Embed Size (px)
Citation preview
DOI: 10.1111/j.1741-6612.2008.00298.x
170
Australasian Journal on Ageing, Vol 27 No 4 December 2008, 170–176© 2008 The Authors
Journal compilation © 2008 ACOTA
Blackwell Publishing Asia
Review Article
Self-management education programs for age-related macular degeneration: A systematic review
Lily Lee
Centre for Research into Disability and Society, School of Occupational Therapy, Curtin University of Technology; and Royal Perth Hospital, Perth, Western Australia, Australia
Tanya L Packer
Centre for Research into Disability and Society, School of Occupational Therapy, Curtin University of Technology; and Association for the Blind of Western Australia, Perth, Western Australia, Australia
Seok Hun Tang
Royal Perth Hospital, Perth, Western Australia, Australia
Sonya Girdler
Centre for Research into Disability and Society, School of Occupational Therapy, Curtin University of Technology, Perth, Western Australia, Australia
Objective:
To review the effectiveness of education programs to improve emotional status, daily living and self-efficacy in adults older than 60 years with age-related macular degeneration (AMD).
Method:
Electronic searches of three databases and manual searches of references lists located randomised controlled trials (RCTs) and quasi-experimental studies. Health education programs aimed at increasing knowledge of AMD, skills training or behavioural change were included. Data extraction and quality assessment were undertaken by two reviewers. A narrative analysis was possible.
Results:
Three protocols were reported in four studies (
n
= 532) with three follow-up studies – all contained elements of self-management programs. Effect sizes for the three outcomes ranged from small to very large (0.14–1.21).
Conclusions:
Self-management programs appear effective for older adults with AMD. Small sample size, use of non-traditional statistics and methodological quality meant only a narrative analysis was possible. Future studies with more robust methodology including intent-to-treat analysis are still required.
Key words:
health education, macular degeneration, older adults, self-management, systematic review.
Introduction
Age-related macular degeneration (AMD) is the leading causeof blindness in Australia, accounting for 48% of severe toprofound vision impairment and over a quarter of the mild to
moderate impairment [1]. In 2004, 24 200 Australians wereblind as a result of AMD, while a further 48 300 had lowvision [1]. The incidence of AMD is strongly age-related withits prevalence tripling each decade among Australians 70 yearsand older [2]. This exponential relationship between age andAMD is predicted to result in dramatic increases in the numberof Australians living with disease as the population ages [2].
AMD is a chronic and progressive eye disease for which thereis limited, if any, effective treatment. The macula, located in thecentre of the retina, is responsible for sharp, central vision.AMD results in reduced visual acuity, central visual field, con-trast sensitivity, colour discrimination and problems with glarerecovery [3].
Vision impairment of any kind, including AMD, is known toresult in functional and financial consequences. For example,in 2004, eye health was estimated to have cost $A9.85 billion;$A1.8 billion due to direct health-care costs, $A3.2 billion dueto indirect costs and a further $A4.8 billion due to disabilityand premature mortality [1]. Older adults with AMD requiremore assistance with personal and instrumental activities ofdaily living (ADL) than people of the same age without visionloss [4]. They have reduced ability to care for self and others[5] with known impacts on reading, leisure participationand shopping [6]. Loss of ability to drive has implications forindependence and self-worth, and is often considered the firststep towards dependence [7]. These difficulties are associatedwith increased risk of hip fractures [8], nursing homeplacements and mortality [9].
Psychosocial consequences have also been documented. Olderadults with vision impairment are three times more likely todevelop depression than their peers with normal vision [10].Regardless of the degree of vision loss, older adults experienceconcerns, frustration and annoyance in relation to their qualityof life [6]. Emotional distress is high, even in comparison topeople with other serious diseases such as chronic obstructivepulmonary disease and acquired immunodeficiency syndrome[11].
Older adults with AMD want to understand their vision lossand learn strategies to manage their everyday lives. In theabsence of medical cure, health education programs, whichmediate the negative impact of AMD on the daily lives of olderadults, are central in managing the condition. The objective ofthis systematic review was to determine the effectiveness ofhealth education programs on emotional status, performanceof ADL and self-efficacy in older adults with AMD.
Correspondence to: Professor Tanya L. Packer, Curtin University of Technology. Email: [email protected]
aja(01)_298.fm Page 170 Thursday, October 23, 2008 3:34 PM

A M D s e l f - m a n a g e m e n t : A s y s t e m a t i c r e v i e w
Australasian Journal on Ageing, Vol 27 No 4 December 2008, 170–176
171
© 2008 The AuthorsJournal compilation © 2008 ACOTA
Methods
The review adopted the principles and techniques of systematicreviews. Electronic searches of three databases were used toidentify and locate relevant studies for inclusion. Eachdatabase was searched from its earliest electronic records(MEDLINE from 1966, EMBASE from 1980, and theCumulative Index of Nursing and Allied Health Literature –CINAHL from 1982) to March 2006. The main search termswere macular degeneration, patient education programs andretinal degeneration. With the assistance of a librarian, allterms were truncated, exploded and adjusted to match thespecific database being searched. To search for randomisedcontrolled trials (RCTs) and quasi-experimental studies, thissearch was combined with the Cochrane Highly Sensitive SearchStrategy phases one, two and three as contained in the
CochraneHandbook for Systematic Reviews of Interventions
[12]. Nolanguage restrictions were placed on the searches, however, theywere limited to published literature. Reference lists of all retrievedrelevant studies were manually searched but searches of ophthal-mology journals and conference proceedings were not undertaken.
A priori
criteria for inclusion of studies were applied first tolocated abstracts and then to full text articles if the abstract didnot provide sufficient information. Studies were included if theintervention was described as a health education programpurporting to increase level of knowledge relating to AMD,providing skills training, or focusing on behaviour changes.The mode, length and frequency of the programs and thediscipline of health-care providers were not limited. Participantsin the studies were restricted to those where adults aged60 years or older with AMD were the sole or majority ofparticipants. Outcomes of interest included emotional statusand functional ability and self-efficacy.
Assessment of methodological quality
Two reviewers independently assessed the quality of each studyusing the assessment tool for quantitative studies developed byKmet et al. [13]. The checklist consists of 14 questions and ascoring system. Guidelines and instructions are provided andwere used to assist the reviewers in answering questions andcalculating quality assessment scores. The reviewers used thecalculated score to define the quality as strong (score of > 80%),good (70–80%), adequate (50–70%) or limited (< 50%).Discrepancies between reviewers were resolved by discussion.
Data extraction
Two reviewers independently extracted data from the potentialstudies using methods set out in Section 7 of the
CochraneHandbook for Systematic Reviews of Interventions
[12]. Dataextracted included: study objective(s), study design, method ofparticipant selection, characteristics of the participants, randomallocation, masking of investigators, masking of participants,outcomes, sample size, analytical methods, estimate of variance,confounding controls, results and conclusions. Any discrepancieswere again resolved by discussion. Once data were extracted,the level of evidence was determined based on the NationalHealth and Medical Research Council guidelines [14].
Data synthesis and analysis
Given the use of non-traditional analyses in three articles andthe small number of protocols (three) reported, meta-analysiswas not possible. Instead, a narrative review was undertaken tosummarise findings and provide an assessment of methodologicalissues. However, where sufficient data were provided, effectsize and confidence intervals were calculated using twosoftware calculators: Thalheimer and Cook [15] and theCochrane Library RevMan software [16]. The Thalheimerand Cook [15] calculator extended the options available inRevMan by calculating effect size when standard deviationswere absent and percentage of change. Using the Thalheimerand Cook [15], Cohen’s d was calculated by dividing the meandifference by the pooled standard deviation. Where the stand-ard deviation was not available, effect size was calculatedusing the
t
-value alone. In RevMan, effect size for continuousdata was calculated using the standardised mean differencewith a fixed effect model (inverse variance method) [16]. Fordichotomous data, the relative risk was calculated usingMantel–Haenszel method [16]. Results of the two methods wereexamined for comparability. In all cases the two estimates werewithin 0.1 of each other – hence, results from the two methodswere considered equal.
Results
Electronic searches located 106 articles from MEDLINE, 109from EMBASE and 51 from CINAHL for a total of 220 potentialarticles after accounting for duplicates. Using the stated inclusioncriteria, titles and abstracts were reviewed, resulting in 208articles judged ineligible. Full texts of the remaining 12 articles(two articles retrieved from the reference lists of the potentialstudies) were reviewed for inclusion.
Of the 12 articles, seven met the inclusion criteria reporting onthree different intervention protocols with a total of 532participants. Authors described them as a psychosocial educationprogram [17], a self-management program [18–20] and ahealth education program [21–23]. Four initial studies ofeffectiveness included three RCTs [18,19,21] and one quasi-experimental study using a pretest–post-test design with acontrol group [17]. Two RCTs [18,21] were further evaluatedin three follow-up studies [20,22,23]. One follow-up study[23] primarily reported on cost-effectiveness, however, con-tained summative data not available in the earlier studies, sowas included. In summary, three author groups reported onthree intervention protocols using four different samples (oneprotocol was used with two independent samples) in sevenarticles (three articles were follow-up studies). Five [24–28]studies were excluded.
Quality assessment of studies
Overall, the methodological quality of the included articlesranged from adequate to very strong (see Table 1). One studyreporting on the psychosocial intervention protocol was ratedas adequate, three reporting on the health education programwere rated as strong and three reporting on the self-managementprotocol were rated as strong to very strong. Shortcomings
aja(01)_298.fm Page 171 Thursday, October 23, 2008 3:34 PM

Le
e
L,
P
ac
ke
r
TL
,
Ta
ng
S
H
e
t
al
.
172
Australasian Journal on Ageing, Vol 27 No 4 December 2008, 170–176©
2008 The AuthorsJournal com
pilation © 2008 ACOTA
Table 1: Description of included studies
First author, year of publication, country
Design AMD criteria Intervention Outcome measures Results Methodological quality
Birk (17) 2004 Germany
Quasi-experimental, pretest/post-test (
n
= 22) Experiment = psychosocial program (
n
= 14) Comparison = no treatment (
n
= 8)
• Assessment of bilateral AMD by ophthalmologist
• Visual acuity < 20/70 in the better eye
Group sessions on • Progressive muscle relaxation • Exchange of experiences • Thoughts, emotion
and behaviour • Resources • Problem-solving • Information
Emotional status
• Positive and negative affect
schedule (German version) • Geriatric Depression
Scale (GDS)
Emotional status
No change in positive affect Significant (
P
= 0.05) change in negative affect GDS – Tendency towards significance
Adequate quality (score = 15/28). Conclusion was limited because of small sample size, no rigorous randomisation and no blinding.
Functional status
• ADL and IADL – Multilevel Assessment Instrument
Functional status
Statistically significant
Self-efficacy
Tentative statistical change for perceived autonomy
Self-efficacy
• Perceived autonomy (11-point Likert scale)
• Active problem orientation (coping with illness)
Brody (19) 1999USA
RCT (
n
= 92)Experiment = self-management program (
n
= 44) Control = waiting list (
n
= 48)
• Diagnosis of AMD by ophthalmologist
• Visual loss due to AMD only • Visual acuity of 20/200 in at least
one eye with best correction • Visual acuity of 20/60 or worse
in the better eye
Experimental
• Didactic presentation • Problem-solving • Cognitive skills training • Behavioural skills training
Emotional status
• POMS
Self-efficacy
• AMD-SEQ
Emotional status
Significantly reduced emotional distress (
P
= 0.04)
Self-efficacy
Improved self-efficacy (
P
= 0.02)
Adequate quality (score = 18/28). Conclusion was limited because of small sample size used to investigate emotion, low statistical power and significant differences in results because of missing data. Further study was required.
Brody (18) 2002 USA
RCT (
n
= 231) Experiment = self-management program (
n
= 86) Control A = tape-recorded health lectures (
n
= 74) Control B = waiting list (
n
= 72)
• Diagnosis of AMD by ophthalmologist and fundus photographs
• Visual loss due to AMD only • Visual acuity of 20/60 or worse
in the better eye • Visual acuity of 20/100 or worse
in the other eye with habitual correction
Experimental
• Didactic presentation • Problem-solving • Cognitive skills training • Behavioural skills training
Control A
• Tape-recorded lectures
Emotional status
• POMS
Self-efficacy
• Macular Degeneration Self-Efficacy Questionnaire (AMD-SEQ)
Functional status
• The National Eye Institute
Visual Function Questionnaire
Emotional status
Interaction noted (
P
= 0.02) indicating reduced emotional distress in self-management group, especially for participants with depression (
P
= 0.001)
Self-efficacy
Interaction (
P
= 0.02) indicating increased self-efficacy in self-management group
Functional status
Interaction (
P
= 0.04) indicating increased functioning in self-management group, especially for depressed participants (
P
= 0.02)
Very strong quality (score = 26/28). Conclusion was appropriate; adequate sample size, interviewer blinded, participants blinded to the hypotheses of the study, number of drop-outs with reasons stated, same education giver and same site.
Brody (20) 2005 USA
Note: 28-month follow-up to Brody (20). Reduced sample size reflects attrition.
RCT (
n
= 214) Experiment = self-management program (
n
= 82) Control A = tape-recorded health lectures (
n
= 66) Control B = waiting list (
n
= 66)
• Diagnosis of AMD by ophthalmologist and fundus photographs
• Visual loss due to AMD only • Visual acuity of 20/60 or
worse in the better eye• Visual acuity of 20/100 or
worse in the other eye with habitual correction
Experimental
• Didactic presentation • Problem-solving• Cognitive skills training• Behavioural skills training
Control A
• Tape-recorded lectures
Emotional status
• POMS
Self-efficacy
• Macular Degeneration Self-Efficacy Questionnaire (AMD-SEQ)
Functional status
• The National Eye Institute
Visual Function Questionnaire
Emotional status
Significantly reduced emotional distress (
P
= 0.008) in the treatment group as compared to the control
Self-efficacy
The self-management group had significantly better self-efficacythan the control group (
P
= 0.006)
Functional status
Significantly better function (
P
= 0.05) reported by the control group
Very strong quality (score = 26/28). Conclusion was appropriate; adequate sample size, interviewer blinded, participants blinded to the hypotheses of the study, number of drop-outs with reasons stated, same education giver and same site.
aja(01)_298.fm Page 172 T
hursday, October 23, 2008 3:34 PM
AM
D
se
lf
-m
an
ag
em
en
t:
A
s
ys
te
ma
ti
c
re
vi
ew
Australasian Journal on Ageing, Vol 27 No 4 December 2008, 170–176
173
© 2008 The Authors
Journal compilation ©
2008 ACOTA
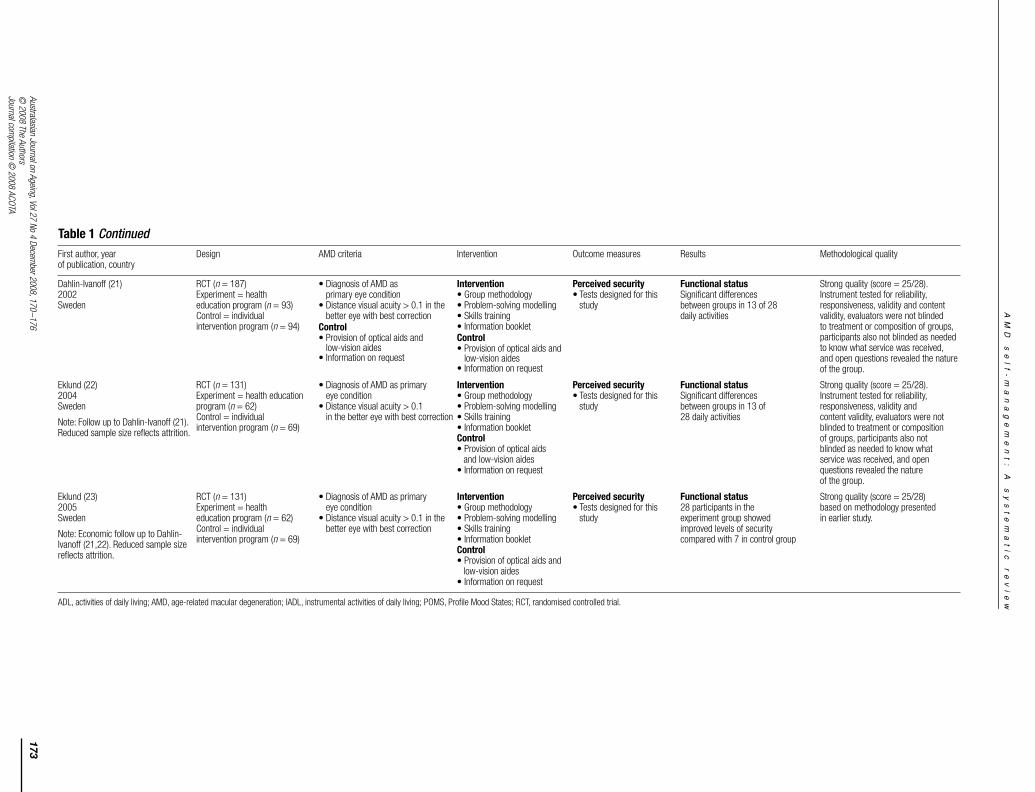
Dahlin-Ivanoff (21) 2002Sweden
RCT (
n
= 187) Experiment = health education program (
n
= 93) Control = individual intervention program (
n
= 94)
• Diagnosis of AMD as primary eye condition
• Distance visual acuity > 0.1 in the better eye with best correction
Control
• Provision of optical aids and
low-vision aides• Information on request
Intervention
• Group methodology • Problem-solving modelling • Skills training • Information booklet
Control
• Provision of optical aids and
low-vision aides• Information on request
Perceived security
• Tests designed for this study
Functional status
Significant differences between groups in 13 of 28 daily activities
Strong quality (score = 25/28). Instrument tested for reliability, responsiveness, validity and content validity, evaluators were not blinded to treatment or composition of groups, participants also not blinded as needed to know what service was received, and open questions revealed the nature of the group.
Eklund (22) 2004 Sweden
Note: Follow up to Dahlin-Ivanoff (21). Reduced sample size reflects attrition.
RCT (
n
= 131)Experiment = health education program (
n
= 62) Control = individual intervention program (
n
= 69)
• Diagnosis of AMD as primary eye condition
• Distance visual acuity > 0.1 in the better eye with best correction
Intervention
• Group methodology • Problem-solving modelling • Skills training • Information booklet
Control
• Provision of optical aids and low-vision aides
• Information on request
Perceived security
• Tests designed for this
study
Functional status
Significant differences between groups in 13 of 28 daily activities
Strong quality (score = 25/28). Instrument tested for reliability, responsiveness, validity and content validity, evaluators were not blinded to treatment or composition of groups, participants also not blinded as needed to know what service was received, and open questions revealed the nature of the group.
Eklund (23) 2005Sweden
Note: Economic follow up to Dahlin-Ivanoff (21,22). Reduced sample size reflects attrition.
RCT (
n
= 131)Experiment = health education program (
n
= 62) Control = individual intervention program (
n
= 69)
• Diagnosis of AMD as primary eye condition
• Distance visual acuity > 0.1 in the better eye with best correction
Intervention
• Group methodology • Problem-solving modelling • Skills training • Information booklet
Control
• Provision of optical aids and low-vision aides
• Information on request
Perceived security
• Tests designed for this study
Functional status 28 participants in the experiment group showed improved levels of security compared with 7 in control group
Strong quality (score = 25/28) based on methodology presented in earlier study.
ADL, activities of daily living; AMD, age-related macular degeneration; IADL, instrumental activities of daily living; POMS, Profile Mood States; RCT, randomised controlled trial.
First author, year of publication, country
Design AMD criteria Intervention Outcome measures Results Methodological quality
Table 1
Continued
aja(01)_298.fm Page 173 T
hursday, October 23, 2008 3:34 PM

L e e L , P a c k e r T L , T a n g S H
e t a l .
174
Australasian Journal on Ageing, Vol 27 No 4 December 2008, 170–176© 2008 The Authors
Journal compilation © 2008 ACOTA
included small sample sizes, lack of blinding and none intent-to-treat analysis (although treatment of missing data wasmostly reported). These shortcomings are common and dif-ficult to overcome in studies that demand active involvementof participants. While some authors reported confidenceintervals for the mean differences, few reported effect sizes. Forthe most part, measurement tools had sound psychometricproperties, typically involving summed scores. The one exceptionwas the Perceived Security Scale used to evaluate the healtheducation program which was designed and tested to measurefunctional status of older adults with AMD [25]. No summa-tive score is produced. Instead, results are reported on the basisof each item, making calculation of effect size difficult.
Interventions
Although the intention of this review was to include all typesof health education programs, it was evident from the studiesretrieved that all programs, despite the names given by theauthors, included elements of self-management educationprograms. One protocol [18–20] was specifically identified asa Self-management Program. The other two protocols (reportedas a Health Education and a Psychosocial Intervention)included education on problem-solving and the intention toincrease self-efficacy; both of which are components thatdifferentiate self-management education programs fromtraditional patient education [29] (see Table 1).
Comparison groups varied. The Self-management Protocolwas evaluated in two separate RCTs (one with a follow-upstudy), one using a wait list control [19] and the other usingtwo control groups: a tape-recorded health lecture group anda no-intervention group [18]. The Psychosocial Program [20]was compared to a no-treatment group, the Health EducationProgram [21–23] to an Individualised Treatment Program.
Outcomes (functional status, emotional status and self-efficacy)
Three broad outcomes; emotional status, functional statusand self-efficacy, were evaluated (see Table 1). Changes inemotional status were examined in four of the seven includedstudies [17–20]; measures included the Profile of Mood States(POMS), the Geriatric Depression Scale and the Positiveand Negative Affect Schedule. The two RCTs by Brodyand colleagues [18,19] found statistically significant improve-ment in the Self-management groups compared to controlsusing the POMS. This was sustained (
P
= 0.008) in the follow-up study (combined face-to-face and taped health lecture)[20]. Calculations, however, indicated that effect sizes weresmall in all three studies (range – 0.15 to – 0.36) (see Table 2).In the pretest–post-test with control study by Birk et al. [17],differences were found on the Negative Affect Scale but notthe Positive Affect Scale, indicating that the control group hadmore severe scores on the Negative Affect Scale. In the samestudy, a tendency towards significance was found using theGeriatric Depression Scale [17]. Effect sizes were found to besmall for the Positive Affect Scale, very large for the NegativeAffect Scale and large for the Geriatric Depression Scale
(Table 2). A small sample size and limited power hamperedthis study, giving rise to speculation that a larger sample sizemay result in significant differences in the Positive Affect andGeriatric Depression scales as well.
All but one study [19] reported on functional status as anoutcome. Despite using different outcome measures (Multi-level Assessment Instrument; National Eye Institute VisualFunction Questionnaire; and Perceived Security) all demon-strated statistically significant differences between theintervention and the control groups. Six-month follow up ofthe Self-management Program [18] indicated that while therewas no difference between those who received the recordedlectures and the face-to-face program, the combined interventiongroup (face-to-face and recorded health lectures) performedsignificantly better (
P
= 0.05) than the no-intervention controlgroups on 15 of 28 items. Effect sizes for the Self-managementand Psychosocial protocols ranged from 0.14 (small) to 1.16(very large) (Table 2). Dahlin-Ivanoff et al. [21] reportedsignificant differences between the Health Education Groupand the usual care (individual treatment program) groups in 13of 28 daily occupations. At follow up, the Health EducationGroup showed a significant tendency towards improved level ofsecurity, while the Individual Intervention Group tended todeteriorate [22]. Insufficient data were provided to calculateeffect size or relative risk from the main RCT studies reportingon the health education program. However, a follow-up studyexamining cost-effectiveness did provide sufficient summativedata to calculate relative risk. People in the intervention group were4.45 times more likely to improve than those in the control group.
Finally, four studies [17–19,21] reported on changes in orcorrelations with self-efficacy or related concepts (coping,autonomy). The AMD Self-efficacy Questionnaire, a disease-specific self-efficacy measure was used in studies examiningthe named self-management program [18–20]. Analysis of cov-ariance found significant differences between the interventionand control groups that were sustained at follow up (
P
= 0.006)[20]. Effect sizes were small to medium (Table 2). Birk et al.[17] reported ‘tentative statistical’ differences between thePsychosocial Program and the no-intervention control groupsusing the Perceived Autonomy Scale (effect size = 0.93) andActive Problem Orientation (effect size 0.88). Both effect sizescan be regarded as large (Table 2).
Discussion
This systematic review found RCT and quasi-experimentalevidence to support the use of self-management and self-management like programs to improve emotional distress,functional ability and self-efficacy in elderly people with AMD.There is sufficient evidence for optimism. Statisticallysignificant improvements were consistently found betweenintervention and control groups. Effect sizes ranged from smallto very large. No adverse effects were reported. However, theresults must be viewed in light of the limitations, the smallnumber of studies, author groups and independent samples aswell as the methodological quality of the studies.
aja(01)_298.fm Page 174 Thursday, October 23, 2008 3:34 PM

A M D s e l f - m a n a g e m e n t : A s y s t e m a t i c r e v i e w
Australasian Journal on Ageing, Vol 27 No 4 December 2008, 170–176
175
© 2008 The AuthorsJournal compilation © 2008 ACOTA
Studies for this review were located from only three databases,although it can be argued that these are the most likely to yieldquality research in this area. Additionally, the search was limitedto published literature and did not include the grey literature;manual searches of ophthalmology, therapy or nursing journalsnor conference proceedings were not undertaken.
The small sample size in the study by Birk et al. [17] must beconsidered when making conclusions and generalising results.Other studies had adequate sample sizes, although it can beargued that some were underpowered. Birk et al. [17] includedonly elderly adults with bilateral AMD, whereas Dahlin-Ivanoff et al. [21] included adults where AMD was not the soleeye disease. Brody [18] included older adults with ‘advancedAMD’. Despite the differences, all studies reflect the reality ofthe population of people with AMD such as advanced age anda high likelihood of additional conditions. Lack of consistencyin outcome measures is typical of clinical studies as is the use
of many different analytical techniques. In the included studiesthree used non-traditional analysis, one used non-parametricanalysis and none reported intent-to-treat analysis.
Despite these limitations, it can be argued that level II (at leastone high quality RCT) evidence is available for each outcome.This is further supported by the fact that, on balance, allmeasures indicated improvement or prevention of furtherdeterioration and no adverse effects were reported. Effect sizesvaried but all were positive.
Improving the emotional and functional rehabilitationoutcomes for older adults with AMD is not only a social, butan economic imperative. Recently, Clear Insight [1], a reportcommissioned by the Centre for Eye Research Australia andthe Eye Research Australia Foundation, estimated that thetotal real costs (direct and indirect) of vision impairment in2004 were more than $A5.0 billion (over 0.6% of GDP). The
Table 2: Effect sizes reported and calculated from published data
Effect size/corrected effect size as
reported by authors
Effect size calculated from t-value using Thalheimer
& Cook 2002
Birk 2004Emotional status 0.23/0.28 0.24 (small)
Positive affectNegative affect 1.14/0.78 1.21 (very large)Depression 0.88/0.44 0.92 (large)
Functional status 1.11/0.66 1.16 (very large)ADL/IADL
Self-efficacy 0.90/1.14 0.93 (large)perceived
AutonomyActive problem 0.84/0.85 0.88 (large)
Orientation
Effect size/corrected effect size as reported
by authors
Effect size calculated from means and standard
deviations using RevMan 2003
Confidence interval calculated using
RevMan
Percentage change calculated using
Thalheimer & Cook 2002
Brody 1999Emotional status
POMS total−0.53 −0.36 (small) −0.90, 0.18 –18% (medium improvement)
Self-efficacy AMD self-efficacy
0.47 0.59 (medium) 0.07, 1.12 12% (small increase)
Brody 2002Emotional status
POMS total−0.15 (small) −0.41, 0.12 –8% (small improvement)
Functional status NEI-VFQ total
0.14 (small) −0.12, 0.41 3% (negligible)
Self-efficacy AMD self-efficacy
0.23 (small) −0.03, 0.50 5% (small increase)
Brody 2005Emotional status
POMS total−0.22 (small) −0.5, 0.05 −12% (small improvement)
Functional status NEI-VFQ total
0.26 (small) −0.02, 0.54 7% (small increase)
Self-efficacy AMD self-efficacy
0.25 (small) −0.02, 0.53 5% (small increase)
Effect size/corrected effect size as reported
by authors
Relative risk calculated
using RevMan
Confidence interval calculated using
RevManEklund 2005Functional status
perceived security4.45 in favour of experimental group 2.09, 9.46
AMD, age-related macular degeneration; NEI-VFQ, National Eye Institute Visual Function Questionnaire; POMS, Profile of Mood States.
aja(01)_298.fm Page 175 Thursday, October 23, 2008 3:34 PM

L e e L , P a c k e r T L , T a n g S H
e t a l .
176
Australasian Journal on Ageing, Vol 27 No 4 December 2008, 170–176© 2008 The Authors
Journal compilation © 2008 ACOTA
cost of suffering and premature death from vision impairmentadded an extra $A4.8 billion to this cost. However, despite theimportance of interventions such as patient educationprograms, there is currently limited understanding of the relativeeffectiveness of various models of service in facilitatingrehabilitation outcomes for older adults with AMD. Findingsfrom this review suggest that self-management and self-management-like interventions can improve the emotional,functional and self-efficacy outcomes. This is particularlyimportant because the comparison group in one study werepeople receiving ‘usual care’. Dahlin-Ivanoff et al. [21] reportedsignificant differences between the intervention and the usualcare consisting of an individualised treatment program.
Although the importance of evidence and research in guidingmodels of service delivery has been reiterated across manyfields including vision rehabilitation, the gap between researchand practice continues [30]. However, with service providersbeing increasingly required to demonstrate both outcomes andefficiencies, the drive to improve and measure practice isgaining momentum. Given that the weight of evidenceindicates self-management programs are effective, andpossibly more effective than individual case management,service providers need to review and evaluate current practicewithin low-vision rehabilitation.
Key Points
• Specifically named self-management programs andprograms with self-management characteristicsappear to be the most common form of educationprogram for people with AMD.
• Self-management-type education programs appearto be effective in improving emotional distress,functional ability and self-efficacy in older peoplewith AMD (level II evidence).
• Additional studies, including replication studies,with robust methodology (particularly using RCTdesign and intent-to-treat analysis) are required tofurther substantiate these findings.
References
1 Access Economics. Clear Insight: The economic impact and cost of visionloss in Australia. A report. Melbourne, Vic.: The Centre for Eye ResearchAustralia, 2004.
2 Weih L, Van Newkirk M, McCarty C, Taylor H. Age-specific causes of bilat-eral vision impairment.
Archives of Ophthalmology
2000; 118: 264–269.3 Russell W, Harper R, Reeves B et al. Randomised controlled trial of an
integrated versus an optometric low vision rehabilitation service forpatients with age-related macular degeneration: Study design andmethodology.
Ophthalmic and Physiological Optics
2001; 21: 36–44.4 Dahlin-Ivanoff S, Sonn U, Lundgren-Lindqvist B, Sjostrand J. Disability in
daily life activities and visual impairment. A population study of 85-yearold people living at home.
Scandinavian Journal of Occupational Therapy
2000; 7: 148–155.5 Stevenson M, Hart P, Montgomery AM et al. Reduced vision in older
adults with age related macular degeneration interferes with ability to
care for self and impairs role as carer.
British Journal of Ophthalmology
2004; 9: 1125–1130.6 Hassell J, Lamoureux E, Keeffe J. Impact of age related macular degeneration
on quality of life.
British Journal of Ophthalmology
2006; 90: 593–596.7 Horowitz A. The prevalence and consequences of vision impairment in
later life.
Topics in Geriatric Rehabilitation
2004; 20: 185–195.8 Ivers R, Norton R, Cumming R et al. Visual impairment and hip fracture.
American Journal of Epidemiology
2000; 152: 633–639.9 Wang J, Mitchell P, Simpson J et al. Visual impairment, age-related cataract,
and mortality.
Archives of Ophthalmology
2001; 119: 1186–1190.10 Rovner B, Ganguli M. Depression and disability associated with impaired
vision: The MoVIES project.
Journal of the American Geriatrics Society
1998; 46: 617–619.11 Williams R, Brody B, Thomas R et al. The psychosocial impact of macular
degeneration.
Archives of Ophthalmology
1998; 116: 514–520.12 Higgins J, Green S. Locating and selecting studies for reviews: Cochrane
Handbook for Systematic Reviews of Interventions 4.2.5.
CochraneLibrary
2005 (2).13 Kmet L, Lee R, Cook L. Standard quality assessment criteria for evaluating
primary research papers for a variety of fields. Available at: http://www.ahfmr.ab.ca/download.php/567d7a28d3767a59f0b05b1999f22d72 Retrieved 12 October 2005.
14 National Health and Medical Research Council (NHMRC).
A Guide to theDevelopment, Implementation and Evaluation of Clinical PracticeGuidelines
. Canberra, ACT: NHMRC, 1999.15 Thalheimer W, Cook S. How to calculate effect sizes from published
research articles: A simplified methodology. Available at: http://work-learningcom/effect_sizeshtm Retrieved August 2002.
16 Cochrane Library Review Manager (RevMan) Edn 4.2 [Computer program]Version 1.0 for Windows. Copenhagen, Denmark: The Nordic CochraneCentre, The Cochrane Collaboration, 2003.
17 Birk T, Hickl S, Wahl H et al. Development and pilot evaluation of apsychosocial intervention program for patients with age-related maculardegeneration.
The Gerontologist
2004; 44: 836–843.18 Brody B, Roch-Levecq A, Ganst A et al. Self-management of age-related
macular degeneration and quality of life.
Archives of Opthalmology
2002;120: 1477–1483.
19 Brody B, Williams R, Thomas R et al. Age-related macular degeneration:A randomised clinical trial of a self-management intervention.
Annals ofBehavioural Medicine
1999; 21: 322–329.20 Brody B, Roch-Levecq A, Thomas R et al. Self-management of age-
related macular degeneration at the 6-month follow-up: A randomisedcontrolled trial.
Archives of Opthalmology
2005; 123: 46–53.21 Dahlin-Ivanoff S, Sonn U, Svensson E. A health education program for
elderly persons with visual impairments and perceived security in theperformance of daily occupations: A randomised study.
American Journalof Occupational Therapy
2002; 56: 322–330.22 Eklund K, Sonn U, Dahlin-Ivanoff S. Long-term evaluation of a health education
programme for elderly persons with visual impairment: A randomisedstudy.
Disability and Rehabilitation
2004; 26: 401–409.23 Eklund K, Sonn U, Nystedt P, Dahlin-Ivanoff S. A cost-effectiveness analysis
of a health education programme for elderly persons with age-relatedmacular degeneration: A longitudinal study.
Disability and Rehabilitation
2005; 27: 1203–1212.24 Dahlin-Ivanoff S, Klepp S, Sjostrand J. Development of a health education
programme for elderly with age-related macular degeneration: A focusgroup study.
Patient Education and Counselling
1998; 34: 63–73.25 Dahlin-Ivanoff S, Sonn U, Svensson E. Development of an ADL instrument
targeting elderly persons with age-related macular degeneration.
Disability and Rehabilitation
2001; 23: 69–79.26 Ferraro J, Mazzoni L, Keeffe J et al. Evaluation of an eye health program:
The vision initiative.
Ophthalmic Epidemiology
2006; 13: 127–135.27 Stone T, Jumper J. Information about age-related macular degeneration
on the Internet.
Southern Medical Journal
2001; 94: 22–25.28 Dahlin-Ivanoff S, Sjostrand J, Klepp S et al. Planning a health education
programme for the elderly visually impaired person: A focus group study.
Disability and Rehabilitation
1996; 18: 515–522.29 Bodenheimer T, Lorig K, Holman H, Grumbach K. Patient self-management
of chronic disease in primary care.
Journal of the American MedicalAssociation
2002; 288: 2469–2475.30 Crews J. The evolution of public policies and services for older people who
are visually impaired. In: Silverstone B, Lang M, Rosenthal B, Faye E, eds.
The Lighthouse Handbook on Vision Impairment and Vision Rehabilitation
,2nd edn. New York: Oxford University Press, 2000: 1287–1300.
aja(01)_298.fm Page 176 Thursday, October 23, 2008 3:34 PM