Embed Size (px)
Citation preview

Antenatal Testing: A Re-EvaluationCAROLINE SIGNORE, MD, MPH, AND CATHERINE Y. SPONG, MD
Guest Editors
T A B L E O F C O N T E N T S
Introduction Caroline Signore and Catherine Y. Spong ............................................. 231
Epidemiology of Stillbirth and Fetal Central Nervous SystemInjury Hamisu M. Salihu ................................................................................... 232
Normal Fetal Physiology and Behavior, and Adaptive Responses withHypoxemia Chester B. Martin Jr ......................................................................... 239
Fetal Movement Assessment J. Frederik Frøen, Alexander E.P. Heazell,Julie Victoria Holm Tveit, Eli Saastad, Ruth C. Fretts, and Vicki Flenady ................... 243
Antenatal Fetal Assessment: Contraction Stress Test, Nonstress Test,Vibroacoustic Stimulation, Amniotic Fluid Volume, Biophysical Profile, andModified Biophysical Profile—An Overview Lawrence D. Devoe ......................... 247
Fetal Doppler: Umbilical Artery, Middle Cerebral Artery, and VenousSystem Giancarlo Mari and Farhan Hanif ........................................................... 253
Monitoring of Fetal Well-Being: Role of Uterine ArteryDoppler Alessandro Ghidini and Anna Locatelli ................................................... 258
Assessing Cardiac and Neurological Maturation During the IntrauterinePeriod Curtis L. Lowery, R. B. Govindan, Pamela Murphy, and Hari Eswaran ...... 263
Antenatal Testing: Diabetes Mellitus Michael P. Nageotte ...................................... 269
Antepartum Testing in Patients with Hypertensive Disorders inPregnancy Roger K. Freeman .............................................................................. 271
Fetal Growth Restriction Jena Miller, Sifa Turan, and Ahmet A. Baschat ................. 274
Antenatal Fetal Assessment: Multifetal Gestation—AnOverview Lawrence D. Devoe ............................................................................... 281
Amniotic Fluid Abnormalities Christopher R. Harman ........................................... 288
Postdates and Antenatal Testing Michael Y. Divon and Noa Feldman-Leidner ......... 295
SEMINARS INPERINATOLOGY
V O L 3 2 , N O 4 A U G U S T 2 0 0 8

Antepartum Testing for Women with Previous Stillbirth Jonathan W. Weeks ........ 301
Management of Decreased Fetal Movements J. Frederik Frøen,Julie Victoria Holm Tveit, Eli Saastad, Per E. Børdahl, Babill Stray-Pedersen,Alexander E. P. Heazell, Vicki Flenady, and Ruth C. Fretts ........................................ 307
New Indications for Antepartum Testing: Making the Case for AntepartumSurveillance or Timed Delivery for Women of Advanced MaternalAge Ruth C. Fretts and Ugonna A. Duru ............................................................. 312
Antenatal Testing—Benefits and Costs Christina M. Scifres andGeorge A. Macones ................................................................................................. 318

Ambitftbpdtal
thderippco
nftmaAtIp
Volume 32, Number 4 August 2008
0d
Introduction
asIiwmik
Atncg
bhtmbop
ntepartum fetal testing aims to improve perinatal andpregnancy outcome, with the ultimate goal of reducing
ortality (fetal death) as well as morbidity, including cere-ral palsy and neonatal encephalopathy. Fetal death occurs
n 6.4/1000 pregnancies in the US, although it is anticipatedhat this is an underestimate. In half of these, antepartum riskactors are present and, of these, 25 to 75% may be amenableo prenatal modification. Cerebral palsy affects 2/1000 live-orn infants; neonatal encephalopathy occurs in 1.9 to 3.8er 1000 births and may result in permanent neurologicisability, as in cerebral palsy. In the vast majority of cases,he neurologic insults resulting in neonatal encephalopathyre felt to arise in the antepartum period, before the onset ofabor.
Electronic techniques for recording fetal heart rate pat-erns in labor were developed in the 1950s and were hoped toave great promise for identifying fetuses at risk for injury oreath, to allow preventive interventions. Use of intrapartumlectronic fetal monitoring (EFM) was widely adopted beforeigorous studies assessing its benefit were conducted. Withts use, the rate of cesarean delivery increased due to intra-artum EFM interpretation; however, the rates of cerebralalsy remained unchanged. Thus, the use of EFM did notonfer significant protection from fetal or newborn morbidityr mortality.Not long after the advent of intrapartum EFM, these tech-
ologies were applied to assessments of fetal well-being be-ore labor. With the introduction and increasing sophistica-ion of ultrasound fetal imaging and Doppler blood floweasurement techniques, a fairly wide armamentarium of
ntepartum fetal tests became available for clinical use.gain, however, the evidence base supporting their use and
he recommendation of one modality over another is limited.t is not clear which antenatal testing strategy best reduces
erinatal mortality and morbidity.146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.001
To review the current state of the art in antenatal fetalssessment and identify areas for further research, a work-hop was convened at the Eunice Kennedy Shriver Nationalnstitute of Child Health and Human Development (NICHD)n August 2007. Titled Antenatal Testing: A Reevaluation, theorkshop goals included describing indications and testingethodologies that are backed by sufficient evidence, and
dentifying those conditions and methods for which gaps innowledge and evidence still exist.Along with cosponsors the NIH Office of Rare Diseases, the
merican College of Obstetricians and Gynecologists, andhe American Academy of Pediatrics, the Pregnancy and Peri-atology Branch of NICHD invited 20 expert researchers andlinicians to summarize and present the latest evidence re-arding a spectrum of issues in antenatal testing:
● The epidemiology of antepartum stillbirth and neuro-logical injury
● Normal fetal physiology and fetal responses to intrauter-ine insults
● The technology and utility of existing and emerging fetalassessment methods
● Maternal and fetal indications for antenatal testing● Costs and benefits of antenatal testing
This issue of Seminars in Perinatology contains articlesased on the presentations given at the Workshop. It isoped that readers will appreciate the strengths and limita-ions of the existing evidence regarding antenatal fetal assess-ent and that the obstetrical and scientific communities will
e inspired to develop research protocols that will increaseur understanding of the optimal use of antenatal testing forrevention of perinatal morbidity and mortality.
Caroline Signore, MD, MPHCatherine Y. Spong, MD
Guest Editors
231

EFH
Swbadbtdh(timddoc
D
T
TA
2
pidemiology of Stillbirth andetal Central Nervous System Injuryamisu M. Salihu, MD, PhD
The epidemiology of stillbirth and fetal central nervous system (CNS) injury is describedwith some emphasis on maternal and feto-placental risk factors. To maximize utility of thediscussion and because it also represents the classical manifestation of fetal CNS injury,we have selected cerebral palsy (CP) to illustrate the epidemiologic aspects of injury to thefetal CNS in general. While trends in stillbirth rates have modestly decreased over time,those of CP seem to be increasing. Interestingly, both stillbirth and CP share traditional aswell as emerging risk factors lending credence to the hypothesis that fetuses that wouldpreviously have been stillborn are increasingly surviving albeit with some form of morbidity.The existence of shared risk factors also suggests that in some cases of stillbirth fetal CNSinjury precedes the in utero fetal demise. Pregnant women bearing these risk indicatorsrepresent potential candidates for appropriate and tailored protocols for antenatal fetaltesting.Semin Perinatol 32:232-238 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS epidemiology, stillbirth, cerebral palsy, risk factors
mtaee
EDSgvptwefrpFemefnd
tillbirth complicates about 1 in every 1000 viable preg-nancies,1,2 although rates vary across populations and
ithin population strata and rises with increase in fetal num-er.3 Worldwide, the World Health Organization estimatesbout 4 million stillbirths annually, and this is likely an un-erestimate because a significant proportion of home still-irth deliveries in developing settings go unrecorded.4 Whilehe epidemiology of stillbirth as a discrete entity has beenescribed and poorly understood factors of risk have beenighlighted,5 the interconnectedness between fetal mortalitystillbirth) and fetal morbidity in those fetuses that have sus-ained injuries but escaped death remains understudied. Thiss important because a recent theory has postulated a com-
on pathway shared by processes leading to both stillbirth,elayed death during infancy, and residual morbidity.6 Ad-itional evidence also supports the view that in certain casesf stillbirth fetal central nervous system (CNS) injury pre-eded the in utero fetal demise.7 It is therefore logical and
epartment of Obstetrics and Gynecology, and Department of Epidemiol-ogy and Biostatistics, University of South Florida, Tampa, FL.
his work was partially supported through a Young Clinical Scientist Awardto Dr. Hamisu Salihu by the Flight Attendant Medical Research Institute(FAMRI).
he funding agency did not play any role in any aspect of the study.ddress reprint requests to Hamisu Salihu, MD, PhD, COPH, 13201 Bruce
B. Downs Blvd., MDC 56, Tampa, FL 33612-3805. E-mail: hamisu.
[email protected]32 0146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1053/j.semperi.2008.04.002
ore useful to examine stillbirth and fetal morbidity underhe same conceptual framework since prevention strategiesre likely to be shared. In this article, we seek to discuss thepidemiology of stillbirth and fetal CNS injuries with somemphasis on risk factors, especially the emerging factors.
pidemiologyefinitions
tillbirth is defined as in utero fetal death at �20 weeks ofestation. Fetal central nervous system injuries encompass aariety of clinical (eg, cerebral palsy, epilepsy, etc) and patho-hysiologic syndromes (eg, periventricular leukomalacia, in-raventricular hemorrhage, neonatal stroke, etc) and it will beell beyond the scope of this endeavor to discuss each and
very entity. Cerebral palsy (CP) is the most common of alletal CNS injuries. It is the most common diagnosis amongeferred cases for pediatric rehabilitation.8 It also encom-asses the other clinical and pathophysiologic syndromes.or instance, 20 to 40% of children with CP suffer frompileptic episodes.9,10 Because CP represents the classicalanifestation of fetal CNS injury, we discuss this clinical
ntity to illustrate the epidemiologic aspects of injury to theetal brain in general. To this end, we define CP as a group ofonprogressive, but often changing, motor impairment syn-romes secondary to lesions or injuries of the brain arising at
ny time during brain development.
PAtbassdtsisof
i1at5wcsaSp41olnbUtT
1w1fvbp
cbsv2iWtbovitihpmc
RSMMM
able on
Epidemiology of stillbirth and fetal CNS injury 233
revalence and Trendsbout half of all perinatal deaths (from 20 weeks of gestation
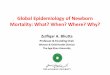
o age 1 year) occur in utero.11 Approximately, 25,000 still-irths on average are recorded annually in the US, and this isbout 10 times as high as deaths from sudden infant deathyndrome.12 Whereas rates of total stillbirths declined con-iderably and consistently from 1950 to 1990, only modestecreases in total stillbirths have occurred subsequently andhese have remained barely noticeable as a result of corre-ponding increases in early stillbirths (Fig. 1). The contrast-ng increases versus decreases in trends for early and latetillbirths, respectively, are indicative of the positive impactf advancement in perinatal technologies over the years onetal survival at later rather than earlier gestational ages.13
In contrast to stillbirth the prevalence of CP has been climb-ng from about 1.5/1000 live births in the 1960s to about 2.5/000 in the 1990s.14-18 The rise in the prevalence of CP has beenttributed to the increased survival of low birth weight and pre-erm infants. Low birth weight newborns now contribute about0% of all cases of CP and just over half of the most severe cases,hereas in the 1960s they accounted for one-third of all CP
ases and only one-sixth of the most severe.18 The rapid rise inurvival of infants with extremely low birth weight values mightlso have contributed to the increase in CP cases over time.alihu and coworkers examined the birth rate and survival ofreviable infants (defined as birth weight within the range 200-99 g) in the US comparing two cohorts, 1985 to 1988 versus995 to 1999.19 The authors noted a 100% rise in the birth ratef previable fetuses between the two periods (from 60.6 per 106
ive births to 131.9 per 106 live births). Survival beyond theeonatal period among these babies also increased considerablyy about 50% between the two periods (from 12.0 to 17.4%).sing modeling approaches, the investigators predicted that by
he year 2010 about one of four of these babies will be a survivor.
0
1
2
3
4
5
6
7
8
9
1990
1991
1992
1993
1994
1995
Ye
Feta
l mor
talit
y ra
te/1
000
Figure 1 Trends for total, early, and late stillbirth in thepublic access data files). (Color version of figure is avail
he rate of CP rises exponentially with falling birth weight: i
.1/1000 for birth weights �2500 g; 11.5/1000 for birtheights 1500 to 2499 g; 77/1000 for birth weights 1000 to499 g; and 90/1000 for birth weights �1000 g.20,21 It is there-ore logical that given the aforementioned projected rise in sur-ival of previable fetuses (who without intervention would haveeen stillborn), the current increase in CP should be expected toersist into the future.In a similar pattern the positive trend in the prevalence of CP
orrelates with the increase in the proportion of preterm liveirths and their survival. In a recent population-based cohorttudy, Vincer and coworkers noted that infant mortality amongery preterm infants decreased by about 55% between 1993 and002.22 Simultaneously, the CP rates among very preterm births
ncreased by about 125% (from 44.4/1000 to 100.0/1000).ithout the current improvement and advances in perinatal
echnology, most of these babies would have either been still-orn or been early neonatal deaths. Paradoxically, while the usef intrapartum fetal monitoring technology has significantly pre-ented unexpected intrapartum stillbirth, the expected positivempact of this technology on CP has not materialized. Clinicalrials have noted a significant increase in CP among pretermnfants followed during labor with electronic monitoring.23 Thisas led some to question whether in fact these already-injuredreterm infants would have simply died in utero but for the fetalonitoring,24 a good example of unavoidable and unintentional
onversion of mortality into morbidity.
isk Factors fortillbirth and Fetal CNS Injuryaternal Factorsaternal Ageaternal age has consistently been associated with stillbirth
6
1997
1998
1999
2000
TotalEarlyLate
States from 1990-2000 (constructed from the NCHSline.)
199
ar
United
n singleton pregnancies. The relationship between stillbirth

aewOrTiuiavospocpsttdia
itTaagv
PTtrntm(ltpbcswt
Uaangfias
ds
OTfuion3ecCsoustdia
awgHhwotdehtacnneaofu
mioas
RTeasch
234 H.M. Salihu
nd maternal age is U-shaped with elevated risks at the twoxtremes of reproductive age. The risk of stillbirth increasesith advancing maternal age in a dose-dependent pattern.25
ne obvious underlying cause is the greater-than-expectedates for fetal stillbirth-related anomalies among older women.26
he increased incidence of medical complications with agings also a factor. With advancing age, infertility sets in and these of Assisted Reproductive Technology to bear children
ncreases in a dose-effect fashion: 4.3, 18.3, 40, and 65%mong young (20-29 years old), mature (30-39 years old),ery mature (40-49 years old), and older mothers (�50 yearsld), respectively.25 Low maternal age is also a risk factor fortillbirth. In a most comprehensive study of stillbirth amongediatric gravidas (mothers aged 10-14 years), the authorsbserved elevated risk for stillbirth in this group with in-rease in fetal number.27 The suspected pathways amongediatric mothers are, however, different from those de-cribed for older gravidas. Biologic immaturity, factors linkedo preterm delivery, and unfavorable social environments arehe suggested pathways for in utero fetal demise among pe-iatric mothers.27 While the risk of stillbirth climbs with
ncrease in fetal number among teenagers,28 it decreases withscending fetal number among older mothers.25
Maternal age also seems to be a risk factor for fetal CNSnjury. Similar to the case for stillbirth, the relationship be-ween maternal age and CP follows a U-shaped distribution.he risk for CP has been reported to be significantly greatermong teen mothers as well as those mothers advanced forge.29 The risk for CP was estimated to be 30, 20, and 40%reater among teen (�19 years), mature (35-39 years), andery mature mothers (�40 years).29
arityhe association between parity and stillbirth follows a trajec-
ory similar to that noted for maternal age and stillbirth. Theisk of stillbirth is U-shaped with higher risk levels amongulliparous30 and extremely parous mothers.31 In a most de-ailed study among multiparous women categorized intooderately parous (1-4 previous live births), highly parous
5-9 previous live births), very highly parous (10-14 previousive births), and extremely parous (�15 previous live births),he risk of stillbirth climbed progressively with increasingarity.31 Further analyses among the extremely parous grouproken down into 15, 16, 17, and �18 previous live birthsonfirmed the dose–effect relationship between parity andtillbirth. The mechanism of stillbirth among highly parousomen is explained by the phenomenon of “uterine exhaus-
ion” because of persistent organ overuse.31
Fetal CNS injury seems to be associated with parity in a-shaped pattern as well, although data in this regard is nots consistent as for stillbirth. In a recent population-basednalyses covering 2303 infants born in Sweden with a diag-osis of CP compared with 1.6 million controls, the investi-ators observed a 20% higher likelihood for CP among in-ants of primiparous women (OR � 1.2; 95% confidencenterval � 1.1-1.3).29 In a review analyses, the rate of CPmong infants of women with parity �3 was found to be
ignificantly greater than expected.32 These findings are ad- bitional evidence suggesting a common shared pathway fortillbirth and fetal CNS injury.
besityhe relationship between gradations of obesity and in utero
etal demise was recently clearly demonstrated in a large pop-lation-wide study covering more than 1.5 million deliveries
n the United States.33 In doing so the authors categorizedbese mothers into the three typical obesity subclasses,amely, class I (BMI � 30.0-34.9); class II (BMI � 35.0-9.9), and extreme obesity (BMI �40). Overall, obese moth-rs were about 40% more likely to experience stillbirth asompared with nonobese gravidas (Hazards ratio � 1.4; 95%I � 1.3-1.5). The investigators also noted that the risk for
tillbirth increased in a monotonic fashion with ascendingbesity class (P � 0.01). Perhaps the most striking andnique finding of the study was the pronounced risk fortillbirth among black obese mothers when compared withheir white counterparts. Equally intriguing is that the blackisadvantage in stillbirth widened significantly with increase
n BMI, with the greatest black–white difference observedmong extremely obese mothers.
A number of hypotheses has been advanced to explain thedverse fetal outcomes associated with maternal obesity. It isell established that obese women are at elevated risk forestational diabetes mellitus and hypertensive disorders.3
owever, even in the absence of these complications, theeightened risk for adverse birth outcomes among obeseomen still persists.34,35 As compared with thinner womenbese mothers are less likely to perceive fetal kick counts sohat in case of diminished fetal movements preceding fetalemise thinner women are more likely to perceive the differ-nce and seek prompt medical care.3 Obese gravidas tend toave hyperlipidemia, which suppresses prostacyclin secre-ion while enhancing peroxidase production.36 This imbal-nce favors vasoconstriction and platelet aggregation, pro-esses that impede the maternal–fetal circulation, hamperingormal fetal growth and development. As compared withonobese mothers, obese pregnant women experience morextended periods of snoring during sleep with more frequentpnea-hypoxia incidents, leading to prolonged episodes ofxygen desaturation.37 This could reduce blood flow to theetus leading to fetal compromise and greater likelihood of intero fetal demise.It is well established that maternal obesity is related to fetalacrosomia and shoulder dystocia, which could lead to fetal
njuries and fetal distress at birth.38,39 Shoulder dystocia andbstetric maneuvers for shoulder release have been associ-ted with increased incidence of peripartal asphyxia and sub-equent cerebral palsy.40
ace/Ethnicityhe most pronounced disparity in stillbirth across racial/thnic groups is that between blacks and whites, especiallymong singleton births. For unknown probably biologic rea-ons, the black–white gap in stillbirth risk narrows with in-rease in fetal number in a dose-dependent fashion.41 Severalypotheses have been advanced to explain black–white still-
irth gap including disparity in socio-economic status, access
taraw
acoSbs
PTaaoneiatqmr
sgptsnlol
MHmettlapOs
pe
nrCbtwhedp
IRIprfbcTitbcevt
it2tsttfp
suivc
T
ININ
R
Epidemiology of stillbirth and fetal CNS injury 235
o quality care, preponderance of hypertensive disordersmong black mothers, and other obstetric complications. Aecent study is also suggestive that the high rate of obesitymong black women could be contributory to the black–hite disparity in stillbirth rates.33
Similar to the findings in stillbirth, black infant survivorsre more likely to develop CP later in life than their whiteounterparts.42 When these racial differences are examinedver time, the black–white gap appears stable but persistent.tudies of CP by race are relatively few and explanations forlack–white CP prevalence differentials have not yet beenufficiently explored.
renatal Smokinghere is evidence linking prenatal smoking and stillbirth,lthough the causal relationship between prenatal smokingnd adverse birth outcomes is frequently confounded byther maternal characteristics including race, socio-eco-omic status, as well as other unknown or immeasurablexposures that could potentially impact and modify the uter-ne environment. Further, gene–environment interaction isn important variable that influences fetal response to theoxic effects of in utero tobacco exposure.43 However, theuantification of gene–tobacco smoke effects is mostly noteasured in case-control study designs because of lack of
elevant data, especially, at the population level.The risk of CP is about 20% greater among infants of
moking mothers as compared with those of nonsmokingravidas.29 Such an association is biologically plausible sincerenatal smoking has also been associated with neuro-cogni-ive abnormalities including reduced intelligence in the off-pring.44 Synthesizing from the literature, it is possible that aumber of tobacco toxins could induce fetal CNS injuries
eading to brain cell deficit, impaired synaptic configuration,r failure of migration of neurons,45,46 processes that areinked to subsequent development of CP.
edical Conditionsypertension and diabetes mellitus are the most importantedical conditions associated with stillbirth. Over the years,
ffective and aggressive management protocols have reducedhe previously high levels of stillbirth rate attributable tohese conditions to rates that are modestly above populationevels.47 It appears that the elevated risk for stillbirth associ-ted with hypertensive disorders is mainly accounted for byreeclampsia/eclampsia rather than chronic hypertension.2
ther medical conditions associated with elevated risk fortillbirth include systemic lupus erythromatosis,48 thrombo-
able 1 Exploratory Pathway for the Association Between IVF
Preterm P Value
VF singleton 6.5% <0.0001on-IVF singleton 3.7%
VF twin 40% 0.004on-IVF twin 33.3%
eprinted with permission from Hvidtjørn and coworkers.60
hilias,49 high hemoglobin concentration,50 and thyroid dis-ase.51
Similar to stillbirth, maternal medical conditions in preg-ancy influence the development of fetal CNS injuries. Theisk of newborn encephalopathy (a precursor for subsequentP) is elevated 2-fold, 6-fold, and 10-fold among infantsorn to women with hypertension, severe preeclampsia, andhyroid disease, respectively.52 Infants of pregnant womenith diagnosed type 2 diabetes have a 100% higher likeli-ood for CP as compared with controls.29 There is somevidence linking thrombophilia in the mother or child to theevelopment of perinatal stroke and subsequent cerebralalsy.53,54
nfertility and Assistedeproduction Technology (ART)
nfertility per se is a risk factor for stillbirth. Spontaneousregnancies in untreated infertile women may be at higherisk for perinatal mortality than spontaneous pregnancies inertile women.55 About 1% of all babies and 18% of multipleirths born in the United States result from ART,56 and re-ently, the procedure has become a focus of increasing study.he risk of stillbirth among ART-conceived singleton births
s more than double that for spontaneously conceived single-ons.57 However, ART-conceived twins bear risks for adverseirth outcomes comparable to those of their spontaneouslyonceived counterparts.58 It is likely that the greater-than-xpected rates of derived singletons (resulting from earlyanishing of a co-twin) among ART-conceived singleton ges-ations might be contributory to these findings.
Similar to the findings in stillbirth, the risk for neurologicalmpairment in ART-conceived children is about four timeshat of naturally conceived children (OR � 3.7; 95% CI �.0-6.6).59 In tandem with comparable findings in stillbirth,he elevated risk for neurological complications is confined toingletons only while twins of both ART and natural concep-ions bear similar risk levels. Table 1 offers the pathwayhrough which ART could cause CP among vulnerableetuses by comparing prematurity versus in utero growtherturbation.60
Although the exact pathways remain poorly understood,ome aspects of the processes involved during ART or annderlying disorder linked to the infertility of couples receiv-
ng fertility treatments could to some extent explain the ele-ated risks for stillbirth and fetal CNS injury among ART-onceived infants.
and Fetal CNS Injury (cerebral palsy)
Preterm P Value SGA P Value
1.8% <0.0001 4.4% <0.00010.8% 3.2%9.5% 0.02 16.0% 0.68.2% 16.0%
-ICSI
Very

RSTofblsf(C4s
qtctptpetp
FMOorwo3bf
ttdoi9qcp1Masst
FSsob
flcpu
vfdmehepi
ic
UAtgspteccio
CWrowg
T
T
I
N
C
G
a
b
A
236 H.M. Salihu
ecurrence oftillbirth and Fetal CNS Injury
he risk for a subsequent stillbirth in a woman whose previ-us pregnancy ended in a stillbirth increases by 2- to 10-old.61,62 Even among women of low baseline risk, prior still-irth event elevates the risk for a subsequent stillbirth by at
east fourfold.63 History of stillbirth confers greater risk forubsequent early (fetal death between 20 and 28 weeks) thanor late stillbirth (fetal death at �29 weeks) [hazards ratioHR) � 10.3; 95% CI � 6.1 to 17.2 versus HR � 2.5; 95%I � 1.0 to 6.0]; and for intrapartum (HR � 12.2; 95% CI �.5-33.3) than for antepartum (HR � 4.2; 95% CI � 2.3-7.7)tillbirth.
In a similar fashion, the risk for CP recurrence in a subse-uent pregnancy increases fivefold,64 about the same magni-ude as for stillbirth recurrence.64 While persistent maternalonditions in subsequent pregnancies might be an explana-ion, the contribution of these factors do not sufficiently ex-lain stillbirth or fetal CNS morbidity recurrence. A recentheory offers an alternative and more convincing biologicathway based on molecular event memory mechanisms toxplain this recurrence.6 The theory provides a frameworkhat bears the potential for possible future intervention torevent stillbirth and fetal CNS morbidity recurrence.
eto-Placental Factorsultiple Pregnancyn average, the proportion of multiple births has increasedver the previous decades mostly as a result of a shift to theight of the maternal age distribution of pregnant women asell as the increasing use of artificial reproduction technol-gy for the treatment of infertility. Multiples now account for% of all births but 10% of all stillbirths.2 The risk for still-irth increases in a dose-dependent pattern with increase inetal number.3
Similarly, the rate of fetal CNS injury increases with mul-iple gestation. In a study encompassing 705 twin pairs (1410wins), 96 sets of triplets (287 triplets excluding one infanteath), and 7 sets of quadruplets (27 quadruplets excludingne infant death), Yokoyama and coworkers65 observed anncreasing trend of CP with rising fetal number in utero:/1000, 31/1000, and 111/1000 among twins, triplets, anduadruplets, respectively. Further, the risk for at least onehild having a CP within a multiple cluster also correlatedositively with fetal number: 15/1000; 80/1000, and 429/000 twin, triplet, and quadruplet clusters, respectively.ost of the data on CP in multiples have been conducted
mong twins only. The risk of CP in twins has also beenhown to be a function of the twin cluster phenotype asummarized in Table 2, with the greatest risk associated withhe co-twin of an affected twin sibling.66
etal Genderex of the fetus is associated with the occurrence of bothtillbirth and CP. The sexual difference in stillbirth has beenbserved in different populations and is therefore unlikely to
e artifactual.67,68 It has been postulated that this sexual dif- aerence might be mediated by physiologic variation at theevel of the maternal response to the conceptus, at the pla-enta, or may be as a result of sexual differences in fetalhysiology.69-72 However, the exact mechanism still remainsnclear.Similarly, fetal CNS injury comprising CP and related de-
elopmental disorders are more common in males than inemales. Most recently pooled data explain the disparity to beue to the greater vulnerability of the male fetus to whiteatter injury and intraventricular hemorrhage.73 Sex differ-
nces in hormonal influences on neuro-protection againstypoxia-ischemic injuries and gender-based intrinsic differ-nces in cell death pathways of growing neurons have beenostulated as likely reasons for greater risk of CP among male
nfants.73
Other feto-placental risk factors for stillbirth and fetal CNSnjury include infection,74,75 congenital malformations,76,77
ord anomalies,78-80 and placental abnormalities.81,82
nexplained Stillbirth and Fetal CNS Injurypproximately half of all stillbirths remain unexplained, and
he proportion of this category of stillbirth increases withestational age.5,83 Identified risk factors for unexplainedtillbirth include unappreciated fetal growth restriction,ostdates, advanced maternal age, suboptimal education at-ainment, primiparity and multiparity (�3), and the pres-nce of cord loops.84-86 Similarly, a significant proportion ofases of cerebral palsy remain unexplained, although the in-reasing use of sophisticated neuro-imaging techniques havemproved elucidation of pathologic pathways and timing ofccurrence of fetal CNS injury.77
onclusionhile the rate of stillbirth is modestly declining, that of ce-
ebral palsy, a consequence of fetal CNS injury, seems to ben the rise. The increasing survival of infants who in the pastould have been stillborn partly explains the rising trend. Arowing number of emerging risk factors for both stillbirth
able 2 Twinning and Incidence of Cerebral Palsy
Twin PhenotypeRate of CP(per 1000)
PValue
wins versus singletons 5.9 versus 1.8(4-fold increase)
<0.0001
n utero partial reduction 47 versus 4.8(10-fold increase)
<0.0001
eonatal partial reduction 63 versus 4.8(11-fold increase)
<0.0001
P of co-twina 118 versus 5.9(20-fold increase)
<0.0001
rowth discordanceb 7.7 versus 4.9(60% greater risk)
>0.05
The greatest risk for CP among twins.No difference between the smaller and the larger twin.dapted from Scher and coworkers.66
nd cerebral palsy are being uncovered. Pregnant women

bfi
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
Epidemiology of stillbirth and fetal CNS injury 237
earing these risk indicators represent potential candidatesor appropriate and tailored protocols for antenatal fetal test-ng.
eferences1. Martin JA, Hoyert DL: The national fetal death file. Semin Perinatol
26:3-11, 20022. Goldenberg RL, Kirby R, Culhane JF: Stillbirth: a review. J Matern Fetal
Med 16:79-94, 20043. Salihu HM, Aliyu MH, Rouse DJ, et al: Potentially preventable excess
mortality among higher-order multiples. Obstet Gynecol 102:679-684,2003
4. Mcclure EM, Nalubamba-Phiri M, Goldenberg RL: Stillbirth in devel-oping countries. Int J Gynecol Obstet 94:82-90, 2006
5. Fretts RC: Etiology and prevention of stillbirth. Am J Obstet Gynecol193:1923-1935, 2005
6. Salihu HM: Fetal loss repetition. Event memory hypothesis. Med Hy-potheses 70:567-571, 2008
7. Sims ME, Turkel SB, Halterman G, et al: Brain injury and intrauterinedeath. Am J Obstet Gynecol 151:721-723, 1985
8. Odding E, Roebroeck ME, Stam HJ: The epidemiology of cerebralpalsy: incidence, impairments and risk factors. Disabil Rehabil 28:183-191, 2006
9. Carlsson M, Hagberg G, Olsson I: Clinical and aetiological aspects ofepilepsy in children and cerebral palsy. Dev Med Child Neurol 45:371-376, 2003
0. Bruck I, Antonuik SA, Spessatto A, et al: Epilepsy in children withcerebral palsy. Arq Neuropsiquiatr 59:35-39, 2001
1. Centers for Disease Control and Prevention: Racial/Ethnic trends infetal mortality—United States, 1990-2000. MMWR Morb Mortal WklyRep 53:529-532, 2004
2. Centers for Disease Control and Prevention: National Center on BirthDefects and Developmental Disabilities. Available at: http://www.cdc.gov/ncbddd/bd/stillbirths.htm. Accessed July, 2007
3. Cnattingius S, Stephansson O: The epidemiology of stillbirth. SeminPerinatol 26:25-30, 2002
4. Pharoah PO, Cooke T, Johnson MA, et al: Epidemiology of cerebralpalsy in England and Scotland, 1984-9. Arch Dis Child Fetal NeonatalEd 79:F21-F25, 1998
5. Anonymous: The Scottish low birthweight study: I. Survival, growth,neuromotor and sensory impairment. Arch Dis Child 67:675-681,1992
6. Evans P, Elliott M, Alberman E, et al: Prevalence and disabilities in 4 to8 year olds with cerebral palsy. Arch Dis Child 60:940-945, 1985
7. Nordmark E, Hagglund G, Lagergren J: Cerebral palsy in southernSweden I. Prevalence and clinical features. Acta Paediatr 90:1271-1276, 2001
8. Colver AF, Gibson M, Hey EN, et al: Increasing rates of cerebral palsyacross the severity spectrum in north-east England 1964-1993. TheNorth of England Collaborative Cerebral Palsy Survey. Arch Dis ChildNeonatal Ed 83:F7-F12, 2000
9. Salihu HM, Emusus D, Aliyu ZY, et al: Survival of “pre-viable” infants inthe United States. Wien Klin Wochenschr 117:324-332, 2005
0. Liu JM, Li S, Lin Q, et al: Prevalence of cerebral palsy in China. Int JEpidemiol 28:949-954, 1999
1. Winter S, Autry A, Boyle C, et al: Trends in the prevalence of cerebralpalsy in a population-based study. Pediatrics 110:1220-1225, 2002
2. Vincer MJ, Allen AC, Joseph KS, et al: Increasing prevalence of cerebralpalsy among very preterm infants: a population-based study. Pediatrics118:e1621-e1626, 2006
3. Shy NE, Luthy DA, Bennett FC, et al: Effects of electronic fetal heart ratemonitoring as compared with periodic auscultation on the neurologicdevelopment of premature infants. N Engl J Med 322:588-593, 1990
4. Clark SL, Hankins GDV: Temporal and demographic trends in cerebralpalsy—fact and fiction. Am J Obstet Gynecol 188:628-633, 2003
5. Salihu HM, Shumpert MN, Slay M, et al: Childbearing beyond maternalage 50 and fetal outcomes in the United States. Obstet Gynecol 102:
1006-1014, 20036. Fretts RC, Usher RH: Fetal deaths in women in the older reproductiveage group. Contemp Rev Obstetr Gynecol 9:173-179, 1997
7. Salihu HM, Ekundayo OJ, Kristensen S, et al: Childhood pregnancy(10-14 years old) and risk of stillbirth in singletons and twins. J Pediatr148:522-526, 2006
8. Alexander MR, Salihu HM, Dwight RJ: Survival of triplets born toUnited States teenagers. Am J Obstet Gynecol 191:2097-2102, 2004
9. Thorngren-Jernick K, Herbst A: Perinatal factors associated with cerebralpalsy in children born in Sweden. Obstet Gynecol 108:1499-1505, 2006
0. Bai J, Wong F, Bauman A, et al: Parity and pregnancy outcomes. Am JObstet Gynecol 186:274-278, 2002
1. Aliyu MH, Salihu HM, Keith LG, et al: Extreme parity and risk ofstillbirth. Obstet Gynecol 106:446-453, 2005
2. Topp M, Langhoff-Roos J, Uldall P: Preterm birth and cerebral palsy.Predictive value of pregnancy complications, mode of delivery, andApgar scores. Acta Obstet Gynecol Scand 76:843-848, 1997
3. Salihu HM, Dunlop A-L, Alio AP, et al: Extreme obesity and risk ofstillbirth among black and white gravidas. Obstet Gynecol 110:552-557, 2007
4. Kristensen J, Vestergaard M, Wisborg K, et al: Pre-pregnancy weightand the risk of stillbirth and neonatal death. BJOG 112:403-408, 2005
5. Cnattingius S, Bergstrom R, Lipworth L, et al: Prepregnancy weight and therisk of adverse pregnancy outcomes. N Engl J Med 338:147-152, 1998
6. Stone JL, Lockwood CJ, Berkowitz GS, et al: Risk factors for severepreeclampsia. Obstet Gynecol 83:357-361, 1994
7. Maasilta P, Bachour A, Teramo K, et al: Sleep-related disordered breath-ing during pregnancy in obese women. Chest 120:1448-1454, 2001
8. Usha Kiran TS, Hemmadi S, Bethel J, et al: Outcome of pregnancy in awoman with an increased body mass index. BJOG 112:768-772, 2005
9. Cedergren MI: Maternal obesity and risk of adverse pregnancy out-come. Obstet Gynecol 103:219-224, 2004
0. Iffy L, Veradi V, Jakobovits A: Common intrapartum denominators ofshoulder dystocia Zentrabl Gynecol 116:33-37, 1994
1. Salihu HM, Kinniburgh BA, Aliyu MH, et al: Racial disparity in stillbirthamong singleton, twin and triplet gestations in the United States. Ob-stet Gynecol 104:734-740, 2004
2. Bhasin TK, Brocksen S, Avchen RN, et al: Prevalence of four develop-mental disabilities among children aged 8 years—Metropolitan AtlantaDevelopmental Disabilities Surveillance Program, 1996 and 2000.MMWR Surveill Summ 55:1-9, 2006
3. Wang X, Zuckerman B, Pearson C, et al: Maternal cigarette smoking,metabolic gene polymorphism, and infant birth weight. JAMA 287:195-202, 2002
4. Yolton K, Dietrich K, Auinger P, et al: Exposure to environmentaltobacco smoke and cognitive abilities among US children and adoles-cents. Environ Health Perspect 113:98-103, 2005
5. Volpe JJ: Overview: normal and abnormal human brain development.Ment Retard Dev Disabil Res Rev 6:1-5, 2000
6. Adams J, Barone S, LaMantia A, et al: Workshop to identify criticalwindows of exposure for children’s health: Neurobehavioral workgroup summary. Environ Health Perspect 108:533-544, 2000(suppl 3)
7. Smulian JC, Ananth CV, Vintzileos AM, et al: Fetal deaths in the UnitedStates: influence of high-risk conditions and implications for manage-ment. Obstet Gynecol 100:1183-1189, 2002
8. Simpson LL: Maternal medical disease: risk of antepartum fetal death.Semin Perinatol 26:42-50, 2002
9. Brenner B, Hoffman R, Blumenfeld Z, et al: Gestational outcome inthrombophilic women with recurrent pregnancy loss treated by enox-aparin. Thromb Haemost 83:693-697, 2000
0. Stephansson O, Dickman PW, Johansson A, et al: Maternal hemoglobinconcentration during pregnancy and risk of stillbirth. JAMA 284:2611-2617, 2000
1. Simpson LL: Maternal medical disease: risk of antepartum fetal death.Semin Perinatol 26:42-50, 2002
2. Badawi W, Kurinczuk JJ, Keogh JM, et al: Antepartum risk factors fornewborn encephalopathy: the Western Australian case-control study.
BMJ 317:1549-1553, 1998
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
7
7
7
7
7
8
8
8
8
8
8
8
238 H.M. Salihu
3. Nelson KB: Thrombophilias, perinatal stroke, and cerebral palsy. ClinObstet Gynecol 49:875-884, 2006
4. Gunther G, Junker R, Strater R, et al: Symptomatic ischemic stroke infullterm neonates: role of acquired and genetic prothrombotic riskfactors. Stroke 31:2437-2441, 2000
5. Allen VM, Wilson RD, Cheung A: Genetics Committee of the Society ofObstetricians and Gynaecologists of Canada (SOGC); ReproductiveEndocrinology Infertility Committee of the Society of Obstetricians andGynaecologists of Canada (SOGC). Pregnancy outcomes after assistedreproductive technology. J Obstet Gynaecol Can 28:220-250, 2006
6. Wright VC, Chang J, Jeng G, et al: Assisted reproductive technologysurveillance—United States, 2003. MMWR Surveill Summ 55:1-22,2006
7. Jackson RA, Gibson KA, Wu YW, et al: Perinatal outcomes in singletonsfollowing in vitro fertilization: a meta-analysis. Obstet Gynecol 103:551-563, 2004
8. Helmerhorst FM, Perquin DA, Donker D, et al: Perinatal outcome ofsingletons and twins after assisted conception: a systematic review ofcontrolled studies. BMJ 328:261-265, 2004
9. Strömberg B, Dahlquist G, Ericson A, et al: Neurological sequelae inchildren born after in vitro fertilisation: a population-based study. Lan-cet 359:461-465, 2002
0. Hvidtjørn D, Grove J, Schendel DE, et al: Cerebral palsy among chil-dren born after in vitro fertilization: the role of preterm delivery—apopulation-based, cohort study. Pediatrics 118:475-482, 2006
1. Greenwood R, Samms-Vaughan M, Golding J, et al: Past obstetric his-tory and risk of perinatal death in Jamaica. Paediatr Perinat Epidemiol8:40-53, 1994 (suppl 1)
2. Samueloff A, Xenakis EM, Berkus MD, et al: Recurrent stillbirth: signif-icance and characteristics. J Reprod Med 38:883-886, 1993
3. Stillbirth recurrence in a population of relatively low-risk mothers.Paediatr Perinat Epidemiol 21:24-30, 2007 (suppl 1)
4. Hemminki K, Li X, Sundquist K, et al: High familial risks for cerebralpalsy implicate partial heritable aetiology. Paediatr Perinat Epidemiol21:235-241, 2007
5. Yokoyama Y, Shimizu T, Hayakawa K: Prevalence of cerebral palsy intwins, triplets and quadruplets. Int J Epidemiol 24:934-938, 1995
6. Scher AI, Petterson B, Blair E, et al: The risk of mortality or cerebralpalsy in twins: a collaborative population-based study. Pediatr Res52:671-681, 2002
7. Gadow EC, Castilla EE, Lopez Camelo J, et al: Stillbirth rate and asso-ciated risk factors among 869 750 Latin American hospital births 1982-1986. Int J Gynaecol Obstet 35:209-214, 1991
8. Smith GCS: Sex, birth weight, and risk of stillbirth in Scotland, 1980-
1996. Am J Epidemiol 151:614-619, 20009. Rivers JP, Crawford MA: Maternal nutrition and the sex ratio at birth.Nature 252:297-298, 1974
0. Ayromlooi J, Essman WB: Sex differences in fetal sheep adrenal steroi-dogenesis. Int J Gynaecol Obstet 17:3-5, 1978
1. Padbury JF, Hobel CJ, Lam RW, et al: Sex differences in lung andadrenal neurosympathetic development in rabbits. Am J Obstet Gy-necol 141:199-204, 1981
2. Montano MM, Wang MH, Vom Saal SF: Sex differences in plasmacorticosterone in mouse fetuses are mediated by differential placentaltransport from the mother and eliminated by maternal adrenalectomyor stress. J Reprod Fertil 99:283-290, 1993
3. Johnston MV, Hagberg H: Sex and the pathogenesis of cerebral palsy.Dev Med Child Neurol 49:74-78, 2007
4. Goldenberg RL, Thompson C: The infectious origins of stillbirth. Am JObstet Gynecol 189:861-873, 2003
5. Wu YW, Escobar GJ, Grether JK, et al: Chorioamnionitis and cerebralpalsy in term and near-term infants. JAMA 290:2677-2684, 2003
6. Wapner RJ, Lewis D: Genetics and metabolic causes of stillbirth. SeminPerinatol 26:70-74, 2002
7. Blair E, Al Asedy F, Badawi N, et al: Is cerebral palsy associated withbirth defects other than cerebral defects? Dev Med Child Neurol 49:252-258, 2007
8. Airas U, Heinonen S: Clinical significance of true umbilical knots: apopulation-based analysis. Am J Perinatol 19:127-132, 2002
9. Collins JH: Umbilical cord accidents: human studies. Semin Perinatol26:79-82, 2002
0. Redline RW: Clinical and pathological umbilical cord abnormalities infetal thrombotic vasculopathy. Hum Pathol 35:1494-1498, 2004
1. Adelson P, Spurrett B, Trudinger B, et al: A New South Wales popula-tion-based study of stillbirths weighing 2,500 g or more. Aust NZ JObstet Gynaecol 33:166-173, 1993
2. Redline RW, Wilson-Costello D, Borawski E, et al: Placental lesionsassociated with neurologic impairment and cerebral palsy in very low-birth-weight infants. Arch Pathol Lab Med. 122:1091-1098, 1998
3. Fretts RC, Boyd ME, Usher RH, et al: The changing pattern of fetaldeath, 1961-1988. Obstet Gynecol 79:35-39, 1992
4. Huang DY, Usher RH, Kramer MS, et al: Determinants of unexplainedantepartum fetal deaths. Obstet Gynecol 95:215-221, 2000
5. Cnattingius S, Haglund B, Kramer MS: Differences in late fetal deathrates in association with determinants of small for gestational age fe-tuses: population based cohort study. BMJ 316:1483-1487, 1998
6. Divon MY, Haglund B, Nisell H, et al: Fetal and neonatal mortality inthe postterm pregnancy: the impact of gestational age and fetal growth
restriction. Am J Obstet Gynecol 178:726-731, 1998
NaC
Thacttndboltm
AtTs
D
A
0d
ormal Fetal Physiology and Behavior,nd Adaptive Responses with Hypoxemiahester B. Martin Jr, MD
The principal objective of antenatal testing is to detect fetal hypoxia before the fetus hassuffered lasting harm. This article summarizes some of the mechanisms by which fetaloxygen consumption is maintained under normal conditions, and adaptations that occur inresponse to hypoxemia. Alterations in the fetal heart rate are prominent in the fetalresponse to hypoxemia and are the basis of some methods of antenatal testing. Theprincipal mechanisms underlying these fetal heart rate changes are described. Adaptationsin the distribution of blood flow that permit the fetus to deal with reduced oxygen levels aresummarized. Developmental trends in fetal motility and behavior are outlined, and also howthese are modified by fetal growth retardation and maternal diabetes. Fetal movements aresuppressed during acute hypoxemia, but with gradually developing hypoxemia, normalmovement patterns may continue until the fetus becomes acidemic. This may limit the useof these biophysical variables in antenatal testing.Semin Perinatol 32:239-242 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS fetus:physiology, hypoxemia, movements, behavior, well-being
mhomurwdvtd
aOpee
fiop
sit
he principal objective of most antenatal testing is to de-tect fetal hypoxemia before the fetus has suffered lasting
arm or even death. Normal fetal physiology involves severaldaptations that permit the fetus to achieve a level of O2
onsumption similar to that in extrauterine life despite rela-ively low O2 tensions in fetal blood. Under normal condi-ions, in fact, O2 delivery to fetal tissues exceeds metaboliceeds. Other adaptations occur in the fetal heart rate, theistribution of the fetal blood flow, and also fetal motility andehavior when fetal O2 levels are reduced. Most of theseperate to favor fetal survival, at least when the insult isimited in severity and duration. Many of these latter adapta-ions can be detected clinically and can be useful in assess-ent of fetal well-being.
daptations that Contributeo Normal Fetal Oxygenationhe most important mechanism sustaining fetal O2 con-umption at levels similar to those in extrauterine life is the
epartment of Obstetrics and Gynecology, Division of Maternal-Fetal Med-icine, School of Medicine and Public Health, University of Wisconsin-Madison, Madison, WI.
ddress reprint requests to Chester B. Martin Jr, MD, Division of Maternal-Fetal Medicine, 6 Center, Meriter Hospital, 202 South Park Street, Mad-
gison, WI 53715. E-mail: [email protected]
146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.003
aintenance of high blood flow rates in fetal tissues. Theseigh flow rates are the result of the high fetal cardiacutput—250 to 300 mL/kg/min compared with approxi-ately 75 mL/kg/min in a resting adult. Important contrib-tors to the high fetal cardiac output are the high fetal heartate and the central shunting that allows the fetal ventricles toork largely in parallel rather than in series. Central intracar-iac shunting also directs the “best” fetal blood— umbilicalein blood bypassing the fetal liver via the ductus venosus—hrough the foramen ovale to the left heart for preferentialistribution to the brain and myocardium.Other factors frequently cited in maintaining fetal oxygen-
tion include high fetal hemoglobin concentrations and the
2 dissociation curve of fetal erythrocytes. The former ap-lies mainly in late pregnancy. The higher O2 affinity of fetalrythrocytes, while favoring O2 loading in the placenta, op-rates in the other direction in fetal tissues.
Changes in the fetal circulation play an important role in theetal adaptation to hypoxemia. The changes include changesn the fetal heart rate and redistribution of the fetal cardiacutput. The fetal cardiac output does not change during hy-oxemia in the absence of significant acidemia.In an intact fetus, the initial fetal heart rate response to
udden hypoxemia is slowing and increased variability. Thiss a chemoreceptor response mediated by the vagus nerve. Ashe hypoxemia is prolonged to 30 to 60 minutes, there is a
radual return of the heart rate toward or even above prehy-239

pco
wssmhowvs
libascatrhaad(i
rta13A“tephfSpphrtpddcfdrhrd
HBMprbaaog
hialdlctts
ptdmcs
ef
b
slpmmsfO
iatpdT
FAhu
240 C.B. Martin
oxemic levels. This is the result of increasing levels of cir-ulating epinephrine and norepinephrine, plus modulationf vagal activity by endogenous opiates.1
Although the gradual development of fetal tachycardiaithout preceding fetal heart rate slowing occurs clinically in
ome complicated pregnancies, tachycardia as an initial re-ponse to hypoxemia has not often been observed experi-entally, perhaps because the rate of reduction of O2 tensionas been too rapid. This explanation is supported by thebservations of Nijland and associates: in a group of fetuseshere the maternal fraction of inspired (FI) O2 was reducedery gradually, the fetal heart rate increased without an initiallowing.2
The role of the arterial chemoreceptors in the fetal circu-atory response to acute hypoxemia has been demonstratedn experiments comparing the changes in fetal heart rate,lood pressure, and blood flow in the carotid and femoralrteries between intact fetuses and those subjected to carotidinus denervation.3 In the intact fetuses, acute hypoxemiaaused an abrupt fall in both fetal heart rate and femoralrtery blood flow. The carotid sinus-denervated fetuses, onhe other hand, showed no significant change in fetal heartate and only a gradual fall in femoral blood flow during theour of hypoxemia—an effect of circulating vasoactivegents. Both groups showed a gradual rise in blood pressurend rather similar increases in carotid artery blood flow in-icating local (brain blood flow) and circulating humoralcatecholamines, other vasoactive substances) mechanismsn those responses.
Similar reflex mechanisms are involved in the fetal heartate response to phasic hypoxia produced by uterine contrac-ions. This was investigated by the use of autonomic blockinggents in fetal sheep.4 Phasic hypoxemia was produced by-minute occlusions of the uterine blood flow, repeated everyminutes. This produced “late” fetal heart rate decelerations.dministration of atropine converted the decelerations tolate accelerations,” demonstrating an adrenergic sympa-hetic response normally masked by the vagal cardiodecel-rator effect. This adrenergic component is important in sup-orting the fetal heart rate during hypoxemia, sinceypoxemia during beta-adrenergic blockade results in pro-ound slowing of the fetal heart rate and circulatory collapse.imultaneous blockade with atropine, phentolamine, andropranolol eliminated the fetal heart rate responses to thehasic hypoxemia in nonacidemic fetuses. On the otherand, when a fetus was made severely acidemic (pH 6.96) byepeated periodic occlusions combined with sustained par-ial reduction of uterine blood flow, administration of atro-ine had no effect on the depth and duration of the lateecelerations, demonstrating that under these conditions theecelerations were due to direct hypoxic depression of myo-ardial chronotropism. Some early observations in humanetuses showed that atropine reduced the amplitude of type 2ips (late decelerations) but did not eliminate them.5 Thus,eflex mechanisms are also involved in late decelerations inuman fetuses. It is likely that late decelerations are largelyeflex at first occurrence and progressively the result of car-
iac depression with increasing hypoxia and acidosis. typoxemia and Fetallood Flow Distribution
ost investigators have found no change in fetal cardiac out-ut with hypoxemia, despite the initial decrease in fetal heartate. The fetal circulation, however, responds to hypoxemiay redistribution of blood flow in favor of some organs andway from others (“centralization of the circulation”). This isccomplished by reflex (mainly adrenergic), local (eg, nitricxide, prostaglandins), and humoral (eg, catecholamines, an-iotensin, vasopressin, serotonin) mechanisms.
Those fetal organs showing increased blood flow duringypoxemia are brain, heart, and adrenals.6 In the brain, the
ncreased flow per 100 g tissue was greatest for the brainstemnd smallest for the cerebral hemispheres, with the cerebel-um being intermediate. Despite the increased flow rates, O2
elivery to the cerebrum and cerebellum was decreased at theowest O2 contents. The increases in blood flow to the myo-ardium and adrenals with hypoxemia were greater per 100 gissue than those to any of the brain divisions. O2 delivery tohe myocardium was maintained over the range of O2 contenttudied.
Blood flow to most other fetal organs—eg, kidney, spleen,ancreas, intestine, and carcass (skin and muscle)—tendedo remain relatively constant during mild hypoxemia and toecrease progressively as O2 content fell below about 1.5mol/L, or approximately 50 to 60% of the normal levels. In
onsequence, O2 delivery to those organs decreased progres-ively with decreasing O2 contents.6
Blood flow to the fetal lungs decreased rapidly and mark-dly below an O2 content of about 4 mmol/L, with littleurther change at lower O2 levels.6
Most investigators have found no change in fetal placentallood flow with hypoxemia.Studies in fetal sheep have demonstrated that the fetus can
ustain its protective circulatory adjustments during pro-onged hypoxemia (4 hours to 4 days) in the absence ofrogressive metabolic acidemia.7-10 Fetal O2 consumption isaintained and O2 delivery to the fetal brain is sufficient foretabolic requirements. With the development of progres-
ive metabolic acidosis, these protective adaptations begin toail, and at pH levels below 7.0 both whole fetal and cerebral
2 consumption fall substantially.7,10
That a similar pattern of blood flow redistribution occursn hypoxemic human fetuses can be inferred from the brainnd heart sparing seen in asymmetrical fetal growth retarda-ion and from the pattern of organ damage following intra-artum asphyxia. Changes in blood flow patterns can also beetected in human fetuses by means of Doppler ultrasound.his will be discussed later in this seminar.
etal Motility and Behaviorlternating periods of rest and activity can be observed inuman fetuses from the time of just detectable movementsntil term.11,12 In general, normal fetuses spend two to three
imes as much time in activity than in rest. Before 20 weeks,
poafswtpp
wllcwFpr
nfpgbifmnergmvq
mpfpHma
EFDsttpahatcd
cdbd
flttoahcdflwatpibpAhstm
tbpmdcss
R
Normal fetal physiology and behavior 241
eriods of absent movements are generally short, 6 minutesr less, but from 32 to 40 weeks the longest duration ofbsent movements in a cohort of healthy fetuses increasedrom 15.5 to 37 minutes.12 These developmental trendshould be kept in mind during ultrasound examinations andhen performing biophysical profiles and antenatal cardio-
ocograms (nonstress tests). For example, a 35- to 40-minuteeriod of fetal inactivity can be normal at 40 weeks but isrobably not normal at 32 weeks and earlier.Fetal motilities are linked. For example, during epochs
hen the fetus is making body movements, it is also moreikely to exhibit breathing and eye movements. It is also moreikely to show a “reactive” fetal heart rate pattern with in-reased variability and accelerations. This linkage increasesith increasing gestational age, especially after 36 weeks.etal breathing movements are about twice as likely to beresent during epochs when the fetal heart rate pattern iseactive than during nonreactive periods.13
Late in the third trimester—36 to 38 weeks in fetuses oformal multiparas and 38 to 40 weeks in healthy nulliparas—etal body movements, eye movements, and fetal heart rateatterns become even more tightly linked with the emer-ence of fetal behavioral states.12,14 Behavioral states are com-inations of particular conditions of variables that are stable
n time and recur. These combinations can be observed be-ore states emerge, but to accept the presence of states there
ust be temporal stability of the combinations and simulta-eous change of the state variables at state transitions. Themergence of fetal behavioral states is disturbed in growth-etarded fetuses and fetuses of even well-controlled diabeticravidas.15,16 From the standpoint of antenatal testing, theost obvious indication that behavioral states have not de-
eloped in late pregnancy is interruption of periods of fetaluiescence by brief bouts of fetal body movements.Fetal brain function can be assessed by observation of fetalotility, fetal behavior, and fetal heart rate variability. Op-ortunities include observation of the variety and vigor ofetal movements during ultrasound examinations or bio-hysical profiles as well as antenatal cardiotocography.ealthy fetuses exhibit a varied repertoire of vigorous move-ents, whereas sick fetuses are more likely to show sluggish
nd stereotyped movements.
ffects of Hypoxemia onetal Motility and Behavioruring acute hypoxemia produced experimentally in fetal
heep, the fetus “powers down”: Fetal movements, includingrunk, limb, breathing, and eye movements, are suppressed,hus reducing fetal O2 needs, and the electrocortical activityattern switches to a high-voltage synchronized one associ-ted with lower O2 uptake.17-20 More prolonged observation,owever, has demonstrated that the decrease in biophysicalctivity in response to moderate hypoxemia shows adapta-ion with return to normal levels after several hours despiteontinuing hypoxemia.21,22 Also, when fetal hypoxia was in-
uced very gradually over 4 days, there was no significanthange in the biophysical variables until the fetuses began toevelop metabolic acidemia.23 Thus, observation of fetalreathing and body movements during a biophysical profileoes not guarantee that the fetus is not hypoxemic.Fetal heart rate accelerations are highly associated with
etal movements, but neuromuscular blockade with gal-amine in fetal sheep only reduced the incidence of accelera-ions by 36%, with no change in their amplitude or dura-ion.24 Therefore, the majority of fetal heart rate accelerationsccur as a result of central nervous system output rather thans a consequence of fetal movements. The occurrence of fetaleart rate accelerations during cardiotocography is generallyonsidered reassuring. However, during the course of fetaleterioration in chronically instrumented rhesus monkeys,etal heart rate accelerations were still present at the onset ofate fetal heart rate decelerations. At this time the fetal pO2
as decreased, but the pH was not. When fetal heart rateccelerations disappeared, the fetal pO2 had decreased fur-her and metabolic acidemia was present.25 In fetal sheep,rolonged hypoxemia in the absence of acidemia led to an
nitial increase in the number of fetal heart rate accelerations,ut after 12 hours the fetal heart rate had returned to normalatterns indistinguishable from those of normoxic fetuses.26
reactive nonstress test, therefore, also does not rule out fetalypoxemia. Thus, a provocative test such as the contractiontress test may detect developing fetal hypoxemia earlier thanests that depend on the biophysical variables of fetal move-ents and heart rate accelerations.Once acidemia has developed, the rate of fetal deteriora-
ion can accelerate. Lowering the pH shifts the oxyhemoglo-in dissociation curve to the right, reducing O2-carrying ca-acity and aggravating the hypoxemia. In diabetic gravidas,oreover, hyperglycemia favors increased fetal lactate pro-uction, thus amplifying the acidemia. Deepening acidosisan lead eventually to circulatory failure and fetal death. Thisequence is probably responsible for many “unexplained”tillbirths following apparently normal antenatal testing.
eferences1. LaGamma EF, Itskovitz J, Rudolph AM: Effects of naloxone on fetal
circulatory responses to hypoxemia. Am J Obstet Gynecol 143:933-940, 1982
2. Nijland R, Jongsma HW, Nijhuis JG, et al: Arterial oxygen saturation inrelation to metabolic acidosis in fetal lambs. Am J Obstet Gynecol172:810-819, 1995
3. Giussani DA, McGarrigle HH, Spencer JA, et al: Effect of carotid dener-vation on plasma vasopressin levels during acute hypoxia in the late-gestation fetal sheep. J Physiol 477:81-87, 1994
4. Martin CB Jr, de Haan J, van der Wildt B, et al: Mechanisms of latedecelerations in the fetal heart rate: a study with autonomic blockingagents in fetal lambs. Eur J Obstet Gynecol Reprod Biol 9:361-373,1979
5. Mendez-Bauer C, Poseiro JJ, Arellano-Hernández G, et al: Effects ofatropine on the heart rate of the human fetus during labor. Am J ObstetGynecol 85:1033-1053, 1963
6. Peeters LLH, Sheldon RE, Jones MD Jr, et al: Blood flow to fetal organsas a function of arterial oxygen content. Am J Obstet Gynecol 135:637-646, 1979
7. Rurak DW, Richardson BS, Patrick JE, et al: Oxygen consumption inthe fetal lamb during sustained hypoxemia with progressive acidemia.
Am J Physiol 258:R1108-R1115, 1990
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
242 C.B. Martin
8. Rurak DW, Richardson BS, Patrick JE, et al: Blood flow and oxygendelivery to fetal organs and tissues during sustained hypoxemia. Am JPhysiol 258:R1116-R1122, 1990
9. Bocking AD, White SE, Homan J, et al: Oxygen consumption is main-tained in fetal sheep during prolonged hypoxaemia. J Dev Physiol 17:169-174, 1992
0. Richardson BS, Rurak D, Patrick JE, et al: Cerebral oxidative metabo-lism during sustained hypoxaemia in fetal sheep. J Dev Physiol 11:37-43, 1989
1. de Vries JI, Visser GHA, Prechtl HFR: The emergence of fetal behaviour.II. Quantitative aspects. Early Hum Dev 12:99-120, 1985
2. Nijhuis JG, Prechtl HFR, Martin CB Jr, et al: Are there behavioural statesin the human fetus? Early Hum Dev 6:177-195, 1982
3. van Vliet MAT, Martin CB Jr, Nijhuis JG, et al: The relationship betweenfetal activity and behavioral states and fetal breathing movements innormal and growth-retarded fetuses. Am J Obstet Gynecol 153:582-588, 1985
4. van Vliet MAT, Martin CB Jr, Nihjuis JG, et al: Behavioural states in thefetuses of nulliparous women. Early Hum Dev 12:121-135, 1985
5. van Vliet MAT, Martin CB Jr, Nihjuis JG, et al: Behavioral states ingrowth-retarded human fetuses. Early Hum Dev 12:183-197, 1985
6. Mulder EHJ, Visser GHA, Bekedam DJ, et al: Emergence of behaviouralstates in the fetuses of type-1 diabetic women. Early Hum Dev 15:231-252, 1987
7. Boddy K, Dawes GS, Fisher R, et al: Foetal respiratory movements,electrocortical activity and cardiovascular responses to hypoxaemia
and hypercapnia in sheep. J Physiol 243:599-618, 19748. Natale R, Clewlow F, Dawes GS: Measurement of fetal forelimb move-ments in the lamb in utero. Am J Obstet Gynecol 140:545-551, 1981
9. Bocking AD, Harding R: Effects of reduced uterine blood flow on elec-trocortical activity, breathing and skeletal muscle activity in fetal sheep.Am J Obstet Gynecol 154:655-662, 1986
0. Richardson BS, Patrick JE, Abdulijabbar H: Cerebral oxidative metab-olism in fetal sheep: relationship to electrocortical activity state. Am JObstet Gynecol 153:426-431, 1985
1. Koos BJ, Kitanaka T, Matsuda K, et al: Fetal breathing adaptation toprolonged hypoxaemia in sheep. J Dev Physiol 10:161-166, 1988
2. Bocking AD, Gagnon R, Milne KM, et al: Behavioral activity duringprolonged hypoxemia in fetal sheep. J Appl Physiol 65:2420-2426,1988
3. Richardson BS, Carmichael L, Homan J, et al: Electrocortical activity,electroocular activity, and breathing movements in fetal sheep withprolonged and graded hypoxemia. Am J Obstet Gynecol 167:553-558,1992
4. Bocking AD, Harding R, Wickham PJ: Relationship between accelera-tions and decelerations in heart rate and skeletal muscle activity in fetalsheep. J Dev Physiol 1:47-54, 1985
5. Murata Y, Martin CB Jr, Ikenoue T, et al: Fetal heart rate accelerationsand late decelerations during the course of intrauterine death in chron-ically catheterized rhesus monkeys. Am J Obstet Gynecol 144:218-223,1982
6. Bocking AD, White S, Gagnon R, et al: Effect of prolonged hypoxemiaon fetal heart rate accelerations and decelerations in sheep. Am J Obstet
Gynecol 161:722-727, 1989
FJJa
FS
Mwuamtsmc
*
†
‡
§
�
¶
T
A
0d
etal Movement Assessment. Frederik Frøen, MD, PhD,*,† Alexander E.P. Heazell, MBChB(Hons),‡
ulie Victoria Holm Tveit, MD,§ Eli Saastad, RN, Rm, MSc,*,� Ruth C. Fretts, MD, MPH,†
nd Vicki Flenady, RN, Rm, MMedSc¶
Maternal perception of fetal movements is the oldest and most commonly used method toassess fetal well-being. While almost all pregnant women adhere to it, organized screeningby fetal movements has seen variable popularity among health professionals. Early resultsof screening were promising and fetal movement counting is the only antepartum testingmethod that has shown effect in reducing mortality in a randomized controlled trialcomparing testing versus no testing. Although awareness of fetal movements is associatedwith improved perinatal outcomes, the quest to define a quantitative “alarm limit” to definedecreased fetal movements has so far been unsuccessful, and the use of most such limitsdeveloped for fetal movement counting should be discouraged.Semin Perinatol 32:243-246 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS fetal movement, fetal monitoring, methods, stillbirth
Tiwppa
shAbpupiaFifttehpbwmo
etal Movements as aign of Fetal Well-Being
aternal perception of fetal movements (FM) is the old-est and most commonly used method to assess fetal
ell-being.1 In most communities today, it is performed asnstructured screening to which almost all pregnant womendhere. Among women who have delivered a live-born baby,ore than 99% agreed with the statement that it was impor-
ant to them to feel the baby move every day.2 When theycreen themselves as “positive” for decreased fetal move-ents (DFM), most will present their concerns to their health
are provider with the expectation of further evaluations.
Division of Epidemiology, Norwegian Institute of Public Health, Oslo,Norway.
Brigham and Women’s Hospital, Division of Maternal-Fetal Medicine,Harvard Medical School, Boston, MA.
Maternal and Fetal Health Research Group, University of Manchester,Manchester, UK.
Department of Obstetrics and Gynecology, and Center for PerinatalResearch, Rikshospitalet-Radiumhospitalet, Universty of Oslo, Oslo,Norway.
Akershus University College, Lillestrøm, Norway.Centre for Clinical Studies, Mater Mothers’ Hospital, School of Medicine,
University of Queensland, Brisbane, Australia.his work was supported in part by The Norwegian Research Council, The
Norwegian Women’s Public Health Association, The Norwegian MedicalAssociation, and Unexpected Child Death Society of Norway.
ddress reprint requests to J. Frederik Frøen, MD, PhD, Norwegian Instituteof Public Health, P.O. Box 4404 Nydalen, N-0403 Oslo, Norway. E-mail:
146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.004
here is little doubt that normal FM are a highly specificndicator of fetal viability, and conversely, as we discuss else-here in this issue of Seminars in Perinatology, that womenresenting with DFM are at increased risk of perinatal com-lications, specifically, stillbirth, fetal growth restriction, andssociated conditions.
Despite the popularity among women, formal or organizedcreening of FM has seen very variable popularity amongealth professionals through the last decades.1 One in sixustralian obstetricians and one in three UK obstetricianselieve screening of FM is of no benefit,3 and many contem-orary guidelines for antenatal care actively discourage these of formal fetal movement counting (FMC).4,5 The pur-ose of FMC may be broadly divided into two understand-
ngs: on one hand, it may be an organized effort to promotewareness among pregnant women and ensure vigilance toM on a daily basis, and thus, to support the ongoing screen-
ng by subjective perceptions of DFM. Alternatively, a moreormal approach to FMC is to implement a structured chartogether with specified quantitative “alarm limits,” or defini-ions of DFM. If these “alarm limits” are reached, women arexpected to present their concerns regarding DFM to theirealth care provider. This latter approach to FMC was ex-ected not only to bring along the improved awareness of FMut also to substitute fallible subjective maternal perceptionsith objective measures of DFM. Neither of the two imple-entations of FMC would introduce a “new” screening but
nly attempt to improve the value of the existing “self-screen-
ng” performed by pregnant women. Although the latter un-243

ddt
sm
SSbTppFpiZ1afieTilpoaraitsWqfbrHdr
poslFcipapcvhci
wctc
utatwlMtcteTagu
MLFTormcm“umoarmnmFctwappsw
puaif
244 J.F. Frøen et al
erstanding of formal FMC has been favored in research, theesign of the research undertaken has purposely or acciden-ally been unable to separate these two effects.
In this article we aimed to review the effects of FMC intillbirth prevention and to discuss which aspects of FMCay be beneficial and which are probably not.
tudies oftillbirth Preventiony Fetal Movement Counting
here have only been two studies in total populations (allregnancies) and two studies in mixed low-risk and high-riskopulations evaluating the effect of FMC for all versus noMC. In the total population studies, both were conducted asrospective cohorts with a control period followed by an
ntervention period. In 1986, Westgate and Jamieson in Newealand reported a relative risk of stillbirth of 0.76 (0.55-.04), and 0.56 (0.35-0.90) for stillbirths perceived as avoid-ble.6 In 1989, Moore and Piacquadio in the US reported therst part of their study, and in 1990, the final results, with thequivalent risks as 0.42 (0.23-0.76) and 0.25 (0.07-0.88).7,8
he two studies in mixed populations were both conductedn single institutions. In 1983, Neldam in Denmark pub-ished the final results of his randomized controlled trial9,10 asart of his PhD thesis from 1986.11 He reported a relative riskf stillbirth, and of avoidable stillbirths, of 0.25 (0.07-0.88)nd 0.27 (0.08-0.93), respectively. This is, in fact, the onlyandomized controlled trial to date of antepartum testing ofny kind versus no testing that has reported reduced mortal-ty. However, as the randomization procedure was based onhe mother’s initial booking number (even or odd numbers),ome investigators find the study methodologically flawed.12
e postulate that the probability of manipulation of the se-uence in which pregnant women were referred and bookedor antenatal care at the National Hospital of Copenhagen toe exceedingly small. In 1985 Lobb and coworkers in the UKeported the comparison of two units at Liverpool Maternityospital with “competing” protocols based on a preexistingifference in protocol, and the unit advocating FMC had theelative risks of 0.92 (0.6-1.35) and 0.86 (0.49-1.52).13
Yet, such encouraging results from cohort studies of wholeopulations and a randomized controlled trial have beenvershadowed by negative findings from a study that de-erves further discussion. In 1989 Grant and coworkers pub-ished a large cluster-randomized controlled trial comparingMC in a total population versus FMC only for risk pregnan-ies in the same population.14 They found no effect of theirntervention. Although this was not a study of FMC com-ared with no FMC, it is without doubt the most referencednd influential1 publication on FMC and is often misinter-reted as evidence against FMC in guidelines for antepartumare.4,5 The use of FMC in both arms of the study (for allersus for risk pregnancies), as well as the use of “withinospital” clusters, in which pregnant women in the sameommunity were either urged to perform FMC or informed
n writing about their inclusion in a FMC study in which they oere not supposed to count FM, must have led to significantontamination between the groups. Overall, perinatal mor-ality decreased during their study period, falling to 2.8/1000ompared with 4/1000 before the intervention.
In the cluster-randomized trial, the mean time participantssed to count their requested 10 FM was 162 minutes, andhe “alarm limit” for when to contact health professionals wasbsence of FM for 1 day or less than 10 FM in 10 hours forwo consecutive days. Only 60% of women were compliantith daily counting, and one in two compliant to the alarm
imits among the 8.4% that reported DFM.14 In comparison,oore and Piacquadio reported the same year that the mean
ime to count to 10 was 20 minutes with a compliance toounting of 94%, and 15.5% of women reported DFM. Inheir study, women were instructed to present for furthervaluations if they had not perceived 10 FM within 2 hours.7
his evokes the next question: are these two interventions atll comparable? It is unlikely that both of these methodolo-ies are equally suitable for screening purposes in total pop-lations.
ethods and Alarmimits for Maternaletal Movement Counting
he concept of maternal FMC in the third trimester is basedn the presumption that maternal perception of FM accu-ately reflects fetal activity or at least gross fetal body or limbovements. A range of methodologies from piezo-electric
rystals to ultrasound scanning have been used for objectiveeasures of FM, but every method has its limitations and a
gold standard” is difficult to define. In comparison with theltrasound, the mean proportion of FM perceived by theother ranges from 37 to 88%,15-23 and in comparison with
ther methodologies from 39 to 90%16,21,24-27; strong gener-lized FM were perceived in the higher end of this scale. Withespect to generalized FM, there is close agreement betweenaternal and objective measures of FM, increasing with theumber of fetal parts contributing to it.17-19,23 The one com-on factor in these studies is that maternal perception ofM was recorded while the mother was lying down and fo-using on FM. This is the only situation in which we knowhat maternal perception of FM has a fair to good correlationith actual fetal activity. Outside such a setting, both the
ctual frequency of FM as well as the mother’s ability toerceive them is affected by many factors such as maternalosition,28,29 activity and exercise,28,30,31 stress,32-34 bloodugar,35,36 caffeine consumption,37 smoking,38 and obviouslyhether she pays attention to FM or not.Maternal counting while lying down and focusing on FM,
referably at a time of day when she knows that the baby issually active, is thus the only method known to be a validpproximation to actual fetal activity. Counting while focus-ng on FM is also the only way women intuitively will per-orm FMC if they are concerned for DFM. Any “alarm limits,”
r definitions of DFM, associated with such FMC should
ti
fobobsnaipcr1“batawabtFhscemtWpr
dfhpoCrt
nsotoraDbwivh
sds
AFWDgsucisbawssqfmtd
Dt1ttcha0ctsaaoompo
R
Fetal movement assessment 245
herefore be based on data from studies of focused countingn a population equivalent to the one being screened.
Many definitions of DFM to be used in conjunction withormal FMC have been proposed, ranging from total absencef FM for a whole day39,40 to less than 10 FM in 2 hours,7
ased on time to count ranging from 12 hours41 to a medianf 15 minutes.42 Most of the early DFM definitions wereased on the data from “Daily Movement Counts,”41 in whichmall groups of high-risk women in hospital were required toote FM through both rest and activities through 12 hours,lthough later versions reduced these to shorter or repeatedntervals. The limits calculated from these materials were notrimarily developed for screening purposes but were simplyutoff limits identifying death and severe morbidity in high-isk patients with an average fetal mortality of 5%.39,40,43,44 In976 and 1977 Pearson published the new concept ofCount to 10” or “Cardiff method.”44,45 This was initiallyased on “Daily Movement Counts” as well, and this “counts you go” method was used in the large randomized con-rolled trial from 1989—explaining the extreme alarm limitsnd long mean time to count to 10 in this study comparedith the mean time to “count to 10” in focused counting of
pproximately 20 minutes.7,46,47 The only definition of DFMased on focused counting data from a total population, andhen subsequently tested as a screening tool in focused formalMC in a total population, is the rule of “10 FM within 2ours” from the study by Moore and Piacquadio.7 In theirtudy, this reflected approximately 5 SD from the mean andorresponds approximately to the 95th percentile from Val-ntin and coworkers.47 This is currently the recommendedethod for FMC by the American Academy of Pediatrics and
he American College of Obstetricians and Gynecologists.48
ith a short time needed to perform counting for normalregnancies, it has the highest compliance and acceptanceates.46
While “10 FM within 2 hours” seems to be the only vali-ated definition of DFM for focused counting, our surveysrom Norway, UK, and Australia indicate that this definitionas little support among obstetricians. The most highly ap-roved definitions of DFM are “10 movements in 10 hours”r other limits derived from the obsolete “Daily Movementounts.”3,49 If women perform focused counting, such limits
epresent extreme deviations from normality, and adheringo them may cause more harm than good.
Although the four studies comparing formal FMC versuso counting, including a randomized controlled trial,trongly suggested benefit, none of them have actually dem-nstrated that their definition of DFM was beneficial. None ofhese studies prevented women from presenting with theirwn subjective perception of DFM, and the beneficial effectseported may have resulted from a combination of highwareness and maternal common sense in terms of definingFM. Indeed, the fact that FMC versus no counting seems toe beneficial irrespective of the chosen definition of DFMould support the hypothesis that benefit was derived from
ncreased maternal vigilance regarding FM. When awareness,igilance, and fetal movement counting is to be promoted, we
ave suggested that a maternal perception of significant andustained reduction in fetal activity should remain the mainefinition of DFM. Any alarm limits, as “10 FM in 2 hours,”hould only be for guidance as a “rule of thumb.”
ny Future for Formaletal Movement Counting?hile self-screened women who present with concerns forFM do manage to identify a high-risk population, the on-oing fetal movement screening overall still achieves limiteduccess. An important limitation to the efficacy of screeningsing FM may be substandard management of mother’s con-erns for DFM, as we discuss elsewhere in this issue of Sem-nars in Perinatology. Currently, far too many women do noteem to appreciate the importance of fetal activity, and still-irths are often preceded by long periods of decreased orbsent FM.50,51 Promoting awareness by recommendingomen to count FM on a daily basis has been associated with
ignificant benefits, and the full potential of this has yet to beeen. On the other hand, formal FM counting with a defineduantitative limit for when women should be subjected tourther evaluation of fetal well-being cannot be recom-ended at this time. Such a single limit, that would be better
han a maternal perception of DFM, probably does not existue to too large interpersonal variations.52
Even the currently best available quantitative definition ofFM, 10 FM in 2 hours, may be of little benefit as a screening
ool. From a total population in Norway, we have collected200 FM charts where the mother has indicated the dailyime to count to 10 at a convenient time of day, starting withhe first perceived FM. By this method, the mean time toount to 10 is less than 10 minutes. The limit of 10 FM in 2ours in the preterm period of the third trimester is indeedssociated with odds ratios of 5.5 (P � 0.001), 3.0 (P �.024), and 2.4 (P � 0.057) for preterm birth, emergencyesarean section, and a birth weight centile below 10, respec-ively. However, the sensitivity of this indicator in predictinguch events is as low as 12, 7, and 6%, respectively, and therea under the curve remains insignificant in receiver oper-ting characteristic curves. For future FMC screening meth-dologies to exploit the full potential of maternal perceptionsf FM as a sign of fetal well-being, significant research effortsust be put into the understanding of which changes inerceived fetal activity are associated with good and adverseutcomes of pregnancy.
eferences1. Frøen JF: A kick from within—fetal movement counting and the can-
celled progress in antenatal care. J Perinat Med 32:13-24, 20042. Saastad E, Ahlborg T, Frøen JF: Maternal awareness towards fetal ac-
tivity associated with SGA. J Midwifery Womens Health 2008 (in press)3. Heazell AE, Green M, Wright C, et al: Midwives’ and obstetricians’
knowledge and management of women presenting with decreased fetalmovements. Acta Obstet Gynecol Scand 87:331-339, 2008
4. National Collaborating Centre for Women’s and Children’s Health:Antenatal Care—Routine Care for the Healthy Pregnant Woman (ed 2).
London, UK, RCOG Press, 2008
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
246 J.F. Frøen et al
5. Klovning, A, Backe B, Eide BI, et al: Sosial- og Helsedirektoratet. Ret-ningslinjer for svangerskapsomsorgen. Oslo, Sosial- og Helsedirektora-tet, 2005
6. Westgate J, Jamieson M: Stillbirths and fetal movements. NZ Med J99:114-116, 1986
7. Moore TR, Piacquadio K: A prospective evaluation of fetal movementscreening to reduce the incidence of antepartum fetal death. Am JObstet Gynecol 160:1075-1080, 1989
8. Moore TR, Piacquadio K: Reply to “Study results vary in count-to-10method of fetal movement screening.” Am J Obstet Gynecol 163:264-265, 1990
9. Neldam S: Fetal movements as an indicator of fetal well-being. Lancet1:1222-1224, 1980
0. Neldam S: Fetal movements as an indicator of fetal well-being. DanMed Bull 30:274-278, 1983
1. Neldam S: Fetal movements as an indicator of fetal well-being. Univer-sity of Copenhagen, 1986
2. Mangesi L, Hofmeyr GJ: Fetal movement counting for assessment offetal well-being. Cochrane Database of Systematic Reviews (Issue 1),2007
3. Lobb MO, Beazley JM, Haddad NG: A controlled study of daily fetalmovement counts in the prevention of stillbirths. J Obstet Gynaecol6:87-91, 1985
4. Grant A, Valentin L, Elbourne D, et al: Routine formal fetal movementcounting and risk of antepartum late death in normally formed single-tons. Lancet 2:345-349, 1989
5. Gettinger A, Roberts AB, Campbell S: Comparison between subjectiveand ultrasound assessments of fetal movement. BMJ 2:88-90, 1978
6. Valentin L, Marsal K, Lindstrom K: Recording of foetal movements: acomparison of three methods. J Med Eng Technol 10:239-247, 1986
7. Hertogs K, Roberts AB, Cooper D, et al: Maternal perception of fetalmotor activity. BMJ 2:1183-1185, 1979
8. Rayburn WF: Clinical significance of perceptible fetal motion. Am JObstet Gynecol 138:210-212, 1980
9. Schmidt W, Cseh I, Hara K, et al: Maternal perception of fetal move-ments and real-time ultrasound findings. J Perinat Med 12:313-318,1984
0. Schmidt W, Cseh I, Hara K, et al: Maternal perception, tocodynamo-metric findings and real-time ultrasound assessment of total fetal activ-ity. Int J Gynaecol Obstet 22:85-90, 1984
1. Sorokin Y, Pillay S, Dierker LJ, et al: A comparison between maternal,tocodynamometric, and real-time ultrasonographic assessments of fetalmovement. Am J Obstet Gynecol 140:456-460, 1981
2. Neldam S, Jessen P: Fetal movements registered by the pregnantwoman correlated to retrospective estimations of fetal movements fromcardiotocographic tracings. Am J Obstet Gynecol 136:1051-1054,1980
3. Prenzlau P, Bayer H, Hoffmann H: [Fetal movement patterns in theexternal cardiotocography and their interpretation by simultaneousultrasound observation]. Zentralbl Gynakol 105:972-976, 1983
4. Ehrstrom C: Fetal movement monitoring in normal and high-risk preg-nancy. Acta Obstetr Gynecol Scand Suppl 1-32, 1979
5. Sadovsky E, Mahler Y, Polishuk WZ, et al: Correlation between elec-tromagnetic recording and maternal assessment of fetal movement.Lancet 1:1141-1143, 1973
6. Sadovsky E, Polishuk WZ, Yaffe H, et al: Fetal movements recorder, useand indications. Int J Gynaecol Obstet 15:20-24, 1977
7. Johnson TRB, Jordan ET, Paine LL: Doppler recordings of fetal move-ment. 2. Comparison with maternal perception. Obstet Gynecol 76:42-43, 1990
8. Cito G, Luisi S, Mezzesimi A, et al: Maternal position during non-stresstest and fetal heart rate patterns. Acta Obstet Gynecol Scand 84:335-
338, 20059. Minors DS, Waterhouse JM: The effect of maternal posture, meals and timeof day on fetal movements. Br J Obstet Gynaecol 86:717-723, 1979
0. Manders MA, Sonder GJ, Mulder EJ, et al: The effects of maternalexercise on fetal heart rate and movement patterns. Early Hum Dev48:237-247, 1997
1. Winn HN, Hess O, Goldstein I, et al: Fetal responses to maternalexercise—effect on fetal breathing and body movement. Am J Perinatol11:263-266, 1994
2. DiPietro JA, Costigan KA, Gurewitsch ED: Fetal response to inducedmaternal stress. Early Hum Dev 74:125-138, 2003
3. Sjostrom K, Valentin L, Thelin T, et al: Maternal anxiety in late preg-nancy: effect on fetal movements and fetal heart rate. Early Hum Dev67:87-100, 2002
4. Groome LJ, Swiber MJ, Bentz LS, et al: Maternal anxiety during preg-nancy: effect on fetal behavior at 38 to 40 weeks of gestation. J DevBehav Pediatr 16:391-396, 1995
5. Eller DP, Stramm SL, Newman RB: The effect of maternal intravenousglucose-administration on fetal activity. Am J Obstet Gynecol 167:1071-1074, 1992
6. Gelman SR, Spellacy WN, Wood S, et al: Fetal movements and ultra-sound: effect of maternal intravenous glucose administration. Am JObstet Gynecol 137:459-461, 1980
7. Devoe LD, Murray C, Youssif A, et al: Maternal caffeine consumptionand fetal behavior in normal 3rd-trimester pregnancy. Am J ObstetGynecol 168:1105-1112, 1993
8. Graca LM, Cardoso CG, Clode N, et al: Acute effects of maternal ciga-rette smoking on fetal heart rate and fetal body movements felt by themother. J Perinat Med 19:385-390, 1991
9. Leader LR, Baillie P, Van Schalkwyk DJ: Fetal movements and fetaloutcome: a prospective study. Obstet Gynecol 57:431-436, 1981
0. Sadovsky E, Ohel G, Havazeleth H, et al: The definition and the signif-icance of decreased fetal movements. Acta Obstet Gynecol Scand 62(5):409-413, 1983
1. Sadovsky E, Yaffe H: Daily fetal movement recording and fetal progno-sis. Obstet Gynecol 41:845-850, 1973
2. Valentin L, Marsal K: Fetal movement in the third trimester of normalpregnancy. Early Hum Dev 14:295-306, 1986
3. Liston RM, Cohen AW, Mennuti MT, et al: Antepartum fetal evaluationby maternal perception of fetal movement. Obstet Gynecol 60:424-426, 1982
4. Pearson JF, Weaver JB: Fetal activity and fetal well-being: an evaluation.BMJ 1:1305-1307, 1976
5. Pearson JF: Fetal movements—a new approach to antenatal care. Nurs-ing Mirror Midwives J 144:49-51, 1977
6. Smith CV, Davis SA, Rayburn WF: Patients’ acceptance of monitoringfetal movement. A randomized comparison of charting techniques. JReprod Med 37:144-146, 1992
7. Valentin L, Lofgren O, Marsal K, et al: Subjective recording of fetalmovements. I. Limits and acceptability in normal pregnancies. ActaObstet Gynecol Scand 63:223-228, 1984
8. Gilstrap LC, Oh W: Guidelines for Perinatal Care. Washington, DC,AAP and ACOG, 2002
9. Saastad E, Frøen JF: [Reduced fetal movements—clinical management,recommendations and information]. Tidsskr Nor Laegeforen 125:2627-2630, 2005
0. Frøen JF, Arnestad M, Frey K, et al: Risk factors for sudden intrauterineunexplained death: epidemiologic characteristics of singleton cases inOslo, Norway, 1986-1995. Am J Obstet Gynecol 184:694-702, 2001
1. Maleckiene L, Nadisauskiene R, Bergstrom S: Socio-economic, demo-graphic and obstetric risk factors for late fetal death of unknown etiol-ogy in Lithuania: a case-referent study. Acta Obstet Gynecol Scand80:321-325, 2001
2. Valentin L: Fetal movements in late pregnancy. Detection of fetal jeop-ardy by objective recording and by maternal counting. University of
Lund, 1986
ASSPL
TirameyfitisTwpcb
S
A
0d
ntenatal Fetal Assessment: Contractiontress Test, Nonstress Test, Vibroacoustictimulation, Amniotic Fluid Volume, Biophysicalrofile, and Modified Biophysical Profile—An Overview
awrence D. Devoe, MD
Antenatal fetal assessment was introduced into the United States in the 1970s. The initialantepartum test, the oxytocin challenge test, later renamed as the contraction stress test,became the gold standard for fetal surveillance. Its labor intensive requirements andcontraindications made it inapplicable to some high-risk pregnancies. Other testingschemes were developed subsequently, the nonstress test and its alternative, vibroacous-tic stimulation, the semiquantitative assessment of amniotic fluid volume, the biophysicalprofile and its modified version, the modified biophysical profile. This article is a briefcritical review of these testing methods and focuses on the following: (1) physiologicbases; (2) testing methodologies; (3) supportive evidence from randomized controlled andobservational trials; and (4) areas needing further investigation.Semin Perinatol 32:247-252 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS antepartum testing, contraction stress test, nonstress test, amniotic fluid,biophysical profile
if
CTOicsuTrraopLvhs
he modern era of fetal assessment was ushered in by theuse of continuous electronic fetal monitoring (EFM) dur-
ng the labors of near-term patients. Intrapartum fetal heartate (FHR) patterns were correlated with neonatal outcomesnd specific FHR patterns emerged that provided surrogateeasures of fetal oxygenation. A consensus was reached
ventually on those patterns predictive of adequate fetal ox-genation or of fetal hypoxia and acidosis.1 Intrapartum EFMndings led to the initial fetal assessment test that was used inhe United States, the oxytocin challenge test (OCT).2 Thencreasing use of obstetric ultrasonography led to other fetalurveillance methods such as the biophysical profile (BPP).he goals of fetal assessment are to identify fetuses that areell oxygenated or at risk for hypoxia and to enable appro-riate intervention so that perinatal mortality and morbidityan be prevented or reduced. This article will describe theasis for these assessment tests, review the evidence support-
ection of Maternal Fetal Medicine, Department of Obstetrics and Gynecol-ogy, Medical College of Georgia, Augusta, GA.
ddress reprint requests to Lawrence D. Devoe, MD, Department of Obstet-rics and Gynecology, Medical College of Georgia, 1120 15th Street,
Augusta, GA 30912. E-mail: [email protected]146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.005
ng their use, and indicate areas of concern and opportunitiesor further research.
ontraction Stress Testhe contraction stress test (CST), formerly known as theCT, was introduced in the early 1970s.2 It was based on
ntrapartum observations that linked recurrent late FHR de-elerations with fetal hypoxemia. Previous studies3 hadhown that as fetal arterial pO2 fell below 20 mm Hg, mostterine contractions would generate a late FHR deceleration.he underlying mechanism for this event is a bradycardicesponse to transient systemic hypertension provoked by aeduction in arterial oxygen levels. As developed by Freemannd colleagues,4 the CST was performed with intravenousxytocin until at least three moderate or strong contractionser 10 minutes were generated in a 20-minute window.ater, maternal nipple stimulation was substituted for intra-enous oxytocin. Except for a possibly higher risk of uterineyperstimulation, the nipple stimulation test has performedimilarly to the standard CST.5,6
Test classification is as follows:
Negative: No late or significant variable decelerations
Positive: Late decelerations with at least 50% of contractions247

dlcsc2MssCiA
cotCctp
STuoNeder
TItroawssaiaan1
adt
aCiaf1NipqoanNscpw
tcmphlta3tctwr
VAabe1ifmworaamscawNt
248 L.D. Devoe
Suspicious: Intermittent late or variable decelerationsHyperstimulation: Decelerations with contractions �90
seconds’ duration or 2-minute frequencyUnsatisfactory: Fewer than three contractions per 10 min-
utes or an uninterpretable tracing
A positive CST could result from maternal conditions (car-iorespiratory disorders, hypovolemia, uterine hyperstimu-
ation) or fetal conditions (placental insufficiency, umbilicalord compression). Variable decelerations prompt ultra-ound evaluation of the amniotic fluid volume and umbilicalord localization.7 Equivocal tests are usually repeated within4 hours unless other indications for delivery are present.anagement of preterm pregnancies with positive CST re-
ults require individualization based on the presence or ab-ence of reactivity and fetal maturity.8 Nonreactive positiveSTs correlate well with fetal growth restriction, increased
ncidence of late decelerations in labor, and low 5-minutepgar scores.9
In a prospective observational cohort study, Freeman andoworkers noted a very low rate of false-negative tests, ie, riskf fetal death within 1 week of a negative CST.10 False-posi-ive rates, ie, delivery of an unaffected infant after a positiveST, have been estimated at approximately 30%.9 Few directomparisons of the CST with other testing methods such ashe nonstress test (NST) or BPP have been obtained throughrospective observational studies.11-13
ummaryhe CST was the first important antepartum assessment testsed in the United States. It has been used less often afterther biophysical testing modalities were introduced, eg, theST, the BPP, and Doppler velocimetry. Most supportive
vidence for use of the CST is based on Level II-2 and II-3ata. It is associated with a very low false-negative rate ofstimated at 0.04% (Level II-1) evidence and false-positiveate estimated at 30% (Level II-3).
he Nonstress Testt was noted that the presence of FHR accelerations modifiedhe significance of an apparently “positive” CST14 and usuallyesulted in the delivery of nonhypoxic infants. The presencef two accelerations in a 20-minute window predicted a neg-tive CST in most cases and formed the basis for the mostidely used test reactivity criteria.15 Other investigators16,17
tudied resting antepartum FHR baseline tracings andhowed that the presence of accelerations was associated withlow likelihood of fetal compromise, while their absence
ncreased the risk of adverse perinatal outcomes (hypoxia,cidosis, growth restriction, placental insufficiency, andnomalies). The conventions of the NST evolved during aumber of studies performed during the late 1970s and early980s as summarized by Devoe.18
NST reactivity occurs through an autonomic neural link-ge between peripheral fetal activity and midbrain car-ioregulatory centers, which strengthens as the fetus ma-
ures. At term, nearly 90% of fetal movements elicit reactive eccelerations. The criteria for nonreactivity varied initially.18
urrent test criteria typically consider an NST to be reactivef there are two accelerations exceeding 15 beats per minutemplitude and 15 seconds’ duration in a 20-minute windowor term pregnancies and 10 beats per minute amplitude and0 seconds’ duration for gestational ages below 32 weeks.9
onreactivity may be associated with three differing scenar-os which fail to meet reactivity criteria, progressing from theresence of accelerations of inadequate amplitude or fre-uency through the absence of accelerations in the presencef fetal movements (uncoupling) to the complete absence ofccelerations and fetal movements. This uncoupling phe-omenon has been well characterized by several groups.19,20
onreactivity may be associated with prolonged fetal sleeptates, immaturity, maternal ingestion of sedatives, and fetalardiac or neurologic anomalies. Cumulative studies of NSTerformance suggest a false-negative rate of 0.3% within 1eek of a reactive NST and a false-positive rate of 50%.18
There have been four randomized controlled trials, con-aining fewer than 1500 patients in which study groups re-eived NSTs and control groups received standard care.21 Aeta-analysis did not show use of the NST reduced rates oferinatal death or neonatal seizures. Two prospective trialsave compared the NST to the CST.11,12 Freeman and col-
eagues, reporting on more than 6000 patients,11 found thathe CST provided better prediction of fetal health (false-neg-tive rate of 0.4/1000) than the NST (false-negative rate of.2/1000); however, this study was heavily weighted towardhe CST as a primary method by a 3:1 ratio. Devoe andoworkers studied nearly 1300 patients who received eitherwice-weekly NSTs or weekly CSTs.12 No perinatal deathsere reported within 1 week of either a negative CST or
eactive NST.
ibroacoustic Stimulation (VAS)variation on the standard NST evolved during the 1980s
nd was based on previous observations that sound and vi-ratory stimuli could elicit changes in FHR baseline.22 Briefxposure to a vibroacoustic signal (producing 82 decibels atmeter in air) has been shown to reduce testing time and the
ncidence of “false” nonreactive NSTs in otherwise healthyetuses.22 This response is present throughout the third tri-ester and results in a typical increase in FHR baselineithin 10 seconds of at least 10 bpm for at least 180 sec-nds.23,24 A positive response is defined as the rapid occur-ence of a qualifying acceleration following VAS. While datare limited, fetal exposure to VAS does not appear to bessociated with adverse long-term effects on child develop-ent.25 Positive (reactive) VAS tests appeared comparable to
tandard reactive NSTs26 and negative CSTs.27 Perinatal out-omes following positive VAS appear to be similar to thosessociated with reactive NSTs, while testing time was shorterith VAS.28 A meta-analysis of the trials comparing VAS andST confirmed that the incidence of nonreactive tests and
est duration were reduced. Testing efficacy could not be
stablished due to the limited sample sizes enrolled.29
SLli(CIfr2tohs
AVAutorIgbmucdute(sccTwesummoag
ocdAtULt
ca
dpavodsoltaagtsb
SVqIvs
FTAbcssarpffmo(alnooe
crop0
Antenatal fetal assessment 249
ummaryevel I evidence supporting the NSTs use comes from
imited trials performed in an early era of antepartum test-ng. Most supportive data come from case control trialsLevel II-2) or retrospective cohort analyses (Level II-3).ompared with the CST, most available evidence (Level
I-3) suggests that the NST has higher false-negative andalse-positive rates. The rate of “false” nonreactivity can beeduced by VAS, extending the observation period beyond0 minutes to account for fetal sleep states,30 and using ges-ational age-specific criteria for preterm gestations.31 A recentverview suggests that use of the NST in antepartum care ofigh-risk patients is associated with an apparent reduction intillbirths (Level II-2, Level II-3).32
mniotic Fluidolume (AFV) Assessment
FV evaluation began in the early 1980s but has rarely beensed as a sole fetal assessment method. AFV fluctuations tendo occur more gradually than do the other dynamic measuresf fetal status; therefore, AFV assessment has been used toeflect a “chronic” measure of the intrauterine environment.33
n the third trimester, AFV is the byproduct of fetal urination,astrointestinal motility, tracheal efflux, and amniotic mem-rane transfer to and from fetal and maternal water compart-ents. The historic “gold standard” for AFV measurementses dye-dilution determinations obtained through amnio-entesis, an approach not feasible for repeated measurementsuring pregnancy. Semiquantitative estimates of AFV usingltrasound measurements of AF pockets became part of BPPesting in the early 1980s.34 Two common approaches forstimating AFV have evolved: maximum vertical pocketMVP) and amniotic fluid index (AFI).35 Nomograms foremiquantitative AFV have been developed also for theourse of normal pregnancy.36 Both MVP and AFI have beenorrelated with actual AFV as measured with dye dilution.37
hese estimates of AFV tend to correlate well with actual AFVithin the normal range but over- and underestimate the
xtremes of AFV, oligohydramnios, and polyhydramnios, re-pectively. With this understanding, AFI and MVP have beensed as markers for intrauterine condition rather than aseasures of actual AFV. Although MVP was the initialethod of assessing AFV,38 Rutherford and coworkers devel-
ped the four-quadrant AFI35 and this method has achievedscendancy in current practice. Alternative schemes usingestational-age nomograms have also been studied.39
Early observational studies correlated adverse perinatalutcomes with MVPs �2 cm and showed increased risks ofongenital anomalies, fetal growth restriction, and perinataleath.40 Although a number of adverse conditions can reduceFV, prolonged gestation exceeding 41 or 42 weeks has been
he best studied of these indications for AFV assessment.41
sing a criterion of AFI above or below 8 cm, studies byagrew and coworkers42 and Wing and coworkers43 suggest
hat at less than 41 weeks gestation, weekly testing is suffi- Tient if AFI exceeds 8 cm, while twice weekly testing shouldpply to pregnancies in which AFI is below 5 cm.
More rigorous assessment of AFV as an independent pre-ictor of perinatal outcome is limited. Few studies have com-ared the relative merits of either MVP or AFI for predictingdverse perinatal outcome. Chauhan and coworkers44 sur-eyed 18 studies with more than 10,000 patients. A criterionf AFI �5 cm predicted a 2.2-fold increased risk for cesareanelivery and a 5.5-fold increased risk for 5-minute Apgarcore below 3. In a prospective trial of BPP using either MVPr AFI, Magann and colleagues45 found that MVP yielded aower frequency of oligohydramnios and equivalent predic-ion of cesarean delivery for fetal distress. These investigatorslso compared three criteria for oligohydramnios: AFI �5 cmnd two nomograms for AFI below the 5th percentile forestational age.39 None of these criteria effectively predictedhe risk of cesarean delivery for fetal distress, 5-minute Apgarcore below 3, umbilical artery pH �7.00, or birth weightelow the 5th percentile.
ummaryarying thresholds and standards have been used for semi-uantitative AFV estimation. The best data (Level II-2 andI-3) suggest that MVP and AFI are similar predictors of ad-erse perinatal outcomes but neither is an effective sole ob-ervation for fetal assessment.
etal Biophysical Profilehe BPP was developed in the early 1980s as evaluation ofFV and fetal breathing, body, and reflex movements coulde obtained with real-time ultrasound systems. Manning andoworkers34 reported on a multiple parameter fetal testingcheme that combined a standard NST with real-time ultra-ound observation of fetal breathing, body movements, reflexctivity, and AFV estimation. The BPP was assigned a scoreanging from 0 to 10 based on the criteria established for eacharameter: (1) Nonstress test, reactive or nonreactive; (2)etal breath movements, present or absent for 30 seconds; (3)etal body movements, present or absent; (4) fetal reflexovements, present or absent; (5) AFV, above threshold for
ligohydramnios. It was proposed that either acute hypoxiaNST, breathing, or movement) or chronic hypoxia (reflexctivity, AFV) could alter each parameter predictably. Vintzi-eos and coworkers46 hypothesized that hypoxia affect theeurologic centers responsible for biophysical behavior in anrder inverse to the timing of their maturation. Subsequentbservations by this group were consistent with this hypoth-sis.47
Based on the observations of Manning,48 score has beenorrelated with the risk of intrauterine asphyxia or death andecommended clinical response obtained from two decadesf observation (Level II-3).49-52 This series of nearly 90,000atients suggests that the BPP has a false-negative rate of.6/1000, based on a weekly interval between normal tests.
he BPP has a false-positive rate of approximately 50%.53
mwnttr
bMBNprn
STspnctfrea
MGittactdiswgm
MbdcafiettswtN
ts1f6
SLes
GCITntdpDctSfaNA
TMhaaAtotdt
TI
PGPDPPDCROP
250 L.D. Devoe
Timing of the initiation of the BPP has varied, althoughost data come from testing after 30 weeks gestation.54 Aeekly testing interval has been recommended following aormal BPP score9; however, prospective trials to supporthis approach are lacking. Consequently, individualization ofesting intervals for specific high-risk conditions has beenecommended.48
Rigorous trials of the efficacy of biophysical testing haveeen limited and compared the full BPP to the NST alone.2
eta-analysis of these trials55 does not show that use of thePP significantly reduced perinatal mortality or morbidities.ageotte and coworkers56 compared the BPP to the CST forrimary surveillance and found the BPP to provide compa-able performance with fewer interventions. This study wasot powered to address the prevention of perinatal death.
ummaryhere is considerable Level II-2 and Level II-3 evidence toupport the BPP as an alternative to the CST or NST forrimary fetal surveillance. The BPP appears to have false-egative rates similar to those of the CST, although directomparisons are very limited. Putative advantages of full BPPesting are its noninvasiveness, potential for observation ofetal anatomy, and parameters that reflect acute and chronicesponses to fetal hypoxia. Conversely, it requires more op-rator skill and time than does the NST or AFV assessmentlone.
odified Biophysical Profileiven the relative labor-intensiveness of the standard BPP,
nterest in developing a simpler screening test grew duringhe 1980s. Termed the modified BPP (MBPP), this schemeook advantage of two biophysical parameters for reflectingcute fetal oxygenation and acid-base balance (NST) andhronic fetal oxygenation (AFV). The NST is believed to behe first parameter usually affected by hypoxia,49 while AFVecreases gradually when perfusion to the brain and heart is
ncreased and renal blood flow is reduced. This model, con-istent with the pathophysiology of fetal growth restriction,as supported by Manning and coworkers, who showed aeometric increase in fetal death as single MVP measure-ents declined from 2.0 cm.57
The standards for reactivity and AFV estimation in theBPP are similar to those of the full BPP. The MBPP has
ecome increasingly popular with surprisingly little objectiveata on its efficacy. An early study of postdates pregnancyompared the MBPP to standard FHR testing, followed by theddition of fetal movement elements of the full BPP, andnally the addition of AFV estimation.58 The addition of AFVstimation appeared to make the greatest improvement inest efficacy. In this study, the MBPP compared favorably tohe CST as a primary screening test. Eden and colleagues59
upported the use of the MBPP as a primary screening testith the full BPP as a backup test. In a retrospective evalua-
ion, of the false-negative rates of the MBPP and the CST,
ageotte and coworkers showed that false-negative rates of whe MBPP and CST were similar.13 The largest observationaleries was reported by Miller and coworkers54on more than5,000 patients undergoing more than 50,000 MBPPs. Theiralse-negative rate was 0.8/1000; their false-positive rate was0%.
ummaryevel II-2 and Level II-3 evidence suggest that the MBPP hasfficacy similar to the CST and full BPP. More rigorous pro-pective and adequately powered trials are still lacking.
eneral Testingonsiderations: Areas of Concern
ndications for Testingable 1 lists indications commonly recommended for ante-atal fetal surveillance.8 Although it is assumed that antepar-um tests will have similar value in for all indications inetermining the risk of adverse perinatal outcome, Konto-oulos and Vintzileos have questioned this assumption.60
evoe and coworkers tested 1000 consecutive patients withommon high-risk indications: hypertension, diabetes melli-us, postdatism, and suspected fetal growth restriction.61
creening performance varied with test indication, being bestor patients with hypertension and fetal growth restrictionnd worst for postdates pregnancies. As individual tests, theST and Doppler velocimetry performed better than didFV assessment for each of these conditions.
iming of Testing Initiationost data on efficacy of antepartum surveillance methods
ave been obtained in near term pregnancies with fewer datas gestational age decreases. The largest studies cited in thisrticle have limited numbers of fetuses �32 weeks gestation.s for a false-positive test resulting in iatrogenic prematurity,
his risk must be weighed against the risk of delaying deliveryf a compromised infant. Miller and colleagues54 addressedhis issue in their retrospective survey of MBPP testing. Theirata showed that all fetal deaths could have been avoided ifesting had started at 28 weeks gestation rather than 32
able 1 Test Indications—Pregnancies at Highest Risk forntrauterine Asphyxia
Obstetric Medical
ostdates Diabetesrowth retardation Chronic hypertensionrevious stillbirth Cardiac diseaseecreased fetal movement Renal diseaseregnancy-induced hypertension Thyroid diseaseremature rupture of membranes SLEiscordant twins (20%) Thrombophiliasholestasis of pregnancyh-isoimmunizationligohydramnios (5 cm)olyhydramnios (24 cm)
eeks. However, there was a 1.5% rate of iatrogenic prema-

tcaaw
SATrUwuWlt
CAaabhqpphoneanatb
R
1
1
1
1
1
1
1
1
1
1
T
CNVAAB
L
S
Antenatal fetal assessment 251
urity for a false-positive test, and 20% of these infants hadomplications due to prematurity. More data are needed toddress the reliability of antepartum testing and the toll ex-cted for test-based interventions in gestations below 32eeks.
election of Testing Methodsummary of the tests examined in this article is presented inable 2. The criteria for level of evidence and strength ofecommendations are based on those recommended by theS Preventive Services Task Force. None of these tests areell supported by the most rigorous trials expected for eval-ation of screening, diagnostic, or therapeutic interventions.hile there is no evidence to support these tests for use in
ow-risk pregnancies, there is only fair evidence to justifyheir use as recommended in high-risk pregnancies.
onclusionsntepartum fetal surveillance has entered its fourth decadend millions of fetuses have been evaluated with at least onentenatal test during this time period. Although the use ofiophysical testing schemes to screen high-risk pregnanciesas become routine, they have evolved with limited high-uality scientific data. Serious questions remain open atresent. What is the best initial testing approach for high-riskregnancies? What is the optimal timing of test initiation andow should high-risk conditions affect test initiation? Howften should antenatal tests be repeated if not completelyormal and reassuring? How should test indications influ-nce the testing method chosen and how might that methodffect the likelihood of adverse outcome? How should ante-atal testing in the fetus between 24 and 32 weeks gestationalge be best conducted? These questions must be answered ifhe best application of antenatal surveillance techniques is toe accomplished.
eferences1. National Institute of Child Health and Human Development Research
Planning Workshop: Electronic fetal heart rate monitoring. researchguidelines for interpretation. Am J Obstet Gynecol 177:1385-1390,1997
2. Ray M, Freeman RK, Pine S, et al: Clinical experience with the oxytocin
able 2 Quality of Evidence and Strength of Recommendation
Test Level of Evidenc
ontraction stress test II-2onstress test II-2ibroacoustic stimulation II-1mniotic fluid volume II-2ssessment (MVP, AFI) II-3iophysical profile II-2
evel of evidence: I, at least one adequate randomized controlled trcohort or case-control trial; II-3, multiple time series reported.
trength of recommendation: A, good evidence to support recomevidence to support or reject recommendation.
challenge test. Am J Obstet Gynecol 114:1-9, 1972
3. Pose SV, Castillo JB, Mora-Rojas EO, et al: Test of fetal tolerance toinduced uterine contractions for the diagnosis of chronic fetal distress.Proc 8th Meeting PAHO Washington 185:96-104, 1969
4. Freeman RK, Anderson G, Dorchester W: A prospective multi-institu-tional study of antepartum fetal heart rate monitoring. I. Risk of peri-natal mortality and morbidity according to antepartum test results.Am J Obstet Gynecol 143:771-777, 1982
5. Capeless EL, Mann LI: Use of breast stimulation for antepartum stresstesting. Obstet Gynecol 64:641-645, 1984
6. Palmer SM, Martin JN, Moreland ML, et al: Contraction stress test bynipple stimulation: efficacy and safety. South Med J 79:1102-1105,1986
7. Devoe LD: Antepartum and intrapartum fetal assessment. Obstetr Gy-necol Clin 26:535-556, 1999
8. American College of Obstetricians and Gynecologists (ACOG): Ante-partum fetal surveillance (Practice Bulletin No. 9). Washington, DC,1999
9. Lagrew DC: The contraction stress test. Clin Obstet Gynecol 38(1):11-25, 1995
0. Freeman RK, Anderson G, Dorchester W: A prospective multi-institu-tional study of antepartum fetal heart rate monitoring. I. Risk of peri-natal mortality and morbidity according to antepartum test results.Am J Obstet Gynecol 143:771-777, 1982
1. Freeman RK, Anderson G, Dorchester W: A prospective multi-institu-tional study of antepartum fetal heart rate monitoring. II. Contractionsstress test versus nonstress test for primary surveillance. Am J ObstetGynecol 143:778-781, 1982
2. Devoe LD, Morrison J, Martin J, et al: A prospective comparative studyof the extended nonstress test and nipple stimulation contraction stresstest. Am J Obstet Gynecol 157:531-537, 1987
3. Nageotte MP, Towers CV, Asrat T, et al: The value of a negative ante-partum test: contraction stress test and modified biophysical profile.Obstet Gynecol 84(2):231-234, 1976
4. Trierweiler M, Freeman R, James J: Baseline fetal heart rate character-istics as an indicator of fetal status during the antepartum period. Am JObstet Gynecol 125:618-623, 1976
5. Everston LR, Gauthier RJ, Schifrin BS, et al: Antepartum fetal heart ratetesting. I. Evolution of the nonstress test. Am J Obstet Gynecol 133:29-33, 1979
6. Lee CY, DiLoreto PC, O’Lane JM: A study of fetal heart rate accelerationpatterns. Obstet Gynecol 45:142-146, 1975
7. Rochard F, Schifrin BS, Goupil F, et al: Nonstressed fetal heart ratemonitoring in the antepartum period. Am J Obstet Gynecol 126:699-706, 1976
8. Devoe LD: The nonstress test, in Eden RD, Boehm FH (eds): Assess-ment and Care of the Fetus: Physiologic, Clinical and MedicolegalPrinciples. East Norwalk, CT, Appleton and Lange, 1990, pp 365-383
9. Baser I, Johnson TR, Paine LL: Coupling of fetal movement and fetalheart rate accelerations as an indicator of fetal health. Obstet Gynecol
Antepartum Test Methods
Recommendation for Primary Screeningin High-Risk Patients
BC
C
B
, well-designed nonrandomized controlled trial; II-2, well-designed
tion; B, fair evidence to support recommendation; C, insufficient
s for
e
ial; II-1
menda
80(1):62-66, 1992

2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
252 L.D. Devoe
0. Visser GH, Bekedam DJ, Ribbert LS: Changes in antepartum heart ratepatterns with progressive deterioration of the fetal condition. I.J Biomed Comput 25(4):239-246, 1990
1. Pattison N, McCowan L: Cardiotocography for antepartum fetal assess-ment. Cochrane Database of Systematic Reviews 1999. Issue 1. Art No.CD001068. DOI:10.1002/14651858
2. Smith CV, Phelan JP, Broussard PM, et al: Fetal acoustic stimulationtesting: a retrospective analysis of the fetal acoustic stimulation test.Am J Obstet Gynecol 153:567-568, 1985
3. Smith CV: Vibroacoustic stimulation. Clin Obstet Gynecol 38:68-77,1995
4. Devoe LD, Gardner P, Arnold P, et al: The effects of vibroacousticstimulation baseline fetal heart rate in term pregnancy. Am J ObstetGynecol 160:1086-1090, 1989
5. Nyman M, Barr M, Westgren M: A four-year follow-up of hearing anddevelopment in children exposed in utero to vibro-acoustic stimula-tion. Br J Obstet Gynaecol 99:685-688, 1992
6. Marden D, McDuffie RS, Allen R, et al: A randomized controlled trial ofa new fetal acoustic stimulation test for fetal well-being. Am J ObstetGynecol 176:1386-1388, 1997
7. Read JA, Miller FC: Fetal heart rate accelerations in response to acousticstimulation as a measure of fetal well-being. Am J Obstet Gynecol129:512-517, 1977
8. Smith CV, Phelan JP, Platt LD, et al: Fetal acoustic stimulation testing.II. A randomized clinical comparison with the nonstress test. Am JObstet Gynecol 155:131-134, 1986
9. Tan KH, Smyth R: Fetal vibroacoustic stimulation for the facilitation oftests of fetal wellbeing. Cochrane Database of Systematic Reviews 2001.Issue 1. Art. No. CD002963. DOI:10.1002/14651858
0. Ware DJ, Devoe LD: The nonstress test: reassessment of the “goldstandard.” Clin Perinatol 21(4):779-796, 1994
1. Castillo RA, Devoe LD, Arthur M, et al: The preterm nonstress test:effects of gestational age and length of study. Am J Obstet Gynecol160:172-175, 1989
2. Devoe LD, Jones CR: Nonstress test: evidence-based use in high-riskpregnancy. Clin Obstetr 45(4):986-992, 2002
3. Vintzileos AM, Campbell WA, Ingardia CJ, et al: The fetal biophysicalprofile and its predictive value. Obstet Gynecol 62(3):271-278, 1983
4. Manning FA, Platt LD, Sipos L: Antepartum fetal evaluation: develop-ment of a fetal biophysical profile. Am J Obstet Gynecol 136:787-795,1980
5. Rutherford SE, Phelan JP, Smith CV, et al: The four quadrant assess-ment of amniotic fluid volume: an adjunct to antepartum fetal heart ratetesting. Obstet Gynecol 70:353-357, 1987
6. Moore TR, Cayle JF: The amniotic fluid index in normal human preg-nancy. Am J Obstet Gynecol 162:1040-1049, 1990
7. Croom CS, Banias BB, Ramos-Santos E, et al: Do semiquantitative am-niotic fluid indices reflect actual volume? Am J Obstet Gynecol 167:995-999, 1992
8. Manning FA, Baskett TF, Morrison I, et al: Fetal biophysical profilescoring: a prospective study in 1184 high-risk patients. Am J ObstetGynecol 140:289-294, 1981
9. Johnson JM, Chauhan SP, Ennen CS, et al: A comparison of 3 criteria ofoligohydramnios in identifying peripartum complications: a secondaryanalysis. Am J Obstet Gynecol 197:207-209, 2007
0. Chamberlain PF, Manning FA, Morrison I, et al: Ultrasound evaluationof amniotic fluid volume. I. The relationship of marginal and decreasedamniotic fluid to perinatal outcome. Am J Obstet Gynecol 150:245-
249, 19841. Phelan JP, Platt LD, Yeh S-Z, et al: The role of ultrasound assessment ofamniotic fluid in the management of postdates pregnancy. Am J ObstetGynecol 151:304-308, 1985
2. Lagrew DC, Pircon RA, Nageotte M, et al: How frequently shouldamniotic fluid index be repeated? Am J Obstet Gynecol 167:1129-1133, 1992
3. Wing DA, Fishman A, Gonzalez C, et al: How frequently should theamniotic fluid index be performed during the course of antepartumtesting? Am J Obstet Gynecol 174:33-36, 1996
4. Chauhan SP, Sanderson M, Hendrix NW, et al: Perinatal outcome andamniotic fluid: a meta-analysis. Am J Obstet Gynecol 181:1473-1478,1999
5. Magann EF, Doherty DA, Field K, et al: Biophysical profile with amni-otic fluid assessments. Obstet Gynecol 104:5-10, 2004
6. Vintzileos AM, Campbell WA, Ingardia CJ, et al: The fetal biophysicalprofile and its predictive value. Obstet Gynecol 62:271-278, 1983
7. Vintzileos AM, Knuppel RA: Multiple parameter biophysical testing inthe prediction of fetal acid-base status. Clin Perinatol 21:823-848,1994
8. Manning FA: Dynamic ultrasound-based fetal assessment: the fetal bio-physical profile score. Clin Obstet Gynecol 38:26-44, 1995
9. Manning FA, Morrison I, Harman CR, et al: The abnormal fetal bio-physical profile score. V. Predictive accuracy according to score com-position. Am J Obstet Gynecol 162:918-924, 1990
0. Manning FA, Harman CR, Morrison I, et al: Fetal assessment based onfetal biophysical profile scoring. IV. An analysis of perinatal morbidityand mortality. Am J Obstet Gynecol 162:703-709, 1990
1. Manning FA, Harman CR, Morrison I, et al: Fetal assessment based onfetal biophysical profile scoring. III. Positive predictive accuracy of thevery abnormal test (biophysical score � 0). Am J Obstet Gynecol 162:398-402, 1990
2. Dayal AK, Manning FA, Berck DJ, et al: Fetal death after normal bio-physical profile score: an eighteen year experience. Am J Obstet Gy-necol 181:1231-1236, 1999
3. Manning FA: Fetal biophysical profile. Obstet Gynecol Clin North Am26:557-577, 1999
4. Miller DA, Rabello YA, Paul RH: The modified biophysical profile:antepartum testing in the 1990s. Am J Obstet Gynecol 174:812-817,1996
5. Alfirevic Z, Neilson JP: Biophysical profile for fetal assessment in highrisk pregnancies. Cochrane Database of Systematic Reviews 1996, Issue2. CD000038. DOI:10.1002/14751858
6. Nageotte MP, Towers CV, Asrat T, et al: Perinatal outcome with themodified biophysical profile. Am J Obstet Gynecol 170:1672-1676,1994
7. Manning FA, Hill LM, Platt LD: Qualitative amniotic fluid volumedetermination by ultrasound: antepartum detection of intrauterinegrowth retardation. Am J Obstet Gynecol 139:254-258, 1985
8. Eden RD, Gergely RZ, Schifrin BS, et al: Comparison of antepartumtesting schemes for the management of the postdate pregnancy. Am JObstet Gynecol 144:683-692, 1982
9. Eden RD, Seifert LS, Kodack LD, et al: A modified biophysical profilefor antenatal fetal surveillance. Obstet Gynecol 71:356-359, 1988
0. Kontopoulos EV, Vintzileos AM: Condition-specific antepartum fetaltesting. Am J Obstet Gynecol 191:1546-1551, 2004
1. Devoe L, Gardner P, Dear C, et al: The diagnostic value of concurrentnonstress testing, amniotic fluid measurement and Doppler velocim-etry in screening a general high risk population. Am J Obstet Gynecol
163:1040-1047, 1990
FMG
U
UvrtgfacGcawtDe
*†
A
0d
etal Doppler: Umbilical Artery,iddle Cerebral Artery, and Venous System
iancarlo Mari, MD,* and Farhan Hanif, MD†
One of the most important applications of Doppler ultrasonography in obstetrics is thedetection of fetal anemia in pregnancies complicated by either red-cell alloimmunization orby other causes of fetal anemia. Doppler of the umbilical artery also has prognostic valuein pregnancies affected by twin–twin transfusion syndrome undergoing in-utero interven-tion. Another potential major application is the use of Doppler ultrasound in the manage-ment of intrauterine-growth-restricted fetuses. At the present time, there is no single testthat appears superior to the other available tests for timing the delivery of the growth-restricted fetus. Therefore, the decision to deliver a fetus, especially at <32 weeks, remainsmostly based on empirical management. Doppler may provide a more reliable and systematicbasis for timing these deliveries. This review emphasizes the three following concepts:(a) normal and abnormal Doppler of the umbilical artery, middle cerebral artery, mitral andtricuspid valves, umbilical vein, and ductus venosus; (b) some clinical applications of Dopplersonography in obstetrics; and (c) potential future research of Doppler in obstetrics.Semin Perinatol 32:253-257 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS feat anemia, IUGR, Doppler, ductus venosus, middle cerebral artery
MAbciftTtsItt
UAccip
AT
mbilical Artery
mbilical artery angle independent indices (pulsatilityindex or systolic/diastolic (S/D) ratio) decrease with ad-
ancing gestation because of a decreased placental vascularesistance, which physiologically occurs with advancing ges-ation.1,2 In pathologic conditions, such as in intrauterine-rowth-restricted (IUGR) fetuses, the umbilical artery wave-orms change and the angle-independent indices becomebnormal (values above their reference ranges). Thesehanges reflect an increased placental vascular resistance.2
iles and coworkers demonstrated that the number of pla-ental arteries per high power field is decreased in cases ofbnormal umbilical artery Doppler.3 Only in pregnanciesith suspected intrauterine growth restriction and/or hyper-
ensive disease of pregnancy does the use of umbilical arteryoppler reduce the number of perinatal deaths and unnec-ssary obstetric interventions.4
Tennessee Maternal Fetal Medicine Institute, Memphis, TN.Department of Obstetrics and Gynecology, Wayne State University, De-
troit, MI.ddress reprint requests to Giancarlo Mari, MD, Director of Tennessee Ma-
ternal Fetal Medicine Institute, Director MFM and Vice Chairman Ob/Gyn, UTHSC, 853 Jefferson Avenue Rout E-102, Memphis, TN 38103-
t2807. E-mail: [email protected]
146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.007
iddle Cerebral Arteryngle-independent indices differ among the different cere-ral arteries.5 The middle cerebral artery is the most studiederebral artery because (a) it is easy to sample; (b) it providesnformation on the cerebral blood flow in normal and IUGRetuses; and (c) it can be sampled at an angle of 0° betweenhe ultrasound beam and the direction of the blood flow.6
herefore, for the middle cerebral artery we are able to de-ermine angle-independent indices (the most used is the pul-atility index) and also the real velocity of blood flow. InUGR fetuses there is a redistribution of the blood flow fromhe fetal periphery to the brain. This phenomenon is calledhe “brain-sparing effect.”7
mbilical Veinfter 15 weeks gestation, the umbilical vein normally has aontinuous blood flow but becomes pulsatile in pathologicalases, such as in IUGR and hydropic fetuses.8 For the umbil-cal vein we use a qualitative assessment: continuous versusulsatile blood flow.
trioventricular Valveshe atrioventricular valves (mitral and tricuspid) are charac-
erized by two peaks—the “E” wave that corresponds to the
253

rstici“ofics
DDt
Hcttitcr
TASDTatbotnu(hiaaftwti
FDoa
254 G. Mari and F. Hanif
apid filling of the ventricles and the “A” wave that corre-ponds to the atrial contraction. The “A” wave is taller thanhe “E” wave,9,10 which may suggest that atrial contraction ismportant in the fetus, and is associated with stiffness of fetalardiac chambers. With advancing gestation, the E/A rationcreases. By contrast, after birth, and also in the adult, theE” wave is taller than the “A” wave. In fact, in the adult, 85%f the blood passes from the atria to the ventricles during therst part of the diastole. In IUGR fetuses the two waves be-ome abnormal (the E/A ratio increases) and, in the mostevere cases, there is tricuspid and mitral regurgitation.11
uctus Venosusuctus venosus waveforms are characterized by two peaks,
he S and D, followed by a nadir, the a wave (Fig. 1).12
igure 1 Flow velocity waveforms of the ductus venosus. S � systole;� 1st phase of the diastole corresponding to the passive rapid filling
f the ventricles; a � 2nd phase of the diastole corresponding to thetrial contraction. (Color version of figure is available online.)
Figure 2 Peak velocity of systolic blood flow in the midindicates the median peak systolic velocity in the middle
the median. (Modified from Mari and colleagues.14)emodynamically, these phases reflect the rapid chronologichange in pressure gradients between the umbilical vein andhe right atrium. In appropriate-for-gestational-age fetuses,here is forward flow at the ductus venosus, and the pulsatil-ty index for veins (S-D/a) decreases with advancing gesta-ion. However, in IUGR fetuses, the pulsatility index in-reases, and in the most severe cases, there is “a” waveeversed flow.
hree Clinicalpplications of Doppleronography in Obstetricsiagnosis of Fetal Anemia
he middle cerebral artery (MCA) can be insonated at anngle of 0° between the ultrasound beam and the direction ofhe blood flow and, consequently, the real velocity of thelood flow can be determined.6 The lowest intra- and inter-bserver variability is obtained when the MCA proximal tohe transducer is sampled soon after its origin from the inter-al carotid artery, without the use of an angle corrector, bysing a 1- to 2-mm sample volume.13 A peak systolic velocityPSV) above 1.50 MoM (Fig. 2), in fetuses at risk for anemia,as a sensitivity for detecting anemia of 100% (CI: 86-100%)
n red cell alloimmunization cases as well as in other cases ofnemia.14-16 The false-positive rate is 12%, but this percent-ge may decrease when serial MCA values are obtained.17 Inetuses at risk for anemia because of red cell alloimmuniza-ion, we use the curve reported in Figure 3 in the followingay. We initially perform three exams, 1 week apart, and
hen obtain the regression line of the three points. If the curves to the right side of the dotted line, we perform the next
ebral artery with advancing gestation. The solid curveal artery, and the dotted curve indicate 1.5 multiples of
dle cercerebr

Mawcfipvlilninsot
wnacwutdttaitb
TDpttnu
aaae
IMatbhhafnrtmmff
PaTIituitcmfismwcpttosliit
pbIip
WW
Fy�5
Fetal Doppler 255
CA Doppler examination between 2 and 4 weeks. For ex-mple, if a patient with an anti-D titer of 1:256 is seen at 17eeks gestation, and her previous pregnancies have not been
omplicated by fetal anemia, and the regression line of herrst three exams is to the right side of the dotted line, weerform the next examination in 4 weeks. However, if thealues are between the dotted line and one of the continuousines, the next examination is performed in 2 weeks. Finally,f the regression line is to the left of one of the continuousines, and the MCA PSV is below 1.50 MoM, we perform theext examination every 2 to 3 days. After 34 weeks gestation,
f we use the 1.50 MoM as the cutoff point, we find that theumber of false positives increases. Therefore we look aterial MCA values rather than at one single value. We deliverur patients at risk for fetal anemia at 38 to 39 weeks gesta-ion.
In 1997, we reported that the accuracy of the MCA PSVas at least as good as that of the delta OD450 in the diag-osis of fetal anemia. (We also noted that the MCA PSV hadn important advantage in that it is noninvasive.)18 The ac-uracy of the MCA PSV was confirmed by Pereira and co-orkers19 in a retrospective study—the same approach wesed. More recently, a multicenter prospective study has de-ermined that the MCA PSV is actually more reliable than theelta OD 450 in the diagnosis of fetal anemia,20 which has ledhe American College of Obstetrics and Gynecology to reporthat the MCA PSV is an excellent tool for the diagnosis of fetalnemia in the hands of trained people.21 Retrospective stud-es have suggested that the MCA PSV can be used for timinghe subsequent transfusions, but a randomized trial shoulde performed to confirm this.
win–Twin Transfusion Syndromeoppler measurements of the umbilical artery are excellentrognostic parameters to assess patients with twin–twinransfusion syndrome. Twin–twin transfusion syndrome pa-ients with absent end-diastolic velocity have a worse prog-osis than patients with forward end-diastolic velocity at the
igure 3 Average regression line for nonanemic fetuses (dotted line,� �17.28 � 1.99x); mildly anemic fetuses (thin line, y � �53.544.17x), and severely anemic fetuses (thick line, y � �76.82 �
.26x). (Reprinted with permission.17)
mbilical artery in one of the twins, when the twins undergo c
mnioreduction or laser therapy.22,23 The MCA PSV is alsonother parameter of choice that allows the diagnosis of fetalnemia and indicates the need for transfusions in the recipi-nt following laser therapy.24
ntrauterine Growth Restrictionost of the studies that report on IUGR have not differenti-
ted between constitutionally and pathologically small fe-uses. Additionally, studies on the pathogenesis of IUGR haveeen limited by the concept that IUGR fetuses represent aomogeneous group. This has created some confusion andas hampered our understanding of the mechanisms that aret the basis of IUGR. We use the term small for gestational ageor those small fetuses with no maternal pathology and withormal umbilical artery and middle cerebral artery Doppleresults. In contrast, growth-restricted fetuses are small fe-uses with a recognizable maternal pathology or an abnor-al umbilical or middle cerebral artery Doppler. When noaternal pathology is present but there is an abnormal
etal Doppler, we define small fetuses as idiopathic IUGRetuses.25,26
lacental Insufficiencynd Idiopathic IUGR Fetuseshe concept that placental insufficiency is THE cause ofUGR is a source of confusion. We believe that placentalnsufficiency is not “THE cause” of the problem but is ratherhe consequence of a disease process that often we do notnderstand.25 We agree with Assali, who defined placental
nsufficiency as “an umbrella that covers our ignorance inerms of etiology and pathogenesis of the utero-placentalhronic dysfunction” (from Bruno Salvadori, personal com-unication). We have recently reported that placental insuf-ciency is a “symptom” and it can be compared with the fevereen in patients with bacterial pneumonia.25 As with pneu-onia, there are many agents that could cause it; similarly,ith placental insufficiency there may be many underlying
auses. If we use an antipyretic in patients with bacterialneumonia, the fever will temporarily subside; however, toreat the entire condition it is necessary to use antibiotics toarget the specific etiologic factor. Similarly, with IUGR, weften view the problem from the wrong direction—as a con-equence of placental insufficiency—and we therefore be-ieve that we should treat the placental insufficiency. In real-ty we should find and treat the specific cause of placentalnsufficiency. The optimal management, however, would behe prevention of IUGR fetuses.
In many IUGR fetuses there is an underlying maternalathology, eg, chronic hypertension or advanced stage dia-etes mellitus, at the basis of placental insufficiency. In otherUGR cases there is not an identifiable cause of placentalnsufficiency; these are the cases that we define as “idio-athic” IUGR fetuses.25,26
hat Is New in IUGR Research?e and others have reported a temporal sequence in the
ardiovascular system of IUGR fetuses.26-29 We have also re-

pttri
teifvebimaet
mfsertrptsedopdosts
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
256 G. Mari and F. Hanif
orted that the MCA PSV is increased in IUGR fetuses andhat this increase predicts perinatal mortality more accuratelyhan the MCA pulsatility index.30 In addition, there is a cor-elation between the MCA PSV and a low pO2 and high pCO2
n IUGR fetuses.31
Recently, there has been much interest in finding a methodo decide when to deliver the IUGR fetus. It has been hypoth-sized that an abnormal ductus venosus Doppler would be anndication for delivery. Although this could be an indicationor delivery after 32 weeks, we do not believe that ductusenosus reversed flow (DVRF) is an indication for deliveryarly in the third trimester in all cases of IUGR fetuses. This isased on our recent reports that, for each week the fetus remains
n utero between 25 and 29 weeks, there is a decreased perinatalortality of 48%,32 and that the majority of fetuses with DVRF
re not acidemic.33 Therefore, the main goal would be to differ-ntiate between those fetuses with DVRF that require early in-ervention from those for which delivery can be delayed.
We believe that undertaking a randomized study to deter-ine the optimal timing of delivery of the growth-restricted
etus is premature, because at the current time, there is notudy that has demonstrated differentiation among the differ-nt IUGR fetuses. Without this information, the results of aandomized study could lead to the adoption of a flawed testo determine the optimal timing for delivery of the growth-estricted fetus. We do not wish to make the mistake ofossibly adopting a test determined to be “the best” in such arial before the full range of observational and randomizedtudies to evaluate all tests in normal and “at risk and dis-ased” pregnancies has been completed. To do so woulduplicate the history and ensuing controversies of adoptionf fetal heart rate monitoring for fetal surveillance. For exam-le, we have learned that idiopathic IUGR fetuses behave in aifferent way than IUGR fetuses seen in preeclamptic patientsr in diabetic patients.34 Therefore, we believe that the firsttep of future research would be to prospectively learn abouthe natural history of the different IUGR fetuses. This is atudy that we are conducting in our ultrasound laboratory.
eferences1. Stuart B, Drumm J, FitzGerald DE, et al: Fetal blood velocity waveforms
in normal pregnancies. Br J Obstet Gynaecol 87:780-785, 19802. Trudinger BJ, Giles WB, Cook CM, et al: Fetal umbilical artery flow
velocity waveforms and placental resistance: clinical significance. Br JObstet Gynaecol 92:23-30, 1985
3. Giles WB, Trudinger BJ, Baird PJ: Fetal umbilical artery flow velocitywaveforms and placental resistance: pathological correlation. Br J Ob-stet Gynaecol 92:31-38, 1985
4. Westergaard HB, Langhoff-Roos J, Lingman G, et al: A critical appraisalof the use of umbilical artery Doppler ultrasound in high-risk pregnan-cies: use of meta-analyses in evidence-based obstetric. Ultrasound Ob-stet Gynecol 17:466-476, 2001
5. Mari G, Moise KJ Jr, Deter RL, et al: Doppler assessment of the pulsa-tility index in the cerebral circulation of the human fetus. Am J ObstetGynecol 160:698-703, 1989
6. Mari G, Adrignolo A, Abuhamad AZ, et al: Diagnosis of fetal anemiawith Doppler ultrasound in the pregnancy complicated by maternalblood group immunization. Ultrasound Obstet Gynecol 5:400-405,
1995 27. Wladimiroff JW, Tonge HM, Stewart PA: Doppler ultrasound assess-ment of the cerebral blood flow in the human fetus. Br J Obstet Gynae-col 93:471-475, 1986
8. Reed KK, Chaffin DG, Anderson CF, et al: Umbilical venous velocitypulsations are related to atrial contraction pressure waveforms in fetallambs. Obstet Gynecol 89:953-956, 1997
9. Rizzo G, Arduini D, Romanini C, et al: Doppler echocardiographicassessment of atrioventricular velocity waveforms in normal and small-for-gestational-age fetuses. Br J Obstet Gynaecol 95:65-69, 1988
0. Hecher K, Campbell S, Snijders R, et al: Reference ranges for fetalvenous and atrioventricular blood flow parameters. Ultrasound ObstetGynecol 4:381-390, 1994
1. Mari G, Deter RL, Hanif F, et al: Sequence of cardiovascular changesoccurring in severe IUGR fetuses—part II. Ultrasound Obstet Gynecol2006;28:390 abstract (OC109)
2. Kiserud T, Eik-Nes SH, Blaas HG, et al: Ultrasonographic velocimetryof the fetal ductus venosus. Lancet 338:1412-1414, 1991
3. Mari G, Abuhamad A, Cosmi E, et al: Middle cerebral artery peaksystolic velocity—technique and Variability. J Ultrasound Med 24:425-430, 2005
4. Mari G, Deter RL, Carpenter RL, et al: Non-invasive diagnosis by Dopp-ler ultrasonography of fetal anemia due to maternal red-cell alloimmu-nization. Collaborative Group for Doppler Assessment of the BloodVelocity in Anemic Fetuses. N Engl J Med 342:9-14, 2000
5. Zimmerman R, Carpenter RJ Jr, Durig P, et al: Longitudinal measure-ment of peak systolic velocity in the fetal middle cerebral artery formonitoring pregnancies complicated by red cell alloimmunisation: Aprospective multicentre trial with intention-to-treat. BJOG 109:746-752, 2002
6. Cosmi E, Mari G, Delle Chiaie L, et al: Noninvasive diagnosis by Dopp-ler ultrasonography of fetal anemia resulting from parvovirus infection.Am J Obstet Gynecol 187:1290-1293, 2002
7. Detti L, Mari G, Akiyama M, et al: Longitudinal assessment of themiddle cerebral artery peak systolic velocity in healthy fetuses andin fetuses at risk for anemia. Am J Obstet Gynecol 187:937-939,2002
8. Mari G, Penso C, Sbracia M, et al: Delta OD 450 and Doppler veloci-metry of the middle cerebral artery peak velocity in the evaluation forfetal alloimmune hemolytic disease. Which is the best? Am J ObstetGynecol 176:S18, 1997
9. Pereira JC, Jenkins TM, Berghella V: Conventional management ofmaternal red cell alloimmunization compared with management byDoppler assessment of middle cerebral artery peak systolic velocity.Am J Obstet Gynecol 189:1002-1006, 2003
0. Oepkes D, Seaward PG, Vandenbussche FP, et al: Doppler ultrasonog-raphy versus amniocentesis to predict fetal anemia. N Engl J Med 13:355-364, 2006
1. ACOG Practice Bulletin. Management of alloimmunization duringpregnancy. Obstet Gynecol 75:457-464, 2006
2. Mari G, Roberts A, Detti L, et al: Perinatal morbidity and mortalityrates in severe twin-twin transfusion syndrome: results of the Inter-national Amnioreduction Registry. Am J Obstet Gynecol 185:708-715, 2001
3. Kontopoulos EV, Quintero RA, Chmait RH, et al: Percent absent end-diastolic velocity in the umbilical artery waveform as a predictor ofintrauterine fetal demise of the donor twin after selective laser photo-coagulation of communication vessels in twin-twin transfusion syn-drome. Ultrasound Obstet Gynecol 30:35-39, 2007
4. Senat MV, Loizeau S, Couderc S, et al: The value of middle cerebralartery peak systolic velocity in the diagnosis of fetal anemia after intra-uterine death of one monochorionic twin. Am J Obstet Gynecol 189:1320-1324, 2003
5. Mari G, Hanif F: Intrauterine growth restriction: how to manage andwhen to deliver. Clin Obstet Gynecol 50:497-509, 2007
6. Cosmi E, Ambrosini G, D’Antona D, et al: Doppler, cardiotocography,and biopgysical profile changes in growth restricted fetuses. ObstetGynecol 106:1240-1245, 2005
7. Hecher K, Bilardo CM, Stigter RH, et al: Monitoring of fetuses with

2
2
3
3
3
3
3
Fetal Doppler 257
intrauterine growth restriction: a longitudinal study. UltrasoundObstet Gynecol 18:564-570, 2001
8. Gembruch U, Harman CR: The sequence of changes in Doppler andbiophysical parameters as severe fetal growth restriction worsens.Ultrasound Obstet Gynecol 18:571-577, 2001
9. Ferrazzi E, Bozzo M, Rigano S, et al: Temporal sequence of abnormalDoppler changes in the peripheral and central circulatory systems ofthe severely growth-restricted fetus. Ultrasound Obstet Gynecol 19:140-146, 2002 Baschat
0. Mari G, Hanif F, Cosmi E, et al: Middle cerebral artery peak systolicvelocity: A new Doppler parameter in the assessment of IUGR fetuses.
Ultrasound Obstet Gynecol 29(3):310-316, 20071. Hanif F, Drennan K, Mari G: Variables affecting the middle cerebralartery peak systolic velocity in anemic and IUGR fetuses. Am J Perinatol28:377-383, 2008
2. Mari G, Hanif F, Cosmi E, et al: Middle cerebral artery peak systolicvelocity: A new Doppler parameter in the assessment of IUGR fetuses.Ultrasound Obstet Gynecol 29(3):310-316, 2007
3. Mari G, Hanif F, Treadwell M, et al: Gestational age at delivery andDoppler waveforms in very preterm IUGR fetuses as predictors of peri-natal mortality. J Ultrasound Med 26:555-559, 2007
4. Mari G, Hanif F, Kruger M: Cardiovascular changes sequence in severeIUGR in pregnancies with and without preeclampsia. Prenat Diagn
28:377-383, 2008
MWA
Dpfddiittipuctasmco
*†
RA
2
onitoring of Fetalell-Being: Role of Uterine Artery Doppler
lessandro Ghidini, MD,* and Anna Locatelli, MD†
Doppler interrogation of the uterine arteries provides information on the physiologictransformation of the spiral arteries during pregnancy. Lack or suboptimal conversion ofsuch arteries by the late second or third trimester of pregnancy is a strong indicator ofincreased risk for adverse pregnancy outcome, in particular, iatrogenic prematurity due tosevere fetal growth restriction or preeclampsia. Uterine artery Doppler can thus play a rolein the presence of medical conditions antedating pregnancy, which have greater risk ofabnormal placentation, like chronic hypertension, to identify the subgroup with increasedpregnancy complications and adverse outcome. In the presence of pregnancy complica-tions related to inadequate placentation, such as fetal growth restriction or preeclampsia,uterine artery Doppler also plays a role, as abnormal findings signal increased severity ofthe disease and thus greater likelihood of unfavorable perinatal outcome.Semin Perinatol 32:258-262 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS uterine artery, Doppler velocimetry, fetal growth restriction, preeclampsia,abnormal placental implantation
mpntsbcnrDtbwcp
TTUwsta�
oppler ultrasonographic interrogation of the arterial ve-locity waveforms allows the estimation of vascular im-
edance to flow by comparing systolic and diastolic wave-orms. In the presence of downstream resistance to flowiastolic velocity diminishes in relation to systolic flow. Un-er the effect of trophoblastic migration into the spiral arter-
es, the uterine vascular bed undergoes marked changes dur-ng pregnancy, becoming a low resistance circuit, with flowhroughout diastole. Concomitantly, as the placental implan-ation progresses, a sharp decrease in uterine artery (UtA)mpedance to flow occurs and the early diastolic notchresent in the nonpregnant UtA disappears. Placentation issually completed by 24 weeks, and indeed less prominenthanges in UtA Doppler occur in the third trimester. Norma-ive data for UtA Doppler throughout gestation are avail-ble.1,2 Abnormal development of the placental vasculature,ignaled by increased impedance to flow at UtA Doppler,ay lead over time to the development of obstetrical compli-
ations, such as fetal growth restriction (FGR), preeclampsia,r abruption.
Perinatal Diagnostic Center, Inova Alexandria Hospital, Alexandria, VA.Department of Obstetrics and Gynecology, University of Milano-Bicocca,
Monza, Italy.eprints not available.ddress correspondence to Alessandro Ghidini, MD, Perinatal Diagnostic
Center, Inova Alexandria Hospital, 4320 Seminary Road, Alexandria, VA
l22304. E-mail: [email protected]58 0146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1053/j.semperi.2008.04.019
In the presence of obstetric complications in the third tri-ester of pregnancy, UtA Doppler is ideally positioned torovide valuable prognostic information allowing the recog-ition of complications associated with abnormal placenta-ion. Several maternal pathologies antedating pregnancy,uch as chronic hypertension, inherited and acquired throm-ophilias, diabetes mellitus, and autoimmune disorders in-luding lupus erythematosus, increase the probability of ab-ormal development of the placental vasculature with theelated risk of obstetric complications. Once again, UtAoppler at completion of placentation has been used to iden-
ify the subset of such high-risk pregnancies, which mayenefit from increased surveillance, whereas in the subsetith appropriate placentation, normal UtA Doppler findings
an provide reassurance to the parents and the health careroviders.
echniquehe technique of UtA Doppler interrogation is fairly simple.sing color-flow mapping, each uterine artery is identifiedhere it crosses over the external iliac artery. The range gate
hould be placed over the entire diameter of the artery distalo the crossover point and before division into branches. Thengle of insonation should be minimized and kept at least60°. Once waveforms are obtained with a clear envelope, at
east three waveforms can be averaged and impedance indi-

cDt
UDoFImddvw�62cuom9ost2tIDetmps
HPcooirFcowsv(ertsl(
DOtafidam
OItpimdsd�
Fwvv
Monitoring of fetal well-being 259
es calculated (Figs. 1 and 2) Interobserver variability of UtAoppler has been reported as approximately 10%, with in-
raobserver variability of 2.5 to 10.1%.3-5
terine Arteryoppler in the Presencef Obstetric Complicationsetal Growth Restriction
n the presence of ultrasonographic evidence of FGR, abnor-al UtA Doppler identifies fetuses at higher risk of pretermelivery and lower birth weight.6,7 Low gestational age atelivery is the most important independent predictor of ad-erse neonatal outcome in FGR.8 In one study of FGR fetusesith abnormal UtA Doppler, only 20% of those delivered at34 weeks had uncomplicated neonatal course, compared with
0% of those delivered at �34 weeks.9 In the largest study of94 FGR fetuses delivered after 34 weeks, adverse neonatal out-ome—defined as admission to the neonatal intensive carenit (NICU) for reasons other than low birth weight alone—ccurred more frequently in cases with abnormal than nor-al UtA Doppler waveforms (35% versus 11%, OR � 3.2;
5% CI, 1.9-5.3) (Table 1). Logistic regression analysis dem-nstrated that abnormal UtA Doppler findings remained aignificant predictor of adverse neonatal outcome after con-rolling for occurrence of preeclampsia (OR � 4.1, 95% CI,.2-7.5).10 Umbilical artery Doppler is a major prognostica-or among FGR cases, particularly those delivered preterm.n cases with normal umbilical artery Doppler findings, UtAoppler prognosticates increased risk for emergency cesar-an section.11 Not surprisingly, UtA Doppler has been foundo be a predictor of perinatal mortality and major neonatalorbidity.9 Finally, abnormal results at UtA Doppler in the
resence of FGR identifies women at increased risk for sub-
igure 1 Abnormal uterine artery Doppler waveform at 28 weeks,ith increased impedance to flow. Color flow mapping is used forisualization of the artery and proper positioning of the sampleolume.
equent development of preeclampsia.12 F
ypertensive Complications of Pregnancylacental vascular lesions due to abnormal placentation are aharacteristic finding in the presence of preeclampsia andther hypertensive complications of pregnancy. UtA Dopplerbtained on admission for such conditions offers preciousnformation, identifying the majority of pregnancies at higherisk for indicated preterm delivery, and neonates with worseGR and need for NICU admission.13-15 For example, in aohort study of 186 cases of preterm preeclampsia diagnosedn average at 31.3 � 3.6 weeks and delivered at 32.8 � 3.3eeks, those with abnormal UtA Doppler findings on admis-
ion had significantly lower gestational age delivery (32.5ersus 35.3 weeks), higher rates of very low birth weight52% versus 5%), and of FGR (70% versus 23%).14 Of inter-st, UtA Doppler predictive ability was independent of labo-atory indicators of severity of preeclampsia.14 The informa-ion provided by UtA Doppler operates along a continuum,o that the risk for such adverse outcomes is directly corre-ated with the severity of abnormal UtA Doppler findings15
Table 2).
ecreased Fetal Movementsnly one study has examined the value of UtA Doppler at the
ime of nonstress test done for decreased fetal movements atmean gestational age of 36 weeks. Abnormal UtA Dopplerndings were significantly associated with delivery within 2ays of testing, with emergency cesarean delivery and oper-tive delivery for fetal distress, but not with more objectiveeasures of adverse neonatal outcome.16
bstetric Complicationsn a large cohort of pregnancies with a variety of complica-ions, including gestational hypertension with or withoutroteinuria, oligohydramnios, suspected FGR, vaginal bleed-
ng, preterm labor, postterm pregnancy, decreased fetalovement, or history of adverse outcome, 54% (399/741)eveloped adverse perinatal outcome, defined as low Apgarcore, low arterial or venous pH, preterm delivery, cesareanelivery for fetal distress, admission to NICU, birth weight2 SD below expected, or perinatal death. UtA Doppler ob-
igure 2 Normal uterine artery Doppler waveform at 28 weeks.

tdatipscbUnpobhcam2(6chaw8
UDPMCSmtawwacTvviirhheac
T
TSWDB
U
R
T>
PGMCCBBUAL
MR
260 A. Ghidini and A. Locatelli
ained at an average of 38.6 weeks (range: 25.6-43.1) pre-icted the occurrence of adverse outcome with odds ratiosnd positive likelihood ratios (LR) directly proportional tohe severity of the UtA Doppler abnormality (Table 3).17 Sim-larly, in a study of 633 pregnancies at high risk due to hy-ertensive complications of pregnancy, oligohydramnios,uspected FGR, vaginal bleeding, postterm pregnancy, de-reased fetal movement, previous adverse outcome (ie, still-irth, small for gestational age (SGA) baby, or preeclampsia),tA Doppler at an average of 35 weeks predicted risk of SGAeonates, need for cesarean delivery, and prematurity, with aredictive ability that was independent and superior to thatf umbilical artery Doppler.18 These findings were confirmedy an independent study of UtA Doppler in 282 women atigh risk due to a variety of medical conditions (includinghronic hypertension, renal or autoimmune disease, as wells history of adverse obstetric outcome). Compared with nor-al UtA Doppler findings, abnormal UtA Doppler results at
8 weeks were associated with higher risk for preeclampsiaLR 7.6, 95% CI, 3.7, 7.6), SGA baby (LR 11.2, 95% CI,.6-18.7), fetal demise (LR 7.3, 95% CI, 2.4-7.3), or severeomplications, defined as the development of preeclampsia,ypertensive disease with a SGA baby, intrauterine demise ofstructurally normal fetus, or elective delivery before 34eeks for maternal or fetal indications (LR 12.5, 95% CI,.8-13.6).19
able 2 Effect of Severity of Uterine Artery Doppler Results o
Score 0 Sc
otal 363 7evere preeclampsia 13% 2eeks at delivery 38 � 2 37elivery <34 weeks 2% 1irth weight <10th centile 2%
terine Artery Score definition: Score 0: normal flow in both arteriepresent); Score 2: two abnormal parameters; Score 3: three abn
able 1 Perinatal Outcome in Relation to Maternal Uterine Art34 weeks
Uterine AAbnormal (
reeclampsia 22%estational age at delivery (wk) 37.7 �econium-stained amniotic fluid 3%esarean delivery (CD) 38%D for non-reassuring fetal testing 27%irth weight (g) 2193 �irth weight percentile 4.8 �mbilical artery pH 7.28 �dmission to NICU 35%ength of stay in NICU (days) 20.7 �
ean � SD or (%).eprinted with permission.10
eprinted with permission.15
terine Arteryoppler in theresence of Preexistingedical Complications
hronic Hypertensionuperimposed preeclampsia and FGR are the two most com-on obstetric complications in women with chronic hyper-
ension and can be predicted by Doppler interrogation of UtAt completion of placentation. In an initial study, 78 womenith chronic hypertension underwent UtA Doppler at 24eeks gestation. The screen positive rate was 32% when
bnormal findings were defined by elevated resistance indi-es, and 17% when defined by presence of bilateral notching.he rates of preeclampsia (12% versus 0%) and FGR (52%ersus 2%) were significantly different between those withersus without increased impedance to flow using resistancendices, as well as between those with versus without notch-ng (preeclampsia: 23% versus 0%; FGR: 85% versus 2%,espectively).20 In another study of 182 women with chronicypertension undergoing UtA Doppler at 29 � 4 weeks, 36%ad increased resistance to flow. Rates of superimposed pre-clampsia (28% versus 5%), SGA fetuses (46% versus 14%),nd severe complications (60% versus 18%) were signifi-antly higher among cases with increased impedance to flow.
bability of Adverse Outcome in Preeclampsia
Score 2 Score 3 Score 4
79 35 1725% 34% 59%
37 � 4 36 � 4 32 � 516% 17% 53%10% 17% 24%
re 1: one abnormal parameter (high Pulsatility Index >1.2 or notchparameters; Score 4: four abnormal parameters.
oppler Waveform in Growth-Restricted Fetuses Delivered at
y09)
Doppler WaveformNormal (n � 185) P value
11% 0.0238.8 � 1.6 <0.001
0.6% 0.3215% <0.00110% <0.001
2524 � 379 <0.0019.3 � 10.2 <0.001
7.29 � 0.07 0.2011% <0.001
16.5 � 10.3 0.14
n Pro
ore 1
66%� 3
6%3%
s; Scoormal
ery D
rtern � 1
2.0
4465.10.07
10.2

M33g
AAUtspwaatwDreU11
DUatcaaa(laawse
CUtilbp
ohlfmntepF
fpteapeaDarc
eunDsrccmhorotpppcn
R
T
U
R
Monitoring of fetal well-being 261
oreover, gestational age at delivery (36.6 � 3.1 versus8.7 � 1.7 weeks) and birth weight (2409 � 698 versus146 � 517 g) were significantly different between the tworoups.21
ntiphospholipid Syndrome (APS)study with over 100 cases of APS showed that abnormaltA Doppler at completion of placentation was present in 20
o 30% of cases and it was independently associated withubsequent occurrence of adverse outcome (defined as FGR,reeclampsia, or stillbirth).22 Similarly, a smaller study of 43omen with APS showed that abnormal UtA Doppler was
ssociated with increased risk of preterm preeclampsia orbruption (LR � 5.6, 95% CI, 2.4-5.6).23 At variance withhese findings, a large study on 170 women with APS (allith history of habitual abortion) showed that abnormal UtAoppler at 24 weeks was not predictive of subsequent occur-
ence of preeclampsia or birth weight �10th centile.24 How-ver, a subanalysis suggested that presence of bilateral notch attA Doppler was a powerful predictor of preeclampsia (LR �2.8, 95% CI, 2.2-75) or SGA neonates (LR � 13.6, 95% CI,.9-96) among the 45 women with lupus anticoagulant.
iabetes MellitustA Doppler in the third trimester independently identifiesmong pregnancies with diabetes mellitus and vasculopathy,hose at increased risk of preeclampsia and greater risk ofesarean delivery for non-reassuring fetal status.25 Oncegain, the information provided by UtA Doppler operateslong a continuum, so that in women with diabetes mellitusntedating pregnancy the risk for adverse perinatal outcomedefined as operative delivery for fetal distress, preterm de-ivery, 5-minuteApgar score �5, low umbilical artery pH,nd SGA infants) is directly correlated with the severity of thebnormal UtA Doppler findings.26 Finally, among womenith gestational diabetes, abnormal UtA Doppler findings are
ignificantly associated with greater risk of subsequent pre-clampsia (positive LR of 10.4, 95% CI, 6.6-10.4).27
onclusionstA Doppler can identify women with obstetrical complica-
ions related to abnormal placentation. Such predictive abil-ty is often independent of other demographic, obstetric, oraboratory characteristics. UtA Doppler has the potential toe incorporated in the routine evaluation of women with
able 3 Predictive Ability of Uterine Artery Score for Adverse
tA Doppler Score Adverse Outcome (n)
0 37% (142/389)1 68% (128/188)2 74% (76/103)3 84% (42/50)4 100% (11/11)
eprinted with permission.17
reexisting medical conditions associated with increased risk
f abnormal placentation, as well as in the evaluation ofealthy women who experience obstetric complications re-
ated to placental vascular pathology. One of the appealingeatures of UtA Doppler is that the evaluation needs to beade only once in the late second or third trimester, as ab-ormal values are unlikely to improve after placental implan-ation is completed. UtA Doppler is also an ideal tool tostablish or rule out placental vascular origin of pathologicrocesses affecting the fetus, for example, in the presence ofGR.Screening of high-risk patients has also potential benefits
or those with normal results, including reassurance to theatient and benefit in quality of life, less need for unnecessaryesting in the third trimester, and reduced time lost frommployment while undergoing evaluations and rest. For ex-mple, a retrospective study on 170 women at high risk forreeclampsia due to history of preeclampsia, preterm deliv-ry, FGR, fetal demise, abruption, chronic hypertension, di-betes mellitus, or renal disease showed that normal UtAoppler at 24 weeks, which was found in 69% of cases, hadnegative-predictive value of 99% for subsequent occur-
ence of preeclampsia.5 Prospective studies are needed toonfirm these potential benefits.
The time is ripe for larger and better designed studies tovaluate the independent predictive ability of UtA Dopplersing multivariate analysis and defining unfavorable preg-ancy outcome with objective criteria. Confirmation of UtAoppler as prognosticator of outcome could herald wide-
pread implementation of this simple technique. It should beemembered that UtA Doppler is of little use for obstetricomplications in which fetal risk is not due to impaired pla-entation, eg, postterm pregnancy or premature rupture ofembranes.28,29 More studies are also needed to establishow UtA Doppler identification of patients at increased riskf adverse outcome can affect their management. It is cur-ently unproven whether increased frequency of monitoringf fetal wellbeing, closer ultrasonographic surveillance of fe-al growth, more frequent monitoring of maternal bloodressure or proteinuria, and administration of corticosteroidrophylaxis for fetal lung maturity may effect the outcome ofatients with abnormal UtA Doppler findings. Finally, theost–benefit analysis of implementation of UtA Doppler stilleeds to be tested.
eferences1. Arduini D, Rizzo G: Normal values of Pulsatility Index from fetal ves-
sels: a cross-sectional study on 1556 healthy fetuses. Perinat Med 18:
atal Outcome in Pregnancies with Obstetric Complications
Odds Ratio (95% CI) Likelihood Ratio
1.0 1.01.64 (1.00 to 2.70) 2.41.86 (1.00 to 3.54) 3.54.03 (1.77 to 10.32) 7.3
� (3.20 to �) �
Perin
165-172, 1990

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
262 A. Ghidini and A. Locatelli
2. Gudmundsson S, Marsal K: Umbilical artery and uteroplacental bloodflow velocity waveforms in normal pregnancy—a cross-sectional study.Acta Obstet Gynecol Scand 67:347-354, 1988
3. Aardema MW, Saro MC, Lander M, et al: Second trimester Dopplerultrasound screening of the uterine arteries differentiates between sub-sequent normal and poor outcomes of hypertensive pregnancy: twodifferent pathophysiological entities? Clin Sci (Lond) 106:377-382,2004
4. Parretti E, Mealli F, Magrini A, et al: Cross-sectional and longitudinalevaluation of uterine artery Doppler velocimetry for the prediction ofpre-eclampsia in normotensive women with specific risk factors. Ultra-sound Obstet Gynecol 22:160-165, 2003
5. Harrington K, Fayyad A, Takur V, et al: The value of uterine arteryDoppler in the prediction of uteroplacental complication in multipa-rous women. Ultrasound Obstet Gynecol 23:50-55, 2004
6. Ferrazzi E, Bulfamante G, Mezzopane R, et al: Uterine Doppler veloci-metry and placental hypoxic-ischemic lesion in pregnancies with fetalgrowth restriction. Placenta 20:389-394, 1999
7. Ghosh G, Breborowicz A, Brazert M, et al: Evaluation of third trimesteruterine artery flow velocity indices in relationship to perinatal compli-cations. J Matern Fetal Neonatal Med 19:551-555, 2006
8. Vergani P, Roncaglia N, Ghidini A, et al: Can we predict adverse neo-natal outcome in fetal growth restriction near term? Am J Obstet Gy-necol 195:S206, 2006 (abstract)
9. Lobos H, Rennie JM, Lees C: The natural history of fetal growth restric-tion in women with abnormal uterine artery Doppler. Prenat Diagn25:331-332, 2005
0. Vergani P, Andreotti C, Roncaglia N, et al: Doppler predictors of ad-verse neonatal outcome in the growth restricted fetus at 34 weeks’gestation or beyond. Am J Obstet Gynecol 189:1007-1011, 2003
1. Severi FM, Bocchi C, Visentin A, et al: Uterine and fetal cerebral Dopp-ler predict the outcome of third-trimester small-for-gestational age fe-tuses with normal umbilical artery Doppler. Ultrasound Obstet Gy-necol 19:225-228, 2002
2. McCowan LM, North RA, Harding JE: Abnormal uterine artery Dopplerin small-for-gestational-age pregnancies is associated with later hyper-tension. Aust NZ J Obstet Gynaecol 41:56-60, 2001
3. van Asselt K, Gudmundsson S, Lindqvist P, et al: Uterine and umbilicalartery velocimetry in pre-eclampsia. Acta Obstet Gynecol Scand 77:614-619, 1998
4. Frusca T, Soregaroli M, Platto C, et al: Uterine artery velocimetry inpatients with gestational hypertension. Obstet Gynecol 102:136-140,2003
5. Li H, Gudnason H, Olofsson P, et al: Increased uterine artery vascular
impedance is related to adverse outcome of pregnancy but is present inonly one-third of late third-trimester pre-eclamptic women.Ultrasound Obstet Gynecol 25:459-463, 2005
6. Korszun P, Dubiel M, Kudla M, et al: Doppler velocimetry for predict-ing outcome of pregnancies with decreased fetal movements. Acta Ob-stet Gynecol Scand 81:926-930, 2002
7. Hernandez-Andrade E, Brodszki J, Lingman G, et al: Uterine arteryscore and perinatal outcome. Ultrasound Obstet Gynecol 19:438-442,2002
8. Gudmundsson S, Korszun P, Olofsson P, et al: New score indicatingplacental vascular resistance. Acta Obstet Gynecol Scand 82:807-812,2003
9. Soregaroli M, Valcamonico A, Scalvi L, et al: Late normalisation ofuterine artery velocimetry in high risk pregnancy. Eur J Obstet GynecolReprod Biol 95:42-45, 2001
0. Frusca T, Soregaroli M: Role of uterine artery Doppler investigation inpregnant women with chronic hypertension. Eur J Obstet Gynecol79:47-50, 1998
1. Roncaglia N, Crippa I, Locatelli A, et al: Prediction of superimposedpreeclampsia using uterine artery Doppler velocimetry in women withchronic hypertension. Prenat Diagn 2008 (in press)
2. Le Thi Huong D, Wechsler B, Vauthier-Brouzes D, et al: The secondtrimester Doppler ultrasound examination is the best predictor of latepregnancy outcome in systemic lupus erythematosus and/or the an-tiphospholipid syndrome. Rheumatology 45:332-338, 2006
3. Farrell T, Dawson T: Can uterine artery Doppler velocimetry predictadverse pregnancy outcome in women with antiphospholipid syn-drome? Acta Obstet Gynecol Scand 80:609-610, 2001
4. Venkat-Raman N, Backos M, Teoh TG, et al: Uterine artery Doppler inpredicting pregnancy outcome in women with antiphospholipid syn-drome. Obstet Gynecol 98:235-242, 2001
5. Bracero LA, Schulman H: Doppler studies of the uteroplacental circu-lation in pregnancies complicated by diabetes. Ultrasound Obstet Gy-necol 1:391-394, 1991
6. Pietryga M, Brazert J, Wender-Ozegowska E, et al: Abnormal uterineDoppler is related to vasculopathy in pregestational diabetes mellitus.Circulation 112:2496-2500, 2005
7. Pietryga M, Brazert J, Wender-Ozegowska E, et al: Placental Dopplervelocimetry in gestational diabetes mellitus. J Perinat Med 34:108-110,2006
8. Brar HS, Horenstein J, Medearis AL, et al: Cerebral, umbilical, anduterine resistance using Doppler velocimetry in postterm pregnancy.J Ultrasound Med 8:187-191, 1989
9. Abramowicz JS, Sherer DM, Warsof SL, et al: Fetoplacental and utero-placental Doppler blood flow velocity analysis in premature rupture of
membranes. Am J Perinatol 9:353-356, 1992
AMC
Afbcsylmhficaminplhn
D
A
0d
ssessing Cardiac and Neurologicalaturation During the Intrauterine Period
urtis L. Lowery, MD, R. B. Govindan, PhD, Pamela Murphy, RN, and Hari Eswaran, PhD
The world’s first magnetoencephalography (MEG) system specifically designed for fetaland newborn assessment has been installed at the University of Arkansas for MedicalSciences. This noninvasive system called SARA (SQUID Array for Reproductive Assess-ment) consists of 151 primary superconducting sensors that detect biomagnetic fields fromthe human body. Since the installation of SARA, significant progress has been made towardthe ultimate goal of developing a clinical neurological assessment tool for the developingfetus. Using appropriate analysis techniques, cardiac and brain signals are recorded andstudied to gain new understanding of fetal maturation. It is clear from our investigationsthat a combination of assessment protocols including both fetal heart and brain activity isnecessary for the development of a comprehensive new method of fetal neurologicaltesting. We plan to implement such a test protocol for fetuses at high risk for neurologicalimpairment due to certain maternal risk factors and/or fetal diagnostic findings.Semin Perinatol 32:263-268 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS fetal magnetoenecephalogram, fetal magnetocardiogram, HRV measures
iapn
arArotifsrddw
AbNoefic
lthough there has been a decrease in perinatal morbidityand mortality rates of the fetus and neonate over the past
our decades, antenatal hypoxia and/or asphyxia continues toe a significant health problem leading to major motor andognitive disabilities such as cerebral palsy, hearing and vi-ual impairment, and mental retardation. Although for manyears both clinicians and the general population have be-ieved that birth trauma and perinatal asphyxia were the pri-
ary cause of these handicaps, clinical studies in recent yearsave disputed this misconception.1-7 Most experts in thiseld have estimated that the incidence of cerebral palsy asso-iated with labor events is around 10%. One major problemrises from the fact that it is currently impossible to deter-ine the timing, the type, the duration, or the severity of the
nsults that are associated with neurological deficits in theewborn. Terms such as perinatal asphyxia, intrapartum as-hyxia, hypoxic-ischemic encephalopathy, neonatal neuro-
ogical dysfunctional syndrome, and fetal-neonatal anemiaave all been used to describe the affected newborn. Theonselective use of these terms has produced great confusion
epartment of Obstetrics and Gynecology, University of Arkansas for Med-ical Sciences, Little Rock, AR.
ddress reprint requests to Curtis L. Lowery, MD, Department of Obstetricsand Gynecology, SARA Research Center, University of Arkansas forMedical Sciences, Little Rock, AR 72205. E-mail: LoweryCurtisL@
auams.edu
146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.006
n the clinical literature. Because a thorough investigationttempting to identify the cause of neonatal neurological de-ression is often not attempted or is incomplete, the diag-oses of perinatal asphyxia is many times made by default.8
Electronic fetal heart rate monitoring is commonly used tossess fetal well-being in utero. While a reassuring fetal heartate pattern predicts the birth of an infant with a 5-minutepgar score of seven or greater with an accuracy 99%, non-eassuring tests have been associated with a false-positive ratef greater than 50%.9 Traditionally the neurological matura-ion of the fetus has been assessed using ultrasound stud-es.10,11 Although it has been possible to observe and evaluateetal neurological development on a limited basis using ultra-ound, direct access to the fetal electro-cortical signals isequired for specific testing and analysis. Currently, evi-ence-based clinical decisions concerning fetal neurologicalamage as a result of hypoxia or asphyxia cannot be madeith conventional techniques.To address these issues, SQUID Array for Reproductive
ssessment (SARA) was developed through a grant providedy the National Institutes of Health/National Institute ofeurological Disorders and Stroke and is currently underperation at the University of Arkansas for Medical Scienc-s.12,13 The system has a 151 primary sensor array curved tot the shape of the maternal abdomen. This instrument isompletely noninvasive and detects weak biomagnetic fields
ssociated with the electrophysiological activity in the human263

bfaiuwatmmoft
MSTUAt6rtdctrww(fnstia
GTaperfihia
dpcpchoradTtasa
RFBuvmonsotdwiwcwsa
baparoatvtwact
stgn
T
*
264 C.L. Lowery et al
ody. To investigate the cardiac and neurological status of theetus, we conduct serial fetal magnetocardiography (fMCG)nd fetal magnetoencepalography (fMEG) recordings start-ng at 28 weeks of gestation.13-19 Newborn follow-up studiessing the same fMEG protocol20 are performed within 2eeks of delivery using a specially designed cradle that can be
ttached to the SARA system. All studies are performed withhe aim of providing improved monitoring techniques foraternal–fetal health and assisting physicians in the manage-ent of pregnancy and delivery. Some of the key results
btained through analysis of the signals obtained by SARArom the fetal cardiac and brain systems will be discussed inhe next sections.
ethodsubjectshe studies performed with SARA were approved by theniversity of Arkansas for Medical Sciences Human Researchdvisory Committee and informed written consent was ob-
ained from all subjects. A total of 433 fetal recordings lastingminutes were performed on fetuses with gestational ages
anging from 27 to 40 weeks. Three hundred seventeen ofhese were acquired from 72 fetuses classified as high riskue to maternal complications such as pregnancy-induced/hronic hypertension, hemoglobinopathies, or smoking21
hat may compromise normal fetal development. The high-isk group was further subdivided into fetuses of mothersho smoked (smokers; 55 datasets from 23 mothers), fetusesho were diagnosed with intrauterine growth restriction
IUGR, 36 datasets from 10 fetuses), and all other high-risketuses. Of the 72 high-risk fetuses, 7 (9 datasets) had pooreonatal outcome. The demographic information of theseubjects is given in Table 1. For details of the inclusion cri-eria for all high-risk mothers we refer to ref.21. The remain-ng 126 recordings were obtained from 37 healthy mothersnd fetuses who were classified as low risk.
eneral Recording Methods and Analysishe routine recording sessions range from 6 to 12 minutes incontinuous mode at a sampling rate of 312.5 Hz and a bandass of direct current (dc) to 100 Hz. The position and ori-ntation of the mother’s abdomen, relative to the sensor ar-ay, are determined using two localization coils placed atduciary points on the mother’s right and left side and one oner spine at the level of the umbilicus. These coils do not
nterfere with the MEG recordings. The fetal head positionnd distance of head from maternal abdominal surface are
able 1 Demographic Information of the High-Risk Mothers
MaternalAge*
Number ofSubjects Race
Number ofSubjects
18 to 20 11 White 3721 to 35 44 Black 3136 to 48 9 Hispanic (Others) 3
pInformation was not available for the remaining seven subjects.
etermined using a portable ultrasound scanner after theatient sits down in front of the array. A fourth localizationoil is then attached to the maternal abdomen at that site torovide additional positional information related to sensoroordinates. The ultrasound examination to evaluate fetalead position and distance from surface is repeated at the endf the study but before the patient moves from the array. Theaw SARA recording consists of maternal heart, fetal heart,nd brain signals. To perform data analysis we nullify theominant maternal heart vectors by orthogonal projection.his method is first applied to the raw signal to remove ma-
ernal heart artifact. At this point, the fetal heart data can benalyzed. This process is then reapplied to the residual dataet (devoid of maternal heart) to remove fetal heart artifact tonalyze the brain signals.
esultsetal Cardiac Systemeat-to-beat intervals were computed for all the fMCG signalssing threshold detection technique. Standard heart rateariability (HRV) measures such as standard deviation of nor-al to normal intervals (SDNN), root mean square deviation
f the successive differences (RMSSD), fraction (p) of theormal intervals greater than the chosen tolerance of x milli-econds from their previous values (pNNx), and the variancef the detrended time series at different time windows s con-aining s number of beat-to-beat intervals. To understand theifferential maturation of the high-risk fetuses comparedith the low-risk fetuses, we divided the data into the follow-
ng three gestational age groups, 27 to 30 weeks, 31 to 35eeks, and 36 to 40 weeks. Although we have repeated re-
ordings from the same subjects in multiple gestation ages,e treat them all independently based on the following as-
umptions: dependency of the heart rate on the gestation agend the state of the fetus.
Unlike SDNN, which captures the global variability in theeat-to-beat intervals, RMSSD captures the short-term vari-bility (and hence high-frequency component of the HRV).NNx is another measure that captures the short-term vari-bility and quantifies the fluctuations in the firing of the sinushythm. It is computed by calculating the ratio of the numberf normal to normal intervals which differ by a chosen toler-nce value of x milliseconds from their previous value to theotal number of intervals. We used three different tolerancealues, namely, 10, 15, and 20 milliseconds, and found thathe best difference between the groups was observed onlyith the tolerance of 10 milliseconds.21 All three measures
re indicators of the alterations in the cardiac dynamics andan be used to quantify the maturation of the fetus based onhe cardiac dynamics.
The results obtained for SDNN, RMSSD, and pNN10 arehown in Figure 1 in different gestational ages. In SDNNhere is a difference between the high-risk and low-riskroups in the 27 to 31 week and 36 to 40 week divisions ando difference in the 31 to 35 week division. In RMSSD and
NN10 there is a significant difference between the low-risk
awfwespfcFfT3wgln
p
PtAt
dilmmpaitdfl
signifi
Assessing cardiac and neurological maturation during the intrauterine period 265
nd high-risk groups in the 31 to 35 week and 360 to 400eek division as well. In the 31 to 35 week division low-risk
etuses had lower values of pNN10 and RMSSD comparedith high-risk fetuses, while in the 36 to 39 week division an
xactly opposite behavior was observed.21 We performed aubgroup analysis by separating the IUGR fetuses and com-ared their pNN10 measures with low-risk fetuses. Weound that in the 31 to 35 week division there was a signifi-ant difference between IUGR fetuses and low-risk fetuses.urther, in this gestational week division the values of pNN10
or IUGR fetuses were less compared with the low-risk fetuses.21
here was no difference between these two groups in the 27 to1 week division. In the 36 to 40 week division no comparisonas made because of fewer number of datasets in the IUGRroup. We did not find any significant difference between theow-risk fetuses and fetuses of the smokers and fetuses with pooreonatal outcome either.For low-risk fetuses there was a positive trend in the
Figure 1 Comparison of HRV measures of low-risk and higSDNN, (B, E, H) RMSSD and (C, F, I) pNN10. The differenin the inset and P � 0.05 was considered to be statistically
NN10 (�2 � 0.052; P � 0.0114) and RMSSD (�2 � 0.048; i
� 0.012) as a function of gestational age, while no suchrend was observed for SDNN (�2 � 0.012; P � 0.220).21
lso no trend was observed in any of the HRV measures forhe high-risk fetuses.
The values of pNN10 and RMSSD in the 31 to 35 weekivision show that high-risk fetuses demonstrate an increase
n maturation rate compared with low-risk fetuses. In theater gestational age, low-risk fetuses tend to mature at nor-
al rates while the high-risk fetuses did not show continuingaturation. This fact combined with the dependency ofNN10 and RMSSD of the low-risk fetuses with gestationalge and absence of such a trend for high-risk fetuses clearlyndicate that the low-risk fetuses show a progressive matura-ion while high-risk fetuses show an early maturation. Theifference in the pNN10 values between low-risk and IUGRetuses in 31 to 35 week division indicate that the later groupack normal maturation.
To quantify the variations in the fetal cardiac beat-to-beat
fetuses in three different gestational age groups (A, D, G)een the groups was assessed using Student’s t-test is givencant. (Color version of figure is available online.)
h-riskce betw
ntervals, we performed detrended time series (DTS) analysis.

Trtots(2fbfaasol
twmwtrpsfaIhasi
266 C.L. Lowery et al
his approach consists of the following three steps: (i) aunning average is performed on the beat-to-beat intervalime series for a chosen window “s” (usually in powers of 2) tobtain a trend series; (ii) The trend obtained is then sub-racted from the beat-to-beat interval to get the DTS; and (iii)tandard deviation (SD) is computed for the DTS. The stepsi-iii) are repeated for different s values usually ranging fromto one-fourth of the length of the data and SD is computed
or each value of s. Here, we varied s from 2 beats to 256eats. In Figure 2 beat-to-beat intervals, the trend obtainedor a window containing 32 beats, and the DTS are shown forlow-risk fetus (Fig. 2A-C), high-risk fetus (Fig. 2D-F), andn IUGR fetus (Fig. 2G-I). In general, SD for a large value ofcorresponds to the quantifying low-frequency componentf the beat-to-beat variability and vice versa. The SDs are
Figure 2 Beat-to-beat intervals (in beats per minute, bpmfetus (B, E, F), respectively, show the moving average os containing 32 beats. (C, F, I) Detrended time series, Dthe trend (shown in the middle panel). Note that qualitalow in the IUGR fetus. (Color version of figure is availab
og-transformed to produce Gaussian-distributed error and p
hen subjected to least-squares regression to identify trendsith gestation age. The residuals resulting from trend re-oval are compared between different groups using t-testsith multiple-comparison adjustment via step-down permu-
ation. These results are given in Table 2. Low-risk and high-isk groups show difference only in the low-frequency com-onent (at large time scales). Low-risk and high-risk fetuseshow significant difference from the IUGR group at high-requency component (at short time scales). This result is ingreement with the pNN10 results obtained for low-risk andUGR fetuses. Further, low-risk and high-risk fetuses showigher variability compared with high-risk and IUGR fetusesnd, between the low-risk and high-risk fetuses, low-riskhowed higher variability. These results point to the fact thatn IUGR fetuses the autonomous nervous system is sup-
(A) low-risk fetus, (D) high-risk fetuses, and (E) IUGRd for the data shown in (A, D, E) for a window size ofich is the original data (shown in the top panel) minus
he fluctuations in DTS are high in the low-risk fetus andine.)
) forbtaineTS, whtively tle onl
ressed.22

FTshfsgp0�bpaed0a
bebtoa
SIwtsTpboattca
R
TC
SSSSSSSS
*T
THI�
HSHLLLILII
*P
Assessing cardiac and neurological maturation during the intrauterine period 267
etal Brain Systemo analyze the fetal brain data, we performed spectral analy-is on the residual data that is devoid of maternal and fetaleart signals. The data were filtered in a band width rangingrom 0.5 to 25 Hz using a band-pass filter. We compared thepectral results of the low-risk fetuses with all the high-riskroup fetuses. For this purpose power spectra were com-uted for all 151 SARA sensors with a frequency resolution of.1 Hz. For each sensor, the spectral power was computed in(0.5-4 Hz), � (4-8 Hz), � (8-13 Hz), and � (13-25 Hz)
ands and normalized by the total power which is sum of theowers in all four bands. The power in each band was aver-ged over all the sensors to get the estimate of the same. Thestimated powers in the four bands were compared betweenifferent groups using Student’s t-test and a P value less than.1 was considered to be statistically significant. The resultsre summarized in Table 3. There is a significant difference
able 2 Comparison of the SD(s) of the Detrended Time Serieompared for the Three Groups of Fetuses
Variable
Low-Risk vs High-Risk
Raw Adjusted
D(2) 0.429 0.532 0D(4) 0.959 0.959 0D(8) 0.822 0.8936 0D(16) 0.373 0.526 0D(32) 0.164 0.283 0D(64) 0.066 0.140 0D(128) 0.030* 0.082* 0D(256) 0.0381 0.097 0
Statistically significant cases.he raw P values and also the P values adjusted for multiple compa
be statistically significant.
able 3 Comparison of the Spectral Power of Low-Risk (LR),igh-Risk (HR), Smokers (SM), and Poor Outcome (PO) and
UGR Fetuses in Four Different Spectral Band � (0.5 to 4 Hz),(4 to 8 Hz), � (8 to 13 Hz), and � (13 to 25 Hz) Using t-Test
Group
P Values Obtained by Testing theNull Hypothesis that the Two Groups
Have the Same Mean Value at theSignificance Level of 0.1
� � � �
R–PO 0.094* 0.690* 0.098* 0.082*M–PO 0.048* 0.513 0.061* 0.053*R–PO 0.536 0.653 0.766 0.536R–HR 0.001* 0.001* 0.001* 0.08*R–SM 0.001* 0.001* 0.001* 0.02*R–PO 0.19 0.001* 0.23 0.001*UGR–LR 0.108 0.298 0.122 0.076*UGR–HR 0.035* 0.001* 0.04* 0.63UGR–PO 0.97 0.003* 0.99 0.002*UGR–SM 0.013* 0.001* 0.02* 0.398
Statistically significant difference.
< 0.1 is considered to be statistically significant.etween the groups at least in one of the spectral bandsxcept of high risk and smokers, where there is no differenceetween them in any of the spectral bands. A further study inhis direction by identifying the continuous and discontinu-us brain patterns may help to understand these differencesnd will be pursued in the future.
ummaryn summary, investigation of magnetic fetal brain responsesith MEG is becoming an established field of research. Using
he SARA system, we have performed many fMEG and fMCGtudies in both low-risk and high-risk patient populations.o improve fetal neurological testing, a combination of com-rehensive assessment protocols including fetal heart andrain activity is valuable. We have developed a combinationf recording parameters using auditory and visual stimulind spontaneous brain activity for a multimodal approach tohe investigation of fetal health. This protocol can be referredo as SNAP (SARA Neurological Assessment Protocol) andan be used to evaluate the neurological status of the fetusnd newborn.
eferences1. Low JA: Reflections on the occurrence and significance of antepartum
fetal asphyxia. Best Pract Res Clin Obstet Gynaecol 18.3:375-382, 20042. Nelson KB: Defining hypoxic-ischemic birth events. Dev Med Child
Neurol 45.1:71-72, 20033. Nelson KB: Neonatal encephalopathy: etiology and outcome. Dev Med
Child Neurol 47(5):292, 20054. Nelson KB, Dambrosia JM, Ting TY, et al: Uncertain value of electronic
fetal monitoring in predicting cerebral palsy. N Engl J Med 334(10):613-618, 1996
5. Nelson KB, Grether KB: Causes of cerebral palsy. Curr Opin Pediatr11(6):487-491, 1999
6. Grether JK, Nelson KB: Maternal infection and cerebral palsy in infantsof normal birth weight. JAMA 278(3):207-211, 1997
7. Grether JK, Nelson KB, Walsh E, et al: Intrauterine exposure to infec-tion and risk of cerebral palsy in very preterm infants. Arch PediatrAdolesc Med 157(1):26-32, 2003
8. Freeman JM, Nelson KB: Intrapartum asphyxia and cerebral palsy.
ifferent Window Sizes for the Three Groups of Fetuses Are
P Value
-Risk vs IUGR High-Risk vs IUGR
Adjusted Raw Adjusted
0.016 0.081 0.6280.003a 0.001a 0.006a
0.026 0.012 0.0350.211 0.058 0.0980.621 0.165 0.1990.704 0.184 0.1990.621 0.079 0.1140.395 0.038 0.081
using step-down permutations are given. P < 0.05 is considered to
s at D
Low
Raw
.005
.001a
.010
.121
.491
.704
.512
.275
risons
Pediatrics 82(2):240-249, 1988

1
1
1
1
1
1
1
1
1
1
2
2
2
268 C.L. Lowery et al
9. Miller DA, Rabello YA, Paul RH: The modified biophysical profile: ante-partum testing in the 1990s. Am J Obstet Gynecol 174(3):812-817, 1996
0. Awoust J, Levi S: Neurological maturation of the human fetus. Ultra-sound Med Biol 2:583-587, 1983
1. Luz NP: Auditory evoked response of the human fetus: simplifiedmethodology. J Perinat Med 19(3):177-183, 1991
2. Robinson SE, Burbank MB, Fife AA, et al: A biomagnetic instrument forhuman reproductive assessment. Biomag 2000, Proceedings of the12th International Conference in Biomagnetism: Nenonen J, et al (eds):Helsinki Univ. of Tech., Espoo, Finland, 2001, pp 919-922
3. Eswaran H, Lowery CL, Robinson SE, et al: The challenges of recordinghuman fetal auditory evoked fields using magnetoencephalography.J Matern Fetal Med 9(5):303-307, 2000
4. Preissl H, Lowery CL, Eswaran H: Fetal magnetoencephalography: cur-rent progress and trends. Exp Neurol 190:S37-S43, 2004
5. Holst M, Eswaran H, Lowery CL, et al: Development of auditory evokedfields in human fetuses and newborns: a longitudinal MEG study. Clin
Neurophysiol 116(8):1949-1955, 20056. Eswaran H, Wilson JD, Preissl H, et al: Short-term serial magnetoen-cephalographic recordings of fetal auditory evoked responses. Neuro-sci Lett 331(2):128-132, 2002
7. Eswaran H, Wilson JD, Preissl H, et al: Magnetoencephalographic re-cordings of visual evoked brain activity in the human fetus. Lancet360(9335):779-780, 2002
8. Eswaran H, Lowery CL, Wilson JD, et al: Functional development ofthe visual system in human fetus using magnetoencephalography. ExpNeurol 190:S52-S58, 2004
9. Rose DF, Eswaran H: Spontaneous neuronal activity in fetuses andnewborns. Exp Neurol 190:S28-S36, 2004
0. Haddad N, Shihabuddin B, Lowery CL, et al: Magnetoencephalographyin healthy neonates. Clin Neurophysiol 117:289-294, 2006
1. Govindan RB, Lowery CL, Campbell JQ, et al: Early maturation of sinusrhythms in high-risk fetuses. Am J Obstet Gynecol 196:572e1-572e7,2007
2. Kikuchi A, Shimizu T, Hayashi A, et al: Nonlinear analyses of heart ratevariability in normal and growth-restricted fetuses. Early Hum Dev
82:217-226, 2006
AM
Pocagcintii
asJdtdCiwo
D
A
0d
ntenatal Testing: Diabetes Mellitusichael P. Nageotte, MD
Diabetes complicating pregnancy is a problem for which fetal surveillance testing isconsidered to be the standard of care. In response to the unacceptable frequency ofstillbirth in such pregnancies, fetal testing historically was first introduced to managewomen whose pregnancies were complicated by diabetes. Essentially all forms of ante-partum testing have been used to assess fetal well-being during the third trimester ofpregnant diabetics. The contraction stress test became established as the “gold standard,”yet other testing protocols have been used successfully. It is clear that control of diabetesthroughout gestation, not just in the later stages, is more important for optimal outcomethan is a specific form of fetal testing. Biweekly testing has become the standard and withwell-controlled diabetics, allowing the gestation to continue until the onset of spontaneouslabor, even when the gestation exceeds 40 weeks, is appropriate management with normaltesting.Semin Perinatol 32:269-270 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS diabetes, fetal surveillance, antepartum testing
bpadUte
NIht2vtpsuNaNirw
N
erinatal mortality in diabetic women continues to be re-ported at significantly higher rates than in women with-
ut diabetes.1 How much of this difference is due to poorontrol of maternal disease, increased risk of congenitalnomalies, pregnancy complications such as intrauterinerowth restriction (IUGR) or preeclampsia, or true uteropla-ental insufficiency is unclear. While sudden unexplainedntrauterine fetal death has became a far less common preg-ancy complication for women with diabetes, concern overhe adequacy of placental function at various gestational agesn such patients has led to the routine use of fetal surveillancen diabetic pregnancies.
Historically, before the implementation of fetal testing, di-betic women often had their delivery date determined by theeverity of their disease. Following a protocol initiated at theoslin Clinic in an effort to prevent stillbirth, women withiabetes complicated by vascular disease were delivered at 35o 36 weeks or earlier. Women with less advanced diseaseelivered no later than 37 to 38 weeks. Many of these wereesarean deliveries and were associated with a significant
ncidence of neonatal respiratory morbidity and mortality. Itas unclear if such management was necessarily improvingutcome when compared with prior management protocols.
epartment of Obstetrics and Gynecology, University of California, Irvine,CA.
ddress reprint requests to Michael P. Nageotte, MD, Associate Chief Med-ical Officer, Long Beach Memorial Medical Center, Professor, Depart-ment of Obstetrics and Gynecology, University of California, Irvine, CA
w90806. E-mail: [email protected]
146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.008
With three main goals of antepartum fetal surveillanceeing avoidance of fetal deaths, early detection of fetal com-romise, and prevention of unnecessary premature birth, di-betes complicating pregnancy poses an ideal metabolic disor-er to assess the potential value of various testing modalities.nfortunately, there have been no adequately sized prospec-
ively randomized studies that compare the efficacy of differ-nt testing protocols.
onstress Test (NST)n many centers today, the NST is the preferred antepartumeart rate test for women with diabetes. While testing is ini-iated generally at 32 weeks gestation, it is started as early as8 weeks gestation in diabetic women with renal disease,ascular disease, or suspected intrauterine growth restric-ion. Golde and Montoro reported using the NST in diabeticatients with the contraction stress (CST) as backup.2 Notillbirths were reported in 107 insulin-dependent patientssing this testing protocol. In a review of 13 studies using theST weekly for fetal surveillance, Lavery reported that
mong the 23 stillbirths reported within a week of a reactiveST which did not result from acute clinical events, 10 were
n women with insulin-dependent diabetes.3 Based on thiseport and others, the recommended frequency of testing foromen with diabetes increased to twice per week.In 1995, Kjos and coworkers reported on twice weekly
ST and amniotic fluid volume assessment in 2134 women
ith diabetes in pregnancy.4 There were no stillbirths within269

4ffloefi
CTportcCapt
mwiiWpsuottl
BTaBpJinonBf
DBsdnra
wOtoacoldima
CFpttmfbtpt
R
1
1
270 M.P. Nageotte
days of the last test and the overall corrected stillbirth rateor the group was 1.4/1000. Further, while use of amnioticuid assessment did not appear significant, factors predictivef a need for Cesarean delivery for fetal labor were the pres-nce of a deceleration, nonreactivity, or the presence of bothndings.
ontraction Stress Testhe CST has a longer history of use for fetal surveillance inregnancies complicated with diabetes than any other meansf testing. Based on the evaluation of the fetal heart rateesponse to uterine contractions, the CST has the potential toest for a chronic condition and serve as a surrogate for pla-ental function. Ray and Freeman reported on the use of theST in a cohort of diabetic women.5 Thirty-eight women hadweekly CST performed with the results blinded. Of the nineatients whose last CST before delivery was a positive test,wo had a fetal demise and three had low 5-minute Apgar.
This led to the wide adoption on the CST in the manage-ent of diabetes in pregnancy. While performed onlyeekly, the predictive value of a negative test remained very
mpressive for various centers implementing this form of test-ng.6 However, there are significant problems with the CST.
hile there are very rarely false-negative results, the false-ositive rates approach 50 to 60%. Further, the frequency ofuch positive testing led to delivery for an abnormal test inpwards of 10% of tested diabetic women. Thus, the CST isverall less efficient, more costly, and more inconvenient thathe NST. Consequently, few perinatal centers continue to usehe CST as their primary means of antepartum fetal surveil-ance.
iophysical Profile (BPP)he BPP combines acute (NST, fetal breathing, movement,nd tone) and chronic (amniotic fluid quantity) markers. ThePP has been used for fetal surveillance in insulin-dependentatients with reportedly excellent negative-predictive value.ohnson and Lange reported on the use of twice weekly BPPn 50 insulin-dependent and 188 gestational diabetic preg-ancies.7 No stillbirths were reported; abnormal BPP rate wasnly 3.3%, and of the eight women whose last BPP was ab-ormal, three had significant neonatal morbidity. Thus, thePP used twice weekly appears to be an adequate test withew unnecessary interventions.
oppler Velocimetryracero and Schulman and Olofsson and coworkers de-cribed the use of umbilical artery Doppler velocimetry iniabetic pregnancies.8,9 Significant positive associations wereoted between systolic/diastolic (S/D) ratio and maternal se-um glucose level. Further, elevated S/D ratios were associ-
ted with subsequent fetal labor intolerance.Landon and Gabbe reported on 35 insulin-dependentomen followed with umbilical artery Doppler studies.10
ne-half of the women with vascular disease complicatingheir diabetes had abnormal Doppler studies, while only 12%f uncomplicated diabetics had such findings. Further, theseuthors stated that the S/D ratio was independent of glycemicontrol. Johnstone and coworkers reported on a large cohortf diabetic pregnancies followed with both BPP and Dopp-er.11 Of concern was the finding that over half of the womenelivered for an abnormal BPP had a normal Doppler but the
nfants were severely depressed. It would appear that mild tooderate fetal acidosis may not be detected by umbilical
rtery Doppler.
onclusionsetal surveillance remains the standard in pregnancies com-licated with diabetes. What is unclear is the efficacy of suchesting for whatever type in patients with well-controlled orrue gestational diabetes. Fetal heart rate monitoring as pri-ary surveillance would appear appropriate with a testing
requency of every 3 to 4 days. Abnormal tests should have aackup test performed due to the high rate of false-positiveesting. This is an area that would benefit from well-designedrospective studies addressing the issue of test type as well asiming and frequency of testing.
eferences1. Kodama Y, Sameshima H, Ikenoue T: Regional population-based study
on pregnancy outcomes in women with diabetes mellitus in Japan. JObstet Gynecol Res 33(1):45-48, 2007
2. Golde SH, Montoro M: The role of nonstress tests, fetal biophysicalprofile and contraction stress tests in the outpatient management ofinsulin-requiring diabetic pregnancies. Am J Obstet Gynecol 148:269-275, 1984
3. Lavery JP: Nonstress fetal heart rate testing. Clin Obstet Gynecol 25:689-694, 1982
4. Kjos SL, Leung A, Henry OA, et al: Antepartum surveillance in diabeticpregnancies: predictors of fetal distress in labor. Am J Obstet Gynecol173(5):1532-1539, 1995
5. Ray M, Freeman R: Clinical experience with the Oxytocin challengetest. Am J Obstet Gynecol 114:1-6, 1972
6. Freeman RK, Anderson G, Dorchester W: A prospective multi-institu-tional study of antepartum fetal heart rate monitoring. I. Risk of peri-natal mortality and morbidity according to the antepartum fetal heartrate test results. Am J Obstet Gynecol 143:771-777, 1982
7. Johnson JM, Lange IR: Biophysical profile scoring in the management ofthe diabetic pregnancy. Obstet Gynecol 72:841-845, 1988
8. Bracero L, Schulman H: Umbilical artery velocimetry in diabetes andpregnancy. Obstet Gynecol 68:654-658, 1986
9. Oloffson P, Lingman G, Marsal K, et al: Fetal blood flow in diabeticpregnancy. J Perinat Med 15:545-553, 1987
0. Landon MB, Gabbe SG: Doppler umbilical artery velocimetry in preg-nancy complicated by insulin-dependent diabetes mellitus. Obstet Gy-necol 73:961-965, 1989
1. Johnstone F, Steel JM, Haddad NG, et al: Doppler umbilical artery flowvelocity waveforms in diabetic pregnancy. Br J Obstet Gynaecol 99:
135-140, 1992
AHR
TtifiipottFcsciddu
U
A
0d
ntepartum Testing in Patients withypertensive Disorders in Pregnancy
oger K. Freeman, MD
Antepartum fetal testing in pregnant patients with hypertensive disorders may be beneficialin preventing stillbirth and hypoxic sequelae in the fetus. The highest risk patients in thiscategory are those with intrauterine growth restriction, superimposed preeclampsia, asso-ciated medical complications such as diabetes, systemic lupus erythematosis, chronicrenal disease, or history of a prior stillbirth. The current recommended method of primarytesting is a twice weekly modified biophysical profile with either a full BPP or a contractionstress test for backup evaluation of those patients with lack of reactivity or decreasedamniotic fluid volume on a modified biophysical profile. Even uncomplicated patients withchronic hypertension or pregnancy-induced hypertension carry an increased risk of peri-natal mortality and for these patients testing should begin at 33 to 34 weeks gestation.Patients with complications of intrauterine growth restriction, preeclampsia, diabetes,systemic lupus erythematosis, or chronic renal disease should have antepartum testingbegin when intervention for fetal indications is judged to be appropriate, usually beginningat about 26 weeks gestation. Doppler velocimetry may be helpful in further evaluation ofthose patients in the early third trimester with abnormal primary testing.Semin Perinatol 32:271-273 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS hypertension, antepartum testing, IUGR, modified biophysical profile
ppcpiapsouttlop
MFiU
here are various hypertensive disorders that may compli-cate pregnancy. The three main entities are chronic hyper-
ension with diagnosis preceding pregnancy, pregnancy-nduced hypertension where the elevated blood pressure isrst recognized during pregnancy, and preeclampsia where
n addition to hypertension developing during pregnancy theatient manifests the onset of proteinuria and may also havether systemic findings including liver function abnormali-ies, platelet count decrease, hemolysis, and in the extremehe patient may develop full-blown eclampsia with seizures.urther complications may affect the mother, the worst beingerebral hemorrhage. Other disorders may have hyperten-ion as part of the disease process including such diagnoses ashronic renal disease, systemic lupus erythematosis, vascularnvolvement with diabetes, and the hemolytic uremic syn-rome. In these later diagnoses sometimes it is difficult toetermine whether the patient has preeclampsia or protein-ria due to one of these other causes.
niversity of California at Irvine, Long Beach Memorial Medical Center, andMiller Children’s Hospital, Long Beach, CA.
ddress reprint requests to Roger K. Freeman, MD, University of Californiaat Irvine, Department of Obstetrics and Gynecology, 2801 Atlantic Ave.,
fLong Beach, CA 90801. E-mail: [email protected]
146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.009
The fetus also is impacted by hypertensive disorders inregnancy. Because of vasoconstriction affecting the utero-lacental circulation, intervillous space blood flow may beompromised and this can result in interruption in the sup-ly of oxygen to the fetus. When uteroplacental insufficiency
s present, another complication may develop, a reduction inmniotic fluid volume. Oligohydramnios may result in loss ofrotection of the umbilical cord from mechanical compres-ion and can further result in decreased respiratory functionf the placenta. Chronic fetal compromise resulting fromteroplacental insufficiency caused by these various hyper-ensive disorders may result in intrauterine growth restric-ion (IUGR) and abnormal fetal heart rate patterns duringabor and may cause permanent CNS damage from fetal hyp-xia and in the extreme may result in antepartum or intra-artum fetal demise.
ethods for Antepartumetal Evaluationn Hypertensive Patientsntil the early 1970s the only methods available to evaluate
etal well-being in such conditions were fetal movement
271

cctshmwemdmsTvcsmfp
rcddtedttataIs
dattbhCutasoapcnRfaraal
lnotwtftss
cbafMamCtafb
mchanBtm
mcpl
WPIwt3aAtnmaripb
272 R.K. Freeman
ounting and clinical measurement of uterine growth. Bio-hemical methods to evaluate uteroplacental function werehe first strategies introduced using laboratory values thathowed some correlation with fetal well-being. Twenty-fourour urinary and plasma estriol determinations were the pri-ary biochemical methods employed for evaluation of fetalell-being in hypertensive gravidas. While there was a gen-
ral correlation with fetal growth, the utilization of theseethods for the timing of delivery aimed at avoiding fetaleath or damage was imprecise.1 In the 1970s biophysicalethods including the contraction stress test (CST), non-
tress test (NST), and imaging ultrasound were introduced.he biophysical profile (BPP) and umbilical artery Dopplerelocimetry were introduced in the 1980s and today variousombinations of these tests for both primary surveillance andecondary evaluation (“backup” support of abnormal pri-ary test results) are the principle methods employed for
etal surveillance in patients with hypertensive disorders inregnancy.IUGR is associated with hypertensive pregnancies and rep-
esents a clinical manifestation signaling significant uteropla-ental insufficiency, placing the fetus at increased risk foreath or damage. For this reason serial ultrasound scans toetect lagging fetal growth are a necessary piece of antenatalesting in hypertensive pregnancies. Scans should occur ev-ry 3 to 4 weeks beginning as early as 26 weeks after initialating scans in the first trimester and anatomical survey inhe second trimester establishing baseline numbers. In pa-ients who develop preeclampsia growth scans should occurt the time of diagnosis and be repeated every 3 to 4 weekshereafter. Doppler velocimetry may be helpful in differenti-ting between growth lag due to uteroplacental insufficiency,UGR due to anomalies, genetic defects, infection, and con-titutional small size.
Antepartum fetal heart rate testing (AFHRT) was originallyone using the CST.2 While this method has been largelybandoned for primary surveillance due to the difficulty andime-consuming nature of the test, and some contraindica-ions to the test such as premature labor, rupture of mem-ranes, or prior classical cesarean section, there is no test thatas proven to have fewer false-negative results than theST.3-5 This test includes an acute marker, which is the eval-ation for fetal heart rate accelerations, and a chronic marker,he fetal heart rate response to uterine contractions, which is
good measure of uteroplacental reserve. Today the CSTerves mainly as a backup test when a NST is not reactive andr the modified BPP is either nonreactive or has reducedmniotic fluid volume. Nipple stimulation has largely re-laced the administration of IV oxytocin for induction ofontractions. The test, when used for primary surveillance,eed be done only once a week following a negative test.eactive positive CSTs do not demand intervention before
etal maturity and if such a patient labors after this test result,bout half of the patients will require intervention for non-eassuring fetal status.6 However, if the CST is nonreactivend positive, the likelihood of tolerating labor is very smallnd one study indicates that there may be significant neuro-
ogical damage in some cases.7 hIn the 1980s the NST was introduced for primary surveil-ance but disappointing results showed it to be no better thano testing in four randomized controlled trials when donence weekly.8-11 A study by Boehm and coworkers showedwice weekly NSTs were less likely to be followed by stillbirthhen done twice weekly but the results did not reach statis-
ical significance.12 While the NST is still used as a sole testor fetal well-being, it is only an acute marker of fetal condi-ion at the time of the test and is not a good predictor of futuretatus of the fetus. For this reason we do not use it as atand-alone test.
In the 1980s Manning and coworkers introduced the con-ept of the BPP, which includes the measurement of fetalreathing, tone, movement, and amniotic fluid volume inddition to the NST.13 With a maximum of two points givenor each function measured, a perfect score of 10 is possible.
ost clinicians consider a score below 6 to be non-reassuringnd depending on the gestational age a decision for deliveryay be made. The BPP has a false-negative rate similar to theST but in addition gives information on fetal malforma-
ions. It contains both acute markers (NST, movement, tone)nd a chronic marker (amniotic fluid index [AFI]). It is usedor both primary surveillance on a once weekly basis and as aackup test for the NST or modified BPP.Eden and coworkers14 first introduced the concept of theodified BPP, which includes an acute marker (NST) and a
hronic marker (AFI), and subsequent evaluations of the testave shown sensitivity and specificity comparable to the CSTnd full BPP for primary surveillance.15 When the NST part ison-reactive or the AFI part of the test is low, a CST or fullPP is used for backup.16 The modified BPP should be donewice weekly. This is the most common primary surveillanceethod used today in hypertensive patients.Doppler umbilical arterial velocimetry appears to have itsaximum use as secondary surveillance especially in pregnan-
ies early in the third trimester where reactivity may not beresent because of gestational age and intervention may be de-
ayed based on the test result in such very premature gestations.
hich Hypertensiveatients Should Be Tested?
n a large multi-institutional study of AFHRT hypertensionas the second most common indication for fetal testing and
he incidence of positive CSTs as the worst test result was.9% compared with 1.6% for postdates and 7.4% for IUGRs the primary indication for testing. In the most recentmerican College of Obstetricians and Gynecologists prac-
ice bulletin on chronic hypertension in pregnancy,17 they doot recommend antepartum fetal testing in patients withild to moderate blood pressure abnormalities and in the
bsence of preeclampsia and/or IUGR. Sibai and coworkersecommended testing all chronic hypertensives in 198318 butn 2007 they recommend testing only those hypertensiveatients with preeclampsia and/or IUGR.19 In a 1994 studyy Rey and Couturier, they found uncomplicated chronic
ypertension to have almost twice the incidence of IUGR and
ogtCwth
WiDajtImTslpetspThlddsrsawwplgwscomT
mrpdbdibcvb
ieeha
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
Antepartum testingtesting for hypertensive disorders 273
ver twice the perinatal mortality rate compared with theeneral population.20,21 In hypertensive patients with a his-ory of a prior stillbirth, we found the incidence of a positiveST to be 12% compared with only 3.7% if a prior stillbirthas the only indication for testing.22 Thus it would appear
hat all patients with a diagnosis of mild to moderate chronicypertension in pregnancy are candidates for AFHRT.
hen to Start AFHRTn Hypertensive Gravidas?epending on when in pregnancy stillbirths are likely to occurnd when AFHRT is likely to result in intervention for fetaleopardy, one must decide when to initiate testing. Assuminghat ultrasound surveillance has been initiated, the detection ofUGR should prompt testing as soon as fetal viability is deter-ined to be sufficient to allow intervention for an abnormal test.his appears to be about 26 weeks in most institutions. In atudy reported in 1991, Pircon and coworkers at our institutionooked at 917 patients with chronic hypertension (n � 408) orregnancy-induced hypertension (PIH) (n � 509) without pre-clampsia followed with CST for primary surveillance.23 Duringhe course of testing some of the patients developed preeclamp-ia and some were found to have IUGR. They also looked at allatients who presented with stillbirths whether tested or not.he results showed that there was only one fetal death in testedypertensive patients and that patient had only NST surveil-
ance. There were nine fetal deaths in untested patients with aiagnosis of chronic hypertension or PIH. There were no fetaleaths in the patients who were followed with CST primaryurveillance and there were no neonatal deaths from prematu-ity in patients who had intervention for abnormal AFHRT re-ults. If one looks at the gestational ages where intervention forbnormal AFHRT results occurred and the gestational agehere fetal death occurred, all cases that occurred before 34eeks were in patients with complicating diagnoses of superim-osed preeclampsia, diabetes, chronic renal disease, or systemic
upus erythematosis. Using the results of this large trial, we be-in testing uncomplicated chronic hypertensives or patientsith PIH without preeclampsia at 33 to 34 weeks. In hyperten-
ive patients with superimposed preeclampsia, IUGR, diabetes,hronic renal disease, or systemic lupus erythematosis we rec-mmend beginning testing as soon as fetal viability is deter-ined to be sufficient to allow intervention for an abnormal test.his is usually about 26 weeks.There are no randomized trials comparing the recom-ended testing protocols described here to no testing with
espect to outcome. However, less rigorous studies of ante-artum testing in the pregnant patient with a hypertensiveisorder appear to suggest a benefit in the reduction of still-irth and may help to avert permanent hypoxia-caused CNSamage in their children. While randomized studies compar-
ng AFHRT to no testing will not be done due to the perceivedenefit and medical–legal considerations, further studiesomparing methods of testing, especially outlining the role ofarious Doppler velocimetry methodologies including um-
ilical, uterine, and middle cerebral artery evaluations, maymprove outcome especially in patients with IUGR in thearly third trimester. There is certainly a great need also tovaluate long-term outcomes in the progeny of patients withypertensive disorders in pregnancy who are followed withntepartum testing for fetal well-being.
eferences1. Neilson JP: Biochemical tests of placental function for assessment on
pregnancy. Cochrane Database Syst Rev (2):CD000108, 20032. Freeman R: The use of the oxytocin challenge test for antepartum
clinical evaluation or uteroplacental respiratory function. Am J ObstetGynecol 121(4):481-489, 1975
3. Freeman R, Anderson G, Dorchester W: A prospective multi-institu-tional study of antepartum fetal heart rate monitoring. I. Risk of peri-natal mortality and morbidity according to antepartum fetal heart ratetest results. Am J Obstet Gynecol 143:771-777, 1982
4. Freeman R, Anderson G, Dorchester W: A prospective multi-institu-tional study of antepartum fetal heart rate monitoring. II. Contractionstress test versus nonstress test for primary surveillance. Am J ObstetGynecol 143:778-781, 1982
5. Nageotte M, Towers C, Asrat T, et al: The value of a negative antepar-tum test: contraction stress test and modified biophysical profile. Ob-stet Gynecol 84:231-234, 1994
6. Braly P, Freeman R: The significance of fetal heart rate reactivity with apositive oxytocin challenge test. Obstet Gynecol 50:689-694, 1977
7. Beischer N, Drew J, Ashton P, et al: Quality of survival of infants withcritical fetal reserve detected by antenatal charditocography. Am J Ob-stet Gynecol 146:662-670, 1983
8. Kidd L, Patel N, Smith R: Non-stress antenatal cardiotocography—aprospective randomized clinical trial. Br J Obstet Gynecol 92:1156-1159, 1985
9. Flynn A, Kelly J, Mansfield H, et al: A randomized controlled trial ofantepartum non-stress cardiotocography. Br J Obstet Gynecol 89:427-433, 1982
0. Brown V, Sawyers S, Parsons R, et al: The value of antepartum cardio-tocography in the management of high risk pregnancy: a randomizedcontrolled trial. Br J Obstet Gynecol 89:716-722, 1982
1. Lumley J, Lester J, Anderson I, et al: A randomized trial of weeklycardiotocography in high-risk obstetric patients. Br J Obstet Gynecol1018-1026, 1983
2. Boehm FH, Salyer S, Shah D: Improved outcome of twice weekly non-stress testing. Obstet Gynecol 67:566-568, 1986
3. Manning F, Platt L, Sipos L: Antepartum fetal evaluation: developmentof a biophysical profile. Am J Obstet Gynecol 136:787-795, 1980
4. Eden R, Seifert R, Kodack L, et al: A modified biophysical profile forantenatal surveillance. Obstet Gynecol 71:365-369, 1988
5. Clark S, Sabey P, Jolley K: Non-stress testing with acoustic stimulationand amniotic volume assessment: 5973 tests without unexpected fetaldeath. Am J Obstet Gynecol 160:694-697, 1989
6. Nageotte M, Towers C, Asrat T, et al: Perinatal outcome with the mod-ified biophysical profile. Am J Obstet Gynecol 170:1672-1676, 1994
7. American College of Obstetricians and Gynecologists Practice BulletinNumber 29. Chronic Hypertension in Pregnancy. Washington, DC,ACOG, July, 2001
8. Sibai B, Abdella T, Anderson G: Pregnancy outcome in 211 patientswith mild chronic hypertension. Obstet Gynecol 61:571-576, 1983
9. Sibai B: Chronic hypertension in pregnancy, in Queenan J (ed): Man-agement of High Risk Pregnancy. Washington, DC, ACOG, 2007
0. Rey E, Couturier A: The prognosis of women with chronic hyperten-sion in pregnancy. Am J Obstet Gynecol 171:410-416, 1994
1. Jain L: Effect of pregnancy induced and chronic hypertensionon preg-nancy outcome. J Perinatol 17:425-427, 199
2. Freeman R, Dorchester W, Anderson G: The significance of a previousstillbirth. Am J Obstet Gynecol 151:7-13, 1985
3. Pircon R, Lagrew D, Towers C, et al: Antepartum testing in the hyper-tensive patient: when to begin. Am J Obstet Gynecol 164:1563-1570,
1991
FJ
NpoefigtFAautq
D
A
2
etal Growth Restrictionena Miller, MD, Sifa Turan, MD, and Ahmet A. Baschat, MD
Normal fetal growth is determined by the genetically predetermined growth potential andfurther modulated by maternal, fetal, placental, and external factors. Fetal growth restric-tion (FGR) is a failure to reach this potential and is clinically suspected if sonographicestimates of fetal weight, size, or symmetry are abnormal. Integration of fetal anatomyassessment, amniotic fluid dynamics, uterine, umbilical, and fetal middle cerebral arteryDoppler is the most effective approach to differentiate potentially manageable placenta-based FGR from aneuploidy, nonaneuploid syndromes, and viral infection. Although pla-cental dysfunction results in a multisystem fetal syndrome with impacts on short- andlong-term outcome, only cardiovascular and behavioral responses are helpful to guidesurveillance and intervention. Early-onset FGR before 34 weeks gestation is readily rec-ognized but challenging to manage as questions about optimal delivery timing remainunanswered. In contrast, near-term FGR provides less of a management challenge but isoften missed as clinical findings are more subtle. Once placenta-based FGR is diagnosed,integrating multivessel Doppler and biophysical profile score provides information onlongitudinal progression of placental dysfunction and degree of fetal acidemia, respec-tively. Choosing appropriate monitoring intervals based on anticipated disease accelera-tion and intervention when fetal risks exceed neonatal risks are the prevailing currentmanagement approaches.Semin Perinatol 32:274-280 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS fetal growth restriction, placental dysfunction, antenatal surveillance, biophysicalprofile scoring, Doppler ultrasound
PPEclbsptvttrpbtnlctt
ormal fetal growth depends on maternal, fetal, placen-tal, and external factors combined with the genetically
redetermined growth potential.1 The multisystem impactsf placental dysfunction produce an increase in the alreadylevated background mortality and morbidity.2,3 In pretermetal growth restriction (FGR) uncertainty about delivery tim-ng increases perinatal mortality and morbidity due to iatro-enic prematurity.4,5 Near-term questions about deliveryiming are less critical. However, difficulty in identifying termGR contributes to over 50% of unexplained stillbirths.6,7
ccurate diagnosis, appropriate surveillance, and certaintybout timing interventions are considered important prereq-isites to improve these statistics. A systematic approach tohe diagnosis and management of placenta-based FGR re-uires recognition of the clinical spectrum of this condition.
epartment of Obstetrics, Gynecology, and Reproductive Sciences, Univer-sity of Maryland, Baltimore, MD.
ddress reprint requests to Ahmet A. Baschat, MD, Department of Obstet-rics, Gynecology, and Reproductive Sciences, University of Maryland,Baltimore, 405 Redwood Street, Baltimore, MD 21201. E-mail:
74 0146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1053/j.semperi.2008.04.010
athophysiology oflacental Dysfunction
ffective first-trimester trophoblastic adherence initiates pla-ental development, ultimately resulting in the formation of aow impedance and high capacitance circulatory interfaceetween the fetal and maternal circulations as well as a carrierystem for principal nutrients.8 Despite this efficiency of thelacental unit in normal pregnancies, the fetus is vulnerableo nutrient deprivation when placental dysfunction super-enes. As the placenta extracts a fixed proportion of the nu-rient stream (70% of glucose and 40% of oxygen supplied tohe uterus), fetal nutrition is restricted to the surplus thatemains after placental demands have been met.8 Even mildlacental dysfunction may restrict nutrient transfer andlood flow to the fetus while placental nutrition is main-ained.9 When growth delay becomes clinically apparent, aumber of fetal responses including adjustments in metabo-
ism, endocrine axes, and hematologic parameters as well asardiovascular and behavioral responses may already haveaken place. Of these, cardiovascular and behavioral manifes-ations can be used in FGR management. While not amenable
o management, adjustments in other organ systems still have
au
MoAsrbcggddcTtksbahb
cesocfptmditlcitanm
DoAwroaflcve
opide
CBtFpbprr
Fbdsciflflw
Fetal growth restriction 275
profound impact on short- and long-term outcome andltimately define the consequences of placental dysfunction.
aturational Impactsf Placental Dysfunctionreduction of uterine perfusion below 0.6 mL/Kg/min mea-
urably decreases fetal glucose and amino acid delivery. Thiseduction in substrate availability leads to downregulation ofoth the insulin and the insulin-like growth factor-1 endo-rine axis and hepatic glucose metabolism.10 The result islycogenolysis with a decrease in liver size, redirection ofluconeogenic amino acids from endogenous protein break-own, and eventually, delayed longitudinal growth.8 A re-uction in fatty acid transfer decreases the availability of pre-ursor molecules for a wide range of bioactive substances.hese changes are important antecedents for the manifesta-
ion of FGR.8 With increased accumulation of lactate andetone bodies the fetal brain, heart, and erythrocytes becomecavengers for these metabolites, thereby maintaining acid–ase balance. Endocrine responses correlate with the degreend level of hypoxemia and include central and peripheralypothyroidism, upregulation of the adrenocortical axis, andone demineralization.8
Hematologic responses of the fetus initially consist of aompensatory increase in red cell mass but eventually mayxacerbate placental vascular dysfunction. Hypoxemia-timulated extramedullary hematopoiesis may no longer bebserved as placental dysfunction escalates.8 Under these cir-umstances the risk for thrombocytopenia may increase 10-old11 and increased blood viscosity, decreased erythrocyteliability, as well as platelet aggregation worsen intraplacen-al blood flow dynamics further.12 Cellular and humoral im-une dysfunction also correlates to the degree of fetal aci-emia and explains the higher susceptibility to postpartum
nfection.8 While these consequences of placental dysfunc-ion have no immediate value in the diagnosis and surveil-ance in FGR, they illustrate the multisystem effects of pla-ental dysfunction. Accordingly, compromise at many levelss undetectable by antenatal surveillance and not amenable toherapy. When FGR manifests early in pregnancy, markedbnormalities of placental function are typically evident. Inear-term FGR these abnormalities are far more subtle anday escape clinical evaluation.
oppler Evidencef Placental Dysfunction
n elevated uterine artery Doppler index and/or persistentaveform notching beyond 24 weeks indicate increased spi-
al artery blood flow resistance in the maternal compartmentf the placenta. In the fetal compartment the earliest sign ofbnormal villous perfusion is a decrease in umbilical venousow.9 Umbilical artery end-diastolic velocity (UA EDV) de-reases and resistance indices become elevated when 30% ofillous vasculature is abnormal.13 Progression to absent- or
ven reversed end-diastolic velocity occurs when 60 to 70% (f the villous vascular tree has been damaged.14 However,lacental vascular dysfunction with fetal hypoxemia may ex-
st in the absence of any of these Doppler findings.15,16 Theetection of such subtle placental dysfunction requires thexamination of fetal responses (Figs. 1-3).
irculatory andehavioral Responses
o Placental Dysfunctionetal circulatory responses to placental insufficiency may beassively mediated by high placental blood flow resistance ory active organ autoregulation. Redistribution of cardiac out-ut toward the left ventricle occurs with relative increases inight ventricular afterload as documented by a decrease in theatio of Doppler indices in cerebral and umbilical arteries
igure 1 Flow velocity waveforms obtained from the uterine arteryeyond 24 weeks gestation. In the first patient (A) high-volumeiastolic flow is established, indicating successful trophoblast inva-ion. Elevated placental vascular resistance is associated with a de-line in diastolic velocities and a subsequent rise in the Dopplerndex (B). Persistence of an early diastolic notch in the uterine arteryow velocity waveform is evidence of increased spiral artery bloodow resistance. Frequently “notching” is more subtle beyond 32eeks (C) than in the late second or early third trimesters
D). (Reprinted with permission.36)

(a(tataa
ipDcdvaf
avidfoitrdmgd
n
fiswgdDBmeae
RFaBbAmEbfcafirsLmp
276 J. Miller, S. Turan, and A.A. Baschat
cerebroplacental Doppler ratio � CPR).16 This is virtuallylways present in fetuses with absent end diastolic velocityAEDV). Diversion of umbilical venous blood from the livero the heart and decrease in cerebral blood flow impedancere active vascular phenomena. Together these compensa-ory responses result in preferential channeling of oxygennd nutrient-rich umbilical venous blood to the myocardiumnd brain (venous redistribution and brain sparing).17
Reversal of umbilical artery end-diastolic velocity and ev-dence of abnormal forward cardiac function indicate therogression to late cardiovascular manifestations. Increasingoppler indices in the precordial veins are the hallmark ofirculatory deterioration. This is most apparent through aecrease in atrial systolic forward velocities in the triphasicenous flow velocity waveform. In extreme cases, increasedtrial pressure waves are transmitted all the way back into theree umbilical vein, resulting in pulsatile flow (Figs. 4 and 5).
Fetal behavioral responses to placental insufficiency canlso be subdivided into early and late. Unlike in the cardio-ascular system, early behavioral abnormalities are not clin-cally apparent as they predominantly consist of maturationalelay. Clinically most relevant is delayed establishment ofetal heart rate reactivity, which may be absent in up to 60%f FGR pregnancies before 32 weeks. Individual fetal behav-ors are lost in a relatively preserved sequence that is relatedo gestational age and the degree of hypoxemia. If fetal heartate reactivity was present, it is lost first. Fetal breathingisappears next followed by decreased gross body move-ents and tone. This sequence is often accompanied by a
radual decline in amniotic fluid volume. Spontaneous lateecelerations may also be observed as a late finding.In preterm FGR before 30 to 32 weeks, late Doppler ab-
Figure 2 The normal umbilical artery flow velocity wavein proportion to systole toward term (A). Moderate abnoresistance and are associated with a decline in end-diastovascular tree is abnormal (50-70%), end-diastolic velocimagnitude of placental blood flow resistance and the fetminimal (D), moderate (E), or severe (F). In the latte(Reprinted with permission.36)
ormalities precede the deterioration of the biophysical pro- p
le score (BPS). While the progression from brain sparing topontaneous late decelerations has been reported within 2eeks, the interval is variable and probably influenced byestational age, maternal factors, and severity of placentalisease.18-22 For the clinician, escalating ductus venosusoppler indices indicate accelerating fetal disease, while thePS may still be normal. In term FGR where Doppler abnor-alities are subtle, isolated brain sparing may provide such
vidence. However, deterioration of the BPS is more likelyssociated with oligohydramnios or may have no anteced-nts.23
elationship Betweenetal Testing Parametersnd Acid–Base Balance
oth Doppler and biophysical parameters predict acid–basealance in FGR. A decreased CPR, brain sparing, and UAEDV indicate an increased risk for hypoxemia with a nor-al pH as long as venous Doppler parameters are normal.levation of venous Doppler indices, either alone or in com-ination with umbilical venous pulsations, increase the riskor acidemia. Dependent on the cutoff (2 versus 3 SD) and theombinations of veins examined, sensitivity for prediction ofcidemia in preterm FGR ranges from 70 to 90% and speci-city from 70 to 80%.24,25 The five-component BPS shows aeliable and reproducible relationship with the fetal pH irre-pective of the underlying pathology and gestational age.26
oss of fetal tone and movement are typically observed at aedian pH of 7.10 and therefore provide the most consistentrediction of prelabor academia.27 In contrast to Doppler
as marked positive end-diastolic velocity that increasesies in the villous vascular structure raise the blood flowocities (B). When a significant proportion of the villousy be absent (C) or even reversed (D). Depending on theiac function, reversal of end-diastolic velocities may beprecordial venous flows were universally abnormal.
form hrmalitlic vel
ties maal cardr case
arameters which are under the influence of several factors,

rats
DGdTisevvcc
DIadpcrenpwgnt
SGAmcBdialsdi
raempcBiotsnmgtAvom
MoGIt
FtrbmbDstaD
Fetal growth restriction 277
egulation of fetal behaviors is more closely linked to oxygen-tion of their regulatory centers. Therefore, a closer correla-ion between behaviors and acid–base status has been ob-erved at steady state.
iagnosis ofrowth Restrictionue to Placental Disease
he diagnosis of FGR due to placental disease is essential todentify the fetus in need of management. This excludes con-titutionally small fetuses and those with other underlyingtiologies where outcomes are unlikely improved by inter-ention. The physical manifestations of FGR and the cardio-ascular signs of placental disease are listed in Table 1. Anyombination of these abnormalities should raise the suspi-
igure 3 The normal middle cerebral artery flow pattern has rela-ively little diastolic flow (A). With elevation of placental blood flowesistance the changes in the middle cerebral artery waveform maye subtle, although the cerebroplacental ratio may become abnor-al as in fetus B. With progressive placental dysfunction there may
e an increase in the diastolic velocity, resulting in a decrease in theoppler index (Brain sparing, C). With marked brain sparing, the
ystolic down slope of the waveform becomes smoother so thathe waveform almost resembles that of the umbilical artery (D). Thessociated rise in the mean velocity results in a marked decline in theoppler index. (Reprinted with permission.36)
ion of placenta-based FGR. In preterm FGR diagnostic t
oppler abnormalities of the umbilical arteries are common.n term FGR attention should focus on the middle cerebralrtery Doppler and amniotic fluid volume. The differentialiagnosis always needs to consider aneuploidy, nonaneu-loid syndromes, viral infection, other toxins (smoking, co-aine), and the constitutionally small fetus. A clinical history,eview of dates, sonographic exclusion of anomalies, consid-ration of invasive tests, and serial observations are oftenecessary to confirm the diagnosis. Once the diagnosis oflacenta-based FGR has been made, perinatal management isarranted. This requires the consideration of fetal status andestational age. A reduction of potentially preventable peri-atal damage therefore relies on an accurate assessment ofhese variables.
urveillance of therowth-Restricted Fetus
s there is no intrauterine therapy for FGR, accurate deter-ination of fetal status by antenatal surveillance is a key
omponent to direct intervention and monitoring intervals.oth of these requirements must be met to decrease perinatalamage. In this context performance of fetal surveillance tests
s greatly influenced by the manifestation of fetal compromisecross gestational age. Biophysical parameters are closely re-ated to acid–base balance and therefore reflect current fetaltatus. Doppler parameters and amniotic fluid volume reflectisease progression and therefore guide in the choice of mon-
toring intervals.The American College of Obstetricians and Gynecologists
ecommends twice weekly modified BPS (nonstress test andmniotic fluid index) and umbilical artery Doppler velocim-try for the surveillance of FGR.28 Application of this recom-endation requires some modification based on the clinicalresentation. If fetal heart rate reactivity is not established, asan be expected in early-onset FGR, a full five-componentPS is required. If there are signs of advancing disease as
ndicated by loss of umbilical artery end-diastolic velocity orligohydramnios, frequency of testing may be increased upo daily testing to avoid unexpected stillbirth.29 In FGR pre-enting before 32 weeks where safe prolongation of preg-ancy may be a key component of improving outcome, aore complex integrated approach has been proposed. Inte-
rated fetal testing requires the concurrent evaluation of ar-erial and venous Doppler with the BPS. In addition to UAEDV and oligohydramnios, onset of brain sparing or ele-ated venous Doppler indices are also considered as markersf accelerating disease requiring appropriate adjustment ofonitoring intervals (Tables 2 and 3).8
anagementf Placenta-Basedrowth Restriction
n the perinatal management of FGR the timing of interven-ions depends on the balance of fetal and neonatal risks. In
erm FGR where the primary problem lies in identifying the
fibdrr
forward flow may be lost (D) or reversed (E, F). (Reprinted wi
Ftrcobserved (B, C, D). (Reprinted with permission.36)
T
P
C
T
●●●●●●●●
278 J. Miller, S. Turan, and A.A. Baschat
etus at risk the neonatal risks are low. There are no random-zed trials of elective delivery once the diagnosis of FGR haseen made near term. However, prospective stillbirth riskata from a large US cohort suggest that in the presence ofisk factors such as FGR delivery as early as 37 weeks may beequired to decrease stillbirth rate.30 From this it may be
e throughout the cardiac cycle under normal circum-obtained at the inlet (A) versus the outlet (B). With
ard flow during atrial systole (C). If progressive atrialth permission.36)
able 1 Manifestations of Diagnostic Value
hysical manifestations of fetal growth delay● Sonographically estimated fetal weight below the 10th
percentile● Abdominal circumference <5th percentile● HC/AC ratio <10th percentile● Individualized growth potential <10th percentile● Femur length/abdominal circumference ratio >23.5● Abdominal circumference growth velocity <11 mm in
14 daysardiovascular manifestations of placental dysfunction● Increased uterine artery Doppler index and/or
notching● Increased umbilical artery Doppler index● Decreased middle cerebral artery Doppler index● Decreased cerebroplacental Doppler ratio● Maximum amniotic fluid pocket <2 cm● Amniotic fluid index <5 cm
able 2 Signs of Accelerating Placental Dysfunction
Umbilical artery absent or reversed end-diastolic velocityDecreased cerebroplacental ratioOnset of brain sparingElevated venous Doppler indicesUmbilical vein pulsationsOligohydramniosAbnormal biophysical profile score
Figure 4 In the ductus venosus blood flow is always antegradstances. Pulsatility is less pronounced in waveform patternsimpaired cardiac forward function there is a decline in forw
igure 5 In the umbilical vein the normally constant waveform pat-ern may show subtle pulsations with elevated placental blood flowesistance (A). With progressive increase in precordial venous indi-es monophasic, biphasic, and even triphasic pulsations may be
Spontaneous late decelerations

ctma
bwcWsnsalamtto
tpasonavcpdrfi
tltvw
asWpctecut
R
T
A
BB
S
F
F
Fetal growth restriction 279
oncluded that a low threshold for delivery should be used inhese fetuses. Delivery criteria may include documented lungaturity, complete arrest of fetal growth, oligohydramnios,
bnormal BPS, and UA AEDV.Matters are more complicated in preterm FGR presenting
efore 34 weeks where deterioration may occur rapidly andhere prematurity-related morbidity is significantly in-
reased compared with appropriately grown counterparts.31
ith early-onset growth restriction viability (50% neonatalurvival) is reached at 26 weeks and over half of these neo-ates do have major morbidity until 29 weeks. The neonatalurvival benefit for each additional day in utero is estimatedt 2% until 29 weeks gestation.32 Moreover, long-term fol-ow-up from the Growth Restriction Intervention Trial showsn increased risk of prematurity provoked neurodevelop-ental delay if these fetuses are delivered too early.33 Unfor-
unately there are no concluded randomized interventionrials that identify optimal intervention in this critical subsetf growth-restricted fetuses.The Growth Restriction Intervention Trial was a prospec-
ive randomized multicenter study of over 500 women withregnancies complicated by FGR. Patients were randomlyssigned to immediate versus delayed delivery based on phy-ician discomfort. No difference in short-term outcome wasbserved but immediate delivery was associated with highereonatal mortality while delayed delivery carried the price ofhigher stillbirth rate. The long-term impacts on neurode-
elopment were not anticipated by these short-term out-omes. Based on these studies it has been concluded that saferolongation of pregnancy offers the best combination ofecreased perinatal mortality, morbidity, and improved neu-odevelopment.34 In this context, the trial of umbilical andetal flow in Europe compares the performance of computer-
able 3 Integrated Fetal Testing in Fetal Growth Restriction
Finding Inter
bnormal UA and/or CPR; normal MCAand veins
Asphyxia extrem
PS >8/10, AFV normal Increased risk folood flow redistributionLow MCA, normal veins Hypoxemia poss
BPS >8/10, AFV normal Increased risk foignificant blood flow redistributionUA A/REDV normal veins BPS > 6/
10, OligohydramniosHypoxemia comm
asphyxia possicompromise
etal compromiseIncreased DV pulsatility BPS >6/10,
OligohydramniosHypoxemia comm
asphyxia likely
etal decompensationCompromise by above criteria, absent
or reversed DV a-wave, pulsatile UVBPS <6/10, Oligohydramnios
Cardiovascular icompromise, shigh perinatalof intervention
zed fetal heart rate analysis with ductus venosus Doppler. In
he integrated fetal management approach multivessel Dopp-er and BPS are combined as indicated in Table 3. This pro-ocol is based on the observation that integration of testingariables provides improved prediction of outcome evenhen the computerized fetal heart rate analysis is used.35
Integrated fetal testing is initiated at 24 weeks. If umbilicalrtery pulsatility is increased but end-diastolic flow is pre-erved, weekly BPS and biweekly Dopplers are performed.
ith the onset of brain-sparing, BPS and Doppler are re-eated weekly. Testing frequency escalates with the degree ofardiovascular compromise. Delivery is based on a combina-ion of late Doppler and biophysical abnormalities. The vari-ty of management approaches to these highest risk pregnan-ies is not based on strong evidence and underlines thergent need for development of randomized managementrials.
eferences1. Gardosi J, Chang A, Kalyan B, et al: Customised antenatal growth
charts. Lancet 339:283-287, 19922. Baschat AA, Gembruch U, Reiss I, et al: Relationship between arterial
and venous Doppler and perinatal outcome in fetal growth restriction.Ultrasound Obstet Gynecol 16:407-413, 2000
3. Bernstein IM, Horbar JD, Badger GJ, et al: Morbidity and mortalityamong very-low-birth-weight neonates with intrauterine growth re-striction. The Vermont Oxford Network. Am J Obstet Gynecol 182:198-206, 2000
4. Zeitlin J, Ancel PY, Saurel-Cubizolles MJ, et al: The relationship be-tween intrauterine growth restriction and preterm delivery: an empir-ical approach using data from a European case-control study. BJOG107:750-758, 2000
5. GRIT Study Group: A randomized trial of timed delivery for the com-promised preterm fetus: short term outcomes and Bayesian interpreta-tion. BJOG 110:27-32, 2003
6. Clausson B, Cnattignius S, Axelsson O: Outcomes of post-term births;the role of fetal growth restriction and malsformations. Obstet Gynecol
tion Action
e Deliver for obstetric, or maternal factorsonly, fortnightly Doppler
partum distress Weekly BPS
sphyxia rare Deliver for obstetric, or maternal factorsonly, weekly Doppler
partum distress BPS 2 times/wk
cidemia ornset of fetal
>34 weeks: deliver; <32 weeks:antenatal steroids repeat all testingdaily
cidemia or >32 weeks: deliver<32 weeks: admit, steroids,
individualize testing daily vs. threetimes per day
lity, metabolich imminent,lity irrespective
Deliver at tertiary care center with thehighest level of NICU care
preta
ely rar
r intra
ible, a
r intra
on, able, o
on, a
nstabitillbirtmorta
94:758-762, 1999

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
280 J. Miller, S. Turan, and A.A. Baschat
7. Froen JF, Gardosi JO, Thurmann A, et al: Restricted fetal growth insudden intrauterine unexplained death. Acta Obstet Gynecol Scand83:801-807, 2004
8. Baschat A: fetal responses to placental insufficiency: an update. BJOG111:1031-1041, 2004
9. Rigano S, Bozzo M, Ferrazzi E, et al: Early and persistent reduction inumbilical vein blood flow in the growth-restricted fetus: a longitudinalstudy. Am J Obstet Gynecol 185:834-838, 2001
0. Reece EA, Wiznitzer A, Le E, et al: The relation between human fetalgrowth and fetal blood levels of insulin-like growth factors I and II,their binding proteins, and receptors. Obstet Gynecol 84:88-95, 1994
1. Baschat AA, Gembruch U, Reiss I, et al: Absent umbilical artery end-diastolic velocity in growth-restricted fetuses: a risk factor for neonatalthrombocytopenia. Obstet Gynecol 96:162-166, 2000
2. Trudinger B, Song JZ, Wu ZH, et al: Placental insufficiency is charac-terized by platelet activation in the fetus. Obstet Gynecol 93:180, 1999
3. Giles WB, Trudinger BJ, Baird PJ: Fetal umbilical artery flow velocitywaveforms and placental resistance: pathological correlation. Br J Ob-stet Gynaecol 92:31-38, 1985
4. Morrow RJ, Adamson SL, Bull SB, et al: Effect of placental embolizationon the umbilical arterial velocity waveform in fetal sheep. Am J ObstetGynecol 161:1055-1060, 1989
5. Hecher K, Spernol R, Stettner H, et al: Potential for diagnosing immi-nent risk to appropriate- and small-for-gestational-age fetuses byDoppler sonographic examination of umbilical and cerebral arterialblood flow. Ultrasound Obstet Gynecol 2:266-271, 1992
6. Bahado-Singh RO, Kovanci E, Jeffers A, et al: The Doppler cerebropla-cental ratio and perinatal outcome in intrauterine growth restriction.Am J Obstet Gynecol 180:750-756, 1999
7. Baschat A: The fetal circulation and essential organs—a new twist to anold tale. Ultrasound Obstet Gynecol 27:349-354, 2006
8. Hecher K, Bilardo CM, Stigter RH, et al: Monitoring of fetuses withintrauterine growth restriction: a longitudinal study. Ultrasound Ob-stet Gynecol 18:564-570, 2001
9. Ferrazzi E, Bozzo M, Rigano S, et al: Temporal sequence of abnormalDoppler changes in the peripheral and central circulatory systems ofthe severely growth-restricted fetus. Ultrasound Obstet Gynecol 19:140-146, 2002
0. Baschat AA, Gembruch U, Harman CR: The sequence of changes inDoppler and biophysical parameters as severe fetal growth restrictionworsens. Ultrasound Obstet Gynecol 18:571-577, 2001
1. Cosmi E, Ambrosini G, D’Antona D, et al: Doppler, cardiotocography,and biophysical profile changes in growth-restricted fetuses. Obstet
Gynecol 106:1240-1245, 20052. Baschat AA, Galan HL, Bhide A, et al: Doppler and biophysical assess-ment in growth restricted fetuses: distribution of test results. UltrasoundObstet Gynecol 27:41-47, 2006
3. Manning FA, Hill LM, Platt LD: Qualitative amniotic fluid volumedetermination by ultrasound: antepartum detection of intrauterinegrowth retardation. Am J Obstet Gynecol 139:254-258, 1981
4. Rizzo G, Capponi A, Talone PE, et al: Doppler indices from inferiorvena cava and ductus venosus in predicting pH and oxygen tension inumbilical blood at cordocentesis in growth-retarded fetuses. Ultra-sound Obstet Gynecol 7:401-410, 1996
5. Baschat AA, Güclü S, Kush ML, et al: Venous Doppler in the predictionof acid-base status of growth-restricted fetuses with elevated placentalblood flow resistance. Am J Obstet Gynecol 191:277-284, 2004
6. Manning FA, Snijders R, Harman CR, et al: Fetal biophysical profilescore. VI. Correlation with antepartum umbilical venous fetal pH. Am JObstet Gynecol 169:755-763, 1993
7. Vintzileos AM, Fleming AD, Scorza WE, et al: Relationship betweenfetal biophysical activities and umbilical cord blood gas values. Am JObstet Gynecol 165:707-713, 1991
8. American College of Obstetricians and Gynecologists (ACOG): Intra-uterine Growth Restriction. ACOG Pract Bull 12:1-12, 2000
9. Divon MY, Girz BA, Lieblich R, et al: Clinical management of the fetuswith markedly diminished umbilical artery end-diastolic flow. Am JObstet Gynecol 161:1523-1527, 1989
0. Kahn B, Lumey LH, Zybert PA, et al: Prospective risk of fetal death insingleton, twin, and triplet gestations: implications for practice. ObstetGynecol 102:685-692, 2003
1. Garite TJ, Clark R, Thorp JA: Intrauterine growth restriction increasesmorbidity and mortality among premature neonates. Am J Obstet Gy-necol 191:481-487, 2004
2. Baschat AA, Cosmi E, Bilardo CM, et al: Predictors of neonatal outcomein early-onset placental dysfunction. Obstet Gynecol 109:253-261,2007
3. Thornton JG, Hornbuckle J, Vail A, et al: GRIT study group. Infantwellbeing at 2 years of age in the Growth Restriction Intervention Trial(GRIT): multicentred randomised controlled trial. Lancet 364:513-520, 2004
4. Lees C, Baumgartner H: The TRUFFLE study—a collaborative publiclyfunded project from concept to reality: how to negotiate an ethical,administrative and funding obstacle course in the European Union.Ultrasound Obstet Gynecol 25:1005-1007, 2005
5. Turan S, Turan OM, Berg C, et al: Computerized fetal heart rate anal-ysis. Doppler ultrasound and biophysical profile score in the predictionof acid-base status of growth-restricted fetuses. Ultrasound Obstet Gy-necol 30:750-756, 2007
6. Baschat AA, Hecher K: Fetal growth restriction due to placental disease.
Semin Perinatol 28:67-80, 2004
AML
Ttrtm
obomtnpfTab
S
A
0d
ntenatal Fetal Assessment:ultifetal Gestation—An Overview
awrence D. Devoe, MD
As prevalence of multifetal gestation has increased in the United States, antenatal surveil-lance of these pregnancies has gained importance. This article focuses on the assessmentof twin pregnancy, since critical data are lacking for the surveillance of higher ordermultiple gestations. Twin pregnancies encounter risks that differ in nature, frequency, andintensity from those seen in singleton pregnancies. Most of these risks stem from subnor-mal or discordant fetal growth or abnormalities of placentation. Sonographic modalitiesplay key roles in antepartum surveillance. These include fetal biometry, serial growthstudies, amniotic fluid volume assessment, Doppler velocimetry of fetal-placental circula-tion, and biophysical profile testing. Fetal heart rate testing, specifically nonstress testing,has also been used extensively in twin surveillance. This article examines the specificapplication of these modalities to twin gestation and reviews the best evidence available fortheir support. Assessment of unique risk conditions of twin–twin transfusion, monoamni-otic twinning, and intrauterine death of one twin is addressed. Based on current data, astrategic outline for assessment of twin pregnancy is presented.Semin Perinatol 32:281-287 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS multifetal gestation, antenatal testing, ultrasound, Doppler velocimetry, fetal heartrate, biophysical profile
mdgmt
gcmpaicwtttotRpwi
his article describes the approaches for antenatal surveil-lance of multifetal gestations. It examines the evidence
hat supports these surveillance tools and strategies and theirelative merits and shortcomings. The focus is on twin gesta-ion as few data exist on the antenatal testing of higher orderultiple gestations.With the increasing use of assisted reproductive technol-
gy, multifetal gestation and, specifically twin pregnancy, hasecome more prevalent in the United States. Greater use ofbstetric ultrasound has also increased the likelihood thatultifetal gestation will be diagnosed before the third trimes-
er of pregnancy, providing increased opportunity for ante-atal surveillance of these pregnancies. Assessment of multi-le fetuses provides unique challenges since it must consideractors that increase the risk of adverse perinatal outcomes.hese risk factors stem from maternal sources (advanced age,nemia, gestational diabetes and hypertension, preterm la-or) and fetal sources (increased rates of congenital malfor-
ection of Maternal Fetal Medicine, Department of Obstetrics and Gynecol-ogy, Medical College of Georgia, Augusta, GA.
ddress reprint requests to Lawrence D. Devoe, MD, Department of Obstet-rics and Gynecology, Medical College of Georgia, 1120 15th Street,
aAugusta, GA 30912. E-mail: [email protected]
146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.011
ations, abnormal placentation and placental vasculature,isorders of amniotic fluid, subnormal and discordantrowth, and prematurity). While perinatal death rates forultifetal pregnancies have declined,1-3 they remain higher
han those for singletons of comparable gestational ages.Twin gestation presents hazards for perinatal survival at all
estational ages. In the first half of pregnancy, there is in-reased fetal wastage (“the vanishing twin”). In the third tri-ester, there is increased risk of fetal growth restriction com-ared with single pregnancies, raising the risk of fetal deathnd early delivery.4,5 Added risks for perinatal mortality aremposed on twins that are monozygous and/or share a mono-horionic placenta.6-8 It has been estimated that after 37 to 38eeks gestation, the risk of intrauterine death is equivalent to
hat of a postterm single gestation.7 Although growth restric-ion and twin–twin transfusion contribute to this excess mor-ality, Barigye and colleagues8 note that being a monochori-nic twin alone may be hazardous. Fetal deaths unrelated tohe above conditions occurred at a rate of nearly 50/1000.8
obinson and coworkers reported that the lowest risk forerinatal death occurs at 37 weeks’ gestation.9 Therefore,hen considering strategies of fetal assessment, it will be
mportant to account for chorionicity and zygosity as well as
ssessment of fetal growth.281

vltega(tvc
AiOntSpwarsprcpr
ASSptftiap
UTiipwrdadttGpp
mmgcatdfs4sbb
stttwt�ot
SNgIvgi
MGStmoamditibc
raatstggs
282 L.D. Devoe
The methods applied to twin gestations were initially de-eloped and evaluated in single pregnancies. As will be notedater, tracking fetal growth is also a different proposition forwin pregnancy. Different standards are needed and consid-rable debate exists on the best standards for biometry androwth nomograms.10 Twin gestations present challenges forntenatal surveillance not encountered in single pregnancies:1) twin–twin transfusion syndrome; (2) monoamnioticwinning; (3) intrauterine death of a single twin fetus. Sur-eillance of these twin-specific complications will be dis-ussed later in this article.
ntepartum Assessmentn Twin Gestation: Initiationnly three decades ago nearly half of twin pregnancies wereot diagnosed before parturition. The benefits of early iden-ification of twin pregnancy were noted during an earlywedish population study11 in which obstetric ultrasonogra-hy was used routinely. Nearly 90% of all twin gestationsere identified. Antenatal detection of twin pregnancy was
ssociated with lower infant mortality and low birth weightates and greater gestational age at delivery. Routine ultra-ound examination of all pregnancies is not endorsed atresent; two-thirds of all pregnancies in the United Stateseceive at least one antenatal ultrasound study.12 This in-reases the likelihood that most twin pregnancies receivingrenatal care will be detected early enough in gestation foreliable dating, anatomic survey, and antenatal assessment.
ntepartum Assessment:election of Test and Follow-Up
hould twins receive the same antenatal tests and testingrotocols as do singletons? While many studies of antenatalesting have been conducted in single gestations, it does notollow necessarily that their outcomes can be applied directlyo the management of twin gestations. These singleton stud-es have been criticized for their predictive shortcomings13 inssessing growth-restricted fetuses, the greatest source oferinatal mortality in the third trimester.1
ltrasonography: Fetal Growthhe cornerstone of fetal assessment in twin pregnancy is the
dentification of abnormal fetal growth or discordancy. Thiss essential to investigate causation (anatomic ultrasonogra-hy) or to assess intrauterine adaptation (fetal testing). Asith singleton pregnancies, the identification of fetal growth
estriction requires accurate fetal biometry and reliable stan-ards for fetal growth patterns at all gestational ages. Theccuracy of such a diagnosis requires the existence of stan-ards for determining normal twin baseline growth. Al-hough numerous standards have been reported for single-ons, the data for twin gestations are quite limited.14
rumbach and colleagues performed one of the most com-rehensive early studies for twin sonographic biometry (bi-
arietal diameter (BPD), abdominal circumference, and fe- wur length).15 During ultrasound examinations performed atonthly intervals during the second half of pregnancy, this
roup found that BPD and abdominal circumference growthurves declined significantly from singleton curves after 31nd 32 weeks, while femur length growth remained similar tohat of singletons. Grennert and coworkers, using a Swedishatabase, indicated impact of zygosity on the evaluation ofetal growth parameters for twin pregnancies. Although thistudy was limited to BPD measurements of 46 dizygous and5 monozygous twin pairs, monozygous twin BPDs weremaller than those of dizygous twins at all gestational ageseyond 28 weeks.16 This was correlated with lower meanirth weights for monozygous twins.Ananth and coworkers applied six singleton and two twin
onographic nomograms for fetal weight to 1302 twin pairso predict birth weight below the 10th percentile for gesta-ional age.10 Singleton nomograms appeared to be applicableo twin gestations in a narrow gestational age range (32 to 34eeks). Singleton nomograms underestimated fetal weight in
wins �32 weeks and overestimated fetal weight in twins34 weeks gestation. They also confirmed that monochori-
nic twins had lower birth weights than those of dichorionicwins.
ummaryomograms for biometry and fetal weight estimation for twinestations are quite limited. Observational studies (LevelI-3) support the need for twin-specific nomograms for indi-idual biometric parameters and fetal weight estimation. Sin-leton nomograms are problematic and may produce errorsn weight estimation and detection of abnormal fetal growth.
ethods for Detection of Subnormalrowth and Fetal Weight Discordance
ubnormal fetal growth and discordant fetal growth betweenwins contribute significantly to perinatal morbidity andortality. Crane and coworkers were among the first to dem-
nstrate that fetal weight differences of more than 20% weressociated with an increased risk for stillbirth.17 Table 1 sum-arizes several studies, evaluating different criteria for theetection of twin discordancy. Most of these studies were
nitiated at 26 weeks gestational age or greater and repeatedheir evaluations at 2- to 4-week intervals. Four reports18-21
dentified estimated fetal weight differences alone or in com-ination with other biometry in their efforts to identify dis-ordant growth.
Doppler velocimetry of the umbilical arteries was incorpo-ated as a separate tool for detecting fetal growth restrictionnd discordance.22-25 The results of these small studies variednd most failed to support Doppler velocimetry as an effec-ive independent tool for this purpose. However, abnormalystolic:diastolic ratios were shown by Degani and coworkerso appear several weeks ahead of abnormal sonographic fetalrowth.25 Divon and colleagues26 compared a variety of sono-raphic parameters in 58 twin pairs of which 30% were sub-equently found to have discordant fetal weights (twin
eight differences exceeding 15%). In this study, a combina-
twa
SFicsgt2tgDfp
NTrrspcfaaNifcNrvgopgpt
(w
STpspNpafm
BSwBtfsBaiaftom
SBrc
DDcf
T
OC
RGS
R essmen
Antenatal fetal assessment: multifetal gestation 283
ion of differences in Doppler velocimetry and estimated fetaleight greater than 15% had the highest sensitivity (78%)
nd specificity (87%) for twin discordance.
ummaryor twin gestation, there is no consensus on the best screen-
ng approach for the detection of growth restriction or dis-ordance. Most reports have used nomograms derived fromingleton rather than twin gestations, although such nomo-rams have limitations in their prediction of growth restric-ion. Discrepancies in estimated fetal weight greater than0% appear to provide the greatest yield for this outcome buthe studies supporting this criterion have examined smallroups with varying prevalences of growth-restricted fetuses.oppler velocimetry may provide added value in screening
or growth disturbances in twin pregnancies; however, sup-ortive evidence is limited (Level II-2; Level II-3).
onstress Tests (NSTs)win gestation presents a specific challenge for fetal heartate testing. Contraction stress tests have been consideredelatively contraindicated due to the concern that contractiontress tests might incite excessive uterine activity in pretermregnancies. There is insufficient evidence to support thisoncern. However, as the NST became the primary methodor fetal heart rate testing in twins, there was obvious need tocquire simultaneous tracings to ensure that each fetus wasctually being monitored. Few studies have reported on theST exclusively in twin pregnancies. The initial reports used
ndependent electronic fetal monitoring systems27-29 for eachetus and reported failure rates of 2 to 15% in successfullyapturing both fetuses. These studies found that reactiveSTs conferred a good prognosis (no perinatal deaths and
ates of growth restriction ranging from 8 to 28%). Con-ersely, nonreactive NSTs were associated with rates of fetalrowth restriction of 55 to 100% and perinatal mortality ratesf 50% or higher. Knuppel and coworkers5 assessed the im-act of initiating routine NSTs on all twins after 31 weeksestation. This study compared a historical group of 129 twinairs not receiving routine NSTs to a subsequent group of 90
able 1 Detection of Twin Discordancy: Summary of Selected
Study No. Criteria
’Brien, et al19 329 �EFW >15%hitkara, et al18 42 �BPD >20%
�AC�EFW�FL
odis, et al20 85 �EFW >20%erson, et al22 52 UA S:D <10%iletorlazzi, et al21 43 �BPD >6 mm
�AC >20 mm�FL >5 mm�EFW >20%
eprinted with permission from Devoe LD, Ware DJ: Antenatal ass
win pairs receiving routine weekly NSTs. Six of 258 fetuses c
2.3%) in the control group had perinatal deaths, while thereere no deaths in the routine NST group.
ummaryhere is limited evidence (Level II-2 and Level II-3) to sup-ort the use of NSTs in twin gestations. The few exclusivetudies on twin gestation suggest that the NST has screeningerformance similar to that seen in singleton populations.onreactivity, when not attributable to fetal immaturity, hasotential value in identifying growth-restricted fetuses thatre at increased risk for perinatal death. The ability to per-orm simultaneous monitoring on a single unit is available inost contemporary fetal monitoring systems.
iophysical Profile Testing (BPP)ince the early 1980s, the BPP has become a leading fetalell-being test.30 Only one study has focused exclusively onPP testing in twin gestations.31 Lodeiro and coworkersested 49 twin pairs, 80% of which had additional indicationsor fetal assessment. Testing began at 26 weeks gestation. BPPcores �8 led repeat testing at weekly intervals until delivery.PP scores �6 led to repeat testing within 4 hours. A nonre-ctive NST and absent breathing in one twin was used as anndication for delivery. They found that a reactive NST waslways associated with a BPP score �8; more than 80% ofetuses with nonreactive NSTs had BPP scores of 8. Althoughhis study had a sensitivity of 83% for adverse outcomes, thenly deaths that occurred were due to complications of pre-aturity, not intrauterine compromise.
ummaryiophysical testing is commonly performed on most high-isk pregnancies in contemporary practice. There are insuffi-ient data to determine its value for twin gestations.
oppler Velocimetry of Umbilical Arteriesoppler velocimetry of the fetal umbilical arteries has be-ome a standard modality in screening singleton pregnanciesor the risk of adverse perinatal outcomes.32 Nimrod and
ies
Sens Spec PPV NPV
70 80 34 9578 90 87 NA
100 85 89 NA90 92 92 NA86 85 85 NA86 80 80 8682 98 90 9671 77 63 8380 85 62 9360 93 75 8780 93 80 93
t of twin gestation. Semin Perinatol 19:413-425, 1995 (Saunders).
Stud
oworkers showed that a discordance in systolic:diastolic

(pra
wsatR3rdgtagdrgfj
SDassI
CACpebaiufDfcclcl
iisdgTpwvpncnnu
SMtcafinlaoou
UCTATptpfttatia
T
DNUAA
R essmen
284 L.D. Devoe
S/D) ratios of more than 50% was associated with a higherrobability of poor outcome in the twin with the higher S/Datio.33 Subsequent larger trials by Gaziano and coworkers34
nd Jensen35 supported these results.Giles and coworkers reported a study of 272 twin sets in
hich umbilical artery S/D ratios were concealed (first 100ets) and revealed to clinicians (remaining 172 sets).36 Thevailability of Doppler results were associated with a reduc-ion in corrected perinatal mortality from 42/1000 to 9/1000.ates of neonatal intensive care admissions decreased from8% in the Doppler-concealed group to 21% in the Doppler-evealed group. Subsequently, Giles and colleagues con-ucted a randomized trial of Doppler assessment in 526 twinestations.37 Their study assigned twin gestations at 25 weekso receive either ultrasound biometry or ultrasound biometrynd umbilical artery Doppler velocimetry at 30 and 35 weeksestation. There were no significant differences in perinataleath rates between the two groups. The perinatal mortalityates of 12/1000 and 8/1000 in the control and Dopplerroups, respectively, were attributed to the potential con-ounding benefits of close surveillance of all enrolled sub-ects.
ummaryoppler velocimetry has been a valuable addition to the fetalssessment strategies for singleton pregnancy. The data toupport similar value in twin gestation are quite limited andomewhat conflictual (Level I; Level II-1, Level II-2, LevelI-3).
ombinations of Currentntenatal Testing Modalitiesomparisons of the screening performance of different ante-artum tests for twin gestations have been limited. How doesach of these approaches contribute individually or in com-ination to the prediction of outcome in twin gestations? Kimnd coworkers studied 100 twin pairs receiving weekly mod-fied BPPs (NST and AFV by maximal vertical pocket) andmbilical artery Doppler velocimetry.38 NSTs were per-
ormed semiweekly (if amniotic fluid volume [AFV] andoppler studies were normal) and ultrasound tracking of
etal growth was performed every 3 weeks. Seventy-one per-ent of twin pregnancies had other medical or obstetric indi-ations for fetal assessment. Abnormal Doppler velocimetryed to increased frequency of testing. Abnormal growthurves or AFVs, or persistently nonreactive NSTs, were fol-
able 2 Prediction of All Adverse Outcomes in Twin Gestatio
Test Sensitivity Specificity
oppler 49 90ST 44 90CG 46 90FV 39 88ll tests 53 88
eprinted with permission from Devoe LD, Ware DJ: Antenatal ass
owed either by delivery (fetal maturity) or by full BPP (fetal s
mmaturity). Follow-up of an abnormal BPP was individual-zed and based on the degree of fetal immaturity. Table 2hows the prediction of adverse perintatal outcome (perinataleath, intrapartum distress, neonatal metabolic acidosis,rowth restriction) according to individual testing method.he addition of Doppler velocimetry to the NST improvedosttest probability for an adverse outcome to 95% if bothere abnormal and decreased posttest probability for an ad-erse outcome to 37% if both tests were normal. The posttestrobability of growth restriction and twin discordancy wasearly 100% when both Doppler velocimetry and growthurves were abnormal and only 23% when both tests wereormal. Nearly all growth-restricted fetuses (86%) had ab-ormal Doppler studies for 1 to 8 weeks before abnormalltrasound growth profiles appeared.
ummaryost twin pregnancies have indications for antenatal testing
hat are similar to those used in singleton gestations. As is thease for singleton surveillance, the sensitivities of individualssessment methods are at or below 50% while their speci-cities typically exceed 90%. Since the data are limited, false-egative or –positive rates for the tests used in twin surveil-
ance are not well established. The major role of AFVssessment occurs when there is disparity between the sizesf the fetal sacs. Doppler velocimetry may improve the utilityf the other tests, especially when combined with NST orltrasound growth curves (Level II-2).
nique Fetalonditions in Twin Assessment
he Role of Doppler Velocimetry in thessessment of Twin Transfusion Syndromewin-to-twin transfusion syndrome (TTS) is a serious com-lication in about 10% to 20% of monozygous twin gesta-ions. Its impact on fetal growth and survival generally de-ends on when the vascular communications becomeunctional. Intact survivorship is strongly related to the na-ure and timing of therapeutic interventions (amnioreduc-ion, fetoscopic photocoagulation). Discordant fetal weightnd AFV often heralds this condition; however, there is con-roversy about the best method for assessing affected fetusesn such pregnancies. The stakes for fetal assessment in TTSre very high as the death of either twin augurs poorly for its
est Outcome
NPV OR (95% CI) Accuracy
84 8.6 (3.5 to 21.1) 8084 7.5 (3.1 to 18.0) 7984 6.5 (2.8 to 15.1) 7881 4.5 (2.1 to 10.5) 7588 9.2 (3.7 to 22.6) 82
t of twin gestation. Semin Perinatol 19:413-425, 1995 (Saunders).
n by T
PPV
6359545255
urviving cotwin. Van Heteren and colleagues report a nearly

5spwlptnpersfcdddgm
SCdufsvo
AoM1amaEaltmrtgvs
SWtb
AoFIc
tettiseb
SIss
CDTFtbiaafnacpco
F
Antenatal fetal assessment: multifetal gestation 285
0% rate of perinatal death or significant morbidity for theurviving twin after in utero death of its cotwin in a TTSregnancy.39 It was anticipated that Doppler velocimetryould assist perinatal surveillance in TTS. However, there is
ack of consensus on this point. Erskine and coworkers re-orted that death of the donor twin did not alter the pulsa-ility index of its surviving cotwin.40 Pretorius and coworkersoted that in eight twin pairs with three surviving infants, allairs had S/D ratio differences that exceeded 0.4; in six ofight sets the donor twin had higher S/D ratios than theecipient twin.41 Giles and coworkers reported on 11 twinets and did not find that the S/D ratio difference was usefulor prediction of TTS in discordant twin pairs.42 Rizzo andoworkers compared the S/D ratio differences in 15 sets ofiscordant twins without TTS and those in 10 sets of discor-ant twins with TTS.43 In the former group, there were majorifferences in S/D ratios at the initial recordings; in the latterroup, these differences were not apparent until other testingodalities, such as NST, became abnormal.
ummaryurrent data on antenatal assessment of TTS gestations areerived from limited or uncontrolled series. Differences inmbilical artery S/D ratios may not differentiate either af-ected twin. This is not surprising as the timing and exten-iveness of the vascular anastomoses involved in TTS mayary considerably. There are few data on the value and resultsf specific posttreatment surveillance in this condition.
ntenatal Assessmentf Monoamniotic Twinsonoamniotic twinning is a rare complication, occurring in
% of monozygous twins. It has the potential for consider-ble perinatal morbidity and mortality. Antenatal diagnosis isade by the failure to detect a dividing amniotic membrane
nd close proximity of the insertions of both umbilical cords.tiologies of perinatal death may stem from intravascularnastomoses as in TTS or umbilical cord entanglement.44 Aarge retrospective survey of 133 sets of monoamnioticwins45 suggested that perinatal loss rates doubled approxi-ately every 2 weeks from 30 to 38 weeks (6, 11, and 22%,
espectively). Two recent small studies suggest that close an-enatal surveillance accompanied by delivery at 32 weeksestation may yield the best outcomes.46,47 Dickinson’s re-iew indicates that there is a scarcity of large well-controlledtudies to resolve this clinical problem.44
ummaryhile the number of reports on monoamniotic twin gesta-
ions have increased, there are insufficient data to support aest testing strategy or timing of delivery.
ntenatal Assessmentf Surviving Cotwin After Singleetal Death in the Third Trimester
n utero death of one member of a twin pair has been impli-
ated in both cerebral impairment and growth restriction of the survivor.48,49 The risk of cerebral damage with multicysticncephalomalacia is much more likely in monochorionicwins with vascular communications than in dichorionicwins. Fetal imaging with ultrasound or magnetic resonancemaging may aid in this diagnosis. Antenatal testing of theurviving twin has been recommended. The interval to deliv-ry is usually short and not always the result of interventionased on antenatal testing.49
ummaryn utero death of a single twin in the third trimester shouldignal the initiation of antenatal surveillance. Data to demon-trate optimal testing schemes or benefits are lacking.
onclusions: Clinicalecision-Making and Antenatalesting in Twin Gestation
igure 1 outlines a model antenatal assessment algorithm forwin gestation. Antenatal assessment of twin gestation shouldegin with ultrasound diagnosis, accurate gestational dat-ng, and anatomic surveys. Conditions that may not beided by antepartum surveillance include preterm labornd fetal anomalies. Conditions that may possibly benefitrom serial antenatal assessment include twins with sub-ormal or discordant growth, single surviving twin, mono-mniotic twins, and TTS. While early identification of rareomplications such as TTS and monoamniotic twins is im-ortant for enabling possible management options, it is notlear that specific fetal well-being tests will improve perinatalutcome once these conditions are known.Selection of individual or grouped fetal surveillance tests,
igure 1 Decision-tree for antenatal assessment and management of
win gestation.
teloafc(mLcpc
pigmpgsvmuni
lngott1mstdthn
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
286 L.D. Devoe
he timing of their initiation, and the frequency of their rep-tition remains an unresolved issue. Although Doppler ve-ocimetry has been well studied in single pregnancies, thenly randomized controlled trial in twin gestation37 was dis-ppointing. Doppler velocimetry may be an early marker foretal growth restriction and may improve prediction of out-ome when added to other biophysical testing methodsLevel II-2 and Level II-3). The routine use of NST as a pri-ary surveillance test in twins is supported by Level II-2 and
evel II-3 evidence. Data on the use of BPP in twin pregnan-ies are very limited (Level II-3 evidence). AFV assessmentlays a principal role in the detection and follow-up of dis-ordant twins at risk for TTS.
A major concern with antepartum surveillance in twinregnancy is the consequence of intervention based on test-
ng methods with known high false-positive rates in singleestations. This creates a major dilemma when tests are nor-al in one twin and abnormal in the other. This is com-ounded by the frequent testing of pregnancies �32 weeksestation, a subgroup for which there are limited data oningleton testing. Iatrogenic prematurity resulting from inter-entions in preterm twin pregnancies may cause significantorbidity, possibly harming both twins. While approachessing more than one antenatal test may reduce positive- andegative-predictive errors and enhance sensitivity, further
nvestigation with larger twin populations will be needed.In summary, all of the commonly used antenatal surveil-
ance methods that have been reported for singleton preg-ancies have received some level of investigation in twinestations. With the exception of Doppler velocimetry, nonef these methods has been subjected to randomized con-rolled evaluation. Of the observational trials performed onhe other testing methods, most have involved fewer than00 twin pairs. It is uncertain that the screening perfor-ances of these antenatal tests are equivalent to those ob-
erved in single pregnancies, particularly at the earlier gesta-ional ages when they are likely to be used. Not only are moreata obtained from larger well-designed trials needed forwin gestation but the paucity of data on surveillance ofigher order multifetal gestations suggests yet another areaeeding future study.
eferences1. Farooqui MO, Grossman JH, Shannon RA: A review of twin pregnancy
and perinatal mortality. Obstet Gynecol Surv 28:144-153, 1973(suppl)
2. Keith L, Ellis R, Berger GS, et al: The Northwestern University multi-hospital twin study. I. A description of 588 twin pregnancies and asso-ciated pregnancy loss, 1971 to 1975. Am J Obstet Gynecol 138:781-789, 1980
3. Chervenak FA, Youcha S, Johnson RE, et al: Twin gestation: antenataldiagnosis and perinatal outcome in 385 consecutive pregnancies. JReprod Med 29:727-730, 1984
4. Hawrylyshyn PA, Barkin M, Bernstein A, et al: Twin pregnancies—acontinuing perinatal challenge. Obstet Gynecol 59:463-466, 1982
5. Knuppel RA, Rattan PK, Scerbo JC, et al: Intrauterine fetal death intwins after 32 weeks’. Obstet Gynecol 65:172-175, 1985
6. Kahn B, Lumey lH, Zybert PA, et al: Prospective risk of fetal death insingleton, twin, and triplet gestations: implications for practice. Obstet
Gynecol 102:685-692, 20037. Sairam S, Costeloe K, Thilaganathan B: Prospective risk of stillbirth inmultiple gestation pregnancies: a population-based analysis. ObstetGynecol 100:638-641, 2002
8. Barigye O, Pasquini L, Galea P, et al: High risk of unexpected late fetaldeath in monochorionic twins despite intensive ultrasound surveil-lance: a cohort study. PLoS Med 2:e172, 2005
9. Robinson J, Healy, Beatty T, et al: The optimal age for twin delivery.Am J Obstet Gynecol 193:S183, 2005
0. Ananth CV, Vintzileos AM, Shen-Schwartz S, et al: Standards of birthweight in twin gestations stratified by placental chorionicity. ObstetGynecol 91:917-924, 1998
1. Persson P, Grennert L, Gennser G, et al: On improved outcome of twinpregnancies. Acta Obstet Gynecol Scand 58:3-7, 1979
2. ACOG Committee on Practice Bulletins: ACOG Practice Bulletin No.58. Ultrasonography in Pregnancy. Obstet Gynecol 104:1449-58, 2004
3. Devoe LD: Antenatal fetal assessment: contraction stress test, nonstresstest, vibroacoustic stimulation, amniotic fluid volume, biophysical pro-file, modified biophysical profile. An Overview. Semin Perinatol 32:247-252, 2008
4. Jones JM, Sbarra AJ, Cetrulo CL, et al: Antepartum management of twingestation. Clin Obstet Gynecol 33:32-41, 1990
5. Grumbach K, Coleman BG, Arger PH, et al: Twin and singleton growthpatterns compared using ultrasound. Radiology 158:237-241, 1986
6. Grennert L, Persson PH, Gennser G, et al: Zygosity and intrauterinegrowth of twins. Obstet Gynecol 55:684-687, 1980
7. Crane JP, Tomich PG, Kopta M: Ultrasonic growth pattern in normaland discordant twins. Obstet Gynecol 55:678-683, 1980
8. Chitkara U, Berkowitz GS, Levine R, et al: Twin pregnancy: routine useof ultrasound examinations in the prenatal diagnosis of intrauterinegrowth retardation and discordant growth. Am J Perinatol 2:49-53,1985
9. O’Brien WF, Knuppel RA, ScerboJ C, et al: Birth weight in twins: ananalysis of discordancy and growth retardation. Obstet Gynecol 67:483-486, 1986
0. Rodis JF, Vintzileos AM, Campbell WA, et al: Intrauterine fetal growthin discordant gestation. J Ultrasound Med 9:443-448, 1990
1. Storlazzi E, Vintzileos AM, Campbell WA, et al: Ultrasonic diagnosis ofdiscordant fetal growth in twin gestations. Obstet Gynecol 69:363-367,1987
2. Gerson A, Johnson A, Wallace D, et al: Umbilical arterial systolic/diastolic values in normal twin gestation. Obstet Gynecol 72:205, 1988
3. Farmakides G, Schulman H, Saldana LR, et al: Surveillance of twinpregnancy with umbilical arterial velocimetry. Am J Obstet Gynecol153:789-792, 1985
4. Hastie SJ, Danskin F, Neilson JP, et al: Prediction of small for gestationalage twin fetus by Doppler umbilical artery waveform analysis. ObstetGynecol 74:730-733, 1989
5. Degani S, Gonen R, Shapiro I, et al: Doppler flow velocity waveforms infetal surveillance of twins. J Ultrasound Med 11:537-541, 1992
6. Divon MY, Girz BA, Sklar A, et al: Discordant twins—a prospectivestudy of the diagnostic value of real-time ultrasonography combinedwith umbilical artery velocimetry. AmJ Ohstet Gynecol 161:757-760,1989
7. Bailey D, Flynn AM, Kelly J: Antepartum fetal heart rate monitoring inmultiple pregnancy. Br J Obstet Gynecol 87:561-564, 1980
8. Devoe LD, Azor H: Simultaneous nonstress fetal heart rate testing intwin pregnancy. Obstet Gynecol 58:450-455, 1981
9. Blake GD, Knuppel RA, Ingardia CJ, et al: Evaluation of nonstress fetalheart rate testing in multiple gestations. Obstet Gynecol 63:528-532,1984
0. Manning FA, Platt LD, Sipos L: Antepartum fetal evaluation: develop-ment of a biophysical profile. AmJ Obstet Gynecol 136:787-791, 1980
1. Lodeiro JG, Vintzileos AM, Feinstein SJ, et al: Fetal biophysical profilein twin gestation. Obstet Gynecol 67:824, 1986
2. Fleischer A: Doppler blood flow studies. Clin Obstet Gynecol 32:627-647, 1989
3. Nimrod C, Davis D, Harder J, et al: Doppler ultrasound prediction offetal outcome in twin pregnancies. Am J Obstet Gynecol 156:402-406,
1987
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
Antenatal fetal assessment: multifetal gestation 287
4. Gaziano EP, Knox E, Bebdel RP, et al: Is pulsed Doppler velocimetryuseful in management of multiple-gestation pregnancies? Am J ObstetGynecol 164:1426-1433, 1991
5. Jensen OH: Doppler velocimetry in twin pregnancy. Eur J Ohstet Gy-necol Reprod Biol 45:9-12, 1992
6. Giles WB, Trudinger BJ, Cook CM, et al: Umbilical artery flow velocimetrywaveforms and twin pregnancy outcome. Obstet Gynecol 72:894-898, 1988
7. Giles W, Gisits A, O’Callaghan S, et al: Doppler assessment in multiplepregnancy: randomised controlled trial of ultrasound biometry versusumbilical artery Doppler ultrasound and biometry in twin pregnancy.BJOG 10:593-597, 2003
8. Kim ES, Croom CS, Devoe LD: Determination of fetal wellbeing in twingestation by Doppler velocimetry, nonstress testing, amniotic fluid vol-ume estimation, and ultrasound assessment of growth. Am J ObstetGynecol 170:320, 1994
9. Van Heteren CF, Nijhuis JG, Semmekrot BA, et al: Risk for survivingtwin after fetal death of co-twin in twin-twin transfusion syndrome.Obstet Gynecol 92(2):215-219, 1998
0. Erskine RLA, Ritchie JWK, Murnaghan GA: Antenatal diagnosis of pla-cental anastomosis in pregnancy using Doppler ultrasound. Br J ObstetGynaecol 93:955-959, 1986
1. Pretorius DH, Manchester D, Barkin S, et al: Doppler ultrasound of
twin transfusion syndrome. J Ultrasound Med 7:117-124, 19882. Giles WB, Trudinger BJ, Cook CM, et al: Doppler umbilical arterystudies in twin transfusion syndrome. Obstet Gynecol 76:1097-1099,1990
3. Rizzo G, Arduini D, Romanini C: Cardiac and extracardiac flows indiscordant twins. Am J Obstet Gynecol 170:1321-1327, 1994
4. Dickinson JE: Monoamniotic twin pregnancy: a review of contempo-rary practice. Aust NZ J Obstet Gynaecol 45:474-478, 2005
5. Roque H, Gillen-Goldstein J, Funai E, et al: Perinatal outcomes inmonoamniotic twin gestations. Matern Fetal Neonatal Med 13:414-421, 2003
6. Pasquini L, Wimalasundera RC, Fichera A, et al: High perinatalsurvival in monoamniotic twins managed by prophylactic sulindac,intensive ultrasound surveillance, and Cesarean delivery at 32weeks’ gestation. Ultrasound Obstet Gynecol 28:681-687, 2006
7. Shveiky D, Ezra Y, Schenker JG, et al: Monoamniotic twins: an updateon antenatal diagnosis and treatment. J Matern Fetal Neonatal Med16:180-186, 2004
8. Pharoah PO, Adi Y: Consequences of in-utero death in a twin preg-nancy. Lancet;355:1597-1602, 2000
9. Kilby MD, Govind A, O’Brien PM: Outcome of twin pregnancies com-plicated by a single intrauterine death: a comparison with viable twin
pregnancies. Obstet Gynecol 84;107-109, 1994
AC
Aflpfmfi
NAprbekici
l““
D
A
2
mniotic Fluid Abnormalitieshristopher R. Harman, MD
The complex nature of amniotic fluid reflects contributions from many fetal systems, manyfunctional roles, and multiple interactions with fetal maturation, obstetric, and maternalfactors. Simple ultrasound measurement, probably done best with the maximum verticalpocket method, has a clinical role in fetal surveillance, substantiated by extensive level IIand some level I evidence. Interventions (amnioinfusion for oligohydramnios, amnioreduc-tion for polyhydramnios) have not been studied effectively in controlled fashion, with theexception of intrapartum applications, where effective reduction of cesarean delivery forfetal distress and perinatal impacts of meconium aspiration may follow amnioinfusion. Awealth of research opportunities exists into regulation of amniotic fluid constituents andtheir relation to preterm delivery.Semin Perinatol 32:288-294 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS amniotic fluid, maximum vertical pocket, perinatal outcome, amnioinfusion,amnioreduction
rtg
lcoccmi“a(sToiuc
AAaarua
mniotic fluid regulation represents a complex interac-tion of many systems—fetal respiratory, cardiovascular,
uid balance, urinary tract, gastrointestinal, skin, neurologic,lacenta and membranes, and maternal factors, to name aew. Several aspects of simple amniotic fluid volume (AFV)
easurement have been studied in randomized, controlledashion, but this likely represents a tiny proportion of thenformation available.
ormal Amniotic Fluidmniotic fluid functions (Table 1) can be categorized ashysical (preventing fetal injury, increasing placental surface,egulating temperature), functional (mobility for practicereathing preventing pulmonary hypoplasia; swallowing ex-rcises the digestive tract; skeletal muscle movement of everyind), and homeostasis (maintaining amnion integrity, fight-
ng infection, discouraging contractions, maintaining cervi-al length and consistency). In this context, it is not surpris-ng that deficiencies in amniotic fluid have multiple impacts.
Such impacts are prominent in midwifery folklore for mil-ennia: “dry birth” suggests stillbirth and lethal anomalies;broken water” suggests sepsis and onset of labor; fluidstaining” accompanies fetal demise; and polyhydramnios is
ivision of Maternal and Fetal Medicine, School of Medicine, University ofMaryland Baltimore, Baltimore, MD.
ddress reprint requests to Christopher R. Harman, MD, University of MarylandBaltimore, Division of Maternal and Fetal Medicine, 22 S. Greene Street,
TRoom N6E10, Baltimore, MD 21201. E-mail: [email protected]
88 0146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1053/j.semperi.2008.04.012
elated to maternal death, abruption, intrapartum complica-ions, and neonatal death (Rh-alloimmune hydrops and con-enital syphilis).
Modern understanding of fetal urinary tract and neuro-ogic and placental impacts on AFV are supplemented byurrent research. Proteomics reveals multiple related amni-tic fluid compounds that predict preterm labor, prematureervical effacement, and fetal infection.1 The inflammatoryascade leading to cervical incompetence, preterm rupture ofembranes, and preterm labor and delivery, all may begin
n the first trimester, according to amniocentesis results.Sludge” on ultrasound suggests inflammatory amniocytesccumulating as inappropriate cervical effacement beginsFig. 1).2 Several of the amniotic fluid defensive propertieshown are significantly elevated in preterm labor (asterisks inable 2). When women fail tocolysis for preterm labor, manyf these protective chemicals are low or absent.3 These qual-tative changes are not detected just by measuring AFV onltrasound—more research will determine the role of amnio-entesis in managing preterm labor.
mniotic Fluid VolumeFV is directly correlated with perinatal mortality (Fig. 2)nd many serious morbidities: fetal abnormalities (renalgenesis with oligohydramnios; duodenal atresia; gross neu-ologic anomalies with polyhydramnios); birth weight (intra-terine growth restriction [IUGR] with oligohydramnios; di-betic macrosomia with polyhydramnios); and so on.4,5
hese correlations determine monitoring decisions and sug-

gt
AaRlmtfiraotrrAwpa“atwO
moA
AEc2(hLuf3agn(iw
IT(m
T
****** ractic
Amniotic fluid abnormalities 289
est specific tests depending on history, ultrasound examina-ion, and progressive changes.
mniotic Fluid Volumend Perinatal Outcomeelationships between AFV and perinatal outcome are estab-
ished in obstetric lore and AFV measurement is crucial toost ultrasound-based systems of fetal assessment, including
he Biophysical Profile Score and modified Biophysical Pro-le (BPP).6 Recently, however, Ott7 suggested “There is noelationship between amniotic fluid volume and gestationalge” and “AFI is not significantly correlated with perinatalutcome.” Reconciling this with dozens of studies to the con-rary requires a few steps. Fewer than 6000 patients wereeviewed retrospectively and had normal outcome, so theange of AFV was narrow, the nadir of Figure 2. Clinically,FV is used longitudinally—this cross-sectional study waseakly predictive for individual cases. When anomalies,ostdates pregnancy, severe IUGR, uncontrolled diabetes,nd other maternal complications are excluded to attainnormal” outcome, many cases of abnormal amniotic fluidre also artificially excluded. The nadir of the AFV curve ishen a flat line, between single pocket depths of 3 to 8 cm,ith no relationship to perinatal mortality or gestational age.f course, this does not eliminate the value of amniotic fluid
able 1 What Is Amniotic Fluid For?
Amnion metabolism * HUterine shape * TSurface area: contractions, vessels * TUmbilical cord mobility * BSpace—cranium, bones, lungs * ARecirculation, urine, spit, regurgitation * P
Figure 1 (A) (upper panel) Cervical funneling at 20 wcervical dilation (lower panel) within 6 days. (B) Simila
(upper panel) is unchanged after several weeks (lower panel).onitoring in an obstetric population. It might be fairer tobserve that obstetric decisions should not be made based anFV alone.
mniotic Fluid Dynamicsarly transudation across skin and placental surfaces be-omes negligible by completion of skin maturation at about2 weeks. Amniotic fluid is formed primarily from lung fluidabout 100 mL per day) and fetal urine (7-10 mL/kg perour) and is eliminated primarily by fetal swallowing, up to 1per day.8 Maturation is important for both—near term,
rine concentration increases and volume of productionalls. Rest between swallowing becomes longer, from about0 minutes at 24 weeks, up to 80 minutes between “feedings”t term. Other normal fetal functions also contribute—regur-itation, diuresis (eg, caffeine or hyperglycemia from mater-al diabetes), and individual efficiency of fetal swallowingsome fetuses make repeated swallowing motions, withoutncreasing stomach diameter; others dilate their stomachsith a few gulps).
mpact of Anomalieshese dynamics are markedly altered by fetal abnormalitiesTable 3). Abnormal swallowing (obstruction or neurologic)eans many fetuses with anomalies, including aneuploidy,
lic protectionregulation
ort—amnion, placentaostaticammatory
e—breathing, swallowing, crying, movement of every kind.
station. Intraamniotic sludge (arrow) associated withal funneling without inflammatory sludge at 20 weeks
ydrauhermoranspacterinti-infl
eeks ger cervic
(Color version of figure is available online.)

hledm
AIrcidc(snitbbptfDebsi
ORtdmqatwpooTpn
sashvn
vdmluradtopo
acrmpabipo
T
*
Fumflbfi
290 C.R. Harman
ave polyhydramnios. Urinary tract anomalies are often re-ated to oligohydramnios. Interaction of multiple effects (forxample, the fetus who has both a T-E fistula and a renalysplasia—reduced elimination and reduced production)ay yield normal AFV in anomalous fetuses.
mniotic Fluid Volume Measurementn invasive studies, using amniocentesis to instill dye, thenemeasuring after mixing, neither single maximum verti-al pocket (MVP) nor the four-quadrant amniotic fluidndex (AFI; Fig. 3) produce very accurate evaluation. Fiveye-dilution trials examined 185 patients: the correlationoefficient for AFI (0.52) is modestly superior to MVPr2 � 0.48). In 11 studies of sensitivity, most found noignificant difference, while specificity for oligohydram-ios was superior for MVP set at 2 cm (a low level reached
n �5% of pregnancies) to the clinically common AFIhreshold of 5 cm.9,10 Categorization of polyhydramniosy MVP is more closely associated with clinical outcome,ut neither method is very accurate. In management com-arisons (especially for oligohydramnios), MVP gives bet-er performance—the same predictive accuracy, feweralse alarms, and better correlation with biophysical andoppler variables. It is true that either method is only anstimate. Clinical correlations, however, are establishedetween these ultrasound estimates and clinical outcome,o direct inference of absolute volume is not a primaryssue.
able 2 Amniotic Fluid Defensive Properties
● Specific inhibition, cell wall destruction of tissue corrodin● Opsonins,* macrophages, chemotactic factors, IL-1 RA,*
psoriasin, PAF inhibitors, MMP3 antagonists● At least 100 unique proteins in amniotic fluid proteome
Elevated in PTL, low in PTL-failed tocolysis.
igure 2 Perinatal mortality varies according to amniotic fluid vol-me, as determined by maximum vertical pocket (MVP) in centi-eters. In the normal range (MVP, 3 to 8 cm), the curve becomes
at (nonsignificant) when all cases with abnormality (IUGR, dia-etic macrosomia, and postdates) are removed. (Color version of
ugure is available online.)
ligohydramnioseduced amniotic fluid triggers a series of questions. Ul-
rasound examination determines if kidneys are present,o they currently work, and will normal renal function beaintained? Does ancillary information suggest inade-
uate prerenal volume (eg, severe IUGR with markedlybnormal placental Dopplers, donor status in twin-to-twinransfusion syndrome, or early midtrimester pregnancyith markedly elevated alpha fetoprotein (AFP) whereerinatal mortality may reach 800/1000)? If all of thesebservations appear to be normal, there may be a uteriner maternal explanation for decreased fluid provision.here may not be any problem with production— occultreterm rupture of membranes (PROM) is often the expla-ation in that case.Oligohydramnios presents several other challenges. Ultra-
ound visualization is more difficult due to lack of contrastnd lack of fetal mobility. If anomalies due to aneuploidy areuspected, amniocentesis may be very difficult. Severe oligo-ydramnios with fetal distress at early gestation means inter-ention (often classical cesarean delivery) is considered witho certainty about a normal outcome.In such dilemmas, amnioinfusion may be helpful. We re-
iewed 155 cases (unpublished data) of ultrasound-guidediagnostic amnioinfusion with warmed normal saline (200L before 28 weeks, 300 mL after 28 weeks) with the fol-
owing results. In 102 cases, postinfusion high-resolutionltrasound found new anomalies. In 32, preterm prematureupture of membranes was diagnosed. In six, a suspectednomaly was disproved, while in 10%, no value could beefined, even in retrospect. A further 6% progressed in pre-erm labor to deliver with fatal outcome, an unexpected “res-lution” of the problem. There were no direct maternal com-lications. Amnioinfusion has an important diagnostic role inligohydramnios of unknown origin.Chronic oligohydramnios itself may produce additional
dverse fetal effects. Even when the fetus is initially normal,hronic oligohydramnios from PROM (iatrogenic from cho-ion villus sampling (CVS) or amniocentesis, or spontaneous)ay cause pulmonary hypoplasia, abnormal chest wall com-liance, contractures, and lethal infection. Onset, duration,nd severity of amniotic fluid loss are important cofactors,ut the gestational age at delivery remains the overriding
ssue. The severity of this problem has generated attempts toatch iatrogenic holes in the membrane, glue the cervix shut,r chronically replace the fluid.In one randomized trial of 34 patients and several well-doc-
teria such as GBS*a-defensins,* lysozyme, lactoferrin,* Ca�� chelaters,
g bacIL-10,*
mented nonrandomized, noncontrolled series totaling more

tHt3f
(qsrW
T
A
Amniotic fluid abnormalities 291
han 250 patients, amnioinfusion for PROM was studied.11,12
igh variability in case selection means it is difficult to translatehese results into clinical action. Study entry ranged from 16 to4 weeks. In 50 to 75% of cases, the procedure was unsuccess-ul. In cases where late gestation or borderline reduced fluid
Figure 3 (A) Maximum vertical pocket (MVP) method of
able 3 Amniotic Fluid Dynamics
Normal Daily Production
Transudation – skin, placenta
Lung fluid 100 mL(20% is exhaled, the rest is swallowed)
Fetal urine 7-10 mL/kg/hr24 weeks 150 mL30 weeks 350 mL34 weeks 600 mL39 weeks 600 mL
RegurgitationFetal diuresisGestational age effect
Decreased Elimination � Polyhydramnios
nomaliesChoanal AtresiaFacial cleftT-E fistulaEsophageal atresiaImperforate anusReduced swallowing:Neurological
BehaviorDrug induced
Polyuria—abnormal kidneys, brain injury, diabetes
index (AFI) method. (Color version of figure is available onlin
AFI of 6-8) suggests retrospectively the procedure was not re-uired, outcomes were good. In 16 to 30%, where amnioinfu-ion did restore MVP �2 cm, outcomes were as good. Thus, it iseasonable to attempt amnioinfusion for early oligohydramnios.
hen AFV is restored, outcomes are likely better, but in the vast
ic fluid measurement. (B) Four-quadrant amniotic fluid
Normal Daily Elimination
allowing up to 1 L/d, about every 30 minutes at 24 weeks,very 40 minutes at 32 weeks, only every 80 minutes aterm
alation (minor)
nal maturity (decreased urine production)
Decreased Production � Oligohydramnios
Urinary Tract ObstructionRenal failure (bad kidneys)OliguriaPlacental failure (hypovolemia and hypoxia)Renal agenesisAbsent lung fluid (eg, tracheal atresia)
amniot
Swet
Inh
Re
e.)

mb
enIetmctrseflpo
mscs
hoibcMaiAmn
tttdtum
d(ocdCsrvvbpfoi
gcttp
rBocdmbcih
tlod4qstavotpahRtststu
T
F
F
A
292 C.R. Harman
ajority, the procedure is not required in the first place or wille unsuccessful.Amnioinfusion for oligohydramnios of unknown origin is
ven less well-documented. Four historic series relate am-ioinfusion to similar cases managed without intervention.13
n general, pregnancies were prolonged up to 30 days, deliv-ries were somewhat later, and babies significantly larger, buthere were no differences in perinatal mortality, short-termorbidity, or long-term morbidity (limited reporting). These
ollective data cannot be termed a meta-analysis, becausehey are so disparate in structure. Further, mounting a formalandomized control trial would be extremely difficult, con-idering variable IUGR severity (which might require deliv-ry on a fetoplacental basis despite normalizing amnioticuid), differing maternal characteristics (eg, severe maternalreeclampsia, again requiring delivery), and differing onsetf subject cases.Overall, amnioinfusion for the restoration of AFV in theidtrimester and early third trimester has been incompletely
tudied. There is probably no maternal danger and fetal out-omes have not been proven to be worse, so it may be con-idered in individual cases.
Three trials and three clinical series examined maternalydration (increased water intake, oral or intravenous withral follow-up) for borderline oligohydramnios (AFI �8 cmn four, �6 cm in two). When oligohydramnios was judgedy AFI, improvement was apparent, but there was no in-rease in borderline fluid or oligohydramnios defined byVP (two studies), no increase in normal AFI (two studies),
nd increased AFI was not sustained �48 hours (three stud-es).14 Clinical benefits were not studied. In practices whereFI �5 cm mandates delivery, these data might improveanagement, but if MVP of 2 cm were applied, most wouldot “require” delivery in the first place.Low risk of hydration and potential reduction in interven-
ion might substantiate a randomized control trial. An impor-ant design issue is uterine tone. On ultrasound, uterine ac-ivity draws in the flanks of the uterus, which has the effect ofecreasing available vertical pockets for the AFI method. Ma-ernal hyperhydration, with its known effect of reducingterine contractility, might simply produce the illusion ofore fluid.Oligohydramnios later in the third trimester presents a
ifferent set of challenges. Since the strictest definitionsMVP �1 cm or MVP �2 cm) relate consistently to adverseutcome, delivery may be appropriate. Such outcomes in-lude stillbirth and neonatal death, fetal distress in labor,elivery pH, Apgar score, and many neonatal complications.riteria for “subjectively reduced AFV” describe “preoligo”
ituations but correlate weakly with poor outcome. Maternalelationships also correlate with MVP �2 cm, including se-ere pre-eclampsia, poor performance on external cephalicersion, reduced success with induction of labor or vaginalirth after cesarean delivery, poor pain control in labor, andostpartum sepsis. As long-term studies relate to compositeetal condition (for example, the Biophysical Profile Score),r to neonatal condition requiring intensive resuscitation, it
s difficult to assign longer term implications directly to oli- rohydramnios alone. Especially when oligohydramnios ac-ompanies abnormal Doppler ultrasound indicating placen-al insufficiency, or abnormal biophysical or fetal heart rateesting indicating increased risk of asphyxia, delivery is therincipal treatment.For isolated oligohydramnios when other fetal testing is
eassuring, amnioinfusion may allow safe vaginal delivery.efore considering these intrapartum amnioinfusion studies,ne must carefully consider the decision to deliver. AFI �5m as a trigger for delivery is associated with increased fetalistress, more Cesarean sections, and significant maternalorbidity. Many of those women would labor on their own
efore the MVP trigger of only 2 cm is reached, with signifi-ant improvement in obstetric parameters—a trial compar-ng doing nothing versus inducing labor with amnioinfusionas not been done.Table 4 displays trials of prophylactic transabdominal or
ranscervical amnioinfusion immediately before or in earlyabor at term, randomly compared with similar women with-ut infusion. Amnioinfusion done to eliminate fetal heart rateecelerations from cord compression (upper section of Table) benefits conduct of labor and baby’s condition.15 Subse-uent trials investigated intermittent versus continuous infu-ion, the role of electronic fetal monitoring, and applicationo specific causes of oligohydramnios, but the studies eitherre too small or reached equivocal conclusions. This inter-ention focuses on reducing Cesarean sections—social andther reasons increasing the cesarean delivery rate may meanhis information has reduced impact. Also, of uncertain im-act in urban settings is amnioinfusion to reduce meconiumspiration syndrome. At least 12 randomized control trialsave evaluated this, summarized in a recent meta-analysis.esults show two distinct patterns. When standard peripar-
um care applies, undiagnosed IUGR, postdates pregnancy,evere oligohydramnios, fetal infection, and undiagnosedwins are rare, and expert neonatal care is immediate. In thisituation, amnioinfusion does not improve outcome. In con-rast, where antenatal and neonatal care are limited, such asnderserved African communities, 75% of meconium aspi-
able 4 Amnioinfusion for Oligohydramnios
Odds Ratio C.I.
or cord compressionFHR abnormal 0.24 0.17 to 0.34C/S “fetal distress” 0.23 0.15 to 0.35All C/S 0.52 0.40 to 0.68Acidemia Umb Art pH < 7.20 0.40 0.30 to 0.55Maternal endometritis 0.60 0.36 to 1.01
or meconium aspirationMAS-standard peripartum
care0.59 0.28 to 1.25
Cesarean section 0.89 0.73 to 1.10Apgar—5 < 7 0.90 0.58 to 1.41MAS-Limited peripartum care 0.25 0.13 to 0.47
bbreviation: MAS, meconium aspiration syndrome
ation syndrome is prevented.16

O
PTgtismp
fddiua
tdps
cswuara
epdntw
uodlwcsgcttetushctpd
nhoshntslncwac
pdecatltpfl
AA
T
MMS
Amniotic fluid abnormalities 293
ligohydramnios Summary● AFV is an established component of perinatal monitoring.● Outcome analysis includes both causes and effects of
chronic oligohydramnios.● MVP �2 cm has significant adverse correlates, while
AFI of 5 cm may be too conservative, introducing un-necessary intervention, reduced specificity, and confu-sion about the relationship.
● Before term oligohydramnios is probably not reliable asa sole factor indicating delivery.
● Amnioinfusion lacks benefit antenatally but has specificintrapartum application.
olyhydramniosable 5 displays the definitions, frequency of different de-rees of excess amniotic fluid, and associated rates of perina-al mortality and congenital abnormality.17 The majority fallnto the mild group and are idiopathic (55%). No long-termequelae are attributed to this and there are many docu-ented cases of women with serial pregnancies affected byolyhydramnios, so maternal factors may be influential.Fetuses with incompletely controlled diabetes account
or about 25%. It is thought that fetal hyperglycemia pro-uces fetal polyuria due to its osmotic effect. Macrosomiciabetic infants also have increased cardiac output and
ncreased blood volume, which increase fetal GFR andrine production. Most polyhydramnios in this group arelso in the mild category.
Twins account for about 7% of polyhydramnios, two-hirds due to recipient status of twin-to-twin transfusion syn-rome, which may reach severe proportions. In this case,ure hypervolemia and corresponding maladaptive re-ponses cause virtually continuous fetal diuresis.
Abnormalities causing gastrointestinal obstruction, in-luding tracheoesophageal (TE) fistula and esophageal atre-ia, may generate polyhydramnios of severe proportion forhich antenatal imaging is often inconclusive. Others havenderlying neurologic disorders and polyhydramnios due tobsent or reduced swallowing. This is often associated witheduced activity, symmetric IUGR, and nongastrointestinalnomalies (eg, cardiac anomalies, spina bifida, akinesia).
Fetuses with borderline cardiac failure or diuresis due tolevated atrial natriuretic peptide (ANP) or brain natriureticeptide (BNP) are associated with mild to moderate polyhy-ramnios. In most, the fetal condition precedes polyhydram-ios, but in some (for example intermittent severe supraven-ricular tachycardia), elevated AFV may exist for severaleeks before the underlying cause is determined.
able 5 Polyhydramnios
Degree SDP AFI
ild >8 >24oderate >11 >32evere >15 >44
Investigation of polyhydramnios should include high-level e
ltrasound, supplemented by appropriate fetal magnetic res-nance imaging, invasive testing for karyotype and metabolicisorders, and multidisciplinary consultation. Severity corre-
ates well with the complexity of the fetal source, so casesith severe polyhydramnios may be transferred to a tertiary
enter care. In poorly controlled diabetics, birth weighthows a linear correlation with amniotic fluid volume, sug-esting an increased risk for shoulder dystocia or neonatalomplications, but the variation in presentation is wide, sohe predictive accuracy is limited. As well as these correla-ions with fetal condition, polyhydramnios severity also gen-rates complications. Preterm labor and delivery, malpresen-ation due to excess fetal mobility, abruption from suddenterine decompression, and a fourfold increase in cesareanections in most studies and a sixfold increase in postpartumemorrhage, all apply. Severe polyhydramnios mandateslose monitoring of contractions, cervical status, and poten-ial interventions to prolong the pregnancy. Discussion ofossible long-term neurologic sequelae is important in pre-elivery counseling.Therapeutic approaches to polyhydramnios include am-
ioreduction and the use of indomethacin, neither of whichave been studied in randomized controlled trials. Comparisonsf rapid versus slow drainage, large volume versus repeatedmall volumes, and the use of tocolysis during amnioreductionave not shown significant differences. Complications of am-ioreduction relate to initial severity, gestational age at presen-ation, and preterm labor. As amniotic fluid is removed, expan-ion of the placenta drains blood from the fetus, which can causeong-term central nervous system and cardiac injury. Serial am-iodrainage has been successfully conducted in a number ofases, reducing the impact of prematurity. This benefit must beeighed against the potential risk to mother and fetus should
ggressive preterm labor or placental abruption follow the pro-edure.
Six series have reported the use of indomethacin to treatolyhydramnios.18 Indomethacin’s renovascular effect re-uces fetal urine production—amniotic fluid volume falls,specially in those with normal amniotic fluid (eg, cases ofervical incompetence), nonobstructive causes (maternalnemia or maternal renal failure), and after 26 weeks gesta-ion (fetal renovascular responsiveness earlier is limited). Theack of randomized control data suggests cautious applica-ion. The tocolytic effect of indomethacin in prolonging suchregnancies should not be overlooked—reduced amnioticuid may simply be a side effect.
mniotic Fluid Researchmniotic fluid is a highly complex mixture, used with good
requency PNM Anomalies
68% 50 6% or less19% 190 Up to 45%13% 540 Up to 65%
F
ffect to inhibit bacterial growth in burn victims, to promote

hpycfliitmnnt
R
1
1
1
1
1
1
1
1
1
294 C.R. Harman
ealing of burns and other skin injury, and the importantulmonary and renal effects of swallowed amniotic fluid haveet to be completely defined. As a source for pluripotentialells and novel anti-inflammatory compounds, amnioticuid is a focal point of research. A number of drugs, includ-
ng thyroid stimulating hormone (TSH), thyroxin, antibiot-cs, Digoxin, and radio-opaque dye are effectively ingested byhe nonasphyxiated human fetus, pointing to other experi-ental potentials. More systematic research approaches areecessary to decide whether deliberate manipulation of am-iotic fluid volumes or specific contents of amniotic fluid areherapeutically worthwhile.
eferences1. Buhimschi CS, Weiner CP, Buhimschi IA: Proteomics part II: the
emerging role of proteomics over genomics in spontaneous pretermlabor/birth. Obstet Gynecol Surg 61(8):543-553, 2006
2. Bujold E, Pasquier JC, Simoneau J, et al: Intra-amniotic sludge, shortcervix and risk of preterm delivery. J Obstet Gynecol Can 28(3):198-202, 2006
3. Vogel I, Thorsen P, Curry A, et al: Biomarkers for the prediction ofpreterm delivery. Acta Obstet Gynecol Scand 84(6):516-525, 2005
4. Chamberlain PF, Manning FA, Morrison I, et al: Ultrasound evaluationof amniotic fluid volume I. The relationship of marginal and decreasedamniotic fluid to perinatal outcome. Am J Obstet Gynecol 150(3):245-249, 1984
5. Chamberlain PF, Manning FA, Morrison I, et al: Ultrasound evaluationof amniotic fluid volume II. The relationship of increased amniotic fluidvolume to perinatal outcome. Am J Obstet Gynecol 150(3):250-254,1984
6. Harman CR: Assessment of fetal health. In: Creasy R, Iams J, Resnik, R
(eds): Maternal–Fetal Medicine, (ed 6). Toronto, WB Saunders, 20077. Ott WJ: Re-evaluation of the relationship between amniotic fluid vol-ume and perinatal outcome. Am J Obstet Gynecol 192(6):1803-1809,2005
8. El-Haddad MA, Desai M, Gayle D, et al: In utero development of fetalthirst and appetite: potential for programming. J Soc Gynecol Investig11(3):123-130, 2004
9. Magann EG, Morton ML, Nolan TE, et al: Comparative efficacy of twosonographic measurements for the detection of aberrations in the am-niotic fluid volume on pregnancy outcome. Obstet Gynecol 83(6):959-962, 1994
0. Magann FG, Chauhan SP, Doherty DA, et al: The evidence for aban-doning the amniotic fluid index in favor of the single deepest pocket.Am J Perinatol 24(9):549-555, 2007
1. Tan LK, Kumar S, Jolly M, et al: Test amnioinfusion to determinesuitability for serial therapeutic amnioinfusion in midtrimester prema-ture rupture of membranes. Fetal Diagn Ther 18(3):183-189, 2003
2. Locatelli A, Vergani P, Di Pirro G, et al: Role of amnioinfusion in themanagement of premature rupture of membranes at �26 weeks gesta-tion. Am J Obstet Gynecol 183(4):878-882, 2000
3. Gramellini D, Fien S, Kaihura C, et al: Antepartum amniofusion: areview. J Matern Fetal Neonatal Med 14(5):291-296, 2003
4. Hofmeyr GJ, Gülmezoglu AM: Maternal hydration for increasing am-niotic fluid volume in oligohydramnios and normal amniotic fluid vol-ume. Cochrane Database Syst Rev (1):CD000134, 2002
5. Hofmeyr GJ: Amnioinfusion for umbilical cord compression in labour.Cochrane Database Syst Rev (2):CD000013, 2000
6. Xu H, Hofmeyr J, Roy C, et al: Intrapartum amnioinfusion for meconi-um-stained amniotic fluid: a systematic review of randomized controltrials. BJOG 114 (4):383-390, 2007
7. Dashe JS, McIntire DD, Ramus RM, et al: Hydramnios: anomaly prev-alence and sonographic detection. Obstet Gynecol 100(1):134-139,2002
8. Rodriguez MH: Polyhydramnios: does reducing the amniotic fluid vol-ume decrease the incidence of prematurity? Clin Perinatol 19(2):359-
366, 1992
PM
P
TAWGmcno
tta
PaSbc
D
A
0d
ostdates and Antenatal Testingichael Y. Divon, MD, and Noa Feldman-Leidner, MD
The standard definition of a prolonged pregnancy is 42 completed weeks of gestation. Theincidence of prolonged pregnancy varies depending on the criteria used to define gestationalage at birth. It is estimated that 4 to 19% of pregnancies reach or exceed 42 weeks gestation.Several studies that have used very large computerized databases of well-dated pregnanciesprovided insights into the incidence and nature of adverse perinatal outcome such as anincreased fetal and neonatal mortality as well as increased fetal and maternal morbidity inprolonged pregnancy. Fetal surveillance may be used in an attempt to observe the prolongedpregnancy while awaiting the onset of spontaneous labor. This article reviews the differentmethodologies and protocols for fetal surveillance in prolonged pregnancies. On the one hand,false-positive tests commonly lead to unnecessary interventions that are potentially hazardousto the gravida. On the other hand, to date, no program of fetal testing has been shown tocompletely eliminate the risk of stillbirth.Semin Perinatol 32:295-300 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS prolonged pregnancy, fetal testing, perinatal morbidity, prenatal mortality, non-stress test, biophysical profile, Doppler
lnasdadiiphscdwpnAsptmppdpo
rolonged Pregnancy
he standard definition of a prolonged pregnancy is 42 com-pleted weeks of gestation. This definition is endorsed by the
merican College of Obstetricians and Gynecologists, Theorld Health Organization, and the International Federation ofynecology and Obstetrics.1-3 In view of more recent perinatalortality data that were derived from accurately dated pregnan-
ies, it would be reasonable to conclude that prolonged preg-ancy should be defined as gestational age at birth greater thanr equal to 41 weeks of gestation.
The incidence of prolonged pregnancy varies depending onhe criteria used to define gestational age at birth. It is estimatedhat 4 to 19% of pregnancies reach or exceed 42 weeks gestationnd 2 to 7% complete 43 weeks of gestation.
rolonged Pregnancy asn Indication for Fetal Testing
everal studies that have used very large computerized data-ases of well-dated pregnancies provide insights into the in-idence and nature of adverse perinatal outcome in pro-
epartment of Obstetrics and Gynecology, Lenox Hill Hospital,New York, NY.
ddress reprint requests to Michael Y. Divon, MD, Department of Obstetricsand Gynecology, Lenox Hill Hospital, 130 E. 77th St., New York, NY
i10075. E-mail: [email protected]
146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.013
onged pregnancy. Divon and coworkers evaluated fetal andeonatal mortality rates in 181,524 accurately dated termnd prolonged pregnancies.4 Their study documented amall but significant increase in fetal mortality in accuratelyated pregnancies that extend beyond 41 weeks gestationnd demonstrated that fetal growth restriction is indepen-ently associated with a large increase in perinatal mortality
n these pregnancies. These results were confirmed by othernvestigators.5,6 Clausson and coworkers documented thaterinatal mortality rates in small for gestational age fetusesad higher odds ratio for stillbirth and neonatal death.6 Thetillbirth rate did not change significantly when fetuses withongenital malformations were excluded. However, an 80%rop in neonatal deaths occurred when malformed neonatesere excluded from the analysis. In addition, prolongedregnancies were associated with an increased frequency ofeonatal convulsions, meconium aspiration syndrome, andpgar score of �4 at 5 minutes. Again, morbidity in posttermmall for gestational age (SGA) infants was higher than inostterm AGA infants. Further support for the concept thathe “small and old” fetus suffers from increased perinatalortality was provided by Campbell and coworkers, whoerformed a multivariate analysis of factors associated witherinatal death among 65,796 singleton postterm (�294ays) births.7 Three variables were identified as independentredictors of perinatal mortality. SGA and maternal age equalr greater than 35 years were associated with a significant
ncrease in perinatal mortality. Interestingly, large for gesta-295

ttphshatp
myspbli3
aam4bgetrmt
FFptmhpi
mtfJtsta
h0tTpo
slt
iwflcrsftfptarcptAsdwuwbtbflabwogvpaa
niwatnfpadt
soose
296 M.Y. Divon and N. Feldman-Leidner
ional age status (ie, birth weight �90th percentile for gesta-ional age) was associated with a modest protective effect forerinatal death. However, macrosomia was associated with aigher incidence of labor dysfunction, obstetrical trauma,houlder dystocia, and maternal hemorrhage. Several studiesave shown that the incidence of macrosomia increases withdvancing gestational between 37 and 43 weeks. In addition,his increase also results in doubling the cesarean rate forrotraction or descent disorders.8-10
There is good evidence to suggest that fetal and maternalorbidity are also increased as gestational age advances be-
ond term. Tunon and coworkers compared neonate inten-ive care unit (NICU) admission rates among 10,048 termregnancies and 246 prolonged pregnancies (�296 days byoth scan and last menstrual period (LMP) dates).11 Pro-
onged pregnancy was associated with a significant increasen NICU admissions (odds ratio, 2.05; 95% CI, 1.35 and.12).Several maternal and fetal complications were evaluated in
large (n � 45,673) retrospective, cohort study by Caugheynd Musci.12 The authors concluded “that risks to bothother and infant increase as pregnancy progresses beyond
0 weeks’ gestation, and that antenatal fetal testing shouldegin sooner than current recommendation of 42 weeks ofestation.” Olesen and coworkers evaluated a large comput-rized Danish database of singleton, live-born term and post-erm (�42 weeks) deliveries to quantify maternal and fetalisks associated with postterm delivery.13 Both perinatal andaternal complications were increased significantly in post-
erm deliveries.
etal Surveillanceetal surveillance may be used in an attempt to observe therolonged pregnancy safely while awaiting the onset of spon-aneous labor. On the one hand, false-positive tests com-only lead to unnecessary interventions that are potentiallyazardous to the gravida. On the other hand, to date, norogram of fetal testing has been shown to completely elim-
nate the risk of stillbirth.Data presented earlier in this review indicate that perinatalortality is significantly increased as early as 41 weeks ges-
ation and possibly even earlier. The optimal gestational ageor the initiation of fetal testing has not been established.azayeri and coworkers provided physiologic evidence of al-ered fetal oxygenation in patients at �41 weeks by demon-trating elevated plasma erythropoietin levels in these pa-ients.14 Thus, it would seem prudent to initiate fetal testingt 41 weeks of gestation.
Extensive experience with biophysical profile testing inigh-risk populations indicates a perinatal mortality rate of.73 per 1000 tested pregnancies within 1 week of a normalest provided that the amniotic fluid volume is normal.15
wice-weekly testing with the biophysical profile was re-orted in a series of 307 patients followed beyond 42 weeks
f gestation. When the profile score was normal, waiting for lpontaneous labor resulted in healthy neonates and a muchower cesarean section rate. No stillbirths were observed inhis small series.16
Several investigators have examined the efficacy of us-ng a nonstress test (NST) as a primary testing modalityith the addition of sonographic assessment of amnioticuid. Clark and coworkers tested 279 prolonged pregnan-ies with this testing scheme. No stillbirths wereecorded.17 Miller and coworkers reported on the use of aimilar protocol in 6390 prolonged pregnancies.18 Thealse-negative rate of this test was 0.8 per 1000 womenested—a rate that favorably compares with those reportedor the contraction stress test or the complete biophysicalrofile.15,19 An analysis of all false-positive tests showedhat the routine use of nonstress testing combined with themniotic fluid index (AFI) resulted in a 60% false-positiveate in the prediction of intrapartum fetal compromiseompared with a 40% false-positive rate using the com-lete biophysical profile. This increase in false-positiveests was felt to be partly due to the poor specificity of theFI in predicting fetal compromise. Alfirevic and Walkin-haw compared the impact on perinatal outcome of twoifferent protocols for antenatal fetal monitoring after 42eeks.20. One hundred forty-five women with singleton,ncomplicated pregnancies after 42 weeks of gestationere randomly allocated to fetal monitoring by either aiophysical profile combined with computerized cardio-ocography or a standard cardiotocography supplementedy measurement of the largest vertical pocket of amnioticuid. Their results documented significantly more abnormalntenatal monitoring tests in the biophysical profile com-ined with the computerized cardiotocography group. Thereere no differences in cord blood gases, neonatal outcome,r outcomes related to labor and delivery between the tworoups, but there was a trend toward more obstetric inter-entions in the biophysical profile combined with the com-uterized cardiotocography group. Amniotic fluid volumefter 42 weeks was more likely to be labeled as abnormal withmniotic fluid index than with largest vertical pocket.
Sylvestre and coworkers evaluated the incidence of ab-ormal testing (NST and AFI) as a function of birth weight
n 792 uncomplicated prolonged pregnancies (�41eeks).21 They showed an inverse relationship between
bnormal testing and birth weight. In addition, small fe-uses were more likely to require a cesarean delivery foron-reassuring fetal status during labor than were all otheretuses. Thus, it is reasonable to conclude that the small,ostterm fetus is not only more likely to die in utero but islso more likely to fail antepartum fetal testing and to beelivered by nonelective cesarean section for an intrapar-um diagnosis of non-reassuring fetal status.
The implicit assumption in the expectant managementtrategy is that the presence of an abnormal fetal test (such asligohydramnios, low biophysical profile score, or spontane-us fetal heart rate decelarations) represents a change in fetaltatus that requires intervention in the from of prompt deliv-ry. A novel view of the regulation of fetal homeostasis during
ate gestation was offered by Onyeije and Divon.22 These
araspw1iere0tcer
utaDprsshs1ccg
tuapsslftawaicvfinpgtcf
so
pdwsic
ntstpaabdlaqot
oetpdui1t1cds1o
ndrsvs2auocbrAatnc
Postdates and antenatal testing 297
uthors studied the incidence of maternal ketonuria (as aeflection of maternal starvation and dehydration) and itsssociation with abnormal fetal surveillance tests. One thou-and eight hundred ninety-five patients were managed ex-ectantly with semiweekly fetal testing. Beginning at 41eeks gestation, clinically detectable ketonuria occurred in0.9% of patients studied. Patients with ketonuria were at
ncreased risk for abnormal test results, including the pres-nce of oligohydramnios (24 versus 9.3%, P � 0.0001), non-eactive NST (6.2 versus 2.15%, P � 0.0001), and the pres-nce of fetal heart rate decelerations (14 versus 9.2%, P �.0039). The authors suggested that reversible maternal ke-onuria contributes to the false-positive test results often en-ountered in fetal testing, and that such patients might ben-fit from treatment of ketonuria rather than be delivered inesponse to the abnormal test results.
The formation of amniotic fluid is a complex and poorlynderstood process. Multiple authors have demonstratedhat amniotic fluid volume decreases as gestational agedvances beyond 32 or 34 weeks gestation. Marks andivon evaluated the AFI in 511 well-dated prolongedregnancies.23 Gestational age at the time of the studyanged from 41 weeks to 43 weeks and 6 days. AFI mea-urements ranged from 1.7 to 24.6 cm, with a mean andtandard deviation of 12.4 � 4.2 cm at 41 weeks. Oligo-ydramnios (AFI �5.0 cm) was detected in 11.5% of thetudy population. Longitudinal data were available from21 patients. These patients demonstrated a mean de-rease in AFI of 25% per week. Thus, the authors con-luded that the majority of pregnancies at �41 weeksestation have a normal volume of amniotic fluid.In the absence of ruptured membranes or fetal urinary
ract abnormalities, diminishing levels of amniotic fluid vol-me may be related to poor placental function.24 Trimmernd coworkers detected diminished urine production inregnancies of 42 weeks or more with oligohydramnios anduggested that decreased fetal urine production was the re-ult of preexisting oligohydramnios, which limited fetal swal-owing of amniotic fluid rather than a decrease in renal per-usion.25 Bar-Hava and coworkers used pulsed-wave Dopplero evaluate resistance index values in the fetal middle cerebralrtery, renal, and umbilical arteries in 57 pregnancies at �41eeks gestation.26 It was expected that, with hypoxia, imped-
nce in the cerebral circulation might decrease as impedancencreased in the renal circulation. Oligohydramnios (AFI �5m) was detected in 15 patients. The various resistance indexalues and the ratios among them were not significantly dif-erent in patients with or without oligohydramnios. Interest-ngly, the mean birth weight in patients with oligohydram-ios was significantly lower than the mean birth weight inatients with a normal AFI. The authors concluded that oli-ohydramnios in these patients is not associated with a no-iceable redistribution of blood flow and suggested that theause of oligohydramnios is probably unrelated to renal per-usion.
The fact that oligohydramnios was found more often in themaller fetuses is intriguing. It suggests that the appearance of
ligohydramnios is a pathologic rather than a physiologic nrocess. It may indicate that the pathophysiology of oligohy-ramnios in prolonged pregnancy is similar to that involvedith the formation of oligohydramnios in the growth-re-
tricted fetus, and overall it is consistent with the concept thatt is the small and “older” fetus that is more prone to compli-ations arising from asphyxia.
Leveno and coworkers used the presence of oligohydram-ios to explain the increased incidence of abnormal antepar-um and intrapartum fetal heart rate (FHR) abnormalitieseen in prolonged pregnancies.27 These authors suggestedhat prolonged FHR decelerations representing cord com-ression preceded 75% of cesarean deliveries for fetal jeop-rdy. The association between reduced amniotic fluid indexnd variable decelerations is well documented, as suggestedy Gabbe and coworkers, and variable FHR decelerationsetected in patients with oligohydramnios are probably re-
ated to increased umbilical cord compression.28 Both Phelannd coworkers and Divon and coworkers found that the fre-uency of nonstress tests demonstrating FHR decelerationsr bradycardia increased as the ultrasonographic estimates ofhe amniotic fluid declined.29-31
The use of an amniotic fluid index �5.0 cm to defineligohydramnios was first suggested by Phelan and cowork-rs in 1987, as an arbitrary cutoff value based on retrospec-ive studies. Nevertheless, it has since gained popular ap-eal.29,30 A meta-analysis evaluated the risk of cesareanelivery for fetal distress, 5-minute Apgar score of �7, andmbilical artery pH �7.00 in patients with antepartum or
ntrapartum AFI �5.0 cm.32 Eighteen reports describing0,551 patients at various gestational ages were included inhe analysis. The overall incidence of oligohydramnios was5.2%. The authors concluded that an AFI �5.0 cm is asso-iated with an increased risk of cesarean delivery for fetalistress (relative risk of 2.2; 95% CI, 1.5-3.4) and an Apgarcore of �7 at 5 minutes (relative risk of 5.2; 95% CI, 24-13). However, no association was demonstrated betweenligohydramnios and severe fetal acidosis.A prospective, blinded observational study of the useful-
ess of ultrasound assessment of amniotic fluid in the pre-iction of adverse outcome in the prolonged pregnancy waseported by Morris and coworkers.33 The authors demon-trated that AFI �5 cm was significantly associated with ad-erse perinatal outcome. Despite these associations, the sen-itivity of an AFI �5 cm was very low, ranging from 11.5 to8.6 for major adverse outcome, fetal distress in labor, ordmission to the NICU. The authors concluded that “routinese is likely to lead to increased obstetric intervention with-ut improvement in perinatal outcome” and that large clini-al trials are necessary to assess the effectiveness of deliveryased on sonographically diagnosed oligohydramnios. In aecent study Lam and coworkers evaluated the usefulness ofFI in the fetal surveillance of postdate pregnancies.34 Theuthors concluded that “although AFI may be used to predicthe occurrence of thick meconium stained liquor and theeed for intervention for fetal distress in postdate pregnan-ies, its role on its own is limited.”
The presence of sonographically diagnosed oligohydram-
ios is often used as an indication for delivery of pregnancies
thnnmtosbnuv
mfslpnDcyuwwfviatpdrdiAfdfiphspdfvtatiipbspmcp
pud
padnvpfcocdfewctptlrgDticfd
uwpcmc
ipspoism
SMtgmdt
298 M.Y. Divon and N. Feldman-Leidner
hat reach term gestation or extend beyond term. One shouldowever realize that up to 50% of patients, who are diag-osed by ultrasound as having oligohydramnios, will have aormal volume of amniotic fluid on artificial rupture of theembranes.35 In addition, there are no large-scale prospec-
ive randomized studies documenting the benefits of deliverynce oligohydramnios has been diagnosed. In the absence ofuch studies, it would seem prudent to deliver patients at oreyond 41 weeks gestation who demonstrate oligohydram-ios primarily because of the large body of data which doc-ments an association between diminished amniotic fluidolume and adverse perinatal outcome.
Doppler velocimetry is often used to identify fetal compro-ise due to altered fetal circulation. Its role in establishing
etal well-being in prolonged pregnancies is unclear. Severaltudies have concluded that the use of umbilical artery Dopp-er velocimetry is not associated with an improvement of theositive-predictive value of fetal testing in prolonged preg-ancy.36-39 Zimmermann and coworkers performed a fetaloppler cross-sectional, prospective study in 153 pregnan-ies beyond 287 days of gestation (36% were followed be-ond 42 weeks of gestation).39 The resistance indices of thembilical artery and the middle cerebral artery waveformsere studied every 2 days until delivery. All velocities fellithin the known 95% confidence intervals for normal term
etuses. Doppler measurements were unable to predict ad-erse fetal outcomes, such as abnormal fetal heart rate trac-ngs, thick meconium, the need for urgent operative delivery,cidemia at delivery, or neonatal encephalopathy. In con-rast, Oz and coworkers studied 147 well-dated, singleton,ostterm pregnancies, of which 21 (14.3%) had oligohy-ramnios.40 The authors assessed the correlation betweenenal and umbilical artery Doppler velocimetry, and oligohy-ramnios. They demonstrated that the renal artery resistance
ndex was significantly higher in cases with oligohydramnios.renal artery Doppler end-diastolic velocity below the mean
or gestational age significantly increased the risk of oligohy-ramnios (relative risk of 1.5 with 95% CI of 1.1-2.0). Theirndings support the hypothesis that increased arterial im-edance is an important factor in the development of oligo-ydramnios in prolonged pregnancies. Two other studiesupport these findings.41,42 Recently, Lam and coworkers in arospective observational study of 118 uncomplicated post-ated pregnancies at 41 weeks evaluated the distribution ofetal cerebro-placental Doppler indices and amniotic fluidolume.41 The correlation with the incidence of passage ofhick meconium in labor was analyzed. The middle cerebralrtery pulsatility index was found to be significantly betterhan amniotic fluid volume or umbilical artery pulsatilityndex in predicting the risk of thick meconium-stained liquorn labor. Figueras and coworkers in a prospective study ofrolonged pregnancies evaluated the value of middle cere-ral artery Doppler indices obtained from different samplingites in predicting umbilical cord gases at delivery.42 Fifty-sixatients were included in the final analysis. The proximaliddle cerebral artery pulsatility index was found to signifi-
antly predict umbilical artery pO2 at delivery but did not
redict pH. oIn conclusion, given the information available at theresent time, it is difficult to define the extent to which these of Doppler velocimetry can improve the positive-pre-ictive value of fetal testing in prolonged pregnancy.Sonographic fetal weight estimates are often obtained as
art of fetal testing in prolonged pregnancies. The accuratend timely prediction of macrosomia may well influenceelivery management decisions. However, one shouldote that the accurate estimation of fetal weight must beiewed in its broad clinical context of feto-pelvic dispro-ortion. Thus, the crucial factor is the relationship of theetal size to the maternal pelvis rather than the commonlinical preoccupation with macrosomia alone. Focusingn either one of these factors in isolation represents aonceptual error.43 Traditionally, obstetricians have pre-icted fetal weight by abdominal palpation or symphysial-undal height measurement. Ultrasound failed to fulfill thexpectation for a more accurate method to estimate fetaleight. Both Chervenak and coworkers and Pollack and
oworkers documented that a sonographic estimate of fe-al weight of �4000 g had low sensitivity and low positive-redictive value and, therefore, the authors concludedhat routine sonographic screening for macrosomia in pro-onged pregnancies is associated with relatively low accu-acy.43-45 In an attempt to improve the accuracy of sono-raphic estimates of fetal weight, O’Reilly-Green andivon used receiver operating characteristic curve analysis
o identify optimal cutoff values of estimate of fetal weightn the prediction of macrosomia in prolonged pregnan-ies.46 The authors concluded that cutoff values derivedrom their analysis resulted in reasonable sensitivities butisappointingly low positive-predictive values.The practical implications of the low predictive value of
ltrasonography have been highlighted by Rouse and co-orkers. These authors have shown that in nondiabeticregnancies the level of intervention and the economicosts of prophylactic cesarean delivery for fetal macroso-ia diagnosed by mean of ultrasonography would be ex-
essive.47,48
It would seem reasonable that as fetal weight continues toncrease with advancing gestational age, delivery of thoseregnancies with a potential for macrosomia might preventome cases of shoulder dystocia and a subsequent brachiallexus injury. However, this intervention could be achievednly by increasing the rate of inductions of labor or by anncreased use of cesarean deliveries, both of which wouldubject the patient to added morbidity or even unnecessaryortality.
ummaryanagement of the prolonged pregnancy is primarily de-
ermined by the interplay of three factors: certainty ofestational dating, the risks associated with expectantanagement, and the likelihood of spontaneous vaginalelivery following an induction of labor. A Cochrane Da-abase of Systematic Review from 2007 assessed the effects
f interventions aimed at either reducing the incidence or
iscitmant
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
Postdates and antenatal testing 299
mproving the outcome of postterm pregnancy. Twenty-ix trials of variable quality were included.49 The authoroncluded that routine early pregnancy ultrasound exam-nation and subsequent adjustment of delivery date appearo reduce the incidence of postterm pregnancy. Further-ore, routine induction of labor after 41 weeks gestation
ppears to reduce perinatal mortality. However, there wasot enough evidence to evaluate the effects of antenatalesting on fetal wellbeing.
eferences1. American College of Obstetricians and Gynecologists (ACOG): Amer-
ican College of Obstetricians and Gynecologists Practice Bulletin. Man-agement of Postterm Pregnancy, September 2004
2. World Health Organization (WHO): Recommended definition termi-nology and format for statistical tables related to perinatal period andrise of new certification for the cause of perinatal deaths. Modificationsrecommended by FIGO as amended, October 14, 1976. Acta ObstetGynecol Scan 56:247-253, 1977
3. Federation of Gynecology and Obstetrics (FIGO): Report of the FIGOsubcommittee on Perinatal Epidemiology and health statistics follow-ing a workshop in Cairo, November 11-18, 1984. London, Interna-tional Federation of Gynecology and Obstetrics 1986, p 54
4. Divon MY, Haglund B, Nisell H, et al: Fetal and neonatal mortality inthe post-term pregnancy: the impact of gestational age and fetal growthrestriction. Am J Obstet Gynecol 178:726-731, 1998
5. Ingemarsson I, Kallen K: Stillbirths and rate of neonatal deaths in76,761 postterm pregnancies in Sweden, 1982-1991: a register study.Acta Obstet Gynecol Scand 76:658-662, 1997
6. Clausson B, Cnattingius S, Axelsson O: Outcomes of post-term births:the role of fetal growth restriction and malformations. Obstet Gynecol94:758-762, 1999
7. Campbell MK, Ostbye T, Irgens LM: Post-term birth: risk factors andoutcomes in a 10-year cohort of Norwegian births. Obstet Gynecol89:543-548, 1997
8. Boyd ME, Usher RH, McLean FH: Fetal macrosomia: prediction, risks,proposed management. Obstet Gynecol 61:715-722, 1983
9. McLean FH, Boyd ME, Usher RH, et al: Post-term infants: too big or toosmall? Am J Obstet Gynecol 164:619-624, 1991
0. Nahum GG, Stanislaw H, Huffaker BJ: Fetal weight gain at term: linearwith minimal dependence on maternal obesity. Am J Obstet Gynecol172:1387-1394, 1995
1. Tunon K, Eik-Nes SH, Grottum P: Fetal outcome in pregnancies de-fined as post-term according to the last menstrual period estimate, butnot according to the ultrasound estimate. Ultrasound Obstet Gynecol14:12-16, 1999
2. Caughey AB, Musci TJ: Complications of term pregnancies beyond 37weeks of gestation. Obstet Gynecol 103:57-62, 2004
3. Olesen AW, Wesergaad JG, Olsen J: Perinatal and maternal complica-tions related to postterm delivery: a national register-based study,1978-1993. Am J Obstet Gynecol 189:222-227, 2003
4. Jazayeri A, Tsibris JC, Spellacy WN: Elevated umbilical cord plasmaerythropoietin levels in prolonged pregnancies. Obstet Gynecol 92:61-63, 1998
5. Manning FA, Morrison I, Harman CR, et al: Fetal assessment based onfetal biophysical profile scoring: experience in 19,221 referred high-risk pregnancies. II. An analysis of false-negative fetal deaths. Am JObstet Gynecol 157:880-884, 1987
6. Johnson JM, Harman CR, Lange IR, et al: Biophysical profile scoring inthe management of the post term pregnancy: an analysis of 307 pa-tients. Am J Obstet Gynecol 154:269-273, 1986
7. Clark SL, Sabey P, Jolley K: Nonstress testing with acoustic stimulationand amniotic fluid volume assessment: 5973 tests without unexpectedfetal death. Am J Obstet Gynecol 160:694-697, 1989
8. Miller DA, Rabello YA, Paul RH: The modified biophysical profile:antepartum testing in the 1990’s. Am J Obstet Gynecol 174:812-817,
19969. Freeman RK, Anderson G, Dorchester W: A prospective multicentermulti institutional study of antepartum fetal heart rate monitoring. II.Contraction stress test versus non-stress test for primary surveillance.Am J Obstet Gynecol 143:778-781, 1982
0. Alfirevic Z, Walkinshaw SA: A randomized controlled trial of simplecompared with complex antenatal fetal monitoring after 42 weeks ofgestation. Br J Obstet Gynaecol 102:638-643, 1995
1. Sylvestre G, Fisher M, Westgren M, et al: Non-reassuring fetal status inthe prolonged pregnancy: the impact of fetal weight. Ultrasound ObstetGynecol 18:244-247, 2001
2. Onyeije CI, Divon MY: The impact of maternal ketonuria on fetal testresults in the setting of postterm pregnancy. Am J Obstet Gynecol184:713-718, 2001
3. Marks AD, Divon MY: Longitudinal study of the amniotic fluid index inpostdates pregnancy. Obstet Gynecol 79:229-233, 1992
4. Gresham El, Rankin JH, Makowski EL, et al: An evaluation of fetalrenal function in chronic sheep preparation. J Clin Invest 51:149-156, 1972
5. Trimmer KJ, Leveno KJ, Peters MT, et al: Observation on the cause ofoligohydramnios in prolonged pregnancy. Am J Obstet Gynecol 163:1900-1903, 1990
6. Bar-Hava I, Divon MY, Sardo M, et al: Is oligohydramnios in post-termpregnancy associated with redistribution of fetal blood flow? Am JObstet Gynecol 173:519-522, 1995
7. Leveno KJ, Quirk JG Jr, Cunningham FG, et al: Prolonged pregnancyobservations concerning the causes of fetal distress. Am J Obstet Gy-necol 150:465-473, 1984
8. Gabbe SG, Ettinger BB, Freeman RK, et al: Umbilical cord compressionassociated with amniotomy: laboratory observations. Am J Obstet Gy-necol 126:353-355, 1976
9. Phelan JP, Smith CV, Broussard P, et al: Amniotic fluid volume assess-ment with the four-quadrant technique at 36-42 weeks’ gestation. JReprod Med 32:540-542, 1987
0. Phelan JP, Ahn MO, Smith CV, et al: Amniotic fluid index measure-ments during pregnancy. J Reprod Med 32:601-604, 1987
1. Divon MY, Marks AD, Henderson CE: Longitudinal measurement ofamniotic fluid index in postterm pregnancies and its association withfetal outcome. Am J Obstet Gynecol 172:142, 1995
2. Chauhan SP, Sanderson M, Hendrix N, et al: Perinatal outcome andamniotic fluid index in the antepartum and intrapartum periods: ameta-analysis. Am J Obstet Gynecol 181:1473-1478, 1999
3. Morris JM, Thompson K, Smithey J, et al: The usefulness of ultrasoundassessment of amniotic fluid in predicting adverse outcome in pro-longed pregnancy: a prospective blinded observational study. BJOG110:989-994, 2003
4. Lam H, Leung WC, Lee CP, et al: Amniotic fluid volume at 41 weeksand infant outcome. J Reprod Med 2006 6:484-488, 2006
5. O’Reilly-Green CP, Divon MY: Predictive value of amniotic fluid indexfor oligohydramnios in patients with prolonged pregnancies. J MaternFetal Med 5:218-226, 1996
6. Strokes HJ, Roberts RV, Newnham JP: Doppler flow velocity waveformanalysis in postdate pregnancies. Aust NZ J Obstet Gynecol 31:27-30,1991
7. Guidetti DA, Divon MY, Cavalieri RL, et al: Fetal umbilical artery flowvelocimetry in postdate pregnancies. Am J Obstet Gynecol 157:1521-1523, 1987
8. Farmakides G, Schulman H, Ducey J, et al: Uterine and umbilicalDoppler velocimetry in post term pregnancy. J Reprod Med 33:259-261, 1988
9. Zimmermann P, Albck T, Koskinen J, et al: Doppler flow velocimetry ofthe umbilical artery, uteroplacental arteries and fetal middle cerebralartery in prolonged pregnancy. Ultrasound Obstet Gynecol 5:189-197,1995
0. Oz AU, Holub B, Mendilcioglu I, et al: Renal artery Doppler investiga-tion of the etiology of oligohydramnios in postterm pregnancy. ObstetGynecol 100:715-718, 2002
1. Lam H, Leung WC, Lee CP, et al: The use of fetal Doppler cerebroplacentalblood flow and amniotic fluid volume measurement in the surveillance of
postdated pregnancies. Acta Obstet Gynecol Scand 84:844-848, 2005
4
4
4
4
4
4
4
4
300 M.Y. Divon and N. Feldman-Leidner
2. Figueras F, Lanna M, Palacio M, et al: Middle cerebral artery Dopplerindices at different sites: prediction of umbilical cord gases in pro-longed pregnancies. Ultrasound Obstet Gynecol 24:529-533, 2004
3. Pollack RN, Hauer-Pollack G, Divon MY: Macrosomia in postdatespregnancies: the accuracy of routine ultrasonographic screening. Am JObstet Gynecol 167:7-11, 1992
4. Chervenak JL, Divon MY, Hirsch J, et al: Macrosomia in the post-datepregnancy: is routine sonography screening indicated. Am J ObstetGynecol 161:753-756, 1989
5. Pollack RN, Divon MY: Problems in detecting fetal macrosomia. Con-temporary Ob/Gyn, October 1991
6. O’Reilly-Green CP, Divon MY: Receiver operating characteristic
curves of sonographic estimated fetal weight for predictionmacrosomia in prolonged pregnancies. Ultrasound Obstet Gynecol9:403-408, 1997
7. Rouse DJ, Owen J: Prophylactic cesarean delivery for fetal macrosomiadiagnosed by means of ultrasonography—a Faustian bargain? Am JObstet Gynecol 181:332-338, 1999
8. Rouse DJ, Owen J, Goldenberg RL, et al: The effectiveness and costs ofelective cesarean delivery for fetal macrosomia diagnosed by ultra-sound. JAMA 276:1480-1486, 1996
9. Crowley P: Interventions for preventing or improving the outcome ofdelivery at or beyond term. Cochrane Database of Systematic Reviews
2, 2007
AWJ
Arttst
EaFWfpddSanr
UF
A
0d
ntepartum Testing foromen with Previous Stillbirth
onathan W. Weeks, MD
Women with past histories of stillbirth have been referred for antepartum surveillance sincethe inception of electronic fetal monitoring. However, this approach was originally based onmid-twentieth century perinatal studies that noted an increase in adverse outcomes inpregnancies subsequent to stillbirth. When these landmark studies were done, Rh immuneglobulin, ultrasonography, and other important medical advances had not yet occurred.This article discusses whether women who have suffered a past stillbirth remain atincreased risk for perinatal mortality and morbidity in future pregnancies and whetherantepartum fetal surveillance can reduce the risk of recurrent stillbirth.Semin Perinatol 32:301-306 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS stillbirth, fetal testing, antepartum surveillance, fetal death, intrauterine fetaldemise
ppvesta
sasissinsiw
rT1qrtoo
history of stillbirth is an accepted indication for antepar-tum surveillance.1,2 The purpose of this article was to
eview the data supporting stillbirth as an indication for fetalesting and to evaluate the reported experience with antepar-um surveillance in women who have suffered a previoustillbirth. We also address the question of whether antepar-um surveillance is effective at preventing recurrent stillbirth.
vidence for Stillbirths a Risk Factor for Pooruture Pregnancy Outcomeomen who have suffered one stillbirth are at increased risk
or perinatal mortality in subsequent pregnancies. This wasroven in large British and U.S. population studies con-ucted in the mid-twentieth century. The U.S. study, con-ucted by the National Institute of Neurological Diseases andtroke, determined that patients with previous stillbirths hadperinatal mortality rate of 73 per 1000 in subsequent preg-ancies and nearly 2% of their surviving children were neu-ologically abnormal at 1 year of age.3 The British study re-
niversity of Louisville School of Medicine, Louisville, KY.rom “Antenatal Testing: A Reevaluation,” a workshop cosponsored by the
Pregnancy and Perinatology Branch (PPB) at the National Institute ofChild Health and Human Development, the Office of Rare Diseases,National Institutes of Health, the American College of Obstetricians andGynecologists, and the American Academy of Pediatrics.
ddress reprint requests to Jonathan W. Weeks, MD, P.O. Box 43578,
tLouisville, KY 40253-0578. E-mail: [email protected]146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.014
orted that the risk of poor outcomes in subsequentregnancies was more than doubled among women with pre-ious stillbirths.4 These historic studies predated the era oflectronic fetal monitoring, but the reported experienceserved as justification for inclusion of stillbirth as an indica-ion for fetal surveillance once the technology became avail-ble.
Based on the aforementioned U.S. and British perinataltudies, utilization of antepartum surveillance in women withpast history of stillbirth seems prudent. However, those
tudies were conducted before the development and widemplementation of several valuable medical breakthroughsuch as Rh immune globulin, ultrasonography, serumcreening for aneuploidy, and use of home glucose monitor-ng devices. Several population-based studies on future preg-ancy outcomes in women who have experienced a previoustillbirth have recently been published.5-7 These newer stud-es have also revealed excess perinatal mortality amongomen with previous stillbirths.In 1993, Samueloff and coworkers published a study of
ecurrent stillbirths at an academic center in San Antonio.he overall stillbirth rate in the 13-year cohort was 8.3 per000 births. Of the 403 women who had pregnancies subse-uent to stillbirths, 34 experienced recurrent stillbirths for aate of 84.3 per 1000 births. Thus, risk was 10-fold higherhan that of multiparous women who had no previous historyf stillbirth. When compared with women with past historiesf stillbirth and a live-born infant in subsequent pregnancies,
he women who had recurrent stillbirths were more likely to301

hr
wpiwipfiCwaie
4sappnssnwbt
fspwsbtw
fmowrwltaeg
sibp
iqtpcjw
EAPHmammpcsaEgttwetocdt
hihtwt
T
BWO
SM
T
TPPPPP
N
302 J.W. Weeks
ave diabetes or hypertension. However, half of women withecurrent stillbirth had no chronic medical conditions.7
Sharma and coworkers studied a large cohort of Missouriomen who gave birth between 1978 and 1997.5 Futureregnancy outcomes in women who experienced a stillbirth
n their first pregnancy were compared with those of womenho delivered a live birth in their first pregnancy. The study
ncluded 404,201 women: 99.5% had a live birth in the firstregnancy and 0.5% (1979) had a stillbirth, which was de-ned as an intrauterine death at 20 weeks gestation or more.ompared with women without a history of stillbirth,omen with a history of stillbirth in their first pregnancy had57% increase in complications in the second pregnancy,
ncluding diabetes, chronic hypertension, preeclampsia,clampsia, and abruptio placenta.
There were 1929 stillbirth cases in the second pregnancy:5 (2.3% of all cases) occurred in women with a history oftillbirth and 1884 (97.7% of all cases) among those withoutstillbirth history. Hence, the stillbirth rate in women with arevious history of fetal death at 20 weeks or more was 22.7er 1000 as compared with 4.7 per 1000 for those who didot have a stillbirth with their first pregnancies. Table 1hows the stillbirth rates stratified by race and history oftillbirth in the first pregnancy. Sharma’s data revealed aearly twofold increase in stillbirth rates among blackomen overall. In pregnancies subsequent to a stillbirth,lack women had a stillbirth risk that was sevenfold greaterhan the national average.
Sharma and coworkers also calculated adjusted estimatesor the relationship between prior stillbirth and subsequenttillbirth recurrence. Several models for relative risk wereresented in which the reference group comprised womenith a live birth in the first pregnancy, live births excluding
mall for gestational age (SGA), live births excluding pretermirths, or live births excluding preterm or SGA. In all modelshe relative risk of stillbirth among the total population ofomen with a previous stillbirth was increased over fourfold.Most studies on stillbirth recurrence comprised patients
rom the general population, which include women withedical complications and risk factors. This could cause an
verestimation of risk in low-risk patients. Sharma and co-orkers have also conducted a population study on stillbirth
ecurrence in a group of relatively low-risk women.5 The dataere again derived from a Missouri database. The relatively
ow-risk population was defined as nonsmoking women, lesshan 35 years of age, who were carrying singleton, non-nomalous fetuses. The study group (n � 1050) had experi-nced a stillbirth in the previous pregnancy, while the control
able 1 Stillbirth Rates by Race and Past History of Stillbirth
History of SB No History of SB
lack 35.9 7.6hite 19.1 4.2verall 22.7 4.7
B rate � SB per 1000 births (live births plus stillbirths).odified from Sharma and coworkers.6
roup had live births (n � 261,384). Nine hundred forty- R
even stillbirths occurred in the second pregnancies; 20 weren women with past stillbirths (stillbirth rate, 19.0 per 1000irths), and 927 were in the control group (stillbirth rate, 3.6er 1000 births; P � 0.001).Although the population studies mentioned above are lim-
ted by their reliance on birth certificate data and the lack ofuantitative assessment of the frequency and severity of ma-ernal conditions, the evidence for stillbirth as a predictor ofoor future pregnancy outcome and recurrent stillbirth isompelling. Even in a relatively low-risk population, the ad-usted risk of stillbirth is nearly sixfold higher among thoseith a past history of stillbirth.5
xperience withntepartum Testing forrevention of Recurrent Stillbirth
aving proven stillbirth as a harbinger of future perinatalortality and morbidity in studies, conducted before and
fter the development of important laboratory, imaging, andedical interventions, the next logical step is to considerethods to mitigate future risk. In the hopes of improvingregnancy outcomes in women with a history of stillbirth,linicians have used antenatal testing since its inception. Pro-pective randomized trials to test whether fetal monitoringctually reduces recurrent stillbirth have never been done.arly in the history of electronic fetal monitoring, there was areat deal of enthusiasm for the technology and high expec-ations of efficacy. The apparent lack of risk associated withhe use of antepartum fetal surveillance also contributed to itside adoption for patients with histories of stillbirth. How-
ver, the real deterrent to randomized trials was, and still is,he low numbers of affected women (stillbirths occur in �1%f pregnancies) and the need to control for a large number ofonfounding variables. In fact, these challenges have led to aearth of retrospective study on the performance of fetalesting to prevent recurrent stillbirth.
Freeman and coworkers reported on 337 women withistories of stillbirth who were followed with antenatal test-
ng.8 These pregnancies were a subset of a total of 7052igh-risk pregnancies undergoing antenatal testing. Al-hough it was a multi-institutional retrospective study ofomen seen between 1976 and 1982, the data on antenatal
esting indications and results were collected prospectively.
able 2 Indications for Fetal Testing Among Stillbirth Patients
Indication for TestingNo. of
Patients Percent
otal stillbirth patients 337 —revious stillbirth only 163 48.3revious stillbirth and hypertension 83 24.6revious stillbirth and diabetes 71 21revious stillbirth and IUGR 29 8.6revious stillbirth and postdates 21 6.2
ote. Multiple diagnoses in some patients.
eprinted with permission.8
AtAfoi
wosffsa
warpahtpwpstsm
ltsnscsitop
p(h5ntiotrwprtWittrredgb
s
TP
ANASSSSS
*R
T
B5LFNN
HR
Antepartum testing for stillbirth 303
pproximately half of the 337 patients with a previous his-ory of stillbirth had no other reason for testing (Table 2).cknowledging that perinatal death was too rare an outcome
or meaningful statistical comparisons, the authors focusedn antenatal test results, morbidity, and need for interventionn the various subgroups.
During the study interval, there were 396 women whoere excluded from the study cohort due to noncompliancer “inadequate testing.” Three of these women had recurrenttillbirths. All were diabetics who were noncompliant withollow-up testing; two had only one test at 35 to 36 weeksollowed by a gap in testing of more than 2 weeks. One had atillborn infant with multiple anomalies delivered 7 days aftern “unsatisfactory test,” owing to massive obesity.
No recurrent stillbirths occurred in the group of patientsho were properly tested. Nineteen of the 337 patients withprevious stillbirth had positive contraction stress test (CST)
esults (5.6%), which was nearly double the rate seen inatients without previous stillbirth (Table 3). However, theverage number of fetal heart rate tests per patient with aistory of stillbirth was 5.0 compared with 2.5 tests per pa-ient for the total population tested. The increased risk ofositive CST results among women with stillbirth historiesas attributable to pregnancies with past stillbirth and hy-ertension and past stillbirth plus intrauterine growth re-triction as the indications for testing (incidence of positiveests 12 and 17%, respectively). Among the patients with pasttillbirth as the only indication for testing (ie, no maternaledical problems, or intrauterine growth restriction), the
able 3 Antenatal Fetal Testing Indications and Incidence ofositive Contraction Stress Test Results
No. Tested No. � CST %
ll tested patients 7052 208 3.0o previous hx SB 6744 194 2.9ll previous SB 337 19 5.6*B � HTN 83 10 12.0*B � diabetes 71 4 5.6B � IUGR 29 5 17.2*B � postdates 21 0 —B only indication 163 6 3.7
P < 0.05 when compared to patients without previous stillbirth.eprinted with permission.8
able 4 Perinatal Outcome for Patients with and Without a P
Hx SB
(n � 337)
Outcome No. %
W <10th centile 17 5.0min Apgar <7 13 3.9
ate decels in labor 29 8.6etal death 0 —eonatal death 1 0.3eonatal RDS 13 3.9
x � history; SB � stillbirth; BW � birth weight.
eprinted with permission.8ikelihood of positive CST was not significantly higher thanhose who had indications for testing, but without a previoustillbirth history (3.7% versus 2.9%). In this study, there waso evaluation of outcomes according to the presence or ab-ence of positive tests results. Therefore, while the studylearly shows that mothers who have experienced a previoustillbirth and who have medical or obstetrical complicationsn future pregnancies are at greater risk for positive contrac-ion stress test results, there is no way to determine if theutcomes in the patients with positive CST results wereoorer.Freeman and coworkers did make perinatal outcome com-
arisons in patients with and without histories of stillbirthTable 4). Patients with a history of stillbirth did not haveigher incidences of intrauterine growth restriction, low-minutes Apgar scores, late decelerations in labor, or peri-atal deaths than the population of patients whose indica-ions for testing did not include stillbirth. However, a signif-cantly higher incidence of respiratory distress syndrome didccur in patients with a history of stillbirth than in all otherested patients (3.9% versus 1.7%; P � 0.05). The authorseported that the increase in respiratory distress syndromeas probably due to a greater number of induced labors andrimary cesareans (without labor) in women who had histo-ies of stillbirth plus hypertensive disorders, diabetes, or in-rauterine growth restriction as their indications for testing.
hen induction of labor or cesarean section was undertakenn women with a stillbirth history and hypertension, diabe-es, or intrauterine growth restriction, approximately half ofhe interventions were for abnormal fetal heart rate testingesults and half were for maternal indications. While respi-atory distress syndrome was increased in neonates deliv-red by mothers with a history of stillbirth, the neonataleath (0.3%) rate was not significantly different than theroup of tested pregnancies without a past history of still-irth (Table 4).The important findings of Freeman and coworkers can be
ummarized as follows:
1. A history of previous stillbirth is associated with agreater number of tests per patient than is seen in otherpatients with high-risk conditions. However, 44% ofpatients without stillbirth had postdates as an indica-tion for testing, which would significantly limit the
s Stillbirth
No Hx SB
(n � 6744)
No. % P
368 5.5 NS178 2.6 NS664 9.8 NS25 0.4 NS52 0.8 NS
112 1.7 < 0.05
reviou

3asic
faosot1tbwnrtbisp
tWwdtteg
rlgmrcnpweshsn
3
T
EBETADCI
SR
304 J.W. Weeks
number of CSTs that would have been done in thatgroup.
2. Patients who have a history of previous stillbirth and achronic maternal condition or intrauterine growth re-striction are at greater risk for having positive contrac-tion stress test results than patients whose indicationsfor testing did not include stillbirth.
3. When a past history of stillbirth was the only indicationfor testing, there was no increased risk of positive con-traction stress test results even though the stillbirthonly group probably had more tests per patient thanthe general antepartum surveillance population. How-ever, patients were high risk (eg, hypertension, diabe-tes, postdates). Without a group of low-risk controls,we cannot conclude that patients with a prior stillbirthas their only risk factor do not deserve monitoring.
4. Antenatal testing has the potential to increase the risk ofpremature delivery. Mothers with medical or obstetri-cal problems and past stillbirths were more likely tohave labor inductions and cesarean sections and theirneonates were more likely to have respiratory distresssyndrome. Presumably, some of these interventionswere the result of false-positive contraction stress testresults.
5. Antenatal testing is likely to reduce recurrent stillbirth.Extrapolating from the perinatal collaborative data ofthe mid-twentieth century, in which perinatal mortalityin pregnancies following at stillbirth was 7.3%, thereshould have been 25 perinatal deaths among the 337women with prior stillbirths. Considering that therewas only one neonatal death and no stillbirths in the337 women who were compliant, antenatal fetal testingprobably confers some protection against recurrentstillbirth. The degree to which the low perinatal mor-tality can be directly attributable to fetal testing as op-posed to advances in medical care in the 25 years afterthe perinatal collaborative studies cannot be quantified.
In 1991, Weeks and coworkers reported on a cohort of00 women whose sole indication for antepartum testing waspast history of stillbirth.9 Whereas Freeman and coworkers
ought to determine if a past history of stillbirth remained anmportant risk factor in the modern obstetrics era, Weeks andoworkers sought to determine if the timing of fetal testing in
able 5 Pregnancy Outcome by Gestational Age of Previous
SB < 32 Weeks (n �
GA delivery 38.9 (2.0)irth weight 3270 (560)GA first test 32.1 (4.0)otal tests 13.9 (10.7)bnormal tests 61.70%elivery for abnormal test 20%/S for fetal indications 3.50%
UGR 5.20%
D � parenthesis; IUGR � intrauterine growth restriction; C/S � c
eprinted with permission.9uture pregnancies is important and whether the gestationalge of the previous stillbirth influenced future pregnancyutcomes. As with the Freeman study, the rarity of recurrenttillbirth meant that outcome data were limited to measuresf morbidity. The study group comprised patients seen atwo institutions in southern California between 1979 and991. For all but the final 2 years, weekly contraction stressesting was used. In the final 2 years, semiweekly modifiediophysical profiles (nonstress test plus amniotic fluid index)ere used. CST or biophysical profiles were performed aseeded to follow-up abnormal modified biophysical profileesults. The study goal was to determine when to initiateesting in such women since a variety of approaches wereeing employed by the referring obstetricians (eg, begin test-
ng 2 to 4 weeks before the gestational age of the previoustillbirth, at 32 weeks for all patients, at 36 weeks for allatients).To assess the relationship between the gestational age of
he previous stillbirth and subsequent pregnancy outcome,eeks and coworkers compared groups who had early (�32eeks) versus late (�36 weeks) stillbirths in the past. Pre-ictably, the early stillbirth group had significantly more fetalests per patient. They also had significantly more abnormalest results; however, interventions for abnormal tests andvidence of fetal compromise did not differ between theroups (Table 5).
There was one recurrent stillbirth and no neonatal deathseported. The one stillbirth occurred in a women who had noive births and two previous stillbirths at 37 to 38 weeksestation. The autopsy results for these stillbirths was nor-al. The mother’s screening for hypertension, diabetes, thy-
oid disease, sexually transmitted disease, and collagen vas-ular disease was negative. Parental karyotypes were alsoormal. Three days after having a normal CST, that patientresented with a complaint of decreased fetal movement. Sheas released after having a reactive nonstress test; no decel-
rations were noted. Despite this, she returned 16 hours latertating that she was totally devoid of fetal movements for 5ours. Intrauterine death was confirmed and the 35-weektillborn proved to be appropriately grown and structurallyormal.Fifty-three of the 300 study patients delivered at less than
8 weeks (18%). In half of those instances the deliveries
rth
) SB > 36 Weeks (n � 148) P
39.1 (2.0) NS3421 (567) 0.0334.2 (3.0) <0.01
8.7 (5.2) <0.0141.90% <0.0120.90% NS6.80% NS2.70% NS
n section; EGA � estimated gestational age; SB � stillbirth.
Stillbi
115
esarea

fdecsfi
ap�AuatO3csm3tc
hrd
w
CDAswpUGlpittstm
oiaft
F
T
PESEAPO
*R
Antepartum testing for stillbirth 305
ollowed spontaneous labor. Approximately one-quarter ofeliveries at less than 38 weeks were due to abnormal orquivocal fetal testing results (Table 6). Figure 1 shows theumulative percentage of patients with positive fetal test re-ults and the cumulative percentage of all women deliveredor positive test results (defined as positive CST or biophys-cal profile (BPP) score of 4/10 or less).
Of the 300 patients tested, 19 had one or more positiventenatal test results (6.4%). There were six patients withositive test results at �36 weeks, three with positive tests at32 weeks, and three with positive tests at 32 to 35 weeks.ll three of the patients with positive results at �32 weeksltimately delivered at term; none of those pregnancies hadbnormal fetal heart rate tracings, intrauterine growth restric-ion, cesarean for fetal distress, or low 5-minute Apgar scores.f the three patients who were delivered for positive tests at2 to 35 weeks, only one had unequivocal evidence of fetalompromise (decreased fetal movement, BPP 2/10, cesareanection for abnormal fetal heart rate tracing). The two re-aining patients were induced for abnormal tests at 32 and
5 weeks gestation. They were appropriately grown, prema-ure neonates without apparent intrapartum or neonatalompromise.
Thirteen of the 19 patients with positive fetal test resultsad their positive results at �36 weeks. The authors did noteport the proportion of that group with unequivocal evi-ence of uteroplacental or fetal compromise.The important findings from the study of Weeks and co-
orkers can be summarized as follows:
1. When otherwise healthy women with histories of pre-vious stillbirth are followed with antepartum fetal test-ing, the stillbirth recurrence risk is low (1 in 300). Thisstillbirth rate of 3.3 per 1000 is well below the nationalrate of 7 to 9 per 1000, suggesting that fetal testing canavert recurrent stillbirths.
2. It is not clear that an earlier gestational age at the time ofthe previous stillbirth correlates with increased risk infuture pregnancies when the mothers do not havechronic medical conditions or concomitant obstetricalproblems. However, clinicians test earlier in patientswhose previous stillbirths occurred early in gestation.
able 6 Delivery Indications by Gestational Age
Gestational Age at Delivery
Reason forDelivery
<38 Weeks(n � 53)
>38 Weeks(n � 247)
ositive CST 4 (7.5%) 10 (4.05%)quivocal fetal test 8 (15.1%) 19 (7.69%)pontaneous labor 27 (50.9%) 156 (63.2%)lective induction 0 58 (23.5%)bruption 3 (5.7%) 1 (0.40%)IH 4 (7.5%) 3 (0.12%)ther* 7 (13.2%) 0
Placenta previa, anxiety, classical scar.eprinted with permission.8
This practice is associated with an increase in total tests d
and in the likelihood of having a positive result (at leastwhen CST is the predominant testing method).
3. In most instances, otherwise healthy women with ahistory of stillbirth should have fetal testing initiatedbeyond 32 weeks gestation. This study provides un-equivocal evidence of an averted stillbirth in one of sixpatients with positive CST results at �36 weeks. How-ever, there is also the potential for positive tests resultswhich could result in increased risk of neonatal mor-bidity owing to prematurity. In this particular study,careful follow-up testing and sound clinical judgmentappears to have minimized this risk. However, it is notclear that this can be widely reproduced.
4. Given that the recurrent stillbirth occurred within 3days of normal CST results in a patient who was com-pliant, it is apparent that antepartum fetal surveillancecannot prevent all stillbirth recurrences, even in other-wise healthy mothers.
linician, Whereo We Go from Here?
s discussed elsewhere in this issue of the journal, a circum-pect approach to the evaluation of stillbirth is paramount ife are to identify and understand a patient’s particularathophysiology and reduce the incidence of stillbirth in thenited States. The American College of Obstetricians andynecologists has recently published a document that out-
ines the essential components of the maternal, fetal, andlacental evaluation and the approach to counseling the fam-
ly.10 Especially important is the clinician’s understanding ofhe value of perinatal autopsy and her ability to communicatehis to the bereaved family. It is often helpful to delay discus-ions of autopsy until the day after delivery and to emphasizehat the evaluation can be done in ways that will allowourners to view the baby at memorial ceremonies.There is compelling evidence that even in the modern
bstetrical era, a history of previous stillbirth portends anncreased risk in future pregnancies. Although the data onntepartum testing of patients with stillbirth as their only riskactor are limited, we can be reasonably confident that fetalesting confers some protection. CST is no longer used as a
igure 1 Cumulative percentage of abnormal fetal test results and
elivery for abnormal fetal testing with advancing gestational age.
psmppmta
IDAbrtpFbwWbph
tbsmmwdttfl
tbmd
R
1
1
1
1
1
1
306 J.W. Weeks
rimary surveillance technique. As long as the fetal testingcheme includes weekly evaluation of acute and chronicarkers of fetal well-being, as with a modified BPP or bio-hysical profiles, outcomes should be similar to those re-orted by Freeman and Weeks. In the absence of chronicedical conditions or concomitant obstetrical complica-
ions, healthy mothers with past stillbirths should start theirntepartum testing at 32 to 36 weeks gestation.
nvestigator, Whereo We Go from Here?
ntepartum surveillance for patients with a previous still-irth is a longstanding standard of care. Hence, a prospectiveandomized trial of testing versus no testing is very unlikelyo be done. Modified BPP and BPP have completely sup-lanted CST. Perhaps retrospective studies similar to those ofreeman and Weeks should be repeated. However, against aackground stillbirth rate of �1%, over 3000 study patientsould be needed to evaluate the risk of recurrent stillbirth.ithout a very large multicenter study which includes data-
ases to track confounding variables, fetal test results, andregnancy outcomes, such a large retrospective study ofealthy women with a history of stillbirth is not feasible.Perhaps the most interesting and feasible area for study is
he utility of fetal movement for assessment of fetal well-eing. The study by Weeks and coworkers suggests that, inome cases, a mother’s perception of decreased fetal move-ent may be more sensitive than fetal testing. After imple-enting universal fetal movement assessment in a group ofomen in San Diego, Moore and Piacquadio11 noted a re-uced stillbirth rate when compared with historical con-rols. More recently, J. Frederick Froen has championedhe concept of assessing changes in maternal perception ofetal movement as opposed to relying on a specified “alarm
imit.”12,13 Approximately half of all stillbirths occur at lesshan 28 weeks gestation.14,15 Whether these early still-irths can be averted with fetal movement assessment orodified antepartum surveillance programs is yet to beetermined.
eferences1. Eller A, Brancy D, Byrne L: Stillbirth at term. Obstetr Gynecol 108(2):
442-447, 20062. Antepartum Fetal Surveillance. ACOG Practice Bulletin #9. American
College of Obstetricians and Gynecologists, 19993. Niswander K, Gordon M: Collaborative Perinatal Study of the National
Institute of Neurologic Disease and Stroke: the women and their preg-nancies. DHEW publication no. (NIH) 73-379, 1972
4. Butler N, Bonham D. Perinatal mortality: the first report of the BritishPerinatal Mortality Survey. Edinburgh, E&S Livingston Ltd., 1963
5. Sharma P, Salihu H, Kirby R: Stillbirth recurrence in a population ofrelatively low-risk mothers. Pediatr Perinat Epidemiol 21(Suppl 1):24-30, 2007
6. Sharma P, Salihu H, Oyelese Y, et al: Is race a determinant of stillbirthrecurrence? Obstetr Gynecol 107(2):391-397, 2006
7. Samueloff A, Xenakis E, Berkus M, et al: Recurrent stillbirth: Signifi-cance and characteristics. J Reprod Med 38(11):883-886, 1993
8. Freeman R, Dorchester W, Anderson G, et al: The significance of pre-vious stillbirth. Am J Obstetr Gynecol 151:7-13, 1985
9. Weeks J, Asrat T, Morsan MA, et al: Antepartum surveillance for ahistory of stillbirth: when to begin? Am J Obstetr Gynecol 172(2):486-492, 1995
0. American College of Obstetricians and Gynecologists (ACOG): Evalu-ation of Stillbirth and Neonatal Deaths. ACOG Committee Opinion No.383. Obstetr Gynecol 110:963-966, 2007
1. Moore T, Piacquadio K: A prospective evaluation of fetal movementscreening to reduce the incidence of antepartum fetal death. Am JObstetr Gynecol 160(5):1075-1080, 1989
2. Caroline C: Federal Update: Research Gaps Identified by AntenatalTesting Workshop. Obstetr Gynecol 110(6):1420-1421,
3. Froen J: A kick from within—fetal movement counting and the can-celled progress in antenatal care. J Perinat Med 32(1):13-24, 2004
4. Froen J, Arnestad M, Frey K, et al: Risk factors for sudden intrauterineunexplained death: epidemiologic characteristics of singleton cases inOslo, Norway, 1986-1995. Am J Obstetr Gynecol 184(4):694-702,2001
5. MacDorman M, Hoyert D, Martin J, et al: Fetal and perinatal mortality,
United States, 2003. Natl Vital Statist Rep 55(6):1-17, 2007
MJEBV
AD
Aar
*
†
‡
§�
¶
#
T
A
0d
anagement of Decreased Fetal Movements. Frederik Frøen, MD, PhD,*,† Julie Victoria Holm Tveit, MD,‡
li Saastad, RN, RM, MSc,*,§ Per E. Børdahl, MD, PhD,�
abill Stray-Pedersen, MD, PhD,‡ Alexander E.P. Heazell, MBChB(hons),¶
icki Flenady, RN, RM, MMedSc,# and Ruth C. Fretts, MD, MPH†
Maternal perception of decreased fetal activity is a common complaint, and one of the mostfrequent causes of unplanned visits in pregnancy. No proposed definitions of decreasedfetal movements have ever been proven to be superior to a subjective maternal perceptionin terms of identifying a population at risk. Women presenting with decreased fetalmovements do have higher risk of stillbirth, fetal growth restriction, fetal distress, pretermbirth, and other associated outcomes. Yet, little research has been conducted to identifyoptimal management, and no randomized controlled trials have been performed. The strongassociations with adverse outcome suggest that adequate management should include theexclusion of both acute and chronic conditions associated with decreased fetal move-ments. We propose guidelines for management of decreased fetal movements that includeboth a nonstress test and an ultrasound scan and report findings in 3014 cases ofdecreased fetal movements.Semin Perinatol 32:307-311 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS decreased fetal movements, guidelines, management, stillbirth, fetal growth re-striction, fetal distress
(omals
pwgmclm
teigs
ta
dverse Outcomes inecreased Fetal Movements
lmost all pregnant women perceive fetal movements andintuitively view their experience of normal fetal activity
s a sign of fetal well-being, engaging in self-screening byeporting their concerns for decreased fetal movements
Division of Epidemiology, Norwegian Institute of Public Health, Oslo,Norway.
Brigham and Women’s Hospital, Div. of Maternal-Fetal Medicine, HarvardMedical School, Boston, MA.
Dept. of Obstetrics and Gynecology, and Center for Perinatal Research,Rikshospitalet, University of Oslo, Oslo, Norway.
Akershus University College, Lillestrøm, Norway.Dept. of Clinical Medicine, Section for Obstetrics and Gynecology, Univer-
sity of Bergen, Bergen, Norway.Maternal and Fetal Health Research Group, University of Manchester,
Manchester, UK.Centre for Clinical Studies, Mater Mothers’ Hospital, School of Medicine,
University of Queensland, Brisbane, Australia.his work was supported in part by The Norwegian Research Council, The
Norwegian Women’s Public Health Association, The Norwegian MedicalAssociation, and Unexpected Child Death Society of Norway.
ddress reprint requests to J. Frederik Frøen, MD, PhD, Norwegian Instituteof Public Health, P.O. Box 4404 Nydalen, N-0403 Oslo, Norway. E-mail:
146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2008.04.015
DFM). In a Western society such as Norway, as many as 51%f women report that they were concerned for DFM once orore in pregnancy.1 Not all these concerns are brought to the
ttention of health care professionals, but in different popu-ations, between 4 and 15% will contact care providers withuch concerns in the third trimester.2
Contemporary guidelines for the management of uncom-licated pregnancies provide little guidance for pregnantomen and their care providers on DFM. While existinguidelines acknowledge the importance of DFM by recom-ending that women should be informed about the need to
ontact health care professionals when they perceive DFM,ittle, if any, provide further guidance in how to define or
anage DFM.3-5
DFM has a well-established role as an adaptive response tohe various stages of placental insufficiency and hypoxia. Inarly stages, DFM may represent compensatory adaptationsn line with the redistribution of blood flow to essential or-ans as the brain, heart, and adrenals, and in later stages, aign of decompensation warning imminent injury and death.
Details of this pathophysiology are beyond the scope ofhis review, but in terms of management, it is important tocknowledge the significant association between DFM and
etal growth restriction (FGR) across difference definitions of307

bt
Flbmmnscdb
DoDcfde
EPDAovlwat
twettnsDhp
tt
fasflbecfpic
ilcisornppcDfA
tCntiviefwefa
T
NUD
N
308 J.F. Frøen et al
oth DFM and FGR.6-16 A dose dependency is also seen be-ween hypoxia/acidemia and DFM in FGR.17-22
In accordance with the association between DFM andGR, studies have reported associations between DFM and
ow birth weight,15,23 oligohydramnios,24-26 pretermirth,13-15,23,27 threatening preterm labor,15,23 congenitalalformations and chromosomal abnormalities,15,23,28 feto-aternal transfusion,29 perinatal brain injuries and disturbedeurodevelopment,30,31 intrauterine infections,32 low Apgarcores and acidemia,19,33 hypoglycemia,15,23 umbilical cordomplications and placental insufficiencies,13,15,23 emergencyeliveries, inductions of labor and cesarean sections, still-irths, and neonatal deaths.10,14,27,33,34
The incidence of adverse outcomes in pregnancies withFM is significant. In a population-based prospective cohortf 38,728 pregnancies in Norway, 2348 cases presented withFM and in a quarter of these a suboptimal pregnancy out-ome was recorded. These adverse outcomes included theollowing: FGR, preterm birth, severe neonatal depression,eath or immediate admission for observation, induction, ormergency delivery.14,27
valuations inregnancies withecreased Fetal Movements
s we discuss elsewhere in this issue of Seminars in Perinatol-gy, there is no widely accepted definition of DFM, as naturalariation restricts the value of any rigid limits. Most pub-ished data on DFM in total populations have been based onomen’s own perception of “decreased” and in practice man-
gement is likewise largely based on that subjective defini-ion.
There are no randomized controlled trials on any aspect ofhe initial evaluation or further management of pregnanciesith decreased fetal movements. As a result of this lack of
vidence, management varies significantly between popula-ions, institutions, and practitioners within single institu-ions.6,9,13,16,26,27,35-37 These approaches to DFM range from aonstress test (NST) or cardiotocography (CTG) as solecreening tool,27 to the hospitalization of all women withFM for clinical examination, NST/CTG every 8 hours for 48ours, ultrasound examination including a structured bio-hysical profile, umbilical artery Doppler, Kleihauer–Betke’s
able 1 The Use and Perceived Usefulness of Tests in Pregn
Test Usage
Perceived as Usefulin Detecting
Abnormalities inTotal
PerceWhe
W
ST/CTG 97.5% 3.2%ltrasound 94.0% 11.6%oppler 47.3% 1.9%
ote. The obstetrician managing the patient has scored whether abit. “Only finding” denotes the frequency of a useful test when the
were recommended initial evaluations, while Doppler was used selectiest, maternal hemoglobin, amnioscopy if �37 weeks of ges-ation, and repeated ante partum testing after discharge.13
The tools used for assessment reflect efforts to detect acuteetal distress, subacute and chronic placental insufficiency,nd other specific pathologies associated with DFM. Whileome authors present observational estimates of true andalse-positive and -negative tests, these estimates may haveittle value. In obstetrics, a positive test may indeed be false,ut the lack of adverse outcome after a positive test is notquivalent to a false-positive test. The suspicion of futureomplications will lead to iatrogenic delivery, and the “per-ect” ante partum tests would therefore have 100% false-ositive tests. As an alternative to interpret the value of test-
ng in observational studies, we have chosen the perceivedlinical utility indicated by the individual practitioner.
In a prospective population-based cohort of 46,132 birthsn Norway (consecutive to the one described above), guide-ines including both NST/CTG and ultrasound scanning foronsultations for DFM were implemented. All delivery unitsn eastern Norway and the city of Bergen were included in thetudy over a 17-month period, ending April 1, 2007. As partf a quality improvement project, pregnancies where womeneported DFM were registered prospectively without mater-al consent to avoid recruitment bias. All health care forregnant women is free of charge in Norway; there are norivate delivery units, and the population is accustomed toontacting their delivery unit with any acute concerns forFM. The study was approved by the Regional Committees
or Medical Research Ethics and advised by the Personal Datact of The Norwegian Data Inspectorate.The study included 3014 pregnancies with DFM in which
he mother presented to hospital with her concerns. A NST/TG was performed in 97.5% of cases, and ultrasound scan-ing was performed in 94.0% of cases (Table 1). According tohe guidelines of the study, the ultrasound scanning wasntended for the estimation of fetal weight, amniotic fluidolume, and fetal movements (FM). A standardized biophys-cal profile was not requested, and umbilical artery Dopplerxaminations were not indicated by the subjective concernsor DFM alone. The obstetrician managing the individualoman would indicate, on a preregistered form, whether the
xamination detected abnormalities (fetal growth restriction,etal distress, oligohydramnios, malformations, or other),nd if so, what investigational tool detected the anomaly.
Presenting with Decreased Fetal Movements (n � 3014)
as Usefulormalityound
Only Finding inDetecting
Abnormalitiesin Total
Only FindingWhen Abnormality
Was Found
4% 1.2% 9.9%2% 8.7% 71.3%1% 0.2% 1.7%
lities were detected, and if so, what tool(s) was useful in detectingTG and/or ultrasound was negative. Only NST/CTG and ultrasound
ancies
ivedn Abn
as F
23.86.14.
normaNST/C
vely.

nwtstsai
aj0stccg�spaptiN
pwaosdaordeoful
MDTtppdWacfic
ip
CAwb
NTio
UFAst
AEamocoaaeci
FAarahgg
dHhcpc
tb
FInraF
Management of decreased fetal movements 309
Overall, NST/CTG and ultrasound scanning identified ab-ormalities in 3.2 and 11.6% of cases, respectively. In caseshere both the ultrasound and the NST/CTG was performed,
he ultrasound detected abnormalities in 8.7% of cases de-pite a normal NST/CTG, and conversely the NST/CTG iden-ified abnormalities in 1.2% of cases despite a negative ultra-ound scanning. Among all cases in which one or morebnormality was detected, ultrasound was the sole tool todentify it in 71.3% of cases.
In 47.3% of cases, a Doppler examination was performeds well. Despite the preselection of cases that would be sub-ected to Doppler, Doppler only identified abnormalities in.2% of cases in which both the NST/CTG and the ultra-ound scanning were normal. Of these three pregnancies,wo appeared to be false-positive tests leading to uncompli-ated outcomes more than 7 weeks later and the remainingase was induced for delivery the next day at 33 � 4 weeks ofestation with a severely growth restricted baby (1900 g;2.5 centile), which should have been detected by the ultra-
ound scanning, suggesting either that ultrasound was noterformed according to guidelines or an underreporting ofctual findings. In summary, with normal and adequatelyerformed NST/CTG and ultrasound scanning, umbilical ar-ery Doppler did not provide uniquely valuable informationn any of the 3014 cases of DFM in a “real-life” setting inorwegian public hospitals.While the effectiveness of each individual tool for ante
artum testing in risk pregnancies is discussed in detail else-here in this issue of Seminars in Perinatology, these results
re consistent with the evidence for ante partum testing inther risk pregnancies. The use of NST/CTG as the solecreening tool in risk pregnancies has been largely aban-oned. Although studies are old, the likely benefit effect, ifny, would be a discouragement of such practice.38 The usef Doppler evaluation of flow patterns in umbilical arteries inisk pregnancies may reduce mortality, but there is no evi-ence of benefit when FGR and hypertensive disorders arexcluded.39 Others have also published no additional benefitf Doppler in the evaluation of DFM.6 The use of ultrasoundor the initial assessment of growth and amniotic liquor vol-me in pregnancies at risk of FGR has remained unchal-
enged as the gold standard.
anagement of Women withecreased Fetal Movements
he goal of ante partum fetal surveillance in cases of DFM iso exclude imminent fetal jeopardy40 and to identify thoseregnancies at increased risk of stillbirth and other adverseregnancy outcome and to provide appropriate care to re-uce this risk while avoiding unnecessary interventions.3
hile improved definitions and randomized controlled trialsre needed to identify the optimal management of pregnan-ies with DFM, current knowledge does inform the choicesor a basic initial evaluation of DFM. In our clinical qualitymprovement project in Norway for the management of de-
reased fetal movements, we have seen significant reductions wn admissions, preterm births, and stillbirths.41 We have im-lemented the following consensus-based strategy.
linical Evaluationstandard clinical evaluation should be undertaken for allomen reporting certain DFM, including measurement oflood pressure, to reevaluate her risk profile.
onstress Test/Cardiotocographyhe CTG/NST may provide immediate reassurance, a record-
ng of maternal perception of activity, and often a valuablepportunity for the woman to focus on fetal activity.
ltrasound Measurementsetal Activitys for any other symptom in pregnancy, the actual complainthould be assessed and documented objectively, in particularo exclude absence of FM.
mniotic Fluid Volumesstimates of amniotic fluid volumes have become standard inntenatal testing of risk pregnancies, and in the U.S. “evenedicolegally essential.”42 The traditional understanding of
ligohydramnios as a predictor of perinatal outcome has re-ently been challenged, and the relation between isolatedligohydramnios and adverse outcomes in total populationst term may be weaker than previously assumed.43,44 Still,mniotic fluid has significant impact on fetal health45 andstimations of the amniotic fluid volume or index adds to thelinical information in cases where impaired fetal well-beings suspected.
etal Growths previously discussed, DFM in risk pregnancies is associ-ted with high risk of FGR, with reported odds ratios (OR)anging from 4.4 to 13.3.2 In total populations the OR isbout 3.2 The latter is in the range seen for risk of FGR inypertensive disorders in pregnancy,46,47 in which fetalrowth assessment in a newly identified risk pregnancy forrowth failure is standard.
As evidence for effective interventions is limited, antenataletection of FGR does not decrease the risk of FGR at birth.owever, a Swedish institution-based study demonstratedow perinatal outcomes deteriorated significantly in 573ases where FGR remained undetected in pregnancy, com-ared with 681 cases identified antenatally (OR 4.1, 95%onfidence intervals, 2.5 to 6.8).48
Ultrasound measures may provide valuable documenta-ion in circumstances where growth failure may be presentefore identifiable FGR.
etal Anatomyn populations screened for fetal anomalies in early preg-ancy, undetected anomalies in pregnancies with DFM areare. In previously unscreened pregnancies, DFM representdditional indication for evaluation. If polyhydramnios orGR is found, a more detailed examination of fetal anatomy is
arranted.
TETdacdbrttplse
ofe
sitga
FFtanv
sftufwa
swtdpfimi
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
310 J.F. Frøen et al
iming of the Initialvaluation and Advice to Womenimely exclusion of imminent and serious risk to the fetusepends on the apparent severity (absence or only decreased)nd maternal certainty in perception of DFM. Maternal con-ern due to being in doubt of whether fetal activity has beenecreasing should not automatically dictate a rapid responsey health care professionals, but guidance and observation toesolve these doubts seems reasonable. We have suggestedhat if there is doubt the women should be advised to con-inue observation for up to 12 hours. However, if there isossible absence of FM, observation should not be continued
onger than 2 hours before contacting her care provider andubsequent evaluation. (See discussion of definitions of DFMlsewhere in this issue of Seminars in Perinatology.)
We suggest the same minimum standards in the timelinessf assessment of fetal health on presenting at a health careacility with DFM, within 2 hours if suspected absence, oth-rwise within 12 hours.
When imminent risk to the fetus is excluded, growth as-essment is not an emergency. Completing all examinationsn sequence is convenient for most, but at inconvenientimes, growth assessment may be postponed. We have sug-ested within 12 hours in cases of DFM, and 2 hours in thebsence of detectable fetal movements.
ollow-Up and Deliveryindings at the initial consultation should guide further ac-ion. No studies of follow-up of women reporting DFM inpparently normal pregnancies exist. In view of the highumber of adverse outcomes associated with DFM, increasedigilance is recommended.
We suggest that women with definite absence of FMhould not be discharged undelivered before the cause isound and managed appropriately. Reassurance by antenatalesting is time limited, and persistent DFM should be reeval-ated after the period of reassurance has passed, earlier ifurther decrease or absence of FM is perceived. All womenith DFM who remain undelivered should have adequate
ntenatal care.The advantages and disadvantages of induced delivery ver-
us continued surveillance should be considered for womenith a term otherwise uncomplicated pregnancy with persis-
ent DFM, and certainly in postterm pregnancies where in-uction of labor at 41 completed weeks reduces the risk oferinatal death.49 The rising risk of unexplained stillbirths
rom about 36 weeks of gestation, the diminishing hazard ofnductions at these gestations, and the possibility that active
anagement of risk may be beneficial should be consideredn the decision-making process.50-52
eferences1. Saastad E, Ahlborg T, Froen JF: Maternal awareness towards fetal ac-
tivity associated with SGA. J Midwifery & Women’s Health 2008 (inpress)
2. Frøen JF: A kick from within—fetal movement counting and the can-
celled progress in antenatal care. J Perinat Med 32:13-24, 20043. American Academy of Pediatrics, The American College of Obstetri-cians and Gynecologists. Guidelines for perinatal care. Washington,DC. AAP and ACOG, 2002
4. National Collaborating Centre for Woman’s and Children’s Health:Antenatal Care—Routine Care for the Healthy Pregnant Women (ed 2).London, UK, RCOG Press, 2008
5. Klovning A, Backe B, Eide BI, et al: Sosial- og Helsedirektoratet. Ret-ningslinjer for svangerskapsomsorgen. Oslo, Sosial- og Helsedirektora-tet, 2005
6. Dubiel M, Gudmundsson S, Thuring-Jonsson A, et al: Doppler veloci-metry and nonstress test for predicting outcome of pregnancies withdecreased fetal movements. Am J Perinatol 14:139-144, 1997
7. Ehrstrom C: Fetal movement monitoring in normal and high-risk preg-nancy. Acta Obstetr Gynecol Scand Suppl 80:1-32, 1979
8. Fischer S, Fullerton JT, Trezise L: Fetal movement and fetal outcome ina low-risk population. J Nurse Midwifery 26:24-30, 1981
9. Heazell AE, Sumathi GM, Bhatti NR: What investigation is appropriatefollowing maternal perception of reduced fetal movements? J ObstetGynaecol 25:648-650, 2005
0. Pearson JF, Weaver JB: Fetal activity and fetal wellbeing: an evaluation.BMJ 1:1305-1307, 1976
1. Rayburn WF, McKean HE: Maternal perception of fetal movement andperinatal outcome. Obstet Gynecol 56:161-164, 1980
2. Sadovsky E, Ohel G, Havazeleth H, et al: The definition and the signif-icance of decreased fetal movements. Acta Obstet Gynecol Scand 62(5):409-413, 1983
3. Sergent F, Lefevre A, Verspyck E, et al: [Decreased fetal movements inthe third trimester: what to do?] Gynecol Obstet Fertil 33:861-869,2005
4. Tveit JV, Saastad E, Børdahl PE, et al: The epidemiology of decreasedfetal movements. Proceedings of the Norwegian Perinatal Society Con-ference, November 2006. 2006
5. Valentin L, Marsal K: Pregnancy outcome in women perceiving de-creased fetal movement. Eur J Obstet Gynecol Reprod Biol 24:23-32,1987
6. Whitty JE, Garfinkel DA, Divon MY: Maternal perception of decreasedfetal movement as an indication for ante partum testing in a low-riskpopulation. Am J Obstet Gynecol 165:1084-1088, 1991
7. Bekedam DJ, Visser GH: Effects of hypoxemic events on breathing,body movements, and heart rate variation: a study in growth-retardedhuman fetuses. Am J Obstet Gynecol 153:52-56, 1985
8. Gagnon R, Hunse C, Fellows F, et al: Fetal heart rate and activitypatterns in growth-retarded fetuses: changes after vibratory acousticstimulation. Am J Obstet Gynecol 158:265-271, 1988
9. Ribbert LS, Nicolaides KH, Visser GH: Prediction of fetal acidaemia inintrauterine growth retardation: comparison of quantified fetal activitywith biophysical profile score. Br J Obstet Gynaecol 100:653-656,1993
0. Sival DA, Visser GH, Prechtl HF: The effect of intrauterine growthretardation on the quality of general movements in the human fetus.Early Hum Dev 28:119-132, 1992
1. Vindla S, James DK, Sahota DS, et al: Computerised analysis of behav-iour in normal and growth-retarded fetuses. Eur J Obstet GynecolReprod Biol 75:169-175, 1997
2. Vindla S, James D, Sahota D: Computerised analysis of unstimulatedand stimulated behaviour in fetuses with intrauterine growth restric-tion. Eur J Obstet Gynecol Reprod Biol 83:37-45, 1999
3. Valentin L: Fetal movements in late pregnancy. Detection of fetal jeop-ardy by objective recording and by maternal counting. Lund, Sweden,University of Lund, 1986
4. Sherer DM, Spong CY, Minior VK, et al: Decreased amniotic fluidvolume at �32 weeks of gestation is associated with decreased fetalmovements. Am J Perinatol 13:479-482, 1996
5. Sival DA, Visser GH, Prechtl HF: Does reduction of amniotic fluid affectfetal movements? Early Hum Dev 23:233-246, 1990
6. Ahn MO, Phelan JP, Smith CV, et al: Ante partum fetal surveillance inthe patient with decreased fetal movement. Am J Obstet Gynecol 157:
860-864, 1987
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
Management of decreased fetal movements 311
7. Frøen JF, Saastad E, Tveit JV, et al: [Clinical practice variation in re-duced fetal movements]. Tidsskr Nor Laegeforen 125:2631-2634,2005
8. Lin CC, Adamczyk CJ, Sheikh Z, et al: Fetal congenital malformations.Biophysical profile evaluation. J Reprod Med 43:521-527, 1998
9. Giacoia GP. Severe fetomaternal hemorrhage: a review. Obstet GynecolSurv 52:372-380, 1997
0. Naeye RL, Lin HM: Determination of the timing of fetal brain dam-age from hypoxemia-ischemia. Am J Obstet Gynecol 184:217-224,2001
1. James DK, Telfer FM, Keating NA, et al: Reduced fetal movements andmaternal medication—new pregnancy risk factors for neurodevelop-mental disability in childhood. J Obstet Gynaecol 20:226-234, 2000
2. Goldstein I, Romero R, Merrill S, et al: Fetal body and breathing move-ments as predictors of intraamniotic infection in preterm prematurerupture of membranes. Am J Obstet Gynecol 159:363-368, 1988
3. Yogev Y, Ben-Haroush A, Horowitz ER, et al: PGE2 induction of laborfor consistent decreased perception of fetal movements at term. Int JGynaecol Obstet 82:173-178, 2003
4. Sadovsky E, Yaffe H: Daily fetal movement recording and fetal progno-sis. Obstet Gynecol 41:845-850, 1973
5. Korszun P, Dubiel M, Kudla M, et al: Doppler velocimetry for predict-ing outcome of pregnancies with decreased fetal movements. Acta Ob-stet Gynecol Scand 81:926-930, 2002
6. Olesen AG, Svare JA: Decreased fetal movements: background, assess-ment, and clinical management. Acta Obstet Gynecol Scand 83:818-826, 2004
7. Heazell AE, Green M, Wright C, et al: Midwives’ and Obstetricians’knowledge and management of women presenting with decreased fetalmovements. Acta Obstet Gynecol Scand 87:331-339, 2008
8. Pattison N, McCowan L: Cardiotocography for ante partum fetal assess-ment. Cochrane Database Syst Rev CD001068, 2000
9. Neilson JP, Alfirevic Z: Doppler ultrasound for fetal assessment in highrisk pregnancies. Cochrane Database Syst Rev CD000073, 1996
0. ACOG practice bulletin. Ante partum fetal surveillance. Number 9,
October 1999 (replaces Technical Bulletin Number 188, January1994). Clinical management guidelines for obstetrician-gynecologists.Int J Gynaecol Obstet 68:175-185, 2000
1. Frøen JF, Tveit JVH, Saastad E, et al: Stillbirths and decreased fetalmovements: prevention by improved information and management.Proceedings of the International Stillbirth Alliance Conference 2007,Birmingham, UK. 2007
2. Moore TR: Sonographic screening for oligohydramnios: does it de-crease or increase morbidity? Obstet Gynecol 104:3-4, 2004
3. Ott WJ: Reevaluation of the relationship between amniotic fluid vol-ume and perinatal outcome. Am J Obstet Gynecol 192:1803-1809,2005
4. Sherer DM, Langer O: Oligohydramnios: use and misuse in clinicalmanagement. Ultrasound Obstet Gynecol 18:411-419, 2001
5. Underwood MA, Gilbert WM, Sherman MP: Amniotic fluid: not justfetal urine anymore. J Perinatol 25:341-348, 2005
6. Odegard RA, Vatten LJ, Nilsen ST, et al: Preeclampsia and fetal growth.Obstet Gynecol 96:950-955, 2000
7. Xiao R, Sorensen TK, Williams MA, et al: Influence of pre-eclampsia onfetal growth. J Matern Fetal Neonatal Med 13:157-162, 2003
8. Lindqvist PG, Molin J: Does antenatal identification of small-for-gesta-tional age fetuses significantly improve their outcome? Ultrasound Ob-stet Gynecol 25:258-264, 2005
9. Gulmezoglu AM, Crowther CA, Middleton P: Induction of labour forimproving birth outcomes for women at or beyond term. CochraneDatabase Syst Rev CD004945, 2006
0. Frøen JF, Arnestad M, Frey K, et al: Risk factors for sudden intrauterineunexplained death: epidemiologic characteristics of singleton cases inOslo. Norway, 1986-1995. Am J Obstet Gynecol 184:694-702, 2001
1. Fretts RC, Elkin EB, Myers ER, et al: Should older women have antepartum testing to prevent unexplained stillbirth? Obstet Gynecol 104:56-64, 2004
2. Nicholson JM, Kellar LC, Cronholm PF, et al: Active management ofrisk in pregnancy at term in an urban population: an association be-tween a higher induction of labor rate and a lower cesarean delivery
rate. Am J Obstet Gynecol 191:1516-1528, 2004
NMTR
IA
ADbsocsdvcrttScolo
*
†A
3
ew Indications for Antepartum Testing:aking the Case for Antepartum Surveillance or
imed Delivery for Women of Advanced Maternal Ageuth C. Fretts, MD, MPH,* and Ugonna A. Duru, MD†
Maternal age is an independent risk factor for stillbirth; a moderate number of these occurin normally formed babies near term. For a woman 40 years of age or older giving birth, herrisk of having a chromosomal anomaly is 1/66. What is not appreciated is that even withoutmedical risk factors, her risk of having a stillbirth after 37 weeks of gestation is 1/116. Thisarticle reviews the risks and benefits of the strategy of antepartum testing and timeddelivery and discusses the limitations of the available data in this field.Semin Perinatol 32:312-317 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS advanced maternal age, late stillbirth, antepartum testing, active management ofrisk
fw“tb
LCfTpndtaoaah23Dpasst
ndications forntepartum Testing
ntepartum testing cannot directly reduce the risk of still-birth, but it can inform as to when to deliver the patient.
elivering the fetus incurs both maternal and fetal risks andenefits. The goal is to minimize perinatal mortality (ie, theum of stillbirths and neonatal deaths) and include a measuref maternal morbidity, mortality, and patient preference. Theurrent management of the most common risk conditionsuch as diabetes mellitus requiring insulin, the hypertensiveisorders, and intrauterine growth restriction already includearious schedules for antepartum testing. This proactive,omprehensive approach has led to the reduction of stillbirthisk, albeit at the cost of an increased risk of iatrogenic pre-erm birth. The role of antepartum testing in women withhese conditions is summarized elsewhere in this edition ofeminars in Perinatology. In less prevalent diseases that mayontribute to fetal loss, such as systemic lupus erythematosis,r in patients with a history of a previous stillbirth, there isittle doubt that the clinician will include multiple modalitiesf antepartum testing to assess the ongoing health of the
Harvard Vanguard Medical Associates, Brigham and Women’s Hospital andNewton Wellesley Hospital, Wellesley, MA.
Brigham and Women’s Hospital, Boston, MA.ddress reprint requests to Ruth C. Fretts, MD, MPH, Assistant Professor,
Harvard Medical School, Harvard Vanguard Medical Associates,Brigham and Women’s Hospital and Newton Wellesley Hospital, 230
oWorchester St., Wellesley, MA 02481. E-mail: [email protected]
12 0146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1053/j.semperi.2008.04.016
etus. Many questions remain however. For example, shoulde treat women with common risk factors for stillbirth as a
high-risk pregnancy” and initiate antepartum testing and orimed delivery and, if so, what are the potential risks andenefits of this approach?
ate Stillbirths andandidate Risk Factors
or Antepartum Screeninghe best opportunity for stillbirth reduction is to identifyatients who have an increased risk of stillbirth, late in preg-ancy, where the downside of antepartum testing and earlyelivery, if warranted, can be minimized. Candidate risk fac-ors include obesity, socio-economical or racial risk factors,nd advanced maternal age. Obesity has many detrimentalbstetrical and maternal consequences. In a recent meta-nalysis of prepregnancy maternal obesity and stillbirth, Chund colleagues estimated the risk of stillbirth to be 1.4-foldigher in overweight women (ie, a body mass index (BMI)5-29.9 kg/m2), and 2.1 times higher in women with a BMI of0 or over, when compared women with a BMI of �25.1 In aanish population, the risk of stillbirth associated withrepregnancy obesity appeared to increase late in pregnancy,nd this additional risk could not be attributed to hyperten-ion or diabetes.2 Indeed, Salihu and coworkers found obe-ity associated with many social, medical, and obstetric fac-ors, which placed women at increased risk for adverse
utcomes. In their study of Missouri births from 1978 to
1oifwawhcwdtepa
rbiUciadU1dwtbdir
w4trae28Cwo
ooidrcoavfr1
tr
hctf3s1rawwsbwgwcitcp1Opsuw
2tf18hrscowfiugsyyogotniwwh
New indications for antepartum testing 313
997, they found that women with a prepregnancy BMI of 30r greater conferred a 1.4-fold risk of stillbirth.3 This increasen risk appears to be dose dependent, and black womenaired worse in all weight categories when compared withhites. Black women who were extremely overweight (defined
s a BMI of 40 or greater) had a 2.7-fold risk above that of normaleight white women, while similarly overweight white womenad a 1.8-fold risk of stillbirth. Unfortunately, however, becauseause and timing of the stillbirths associated with obesity is notell known in the American population, there are insufficientata at this time to make a recommendation for routine antepar-um testing based on maternal weight alone. For now, the strat-gies necessary to manage these patients and minimize adverseerinatal outcomes need to be individualized, based on obesitynd other comorbid conditions.
In the United States, perinatal statistics are stratified byace. Obvious differences in neonatal and stillbirth rates maye due to many factors including access to obstetrical care, qual-
ty of care, stress, diet, and biological factors. Black women in theS, for example, experience a two-fold risk of stillbirth whenompared with whites with a higher rate of stillbirth both earlyn gestation and late in gestation.4 There are no trials specificallyddressing the potential role of antepartum testing and timedelivery in black women, although Yuan and colleagues usingS data compared induction and stillbirth rates in 1997 versus991.4 Comparing the two time periods, they noted a 20%ecrease in the number of stillbirths after 40 weeks of gestation,hich was largely attributed to an increase in the rate of induc-
ions after 41 weeks. These authors did note however thatlack women were less likely that white women to be in-uced before 43 weeks.4 This is one area in which earlier
ntervention could ameliorate the disproportionate stillbirthate that is experienced by black women late in pregnancy.
Currently in the United States, approximately 15% ofomen giving birth are 35 years of age or older, and 2.5% are0 years of age or older. Indeed, the birth rate to women 35o 39 years of age has increased every year since 1978 and hasisen 43% since 1990. The rate of women giving birth whore 40 years of age or older has also continued to rise. Forxample, based on the final birth statistics from 2003 and004, the rate for women 40 years of age or older rose from.7 births per 1000 women to 8.9 per 1000. Interestingly, theenters for Disease Control now reports birth rates foromen aged 45 to 49 and 50 to 54, but these births representnly a small fraction of total births (0.15%).5
Many patients and practitioners alike have the belief that iflder women are without medical problems such as diabetesr hypertension, the additional risk of conferred by advanc-ng age is probably relatively low for adverse outcomes. In-eed small studies directed at this issue have been generallyeassuring.6 However, a large Canadian study by Fretts andoworkers, after controlling for many factors that occur moreften in older women (eg, hypertension, diabetes, previousbortion, previous stillbirth, multiple gestation, placenta pre-ia, placental abruption, parity, and martial status), theyound that advanced maternal age remained an independentisk factor for stillbirth. Women 35 to 39 years of age had a
.8-fold risk of stillbirth when compared with women less shan 30 years of age; for women 40 years of age or older theisk was 2.4-fold higher.7
Using the McGill Obstetrical Neonatal database, whichad over 100,000 births, Fretts and Usher found that theauses of stillbirth in older women has changed over the pasthree to four decades. Historically, the only specific cause ofetal death that occurred significantly more often in women5 years of age or older, compared with younger women, wastillbirths related to congenital anomalies (OR, 3.2; 95% CI,.6-6.5).8 Later in the study period after the introduction ofoutine prenatal screening, diagnosis, and the availability ofbortion, the number of stillbirths due to anomalies in olderomen reduced almost statistically below that of youngeromen (OR, 0.2; 95% CI, 0.003-1.5). Of course these are
till significant losses, but they no longer appear in the still-irth statistics. What was notable in the 1978-1995 periodas that the unexplained stillbirth rate (ie, an appropriatelyrown fetus and without obstetrical or maternal risk factors)as 2.2-fold higher in women 35 years of age or older when
ompared with younger women.8 Froen and coworkers, us-ng a Norwegian database of over 500,000 women, foundhat women 35 years of age or older to be at a 5.1-fold in-reased risk of having an unexplained stillbirth when com-ared with women less than 25 years of age (95% CI, 1.3-9.6).9 Huang and coworkers, also using the McGillbstetrical Neonatal database, found that 60% of the unex-lained stillbirths occurred after 36 weeks of gestation.10 In aeparate study, this group showed that the increased risk ofnexplained stillbirth late in pregnancy was notably higher inomen 35 years of age or older.11
Reddy and colleagues using US data from 36 states from001 and 2002 (N � 5,458,735) performed an analysis ofhe risk of stillbirth by maternal age throughout pregnancyor nonanomalous singleton pregnancies.12 In their study,0.4% of their population was 35 to 39 years of age, with.1% reported to have a concomitant medical condition (eg,ypertension and diabetes, which were the most commonlyeported conditions). Women 40 years of age or older con-tituted 2.2% of births, 14.4% of which reported a medicalondition. The risk of stillbirth for women 40 years of age orlder was higher at all gestational ages, but the risk differenceas accentuated after 38 weeks of gestation (Fig. 1).12 Thisgure demonstrates that older women have stillbirth riskssually associated with postdates but this occurs earlier inestation. For example, at 41 weeks of gestation, the risk oftillbirth is approximately 0.95/1000 for women 30 to 34ears of age; this is the equivalent rate for women 35 to 39ears of age at 40 weeks of gestation, and for women 40 yearsf age and older this rate of stillbirth occurs at 39 weeks ofestation. Only about 10% women who were 35 years of ager older had reported a medical condition that might increasehe risk of stillbirth, so it is useful to remember than 90% didot. When women with known medical problems were elim-
nated from the analysis, the results regarding stillbirth ratesere unchanged. It is also important to note that primiparousomen had the highest risk of stillbirth and black womenad a higher rate than white women (Table 1).12 These ob-
ervations support a case for treating these pregnancies in a
mtHsswtr
awprscmiscaettb
oaaowtklo
AABsaaisgatw
line.)
T
*A
314 R.C. Fretts and U.A. Duru
anner similar to “postdates” pregnancies, by consideringhe options of antepartum testing and/or timed delivery.owever, there are no prospective clinical trials however that
pecifically address this issue for older women, and for rea-ons of logistics and statistical power, it unlikely that thereill be good, “Level 1” evidence in the near future. For now,
he clinicians must use their clinical judgment to weigh theisks and benefits of such a strategy.
In this setting, it is a useful exercise to compare the risk oflate stillbirth to other adverse outcomes that occur inomen of advanced maternal age (Table 1).12,13 Much em-hasis has been placed on prenatal diagnosis to reduce theisk of having a live-born infant with a significant chromo-omal anomaly. Indeed, if a woman had not been sufficientlyounseled that her risk of a chromosomal anomaly was esti-ated to be 1/66 at the age of 40, and had not been offered
nvasive testing, she (and her lawyer) could easily demon-trate that her care fell outside the bounds of the standard ofare. It appears that if an older woman has been able tochieve pregnancy, has been lucky enough to not have anarly miscarriage, and has navigated through the many op-ions of prenatal screening and invasive diagnostic testing,hat the risk of having a late stillbirth in a normally formedaby after 37 weeks of gestation has not caught the attention
Figure 1 The risk of stillbirth for singleton births withoutand colleagues.13 (Color version of figure is available on
able 1 Rates of Chromosomal Abnormalities in Live-Born Co
MaternalAge at
DeliveryRisk of
Trisomy 21
Risk of AnyChromosomalAbnormality
Risk of StAfter 37
Multip
20 to 34 1/1667 to 1/485* 1/562 to 1/238* 1/7735 to 39 1/378 1/192 1/50
40� 1/106 1/66 1/30
Estimates range from 20 years to age to 34 years of age.
dapted from Reddy and colleagues,12 and Hook.13f both the provider and the patient. For women 40 years ofge or older having her first birth, the risk of late stillbirthfter 37 weeks of gestation is 1/116 (Table 1). Given thatlder women have fewer reproductive opportunities, it isorth reviewing these risks with the patient and reviewing
he options available to her (eg, expectant management withick-counting, formal antepartum testing, and/or timed de-
ivery). It is also worth mentioning that there is no standard-f-care or consensus practice guideline at the present time.
Strategy ofntepartum Testing at Term
y choosing a strategy of antepartum testing, the benefit ofuch a strategy depends on the underlying risk of stillbirthnd the sensitivity and specificity of the test. Currently therere no data to permit the generalization that antepartum test-ng typically used for a postdates pregnancy will function in aimilar way for older women at earlier gestational ages. Ineneral, for a postdates pregnancy, the available data to datere insufficient to guide as to which intervention(s) has con-ributed most to the observed reduction of stillbirths after 41eeks of gestation. Has the often routine induction after 41
nital anomalies by gestational age. Adapted from Reddy
ed to the Age-Related Risk of Stillbirth
hs
Risk of StillbirthAfter 37 Weeks
Nulliparous
Risk of Stillbirth for All BlackWomen After 37 Weeks withNo Known Medical Problems
1/269 1/3261/156 1/2471/116 1/230
conge
mpar
illbirtWeekara
524

w“attptcv
tap3roaidoitfwwttt
iwe
oIur1hspdetlowriet
ftwliratpdttt
T
FFFTTIC
OA
T
FFTTIC
OA
New indications for antepartum testing 315
eeks contributed more to the stillbirth reduction or was it aless-than-perfect” evaluation of fetal well-being that led ton induction? Crowley, for example, has estimated that, inhe general population at 41 weeks, it would take 400 induc-ions to prevent one stillbirth.14 Since all estimates of a “true-ositive test” and a “false-positive test” are driven by the facthat our interventions are designed to prevent stillbirth, alinician will probably never know which of the 400 inter-entions saved a baby.
In an attempt to quantify the risks and benefits of antepar-um testing late in pregnancy, Fretts and colleagues designeddecision analysis based on the week-specific risk of unex-lained stillbirth (the most frequent type of loss) in women5 years of age or older having their first birth.15 Estimates ofelative risk of unexplained stillbirth by maternal age werebtained from the McGill Obstetrical Neonatal Database (ie,Canadian hospital-based data). To estimate the possible
ncreased risk of cesarean delivery, they used the week-specificifference of cesarean delivery in labors that occurred spontane-usly versus those that were induced, in two large Boston teach-ng hospitals.16 A sensitivity analysis of the characteristics of theest was included, varying both the sensitivity and the specificityrom 70 to 90%. For the main model it assumed that the testingould begin in the 37th week, and it was assumed that 10% ofomen would have an abnormal test and that this would lead
o an induction, regardless of cervical status. It also assumedhat, despite testing, 30% of babies would die anyway andhat there were no intrapartum deaths.
In this model, the odds ratio for stillbirth was the mostmportant factor in stillbirth reduction (Table 2). Womenho had an underlying five-fold increased risk, using a strat-
gy of antepartum testing, would theoretically reduce the rate
able 2 Effect of Unexplained Stillbirth Risk on Outcomes of
Outcome OR 1
etal deaths per 1000 with no testing 1.6etal death per 1000 with testing 0.4etal deaths averted with testing 1.2ests per pregnancy 3.4ests per fetal death averted 2862nductions per fetal death averted 233esarean deliveries per fetal death averted 44
utcomes from week 37 through 41 weeks assumes test characdapted from Fretts and colleagues.15
able 3 Base-Case Results for Nulliparous Women Aged 35
Outcome of Unexplained Fetal Deaths No Te
etal deaths/1000 5.etal deaths averted —est per pregnancy —est per fetal death averted —nduction per fetal death averted —esarean deliveries per fetal death averted —
utcomes from week 37 through 41 weeks assumes test charac
dapted from Fretts and colleagues.15f unexplained stillbirth from 1/128 to 1/526 ongoing births.t is also useful to note women at low risk (ie, an OR � 1.0)sing a similar strategy would have a more limited benefit,educing the risk of late unexplained stillbirth from1/625 to/833. For example, women 35 years of age or older havinger first birth, who have an estimated rate of late unexplainedtillbirth of 5.2/1000 after 37 weeks of gestation, the modelredicts that the rate of unexplained stillbirth could be re-uced to as low as 1.3/1000. This strategy however wouldntail 863 antepartum tests per fetal death averted, 71 induc-ions per fetal death averted, and 14 additional cesarean de-iveries per fetal death averted (Table 3). It is interesting whenne compares this approach to a strategy of no testing, butith a planned induction at 41 weeks. In this scenario, the
ate of induction and cesarean delivery per fetal death averteds much greater (429 and 219, respectively) than with a strat-gy of antepartum testing. That is because a large portion ofhe stillbirths have already occurred, before 41 weeks.15
Of course this is only a model and is limited by manyactors. As previously stated, it is not known if antepartumesting in women of advanced maternal age late in pregnancyill reveal abnormalities before a demise. However, if paral-
els can be drawn to other high-risk conditions, a strategy ofmplementing antepartum testing has been associated with aeduction in the risk of stillbirth in women with hypertensionnd diabetes to that just slightly above the general popula-ion. Another limitation is that the study model did not em-loy twice weekly testing (a standard protocol used for post-ates pregnancies) nor did it account for the effect of serialesting. Typically, if one test is abnormal, it would be routineo perform a second, follow-up test. This would be especiallyrue in the setting where the patient was 35 years of age or
ly Antepartum Testing Starting at 37 Weeks
OR 2 OR 3 OR 4 OR 5
3.2 4.7 6.2 7.80.8 1.2 1.5 1.92.4 3.5 4.7 5.93.4 3.3 3.3 3.3
1418 950 711 569116 78 58 4722 15 11 9
s to be 70% sensitive and 90% specific.
and Older
Weekly Testing Startingat Week 37
Induction at41 Weeks
1.3 4.33.9 0.93.3 —
863 —71 46914 219
s to be 70% sensitive and 90% specific.
Week
teristic
Years
sting
2
teristic

owwc“dta
tticbd
OTTsapatW3htidtPifcdbk2twilmt5ntnfimiasit
fhogbbtpwipm
RWattgtrnrwicrfwicm3ldudhitsr“rd
Pvl�masfsc
316 R.C. Fretts and U.A. Duru
lder, at 37 weeks, with an unfavorable cervix. Contrast thisith the threshold to induce in the setting of a 43-year-oldoman with mild oligohydramnios at term, where the clini-
ian might be relieved that at 39 weeks there is now anindication” for delivery. This decision analysis does not ad-ress the type and the cost of antepartum testing, the poten-ial maternal risks of additional cesareans, nor the effect ofntepartum testing on maternal anxiety and confidence.
In summary, the sensitivity and specificity of antepartumesting has been greatly debated. In this model, however, ifhe specificity were lowered from 90 to 70% (thereby increas-ng the “false-positive” rate to 30%, and consequently in-reasing the induction rate), there was a reduction of still-irths, reminding us once again that if the patient iselivered, she is no long at risk for stillbirth.15
ptimal Timing ofesting and Delivery
heoretically, each medical condition has an optimal time totart antepartum testing, and an optimal time for delivery,fter taking into account both fetal and maternal factors. Forregnant women with insulin-dependent diabetes, Rousend colleagues estimated the optimal time to begin antepar-um testing was about 34 weeks of gestation.17 Similarly,
eeks and colleagues, using results of antepartum testing in00 women with a previous stillbirth, estimated in otherwiseealthy women that antepartum surveillance be initiated af-er 32 weeks of gestation.18 Early interventions led to anncreased risk of admission to the neonatal intensive care, butelaying fetal evaluation and delayed delivery can increasehe risk of stillbirth or delivery of a baby in poor condition.ostdates pregnancies can also put the mother at risk for
ncreased obstetrical trauma, because of the increased rate ofetal macrosomia. Nicholson and colleagues, for example,ompared maternal and fetal outcomes in women with goodating, who were at term and who were eligible for a vaginalirth.19 The database included 11,724 women without anynown risk factors, who were less than 35 years of age, and373 women who were 35 years of age or older. Six hundredhirty-five women had a diagnosis of hypertension, and 460omen had diabetes. Women with multiple risk factors were
ncluded in each subgroup. The study was not powered toook at perinatal mortality. The investigators evaluated the
aternal cesarean section rate, the newborn admission rate,he incidence of maternal 3rd- and 4th-degree tears, and the-minute Apgar of 0 to 6 rate. The most important compo-ent of this study’s outcomes that defined the lower limits ofhe optimal time of delivery was the admission rate to theeonatal intensive care unit. The outcome that largely de-ned the upper limit of the optimal time of delivery was theaternal cesarean section rate. Given the design of this study,
ncluding the prespecified goals of minimizing both neonataldmissions and cesarean sections, these investigators de-cribed the optimal time of delivery to be where these risksntersected the 95% CI around these points. The “optimal
imes of delivery” were described as 37 1/7 to 41 0/7 weeks �or low-risk women, 39 2/7 to 40 1/7 weeks for women withypertension, and for women 35 years of age or older, theptimal timing of delivery was 38 5/7 to 39 6/7 weeks ofestation. Interestingly their model did not work well for dia-etic women, because a large proportion of babies born to dia-etics spent time in the neonatal intensive care unit, presumablyo monitor the baby’s glucose, monitoring that was not routinelyerformed on infants born to nondiabetic mothers. This study,hile interesting, did not assess the impact of antepartum test-
ng or induction. There were also many questions on how com-eting outcomes should be weighed and how patient preferenceight have altered these outcomes.
isk of Induction Near Termhile there is no measurable long-term neonatal mortality
ssociated with delivery after 37 weeks, there is an increase inhe incidence of neonatal respiratory distress and transientachypnea at term, and the rate is higher before 38 weeks ofestation and with those having a cesarean delivery.20,21 Mul-iparous women of advanced maternal age are at an increasedisk of stillbirth late in pregnancy, but for them inductionear term does not materially increase the cesarean sectionate.16,20 The greater management dilemma is for nulliparousomen. There are many cohort studies addressing the role of
nduction in nulliparous women. While most have not in-luded information on cervical status or the use of cervicalipening agents, there appears to be an approximately two-old increased risk of cesarean delivery when comparing womenho present in spontaneous labor compared with those that are
nduced.16 The most appropriate comparison however is toompare elective induction (with cervical ripening) to expectantanagement. With the nadir of cesarean section being between
8 and 39 weeks, expectant management is associated with botharger babies and an increasing opportunity for late placentalysfunction.22 In an elegant analysis, Caughey and coworkers,sing a retrospective cohort of women eligible for a vaginalelivery at University of California San Francisco, demonstratedow using the traditional comparison of spontaneous versus
nduced labor generated a two-fold increase in cesarean sec-ions for nulliparous women.23 However, when the cesareanection rate of induced women was compared with the totalisk of a cesarean delivery over the last weeks of gestation (ie,the prospective risk of cesarean” similar to the “prospectiveisk of stillbirth”), it appears that induction may actually re-uce the risk of cesarean delivery (Table 4).A novel approach called the “Active Management of Risk in
regnancy at Term” (AMOR-IPAT), used by groups at the Uni-ersity of Pennsylvania, does show some promise.24 They pub-ished a cohort study comparing outcomes in AMOR-IPAT (N
100) and non-AMOR-IPAT groups (N � 300). In the activeanagement group, early dating was performed. At term, a risk-
ssessment was performed that included the presence or ab-ence of factors that might increase uterine and placental dys-unction (eg, hypertension, diabetes, advanced maternal age,moking, size-less-than-dates, and other factors). They also in-luded risk factors for cephalopelvic disproportion (eg, BMI
30, short stature, gestational diabetes, size-greater-than-dates,
estna2cm4astfibopi
SWtrtmiwstpp
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
T
E*†A
New indications for antepartum testing 317
tc). Cervical ripening was used for all women with a Bishopcore less than 5. The AMOR-IPAT group had a median gesta-ional age at delivery which was significantly lower than theon-AMOR-IPAT group (38.9 versus 40.1 weeks; P � 0.001),s well as a significantly higher induction rate (63% versus5.7%; P � 0.001), but they also had a surprisingly lowesarean section rate (4% versus 16.7%). The active manage-ent group also had a statistically lower rate of 3rd- and
th-degree tears and a lower NICU admission rate. If thispproach were to be widely adopted, the result would be aea of change for obstetrics, necessitating a very high induc-ion rate. While the utility of this approach needs to be con-rmed and validated, issues of patient acceptability will alsoe an important measure. Modern obstetrics is often accusedf medicalization of the birthing process; it is not clear whatroportion of women would embark on a strategy that would
nvolve a 60% induction rate.
ummaryhile there is no “level 1” evidence to recommend antepar-
um testing or timed delivery in patients with an increasedisk of stillbirth late in pregnancy, we need to appreciate thathis a gap in our knowledge. Many times we as practitionersust function in the “gray” area of imperfect knowledge. It is
mportant however to accurately assess risk. The 40-year-oldoman having her first baby should be told that her risk of
tillbirth in late pregnancy is 1/116. When she and her prac-itioner travel down the “gray” roads together, it behooves theractitioner to describe the risks and benefits of these ap-roaches within the limits of our knowledge.
eferences1. Chu SY, Kim SY, Lau J, et al: Maternal obesity and the risk of stillbirth:
a metaanalysis. Am J Obstet Gynecol 2007. Available at: www.AJOG.org. Accessed September 12, 2007
2. Nohr EA, Bech BH, Davies MJ, et al: Prepregnancy obesity and fetaldeath: a study within the Danish National Birth Cohort. Obstet Gynecol206:250-259, 2006
3. Salihu HM, Dunlop AL, Hedayatzadeh Alio AP, et al: Extreme obesityand the risk stillbirth among black and white gravidas. Obstet Gynecol110:552-557, 2007
4. Yuan H, Platt RW, Morin L, et al: Fetal deaths in the United States, 1997vs 1991. Am J Obstet Gynecol 193:489-495, 2005
5. Martin JA, Hamilton BE, Sutton PD, et al: National Vital Statistics Reports.Births: Final Data for 2004. Available at: www.cdc.gov. Accessed Septem-
able 4 Induction of Labor Compared to Expectant Managem
Week ofInduction
Induction of LaborC/S Rate
Expectant MC/S
38 15.6% 17.39 18.6% 19.40 22.5% 24.41 29.3% 33.
xpectant management group includes all women delivered beyondControlling for maternal ethnicity, BMI, insurance, preeclampsia, dP value < 0.01 when comparing induction of labor group to the spdapted from Reddy and colleagues,12 and Hook.13
ber 29, 2006
6. Berkowitz GS, Skovron ML, Lapinski RH, et al: Delayed childbearingand outcome of pregnancy. N Engl J Med 332:659-664, 1990
7. Fretts RC, Schmittdiel J, McLean FH, et al: Increased maternal age andthe risk for fetal death. N Engl J Med 333:953, 1995
8. Fretts RC, Usher RH: Causes of fetal death in women of advancedmaternal age. Obstet Gynecol 89:40-45, 1997
9. Froen JF, Arnestad M, Frey K, et al: Risk factors for sudden intrauterineunexplained death: epidemiological characteristics of singleton cases inOslo. Norway, 1986-1995. Am J Obstet Gynecol 184:694, 2001
0. Huang DY, Usher RH, Kramer MS, et al: Determinants of unexplainedantepartum fetal deaths. Obstet Gynecol 95:215, 2000
1. Fretts RC, Usher RH: Fetal death in women in the older reproductiveage group. Contemp Rev Obstet Gynecol 9:173-179, 1997
2. Reddy UM, Ko CW, Willinger M: Maternal age and the risk of stillbirththroughout pregnancy in the Unites States. Am J Obstet Gynecol 195:764-770, 2006
3. Hook EB: Rates of chromosome abnormalities at different maternalages. Obstet Gynecol 58:282, 1981
4. Crowley P: Elective induction of labor at 41� weeks gestation. In:Enkin M, Keirse MJNC, Renfrew MJ, et al (eds): Cochrane Database ofSystematic Reviews. Review 4144
5. Fretts RC, Elkin EB, Myers ER, et al: Should older women have ante-partum testing to prevent unexplained stillbirth? Obstet Gynecol 104:56, 2004
6. Heffner LJ, Elkin E, Fretts RC: Impact of labor induction, gestationalage and maternal age on cesarean section delivery rates. Obstet Gynecol120:287-293, 2003
7. Rouse DJ, Owen J, Goldenberg RL, et al: Determinants of the optimaltime in gestation to initiate antenatal fetal testing: a decision-analyticapproach. Am J Obstet Gynecol 173:1357-1363, 1995
8. Weeks JW, Asrat T, Morgan MA, et al: Antepartum surveillance for ahistory of stillbirth: when to begin? Am J Obstet Gynecol 172:486-492,1995
9. Nicholson JM, Kellar LC, Kellar GM: The impact of the interactionbetween increasing gestational age and obstetrical risk on birth out-comes: evidence of a varying optimal time of delivery. J Perinatol 26:392-402, 2006
0. Tylleskar J, Finnstrom O, Leijon I, et al: Spontaneous labor and electiveinduction—a prospective randomized study.I. Effects on mother andfetus. Acta Obstet Gynecol Scand 58:513, 1979
1. Morrison JJ, Rennie JM, Milton PJ: Neonatal respiratory morbidity andmode of delivery at term: influence of timing of elective caesareansection. Br J Obstet Gynaecol 102:101, 1995
2. Stallmach T, Hebisch G, Meier K, et al: Rescue by birth: defectiveplacental maturation and late fetal mortality. Obstet Gynecol 97:505-509, 2001
3. Caughey AB, Nicolson JM, Cheng YM, et al: Induction of labor and cesar-ean delivery by gestational age. Am J Obstet Gynecol 195:700-705, 2006
4. Nicholson JM, Keller LC, Cronholm PF, et al: Active management ofrisk at term in an urban population: an association between a higherinduction of labor rate and a lower cesarean delivery rate. Am J Obstet
Nulliparous
ement Adjusts OR(95% CI)*
Spontaneous LaborC/S Rate
1.9 (1.3 to 2.9) 9.0%†
1.5 (1.1 to 2.1) 11.6%†
1.6 (1.2 to 2.2) 15.2%†
1.3 (1.0 to 1.8) 19.3%†
rticular gestational age of the induction of labor comparison group.s, and epidural use.ous labor group.
ent in
anagRate
6%9%3%1%
the paiabeteontane
Gynecol 191:1516-1528, 2004

AC
AmcmgtuttuTpdf
GTatta
WA
3
ntenatal Testing—Benefits and Costshristina M. Scifres, MD, and George A. Macones, MD, MSCE
Antenatal testing is a common component of care for the high-risk pregnancy. The goals ofantenatal testing include the prevention of stillbirth and the detection of the hypoxic fetusto allow intervention before acidosis and long-term damage. Data regarding the efficacy ofantenatal testing are limited by a lack of randomized controlled trials. The majority ofavailable data hinge on observational studies with the inherent potential for bias. There isalso a paucity of data comparing the various testing modalities and addressing the issue ofthe optimal timing of initiation of testing. As well, data are limited regarding the variousconditions most likely to benefit from testing and the frequency with which testing shouldbe performed. The issue of cost relating to antenatal testing is an important one. Central tothe issue of estimating cost is an understanding of the efficacy of the test. Given our currentlimitations, we have significant difficulty accurately estimating the cost of antenatal testing;however, rough estimates of cost are made.Semin Perinatol 32:318-321 © 2008 Elsevier Inc. All rights reserved.
KEYWORDS antenatal testing, cost analysis, nonstress test, biophysical profile
pwfttita
ETripHiwcotuoctaM
ntenatal testing was introduced into clinical practicewith the primary goal of stillbirth prevention. Multiple
ethods of antenatal testing have been studied, including theontraction stress test, nonstress test, biophysical profile, andodified biophysical profile. Little has been published re-
arding the benefits and costs associated with each of theseesting modalities. The first step in any analysis of cost is tonderstand the efficiency and effectiveness of an interven-ion. Significant difficulties in evaluating the costs of antepar-um testing arise from limitations in the data addressing thesefulness of testing in preventing stillbirth as a primary goal.he purpose of this review is to discuss some of the dataertaining to the effectiveness of antenatal testing, to use thisata to estimate the costs of antenatal testing, and to exploreuture research areas in this field.
oals of Antepartum Testinghe optimal method of antepartum testing would have thebility to prevent stillbirth. An ideal test would also identifyhe hypoxic or acidemic fetus and allow intervention beforehe onset of either death or disability. This ideal test wouldlso be inexpensive, require minimal effort of the part of the
ashington University, St. Louis, MO.ddress reprint requests to Christina M. Scifres, MD, Department of Obstet-
rics and Gynecology, 4911 Barnes Jewish Hospital Plaza, Box 8064, St.
pLouis, MO 63110. E-mail: [email protected]18 0146-0005/08/$-see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1053/j.semperi.2008.04.017
atient, and be easily and reliably interpreted by the clinicianith good intra- and inter-observer variability, and with low
alse-positive rates. The first goal of this review is to examinehe available literature relating to the efficacy of antepartumesting. Importantly, we will also discuss some of the signif-cant limitations present in this body of literature. Fromhere, we discuss some of the issues relating to the costsssociated with antenatal testing.
fficacy of Antepartum Testinghere are a number of studies available addressing stillbirthates following each of the various methods of antenatal test-ng, including the contraction stress test, nonstress test, bio-hysical profile, and modified biophysical profile (Table 1).owever, strong evidence for the efficacy of antepartum test-
ng is lacking. Many of the studies are observational studies,hich do not report stillbirth rates in an untested group,
ompare tested to untested subjects at the same institution,r compare stillbirth rates before and after the initiation ofesting. These observational studies leave large gaps in ournderstanding of the true sensitivity and specificity for eachf the specific antenatal tests. The observational studies thatompare tested to untested populations at the same institu-ion are significantly limited by the fact that little is knownbout the untested population. For example, in the work byiller and coworkers,4 utilizing the modified biophysical
rofile for antenatal testing the uncorrected stillbirth rate in

tsrartiwtptitwlctfigCcttef
aoprsdimtifthtptaw5cp
iwo
slstaafltdpttn
ttaentcpdscpvdTtm
CEshticddwrwmCebwr
T
NCBM
Antenatal testing 319
he untested population is 10.8/1000, while the correctedtillbirth rate (fetuses with lethal anomalies, mothers whoefused intervention excluded) in patients who underwentntenatal testing is 0.8/1000. While the overall stillbirthates following any of the antenatal tests are low, the ques-ion that naturally arises is this—if the patients undergo-ng testing are going to be compared with patients whoere not undergoing testing, do the untested patients in
he above study represent a high- or low-risk group ofatients? If indeed they are truly a low-risk population,hen the reduction in stillbirth achieved by antenatal test-ng may be notable. However, if the stillbirths in the un-ested population represent a high-risk group of patientsho otherwise may not have been receiving care or if a
arge number of fetuses with lethal anomalies are in-luded, then it remains highly possible, if not likely, thathe differences in stillbirth rates may be secondary to otheractors unrelated to the antenatal test. Four small random-zed studies involving a total of 1588 pregnancies under-oing cardiotocography were included in a review by theochrane Collaboration.5 There was a trend toward in-reased perinatal deaths in the group undergoing moni-oring (odds ratio, 2.85; 95% CI, 0.99-7.12) and the au-hors of the review concluded that there is not enoughvidence to evaluate the use of antenatal cardiotocographyor fetal assessment.
In addition, another significant limitation of the current avail-ble literature is the lack of information on potential adverseutcomes related to antenatal testing. Antenatal testing has theotential for not only false-negative results (stillbirth following aeassuring test) but also false-positive results. False-positive re-ults have the potential to result in iatrogenic prematurity withownstream adverse neonatal outcomes and also unnecessary
nterventions with secondary adverse maternal outcomes. Inuch of the published literature regarding antenatal testing
hese important outcomes are not discussed. For one example,n the article by Miller and coworkers4 discussed above, thealse-positive rate resulting in preterm delivery was 1.5% of theotal population tested before 37 weeks. Many of these patientsad testing initiated at 34 weeks, but it is intuitive that if earlieresting is utilized, the potential risks associated with iatrogenicreterm birth may increase. In addition, the overall false-posi-ive rate was 60% if the false-positive rate was defined as anbnormal test that prompted delivery but was not associatedith fetal distress, meconium-stained amniotic fluid, low-minute Apgar score, or intrauterine growth restriction. Theesarean section rate was 24% in the tested population com-
able 1 Corrected Stillbirth Rates Following Antepartum Tests
Antepartum TestCorrected
Stillbirth Rate
onstress test 1.9 to 3.2/10001,2
ontraction stress test 0.4/10002
iophysical profile 0.7/10003
odified biophysical profile 0.8/10004
ared with a rate of 13.2% in the untested population but it is v
mpossible to distinguish how many of these cesarean sectionsere indicated or associated with improved fetal and neonatalutcomes.
Another important consideration which is poorly under-tood is the potential contribution of antenatal testing toong-term outcomes in children. For example, a significant con-ideration is whether or not antenatal testing allows us to iden-ify the compromised infant and intervene before the onset ofdverse neurologic outcomes. This is certainly a primary goal ofntenatal testing, but there is a paucity of published long-termollow-up on these children. The general assumption in theiterature is that our intervention for an abnormal antepartumest results in a good outcome. However, in the absence ofata we cannot be assured that our interventions, even if theyrevent stillbirth, may not involve a tradeoff between long-erm neurologic dysfunction and fetal death. Such informa-ion would play a vital role in determining both the effective-ess and the cost of antenatal testing.Finally, another important question regarding the effec-
iveness of antepartum testing is whether or not there are datao support the use of one antepartum test over another. Therere no adequately powered randomized trials to examine thefficacy of one testing modality over another, although, asoted earlier, the stillbirth rates following any of the antepar-um testing modalities are overall quite low. Freeman andoworkers2 published a nonrandomized cohort study com-aring the contraction stress test to the nonstress test whichemonstrated overall low stillbirth rates for each test but thistudy design prohibits an accurate comparison. Platt andoworkers6 conducted a small quasi-randomized trial com-aring management based on the results of nonstress testingersus the biophysical profile. They were unable to detect aifference in the stillbirth rates between the two populations.he above data leave the clinician with a paucity of informa-
ion on which to base clinical choices among the variousethods of antenatal assessment.
osts of Antenatal Testingconomic analysis remains an important part of health careecondary to the fact that resources are limited and overallealth care costs are rising quickly. For example, in 2002otal health care spending was $1.6 trillion dollars amount-ng to total expenditures of $5440/person. In addition, healthare expenditures are growing 5.7% faster than the grossomestic product and overall account for 14.2% of the grossomestic product. As health care resources become limited,hat is spent on programs such as antenatal testing diverts
esources from other programs. That being said, we must askhether or not cost is likely to drive our clinical decision-aking when it comes to the utilization of antenatal testing.urrently, very little in obstetrics is driven solely by cost. Forxample, the utilization of Down syndrome screening hasecome widespread. Cost estimates per live birth of a childith Down syndrome avoided with screening programs
ange from 0.67 to 1.35 million dollars7 but cost has played
ery little in the decision to recommend screening.
lpmrwsscnaf
fnhvca1iwwfrt$stttdtbptet
oepct
asdotwttldwnwctogf
CAoltdatpgrmailippcr
R1
2
3
4
5
TU
54
H
3
320 C.M. Scifres and G.A. Macones
The fundamental principles of cost assessment are re-ated to the evaluation of the effectiveness and efficacy of aarticular intervention. Effectiveness refers to the improve-ent in health as measured by explicit health outcomes in
eal world settings (eg, does the intervention work?),hereas efficacy refers to improvement in health as mea-
ured by these same health outcomes in ideal or researchettings.8 The best and least biased way to establish effi-acy is from randomized controlled trials but unfortu-ately this data are not available for the various methods ofntenatal assessment, which limits our ability to perform aormal cost assessment.
However, it does appear that the best data availablerom the literature to assess the costs pertaining to ante-atal testing is the article by Miller and coworkers.4 Weave discussed this particular article throughout this re-iew but will now examine some of the details and how wean use this data to make at least rough estimates of costsssociated with antenatal testing. This study involved5,482 high-risk obstetric patients who underwent mod-
fied biophysical profile testing. A total of 54,617 examsere performed. The cost of a modified biophysical profileas estimated by assessing the professional and technical
ees at our own institution and then applying a cost:chargeatio of 0.6. This leads to an estimate of cost for a nonstressest of $48.00, $236.00 for an amniotic fluid index, and295.00 for a biophysical profile. The estimated costs as-ociated with testing are listed in Table 2. The total cost forhis testing program was $17,192,661. If one calculateshat 158 stillbirths were potentially prevented by antepar-um testing, the cost per stillbirth averted is $108,814. Asiscussed throughout this article, there are many difficul-ies with these calculations. It is unclear how many still-irths are truly prevented by this, or any, antenatal testingrogram. In addition, it is difficult to estimate the poten-ial costs associated with induction of labor, excess cesar-an sections, and maternal complications directly relatedo intervention.
The costs of antenatal testing depend highly on the efficacyf the test. For example, we can assume the extremes offfectiveness to further examine potential costs. In this sameopulation of patients, if only 10 stillbirths are prevented, theost per stillbirth averted is $1,719,000. At the other ex-reme, if testing prevents 300 stillbirths, the cost per stillbirth
able 2 Costs Associated with an Antenatal Testing Programtilize the Modified Biophysical Profile as an Initial Test
Contributors to Cost Cost
4,617 modified biophysical profiles $15,551,228070 excess biophysical profilessecondary to nonreactivenonstress test
$1,200,650
ospital admissions secondary toabnormal testing
$393,120
2 iatrogenic preterm deliveries $47,663
6(>34 weeks)
verted is $57,300. Even the high-end cost of $1,719,000 pertillbirth prevented may be quite reasonable if it results inelivery of a healthy neonate. The gestational age at initiationf testing plays a central role is estimation of cost as well. Inhe Miller article, testing was initiated at greater than 34eeks in almost all cases. However, the earlier testing is ini-
iated, the higher the potential for significant costs related tohe care of premature neonates as well as the increased like-ihood of long-term sequelae of prematurity. This was ad-ressed in a decision analysis performed by Rouse and co-orkers,9 which examined relationship of fetal death,eonatal death, and moderate to severe disability in patientsith diabetes over a range of gestational ages at which testing
ould be initiated. This model demonstrated that initiatingesting around 34 weeks may provide the most favorableutcomes. Estimates of the cost of an antenatal testing pro-ram also hinge on how frequently testing should be per-ormed.
onclusionss we have reviewed throughout this document, the efficacyf antepartum testing is uncertain. There is also a significantack of data relating to the comparative efficacy of each of theesting modalities and a paucity of information to guide us inetermining the optimal time to initiate testing. The safety ofntepartum testing clearly relates to the timing of initiation ofesting. Given the lack of data pertaining to efficacy of testing,reventing iatrogenic prematurity seems to be an importantoal of testing. Although we have explored issues of costelating to antenatal testing, this is unlikely to drive decision-aking regarding whether or not to test. If we could be
ssured that antenatal testing was highly effective in prevent-ng stillbirth of an otherwise normal fetus, society would beikely to endorse testing even at very high cost. For example,f antenatal testing is highly effective, with low rates of false-ositive results, expanding indications for testing or even aolicy of universal testing may be a reasonable approach toonsider. However, with the current available data, the aboveemains speculative.
eferences. Freeman R, Anderson G, Dorchester W: A prospective multi-institu-
tional study of antepartum fetal heart rate monitoring. Risk of perinatalmortality and morbidity according to antepartum fetal heart rate testresults. Am J Obstet Gynecol 143:771-777, 1982
. Freeman R, Anderson G, Dorchester W: A prospective multi-institu-tional study of antepartum fetal heart rate monitoring. Contraction stresstest versus nonstress test for primary surveillance. Am J Obstet Gynecol143:778-781, 1982
. Manning F, Morrison I, Harman C, et al: Fetal assessment based on fetalbiophysical profiling: experience in 19,221 referred high risk pregnan-cies. Am J Obstet Gynecol 157:880-884, 1987
. Miller D, Rabello Y, Paul R: The modified biophysical profile: ante-partum testing in the 1990’s. Am J Obstet Gynecol 174:812-817,1996
. Pattison N, McCowan L: Cardiotocography for antepartum fetal assess-ment. Cochrane Database of Systematic Reviews 1999;(1):CD001068.DOI:10.1002/14651858
. Platt L, Walla C, Paul R, et al: A prospective trial of the fetal biophysical

7
8
9
Antenatal testing 321
profile versus the nonstress test in the management of high-riskpregnancies. Am J Obstet Gynecol 153:624-633, 1985
. Biggio JR, Owen J, Wenstrom KD, et al: An outcomes analysis of 5prenatal screening strategies for trisomy 21 in women less than 35 years.
Am J Obstet Gynecol 185:1016-1020, 2001. Macones G, Goldie S, Peipert J: Cost-effectiveness analysis: an introduc-tory guide for clinicians. Obstet Gynecol Surv 54:663-672, 1999
. Rouse D, Owen J, Goldenberg R, et al: Determinants of the optimal timein gestation to initiate antenatal fetal testing: a decision-analytic ap-
proach. Am J Obstet Gynecol 173:1357-1363, 1995