Embed Size (px)
Citation preview

TRACHEOSTOMY
DR NEEMU HAGE

DEFINITIONTracheotomy Greek origin: ‘tom’- ‘to cut’ the
trachea Surgical opening of the trachea
Tracheostomy Greek origin: ‘stom’- ‘mouth’ Creation of a stoma between
trachea and cervical skin

HISTORY1st known reference- rig veda dated
2000 BC.Ebers papyrus (dated 1550 BC)-
Egyptian medical papyrus mentions tracheotomy
Alexander the GreatAntyllus (2 AD), Greek surgeon- performed tracheostomies in oral surgeriesTracheotomy well documented in Indian and Arabian literature in middle ages.

Tracheostomy gained popularity in 1800s
Two methods: High- by dividing cricoid Low- trachea entered directlySignificant problems associated with
high methodTill the end of 19th century
tracheostomy considered hazardousChevalier Jackson in 1923
established principles of tracheostomy

PHYSIOLOGICAL EFFECTS
Reduction in
respiratory dead space
Laryngeal bypass
Nasociliary clearance
and humidificat
ion lostRedundant
area between
stoma and larynx
Disruption of normal
swallowing mechanism

INDICATIONSUpper airway obstruction Congenital Laryngeal web/cysts, B/L choanal atresia,
Tracheo-esophageal fistula, Craniofacial anomalies, Subglottic/tracheal stenosis
Infective Acute epiglottitis, Diphtheria, Acute layngotracheobronchitis, Ludwig’s angina
Trauma External injury to larynx/trachea, maxillofacial injury, corrosive injury, inhalational injury
Neoplasm Tumours of larynx, pharynx, tongue, upper trachea
Foreign Body
Foreign body lodged in larynx
Vocal cords B/L abductor paralysis, Bulbar palsy

Removal of secretions and protection of tracheobronchial tree from aspiration
Neurological diseases- GBS, MS, Bulbar palsy
Coma- head injury, poisoning, tumour
In such situations- laryngeal/pharyngeal incompetence
Cuffed tube useful

Respiratory failure Tracheostomy- dead space, effort
of breathing, alveolar ventilation Ease of removal of secretions Pulmonary diseases- exacerbation of
chronic bronchitis, emphysema, severe pneumonia
Neurological diseases- MS, Motor neuron disease
Severe chest injury- flail chest

Prolonged ventilation T-tube more secure than ET tube;
easier to wean off vent >3wks of intubation length of ventilation and hospital
stay
As a part of another procedure Temporary tracheostomy in head
and neck surgeries

TYPESTEMPORARY/PERMANENT:Temporary tracheostomy- elective or
emergencyPermanent tracheostomy-as part of
operation involving removal of larynx
HIGH/MID/LOW: High- above isthmus via 1st tracheal
ring Mid- through 2nd-3rd tracheal ring,
preferred Low- below level of isthmus

PREOPERATIVE ASSESSMENT
Informed consent Coagulation profile adequate,
platelet count >50000/cumm Neck examination- to anticipate
difficulties in procedure as in enlarged thyroid, limited neck extension.
T-tube arranged, checked and prepared

Surgical tracheostomyMinitracheostomy Paediatric tracheostomyPercutaneous dilatational
tracheostomy

SURGICAL TRACHEOSTOMY









COMPLICATIONS Immediate Haemorrhage Local injury-cricoid cartilage, 1st tracheal ring, carotid artery recurrent laryngeal nerveAir embolismApnoeaCardiac arrest

Intermediate (1st few hours or days) Secondary haemorrhage

Tube displacement Tube blockage Subcutaneous emphysema Pneumothorax

InfectionTracheal necrosisLate complicationsHaemorrhageGranuloma formationTracheo-oesophageal fistulaTracheo-cutaneous fistulaLaryngotracheal stenosisDifficult decannulationTracheostomy scar

MINITRACHEOSTOMY OR CRICOTHYROTOMY
Procedure for opening airway through cricothyroid membrane
Minitracheostomy kits commercially available

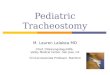
PAEDIATRIC TRACHEOSTOMY
Anatomy of paediatric upper airway different from adults
Age of child critical when deciding appropriate size of tube
Standard of paediatric intensive care facilities have improved in last 2 decades
Reduced rate of tracheostomy in paediatric population
Speech development may be impaired in long term tracheostomies

INDICATIONSUpper airway obtruction
Oropharynx, Tongue base
Macroglossia, Treacher Collins syndrome, Goldenhar syndrome, Cystic hygroma, Diphtheria
Nose, Nasopharynx
B/L choanal atresia
Supraglottis Supraglottic cyst, Acute Epiglottitis Glottis Vocal cord palsy, Laryngeal oedema,
Physical trauma, Juvenile respiratoty papillomatosis
Subglottis Subglottic stenosis, Hemangioma Trachea Acute laryngotracheobronchitis,
Tracheomalacia, Tracheal stenosis

Prolonged intubation Indicated for patients requiring long term
PPV such as- PT neonate, CNS disease, severe burns
Long term intubation leads to complications and difficult decannulation
>3 weeks of intubation
Pulmonary toilet For intractable aspiration- decreases dead
space and eases work of pulmonary toilet

ANATOMICAL CONSIDERATIONS IN PAEDIATRIC TRACHEOSTOMY
Structures lie higher up
Soft and compressible airway
Structures from superior mediastinum pulled up during extension of neck
Small tracheal lumen Trachea, a
developing structure Funnel shaped larynx
with narrowest part being subglottis

TECHNIQUE

TRACHEOSTOMY CARESuction Regular suctioning Frequency depends on individual basis Indications Appropriate size of Suction catheter Method

Humidification Upper respiratory tract
bypassed, conditioning of inspired gas lost
Different preferences in diffirent set ups
Types: -cold water humidifiers -hot water humidifiers
-heat and moisture exchangers
-stoma protector Nebulization

Tracheostomy tube change 1st tube change- 5-7 days Frequency of tube change- no
standard interval ‘if you can hear a tube, you should
change it’ Bougies or guidewires

Wound care

TYPES OF TRACHEOSTOMY TUBES
cuffed or uncuffed

Single or double lumen tubes

Adjustable flange long tubeSuction aid tracheostomy tube

Tracheostomy with speaking valve

Types of tubes based on material: PVC Silicone Siliconed PVC Silastic Silver Armoured Fullers tube

PERCUTANEOUS DILATATIONAL TRACHEOSTOMY
1st described by Shelden & Pudenz (1957) Tracheostomy: Indications & complications Contraindications: Absolute: -cervical injury -coagulopathy -emergency airway Relative : -short fat neck/obesity -enlarged thyroid -inability to extend neck (cervical injury/prior tracheostomy)

DECANNULATIONConsidered when original condition
requiring tracheostomy has improved
Approached in a step-wise manner In paediatric group endoscopic
assessment prior to decannulation essential
Fenestrated tube> occlusion cap> occlusion cap for 12 hrs > 24 hrs>decannulation

THANK YOU