Embed Size (px)
Citation preview
SECTION – I(Course Content)
ABDOMEN, PELVIS, PERINEUM
SCHEDULE1
ANTERIOR ABDOMINAL WALL AND EXTERNAL GENITALIA.
Lecture: 03 hrs
Dissection/ Prosection: 10 hrsTutorials: 01 hr
LECTURES:
Planes and regions of the abdomen. Inguinal canal, spermatic cord, testis coverings and descent. Rectus sheath
DISSECTION/ PROSECTION: Relevant morphological features: linea alba; umbilicus; linea semilunaris;
midaxillary line; posterior axillary line.Subcutaneous structures: anterior and lateral cutaneous branches of lower intercostal nerves; subcostal nerve; iliohypogastric nerve;ilioinguinal nerve; superficial epigastric artery; dartos muscle; fatty and membranous layers of the superficial fascia.Muscles: obliquus externus abdominis; obliquus internus abdominis; cremastermuscle; transversus abdominis; rectus abdominis; pyramidalis.Nerves: muscular branches of lower intercostal; subcostal; iliohypogastric; ilioinguinal; genitofemoral.Arteries: lower posterior intercostal; subcostal; lumbar; superior epigastric; inferior epigastric; deep circumflex iliac.Veins: veins accompanying the above arteries.External genitalia:
Male: testis and its coverings; spermatic cord and contents.Female: round ligament.
Surface anatomy: superficial inguinal ring; deep inguinal ring; inguinal canal.Applied anatomy: surgical incisions of the anterior abdominal wall; vasectomy; inguinal hernia; hydrocoele; undescented testis.
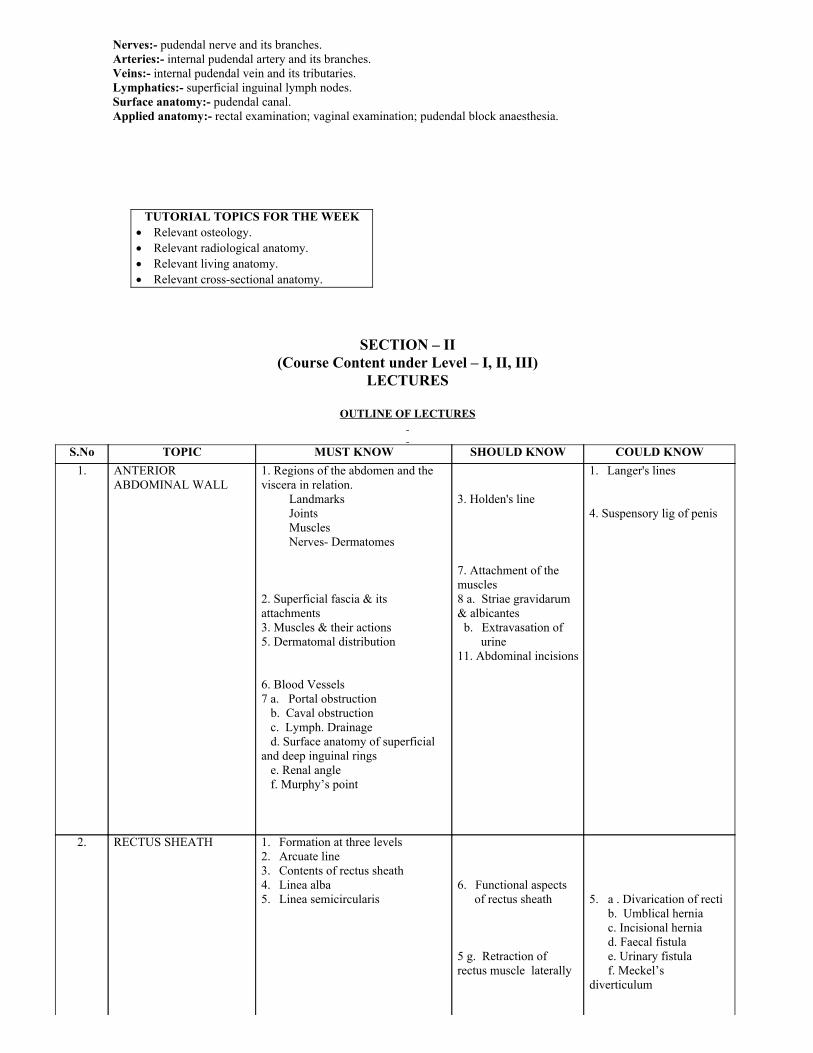
TUTORIAL TOPICS FOR THE WEEK Relevant osteology. Relevant radiological anatomy. Relevant living anatomy. Relevant crosssectional anatomy.
SCHEDULE2.
ABDOMINAL CAVITY, STOMACH AND INTESTINES.
Lecture: 03 hrsDissection/ Prosection: 10 hrs
Tutorials: 01 hr
LECTURES:
Peritoneum, Stomach, jejunum and ileum Caecum and appendix.
DISSECTION/ PROSECTION:Planes of abdomen: vertical; subcostal; transtubercular; transpyloric.Regions of abdomen: epigastric; umbilical; hypogastric, right and left hypochondriac; right and left lumbar; right and left iliac.Peritoneum: parietal; visceral; greater sac; lesser sac; foramen of Winslow; median umbilical fold; medial umbilical folds; lateralumbilical folds; falciform ligament; left triangular ligament; lesser omentum; greater omentum; gastrosplenic ligament; lienorenal
liganment; mesentry; mesoappendix; transverse mesocolon; phrenicocolic ligament.Viscera: Liver lower margin; fissure for ligamentum teres; fissure for ligamentum venosum; porta hepatis; caudate lobe; Gall bladderfundus, neck, body; Stomach fundus; body; pyloric part; greater and lesser curvatures; incisura angularis; sulcus intermedius; stomachbed; interior of the stomach; arterial supply; venous drainage; lymphatic drainage; nerve supply; jejunum and ileum extent; differencesarterial supply; venous drainage; lymphatic drainage; nerve supply; appendix position, arterial supply; caecum posterior relations; colon ascending, transverse, descending; pelvic; arterial supply; venous drainage; lymphatic drainage; nerve supply.Portal vein: formation, location.Surface anatomy: fundus of gall bladder; cardiac and pyloric orifices of the stomach; caecum and appendix.Applied anatomy: referred pain over the umbilical region and pain over the right iliac fossa in appendicitis.
TUTORIAL TOPICS FOR THE WEEK Relevant osteology. Relevant radiological anatomy. Relevant living anatomy. Relevant crosssectional anatomy.
SCHEDULE3
LIVER, PANCREAS, DUODENUM AND SPLEEN.
Lecture: 03 hrsDissection/ Prosection: 10 hrs
Tutorials: 01 hr
LECTURES:
Duodenum and pancreas Liver and extrahepatic biliary apparatus Portal vein
DISSECTION/ PROSECTION:
Liver: surfaces and margins; lobes; relations; structures passing through porta hepatis; bare area; common bile duct.Gall bladder: parts; cystic duct; arterial supply.Duodenum: subdivisions; relations; arterial supply; venous drainage; lymphatic drainage; opening of the bile duct.
Pancreas: subdivisions; relations; arterial supply; venous drainage; openings ofthe pancreatic ducts.Spleen: position; relations.Portal vein: Formation and its tributaries; portosystemic anastomoses.Surface anatomy: liver; gall bladder; common bile duct; duodenum; spleen.Applied anatomy: portal obstruction; biliary colic.
TUTORIAL TOPICS FOR THE WEEK Relevant osteology. Relevant radiological anatomy. Relevant living anatomy. Relevant crosssectional anatomy.
SCHEDULE4
KIDNEY, SUPRARENAL AND POSTERIOR ABDOMINAL WALLLecture: 03 hrs
Dissection/ Prosection: 10 hrsTutorials: 01 hr
LECTURES:
Kidneys, ureters, suprarenals
Abdominal aorta; Inferior venacava; posterior abdominal wall Diaphragm
DISSECTION/ PROSECTION:Kidney: coverings; relations; arterial supply; venous drainage; hilum.Ureter: course; constrictions; arterial supply; nerve supply.Suprarenal: relations; arterial supply; venous drainage.
Posterior abdominal wall.
Muscles: diaphragm; psoas; quadratus lumborum; tranversus abdominis; iliacus.Nerves: subcostal; lumbar plexus and branches; sympathetic trunk; coeliac, renal, intermesenteric and hypogastric plexuses.Arteries: Aorta and its branches.Veins: subcostal; inferior venacava and its tributaries; azygos.Lymphatics: cisterna chyli.Surface anatomy: kidney; ureter; spleen; aorta; inferior venacava.Applied anatomy: inferior venacaval obstruction; renal infarction; polycystic kidneys; ureteric colic.
TUTORIAL TOPICS FOR THE WEEK Relevant osteology. Relevant radiological anatomy. Relevant living anatomy. Relevant crosssectional anatomy.
PELVIS
SCHEDULE5
PELVIC VISCERA.
Lecture: 03 hrsDissection/ Prosection: 10 hrs
Tutorials: 01 hr
LECTURES:
Uterus and adnexa. Rectum. Urinary bladder and prostate.
DISSECTION/ PROSECTION:Identification of relevant skeletal features:hip bones ilium; ischium; pubis;sacrum ala; anterior sacral foramina.coccyx coccygeal vertebrae; sacrococcygeal articulation.bony pelvis inlet, oulet; diametres; ligaments.Peritoneum: Male: pelvic mesocolon; rectovesical pouch Female: pelvic mesocolon; rectouterine puch; uterovesical
pouch; broad ligament of the uterus; mesovarium;uterosacral folds.
Rectum: flexures;ampulla; relations; arterial supply; venous drainage; supports.Uterus: position; parts; cavity; arterial supply; venous drainage; supports; transverse cervical ligament; uterosacral ligament; roundligament.Fallopian tube: intramural part; isthmus; ampulla; infundibulum; fimbriae; abdominal ostium.Ovary: attachments; relations; arterial supply; venous drainage; nerve supply; lymphatic drainage; ligament of ovary.Vagina: fornices; relations.Urinary bladder: shape; surfaces; relations in both the sexes; arterial supply; venous drainage; lymphatic drainage; nerve supply.Ureter: pelvic part course; termination; arterial supply in both the sexes.Ductus deferens: course; termination.Seminal vesicle: shape, position, ducts.
Prostate: shape; size; position; subdivisions; capsules; prostatic venous plexus; prostatic urethra; opening of the ducts.Surface anatomy: fundus of the urinary bladder.Applied anatomy: prolapse of the uterus;prolapse of the rectum; enlargement of the prostate; spread of cancer from pelvic viscera.
TUTORIAL TOPICS FOR THE WEEK Relevant osteology. Relevant radiological anatomy. Relevant living anatomy. Relevant crosssectional anatomy.
SCHEDULE6
BLOOD VESSELS, NERVES AND MUSCLES OF THE PELVIS.
Lecture: 02 hrsDissection/ Prosection: 10 hrs
Tutorials: 01 hr LECTURES:
Internal iliac artery and its branches.and lymphatics of the pelvis.
Pelvis diaphragm.
DISSECTION/ PROSECTION:Arteries: internal iliac; divisions and branches; median sacral.Veins: internal iliac and its tributaries.Nerves: sacral plexus; coccygeal plexuses; autonomic plexuses.Muscles:piriformis; obturator internus; coccygeus; levator ani and its subdivisions; pelvic diaphragm.Applied anatomy: pelvic diaphragm and mechanics of labour.
TUTORIAL TOPICS FOR THE WEEK Relevant osteology. Relevant radiological anatomy. Relevant living anatomy. Relevant crosssectional anatomy.
SCHEDULE7
PERINEUM
Lecture: 01 hrsDissection/ Prosection: 10 hrs
Tutorials: 01 hr
LECTURE:
Ischiorectal fossa.
DISSECTION/ PROSECTION:Anal triangle: rectum and anal canal sphincters; relations; mucous membrane; arterial supply; venous drainage; portosystemicanastomoses; nerev supply.Ischiorectal fossa: boundaries and contents.Urogenital triangle: superficial perineal pouch and its contents; deep perineal pouch and its contents.
Nerves: pudendal nerve and its branches.Arteries: internal pudendal artery and its branches.Veins: internal pudendal vein and its tributaries.Lymphatics: superficial inguinal lymph nodes.Surface anatomy: pudendal canal.Applied anatomy: rectal examination; vaginal examination; pudendal block anaesthesia.
TUTORIAL TOPICS FOR THE WEEK Relevant osteology. Relevant radiological anatomy. Relevant living anatomy. Relevant crosssectional anatomy.
SECTION – II(Course Content under Level – I, II, III)
LECTURES
OUTLINE OF LECTURES
S.No TOPIC MUST KNOW SHOULD KNOW COULD KNOW1. ANTERIOR
ABDOMINAL WALL
1. Regions of the abdomen and theviscera in relation. Landmarks Joints Muscles Nerves Dermatomes 2. Superficial fascia & itsattachments3. Muscles & their actions5. Dermatomal distribution 6. Blood Vessels7 a. Portal obstruction b. Caval obstruction c. Lymph. Drainage d. Surface anatomy of superficialand deep inguinal rings e. Renal angle f. Murphy’s point
3. Holden's line 7. Attachment of themuscles8 a. Striae gravidarum& albicantesb. Extravasation of
urine11. Abdominal incisions
1. Langer's lines 4. Suspensory lig of penis
2. RECTUS SHEATH
1. Formation at three levels2. Arcuate line3. Contents of rectus sheath4. Linea alba5. Linea semicircularis
6. Functional aspects
of rectus sheath 5 g. Retraction ofrectus muscle laterally
5. a . Divarication of recti b. Umblical hernia c. Incisional hernia d. Faecal fistula e. Urinary fistula f. Meckel’sdiverticulum
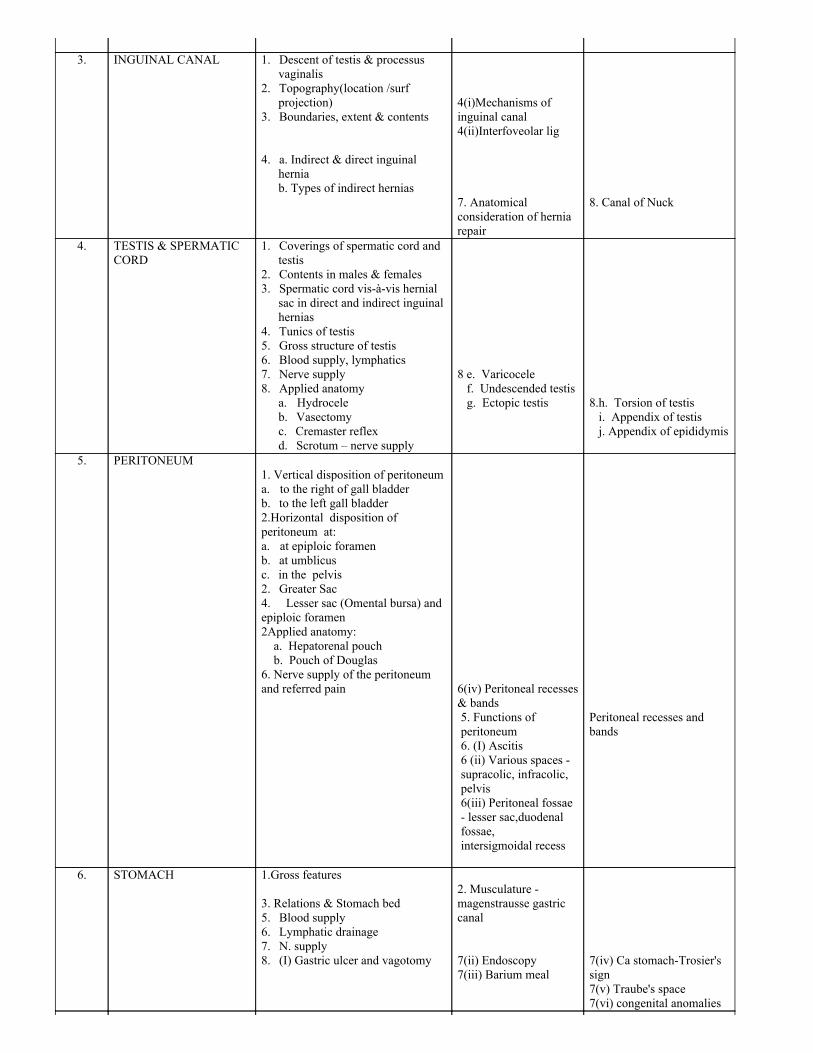
3. INGUINAL CANAL 1. Descent of testis & processus
vaginalis2. Topography(location /surf
projection)3. Boundaries, extent & contents 4. a. Indirect & direct inguinal
herniab. Types of indirect hernias
4(i)Mechanisms ofinguinal canal4(ii)Interfoveolar lig 7. Anatomicalconsideration of herniarepair
8. Canal of Nuck
4. TESTIS & SPERMATICCORD
1. Coverings of spermatic cord andtestis
2. Contents in males & females3. Spermatic cord visàvis hernial
sac in direct and indirect inguinalhernias
4. Tunics of testis5. Gross structure of testis6. Blood supply, lymphatics7. Nerve supply8. Applied anatomy
a. Hydroceleb. Vasectomyc. Cremaster reflexd. Scrotum – nerve supply
8 e. Varicocele f. Undescended testis g. Ectopic testis
8.h. Torsion of testis i. Appendix of testis j. Appendix of epididymis
5. PERITONEUM 1. Vertical disposition of peritoneuma. to the right of gall bladderb. to the left gall bladder2.Horizontal disposition ofperitoneum at:a. at epiploic foramenb. at umblicus c. in the pelvis2. Greater Sac4. Lesser sac (Omental bursa) andepiploic foramen2Applied anatomy: a. Hepatorenal pouch b. Pouch of Douglas6. Nerve supply of the peritoneumand referred pain
6(iv) Peritoneal recesses& bands5. Functions ofperitoneum6. (I) Ascitis6 (ii) Various spaces supracolic, infracolic,pelvis6(iii) Peritoneal fossae lesser sac,duodenalfossae,intersigmoidal recess
Peritoneal recesses andbands
6. STOMACH
1.Gross features 3. Relations & Stomach bed5. Blood supply6. Lymphatic drainage7. N. supply8. (I) Gastric ulcer and vagotomy
2. Musculature magenstrausse gastriccanal 7(ii) Endoscopy7(iii) Barium meal
7(iv) Ca stomachTrosier'ssign7(v) Traube's space7(vi) congenital anomalies
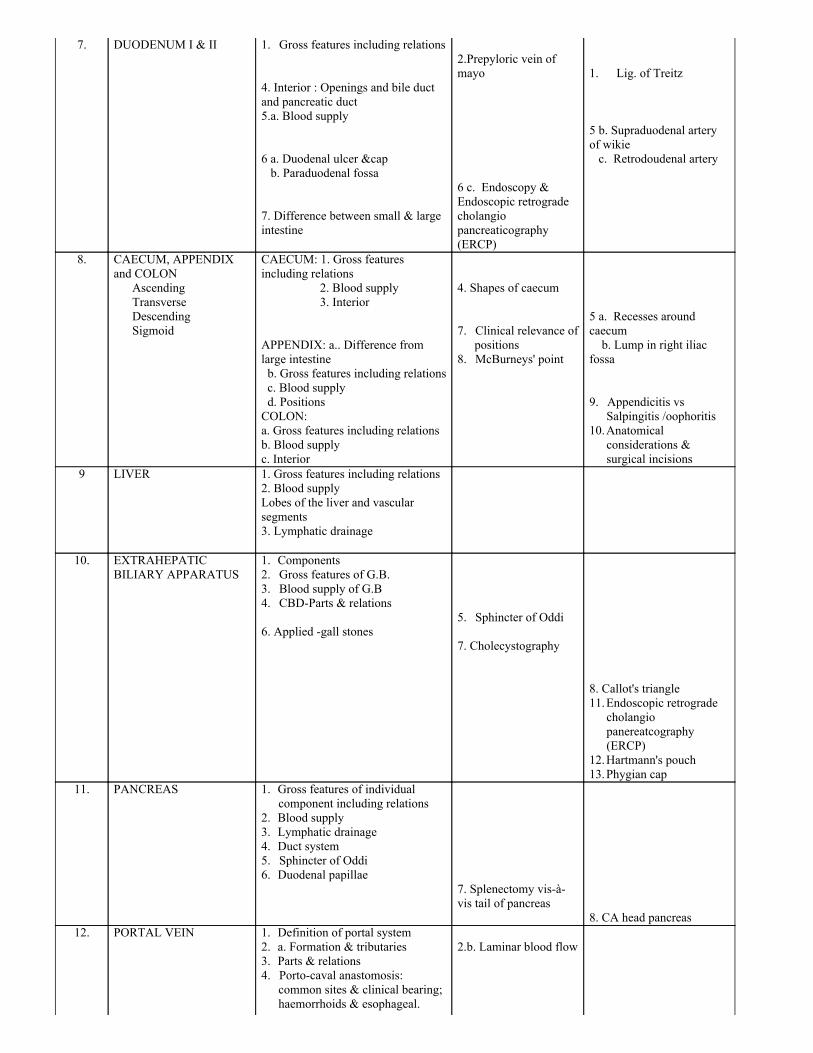
7. DUODENUM I & II 1. Gross features including relations 4. Interior : Openings and bile ductand pancreatic duct5.a. Blood supply 6 a. Duodenal ulcer &cap b. Paraduodenal fossa 7. Difference between small & largeintestine
2.Prepyloric vein ofmayo 6 c. Endoscopy &Endoscopic retrogradecholangio pancreaticography(ERCP)
1. Lig. of Treitz 5 b. Supraduodenal arteryof wikie c. Retrodoudenal artery
8. CAECUM, APPENDIX and COLON Ascending Transverse Descending Sigmoid
CAECUM: 1. Gross featuresincluding relations 2. Blood supply 3. Interior APPENDIX: a.. Difference fromlarge intestine b. Gross features including relations c. Blood supply d. PositionsCOLON:a. Gross features including relationsb. Blood supplyc. Interior
4. Shapes of caecum 7. Clinical relevance of
positions8. McBurneys' point
5 a. Recesses aroundcaecum b. Lump in right iliacfossa 9. Appendicitis vs
Salpingitis /oophoritis10. Anatomical
considerations &surgical incisions
9 LIVER 1. Gross features including relations2. Blood supplyLobes of the liver and vascularsegments3. Lymphatic drainage
10. EXTRAHEPATICBILIARY APPARATUS
1. Components2. Gross features of G.B.3. Blood supply of G.B4. CBDParts & relations 6. Applied gall stones
5. Sphincter of Oddi 7. Cholecystography
8. Callot's triangle11. Endoscopic retrograde
cholangiopanereatcography(ERCP)
12. Hartmann's pouch13. Phygian cap
11. PANCREAS 1. Gross features of individualcomponent including relations
2. Blood supply3. Lymphatic drainage4. Duct system5. Sphincter of Oddi6. Duodenal papillae
7. Splenectomy visàvis tail of pancreas
8. CA head pancreas
12. PORTAL VEIN 1. Definition of portal system2. a. Formation & tributaries3. Parts & relations4. Portocaval anastomosis:
common sites & clinical bearing;haemorrhoids & esophageal.
2.b. Laminar blood flow
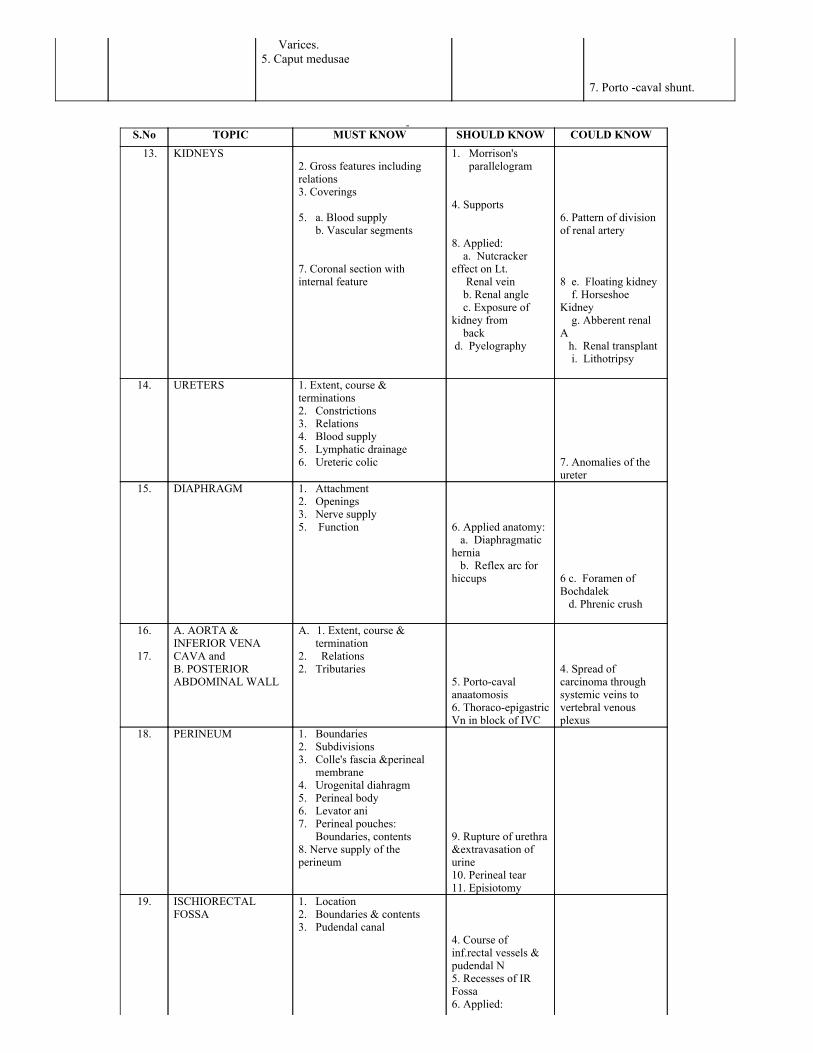
Varices.5. Caput medusae
7. Porto caval shunt.
S.No TOPIC MUST KNOW SHOULD KNOW COULD KNOW
13. KIDNEYS
2. Gross features includingrelations3. Coverings 5. a. Blood supply
b. Vascular segments 7. Coronal section withinternal feature
1. Morrison'sparallelogram
4. Supports 8. Applied: a. Nutcrackereffect on Lt. Renal vein b. Renal angle c. Exposure ofkidney from back d. Pyelography
6. Pattern of divisionof renal artery 8 e. Floating kidney f. HorseshoeKidney g. Abberent renalA h. Renal transplant i. Lithotripsy
14. URETERS 1. Extent, course &terminations2. Constrictions3. Relations4. Blood supply5. Lymphatic drainage6. Ureteric colic
7. Anomalies of theureter
15. DIAPHRAGM 1. Attachment2. Openings3. Nerve supply5. Function
6. Applied anatomy: a. Diaphragmatichernia b. Reflex arc forhiccups
6 c. Foramen ofBochdalek d. Phrenic crush
16. 17.
A. AORTA &INFERIOR VENA CAVA andB. POSTERIORABDOMINAL WALL
A. 1. Extent, course &termination
2. Relations2. Tributaries
5. Portocavalanaatomosis6. ThoracoepigastricVn in block of IVC
4. Spread ofcarcinoma throughsystemic veins tovertebral venousplexus
18. PERINEUM
1. Boundaries2. Subdivisions3. Colle's fascia &perineal
membrane4. Urogenital diahragm5. Perineal body6. Levator ani7. Perineal pouches:
Boundaries, contents8. Nerve supply of theperineum
9. Rupture of urethra&extravasation ofurine10. Perineal tear11. Episiotomy
19. ISCHIORECTALFOSSA
1. Location2. Boundaries & contents3. Pudendal canal
4. Course ofinf.rectal vessels &pudendal N5. Recesses of IRFossa6. Applied:
6(I) Ischiorectalabscess6(ii) Fistula in ano &Goodsall's rule
6(iii) Hiatus ofSchwalbe
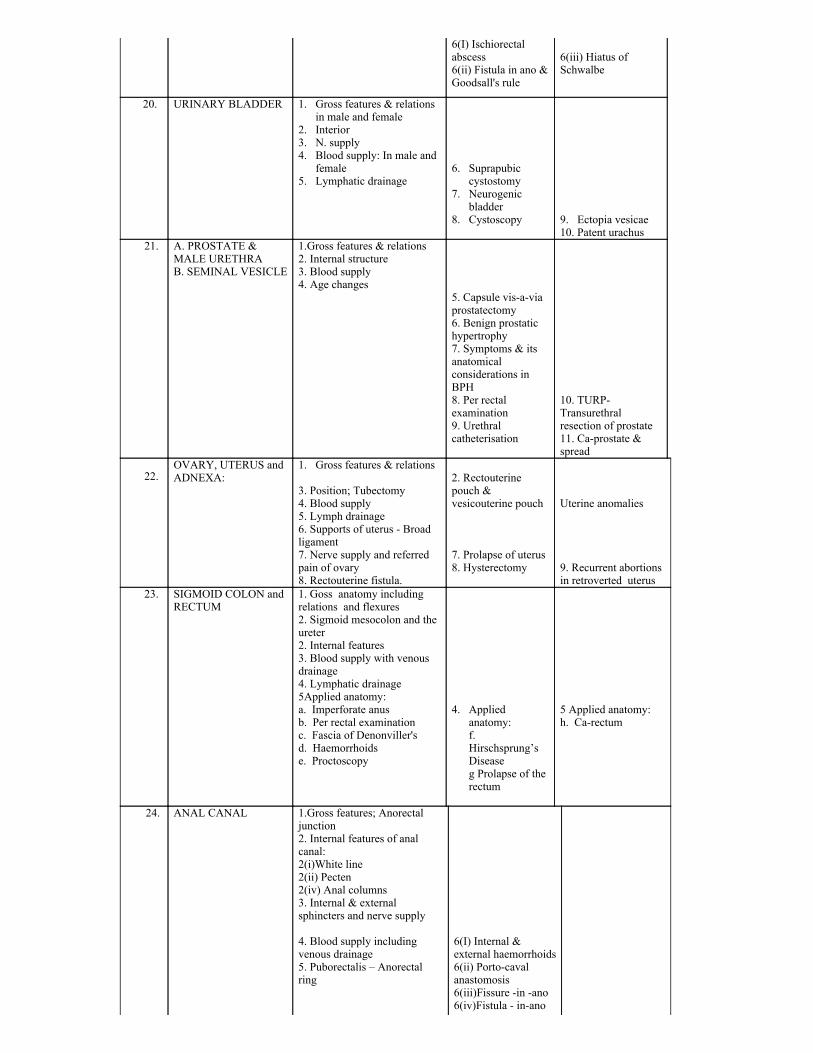
20. URINARY BLADDER 1. Gross features & relationsin male and female
2. Interior3. N. supply4. Blood supply: In male and
female5. Lymphatic drainage
6. Suprapubic
cystostomy7. Neurogenic
bladder8. Cystoscopy
9. Ectopia vesicae10. Patent urachus
21. A. PROSTATE &MALE URETHRAB. SEMINAL VESICLE
1.Gross features & relations2. Internal structure3. Blood supply4. Age changes
5. Capsule visaviaprostatectomy6. Benign prostatichypertrophy7. Symptoms & itsanatomicalconsiderations inBPH8. Per rectalexamination9. Urethralcatheterisation
10. TURPTransurethralresection of prostate11. Caprostate &spread
22.OVARY, UTERUS andADNEXA:
1. Gross features & relations 3. Position; Tubectomy4. Blood supply5. Lymph drainage6. Supports of uterus Broadligament7. Nerve supply and referredpain of ovary8. Rectouterine fistula.
2. Rectouterinepouch &vesicouterine pouch 7. Prolapse of uterus8. Hysterectomy
Uterine anomalies 9. Recurrent abortionsin retroverted uterus
23. SIGMOID COLON andRECTUM
1. Goss anatomy includingrelations and flexures2. Sigmoid mesocolon and theureter2. Internal features3. Blood supply with venousdrainage4. Lymphatic drainage5Applied anatomy:a. Imperforate anusb. Per rectal examinationc. Fascia of Denonviller'sd. Haemorrhoidse. Proctoscopy
4. Applied
anatomy:f. Hirschsprung’sDiseaseg Prolapse of therectum
5 Applied anatomy:h. Carectum
24. ANAL CANAL
1.Gross features; Anorectaljunction2. Internal features of analcanal:2(i)White line2(ii) Pecten2(iv) Anal columns3. Internal & externalsphincters and nerve supply 4. Blood supply includingvenous drainage5. Puborectalis – Anorectalring
6(I) Internal &external haemorrhoids6(ii) Portocavalanastomosis6(iii)Fissure in ano6(iv)Fistula inano
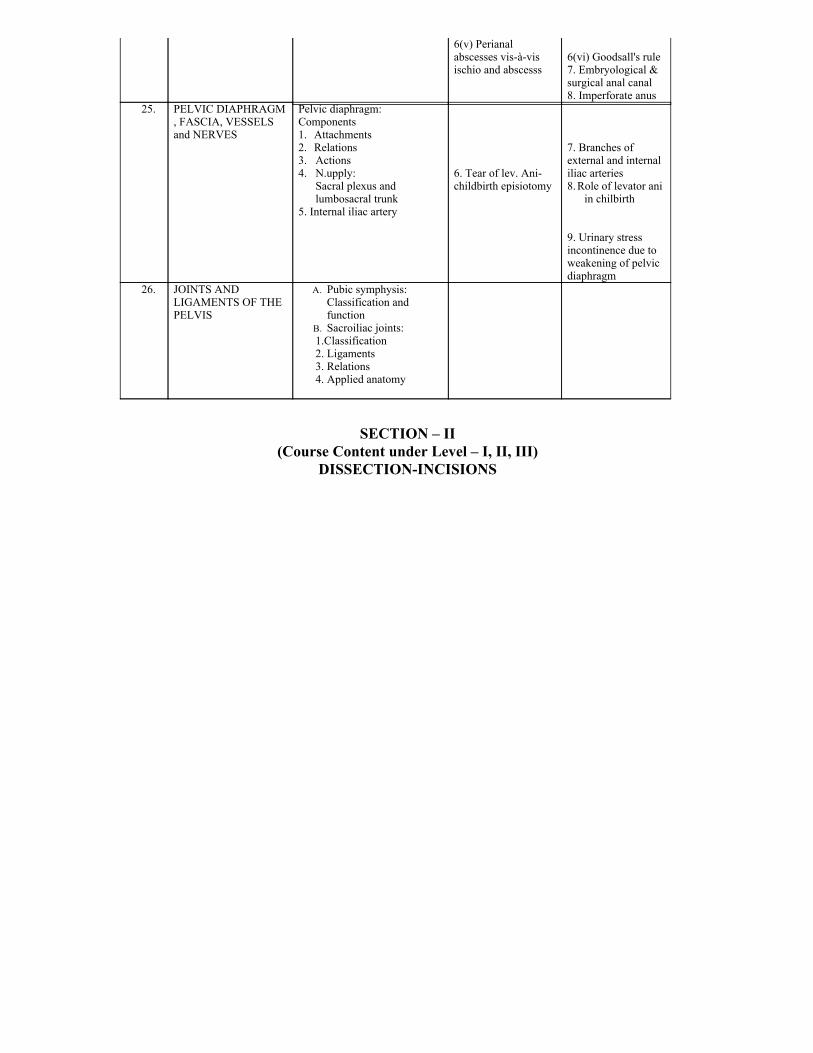
6(v) Perianalabscesses visàvisischio and abscesss
6(vi) Goodsall's rule7. Embryological &surgical anal canal8. Imperforate anus
25. PELVIC DIAPHRAGM, FASCIA, VESSELSand NERVES
Pelvic diaphragm:Components1. Attachments2. Relations3. Actions4. N.upply:
Sacral plexus andlumbosacral trunk
5. Internal iliac artery
6. Tear of lev. Anichildbirth episiotomy
7. Branches ofexternal and internaliliac arteries8. Role of levator ani
in chilbirth 9. Urinary stressincontinence due toweakening of pelvicdiaphragm
26. JOINTS ANDLIGAMENTS OF THEPELVIS
A. Pubic symphysis:Classification andfunction
B. Sacroiliac joints:1.Classification2. Ligaments3. Relations4. Applied anatomy
SECTION – II(Course Content under Level – I, II, III)
DISSECTIONINCISIONS
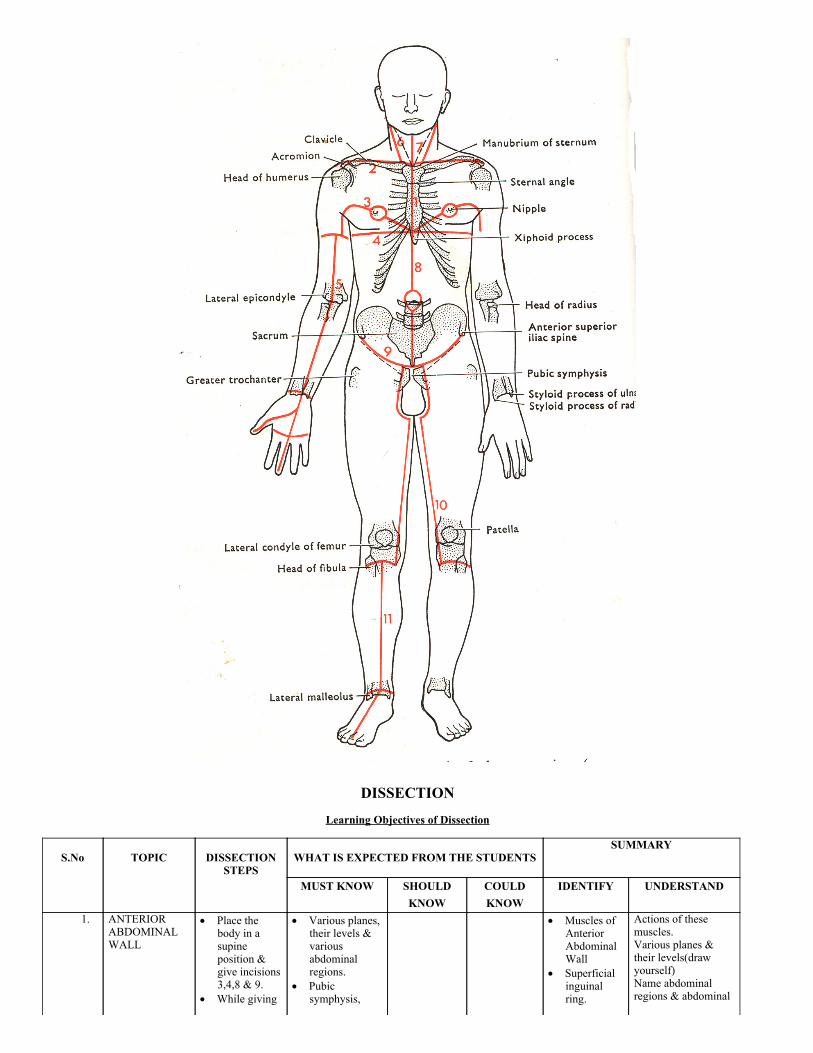
DISSECTION
Learning Objectives of Dissection
S.No
TOPIC
DISSECTION
STEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
1. ANTERIORABDOMINALWALL
Place thebody in asupineposition &give incisions3,4,8 & 9.
While giving
Various planes,their levels &variousabdominalregions.
Pubicsymphysis,
Muscles ofAnteriorAbdominalWall
Superficialinguinalring.
Actions of thesemuscles.Various planes &their levels(drawyourself)Name abdominalregions & abdominal
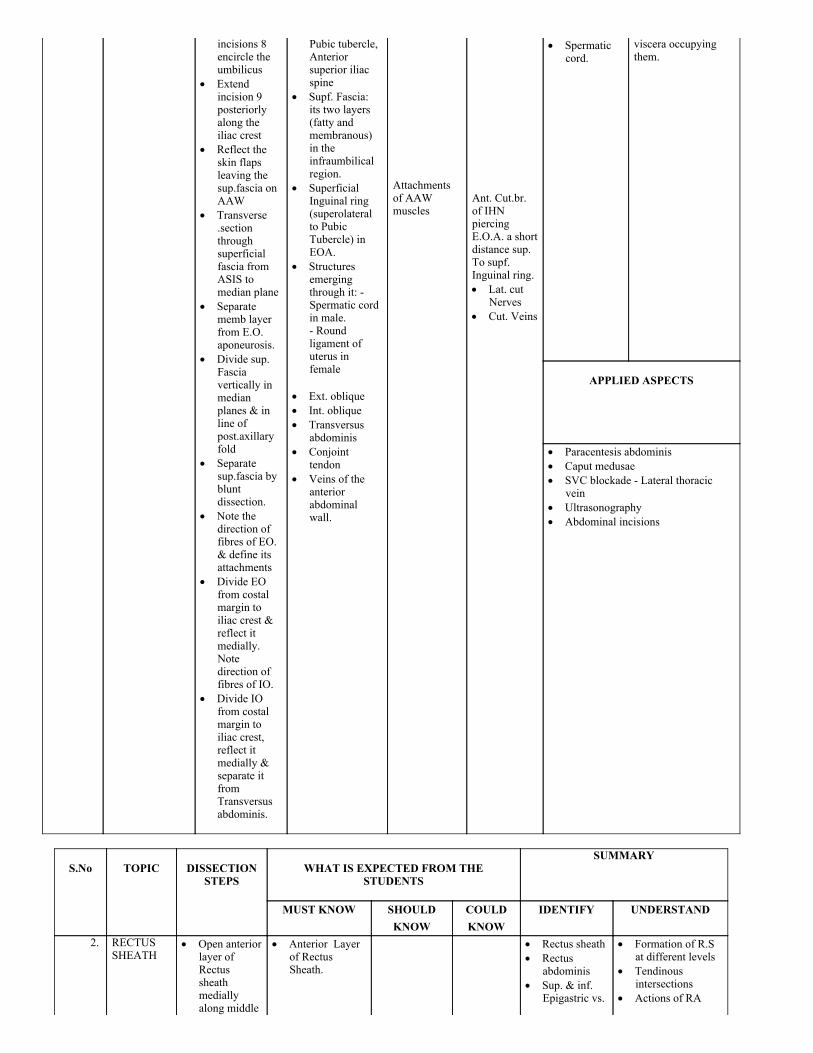
incisions 8encircle theumbilicus
Extendincision 9posteriorlyalong theiliac crest
Reflect theskin flapsleaving thesup.fascia onAAW
Transverse.sectionthroughsuperficialfascia fromASIS tomedian plane
Separatememb layerfrom E.O.aponeurosis.
Divide sup.Fasciavertically inmedianplanes & inline ofpost.axillaryfold
Separatesup.fascia bybluntdissection.
Note thedirection offibres of EO.& define itsattachments
Divide EOfrom costalmargin toiliac crest &reflect itmedially.Notedirection offibres of IO.
Divide IOfrom costalmargin toiliac crest,reflect itmedially &separate itfromTransversusabdominis.
Pubic tubercle,Anteriorsuperior iliacspine
Supf. Fascia:its two layers(fatty andmembranous)in theinfraumbilicalregion.
Superficial Inguinal ring(superolateralto PubicTubercle) inEOA.
Structuresemergingthrough it: Spermatic cordin male. Roundligament ofuterus infemale
Ext. oblique Int. oblique Transversus
abdominis Conjoint
tendon Veins of the
anteriorabdominalwall.
Attachmentsof AAWmuscles
Ant. Cut.br.of IHNpiercingE.O.A. a shortdistance sup.To supf.Inguinal ring. Lat. cut
Nerves Cut. Veins
Spermaticcord.
viscera occupyingthem.
APPLIED ASPECTS
Paracentesis abdominis Caput medusae SVC blockade Lateral thoracic
vein Ultrasonography Abdominal incisions
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE
STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
2. RECTUSSHEATH
Open anteriorlayer ofRectussheathmediallyalong middle
Anterior Layerof RectusSheath.
Rectus sheath Rectus
abdominis Sup. & inf.
Epigastric vs.
Formation of R.Sat different levels
Tendinousintersections
Actions of RA
of R.ectusAbdominismuscle
Detach itfrom thetendinousintersections.
Reflect ant.Layer of R.S.medially &laterally.
Lift R.A. &identifyintercostalNs. &subcostal Ns.
Divide R.A.transvereslyat the middle& turn theparts sup. &inf. Andidentify
Rectusabdominis
Pyramidalis, ifpresent
Posterior layer
of RectusSheath.
Superior &inferior.Epigastric veins.
Arcuate line Linea alba Linea
semilinaries Linea
semicircularis
Intercostal
Ns. Subcostal
nerve
Arcuate line Linea
semilunaris
APPLIED ASPECTS
Umblical hernia Paraumblical hernia Epigastric hernia Rationale of ant. Abdo.wall incisions. Reflection of R.A. laterally Divarication of recti Abdominal paracentesis
S.No
TOPIC
DISSECTION
STEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULD KNOW COULD KNOW IDENTIFY UNDERSTAND 3. TESTIS AND
SPERMATICCORD
Make a longincisionextending fromsupfl. Ringthroughanterolateralaspect ofscrotum
Reflect thedartos from theskin
Reflect dartosfrom loosearticular tissuedeep to it.
Lift testis &spermatic cordfrom thescrotum.
Cut thespermatic cordat the sup, ring& remove italong withtestis.
Clean and traceblood vs. intotestis
Free tail andbody ofepididymis fromthe testis.
Make atransverseincision throughthe testisexamine it witha hand lens &identify
Spermatic cord &structures in itesp. ductusdeference &testicular artery.
Epididymis Dartos Scrotum and its
nerve supply Epididymis and
its various parts Sinus of
epididymis(opens laterally)
Mediatinumtestis
Penis parts Vessels and
nerves of thepenis
Penile urethra TS of the penis
Coverings of
spermatic cord& testis.
Testicular vein
formation Genitofemoral
nerve andcremastericreflex
Testis and its
normalorientation & sidedetermination
Sinus ofepididymis
Spermatic cord Ductus
deferens Testis Epididymis
Coverings ofspermaticcord andtestis
Descent oftestis
APPLIED ASPECTS
Hydrocoele Incomplete descent of testis Ectopic testis Vasectomy Torsion of the testis
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULD KNOW IDENTIFY UNDERSTAND
4. INGUINAL Study the Boundaries of Inguinal Coverings of
CANAL formation ofthe inguinalcanal
inguinal canal Ant. wall Post. wall Floor Roof.
Openings:Inguinal ring inEOA superolat.To P.TDeep ing. Ring inF.T. Structures
passingthroughsuperficialinguinal ring:
spermatic cordin males
round lig. ofuterus infemale
Fasciatransversalis
Ilioinguinal N Iliohypogastric
nerve Umbilical
hernia
Compareinguinalhernia withfemoralhernia
Hasselbach'striangle
Ventral
incisionalhernia
ligament Sup. Ing.
Ring Deep
ing.ring Spermatic
cord inmales
Round lig.in females
Conjointtendon
different typesof hernia
Direct VsIndirectinguinal hernia
Factors
preventinginguinal hernia
APPLIED ASPECTS
Inguinal herniae Anatomical consideration in
repair or hernia
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULD KNOW COULDKNOW
IDENTIFY UNDERSTAND
5. DISSECTIONOF THE LOIN:EXPOSURE OFTHE KIDNEYFROM THEBACK
Place the body inthe proneposition
Follow inf. partof lat. Dorsi toiliac crest
Expose free post.border of ext.oblique & notethe intervalbetween the twomuscles
Reflect the lat.Dorsi nf. AndExt. obliqueanteriorly.Exposeint.oblique (post.part) andthoracolumbarfascia.
Remove remainsof lat. Dorsi &detach serr. Postfrom T.L fascia(post layer)
Cut verticallythrough postlayer from 12thrib to iliac crestand transverse atupper and lowerends. Reflect thelayer and exposeerector spinae
Pull erectorspinae medially& follow middlelayer of theT.L.F ant to themuscle
Define
Lat dorsi Ext. oblique Lumbar triangle
of petit Int. oblique Erector spinae Quadratus
lumborum Subcostal Iliohypogastric Ilioinguinal
Thoracolumbar
fascia(post.layer)
Thoracolumbar
fascia (postlayer)
Subcostal N Iliohypogastric
N Ilioinguinal N
MusclesLat dorsiInt. obliqueEretor spinaeQ. lumborum Fascia TLF NervesSubcostalIliohypogastricIlioinguinal TriangleLumbar triangle Lower pole
of kidney
Arrangement& attachmentsof ThoracoLumbar fascia
APPLIED ASPECTS
attachments ofmiddle layer ofthoracolumbarfascia and cutthrough its sup.Med. & & inf.Attachments &reflect it laterally
Push Quadlumborummedially & feelpost surface ofant. layer byfinger
Divide ant. layer& expose lowerpart of kidney &nerves runningover postr.Surface ofkidney.
Renal angle: incision pleura Bimanual palpation of kidney Lumbar hernia through lumbar
triangle
S.No
TOPIC
DISSECTION STEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
6. PERITONEUMANDDISPOSITIONOF THEVISCERA INSITU
Cut parietalperitoneumtransversely atumbilicus and turnupper and lowerparts sup. & inf.Respectively
Examine and
identify ligamentsin infraumbilicalportion from deeperaspects.
Identify various
abdo. Organs insitu,
Identify Pull stomach down
& to left and liverup and to right.
Ientify epiploicforamen. Pass indexand middle fingersof left hand throughit.
Parietalperitoneum
Verticaldisposition Rt.Of GB. Lt of GB
Horizontaldisposition E.foramen. Umb.Pelvic .
Ligamentumteres
Falciformligament.
Greater sac Lesser sac Compartments Supracolic Infracolic Greater omentum Lesser omentum
parts Epiploic foramen
& its boundaries Omental bursa
and parts Transverse
mesocolon
Median umb.
Lig.
Medial umb.
Lig Lat. Umb.
Lig Internal
hernias
Parietalperitoneum
Peritonealligs.Falciform
Lig. teres Peritoneal
reflectionsGr. Omentum &partsLesser omentum& parts Abdo. Organs
in situSupracoliccompt
Epiploic for.
Peritoneum &its reflections
Def. &examples ofOmetum
Mesentry Ligaments
APPLIED ASPECTS
Peritoneal efusion Paracentesis Peritonitis H.R. pouch Peritoneal spaces Peritoneal recesses Pouch of douglas
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULD KNOW COULDKNOW
IDENTIFY UNDERSTAND
7. SPLEEN Palpate the spleenin the lefthypochondrium
Push stomach toright and identifyupper part ofgreater curvature.
Spleen Anatomical
position Impressions on
visceral surface Ligaments of
Gastrosplenic
ligament(GSL).
Spleen and itsanatomicalposition
Impressions onits visceralsurface
Hilum of
Peritonealreflections oforgan
Ligaments ofspleen
Blood circulationthrough it
Identify fold ofperitoneumextending fromthere to hilum ofspleen.
Identify Vs. inGSL
Push Tr. Colondownward on theleft side includingleft colic flexureand push spleenupward towardleft dome ofdiaphragm ¬e fold ofperitoneumextendingbetween spleenand Lt. Kidney
Study the organin situ. And noteits relations
Cut ligaments athilum of spleenand remove theorgan & study itsgross features
spleen Blood supply
Linorenal
ligament TS at L1 showing
epiploic foramen& lesser sac
Short
gastricVeins
spleen
Functional aspectsof the organ
APPLIED ASPECTS
Palpation of spleen Splenomegaly direction, costal arch. Referred pain in splenic rupture : Kehr's
sign Splenectomy Accessory spleen Splenic puncture
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE
STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
8. COELIACTRUNK
Push liverupwards &trace theperitonealreflection fromliver to lessercurvature ofstomach
Cut and removeboth layers oflesseromentum &identify bloodVessels.
Trace Lt.
Gastric vessels,coursing alonglesser curvature
Trace rt.Gastric vs.coursing alonglower part oflesser curvature
Follow Rt.Gastric art. Tohepatic art
Identifystructures inlesseromentum(in itsrt. Free margin)& note theirpositions
Trace these
Lesser omentum Coeliac trunk and
its three branchesLt. GastricHepaticSplenic Lt. Gastric Vs. Rt. Gastric Vs. Hepatic Art.
Proper Three structuresCommon hepaticart.Portal veinBile duct Tortuous splenic
art Common hepatic
art Gastroduodenal
art Rt. Gastric art.
Coeliac
ganglion
Coeliac trunkand its threebranches
Branches ofhepatic art.
Splenic Vs.behindstomach
Area supplied bycoeliac trunk & itsanatomical basis
Course of hepatic art.
APPLIED ASPECTS
oesophageal varices
structures toporta hepatis ¬e theirrelations
Identify splenicvs. behindstomach
Clean anddefine branchesof hepatic artproper
S.No
TOPIC
DISSECTION
STEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
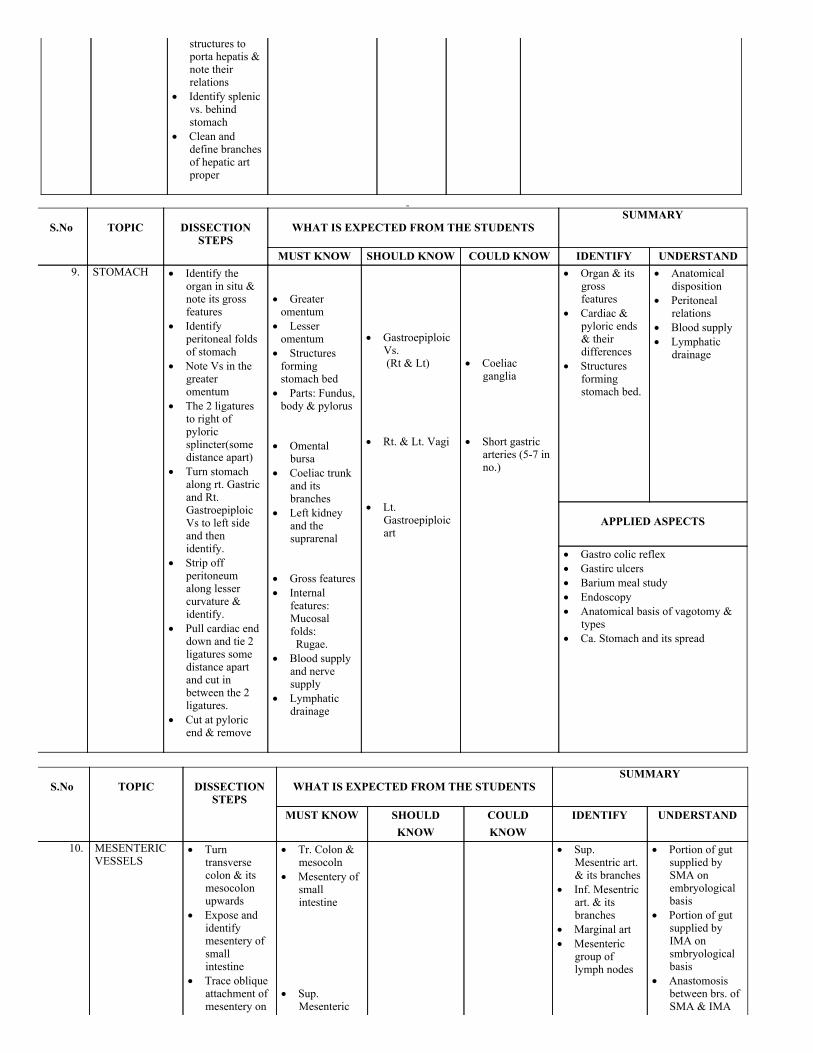
MUST KNOW SHOULD KNOW COULD KNOW IDENTIFY UNDERSTAND 9. STOMACH Identify the
organ in situ ¬e its grossfeatures
Identifyperitoneal foldsof stomach
Note Vs in thegreateromentum
The 2 ligaturesto right ofpyloricsplincter(somedistance apart)
Turn stomachalong rt. Gastricand Rt.GastroepiploicVs to left sideand thenidentify.
Strip offperitoneumalong lessercurvature &identify.
Pull cardiac enddown and tie 2ligatures somedistance apartand cut inbetween the 2ligatures.
Cut at pyloricend & remove
Greateromentum
Lesseromentum
Structuresformingstomach bed
Parts: Fundus,body & pylorus
Omental
bursa Coeliac trunk
and itsbranches
Left kidneyand thesuprarenal
Gross features Internal
features:Mucosalfolds:
Rugae. Blood supply
and nervesupply
Lymphaticdrainage
Gastroepiploic
Vs. (Rt & Lt) Rt. & Lt. Vagi Lt.
Gastroepiploicart
Coeliac
ganglia Short gastric
arteries (57 inno.)
Organ & itsgrossfeatures
Cardiac &pyloric ends& theirdifferences
Structuresformingstomach bed.
Anatomicaldisposition
Peritonealrelations
Blood supply Lymphatic
drainage
APPLIED ASPECTS
Gastro colic reflex Gastirc ulcers Barium meal study Endoscopy Anatomical basis of vagotomy &
types Ca. Stomach and its spread
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
10. MESENTERICVESSELS
Turntransversecolon & itsmesocolonupwards
Expose andidentifymesentery ofsmallintestine
Trace obliqueattachment ofmesentery on
Tr. Colon &mesocoln
Mesentery ofsmallintestine
Sup.
Mesenteric
Sup.Mesentric art.& its branches
Inf. Mesentricart. & itsbranches
Marginal art Mesenteric
group oflymph nodes
Portion of gutsupplied bySMA onembryologicalbasis
Portion of gutsupplied byIMA onsmbryologicalbasis
Anastomosisbetween brs. ofSMA & IMA
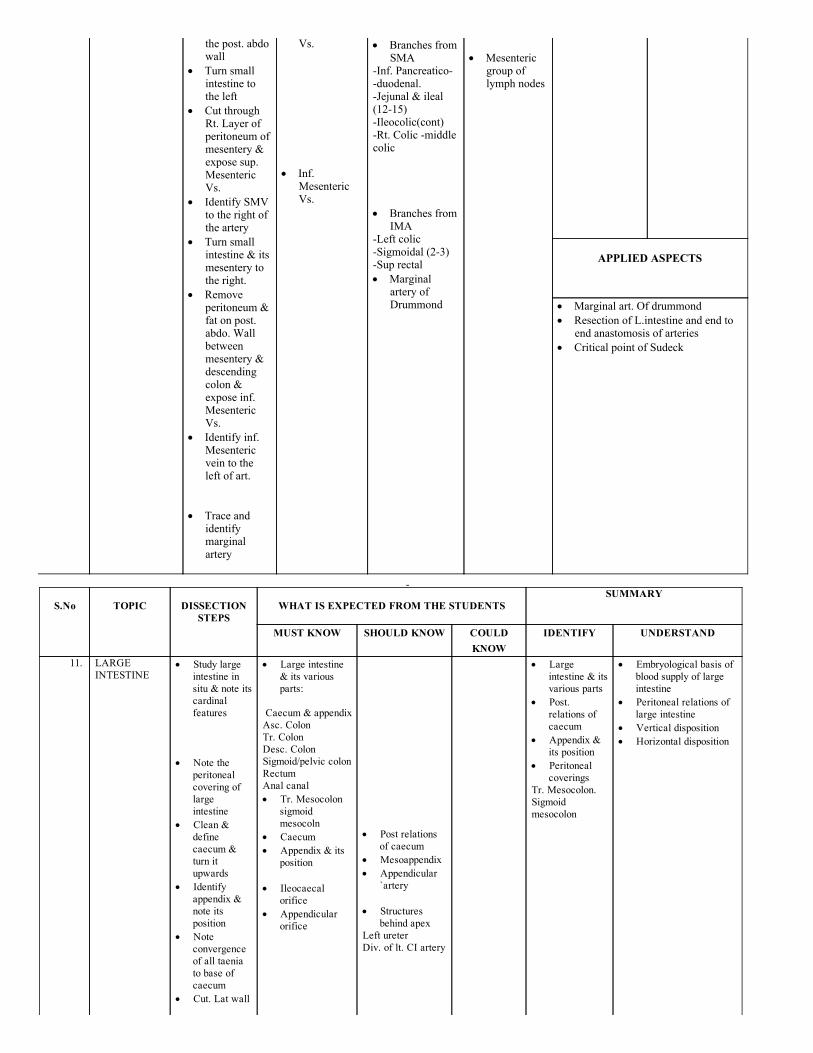
the post. abdowall
Turn smallintestine tothe left
Cut throughRt. Layer ofperitoneum ofmesentery &expose sup.MesentericVs.
Identify SMVto the right ofthe artery
Turn smallintestine & itsmesentery tothe right.
Removeperitoneum &fat on post.abdo. Wallbetweenmesentery &descendingcolon &expose inf.MesentericVs.
Identify inf.Mesentericvein to theleft of art.
Trace and
identifymarginalartery
Vs. Inf.
MesentericVs.
Branches fromSMA
Inf. Pancreaticoduodenal.Jejunal & ileal(1215)Ileocolic(cont)Rt. Colic middlecolic Branches from
IMALeft colicSigmoidal (23)Sup rectal Marginal
artery ofDrummond
Mesenteric
group oflymph nodes
APPLIED ASPECTS
Marginal art. Of drummond Resection of L.intestine and end to
end anastomosis of arteries Critical point of Sudeck
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULD KNOW COULDKNOW
IDENTIFY UNDERSTAND
11. LARGEINTESTINE
Study largeintestine insitu & note itscardinalfeatures
Note the
peritonealcovering oflargeintestine
Clean &definecaecum &turn itupwards
Identifyappendix ¬e itsposition
Noteconvergenceof all taeniato base ofcaecum
Cut. Lat wall
Large intestine& its variousparts:
Caecum & appendixAsc. ColonTr. ColonDesc. ColonSigmoid/pelvic colonRectumAnal canal Tr. Mesocolon
sigmoidmesocoln
Caecum Appendix & its
position Ileocaecal
orifice Appendicular
orifice
Post relations
of caecum Mesoappendix Appendicular
`artery Structures
behind apexLeft ureterDiv. of lt. CI artery
Largeintestine & itsvarious parts
Post.relations ofcaecum
Appendix &its position
Peritonealcoverings
Tr. Mesocolon.Sigmoidmesocolon
Embryological basis ofblood supply of largeintestine
Peritoneal relations oflarge intestine
Vertical disposition Horizontal disposition
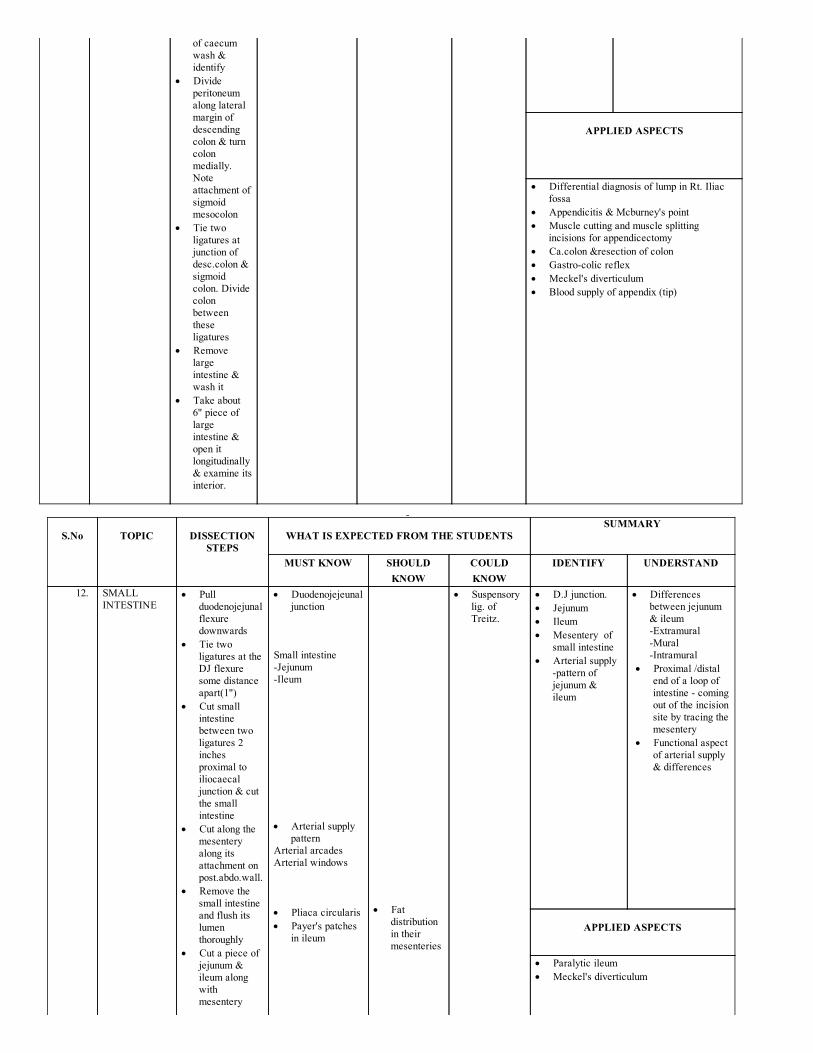
of caecumwash &identify
Divideperitoneumalong lateralmargin ofdescendingcolon & turncolonmedially.Noteattachment ofsigmoidmesocolon
Tie twoligatures atjunction ofdesc.colon &sigmoidcolon. Dividecolonbetweentheseligatures
Removelargeintestine &wash it
Take about 6" piece oflargeintestine &open itlongitudinally& examine itsinterior.
APPLIED ASPECTS
Differential diagnosis of lump in Rt. Iliacfossa
Appendicitis & Mcburney's point Muscle cutting and muscle splitting
incisions for appendicectomy Ca.colon &resection of colon Gastrocolic reflex Meckel's diverticulum Blood supply of appendix (tip)
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
12. SMALLINTESTINE
Pullduodenojejunalflexuredownwards
Tie twoligatures at theDJ flexuresome distanceapart(1")
Cut smallintestinebetween twoligatures 2inchesproximal toiliocaecaljunction & cutthe smallintestine
Cut along themesenteryalong itsattachment onpost.abdo.wall.
Remove thesmall intestineand flush itslumenthoroughly
Cut a piece ofjejunum &ileum alongwithmesentery
Duodenojejeunaljunction
Small intestineJejunumIleum Arterial supply
patternArterial arcadesArterial windows Pliaca circularis Payer's patches
in ileum
Fat
distributionin theirmesenteries
Suspensorylig. ofTreitz.
D.J junction. Jejunum Ileum Mesentery of
small intestine Arterial supply
pattern ofjejunum &ileum
Differencesbetween jejunum& ileumExtramuralMuralIntramural
Proximal /distalend of a loop ofintestine comingout of the incisionsite by tracing themesentery
Functional aspectof arterial supply& differences
APPLIED ASPECTS
Paralytic ileum Meckel's diverticulum
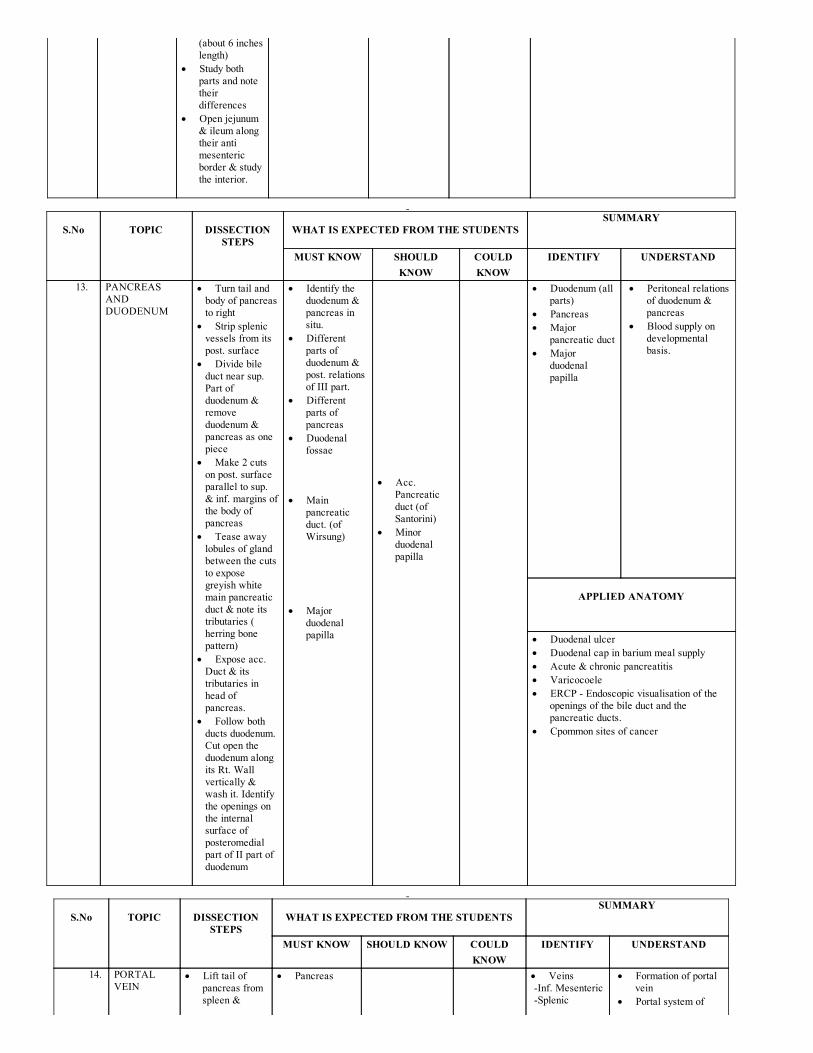
(about 6 incheslength)
Study bothparts and notetheirdifferences
Open jejunum& ileum alongtheir antimesentericborder & studythe interior.
S.No
TOPIC
DISSECTION
STEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
13. PANCREASANDDUODENUM
Turn tail andbody of pancreasto right
Strip splenicvessels from itspost. surface
Divide bileduct near sup.Part ofduodenum &removeduodenum &pancreas as onepiece
Make 2 cutson post. surfaceparallel to sup.& inf. margins ofthe body ofpancreas
Tease awaylobules of glandbetween the cutsto exposegreyish whitemain pancreaticduct & note itstributaries (herring bonepattern)
Expose acc.Duct & itstributaries inhead ofpancreas.
Follow bothducts duodenum.Cut open theduodenum alongits Rt. Wallvertically &wash it. Identifythe openings onthe internalsurface ofposteromedialpart of II part ofduodenum
Identify theduodenum &pancreas insitu.
Differentparts ofduodenum &post. relationsof III part.
Differentparts ofpancreas
Duodenalfossae
Main
pancreaticduct. (ofWirsung)
Major
duodenalpapilla
Acc.
Pancreaticduct (ofSantorini)
Minorduodenalpapilla
Duodenum (allparts)
Pancreas Major
pancreatic duct Major
duodenalpapilla
Peritoneal relationsof duodenum &pancreas
Blood supply ondevelopmentalbasis.
APPLIED ANATOMY
Duodenal ulcer Duodenal cap in barium meal supply Acute & chronic pancreatitis Varicocoele ERCP Endoscopic visualisation of the
openings of the bile duct and thepancreatic ducts.
Cpommon sites of cancer
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULD KNOW COULDKNOW
IDENTIFY UNDERSTAND
14. PORTALVEIN
Lift tail ofpancreas fromspleen &
Pancreas
Veins Inf. Mesenteric Splenic
Formation of portalvein
Portal system of
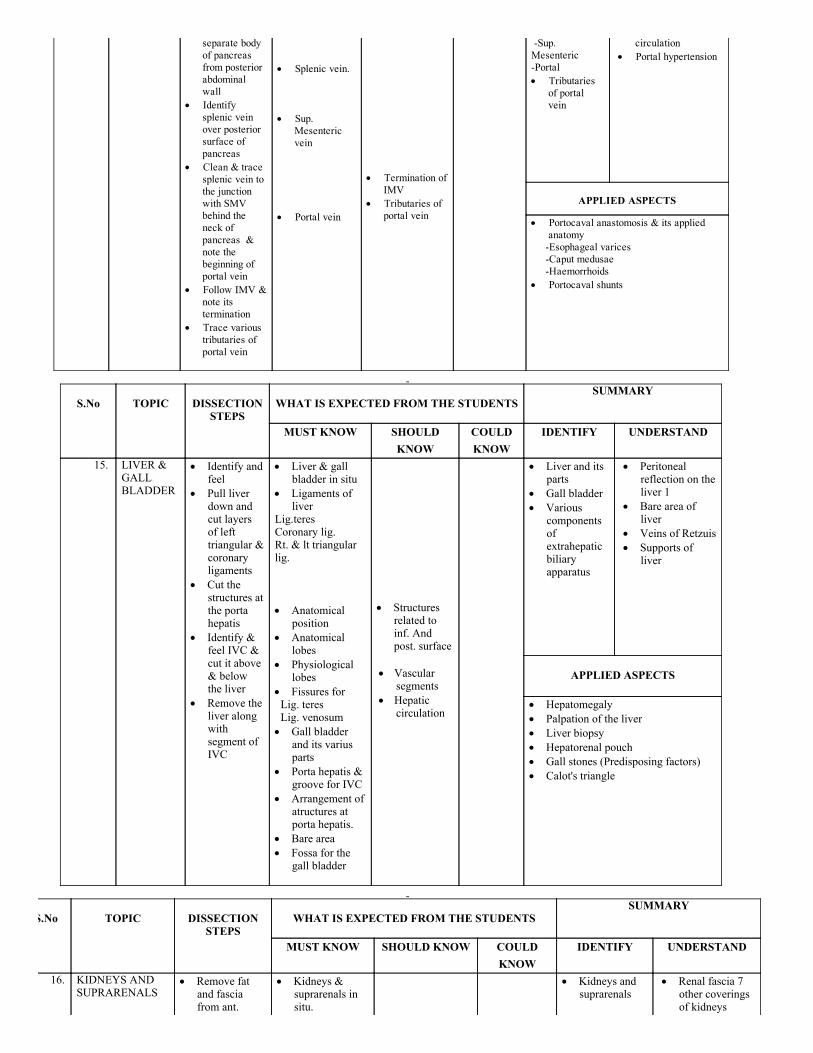
separate bodyof pancreasfrom posteriorabdominalwall
Identifysplenic veinover posteriorsurface ofpancreas
Clean & tracesplenic vein tothe junctionwith SMVbehind theneck ofpancreas ¬e thebeginning ofportal vein
Follow IMV ¬e itstermination
Trace varioustributaries ofportal vein
Splenic vein. Sup.
Mesentericvein
Portal vein
Termination of
IMV Tributaries of
portal vein
Sup.MesentericPortal Tributaries
of portalvein
circulation Portal hypertension
APPLIED ASPECTS
Portocaval anastomosis & its appliedanatomy
Esophageal varices Caput medusae Haemorrhoids Portocaval shunts
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
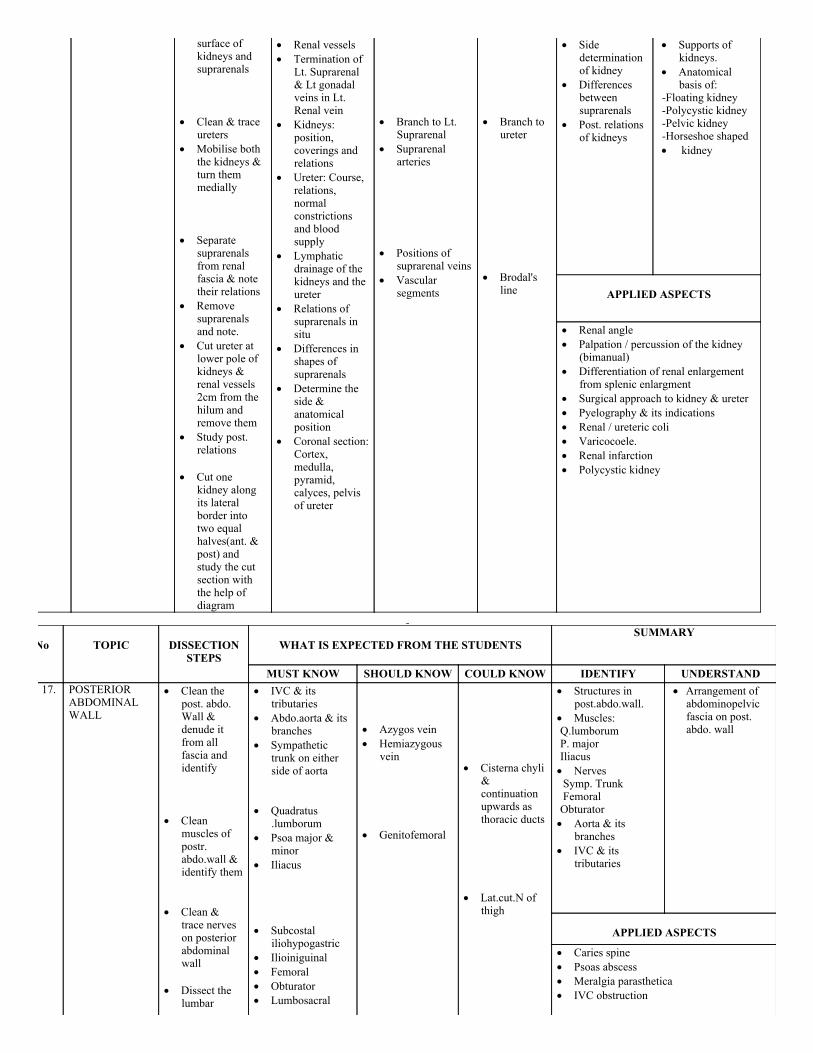
15. LIVER &GALLBLADDER
Identify andfeel
Pull liverdown andcut layersof lefttriangular &coronaryligaments
Cut thestructures atthe portahepatis
Identify &feel IVC &cut it above& belowthe liver
Remove theliver alongwithsegment ofIVC
Liver & gallbladder in situ
Ligaments ofliver
Lig.teresCoronary lig.Rt. & lt triangularlig. Anatomical
position Anatomical
lobes Physiological
lobes Fissures for Lig. teres Lig. venosum Gall bladder
and its variusparts
Porta hepatis &groove for IVC
Arrangement ofatructures atporta hepatis.
Bare area Fossa for the
gall bladder
Structures
related toinf. Andpost. surface
Vascular
segments Hepatic
circulation
Liver and itsparts
Gall bladder Various
components ofextrahepatic biliaryapparatus
Peritonealreflection on theliver 1
Bare area ofliver
Veins of Retzuis Supports of
liver
APPLIED ASPECTS
Hepatomegaly Palpation of the liver Liver biopsy Hepatorenal pouch Gall stones (Predisposing factors) Calot's triangle
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULD KNOW COULDKNOW
IDENTIFY UNDERSTAND
16. KIDNEYS ANDSUPRARENALS
Remove fatand fasciafrom ant.
Kidneys &suprarenals insitu.
Kidneys andsuprarenals
Renal fascia 7other coveringsof kidneys
surface ofkidneys andsuprarenals
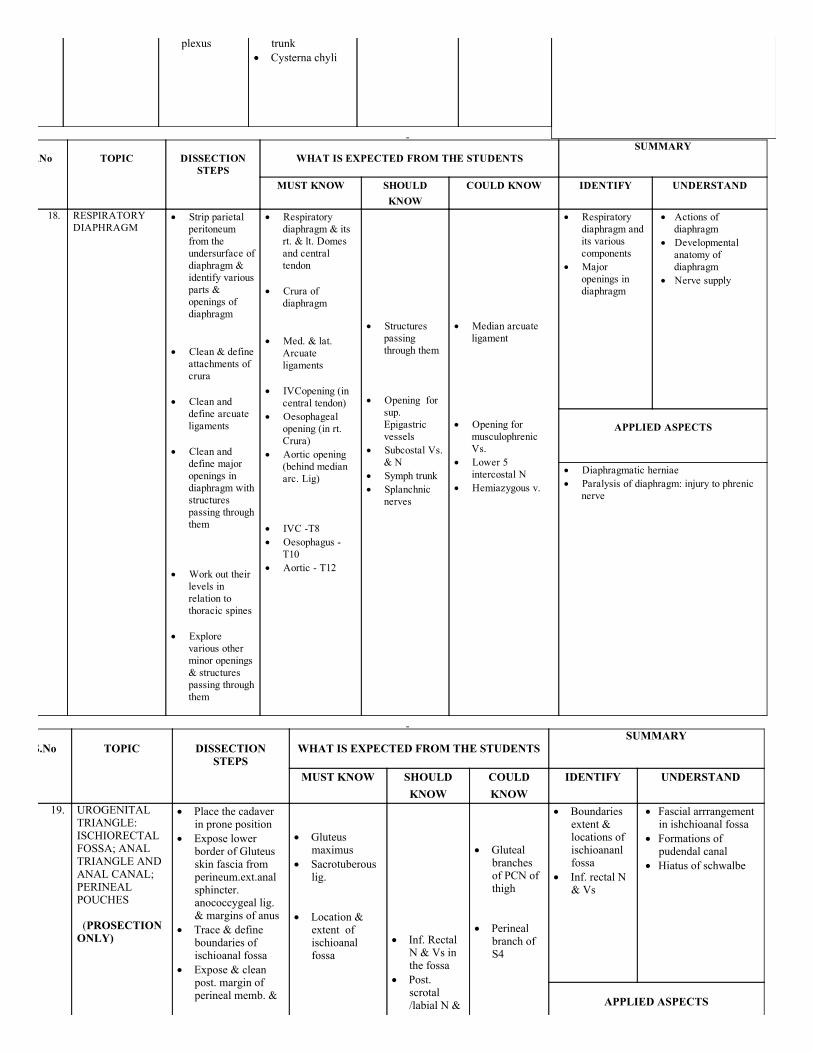
Clean & trace
ureters Mobilise both
the kidneys &turn themmedially
Separate
suprarenalsfrom renalfascia & notetheir relations
Removesuprarenalsand note.
Cut ureter atlower pole ofkidneys &renal vessels2cm from thehilum andremove them
Study post.relations
Cut one
kidney alongits lateralborder intotwo equalhalves(ant. &post) andstudy the cutsection withthe help ofdiagram
Renal vessels Termination of
Lt. Suprarenal& Lt gonadalveins in Lt.Renal vein
Kidneys:position,coverings andrelations
Ureter: Course,relations,normalconstrictionsand bloodsupply
Lymphaticdrainage of thekidneys and theureter
Relations ofsuprarenals insitu
Differences inshapes ofsuprarenals
Determine theside &anatomicalposition
Coronal section:Cortex,medulla,pyramid,calyces, pelvisof ureter
Branch to Lt.
Suprarenal Suprarenal
arteries Positions of
suprarenal veins Vascular
segments
Branch to
ureter Brodal's
line
Sidedeterminationof kidney
Differencesbetweensuprarenals
Post. relationsof kidneys
Supports ofkidneys.
Anatomicalbasis of:
Floating kidneyPolycystic kidneyPelvic kidneyHorseshoe shaped kidney
APPLIED ASPECTS
Renal angle Palpation / percussion of the kidney
(bimanual) Differentiation of renal enlargement
from splenic enlargment Surgical approach to kidney & ureter Pyelography & its indications Renal / ureteric coli Varicocoele. Renal infarction Polycystic kidney
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULD KNOW COULD KNOW IDENTIFY UNDERSTAND 17. POSTERIOR
ABDOMINALWALL
Clean thepost. abdo.Wall &denude itfrom allfascia andidentify
Clean
muscles ofpostr.abdo.wall &identify them
Clean &
trace nerveson posteriorabdominalwall
Dissect the
lumbar
IVC & itstributaries
Abdo.aorta & itsbranches
Sympathetictrunk on eitherside of aorta
Quadratus
.lumborum Psoa major &
minor Iliacus Subcostal
iliohypogastric Ilioiniguinal Femoral Obturator Lumbosacral
Azygos vein Hemiazygous
vein Genitofemoral
Cisterna chyli
&continuationupwards asthoracic ducts
Lat.cut.N of
thigh
Structures inpost.abdo.wall.
Muscles: Q.lumborum P. major Iliacus Nerves Symp. Trunk Femoral Obturator Aorta & its
branches IVC & its
tributaries
Arrangement ofabdominopelvicfascia on post.abdo. wall
APPLIED ASPECTS
Caries spine Psoas abscess Meralgia parasthetica IVC obstruction
plexus
trunk Cysterna chyli
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULD KNOW IDENTIFY UNDERSTAND
18. RESPIRATORYDIAPHRAGM
Strip parietalperitoneumfrom theundersurface ofdiaphragm &identify variousparts &openings ofdiaphragm
Clean & define
attachments ofcrura
Clean and
define arcuateligaments
Clean and
define majoropenings indiaphragm withstructurespassing throughthem
Work out their
levels inrelation tothoracic spines
Explore
various otherminor openings& structurespassing throughthem
Respiratorydiaphragm & itsrt. & lt. Domesand centraltendon
Crura of
diaphragm Med. & lat.
Arcuateligaments
IVCopening (in
central tendon) Oesophageal
opening (in rt.Crura)
Aortic opening (behind medianarc. Lig)
IVC T8 Oesophagus
T10 Aortic T12
Structures
passingthrough them
Opening for
sup.Epigastricvessels
Subcostal Vs.& N
Symph trunk Splanchnic
nerves
Median arcuate
ligament Opening for
musculophrenicVs.
Lower 5intercostal N
Hemiazygous v.
Respiratorydiaphragm andits variouscomponents
Majoropenings indiaphragm
Actions ofdiaphragm
Developmentalanatomy ofdiaphragm
Nerve supply
APPLIED ASPECTS
Diaphragmatic herniae Paralysis of diaphragm: injury to phrenic
nerve
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
19. UROGENITALTRIANGLE:ISCHIORECTALFOSSA; ANALTRIANGLE ANDANAL CANAL;PERINEALPOUCHES (PROSECTIONONLY)
Place the cadaverin prone position
Expose lowerborder of Gluteusskin fascia fromperineum.ext.analsphincter.anococcygeal lig.& margins of anus
Trace & defineboundaries ofischioanal fossa
Expose & cleanpost. margin ofperineal memb. &
Gluteus
maximus Sacrotuberous
lig. Location &
extent ofischioanalfossa
Inf. Rectal
N & Vs inthe fossa
Post.scrotal/labial N &
Gluteal
branchesof PCN ofthigh
Perineal
branch ofS4
Boundariesextent &locations ofischioananlfossa
Inf. rectal N& Vs
Fascial arrrangementin ishchioanal fossa
Formations ofpudendal canal
Hiatus of schwalbe
APPLIED ASPECTS
identify Trace inf. Rectal N
& Vs to lat. Wallof fossa
Remove all fatfrom the fossa
Clean and definepudendal canal onlat. Wall of fossa
Remove all fatfrom the fossa
Clean and definepudendal canal onlat. Wall of fossa
Vs Pudendal
canal Pudendal
nerve Internal
pudendal vessels.
Ischioanal abscess Pain Drainage Ischiorectal hernia
S.No
TOPIC
DISSECTIONSTEPS
WHAT IS EXPECTED FROM THE STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
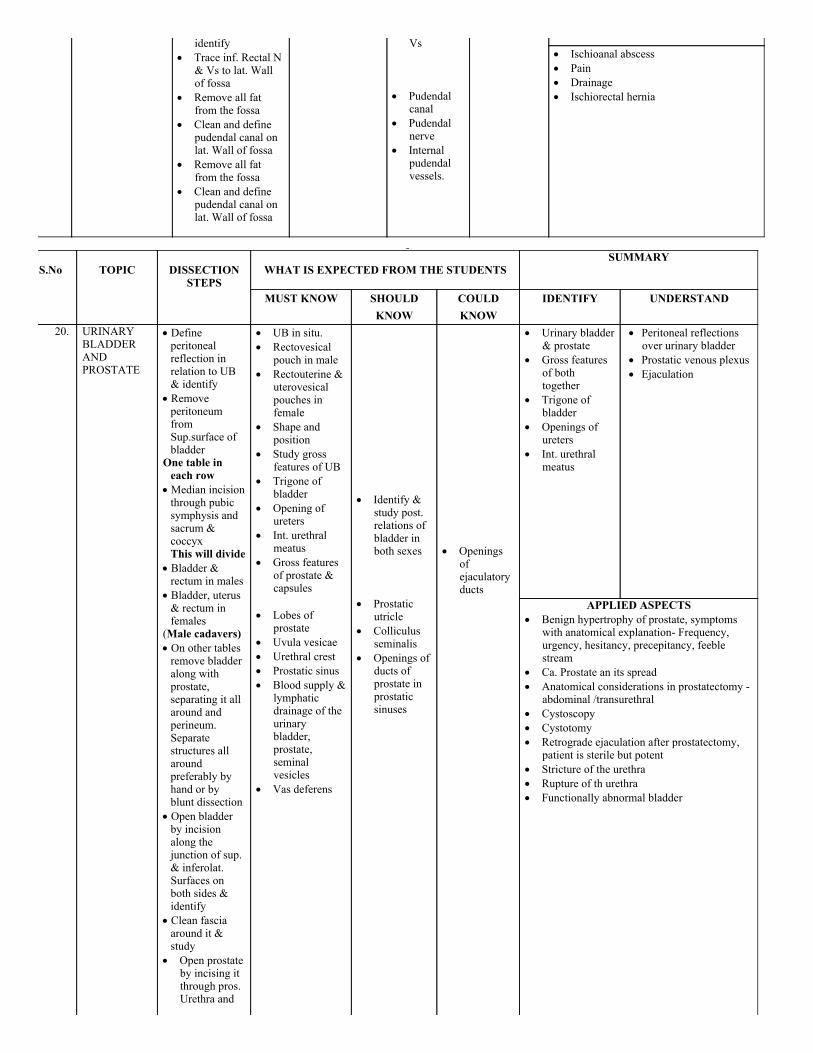
20. URINARY BLADDERANDPROSTATE
Defineperitonealreflection in relation to UB& identify
RemoveperitoneumfromSup.surface ofbladder
One table ineach row
Median incisionthrough pubicsymphysis andsacrum &coccyxThis will divide
Bladder &rectum in males
Bladder, uterus& rectum infemales
(Male cadavers) On other tablesremove bladderalong withprostate,separating it allaround andperineum.Separatestructures allaroundpreferably byhand or byblunt dissection
Open bladderby incisionalong thejunction of sup.& inferolat.Surfaces onboth sides &identify
Clean fasciaaround it &study
Open prostateby incising itthrough pros.Urethra and
UB in situ. Rectovesical
pouch in male Rectouterine &
uterovesicalpouches infemale
Shape andposition
Study grossfeatures of UB
Trigone ofbladder
Opening ofureters
Int. urethralmeatus
Gross featuresof prostate &capsules
Lobes of
prostate Uvula vesicae Urethral crest Prostatic sinus Blood supply &
lymphaticdrainage of theurinarybladder,prostate,seminalvesicles
Vas deferens
Identify &
study post.relations ofbladder inboth sexes
Prostatic
utricle Colliculus
seminalis Openings of
ducts ofprostate inprostaticsinuses
Openings
ofejaculatoryducts
Urinary bladder& prostate
Gross featuresof both together
Trigone ofbladder
Openings ofureters
Int. urethralmeatus
Peritoneal reflectionsover urinary bladder
Prostatic venous plexus Ejaculation
APPLIED ASPECTS Benign hypertrophy of prostate, symptoms
with anatomical explanation Frequency,urgency, hesitancy, precepitancy, feeblestream
Ca. Prostate an its spread Anatomical considerations in prostatectomy
abdominal /transurethral Cystoscopy Cystotomy Retrograde ejaculation after prostatectomy,
patient is sterile but potent Stricture of the urethra Rupture of th urethra Functionally abnormal bladder
identify
S.No
TOPIC
DISSECTION
STEPS
WHAT IS EXPECTED FROM THE
STUDENTS
SUMMARY
MUST KNOW SHOULDKNOW
COULDKNOW
IDENTIFY UNDERSTAND
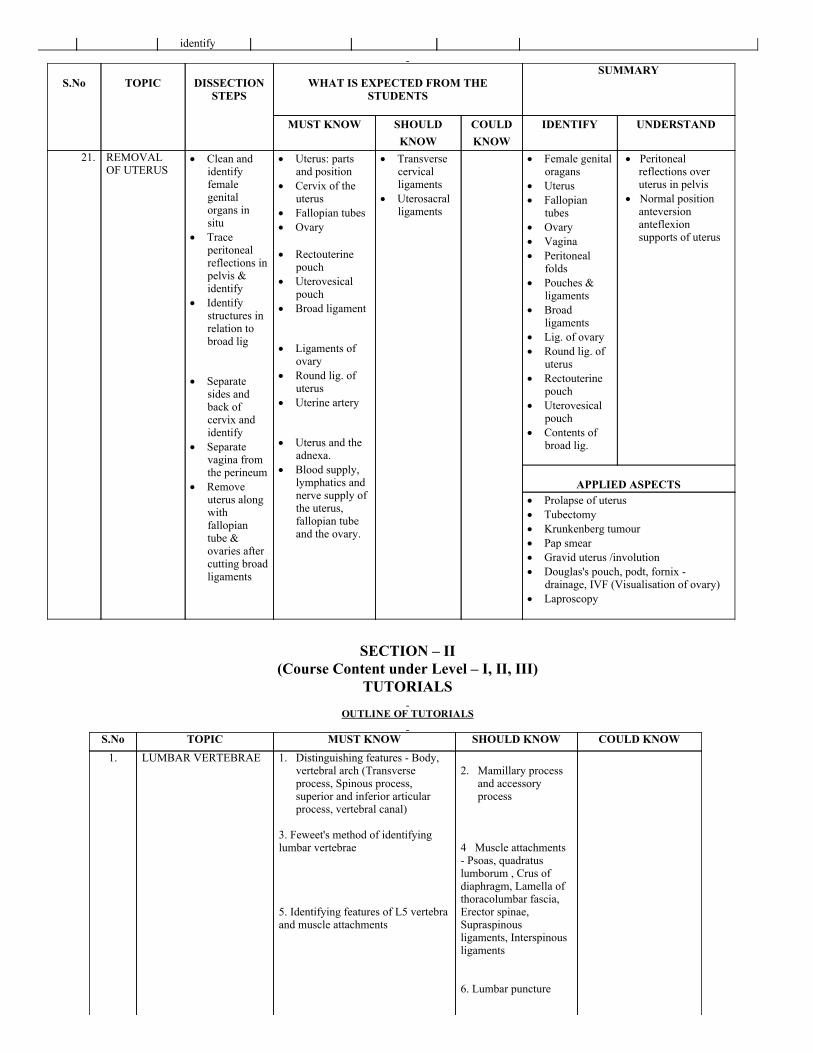
21. REMOVALOF UTERUS
Clean andidentifyfemalegenitalorgans insitu
Traceperitonealreflections inpelvis &identify
Identifystructures inrelation tobroad lig
Separate
sides andback ofcervix andidentify
Separatevagina fromthe perineum
Removeuterus alongwithfallopiantube &ovaries aftercutting broadligaments
Uterus: partsand position
Cervix of theuterus
Fallopian tubes Ovary Rectouterine
pouch Uterovesical
pouch Broad ligament Ligaments of
ovary Round lig. of
uterus Uterine artery Uterus and the
adnexa. Blood supply,
lymphatics andnerve supply ofthe uterus,fallopian tubeand the ovary.
Transversecervicalligaments
Uterosacralligaments
Female genitaloragans
Uterus Fallopian
tubes Ovary Vagina Peritoneal
folds Pouches &
ligaments Broad
ligaments Lig. of ovary Round lig. of
uterus Rectouterine
pouch Uterovesical
pouch Contents of
broad lig.
Peritonealreflections overuterus in pelvis
Normal positionanteversionanteflexionsupports of uterus
APPLIED ASPECTS
Prolapse of uterus Tubectomy Krunkenberg tumour Pap smear Gravid uterus /involution Douglas's pouch, podt, fornix
drainage, IVF (Visualisation of ovary) Laproscopy
SECTION – II(Course Content under Level – I, II, III)
TUTORIALS
OUTLINE OF TUTORIALS
S.No TOPIC MUST KNOW SHOULD KNOW COULD KNOW1. LUMBAR VERTEBRAE
1. Distinguishing features Body,
vertebral arch (Transverseprocess, Spinous process,superior and inferior articularprocess, vertebral canal)
3. Feweet's method of identifyinglumbar vertebrae 5. Identifying features of L5 vertebraand muscle attachments
2. Mamillary process
and accessoryprocess
4 Muscle attachments Psoas, quadratuslumborum , Crus ofdiaphragm, Lamella ofthoracolumbar fascia,Erector spinae,Supraspinousligaments, Interspinousligaments 6. Lumbar puncture
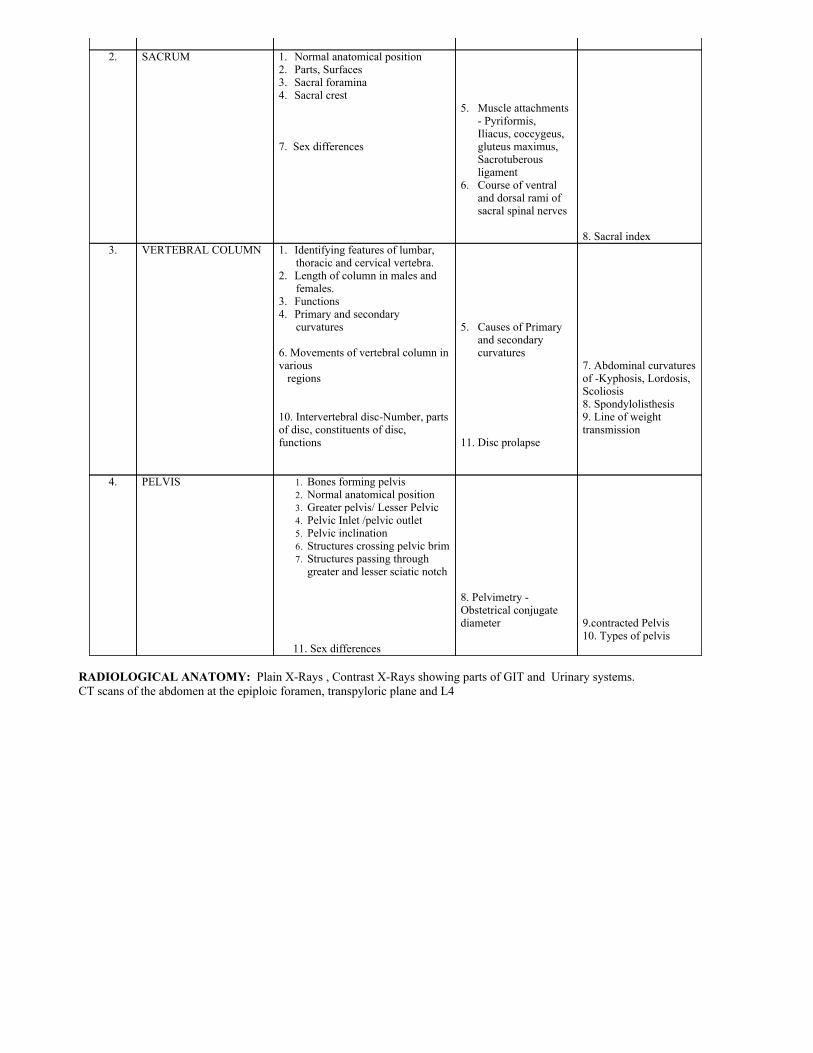
2. SACRUM 1. Normal anatomical position
2. Parts, Surfaces3. Sacral foramina4. Sacral crest 7. Sex differences
5. Muscle attachments
Pyriformis,Iliacus, coccygeus,gluteus maximus,Sacrotuberousligament
6. Course of ventraland dorsal rami ofsacral spinal nerves
8. Sacral index
3. VERTEBRAL COLUMN 1. Identifying features of lumbar,thoracic and cervical vertebra.
2. Length of column in males andfemales.
3. Functions4. Primary and secondary
curvatures 6. Movements of vertebral column invarious regions 10. Intervertebral discNumber, partsof disc, constituents of disc,functions
5. Causes of Primary
and secondarycurvatures
11. Disc prolapse
7. Abdominal curvaturesof Kyphosis, Lordosis,Scoliosis8. Spondylolisthesis9. Line of weighttransmission
4. PELVIS 1. Bones forming pelvis2. Normal anatomical position3. Greater pelvis/ Lesser Pelvic4. Pelvic Inlet /pelvic outlet5. Pelvic inclination6. Structures crossing pelvic brim7. Structures passing throughgreater and lesser sciatic notch
11. Sex differences
8. Pelvimetry Obstetrical conjugatediameter
9.contracted Pelvis10. Types of pelvis
RADIOLOGICAL ANATOMY: Plain XRays , Contrast XRays showing parts of GIT and Urinary systems.CT scans of the abdomen at the epiploic foramen, transpyloric plane and L4





























