Embed Size (px)
Citation preview

Department of medical physiology
Semester: winterStudy program: Sleep medicineLecture: RNDr. Soňa Grešová, PhD.Department of medical physiologyFaculty of Medicine PJŠU

Department of medical physiology
1. Regulation of the respiratory activity
2. Sleep disorders breathing
3. PSG parameters
4. PSG record

1. Regulation of the respiratory activity
• 4 control mechanisms play a role in the regulation of breathing disorders and theircompensation :
1. neural mechanisms of brainstem
2. chemical control
3. reflex mechanisms
4. voluntary respiration

1. Regulation of the respiratory activity
• Respiratory centers located in the medulla, where there are two groups of neurons:
• Dorsal respiratory group
- The apneustic center
- Pneumotaxic center
• The ventral respiratory group
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

• composed only of inspiratory neurons (PACEMAKER). Is the switching station of many respiratory reflexes. The activity of this group is transferred to the main breathing muscle (C3,C4,C5-diaphragm), ex.intercostalmuscles.
• Ondine´s curse
1. Regulation of the respiratory activityDorsal respiratory group
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

1. Regulation of the respiratory activityDorsal respiratory group
• Sets the basic respiratory rate.
• Stimulates the inspiratory muscles to contract (diaphragm).
• The signals it sends for inspiration start weakly and steadily increase for ~ 2 sec. This is called a rampand produces a gradual inspiration.
• The ramp then stops abruptly for ~ 3 sec and the diaphragm relaxes.
The vagus nerve and glossopharyngealnerves receive input from:
• Peripheral chemoreceptors
• Baroreceptors
• Several pulmonary receptors Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

1. Regulation of the respiratory activityThe apneustic center
Located in the lower pons.• Excitatory to DRG which
prevents the SWITCH OFF of the ramp signal .
• Therefore activity in the apneustic center stimulates DRG or Inspiratory Center and causes Apneusis.
• Apneusis is a prolonged inspiratory spasm that resembles breath holding.
• Inhibited by signals from Pneumotaxic centre & by Vagus
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

1. Regulation of the respiratory activityPneumotaxic center
• Controls stopping point of the dorsal group ramp.
• SWITCH OFF centre of inspiratory neurons(PACEMAKER)
• Strong pneumotaxicstimulation shortens the duration of inspiration and expiration.
• Weak pneumotaxicstimulation can increaseand prolong the duration of inspiration
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

1. Regulation of the respiratory activityVentral respiratory group
• Composed of inspiratory and expiratory neurons. Provide motor innervation of accessory respiratory muscles.
• Inactive during normal, quiet respiration.
• At times of increased ventilation, signals from the dorsal group stimulate the ventral group.
• The ventral group then stimulates both inspiratory and expiratory muscles. E.g., the abdominal muscles are stimulated to contract and help force expiration.
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

1. Regulation of the respiratory activity2. chemical control
• Chemical control of respiration.
• Importance: It adjusts ventilation so as to maintain the arterial PO2,PCO2and H+ concentration in the normal range.
• The Respiratory Center stimulated by-1. Hypoxia - Fall in arterial PO22.Acidosis- Fall in pH or increase H+ concentration of arterial blood.3. Hypercapnia -Rise in arterial PCO2 .
• Mediated through the Chemoreceptors.

1. Regulation of the respiratory activity2. chemical control. Central chemoreceptors
• In the chemosensitive areas of the respiratory center(ventrolateral area), increased H+
is the main stimulus.
• The blood-brain barrier is not very permeable to H+; however, CO2 easily diffuses across the BBB.
• Increases in CO2 cause increases in H+.
• CO2 diffuses into the chemosensitive regions of the CNS, H+ is formed and stimulates the dorsal group and thus increase the respiration rate.

1. Regulation of the respiratory activity2. chemical control. Peripheral chemoreceptors
• Peripheral chemoreceptors are located in carotid and aortic bodies and sense the level of O2 (PO2), low sense the level of H+ (independent of CO2 level) and PCO2
• Blood flow to the receptors is very high; so very little deoxygenated (venous) blood accumulates.
• Low PO2 levels stimulates the dorsal respiratory group(PO2 < 60mmHg). K dependent-AP,neurotransmitter – Dopamin.
• The signal is sent to the respiratory center DRG via the vagus (X.) or glossopharyngeal nerve (IX) increase ventilation.
Copyright: https://quizlet.com/19158008/respiratory-physiology-flash-cards/

1. Regulation of the respiratory activity3. reflex mechanisms. Pulmonary Stretch Receptors:
• Over inflation of lung will stimulate stretch receptors located in the smooth muscle of the airways via vagi (X.) inhibit DRG -(Expiration occur) Hering-Breuer Inflation Reflex
• Protective mechanism for preventing excess lung inflation
• Threshold for this reflex is 1-1.5 L of Tidal volume

1. Regulation of the respiratory activity3. reflex mechanisms. J Receptors
• Present between alveolar wall and the pulmonary capillary.(Juxta-capillary)
• Stimulated by pulmonary edema fluid alveolus),
exercise, between capillary an inhalation of irritant gases etc.
• Stimulation of J receptors causes tachypnoea that is rapid shallow respiration.
Copyright: http://www.emsworld.com/article/10263561/regulation-of-ventilation

1. Regulation of the respiratory activity3. reflex mechanisms. Irritant receptors
• Irritant receptors are myelinated vagal afferent nerve endings which are located in the large airways like trachea up to respiratory bronchiole.
• Stimulation: The irritant receptors are stimulated by
smoke, chemicals, or mechanical irritants.
• They produce reflex coughing, rapid shallow breathing, bronchial constriction and breath holding.

1. Regulation of the respiratory activity3. reflex mechanisms. Other receptors cooperating with the respiratory center
Role of afferents from higher centers.
• Painful stimuli, emotional stimuli affect respiration. The afferents are from the limbic system and the hypothalamus to the respiratory neurons.
Role of afferents from proprioceptors.
• During muscular exercise proprioceptors presents in muscles tendons and joints send afferent impulses to the DRG and stimulate respiration. Respiratory rate increase in muscular exercise.
Role of arterial baroreceptor stimulation on respiration
• Afferent stimulation from carotid sinus baroreceptors (caused by increase blood pressure) inhibits DRG and causes Apnea. Other effects of baroreceptor stimulation are hypotension and bradycardia.

1. Regulation of the respiratory activity4. voluntary respiration
• It originates in the cerebral cortex and sends impulses to the nerves of the respiratory muscles via the corticospinaltracts. In addition, ingoing impulses from many parts of the body modify the activity of the respiratory centers and consequently alter the outgoing impulses to the respiratory muscles to coordinate rhythm, rate or depth of breathing with other activities of the body.
• Emotional stimuly actingthrough the limbic system and hypothalamus.
Copyright: http://intranet.tdmu.edu.ua/data/kafedra/internal/normal_phiz/classes_stud/en/med/lik/2%20course/4%20Cycle%20Physiology%20of%20breathing/02%20%20Regulation%20of%20breathing.htm

2. Sleep disorders breathing
• Central breathing disorders
– lack of respiratory effort caused by either a central nervous disorder or cardiac dysfunction
• Obstructive breathing disorders
– Obstruction, usually in the upper airway, and often associated with obesity, large tongue, tonsils, or adenoids, or inflamed tissue in the upper airway

2. Sleep disorders breathingObstructive sleep apnea
• Obstructive apneas
– the decrease in airflow at least 90% in amplitude with duration min. 10s
• Hypopneas
– the decrease in airflow is 30-90% in amplitude with duration min. 10s
• EEG arousals
• Oxygen desaturation

2. Sleep disorders breathingObstructive sleep apnea

2. Sleep disorders breathingObstructive sleep apnea

2. Sleep disorders breathingHypopnea

2. Sleep disorders breathingCentral sleep apnea
• Central apneas
– the decrease in airflow at least 90% in amplitude with duration min. 10s
– Repeated cessation of airflow and concurrent cessation of respiratory effort
• EEG arousals
• Oxygen desaturation

2. Sleep disorders breathingCentral sleep apnea

2. Sleep disorders breathingCentral sleep apnea

3. PSG parameters
• EEG
• EOG
• ECG
• EMG
• Flow
• Thorax
• Abdomen
• SpO2

3. PSG parameters. EEG

3. PSG parameters. EOG

3. PSG parameters. EMG

3. PSG parameters. EMG

3. PSG parameters. Snore sensor

3. PSG parameters. Respiratory belt

Types of sleep
1. SWS (Slow-Wave Sleep),• in this type of sleep the brain waves are very
strong and very low frequency
• It is also called Non-Rapid Eye Movement (NREM) sleep it is not associated with rapid eye movements
2. REM sleep (Rapid Eye Movement ),– in this type of sleep the eyes undergo rapid
movements despite the fact that the person is still asleep

NREM sleep (SWS)• is divided into 4 stages :1. Stage 1 NREM
– when a person is initially falling asleep. Characterized by low-amplitude, fast activity
2. Stage 2 NREM – Marked by appearance of Sleep
Spindles. These are bursts of alpha-like 8-13 cycles per second , 50 µV waves
3. Stage 3 NREM – Lower frequency (mainly theta),
higher amplitude EEG waves 4. Stage 4 NREM
– Still slower frequency (mainly delta) & still higher amplitude waves

REM sleep1. Associated with active dreaming and active bodily muscle movements
2. more difficult to arouse by sensory stimuli than during deep slow-wave sleep,
and yet people usually awaken spontaneously in the morning during an episode of
REM sleep.
3. Muscle tone throughout the body is exceedingly depressed, indicating strong
inhibition of the spinal muscle control areas.
4. Heart rate and respiratory rate usually become irregular, which is characteristic of
the dream state.
5. Despite the extreme inhibition of the peripheral muscles, irregular muscle
movements do occur. These are in addition to the rapid movements of the eyes.
6. The brain is highly active in REM sleep, and overall brain metabolism may be
increased as much as 20 per cent. The electroencephalogram (EEG) shows a
pattern of brain waves similar to those that occur during wakefulness.
This type of sleep is also called paradoxical sleep because it is a paradox that aperson can still be asleep despite marked activity in the brain

4. PSG recordAlpha waves (8-13Hz)-EEG arousals
Theta waves (4-7Hz)-N1, N2 and REM
Sleep spindles (11-16Hz)-N2
K-Complex : sharp neg. wave followed slower positive component-N2
Slow waves (0.2-2Hz) amplitude 75 μV- N3

4. PSG recordStage Wake

4. PSG recordStage N1

4. PSG recordStage N2

4. PSG recordStage N3

4. PSG recordStage REM

4. PSG recordEMG

4. PSG recordSpO2

4. PSG recordObstructive apnea

4. PSG recordObstructive apnea
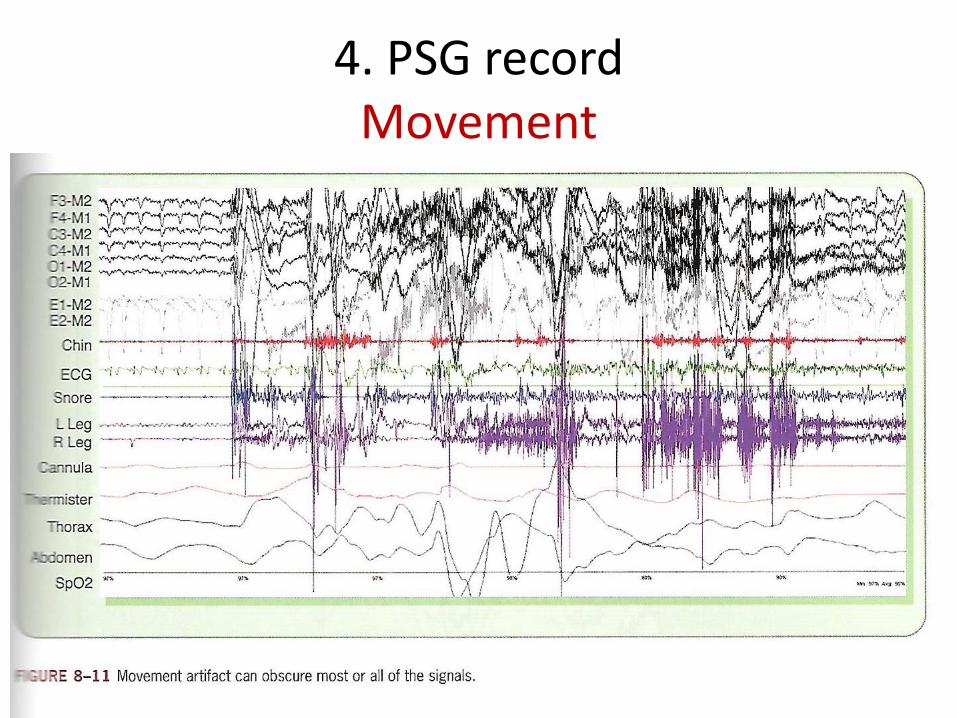
4. PSG recordMovement

4. PSG recordCentral apnea

4. PSG recordMixed apnea

Department of medical physiology
Semester: winterStudy program: Sleep medicineLecture: RNDr. Soňa Grešová, PhD.Department of medical physiologyFaculty of Medicine PJŠU

Department of medical physiology
1. Epidemiology, pathogenesis of sleep disordered breathing (SDB), predisposition factors, metabolic complications, diabetes 1,2 type. Their diagnostic and therapy
2. Cardiovascular complications (hypertension, arrhythmias, sudden cardiac death). Their diagnostic, prevention and therapy

1. Sleep Related Breathing Disorders
• are characterized by abnormalities of respiration during sleep
• Obstructive sleep apnea (OSA) disorders,
• Central sleep apnea disorders,
• Sleep related hypoventilation disorders,
• Sleep related hypoxemia disorder.

1. Sleep Related Breathing Disorders
• The AASM Manual forthe Scoring of Sleep and Associated Eventsincludes different scoringrules for adult and pediatric individuals, definitions of obstructiveand central apneas and hypopneas, and rules forscoring Cheyne-Stokesbreathing and hypoventilation

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• are characterized by upper airway narrowing or closure during sleep while respiratory effort continues (at least during some portion of the event)

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Diagnostic Criteria - the presence of one or more of the following:
1. The patient complains of sleepiness, nonrestorative sleep, fatigue, or insomnia symptoms
2. The patient wakes with breath holding, gasping, or choking
3. The bed partner or other observer reports habitual snoring, breathing interruptions, or both during the patient’s sleep
4. The patient has been diagnosed with hypertension, a mood disorder, cognitive dysfunction, coronary artery disease, stroke, congestive heart failure, atrial fibrillation, or type 2 diabetes mellitus

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Diagnostic Criteria - Polysomnography(PSG) or OCST demonstrates:
1. Five or more predominantly obstructive respiratory events (obstructive and mixed apneas, hypopneas, or respiratory effort related arousals [RERAs]) per hour of sleep during a PSG or per hour of monitoring Out of center sleep testing (OCST)
OR1. Fifteen or more predominantly obstructive
respiratory events (apneas, hypopneas, or RERAs) per hour of sleep during a PSG or per hourof monitoring (OCST)

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Essential Features• OSA is characterized by repetitive episodes of complete (apnea) or partial (hypopnea)
(minimum of 10s) upper airway obstruction occurring during sleep
• These events often result in reductions in blood oxygen saturation and are usually terminated by brief arousals from sleep
• Events can occur in any stage of sleep but more frequently occur in stages N1, N2, and R sleep than in stage N3 sleep
• Events are usually longer and associated with more severe decreases in oxygen saturation when they occur in stage R sleep and when the individual is sleeping supine
• Bad partners – disrupt sleep
• Most patients awaken in the morning feeling tired and unrefreshed regardless of the duration of their time in bed
• Apneas, hypopneas, and snoring may be exacerbated following the ingestion of alcohol, use of sedating medications prior to sleep, or following an increase in body weight
• Excessive sleepiness is most evident during relaxing or inactive situations
• With extreme sleepiness, sleep may occur while actively conversing, eating, walking, or driving
• In some cases, affected individuals will not endorse any symptoms or confirm any bed partner observations

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Associated Features
• Systemic hypertension is a common finding in patients with OSA
• OSA is frequently observed in patients with coronary artery disease, atrial fibrillation, and stroke, and it may be an independent risk factor for these conditions.
• OSA is also associated with type 2 diabetes, and there are accumulating data to suggest that it is a risk factor for the development of type 2 diabetes.
• Patients with severe disease may be at risk for developing pulmonary hypertension and cor pulmonale (patients with daytime hypercapnia due to comorbid conditions such as morbid obesity or chronic obstructive pulmonary disease (COPD).
• When OSA coexists with dilated cardiomyopathy or ischemic heart disease, there may be worsening of the underlying heart disease and predisposition to congestive heart failure
• Gastroesophageal reflux symptoms, nocturia, mood disturbance, and erectile dysfunction are sometimes reported in patients with OSA

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Clinical and Pathophysiological Subtypes
• Apneas and hypopneas are believed to have similar pathophysiology and consequences
• COPD and OSA frequently coexist, but there is no common pathophysiologic relationship

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Demographics• OSA associated with daytime sleepiness occurs in 3% to 7% of
adult men and 2% to 5% of adult women
• The prevalence of OSA increases with age, although it appears to plateau in the elderly
• OSA occurs in all racial and ethnic groups
• In younger and elderly groups, but not in middle-aged groups, OSA has been reported to be more prevalent in blacks than whites.
• The prevalence of OSA in Asian patients is comparable to that of whites, despite having a generally lower body mass index (BMI). Differences in craniofacial features that predispose Asians to developing OSA are the likely explanation

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Predisposing and Precipitating Factors• The major predisposing factor for OSA is excess body weight
• upper airway obstruction due to a localized structural abnormality such as a maxillomandibular malformation or adenotonsillar enlargement
• Increasing neck circumference predicts higher AHIs; it is not, however, independent of BMI
• Menopause is a risk factor for this disorder in women, even after adjustment for age and BMI
• There are conflicting data concerning smoking as a risk factor for OSA
• Various abnormalities of the bony and soft tissue structures of the head and neck may predispose the individual to having OSA
• Endocrine disorders such as acromegaly and hypothyroidism are risk factors for OSA
• Adults and children with Down syndrome also have a high prevalence of OSA.
• OSA is common in patients with some neurologic disorders that affect peripheral muscles, such as myotonic dystrophy.
• OSA is likely made worse following alcohol consumption or use of sedating medications before sleep and by nocturnal nasal restriction or congestion due to abnormal morphology, rhinitis, or both

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Familial Patterns• OSA is a heritable condition as demonstrated by familial clustering of OSA
patients. First-degree relatives of OSA patients are twice as likely to have OSA in comparison to those not affected. Clustering of symptoms that are associated with OSA such as snoring, daytime sleepiness, and snorting or gasping also occurs.
• Heritability explains approximately one third of the variation in the AHI, with a substantial proportion of the heritability explained by obesity.
• Other inherited traits that might predispose an individual to developing OSA include craniofacial morphology and ventilatory control.
• Familial environmental factors such as physical activity and eating habits may play a role as well. Nevertheless, genetic studies to date have not identified a unique gene or genes responsible for OSA heritability.

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Onset, Course, and Complications• OSA becomes more severe in patients whose BMI
increases, but may improve with weight reduction• Substantial evidence implicates OSA as a risk factor for
incident systemic hypertension, coronary artery disease, congestive heart failure, stroke, and premature mortality
• OSA is a risk factor for the development of type 2 diabetes mellitus independent of obesity
• Evidence suggests that OSA is particularly related to the onset and recurrence of atrial fibrillation
• OSA may increase the severity of depression

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Developmental Issues
• OSA can occur in any age group, but in adults, prevalence accelerates between young adulthood and middle age, with a plateau reached after approximately age 65 years
• OSA occurs in the elderly, it is commonly observed with few symptoms

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Pathology and Pathophysiology• The pathophysiology underlying upper airway narrowing during sleep is
multifactorial e.g. (tongue, soft palate, and lateral pharyngeal walls)• In persons with OSA, the activity of the pharyngeal dilating muscles
becomes insufficient to prevent narrowing and/or closure of the upper airway
• There is a further reduction in tone and phasic activity of pharyngeal dilating muscles during REM sleep, particularly in phasic REM, which likely contributes to apneas and hypopneas that are longer and more pronounced- event termination may occur with or without an associated arousal
• sleep fragmentation from arousals is nevertheless believed to be a significant cause of excessive daytime sleepiness
• Apneas and hypopneas typically last considerably longer in REM and, in some patients, are only present in this sleep stage

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Pathology and Pathophysiology
• Accumulating evidence indicates that persons with OSA have elevated levels of circulating inflammatory mediators related to repetitive episodes of oxygen desaturation and increased sympathetic nervous system activity.
• Both of these findings may be important in the pathogenesis of hypertension and cardiovascular disease related to OSA.

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Objective Findings
• Obstructive apneas are documented by a cessation of airflow with ongoing respiratory efforts during PSG or an OCST
• When breathing effort is recorded, it typically shows paradoxical movement of the rib cage and abdomen
• Oxygen saturation typically declines for a variable period of time following the onset of an event (apnea or hypopnea), with the nadir usually occurring after normal breathing resumes
• RERAs -These events are presumed to have the same underlying pathophysiology as obstructive apneas and hypopneas (upper airway obstruction) and are considered to be as much of a risk factor for symptoms of unrefreshing sleep, daytime somnolence, and fatigue as frank apnea or hypopnea

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders

1. Sleep Related Breathing DisordersHypopnea

1. Sleep Related Breathing DisordersObstructive sleep apnea (OSA) disorders
• Differential Diagnosis
• Patients with central sleep apnea have predominantly central ratherthan obstructive apneas, hypopneas, or RERAs as the primaryfinding on PSG or OCST. If mixed apneas are predominant, a diagnosis of OSA should be made
• Patients with obesity hypoventilation syndrome will demonstratedaytime hypercapnia. Snoring may not be a prominent feature, although daytime sleepiness can occur.
• Patients with sleep related hypoventilation disorders may show episodes of oxygen desaturation without evidence of airflowobstruction on PSG or OCST
• OSA must be differentiated from other causes of sleepiness suchas narcolepsy, idiopathic hypersomnia, and insufficient sleep

1. Sleep Related Breathing DisordersCentral sleep apnea disorders
1. Central Sleep Apnea with Cheyne-Stokes Breathing2. Central Apnea Due to a Medical Disorder without
Cheyne-Stokes Breathing3. Central Sleep Apnea Due to High Altitude Periodic
Breathing4. Central Sleep Apnea Due to a Medication or
Substance5. Primary Central Sleep Apnea6. Primary Central Sleep Apnea of Infancy7. Primary Central Sleep Apnea of Prematurity8. Treatment-Emergent Central Sleep Apnea

1. Sleep Related Breathing DisordersCentral sleep apnea disorders
• are characterized by reduction or cessation of airflow due to absent or reduced respiratory effort
• central apnea or hypopnea may occur in a cyclical or intermittent fashion
• patients with central sleep apnea of various etiologies may also exhibit OSA

1. Sleep Related Breathing DisordersCentral sleep apnea disorders
1. Central Sleep Apnea with Cheyne-Stokes Breathing
• CSA-CSB is characterized by recurrent central apneas or central hypopneasalternating with a respiratory phase exhibiting a crescendo-decrescendo pattern of flow (or tidal volume)
• The vast majority of patients with CSA-CSB have either systolic or diastolicheart failure
• Patients with CSA-CSB have normal or low daytime arterial PCO2 (PaCO2)
• A diagnosis of CSA-CSB requires that events be predominantly centralapneas and hypopneas with an average frequency of at least 5/hourduring a diagnostic PSG
• In patient with CSA-CSB, arousal from sleep tends to occur at the zenith of respiratory effort between contiguous central apneas or hypopneas
• patients may complain of disturbed nocturnal sleep or nocturnal dyspnearather than daytime sleepiness

1. Sleep Related Breathing DisordersCentral sleep apnea disorders
1. Central Sleep Apnea with Cheyne-StokesBreathing
• studies have shown that approximately 60% of patients with heart failure have some form of sleep apnea, a high index of suspicion isindicated
• CSA-CSB can rarely present in an idiopathicform or be associated with renal failure

1. Sleep Related Breathing DisordersCentral sleep apnea disorders
1. Central Sleep Apnea with Cheyne-Stokes Breathing
• As in other forms of CSA, apneas and hypopneas are associated with absent or reduced ventilatory effort, respectively, due to diminished central respiratorydrive.
• Of interest, a longer respiratory phase between apneasis associated with a longer circulation time and delay in the saturation nadir.
• The CSB breathing pattern is characteristically observedduring stages N1 and N2 and usually resolves or isattenuated during REM sleep

1. Sleep Related Breathing DisordersCentral sleep apnea disorders

1. Sleep Related Breathing DisordersCentral Sleep Apnea with Cheyne-Stokes Breathing

1. Sleep Related Breathing DisordersCentral sleep apnea disorders
1. Central Sleep Apnea with Cheyne-Stokes Breathing• Some patients have combined OSA and CSA, and the CSA-
CSB may not manifest until the patient is placed on positiveairway pressure treatment
• CSA with CSB generally is seen in subjects older than 60 years
• The prevalence of this breathing disorder in the setting of chronic congestive heart failure has been reported to be25% to 40%, depending on how patients are divided intothose with predominant OSA and those with CSA
• Some form of sleep apnea is reported in 50% to 70% of patients following stroke, depending on the AHI cutoff usedfor diagnosis

1. Sleep Related Breathing DisordersCentral sleep apnea disorders
1. Central Sleep Apnea with Cheyne-Stokes Breathing
• The most important predisposing factors are thepresence of congestive heart failure, stroke, and possibly renal failure.
• Within the heart failure population, risk factors for CSB pattern during sleep include male sex, age older than60 years, the presence of atrial fibrillation, and daytimehypocapnia (i.e., awake PaCO2 of 38 mm Hg or less).
• In general, greater pulmonary congestion (higher leftventricular end-diastolic pressure) predicts lowerPaCO2

1. Sleep Related Breathing DisordersCentral sleep apnea disorders
1. Central Sleep Apnea with Cheyne-Stokes Breathing• Pathology and Pathophysiology• CSA with CSB generally arises because of instability in the
respiratory control system. A high ventilatory drive and delay in chemoreceptor response to changes of PaCO2 and PaO2 (due to increased circulation time) are likely the major factors
• Hyperventilation occurs due to an increase in the responsiveness of the peripheral and central chemoreceptors.
• The increased responsiveness is believed to be due to bothincreased sympathetic tone and stimulation of vagal irritantreceptors in the lungs by pulmonary congestion
• The most common trigger factor for central apnea is an arousalfrom sleep, which abruptly augments ventilation and drives PaCO2 below the apneic threshold

Sleep Related Breathing DisordersSleep related hypoventilation disorders
1. Obesity Hypoventilation Syndrome2. Congenital Central Alveolar Hypoventilation
Syndrome3. Late-Onset Central Hypoventilation with
Hypothalamic Dysfunction4. Idiopathic Central Alveolar Hypoventilation5. Sleep Related Hypoventilation Due to a
Medication or Substance6. Sleep Related Hypoventilation Due to a
Medical Disorder
Sleep Related Breathing DisordersSleep related hypoventilation disorders
• resulting in abnormally elevated arterial partial pressure of carbon dioxide (PaCO2) during sleep
• In addition, demonstration of daytime hypoventilation is required for a diagnosis of obesity hypoventilation syndrome (OHS)
• Awake hypoventilation is defined as an arterial partial pressure of carbon dioxide (PaCO2) greater than 45 mm Hg
• In the sleep related hypoventilation disorders other than OHS, daytime hypoventilation may or may not be present
• If hypoventilation is present during wakefulness, it worsens during sleep in all of these disorders
Sleep Related Breathing DisordersSleep Related Hypoxemia
• PSG, OCST or nocturnal oximetry shows the arterial oxygen saturation (SpO2) during sleep of ≤ 88% in adults or ≤ 90% in children for ≥ 5 minutes