Embed Size (px)
Citation preview

SENSORY RECEPTORS
RECEPTORS
GATEWAY TO THE PERCEPTION
AND SENSATION

Registering of inputs, coding, integration
and adequate response

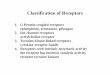
CLASSIFICATION OF THE RECEPTORS
According the type of the stimulus: According to function:
MECHANORECEPTORS Telereceptors
CHEMORECEPTORS Exteroreceptors
THERMORECEPTORS Proprioreceptors
PHOTORECEPTORS interoreceptors
NOCICEPTORS
Reception
Receptor – modified nerve or epithelial cell responsive to changes in external
or internal environment with the ability to code these changes as electrical potentials
Adequate stimulus – stimulus to which the receptor has lowest threshold – maximum
sensitivity
Transduction – transformation of the stimulus to membrane potential – to generator
potential– to action potential
Transmission – stimulus energies are transported to CNS in the form of action
potentials
Integration – sensory information is transported to CNS as frequency code (quantity
of the stimulus, quantity of environmental changes)

CLASSIFICATION OF
RECEPTORS
PHASIC– RAPIDLY ADAPTING
TONIC – SLOWLY ADAPTING
- NONADAPTING – PAIN
CONSTANT FIRING BY
CONSTANT STIMULUS
ACCOMODATION –
CHARACTERISTIC OF PHASIC
RECEPTORS

TYPES OF RECEPTORS

Sensory organs Sensory receptors – they convert the energy from outer
environment to action potentials (electicity) to be sent to the central nervous system and brain cortex for perception, sensation and integration.
QUALITY OF THE STIMULUS (modality) depends on the receptor localisation and the fibers that connect the receptor with the projection centres (cortex)
Adequate stimulus1) produces receptor (generator, local) potential
– does not propagate, is only local 2) After reaching threshold level of depolarisation the action
potential arises – propagate to the brain centres (projection areas)
Example: Once we see the light, means, that the threshold was rerached, the action potential was created and propagated to the brain representation areas
QUANTITY OF THE STIMULUS (MODALITY) depends on the frequency of action potentials that arrive in defined time duration to the projection areas in the brain cortex

SENSORY RECEPTORS
RECEPTORS
GATEWAY TO THE PERCEPTION
AND SENSATION
THE EYE

The light must pass through
various layers of nerve cells and
vessels before reaching
the photoreceptors on the back of
retina.
CORNEA, ANTERIOR AND
POSTERIOR
CHAMBERS, IRIS, PUPIL, LENS,
VITREOUS BODY, RETINA
THE PHOTORECEPTORS ARE
PLACED ON RETINA

COMPUTER
PERIMETRY
SKOTOMA
PERIMETRY – VISUAL FIELD IN GLAUCOMA
LEFT EYE
PERIMETERY
GLAUCOMAA CONDITION OF INCREASED
INTRAOCULAR PRESSURE
Auqeous humor maintains the
Intraoccular pressure within the
Anterior and posterior chambres.
The liquid is secreted is secreted
into the posterior chamber, flows
through the pupil and drains to the
canal of Schlemm.

ACCOMODATION
ACCOMODATION TRIAS
1. LENS ACCOMODATION
Contraction of cilliary muscle
decreases its diameter and loosens
Zonular fibers that makes the lens
thicker
2. MIOSIS
Constriction of the pupil enables the
light to concentrate to fovea centralis –
The site of the sharpest vision
3. CONVERGENCY OF THE BULBS
The eyes converge so as the image is
cast upon the fovea centralis
in both eyes

EMETROPY -
AMETROPY
AMETROPY1) AXIAL = THE LENGTH OF THE BULB IS INADEQUATE TO THE REFRACTION
2) REFRACTION = REFRACTION OF THE LENS IS INADEQUATE TO THE LENGTH
OF THE BULB
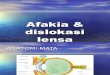
CATARACT
AFAKIA – the eye without the lens
NEARSIGHTEDNESS
Light rays focus in front
of the retina
FARSIGHTEDNESS
Light rays focus behind
the retina
Concave lens
Convex lens

IRIS - MIOSIS, MYDRIASIS
Iris – is made of muscles that enable dilation
or constriction of the pupil – opening in the iris
Pigments of iris give colour to the eyes
In dim light radially arranged smooth muscle fibers
are stimulated to contract by activation of
sympaticus – the consequence is DILATION
In bright light the circularly arranged muscle fibers
Are stimulated to contract by parasympaticus –
the consequence is CONSTRICTION

THE HUMAN EYE IS SENSITIVE TO ELECTROMAGNETIC
LIGHT OF CERTAIN WAVELENGTH 400 – 700 nm
= VISIBLE LIGHT SPECTRUM
ULTRAVIOLET LIGHT (X-RAYS, GAMMA RAYS)
INFRARED LIGHT (MICROWAVES, RADIO WAVES)
= NONVISIBLE LIGHT SPECTRUM

RODS – scotopic vision CONES – photopic vision
VISIONRETINAL RECEPTORS ARE SENSITIVE TO ELECTROMAGNETIC WAVES –
ADEQUATE STIMULI
Štruktúry oka

CONES – receptors for colour
vision – PHOTOPIC VISIONTRICHROMATIC THEORY
(YOUNG)
PRIMARY COLOURS – RED - 560 nm
- GREEN - 530 nm
- BLUE - 430 nm
COMPLEMENTARY (OPONENT)
COLOURSRED-GREEN,
BLUE YELLOW,
WHITE-BLACK
RODS – receptors for black and
white vision- SCOTOPIC VISION
HORIZONTAL CELLS
AMACRINE CELLS
PHOTORECEPTORS
BIPOLAR CELLS
GANGLION CELLS

EXAMINATION OF COLOUR PERCEPTION
Ishihara pseudoisochromatic charts – for detection red-green deficiency
Protanopia – red deficiency
Deuteranopia – green deficiency
Daltonism – red-green deficiency
Tritanopia – blue deficiency
This colours can be distiguishes also by
colour blind people
This colours cannnot be distinguished
by people with the impairment
of red - green colour perception

DISTRIBUTION OF RODS AND
CONES IN THE RETINA



Binocular disparity – the pictures are focused in both eyes on disparate sites of the retina
(not exactly on the same place in each eye) that causes shift. The consequence is 3D
vision
Larger difference causes DIPLOPIA no difference causes 2D vision
Monocular keys
Perspective
Moving paralax
STEREOSCOPIC
VISION

ADAPTATION TO DARK
RHODS
CONES
PHOTOPIC VISION
SCOTOPIC VISION
In dim light less intensity is needed
for light perception,
the adapatation to dark vision lasts
up to 20 minutes
Rods are responsible for dark vision
Red colour is almost not seen in dark
perceived as dark
Blue colour is better seen in dark
perceived as less dark
Dark vision is black and white vision

Ophtalmoscopic view of the retina(eye background)
Visual pathway. From nasal halves of the retina through
crossing (chiasma opticum), from temporal halves of the
retina uncrossed to the thalamus and through optic
radiation to primary visual cortex in the occipital lobe (BA 17)
RETINA – rods and cones
are the receptors enabling
vision (dark, light)
through bipolar and
ganglion cells - transmit the
potentials to optic nerve

SENSORY RECEPTORS
RECEPTORS
GATEWAY TO THE PERCEPTION
AND SENSATION
THE EAR

THE EAROUTER - AIR
MIDDLE - LIQUID
INNER - LIQUID
AUDITORY PATHWAY
From the receptors (hair cells) in the
organ of Corti through vestibulocochlear
nerve (VIII.) to thalamus and to primary
auditory cortex in temporal lobes

HEARING - SOUND RECEPTORY
MECHANORECEPTORS IN COCHLEA (INNER EAR)Scala vestibuli
Scala media – hair cells - mechanoreceptors
Scala tympani

PERCEPTION OF SOUND FREQUENCIES

ORGAN OF CORTI IN THE INNER EAR

Normal audiogram Perception hypoacusis
AUDIOMETRY
HEARING IMPAIRMENTS –
PERCEPTION DEAFNESS
due to impairments of
receptors, nerves or brain
centres – cochlear implates

AUDIOMETRYHEARING IMPAIRMENTS
CONDUCTION DEAFNESSDue to impairments of outer or middle ear
-otosclerosis
Blue line – hearing conducted by bone through mastoid process
Red line – hearing conducted by air through outer and inner,
this line normally lies more or less above the blue line

SENSORY RECEPTORS
RECEPTORS
GATEWAY TO THE PERCEPTION
AND SENSATION
THE PAIN

PAIN RECEPTORS AND TRANSMISSION OF PAIN STIMULI
Pain receptors are free nerve endings in the superficial lAyers of the skin and internal tissues
Excitation of receptors by mechanical thermal and chemical stimuli
Pain receptors are nonadapting for being apprised of damaging stimulus
– the increase of sensitivity – HYPERALGESIA
- the decrease of sensitivity – HYPOALGESIA
Dual transmission of pain signals – two separate pathways for transmitting pain signals
correspond to the two types of pain
FAST (SHARP) PAIN – mechanical or thermal stimulation
Transmission by fast A delta fibers (6-30 m/s)
Makes the person to know where is the pain and to react immediately to remove the particular
part of the body from the stimulus
THALAMUS and spreading of the singnals throughout the brain cortex
SLOW (CHRONIC) PAIN – chemical stimulation or chronic mechanical and thermal s.
Transmission by slow C fibers (0,5 – 2 m/s)
Becomes more and more painful over a period of time, intolerable suffering
Spinothalamic tract, thalamocortical tract to somatic sensory areas

PERCEPTION AND SENSATION OF PAIN
CLASIFICATION OF PAIN:
SURFACE (FROM SKIN RECEPTORS)
a) FAST (pricking)
Sharp pain, short duration, precise localization
via A delta fibersCauses: techykardia, BP increase, increase of blood sugar, sweating,
Decrease of GIT motility
b) SLOW (burns)
Less precise localization, persisting
via C fibers
DEEP
a) VISCERAL
(spasms a distension of smooth m.,tumors, inflamations)
Not precise but constant localization
– „referred pain“
Via C fibersCauses: bradykardia, hypotension (fainting), vomiting, sweating
b) SOMATIC (muscle and joint destruction)
Not precise localization
Via A delta and C fibers, release of substance P

QUANTIFICATION OF PAIN SENSATION AND PERCEPTION
Sensation of pain is uniform
Proof: dolorimeter developed by HARDY
(system of lenses, heat from the condensed light
centered on the black-coloured skin)
Unit – 1 JND (just noticeable difference)
0 JND – subthreshold pain
1 JND – threshold pain
21 JND – maximal (intolerable) pain
HYPOALGESIA– LOWER PERCEPTION OF PAIN
(acupuncture, acupressure, wounds in war)
ANALGESIA – NO PAIN PERCEPTION
(local, regional)
HYPERALGESIA – HIGHER PERCEPTION OF PAIN
(thalamic syndrom in postero-inferior infarction of the
thalamus – facilitation of pain transmission

REFERRED PAIN
CONVERGENCE THEORY
Less number of second order neurons
than afferent fibers from receptors –
convergence of stimuli from particular sites
of the skin and visceral organs on spinal
neurons (the heart and skin of the left arm)
- symptoms of myocardial infarction
FACILITATION THEORY
AP from visceral organ facilitate –
predepolarises the second order neuron,
weak stimulus from somatic structure
excite afferent neuron, on which both of them
converge, but the sensation comes from
somatic structure

REFERRED PAIN

PHANTOM PAINCNS identifies quality and location of pain via
receptors and ascending tracts, that transmit AP
CNS cannot distinguish AP from receptors
and those which were elicited on ascending fibers

MECHANISMS OF HYPOALGESIA
CENTRIFUGAL INHIBITION OF PAIN
Influence of second order neuron
via interneurons from reticular formation
descending collaterals inhibit
pain afferentations by decrease
of neurotransmitter on ascending neuron
– lower frequency of AP transmission to
thalamus

MECHANISM OF PRESYNAPTIC
INHIBITION - PAIN GATING
MECHANISMS OF HYPOALGESIA
Non-painful sensations e.g. from pressure
receptors in the skin overlay painful sensation
from the same skin locality, because the
nerve fibers of both converge
on the same afferent neuron
Mechanism:
- Collaterals of non-painful fibers form
axo-axonal synapse with “pain” fibers
and predepolarize them
- AP on pain fibre loses its previous
amplitude
- less neurotransmiter is released on
target neuron
- Transmission of AP to second order neuron
is less probable










![[Pharma] receptors](https://img.pdfslide.us/doc/110x75/55c466e6bb61eb94478b470c/pharma-receptors.jpg)

















