Embed Size (px)
Citation preview

Troels Staehelin Jensen, MD, Ph.D
Dept. of Neurology &
Danish Pain Research Center
Aarhus University Hospital, Denmark
Sensitization and pain: HCM city, December 2012

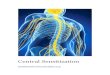
Pain transmission and modulation
Courtesy I. Tracey 2008

Sensory brain Thalamus S I and S II
Non-sensory brain DLPFC Insula Cingulate cortex Amygdala
Pain: more than a sensory experience
Sensory Affective Cognitive
ACC
DLPFC
Thalamus Insula
Amygdala
S I
Casey, Handb Clin Neurol , 2006

Pain modulation
Nociceptive modulation: On cells, off-cells In brainstem
Basbaum & Fields, 1984 Fields HL, 1991, 2004
RVM
PAG
Nociceptive modulation: Noxious input activates descending control
Jensen & Yaksh 1992
response
stimulus
Increased
facilitation
Normal
response
stimulus
Increased
inhibition
Normal
Clinical pain modulation: Facilitation and inhibition

PAG
Spinal
neuron
RVM
LC
Spinal
neuron
ParBr
Thalamus
Sensory Emotional
Noxious input
Pain
S I
DLPFC
Amygdala Insula
Cognitive

Following injury: Peripheral and central changes contribute to pain
Peripheral sensitization: Amplification of signalling in nociceptive fibers that elicits pain hypersensitivity
Central sensitization: Amplification of CNS signalling that elicits pain hypersensitivity (Woolf, Pain 2011)

Change in flexor reflex threshold following a 1 min burn injury to the lat. foot
hr min hr
Nature 1983; 306; 686-688
Spont. activity in α-motoneuron of biceps femoris after foot injury
Threshold for evoking response ipsi (circle) and contralat (triangel) after foot injury
Response in a single biceps unit before and after injury First demonstration: long term consequences of noxious stimulation result from peripheral and and central changes

Radial nerve block
Ulanr nerve block
A: regions anesthetic to all modalities B: Overlapping innervation territories C: Spread of brush allodynia into radial nerve territory after capsaicin
Extension of hyperalgesia and allodynia beyond ulnar nerve territory Positive values are areas outside ulanr nerve territory
Sang et al. Anesthesiology 1996.
C-nociceptor acivation evoke central sensitization: Capsaicin allodynia/hyperlgesia cross nerve territories

Sensitization
Components of central sensitization: Facilitation of output persisting after a painful input Non-painful input produce output mimicking a painful stimulus Reduced inhibition, Increased facilitation
C-fibres
Aβ-fibres
Normal state
C-fibres
Aβ-fibres
Peripheral sensitization
C-fibres
Aβ-fibres
Central sensitization

Capsaicin : model for peripheral and central sensitization

Neuronal hyperexcitability: Clinical translation
Peripheral changes • Spontaneous activity periphery and DRG
• Lowered threshold
• Increased response to suprathreshold stimuli
Clinical • Spontaneous and provoked pain
• Hyperalgesia
Inflammation
Nerve injury

Tissue inflammation
Ion channels Na+, K+, Ca++
TrkA
NGF
Bradykinin B2
Heat/Capsaicin/H+
H+
PGE2
ATP
ATP
Cold
TRPM8 P2Y
P2X3
EP
ASIC
TRPV1
Inflammation sensitization: NGF-TrkA activate signaling pathways NGF transport to DRG: increase in: SP, TRPV1, Nav 1.XX Cytokine release ; Il-1, Il-6 ,TNF- Protons act on TRPV1 and on ASIC’s, etc
Nerve injury
Nerve Injury sensitization: Upregulation of ion Na+ and K+ channels and TRPV1 in non-injured fibres NGF and Cytokines increase after nerve injury Rythmic firing burst from damaged nerve fibres
Expressed N. injury
Nav 1.1 Non-noc cells
Nav 1.2
Nav 1.3 Expr in injury
Nav1.4 Heart
Nav1.5 Heart
Nav1.6 Non-noc cells
Nav1.7 All sens cells
Nav1.8 A and C cells
Nav1.9 In noc. C cells
NaX

Neuronal hyperexcitability: Clinical translation
Peripheral changes • Spontaneous activity periphery and DRG
• Lowered threshold
• Increased response to suprathreshold stimuli
Clinical • Spontaneous and provoked pain
• Hyperalgesia
• Localized pain
AMPA NK1
NMDA NMDA
NMDA
Ca++
Inflammation
Nerve injury

Neuronal hyperexcitability: Clinical translation
AMPA NK1
NMDA NMDA
NMDA
Ca++
Nerve injury
Inflammation
Central changes • Spontaneous and evoked activity
• Recruitement of silent cells
• Increase in receptive fields
• Abnormal temp summation
• Spread up and down spinal cord
• Sensitization of brain areas
• Neuroplastic changes
Clinical • Spontaneous and provoked pain
• Spread of pain to other tissues
• Spread of pain outside injured area
• Hyperalgesia/allodynia
• Abnormal temporal summation
• Aftersensations
• Cognitive and emotional changes

Spinal cord
Central sensitization following inflammation Neuronal hyperexcitability Lowering of threshold Recruitment of silent nociceptors Abnormal temporal summation (wind-up) Aftersensations Normalization when inflammation subsides
Spinal cord Spinal cord Spinal cord
Inflammation

Spinal cord Spinal cord
Central sensitization following nerve injury Nuronal hyperexcitability Lowering of threshold Recruitment of silent nociceptors Abnormal temporal summation (wind-up) Aftersensations Maladaptive changes following continuous input
Spinal cord
Nerve injury

Chronic pain: different etiologies, common symptoms
PHN
Peripheral Neuropathy
Post stroke pain
Cancer pain
Low back pain CRPS
Spinal cord injury pain

Nociceptive Neuropathic Idiopathic
Osteoarthritis Nerve injury Fibromyalgia
Rheumatoid arthritis Neuropathies Whiplash syndrome
Myositis Plexopathy Interstitial cystitis
Tendinitis Amputation Irritable bowel
disorder
Colitis Trigeminal neuralgia Persistent Idiopathic
facial pains
Postoperative pain Postoperative pain Gulf War Syndrome
Migraine ? MS Chronic fatigue
syndrome
CRPS ? Stroke
Chronic Non-malignant types of pain: Examples

Characteristics
• Sensory loss
• Motor loss
• Spontaneous + evoked pain
• Allodynia/hyperalgesia
• Specific sensory pattern
• Aftersensations
• Abnormal summation Nerve root damage
1. Low back pain and radiculopathy
• 55 yr. old M • Previously operated for L4 herniated disc • Recurrence of radicular pain after 1 yr. • Reoperated twice • Now constant burning pain in the S1 area • intermittent radicular pain and ”foot drop” gait •Pain has increased within the last month • VAS pain: 5-10

Causes of pain: Low back
Definition • Pain • Muscle tension • Stifness • Below costal margin and above inf. gluteal folds
Classification: • Specific • Non-specific Duration: • Acute pain: <6 wks • Subacute. 6 wks -3mths • Chronic: >3 mths Neuropathic pain LBP: • 5-37% ?
Neurogenic mechanisms of LBP Root compression
– Herniated disc,
– Spinal stenosis
– Arachnoiditis
Peripheral nerve Lesion
– Spinal nerve compression
– Neuropathy
– Nerve injury
Lumbar plexus
– Tumor
– Psoas absces
– Neuritis

Characteristics
• Sensory loss in peroneal nerve territory
• Spontaneous and evoked pain
• Touch-evoked pain outside injured nerve territory
• Hyperalgesia outside injured nerve territory
Neuropathic Pain: case
• 42 yr. old F • Tibial fracture 1996 • 1996 removal of ostesynthesis • 1998 removal of neuroma peronal nerve • Constant burning pain in malleol area • Evoked pain in lower leg and foot • VAS pain: 5-10

Characteristics
• Sensory loss
• Spont + evoked pain
• Allodynia/hyperalgesia
• Specific sensory pattern
• Paroxysms
• Aftersensations
• Abnormal summation
• Mood and sleep cognitive changes
Neuropathic Pain case

2. Neuropathic pain
History and symptoms
• 31 yr old Female
• 1998: removal of melanoma
• 1999: exploration f. neurinoma
• Const. pricking pain in scar
• Abnormal cold sensation on back
• Light clothes on back is painful
Findings • sensory loss
• Spontaneous pain
• evoked pain
• Pinprick hyperalgesia
• dynamic allodynia
• Cold allodynia
• Static hyperalgesia
• Temp summation
• Aftersensations
0 3 0 6 0 9 0 1 2 0 1 5 0 1 8 0 2 1 0 2 4 0
0
2 0
4 0
6 0
8 0
1 0 0
VAS
2.0 Hz
0.2 Hz
Aftersensation
Sec

Pain after herniotomy
Reduced sensitivity
Increased sensitivity
Ilioinguinal N
Genitofemoral N
Iliohyogastric N
60-yr M, healthy; Fulltime worker as a work manager; Is active in sport
2003: Inguinal herniotomy uncomplicated , but immediately after operation he had pain in the groin
Constant pain: VAS: 2
Pain on movement : VAS:7
Wake up 1-2 times during night because of pain
Can't do sports, Works only part-time. Can't walk with his dog. Has put on 5 kg.

Surgical procedures CABG Cranofacial surgery Amputation Hernia Nerve lysis Mastectomy Thoracotomy Vascular graft SNB and LND Hip arthroplasty Hysterectomy Cholecystectomy?
Postoperative Pain: Epidemiology
Surgical procedure
Incidence of pain (%)
Severe pain (%)
Limb amputation 30–50 5–10
Breast surgery (mastectomy)
30–40 5–10
Inguinal hernia repair
10 2–4
Thoracotomy 30–40 ~10 ?
Coronary bypass 30–50 5–10
Caesarean section 10 ~4
Hip arthroplasty 20 <5
Craniofacial surgery
5
Lymp node dissection
34 <12

Post Stroke Pain: 3 days after stoke: L. pricking pain; Cold allodynia 3 yrs after stroke: Constant pain L. face, arm, trunc Deep burning, pricking pain VAS pain intensity: 8
Acute MR – DWI CTC Day 2
Stroke 48 yr, F. sudden L. hemiparesis Gaze palsy, L hemiparalysis L. sensory loss DWI lesion R. hemisphere Thrombolysis Day 2 large MCI infarction

CPSP
• Pain in area of sensory abnormality • Pain area: Fraction of sensory loss • Sensory loss and hypersensitivity. • Loss of input to thalamus Pain in
corresponding body territory
Reticular N
Anterior
Lateral Medial
stroke
Sensory loss Pain

Spinal cord injury (SCI) Etiology
• Sports and leisure activities
• Assaults
• Transport activities
• Falls
• Other traumatic causes
• Nontraumatic causes
Consequences
• Paresis
• Bladder, bowel and sexual dysfunction
• Autonomic changes
• Spasticity
• Sensory changes and pain

Neuropathic pain following SCI
At-level
Below-level
Other
Bryce et al. Spinal Cord 2011 Epub
Within the dermatome of the
neurological level and three
dermatomes below this level
More than three dermatomes
below the neurological level
but may extend to the “at-
level” region
Neuropathic pain unrelated
or indirectly related to the
SCI

Classification Neuropathic pain at level
Neuropathic pain below level
Musculoskeletal pain
Visceral pain
Spinal cord injury pain
STT neurons
Spinal
lesion
Propriospinal system
Spinal cord
Finnerup unpublished obs

Finnerup et al. 2003
Sensory disturbance
after spinal lesion
Pain Localisation
after spinal lesion

SCI: Sensory function
Brush allodynia Pinprick hyperalgesia
Cold allodynia Cold allodynia
Dorsal column
Postion, vibration
Spinothalamic tract
Touch, pinprick,
temperature

Classification Neuropathic pain at level Neuropathic pain below level
STT
Spinal lesion
Propriospinal system
Spinal cord
Mechanism SCI pain at and below level •Deafferentation •Spinothalamic loss necessary •Spinothalamic loss not sufficient •Hyperexcitability at injury level •Grey matter loss above injury level

Central sensitization after nerve injury: Injury triggers sensitization in spinal cord (homo- and hetero-synaptic) Spinal sensitization involves a series of mechanisms and substances Spinal sensitization spreads to the brain Brain activation: areas controlling sensation, emotions, cognition Changed descending control
Locations: Periperal nerves Spinal cord Brainstem Thalamus Cortical/Subcortical
Conclusion: Sensitization

Thanks to all collaborators at DPRC: Birgitte Brandsborg, Erisela Querama, Lene Vase, Lone Nikolajsen, Anders D Kristensen, Hanne Gottrup, Nanna Finnerup, Cathrine Baastrup, Henriette Klit, Lise Gormsen, Astrid Terkelsen, Annette T. Møller, Helle O. Andersen, Camilla Maersk-Møller, Anne Hansen, Lene Christensen, Casper Skau-Madsen, Kaare Brinck, Paal Karlsson

![Abstract 7 - DASAIM · [1] Arendt-Nielsen et al, Sensitization in patients with painful knee osteoarthritis, Pain 2010;149:573-581. [2] Grosu et al, Pain after knee arthroplasty:](https://img.pdfslide.us/doc/110x75/5ee0b227ad6a402d666bd65f/abstract-7-1-arendt-nielsen-et-al-sensitization-in-patients-with-painful-knee.jpg)