-
Secondary pulmonary TB
Lu huaDept. of Pathology Three Gorges University Medical
College
www.rxdentistry.blogspot.com
-
Secondary pulmonary TB() Outline usually results from
reactivation of dormant, endogenous tubercle bacilli in a
sensitized patient who has had previous contact with the tubercle
bacillus.
www.rxdentistry.blogspot.com
-
1. Reinfectionusually adults adult type pulmonary TBInitiated
from apex of lung secondary focus
www.rxdentistry.blogspot.com
-
2. Pathogenesis Exogenous reinfection not related to primary
infection Endogenous reinfection PP TB spread via bloodstream
Primary bronchial Extrapulmonary TBbloodlung
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
() Features of lesion
www.rxdentistry.blogspot.com
-
1. Initial focus: Site : apex of the lung local resistence Stand
A pressure poor circulation macrophageAb Bad ventilation
www.rxdentistry.blogspot.com
-
2. Features of lesion Hypersensitivity: Easily caseous necrosis,
liquefy,cavity Immune response: stronger localized focus
proliferation tubercle
www.rxdentistry.blogspot.com
-
3. The ways of spread Lymphatics Bloodstream less prominently
involved Bronchia : main
www.rxdentistry.blogspot.com
-
4. Clinical course long period of time better or worse new and
old lesion mixed up
www.rxdentistry.blogspot.com
-
Pathological change and types1.Focal pulmonary TB2.Infiltrative
pulmonary TB3. Chronic fibro-cavitative4. Caseous pneumonia5.
Tuberculoma6. Tuberculous pleuritis
www.rxdentistry.blogspot.com
-
Pathological change and types1.Focal pulmonary TBinitial lesion
of secondary pulmonary TB(1) Lesion usually below apex 2-4cm ,
0.5-1cm in size , clear edge proliferation main
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
(2) Results Healing in most cases: fibrosis, calcification
Progressinfiltrative pulmonary TB
www.rxdentistry.blogspot.com
-
2. Infiltrative pulmonary TBmost common type of active pulmonary
TB
Arising in:progress of focal pulmonary TBfew cases occur
initially
www.rxdentistry.blogspot.com
-
(2) Lesion sitebelow clavicle, unclear edge center: smaller
caseous necrosis surrounding: surrounded by inflammation exudative
serous fluid, monocytes, LC, neutrophils
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
(3) Clinical features Symptoms: low-grade fever, anorexia ,
fatigue, weight loss, night sweats , general malaise cough .
hemoptysis (cavitary disease). Tubercle bacilli (+)
www.rxdentistry.blogspot.com
-
(4) Results Healing: treatment earlier
absorption, fibrosis, encapsulation, calcification
www.rxdentistry.blogspot.com
-
Progress Caseous necrosis liquefied
bronchialcaseous pneumonia
destroy pleura spontaneous pneumothorax
thoracic cavitytuberculous pyopneumothorax
persistentchronic fibro-cavitative pulmonary TB
www.rxdentistry.blogspot.com
-
fibrosisabsorbedcalcificationspreadFinal result:Most healingLess
solution and spread
www.rxdentistry.blogspot.com
-
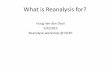
3. Chronic fibro-cavitative pulmonary TB adult, common type(1)
Arising in: usually acute cavity of infiltrative pulmonary TB
www.rxdentistry.blogspot.com
-
Formation of thick wall cavity one or more bilateral lung upper
lobe of lung variation in size irregular shape(2) Features of
lesion
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
Cavity wall (LM) : three layers1.inner:caseous necrosis
2.midial:tuberculous granulation tissue
3.outer: fibrous tissue123
www.rxdentistry.blogspot.com
-
123
www.rxdentistry.blogspot.com
-
within cavity: bridge like appearance
vessels which have thrombosis organization
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
Unilateral or bilateral lung: new or old, variation in size,
different types of lesion Adjacent tissue widely fibrosis pleura
thickened
sclerosing pulmonary TB
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
(3) Clinical features
Origin of infection open pulmonary tuberculosis Hemoptysis
(eroding large vessels)
Death
www.rxdentistry.blogspot.com
-
An 80-year-old female who exsanguinated from massive hemoptysis
due to tuberculosis and bronchiectasis.
www.rxdentistry.blogspot.com
-
Widely fibrosis pulmonary hypertension cor pulmonale Small
cavityscar Large cavityopen healing
www.rxdentistry.blogspot.com
-
Sputum with bacteria throat and intestinal TB Destroy pleura:
pneumothorax pyopneumothorax
www.rxdentistry.blogspot.com
-
4. Caseous pneumonia(1) Arising in:immunity, allergyinfiltrative
type pulmonary TBbacteria in acute or chronic cavity, disseminated
by bronchi
www.rxdentistry.blogspot.com
-
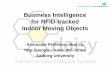
(2) Lesions lobular lobar Gross: enlargement of lobe,
consolidation ,acute cavity LM: alveoli filled with serofibrous
exudates, many macrophages, widely caseous necrosis necrosis
exudation, Bac (+)
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
(3) Clinical features bad prognosis
deathgalloping consumption
www.rxdentistry.blogspot.com
-
5. Tuberculoma(1) Arising in:Infiltrative P.TB large necrotic
focus F. encapsulationCavity: draining bronchi blocked cavity
filled with necrosisFusion of several focus
www.rxdentistry.blogspot.com
-
(2) Lesions solitary, fibrous encapsulated, clear edge, round,
caseous necrosis focusdiameter: 2-5cm
number: usually one, sometime multiple site: upper lobe
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
(3) Clinical ferturesrelative motionlesshealing: organization,
calcificationdevelopment: Necrosis , focus
extensionLiquefiedcavitySpread by bronchi
www.rxdentistry.blogspot.com
-
6. Tuberculous pleuritis(1) Arising in: primary and all stage of
secondary pulmonary TB
www.rxdentistry.blogspot.com
-
(2) Lesions Exudative TB pleuritis(siccus) Source: primary
pulmonary TB ( primary focus or TB of LN )
same side pleura
www.rxdentistry.blogspot.com
-
bacilli of focus or hilar lymphonodusspreadpleura sensitive
reaction: bacteria protein
www.rxdentistry.blogspot.com
-
Lesion: serofibrous inflammationResults: absorption completely:
hydrothorax organization: thicken, adhesion
www.rxdentistry.blogspot.com
-
Proliferative TB pleuritis (humectus) source: focus below pleura
extending directly
lesions: usually apex of lung, localized proliferation mainly,
less hydrothorax
results: fibrosispleura thicken, adhesion
Caseous pleurisy: not frequently seen special type
www.rxdentistry.blogspot.com
-
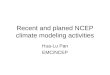
Primary SecondaryInfection Primary SecondaryPatients Children
Adult Immune or None Establishedhypersensitivity Characteristics
Primary complex VariableInitial focus Lower part of upper lobe Apex
of the lung upper part of lower lobe close to the pleuraFeatures
Exudation and necrosis Proliferation and necrosisDissemination
Lymphatic or hematogenous BronchialClinical course
Short,spontaneous healing Long, instable
www.rxdentistry.blogspot.com
-
primary PTBsecondary PTBextrapulmonaryderived from. Hematogenous
TB
www.rxdentistry.blogspot.com
-
1. Acute systemic miliary TBprimary focuseroding vein of
lungleft heartall the organs (lung, liver, brain, spleen,
kidney)miliary TBv
www.rxdentistry.blogspot.com
-
(1) Gross: scattered uniformly , similar size resemblance to
millet , yellow-white with clear edge(2) LM: main :proliferative
lesion tubercle exudation or necrosis
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
(3) Clinical course: obvious symptoms treatment in time well
prognosis lesstuberculous meningitisdeath
www.rxdentistry.blogspot.com
-
2. Chronic systemic miliary TB: common in adultexudation +
proliferation + necrosislesionuneven
www.rxdentistry.blogspot.com
-
3. Acute pulmonary miliary TBa part of acute systemic miliary
TB: commonlimited in lung: less
www.rxdentistry.blogspot.com
-
Caseous necrosis of tracheo-bronchial and mediastinal, hilar LN
vein corner right heartlungacute miliary tuberculosis
www.rxdentistry.blogspot.com
-
Gross: both lung congestion, increasing weight, cut surface
dark-red in color, numerous grey or grey-yellow miliary nodules in
size rising on surface of lung
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
www.rxdentistry.blogspot.com
-
4. Chronic pulmonary miliary TB common in
adultExtrapulmonary-TBTB bacilli (outside lung)long period
intermissionbloodnew or old lesion
www.rxdentistry.blogspot.com
-
Import knowledges:Tuberculoma2. Caseous pneumoniaQuestion:The
difference between Primary P TB and Secondary P TB .
www.rxdentistry.blogspot.com