Embed Size (px)
Citation preview

Poster Print Size: This poster template is 44” high by 44” wide. It can be used to print any poster with a 1:1 aspect ratio.
Placeholders: The various elements included in this poster are ones we often see in medical, research, and scientific posters. Feel free to edit, move, add, and delete items, or change the layout to suit your needs. Always check with your conference organizer for specific requirements.
Image Quality: You can place digital photos or logo art in your poster file by selecting the Insert, Picture command, or by using standard copy & paste. For best results, all graphic elements should be at least 150-200 pixels per inch in their final printed size. For instance, a 1600 x 1200 pixel photo will usually look fine up to 8“-10” wide on your printed poster.
To preview the print quality of images, select a magnification of 100% when previewing your poster. This will give you a good idea of what it will look like in print. If you are laying out a large poster and using half-scale dimensions, be sure to preview your graphics at 200% to see them at their final printed size.
Please note that graphics from websites (such as the logo on your hospital's or university's home page) will only be 72dpi and not suitable for printing.
[This sidebar area does not print.]
Change Color Theme: This template is designed to use the built-in color themes in the newer versions of PowerPoint.
To change the color theme, select the Design tab, then select the Colors drop-down list.
The default color theme for this template is “Office”, so you can always return to that after trying some of the alternatives.
Printing Your Poster: Once your poster file is ready, visit www.genigraphics.com to order a high-quality, affordable poster print. Every order receives a free design review and we can deliver as fast as next business day within the US and Canada.
Genigraphics® has been producing output from PowerPoint® longer than anyone in the industry; dating back to when we helped Microsoft® design the PowerPoint® software.
US and Canada: 1-800-790-4001
Email: [email protected]
[This sidebar area does not print.]
The Global Tracheostomy Collaborative (GTC) Impact of a Quality Improvement Collaborative in Otolaryngology – Head & Neck Surgery
Karen Watters 1,2,3; Hannah Zhu1,4 Michael Brenner1,5; Tanis Cameron1,6; Anthony Narula1,7; David Roberson1,2,3 ; Rahul Shah1,8
1The Global Tracheostomy Collaborative, 2Boston Children’s Hospital, Boston , USA; 3Department of Otology and Laryngology, Harvard Medical School, Boston, USA; 4 King’s College Hospital NHS Foundation Trust, London, UK; 5Department of Otolaryngology, University of Michigan School of Medicine, Michigan, USA ; 6Tracheostomy Review and Management Service, Austin Health, Melbourne, Australia; 7ENT Department St. Mary’s Hospital NHS T, London, UK;
8Children’s National Medical Center, Washington, DC, USA. .
Karen Watters, MB BCH BAO, MPH Boston Children’s Hospital Email: [email protected]
Contact
References
Objective: The Global Tracheostomy Collaborative (GTC), established in 2013, is an international
multidisciplinary Quality Improvement (QI) collaborative established to improve processes and
outcomes in adult and pediatric tracheostomy care (www.globaltrach.org). The aim of this study is
to evaluate the initial effectiveness of such a collaborative in Otolaryngology – Head & Neck Surgery.
Study Design: Observational. Qualitative Interviews.
Methods: Analysis of GTC membership and attendance at three international kickoff meetings was
performed. Qualitative interviews were conducted either face-to-face or via telephone with care
teams from GTC member hospitals.
Results: 570 individuals representing 125 institutions attended kickoff meetings in Boston (April
2014), London (July 2014) and Melbourne (October 2014); 1000 additional individuals from more
than 20 countries and all continents except Africa attended a kickoff meeting using virtual
technology. Attendees were from a range of disciplines; otolaryngology, anesthesia, neonatology,
pulmonary, critical care, respiratory therapy/physiotherapy, nursing, speech pathology, and hospital
management. As of October 2014, over 35 hospitals in the United States, United Kingdom, Sweden,
Singapore, Qatar, and Australia have joined, and another 7 hospitals are considering
joining. Preliminary data collection has been successful with >380 new tracheostomy cases entered
in an international, HIPPA-compliant REDCap database within the first 6 months of launch.
Qualitative interviews reveal that many sites have instituted new practices in response to joining.
Conclusion: It is widely recognized that there is a need to improve the speed at which successful
care models disseminate. Quality Improvement collaboratives have been successful at accelerating
improvement in many disciplines. The GTC may be an exemplar of this new methodology in
Otolaryngology.
Abstract
GTC Timeline shown in Figure 1.
Kick-Off Meetings:
• 570 individuals from over 125 institutions attended GTC kick-off
meeting in Boston (April 2014), London (July 2014) or Melbourne
(October 2014)
• 1,000 individuals from 20 countries attended via live webcast
• Disciplines represented - anesthesia, critical care, pulmonary,
respiratory care, physiotherapy, speech therapy, nursing, social work,
quality/safety, family/patient and hospital management
• 3 webinars and online discussion groups held.
Membership:
• First member hospital enrolled in January 2014
• 35 hospitals have joined (UK, Sweden, United States, Singapore,
Qatar, and Australia)
• 75 hospitals preparing to join
Data Collection:
• Data entry went live in August 2014, HIPPA-compliant database
• >380 new tracheostomy cases has been entered
Member Hospital Interviews:
• Interviews with 16 member sites to identify deficiencies and new
practices in tracheostomy care
Reasons cited for joining;
• Desire to learn from others and share experiences (88%)
• Need to standardize care (69%)
• Need support for change initiatives (56%)
• Need for maintenance of staff education (50%)
• Recent adverse tracheostomy events (>50%)
• Need to create a Multi-Disciplinary Tracheostomy (MDT) program
56% of interviewed hospitals do not have a MDT program
New tracheostomy practices planned/instituted:
• Weekly MDT ward rounds
• Standardization of protocols
• Mandatory training modules for staff and families
• Improved discharge planning
• Improved patient/family feedback with “Family Tracheostomy Days”
• All member hospitals reported a staff commitment to work for change
Background
• Analysis of GTC membership and attendance at 3 international
kickoff meetings.
• Qualitative interviews with 16 GTC member hospitals from 3 continents.
Methods
• Tracheostomy care is high risk with significant morbidity and
mortality.1
• Patients and families with tracheostomy experience extremely
disorganized, fragmented care.
• The Global Tracheostomy Collaborative (GTC), 2013, is an
international multidisciplinary Quality Improvement Collaborative
(QIC) initiated to improve patient outcomes in tracheostomy care.
THE GTC WORKS THROUGH 5 KEY DRIVERS;
1. Coordinated Multidisciplinary Tracheostomy Care Team
2. Coordinated interdisciplinary staff education
3. Institution-Wide Interdisciplinary Tracheostomy Protocols
4. Patient and Family centered Tracheostomy Care
5. Create outcome-based metrics and gather data using a HIPAA-
compliant database
• Exemplar institutions have demonstrated that care can be
dramatically improved and tracheostomy related adverse events
radically reduced through integrated tracheostomy care teams (Table
1, 2).2, 3
• GTC is the first international Quality Improvement Collaborative in
Otolaryngology -- Head & Neck Surgery
• GTC has received a robust international response, reflecting the
global need for improving tracheostomy care
• Membership of GTC offers the opportunity to standardize
tracheostomy processes and improve outcomes
• Qualitative interviews have shown very favorable feedback and that
the program makes a positive difference for patients and families
Conclusions Results
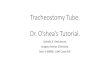
SeriousTracheostomyClinicalIncidents
27%
20%
10% 10%
4% 0%0
5
10
15
20
25
30
2003/4 2004/5 2005/6 2006/7 2007/8 2008/9
Year
Pro
po
rtio
n O
f S
evere
Clin
ical In
cid
en
ts
CareBundleintroduced
TracheostomyMul disciplinaryWardRound
Auditini ated
St.Mary’sHospital,London;usedbypermission
Improvingtracheostomymanagementthroughdesign,implementa onandprospec veauditofacarebundle:howwedoit.He geR,etal.ClinOtolaryngol.2008Oct;33(5):488-91.
The Global Tracheostomy Collaborative has received unrestricted educational grants from Smiths Medical, Boston Medical, and Boston Children's Hospital Department of Otolaryngology.
This poster has been submitted on behalf of all the members of the Steering Committee of the Global
Tracheostomy Collaborative: Asit Arora, Jo Harrison, Linda L Morris, Neil Bateman, Jay G Berry, Melissa
Ciardulli, Preety Das, Stacey Halum, Haytham Kubba, Christine Milano, Melody Paine, Alon Peltz, Rosh Sethi,
Margaret Skinner, Joanne Sweeney, Stephen Warrillow, Ralph Woodhouse, Hannah Zhu.
Financial Disclosure
1. Tracheotomy-Related Catastrophic Events: Results of a National Survey. Das P, Zhu H, Shah RK, Roberson DW, Berry J, et al. Laryngoscope, 122:30–37, 2012 . 2. Improving tracheostomy care: a prospective study of the multidisciplinary approach. Cetto R, Arora A, Hettige R, Nel M, Benjamin L, Gomez CM, Oldfield WL, Narula
AA. Clin Otolaryngol. 2011 Oct;36(5):482-8. 3. Outcomes of patients with spinal cord injury before and after introduction of an interdisciplinary tracheostomy team. Cameron TS, McKinstry A, Burt SK, Howard ME,
Bellomo R, Brown DJ, Ross JM, Sweeney JM, O’Donoghue FJ. Critical Care Resusc. 2009;11:14-19.
“Majority of patients are decannulated before discharge, but those who
aren’t are a major issue since we don’t have a procedure for what
happens on discharge with a trach. “
“The 2am test –making sure that at 2am there are staff who can sort out
problems with trachs,”
“Families don’t trust staff when kids are inpatient and stay 24-7 to provide
care for their child”
“nursing staff in certain areas of the hospital are still uncomfortable
taking care of tracheostomies”
“We constantly evaluate our services, have weekly meetings, have
streamlined our care coordination and discharge planning. For example,
we’re currently developing a protocol for discharging trach patients…
Table 2: Effect of Integrated Tracheostomy Bundle on Adverse Events
Table 1: Decrease in Critical Tracheostomy Events
Comments from Member Interviews