-
Patient PreparationPrior to starting to take films, the patient
must be positioned properly. Seat the patient and ask them to
remove their glasses and any removable appliances. Adjust the
headrest to support the head while taking films. Raise or lower the
chair to a comfortable height for the operator. Place the lead
apron and thyroid collar on the patient. You are now ready to begin
taking films.
It is a good idea to inform the patient about the number of
films you will be taking so they know what to expect.
-
Bisecting Angle Technique
-
The Bisecting Angle Technique is an alternative to the
paralleling technique for taking periapical films. The paralleling
technique is recommended for routine periapical radiography, but
there are some instances when it is very difficult due to patient
anatomy or lack of cooperation. In these situations, the bisecting
angle technique may be used. The film can be held in the mouth with
the thumb or index finger or a bisecting instrument may be
used.
-
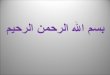
In the Bisecting Angle Technique, the x-ray beam is directed
perpendicular to an imaginary line which bisects (divides in half)
the angle formed by the long axis of the tooth and the long axis of
the film (see diagram below).X-ray beamLong axis of toothBisecting
lineLong axis of film
-
Bisecting Angle Technique (Advantages)When comparing the two
periapical techniques, the advantages of the bisecting angle
technique are: 1. More comfortable: because the film is placed in
the mouth at an angle to the long axis of the teeth, the film
doesnt impinge on the tissues as much. 2. A film holder, although
available, is not needed. Patients can hold the film in position
using a finger. 3. No anatomical restrictions: the film can be
angled to accommodate different anatomical situations using this
technique
-
Bisecting Angle Technique (Disadvantages)When comparing the two
periapical techniques, the disadvantages of the bisecting angle
technique are: 1. More distortion: because the film and teeth are
at an angle to each other (not parallel) the images will be
distorted (see next slide). 2. Harder to position x-ray beam: as
mentioned previously, because a film holder is often not used it is
difficult to visualize where the x-ray beam should be directed. 3.
Film less stable: using finger retention, the film has more chance
of moving during placement
-
In the bisecting technique, the long axis of the tooth is not
parallel with the long axis of the film. This results in a
distortion of the image produced using this technique. In the left
radiograph below, the buccal roots appear much shorter than the
palatal root, even though in the actual tooth the lengths are not
that much different. In the other radiograph taken with the
paralleling technique, the lengths are projected in their proper
relationship (minimal
distortion).Distortionbisectingparalleling
-
(head tipped back)Maxilla Mandible Head PositionWhen using a
bisecting instrument, head position is not critical. However, when
using finger retention, head position is important. When
radiographing the maxillary arch, the head should be positioned so
that the maxillary arch is parallel to the floor. For mandibular
films, the head is tipped back slightly so that the mandible is
parallel to the floor when the mouth is open . Make sure head is
supported by headrest. headrest
-
MSPfloorHead PositionWhen viewed from the front of the patient,
the Midsagittal Plane (which divides the head into right and left
halves) is perpendicular to the floor.
-
anteriorposteriorBisecting Angle TechniqueFilm Selection for
AdultsThe # 2 size film is routinely used for all periapical films
using the bisecting angle technique. The long axis of the film is
vertical for anterior films and horizontal for posterior
films.#2
-
#0#0anteriorposteriorBisecting Angle TechniqueFilm Selection for
ChildrenFor children with small mouths, the # 0 size film is used
for both anterior and posterior periapical films.
-
Anterior PeriapicalThe # 2 (or # 0) size film is positioned
vertically with the all-white side of the film facing the teeth.
The identifying dot is placed at the incisal edge of the teeth. The
thumb or finger is applied to the back (colored) side of the film .
The film should extend beyond the incisal edges of the teeth.
-
Posterior Periapical
-
Bisecting InstrumentThe Bisecting Angle Instrument is shown
below. Notice that the biteblock support, against which the film
will be aligned, is not parallel with the ring; it is slightly
angled to accommodate the bisecting technique. This slight tilt of
the film does little to make film placement more comfortable for
the patient over the paralleling technique; that is why finger
placement is recommended if the bisecting technique is
indicated.
-
Snap-A-RayAnother instrument that may be used for posterior
periapical films is the Snap-A-Ray shown below. The alligator jaws
hold the film tightly and, since there is no support behind the
film, the film can flex as the patient closes. This makes it more
comfortable for the patient.
-
When using finger placement, always use the hand opposite to the
side of the mouth being radiographed. (e.g., use the left index
finger when taking the right maxillary premolar film). Use either
thumb for the max. incisor film, the thumb or index finger
(opposite hand) for the maxillary canines, and the index finger for
all mandibular films and for the maxillary posterior films
(opposite hand). Help the patient by positioning their thumb or
finger where you want them to apply pressure.Finger Retention
-
Bisecting Angle Film PlacementThe film placements below are
appropriate for both maxillary and mandibular arches.
-
Using finger retention of the film, there is no external guide
to help you align the x-ray beam, as there is when using the
paralleling instrument. You have to imagine where the bisecting
line is and align the beam perpendicular to this line. This makes
the technique much more difficult, but with practice it can be a
beneficial adjunct to your radiographic technique.
When using this technique, keep in mind that all teeth incline
slightly toward the middle of the head; they are not straight
up-and-down. This will influence your visualization of the long
axis of the tooth and the angle it forms with the film.Vertical
Angulation
-
The x-ray beam is directed perpendicular to the bisecting line
shown below. You can see the film long axis, but you have to
visualize the inclination of the long axis of the tooth. Once you
determine the angle, imagine the bisecting line and direct the
x-ray beam at a 90-degree angle (perpendicular) to this line. This
is the vertical angulation. X-ray beamLong axis of toothBisecting
lineLong axis of film Vertical Angulation
-
In the diagram below, the tooth is imagined to be more upright
than it really is. As the tooth is rotated into its correct
inclination (click to rotate), the angle changes and the bisecting
line (green dotted line) is less steep, requiring an increased
vertical angulation (green arrow). Because most people imagine the
tooth to be more upright than it really is, it is recommended that
5 degrees be added to the vertical angulation you have
chosen.Vertical Angulation0
-
The horizontal angulation is adjusted so that a line connecting
the front and back edge of the PID (yellow line below) is parallel
with a line connecting the buccal surfaces of the premolars and
molars (green line below). The x-rays will then be perpendicular to
the film. Horizontal Angulation
-
For the anterior periapicals it is easy to see the sides of the
film and makes it easy to center the beam on the film side-to-side.
You then need to make sure the PID extends below the visible
(incisal) edge of the film (maxillary arch) or above the visible
edge (mandible). In the posterior region, the front edge of the PID
should be anterior to the front edge of the film and the PID should
extend beyond the visible (occlusal) edge of the film (above or
below, depending on which arch is being radiographed). These steps
will help to insure that the film is completely covered by the
x-ray beam, avoiding cone-cuts.Centering the Beam
-
Maxillary IncisorsThe film is held in place using the thumb of
either hand. The x-ray beam is directed perpendicular to the
bisecting line vertically and the horizontal angulation aligns the
x-ray beam perpendicular to the film. The x-ray beam is centered on
the film. The film shows both central incisors and most of the
lateral incisorstt (tube angle 60 cauded).
-
Maxillary CanineThe film is held in place using the thumb or
index finger of the opposite hand. (Right hand for maxillary left
canine pictured below). The x-ray beam is directed perpendicular to
the bisecting line vertically and the horizontal angulation should
open the contact between the canine and first premolar (see next
slide). The x-ray beam is centered on the film. . (tube angle 50
degree cauded).
-
Canine Horizontal AngulationIf you direct the beam perpendicular
to the canine, there will normally be overlap between the canine
and first premolar. In order to open this contact, the horizontal
angulation must be rotated posteriorly. Try to imagine the mesial
surface of the first premolar and align the beam parallel with this
surface. (see diagram below right). Incorrect Correct
-
diagonal placement (narrow arch)0Maxillary CanineIn many
patients, especially ones with narrow maxillary arch widths, it is
difficult to align the film ideally because the top edge of the
film contacts the palate on the opposite side and doesnt allow
enough film to register the apex of the canine. By rotating the
film into a diagonal placement, this wont be a problem.Film cant be
placed far enough into the mouth
-
Maxillary PremolarUsing the index finger of the opposite hand,
position the film properly and align the beam vertically and
horizontally. Center the x-ray beam on the film(tube angle 40degree
cauded)..
-
Maxillary MolarUsing the index finger of the opposite hand,
position the film properly and align the beam vertically and
horizontally. Center the x-ray beam on the film. (tube angle 30
degree cauded).
-
Sometimes it is difficult to get the film far enough back to
cover the third molar region due to gagging or anatomy, and all of
the third molar will not be seen on the film (see diagram at left).
By rotating the tubehead so that the beam is directed more
anteriorly (diagram at right), the third molar is projected on to
the film, giving us the needed information. Note, however, the
increase in overlap that results.
-
Mandibular IncisorsUsing the index finger of either hand,
position the film properly and align the PID as discussed earlier.
All four incisors appear on the film.(tube angle 30 cevalic)..
-
Mandibular CanineUsing the index finger of the opposite hand,
position the film properly and align the beam vertically and
horizontally. Center the x-ray beam on the film. # 22 is shown on
the film below(tube angle 20 degree caviled )..
-
Mandibular PremolarUsing the index finger of the opposite hand,
position the film properly and align the beam vertically and
horizontally. Center the x-ray beam on the film. (tube angle 10
caviled).
-
Mandibular MolarUsing the index finger of the opposite hand,
position the film properly and align the beam vertically and
horizontally. Center the x-ray beam on the film. This film clearly
shows all of the third molar roots . (tube centre at right angle
zero degree.
-
Adult full-mouth series, BisectingTechniqueUsing all # 2 size
film, an adult full-mouth series of films consists of 14 periapical
films; 6 anterior (from canine to canine, 3 maxillary and 3
mandibular) and 8 posterior (premolar and molar films in each
quadrant). RLAll # 2 films0
-
Anterior FirstWhen taking films on a patient, you should always
start with the anterior films. If you are doing a full series,
start with the maxillary canine film and then finish all the
anterior films, both maxillary and mandible. Then complete the
posterior films, starting with the premolar, then molar, in each
quadrant. When doing only a few films on a patient, start with the
most anterior film and work your way back in the mouth. This
sequence of taking films allows the patient to get used to the
procedure with a minimum of discomfort and helps to avoid
stimulation of the gag reflex.
-
Bisecting Angle TechniqueErrorsThe following slides identify
some of the most common errors seen when using the bisecting angle
technique.
-
Elongation If you have too little vertical angulation, as in the
diagram below, the image will be elongated or stretched out on the
film. The angle the x-ray beam forms with the bisecting line is
less than 90. The red lines on the film represent the actual length
of tooth # 9; the black arrow points to the end of the image of the
tooth.long axis of toothbisecting linefilmbisecting linex-ray
beam
-
Foreshortening long axis of toothbisecting linefilmIf you have
too much vertical angulation, as in the diagram below, the image
will be foreshortened or reduced in length. The angle the x-ray
beam forms with the bisecting line is greater than 90. The red
lines on the film represent the actual length of tooth # 9; the
black arrow points to the end of the image of the tooth.
-
>90 = foreshortening90 the apex will be imaged lower on the
film, shortening the overall image. Remember, a 90 angle between
the x-ray beam and the bisecting line is the ideal alignment.image
lengths
-
Improper Film PlacementAs with the paralleling technique,
improper film placement is one of the most common errors seen in
the bisecting angle technique. In the molar film below, the film
was placed too far forward, cutting off the distal root of the
second molar and failing to image the third molar region.Mandibular
molar periapical
-
Film PlacementWith finger retention, it may be hard to keep the
film from rotating around the end of the finger as it presses the
film against the teeth. This may result in a tipped film as seen
below. Notice the tip of the second molar is not visible, resulting
in the need for a retake. (The teeth are also elongated; is this
too little or too much vertical angulation?)Too little (not enough)
vertical angulation0
-
0Film PlacementIt is important to place the film so that of film
extends beyond the incisal edge (anterior) or occlusal surface
(posterior). However, if too much film extends beyond, the roots of
the teeth will usually not appear on the film, as seen below.
-
Film PlacementWhen placing the film using finger retention, it
is important to make sure that finger pressure is applied where the
film is supported by tooth structure, ideally at the junction of
the crown of the tooth with the gingiva. If the film is not
supported, film bending will result. In the canine film below, the
canine root bends off of the film. What other error is seen on this
film? Film not centered on canineCanine periapical0
-
Reversed filmIf the colored portion of the film faces the teeth
being radiographed, the lead foil in the film packet will be
between the teeth and the film. This results in the pattern stamped
on the lead foil appearing on the film (see right side of film
below). The film will also be lighter than the other films taken at
the same time. What other situations could result in a film that is
too light?Underexposure or processing error (e.g., developer
solution too cold)0
-
Cone-cutting If the x-ray tubehead is not positioned properly,
the x-ray beam may not cover the entire film. This is known as
conecutting, which results in a clear (white) area on the film
where the silver halide crystals were not exposed to x-rays (see
film below). In the diagram below left, the dotted circle
represents where the x-ray beam should have been positioned; the
solid circle shows the actual position of the x-ray beam (too
posterior).
-
Overlap (incorrect horizontal angulation) Overlap is the
superimposition of part of one tooth with part of the adjacent
tooth (dotted circles below left). The red arrow represents the
direction of the x-ray beam; the x-ray beam should be perpendicular
to the dotted line below. (See discussion of horizontal angulation
on earlier slide).
-
If you try to make the film more comfortable for the patient by
softening the edges, the emulsion of the film will be affected,
resulting in black lines (see film below). With finger retention,
film placement is usually not very uncomfortable; therefore, film
softening is not needed. Film Softening
-
Double exposureWhen taking films, you should always place each
film in a container or paper bag immediately after it is exposed.
Exposed films should never be placed in the same area where
unexposed films are located. The film at left shows images of
mandibular posterior teeth , both upright and inverted. The film
was used for both the premolar and molar films on the same
side.
-
Patient Movement If the patient moves slightly during the
exposure of the radiograph, the image will be blurred as in the
film below. Always advise the patient to remain still for the very
short time it takes to complete the exposure. What other error is
evident on this film?Less than 1/4 of film was extending above the
occlusal surface on this premolar periapical film, cutting off the
top part of the crowns of the teeth.0
-
Thyroid collarWith finger retention of films in the mandibular
arch, the tubehead may be positioned so that the x-ray beam passes
through part of the thyroid collar (see photo below). This lead in
the thyroid collar prevents x-rays from passing through, resulting
in an unexposed, clear area on the film as seen below right.
-
overexposureunderexposureIncorrect Exposure Factors correct
exposureThe standard exposure settings on your x-ray machine will
be acceptable for the majority of your patients. However, if you
are taking radiographs on a child you would need to decrease the
settings. If your patient is very large, you would need to increase
the settings. Underexposure results when the exposure factors are
set too low for the patient size. Overexposure results when the
exposure factors are set too high.
-
Occlusal Technique
-
Occlusal FilmThe occlusal film is used to: identify the extent
of lesions in a buccolingual direction identify the buccolingual
location of impacted teeth or other abnormalities show the location
of developing teeth in children, using # 2 size film image patients
with trismus that have limited mouth opening
-
Occlusal TechniqueHead PositionMaxillary film: the maxillary
arch is parallel to the floor; the midsagittal plane is
perpendicular to the floor.Mandibular film: the head is tipped back
so that the mandibular arch is as close to perpendicular to the
floor as possible.
-
Occlusal TechniqueFilm positionThe film is placed so that the
all-white side of the film (# 4 for adults, # 2 for children) faces
the arch being radiographed. The film is usually placed with the
long axis side-to-side, but this is not critical. The film is large
enough to normally cover the entire arch, but make sure it covers
the area of interest. Position the film as far back in the mouth as
possible and the patient gently bites on it to keep it in
place.
-
Occlusal TechniqueX-ray Beam PositionThere are three types of
occlusal films (to be discussed on the following slides): Normal
Maxillary True Maxillary Mandibular
For all three of these, the x-ray beam is centered on the area
of interest. Because of the curved beam, the corners of the film
that sticks out of the mouth are often not exposed, resulting in
slight conecuts. This is not an error, since these areas contain no
needed information.
-
Normal Maxillary OcclusalThe Normal Maxillary Occlusal film is
the most common occlusal film taken in the maxillary arch. The
vertical angulation is set at 65 degrees. Because of this angle,
structures located toward the back of the mouth may be projected
off the back edge of the film and not be imaged.
-
True Maxillary OcclusalThe True Maxillary Occlusal film is not
often used because of the much higher exposure time needed to
properly expose the film. (Because the vertical angulation is 90
degrees, the x-ray beam passes through the very dense frontal bone;
this is the reason for the increased exposure). Structures located
farther back in the mouth are more likely to be imaged on this
film.90 degrees
-
Mandibular OcclusalWith the head tipped back as much as
possible, the x-ray beam is directed at a 90 degree angle to the
film. Bony expansions of the mandible as well as abnormalities or
pathology in the floor of the mouth can be imaged with this
film.
-
Occlusal TechniqueExposure SettingsThe exposure times for the
normal maxillary and mandibular occlusal films are the same as for
a periapical or bitewing film of comparable film speed. For the
true maxillary occlusal film, the exposure time is four times as
long, allowing enough x-rays to pass through the frontal bone and
properly expose the film.
-
Normal Maxillary OcclusalImpacted canineSupernumerary toothPedo
anterior
-
Mandibular OcclusalPathology SialolithsPedo anterior
-
Modified Bisecting OcclusalIf a patient has difficulty opening
the mouth due to trismus, an occlusal film can be used to provide a
reasonable image of the teeth. The film is centered on the side of
interest with the long axis front to back. The beam is aligned
using the Bisecting Angle technique. The images will be greatly
distorted, but may provide the necessary information.
-
This concludes the section on Bisecting Angle and Occlusal
Techniques. Additional self-study modules are available at:
http://dent.osu.edu/radiology/resources.htm
If you have any questions, you may e-mail me at
[email protected].
Robert M. Jaynes, DDS, MSDirector, Radiology GroupCollege of
DentistryOhio State University0