Embed Size (px)
Citation preview

Biomarkers in MS (preventing end-organ damage)
Gavin Giovannoni
Barts and The London

Disclosures
Professor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical trial design, trial steering committees and data and safety monitoring committees from: Abbvie, Bayer-Schering Healthcare, Biogen-Idec, Canbex, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW Pharma, Ironwood, Merck-Serono, Novartis, Pfizer, Roche, Sanofi-Aventis, Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals.
Regarding www.ms-res.org survey results in this presentation: please note that no personal identifiers were collected as part of these surveys and that by completing the surveys participants consented for their anonymous data to be analysed and presented by Professor Giovannoni.
Professor Giovannoni would like to acknowledge and thank Biogen-Idec, Genzyme, Merck-Serono and Novartis for making available data slides on natalizumab, alemtuzumab, oral cladribine and fingolimod for this presentation.

Why MS biomarkers?
• Diagnostic testing
• Positive & negative predictive testing
• Pathogenesis
• Immunology
• Aetiology
• Disease progression & recovery
• Disease heterogeneity
• Pharmacovigilance
• Monitor disease processes
• Prognosis (high vs. low risk patients)
• Monitoring effect of therapeutic interventions

MS is an iceberg?
Clinical
MRI
Pathology

Unreported relapses
Documented relapses
Subclinical relapses
focal MRI activity – new T2 and Gd-enhancing T1 lesions
Focal gray and white matter lesions not detected by MRI
Brain atrophy and spinal fluid neurofilament levels
“The MS Iceberg”
“Above the surface”
“Below the surface”

End-organ damage


ESRF end-stage renal failure

Control Multiple sclerosis

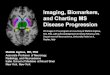
Treatment-effect on atrophy correlates with treatment-effect on disability
Sormani et al. Ann Neurol 2014;75:43–49.

Treatment effect on disability predicted by effect on T2-lesion load and brain atrophy
Meta-analysis of treatment effect on EDSS worsening (y) vs effects on MRI lesions
and brain atrophy, individually or combined, in 13 placebo-controlled RRMS trials
(13,500 patients)
Sormani MP et al. Ann Neurol. 2014;75:43-49.

Emerging concepts in MS
Hagan M, et al. Int J Radiat Oncol Biol Phys 2004; 59:329−340.
NEDD – no evidence of detectable disease (oncology)
NEDA - no evident disease activity (msologoy)
DAF – disease activity free
T2T; treat-2-target (rheumatology)
10 9 7 6 5 4 3 2 1 0 8
0.8
0.6
0.4
0.2
0.0
1.0
Adjuvant (n = 50)
Salvage (n = 118)
p = 0.002
Su
rviv
al
Time since radiotherapy (years)
Biochemical relapse-free survival
ZeTo; zero tolerance

No evident disease activity: NEDA
Gd, gadolinium. 1. Havrdova E, et al. Lancet Neurol 2009; 8:254–260; 2. Giovannoni G, et al. Lancet Neurol 2011; 10:329–337.
Treat-2-target
No evidence of disease activity defined as:1,2
× No relapses
× No sustained disability progression
× No MRI activity
× No new or enlarging T2 lesions
× No Gd-enhancing lesions

-1.0%
-0.8%
-0.6%
-0.4%
-0.2%
0.0% Years 0-2
-0.82%
-0.80%
P=0.822†
Placebo (N=315) Natalizumab (N=627)
Year 0-1* Year 1-2
-0.40%
-0.56%
-0.43%
-0.24%
P=0.004†
P=0.002†
†Difference between treatments; ‡Change from baseline; Miller DH et al. Neurology 2007;68:1390-1401.
AFFIRM Study: natalizumab and brain atrophy
Mean
(S
E)
perc
en
tag
e c
han
ge i
n B
PF

Fingolimod has an early and sustained effect on the rate of brain atrophy compared with placebo and IFNb-1a IM
FREEDOMS, 2 years
Fingolimod 0.5 mg (n = 356)
Placebo (n = 329)
***
*
**
6 0 12 24
Time (months)
0
-0.4
-0.8
-1.2
-1.6
-2.0
−38%
vs placebo p<0.001
Ch
ange
in m
ean
BV
fro
m
bas
elin
e (%
)
TRANSFORMS, 1 year
0 12
Time (months)
0.0
-0.4
-0.6
-1.0
IFNb-1a IM (n = 359)
Fingolimod 0.5 mg (n = 368)
−40%
vs IFNb-1a IM p<0.001
*** -0.2
-0.8
Ch
ange
in m
ean
BV
fro
m
bas
elin
e (%
)
ITT population with evaluable MRI images. Note: n numbers for FREEDOMS data reflect the number of patients with available data at 24 months. *p<0.05; **p<0.01; ***p<0.001 vs comparator; p-values are for comparisons over Months 0-6, Months 0-12, Months 0-24 BV, brain volume; ITT, intent-to-treat. Gilenya™ Prescribing Information 19 April 2012. Reproduced with permission. Kappos L et al. N Engl J Med 2010; 362: 387-401, and Cohen JA et al. N Engl J Med 2010; 362: 402-415. Copyright © 2011 Massachusetts Medical Society. All rights reserved

Reduction in brain atrophy on alemtuzumab

Alemtuzumab Improves Brain MRI Outcomes
in Patients With Active Relapsing-Remitting
Multiple Sclerosis: Three-Year Follow-up of the
CARE-MS Studies
Douglas L Arnold,1,2 Elizabeth Fisher,3 Jeffrey A Cohen,4 Frederik Barkhof,5
Krzysztof W Selmaj,6 David H Margolin,7 Jeffrey Palmer,7 Edward J Fox8
AAN 2014
Blitz S65-008
1NeuroRx Research, Montréal, Québec, Canada, and 2Department of Neurology and Neurosurgery, Montreal
Neurological Institute, McGill University, Montreal, Québec, Canada; 3Department of Biomedical Engineering,
Cleveland Clinic, Cleveland, OH, USA; 4Cleveland Clinic, Cleveland, OH, USA; 5VU University Medical Centre,
Amsterdam, Netherlands; 6Department of Neurology, Medical University of Łódź, Łódź, Poland; 7Genzyme, a
Sanofi company, Cambridge, MA, USA; 8University of Texas Medical Branch, Round Rock, TX, USA

CARE-MS I & II Three-Year MRI Outcomes Change in Brain Parenchymal Fraction (BPF)
Alemtuzumab slowed brain volume loss over 3 years, as assessed by change in BPF
For both patient populations, the median percentage reduction in BPF observed in in Year 3 (0.19% and 0.10%, respectively) was smaller than that observed in Year 1 (0.59% and 0.48%) and Year 2 (0.25% and 0.22%)
Percentage Change in BPF in Formerly Treatment-Naive Patients (CARE-MS I)
Percentage Change in BPF in Patients Who Relapsed on Prior Therapy (CARE-MS II)
Me
dia
n C
ha
ng
e F
rom
Ba
se
lin
e, %
(9
5%
CI)
Year No. of Patients 371 367 351 323
% Change from Previous Year – –0.59% –0.25% –0.19%
Me
dia
n C
ha
ng
e F
rom
Ba
se
lin
e, %
(9
5%
CI)
Year 428 414 405 359
– –0.48% –0.22% –0.10%
No. of Patients
% Change from Previous Year
0 1 2 3
-1 .5 0
-1 .2 5
-1 .0 0
-0 .7 5
-0 .5 0
-0 .2 5
0 .0 0
0 1 2 3
-1 .5 0
-1 .2 5
-1 .0 0
-0 .7 5
-0 .5 0
-0 .2 5
0 .0 0
AAN 2014
Blitz S65-008

CARE-MS I & II Three-Year MRI Outcomes Proportion of Patients Free of Gd Lesions, T2 Lesions, and MRI Activity
The majority of alemtuzumab-treated patients were free of MRI activity (absence of Gd-enhancing lesions and new/enlarging T2 hyperintense lesions) at Year 2 and Year 3
MRI activity-free: absence of both Gd-enhancing and new or enlarging T2 hyperintense lesions; CARE-MS=Comparison of
Alemtuzumab and Rebif® Efficacy in Multiple Sclerosis; CI=confidence interval; DMT=disease-modifying therapy; Gd=gadolinium;
MRI=magnetic resonance imaging; Y=year
No. of Patients 359 370 336 356 370 325 354 369 326
Y1 Y2 Y3 Y1 Y2 Y3 Y1 Y2 Y3
Pro
po
rtio
n o
f P
ati
en
ts,
% (
95
% C
I)
0
20
40
60
80
100
Gd-enhancing
lesion-free
New/enlarging
T2 lesion-free
MRI
activity-free
% MRI Activity Free in Treatment-Naive
Patients (CARE-MS I)
% MRI Activity Free in Patients Who
Relapsed on Prior Therapy (CARE-MS II)
No. of Patients 412 421 364 405 423 361
Gd-enhancing
lesion-free
New/enlarging MRI
activity-free
402 414 361
Pro
po
rtio
n o
f P
ati
en
ts,
% (
95
% C
I)
0
20
40
60
80
100
Y1 Y2 Y3 Y1 Y2 Y3 Y1 Y2 Y3
T2 lesion-free
Patients were treated with alemtuzumab 12 mg at baseline and 12 months later
Re-treatment in Year 3 was administered upon recurrence of disease activity
18% of CARE-MS I patients and 20% of CARE-MS II patients were re-treated
with alemtuzumab in Year 3; <3% were treated with another DMT in Year 3
AAN 2014
Blitz S65-008

17yr female,
diagnosed
with CIS
after
presenting
with myelitis
18yr, 1st year
university
diagnosed
with MS after
having L optic
neuritis
Abnormal MRI; >9
T2 lesions on brain
MRI and spinal cord
lesion at C5
2000 2001
clumsy
left
hand
pins &
needles
in legs
IFN-beta
2002 2003
R optic
neuritis
2004
Bladder dysfunction
Graduate
trainee
marketing
Full
time
employment
Off work
~3 months
of the year
Dec 2007
Brainstem
syndrome;
diplopia
and ataxia
? glatiramer
acetate
Cervical cord
relapse
weak L arm
with pain
High lesion
load with
brain
atrophy
Gd-enhancing
lesion of upper
cervical cord
Splits from
her partner
depression ,
anxiety and fatigue
Reduced mobility
Occupational
health
assessment
natalizumab
New
partner
New job
junior management
position
Residual deficits:
Normal walking 300m, unable to run &
exercise. Intermittent sensory symptoms
in L arm. Mild urinary frequency
Jan 2008
JCV
positive
3-monthly MRI
monitoring
? fingolimod
Oct 2013
Annual MRI
monitoring
JCV
high positive
Final
year of
school
University
Early or late?
20
Mo
nito
rin
g
Tre
atm
ent
Clin
ica
l O
ccu
p &
so
cia
l

17yr female,
diagnosed
with CIS
after
presenting
with myelitis
18yr, 1st year
university
diagnosed
with MS after
having L optic
neuritis
Abnormal MRI; >9
T2 lesions on brain
MRI and spinal cord
lesion at C5
2000 2001
clumsy
left
hand
pins &
needles
in legs
IFN-beta
2002 2003
R optic
neuritis
2004
Bladder dysfunction
Graduate
trainee
marketing
Full
time
employment
Off work
~3 months
of the year
Dec 2007
Brainstem
syndrome;
diplopia
and ataxia
? glatiramer
acetate
Cervical cord
relapse
weak L arm
with pain
High lesion
load with
brain
atrophy
Gd-enhancing
lesion of upper
cervical cord
Splits from
her partner
depression ,
anxiety and fatigue
Reduced mobility
Occupational
health
assessment
natalizumab
New
partner
New job
junior management
position
Residual deficits:
Normal walking 300m, unable to run &
exercise. Intermittent sensory symptoms
in L arm. Mild urinary frequency
Jan 2008
JCV
positive
3-monthly MRI
monitoring
? fingolimod
Oct 2013
Annual MRI
monitoring
JCV
high positive
Final
year of
school
University
Early or late?
21
Mo
nito
rin
g
Tre
atm
ent
Clin
ica
l O
ccu
p &
so
cia
l
Dec 2007 Jul 2010 Jul 2013

MS is an iceberg?
Clinical
MRI
Pathology

Pathogenic markers

“Inflammation”
“Oligodendrocyte Toxicity & Demyelination”
Axonal Toxicity (conduction block)
Axonal & Neuronal Loss
Gliosis
Remyelination & Axonal Recovery
“Inflammation”
Central Adaptation & Plasticity
Key pathological processes in MS

The Shredder - 11,000 to 1
Trapp, et al. NEJM 1998;338:278-85

Petzold, J Neurol Sci. 2005 Jun 15;233(1-2):183-98.


Petzold et al. J Neurol Neurosurg Psychiatry. 2005 Feb;76(2):206-11.
Spinal fluid neurofilament levels

Neurofilament protein in cerebrospinal fluid: a potential marker of activity in multiple sclerosis
Lyke et al. J Neurol Neurosurg Psychiatry 1998;64:402–404.

Petzold et al. J Neurol Neurosurg Psychiatry. 2005 Feb;76(2):206-11.
Spinal fluid neurofilament levels

Axonal damage in R-MS is markedly reduced by Natalizumab
Gunnarsson et al. Ann Neurol 2010; Epub.

-1.0%
-0.8%
-0.6%
-0.4%
-0.2%
0.0% Years 0-2
-0.82%
-0.80%
P=0.822†
Placebo (N=315) Natalizumab (N=627)
Year 0-1* Year 1-2
-0.40%
-0.56%
-0.43%
-0.24%
P=0.004†
P=0.002†
†Difference between treatments; ‡Change from baseline; Miller DH et al. Neurology 2007;68:1390-1401.
AFFIRM Study: natalizumab and brain atrophy
Mean
(S
E)
perc
en
tag
e c
han
ge i
n B
PF

Natalizumab treatment of progressive multiple sclerosis reduces
inflammation and tissue damage
- results of a phase 2A proof-of-concept study
ClinicalTrials.gov Identifier: NCT01077466
J. Romme Christensen1, R. Ratzer1, L. Börnsen1, E. Garde2, M. Lyksborg2, H.R. Siebner2, T.B. Dyrby2, P. Soelberg Sørensen1 and F. Sellebjerg1

Natalizumab treatment of progressive MS reduces inflammation and tissue damage: CSF markers of axonal damage
Romme Christensen et al. ECTRIMS 2012.

Bas
elin
e
Follow-u
p
0
500
1000
1500
2000
2500
NfL
(p
g/m
l)
Cerebrospinal fluid NfL Fingolimod 0.5mg/1.25 mg versus placebo treated patients
p<0.001
Fingolimod, n=23 Placebo, n=12
p=0.470
Fingolimod 0.5 mg Fingolimod 1.25 mg
Baseline Follow-up Baseline Follow-up
Median (pg/ml)
644 321 (-50%) 886 738 (-17%)
*Non-parametric Wilcoxon matched pairs test; p value is calculated with inclusion of outliers Dr Jens Khule, ECTRIMS 2013
0
1000
2000
10000
NfL
(p
g/m
l)

Fingolimod has an early and sustained effect on the rate of brain atrophy compared with placebo and IFNb-1a IM
FREEDOMS, 2 years
Fingolimod 0.5 mg (n = 356)
Placebo (n = 329)
***
*
**
6 0 12 24
Time (months)
0
-0.4
-0.8
-1.2
-1.6
-2.0
−38%
vs placebo p<0.001
Ch
ange
in m
ean
BV
fro
m
bas
elin
e (%
)
TRANSFORMS, 1 year
0 12
Time (months)
0.0
-0.4
-0.6
-1.0
IFNb-1a IM (n = 359)
Fingolimod 0.5 mg (n = 368)
−40%
vs IFNb-1a IM p<0.001
*** -0.2
-0.8
Ch
ange
in m
ean
BV
fro
m
bas
elin
e (%
)
ITT population with evaluable MRI images. Note: n numbers for FREEDOMS data reflect the number of patients with available data at 24 months. *p<0.05; **p<0.01; ***p<0.001 vs comparator; p-values are for comparisons over Months 0-6, Months 0-12, Months 0-24 BV, brain volume; ITT, intent-to-treat. Gilenya™ Prescribing Information 19 April 2012. Reproduced with permission. Kappos L et al. N Engl J Med 2010; 362: 387-401, and Cohen JA et al. N Engl J Med 2010; 362: 402-415. Copyright © 2011 Massachusetts Medical Society. All rights reserved

Coles et al. J Neurol. 2006 Jan;253(1):98-108.
Post-inflammatory neurodegeneration

Axonal damage in R-MS is markedly reduced by Natalizumab
Gunnarsson et al. Ann Neurol 2010; Epub.

Gunnarsson et al. Ann Neurol 2010; Epub.
CSF NFL

Active tablet
Placebo tablet
Year 1 Year 2 Year 3
600 MSers
300 MSers
300 MSers

Recruitment Trial Data analysis
6 months
6 months 60 MSers
6 months
LP1 LP2 LP3
30 MSers active tablet
30 MSers placebo tablet
2 years
6 months

600 MSers for 7 years 60 MSers for 2 years
3 LPs = 10x as many trials in a ⅓ of the time


13%
66%
21%
n = 127

MRI Events
1st clinical attack
Time (Years)
Subclinical disease
Inflammation
Brain volume loss
Neuroaxonal loss
Dis
eas
e S
eve
rity
SPMS RRMS
1st MRI lesion
Relapses
CIS RIS R-SPMS
RIS = radiologically isolated syndrome; CIS = clinically isolated syndrome, RRMS = relapsing-remitting MS; R-SPMS = relapsing secondary progressive MS; SPMS = secondary progressive MS; PPMS = primary progressive MS
SPMS: Natalizumab, Siponimod
Late SPMS: SMART STUDY ibudilast, amiloride, riluzole
Early SPMS: PROXIMUS oxcarbazepine
CIS: PHENYTOIN RRMS: ? DE-FLAMES STUDY
PPMS
PPMS: Fingolimod, Ocrelizumab, Laquinimod

Brain atrophy occurs across all stages of the disease
De Stefano, et al. Neurology 2010
n= 963 MSers

MRI Events
1st clinical attack
Time (Years)
Subclinical disease
Inflammation
Brain volume loss
Neuroaxonal loss
Dis
eas
e S
eve
rity
SPMS RRMS
1st MRI lesion
Relapses
CIS RIS R-SPMS
RIS = radiologically isolated syndrome; CIS = clinically isolated syndrome, RRMS = relapsing-remitting MS; R-SPMS = relapsing secondary progressive MS; SPMS = secondary progressive MS; PPMS = primary progressive MS
SPMS: Natalizumab, Siponimod
Late SPMS: SMART STUDY ibudilast, amiloride, riluzole
Early SPMS: PROXIMUS oxcarbazepine
CIS: PHENYTOIN RRMS: ? DE-FLAMES STUDY
PPMS
PPMS: Fingolimod, Ocrelizumab, Laquinimod

Tur et al. Interferon Beta-1b for the Treatment of Primary Progressive Multiple Sclerosis: Five-Year Clinical Trial Follow-up. Arch Neurol. 2011 Nov;68(11):1421-7.
Therapeutic Lag

Motor system to legs
Cerebellar or balance systems
Bladder Therapeutic window 1
Therapeutic window 2
Therapeutic window 3
Upper limbs
Sensory
Cognition
Vision
Etc.
Therapeutic window 4
Therapeutic window 5
Therapeutic window 6
Therapeutic window 7
Therapeutic window 8, etc….
Diagnosis of Progressive MS
Effective DMTs could still target the remaining windows of therapeutic opportunity for individual neurological
systems
The Asynchronous Progressive MS hypothesis

Control Multiple sclerosis
End-organ damage

750
800
850
900
950
1000
1050
1100
1150
1200
1250
1300
1350
1400
1450
1500
30 35 40 45 50 55 60 65 70 75 80
Bra
in V
olu
me
(m
L)
Age (years)
Brain atrophy curves
Lower limit of normal
Average
Upper limit of normal
Hypothetical treatment effects

750
800
850
900
950
1000
1050
1100
1150
1200
1250
1300
1350
1400
1450
1500
30 35 40 45 50 55 60 65 70 75 80
Bra
in V
olu
me
(m
L)
Age (years)
Brain atrophy curves
MS lower limit
MS Average
MS Upper limit
-5%
-30%
Hypothetical treatment effects

-5%
-30%
750
800
850
900
950
1000
1050
1100
1150
1200
1250
1300
1350
1400
1450
1500
30 35 40 45 50 55 60 65 70 75 80
Bra
in V
olu
me
(m
L)
Age (years)
Brain atrophy curves
MS Average
Hypothetical treatment effects

-5%
-20%
750
800
850
900
950
1000
1050
1100
1150
1200
1250
1300
1350
1400
1450
1500
30 35 40 45 50 55 60 65 70 75 80
Bra
in V
olu
me
(m
L)
Age (years)
Brain atrophy curves
late treatment
Hypothetical treatment effects

750
800
850
900
950
1000
1050
1100
1150
1200
1250
1300
1350
1400
1450
1500
30 35 40 45 50 55 60 65 70 75 80
Bra
in V
olu
me
(m
L)
Age (years)
Brain atrophy curves
-5%
-18%
early treatment
late treatment
Hypothetical treatment effects

750
800
850
900
950
1000
1050
1100
1150
1200
1250
1300
1350
1400
1450
1500
30 35 40 45 50 55 60 65 70 75 80
Bra
in V
olu
me
(m
L)
Age (years)
Brain atrophy curves
-5% -11%
early very
highly-effective
treatment
late very
highly-effective
treatment
-15%
Hypothetical treatment effects

NEDA
Gd, gadolinium. 1. Havrdova E, et al. Lancet Neurol 2009; 8:254–260; 2. Giovannoni G, et al. Lancet Neurol 2011; 10:329–337.
Treat-2-target
Brain volume loss and CSF neurofilament levels should be included in our definition for NEDA
No evidence of disease activity defined as:1,2
× No relapses
× No sustained disability progression
× No MRI activity
× No new or enlarging T2 lesions
× No Gd-enhancing lesions

Conclusions
• MS is a bad disease • Mortality, disability, unemployment, divorce, cognitive impairment, etc.
• Early highly-effective therapy is the only realistic option of preventing end-organ damage • Now an established treatment option in the EU
• NEDA (DAF) and T2T are entering the neurology lexicon
• Zero tolerance or ZeTo
• We need an acceptable working definition of an MS cure • NEDA x 15 years?
• Only possible with induction therapies (alemtuzumab, cladribine, BMT, ? anti-CD20)
• Is it fair to make people with MS wait 20 years for the outcome of an ongoing experiment?

Acknowledgements
• Giovannoni
• Sharmilee Gnanapavan
• David Baker
• Gareth Pryce
• Sarah Al-Izki
• Sam Jackson
• Katie Lidster
• Yuti Chernajovsky
• Alex Annenkov
• Anne Rigby
• Michelle Sclanders
• Larry Steinman
• Peggy Ho
• Charles ffrench-Constant • Robin Franklin
• Siddharthan Chandran • David Hampton
• Ian Duncan • Sam Jackson
• Peter Calabresi • Avi Nath
• Raj Kapoor • John Zajicek • Doug Brown • UK MS Clinical Trial Network • BioMS
• Co-investigators
• NABINMS • Affirm study • Care MS 1 & 2 studies • Select trial