p. 565-73. 71. Lai, C.-Q., et al., Population admixture associated with disease prevalence in the
Boston Puerto Rican health study. Human Genetics, 2009. 125(2): p. 199-209. 72. Mattei, J., et al., Apolipoprotein A5 polymorphisms interact with total dietary fat
intake in association with markers of metabolic syndrome in Puerto Rican older
adults. Journal of Nutrition, 2009. 139(12): p. 2301-8. 73. Mattei, J., et al., Disparities in allele frequencies and population differentiation
for 101 disease-associated single nucleotide polymorphisms between Puerto
Ricans and non-Hispanic whites. BMC Genetics, 2009. 14(10): p. 45.

82
TABLE 1.1: Descriptive characteristic of men and women in the Boston Puerto Rican Health Study (BPRHS) & Boston Puerto Rican Osteoporosis Study (BPROS)
Baseline (n=1504) Two Year (n=970 )
Women (n=1060)
Men (n=444)
Women (n=700)
Men (n=270)
Age (y) 57.0 ± 7.3 56.0 ± 8.0 60.3 ± 7.5 59.5 ± 8.0
Education (>8th grade %) 51.5 55.5 -- --
Poverty (%) 60.0 49.0$$ 59.0 48.5$$
25(OH)D (nmol/L) §§§ 44.0± 17.4 43.0 ± 16.5 50.1 ± 19.0 47.0 ± 17.5*
Follow-up time (months) -- -- 33.3± 12 30.5± 49
Serum Lipids
HDL (mg/dL) §§§ 47.1 ± 12.2 40.5 ± 12.5*** 48.1 ± 12.5 41.2 ± 12.0***
LDL (mg/dL) §§§ 110 ± 34.4 101 ± 35.2*** 112 ± 35.3 103 ± 34.5**
Triglyceride (mg/dL) §§ 157 ± 99.0 175 ± 140** 154 ± 78.5 178± 151*
Total cholestrol (mg/dL) §§§ 188 ± 40.5 174 ± 43.0*** 190 ± 42.0 177± 42.2***
Creatinine (µmol/L) §§§ 68.0 ± 27.5 88.0 ± 45.0*** 69.4 ± 20.2 88.6 ± 29.4***
Heart disease (%) 20.5 22.0 23.0 24.0
Cardiovascular meds (%) 61.5 57.3 68.0 64.3
Lipid-lowering meds (%) 41.0 38.5 48.0 44.0
Adiposity Measures
BMI (kg/m2) 33.2 ± 7.0 30.0 ± 5.3*** 33.0 ± 7.0 30.2 ± 5.5***
Waist Circumference(cm) §§§ 102.2 ± 15.4 103.0 ± 13.5 104.0 ± 15.0 104.3 ± 14.3
Other Covariates

83
Miles walking/day§§§ 1.0 ± 1.5 1.4 ± 2.0*** 1.4 ± 2.0 2.0 ± 2.4 ***
Physical Activity Score # 31.0 ±1.13 32.1±1.20*** 31.3 ± 1.1 32.5 ± 1.2***
Smoking (%) 20.1 32.5$$$ 19.0 29.0$$
Alcohol drinking (%) 36.0 52.0$$$ 28.0 43.0$$$
Alcohol intake (gm/day) ** 3.0 ± 13.5 14.0 ± 45.0$$$ 2.5 ±17.0 7.0 ± 24.0$$$
Vitamin D supp (>200IU/day) (%)
30.0 24.1 30.2 18.5$$
Total vitamin D (IU/day) 290.5±172.0 280.0± 178.0 287.5±152.0 257.0±123.0**
Total Energy (kcal/day) §§§ 2100 ± 1100 2750 ± 1430*** 1750 ±865 2215 ±1120***
BMI, body mass index; 25(OH)D, 25-hydroxyvitamin D. # Geometric mean ± SD 1Data are presented as mean ± SD for continuous variables or as % for categorical variables Means were compared using t-test for between sex (within each time points): *P -value <0.05, ** P -value <0.001, ***P-value <0.0001
Means were compared using paired t-test for between time points: §P -value <0.05, §§P -
value <0.001, §§§P-value <0.0001
Percentages were compared using Chi-square test for between sex (within each time points): $P -value <0.05, $$
P -value <0.001, $$$ P-value <0.0001

84
TABLE 1.2: Pearson partial linear correlation of serum 25(OH)D concentration and
adiposity phenotype at baseline and 2-year follow-up
Lipid Profile
Components
(mg/dL)
Baseline Two-Year
25(OH)D p-value 25(OH)D p-value
HDL-C 0.01 0.7 0.1 0.01
LDL-C 0.01 0.7 -0.02 0.4
TC -0.03 0.3 -0.03 0.3
TG 0.005 0.8 -0.01 0.7
Pearson partial linear correlation coefficient (r) is age, sex and seasonality adjusted Abbreviations: high-density lipoprotein (HDL-C); low-density lipoprotein (LDL-C); triglycerides (TG); total cholesterol (TC); 25-hydroxy vitamin D concentration (25(OH)D)

85
TABLE 1.3 Regression coefficients (± SE) from longitudinal linear regression analysis of lipid profile components and baseline
serum 25(OH)D concentration
Lipid Profile Components
Baseline 25(OH)D
(nmol/L)
Change in HDL-C Change in LDL-C
ALL
(n=866)
Men
(n=246)
Women
(n=620)
ALL
(n=864)
Men
(n=245)
Women
(n=619)
β ± SE p β ±SE p β ± SE p β ± SE p β ±SE p β ± SE p
Risk Factor model -0.025
± 0.01
0.1
-0.01
±0.02
0.6
- 0.03
± 0.01
0.1 -0.05
±0.05
0.3
-0.20
± 0.1
0.07
-0.003
±0.1
0.9
Life-Style
model
-0.045
±0.01
0.007
-0.04
± 0.03
0.2
- 0.05
± 0.02
0.01 -0.12
±0.06
0.05
-0.22
±0.12
0.07
-0.1
± 0.1
0.2
CVD Model -0.04
±0.02 0.01
-0.035
±0.03 0.2
- 0.043
± 0.02 0.02
-0.01
±0.05 0.09
-0.2 ±
0.1 0.1
-0.1
± 0.1 0.2
Risk factor model: adjusted for age, BMI, baseline-lipid-component (mg/dL), follow-up time (mos), and sex, in the case of the combined data1

86
Life-Style model: adjusted for model 1 variables physical activity, total energy (kcal/day), alcohol, smoking, seasonality, poverty level, education and sex in the case of the combined data1
CVD model: adjusted for model 1+ 2 variables plus heart-disease (y/n), taking cardiovascular agents (y/n) and sex in the case of the combined data1

87
TABLE 1.4 Regression coefficients (± SE) from longitudinal linear regression analysis of lipid profile components and baseline
serum 25(OH)D concentration
Lipid Profile Components
Baseline 25(OH)D
(nmol/L)
Change in TG Change in TC
ALL
(n=844)
Men
(n=228)
Women
(n=615)
ALL
(n=844)
Men
(n=228)
Women
(n=615)
β ± SE p β ±SE p β ± SE p β ± SE p β ±SE p β ± SE p
Risk Factor model 0.22
± 0.2
0.2
0.3
± 0.5
0.6
0.2
± 0.15
0.2 -0.04 ±
0.06
0.5
-0.11
± 0.1
0.4
-0.02
± 0.1
0.7
Life-Style
model
0.4
± 0.2
0.03
1.0
± 0.5
0.1
0.2
± 0.17
0.2 - 0.12 ±
0.1
0.08
-0.1
± 0.1
0.5
- 0.14
± 0.1
0.08
CVD Model 0.34
± 0.2 0.05
1.0
± 0.5 0.08
0.16
± 0.15 0.3
-0.11
± 0.1 0.1
-0.05
± 0.1 0.7
-0.13
± 0.1 0.09
Risk factor model: adjusted for age, BMI, baseline-lipid-component, time f/up (mos), and sex in the case of the combined data1 Life-Style model: adjusted for model 1 variables physical activity, total energy (kcal/day), alcohol, smoking, seasonality, poverty level, education and sex in the case of the combined data1

88
CVD model: adjusted for model 1 variables plus heart-disease (y/n), taking cardiovascular agents (y/n) and sex in the case of the combined data1.

89
FIGURE 1.1 Prevalence of low serum 25-hydroxyvitamin D concentration among Puerto Rican men (n=254) and women (n=667). Serum 25(OH)D concentration was categorized as: severe deficiency ≤ 25 nmol/l; deficiency 25-50 nmol/l, insufficiency 50-75 nmol/L, and sufficiency ≥ 75 nmol/L. Values are percentage of individuals.
0
10
20
30
40
50
60
Baseline 2-YR Baseline 2-YR
PE
RC
EN
TA
GE
≤ 25 nmol/L
25- 50 nmol/L
50 - 75 nmol/L
≥75 nmol/L
Men (n=254) Women (n=667)

90
FIGURE 1.2 The association between serum (25)OH at baseline and the change in HDL a (mg/dL) over time modified by smoking . M1: adjusted for age, BMI, baseline-lipid-component (mg/dL), time f/up (mos), and sex. M2: adjusted for model 1 variables physical activity, total energy (kcal/day), alcohol, seasonality, poverty level, education. M3: adjusted for model 1 + 2 variables plus heart-disease (y/n), taking cardiovascular agents (y/n)

91
FIGURE 1.3 The association between serum (25)OH at baseline and the change in LDL among
others over time modified by smoking. M1: adjusted for age, BMI, baseline-lipid-component (mg/dL), time f/up (mos), and sex. M2: adjusted for model 1 variables plus physical activity score, total energy (kcal/day), alcohol, seasonality, poverty level, education M3: adjusted for model 1+ 2 variables plus heart-disease (y/n), taking cardiovascular agents (y/n)

92
CHAPTER THREE
An Inverse Association of Vitamin D Serum Concentration and Inflammatory
Markers
The Boston Puerto Rican Osteoporosis Study
Aziza Jamal-Allial1, John L. Griffith2,3, Katherine L. Tucker 3
1Department of Pharmaceutical Science Department. 3Department of Health Sciences, 2Bouvé
College of Health Sciences. Northeastern University.
Boston, MA, USA 02115
Presented as a Poster at Experimental Biology 2013

93
ABSTRACT
Vitamin D deficiency has been linked to obesity, metabolic syndrome and autoimmune
diseases. Several reports suggest an association between serum 25-hydroxy vitamin D
concentration (25(OH)D) and inflammatory markers. We cross-sectionally examined the
relation between serum 25(OH)D concentration and serum inflammatory markers in 963 Puerto
Rican adults: 268 men and 695 women, aged 45-75 years. After adjusting for age, sex, and
seasonality, serum 25(OH)D was significantly negatively associated with tumor necrosis factor-
alpha (TNF-α) and Interleukin 6 (IL-6) (P<0.01 and P<0.04, respectively), but not with high-
sensitivity C-reactive protein (hsCRP). These associations remained significant adjusting for
waist circumference (WC), total body fat (TBF), and abdominal fat mass; and for smoking
status, alcohol intake, vitamin D supplementation and physical activity. In conclusion, lower
serum 25(OH)D concentration was significantly associated with higher concentration of
inflammatory markers in this population of older Puerto Rican adults living in the Boston area.
Longitudinal studies are needed to clarify causal pathways.

94
Abbreviations:
25-hydroxyvitamin D concentration (25(OH)D); android fat-mass (AFM); cardiovascular disease
(CVD); confidence interval [CI]; dual-energy x-ray absorptiometry (DXA); gynoid fat-mass
(GFM); high-sensitivity C-reactive protein (hsCRP); Human tumor necrosis factor-alpha (TNF-
α); Interleukin 6 (IL-6); Life-style model (LS-model); Non-steroidal anti-inflammatory drugs
(NSAIDs); Obesity model (O-model); Intact parathyroid hormone (iPTH); percent body fat
(%TBF); Risk factor model (RF-model); total body fat (TBF); white blood cell (WBC); food-
frequency questionnaire (FFQ).

95
INTRODUCTION
It is well recognized that vitamin D actions extend beyond calcium metabolism and bone
health [93, 94]. As a steroid hormone, vitamin D functions as a gene modulator for several
hundred genes. It regulates both-directly and indirectly the proliferation and differentiation of
immune cells including macrophages, monocytes and lymphocytes; initiating a phosphorylation
cascade of mitogen-activated protein kinases (MAPK) and extracellular signal-regulated kinase
(ERK); potentially participating in a cross-talk with the genomic pathway to modulate gene
expression [37-39, 144]. The expression of VDR in various types of cells, including immune
cells, supports the assumption that vitamin D may exert some immune modulator actions [4, 145,
146]. To date, a wide range of immune responses have been reported for vitamin D, including
the down regulation of a number of inflammatory responses, such as Interleukin 6 (IL-6), Human
tumor necrosis factor-alpha (TNF-α); and interferon-γ (IFN- γ) [4, 72, 145, 147] as well as high-
sensitivity C-reactive protein (hsCRP), a non-specific inflammatory marker [148, 149].
However, most of these reports are from animal studies, along with some in vitro work [147,
150-152]. Few have investigated the association of vitamin D and inflammation in humans [98,
153-155]. One observational study showed that serum 25(OH)D concentration was inversely
associated with TNF-α in women, after controlling for potential covariates [154]. Another study
showed that not only TNF-α, but also IL-6 and hsCRP, were inversely associated with 25(OH)D
[98]. In a double-blind, randomized, placebo-controlled trial (RCT), nine months of daily
supplementation with 2000 IU of vitamin D and 500 mg of calcium resulted in an improved
cytokine profile; in particular, lower TNF-α concentration were seen compared to baseline [153].
In a large randomized intervention trial, Beilfuss and colleagues demonstrated one year of
supplementation with vitamin D in the range between 40,000 to 20,000 IU/week, led to

96
marginally significant lower serum IL-6 concentration in the intervention arm compared to the
placebo arm. Interestingly, however, they observed significantly elevated hsCRP concentration
within the intervention arm [155].
Ethnic minorities generally, and Puerto Ricans specifically, carry a higher burden of
health disparities compared to non-Hispanic whites; which translates to a greater risk of chronic
disease [109-111]. Several studies have reported that ethnic minorities tend to have higher
concentration of inflammatory marker [156]. One systematic review showed that ethnic
minorities were considerably more likely to have vitamin D deficiency, across all age groups.
They concluded a number of potential mechanisms link vitamin D deficiency to obesity-related
chronic disease, including inflammation [112].
The aim of this study was to determine the cross-sectional association between serum
25(OH)D concentration and inflammatory markers, namely, IL-6, TNF-α, and hsCRP, among
participants of the Boston Puerto Rican Osteoporosis Study (BPROS).
MATERIALS AND METHODS
Study Population and Data Collection
Recruitment and data collection for the BPROS are described in detail elsewhere [113].
In brief, a bilingual interviewer conducted home visits and administrated a questionnaire that
collects information on socioeconomic status, education, household income, health and health
behaviors, medical diagnoses, current medications, depression, and psychological acculturation.
The interviewer measured anthropometrics, physical performance and blood pressure. The
following day, the study phlebotomist collected 24-hr urine, 12-hr fasting blood and saliva.

97
Participants were provided with written instructions for collecting urine, taking PABA tablets,
and fasting for the blood draw. Two days before the scheduled visit, participants were given a
reminder phone call and reinforced instruction for urine collection and overnight fasting.
Participants were asked to provide the 24-hour urine collection in two containers, one for every
12 hours. Once the 2-yr follow up visit was complete, participants were re-consented for the
BPROS. They visited the Human Nutrition Research Center on Aging (HNRCA) at Tufts
University for bone density and body composition measurements, and an additional blood draw.
Participants then completed additional questionnaires on sun exposure, family history of
osteoporosis, and history of fracture. All laboratory measurements for this study were performed
by the Nutrition Evaluation Laboratory at Tufts University.
By May 2013, 1257 participants completed 2year follow-up visits and 970 completed the
BPROS study. All study protocols were approved by the Institutional Review Boards at Tufts
Medical Center and Northeastern University, and each participant provided written informed
consent. There were no significant differences in socio-demographic characteristics between
those with complete or incomplete information. The present study includes complete data for 700
Puerto Rican women and 270 Puerto Rican men.
Covariates and Exposure Assessments
At each time point, in addition to the designed questionnaires, physical function tests
were completed and anthropometric measures were taken. w. Weight, and waist and hip
circumferences were measured in duplicate. Weight was measured using a clinical scale (Toledo
Weight Plate, Model I5S, Bay State, and Systems Inc. Burlington, MA). Body mass index (BMI)

98
was calculated as weight (kg) divided by height (m) squared [84, 85]. Diastolic and systolic
blood pressure were measured with an electronic sphygmomanometer (Dinamap TM Model
8260, Critikon, Tampa, FL), at three time points during home visits by trained interviewers: once
near the beginning, the middle, and then near the end of the interview, after a short rest during
which the subject was seated quietly. The average of the second and third readings was used in
the analysis.
Education was measured at baseline and defined using the 8th grade as a cutoff point;
poverty was measured at each time point and defined by the U.S. Department of Health and
Human Services federal poverty levels. Dietary vitamin D intake was estimated from a semi-
quantitative food-frequency questionnaire (FFQ) that was specifically designed for this
population [91]. This FFQ has been validated against serum carotenoids [116], and vitamin B12
[117] in a Hispanic population aged ≥ 60 years. Those with energy intakes < 600 or > 4800
kilocalories and/or > 10 questions blank on the FFQ were excluded from the analyses. Nutrient
intakes were calculated with the Nutrition Data System for Research (NDS-R) software version
2007 (Nutrition Coordinating Center, University of Minnesota, Minneapolis, MN, Food and
Nutrient Database 2007, released 2007). Alcohol intake (gm) was captured by the FFQ. For the
purpose of this paper, vitamin D deficiency was defined as serum 25(OH)D concentration below
50 nmol/L, insufficiency between 50-75 nmol/L, and sufficiency above 75 nmol/L [26, 157].
Seasonality was defined as summer, July to September; fall, October to December; winter,
January to March; and spring, April to June. Smoking status was categorized as yes or no for the
current behavior. Vitamin D from supplements was defined as: minimal 0-10 µg/day (200-400
IU/day); and high ≥ 10 µg/day (≥ 400 IU/day).

99
Laboratory assays
Fasting blood samples (12-h) were drawn by a certified phlebotomist at the participant’s
home on the morning after the home interview, or as soon thereafter as possible. Aliquots were
saved and stored at -80°C until processed. Serum 25(OH)D concentration was measured by
extraction, followed by 25I radioimmunoassay Packard COBRA II Gamma Counter (DiaSorin
Inc., Stillwater, MN 55082 catalog # 68100E); intra- and inter-assay CV% were 10.8% and
9.4%, respectively. Intact serum parathyroid hormone (IPTH) was detected by two-site
chemiluminescent enzyme-labeled immunometric assay (Diagnostic Products Corporation
(DCP) Los Angeles, CA ) [158]; intra- and inter-assay CV% were 5.5%, and 7.9%, respectively.
Serum creatinine was assessed with a colorimetric, kinetic reaction using the Olympus AU400e
with Olympus Creatinine Reagents (OSR6178) (Olympus America Inc., Melville, NY); intra-
and inter-assay CV% were 2.0%, and 4.0%, respectively. The hsCRP was measured by solid-
phase chemiluminescent immunometric assay; intra- and inter-assay CV% were 6.0%, and 7.3%,
respectively. Both IL-6 was and TNF-α were measured using commercial radioimmunoassay kit
(R&D Systems Inc, Minneapolis, MN). For IL-6, the intra- and inter-assay CV% was 1.6-4.2 %
and 3.3-6.4 %, respectively. For TNF-α, the intra- and inter-assay CV% was 5.3-8.8 %% and
10.8-16.7 % respectively. WBC (mm3) was measured by electronic impedance using ABX
Pentra 60 C+ (Baker Instruments Corp., Allentown, PA)
Statistical analyses:
All statistical analyses were conducted with SAS 9.1.3 (SAS Institute Inc, Cary, NC); and
all tests were 2-sided, with P <0.05 considered statistically significant. Dependent skewed
variables were natural log-transformed to normalize their distributions before the analysis.

100
Demographic and clinical characteristics were compared using Student’s t-tests for continuous
variables, and chi square tests for categorical variables. Characteristics were compared across sex
using two-tailed t-tests for two independent samples, and χ2 test for differences in proportion. We
applied Pearson Linear correlations to examine relationships between serum 25(OH)D
concentration and the different inflammatory markers, adjusting for age and sex. Further, we
applied the general linear models procedures (PROC GLM) to model the cross-sectional
associations between 25(OH)D (continuous) and inflammatory markers (continuous), and
adjusted for potential confounding variables. Linear trends of the inflammatory variables across
tertiles of 25(OH)D were adjusted for sex, seasonality, and age as well as other potential
covariates. The multivariate regression models for both IL-6 and TNF-α are: Risk-Factor model
(RF-model): adjusted for age (y), sex, seasonality, WBC count (mm3), and use of non-steroidal
anti-inflammatory (Y/N); the Obesity model (O-model): serum iPTH (pg/ml), BMI, total-fat
mass (g), and abdominal fat-mass (AFM), in addition to the prior model’s covariates; the Life-
Style model (LS-model): adjusted for the prior two models, in addition to physical activity,
current smoking status (y/n), alcohol intake (g/d), poverty level, and education. Some models
were adjusted for further covariates. The multivariate regression models for hsCRP are: Risk-
Factor model (RF-model): Sex, age seasonality, the use of non-steroidal anti-inflammatory
medication (Y/N), energy intake (kcal/day), smoking (Y/N), and WBC count (mm3) (to control
for current infection). Obesity model (O-model): RF-model+ BMI, total fat-mass (g), diastolic
blood pressure and diabetes (Y/N). Comprehensive Model (C-model): RF-model+ O-model,
poverty, and education. Linear trend tests were performed by assigning each participant the
median 25(OH)D for each tertile category, and using it as a continuous variable in PROC GLM.
For all linear models, we checked the assumptions of linearity and homogeneity through

101
examining the outcome residuals against the exposure. For all final models, we performed
influence diagnostics tests to check for outliers and influential points.
RESULTS
The mean ages of women and men were 60.3 ± 7.5 and 59.5 ± 8.0, respectively (Table
2.1). The mean serum 25(OH)D concentration for women was 50.1 ± 19.0, and was significantly
higher (P = 0.01) than for men, 47.0 ± 17.5 nmol/L. There was no significant difference between
men and women for most inflammatory markers, with the exception of hsCRP; where women
had significantly higher concentration than men, 3.5± 3.3 and 2.3±3.2 mg/L, respectively.
Women also had significantly higher adiposity measures than men, with the exception of WC,
where no significant difference was found (although this implies higher WC for women relative
to recommended WC). Puerto Rican women had significantly higher dietary vitamin D and
supplement intakes, and lower total energy intake (kcal/day) than men. Puerto Rican men walked
significantly more miles/day and had higher physical activity score compared to women. More
men reporting current smoking and current alcohol consumption compared to women, while
more women used non-steroidal anti-inflammatory drugs (NSAID) than did men 34.0% vs.
18.0%, respectively.
Both IL-6 and TNF-α concentrations showed significant inverse associations with
25(OH)D, (r = -0.1, P =0.0005) and (r = -0.11, P =0.001), respectively (Table 2.3). Per unit
increase in 25(OH)D, there was a corresponding significant reduction in IL-6 (β= -0.03 ±0.001,
P =0.01) and TNF-α (β=-0.002 ± 0.001, P =0.02). Further adjustment for covariates of both the

102
obesity and the life-style models did not attenuate these significant inverse associations.
Conversely, hsCRP showed no significant association with 25(OH)D in any model (Table 2.4).
We further evaluated the adjusted means of each inflammatory marker across the tertiles
of serum 25(OH)D concentration. Participants in the second and third tertile of 25(OH)D had
significantly lower IL-6 concentration compared to those in the lowest tertile, < 40 nmol/L, P
=0.04 and P =0.003, respectively (Figure 2.1). A similar trend was observed for TNF-α; those in
the highest tertile of 25(OH)D had significantly lower TNF-α concentration compared to those in
the lowest tertile of 25(OH)D, < 40 nmol/L (P =0.007) (Figure 2.2). There were significant
decreasing trends in IL-6 and TNF-α (P-trend = 0.002 and P-trend = 0.001) across 25(OH)D
tertiles. No significant trend was observed for hsCRP concentration (Figure 2.3)
DISCUSSION
The present study provides evidence of an inverse association between serum 25(OH)D
and inflammatory markers, namely, IL-6 and TNF-α, among participants of the BPROS;
irrespective of age, sex, seasonality, adiposity phenotype and lifestyle factors that include
smoking, physical activity and alcohol consumption. This population, as reported before,
exhibits a high prevalence of vitamin D deficiency [159]. After adjustment for potential
covariates, serum 25(OH)D concentration remained significantly associated with IL-6 and TNF-
α, but was not associated with hsCRP., These results are in accordance with several other reports
on the association between lower serum 25(OH)D concentration and inflammatory markers [98,
154, 155]. These results are also consistent with in vitro and animal studies that showed TNF-α
suppression by vitamin D [97, 152, 160, 161] and IL-6 [97, 147, 162]. One RCT, in heart failure

103
patients, demonstrated that 9 months of daily supplementation with 2000 IU of vitamin D and
500 mg of calcium significantly lowered serum TNF-α concentration [153]. Another RCT also
demonstrated a suppression of TNF-α concentration with a daily dose of a preparation that
contained 3332 IU of vitamin D [129].
The lack of association between serum 25(OH)D and hsCRP is not in agreement with a
number of cross-sectional reports [98, 163]. Possible explanations include that, first, hsCRP
concentration can be affected by acute phase reactions due to viral infection, which may increase
hsCRP by 50,000 fold. However, this is unlikely to be the case with the presence of constant yet
potent stimuli [149]. Another point to emphasize is that this specific population has a high
prevalence of health disparities that include metabolic syndrome, depression, and diabetes, which
might mask the association [109, 164]. Additionally, in this population the mean of 25(OH)D
concentration is low, with widespread vitamin D deficiency and thus, limited distribution and a
very low number of sufficient levels to show significant differences. In our analysis, the
adjustment of white blood cell counts, which is an indicator of current infection, did not improve
the null association between hsCRP and serum 25(OH)D concentration.
Higher serum concentration of inflammatory markers such TNF-α, IL-6 and hsCRP have
emerged as independent risk factors for CVD, diabetes and several autoimmune diseases, and are
often correlated with clinical impairment [165, 166]. Therefore, attenuating inflammatory marker
concentration may reduce risk of these conditions. When bound to its receptor, 1,25(OH)2D, the
active metabolite, has the ability to attenuate the high levels of inflammatory markers by down-
regulating a number of related genes [37-39, 144]. Our data suggest that serum 25(OH)D
concentration explains about 6-20% of the variation in the IL-6 and TNF-α concentration,
respectively, among our participants.

104
The findings of this report need to be understood in the context of some limitations. As a
cross-sectional study, it cannot provide further insight about causation or long-term status.
Longitudinal studies with two or more time points are needed to investigate the role of serum
25(OH)D concentration on inflammatory response. Although we were able to adjust for a
number of known cofounders, residual confounding might still a possibility.
In conclusion, the present study supports the hypothesis that inflammatory markers such
as IL-6 and TNF-α are inversely associated with serum 25(OH)D concentration in Puerto Rican
adults. These findings support the need to re-examine the determination of optimal vitamin D
status. However, more studies, especially longitudinal prospective studies, are needed to fully
characterize the relationship between serum 25(OH)D concentration and inflammatory markers.

105
BIBLIOGRAPHY
1. Holick, M.F., The vitamin D deficiency pandemic and consequences for nonskeletal
health: mechanisms of action. Mol Aspects Med, 2008. 29(6): p. 361-8. 2. Holick, M.F., Vitamin D: extraskeletal health. Endocrinology and metabolism clinics of
North America, 2010. 39(2): p. 381-400, table of contents. 3. Plum, L.A. and H.F. DeLuca, Vitamin D, disease and therapeutic opportunities. Nat Rev
Drug Discov, 2010. 9(12): p. 941-55. 4. Deeb, K.K., D.L. Trump, and C.S. Johnson, Vitamin D signalling pathways in cancer:
potential for anticancer therapeutics. Nature reviews. Cancer, 2007. 7(9): p. 684-700. 5. POLLY, P., et al., VDR-Alien: a novel, DNA-selective vitamin D3 receptor-corepressor
partnership. The FASEB Journal, 2000. 14(10): p. 1455-1463. 6. 2010 ICD-9-CM.
7. Guillot, X., et al., Vitamin D and inflammation. Joint Bone Spine, 2010. 77(6): p. 552-557.
8. Krishnan, A.V. and D. Feldman, Mechanisms of the anti-cancer and anti-inflammatory
actions of vitamin D. Annual review of pharmacology and toxicology, 2011. 51: p. 311-36.
9. Querfeld, U., Vitamin D and inflammation. Pediatr Nephrol, 2013. 28(4): p. 605-10. 10. Dickie, L.J., et al., Vitamin D3 down-regulates intracellular Toll-like receptor 9
expression and Toll-like receptor 9-induced IL-6 production in human monocytes. Rheumatology (Oxford), 2010. 49(8): p. 1466-1471.
11. Jacques M, L., Immunomodulatory actions of 1,25-Dihydroxyvitamin D3. The Journal of Steroid Biochemistry and Molecular Biology, 1995. 53(1–6): p. 599-602.
12. Wilson, A.M., M.C. Ryan, and A.J. Boyle, The novel role of C-reactive protein in
cardiovascular disease: risk marker or pathogen. Int J Cardiol, 2006. 106(3): p. 291-7. 13. Gabay, C. and I. Kushner, Acute-phase proteins and other systemic responses to
inflammation. N Engl J Med, 1999. 340(6): p. 448-54. 14. Rigby, W.F., S. Denome, and M.W. Fanger, Regulation of lymphokine production and
human T lymphocyte activation by 1,25-dihydroxyvitamin D3. Specific inhibition at the
level of messenger RNA. The Journal of Clinical Investigation, 1987. 79(6): p. 1659-1664.
15. Rigby, W.F., T. Stacy, and M.W. Fanger, Inhibition of T lymphocyte mitogenesis by 1,25-
dihydroxyvitamin D3 (calcitriol). The Journal of Clinical Investigation, 1984. 74(4): p. 1451-1455.
16. Zhu, Y., et al., Calcium and 1α,25-dihydroxyvitamin D3 target the TNF-α pathway to
suppress experimental inflammatory bowel disease. European Journal of Immunology, 2005. 35(1): p. 217-224.
17. Schleithoff, S.S., et al., Vitamin D supplementation improves cytokine profiles in patients
with congestive heart failure: a double-blind, randomized, placebo-controlled trial. American Journal of Clinical Nutrition, 2006. 83(4): p. 754-9.
18. Peterson, C. and M. Heffernan, Serum tumor necrosis factor-alpha concentrations are
negatively correlated with serum 25(OH)D concentrations in healthy women. Journal of Inflammation, 2008. 5(1): p. 10.

106
19. Beilfuss, J., et al., Effects of a 1-year supplementation with cholecalciferol on interleukin-
6, tumor necrosis factor-alpha and insulin resistance in overweight and obese subjects. Cytokine, 2012. 60(3): p. 870-4.
20. Bellia, A., et al., Serum 25-hydroxyvitamin D levels are inversely associated with
systemic inflammation in severe obese subjects. Internal and Emergency Medicine, 2013. 8(1): p. 33-40.
21. Mattei, J., et al., Allostatic load is associated with chronic conditions in the Boston
Puerto Rican Health Study. Social Science & Medicine, 2010. 70(12): p. 1988-96. 22. Tucker, K.L., et al., Self-reported prevalence and health correlates of functional
limitation among Massachusetts elderly Puerto Ricans, Dominicans, and non-Hispanic
white neighborhood comparison group. J Gerontol A Biol Sci Med Sci, 2000. 55(2): p. M90-7.
23. Tucker, K.L., O.I. Bermudez, and C. Castaneda, Type 2 diabetes is prevalent and poorly
controlled among Hispanic elders of Caribbean origin. Am J Public Health, 2000. 90(8): p. 1288-93.
24. Ranjit, N., et al., Socioeconomic Position, Race/Ethnicity, and Inflammation in the Multi-
Ethnic Study of Atherosclerosis. Circulation, 2007. 116(21): p. 2383-2390. 25. Renzaho, A.M., J.A. Halliday, and C. Nowson, Vitamin D, obesity, and obesity-related
chronic disease among ethnic minorities: a systematic review. Nutrition, 2011. 27(9): p. 868-79.
26. Bhupathiraju, S.N., et al., Centrally located body fat is associated with lower bone
mineral density in older Puerto Rican adults. The American Journal of Clinical Nutrition, 2011. 94(4): p. 1063-1070.
27. Bermudez, O.I., E.K. Becker, and K.L. Tucker, Development of sex-specific equations for
estimating stature of frail elderly Hispanics living in the northeastern United States. American Journal of Clinical Nutrition, 1999. 69(5): p. 992-8.
28. Chumlea, W., et al., Stature prediction equations for elderly non-Hispanic white, non-
Hispanic black, and Mexican-American persons developed from NHANES III data. J Am Diet Assoc, 1998. 98: p. 137 - 142.
29. Tucker, K., et al., Adaptation of a food frequency questionnaire to assess diets of Puerto
Rican and non-Hispanic adults. American Journal of Epidemiology, 1998. 148(5): p. 507 - 518.
30. Bermudez, O., et al., Hispanic and non-Hispanic white elders from Massachusetts have
different patterns of carotenoid intake and plasma concentrations. Journal of Nutrition, 2005. 135(6): p. 1496 - 1502.
31. Kwan, L.L., O.I. Bermudez, and K.L. Tucker, Low vitamin B-12 intake and status are
more prevalent in Hispanic older adults of Caribbean origin than in neighborhood-
matched non-Hispanic whites. Journal of Nutrition, 2002. 132(7): p. 2059-64. 32. Dawson-Hughes, B., et al., Estimates of optimal vitamin D status. Osteoporosis
International, 2005. 16(7): p. 713-716. 33. Holick, M.F., Vitamin D deficiency. N Engl J Med, 2007. 357(3): p. 266-81. 34. Document : PILKCR-7, 2003-11-25, High sensitivity CRP, and according to Immulate
1000 Operating Manual, Document #600467, rev B1, revision 5.XX August 2003, , D.P.C. (DCP), Editor 2003.

107
35. Jamal-Allial, A.A. and K.L. Tucker, Serum Vitamin D Concentrations, Dietary Sources,
and its relation to BMI among Puerto Ricans Living in the Greater Boston Area. To be submitted, 2013.
36. Giovannini, L., et al., 1,25-dihydroxyvitamin D3 dose-dependently inhibits LPS-induced
cytokines production in PBMC modulating intracellular calcium. Transplantation Proceedings, 2001. 33(3): p. 2366-2368.
37. Cohen, M., et al., Regulation of TNF-[agr] by 1[agr],25-dihydroxyvitamin D3 in human
macrophages from CAPD patients. Kidney International, 2001. 59(1): p. 69–75. 38. Alvarez-Rodriguez, L., et al., Age and low levels of circulating vitamin D are associated
with impaired innate immune function. Journal of Leukocyte Biology, 2012. 91(5): p. 829-838.
39. Nonn, L., et al., Inhibition of p38 by Vitamin D Reduces Interleukin-6 Production in
Normal Prostate Cells via Mitogen-Activated Protein Kinase Phosphatase 5:
Implications for Prostate Cancer Prevention by Vitamin D. Cancer Research, 2006. 66(8): p. 4516-4524.
40. Zittermann, A., et al., Vitamin D supplementation enhances the beneficial effects of
weight loss on cardiovascular disease risk markers. The American Journal of Clinical Nutrition, 2009. 89(5): p. 1321-1327.
41. Amer, M. and R. Qayyum, Relation between serum 25-hydroxyvitamin D and C-reactive
protein in asymptomatic adults (from the continuous National Health and Nutrition
Examination Survey 2001 to 2006). American Journal of Cardiology, 2012. 109(2): p. 226-30.
42. Falcon, L.M. and K.L. Tucker, Prevalence and correlates of depressive symptoms among
Hispanic elders in Massachusetts. J Gerontol B Psychol Sci Soc Sci, 2000. 55(2): p. S108-16.
43. Fantuzzi, G., Adipose tissue, adipokines, and inflammation. The Journal of allergy and clinical immunology, 2005. 115(5): p. 911-9; quiz 920.
44. Van Lente, F., Markers of inflammation as predictors in cardiovascular disease. Clin Chim Acta, 2000. 293(1-2): p. 31-52.
45. Dietary Reference Intakes for Calcium and Vitamin D. Committee to Review Dietary
Reference Intakes for Vitamin D and Calcium. , in 2010, Institute of Medicine: Washington, DC: National Academy of Sciences.

108
TABLE 2.1 Descriptive characteristic of the men and women of The Boston Puerto Rican
Osteoporosis Study
Variables Women (n=699 )
Men (n=273 )
P-value
Age (y) 60.3 ± 7.5 59.5 ± 8.0 0.2
Education (above 8th grade %) 49.0 44.3 0.1
Poverty (%) 59.0 49.2 0.009
Serum 25(OH)D (nmol/L) 50.1 ± 19.0 47.0 ± 17.5 0.01
Adiposity Variables
BMI (kg/m2) 33.0 ± 7.0 30.2 ± 5.5 <0.0001
Waist Circumference (cm) 104 ± 15 104 ± 14 0.4
Total Fat Mass (kg) 36.0 ± 1.5 26.5 ± 1.1 <0.0001
Android Fat mass (kg) 3.4 ± 1.3 3.0 ± 1.4 0.0007
Inflammatory Markers
Serum hsCRP (mg/L) $ 3.5± 3.3 2.3 ± 3.2 <0.0001
Serum TNF-α (pg/ml) $ 3.0 ± 1.5 3.1 ± 1.5 0.6
Serum IL-6 (pg/ml) $ 3.2 ± 2.3 3.1 ± 2.1 0.9
WBC x103/mm3 6.7 ± 2.1 6.8 ± 2.0 0.8
Other Covariates
Use of NSAIDs (%) 34.0 18.0 <0.0001
Current- smoking (%) 18.0 30.0 <0.0001

109
Current- alcohol drinking (%) 28.2 42.5 <0.0001
Physical Activity Score$‡ 31.3 ± 4.0 33.0 ± 6.0 <0.0001
Miles walking/day$‡ 1.4 ± 2.0 2.0 ± 2.4 0.0002
Dietary Measures
Vitamin D Supplement (>200IU/day) # (%)
30.2 18.5 0.0002
Total vitamin D intake (IU/day) || 288 ± 152 257 ± 123 0.002
Total energy intake (kcal/day) 1770 ± 825 2250± 1200 <0.0001
BMI, body mass index; 25(OH)D, 25-hydroxyvitamin D. 1Data are presented as mean ± SD for continuous variables or as % for categorical variables $Geometric mean ± SD Means were compared using t-tests. Percentages were compared using the Chi-square test (χ2) . ‡ The range for the physical activity score = 0-35.5 for Puerto Rican men and 26.4 for Puerto Rican women. Range for Miles/day =0- 22 for men and 0-20 miles/day for Puerto Rican women. #The recommended dietary allowance (RDA) for vitamin D for men and women aged 19-70 years =15 ug /day [82] ||Adjusted for energy intake using ANOVA (PROC GLM; SAS Institute, Cary, NC).

110
TABLE 2.2 Relationships between serum 25(OH)D concentration and inflammatory markers
Inflammatory Markers Serum 25(OH)D concentration
r p-value
Serum hsCRP (mg/L) - 0.05 0.1
Serum TNF-α (pg/ml) - 0.1 0.0005
Serum IL-6 (pg/ml) - 0.11 0.001
Pearson partial linear correlation coefficient (r) is age and sex adjusted 25(OH)D, 25-hydroxyvitamin D; hsCRP, high-sensitivity C-reactive protein; TNF-α, Tumor necrosis factor-alpha; IL-6, Interleukin 6.

111
TABLE 2.3: Adjusted associations between inflammatory markers and 25(OH)D concentration.
Serum 25(OH)D (nmol/L)
IL-6 TNF-α
β 1 SE p β SE p
Risk Factor - 0.003 0.001 0.01 - 0.002 0.001 0.02
Obesity - 0.003 0.001 0.01 - 0.0015 0.001 0.03
Life Style - 0.0024 0.001 0.03 - 0.002 0.001 0.02
1Regression coefficients (± SE) Risk Factor Model: Sex, age seasonality, WBC count (mm3), and use of Aspirin (Y/N) Obesity Model: Risk factor model + BMI, total fat-mass and android fat-mass Life Style Model: Risk-factor-model+ Obesity-model, smoking and Physical Activity Score

112
TABLE 2.4: Regression coefficients (± SE) from multivariate regression analysis of hsCRP
(mg/dL) and serum 25(OH)D concentration.
Serum 25(OH)D (nmol/L)
hsCRP (mg/dL)
β SE p
Risk Factor Model 0.002 0.002 0.3
Obesity Model 0.001 0.001 0.3
Comprehensive Model 0.0005 0.001 0.5
Risk Factor Model: Sex, age seasonality, WBC count (mm3), and use of non-steroidal anti-inflammatory (Y/N), energy intake (kcal/day) smoking (Y/N). Obesity Model: Risk factor model + BMI, total fat-mass (g) and android fat-mass (g), diastolic blood pressure and diabetes (Y/N) Comprehensive Model: Risk-factor-model+ Obesity-model, poverty, and education.

113
FIGURE 2.1 Adjusted means (±SEM) of IL-6 concentration (pg/ml) by tertiles of adjusted
serum 25(OH)D concentration among 893 Puerto Rican men and women. The LS-Means
adjusted for sex, age, BMI, total fat-mass, android fat-mass, physical activity, and smoking.
* Different from referent group (25(OH)D < 40 nmol/L) (Dunnett adjustment for multiple
comparisons; P < 0.05)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
< 40 nmol/L 41-55 nmol/L > 56 nmol/L
Seu
m I
L-6
con
cen
trati
on
(p
g/m
l)
Vitamin D Tertiles (nmol/L)
P-trend = 0.002
**

114
FIGURE 2.2 Adjusted means (±SEM) of TNF-α concentration (pg/ml) by tertiles of adjusted
serum 25(OH)D concentration among 893 Puerto Rican men and women. The LS-Means
adjusted for sex, age, BMI, total fat-mass, android fat-mass, physical activity, and smoking.
* Different from referent group (25(OH)D < 40 nmol/L) (Dunnett adjustment for multiple
comparisons; P < 0.05)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
< 40 nmol/L 41-55 nmol/L > 56 nmol/L
Seu
m T
NF
-αco
nce
ntr
ati
on
(p
g/m
l)
Vitamin D Tertiles (nmol/L)
P-trend = 0.001
*

115
FIGURE 2.3 Adjusted means (±SEM) of hsCRP concentration (mg/dL) by tertiles of adjusted
serum 25(OH)D concentration among 893 Puerto Rican men and women. The LS-Means
adjusted for sex, age, BMI, total fat-mass, WC count, use of NSAID’s, physical activity, and
smoking. Dunnett adjustment for multiple comparisons; P > 0.05
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
< 40 nmol/L 41-55 nmol/L > 56 nmol/L
Ser
um
hs-
CR
P
con
cen
trati
on
(m
g/d
L)
Vitamin D Tertiles (nmol/L)

116
Poster Presentation:
PDF of the presentation of Chapter Two data at Experimental Biology 2013

117
CHAPTER FOUR
Longitudinal Association of Vitamin D Serum Concentration & Adiposity
Phenotypes
Aziza Jamal-Allial1, John L. Griffith2,3, Katherine L. Tucker 3
1Department of Pharmaceutical Science. 3Department of Health Sciences, 2Bouvé College of
Health Sciences. Northeastern University.
Boston, MA, USA 02115
Submitted to the Journal of Steroid Biochemistry & Molecular Biology

118
ABSTRACT
Vitamin D deficiency is prevalent, especially among ethnic minorities. There are several
cross-sectional studies on the association between serum 25-hydroxy vitamin D concentration
(25(OH)D) concentration and adiposity measures such as body mass index (BMI), and waist
circumference (WC). We examined the longitudinal association between BMI and WC on serum
25(OH)D concentration in 970 Puerto Rican adults: 270 men and 700 women, aged 45-75 years.
Our analyses showed negative linear correlations at two time points between BMI (r = -0.1, P
=0.02) and WC (r = -0.1, P =0.009) and serum 25(OH)D concentration. Multivariate analysis
showed that baseline-BMI was significantly inversely associated with change in serum 25(OH)D
concentration (P<0.02), controlling for age and sex. This association remained significant after
adjusting for vitamin D supplement use, smoking, physical activity and alcohol intake. Baseline-
WC was not significantly associated with change in serum 25(OH)D concentration. The major
finding of the present study is that obesity appears to have a negative consequence on serum
25(OH)D concentration in this population of older Puerto Rican adults living in the Boston area,
which might accelerate vitamin D deficiency status.

119
ABBREVIATIONS:
25-hydroxyvitamin D (25(OH)D); cardiovascular disease (CVD); confidence interval (CI);
United States (USA); food-frequency questionnaire (FFQ); body mass index (BMI)

120
INTRODUCTION
The prevalence of overweight and obesity has increased among all socioeconomic
classes, leading to an increased risk of associated mortality and morbidity [167]. A recent report
suggested that vitamin D deficiency is another re-emerging global health problem that might
further contribute to an increase in the prevalence of related-chronic diseases [168]. Several
factors are known to influence 25-hydroxy vitamin D [25(OH)D] concentration, including age,
sex, sun exposure, skin pigmentation, ethnicity, adiposity, and physical activity [55, 56].
Ethnic minorities, generally, and Puerto Ricans, specifically, shoulder the greatest burden
of health disparities, including a greater risk of chronic disease [109-111]. In the United States
obesity continues to rise, specifically among minorities such as Hispanics, i.e. 39.1% [169, 170].
Additionally, a systematic review concluded that ethnic minorities have a significantly higher
risk of vitamin D deficiency among all age groups. They further concluded that there is a number
of indications that link vitamin D deficiency to obesity-related chronic disease [112].
The association between vitamin D deficiency and obesity has been consistently
documented, indicating that obesity is inversely associated with serum 25(OH)D [132, 171-173].
One of the postulated theories to explain this phenomenon is the sequestering of vitamin D into
adipose tissue, thus affecting its bioavailability for further metabolism [174, 175]. Another is that
obese individuals tend to have lower outdoor physical activity and greater time spent indoors
[173]. In the cross-sectional Tromsø study, BMI was significantly inversely associated with
serum 25(OH)D [132]. The Insulin Resistance Atherosclerosis (IRAS) Family study reported
that among Hispanics, 25(OH)D was inversely associated with adiposity phenotype; however, it
was not associated with 5-yr change in adiposity [176]. Another study demonstrated that serum

121
25(OH)D concentration was inversely associated with BMI (r = -0.18, P =0.005) and WC (r = -
0.14, P =0.03) [177].
The aim of this study was to determine the longitudinal association between serum
25(OH)D concentration in relation to BMI and WC among participants of the Boston Puerto
Rican Health Study (BPRHS) and the Boston Puerto Rican Osteoporosis Study (BPROS) in the
Greater Boston Area.
MATERIALS AND METHODS
Study Population and Data Collection
Recruitment and methods of the BPRHS [83] and its ancillary study, the BPROS [113],
are described in detail elsewhere. Concisely, at both time points, a bilingual interviewer
conducted home visits and administrated detailed questionnaires on general background,
socioeconomic status, education, household income, health and health behaviors that include
medical diagnosis, detailed use of medication(s), depression and a psychological acculturation
scale. They also answered questionnaires on dietary intake, food security, activities of daily
living, migration status, stress, depressive symptomology, and cognitive function. Moreover, the
interviewer collected information about anthropometrics, physical performance measures and
blood pressure. The following day, the study phlebotomist collected 12-hr urine, 12-hr fasting
blood and saliva. By December 2010, 1504 participants completed baseline visits. Once the 2-yr
follow up was completed, participants were re-consented for the BPROS. By May 2013, 1257
participants completed 2year follow-up visits and 970 of which completed the BPROS study.
These participants contributed 24-hr urine measures as well. All study protocols were approved

122
by the Institutional Review Boards at Tufts Medical Center and Northeastern University, and
each participant provided written informed consent.
There were no significant differences in socio-demographic characteristics between those
with complete or incomplete information. The present study includes complete longitudinal data
for 700 Puerto Rican women and 270 Puerto Rican men.
Covariates Assessments and Definition
Enrolled participants completed questionnaires that captured information on general
background and socioeconomic status, dietary intake, food security, health history, health
behaviors, health insurance, medical conditions and detail use of medication(s), activities of
daily living instrument, migration status, stress, depressive symptomology, and cognitive
function. Moreover, anthropometric and blood pressure measures, and physical function tests,
were completed. Weight, and waist and hip circumferences were measured in duplicate. Weight
was measured using a clinical scale (Toledo Weight Plate, Model I5S, Bay State, and Systems
Inc. Burlington, MA). Body mass index (BMI) was calculated as weight (kg) divided by height
(m) squared [27, 28]; BMI was categorized into: recommended (BMI <25), overweight (25-30),
and obese (≥ 30) [43]. For the purpose of this analysis, vitamin D deficiency was defined as
serum 25(OH)D concentration below 50 nmol/L, insufficiency between 50-75 nmol/L, and
sufficiency above 75 nmol/L [44, 45]. Seasonality was defined as summer, July to September;
fall, October to December; winter, January to March; and spring, April to June. Smoking status
was categorized into yes and no for the current behavior. Vitamin D from supplements was
defined as: minimal 0-10 µg/day (200-400 IU/day); and high ≥ 10 µg/day (≥ 400 IU/day).

123
Education level was measured at baseline and defined using the cutoff point of 8th grade while
poverty was measured at each time point and defined following the U.S. Department of Health
and Human Services. Dietary vitamin D intake was estimated from a semi-quantitative food-
frequency questionnaire (FFQ) that was specifically designed for this population [46]. This FFQ
has been validated against serum carotenoids [47], and vitamin B12 [48] in a Hispanic
population aged ≥ 60 years. Those with energy intakes < 600 or > 4800 kilocalories and/or > 10
questions blank on the FFQ were excluded from the analyses. Nutrient intakes were calculated
with the Nutrition Data System for Research (NDS-R) software version 2007 (Nutrition
Coordinating Center, University of Minnesota, Minneapolis, MN, Food and Nutrient Database
2007, released 2007). Alcohol intake (gm) was captured by the FFQ. Heart disease status was
self-reported by the participants.
Laboratory assays
Fasting blood samples (12-h) were drawn by a certified phlebotomist at the participant’s
home on the morning after the home interview, or as soon thereafter as possible. Aliquots were
saved and stored at -80°C until processed. Serum 25(OH)D concentration was measured by
extraction followed by 25I radioimmunoassay Packard COBRA II Gamma Counter (DiaSorin
Inc., Stillwater, MN 55082) catalog # 68100E with intra-assay and inter-assay CV% of 10.8%
and 9.4%, respectively. Serum creatinine was assessed with a colorimetric, kinetic reaction using
the Olympus AU400e with Olympus Creatinine Reagents (OSR6178) (Olympus America Inc.,
Melville, NY) with intra-assay and inter-assay CV% of 2.0%, and 4.0%, respectively.

124
Statistical analyses:
All statistical analyses were conducted with SAS 9.1.3 (SAS Institute Inc., Cary, NC);
and all tests were 2-sided with P <0.05 considered statistically significant. Dependent skewed
variables were natural log-transformed to normalize their distributions before the analysis.
Demographic and clinical characteristics were compared using student t-test for continuous
variables and chi square for categorical variables. Characteristics were compared by sex using
two-tailed t-test for two independent samples, and with χ2 test for differences in proportion.
Paired t-test was used to compare characteristics across time points. Pearson partial linear
correlation analysis was used to examine the relationship between serum 25(OH)D concentration
with adiposity phenotype at each time point, adjusting for age and sex. We constructed general
linear models (PROC GLM) to model longitudinal associations between the change in 25(OH)D
concentration (continuous) and adiposity phenotype (continuous). Because adiposity phenotype
might be sex-specific, we constructed sex-stratified analyses in addition to the full model, even if
the by-sex interaction term was not significant. Model-1 was adjusted for age (y), baseline-
25(OH)D (nmol/L/), serum creatinine (µmol/L), follow-up time (months), and sex in the full
model. In addition to model-1 covariates, model-2 included seasonality, dietary vitamin D &
supplements intake. Model-3 was adjusted for model-1 and 2 covariates plus physical activity,
alcohol intake (g), current smoking status (y/n), poverty level and education. Least-square means
and linear trends of 25(OH)D across the BMI categories were assessed using PROC GLM and
adjusted for multiple comparisons using Dunnett’s adjustment, with the lowest group as the
reference group. The model was repeated for each time point, independent of the other. The
model was adjusted for age (y), sex, seasonality, current smoking status (y/n), total energy intake
(kcal/d), physical activity, serum creatinine, dietary vitamin D & vitamin D supplement intake.

125
For all multivariate regression models, we checked the assumptions of linearity and
homogeneity through examining the outcome residuals against the exposure. For all final
models, we performed influence diagnostics tests to check for outliers and influential points. We
also tested all of our models for potential effect modifications by sex, with covariates such as
smoking, by including interaction terms in the model. The baseline concentration of each lipid
profile component was included as a covariate to all of our models to control for regression to
the mean [121]. To reduce bias and augment precision, we conducted multiple imputation
analysis to consider the uncertainty that missing values might convoy within our dataset. We
created a total of five imputed data sets with (seed= 32, 37854) using procedure (PROC MI); we
included all covariates that are considered risk factors and being used in any of our models. We
used (PROC MIANALYZE) to combine all the five imputed data sets, thus, producing valid
statistical inferences that accounts for within and between imputation variation [122]. We found
that these missing values produced no significant impact on our analysis.
RESULTS
Serum 25(OH)D concentration was available for 650 women and 255 men at baseline
and 2-yr. The mean ages of men and women were 59.5 ± 8.0 and 60.5 ± 8.0, respectively. The
mean follow-up time for women was 33.3± 12 months while men had a mean follow-up time
equal to 30.5 ± 49 months. At baseline, the mean serum 25(OH)D of the women and men was,
44.0 ± 17.5 and 43.0 ± 16.1 nmol/L, respectively, while the 2-year 50.1 ± 19.0 and 47.0 ± 17.5
nmol/L, respectively. Among all participants, the mean of 25(OH)D at 2-yr was 5.5 nmol/L
higher compared to baseline (P<0.0001). Compared to men, women at the 2-yr time point had

126
significantly higher serum 25(OH)D (p=0.02). Figure 3.1 shows the monthly distribution of
serum 25(OH)D for the two time points.
While BMI values did not differ between the two time points within each sex, Puerto
Rican women did exhibit significantly higher BMI compared to Puerto Rican men, i.e. 33.0 and
30 (P < 0.0001), respectively. On the contrary, WC did not differ between both sex, but it was
significantly higher at 2-yr compared to baseline (P < 0.0001). No significant change in the
participants’ dietary vitamin D intake. However, Puerto Rican women had higher dietary vitamin
D intake (IU/day) and higher use-rate of VD-containing supplements. Overall men had higher
energy intake (kcal/day) compared to women at both time points. On the other hand, there was a
clear significant reduction in total calories consumed, i.e. µ=365 kcal/day (P < 0.001) within the
2.5 years of follow-up.
Table 2 shows the age and sex Pearson linear correlation coefficients of serum 25(OH)D
concentration and adiposity phenotype. BMI and WC showed significant negative linear
correlation with serum 25(OH)D serum 25(OH)D at both time points. Baseline-BMI (r = -0.1, P
=0.006) and Baseline-WC (r = -0.1, P =0.02), 2yr-BMI (r = -0.1, P =0.01), 2yr-WC (r = -0.1, P
=0.01).
The longitudinal linear regression model (Table 3) showed that baseline-BMI was
significantly inversely associated with change in serum 25(OH)D concentration (β = -0.17, P
=0.04) controlling for age, sex, creatinine, and follow-up time. In model-2, the inclusion of
seasonality, dietary vitamin D & supplements did not alter the regression coefficient or its
significance. Nevertheless, the additional adjustment of the association for miles/day, alcohol,
smoking, poverty index, and education status (model-3), strengthened the inverse association (β
= - 0.21, P =0.01). The adjusted-mean serum 25(OH)D was significantly lower with increased

127
obesity among the participants at both time points, P-trend <0.01 and <0.002, respectively (Fig.
1). At baseline, participants with BMI ≥ 40 had significantly lower 25(OH)D (38.5 ± 1.5 nmol/L)
compared to BMI ≤ 25 (44.5 ± 1.2 nmol/L), while at the 2-yr time point, participants with BMI
who were classified as obese had significantly lower 25(OH)D (45.5 ± 1.2 nmol/L) compared to
BMI ≤ 25 (50.1 ± 1.5 nmol/L).
DISSCUSION
The results of our longitudinal analysis confirm the inverse association between low
serum 25(OH)D concentration and BMI. Our observation of lower adjusted mean serum
25(OH)D concentration in obese, severely obese and morbidly obese participants is in agreement
with many studies [132, 172, 176, 177]. Our longitudinal multivariate linear regression showed
that baseline-BMI was negatively associated with the change in serum 25(OH)D concentration
(P =0.01), independent of covariates including age, sex, serum creatinine, physical activity,
smoking, alcohol, seasonality, poverty and education. Conversely, we did not observe similar
longitudinal associations with WC, although it was significantly correlated with serum 25(OH)D
at both time points.
The mechanism that can explain the phenomena of low serum 25(OH)D and increased
adiposity risk is not clear. A review by Earthman and colleague discusses a number of proposed
theories that link Vitamin D deficiency to adiposity [178]. One theory suggests that because
Vitamin D is fat-soluble, it might be sequestered within adipose tissue. They further suggest that
the adipose tissue of obese individuals might have higher 25(OH)D uptake and storage relative to
lean individuals [48, 178]. Another theory suggests that due to the fact that adiposity, especially

128
visceral adiposity, contributes to a high inflammatory state, this in turn, contributes to lower
serum 25(OH)D concentration [178, 179]. Another hypothesis suggests that because of increased
adiposity, there may possibly be an increase of the action of 24-hydroxylase, leading to amplified
catabolism of vitamin D [178, 180]. Consequently, further research is needed to elucidate our
understanding of how vitamin D may be affected by adiposity or how vitamin D affects obesity.
More than 60% of the participants of BPROS had serum 25(OH)D concentration below
50 nmol/L, which is considered deficient, according to the Endocrine Society [115]. A recent
report by the National Health and Nutrition Examination Survey (NHANES) III, showed that
more than 42% of their 2001-2006 participants had a vitamin D concentration below 50 nmol/L;
when stratified by ethnicity, Hispanics were second highest in vitamin D deficiency with 70%
[181]. Our prior report indicated that among 1502 participants of the BPRHS, more than 70%
had serum 25(OH)D concentration below 50 nmol/L at baseline, concurring with the NHANES
III data [159]. This greater risk of vitamin D deficiency may be related to greater risk of health
disparities [182]. A report by Palacios and colleagues showed that Puerto Ricans who are
residing in Puerto Rico, had higher serum 25(OH)D concentration, approximately 75 nmol/L,
compared to our population, at baseline 43.4 ± 17.2 nmol/L [159] and 2yr 50.0 ± 19.0 nmol/L.
This difference in serum 25(OH)D concentration is likely due to sun exposure, generally, and
latitude, specifically, i.e. Puerto Rico is at 18.26° while Boston is at 42.35° [26].
The present study has limitations: we did not have direct measures of sun exposure at
baseline. However, our study has substantial strengths: a total large sample size with low attrition
and the use of a detailed questionnaire with an FFQ that allowed detailed information.

129
In summary, serum 25(OH)D concentration was inversely associated with 2.5-yr change
in BMI. The adjusted-mean serum 25(OH)D concentration showed a declining trend, at both
time points, with greater BMI, especially when reaching class III obesity.

130
BIBLIOGRAPHY
1. Organization, W.H., Noncommunicable diseases country profiles 2011. WHO global
report, 2011. p. 209.
2. Mithal, A., et al., Global vitamin D status and determinants of hypovitaminosis D.
Osteoporosis International, 2009. 20(11): p. 1807-20.
3. Holick, M.F., Vitamin D status: measurement, interpretation, and clinical application.
Ann Epidemiol, 2009. 19(2): p. 73-8.
4. Holick, M.F. and T.C. Chen, Vitamin D deficiency: a worldwide problem with health
consequences. Am J Clin Nutr, 2008. 87(4): p. 1080S-6S.
5. Mattei, J., et al., Allostatic load is associated with chronic conditions in the Boston
Puerto Rican Health Study. Social Science & Medicine, 2010. 70(12): p. 1988-96.
6. Tucker, K.L., et al., Self-reported prevalence and health correlates of functional
limitation among Massachusetts elderly Puerto Ricans, Dominicans, and non-Hispanic white
neighborhood comparison group. J Gerontol A Biol Sci Med Sci, 2000. 55(2): p. M90-7.
7. Tucker, K.L., O.I. Bermudez, and C. Castaneda, Type 2 diabetes is prevalent and poorly
controlled among Hispanic elders of Caribbean origin. Am J Public Health, 2000. 90(8): p.
1288-93.
8. Ogden CL, C.M., Kit BK, Flegal KM., Prevalence of obesity in the United States, 2009–
2010. NCHS data brief, 2012, National Center for Health.
9. Flegal Km, C.M.D.K.B.K.O.C.L., Prevalence of obesity and trends in the distribution of
body mass index among us adults, 1999-2010. JAMA, 2012. 307(5): p. 491-497.
10. Renzaho, A.M., J.A. Halliday, and C. Nowson, Vitamin D, obesity, and obesity-related
chronic disease among ethnic minorities: a systematic review. Nutrition, 2011. 27(9): p. 868-79.
11. Renzaho, A.M.N., J.A. Halliday, and C. Nowson, Vitamin D, obesity, and obesity-related
chronic disease among ethnic minorities: A systematic review. Nutrition, 2011. 27(9): p. 868-
879.
12. Jorde, R., et al., Cross-sectional and longitudinal relation between serum 25-
hydroxyvitamin D and body mass index: the Tromsø study. European Journal of Nutrition, 2010.
49(7): p. 401-407.
13. Snijder, M.B., et al., Adiposity in relation to vitamin D status and parathyroid hormone
levels: a population-based study in older men and women. Journal of Clinical Endocrinology &
Metabolism, 2005. 90(7): p. 4119-23.
14. Brock, K., et al., Low vitamin D status is associated with physical inactivity, obesity and
low vitamin D intake in a large US sample of healthy middle-aged men and women. J Steroid
Biochem Mol Biol, 2010. 121(1-2): p. 462-6.
15. Norman, A.W., Minireview: vitamin D receptor: new assignments for an already busy
receptor. Endocrinology, 2006. 147(12): p. 5542-8.

131
16. Tuohimaa, P., Vitamin D and aging. Journal of Steroid Biochemistry & Molecular
Biology, 2009. 114(1-2): p. 78-84.
17. Young, K.A., et al., Association of Plasma Vitamin D Levels with Adiposity in Hispanic
and African Americans. Journal of Clinical Endocrinology & Metabolism, 2009. 94(9): p. 3306-
3313.
18. McGill, A.-T., et al., Relationships of low serum vitamin D3 with anthropometry and
markers of the metabolic syndrome and diabetes in overweight and obesity. Nutrition Journal,
2008. 7: p. 4.
19. Tucker, K., et al., The Boston Puerto Rican Health Study, a longitudinal cohort study on
health disparities in Puerto Rican adults: challenges and opportunities. BMC Public Health,
2010. 10(1): p. 107.
20. Bhupathiraju, S.N., et al., Centrally located body fat is associated with lower bone
mineral density in older Puerto Rican adults. The American Journal of Clinical Nutrition, 2011.
94(4): p. 1063-1070.
21. Holick, M.F., et al., Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an
Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology &
Metabolism, 2011. 96(7): p. 1911-1930.
22. Dawson-Hughes, B., et al., Estimates of optimal vitamin D status. Osteoporos Int, 2005.
16(7): p. 713-6.
23. Flegal, K.M., et al., Overweight and obesity in the United States: prevalence and trends,
1960-1994. International journal of obesity and related metabolic disorders : journal of the
International Association for the Study of Obesity, 1998. 22(1): p. 39-47.
24. Tucker, K., et al., Adaptation of a food frequency questionnaire to assess diets of Puerto
Rican and non-Hispanic adults. American Journal of Epidemiology, 1998. 148(5): p. 507 - 518.
25. Bermudez, O., et al., Hispanic and non-Hispanic white elders from Massachusetts have
different patterns of carotenoid intake and plasma concentrations. Journal of Nutrition, 2005.
135(6): p. 1496 - 1502.
26. Kwan, L.L., O.I. Bermudez, and K.L. Tucker, Low vitamin B-12 intake and status are
more prevalent in Hispanic older adults of Caribbean origin than in neighborhood-matched non-
Hispanic whites. Journal of Nutrition, 2002. 132(7): p. 2059-64.
27. Earthman, C.P., et al., The link between obesity and low circulating 25-hydroxyvitamin D
concentrations: considerations and implications. Int J Obes, 2012. 36(3): p. 387- 96.
28. Wortsman, J., et al., Decreased bioavailability of vitamin D in obesity. The American
Journal of Clinical Nutrition, 2000. 72(3): p. 690-693.
29. Compher, C. and K.O. Badellino, Obesity and Inflammation: Lessons From Bariatric
Surgery. Journal of Parenteral and Enteral Nutrition, 2008. 32(6): p. 645-647.
30. Li, J., et al., 1α,25-Dihydroxyvitamin D hydroxylase in adipocytes. The Journal of Steroid
Biochemistry and Molecular Biology, 2008. 112(1–3): p. 122-126.

132
31. Looker, A.C.J., C L. Lacher, D A. Pfeiffer, C M. Schleicher, R L. Sempos, C T.,
Vitamin D status: United States, 2001–2006, in NCHS data brief2011, National Center for
Health Statistics: Hyattsville, MD.
32. Jamal-Allial, A.A. and K.L. Tucker, Serum Vitamin D Concentrations, Dietary Sources,
and its relation to BMI among Puerto Ricans Living in the Greater Boston Area. To be
submitted, 2013.
33. Forrest, K.Y.Z. and W.L. Stuhldreher, Prevalence and correlates of vitamin D deficiency
in US adults. Nutrition Research, 2011. 31(1): p. 48-54.
34. Holick, M.F., Vitamin D deficiency. N Engl J Med, 2007. 357(3): p. 266-81.

133
TABLE 3.1 Descriptive characteristic of men and women in the Boston Puerto Rican Health
Study (BPRHS) & Boston Puerto Rican Osteoporosis Study (BPROS)
Baseline (n=1504)
Two Year (n=970)
Women (n=1050)
Men (n=445)
Women (n=700 )
Men (n=270)
Age (y) 57.0 ± 7.3 56.0 ± 8.0 60.3 ± 7.5 59.5 ± 8.0
Education (>8th grade %) 51.5 55.5 -- --
Poverty (%) 60.0 49.0$$ 59.0 48.5$$
Serum 25(OH)D (nmol/L) §§§ 44.0± 17.4 43.0 ± 16.5 50.1 ± 19.0 47.0 ± 17.5*
Follow-up time (months) -- -- 33.3± 12 30.5± 49
BMI (kg/m2) 33.2 ± 7.0 30.0 ± 5.3*** 33.0 ± 7.0 30.2 ± 5.5***
Waist Circumference (cm) §§§ 102.2 ± 15.4 103 ± 14 104 ± 15 104 ± 14
Miles walking/day§§§ 1.0 ± 1.5 1.4 ± 2.0*** 1.4 ± 2.0 2.0 ± 2.4 ***
Current- smoking (%) 20.1 32.5$$$ -- --
Current- alcohol drinking (%) 36.0 51.0$$$ -- --
Vitamin D Supplement (>200IU/day) (%)
30.0 24.1 30.2 18.5$$
Total vitamin D intake (IU/day) 291 ± 172 280 ± 178 288 ± 152 257 ± 123.*
BMI, body mass index; 25(OH)D, 25-hydroxyvitamin D. 1Data are presented as mean ± SD for continuous variables or as % for categorical variables Means were compared using t-test for between sex (within each time points): *P -value <0.05, ** P -value <0.001, ***P-value <0.0001
Means were compared using paired t-test for between time points: §P -value <0.05,
§§P -value
<0.001, §§§
P-value <0.0001
Percentages were compared using Chi-square test for between sex (within each time points): $P -value <0.05, $$
P -value <0.001, $$$ P-value <0.0001

134
TABLE 3.2 Pearson partial linear correlation of serum 25(OH)D concentration and adiposity
phenotype at baseline and 2-year
Baseline Two-Year
25(OH)D p-value 25(OH)D p-value
BMI -0.1 0.006 -0.1 0.01
WC -0.1 0.02 -0.1 0.01
Pearson partial linear correlation coefficient (r) is age and sex adjusted Abbreviations: BMI, body mass index; 25(OH)D, 25-hydroxyvitamin D; WC, waist circumference; AFM, abdominal fat mass; TBF, total body fat; %TBF, total body fat percentage

135
TABLE 3.3 Regression coefficients (± SE) of adiposity phenotypes on plasma 25(OH)D concentration
Adiposity Phenotype
Change in 25(OH)D (nmol/L)
Baseline-BMI β ± SE P-value
Baseline-WC β ± SE P-value
ALL (n=866)
Men (n=246)
Women (n=620)
ALL
(n=864) Men
(n=245) Women (n=619)
β ± SE p β ±SE p β ± SE p β ± SE p β ±SE p β ± SE p
Model 1 -0.17 (± 0.1)
0.04 -0.25 (± 0.2)
0.1 -0.13 (± 0.1)
0.1 -0.03 (± 0.03)
0.3 -0.06 (± 0.07)
0.3 -0.02 (± 0.04)
0.5
Model 2 -0.22 (± 0.1)
0.01 -0.26 (± 0.2)
0.1 -0.15 (± 0.1)
0.1 -0.03 (± 0.03)
0.3 -0.06 (± 0.1)
0.3 -0.02 (± 0.04)
0.6
Model 3 -0.22 (± 0.1)
0.01 -0.3 (± 0.2)
0.1 -0.20 (± 0.1)
0.04 -0.03 (± 0.03)
0.3 -0.06 (± 0.1)
0.3 -0.03 (± 0.04)
0.4
Model 1: adjusted for age, baseline 25(OH)D, serum creatinine, time f/up (mos), and sex in the case of the combined data1 Model 2: adjusted for model 1 variables plus seasonality, dietary vitamin D & supplements and sex in the case of the combined data1
Model 3: adjusted for model 1 variables plus physical activity, alcohol, smoking, poverty level, education and sex in the case of the combined data1

136
FIGURE 3.1 The monthly distribution of serum 25(OH)D for the participants of BPRHS at both time points

137
FIGURE 3.2 The adjusted means of serum 25(OH)D concentration within the categories of class III obesity LS-Means adjusted for Sex, age seasonality, miles/day, vitamin D supplements, dietary VD, smoking, and total calories. * Different from referent group (BMI ≥ 25) (Dunnett adjustment for multiple comparisons; P < 0.05)
35
37
39
41
43
45
47
49
51
53
55
25 & lessIdeal
25-30Overwieght
30-35 Obese 35-40 Severeobesity
40 & moreMorbidobesity
Ser
um
25(O
H)D
nm
ol/
L
BMI Categories
Baseline
Two-Year
*
*
P-trend < 0.002
P-trend < 0.01

138
Poster Presentation:
PDF of the presentation of Chapter Three data at Vitamin D Workshop 2013

139
CHAPTER FIVE
The Association of Total and Regional Adiposity with Serum 25-
hydroxyvitamin D Concentration
The Boston Puerto Rican Osteoporosis Study (BPROS)
Aziza Jamal-Allial1, John L. Griffith2,3, Katherine L. Tucker 3
1Department of Pharmaceutical Science Department. 3Department of Health Sciences,
2Bouvé College of Health Sciences. Northeastern University.
Boston, MA, USA 02115

140
ABSTRACT
Vitamin D deficiency is prevalent, especially among ethnic minorities. There are
several cross-sectional studies on the association between serum 25-hydroxyvitamin D
concentration (25(OH)D) and adiposity phenotype; specifically: total body fat (TBF),
percent body fat (%TBF), android fat-mass (AFM) and gynoid fat-mass (GFM), using
dual-energy x-ray absorptiometry (DXA). We examined this association among 970
Puerto Rican adults, 270 men and 700 women; aged 45-75, years from the Boston Puerto
Rican Osteoporosis study. Our analyses showed that TBF-in kilograms-or %TBF was
not significantly associated with serum 25(OH)D. Moreover, AFM showed inverse
significant association with serum 25(OH)D in both Puerto Rican men and women,
whereas GFM showed a positive significant association with serum 25(OH)D among
Puerto Rican women only. This suggests that obesity is negatively associated with serum
25(OH)D concentration in this population of older Puerto Rican adults living in the
Boston area.

141
ABBREVIATIONS:
25-hydroxyvitamin D concentration (25(OH)D); android fat-mass (AFM); cardiovascular
disease (CVD); 95% confidence interval (95% CI); dual-energy x-ray absorptiometry
(DXA);gynoid fat-mass (GFM) ;Life-Style model (LS-model); Obesity model (O-model);
Parathyroid Hormone, Intact (iPTH); percent body fat (%TBF); Risk Factor model (RF-
model); total body fat (TBF); United States (USA).

142
INTRODUCTION
Ethnic minorities, generally, and Puerto Ricans, specifically, are shown to carry a
greater burden of health disparities than non-Hispanic whites, which results in a greater
risk of chronic disease [109-111]. Obesity in the United States (USA) is on the rise,
especially among minorities such as Hispanics, i.e. 38.7% (95% confidence interval [CI],
33.5%- 43.9%) [169, 170, 183]. A 2010 report by Flegal indicated that Hispanic men and
women exhibit different prevalence of obesity after the age 40; 37.4% (95% CI, 29.0-
45.8) and 46.6% (95% CI, 37.3-55.9), respectively [183]. Casa and colleagues found that
ethnicity might be associated with moderately higher prevalence of obesity compared to
non-Hispanic whites; with about a 5% higher BMI. They also reported that percentage
body-fat was about 4% greater among Hispanic, relative to non-Hispanic white, women-
especially in the arms and trunks areas [184].
Android obesity, or central obesity, is when the predominant fat deposition is in
the abdomen, while gynoid obesity is when the predominant fat deposition occurs in the
hip area [185]. Android obesity is thought to be related to increased risk of cardiovascular
disease (CVD), while gynoid obesity is less related to CVD [186]. Whereas most of the
research on the association between serum 25(OH)D concentration and adiposity
measures have focused on BMI, it is not clear how AFM and GFM are associated with
serum 25(OH)D concentration.
Vitamin D deficiency is emerging as a global health problem that may lead to an
increase of chronic disease, including CVD, osteoporosis and other immune-related
diseases [56, 168]. Several factors are known to influence serum 25(OH)D concentration,

143
including age, sex, sun exposure, skin pigmentation, ethnicity, adiposity, and physical
activity [49, 55, 56]. It is suggested that some ethnic minorities are more susceptible to an
increased risk of vitamin D deficiency than others [176, 187]. In a systematic review,
Renzaho and colleagues discuss that ethnic minorities have a significantly higher risk of
vitamin D deficiency among all age groups. They conclude that there is a number of
indications linking vitamin D deficiency to obesity-related chronic disease among
minorities [112]. Our prior report showed that the mean serum 25(OH)D concentration
in Puerto Rican adults in the Greater Boston Area was 43.5 ± 16.5 nmol/L [159]. One
postulated theory to explain this phenomenon is the sequestering of vitamin D into
adipose tissue, thus affecting its bioavailability for further metabolism [49, 174, 175].
Another is that people who are obese tend to have lower outdoor physical activity, and
increased time spent indoors [173]. Numerous studies have investigated the association
between adiposity and serum 25(OH)D concentration, applying different indexes of
adiposity [48, 60, 64, 132, 172, 173, 176, 184, 188-190]. The Longitudinal Aging Study
Amsterdam showed that TBF was inversely associated with 25(OH)D [172]. A study in
south-east Texas showed that among Hispanics, the mean serum 25(OH)D was 48
nmol/L, and was inversely associated with %TBF (r = -0.28, P < 0.001) and TBF (r = -
0.33, P < 0.001) [188]. A study of Puerto Ricans in Puerto Rico showed that serum
25(OH)D was significantly inversely correlated with %TBF (r = -0.24, P=0.02) [60].
The aim of this cross-sectional study was to determine the association between
serum 25(OH)D concentration in relation to total body fat-mass (TBF) and percent-body-
fat (%TBF), and its various components, in the participants of the Boston Puerto Rican

144
Osteoporosis Study (BPROS). We included android fat-mass (AFM) and gynoid fat-mass
(GFM), using dual-energy x-ray absorptiometry (DXA).
MATERIALS AND METHODS
Study Population and Data Collection
Description of the recruitment and methods of the BPROS are described in detail
elsewhere [113]. Concisely, a bilingual interviewer conducted home visits and
administrated a detailed questionnaire on socioeconomic status, education, household
income, health and health behaviors that includes: medical diagnosis and current
medication use, depression, and psychological acculturation. Additionally, the
interviewer collected anthropometrics, physical performance measures, and measured
blood pressure. The day after this interview, the study phlebotomist collected 12-hr urine
and 12-hr fasting blood and saliva. Once the 2-yr follow up was complete, participants
were re-consented for the BPROS. By May 2013, 1257 participants completed 2year
follow-up visits and 970 had completed the BPROS study, which included a 24-hr urine
collection. All study protocols were approved by the Institutional Review Boards at Tufts
Medical Center and Northeastern University, and each participant provided written
informed consent.
There were no significant differences in socio-demographic characteristics
between those with complete or incomplete information. The present study includes
complete data for 700 Puerto Rican women and 270 Puerto Rican men.

145
Covariates Assessments and Definition
For the purpose of this analysis, vitamin D deficiency was defined as serum
25(OH)D concentration below 50 nmol/L, insufficiency between 50-75 nmol/L, and
sufficiency above 75 nmol/L [26, 157]. Seasonality was defined as summer, July to
September; fall, October to December; winter, January to March; and spring, April to
June. Smoking status was categorized into yes or no for the current behavior. Vitamin D
from supplements was defined as: minimal 0-10 µg/day (200-400 IU/day); and high ≥ 10
µg/day (≥ 400 IU/day). Participant’s education was measured at baseline and defined
using the cutoff point of 8th grade while poverty was measured at each time point and
defined by the U.S. Department of Health and Human Services federal poverty levels.
Dietary vitamin D intake was estimated from a semi-quantitative food-frequency
questionnaire (FFQ) specifically designed for this population [91]. This FFQ has been
validated against serum carotenoids [116], and vitamin B12 [117] in a Hispanic
population aged ≥ 60 years. Those with energy intakes < 600 or > 4800 kilocalories
and/or > 10 questions blank on the FFQ were excluded from the analyses. Nutrient
intakes were calculated with the Nutrition Data System for Research (NDS-R) software
version 2007 (Nutrition Coordinating Center, University of Minnesota, Minneapolis,
MN, Food and Nutrient Database 2007, released 2007). Alcohol intake (g) was captured
by the FFQ.

146
Exposure Assessment:
All fat-mass measures were obtained using DXA whole-body scans (Lunar
Prodigy, GE Healthcare, Madison, WI) using software Encore version 6.1. Total body
scans were carried out on consenting participants, and all scans followed a standardized
protocol to ensure consistency. Daily quality assurance scans were performed, as well as
weekly scans of various thickness phantoms to examine the stability of the instrument.
The precision of the total body fat and lean tissue were, 0.94% and 0.77%, respectively
[191]. Android and gynoid measurements were based on the percentage of fat within each
body region. AFM (kg) was defined as the area between the ribs and the pelvis. The
upper demarcation is 20% of the distance between the iliac crest or the pelvis and the
femoral neck. The GFM (kg) was defined as the region including the hips and upper
thighs overlapping leg and trunk regions. Its upper demarcation, below the pelvis cut, is
defined as 1.5 times the android height, with total height as twice the height of the AFM
region (Figure 4.1). The lateral boundaries of both AFM and GFM were defined as arms
and legs [192]. Percentage total body fat, %TBF, is determined as a ratio of total-fat-mass
to total body mass, both in (kg).
Laboratory assays
Fasting blood samples (12-h) were drawn by a certified phlebotomist at the
participant’s home on the morning after the home interview, or as soon thereafter as
possible. Aliquots were saved and stored at -80°C until processed. Serum 25(OH)D
concentration was measured by extraction followed by 25I radioimmunoassay Packard
COBRA II Gamma Counter (DiaSorin Inc., Stillwater, MN 55082) catalog # 68100E

147
with intra-assay and inter-assay CV% of 10.8% and 9.4%, respectively. Serum intact
parathyroid hormone (iPTH) was detected by solid-phase, two-site chemiluminescent
enzyme-labeled immunometric assay using the Immulate 1000 Diagnostic Products
Corporation (Los Angeles, CA 90045-5597) with intra-assay and inter-assay CV% of
5.5%, and 7.9%, respectively. Serum creatinine was assessed with a colorimetric, kinetic
reaction using the Olympus AU400e with Olympus Creatinine Reagents (OSR6178)
(Olympus America Inc., Melville, NY) with intra-assay and inter-assay CV% of 2.0%,
and 4.0%, respectively.
Statistical analyses:
All statistical analyses were conducted with SAS 9.1.3 (SAS Institute Inc, Cary,
NC); and all tests were 2-sided with P <0.05 considered statistically significant.
Dependent skewed variables were natural log-transformed to normalize their distributions
before the analysis. Demographic and clinical characteristics were compared using
Student’s t-test for continuous variables and chi square tests for categorical variables.
Characteristics were compared by sex using two-tailed t-test for two independent
samples, and with χ2 test for differences in proportion. Pearson partial linear correlation
analysis was used to examine the relationship between serum 25(OH)D concentration
with adiposity, adjusting for age and sex. We constructed general linear models (PROC
GLM) to model the cross-sectional associations between 25(OH)D (continuous) and fat-
mass (continuous). The Risk Factor model (RF-model) was adjusted for age (y), serum
creatinine (nmol/L), serum iPTH (pg/ml), and sex in the full model. The Dietary model
(D-model) included serum seasonality, dietary vitamin D and supplements, and total

148
energy (kcal/day) in addition to the prior model covariates. The Life-Style model (LS-
model) was adjusted for prior models in addition to physical activity, current smoking
status (y/n), alcohol intakes (g/d), poverty level, and education. For all linear models, we
checked the assumptions of linearity and homogeneity through examining the outcome
residuals against the exposure. For all final models, we performed influence diagnostics
tests to check for outliers and influential points.
RESULTS
The mean ages of women and men were 60.3 ± 7.5 and 59.5 ± 8.0, respectively
(Table 1). The mean serum 25(OH)D for women was 50.1 ± 19.0, significantly higher (P
= 0.01) compared to men, 47.0 ± 17.5 nmol/L. Women had significantly higher adiposity
than men for most measures. Women also had significantly higher dietary vitamin D and
supplement intakes. Men walked significantly more miles/day and had higher physical
activity scores compared to women. Men also reported higher levels of smoking and
alcohol consumption compared to the women.
Only AFM was significantly negatively correlated with serum 25(OH)D (r = -0.1,
P =0.02), while TBF approached significance (r = -0.06, P =0.07) (Table 4.3). The
multivariate regression analysis of the associations of DXA TBF-in kilogram-or %TBF-
were not significantly associated with serum 25(OH)D, adjusting for potential covariates
(Table 4.3).
In the RF-model, AFM was significantly negatively associated with serum
25(OH)D (β = -0.003, P =0.009). This inverse association remained significant after
further adjustment for the covariates (β = -0.003, P =0.01). Even though the interaction

149
term of AFM and sex was not significant, but regional adiposity might be sex-specific,
thus, we stratified by sex. Among Puerto Rican men, the additional adjustment for the
covariates of the LS-model did not attenuate the association between AFM and serum
25(OH)D (β = -0.002, P =0.008) explaining approximately 22% of the variability in
serum 25(OH)D. Among Puerto Rican women, only the additional adjustments of LS-
model covariates appreciably emphasized the significantly inverse association between
AFM and 25(OH)D (β = -0.003, P =0.03).
GFM was not a significant predictor of serum 25(OH)D when controlling for the
covariates of the RF-model. However, with additional adjustment for the covariates of D-
model and LS-model, GFM was positively significantly associated with 25(OH)D (β =
0.002, P =0.02). Interestingly, when the analyses were stratified by sex, the positive
associations remained significant among Puerto Rican women only (β = 0.002, P =0.04)
(Figure 4.2).
DISCUSSION
These results provide support to the current dialogue on adiposity, in general, and
fat-mass-in terms of amount and region-in particular, with vitamin D status. By initially
focusing on TBF-as measured by DXA-and serum 25(OH)D concentration, we did not
discern any significant association. Similarly, none of our models were significant for
%TBF. On the other hand, when we further investigated the role of regional adiposity,
precisely, android and gynoid fat-mass, our results showed a distinct picture. AFM was
negatively associated with serum 25(OH)D after adjusting for several potential covariates

150
including, age, serum creatinine, serum iPTH, seasonality, supplements and dietary
vitamin D, smoking, alcohol, and total energy, thus, demonstrating the independent
negative association of android adiposity on serum 25(OH)D concentration. In contrast,
GFM was significantly positively associated with serum 25(OH)D (P =0.02) independent
of age, serum creatinine, serum iPTH, seasonality, supplements and dietary vitamin D,
smoking, alcohol, and total energy.
We reported earlier that vitamin D deficiency remains prevalent in this Hispanic
subgroup, indicating that vitamin D deficiency is not a transient health concern, thus,
predisposing this population to higher levels of mortality and morbidity [182]. Recently,
we reported that the change in BMI over time was negatively associated with the change
in serum 25(OH)D concentration (P =0.01) independent of various known factors
including age, sex, serum creatinine, physical activity, smoking alcohol, seasonality,
poverty and education [193]. Taken together, our results are in agreement with a number
of epidemiological studies demonstrating that measures of adiposity including TBF, BMI,
and regional adiposity are inversely associated with serum 25(OH)D concentration [48,
49, 132, 171-173].
The association between vitamin D and adiposity, in general, and regional
adiposity, specifically, was explained by Lumb and colleagues in 1971. They were the
first to introduce the hypothesis of vitamin D sequestration in the adipose tissue and
muscle [76]. Later on, they substantiated that hypothesis and confirmed the link between
adiposity and vitamin D [77]. Subsequently, Wortsman and colleagues confirmed the
aforementioned premise, stating that deposition within the adipose tissue lowers the
bioavailability of serum 25(OH)D and 1,25(OH)2D leading to vitamin D

151
insufficiency/deficiency. They showed lower serum 25(OH)D and higher iPTH among
obese people [48]. AFM has been associated with higher mortality independent of BMI
[194] and is a known risk factor for many serious health disparities including CVD,
hypertension, dyslipidemia and insulin resistance [194-196], as well as inflammation
[179, 197].
The results of our study should be interpreted within the context of some
limitations. First, due to the cross-sectional nature, causality cannot be inferred, but the
results are in agreement with a number of cross-sectional studies [172, 188, 190].
Another potential limitation is that with the use of DXA, the differentiation between
visceral and subcutaneous fat is not feasible. However, it was shown by Savgan-Gurol
and colleagues that the percentage fat shown by DXA was significantly associated with
visceral fat (r = -0.83, P < 0.0001), while the association with subcutaneous was lower (r
= -0.77, P < 0.001) [198]. This only suggests that the importance of android fat-mass as
an indicator of central obesity might be greater compared to the relative distribution of
visceral and subcutaneous fat.
In conclusion, our findings of the negative, significant association of AFM on
serum 25(OH)D concentration; while GFM was positively associated with serum
25(OH)D concentration, highlights the importance of differences in body composition on
vitamin D status. Although it is clear that some of the association between regional
adiposity and serum 25(OH)D concentration may be attributed to the sequestration of
vitamin D in adipose tissues, it is still considered a complex relationship and more work
is needed to elucidate the relationship between adipose tissue and vitamin D and the
effect both to overall health.

152
BIBLIOGRAPHY
1. Mattei, J., et al., Allostatic load is associated with chronic conditions in the
Boston Puerto Rican Health Study. Social Science & Medicine, 2010. 70(12): p. 1988-96.
2. Tucker, K.L., et al., Self-reported prevalence and health correlates of functional
limitation among Massachusetts elderly Puerto Ricans, Dominicans, and non-Hispanic
white neighborhood comparison group. J Gerontol A Biol Sci Med Sci, 2000. 55(2): p.
M90-7.
3. Tucker, K.L., O.I. Bermudez, and C. Castaneda, Type 2 diabetes is prevalent and
poorly controlled among Hispanic elders of Caribbean origin. Am J Public Health, 2000.
90(8): p. 1288-93.
4. Ogden CL, C.M., Kit BK, Flegal KM., Prevalence of obesity in the United States,
2009–2010. NCHS data brief, 2012, National Center for Health.
5. Flegal Km, C.M.D.K.B.K.O.C.L., Prevalence of obesity and trends in the
distribution of body mass index among us adults, 1999-2010. JAMA, 2012. 307(5): p.
491-497.
6. Flegal, K.M., et al., PRevalence and trends in obesity among us adults, 1999-
2008. JAMA, 2010. 303(3): p. 235-241.
7. Casas, Y.G., et al., Total and regional body composition across age in healthy
Hispanic and white women of similar socioeconomic status. The American Journal of
Clinical Nutrition, 2001. 73(1): p. 13-18.
8. Bermudez, O.I. and K.L. Tucker, Total and central obesity among elderly
Hispanics and the association with Type 2 diabetes. Obes Res, 2001. 9(8): p. 443-51.
9. Bhupathiraju, S.N., et al., Centrally located body fat is associated with lower bone
mineral density in older Puerto Rican adults. The American Journal of Clinical Nutrition,
2011. 94(4): p. 1063-1070.
10. Wiklund, P., et al., Abdominal and Gynoid Fat Mass Are Associated with
Cardiovascular Risk Factors in Men and Women. Journal of Clinical Endocrinology &
Metabolism, 2008. 93(11): p. 4360-4366.

153
11. McCarty, M.F., A paradox resolved: the postprandial model of insulin resistance
explains why gynoid adiposity appears to be protective. Medical Hypotheses, 2003.
61(2): p. 173-176.
12. Mithal, A., et al., Global vitamin D status and determinants of hypovitaminosis D.
Osteoporosis International, 2009. 20(11): p. 1807-20.
13. Holick, M.F. and T.C. Chen, Vitamin D deficiency: a worldwide problem with
health consequences. Am J Clin Nutr, 2008. 87(4): p. 1080S-6S.
14. Holick, M.F., Vitamin D status: measurement, interpretation, and clinical
application. Ann Epidemiol, 2009. 19(2): p. 73-8.
15. Liel, Y., et al., Low circulating vitamin D in obesity. Calcified tissue international,
1988. 43(4): p. 199-201.
16. Weishaar, T. and J.M. Vergili, Vitamin D Status Is a Biological Determinant of
Health Disparities. Journal of the Academy of Nutrition and Dietetics, 2013. 113(5): p.
643-651.
17. Young, K.A., et al., Association of Plasma Vitamin D Levels with Adiposity in
Hispanic and African Americans. Journal of Clinical Endocrinology & Metabolism,
2009. 94(9): p. 3306-3313.
18. Jamal-Allial, A.A. and K.L. Tucker, Serum Vitamin D Concentrations, Dietary
Sources, and its relation to BMI among Puerto Ricans Living in the Greater Boston Area.
To be submitted, 2013.
19. Renzaho, A.M., J.A. Halliday, and C. Nowson, Vitamin D, obesity, and obesity-
related chronic disease among ethnic minorities: a systematic review. Nutrition, 2011.
27(9): p. 868-79.
20. Norman, A.W., Minireview: vitamin D receptor: new assignments for an already
busy receptor. Endocrinology, 2006. 147(12): p. 5542-8.
21. Tuohimaa, P., Vitamin D and aging. Journal of Steroid Biochemistry & Molecular
Biology, 2009. 114(1-2): p. 78-84.
22. Brock, K., et al., Low vitamin D status is associated with physical inactivity,
obesity and low vitamin D intake in a large US sample of healthy middle-aged men and
women. J Steroid Biochem Mol Biol, 2010. 121(1-2): p. 462-6.

154
23. McKinney, K., C.R. Breitkopf, and A.B. Berenson, Association of race, body fat
and season with vitamin D status among young women: a cross-sectional study. Clinical
Endocrinology, 2008. 69(4): p. 535-541.
24. Wortsman, J., et al., Decreased bioavailability of vitamin D in obesity. The
American Journal of Clinical Nutrition, 2000. 72(3): p. 690-693.
25. Snijder, M.B., et al., Adiposity in relation to vitamin D status and parathyroid
hormone levels: a population-based study in older men and women. Journal of Clinical
Endocrinology & Metabolism, 2005. 90(7): p. 4119-23.
26. Parikh, S.J., et al., The Relationship between Obesity and Serum 1,25-Dihydroxy
Vitamin D Concentrations in Healthy Adults. Journal of Clinical Endocrinology &
Metabolism, 2004. 89(3): p. 1196-1199.
27. Palacios, C., et al., Determinants of vitamin D status among overweight and obese
Puerto Rican adults. Ann Nutr Metab, 2012. 60(1): p. 35-43.
28. Jorde, R., et al., Cross-sectional and longitudinal relation between serum 25-
hydroxyvitamin D and body mass index: the Tromsø study. European Journal of
Nutrition, 2010. 49(7): p. 401-407.
29. Botella-Carretero, J.I., et al., Vitamin D deficiency is associated with the
metabolic syndrome in morbid obesity. Clinical Nutrition, 2007. 26(5): p. 573-80.
30. Arunabh, S., et al., Body Fat Content and 25-Hydroxyvitamin D Levels in Healthy
Women. Journal of Clinical Endocrinology & Metabolism, 2003. 88(1): p. 157-161.
31. Dawson-Hughes, B., et al., Estimates of optimal vitamin D status. Osteoporosis
International, 2005. 16(7): p. 713-716.
32. Holick, M.F., Vitamin D deficiency. N Engl J Med, 2007. 357(3): p. 266-81.
33. Tucker, K., et al., Adaptation of a food frequency questionnaire to assess diets of
Puerto Rican and non-Hispanic adults. American Journal of Epidemiology, 1998.
148(5): p. 507 - 518.
34. Bermudez, O., et al., Hispanic and non-Hispanic white elders from Massachusetts
have different patterns of carotenoid intake and plasma concentrations. Journal of
Nutrition, 2005. 135(6): p. 1496 - 1502.

155
35. Kwan, L.L., O.I. Bermudez, and K.L. Tucker, Low vitamin B-12 intake and status
are more prevalent in Hispanic older adults of Caribbean origin than in neighborhood-
matched non-Hispanic whites. Journal of Nutrition, 2002. 132(7): p. 2059-64.
36. White, J., et al., Precision of single vs bilateral hip bone mineral density scans.
Journal of clinical densitometry : the official journal of the International Society for
Clinical Densitometry, 2003. 6(2): p. 159-62.
37. Mazess, R.B., et al., Dual-energy x-ray absorptiometry for total-body and
regional bone-mineral and soft-tissue composition. The American Journal of Clinical
Nutrition, 1990. 51(6): p. 1106-12.
38. Forrest, K.Y.Z. and W.L. Stuhldreher, Prevalence and correlates of vitamin D
deficiency in US adults. Nutrition Research, 2011. 31(1): p. 48-54.
39. Jamal-Allial, A.A., J.L. Griffith, and K.L. Tucker, The Longitudinal Association
of Vitamin D Serum Concentrations & Adiposity Phenotypes. To be submitted, 2013.
40. Renzaho, A.M.N., J.A. Halliday, and C. Nowson, Vitamin D, obesity, and obesity-
related chronic disease among ethnic minorities: A systematic review. Nutrition, 2011.
27(9): p. 868-879.
41. Lumb, G.A., E.B. Mawer, and S.W. Stanbury, The apparent vitamin D resistance
of chronic renal failure: A study of the physiology of vitamin D in man. The American
Journal of Medicine, 1971. 50(4): p. 421-441.
42. Mawer, E.B., et al., The distribution and storage of vitamin D and its metabolites
in human tissues. Clin Sci, 1972. 43(3): p. 413-31.
43. Jacobs, E.J., et al., WAist circumference and all-cause mortality in a large us
cohort. Archives of Internal Medicine, 2010. 170(15): p. 1293-1301.
44. Panagiotakos, D.B., et al., The implication of obesity and central fat on markers
of chronic inflammation: The ATTICA study. Atherosclerosis, 2005. 183(2): p. 308-315.
45. Dos Santos, R.E., et al., Relationship of body fat distribution by waist
circumference, dual-energy X-ray absorptiometry and ultrasonography to insulin
resistance by homeostasis model assessment and lipid profile in obese and non-obese
postmenopausal women. Gynecological Endocrinology, 2005. 21(5): p. 295-301.

156
46. Compher, C. and K.O. Badellino, Obesity and Inflammation: Lessons From
Bariatric Surgery. Journal of Parenteral and Enteral Nutrition, 2008. 32(6): p. 645-647.
47. Fontana, L., et al., Visceral Fat Adipokine Secretion Is Associated With Systemic
Inflammation in Obese Humans. Diabetes, 2007. 56(4): p. 1010-1013.
48. Savgan-Gurol, E., et al., Waist to hip ratio and trunk to extremity fat (DXA) are
better surrogates for IMCL and for visceral fat respectively than for subcutaneous fat in
adolescent girls. Nutrition & Metabolism, 2010. 7(1): p. 86.
49. Dietary Reference Intakes for Calcium and Vitamin D. Committee to Review
Dietary Reference Intakes for Vitamin D and Calcium. , in 2010, Institute of Medicine:
Washington, DC: National Academy of Sciences.

157
FIGURE 4.1 The illustrations of android region (AFM) and gynoid region (GFM)

158
FIGURE 4.2 The β coefficients of the association between serum 25(OH)D concentration with gynoid and android fat among Puerto Rican men and women adjusted for age and serum creatinine (mg/dL), serum iPTH (pg/ml), total fat-mass (g), seasonality, dietary vitamin D and supplements, total energy (kcal/day), physical activity, alcohol, smoking, poverty level, education and sex in the All data.

159
TABLE 4.1 Descriptive characteristics of men and women in Boston Puerto Rican
Osteoporosis Study (BPROS)
Variables Women (n=699 )
Men (n=273 )
P-value
Age (y) 60.3 ± 7.5 59.5 ± 8.0 0.2
Education (above 8th grade %) 49.0 44.3 0.1
Poverty (%) 59.0 49.2 0.009
Serum 25(OH)D (nmol/L) 50.1 ± 19.0 47.0 ± 17.5 0.01
Adiposity Variables
BMI (kg/m2) 33.0 ± 7.0 30.2 ± 5.5 <0.0001
Waist Circumference (cm) 104.0 ± 15.0 104.3 ± 14.3 0.4
Total Fat-mass (kg) 36.0 ± 1.5 26.5 ± 1.1 <0.0001
Android Fat-mass (kg) 3.4 ± 1.3 3.0 ± 1.4 0.0007
Gynoid Fat-mass (kg) 6.0 ± 2.1 4.1± 2.0 <0.0001
Andriod:Gynoid 1.05 ± 0.13 1.3 ± 0.22 <0.0001
Average fat percentage 44.4 ± 6.5 30.0± 7.5 <0.0001
Other Covariates
Current- smoking (%) 18.0 30.0 <0.0001
Current- alcohol drinking (%) 36.0 51.0 <0.0001
Physical Activity Score$‡ 31.3 ± 4.0 33.0 ± 6.0 <0.0001
Miles walking/day$‡ 1.4 ± 2.0 2.0 ± 2.4 0.0002

160
Dietary Measures
Vitamin D supplement (>200IU/day) # (%) 30.2 18.5 0.0002
Total vitamin D intake (IU/day) || 287.5 ± 152.0 257.0 ± 123.0 0.002
Total energy intake (kcal/day) 1770.0 ± 825 2250± 1200 <0.0001
BMI, body mass index; 25(OH)D, 25-hydroxyvitamin D. 1Data presented as mean ± SD for continuous variables, or as % for categorical variables $Geometric mean ± SD For between sex’s comparisons, t-test was used for means and Chi-square test χ2- test was used for percentages. ‡ Range for Physical Activity Score = 35.5 for men and 26.4 for women. Range for Miles/day = 22 for men and 20 miles/day for women. #The recommended dietary allowance (RDA) for vitamin D for men and women aged 19-70 years =15 ug /day [82] ||Adjusted for energy intake using ANOVA

161
TABLE 4.2 Pearson partial linear correlation of serum 25(OH)D concentration and
adiposity phenotype at 2-year
2-year
25(OH)D p-value
TBF - 0.06 0.07
%TBF - 0.03 0.3
AFM -0.1 0.02
GFM -0.04 0.2
Pearson partial linear correlation coefficient (r) is age and sex adjusted Abbreviations: BMI, body mass index; 25(OH)D, 25-hydroxyvitamin D; WC, waist circumference; AFM, abdominal fat-mass; TBF, total body fat; %TBF, total body fat percentage

162
TABLE 4.3 Regression coefficients (± SE) from cross-sectional regression analysis of
TBF and %TBF on plasma 25(OH)D concentration.
Serum 25(OH)D (nmol/L)
Adiposity Phenotype
TBF
%TBF
β SE P-value β SE P-value
Risk Factor Model
- 0.0001 0.00005 0.2 - 0.03 0.1 0.7
Dietary Model
- 0.00005 0.00005 0.2 - 0.03 0.1 0.6
Life-Style Model
- 0.0001 0.00005 0.1 - 0.1 0.1 0.3
TBF, total body fat; TBF%, total body fat percentage Risk Factor Model: adjusted for age and creatinine (mg/dL), serum iPTH (pg/ml) and Dietary Model: adjusted for model 1 variables plus seasonality, dietary vitamin D and supplements, total energy (kcal/day).
Life-Style Model: adjusted for model 1+ 2 variables plus physical activity, alcohol, smoking, poverty level and education.

163
TABLE 4.4 Regression coefficients (± SE) from cross-sectional regression analysis of AFM and GFM on plasma 25(OH)D
concentration.
Adiposity Phenotype
Serum 25(OH)D (nmol/L)
AFM β ± (SE)
GFM β ± (SE)
All1 Men Women All1 Men Women
β ± SE P β ± SE P β ± SE P β ± SE P β ± SE P β ± SE P
Risk Factor Model
-0.003 ± 0.001
0.009 -0.004 ± 0.003
0.1 -0.002 ± 0.001
0.1 0.001 ± 0.001
0.06 0.001 ± 0.002
0.1 0.002 ± 0.001
0.09
Dietary Model:
-0.003 ± 0.001
0.01 -0.002 ± 0.001
0.008 -0.001 ± 0.0005
0.2 0.002 ± 0.001
0.03 0.001 ± 0.002
0.4 0.002 ± 0.001
0.04
Life-Style Model
-0.003 ± 0.001
0.01 -0.002 ± 0.001
0.01 -0.003 ± 0.001
0.03 0.002 ± 0.001
0.02 0.001 ± 0.002
0.5 0.002 ± 0.001
0.04
AFM, android- fat-mass; GFM, gynoid-fat-mass. Risk Factor Model: adjusted for age and serum creatinine (mg/dL), serum iPTH (pg/ml), total fat-mass (g) and sex in the case of the combined data1 Dietary Model: adjusted for model 1 variables plus seasonality, dietary vitamin D and supplements, total energy (kcal/day).
Life-Style Model: adjusted for model 1+ 2 variables plus physical activity, alcohol, smoking, poverty level, education.

164
CHAPTER SIX
DISCUSSION AND SUMMARY
Understanding the association between plasma 25-hydroxyvitamin D concentration
(25(OH)D) concentration and cardiovascular disease (CVD) is important. . This dissertation was
designed to examine the multiple pathways through which serum 25(OH)D as the biomarker of
vitamin D status could affect longitudinally as well as cross-sectionally a number of CVD
associated risk factors, namely, lipid profile, adiposity, and inflammation among the participants
of the Boston Puerto Rican Health Study (BPRHS) and the Boston Puerto Rican Osteoporosis
Study (BPROS).
Foremost, it is well documented in the literature that dyslipidemia, i.e. high plasma LDL-
C, TG and low plasma HDL-C, is highly associated with increased risk of CVD along with other
factors such as high blood pressure [2, 128, 199]. In the first report of this doctoral work, our
results are in apparent contrast to scores of reports that indicate serum 25(OH)D concentration is
positively associated with plasma high-density lipoprotein (HDL-C), and negatively associated
with plasma low-density lipoprotein (LDL-C), total cholesterol (TC), and triglycerides (TG) [4-
10]. We showed that even though serum 25(OH)D concentration was positively associated with
plasma HDL-C cross-sectionally, the longitudinal analyses illustrated different yet interesting
associations; it showed that baseline-25(OH)D demonstrated a negative, yet significant,
association with 2.5-year change in plasma HDL-C concentration (β = -0. 04, P =0.01); an
association independent of important putative confounders including age, sex, body mass index
(BMI), total energy, physical activity, smoking, alcohol, seasonality, poverty and education. We

165
demonstrated this association not only within the life-style model, but throughout the
confounding by indication adjustment in our CVD-model. Similar relationships were found with
plasma TG, but not with LDL-C and TC. In the prospective Health Professionals Follow-up
Study (HPFS), Giovannucci and colleagues demonstrated a positive linear trend of LDL-C,
HDL-C and TC, as well as a negative trend with plasma TG across serum 25(OH)D quartiles
among 900 US men, ages 64 and older [125]. Another study showed that serum 25(OH)D was
independently associated with higher HDL-C and lower TG; but not TC [107]. Interestingly, two
studies reported that both HDL-C and LDL-C were positively associated with serum 25(OH)D
concentration, thus, both are being affected in a the same direction, i.e. increasing their plasma
concentration. It is well known that one favorable approach to lower CVD risk is to increase
HDL-C and lower LDL-C [2, 128]. A report by Melamed and colleagues, found that when
analyzing Third National Health and Nutrition Examination Survey (NHANES III), serum
25(OH)D concentration were significantly inversely associated with TC, among 13,331 US men
and women ages 20 years and older. However, they found no association between plasma HDL-
C and serum 25(OH)D among their participants [96]. Another longitudinal study with a 14 year
follow up found that among 1762 participants, serum 25(OH)D and plasma TG were inversely
associated [104]. Few key differences can be outlined and prior studies are mostly cross-
sectional; no proof of a causal relationship can be inferred. One difference to illustrate is that our
results are longitudinal, and we have controlled for numerous confounders, which were not
necessarily available among previous cross-sectional studies.
On the contrary our results are in accordance with a number of reports that found serum
25(OH)D concentration might not be associated with atheroprotective lipid profile [96, 104, 105,
123, 127]. A study by Jorde and colleagues found that TC was significantly associated with

166
increased serum 25(OH)D concentration among 8,018 Norwegian men and women, ages 43-70
years [104]. Two other studies found that plasma TG were positively associated with serum
25(OH)D; however, both studies investigated this effect among children [123, 127]. Intervention
studies in the form of placebo-controlled randomized trials (RCT’s) are designed to confirm or
dispute any causal relationship. Exceptionally few RCT have been conducted to investigate the
question in discussion, and their results have largely been inconsistent on the effect of vitamin D
supplementations on improving lipid profile [108, 129-131]. A study by Zittermann and
colleagues showed that daily vitamin D supplementation (3320 IU/day) for one year had a
significant effect on plasma lipids. They found that the supplemented group had lower plasma
TG compared to the placebo, -13.5% and +3% (P =0.001) correspondingly; nonetheless, the
supplemented group exhibited a significant increase in plasma LDL-C [129]. Conversely, this
was not the case for the study by Jorde and colleagues; they were not able to demonstrate that
one year of vitamin D supplementation, 40, 000 IU/week, improved the plasma lipids of the 438
overweight/obese participants [108]. Another study showed that vitamin D supplementation
might not be atheroprotective among postmenopausal women [130]. Most of these RCT’s can be
criticized for a rather low sample size, which might have contributed to the null results.
The relationship between plasma HDL-C and serum 25(OH)D concentration is
particularly noteworthy. The significance of the interaction term of smoking status with serum
25(OH)D was interesting. The significant impact of serum 25(OH)D on HDL-C among non-
smokers was unexpected, however similar results were reported by Jorde and colleagues [132].
They found that among the participants of the Tromsø study, smokers had higher levels of serum
25(OH)D concentration; about 15-20%, compared to non-smokers. They thought it might be due
to a difference in methodology, i.e. immunological vs. LC-MSMS, and excluded them from the

167
analysis. The pathophysiological mechanism by which smoking may impact serum 25(OH)D
concentration or the metabolism of 1,25(OH)2D has not been investigated. However, it has been
discussed that smoking might influence 25-hydroxylase (CYP2R1) thus, lowering serum
25(OH)D concentration [133]. Another point that might explain this paradox is that, smoking
contains nicotine, which exerts anti-inflammatory properties [134, 135].
Despite the disagreement of our results with many epidemiologic and ecological studies
for the protective effective role of serum 25(OH)D on lipid profile as a major risk factor for
CVD, the contradictory yet significant evidence we show cannot be disregarded. One
explanation for these phenomena is that vitamin D induces the intestinal absorption of dietary
calcium, thus lowering calcium fecal excretion [37, 95]. This might affect the amount of fatty
acids in the fecal due to the reduction in the formation of insoluble fatty soaps [136]. Thus,
leading to an increased rate of the absorption of fat, thus higher plasma LDL-C and TG
concentration, in particular, and TC in general [137]. In addition, higher vitamin D might
decrease cholesterol excretion because of the lower availability of calcium within the intestine,
and hence less binding to bile acids [138]; this would translate into less cholesterol converting
into bile acids. One study suggested that higher calcium intake might augment the prior
phenomena and lower LDL-C by increasing not only vitamin D but it has been accompanied by
calcium supplements. A 15-week weight loss trial study by Major and colleagues showed that
among 63 healthy, overweight/obese women, the daily supplementation of 600 mg of calcium
and 200 IU of vitamin D significantly improved LDL-C as well as LDL: HDL-C ratio, while
HDL-C and TG approached significance level [139].
Secondly, there is considerable evidence that inflammation is one element of the
development of CVD. Higher serum concentration of inflammatory markers such TNF-α, IL-6

168
and hsCRP have emerged as independent risk factors for CVD [165, 166]. Therefore, attenuating
these inflammatory markers concentration may influence risk of such illnesses. Vitamin D may
have the ability to attenuate the high levels of inflammatory markers by down-regulating a
number of genes [37-39, 144].
A second aim of this doctoral work was to study the cross-sectional association between
serum 25(OH)D and inflammatory markers, namely, interleukin 6 (IL-6) and tumor necrosis
factor-alpha (TNF-α) as well as high-sensitivity C-reactive protein (hsCRP) among the
participants of the BPROS. Our data suggest that serum 25(OH)D concentration explained about
6-20% of the variation in the IL-6 and TNF-α concentration, respectively. Our data provides
evidence of an inverse association between serum 25(OH)D and inflammatory markers, namely,
IL-6 and TNF-α, among the participants of the BPROS; irrespective of age, sex, seasonality,
adiposity phenotype and lifestyle factors that include smoking, physical activity and alcohol
consumption. This population, as reported before, exhibits a high prevalence of vitamin D
deficiency [159]. Our findings from the multivariate regression analysis, especially for IL-6 and
TNF-α, showed that irrespective of the various constructed models, serum 25(OH)D
concentration remained a significant predictor of IL-6 and TNF-α, but not of hsCRP, after
controlling for potential covariates. These results are in accordance with other reports on the
association between serum 25(OH)D concentration and inflammatory markers [98, 154, 155]. In
further support, our results are consistent with in vitro and animal studies that showed TNF-α
suppression by vitamin D [97, 152, 160, 161] and IL-6 [97, 147, 162]. A RCT by Schleithoff and
Colleagues, demonstrated that 9 months of daily supplementation of 2000 IU of vitamin D and
500 mg of calcium significantly lowered serum TNF-α concentration compared to baseline

169
among congestive heart failure participants [153]. In addition, another RCT demonstrated an
inhibition of TNF-α concentration with 3332 IU of vitamin D daily [129].
The lack of association between serum 25(OH)D and hsCRP is not in concurrence with a
number of cross-sectional reports [98, 163]; there are a number of plausible explanations. First,
hsCRP concentration can be affected by acute phase reactant due to viral infection. However,
that might not be the case with the presence of constant yet potent stimuli [149]. Another point to
emphasize is that this specific population has a high prevalence of health disparities that includes
metabolic syndrome, depression, and diabetes, which might mask the association [109, 164].
Additionally, in this population the mean of 25(OH)D concentration reaches only to 50 nmol/L;
indicating widespread vitamin D deficiency and thus, very limited distribution and a very low
number of sufficient levels to show significant differences. In our analysis, the adjustment of
white blood cell counts, which is an indicator of current infection, did not improve the null
association between hsCRP and serum 25(OH)D concentration.
Thirdly, adiposity increases the risk of numerous chronic diseases such as CVD and
type-2-diabet among others [200, 201]. We intended for our third report of this doctoral work to
investigate the magnitude of serum 25(OH)D concentration being affect by adiposity phenotype
over time. Our results confirm an inverse association between low serum 25(OH)D concentration
and adiposity phenotype i.e. body mass index (BMI) and waist circumference (WC). Our
observation of lower adjusted mean serum 25(OH)D concentration in obese, severely obese and
morbidly obese participants is in agreement with many studies [132, 172, 176, 177]. Baseline-
BMI was negatively associated with the change in serum 25(OH)D concentration (P =0.01),
independent of known factors including age, sex, serum creatinine, physical activity, smoking,
alcohol, seasonality, poverty and education. We adjusted for covariates in three different models,

170
all of which showed significant longitudinal negative association. Conversely, we did not
observe similar associations with WC, even though it was significantly correlated with serum
25(OH)D at both time points.
A mechanism that can explain the phenomena of low serum 25(OH)D and increased
adiposity risk is not clear. The review by Earthman and colleague discusses number of proposed
theories that link Vitamin D deficiency to adiposity [178]. One of the theories suggests that since
Vitamin D is fat-soluble it might be sequestered within adipose tissue. They further suggest that
the adipose tissue of obese individuals may have higher 25(OH)D uptake and storage relative to
lean individuals [48, 178]. An additional theory suggests that due to the fact that adiposity,
especially visceral adiposity, is considered a high inflammatory state, this contributes to lower
serum 25(OH)D concentration [178, 179]. Finally, with increased adiposity, there may be an
increase of the action of 24-hydroxylase, thus, leading to amplified catabolism of Vitamin D
[178, 180]. Consequently, further research is needed to further elucidate our understanding of
how vitamin D might be affected by adiposity or even how vitamin D affects obesity itself.
The majority of the participants of BPROS- more than 60%- had serum 25(OH)D
concentration below 50 nmol/L, which is considered a deficiency according to the Endocrine
Society [115]. The most recent report by the National Health and Nutrition Examination Survey
(NHASES) III, showed that more than 42% of their 2001-2006 participants had vitamin D below
50 nmol/L; when stratified by ethnicity, Hispanics were second highest in vitamin D deficiency
with 70% [181]. Our prior report indicated that among 1502 participants of the BPRHS, more
than 70% had serum 25(OH)D concentration below 50 nmol/L at baseline, concurring with the
NHANES III data [159]. This greater risk of vitamin D deficiency may be related to greater risk
of health disparities [182]. A report by Palacios and colleagues showed that Puerto Ricans who

171
are residing in Puerto Rico, had higher serum 25(OH)D concentration, approximately 75 nmol/L,
compared to our population, at baseline 43.4 ± 17.2 nmol/L [159] and 2yr 50.0 ± 19.0 nmol/L.
One theory to illustrate here is that this difference in serum 25(OH)D concentration might be due
to sun exposure, generally, and latitude, specifically, i.e. PR’s latitude is 18.26° while Boston’
latitude is 42.35° [26].
Lastly, we aspired in our fourth report of this doctoral work to not only explore the
association between serum 25(OH)D concentration and adiposity phenotype, in general, but
rather to investigate in more depth that association total as well as regional fat mass. Our report
initially focused on total body fat (TBF)-as measured by dual-energy x-ray absorptiometry
(DXA) and serum 25(OH)D concentration. Similarly, percent body fat (%TBF) was not
significantly associated with 25(OH)D. On the other hand, when we further investigated the role
of regional adiposity, android (AFM) and gynoid fat-mass (GFM), results differed. AFM, was
negatively associated with serum 25(OH)D after adjusting for several potential covariates
including, age, serum creatinine, serum iPTH, seasonality, supplements and dietary vitamin D,
smoking, alcohol, and total energy. On the other hand, GFM was significantly positively
associated with serum 25(OH)D (P =0.02) independent of age, serum creatinine, serum PTH,
seasonality, supplements and dietary vitamin D, smoking, alcohol, and total energy.
We reported earlier that vitamin D deficiency remains prevalent in this Hispanic
subgroup, indicating that vitamin D deficiency is not a transient health concern, thus,
predisposing this population to higher levels of mortality and morbidity [182]. Recently, we
reported that the change in BMI over time was negatively associated with the change in serum
25(OH)D concentration (P =0.01) independent of various known factors including age, sex,
serum creatinine, physical activity, smoking alcohol, seasonality, poverty and education [193].

172
Taken together, our results are in agreement with a number of epidemiological studies
demonstrating that measures of adiposity including TBF, BMI, and regional adiposity are
inversely associated with serum 25(OH)D concentration [48, 49, 132, 171-173].
Our findings should be interpreted within the context of a few limitations. First, our
population is primarily Puerto Ricans, therefore our findings could be very specific to this
particular admixture population, with genetic variation interacting not only with the
environment, but social factors as well [140-143]; thus, generalizability may not be an option.
Additionally, even though we have controlled for all the known potential covariates, residual
confounding is still be a possibility.
Some of our findings came from our cross-sectional study; hence, it provides neither
further insights about causation nor long-term status. Longitudinal studies with two or more time
points are ideal alternative to investigate the role of serum 25(OH)D concentration on CVD risk
factors; because serum 25(OH)D concentration can be assessed before the outcome, thus,
allowing us to avoid any potential bias. Nevertheless, our findings show very unique results to
the Puerto Rican population. Another limitation is that we have no direct measure of sun
exposure at baseline. Another potential limitation is that with the use of DXA, the differentiation
between visceral and subcutaneous fat is not feasible. However, it was shown by Savgan-Gurol
and colleagues that the percentage fat shown by DXA was significantly associated with visceral
fat (r = -0.83, P < 0.0001), while the association with subcutaneous was lower (r = -0.77, P <
0.001) [198]. This only suggests that the importance of android fat-mass as an indicator of
central obesity might be greater compared to the relative distribution of visceral and
subcutaneous fat. Another potential bias that might affect our results is selection bias that might
have occurred in our study. Even though selection bias may not be possible to appropriately

173
evaluate how it may affected our results, it is possible that those who declined to participate in
our study may have a higher socioeconomic status, as well as highly educated, thus, may higher
probability of having sufficient serum 25(OH)D concentration [187]
In conclusion, our longitudinal analysis showed that higher 25(OH)D serum
concentration did not translate into an increase of the atheroprotective plasma HDL-C, nor a
decrease of the un-atheroprotective plasma TG in this population of older Puerto Rican adults
living in the Boston area. Moreover, our results showed that smoking might be an effect modifier
of the longitudinal association of serum 25(OH)D and HDL-C, as well as LDL-C. Granted our
work should be replicated in other populations, our findings provide opposing yet significant
evidence of the effect of vitamin D on plasma lipid profile.
Secondly, our study supports the hypothesis that inflammatory markers such as IL-6 and
TNF-α are inversely associated with serum 25(OH)D concentration among the participants of the
BPROS. These findings support the need to re-examine the determination of optimal vitamin D
status. However, more studies, especially longitudinal prospective studies, are needed to fully
characterize the relationship between serum 25(OH)D concentration and inflammatory markers.
Thirdly, serum 25(OH)D concentration was inversely associated with 2.5-yr change in
BMI. The adjusted-means of serum 25(OH)D concentration showed declining trend, at both time
points, with the increase in BMI especially when reaching class III obesity. Our findings of the
negative significant association of AFM on serum 25(OH)D concentration provides compelling
evidence that AFM may affect serum 25(OH)D concentration; while GFM was positively
associated with serum 25(OH)D concentration, Even though it is clear that some segments of the
regional adiposity and serum 25(OH)D concentration relationships may be attributed to the
sequestration of vitamin D in adipose tissues, it is still considered a complex relationship and

174
more work is needed to elucidate the relationship between adipose tissue and vitamin D and the
effect both to overall health.
Taken together, it appears that serum 25(OH)D concentration is strongly influenced by
adiposity, which is considered a chronic low-grade inflammatory condition, thus, by sequestering
25(OH)D within the adipose tissue, neither the high inflammatory condition might be
ameliorated nor dyslipidemia could be improved by vitamin D. Figure 5.1 summarize the
findings of this dissertation work.
Vitamin D deficiency/insufficiency has emerged as an autonomous risk factor of
cardiovascular mortality. Thus, the need for an enhanced understanding of the epidemiological
data as well as the pathophysiological pathways by which this pleiotropic hormone may or may
not affect cardiovascular health is imperative. This understanding will result in better informing
of future clinical trials and ultimately results in improved evidence-based therapeutic
recommendations. Research findings by Bidchoff-Ferrari and Colleagues estimated that 1000
IU/day of vitamin D supplements 50% of the younger and older adults to sufficient levels of
serum 25(OH)D concentration, i.e. 75 nmol/L. However, it will take twice as much of that,
meaning 2000 IU/day to bring 85-90% of the population to those sufficient concentration [202].
Thus, for ethnic minorities who are facing higher health disparities may require 2000 IU/day of
vitamin D supplement. Despite the fact that it is premature to make such recommendations for
the rationale of precluding CVD risk, achieving sufficient concentration of 25(OH)D is essential.
Even though there is plethora of scientific information of vitamin D and its receptor, there is an
urgent necessity to further understand and elucidate the biochemical and transcriptional effect of
vitamin D and its various analogs on CVD, as well as to search for new targets to treat CVD and
ultimately reduce health disparities.

175
Notwithstanding the above limitations, our study has substantial strengths: a large sample
size with low attrition ; we have complete data on 1504 Puerto Rican men and women at
baseline, 1257 at 2-year and 970 within the ancillary bone study. This large sample size is ample
to detect differences with minimally 90% power. In addition, we have used detailed
questionnaires along with an FFQ that allowed detailed information.
In summary, our findings suggest that risk factors of CVD are highly associated with
lower 25(OH)D concentration among Puerto Rican men and women. Results from this
dissertation work may provide guidance for future interventional studies for an understudied yet
fast growing population that appears to have high health disparities. Improving vitamin D status
may not solve all of their health disparities; however, it might lower their risk of developing
chronic disease.

176
FIGURE 5.1 Diagram illustrates the relationship between serum 25(OH)D and the various CVD risk factors among the participants of the BPRHS

177
BIBLIOGRAPHY
1. Roger, V.L., et al., Heart disease and stroke statistics--2011 update: a report
from the American Heart Association. Circulation, 2011. 123(4): p. e18-e209.
2. Bonow, R.O., Primary Prevention of Cardiovascular Disease. Circulation, 2002.
106(25): p. 3140-3141.
3. Balagopal, P., et al., Nontraditional Risk Factors and Biomarkers for Cardiovascular
Disease: Mechanistic, Research, and Clinical Considerations for Youth. Circulation,
2011. 123(23): p. 2749-2769.
4. Giovannucci, E., et al., 25-hydroxyvitamin d and risk of myocardial infarction in men: A
prospective study. Archives of Internal Medicine, 2008. 168(11): p. 1174-1180.
5. Maki, K.C., et al., Serum 25-hydroxyvitamin D is independently associated with high-
density lipoprotein cholesterol and the metabolic syndrome in men and women. Journal
of Clinical Lipidology, 2009. 3(4): p. 289-296.
6. Melamed, M.L., et al., 25-hydroxyvitamin d levels and the risk of mortality in the general
population. Archives of Internal Medicine, 2008. 168(15): p. 1629-1637.
7. Jorde, R., et al., High serum 25-hydroxyvitamin D concentrations are associated with a
favorable serum lipid profile. European Journal of Clinical Nutrition, 2010. 64(12): p.
1457-64.
8. Delvin, E.E., et al., Vitamin D Status Is Modestly Associated with Glycemia and
Indicators of Lipid Metabolism in French-Canadian Children and Adolescents. The
Journal of Nutrition, 2010. 140(5): p. 987-991.
9. Williams, D.M., A. Fraser, and D.A. Lawlor, Associations of vitamin D, parathyroid
hormone and calcium with cardiovascular risk factors in US adolescents. Heart, 2011.
97(4): p. 315-320.
10. Karhapää, P., et al., Diverse associations of 25-hydroxyvitamin D and 1,25-dihydroxy-
vitamin D with dyslipidaemias. Journal of Internal Medicine, 2010. 268(6): p. 604-610.
11. Zittermann, A., et al., Vitamin D supplementation enhances the beneficial effects of
weight loss on cardiovascular disease risk markers. The American Journal of Clinical
Nutrition, 2009. 89(5): p. 1321-1327.

178
12. Heikkinen, A., et al., Long-term vitamin D3 supplementation may have adverse effects on
serum lipids during postmenopausal hormone replacement therapy. European Journal of
Endocrinology, 1997. 137(5): p. 495-502.
13. Jorde, R., et al., No improvement in cardiovascular risk factors in overweight and obese
subjects after supplementation with vitamin D3 for 1 year. Journal of Internal Medicine,
2010. 267(5): p. 462-472.
14. Nagpal, J., J.N. Pande, and A. Bhartia, A double-blind, randomized, placebo-controlled
trial of the short-term effect of vitamin D3 supplementation on insulin sensitivity in
apparently healthy, middle-aged, centrally obese men. Diabetic Medicine, 2009. 26(1): p.
19-27.
15. Jorde, R., et al., Cross-sectional and longitudinal relation between serum 25-
hydroxyvitamin D and body mass index: the Tromsø study. European Journal of
Nutrition, 2010. 49(7): p. 401-407.
16. Yoon, V., N.M. Maalouf, and K. Sakhaee, The effects of smoking on bone metabolism.
Osteoporosis International, 2012. 23(8): p. 2081-2092.
17. Lacour, B., et al., Parathyroid function and lipid metabolism in the rat. Miner Electrolyte
Metab, 1982. 7(3): p. 157-65.
18. Deeb, K.K., D.L. Trump, and C.S. Johnson, Vitamin D signalling pathways in cancer:
potential for anticancer therapeutics. Nature reviews. Cancer, 2007. 7(9): p. 684-700.
19. Reid, I.R., Effects of calcium supplementation on circulating lipids: potential
pharmacoeconomic implications. Drugs Aging, 2004. 21(1): p. 7-17.
20. Hu, F.B., J.E. Manson, and W.C. Willett, Types of Dietary Fat and Risk of Coronary
Heart Disease: A Critical Review. Journal of the American College of Nutrition, 2001.
20(1): p. 5-19.
21. Van der Meer, R., et al., Effects of supplemental dietary calcium on the intestinal
association of calcium, phosphate, and bile acids. Gastroenterology, 1990. 99(6): p.
1653-9.
22. Major, G.C., et al., Supplementation with calcium + vitamin D enhances the beneficial
effect of weight loss on plasma lipid and lipoprotein concentrations. American Journal of
Clinical Nutrition, 2007. 85(1): p. 54-9.

179
23. Fantuzzi, G., Adipose tissue, adipokines, and inflammation. The Journal of allergy and
clinical immunology, 2005. 115(5): p. 911-9; quiz 920.
24. Van Lente, F., Markers of inflammation as predictors in cardiovascular disease. Clin
Chim Acta, 2000. 293(1-2): p. 31-52.
25. Plum, L.A. and H.F. DeLuca, Vitamin D, disease and therapeutic opportunities. Nat Rev
Drug Discov, 2010. 9(12): p. 941-55.
26. POLLY, P., et al., VDR-Alien: a novel, DNA-selective vitamin D3 receptor-corepressor
partnership. The FASEB Journal, 2000. 14(10): p. 1455-1463.
27. 2010 ICD-9-CM.
28. Jamal-Allial, A.A. and K.L. Tucker, Serum Vitamin D Concentrations, Dietary Sources,
and its relation to BMI among Puerto Ricans Living in the Greater Boston Area. To be
submitted, 2013.
29. Bellia, A., et al., Serum 25-hydroxyvitamin D levels are inversely associated with
systemic inflammation in severe obese subjects. Internal and Emergency Medicine, 2013.
8(1): p. 33-40.
30. Peterson, C. and M. Heffernan, Serum tumor necrosis factor-alpha concentrations are
negatively correlated with serum 25(OH)D concentrations in healthy women. Journal of
Inflammation, 2008. 5(1): p. 10.
31. Beilfuss, J., et al., Effects of a 1-year supplementation with cholecalciferol on interleukin-
6, tumor necrosis factor-alpha and insulin resistance in overweight and obese subjects.
Cytokine, 2012. 60(3): p. 870-4.
32. Zhu, Y., et al., Calcium and 1α,25-dihydroxyvitamin D3 target the TNF-α pathway to
suppress experimental inflammatory bowel disease. European Journal of Immunology,
2005. 35(1): p. 217-224.
33. Giovannini, L., et al., 1,25-dihydroxyvitamin D3 dose-dependently inhibits LPS-induced
cytokines production in PBMC modulating intracellular calcium. Transplantation
Proceedings, 2001. 33(3): p. 2366-2368.
34. Cohen, M., et al., Regulation of TNF-[agr] by 1[agr],25-dihydroxyvitamin D3 in human
macrophages from CAPD patients. Kidney International, 2001. 59(1): p. 69–75.

180
35. Alvarez-Rodriguez, L., et al., Age and low levels of circulating vitamin D are associated
with impaired innate immune function. Journal of Leukocyte Biology, 2012. 91(5): p.
829-838.
36. Dickie, L.J., et al., Vitamin D3 down-regulates intracellular Toll-like receptor 9
expression and Toll-like receptor 9-induced IL-6 production in human monocytes.
Rheumatology (Oxford), 2010. 49(8): p. 1466-1471.
37. Nonn, L., et al., Inhibition of p38 by Vitamin D Reduces Interleukin-6 Production in
Normal Prostate Cells via Mitogen-Activated Protein Kinase Phosphatase 5:
Implications for Prostate Cancer Prevention by Vitamin D. Cancer Research, 2006.
66(8): p. 4516-4524.
38. Schleithoff, S.S., et al., Vitamin D supplementation improves cytokine profiles in patients
with congestive heart failure: a double-blind, randomized, placebo-controlled trial.
American Journal of Clinical Nutrition, 2006. 83(4): p. 754-9.
39. Amer, M. and R. Qayyum, Relation between serum 25-hydroxyvitamin D and C-reactive
protein in asymptomatic adults (from the continuous National Health and Nutrition
Examination Survey 2001 to 2006). American Journal of Cardiology, 2012. 109(2): p.
226-30.
40. Gabay, C. and I. Kushner, Acute-phase proteins and other systemic responses to
inflammation. N Engl J Med, 1999. 340(6): p. 448-54.
41. Falcon, L.M. and K.L. Tucker, Prevalence and correlates of depressive symptoms among
Hispanic elders in Massachusetts. J Gerontol B Psychol Sci Soc Sci, 2000. 55(2): p.
S108-16.
42. Mattei, J., et al., Allostatic load is associated with chronic conditions in the Boston
Puerto Rican Health Study. Social Science & Medicine, 2010. 70(12): p. 1988-96.
43. Barcelo, A., et al., Waist circumference, BMI and the prevalence of self-reported diabetes
among the elderly of the United States and six cities of Latin America and the Caribbean.
Diabetes Res Clin Pract, 2007. 78(3): p. 418 - 427.
44. McTigue K, L.J.C.V.A. and et al., MOrtality and cardiac and vascular outcomes in
extremely obese women. JAMA, 2006. 296(1): p. 79-86.

181
45. Snijder, M.B., et al., Adiposity in relation to vitamin D status and parathyroid hormone
levels: a population-based study in older men and women. Journal of Clinical
Endocrinology & Metabolism, 2005. 90(7): p. 4119-23.
46. McGill, A.-T., et al., Relationships of low serum vitamin D3 with anthropometry and
markers of the metabolic syndrome and diabetes in overweight and obesity. Nutrition
Journal, 2008. 7: p. 4.
47. Young, K.A., et al., Association of Plasma Vitamin D Levels with Adiposity in Hispanic
and African Americans. Journal of Clinical Endocrinology & Metabolism, 2009. 94(9): p.
3306-3313.
48. Earthman, C.P., et al., The link between obesity and low circulating 25-hydroxyvitamin D
concentrations: considerations and implications. Int J Obes, 2012. 36(3): p. 387- 96.
49. Wortsman, J., et al., Decreased bioavailability of vitamin D in obesity. The American
Journal of Clinical Nutrition, 2000. 72(3): p. 690-693.
50. Compher, C. and K.O. Badellino, Obesity and Inflammation: Lessons From Bariatric
Surgery. Journal of Parenteral and Enteral Nutrition, 2008. 32(6): p. 645-647.
51. Li, J., et al., 1α,25-Dihydroxyvitamin D hydroxylase in adipocytes. The Journal of Steroid
Biochemistry and Molecular Biology, 2008. 112(1–3): p. 122-126.
52. Holick, M.F., et al., Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an
Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology &
Metabolism, 2011. 96(7): p. 1911-1930.
53. Looker, A.C.J., C L. Lacher, D A. Pfeiffer, C M. Schleicher, R L. Sempos, C T.,
Vitamin D status: United States, 2001–2006, in NCHS data brief2011, National Center
for Health Statistics: Hyattsville, MD.
54. Forrest, K.Y.Z. and W.L. Stuhldreher, Prevalence and correlates of vitamin D deficiency
in US adults. Nutrition Research, 2011. 31(1): p. 48-54.
55. Holick, M.F., Vitamin D deficiency. N Engl J Med, 2007. 357(3): p. 266-81.
56. Jamal-Allial, A.A., J.L. Griffith, and K.L. Tucker, The Longitudinal Association of
Vitamin D Serum Concentrations & Adiposity Phenotypes. To be submitted, 2013.

182
57. Renzaho, A.M.N., J.A. Halliday, and C. Nowson, Vitamin D, obesity, and obesity-related
chronic disease among ethnic minorities: A systematic review. Nutrition, 2011. 27(9): p.
868-879.
58. Brock, K., et al., Low vitamin D status is associated with physical inactivity, obesity and
low vitamin D intake in a large US sample of healthy middle-aged men and women. J
Steroid Biochem Mol Biol, 2010. 121(1-2): p. 462-6.
59. Liel, Y., et al., Low circulating vitamin D in obesity. Calcified tissue international, 1988.
43(4): p. 199-201.
60. Lumb, G.A., E.B. Mawer, and S.W. Stanbury, The apparent vitamin D resistance of
chronic renal failure: A study of the physiology of vitamin D in man. The American
Journal of Medicine, 1971. 50(4): p. 421-441.
61. Mawer, E.B., et al., The distribution and storage of vitamin D and its metabolites in
human tissues. Clin Sci, 1972. 43(3): p. 413-31.
62. Jacobs, E.J., et al., WAist circumference and all-cause mortality in a large us cohort.
Archives of Internal Medicine, 2010. 170(15): p. 1293-1301.
63. Panagiotakos, D.B., et al., The implication of obesity and central fat on markers of
chronic inflammation: The ATTICA study. Atherosclerosis, 2005. 183(2): p. 308-315.
64. Dos Santos, R.E., et al., Relationship of body fat distribution by waist circumference,
dual-energy X-ray absorptiometry and ultrasonography to insulin resistance by
homeostasis model assessment and lipid profile in obese and non-obese postmenopausal
women. Gynecological Endocrinology, 2005. 21(5): p. 295-301.
65. Fontana, L., et al., Visceral Fat Adipokine Secretion Is Associated With Systemic
Inflammation in Obese Humans. Diabetes, 2007. 56(4): p. 1010-1013.
66. Junyent, M., et al., The effects of ABCG5/G8 polymorphisms on plasma HDL cholesterol
concentrations depend on smoking habit in the Boston Puerto Rican Health Study.
Journal of Lipid Research, 2009. 50(3): p. 565-73.
67. Lai, C.-Q., et al., Population admixture associated with disease prevalence in the Boston
Puerto Rican health study. Human Genetics, 2009. 125(2): p. 199-209.

183
68. Mattei, J., et al., Apolipoprotein A5 polymorphisms interact with total dietary fat intake in
association with markers of metabolic syndrome in Puerto Rican older adults. Journal of
Nutrition, 2009. 139(12): p. 2301-8.
69. Mattei, J., et al., Disparities in allele frequencies and population differentiation for 101
disease-associated single nucleotide polymorphisms between Puerto Ricans and non-
Hispanic whites. BMC Genetics, 2009. 14(10): p. 45.
70. Savgan-Gurol, E., et al., Waist to hip ratio and trunk to extremity fat (DXA) are better
surrogates for IMCL and for visceral fat respectively than for subcutaneous fat in
adolescent girls. Nutrition & Metabolism, 2010. 7(1): p. 86.
71. Holick, M.F., Vitamin D status: measurement, interpretation, and clinical application.
Ann Epidemiol, 2009. 19(2): p. 73-8.
72. Weishaar, T. and J.M. Vergili, Vitamin D Status Is a Biological Determinant of Health
Disparities. Journal of the Academy of Nutrition and Dietetics, 2013. 113(5): p. 643-651.
73. Bischoff-Ferrari, H.A., et al., Estimation of optimal serum concentrations of 25-
hydroxyvitamin D for multiple health outcomes. The American Journal of Clinical
Nutrition, 2006. 84(1): p. 18-28.

184
APPENDIX

185
Serum Vitamin D Concentration, Dietary Sources, and its relation to BMI among Puerto
Ricans Living in the Greater Boston Area1-2
Aziza Jamal-Allial3, Katherine L. Tucker 4*
3Pharmaceutical Science, Bouvé College of Health Sciences, Northeastern University. 4 Health
Sciences, Bouvé College of Health Sciences, Northeastern University, Boston, MA.
Word count: 447
FIGUREs: 4. Tables: 4. No OSM submitted
Running title: Vitamin D deficiency and obesity in Puerto Ricans
1 Supported by the National Institutes of Health (P01 AG023394, P50 HL105185, and R01
AG027087-01A1).
2 Author disclosures: A. Jamal-Allial, K. L. Tucker, no conflicts of interest.
Abbreviations used: Boston Puerto Rican Health Study (BPRHS), 25-hydroxyvitamin D
(25(OH)D), body mass index (BMI), National Health and Nutrition Examination Survey
(NHANES), Recommended Dietary Allowance (RDA).
*To whom correspondence should be addressed. Department of Health Sciences, Northeastern
University 208 Robinson Hall, 360 Huntington Avenue, Boston, MA 02115. Phone: (617) 373-
7952; Fax: (617) 373-2968. Email: [email protected]

186
ABSTRACT
Puerto Ricans have greater health disparities compared to the general population.
Vitamin D deficiency is highly prevalent among ethnic minorities. Cross-sectional analyses
included data from 1504 Puerto Ricans, 445 men and 1050 women, aged 45-75 years in Boston,
Massachusetts. Our aim was to determine serum 25-hydroxy vitamin D concentration (25(OH)D)
and associated contributing factors as well as test the hypothesis that lower serum 25(OH)D is
inversely associated with body mass index (BMI). Associations between 25(OH)D and likely
determinants were tested with multivariable linear regression. Low 25(OH)D concentration was
defined as <50 nmol/L. Dietary data from food frequency questionnaire were used to rank intake
sources of vitamin D using PROC RANK. Mean serum 25(OH)D concentration was 43.5 ± 16.5
nmol/L for men and 43.1 ± 16.0 nmol/L for women. 70.0% of participants had 25(OH)D <50
nmol/L. Milk products contributed 34% of total vitamin D intake, followed by supplements,
21.5%. Among women, but not men, higher intake of supplements was associated with
significantly higher serum 25(OH)D concentration. Never-smokers had significantly higher
serum 25(OH)D compared to current-smokers (P=0.01), but alcohol intake was not associated
with vitamin D status. The multivariate model showed that season (summer vs. others),
supplement use, dietary vitamin D intake, number of miles walked/day and serum albumin were
each positively associated (all P<0.05), while BMI was inversely associated (P=0.0007), with
serum 25(OH)D. Women with BMI ≥40 had significantly lower serum 25(OH)D concentration
compared to lower BMI. In conclusion, vitamin D deficiency is prevalent among Puerto Rican
adults living in Boston, MA, and this is associated with BMI and several behavioral measures,
including intake, smoking and outdoor walking.

187
INTRODUCTION
Vitamin D is naturally present in a limited number of food sources; but is available
through synthesis from its subcutaneous precursors with sun exposure[82]. Although 25-hydroxy
vitamin D [25(OH)D] is the measureable form and best clinical measure of status, there is no
consensus on a cutoff point for adequate vitamin D concentration. Most experts define deficiency
as 25(OH)D <50 nmol/L[115, 157]. Worldwide, vitamin D insufficiency is a major problem,
affecting more than 1 billion children and adults [26]. In the US, data from the Third National
Health and Nutrition Evaluation Survey (NHANES III) showed that approximately 41% of men
and 53% of women were considered vitamin D deficient [203]. A more recent NHANES report
indicated that vitamin D deficiency was more prevalent among blacks and Hispanics than non-
Hispanic whites, at 82.1% and 69.2% respectively [182]. A systematic review reported that the
mean of serum 25(OH)D for immigrants and/or ethnic minorities ranged between 24 to 60
nmol/L [171]. Vitamin D deficiency results in calcium and phosphorous abnormalities and may
lead to secondary hyperparathyroidism [115]. Due to its fat-soluble nature, adults with BMI >30
are at higher risk of vitamin D deficiency, which may be due, in part, to body fat sequestration
[115]. Several studies have reported associations between obesity and lower serum 25(OH)D
concentration [48, 49, 64, 173].
In the US, Puerto Ricans are the second largest Hispanic subgroup [204]. Recent
publications have confirmed the presence of important health disparities as well as low
socioeconomic status and education in this population [205]. Several reports have discussed the
high prevalence of obesity, type 2 diabetes, hypertension, depression and cognitive decline
among Puerto Ricans, relative to other Hispanic groups [164, 205-207]. However, we are aware
of no reports of vitamin D status in this population. Therefore, our aim was to describe the

188
distribution of serum 25(OH)D concentration among Puerto Rican men and women living in the
greater Boston area, and to explore its relationship with traditional determinants of 25(OH)D,
including BMI.
MATERIALS AND METHODS
Study Population
Self-identified Puerto Rican adults, aged between 45-75 years, were recruited in the greater
Boston area as participants in the Boston Puerto Rican Health Study (BPRHS). The BPRHS is an
ongoing longitudinal study, started in 2005, to examine the role of social and psychological
stress on physiological dysfunction and related health outcomes among 1504 participants. Study
design, sampling, and recruitment methods have been described in detail [83]. Briefly, after
selecting census tracks that contained at least 25 Puerto Rican adults, aged 45 years and older,
blocks that contained ≥ 10 Hispanic adults, aged 45 and older, were enumerated. Other
recruitment methods were through random approach at community events (9.4%) or as
respondents to flyers or community members’ referral (6.9%). Participants were excluded if they
had serious health conditions or advanced dementia, had no permanent address, or planned to
move away within two years. The study protocol was approved by the Institutional Review
Boards at Tufts Medical Center and Northeastern University, and each participant provided
written informed consent.
For the current analysis, participants with missing data on variables needed for the analysis were
excluded (n=93) as well as those with serum 25(OH)D concentration greater than 250 nmol/L
(n=1) [55]. There were no significant differences in baseline sociodemographic characteristics

189
between those with complete or incomplete information. The present study includes 1400
participants with complete baseline data available at the time of analysis.
Field data collection
During home interviews, data on age, sex, education, household income, smoking status,
alcohol use, medical history and current medication use were collected by interviewer
administered questionnaire. Detailed description of the field data collection is available in
previous publications [83, 109]. Serum 25(OH)D concentration was categorized as deficient
when <50 nmol/L, insufficient between 50-75 nmol/L, and sufficient when > 75 nmol/L[26,
157]. BMI was calculated as weight (kg) divided by height (m)2 and defined by World Health
Organization criteria: recommended (BMI<25), overweight (25-30), obese (30-35), and very
obese (≥40) [208]. For subset analyses, we further categorized BMI using the class III obesity
definition [114]. Seasonality was defined as summer, July to September; fall, October to
December; winter, January to March; and spring, April to June. Age was categorized into two
groups: 45 to 59 years and 60-75 years. Both smoking status and alcohol were categorized into
yes and no for the current behavior.
Dietary vitamin D intake was estimated from a semi-quantitative food-frequency
questionnaire (FFQ) that was specifically designed for this population [91]. This FFQ has been
validated against serum carotenoids [116], and vitamin B12 [117] in a Hispanic population aged
≥ 60 years. Those with energy intakes < 600 or > 4800 kilocalories and/or > 10 questions blank
on the FFQ were excluded from the analyses. Nutrient intakes were calculated with the Nutrition
Data System for Research (NDS-R) software version 2007 (Nutrition Coordinating Center,

190
University of Minnesota, Minneapolis, MN, Food and Nutrient Database 2007, released 2007).
Vitamin D from supplements was defined as: minimal or no supplement < 5 µg/day (≤
200IU/day); moderate 5-10 µg/day (200-400 IU/day); and high ≥ 10 µg/day (≥ 400 IU/day).
Total vitamin D (food and supplements) was categorized according to the current RDA (15
µg/day or 600 IU/day) for vitamin D as: ≤ ½ the RDA (7.5 µg/day or 300 IU/day); >½ RDA- the
RDA (7.5-15 µg/day or 300-600 IU/day); and ≥ the RDA (10 µg/day or 600 IU/day) [209].
Dietary only vitamin D (µg/day) was categorized into quintiles. Serum creatinine concentration
(nmol/L) was categorized into quartiles. Serum albumin (g/L) was categorized as normal 34 – 54
g/L, or high, ≥ 54 g/L. Miles/day walked was calculated from blocks reported and categorized as:
0 miles/day, up to 0.5 mile/day, and more than 0.5 mile/day.
Laboratory assays
Fasting blood samples (12-h) were drawn by a certified phlebotomist at the participant’s
home on the morning after the home interview, or as soon thereafter as possible. Aliquots were
saved and stored at -80°C until processed. Serum 25(OH)D concentration were measured by
extraction followed by 25I radioimmunoassay Packard COBRA II Gamma Counter (DiaSorin
Inc., Stillwater, MN 55082) catalog # 68100E with intra-assay and inter-assay coefficients of
variation of 10.8% and 9.4%, respectively. Serum albumin was detected with a dye binding,
endpoint reaction using the Olympus AU400e with Olympus Albumin Reagents (OSR6102)
(Olympus America Inc., Melville, NY) Serum creatinine was assessed with a colorimetric,
kinetic reaction using the Olympus AU400e with Olympus Creatinine Reagents (OSR6178)
(Olympus America Inc., Melville, NY).

191
Statistical analyses
All statistical analyses were conducted with SAS 9.1.3 (SAS Institute Inc, Cary, NC); and
all tests were 2-sided with P <0.05 considered statistically significant. Skewed variables were
natural log-transformed to normalize their distributions before analysis. We calculated age-
adjusted mean serum 25(OH)D concentration across categories for known and potential
determinants of vitamin D status, and tested for linear trend with the general linear models
procedure (PROC GLM). Dunnett’s and Tukey’s tests were used for multiple comparison
adjustment. Linear regression analysis was used to quantify the association between age, sex,
education, poverty status, smoking status (yes/no), alcohol use (yes/no), number of miles
walked/day, BMI, serum albumin, and serum creatinine as independent variables, and serum
25(OH)D concentration as a dependent variable. Age-adjusted mean serum 25(OH)D was
calculated and plotted against medians for deciles of vitamin D intake. For comparison with
general U.S. adult dietary intakes, food groups were constructed according to the USDA
classification. Food sources of vitamin D intake were identified and ranked by the total intake
from foods. All dietary variables were energy adjusted
RESULTS
Complete serum 25(OH)D concentration and dietary intake information was available for
1316 participants, 935 women and 381 men. The mean of serum 25(OH)D among the BPRHS
participants was about 43.5± 16.1 nmol/L. Approximately 70% had low vitamin D status, <50
nmol/L, whereas only 4.2% of men and 3.5% of women had serum 25(OH)D concentration >75
nmol/L (Figure 6.1). The mean ages of men and women were 56.6 ± 8 and 57.3 ± 7.5,

192
respectively (Table 6.1). Women had significantly lower serum albumin, serum creatinine, and
walked fewer miles/day compared to men. In addition, women had significantly higher BMI and
poverty status than did men. More women than men were taking supplements with vitamin D,
and women tended to have higher total vitamin D intake. Serum 25(OH)D concentration was
associated with total vitamin D intake as defined by the RDA. The consumption of less than >½
RDA (7.5 µg/day) of total vitamin D intake was significantly lower than the >½ RDA –RDA and
≥ RDA increased serum 25(OH)D concentration significantly compared to lower amounts, 48
and 50 nmol/L compared to 40.3 nmol/L (Figure 6.2). The median intake of dietary vitamin D
(5.3 µg/day) and higher contributed to significantly higher serum 25(OH)D concentration
(nmol/L) compared to the referent group intake of 5.22 µg/day (P = 0.02, P = 0.005 and P =
0.01, respectively (Figure 6.3).
Men and women consuming daily supplements with at least 5µg/day of vitamin D had
significantly higher serum 25(OH)D concentration than those consuming supplements with less
than 5µg/day of vitamin D (P <0.0001) (Table 6.2). The season of examination was associated
with serum 25(OH)D concentration (P <0.0001), with lower concentration in the winter and
spring, relative to the summer. Higher serum creatinine concentration was associated with
significantly higher serum 25(OH)D concentration (P = 0.009 and P = 0.02 for men and women,
respectively). Among women only, older women, aged 60-75 years, had significantly higher
serum 25(OH)D than did women aged 45-59 y (P = 0.007). BMI had an inverse relationship with
age-adjusted serum 25(OH)D concentration (P-trend (0.001). Compared to never-smokers,
women who were current smokers had significantly lower 25(OH)D concentration (P = 0.02).
Women, but not men, had significantly higher serum 25(OH)D concentration when walking
more miles/day (P-trend =0.01). Among men, lower serum albumin concentration was associated

193
with lower serum 25(OH)D (P= 0.05). Alcohol intake was not significantly associated with
25(OH)D.
In a full model with adjustment for other variables, serum 25(OH)D remained
significantly associated with dietary vitamin D intake (P <0.0001), use of vitamin D-containing
supplements (P <0.0001), seasonality (P <0.0001), and number of miles walked/day (P <0.05)
(Table 6.3). There was a significant interaction between sex and vitamin D supplement use (P =
0.008) (Figure 6.4). Among women, supplements with vitamin D in the range of 4.5-10 µg/day
and those ≥ 10 µg/day, were associated with significantly higher mean serum 25(OH)D
concentration, 45 nmol and 51.3 nmol/L, respectively, compared with non-supplement use (P
<0.0001), 40 nmol/L. However, among men, only supplements providing 5-10 µg/day of vitamin
D were associated with significantly higher mean serum 25(OH)D concentration compared with
non-supplement use (P <0.0001).
Another interaction was between seasonality and age (P = 0.0008) (Figure 6.5). Younger
participants, ages 45-59 years, had significantly higher 25(OH)D in both summer and fall, 50.5
nmol/L and 49.0 nmol/L, respectively, relative to winter and spring, (41.5 nmol/L and 39.0
nmol/L, respectively, P <0.0001). However, among older participants, ages 56 - 75 years, serum
25(OH)D did not differ significantly across the four seasons.
Subset analyses of the women showed that serum 25(OH)D was significantly lower with
increased obesity (P-trend = 0.001) when BMI was further categorized into obesity categories.
Women with class III obesity, BMI ≥ 40, had significantly lower serum 25(OH)D concentration
(41.6 nmol/L) compared to lower BMI (Figure 6.4) adjusting for age, seasonality and vitamin D
supplements, and number of miles walked/day. In addition to supplements, a range of foods
contributed to vitamin D intake (Table 6.4). Fortified milk was the major contributor, at 34% of

194
total vitamin D intake from food. Fish ranked second, at 16.2%, as one of the food sources that is
naturally rich of vitamin D. Eggs and ready-to-eat cereal each contributed about 4.5% to total
dietary vitamin D intake.
DISCUSSION
These results highlight the high prevalence of vitamin D deficiency among Puerto Rican
adults living in the greater Boston area, and show an inverse relationship between BMI and
serum 25(OH)D concentration. The majority (70%) of the men and women in our study had low
vitamin D status, with a mean circulating of 25(OH)D of 44.0 nmol/L—which is lower than that
reported in the literature for several other populations [182, 210-212]. Our data concur with a
recent NHANES report showing that 69.2% of U.S. Hispanics had low vitamin D. This greater
risk of vitamin D deficiency may translate into greater risk of health disparities [182]. Although
debated, most current recommendations suggest that serum concentration should be above 75
nmol/L [26, 29, 51, 82, 182]. We found that only 3% of Puerto Rican men and 4% of women
achieved this [213]. This disparity may have various explanations, including skin pigmentation
[31, 182]. Darker skin is associated with lower 7-dehydrocholesterol conversion to its active
metabolite, which requires longer sunlight exposure [214]. In addition, these participants reside
in Boston, which lies on the 43.3°N, with relatively low UV-B exposure [31]. Moreover, 50% of
the BPRHS participants reported incomes below the poverty line, and 60% reported education of
less than 8th grade [83] indicating low socioeconomic status. This may translate into fewer
healthy food choices and limited access to supplements.

195
Unlike many reports, aging was not negatively associated with serum 25(OH)D
concentration in this population [212, 215] . With aging, the presence of vitamin D precursors
within the skin declines, which puts the elderly at higher risk of vitamin D deficiency [26, 216].
A recent report using NHANES III data reported significant declines with aging [215, 217] while
others have reported no significant difference across age groups [182]. In our sample, the
difference appears to be due to greater use of supplements, particularly among older women,
relative to younger individuals. Vitamin D supplements as well as dietary vitamin D have
previously been shown to be associated with serum 25(OH)D concentration[218, 219]. This
study confirms the importance of vitamin D from supplementation and dietary sources,
especially among women, on improving vitamin D status. In our population, 30% of women
were consuming supplements with higher vitamin D concentration (≥ 5 µg/day or 200 IU/day)
compared to 24% of men. In general, women tend to be more likely than men to be prescribed
vitamin D-containing supplements, often for osteoporosis prevention. When compared to the
RDA, levels, only 5% of this population is meeting the current RDA of vitamin D, which is 15
µg/day or 600 IU/day [209]. This low percentage meeting the RDA is consistent with poor health
status, which has been observed among this population [109, 113, 220].
The relationship between BMI and serum 25(OH)D concentration among Puerto Rican
women is noteworthy. Our results showed that with increased obesity, especially when reaching
class III obesity, serum 25(OH)D concentration declined significantly. Our results indicate that
serum 25(OH)D concentration reached a plateau at BMI 35 or less, compared to severely obese
categories. Most studies have found an inverse relationship between obesity and serum 25(OH)D
concentration [48, 64, 173]. One of the proposed theories that links obesity to lower 25(OH)D is
that the latter leads to an increase in iPTH concentration, resulting in interference with lipolysis

196
and greater expression of fatty acid synthase [221]. Another theory suggests that lower 25(OH)D
may be one of the causes of increased fat mass during the winter season [222]. It has also been
shown that there is increased sequestration of 7-dehydrocholesterol in adipose tissue, thus fewer
precursor molecules are available [48, 49]. This population has a high (57%) prevalence of
obesity [83, 113, 223], combined with very low physical activity [83], both of which translate
into low outdoor activity, thus reduced sun exposure, all of which are strong predictors of lower
serum 25(OH)D concentration. This complex of factors may explain why this Puerto Rican
population has very low serum 25(OH)D concentration.
Several limitations of our study should be noted. First, due to the cross-sectional design,
associations cannot be translated into cause and effect relationships. In addition, residual
confounding remains a possibility, even though we adjusted for several essential covariates.
Third, we did not have a measure of sun exposure, which would have added predictive ability to
the models, although we did include a measure of outdoor physical activity which is a likely
proxy. Nevertheless, our study design was strengthened by the use of our validated FFQ that has
been designed for this particular ethnicity group [116, 117]. This report of vitamin D status
shows high prevalence of vitamin D deficiency in a large Puerto Rican adult population. Because
vitamin D status has been associated with numerous health outcomes, it is likely that improving
vitamin D status in this population at high risk of health disparities, could contribute to reducing
health disparities.

197
BIBLIOGRAPHY
1. Organization, W.H., Cardiovascular diseases (CVDs), in Fact sheet N°3172011, WHO: Geneva.
2. Balagopal, P., et al., Nontraditional Risk Factors and Biomarkers for Cardiovascular
Disease: Mechanistic, Research, and Clinical Considerations for Youth. Circulation, 2011. 123(23): p. 2749-2769.
3. Lusis, A.J., Atherosclerosis. Nature, 2000. 407(6801): p. 233-241. 4. Krishnan, A.V. and D. Feldman, Mechanisms of the anti-cancer and anti-inflammatory
actions of vitamin D. Annual review of pharmacology and toxicology, 2011. 51: p. 311-36.
5. Tomaschitz, A., et al., Independent association between 1,25-dihydroxyvitamin D, 25-
hydroxyvitamin D and the renin–angiotensin system: The Ludwigshafen Risk and
Cardiovascular Health (LURIC) study. Clinica Chimica Acta, 2010. 411(17–18): p. 1354-1360.
6. Vacek, J.L., et al., Vitamin D Deficiency and Supplementation and Relation to
Cardiovascular Health. The American Journal of Cardiology, 2012. 109(3): p. 359-363. 7. Sherry L. Murphy, B.S.J.X., M.D.; and Kenneth D. Kochanek, M.A., Deaths:
Preliminary Data for 2010, in National Vital Statisictis Report2012, CDC: Division of Vital Statistics.
8. Writing Group, M., et al., Heart disease and stroke statistics--2010 update: a report from
the American Heart Association. Circulation, 2010. 121(7): p. e46-e215. 9. Members, W.G., et al., Executive Summary: Heart Disease and Stroke Statistics—2011
Update. Circulation, 2011. 123(4): p. 459-463. 10. Wilson, P.W. and B.F. Culleton, Epidemiology of cardiovascular disease in the United
States. American Journal of Kidney Diseases, 1998. 32(5 Suppl 3). 11. Lloyd-Jones, D.M., et al., Lifetime risk for developing congestive heart failure: the
Framingham Heart Study. Circulation, 2002. 106(24): p. 3068-72. 12. Tedgui, A. and Z. Mallat, Cytokines in Atherosclerosis: Pathogenic and Regulatory
Pathways. Physiological Reviews, 2006. 86(2): p. 515-581. 13. Ross, R., Atherosclerosis is an inflammatory disease. Am Heart J, 1999. 138: p. S419-20. 14. Davignon, J. and P. Ganz, Role of Endothelial Dysfunction in Atherosclerosis.
Circulation, 2004. 109(23 suppl 1): p. III-27-III-32. 15. Lind, L., Lipids and endothelium-dependent vasodilation—A review. Lipids, 2002. 37(1):
p. 1-15. 16. Deshpande, D.D., D.R. Janero, and M.M. Amiji, Therapeutic strategies for endothelial
dysfunction. Expert opinion on biological therapy, 2011. 11(12): p. 1637-54. 17. Ridker, P.M., Clinical application of C-reactive protein for cardiovascular disease
detection and prevention. Circulation, 2003. 107(3): p. 363-9. 18. Shishehbor, M.H. and D.L. Bhatt, Inflammation and atherosclerosis. Current
Atherosclerosis Reports, 2004. 6(2): p. 131-9. 19. Almirall, J., et al., Association of low serum 25-hydroxyvitamin D levels and high arterial
blood pressure in the elderly. Nephrology Dialysis Transplantation, 2010. 25(2): p. 503-9.

198
20. Ameri, P., et al., High prevalence of vitamin D deficiency and its association with left
ventricular dilation: an echocardiography study in elderly patients with chronic heart
failure. Nutrition Metabolism & Cardiovascular Diseases, 2010. 20(9): p. 633-40. 21. Baz-Hecht, M. and A.B. Goldfine, The impact of vitamin D deficiency on diabetes and
cardiovascular risk. Current Opinion in Endocrinology, Diabetes & Obesity, 2010. 17(2): p. 113-9.
22. Bostick, R.M., et al., Relation of calcium, vitamin D, and dairy food intake to ischemic
heart disease mortality among postmenopausal women. American Journal of Epidemiology, 1999. 149(2): p. 151-61.
23. Giovannucci, E., et al., 25-hydroxyvitamin D and risk of myocardial infarction in men: a
prospective study. Archives of Internal Medicine, 2008. 168(11): p. 1174-80. 24. Oh, J., et al., 1,25(OH)2 Vitamin D Inhibits Foam Cell Formation and Suppresses
Macrophage Cholesterol Uptake in Patients With Type 2 Diabetes Mellitus. Circulation, 2009. 120(8): p. 687-698.
25. Sugden, J.A., et al., Vitamin D improves endothelial function in patients with Type 2
diabetes mellitus and low vitamin D levels. Diabet Med, 2008. 25(3): p. 320-5. 26. Holick, M.F., Vitamin D deficiency. N Engl J Med, 2007. 357(3): p. 266-81. 27. Armas, L.A., B.W. Hollis, and R.P. Heaney, Vitamin D2 is much less effective than
vitamin D3 in humans. Journal of Clinical Endocrinology & Metabolism, 2004. 89(11): p. 5387-91.
28. Holick, M.F., et al., The vitamin D content of fortified milk and infant formula. N Engl J Med, 1992. 326(18): p. 1178-81.
29. Holick, M.F., High prevalence of vitamin D inadequacy and implications for health. Mayo Clin Proc, 2006. 81(3): p. 353-73.
30. Holick, M.F., Resurrection of vitamin D deficiency and rickets. J Clin Invest, 2006. 116(8): p. 2062-72.
31. Holick, M.F., Deficiency of sunlight and vitamin D. Bmj, 2008. 336(7657): p. 1318-9. 32. Ramos-Lopez, E., et al., CYP2R1 (vitamin D 25-hydroxylase) gene is associated with
susceptibility to type 1 diabetes and vitamin D levels in Germans. Diabetes/Metabolism Research and Reviews, 2007. 23(8): p. 631-636.
33. Rhieu, S.Y., et al., A new insight into the role of rat cytochrome P450 24A1 in
metabolism of selective analogs of 1alpha,25-dihydroxyvitamin D. Archives of biochemistry and biophysics, 2011. 509(1): p. 33-43.
34. Prosser, D.E. and G. Jones, Enzymes involved in the activation and inactivation of
vitamin D. Trends in biochemical sciences, 2004. 29(12): p. 664-73. 35. Cheng, J.B., et al., Genetic evidence that the human CYP2R1 enzyme is a key vitamin D
25-hydroxylase. Proceedings of the National Academy of Sciences of the United States of America, 2004. 101(20): p. 7711-5.
36. Jones, G., Pharmacokinetics of vitamin D toxicity. The American Journal of Clinical Nutrition, 2008. 88(2): p. 582S-586S.
37. Deeb, K.K., D.L. Trump, and C.S. Johnson, Vitamin D signalling pathways in cancer:
potential for anticancer therapeutics. Nature reviews. Cancer, 2007. 7(9): p. 684-700. 38. Plum, L.A. and H.F. DeLuca, Vitamin D, disease and therapeutic opportunities. Nat Rev
Drug Discov, 2010. 9(12): p. 941-55.

199
39. POLLY, P., et al., VDR-Alien: a novel, DNA-selective vitamin D3 receptor-corepressor
partnership. The FASEB Journal, 2000. 14(10): p. 1455-1463. 40. Holick, M.F., Evolution and function of vitamin D. Recent Results Cancer Res, 2003.
164: p. 3-28. 41. Holick, M.F., The influence of vitamin D on bone health across the life cycle. J Nutr,
2005. 135(11): p. 2726S-7S. 42. Etten, E.v. and C. Mathieu, Immunoregulation by 1,25-dihydroxyvitamin D3: Basic
concepts. The Journal of Steroid Biochemistry and Molecular Biology, 2005. 97(1–2): p. 93-101.
43. Bertone-Johnson, E.R., et al., Plasma 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D
and risk of breast cancer. Cancer Epidemiol Biomarkers Prev, 2005. 14(8): p. 1991-7. 44. Chen, T.C., et al., Prostatic 25-hydroxyvitamin D-1alpha-hydroxylase and its implication
in prostate cancer. J Cell Biochem, 2003. 88(2): p. 315-22. 45. Chen, T.C. and M.F. Holick, Vitamin D and prostate cancer prevention and treatment.
Trends Endocrinol Metab, 2003. 14(9): p. 423-30. 46. Judd, S.E. and V. Tangpricha, Vitamin D deficiency and risk for cardiovascular disease.
American Journal of the Medical Sciences, 2009. 338(1): p. 40-4. 47. Kim, D.H., et al., Prevalence of hypovitaminosis D in cardiovascular diseases (from the
National Health and Nutrition Examination Survey 2001 to 2004). American Journal of Cardiology, 2008. 102(11): p. 1540-4.
48. Wortsman, J., et al., Decreased bioavailability of vitamin D in obesity. The American Journal of Clinical Nutrition, 2000. 72(3): p. 690-693.
49. Liel, Y., et al., Low circulating vitamin D in obesity. Calcified tissue international, 1988. 43(4): p. 199-201.
50. Michael F, H.P.D., M.D., ed. Vitamin D. Physiology, Molecular Biology, and clinical
applications. Second ed. NUTRITION AND HEALTH, ed. P. Adrianne Bendich. 2010, Springer Humana Press. 1155.
51. Bischoff-Ferrari, H.A., et al., Estimation of optimal serum concentrations of 25-
hydroxyvitamin D for multiple health outcomes. American Journal of Clinical Nutrition, 2006. 84(1): p. 18-28.
52. Chapuy, M.C., et al., Prevalence of vitamin D insufficiency in an adult normal
population. Osteoporos Int, 1997. 7(5): p. 439-43. 53. Malabanan, A., I.E. Veronikis, and M.F. Holick, Redefining vitamin D insufficiency.
Lancet, 1998. 351(9105): p. 805-6. 54. Dawson-Hughes, B., et al., Estimates of optimal vitamin D status. Osteoporos Int, 2005.
16(7): p. 713-6. 55. Holick, M.F., Vitamin D status: measurement, interpretation, and clinical application.
Ann Epidemiol, 2009. 19(2): p. 73-8. 56. Holick, M.F. and T.C. Chen, Vitamin D deficiency: a worldwide problem with health
consequences. Am J Clin Nutr, 2008. 87(4): p. 1080S-6S. 57. Gordon, C.M., et al., Prevalence of vitamin D deficiency among healthy adolescents.
Arch Pediatr Adolesc Med, 2004. 158(6): p. 531-7. 58. Sullivan, S.S., et al., Adolescent girls in Maine are at risk for vitamin D insufficiency. J
Am Diet Assoc, 2005. 105(6): p. 971-4.

200
59. Araujo, A., et al., Serum 25-hydroxyvitamin D and bone mineral density among Hispanic
men. Osteoporosis International, 2009. 20(2): p. 245-255. 60. Palacios, C., et al., Determinants of vitamin D status among overweight and obese Puerto
Rican adults. Ann Nutr Metab, 2012. 60(1): p. 35-43. 61. Zgaga, L., et al., Diet, environmental factors, and lifestyle underlie the high prevalence of
vitamin D deficiency in healthy adults in Scotland, and supplementation reduces the
proportion that are severely deficient. Journal of Nutrition, 2011. 141(8): p. 1535-42. 62. Michos, E.D., et al., 25-Hydroxyvitamin D deficiency is associated with fatal stroke
among whites but not blacks: The NHANES-III linked mortality files. Nutrition, (0). 63. Freedman, D.M., et al., Serum Levels of Vitamin D Metabolites and Breast Cancer Risk
in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Cancer Epidemiology Biomarkers & Prevention, 2008. 17(4): p. 889-894.
64. Botella-Carretero, J.I., et al., Vitamin D deficiency is associated with the metabolic
syndrome in morbid obesity. Clinical Nutrition, 2007. 26(5): p. 573-80. 65. Oh, J.H., et al., The level of vitamin D in the serum correlates with fatty degeneration of
the muscles of the rotator cuff. Journal of Bone & Joint Surgery - British Volume, 2009. 91(12): p. 1587-93.
66. Visser, M., et al., Low vitamin D and high parathyroid hormone levels as determinants of
loss of muscle strength and muscle mass (sarcopenia): the Longitudinal Aging Study
Amsterdam. Journal of Clinical Endocrinology & Metabolism, 2003. 88(12): p. 5766-72. 67. Kragt, J., et al., Higher levels of 25-hydroxyvitamin D are associated with a lower
incidence of multiple sclerosis only in women. Multiple Sclerosis, 2009. 15(1): p. 9-15. 68. Wang, T.J., et al., Vitamin D deficiency and risk of cardiovascular disease. Circulation,
2008. 117(4): p. 503-11. 69. Pilz, S., et al., Association of Vitamin D Deficiency with Heart Failure and Sudden
Cardiac Death in a Large Cross-Sectional Study of Patients Referred for Coronary
Angiography. Journal of Clinical Endocrinology & Metabolism, 2008. 93(10): p. 3927-3935.
70. Autier, P. and S. Gandini, Vitamin D supplementation and total mortality: a meta-
analysis of randomized controlled trials. Archives of Internal Medicine, 2007. 167(16): p. 1730-7.
71. Chung, I., et al., Anti-proliferative effects of calcitriol on endothelial cells derived from
two different microenvironments. The Journal of Steroid Biochemistry and Molecular Biology, 2007. 103(3–5): p. 768-770.
72. Jacques M, L., Immunomodulatory actions of 1,25-Dihydroxyvitamin D3. The Journal of Steroid Biochemistry and Molecular Biology, 1995. 53(1–6): p. 599-602.
73. Berk, B.C., et al., Endothelial Atheroprotective and Anti-inflammatory Mechanisms. Annals of the New York Academy of Sciences, 2001. 947(1): p. 93-111.
74. de Vries-van der Weij, J., et al., Anti-inflammatory salicylate beneficially modulates pre-
existing atherosclerosis through quenching of NF-κB activity and lowering of
cholesterol. Atherosclerosis, 2010. 213(1): p. 241-246. 75. Talmor, Y., et al., Calcitriol blunts pro-atherosclerotic parameters through NFkappaB
and p38 in vitro. Eur J Clin Invest, 2008. 38(8): p. 548-54.

201
76. Lumb, G.A., E.B. Mawer, and S.W. Stanbury, The apparent vitamin D resistance of
chronic renal failure: A study of the physiology of vitamin D in man. The American Journal of Medicine, 1971. 50(4): p. 421-441.
77. Mawer, E.B., et al., The distribution and storage of vitamin D and its metabolites in
human tissues. Clin Sci, 1972. 43(3): p. 413-31. 78. Becker, L.E., et al., Effect of paricalcitol and calcitriol on aortic wall remodeling in
uninephrectomized ApoE knockout mice. American Journal of Physiology - Renal Physiology, 2011. 300(3): p. F772-F782.
79. Husain, K., et al., Effects of Paricalcitol and Enalapril on Atherosclerotic Injury in
Mouse Aortas. American Journal of Nephrology, 2010. 32(4): p. 296-304. 80. Takeda, M., et al., Oral Administration of an Active Form of Vitamin D3 (Calcitriol)
Decreases Atherosclerosis in Mice by Inducing Regulatory T Cells and Immature
Dendritic Cells With Tolerogenic Functions. Arteriosclerosis, Thrombosis, and Vascular Biology, 2010. 30(12): p. 2495-2503.
81. Wang, X.X., et al., Vitamin D receptor agonist doxercalciferol modulates dietary fat-
induced renal disease and renal lipid metabolism. American Journal of Physiology - Renal Physiology, 2011. 300(3): p. F801-F810.
82. Dietary Reference Intakes for Calcium and Vitamin D. Committee to Review Dietary
Reference Intakes for Vitamin D and Calcium. , in 2010, Institute of Medicine: Washington, DC: National Academy of Sciences.
83. Tucker, K., et al., The Boston Puerto Rican Health Study, a longitudinal cohort study on
health disparities in Puerto Rican adults: challenges and opportunities. BMC Public Health, 2010. 10(1): p. 107.
84. Bermudez, O.I., E.K. Becker, and K.L. Tucker, Development of sex-specific equations for
estimating stature of frail elderly Hispanics living in the northeastern United States. American Journal of Clinical Nutrition, 1999. 69(5): p. 992-8.
85. Chumlea, W., et al., Stature prediction equations for elderly non-Hispanic white, non-
Hispanic black, and Mexican-American persons developed from NHANES III data. J Am Diet Assoc, 1998. 98: p. 137 - 142.
86. Allain, C.C., et al., Enzymatic determination of total serum cholesterol. Clin Chem, 1974. 20(4): p. 470-5.
87. Friedewald, W.T., R.I. Levy, and D.S. Fredrickson, Estimation of the concentration of
low-density lipoprotein cholesterol in plasma, without use of the preparative
ultracentrifuge. Clin Chem, 1972. 18(6): p. 499-502. 88. Dreon, D., et al., Use of NHANES Data to Assign Nutrient Densities to Food Groups in a
Multiethnic Diet History Questionnaire. Nutrition and Cancer, 1993. 20: p. 223 - 230. 89. Delgado, J.L., et al., Hispanic Health and Nutrition Examination Survey: methodological
considerations. Am J Public Health, 1990. 80 Suppl: p. 6-10. 90. Block, G. and A.F. Subar, Estimates of nutrient intake from a food frequency
questionnaire: the 1987 National Health Interview Survey. J Am Diet Assoc, 1992. 92(8): p. 969-77.
91. Tucker, K., et al., Adaptation of a food frequency questionnaire to assess diets of Puerto
Rican and non-Hispanic adults. American Journal of Epidemiology, 1998. 148(5): p. 507 - 518.

202
92. Brecher, G., M. Schneiderman, and G.Z. Williams, Evaluation of electronic red blood
cell counter. Am J Clin Pathol, 1956. 26(12): p. 1439-49. 93. Holick, M.F., The vitamin D deficiency pandemic and consequences for nonskeletal
health: mechanisms of action. Mol Aspects Med, 2008. 29(6): p. 361-8. 94. Holick, M.F., Vitamin D: extraskeletal health. Endocrinology and metabolism clinics of
North America, 2010. 39(2): p. 381-400, table of contents. 95. Lacour, B., et al., Parathyroid function and lipid metabolism in the rat. Miner Electrolyte
Metab, 1982. 7(3): p. 157-65. 96. Melamed, M.L., et al., 25-hydroxyvitamin d levels and the risk of mortality in the general
population. Archives of Internal Medicine, 2008. 168(15): p. 1629-1637. 97. Alvarez-Rodriguez, L., et al., Age and low levels of circulating vitamin D are associated
with impaired innate immune function. Journal of Leukocyte Biology, 2012. 91(5): p. 829-838.
98. Bellia, A., et al., Serum 25-hydroxyvitamin D levels are inversely associated with
systemic inflammation in severe obese subjects. Internal and Emergency Medicine, 2013. 8(1): p. 33-40.
99. Pittas, A.G., et al., Systematic Review: Vitamin D and Cardiometabolic Outcomes. Annals of Internal Medicine, 2010. 152(5): p. 307-314.
100. Zittermann, A., et al., Vitamin D supplementation enhances the beneficial effects of
weight loss on cardiovascular disease risk markers. American Journal of Clinical Nutrition, 2009. 89(5): p. 1321-7.
101. Kannel, W.B., et al., Serum Cholesterol, Lipoproteins, and the Risk of Coronary Heart
DiseaseThe Framingham Study. Annals of Internal Medicine, 1971. 74(1): p. 1-12. 102. Gordon, T., et al., High density lipoprotein as a protective factor against coronary heart
disease: The Framingham study. The American Journal of Medicine, 1977. 62(5): p. 707-714.
103. Hypponen, E., et al., 25-hydroxyvitamin D, IGF-1, and metabolic syndrome at 45 years
of age: a cross-sectional study in the 1958 British Birth Cohort. Diabetes, 2008. 57(2): p. 298-305.
104. Jorde, R., et al., High serum 25-hydroxyvitamin D concentrations are associated with a
favorable serum lipid profile. European Journal of Clinical Nutrition, 2010. 64(12): p. 1457-64.
105. Karhapää, P., et al., Diverse associations of 25-hydroxyvitamin D and 1,25-dihydroxy-
vitamin D with dyslipidaemias. Journal of Internal Medicine, 2010. 268(6): p. 604-610. 106. Kazlauskaite, R., et al., Vitamin D is associated with atheroprotective high-density
lipoprotein profile in postmenopausal women. Journal of Clinical Lipidology, 2010. 4(2): p. 113-119.
107. Maki, K.C., et al., Serum 25-hydroxyvitamin D is independently associated with high-
density lipoprotein cholesterol and the metabolic syndrome in men and women. Journal of Clinical Lipidology, 2009. 3(4): p. 289-296.
108. Jorde, R., et al., No improvement in cardiovascular risk factors in overweight and obese
subjects after supplementation with vitamin D3 for 1 year. Journal of Internal Medicine, 2010. 267(5): p. 462-472.
109. Mattei, J., et al., Allostatic load is associated with chronic conditions in the Boston
Puerto Rican Health Study. Social Science & Medicine, 2010. 70(12): p. 1988-96.

203
110. Tucker, K.L., et al., Self-reported prevalence and health correlates of functional
limitation among Massachusetts elderly Puerto Ricans, Dominicans, and non-Hispanic
white neighborhood comparison group. J Gerontol A Biol Sci Med Sci, 2000. 55(2): p. M90-7.
111. Tucker, K.L., O.I. Bermudez, and C. Castaneda, Type 2 diabetes is prevalent and poorly
controlled among Hispanic elders of Caribbean origin. Am J Public Health, 2000. 90(8): p. 1288-93.
112. Renzaho, A.M., J.A. Halliday, and C. Nowson, Vitamin D, obesity, and obesity-related
chronic disease among ethnic minorities: a systematic review. Nutrition, 2011. 27(9): p. 868-79.
113. Bhupathiraju, S.N., et al., Centrally located body fat is associated with lower bone
mineral density in older Puerto Rican adults. The American Journal of Clinical Nutrition, 2011. 94(4): p. 1063-1070.
114. Flegal, K.M., et al., Overweight and obesity in the United States: prevalence and trends,
1960-1994. International journal of obesity and related metabolic disorders : journal of the International Association for the Study of Obesity, 1998. 22(1): p. 39-47.
115. Holick, M.F., et al., Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an
Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism, 2011. 96(7): p. 1911-1930.
116. Bermudez, O., et al., Hispanic and non-Hispanic white elders from Massachusetts have
different patterns of carotenoid intake and plasma concentrations. Journal of Nutrition, 2005. 135(6): p. 1496 - 1502.
117. Kwan, L.L., O.I. Bermudez, and K.L. Tucker, Low vitamin B-12 intake and status are
more prevalent in Hispanic older adults of Caribbean origin than in neighborhood-
matched non-Hispanic whites. Journal of Nutrition, 2002. 132(7): p. 2059-64. 118. Pharmacists, A.S.o.H.-S., AHFS Pharmacologic-Therapeutic Classification 2008,
American Society of Health-System Pharmacists. 119. Friedewald, W.T., R.I. Levy, and D.S. Fredrickson, Estimation of the Concentration of
Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative
Ultracentrifuge. Clinical Chemistry, 1972. 18(6): p. 499-502. 120. Signorello, L.B., et al., Confounding by indication in epidemiologic studies of commonly
used analgesics. American Journal of Therapeutics, 2002. 9(3): p. 199-205. 121. Barnett, A.G., J.C. van der Pols, and A.J. Dobson, Regression to the mean: what it is and
how to deal with it. International Journal of Epidemiology, 2005. 34(1): p. 215-220. 122. Sterne, J.A.C., et al., Multiple imputation for missing data in epidemiological and clinical
research: potential and pitfalls. BMJ, 2009. 338. 123. Delvin, E.E., et al., Vitamin D Status Is Modestly Associated with Glycemia and
Indicators of Lipid Metabolism in French-Canadian Children and Adolescents. The Journal of Nutrition, 2010. 140(5): p. 987-991.
124. Forouhi, N.G., et al., Baseline Serum 25-Hydroxy Vitamin D Is Predictive of Future
Glycemic Status and Insulin Resistance: The Medical Research Council Ely Prospective
Study 1990–2000. Diabetes, 2008. 57(10): p. 2619-2625. 125. Giovannucci, E., et al., 25-hydroxyvitamin d and risk of myocardial infarction in men: A
prospective study. Archives of Internal Medicine, 2008. 168(11): p. 1174-1180.

204
126. Pilz, S., et al., Vitamin D and mortality in older men and women. Clinical Endocrinology, 2009. 71(5): p. 666-672.
127. Williams, D.M., A. Fraser, and D.A. Lawlor, Associations of vitamin D, parathyroid
hormone and calcium with cardiovascular risk factors in US adolescents. Heart, 2011. 97(4): p. 315-320.
128. Bonow, R.O., Primary Prevention of Cardiovascular Disease. Circulation, 2002. 106(25): p. 3140-3141.
129. Zittermann, A., et al., Vitamin D supplementation enhances the beneficial effects of
weight loss on cardiovascular disease risk markers. The American Journal of Clinical Nutrition, 2009. 89(5): p. 1321-1327.
130. Heikkinen, A., et al., Long-term vitamin D3 supplementation may have adverse effects on
serum lipids during postmenopausal hormone replacement therapy. European Journal of Endocrinology, 1997. 137(5): p. 495-502.
131. Nagpal, J., J.N. Pande, and A. Bhartia, A double-blind, randomized, placebo-controlled
trial of the short-term effect of vitamin D3 supplementation on insulin sensitivity in
apparently healthy, middle-aged, centrally obese men. Diabetic Medicine, 2009. 26(1): p. 19-27.
132. Jorde, R., et al., Cross-sectional and longitudinal relation between serum 25-
hydroxyvitamin D and body mass index: the Tromsø study. European Journal of Nutrition, 2010. 49(7): p. 401-407.
133. Yoon, V., N.M. Maalouf, and K. Sakhaee, The effects of smoking on bone metabolism. Osteoporosis International, 2012. 23(8): p. 2081-2092.
134. Lakhan, S. and A. Kirchgessner, Anti-inflammatory effects of nicotine in obesity and
ulcerative colitis. Journal of Translational Medicine, 2011. 9(1): p. 129. 135. Wang, H., et al., Nicotinic acetylcholine receptor alpha7 subunit is an essential regulator
of inflammation. Nature, 2003. 421(6921): p. 384-8. 136. Reid, I.R., Effects of calcium supplementation on circulating lipids: potential
pharmacoeconomic implications. Drugs Aging, 2004. 21(1): p. 7-17. 137. Hu, F.B., J.E. Manson, and W.C. Willett, Types of Dietary Fat and Risk of Coronary
Heart Disease: A Critical Review. Journal of the American College of Nutrition, 2001. 20(1): p. 5-19.
138. Van der Meer, R., et al., Effects of supplemental dietary calcium on the intestinal
association of calcium, phosphate, and bile acids. Gastroenterology, 1990. 99(6): p. 1653-9.
139. Major, G.C., et al., Supplementation with calcium + vitamin D enhances the beneficial
effect of weight loss on plasma lipid and lipoprotein concentrations. American Journal of Clinical Nutrition, 2007. 85(1): p. 54-9.
140. Junyent, M., et al., The effects of ABCG5/G8 polymorphisms on plasma HDL cholesterol
concentrations depend on smoking habit in the Boston Puerto Rican Health Study. Journal of Lipid Research, 2009. 50(3): p. 565-73.
141. Lai, C.-Q., et al., Population admixture associated with disease prevalence in the Boston
Puerto Rican health study. Human Genetics, 2009. 125(2): p. 199-209. 142. Mattei, J., et al., Apolipoprotein A5 polymorphisms interact with total dietary fat intake in
association with markers of metabolic syndrome in Puerto Rican older adults. Journal of Nutrition, 2009. 139(12): p. 2301-8.

205
143. Mattei, J., et al., Disparities in allele frequencies and population differentiation for 101
disease-associated single nucleotide polymorphisms between Puerto Ricans and non-
Hispanic whites. BMC Genetics, 2009. 14(10): p. 45. 144. 2010 ICD-9-CM.
145. Guillot, X., et al., Vitamin D and inflammation. Joint Bone Spine, 2010. 77(6): p. 552-557.
146. Querfeld, U., Vitamin D and inflammation. Pediatr Nephrol, 2013. 28(4): p. 605-10. 147. Dickie, L.J., et al., Vitamin D3 down-regulates intracellular Toll-like receptor 9
expression and Toll-like receptor 9-induced IL-6 production in human monocytes. Rheumatology (Oxford), 2010. 49(8): p. 1466-1471.
148. Wilson, A.M., M.C. Ryan, and A.J. Boyle, The novel role of C-reactive protein in
cardiovascular disease: risk marker or pathogen. Int J Cardiol, 2006. 106(3): p. 291-7. 149. Gabay, C. and I. Kushner, Acute-phase proteins and other systemic responses to
inflammation. N Engl J Med, 1999. 340(6): p. 448-54. 150. Rigby, W.F., S. Denome, and M.W. Fanger, Regulation of lymphokine production and
human T lymphocyte activation by 1,25-dihydroxyvitamin D3. Specific inhibition at the
level of messenger RNA. The Journal of Clinical Investigation, 1987. 79(6): p. 1659-1664.
151. Rigby, W.F., T. Stacy, and M.W. Fanger, Inhibition of T lymphocyte mitogenesis by 1,25-
dihydroxyvitamin D3 (calcitriol). The Journal of Clinical Investigation, 1984. 74(4): p. 1451-1455.
152. Zhu, Y., et al., Calcium and 1α,25-dihydroxyvitamin D3 target the TNF-α pathway to
suppress experimental inflammatory bowel disease. European Journal of Immunology, 2005. 35(1): p. 217-224.
153. Schleithoff, S.S., et al., Vitamin D supplementation improves cytokine profiles in patients
with congestive heart failure: a double-blind, randomized, placebo-controlled trial. American Journal of Clinical Nutrition, 2006. 83(4): p. 754-9.
154. Peterson, C. and M. Heffernan, Serum tumor necrosis factor-alpha concentrations are
negatively correlated with serum 25(OH)D concentrations in healthy women. Journal of Inflammation, 2008. 5(1): p. 10.
155. Beilfuss, J., et al., Effects of a 1-year supplementation with cholecalciferol on interleukin-
6, tumor necrosis factor-alpha and insulin resistance in overweight and obese subjects. Cytokine, 2012. 60(3): p. 870-4.
156. Ranjit, N., et al., Socioeconomic Position, Race/Ethnicity, and Inflammation in the Multi-
Ethnic Study of Atherosclerosis. Circulation, 2007. 116(21): p. 2383-2390. 157. Dawson-Hughes, B., et al., Estimates of optimal vitamin D status. Osteoporosis
International, 2005. 16(7): p. 713-716. 158. Document : PILKCR-7, 2003-11-25, High sensitivity CRP, and according to Immulate
1000 Operating Manual, Document #600467, rev B1, revision 5.XX August 2003, , D.P.C. (DCP), Editor 2003.
159. Jamal-Allial, A.A. and K.L. Tucker, Serum Vitamin D Concentrations, Dietary Sources,
and its relation to BMI among Puerto Ricans Living in the Greater Boston Area. To be submitted, 2013.

206
160. Giovannini, L., et al., 1,25-dihydroxyvitamin D3 dose-dependently inhibits LPS-induced
cytokines production in PBMC modulating intracellular calcium. Transplantation Proceedings, 2001. 33(3): p. 2366-2368.
161. Cohen, M., et al., Regulation of TNF-[agr] by 1[agr],25-dihydroxyvitamin D3 in human
macrophages from CAPD patients. Kidney International, 2001. 59(1): p. 69–75. 162. Nonn, L., et al., Inhibition of p38 by Vitamin D Reduces Interleukin-6 Production in
Normal Prostate Cells via Mitogen-Activated Protein Kinase Phosphatase 5:
Implications for Prostate Cancer Prevention by Vitamin D. Cancer Research, 2006. 66(8): p. 4516-4524.
163. Amer, M. and R. Qayyum, Relation between serum 25-hydroxyvitamin D and C-reactive
protein in asymptomatic adults (from the continuous National Health and Nutrition
Examination Survey 2001 to 2006). American Journal of Cardiology, 2012. 109(2): p. 226-30.
164. Falcon, L.M. and K.L. Tucker, Prevalence and correlates of depressive symptoms among
Hispanic elders in Massachusetts. J Gerontol B Psychol Sci Soc Sci, 2000. 55(2): p. S108-16.
165. Fantuzzi, G., Adipose tissue, adipokines, and inflammation. The Journal of allergy and clinical immunology, 2005. 115(5): p. 911-9; quiz 920.
166. Van Lente, F., Markers of inflammation as predictors in cardiovascular disease. Clin Chim Acta, 2000. 293(1-2): p. 31-52.
167. Organization, W.H., Noncommunicable diseases country profiles 2011. WHO global
report, 2011. p. 209. 168. Mithal, A., et al., Global vitamin D status and determinants of hypovitaminosis D.
Osteoporosis International, 2009. 20(11): p. 1807-20. 169. Ogden CL, C.M., Kit BK, Flegal KM., Prevalence of obesity in the United States, 2009–
2010. NCHS data brief, 2012, National Center for Health. 170. Flegal Km, C.M.D.K.B.K.O.C.L., Prevalence of obesity and trends in the distribution of
body mass index among us adults, 1999-2010. JAMA, 2012. 307(5): p. 491-497. 171. Renzaho, A.M.N., J.A. Halliday, and C. Nowson, Vitamin D, obesity, and obesity-related
chronic disease among ethnic minorities: A systematic review. Nutrition, 2011. 27(9): p. 868-879.
172. Snijder, M.B., et al., Adiposity in relation to vitamin D status and parathyroid hormone
levels: a population-based study in older men and women. Journal of Clinical Endocrinology & Metabolism, 2005. 90(7): p. 4119-23.
173. Brock, K., et al., Low vitamin D status is associated with physical inactivity, obesity and
low vitamin D intake in a large US sample of healthy middle-aged men and women. J Steroid Biochem Mol Biol, 2010. 121(1-2): p. 462-6.
174. Norman, A.W., Minireview: vitamin D receptor: new assignments for an already busy
receptor. Endocrinology, 2006. 147(12): p. 5542-8. 175. Tuohimaa, P., Vitamin D and aging. Journal of Steroid Biochemistry & Molecular
Biology, 2009. 114(1-2): p. 78-84. 176. Young, K.A., et al., Association of Plasma Vitamin D Levels with Adiposity in Hispanic
and African Americans. Journal of Clinical Endocrinology & Metabolism, 2009. 94(9): p. 3306-3313.

207
177. McGill, A.-T., et al., Relationships of low serum vitamin D3 with anthropometry and
markers of the metabolic syndrome and diabetes in overweight and obesity. Nutrition Journal, 2008. 7: p. 4.
178. Earthman, C.P., et al., The link between obesity and low circulating 25-hydroxyvitamin D
concentrations: considerations and implications. Int J Obes, 2012. 36(3): p. 387- 96. 179. Compher, C. and K.O. Badellino, Obesity and Inflammation: Lessons From Bariatric
Surgery. Journal of Parenteral and Enteral Nutrition, 2008. 32(6): p. 645-647. 180. Li, J., et al., 1α,25-Dihydroxyvitamin D hydroxylase in adipocytes. The Journal of Steroid
Biochemistry and Molecular Biology, 2008. 112(1–3): p. 122-126. 181. Looker, A.C.J., C L. Lacher, D A. Pfeiffer, C M. Schleicher, R L. Sempos, C T.,
Vitamin D status: United States, 2001–2006, in NCHS data brief2011, National Center for Health Statistics: Hyattsville, MD.
182. Forrest, K.Y.Z. and W.L. Stuhldreher, Prevalence and correlates of vitamin D deficiency
in US adults. Nutrition Research, 2011. 31(1): p. 48-54. 183. Flegal, K.M., et al., PRevalence and trends in obesity among us adults, 1999-2008.
JAMA, 2010. 303(3): p. 235-241. 184. Casas, Y.G., et al., Total and regional body composition across age in healthy Hispanic
and white women of similar socioeconomic status. The American Journal of Clinical Nutrition, 2001. 73(1): p. 13-18.
185. Wiklund, P., et al., Abdominal and Gynoid Fat Mass Are Associated with Cardiovascular
Risk Factors in Men and Women. Journal of Clinical Endocrinology & Metabolism, 2008. 93(11): p. 4360-4366.
186. McCarty, M.F., A paradox resolved: the postprandial model of insulin resistance
explains why gynoid adiposity appears to be protective. Medical Hypotheses, 2003. 61(2): p. 173-176.
187. Weishaar, T. and J.M. Vergili, Vitamin D Status Is a Biological Determinant of Health
Disparities. Journal of the Academy of Nutrition and Dietetics, 2013. 113(5): p. 643-651. 188. McKinney, K., C.R. Breitkopf, and A.B. Berenson, Association of race, body fat and
season with vitamin D status among young women: a cross-sectional study. Clinical Endocrinology, 2008. 69(4): p. 535-541.
189. Parikh, S.J., et al., The Relationship between Obesity and Serum 1,25-Dihydroxy Vitamin
D Concentrations in Healthy Adults. Journal of Clinical Endocrinology & Metabolism, 2004. 89(3): p. 1196-1199.
190. Arunabh, S., et al., Body Fat Content and 25-Hydroxyvitamin D Levels in Healthy
Women. Journal of Clinical Endocrinology & Metabolism, 2003. 88(1): p. 157-161. 191. White, J., et al., Precision of single vs bilateral hip bone mineral density scans. Journal of
clinical densitometry : the official journal of the International Society for Clinical Densitometry, 2003. 6(2): p. 159-62.
192. Mazess, R.B., et al., Dual-energy x-ray absorptiometry for total-body and regional bone-
mineral and soft-tissue composition. The American Journal of Clinical Nutrition, 1990. 51(6): p. 1106-12.
193. Jamal-Allial, A.A., J.L. Griffith, and K.L. Tucker, The Longitudinal Association of
Vitamin D Serum Concentrations & Adiposity Phenotypes. To be submitted, 2013. 194. Jacobs, E.J., et al., WAist circumference and all-cause mortality in a large us cohort.
Archives of Internal Medicine, 2010. 170(15): p. 1293-1301.

208
195. Panagiotakos, D.B., et al., The implication of obesity and central fat on markers of
chronic inflammation: The ATTICA study. Atherosclerosis, 2005. 183(2): p. 308-315. 196. Dos Santos, R.E., et al., Relationship of body fat distribution by waist circumference,
dual-energy X-ray absorptiometry and ultrasonography to insulin resistance by
homeostasis model assessment and lipid profile in obese and non-obese postmenopausal
women. Gynecological Endocrinology, 2005. 21(5): p. 295-301. 197. Fontana, L., et al., Visceral Fat Adipokine Secretion Is Associated With Systemic
Inflammation in Obese Humans. Diabetes, 2007. 56(4): p. 1010-1013. 198. Savgan-Gurol, E., et al., Waist to hip ratio and trunk to extremity fat (DXA) are better
surrogates for IMCL and for visceral fat respectively than for subcutaneous fat in
adolescent girls. Nutrition & Metabolism, 2010. 7(1): p. 86. 199. Roger, V.L., et al., Heart disease and stroke statistics--2011 update: a report from the
American Heart Association. Circulation, 2011. 123(4): p. e18-e209. 200. Barcelo, A., et al., Waist circumference, BMI and the prevalence of self-reported diabetes
among the elderly of the United States and six cities of Latin America and the Caribbean. Diabetes Res Clin Pract, 2007. 78(3): p. 418 - 427.
201. McTigue K, L.J.C.V.A. and et al., MOrtality and cardiac and vascular outcomes in
extremely obese women. JAMA, 2006. 296(1): p. 79-86. 202. Bischoff-Ferrari, H.A., et al., Estimation of optimal serum concentrations of 25-
hydroxyvitamin D for multiple health outcomes. The American Journal of Clinical Nutrition, 2006. 84(1): p. 18-28.
203. Zadshir, A., et al., The prevalence of hypovitaminosis D among US adults: data from the
NHANES III. Ethnicity & disease, 2005. 15(4 Suppl 5): p. S5-97-101. 204. Affairs, C.o.S., U.S. Census Bureau 2006. American Community Survey: ACS
Demographic and Housing Estimates
Hispanic Health in the United States. JAMA, 2006. 265(2): p. 248 - 252. 205. Tucker, K., et al., Self-reported prevalence and health correlates of functional limitation
among Massachusetts elderly Puerto Ricans, Dominicans, and non-Hispanic white
neighborhood comparison group. J Gerontol A Biol Sci Med Sci, 2000. 55(2): p. M90 - 97.
206. Lin, H., et al., Hypertension among Hispanic elders of a Caribbean origin in
Massachusetts. Ethn Dis, 2002. 12(4): p. 499-507. 207. Warnecke, R., et al., Approaching health disparities from a population perspective: the
National Institutes of Health Centers for Population Health and Health Disparities. Am J Public Health, 2008. 98(9): p. 1608 - 1615.
208. Organization, W.H., Obesity: preventing and managing the global epidemic., in Report of
a WHO Consultation on Obesity World Health Organization1998, World Health Organization: Geneva, Switzerland.
209. Ross, A.C., The 2011 report on dietary reference intakes for calcium and vitamin D. Public Health Nutr, 2011. 14(5): p. 938-9.
210. Zittermann, A., et al., Vitamin D deficiency and mortality risk in the general population:
a meta-analysis of prospective cohort studies. The American Journal of Clinical Nutrition, 2012. 95(1): p. 91-100.
211. Greene-Finestone, L.S., et al., 25-Hydroxyvitamin D in Canadian adults: biological,
environmental, and behavioral correlates. Osteoporos Int, 2011. 22(5): p. 1389-99.

209
212. Janssen, H.C., et al., Determinants of vitamin D status in healthy men and women aged
40-80 years. Maturitas, 2013. 74(1): p. 79-83. 213. Diaz, V.A., et al., The Association of Vitamin D Deficiency and Insufficiency with
Diabetic Nephropathy: Implications for Health Disparities. The Journal of the American Board of Family Medicine, 2009. 22(5): p. 521-527.
214. Holick, M.F., J.A. MacLaughlin, and S.H. Doppelt, Regulation of Cutaneous Previtamin
D: Photosynthesis in Man: Skin Pigment is not an Essential Regulator. Science, 1981. 211(4482): p. 590-593.
215. Jacques, P.F., et al., Plasma 25-hydroxyvitamin D and its determinants in an elderly
population sample. Am J Clin Nutr, 1997. 66(4): p. 929-36. 216. Zhang, R. and D. Naughton, Vitamin D in health and disease: Current perspectives.
Nutrition Journal, 2010. 9(1): p. 65. 217. Martins, D., et al., Prevalence of Cardiovascular Risk Factors and the Serum Levels of
25-Hydroxyvitamin D in the United States: Data From the Third National Health and
Nutrition Examination Survey. Archives of Internal Medicine, 2007. 167(11): p. 1159-1165.
218. Holick, M.F., et al., Vitamin D2 is as effective as vitamin D3 in maintaining circulating
concentrations of 25-hydroxyvitamin D. J Clin Endocrinol Metab, 2008. 93(3): p. 677-81. 219. LIPS, P., et al., The Effect of Vitamin D Supplementation on Vitamin D Status and
Parathyroid Function in Elderly Subjects. Journal of Clinical Endocrinology & Metabolism, 1988. 67(4): p. 644-650.
220. van Rompay, M.I., et al., Acculturation and Sociocultural Influences on Dietary Intake
and Health Status among Puerto Rican Adults in Massachusetts. Journal of the Academy of Nutrition and Dietetics, 2012. 112(1): p. 64-74.
221. Jorde, R. and G. Grimnes, Vitamin D and metabolic health with special reference to the
effect of vitamin D on serum lipids. Progress in Lipid Research, 2011. 50(4): p. 303-312. 222. Foss, Y.J., Vitamin D deficiency is the cause of common obesity. Med Hypotheses, 2009.
72(3): p. 314-21. 223. Rompay, M., et al., Prevalence of Cardiovascular Disease Risk Factors Among Older
Puerto Rican Adults Living in Massachusetts. Journal of Immigrant and Minority Health, 2011. 13(5): p. 825-833.

210
TABLE 6.1 Descriptive characteristics of men and women in the Boston Puerto Rican Health
Study (BPRHS) 1
Women
(n=1050)
Men
(n=445) P
value
Age (y) 57.3 ± 7.5 56.6 ± 8.0 0.1*
Education (< 8th grade %) 48.0 44.0 0.1†
Poverty (%) 62.0 51.0 0.0003†
BMI (kg/m2) 33.0 ± 7.0 30.0 ± 5.2 <.0001*
Serum Albumin (g/L) 42.5 ± 3.1 43.2 ± 3.6 0.001*
Serum Creatinine (nmol/L) 68.0 ± 27.5 88.0 45.1 <.0001*
Number of Miles Walked/day ‡ 1.0 ± 1.4 1.3 ± 1.6 <.0001*
25(OH)D (nmol/L) 43.1 ± 17.0 43.5 ± 16.5 0.6 *
Vitamin D Supplement use (> 5µg/day)
(%) 30.0 24.0 0.02†
Dietary vitamin D intake•|| (µg/day) 5.3± 2.7 5.2 ± 3.4 0.5 *
Total vitamin D intake•|| (µg/day) 7.3 ± 3.3 6.6 ± 4.2 0.001*
BMI, body mass index; 25(OH)D, 25-hydroxyvitamin D. 1Data are presented as mean ± SD for continuous variables or as % for categorical variables * Values were compared using t-test. † Values were compared using χ2- test ‡ Range = 0-10 miles/day • The recommended dietary allowance (RDA) for vitamin D for men and women aged 19-70 years =15 ug /day [82] ||Adjusted for energy intake using ANOVA (PROC GLM; SAS Institute, Cary, NC).

211
TABLE 6.2 Age-adjusted means of serum 25-hydroxyvitamin D (25(OH)D) concentration stratified by sex for different
characteristics among BPRHS participants, ages 45-75 years
Variables Women Men
n (%)* LSM SEM P value n (%) LSM SEM P
value
Age (y)
45-59 651 (61.5%) 42.0 0.64 281 (63.0%) 44.4 1.00
60-75 407 (38.5%) 45.0 0.81 0.007 164 (37.0%) 42.0 1.33 0.1
Vitamin D Supplement (IU/day) † †‡
≤ 200 738 (70.0%) 41.1 0.6 338 (77.3%) 41.5 0.8
200-400 224 (21.5%) 46.5 1.1 <.0001 90 (20.5%) 51.0 1.6 <.0001
≥ 400 77 (8.5%) 53.1 2.0 <.0001 9 (2.1 %) 39.2 5.36 0.9
<.0001 || <.0001
||
Season of measurement†
Summer (July-September) 356 (34.5%) 44.5 0.9 137 (32.0%) 46.5 1.4
Fall (October- December) 264 (26.0%) 46.0 0.8 0.4 124 (29.0%) 48.7 1.4 0.6
Winter (January-March) 184 (18.0%) 41.1 1.2 0.05 78 (18.0%) 37.5 1.8 <.0001
Spring (April-June) 224 (21.5%) 38.2 1.1 <.0001 91 (21.3%) 37.0 1.6 <.0001
<.0001 || <.0001
||
Body Mass Index (kg/m2) †
≤ 25 114 (11.0%) 44.0 1.5 80 (18.5%) 43.5 2.0
25-30 282 (27.3%) 45.5 0.9 0.8 164 (37.5%) 44.0 1.3 0.9
30-35 307 (29.3%) 44.5 0.9 0.9 130 (30.2%) 43.0 1.5 0.9
≥ 35 307 (29.3%) 44.5 0.9 0.08 130 (30.2%) 43.0 1.5 0.9

212
0.001 || 0.9
||
Smoking Status†
No 832 (79.5%) 44.0 1.1 291 (66.0%) 44.0 1.0
Yes 217 (20.5%) 41.0 0.5 0.01 149 (34.0%) 43.0 1.4 0.6
Alcohol Intake†
No 675 (64.5%) 43.0 0.7 211 (49.0%) 44.5 1.2
Yes 376 (35.5%) 44.0 0.8 0.4 228 (51.0%) 43.0 1.1 0.2
Serum Albumin† (g/L)
< 38 49 (5%) 42.0 2.2 16 (4.0%) 35.0 4.0
≥ 38 964 (95%) 43.1 0.5 0.5 410 (96.0%) 44.0 0.8 0.03
Serum Creatinine (nmol/L) †•
35.5 - 61.0 280 (27.5%) 41.5 1.0 19 (4.5%) 34.5 4.0
62.0 -70.0 298 (29.0%) 42.5 1.0 0.6 46 (11.0%) 40.0 2.4 0.3
71.0 -79.5 223 (22.0%) 45.3 1.1 0.009 92 (21.5%) 42.0 2.0 0.1
80.0 - 698 221 (22.0%) 44.1 1.1 0.1 270 (63.0%) 45.3 1.0 0.01
0.02 || 0.009
||
Miles Walked/day†
0 mile/day 263 (25.0%) 41.3 1.1 52 (12.0%) 40.5 2.4
0- 0.5 mile/day 395 (38.0%) 42.5 0.8 0.5 140 (32.0%) 44.0 1.4 0.3
> 0.5 mile/day 367 (37.0%) 45.0 1.0 0.01 247 (56.3%) 44.0 1.1 0.3
0.01 || 0.4
||
† Age-adjusted means were calculated with LSMEANS ANOVA (PROC GLM; SAS Institute, Cary, NC). Values presented are means || P-values for trend are calculated based on Dunnett adjustment for multiple comparisons (P > 0.05)

213
TABLE 6.3 Correlates1of serum 25(OH)D concentration among Puerto Rican adults stratified by
sex.
Variable
Women (n=935) Men (n=381)
β* SEM P
value† β
* SEM P value†
Age (years) 0.15 10 0.01 -0.03 0.1 0.7
Seasonality
Fall vs. Summer 2.0 1.3 0.15 2.04 2.02 0.3
Winter vs. Summer - 3.0 1.5 0.04 - 9.5 2.3 <.0001
Spring vs. Summer -6.1 1.4 <.0001 - 10.5 2.3 <.0001
BMI (kg/m2) -0.24 0.1 .002 0.04 0.15 0.7
Miles walked/day 0.6 0.3 0.05 0.7 0.5 0.1
Vitamin D supplement (µg/day)
< 5 vs. 10 µg/day -11.0 2.0 <.0001 1.1 5.6 0.8
5-10 vs. 10 µg/day -6.5 2.0 0.002 9.3 5.7 0.1
Dietary vitamin D (µg/day) †
1.0 0.2 <.0001 0.3 0.2 0.2
Serum Albumin (g/L) 0.5 0.2 0.006 0.6 0.2 0.008
Smoking (No vs. Yes) 3.5 1.3 0.008 0.2 2.0 0.8
1β-coefficients, SEM and P-values were calculated using PROC GLM; (SAS Institute, Cary,
NC). All covariates were included in the model simultaneously, including adjustment for serum creatinine, alcohol intake education (< 8th grade %) and poverty. †Dietary vitamin D adjusted for energy intake.

214
TABLE 6.4 The least-square means of serum 25(OH)D concentration for the effect of vitamin
D supplements categories by sex
Women (n=935) Men (n=381) β SEM β SEM
≤ 200 IU/day 40.25a 0.70 40a 1.0
200-400 45.0b 1.14 48.3ab 1.81
≥ 400 IU/day 51.0c 1.85 37ac 5.40
β coefficients, SEM and P-values were calculated using PROC GLM; (SAS Institute, Cary, NC). The model was adjusted for age, BMI, season, dietary vitamin D, miles walking/day, serum albumin, serum creatinine, smoking, alcohol intake education (< 8th grade %) and poverty.

215
TABLE 6.5 The least-square means of serum 25(OH)D concentration and seasons categories by
age groups
40-59 Years 60-75 Years β
* SEM β* SEM
Summer 50 1.50 46 1.5 Fall 50.3 1.15 48.5 1.32
Winter 41.3 1.35 45.2 1.75 Spring 38.4 1.32 43.4 1.65
β coefficients, SEM and P-values were calculated using PROC GLM; (SAS Institute, Cary, NC). The model was adjusted for sex, BMI, dietary vitamin D, miles walking/day, serum albumin, serum creatinine, smoking, alcohol intake education (< 8th grade %) and poverty.

216
TABLE 6.6 Major Dietary Sources of Vitamin D intake among Puerto Rican adults *
Rank Food Groups % contribution of dietary vitamin D intake
1 Milk (whole, 2%,1% & milk products) 32.4 2 Supplements 28.7 3 Fish 16.2 4 Eggs 4.5 5 Cereal, Ready-to-eat, Cold 4.3 6 Beef 2.3 7 Processed Meat, Sausage, Frank 2.1 8 Chicken/Turkey 2.0 9 Pork 1.3 10 Ice cream, Sherbet, Frozen Yogurt 1.2 11 Yogurt 1.1 12 Cheese 0.9
* Food groups listed were the ones that contributed more than 0.8% of dietary vitamin D intakes.

217
FIGURE 6.1 Prevalence of low serum 25-hydroxyvitamin D concentration among Puerto Rican
men (n=426) and women (n=1015). Serum 25(OH)D concentration was categorized: deficient ≤
50 nmol/l, insufficient 50-75 nmol/L, and sufficient ≥ 75 nmol/L. Values are percentage of
individuals.
0
10
20
30
40
50
60
70
80
Men Women
Per
cen
tage
%
<50
50 - 75
75 nmol/L

218
FIGURE 5.2 Association between the median intake of total vitamin D as defined by the RDA
and serum 25(OH)D concentration (nmol/L) for BPRHS participants (n=1433). The vitamin D
RDA is 15 µg/day = 600 IU/day. Data points are least square means for serum 25(OH)D,
adjusted for age, sex, and season, plotted against category of the RDA of vitamin D intake (P-
trend <0.0001). RDA categories are significantly different from referent group ≤ ½ RDA
(Dunnett adjustment for multiple comparisons; P < 0.05).
30
35
40
45
50
55
60
≤ ½ RDA ½ RDA - RDA ≥ RDA
Ser
um
25(O
H)D
nm
ol/
L
Median intake of vitamin D by µg/day the RDA

219
* *
FIGURE 6.3 Association between vitamin D intake from food only sources (µg/day) and serum
25(OH)D concentration (nmol/L) among non-supplement users of the BPRHS participants
(n=1036). Data points are least square means, adjusted for age, sex, and season, plotted at the
median for each quintile category of energy-adjusted vitamin D intake from food (P-trend =
0.0007). Dietary intake of vitamin D equal to 5.28 µg/day and higher contributed to a
significantly higher serum 25(OH)D concentration (nmol/L) compared to the referent group
5.23µg/day (Dunnett adjustment for multiple comparisons; P < 0.05).
30
35
40
45
50
55
5.23 5.26 5.28 5.31 5.37
Ser
um
25(O
H)D
con
cen
trati
on
(n
mol/
L)
Dietary intakes of vitamin D µg/day by quintiles
*

220
FIGURE 6.4 Mean serum 25(OH)D concentration by BMI categories of Puerto Rican women
(n=990), adjusted for age, season, dietary vitamin D and vitamin D supplement use (P-trend =
0.001). BMI ≥40 is significantly different from the referent group BMI ≥ 25; (Dunnett
adjustment for multiple comparisons; P < 0.05).
35
37
39
41
43
45
47
49
51
53
≤ 25 25-30 30-35 35-40 ≥ 40
Ser
um
25(O
H)D
con
cen
trati
on
(n
mol/
L)
BMI (kg/m2)
*













![EFFECTS OF SOY CONSUMPTION ON SERUM LIPIDS AND … OF SOY CONSUMPTION ON... · concentration of lipoprotein(a) [Lp(a)], are one of the major risk factors for cardiovascular disease](https://img.pdfslide.us/doc/110x75/5c90954309d3f2213e8c7f61/effects-of-soy-consumption-on-serum-lipids-and-of-soy-consumption-on-concentration.jpg)