Embed Size (px)
Citation preview

Selective Executive Dysfunction but Intact Risky Decision-Making inEarly Huntington’s Disease
Anna K. Holl, MD,1,2 Leonora Wilkinson, PhD,1,3 Sarah J. Tabrizi, MD,4 Annamaria Painold, MD,2 and Marjan Jahanshahi, PhD1*
1Sobell Department of Motor Neuroscience and Movement Disorders, University College London, Institute of Neurology, London, United Kingdom2Department of Psychiatry, Graz Medical University, Graz, Austria
3Behavioral Neurology Unit, National Institute of Neurological Disorders and Stroke, Bethesda, Maryland, USA4Department of Neurodegenerative Disease, University College London, Institute of Neurology, London, United Kingdom
ABSTRACT: Executive dysfunction, includingproblems with decision-making, inhibition of prepotentresponses, and verbal fluency, are main features of Hun-tington’s disease (HD). The decline of executive function inHD is related to the anatomical progression of HD pathol-ogy in the basal ganglia, where the earliest changes of neu-ronal cell death are seen in the dorsolateral caudate. Toexamine the specific pattern of executive dysfunction inearly HD, 18 patients with early HD were assessed on: (1)the Iowa Gambling Task to measure risky decision making,(2) the Stroop test to measure inhibition of prepotentresponses, and (3) the verbal fluency test to measure inter-nally guided word search and production, necessitatingsuppression of retrieval/production of inappropriate wordsand monitoring of the output. Patients with early HD weresignificantly impaired on the Stroop and verbal fluency testsrelative to controls. However, Iowa Gambling Task perform-
ance was comparable across the 2 groups. This pattern ofselective executive dysfunction in early HD probablyreflects the fact that inhibitory processing involved in boththe Stroop and verbal fluency tests recruits the dorsolateralcaudate and its cortical connections, which are dysfunc-tional in early HD, whereas risky decision-making duringthe Iowa Gambling Task recruits the ventromedial caudateand its connections, which remain spared early on in thedisease. The current results demonstrate that the deteriora-tion of executive functioning in HD is variable and thatsome types of executive processing might already beimpaired in early HD, whereas others remain intact. VC 2013Movement Disorder Society
Key Words: Huntington’s disease; executivefunction; Iowa Gambling Task; Stroop task; decision-making
Huntington’s disease (HD) is an autosomal-domi-nant trinucleotide repeat disorder that leads to severeneurologic, psychiatric, and cognitive symptoms. Theunderlying defect in HD is a pathologic elongatedgene, resulting from a base triplet elongation (CAG)
on chromosome 4. This gene produces a protein called
Huntingtin, leading to neural apoptosis especially in the
striatum. Deterioration of attention and executive func-tions is commonly observed before the onset of the motor
or neurologic signs of HD, which are typically used todefine the onset of disease.1,2 The cognitive deficits in HD
resemble those that occur in people with lesions of thefrontal cortex.3 This frontal pattern of cognitive deteriora-
tion in HD is considered to result from dysfunction infrontostriatal circuits,4 particularly the associative circuitbetween the dorsolateral prefrontal cortex (DLPFC) andthe dorsolateral part of the caudate head.
Executive dysfunction, including deficits in planning,monitoring, and behavioral regulation, are clinicallyimportant, because they affect the patients’ daily activ-ities. However, the course of deterioration of executivefunctioning in HD is variable. Executive functions donot deteriorate simultaneously, and, during the courseof the disease, a patient may already have difficultywith 1 type of executive processing while othersremain intact.5,6 This pattern probably is caused by
------------------------------------------------------------*Correspondence to: Prof. Jahanshahi, Sobell Department of MotorNeurosciences and Movement Disorders, UCL, Institute of Neurology, 33Queen Square, London, WC1N 3BG, United Kingdom,[email protected]
Funding agencies: This work was supported by a Career DevelopmentFellowship from Parkinson’s UK to Leonora Wilkinson.
Relevant conflicts of interest/financial disclosures: Nothing to report.Full financial disclosures and author roles may be found in the online ver-sion of this article.Contract grant sponsor: Career Development Fellowship.
Received: 19 June 2012; Revised: 18 December 2012; Accepted: 10January 2013Published online 00 Month 2013 in Wiley Online Library(wileyonlinelibrary.com).DOI: 10.1002/mds.25388
R E S E A R C H A R T I C L E
Movement Disorders, Vol. 00, No. 00, 2013 1
the gradual progression of neuronal death in the cau-date in HD. Neuronal death in the caudate proceedsfrom dorsal to ventral and from medial to lateral,with the earliest changes observed in the medial para-ventricular caudate, caudate tail, and dorsal putamen.7
It follows that, in early HD, the associative circuit,between the dorsolateral caudate and the DLPFC, isdysfunctional, whereas the orbitofrontal circuit (OFC)connecting the ventromedial caudate to the OFC andthe limbic circuit between the anterior cingulate andthe ventral striatum remains intact. This is supportedby a study of intradimensional and extradimensionalset shifting in HD.6 Although patients with early HDwere significantly impaired on the “shift stage,” theywere unimpaired on the “reversal stage.” In contrast,patients with late stage HD did poorly on both com-ponents of the task. Lawrence suggested that the“reversal stage” recruits the ventromedial head of thecaudate, whereas the “shift stage” recruits the dorsalcaudate, which is already deteriorated in early HD.Two studies have demonstrated impaired and risky de-cision-making during the Iowa Gambling Task (IGT)in patients with HD,8,9 which is consistent with theidea that this type of decision-making (being depend-ant on the limbic loop) only becomes impaired as thedisease progresses to later stages.
The aim of the present study was to examine pat-terns of executive functioning in early HD. Weassessed patients with early HD using different tests ofexecutive function that reportedly are mediated by dif-ferent corticostriatal circuits. This included the IGT toassess risky decision-making, the Stroop test to mea-sure conflict resolution and inhibition of prepotentresponses, and the verbal fluency (VF) test to assessinternally guided word search and production necessi-tating the suppression of retrieval/production of inap-propriate words and monitoring the output. We
hypothesized that, because of the differential involve-ment of corticostriatal circuits in early HD, the 3 dif-ferent tests of executive functioning mediated by thesecircuits would show variable results: specifically, thatdecision-making would be unimpaired, whereas con-flict resolution and inhibition of prepotent responsesand VF would be impaired.
Patients and Methods
Participants
Eighteen patients with genetically proven HD werestudied. The patients were recruited from theNational Hospital for Neurology and Neurosurgeryand from the Department of Psychiatry at Graz Medi-cal University. Seventeen patients were in the earlystages of the disease with scores on the Unified Hun-tington’s Disease Rating Scale Total FunctionalCapacity (UHDRS TFC)10,11 > 10, and 1 patient wasin a late early stage with a score on the TFC>7. Allpatients presented with positive genetic tests for theHD gene) and had CAG repeat expansion between 41and 48 (Table 1).
Fifteen of 18 patients were not demented, as demon-strated by scores > 27 on the Mini-Mental State Ex-amination (MMSE),12 and 3 of 18 patients presentedwith mild dementia, with MMSE scores between 23and 27. We included these individuals in the studybecause they met only some minor criteria for demen-tia according to the International Classification of Dis-eases 10th edition. Patients were screened fordepression (Beck Depression Inventory [BDI]).13 Onepatient had a BDI score of 24 (moderate depression)but did not meet the criteria for depression in a psy-chiatric interview. All other patients scored in the non-depressed range. At the time of testing, 3 patientswere treated with antipsychotics, mainly for the
TABLE 1. Demographic information and characteristics of patients with Huntington’s disease and controls
Mean 6 SD
Group
Huntington’s
disease, n 5 18
Controls,
n 5 20 T test P
Age, y 53.566 10.2 54.556 13.1 20.26 0.80Education, y 12.756 2.6 14.636 3.7 21.77 0.09Mini-Mental State Examination (score range, 0–30) 28.676 1.9 29.616 0.6 22.00 0.06Premorbid IQ 109.206 9.47 114.656 9.18 21.72 0.10Handedness inventory 53.106 69.8 55.566 51.6 20.11 0.91Beck Depression Inventory (score range, 0–63) 6.426 7.2 6.836 5.1 20.19 0.86Total functional capacity (score range, 0–13) 11.786 1.7Unified Huntington’s Disease Rating Scaletotal motor score (range, 0–124)
24.506 10.3
Age at disease onset, y 46.336 10.0No. of CAG repeats 446 2.3Disease duration, y 7.066 5.4
SD, standard deviation; IQ, intelligence quotient.
H O L L E T A L .
2 Movement Disorders, Vol. 00, No. 00, 2013
treatment of choreatic movements; 1 patient wastreated with a combination of antipsychotics and anti-depressants; and 1 patient was treated withantidepressants.
Twenty healthy volunteers took part in the study.None of the controls had any neurological disorder,psychiatric illness, head injury, or history of alcoholor drug abuse and had normal scores on the MMSEand the BDI. For UK participants, the premorbid intel-ligence quotient (IQ) was estimated with the NationalAdult Reading Test.14 For Austrian patients, premor-bid IQ was assessed with the Mehrfachwahl-Wort-schatz-Intelligenztest (MWT-B).15
The study was approved by the Joint Ethics Committeeof the Institute of Neurology and the National Hospitalfor Neurology and Neurosurgery and by the Ethics Com-mittee of Graz Medical University. Informed consentwas obtained before participation in the study from allparticipants. Controls were paid a fee of £7 per hour.The traveling expenses of patients were reimbursed.
Material
A computerized version of the IGT16 was used. Atthe beginning of the task, participants were given£2000 in fake money. This task comprises 100 trials,and participants were presented with 4 decks of cards,labeled A through D. On each trial, they had to choose1 of the 4 decks. After their selection, money was eitheradded or subtracted from the total winnings, and a lossor gain was indicated to participants by a message onthe screen. Unbeknownst to participants, for decks Aand B, the immediate gains were higher than in decks Cand D; however, at unpredictable point, a win in decksA and B was followed by a high loss. In contrast, fordecks C and D, the gains were much smaller; however,overall, decks C and D were more advantageous thandecks A and B.
The Stroop test from the Delis-Kaplan ExecutiveFunction (DKEF) system was used.17 In each condition,participants are presented with 10 rows of 10 stimuli towhich they must make a verbal response as fast as pos-sible. In the color-naming condition, the stimuli werecolored rectangles, and participants were instructed toname aloud the color. In the word-reading condition,the stimuli were the words blue, red, and green printedin black ink. In the inhibition condition, participantswere instructed to name the color of the ink of thewords blue, red, or green, which were printed in anincongruent color. The inhibition/switching conditioninvolves switching response set between naming thecolor of ink in which colored words are printed orreading the words if they are surrounded by a box. Thetime taken to complete each subtest was noted.
The DKEF VF test was used. Participants wererequired to verbally generate words that fit a particu-lar linguistic constraint for 1 minute. In the phonemic
version, participants had to generate as many wordsas possible beginning with a certain letter. In thesemantic version, participants had to generate as manywords as possible belonging to a particular category;and, in the switching version, participants had toalternate between generating words belonging to 1 of2 categories. For all 3 versions, the total number ofaccurate words was recorded.
Results
Controls and patients did not differ in terms of age,years of education, global cognitive ability, premorbidIQ, handedness, or mood (P> 0.05 for all).
Iowa Gambling Task
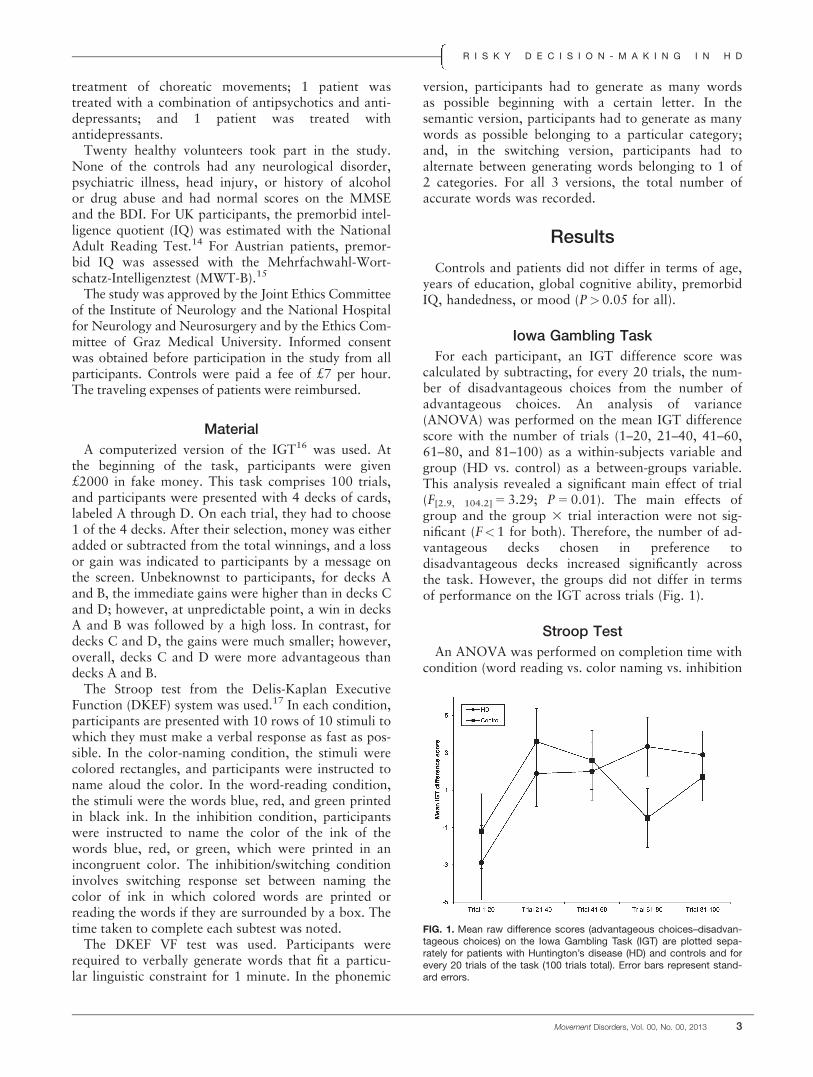
For each participant, an IGT difference score wascalculated by subtracting, for every 20 trials, the num-ber of disadvantageous choices from the number ofadvantageous choices. An analysis of variance(ANOVA) was performed on the mean IGT differencescore with the number of trials (1–20, 21–40, 41–60,61–80, and 81–100) as a within-subjects variable andgroup (HD vs. control) as a between-groups variable.This analysis revealed a significant main effect of trial(F[2.9, 104.2] 5 3.29; P 5 0.01). The main effects ofgroup and the group 3 trial interaction were not sig-nificant (F<1 for both). Therefore, the number of ad-vantageous decks chosen in preference todisadvantageous decks increased significantly acrossthe task. However, the groups did not differ in termsof performance on the IGT across trials (Fig. 1).
Stroop Test
An ANOVA was performed on completion time withcondition (word reading vs. color naming vs. inhibition
FIG. 1. Mean raw difference scores (advantageous choices–disadvan-tageous choices) on the Iowa Gambling Task (IGT) are plotted sepa-rately for patients with Huntington’s disease (HD) and controls and forevery 20 trials of the task (100 trials total). Error bars represent stand-ard errors.
R I S K Y D E C I S I O N - M A K I N G I N H D
Movement Disorders, Vol. 00, No. 00, 2013 3
vs. inhibition/switching) as a within-subjects variableand group as a between-groups variable. This ana-lysis revealed significant main effects of condition(F[2.0, 53.2] 5 86.62; P< 0.001) and group (F[1] 5 48.52;P< 0.001] and a significant interaction between group3 condition (F[3, 81] 5 15.48; P<0.001). Therefore,the performance differed significantly between patientsand controls across all 4 conditions (Fig. 2).
In light of the significant group 3 condition interac-tion, the mean completion time was comparedbetween groups and in each of the 4 conditions. Forall 4 conditions, patients took significantly longer toperform tasks relative to controls (word reading:t[32] 5 4.98; P< 0.001; color naming: t[21.8] 5 4.28;P< 0.001; inhibition: t[16.9] 5 3.95; P 5 0.001; inhibi-tion/switching: t[10.5] 5 4.23; P 5 0.002).
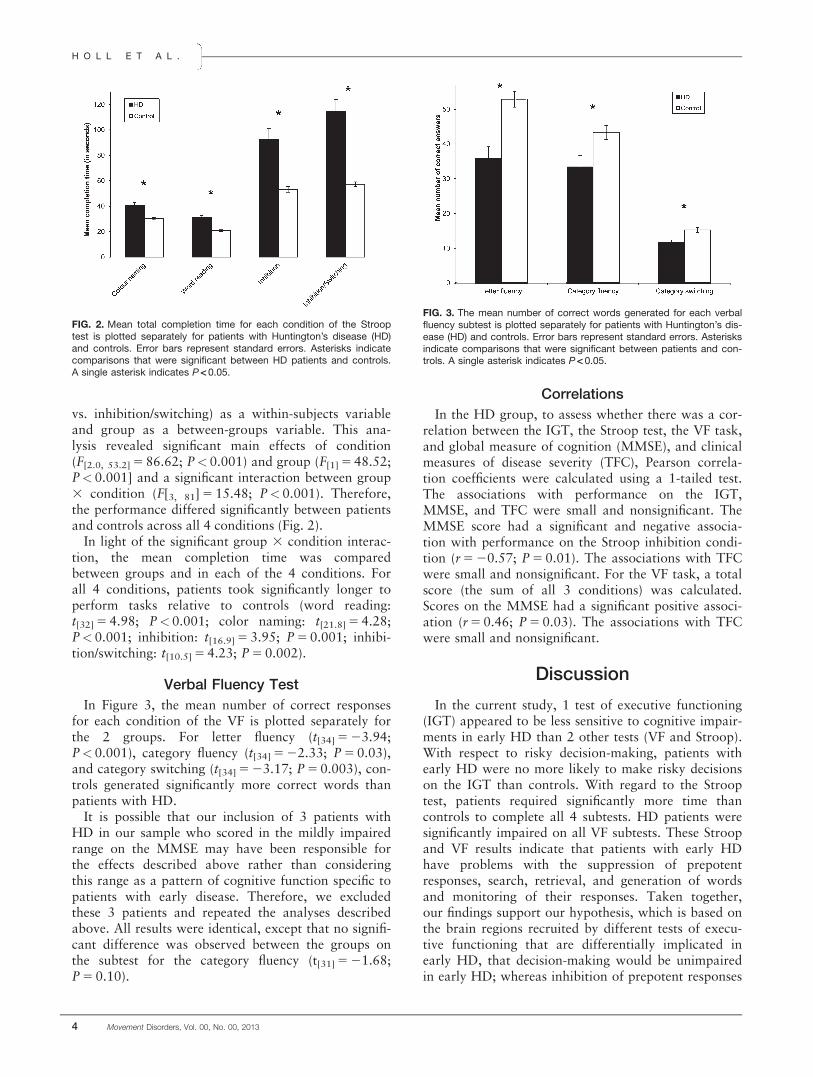
Verbal Fluency Test
In Figure 3, the mean number of correct responsesfor each condition of the VF is plotted separately forthe 2 groups. For letter fluency (t[34] 5 23.94;P< 0.001), category fluency (t[34] 5 22.33; P 5 0.03),and category switching (t[34] 5 23.17; P 5 0.003), con-trols generated significantly more correct words thanpatients with HD.
It is possible that our inclusion of 3 patients withHD in our sample who scored in the mildly impairedrange on the MMSE may have been responsible forthe effects described above rather than consideringthis range as a pattern of cognitive function specific topatients with early disease. Therefore, we excludedthese 3 patients and repeated the analyses describedabove. All results were identical, except that no signifi-cant difference was observed between the groups onthe subtest for the category fluency (t[31] 5 21.68;P 5 0.10).
Correlations
In the HD group, to assess whether there was a cor-relation between the IGT, the Stroop test, the VF task,and global measure of cognition (MMSE), and clinicalmeasures of disease severity (TFC), Pearson correla-tion coefficients were calculated using a 1-tailed test.The associations with performance on the IGT,MMSE, and TFC were small and nonsignificant. TheMMSE score had a significant and negative associa-tion with performance on the Stroop inhibition condi-tion (r 5 20.57; P 5 0.01). The associations with TFCwere small and nonsignificant. For the VF task, a totalscore (the sum of all 3 conditions) was calculated.Scores on the MMSE had a significant positive associ-ation (r 5 0.46; P 5 0.03). The associations with TFCwere small and nonsignificant.
Discussion
In the current study, 1 test of executive functioning(IGT) appeared to be less sensitive to cognitive impair-ments in early HD than 2 other tests (VF and Stroop).With respect to risky decision-making, patients withearly HD were no more likely to make risky decisionson the IGT than controls. With regard to the Strooptest, patients required significantly more time thancontrols to complete all 4 subtests. HD patients weresignificantly impaired on all VF subtests. These Stroopand VF results indicate that patients with early HDhave problems with the suppression of prepotentresponses, search, retrieval, and generation of wordsand monitoring of their responses. Taken together,our findings support our hypothesis, which is based onthe brain regions recruited by different tests of execu-tive functioning that are differentially implicated inearly HD, that decision-making would be unimpairedin early HD; whereas inhibition of prepotent responses
FIG. 2. Mean total completion time for each condition of the Strooptest is plotted separately for patients with Huntington’s disease (HD)and controls. Error bars represent standard errors. Asterisks indicatecomparisons that were significant between HD patients and controls.A single asterisk indicates P < 0.05.
FIG. 3. The mean number of correct words generated for each verbalfluency subtest is plotted separately for patients with Huntington’s dis-ease (HD) and controls. Error bars represent standard errors. Asterisksindicate comparisons that were significant between patients and con-trols. A single asterisk indicates P < 0.05.
H O L L E T A L .
4 Movement Disorders, Vol. 00, No. 00, 2013

and VF would be impaired. We cannot rule out thepossibility that the results reported above may alsoreflect a difference in task difficulty.
Imaging studies have demonstrated that, in healthycontrols, there is activation of the OFC and ventrome-dial prefrontal cortex during performance of theIGT.18 The ventromedial prefrontal cortex is con-nected with the basal ganglia via the limbic circuitbetween the ventral striatum, the ventromedial pre-frontal cortex, and the anterior cingulate; whereas theOFC connects to the basal ganglia via the OFCbetween the ventromedial caudate and the lateralOFC. Both of these circuits involve the ventromedialhead of the caudate, which does not degenerate inearly stages of HD. Therefore, this evidence that thefrontostriatal circuits, which are not implicated inearly HD, mediate performance on the IGT is consist-ent with our finding that performance on the IGT isintact in patients with early HD relative to controls.7
Based on imaging studies, both the Stroop test andthe VF task recruit the limbic circuit and the associa-tive circuit between the DLPFC and the dorsolateralpart of the caudate head.19–21 It is likely that ourpatients with early HD were impaired on the Stoopand VF tests, because the associative circuit isimpaired, and these patients already have early degen-eration of the dorsolateral caudate, where the firstneural cell loss is found.7 Because cortical changes arealready observed early in the course of the disease, wecannot rule out the possibility that cortical deteriora-tion in HD also contributes to the deficits on thesecognitive tests. Nevertheless, degeneration of the basalganglia and their cortical interconnections seems tomake the main contribution to cognitive and motordeficits in HD.
Our finding that patients with early HD are nomore likely to make risky choices than healthy con-trols is in contrast to 2 previous studies of the IGT inHD, in which patients were significantly impaired onthe IGT relative to healthy controls.8,9 It is possiblethat the difference between our findings and those ofStout et al. and Campbell et al. can be explained bythe fact that their patients had more severe HD thanthe patients tested in our current study. Whereas,in the study by Stout et al., only 58% of their patientswere in the normal range on the Mattis Dementia Rat-ing Scale; in the present study, 83.3% of our patientswere not demented. In HD, the deterioration of cogni-tive functions correlates with progression of disease.This is supported by the observation by Stout et al.that more advantageous choices were related to lesssevere cognitive dysfunction.9 Similarly, Campbellet al. observed a significant correlation between IGTperformance and dementia severity, supporting theproposal that only patients in more advanced stagesshow significant deterioration on the IGT.8
A functional magnetic resonance imaging study byGray and colleagues supports our hypothesis that onlysome executive functions are impaired early in thecourse of the disease because of their dependence onthe DLPCF and the early degeneration of the dorsolat-eral caudate head.22 Gray and colleagues assessed ex-ecutive function of symptomatic HD patients with the“shifting response set (SRS) paradigm” and observedthat symptomatic patients were significantly impairedin this task compared with controls and presympto-matic patients. In addition, for symptomatic HDpatients, a significant correlation between DLPFC ac-tivity and SRS performance was reported, indicatingthat early degeneration of the dorsolateral caudatehead leads to dysfunction of the associative circuit andimpaired performance on the SRS task.
Our findings have clinical implications, because ex-ecutive processes are essential for engaging in goal-directed behaviors in daily life. The striatum may startto degenerate significantly up to 11 years before thefirst motor symptoms occur, and patients are consid-ered presymptomatic during this period. Nevertheless,executive dysfunction may develop when patients withHD are still neurologically unimpaired and are consid-ered presymptomatic.23 Subtle difficulties with execu-tive function may already occur in thispresymptomatic stage, when patients still may beworking and have to fulfill financial and social obliga-tions. Although psychiatric problems have a severeimpact on the caregiver in later stages of HD, execu-tive dysfunction affects the patient’s ability to fulfilltheir daily activities early in the course of the dis-ease.24 Executive function refers to a diverse range ofprocesses, and our results demonstrated that the pat-tern of executive function deterioration in HD is vari-able, and some executive functions are impaired inearly HD, whereas others, such as risky decision-mak-ing, remain intact. The more insight clinicians gaininto the time course and characteristics of executivedysfunction in early HD, the better placed they will beto provide advice to patients and caregivers.
Acknowledgments: We are grateful to the HD patients andhealthy controls who took part in this study.
References
1. Ho AK, Sahakian BJ, Brown RG, et al. Profile of cognitive progres-sion in early Huntington’s disease. Neurology 2003;61:1702–1706.
2. Kirkwood SC, Siemers E, Hodes ME, Conneally PM, Christian JC,Foroud T. Subtle changes among presymptomatic carriers of theHuntington’s disease gene. J Neurol Neurosurg Psychiatry2000;69:773–779.
3. Brown RG, Marsden CD. Subcortical dementia- the neuropsycho-logical evidence. Neuroscience 1988;25:363–387.
4. Alexander GE, DeLong MR, Strick PL. Parallel organization offunctionally segregated circuits linking basal ganglia and cortex.Annual Review of Neurosciences 1986;9:357–381.
R I S K Y D E C I S I O N - M A K I N G I N H D
Movement Disorders, Vol. 00, No. 00, 2013 5

5. Lawrence AD, Sahakian BJ, Hodges JR, Rosser AE, Lange KW,Robbins TW. Executive and mnemonic functions in early Hunting-ton’s disease. Brain 1996;119:1633–1645.
6. Watkins LH, Rogers RD, Lawrence AD, Sahakian BJ, Rosser AE,Robbins TW. Impaired planning but intact decision making inearly Huntington’s disease: implications for specific fronto-striatalpathology. Neuropsychologia 2000;38:1112–1125.
7. Vonsattel JP, Myers RH, Stevens TJ, Ferrante RJ, Bird ED,Richardson EP Jr. Neuropathological classification of Huntington’sdisease. J Neuropathol Exp Neurol 1985;44:559–577.
8. Campbell MC, Stout JC, Finn PR. Reduced autonomic responsive-ness to gambling task losses in Huntington’s disease. J Int Neuro-psychol Soc 2004;10:239–245.
9. Stout JC, Rodawalt WC, Siemers ER. Risky decision making inHuntington’s disease. J Int Neuropsychol Soc 2001;7:92–101.
10. Shoulson I, Fahn S. Huntington disease: clinical care and evalua-tion. Neurology 1979;29:1–3.
11. Huntington Study Group. Unified Huntington’s Disease RatingScale: reliability and consistency. Mov Disord 1996;11:136–142.
12. Folstein MF, Folstein SE, McHugh PR. "Mini-Mental State". Apractical method for grading the cognitive state of patients for theclinician. J Psychiatr Res 1975;12:189–198.
13. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventoryfor measuring depression. Arch Gen Psychiatry 1961;4:561–571.
14. Nelson HE. National Adult Reading Test: Test Manual 1982.Windson, Berks, UK: NFER-Nelson; 1982.
15. Lehrl S, Triebig G, Fischer B. Multiple choice vocabulary testMWT as a valid and short test to estimate premorbid intelligence.Acta Neurol Scand 1995;91:335–345.
16. Bechara A, Damasio H, Tranel D, Damasio AR. Deciding advanta-geously before knowing the advantageous strategy. Science1997;275:1293–1295.
17. Delis DC, Kramer JH, Kaplan E, Holdnack J. Reliability and valid-ity of the Delis-Kaplan Executive Function System: an update. J IntNeuropsychol Soc 2004;10:301–303.
18. Bechara A, Tranel D, Damasio H. Characterization of the deci-sion-making deficit of patients with ventromedial prefrontal cortexlesions. Brain 2000;123:2189–2202.
19. Frith CD, Friston KJ, Liddle PF, Frackowiak RS. A PET study ofword finding. Neuropsychologia 1991;29:1137–1148.
20. Martin RC, Loring DW, Meador KJ, Lee GP. The effects of later-alized temporal lobe dysfunction on formal and semantic word flu-ency. Neuropsychologia 1990;28:823–829.
21. Saykin AJ, Stafiniak P, Robinson LJ, et al. Language before and af-ter temporal lobectomy: specificity of acute changes and relation toearly risk factors. Epilepsia 1995;36:1071–1077.
22. Gray MA, Egan GF, Ando A, Churchyard A, Chua P, Stout JC,Georgiou-Karistianis N. Prefrontal activity in Huntington’s diseasereflects cognitive and neuropsychiatric disturbances: the IMAGE-HD study. Exp Neurol 2012;239C:218–228.
23. Aylward EH, Sparks BF, Field KM, et al. Onset and rate of striatalatrophy in preclinical Huntington’s disease. Neurology 2004;63:66–72.
24. Reedeker W, van der Mast RC, Giltay EJ, Kooistra TA, Roos RA,van Duijn E. Psychiatric disorders in Huntington’s disease: a 2-year follow-up study. Psychosomatics 2012;53:220–229.
H O L L E T A L .
6 Movement Disorders, Vol. 00, No. 00, 2013





























