Embed Size (px)
Citation preview

APPROACH TO A PATIENT WITH SUSPECTED KIDNEY DISEASEELIZABETH ROMANO-SEBASTIAN MD FPCP FPSN

A 28 yo female came to your clinic for bi pedal edema of 2 weeks duration. PE showed puffy eyelids, pale conjunctiva, + friction rub, decrease breath sounds and Gr 2 pedal edema. She denies any intake of any meds.

Creatinine
2.4 mg/dl

ELECTROLYTES
Na – 138
K – 5.5
iCal – 4.8
Phos – 3

URINALYSIS

ColorNormal:
pale to dark depending on the concentration of the urine.
Pathologic conditions:
gross hematuria
hemoglobinuria
myoglobinuria (pink, red, brown or black) ;
jaundice (dark yellow to brown);
chyluria (white,milky)
massive uric acid crystalluria (pink)
Drugs:
rifampin (yellow-orange to red; phenytoin (red), nitrofurantoin (brown);
metronidazole, imipinem, methyldopa (darkening on standing)

Odor
Pungent UTI due to production of ammonia)
Sweet ketones
Musty pku

Turbidity
Usually transparent but can be due to inc concentration of any particle

FOAM
Indicates the amount of protein in the urine

Chemical Analysis Dipstick
pH
Hemoglobin
Glucose
Albumin
Leukocyte esterase
Nitrates
Bilirubin
Specific gravity

pH
presence of H+ ions due to the secretion of acid in the collecting ductlow ph:
metabolic acidosis, high protein meals, (generate more acid and ammonia) and with volume depletion- aldosterone is stimulated resulting in acidic urine)
high ph:RTA, vegetable diets, infection with urease + like proteus)
Range: 5-8.5

Hemoglobin
Pseudoperoxidase activity of the heme moiety of Hgb, which catalyzes peroxide and chromagen ---colored product
False positive: hemoglobinuria from intravascular hemolysismyoglobinuria from rhabdomyolysishigh concentration of bacteria with enterobacter staphylococci, strep
False negative: ascorbic acid

RBC- Hematuria – blood in the urineDifferentiated by centrifugation

Glycosuria
Used for testingMultistix – glucose oxodase reaction
Clinitest – modified Benedict’s test for reducing substances
Types of glycosuriaOverflow glycosuria – above 180mg/dl
Renal glycosuria – associated with Fanconi Syndrome

ProteinPhysiologic
Daily production – 40-150 mg/day40% albumin, 40% tissue, 15% Ig and fragments, 5% other plasma proteins 150 mg/24 hrs adults, 140 mg/m2 in childrenMethod is sensitive to albumin
First morning Random protein crea ratio (same time for follow-up)
Types of ProteinuriaOverflow – contains Bence-Jones proteins, myoglobin, HgbGlomerular permeability
Selective - albuminNon-selective
Tubular – decrease reabsorption of filtered protein; caused by antibiotics, heavy metalsHemodynamic – caused by CHF, heat, seizures, exercise

Parameter False Positive False Negative
Specific Gravity Reduced when in the presence of glucose, urine pH>6.5
Increased when in the presence of keto acids,
protein >7g/L
pH Reduced when in the presence of formaldehyde
Hemoglobin Ascorbic acid, delayed examination, high density of
urine, formaldehyde (>0.5 g/L)
Myoglobin, microbial peroxidise, oxidizing agent,
HCl
Glucose Ascorbic acid, bacteria Oxidizing detergents, HCl
Albumin Ig light chains, tubular proteinuria, globulins,
abnormally colored urine, HCl
Urine pH >9, quaternary ammonium detergents,
chlorhexidines, polyvinylpyrolidone
Leukocyte esterase High density of urine, high Vitamin C intake, protein >5g/L , glucose >20g/L,
cephalosporin,
Oxidizing detergents, formaldehyde (>0.4 g/L), sodium azide, abnormally colored urine due to beet
Nitrites No vegetables in diet, short bladder incubation time,
vitamin C, bacteria that do not reduce nitrates to nitrites
Abnormally colored urine

Microscopic Examination
Sediment OverviewTechnique for preparation and examinationMorning specimen is the most concentratedCentrifugation done in a conical tube for 3 to 5 minutes at 3000-5000 rpm Pipetting
Decant supernatant liquidPipette while invertedAspirate buttonMay resuspend if too thick
Cover slip: avoid bubbles, examine periphery for formed elements

ExaminationScan entire entire field at low power
Magnify selected areas
Stop down diaphragm or move light source for contrast
Stain if necessary

Microscopic Formed elementsCellular elements
WBC- easiest to find due to granular cytoplasm and lobulated nucleus
Marker for upper or lower tract infections
In women may be found as contaminant
May also be GN, Interstitial nephritis

RBCChanging the focus, causes red cells to appear as black tires, appear concave
NormalDysmorphic RBC’sCrenated RBC- occurs in hypertonic urineAcanthocytes- doughnut-like with blebs (mickey mouse ears)Discocyte→echinocytes→stomatocyte- transition inducible in changes in pH, osmolality and protein concentrations

Casts
Can only come from the tubules
Primarily Tamm- Horsfall mucoprotein
Secreted in TAL as monomers
Polymerized into casts in distal tubules and collecting ducts
Incorpotate material that is within the tubules
Favored by low flow rates, low pH, high luminal Na
Larger casts from larger tubules especially with decreased flows

Hyaline cast
Fine granular cast

Broad coarsely granular cast
Fatty cast
Waxy cast

Acute Tubular Necrosis

RBC Cast-
indicative of Glomerular injury

White Blood cell castAcute interstitial nephritis,
acute pyelonephritis, proliferative glomerulonephritis

Casts Main Clinical association
Hyaline Normal subject and renal disease
Hyaline granule Normal subject and renal disease
Granular Renal disease
Waxy Renal insufficiency and rapidly progressing renal disease
Fatty Marked proteinuria, nephritic syndrome
Erythrocyte Glomerular bleeding, proliferating/ necrotizing glomerulonephritis
Hemoglobin Same as erythrocytic cast + hemoglobinuria
Leukocyte Acute interstitial nephritis, acute pyelonephritis, proliferative glomerulonephritis
Epithelial Acute tubular necrosis, acute interstitial nephritis, glomerulonephritis
Myoglobin Rhabdomyolysis
Bacteria/ Fungi Bacterial/ fungal infection in kidney

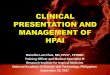
pH 6
Sg 1.02
Protein ++++
RBC 8/hpf
WBC 9/hpf
Epithelial cells many
RBC casts, fine granular casts

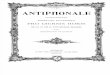
USG
Size
Cortical thickness
Echogenicity
Calyxes
Ureter
Normal sized kidneys with hypoechoic parenchyma

54 yo male known hypertensive, known diabetic admitted for decreasing urine output

A 32 yo male known to have a solitary functioning R kidney came in for R flank pain radiating to the R testicle with no urine output for the past 8 hours

TAKE HOME MESSAGESHistory and PE will determine the type of exams to be requested
In approaching a patient with elevated creatinine, the first step is to differentiate acute from chronic kidney disease
Trend of creatinine more important than a single determination
Proper collection of urine must be emphasized to a patient
Be systematic in interpreting laboratory results.