Embed Size (px)
Citation preview
International Journal of Dermatology, Vol. 33, No. 11, November 1994
REPORT
ELEVATED SERUM NICKEL CONCENTRATION INPSORIASIS VULGARIS
STEVEN A. SMITH, M.D., FARAH AAMIR, M.B.B.S., AND MICHAEL P. B. OTIS
AbstractBackground. Psoriasis vulgaris is a common skin diseaseafflicting 1-3% of the American population. Its pathogene-sis remains unknown despite concerted research efforts.Our purpose was to study baseline serum nickei concentra-tions in psoriasis vulgaris subjects and in healthy controlsubjects.
Methods. Sixteen psoriasis vulgaris subjects with activedisease (in 14 of moderate to marked severity), and 11 age-and sex-matched healthy control subjects were studied.Serum nickel determinations were performed using elec-trothermal atomic absorption spectrophotometry (ETAAS).
Results. Despite the relatively small sample size, signifi-cant elevation of mean serum nickel concentration wasfound in the psoriasis group compared to the control group(P = 0.019).
Conclusions. Recognition of abnormal nickel homeostasiscould point the way to greater understanding of the prima-ry biochemical defect in the psoriatic process. Alternatively,this finding may mark an association without pathogenicsignificance. Further investigation is needed.
Int J Dermatol 1994; 33:783-785
Psoriasis is a chronic intractable skin disease affecting1-3% of the American population; its pathogenesis re-mains unexplained.' A simple biochemical explanationof this ancient disease has been clouded by complexmodern immunologic theories.
Considerable interest in trace and ultratrace miner-als and their relationship to psoriasis has been shownfor some time. Most thoroughly investigated have beenzinc, copper, and selenium.^"-' The search for a simplebiochemical understanding of this disease continues tobe elusive.
Certain tnineral deficiency states that cause psoriasi-fortn findings bave stimulated considerable interest.For example, hereditary (acrodermatitis enteropatliica)and acquired (associated with total parenteral nutri-
From the Department of Dermatology, University of Okla-homa Health Science Center, Tulsa, Oklahoma.
Address for correspondence: Steven A. Smith, M.D., 3010 S.Harvard, Suite #234, Tulsa, OK 74114-6114.
tion (TPN), chronic liver disease, etc.) zinc deficiencystates can cause psoriasiform abnormalities.*'^
Nickel is a transition element, similar to zinc, cop-per, cobalt, and iron. Since scaly, crusty, rough skinhas been experimentally induced in nickel-deprivedgoats and minipigs,^ we chose to measure serum nickelconcentrations in subjects witb psoriasis vulgaris com-paring them to healthy control subjects.
MethodsSerum nickel concentrations were determined for 16 psori-asis vulgaris subjects with active disease of varying severi-ty (in 14 moderately to markedly severe), and 11 age- andsex-matched healthy controls. Student's t-test was used todetermine if there were statistically significant differencesbetween these groups. Since ultratrace nickel concentra-tions were being studied in serum (less than 1 pg/L), mod-ern methods to avoid external nickel contamination werefollowed meticulously, including all stages of specimen col-lection, handling, storage, transport, and analysis.'-'" Speci-mens were analyzed in batches, using electrothermalatomic absorption spectrophotometry (ETAAS), at the Uni-versity of Virginia Health Sciences Center, Clinical Labora-tories, Charlottesville, Virginia.
RESULTS
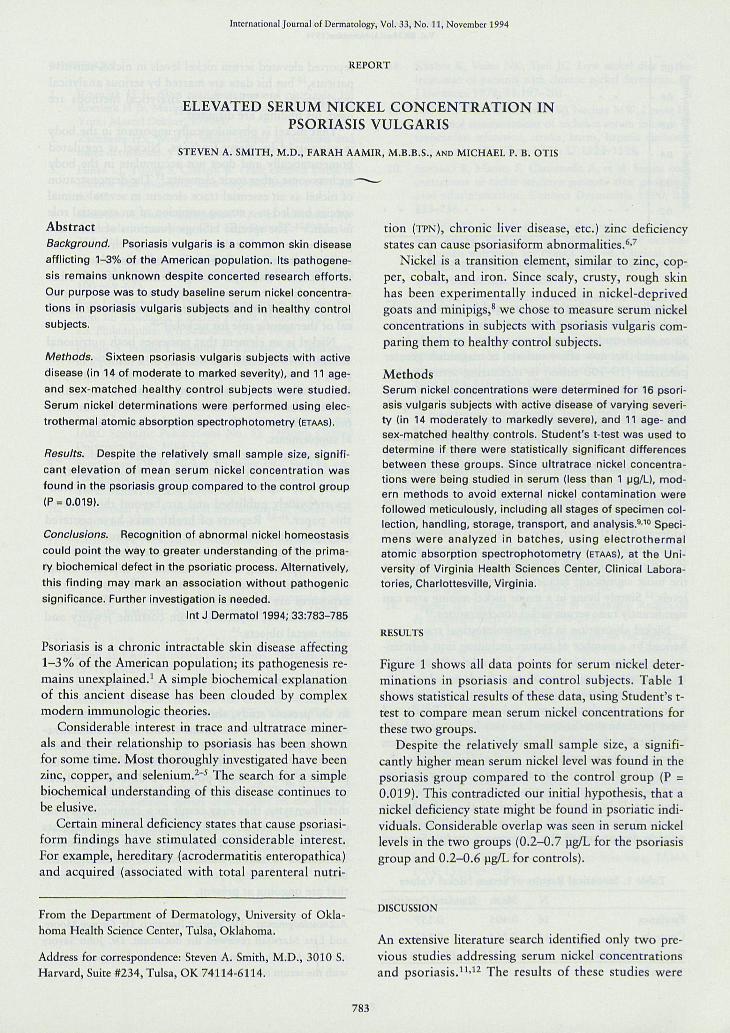
Figure 1 shows all data points for serum nickel deter-minations in psoriasis and control subjects. Table 1shows statistical results of tbese data, using Student's t-test to compare mean serum nickel concentrations forthese two groups.
Despite the relatively small sample size, a signifi-cantly higher mean serum nickel level was found in thepsoriasis group compared to the control group (P =0.019). This contradicted our initial hypothesis, that anickel deficiency state might be found in psoriatic indi-viduals. Considerable overlap was seen in serum nickellevels in the two groups (0.2-0.7 jag/L for the psoriasisgroup and 0.2-0.6 jig/L for controls).
DISCUSSION
An extensive literature search identified only two pre-vious studies addressing serum nickel concentrationsand psoriasis.'^'^^ The results of these studies were
783
International Journal of DermatologyVol. 33, No. t l , November t994
0.7 -
0.6 -
0.5 -
.10 0.3 -B'^ 0.2 -
Psoriasis Control
Figure 1. Data points for serum nickel concentrations.
contradictory and both were marred by serious meth-odologic errors and/or serious analytic inaccuracies.Since these studies were done, analytic methods haveadvanced that now allow order(s) of magnitude greaterprecision (10-100 times) in measuring serum nickelconcentrations.' Furthermore, much greater accuracyis possible today with greater awareness of the impor-tance of avoiding specimen contamination.'"
To our knowledge, the present study reflects a freshinsight into psoriatic nickel homeostasis that could playa role in understanding better the possible underlyingbiochemical/genetic defect. Many factors may affectnickel levels in the body. Day to day factors such asstress, strain, or physical effort have been only brieflyaddressed in the literature." Seasonal serum nickelvariations are not known. Certain occupational and en-vironmental exposures have been well studied and arethe most signiflcant factors in elevating serum nickellevels.'^ Simply living in a major nickel mining area cansignificantly raise serum nickel concentrations.^''
Nickel absorption in the gastrointestinal tract is en-hanced by a number of factors including iron deflcien-cy, pregnancy, and lactation." It is markedly inhibitedby simultaneous ingestion of most foods and drinks.'^
Certain chelating agents such as disulfiram havebeen shown to elevate serum nickel levels.''' Foods andfood processing techniques can also lead to a high di-etary intake of nickel and restriction of these has beenshown to reduce signiflcantly renal nickel excretion.'*
Serum nickel levels may rise significantly with someacute illnesses such as burns, stroke, and myocardialinfarction.'' In contrast, psoriasis is the only chronicdisease in which elevated serum nickel levels have beenreliably demonstrated (by the present study). Santucci
Tahle 1. Statistical Results of Serum Nickel Values
N Mean Standard Deviation
Psoriatics 16 0.405 0.157
Controls 11 0.264 0.143
Results of Student's t-test t = 2.435 P* = 0.019
* two-tailed test.
reported elevated serum nickel levels in nickel-sensitivepatients,^" but his data are marred by serious analyticalinaccuracies.'''" When better analytical methods areused, his findings are disputed.'^
That nickel is physiologically important in the bodyis supported by many findings. Nickel is regulatedhomeostatically and does not accumulate in the bodysuch as some other toxic elements.'^ The demonstrationof nickel as an essential trace element in several animalspecies has led to a strong suspicion of an essential rolein man.^'^' The specific biologic functions of nickel arepoorly understood at this time, although circumstantialevidence points to a potential metalloenzyme(s) cofac-tor function.^^ Multiple biologic interactions with otherclosely related transition elements, such as iron, copper,and zinc, lend further credibility to a possible biochemi-cal or therapeutic role for nickel.̂ ^"^^
Nickel is an element that possesses both nutritionaland potentially toxic or carcinogenic properties. In thepast, it was used therapeutically for a wide variety ofchronic ailments, including epilepsy, headache, neural-gia, amenorrhea, and diarrhea.^^"3° Nickel is currentlybeing incorporated into some multivitamin and miner-al supplements.
Many studies on nickel have focused on the nega-tive aspects of various nickel compounds (e.g., theirtoxic, carcinogenic, and allergic potential). These stud-ies are widely published and are beyond the scope ofthis paper.^'-33 Reports of health risks have centeredlargely around the acute toxicity of exposure to nickelcarbonyP'' and the epidemiologic and laboratory evi-dence implicating certain inhaled or injected nickelcompounds as potential carcinogens.^^ Topical nickelexposures are frequently associated with allergic con-tact dermatitis, especially from costume jewelry andother metal objects.^^
CONCLUSIONS
In the present study, there is a statistically signiflcantdifference between the mean serum nickel concentra-tions in patients with psoriasis and in control subjects(P = 0.019). These higher nickel concentrations in thepsoriatic group could point to a defective cellulartransport mechanism or a defective nickel-dependentmetalloenzyme that may result in a compensatory in-crease in nickel absorption/retention. This suggeststhat a biochemical defect in the psoriatic process couldbe related to nickel homeostasis or function in thebody. These findings point the way to further studiesthat are ongoing at present.
Acknowledgments: Dr. Vincent Barranco, Dr. George Moore,and Lisa Marshall reviewed the document. Dr. John Savoryand Mr. Jitn Nicholson of the University of Virginia assistedwith the serum nickel analysis.
784
Elevated Serum Nickel in PsoriasisSmith, Aamir, and Otis
REFERENCES
1. Roenigk H Jr. Skin manifestations of psoriasis. In:Roenigk H Jr, Maibach H, eds. Psoriasis. 2nd Ed. NewYork: Marcel Dekker, 1991:3.
2. Zackheim HS, Wolf P. Serum copper in psoriasis andother dermatoses. J Invest Dermatol 1972; 58:28-32.
3. Hinks LJ, Young S, Clayton B. Trace element status ineczema and psoriasis. Clin Exp Dermatol 1987; 12:93-97.
4. Donadini A, Fiora C, Regazzini R, et al. Selenium plas-ma levels in psoriasis. Clin Exp Dermatol 1992; 17:214-216.
5. Voorhees JJ, Chokrabarti SG, Botero F, et al. Zinc ther-apy and distribution in psoriasis. Arch Dermatol 1969;100:669-673.
6. Fine J, Moschella S. Diseases of nutrition and metabo-lism. In: Moschella S, Hurley H, eds. Dermatology. 2ndEd. Philadelphia: WB Saunders, 1985: 1438.
7. Parodi A, Priano L, Rebora A. Chronic zinc deficiencyin a patient with psoriasis and alcoholic liver cirrhosis.IntJ Dermatol 1991; 30:45-47.
8. Anke M, Groppel B, Kronemann H, Grtin M. Nickel:an essential element. In: Sunderman FW Jr, Aitio A,Berlin A, et al, eds. Nickel in the human environment.IARC Scientific Publications No. 53. Oxford: OxfordUniversity Press, 1984:339.
9. Sunderman FW Jr. Nickel. In: Seiler HG, Sigel H, eds.Handbook on toxicity of inorganic compounds. NewYork: Marcel Dekker, 1988:453.
10. Sunderman FW. Analytical biochemistry of nickel. PureAppI Chem 1980; 52:527-544.
11. Fidarov AA. Nickel and cobalt levels in blood serum ofpsoriatic patients. Vestn Dermatol Venereol 1968; 42:46-48.
12. Donadini A, Pazzaglia A, Desirello G, et al. Plasma lev-els of zinc, copper and nickel in healthy controls and inpsoriatic patients. Acta Vitaminol Enzymol 1980; 2:9-16.
13. Spruit D, Bongaarts PJM. Nickel content of plasma,urine and hair in contact dermatitis. Dermatologica1977; 154:291-300.
14. McNeely MD, Nechay MW, Sunderman FW Jr. Mea-surements of nickel in serum and urine as indices of en-vironmental exposure to nickel. Clin Chem 1972; 18:992-995.
15. Nielsen FH. Is nickel nutritionally important? NutrToday 1993; 28:14-19.
16. Solomons NW, Viteri F, Shuler TR, Nielsen FH.Bioavailability of nickel in man: effects of foods andchemically defined dietary constituents on the absorp-tion of inorganic nickel. J Nutr 1982; 112:39-50.
17. Kaaber K, Menne T, Tjell JC, Veien N. Antabuse®treatment of nickel dermatitis. Chelation—a new prin-ciple in the treatment of nickel dermatitis. Contact Der-matitis 1979; 5:221-228.
18. Kaaber K, Veien NK, Tjell JG. Low nickel diet in thetreatment of patients with chronic nickel dermatitis. BrJ Dermatol 1978; 98:197-201.
19. McNeely MD, Sunderman FW, Nechay MW, Levine H.Abnormal concentrations of nickel in serum in cases ofmyocardial infarction, stroke, burns, hepatic cirrhosis,and uremia. Clin Chem 1971; 17:1123-1128.
20. Santucci B, Manna F, Christaudo A, et al. Serum con-centrations of nickel-sensitive patients after prolongedoral administration. Contact Dermatitis 1990; 22:253-256.
21. Nielsen FH. Possible future implications of nickel, ar-senic, silicon, vanadium, and other ultratrace elementsin human nutrition. In: Prasad AS, ed. Clinical, bio-chemical and nutritional aspects of trace elements. NewYork: Alan R. Liss, 1982:379.
22. Nielsen FH. Nutritional requirements for boron, sili-con, vanadium, nickel, and arsenic: current knowledgeand speculation. FASEB J 1991; 5:2661-2667.
23. Nielsen FH, Shuler TR, McLeod TG, Zimmerman TJ.Nickel influences iron metabolism through physiologic,pharmacologic and toxicologic mechanisms in the rat. JNutr 1984; 116:1280-1288.
24. Nielsen FH. Possible functions and medical significanceof the abstruse trace metals. In: Martell AE, ed. Inor-ganic chemistry in biology and medicine. Washington,DC: American Chemical Society, 1980:23.
25. Spears JW, Hatfield EE, Forbes RM. Nickel-copper in-terrelationship in the rat. Proc Soc Exp Biol Med 1977;156:140-143.
26. Spears JW, Hatfield EE, Forbes RM. Interrelationshipbetween nickel and zinc in the rat. J Nutr 1978; 108:307-312.
27. Simpson JY. Notes on the therapeutic action of fur-furine, nickel etc. In: Priestly WO, Storer HR, eds. Ob-stetric memoirs and contributions of James Y. Simpson.Edinburgh: A & C Black, 1855-56:270.
28. Palmer JD. Sulphate of nickel in neuralgia. Richmond&c Louisville Med J 1868; 5:270-271.
29. Leaman R. Some clinical observations on the therapeu-tic uses of bromide of nickel. Med News 1885; 46:427-429.
30. DaCosta JM. Observations on the salts of nickel, espe-cially the bromide of nickel. Med News 1883; 43:337-338.
31. Coogan TP, Latta DM, Snow ET, Costa M. Toxicity andcarcinogenicity of nickel compounds. GRC Crit RevToxicol 1989; 19:361-384.
32. U.S. Environmental Protection Agency (EPA). Healthassessment document for nickel and nickel compounds.EPA/600/8-83/012FF. Boca Raton, FL: GRG Press,1986.
33. Maibach H, Menne T, eds. Nickel and the skin: im-munology and toxicology. Boca Raton: CRC Press, 1989.
34. Sunderman FW, Kincaid JF. Nickel poisoning. JAMA1954; 155:889-894.
785












![[PPT]PowerPoint Presentation · Web viewSerum Lipase CBC Increased Hb Thrombocytosis Leukocytosis Liver Function Test Serum Bilirubin elevated Alkaline Phosphatase elevated Aspartate](https://img.pdfslide.us/doc/110x75/5acf74047f8b9a1d328d07bc/pptpowerpoint-viewserum-lipase-cbc-increased-hb-thrombocytosis-leukocytosis-liver.jpg)

















