Embed Size (px)
Citation preview

1417
ClinicalChemistry 42:9
1417-1425 (1996)
Sensitive and specific quantification of sirolimus(rapamycin) and its metabolites in blood of kidney
graft recipients by HPLC/electrospray-mass spectrometry
FRANK STREIT,”2 UWE CHRISTIANS,3* HANS-MARTIN SCHIEBEL,2 KIMBERLY L. NAPOLI,4
LUDGER ERNST,5 ANNETTE LINcK,’ BARRY D. KAHAN,4 and KARL-FRIEDRICH SEWING2
Sirolimus (rapamycin) has a macrolide structure and isunder clinical investigation as an immunosuppressant after
organ transplantation. An 1-IPLC/mass spectrometry assay
to quanti1 sirolimus in blood was developed. 28-O-Acetylsirolimus was used as internal standard. Blood samples wereextracted with C18 columns. The extracts were injected into
an HPLC system and isocratically eluted with methanol/i %
formic acid (90/10 byvol) from a 150 x 4mm C18 analytical
column. The HPLC system was connected to a triple-stagequadrupole mass spectrometer with an electrospray inter-
face and positive ions were detected. The limit of quantifi-cation in 1 mL of blood was 0.25 i.eg/L and the calibration
curve in blood was linear up to 250 zg/L. The recoveryfrom blood was 88 ± 26% and interassay variation at 1 pgfL
was 19% and at 15 pgfL 9.3%. Hydroxy, dihydroxy, de-
methyl, and didemethyl siroliinus as well as sirolimus were
detected in blood of kidney graft patients.
INDEXING mIuis: therapeutic drug monitoring #{149}organ trans-
plantation #{149}macrolides
Sirolimus (rapamycin, AY-22,989; Wyeth-Ayerst, Princeton,
NJ) is a 31-membered macrolide lactone C51H79N013 [1-3]with a molecular mass of9 13.6 Da (Fig. 1). In solution, sirolimus
forms two conformational trans-, cis-isomers with a ratio of 4:1
Institut f#{252}rAllgemeine Pharmakologie, Medizinische Hochschule Han-
foyer, Hannover, Germany.
Instituts f#{252}r2 Organische Chemie and Anorganische Chemie und Analytik,Technische Universit#{228}tBraunschweig, Braunschweig, Germany.
Department of Biopharmaceutical Sciences, Room S-834, School of Phar-
macy, University of Califomia at San Francisco, 513 Pamassus Ave., San Fran-cisco, CA 94143-0446.
Division of Immunology and Organ Transplantation, Department of Sur-
gery, University of Texas Medical School at Houston, Houston, TX.
*Author for correspondence. Fax 41 5-476-8887; e-mail [email protected] October 23, 1995; accepted April 17, 1996.
(chloroform) due to hindered rotation around the pipecolic acid
amide bond [3, 4]. Because of its triene structure, sirolimus has
ultraviolet (UV) absorption maxima at 288, 276, and 266 nm.6 It
is sparingly soluble in water, aliphatic hydrocarbons, and diethyl
ether, whereas it is soluble in alcohols, halogenated hydrocar-
bons, and dimethyl sulfoxide [1, 5, 6]. Sirolimus is unstable in
solution and degrades in plasma and low- and neutral-pH
buffers at 37 #{176}C,with a half-life of <10 h [6, 7]. The structuresof the degradation products have recently been characterized
[8].
Sirolimus is isolated from Si-reptomyces hygroscopicus [5, 9] and
was originally developed as an antifungal [6, 10, Ii] and anti-
cancer drug [6, 12]. Interest has also focused on its immunosup-
pressive activity [13]. Although it shares structural homology
with the immunosuppressant tacrolimus and binds to the same
intracellular binding protein in lymphocytes [14, 15], it inhibits
S6p70-kinase and therefore has a mechanism of immunosup-pressive action distinct from that of tacrolimus [6, 16]. Sirolimus
was found to prolong graft survival of different transplants in
several species alone [6, 17-19] or in combination with other
immunosuppressants [6, 20, 21]. In animal models its spectrum
of toxic effects is different from that of cyclosporine or tacroli-
mus [6, 22], comprising impairment of glucose homeostasis,stomach ulceration, weight loss, and thrombocytopenia
[6, 17, 21], although no nephrotoxicity has been detected
[18, 21]. Sirolimus is under clinical investigation as an immuno-
suppressant after kidney transplantation.Sirolimus is metabolized by cytochrome P-450 3A to at least
six metabolites [23, 24]. During incubation with human liver and
small intestinal microsomes, sirolimus was hydroxylated and (or)
demethylated, and the structure of 39-O-demethyl sirolimus was
identified [24]. In bile of sirolimus-treated rats, >16 hydroxyl-
6 Nonstandard abbreviations: UV, ultraviolet; ESI, electrospray ionization;
MS, mass spectrometry; and CAD, collision-activated dissociation.

Fig. 1. Structure of sirolimus and its meta-bolic pathways.Numbering of atoms follows the rules of the Cam-bridge Structure Data Bank: first numbering of themain chain, then of the methyl groups.
Me OMe Me Me
further hydroxylated- and/or demethylated metabolitesfr
1418 Streit et al.: ESJIMS of sirolimus
si roll mus
ated and (or) demethylated metabolites were detected by
HPLC/electrospray-mass spectrometry (ESI-MS) [25].
HPLC assays have been described by several authors
[24, 26-29]. Most of these methods do not allow quantification
of sirolimus metabolites [26-29] and have other serious draw-
backs: The method described by Sattler et al. [23] does not
report any specifications, Napoli and Kahan [26] did not show
that their method is able to quantify sirolimus in biological
samples, and Yatscoff et al. [27] used demethyl sirolimus as
internal standard, which is a potential sirolimus metabolite [24]
and is present in blood of patients in concentrations equal to thatof sirolimus (vide infra). The only HPLC/IJV assay described so
far that is used for therapeutic drug monitoring of sirolimus-
treated patients is that described by Napoli and Kahan [29]. This
assay does not allow quantification of metabolites and its
sensitivity is limited to 2 gfL. Because of its high immunosup-pressive potency [6,16,30],a sensitive and specific assay for
sirolimus and its metabolites that detects concentrations <1
g/L in tissue and biological fluids is required to evaluate itspharmacokinetics [6].
MaterialsandMethodsINSTRUMENTS AND CHEMICALS
The following HPLCIESI-MS/MS system was used: A TSQ
700 mass spectrometer with electrospray fast-flow interface
(Finnigan MAT, Bremen, Germany) was combined with an
L6200 HPLC pump and an L7200 autosampler (Merck-Hita-chi, Darmstadt, Germany). A 3.9 X 150 mm Resolve#{174}analytical
C18 colunm with 5-pm particle size (‘Waters Millipore, Milford,
MA) was used as analytical column and all solvents for sample
extraction or HPLC/MS analysis were purchased from Merck(Darmstadt, Germany) and were of HPLC quality. For semi-
preparative isolation of sirolimus metabolites as well as the
internal standard, an HP 1084B chromatograph (Hewlett Pack-
ard, Waldbronn, Germany) in combination with a 655A-40
injector and a D-2000 integrator (both Merck-Hitachi) and a10 X 250 mm column filled with Nucleosil#{174}C8 reversed-phase
material (Macherey-Nagel, Duren, Germany) with 7-sm patti-
cle size were used. Acetic acid anhydride for synthesis of the
internal standard was of reagent grade and purchased from
Merck. Samples were extracted on 3-mL C, columns (Recipe,
39-0-demethyl sirolimus
CYP3A
Me OMe Me Me
Munich, Germany) with a SpeedMate#{174} extraction bench
(Zinsser Analytic, Frankfurt, Germany). Sirolimus was a kind
gift from S.N. Sehgal (Wyeth-Ayerst, Princeton, NJ). Blood
samples were taken from four stable kidney graft recipients (avg.
89 days after transplantation, ranging from 25 to 155 days)
receiving oral sirolimus therapy who were included in the phase
II clinical trial at the Texas Medical Center (Houston, TX). The
patients received a mean sirolimus dose of 1.35 mg/day (range:
0.9-1.9 mg/day). All patients received cyclosporine and pred-
nisolone as additional immunosuppressants. Samples were anti-
coagulated with EDTA. The collection of blood samples for
measurement of sirolimus concentrations was part of the study
protocol, which was in accordance with the Declaration of
Helsinki of 1975 and its revisions and was approved by the local
ethics committee.
STORAGE OF PATIENTS’ SAMPLES AND STOCK SOLUTIONS
Because the instability of sirolimus is one of the critical issues of
its analytics, all patients’ samples were placed on ice immedi-
ately, deep frozen at -40 #{176}Cas soon as possible, and were
mailed on dry ice. Stock solutions of sirolimus and its internal
standard 2 8-O-acetyl sirolimus were dissolved in methanol and
stored at -80 #{176}C.Under these conditions, patients’ samples and
stock solutions were stable for at least 6 months. After 6 months
the concentration of sirolimus was 88 (1 l)% [mean (SD), n = 81
of the initial concentration. After a second freeze/thaw cycle, the
concentration of sirolimus was significantly reduced or below
the detection limit. Stability of sirolimus and its metabolites
during HPLC/MS analysis was checked as follows: Sirolimus
was metabolized by human liver microsomes as described pre-
viously [23] and sirolimus and its metabolites were quantified by
HPLC-UV [23]. To 1 mL of blood, 100 L of the extracted
microsomes containing sirolimus and its metabolites as well as
250 ng of internal standard were added. The blood samples were
extracted as described below. The extracts were pooled and
placed in the autosampler of the HPLC/MS system. One
hundred microliters was injected and analyzed five times imme-
diately after extraction and after 1, 3, 5, and 7 days as described
below. The results of days 1-7 were expressed in percent of the
concentrations measured right after extraction ( 100%).

A
B
D
5 10 15 20 25 30 35 40
Clinical Chemistry 42, No. 9, 1996 1419
SYNTHESIS AND PURIFICATION OF THE INTERNAL
STANDARD
The internal standard 28-O-acetyl sirolimus and two other
mono- as well as one diacetylated sirolimus derivative were
synthesized as follows: 12.85 mg of sirolimus was dissolved in 13
mL (137.5 mmol) of acetic acid anhydride, resulting in a final
concentration of 14 mmol/L, and incubated for 3 h at 55 #{176}C.
The mixture was dried under a stream of nitrogen and theresidue was dissolved in 2 mL of acetonitrile/sulfuric acid, pH 3,
(75/25 by vol) and injected into a semipreparative HPLC
system. The acetylated sirolimus derivatives were separated on a
250 X 10 mm C8 7-sm column by using the following
acetonitrile/sulfuric acid (pH 3) gradient: analysis time 0 mm,
400 mL/L acetonitrile; analysis time 38 mm, 700 mL/L aceto-
nitrile; analysis time 45 mm, 800 mLIL acetonitrile. The flow
was set to 4.5 mL/min, the column temperature to 35 #{176}C,and
the UV detection wavelength to 276 nm. 28-O-Acetyl sirolimus
was eluted from the HPLC column with a retention time of 32
mm (Fig. 2). Fractions were manually collected and extracted
with equal volumes of dichloromethane. The organic phase was
dried over MgSO4 and evaporated under vacuum. Structuresand purity of the internal standard were confirmed by ESI-
MS/MS and collision-activated dissociation (CAD). For CAD,
argon was used as collision gas with a collision energy of 49 eV.
Structural identification of the internal standard was based upon
analysis of the fragmentation pattern shown in Figs. 3 and 4 and
described in refs. 31 and 32.
GENERATION AND PURIFICATION OF SIROLIMUS
METABOLITES
Sirolimus metabolites were generated as previously described
[24]. Human liver microsomes were isolated by using standard
centrifugation techniques [33]and the protein concentration
adjusted to 3 g/L with 0.1 mmol/L phosphate buffer. Sirolimus
was dissolved in acetonitrile/suiftiric acid (pH 3, 75/25 by vol)
and incubated with 1 mL of the microsomal suspension and 0.5mL of an NADPH-producing system (2 mmol/L EDTA, 10
mol/L MgC12, 0.84 mmolJL NADP, 18 mmolIL isocitric acid,
and 667 U/L isocitrate dehydrogenase dissolved in 0.1 mmol/Lphosphate buffer, pH 7.4) for 30 mm at 37 #{176}C.The reaction was
stopped by addition of 0.5 mL of acetonitrile. The samples were
centrifuged at 2SOOg for 2 mm and the supernatant drawn
through glass extraction columns (Krannich, Gottingen, Ger-
many) filled with C8 LiChroprep#{174}(Merck) of 25-40-jimparticle size and previously washed with 3 mL of acetonitrile and3 mL of sulfuric acid (pH 3). The samples were washed on the
columns with 3 mL of methanol/sulfuric acid (pH 3, 50/50 by
vol) and I mL of hexane and eluted with 1.5 mL of dichlo-
romethane. The dichloromethane eluates were pooled, evapo-rated at 40 #{176}Cunder a stream of nitrogen, and the residues
dissolved in 1.5 mL of acetonitrile/sulfuric acid (pH 3, 75/25 byvol). The sample was washed with the same volume of hexane
and then injected into the HPLC system. Sirolimus and its
metabolites were eluted from a 250 X 4mm C8, 3-j.m Nucleosil
column with the following gradient: analysis time 0 mm, 470
mL/L acetonitrile; 7 mm, 470 mL/L acetonitrile; 20 mm, 500
mL/L acetonitrile; 40 mm, 550 mL/L acetonitrile; 45 mm,610 mLIL acetonitrile. The flow was set to 0.7 mL/min, the
oven temperature to 35 #{176}C,and the detection wavelength to 276
nm. Fractions containing the metabolites were manually col-
lected and the metabolites identified by HPLC/ESI-MS/MS as
previously described [24] and as described for the internal
standard above (key fragments of 39-O-demethyl sirolimus: see
Fig. 4). Purity of the isolated metabolites was >95% as esti-
mated by HPLC/UV [24]. Furthermore, the metabolites were
used to compare the signal intensities of the different sirolimus
Fig. 2. Isolation of the internal standard 28-O-acetyl sirolimus and other acetylated siroli-mus derivatives by semipreparative HPLC.
Chromatogram of 28-O-acetyl sirolimus during semi-preparative isolation by HPLC. HPLC conditions:250 x 10 mm C8 7-.em column, acetonitrile/sulfuric acid (pH 3) gradient: analysis time 0 mm,500 mL/L acetonitrile; analysis time 20 mm, 550mL/L acetonitrile; analysis time 35 mm, 650 mL/Lacetonitrile; analysis time 40 mm, 750 mL/L ace-tonitrile. Flow 4.5 mL/min, column temperature35 C, LIV detectionwavelength 276 nm. A repre-sentativechromatogram is shown. Retention time(t5) 28.5 mm, sirolimus (A, larger peak); t 32.9mm, 28-O-acetyl sirolimus (B, larger peak); t 34.9mm, 40-O-acetyl sirolimus(C, larger peak); t 37.6mi 28,40-O-diacetylsirolimus (D, larger peak).The smaller peaks behind the sirolimus and derive-tive peaks with retention times of 29.9 mm, 33.8mm, 36.0 mm, and 38.5 mm, respectively,repre-sent the separated rotameres.

1420 Streit et al.: ESI/MS of sirolimus
A 936.6% 100
eo’
60’
40’
20
409 .3
1 693453.1345.232 0...j.,
582.4..
ILdA I.______200 4#{212}0 600
73j. 575.5 Do4....
i I.iI41.-#{176}
B
$ oo’95.4
I1II .3
773.2Fig. 3. CAD mass spectra of sirolimus (A) andthe internal standard 28-0-acetyl sirolimus
The fragments used for identification according toFIg. 4 are marked by arrows.
1000 en
derivatives and recoveries of single metabolites during extrac-
tion with those of sirolimus and the internal standard.
EXTRACTION OF BLOOD SAMPLES
To 1 mL of blood, 25 jiL of the internal standard solution (Img/L in methanol) and for protein precipitation 2 mL of
methanol/water saturated with zinc sulfate (70/3 0 by vol) were
added. Samples were vortex-mixed for 20 s and centrifuged at
2000g for 2 mm. The supernatants were drawn through C18
extraction columns that had previously been primed with 2 mLof acetonitrile and 2 mL of sulfuric acid (pH 3). The pressurewas adjusted to -5 mmHg. The extraction columns were
washed with 2 mL of sulfuric acid (pH 3) and dried by drawing
air through the columns for 2 mmn. Sirolimus, its metabolites,
and the internal standard were eluted with 400 j.LL of acetoni-
trile/l % formic acid (90/10 by vol). Two hundred microliters
were transferred into an HPLC microvial (Hewlett-Packard)
and 100 1.L of the extract was injected into the HPLC system.
HPLC/ESI-MS
Sirolimus, its metabolites, and the internal standard were eluted
isocratically from the analytical column with methanolll%
formic acid (90/10 by vol) at a flow rate of 0.4 mL/min. The
column temperature was 35 #{176}C.The mass spectrometer was
tuned with 0.5g/L sirolimus dissolved in the mobile phase and
delivered by a syringe pump at 5 jLL/min, bypassing the HPLC
column. The capillary temperature was 200 #{176}C.The auxiliarygas pressure was 175 kPa and the gas was not heated. The sheath
gas pressure was 175 kPa. The needle voltage was adjusted to 5.5
kV and the capillary exit voltageto -200 V. The mass spec-
trometer was run in the positive ion mode. The multiplier
voltage was set to 1400 V and the conversion dynode to -15 kV.
For single ion detection, the MS was focused on the [M+Na}
of didemethyl sirolimus [908 atomic mass unit (amu)], demethyl
sirolimus (922 amu), sirolimus (936 amu), hydroxy sirolimus
(952 amu), dihydroxy sirolimus (968 amu), trihydroxy sirolimus
(984 amu), as well as 28-O-acetyl sirolimus (978 amu). The
resolution was set to 1000 (10%-valley definition) and a mass
was scanned within 0.25 s.
Because sirolimus and its metabolites gave the same detector
response after MS analysis as equal amounts of the internal
standard, similar slope and intercept of the calibration curves, as
well as equal recoveries (see below), concentrations of sirolimus
and its metabolites were calculated as follows: sirolimus or
metabolite (pg/L) = (areas sirolimus or metabolite/areas inter-
nal standard) . internal standard added (p.gfL). Determination of
recoveries, inter- and intraassay variation, calibration curves,
and lower limit of quantification were based on blood collected
from healthy volunteers, to which sirolimus or the purified
metabolites dissolved in acetonitrile/sulfuric acid (pH 3, 7/3 by
vol) were added. Calibration curves were made up of six data
points (0, 1, 5, 10, 50, and 250 j.tg/L with n = 5). The
concentration of sirolimus or its metabolites was calculated by
using the internal standard and the formula described above.
Data were analyzed by using linear regression analysis (REG
procedure, SAS version 6.05;SAS Institute, Cary, NC). The
accuracy was calculated as the deviation from the nominal
concentration added to 1-mL blood samples of healthy volun-
teers and are given in percent of the nominal concentration. As
for the calibration curve, concentrations were calculated with
fragment of sirolimus ,, o fragment of 40-0-acetyl sirolimua
HYlCcOH H,LYfoH HYccOMMs Ms Na A m/z 331 Me Me Na
mlz 387/simlimus c51HNo13NaR’Me,R =H,RHm/z938.6
39-0-demethyl sirolimus CwHnNO,3NaR’ H, R2 = H, R3 =Hmiz 922.6
40-0-acetyl sirolimus cH81NO,4Na=Me. R2 =coCH3,R3 =H
m/z 978.6
28-0-acetylsirolimusC5,H81N0,4NaR1=Me, R2 H, R3= COCH3m/z =978.8
fragment of 28-O.acetyl sirolimus
Me OMe Me Mem/z 649
fragment of sirolimus
MoMe
m/z =607
Clinical Chemistry 42, No. 9, 1996
fragment of39-O-demethyl sirolimus
1421
m/z = 345
fragment of 28-0-acetyl sirolimus
Me OM. Me Me
mlz = 589
the internal standard. For determination of the lower limit of
quantification, samples containing the following concentrations
were prepared: 0, 0.1, 0.25, 0.5, 1, 2.5, 5, and 10 jLg/L. The
lower limit of quantification was calculated as the percentage
deviation from the nominal concentration obtained by inverseprediction from the standard regression curve. For acceptance as
lower limit of quantification, the percentage deviation for a
certain concentration had to be <25% for at least 80% of the
samples.To assess a potential interference with the sirolimus degra-
dation products described by Wang et al. [8], these wereproduced by using the method described [8] with a few modifi-
cations: One milligram of sirolimus was dissolved in 100 L of
ethanol and incubated with 2 mL of 0.1 mol/L ammonium
acetate (pH 8). The degradation products were separated on a250 x 4 mm column filled with Hypersil C18 3-p.m material.
The flow rate was 0.7 mL/min and the same methanollO.05
mol/L ammonium acetate gradient as in the original method [8]was run. The UV-detector wavelength was set to 276 nm and
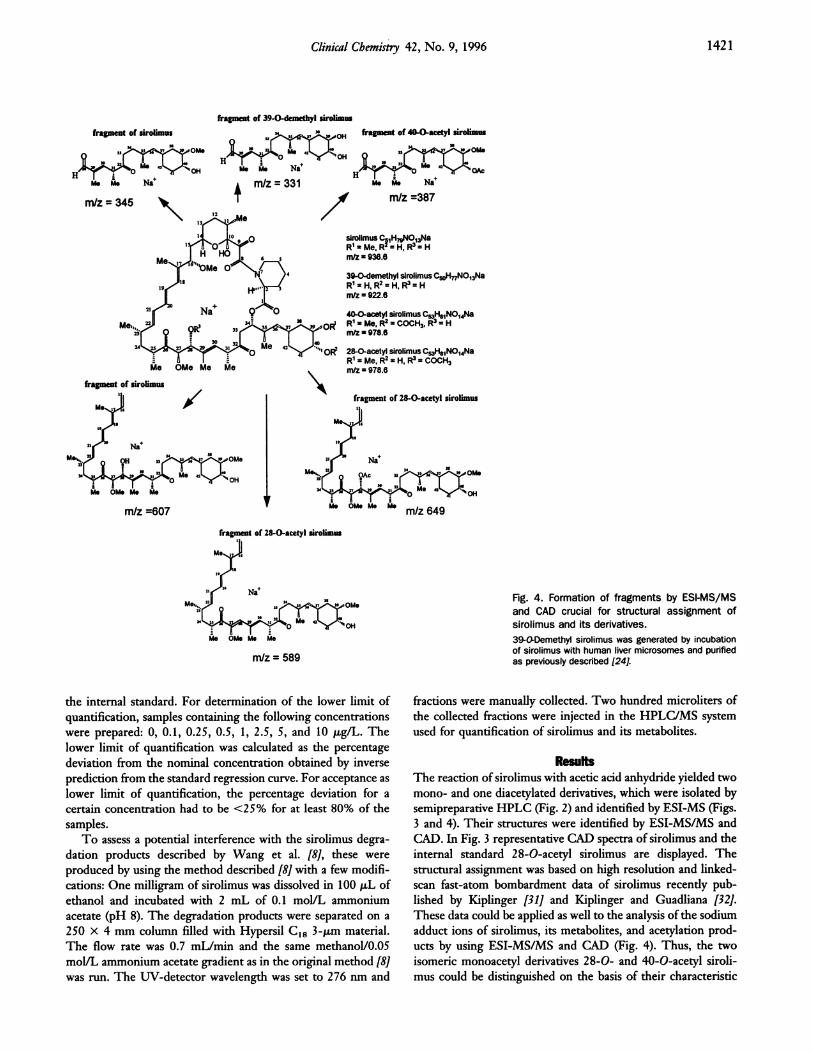
Fig. 4. Formation of fragments by ESI-MS/MSand CAD crucial for structural assignment ofsirolimus and its derivatives.39-O.Demethyl sirolimus was generated by incubationof sirolimus with human mmvermicrosomes and purifiedas previously described [24].
fractions were manually collected. Two hundred microliters of
the collected fractions were injected in the HPLC/MS system
used for quantification of sirolimus and its metabolites.
ResultsThe reaction of sirolimus with acetic acid anhydride yielded two
mono- and one diacetylated derivatives, which were isolated by
semipreparative HPLC (Fig. 2) and identified by ESI-MS (Figs.
3 and 4). Their structures were identified by ESI-MS/MS and
CAD. In Fig. 3 representative CAD spectra of sirolimus and the
internal standard 28-O-acetyl sirolimus are displayed. The
structural assignment was based on high resolution and linked-
scan fast-atom bombardment data of sirolimus recently pub-lished by Kiplinger [31] and Kiplinger and Guadliana [32].
These data could be applied as well to the analysis of the sodium
adduct ions of sirolimus, its metabolites, and acetylation prod-
ucts by using ESI-MS/MS and CAD (Fig. 4). Thus, the two
isomeric monoacetyl derivatives 2 8-0- and 40-0-acetyl siroli-
mus could be distinguished on the basis of their characteristic

120 r
100
80 I-
601-
40 F
20 I-
0
-0--
-0-
922 amu936 amu952 amu978 amu
0 62 4
Time (days)
Fig. 5. In-process stability of sirolimus, its metabolites, and theinternal standard 28-O-acetymsirolimus.Samples were prepared and analyzed as described in Materials and Methods.They were stored in the autosampler at room temperature. Concentrations werecalculated with an external sirolimus calibration curve. The results of days 1-7wereexpressed inpercentofthe concentrations measured right afterextraction(=100%). Each data point is the mean (SD) of five subsequent injections.
1422 Streit et al.: ESIJMS of sirolimus
fragments at m/z 589 and 387, respectively (Fig. 4). As checked
by HPLC/MS, the internal standard preparation was not con-taminated with sirolimus. When the internal standard solution
was added to blank blood samples, no material interfering with
the quantification of sirolimus or its metabolites was detected.
The stability of sirolimus, the internal standard, and two
metabolites are shown in Fig. 5. The concentrations measured at
different days were compared by analysis of variance combinedwith Duncan grouping (GLM procedure, SAS version 6.05),
which indicated significant differences (P <0.0001 for sirolimus
and all derivatives). Duncan grouping showed that the concen-
trations of sirolimus and 39-0-demethyl sirolimus at day 5 and
that the concentrations of all sirolimus derivatives at day 7 were
lower than those measured earlier. There was no significant
difference when the concentrations of sirolimus, 28-0-acetyl
sirolimus, and the metabolites measured on the same day were
compared with each other (analysis of variance). When the
concentrations were calculated by using the internal standard,
analysis of variance showed that the concentrations were equal
until day 5. Concentrations of sirolimus (P <0.04) and 39-0-
deinethyl sirolimus (P <0.03) measured at day 7 were signifi-cantly different from those during the first 5 days because of
signals close to the detection limit and unreliable quantification.
Thus, extracts containing sirolimus, the internal standard, and
sirolimus metabolites stored at room temperature in an au-
tosampler were stable for at least 3 days and allowed a reliablequantification until 5 days after sample preparation.
During the extraction procedure, 88.3 (26)% sirolimus
mean (SD), n = 10], 85 (l4.7)% 39-0-demethyl sirolimus, 90.6
(23)% hydroxy sirolimus,90.5 (25)% dihydroxy sirolimus,and
86.3 (lo.2)% internal standard were recovered. The recoveries
were not different from each other (analysis of variance). The
detection of positive ions proved to be 10 times more sensitive
than the detection of negative ions. In blood samples, sirolimus,
itsmetabolites,and the internal standard were mainly detected
as the sodium adduct [M+Na]: The relative intensity of
[M + H] ± was <5% of the sodium adduct. No fragments were
detected at a nozzle-skimmer voltage > -250 V. The [M + Na]were detected with the highest sensitivity at -200 V. At a
nozzle-skimmer voltage <-250 V, fragmentation into the two
main fragments [24] and several smaller fragments (<m/z250) was induced. Injection of 1 ng of sirolimus resulted in a
detector response of 4326 (745) areas [mean (SD), n = 6], of I
ng of 39-0-demethyl sirolimus in 3978 (545) areas, of I ng ofhydroxy sirolimusin4193 (264)areas,and of 1 ng oftheinternal
standard28-0-acetylsirolimusin4006 (305)areas.The detector
responses were equal (analysisof variance).At >500 mL/L
methanol in the mobile phase, sensitivity of sirolimus detectionwas independent of the mobile phase composition. Sirolimus
(retention time tR = 6.5 mm afterinjection),itsmetabolites(tR
= 3.8-5.4 mm), and the internalstandard (tR = 6.8 mm) were
eluted from the analyticalcolumn as differentpeaks. The
absolutelimitof detectiondefinedasthe signal-to-noiseratioof
3:1 after flow injection of sirolimus calibration solutions was 25pg. The lower limit of quantification after extraction from 1 mL
of blood, injection of 100 p.L of the extract into the HPLC
system, and elution from the analytical column was 250 pg forsirolimus, its metabolites 39-0-demethyl and hydroxy sirolimus,
and the internal standard. The calibration curve of sirolimus in
blood was linearfrom 0.25 to 250 p.g/L,withy = 0.91 (0.03)x+ 0.9 (1.8) [mean (SD); r = 0.98, P <0.0001]. Regression
analysisof the calibrationcurves of 39-0-demethyl, hydroxy,
and 28-0-acetylsirolimusgave the followingrespectiveresults:
y = 0.86 (0.04)x + 1.5 (0.8) (r = 0.97, P <0.0001),y = 1.03
(0.09)x- 0.5 (1.3) (r = 0.98, P <0.0001),andy = 0.95 (0.07)x-
1.1(2.1)(r= 0.98, P <0.0001). The accuracywas -2.5% (range
-17-10%, n = 10),+6.9% (range -18-19%, n = 10), and
-4% (range -22-7.2%, n = 6) for 1-mL blood samples to
which 1, 5, and 250 ng of sirolimus were added, respectively.
The inter- and intraassay variations at different sirolimus con-
centrations are listed in Table 1. The intraassay variation of
39-0-demethyl sirolimus was 10.3% [concentration 5.6 (0.6)mean (SD), n = 6] and the interassayvariation11.8%
[concentration 5.3 (0.6) p.g/L, n = 6];the intraassay variation ofhydroxy sirolimus was 9.5% [concentration 4.9 (0.5) p.g/L, n =
6] and the interassay variation 12.3% [concentration 4.7 (0.6)
n = 6].The run time of a sample was 8 mm and the
sample turnover time was 6 mm, since samples were injected 2
Table 1. Intra- and interassay variation of the measurement
of sirolimus concentrations in blood by HPLC/ESl-MS.Intrassay Interassay
n Mean (SD),p.EJL CV, % n Mean (SD),tg/L CV, %
10 0.96 (0.14) 15.4 10 1.1 (0.2) 19.5
10 4.6 (0.45) 9.9 10 4.7 (0.6) 12.8
10 14.6 (0.9) 59 7 14.8 (1.4) 9.3
8 39.6 (4.5) 11.4 8 41.3 (6) 14
6 247.3 (28.8) 11.6 6 241.7 (31) 13

4
6.07 12.25 22.822361601 176074 2228001 29.14 37.93
1 163717 215174
L9.23j is 26.39j. 35.0520441 7910
3.322298
44.1130791 9796
5 10 15 20 25
Fig. 6. HPLC/ESI-MS ion chromatogram of sirolimus and its
metabolites in five blood samples obtained from kidney
graft patients.
HPLC: 3.9 x 150 mm analytical column filled with 3-ljm C15material, isocratic elution with methanol/1% acetic acid (90/10 byvol), flow 0.4 mL/min. To save time, the next sample was injectedduring the run of the previous sample. All ions were detected assodium adducts IM+NaY. (A) total ion count, (B) 936.7 amu:sirolimus, (C) 978.7 amu: 28-O.acetyl sirolimus (internal standard),(D) 922.7 amu: demethyl sirolimus, )E) 952.7 amu: hydroxy siroli-mus.
Clinical Chemistry 42, No. 9, 1996 1423
mm before the end of the previous analysis. The HPLC/
ESI-MS system was stable for at least 200 subsequent injections
of blood sample extracts. No interferenceof sirolimusdegrada-
tion products with the quantification of sirolimus or its metab-
olites was detected.Sirolimus and its metabolites were quantified in blood of
kidney graft patients. Typical ion chromatograms of patients’
samples in blood are shown in Fig. 6.In blood at various times
after sirolimus application comprising peak as well as trough
concentrations, hydroxy (1.4-2 3 p.g/L), dihydroxy (2.2-11 p.g/
L), demethyl (0-15 p.g/L), and didemethyl (0-15 p.g/L) siroli-
mus were found. Sirolimus concentrations ranged from 3 to 42
p.g/L (n = 13). In trough blood samples, the metabolites
accounted for 56 (9)% [mean (SD)] of all sirolimus derivatives
measured with hydroxy sirolimus,reaching 71.8 (68)% of the
sirolimusconcentration,demethyl sirolimus35 (42)%, dihy-
droxy sirolimus20 (20)%, and didemethyl sirolimus20 (31)%.
The trough blood concentrations of sirolimus ranged from 3 to
26 p.g/L (n = 5).
DiscussionHPLC/ESI-MS represents a simple and sensitive technique for
the specific quantification of sirolimus and its metabolites in
blood and probably in other biological fluids as well. Analysis of
sirolimusiscomplicated by itsinstabilityand the formation of
conformational rotameres. Its instability [6] required long-term
storage of samples at -80 #{176}Cand the development of an
extraction procedure that avoided thermically induced degrada-tion of the sirolimusderivativessuch as evaporationsteps.In
previouslydescribedextractionprocedures[23, 24, 27], samples
had to be washed to remove material interfering with UV
detection before HPLC analysis. Such a step was unnecessary
forMS analysis.The conformationalrotameresof sirolimuscan
be incompletely separated on analytical HPLC columns leading
to broad peaks [26]. Peak broadening was avoided by using the
chromatographic conditions described by Napoli and Kahan
[26]. The specific mass spectrometric detection allowed quanti-
fication of hydroxylated and (or) demethylated metabolites. The
chromatographic method described was not able to discriminate
I I I I37.93
oO 8.07 12.25 22.82 29.14 30554339899
4.69 - 10.9438926 28321
D I5.45 1 36.56
12870 I 19.94 21.77 1060937.31 445
.- La_= J,,L1JC1-ie
19.87 28.26
936 41969 28359 38.49 44.18
:LT12

1424 Streit et al.: ESIIMS of sirolimus
metabolites with the same modifications in different positions.
The method was also not able to distinguish between the
‘3C-signal of hydroxylated and the ‘2C signal of demethylated
and hydroxylated metabolites such as hydroxy sirolimus and
dihydroxydemethyl sirolimus. Such metabolites can only be
differentiated by using time-consuming gradient elution [23-
25]. Since it was shown that in the HPLC/MS method de-
scribed, sensitivity of sirolimus detection is independent of the
composition of the methanol/water phase, it can be combined
with gradient elution to increase specificity of metabolite detec-
tion. Only the metabolites 39-O-demethyl and hydroxy siroli-
mus were availableforthisstudy. Therefore, only these metab-
olites were included in the method validation. Additionally,
didemethyl and dihydroxy sirolimus could be detected in blood
of patients. Quantification of these metabolites had to be based
on the assumption that their recoveries from blood, the calibra-
tion curves, and their ionization and detection in the MS was
similar to that of sirolimus, the internal standard, and the other
metabolites.
For quantification of the structurally related macrolide im-
munosuppressant tacrolimus and its metabolites, an MS method
based on a particle beam interface and chemical ionization has
been described [34, 35]. This technique could not be used for
sirolimus because of its extensive fragmentation during ioniza-
tion. The use of an internal standard was necessary to compen-
sate for losses during extraction, in-process instability of siroli-
mus and its metabolites, transport of extracted samples, and for
decreased sensitivity of mass spectrometric detection due to
contamination, especially of the electrospray interface. Acetyl-ated derivatives have been used for MS quantification of tacroli-
mus as well [34,35].They result in an m/z that, in contrast todemethyl sirolimus, which has also been used as an internal
standard for an HPLC assay[27],can clearlybe distinguished
from sirolimus and its metabolites. Internal standards other than
sirolimus derivatives such as tacrolimus or 13-estradiol-3-methylether [29] seem to be unsuitable since their stability during
storage and their in-process stability may be different from that
of sirolimus.In the present study, identification of the structures of the
acetylated sirolimus derivatives and the metabolites was based
on the fast-atom bombardment results described by Kiplinger
and Guadliana [32].High-energy single-collision CAD frag-mentation observed in magnetic sector instruments [32] might
differ from that observed in low-energy multiple-collision CAD
fragmentation in a triple-stage quadrupole instrument as used in
the present study. However, since fragmentation patterns cor-
responded to those observed by Kiplinger and Guadliana [32], it
could be assumed that during low- as well as high-energy CAD,
sirolimus and its derivatives were undergoing comparable frag-
mentation pathways.
The issue of whether to measure immunosuppressants in
plasma or blood has been discussed for cyclosporine and tacroli-
mus [36-38]. Because of their temperature-, concentration-, and
hematocrit-dependent distribution in blood and their high
affinity for the cellular components, blood is currently the
generally accepted matrix for these immunosuppressants. Since
almost 95% of sirolimus in blood is found in erythrocytes, blood
was recommended as the matrix for sirolimus as well [39] and
therefore chosen as the matrix in this study.Several metabolites isolated after in vitro metabolism of
sirolimus [24] and detected in bile of sirolimus-treated rats [25]
were present in the blood of kidney transplant patients. In
contrast to tacrolimus, which accounts for >80% of all tacroli-
mus derivatives in the blood of patients with stable liver
function, sirolimus metabolites add up to higher concentrations
than the unchanged drug.
Sirolimus has a low oral bioavailability and a narrow thera-
peutic range in animal models [22]. Its elimination is very likely
dependent on liver function, and drug-related side effects appear
to be trough concentration related [22]. Furthermore, sirolimusis metabolized by enzymes of the cytochrome P-450 3A sub-
family in the liver and small intestine [23, 24], with the potential
risk of numerous interactions at this level with drugs usually
administered after organ transplantation [40], resulting in mod-
ification of its trough blood concentrations. All this, as well asexperience with tacrolimus and cyclosporine, requires the clar-
ification of whether or not blood concentration-guided dose
adjustments and regular therapeutic drug monitoring of siroli-
mus will be necessary. HPLC/UV has been proposed as the
method of choice [22], mainly on the basis of animal studies[22, 41]; the trough and peak blood concentrations in patients
reported in our study are lower than those reported in animal
studies [42]. Furthermore, the metabolites have generally lower
concentrations [6, 42], which allows even lower doses resulting
in lower blood concentrations. In this regard, modification of
this HPLC/ESI-MS will allow quantification of cyclospormne
and sirolimus as well as their metabolites within one run. In
comparison with HPLC, HPLCIESI-MS requires less elaborateextraction of blood samples than HPLC/UV and allows quan-
tification of sirolimus and its metabolites within 6 mm. In
comparison, an HPLC/UV assay that is used for therapeuticdrug monitoring of sirolimus [29] takes >30 mm to quantify
sirolimus and does not determine its metabolites. HPLC/
ESI-MS allows analysis of an urgent sample within <1 h as well
as analysis of large numbers of samples for pharmacokmnetic
studies and therapeutic drug monitoring.
This study was supported by the Deutsche Forschungsgemein-
schaft, grant SFB 265/A7.
References1. Findlay JA, Radics L. On the chemistry and high field nuclear
magnetic resonance spectroscopy of rapamycin. Can J Chem1980;58:579-90.
2. Swindels DCN, White PS, Findlay JA. The X-ray crystal structure ofrapamycin,C51H79N013. Can J Chem 1978;56:2491-3.
3. McAlpineJB,Swanson SJ,JacksonM, WhitternDN. RevisedNMR
assignmentsofrapamycin.J Antibiot(Tokyo)1991;44:688-90.
4. Kessler H, Haessner R, Sch#{252}lerW. Structure of rapamycin: anNMR and moleculardynamics investigation.HeIv Chim Acta1993;76:117-30.
5. Sehgal SN, Baker H, V#{233}zinaC. Rapamycin (AY-22, 989), a newantifungal antibiotic. II. Fermentation, isolation and characteriza-tion. J Antibiot (Tokyo) 1975:28:727-30.
Clinical Chemistry 42, No. 9, 1996 1425
6. MorrisRE. Rapamycins:antifungal,antitumor,antiproliferative,and immunosuppressive macrolides. Transplant Rev 1992;6:39-
87.
7. Stella Vi, Kennedy PE. Prodrugs of rapamycin. US Patent no4,650,803, March 17, 1987.
8. Wang PC, Chan KW, Schiksnis RA, Scatina I, Sisenwine SF. Highperformance liquid chromatographic isolation, spectroscopic char-
acterization, and immunosuppressive activities of two rapamycindegradation products. I Liq Chromatogr 1994;17:3383-92.
9. V#{233}zinaC, Kudelski A, Sehgal SN. Rapamycin (AY-22, 989), a new
antifungal antibiotic. I. Taxonomy of the producing streptomycetesand isolation of the active principle. I Antibiot (Tokyo) 1975:28:
721-6.10. Baker H, SidorowiczA, Sehgal SN. Rapamycin (AY-22, 989), a new
antifungal antibiotic. Ill. In vitro and in vivo evaluation. I Antibiot(Tokyo) 1978:31:539-45.
11. Singh K, Sun S, V#{233}zinaC. Rapamycin (AY-22, 989), a new
antifungalantibiotic.IV. Mechanism of action. J Antibiot (Tokyo)
1979;32:630-45.
12. Eng CP, Sehgal SN, V#{233}zinaC. Activity of rapamycin (AY-22,989)against transplanted tumors. I Antibiot (Tokyo) 1984;37:1231-7.
13. Martell RR, Klicius I, GaletS. Inhibition of the immune response
by rapamycin, a new antifungal antibiotic. Can J Physiol Pharmacol1977;55:48-51.
14. Schreiber SL. Chemistry and biology of immunophilins and their
immunosuppressive ligands. Science 1991:251:283-7.15. Schreiber SL, Crabtree GR. The mechanism of action of cyclospo-
rin A and FK506. Immunol Today 1992;13:136-42.16. Dumont FJ, Staruch Mi, Koprak SL, Melino MR, Sigal NH. Distinct
mechanisms of suppression of murine T-celI activation by relatedmacrolides FK 506 and rapamycin. I Immunol 1990;144:251-8.
17. Kahan BD, Chang JY, Sehgal SN. Preclinical evaluation of a newpotent immunosuppressive agent, rapamycin. Transplantation1991;52:185-91..
18. Diioseph iF, Sharma RN, Chang JY. The effectofrapamycinonkidney function in the Sprague-Dawley rat. Transplantation 1992;
53:507-13.19. Almond PS, Moss A, Nakhleh RE. Rapamycin: immunosuppres-
sion, hyporesponsiveness, and side effects in a porcine renalallograftmodel.Transplantation1993;56:275-81.
20. Wang J,MorrisRE. Effectofsplenectomyand mono orcombina-tiontherapywith rapamycin, the morpholinoethyl ester of myco-phenolic acid and desoxysperguanilin on cardiac xenograft sur-vival. Transplant Proc 1991;23:699-702.
21. Fryer I, Yatscoff RW, Pascoe EA, Thliveris I. The relationship of
blood concentrations of rapamycin and cyclosporine to suppres-sion of allograft rejection in a rabbit heterotopic heart transplantmodel. Transplantation 1993;55:340-5.
22. Yatscoff R, Shaw L. Therapeutic drug monitoring of cyclosporine,FK-506, and rapamycin [Editorial]. Ther Drug Monit 1992;14:267-8.
23. Sattler M, Guengerich FP, Yun CH, Christians U, Sewing KF.Cytochrome P450 3A enzymes are responsibleforbiotransforma-tionofFK506 and rapamycin in man and rat. Drug Metab Dispos1992;20:753-61.
24. ChristiansU,SattlerM, SchiebelHM, KruseC, Radeke HH, LinckA, Sewing KF. Isolationof two immunosuppressivemetabolitesafter in vitrometabolism of rapamycin.Drug Metab Dispos1992;20:186-91.
25. Chan K, Wang P, Scatina I, et al. Characterization of biliary
rapamycin metabolites by ionspray liquid chromatography/massspectrometry [Abstract]. Proceedings of the 41st ASMS Confer-ence on Mass Spectrometty and Allied Topics, San Francisco, May31-June 4, 1993;545.
26. Napoli KL, Kahan BD. High-performance liquid chromatography ofrapamycin [Tech Briefi. Clin Chem 1991:37:294-5.
27. Yatscoff RW, Faraci C, Bolingbroke P. Measurement of rapamycinin whole blood using reverse-phase high-performance liquid chro-matography. Ther Drug Monit 1992;14:138-41.
28. Supko JG, Malspeis L. Dose-dependent pharmacokinetics ofrapamycin prodrug (NSC 506698) [Abstract]. Proc Am AssocCancer Res 1990;31:382.
29. Napoli KL, Kahan BD. Sample clean-up and high-performanceliquid chromatographic techniques for measurement of wholeblood rapamycin concentrations. I Chromatogr Biomed AppI1994;654:111-20.
30. Metcalfe SM, Richards FM. Cyclosporine, FK506 and rapamycin.Some effects on early activation events in serum-free, mitogen-stimulated mouse spleen cells. Transplantation 1990:49:798-802.
31. Kiplinger JP. Dilithiated fragments of a monolithiated precursorion? Unraveling linked scan spectra at constant B/E using labeledlithium ions. Rapid Commun Mass Spectrom 1993:7:320-2.
32. Kiplinger IP, Guadliana MA. Structural analysis of rapamycin andrelated compounds using [M+Li] ions generated by liquid sec-ondary ion mass spectrometry. Org Mass Spectrom 1994:29:445-53.
33. GuengerichFP. Microsomal enzymes involved in toxicology-analysis and separation. In: Hayes AW, ed. Principles and meth-
ods of toxicology. New York: Raven Press, 1982:609-37.34. Christians U, Braun F, Kosian N, Schmidt M, Schiebel HM, Ernst
L, et al. High performance liquid chromatography/mass spectrom-etry of FK506 and its metabolites in blood, bile and urine of livergrafted patients. Transplant Proc 1991:23:2741-4.
35. Christians U, Braun F, Schmidt M, Kosian N, Schiebel NM, ErnstL, et al. Specific and sensitive measurement of FK506 and itsmetabolitesinbloodand urine of liver-graft recipients. Clin Chem1992;38:2025-32.
36. Shaw LM, Bowers LD, Demers L, Freeman D, Moyer T, Sanghvi A,et al. Critical issues in cyclosporine monitoring: report of the TaskForceon CyclosporineMonitoring.ClinChem 1987;33:1269-88.
37. Kahan BD, Shaw LM, Holt D, Seltmann H, Venkataramanan R,Grevel I, Johnston A. Consensus document: Hawk’s Cay Meetingon therapeutic drug monitoring of cyclosporine. Clin Chem 1990;36:1510-6.
38. Winkler M, Ringe B, Baumann J, Loss M, Wonigeit K, Pichlmayr R.Plasma vs whole blood for therapeutic drug monitoring of patientsreceiving FK 506 for immunosuppression Clin Chem 1994:40:2247-53.
39. Yatscoff R, LeGatt D, Keenan R, ChackowskyP.Blooddistributionof rapamycin. Transplantation 1993;56:1202-6.
40. Pichard L, Fabre I, Fabre G, Domergue I, Saint Aubert B, MouradG, Maurel P. CyclosporinA drug interactions. Screening forinducers and inhibitorsof cytochromeP-450 (cyclosporinA oxi-dase) in primary cultures of human hepatocytes and liver micro-somes. Drug Metab Dispos1990:18:595-606.
41. HoncharikN, FryerI,YatscoffR.Pharmacokineticsofrapamycin:singledose studiesin rabbit. Ther Drug Monit 1992;14:475-8.
42. Kahan BD. Cyclosporine: the base of immunosuppressive thera-py-present and future. Transplant Proc 1993;25:508-10.





![TOP 10 RouterOS configuration mistakes - MikroTik · PDF filePresenter –Andis Arins andis[at]router.lv 2 MikroTik Consultant at MikroTik/ Microsoftcertified trainer Member of the](https://img.pdfslide.us/doc/110x75/5a79d4447f8b9ab05f8cc617/top-10-routeros-configuration-mistakes-mikrotik-andis-arins-andisatrouterlv.jpg)























