Embed Size (px)
Citation preview

Sertraline Use in Pediatric Population:A Risk Benefit Discussion
Sertraline Use in Pediatric Population:A Risk Benefit Discussion
Steven J. Romano, MD
September 13, 2004
Steven J. Romano, MD
September 13, 2004
Joint Meeting of the CDER Psychopharmacology Drugs Advisory Committee and the FDA
Pediatric Advisory Committee
Joint Meeting of the CDER Psychopharmacology Drugs Advisory Committee and the FDA
Pediatric Advisory Committee

Points to Consider in Assessmentof Risk BenefitPoints to Consider in Assessmentof Risk Benefit
MDD is a serious illness that affects many children and adolescents in the US and is associated with suicidal behavior
Physicians have limited approved treatment options for pediatric patients with MDD
The risk/benefit of antidepressant use in pediatric depression should be assessed on an individual product basis• Antidepressants differ with regard to chemical structure,
pharmacological profile, pharmacokinetics, adverse events and discontinuation symptom profile
• Results of the studies reviewed in FDA analysis vary
Approaching this issue as a class effect might jeopardize beneficial treatments for children and adolescents with MDD
MDD is a serious illness that affects many children and adolescents in the US and is associated with suicidal behavior
Physicians have limited approved treatment options for pediatric patients with MDD
The risk/benefit of antidepressant use in pediatric depression should be assessed on an individual product basis• Antidepressants differ with regard to chemical structure,
pharmacological profile, pharmacokinetics, adverse events and discontinuation symptom profile
• Results of the studies reviewed in FDA analysis vary
Approaching this issue as a class effect might jeopardize beneficial treatments for children and adolescents with MDD

Suicide-Related Behavior and MDD in the Pediatric PopulationSuicide-Related Behavior and MDD in the Pediatric Population
Suicide is the third leading cause of death in adolescents 15-19 years old1
Annual prevalence of MDD2
• Children (8-12): 2-3%• Adolescents (11/12-18): Up to 8%
Diagnostic criteria (DSM IV-R) includes recurrent thoughts of death, suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide
Suicidality in depressed children and adolescents at time of study entry3
• Suicide attempts: 9%• Suicidal ideation: 66%
Suicide is the third leading cause of death in adolescents 15-19 years old1
Annual prevalence of MDD2
• Children (8-12): 2-3%• Adolescents (11/12-18): Up to 8%
Diagnostic criteria (DSM IV-R) includes recurrent thoughts of death, suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide
Suicidality in depressed children and adolescents at time of study entry3
• Suicide attempts: 9%• Suicidal ideation: 66%
1Anderson RN. Deaths: leading causes for 2000. Natl Vital Stat Rep. 2002; 50:1-852American Academy of Child and Adolescent Psychiatry (1998), Practice Parameters for the Assessment and Treatment of Children and Adolescents with Depressive Disorders. J Amer Acad Child Adolesc Psychiatry 37 (10 suppl);3Kovacs et al. Suicidal behaviors and childhood-onset depressive disorders: a longitudinal investigation. J Amer Acad Child Adolesc Psychiatry 1993; 32 (1): 8-20

Pfizer Sponsored Placebo-Controlled* Pediatric Studies with SertralinePfizer Sponsored Placebo-Controlled* Pediatric Studies with Sertraline
Ongoing, Blinded Ongoing, Blinded
9292
9797
9292
SertralineSertraline
A0501033*** A0501033*** OCD Ongoing, Blinded 38 Weeks 6-17OCD Ongoing, Blinded 38 Weeks 6-17
6-176-1710 Weeks10 WeeksPTSDPTSDA0501061**A0501061**
6-176-1710 Weeks10 Weeks9393MDDMDDA0501017A050101722
6-176-1710 Weeks10 Weeks9191MDDMDDA0501001A050100122
6-176-1712 Weeks12 Weeks9595OCDOCD90-CE21-049890-CE21-049811
PlaceboPlacebo
Age Range (Yrs)Age Range (Yrs)Treatment Treatment DurationDurationNumber of SubjectsNumber of SubjectsIndicationIndicationStudy NumberStudy Number
*Pfizer performed 6 additional uncontrolled studies with sertraline in pediatric population which are published or being submitted for publication**A total of 75 patients have been enrolled to date***A total of 24 patients have been enrolled to date
1March JS et al., JAMA 1998; 280 (20): 1752-17562Wagner KD et al., JAMA 2003; 290 (8): 1033-1041 (pooled analysis of 2 studies)

Placebo-Controlled Pediatric OCD Study with Sertraline – Primary Efficacy Results Placebo-Controlled Pediatric OCD Study with Sertraline – Primary Efficacy Results
-9
-8
-7
-6
-5
-4
-3
-2
-1
0
Baseline Week 1 Week 2 Week 4 Week 6 Week 8 Week 10 Week 12 End
Sertraline (N=92) Placebo (N=95)
-9
-8
-7
-6
-5
-4
-3
-2
-1
0
Baseline Week 1 Week 2 Week 4 Week 6 Week 8 Week 10 Week 12 End
Sertraline (N=92) Placebo (N=95)
CY
-BO
CS
Ch
an
ge
Sco
reC
Y-B
OC
S C
ha
ng
e S
core
*p= < 0.05March JS et al., JAMA 1998; 280 (20): 1752-1756
**
**
**
****
**
CY-BOCS: Children’s Yale-Brown Obsessive Compulsive Scale Baseline score = 23CY-BOCS: Children’s Yale-Brown Obsessive Compulsive Scale Baseline score = 23

Placebo-Controlled Pediatric MDD Studies with Sertraline – CDRS-R ResultsPlacebo-Controlled Pediatric MDD Studies with Sertraline – CDRS-R Results
SertralineSertraline PlaceboPlacebo P-ValueP-Value
Study A0501001Study A0501001 N=N= 9393 8888
CDRS-R: Baseline CDRS-R: Baseline Endpoint Endpoint 64.2 64.2 38.1 38.1 63.8 63.8 41.9 41.9 0.080.08
CDRS-R: Responders, %CDRS-R: Responders, % 62.4%62.4% 56.8%56.8% 0.460.46
Study A0501017Study A0501017 N=N= 9292 9191
CDRS-R: Baseline CDRS-R: Baseline Endpoint Endpoint 64.4 64.4 36.1 36.1 65.4 65.4 39.3 39.3 0.170.17
CDRS-R: Responders, %CDRS-R: Responders, % 75.0%75.0% 60.4%60.4% 0.030.03
Pooled Study Data (A0501001+A0501017)Pooled Study Data (A0501001+A0501017)11 N=N= 185185 179179
CDRS-R: Baseline CDRS-R: Baseline Endpoint Endpoint 64.3 64.3 37.1 37.1 64.6 64.6 40.6 40.6 0.030.03
CDRS-R: Responders, %CDRS-R: Responders, % 68.7%68.7% 58.7%58.7% 0.050.05
Primary analysis: Change from baseline in CDRS-R total score at endpoint (LOCF)CDRS-R Responders: ≥ 40% decrease on CDRS total score from baselineANCOVA for CDRS-R change from baseline to LOCF endpoint; CMH test for responder rate
1Wagner KD et al., JAMA 2003; 290 (8): 1033-1041 (pooled analysis of 2 studies)
CDRS-R: Children’s Depression Rating Scale – RevisedCDRS-R: Children’s Depression Rating Scale – Revised

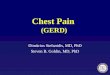
72.6
65.366.7
51.1
0
10
20
30
40
50
60
70
80
Children (age 6-11) n = 171 Adolescents (age 12-17) n=193
Sertraline Placebo
72.6
65.366.7
51.1
0
10
20
30
40
50
60
70
80
Children (age 6-11) n = 171 Adolescents (age 12-17) n=193
Sertraline Placebo
Placebo-Controlled Pediatric MDD Studies with Sertraline – CDRS-R Response Rates in Children vs AdolescentsPlacebo-Controlled Pediatric MDD Studies with Sertraline – CDRS-R Response Rates in Children vs Adolescents
*p<0.05Response rate defined as a ≥40% decrease on CDRS total score from baseline
CDRS-R response rates (%)CDRS-R response rates (%)
**
84 87 101 92

Placebo-Controlled Pediatric MDD Studies with Sertraline – CDRS-R Item 13 (“Suicidal Ideation”) Placebo-Controlled Pediatric MDD Studies with Sertraline – CDRS-R Item 13 (“Suicidal Ideation”)
1.0
1.2
1.4
1.6
1.8
2.0
Baseline Week 1 Week 2 Week 3 Week 4 Week 6 Week 8 Week 10
Sertraline (N=188) Placebo (N=182)
1.0
1.2
1.4
1.6
1.8
2.0
Baseline Week 1 Week 2 Week 3 Week 4 Week 6 Week 8 Week 10
Sertraline (N=188) Placebo (N=182)
Suicidal Ideation Mean score from Baseline to Endpoint(LOCF)
Suicidal Ideation Mean score from Baseline to Endpoint(LOCF)
CD
RS
-R T
ota
l Sc
ore
CD
RS
-R T
ota
l Sc
ore

Placebo-Controlled Pediatric Studies with SertralinePlacebo-Controlled Pediatric Studies with Sertraline
SertralineSertraline PlaceboPlacebo
DiagnosisDiagnosis n/Nn/N Incidence % Incidence % [95% CI][95% CI] n/Nn/N Incidence % Incidence %
[95% CI][95% CI]
MDDMDD 2/1892/189 1.1 1.1 [[0.1-3.80.1-3.8]]
2/1842/184 1.1 1.1 [[0.1-3.90.1-3.9]]
OCDOCD 0/920/92 0 0 [[0-3.210-3.21]]
0/950/95 0 0 [[0-3.100-3.10]]
CombinedCombined 2/2812/281 0.7 0.7 [[0.1-2.60.1-2.6]]
2/2792/279 0.7 0.7 [[0.1-2.60.1-2.6]]
Suicide AttemptsSuicide Attempts
FDA analysis is consistent with Pfizer analysis; no new cases of suicide-related behavior identified by Columbia University FDA review compared to Pfizer’s submissions

Placebo-Controlled Pediatric Studies with Sertraline Placebo-Controlled Pediatric Studies with Sertraline
SertralineSertraline PlaceboPlacebo
Diagnosis/Diagnosis/StudyStudy n/Nn/N Incidence % Incidence %
[[95% CI95% CI]]n/Nn/N Incidence % Incidence %
[[95% CI95% CI]]
MDDMDD 3/1893/189 1.6 1.6 [[0.33-4.570.33-4.57]]
0/1840/184 00[0-1.61][0-1.61]
OCDOCD 0/920/92 0 0 [[0-3.210-3.21]]
1/951/95 1.1 1.1 [[0.03-5.730.03-5.73]]
CombinedCombined 3/2813/281 1.1 1.1 [[0.22-3.090.22-3.09]]
1/2791/279 0.4 0.4 [[0.01-1.980.01-1.98]]
Suicidal IdeationSuicidal Ideation
FDA analysis is consistent with Pfizer analysis; no new cases of suicide-related behavior identified by Columbia University / FDA review compared to Pfizer’s submissions

Placebo-Controlled Pediatric Studies with Sertraline – Timing of EventsPlacebo-Controlled Pediatric Studies with Sertraline – Timing of Events
Patient ID Age, Sex SA/SI Day of event
Sertraline
2006 12, M SI 49
1089 10, F SI 35
1022 11, M SI 21
4022 16, F SA 50
3095 6, M SA 34
Placebo
4329 17, F SA 9
4321 15, F SA x 2 63, 66
19 (OCD) 6, F SI 12
No specific pattern in time of event
No association between time of event and dose increases
Most events associated with immediate psychosocial precipitant
No specific pattern in time of event
No association between time of event and dose increases
Most events associated with immediate psychosocial precipitant

Placebo-Controlled Pediatric Studies with Sertraline – SummaryPlacebo-Controlled Pediatric Studies with Sertraline – Summary
Sertraline is effective and safe in the treatment of pediatric OCD
The a-priori pooled analysis of the sertraline clinical studies in pediatric MDD demonstrated a statistically significant effect on CDRS-R• Benefit relative to placebo was modest due to a high placebo response,
primarily in children
There were no suicides in any pediatric study with sertraline
No statistically significant difference between sertraline and placebo in placebo-controlled studies of MDD or OCD with respect to:• Suicide attempts (2 patients/2 attempts in sertraline and
2 patients/3 attempts in placebo group)• Suicidal ideation (3 patients in sertraline, 1 in placebo)
No temporal association between onset of double-blind treatment or dose increases and suicide-related events
Sertraline is effective and safe in the treatment of pediatric OCD
The a-priori pooled analysis of the sertraline clinical studies in pediatric MDD demonstrated a statistically significant effect on CDRS-R• Benefit relative to placebo was modest due to a high placebo response,
primarily in children
There were no suicides in any pediatric study with sertraline
No statistically significant difference between sertraline and placebo in placebo-controlled studies of MDD or OCD with respect to:• Suicide attempts (2 patients/2 attempts in sertraline and
2 patients/3 attempts in placebo group)• Suicidal ideation (3 patients in sertraline, 1 in placebo)
No temporal association between onset of double-blind treatment or dose increases and suicide-related events

Points to Consider in Assessmentof Risk BenefitPoints to Consider in Assessmentof Risk Benefit
MDD is a serious illness that affects many children and adolescents in the US and is associated with suicidal behavior
Physicians have limited approved treatment options for pediatric patients with MDD
The risk/benefit of antidepressant use in pediatric depression should be assessed on an individual product basis• Antidepressants differ with regard to chemical structure,
pharmacological profile, pharmacokinetics, adverse events and discontinuation symptom profile
• Results of the studies reviewed in FDA analysis vary
Approaching this issue as a class effect might jeopardize beneficial treatments for children and adolescents with MDD
MDD is a serious illness that affects many children and adolescents in the US and is associated with suicidal behavior
Physicians have limited approved treatment options for pediatric patients with MDD
The risk/benefit of antidepressant use in pediatric depression should be assessed on an individual product basis• Antidepressants differ with regard to chemical structure,
pharmacological profile, pharmacokinetics, adverse events and discontinuation symptom profile
• Results of the studies reviewed in FDA analysis vary
Approaching this issue as a class effect might jeopardize beneficial treatments for children and adolescents with MDD

Pfizer’s PositionPfizer’s Position
Current class labeling for monitoring during treatment with antidepressants accurately reflects the risk of suicidality in adult and pediatric patients• Such labeling should be applied to all medications indicated for
the treatment of depression and not just SSRIs/SNRIs
If the FDA considers a label change is necessary, product specific labeling would be most beneficial to prescribers and patients• Inclusion of specific event rates of suicide-related behavior for
the placebo-controlled clinical trials in the Adverse Event section of the Label
Current class labeling for monitoring during treatment with antidepressants accurately reflects the risk of suicidality in adult and pediatric patients• Such labeling should be applied to all medications indicated for
the treatment of depression and not just SSRIs/SNRIs
If the FDA considers a label change is necessary, product specific labeling would be most beneficial to prescribers and patients• Inclusion of specific event rates of suicide-related behavior for
the placebo-controlled clinical trials in the Adverse Event section of the Label