Embed Size (px)
DESCRIPTION
Diseases of the Respiratory System Lu hua. Dept. of Pathology Three Gorges University Medical College. Emphysema. Definition - PowerPoint PPT Presentation
Citation preview
Diseases of the Respiratory System
Lu hua
Dept. of Pathology Three Gorges University Medical College

Emphysema

DefinitionEmphysema is a condition of the lung characterized by abnormal permanent enlargement of the airspaces distal to the terminal bronchiole, accompanied by destruction of their walls and without obvious fibrosis.

In contrast, the enlargement of airspaces unaccompanied by destruction is termed "overinflation“.Interstitial emphysema--is characterized by the entrance of air into the connective tissue stroma of the lung, mediastinum, or subcutaneous tissue . (rib fracture , penetrating injury of chest, coughing plus some bronchiolar obstruction, etc.)
Compensatory emphysema-- the distention of airspaces that occurs in the remaining lung parenchyma that follows surgical removal of a diseased lung or lobe.
senile emphysema--For the elastic force of older pulmonary tissue change to weakened, it make pulmonary residual volume increased and cause lung expansion.
Obstructive Overinflation--Obstructive overinflation refers to the condition in which the lung expands because air is trapped within it. A common cause is subtotal obstruction by a tumor or foreign object.
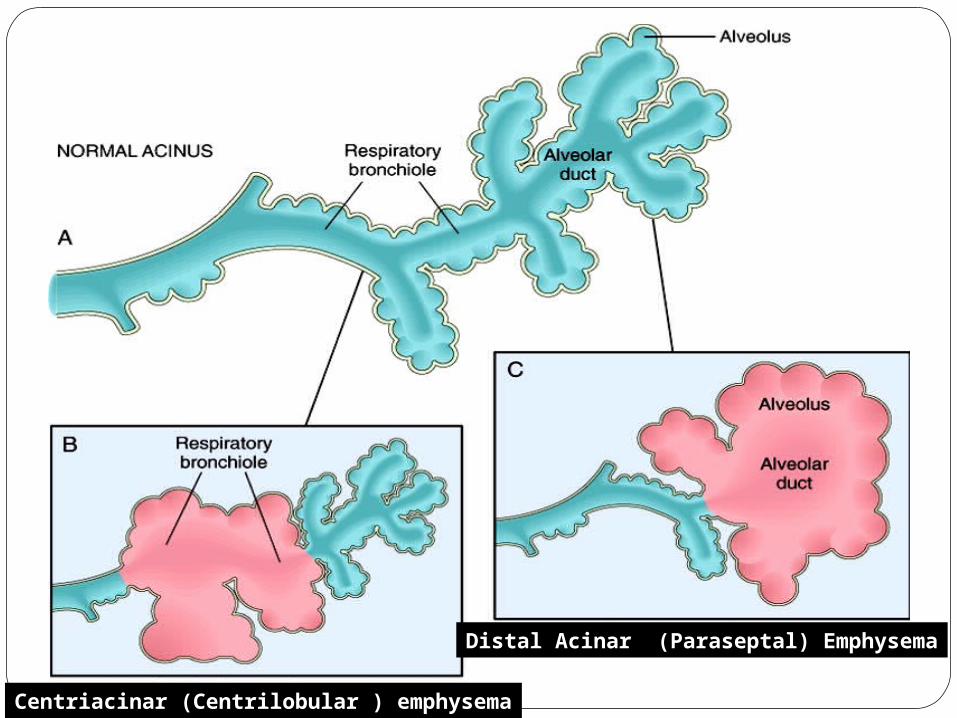
Types of true emphysema: four major types
•Centriacinar (Centrilobular ) emphysema
•The central or proximal parts of the acini, formed by respiratory bronchioles, are affected, whereas distal alveoli are spared.
•Distal Acinar (Paraseptal) Emphysema
•The proximal portion of the acinus is normal, but the distal part is predominantly involved.
•Panacinar (Panlobular) Emphysema•The acini are uniformly enlarged from the level of the respiratory bronchiole to the terminal blind alveoli
•Irregular Emphysema (Airspace Enlargement with Fibrosis)
Irregular emphysema, so named because the acinus is irregularly involved, is almost invariably associated with scarring.
Thus, it may be the most common form of emphysema because careful search of most lungs at autopsy shows one or more scars from a healed inflammatory process.
In most instances, these foci of irregular emphysema are often asymptomatic, clinically insignificant and only an accidental autopsy finding.
Distal Acinar (Paraseptal) Emphysema
Centriacinar (Centrilobular ) emphysema
Pathogenesis: synergy of many factors
Two main factors:
1.Bronchial obstruction
2.The protease-antiprotease theory
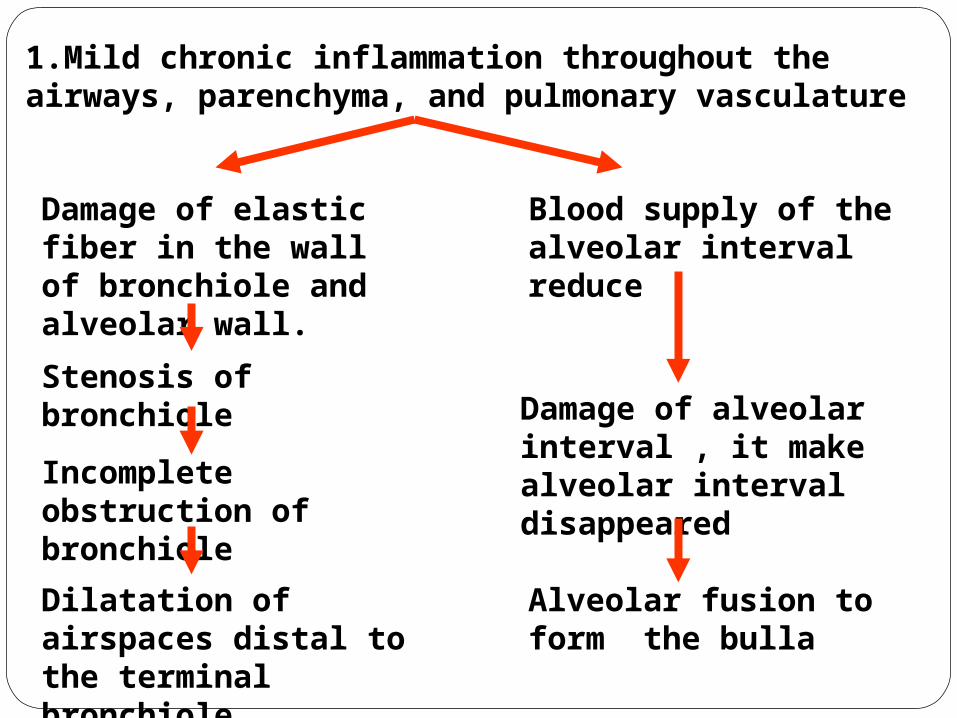
1.Mild chronic inflammation throughout the airways, parenchyma, and pulmonary vasculature
Damage of elastic fiber in the wall of bronchiole and alveolar wall.
Stenosis of bronchiole
Incomplete obstruction of bronchiole
Dilatation of airspaces distal to the terminal bronchiole
Blood supply of the alveolar interval reduce
Damage of alveolar interval , it make alveolar interval disappeared
Alveolar fusion to form the bulla

Inadequate ventilation Less perfusion Narrowed bronchioleDestruction of alveolar walls
2.The protease-antiprotease theory
The most plausible hypothesis to account for the
destruction of alveolar walls is the protease-antiprotease
mechanism, aided and abetted by oxidant-antioxidant
imbalance.
The protease-antiprotease theory holds that alveolar
wall destruction results from an imbalance between
proteases (mainly elastase) and antiproteases in the
lung.
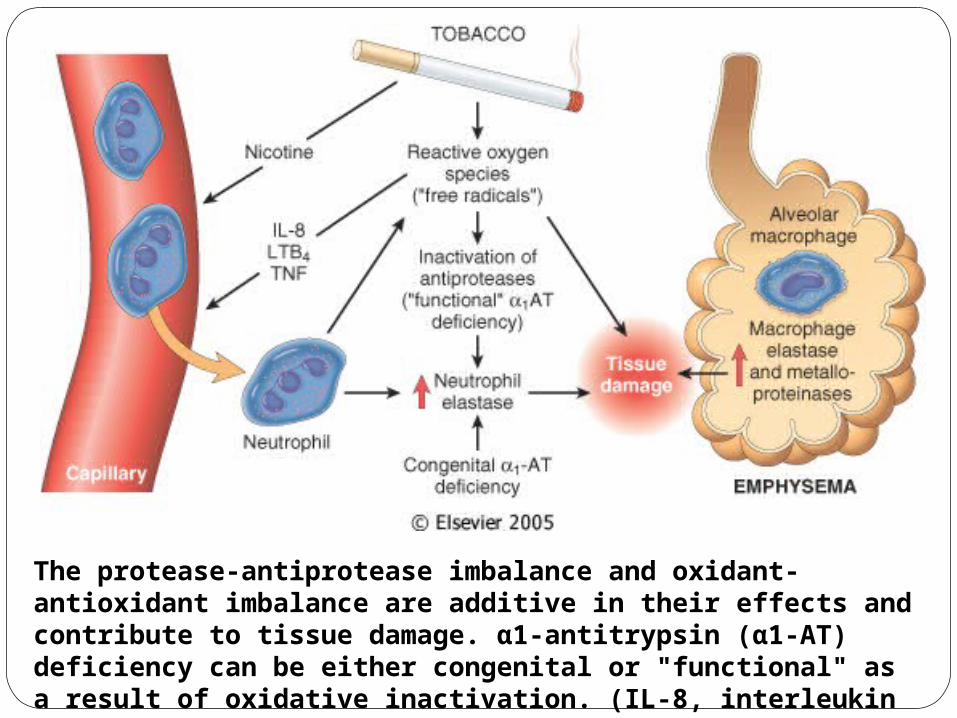
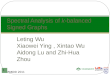
The protease-antiprotease imbalance and oxidant-antioxidant imbalance are additive in their effects and contribute to tissue damage. α1-antitrypsin (α1-AT) deficiency can be either congenital or "functional" as a result of oxidative inactivation. (IL-8, interleukin 8; LTB4, leukotriene B4; TNF, tumor necrosis factor.)
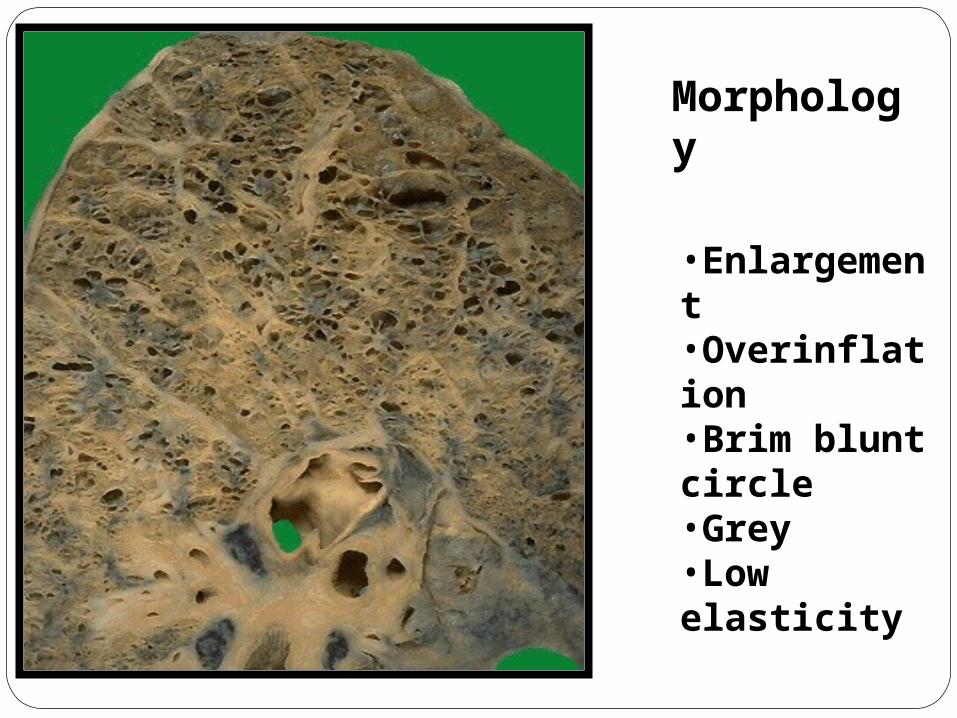
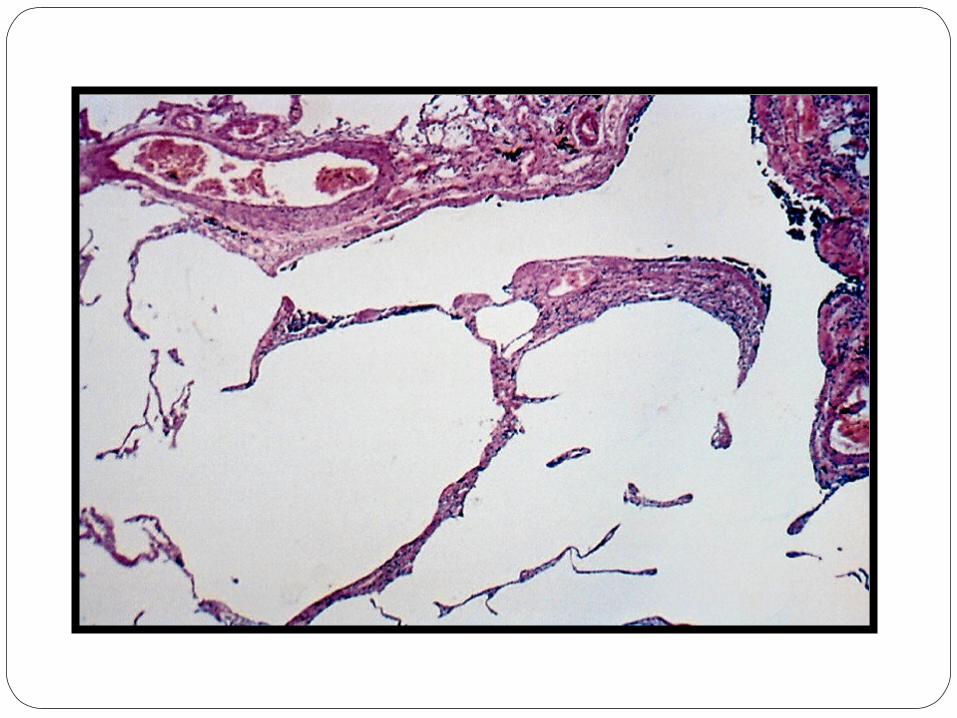
Morphology
•Enlargement•Overinflation•Brim blunt circle•Grey•Low elasticity
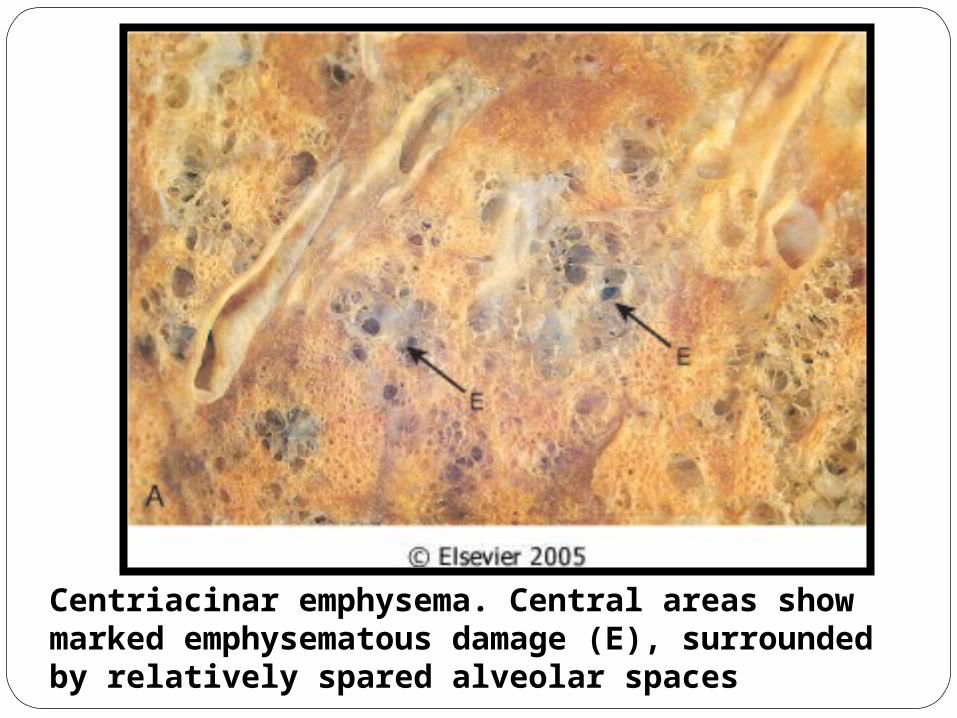
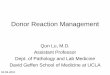
Centriacinar emphysema. Central areas show marked emphysematous damage (E), surrounded by relatively spared alveolar spaces
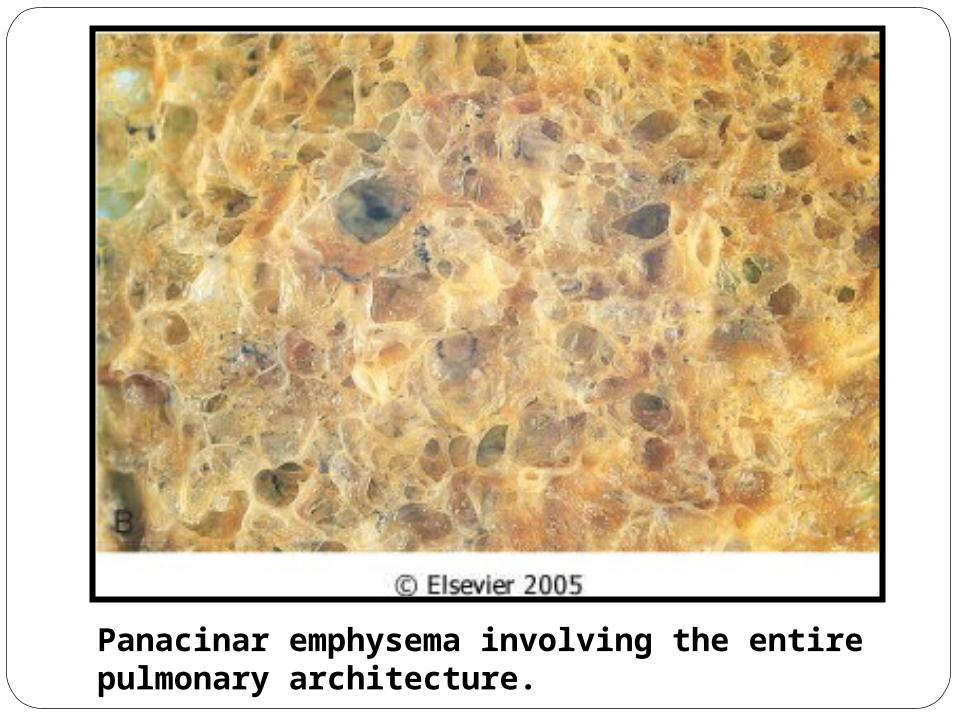
Panacinar emphysema involving the entire pulmonary architecture.

镜下:
Thin and stretched alveolar walls
Spurs of broken septa
Distended alveoli and alveolar duct
Inflammatory changes are usually absent.
Clinical features: The clinical manifestations of emphysema do not appear until at least one third of the functioning pulmonary parenchyma is damaged.
Dyspnea----it is usually the first symptom; it begins insidiously but is steadily progressive.
Cough and expectoration----these are extremely variable and depend on the extent of the associated bronchitis.
Weight loss— it is common and can be so severe as to suggest a hidden malignant tumor.
Barrel-chested
Such patients may overventilate and remain well oxygenated and therefore are somewhat ingloriously designated as pink puffers (PP type).
Patients with chronic bronchitis more often have a history of recurrent infection, abundant purulent sputum, hypercapnia, and severe hypoxemia, prompting the equally inglorious designation of blue bloaters (BB type).
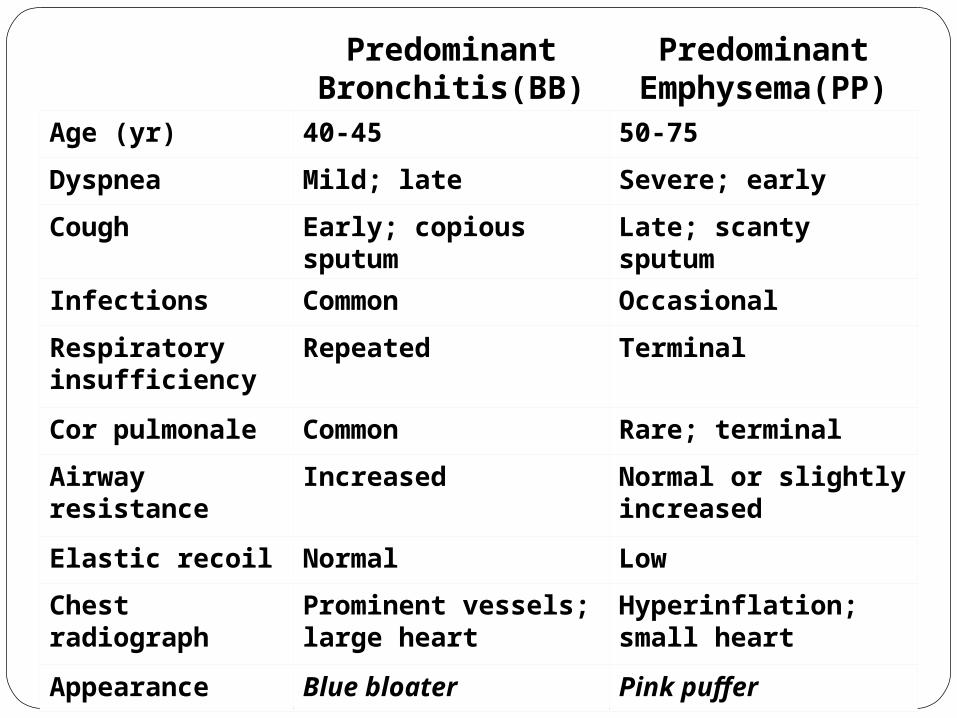
Predominant
Bronchitis(BB)Predominant
Emphysema(PP)Age (yr) 40-45 50-75
Dyspnea Mild; late Severe; early
Cough Early; copious sputum Late; scanty sputum
Infections Common Occasional
Respiratory insufficiency
Repeated Terminal
Cor pulmonale Common Rare; terminal
Airway resistance Increased Normal or slightly increased
Elastic recoil Normal Low
Chest radiograph Prominent vessels; large heart
Hyperinflation; small heart
Appearance Blue bloater Pink puffer
Death in most patients is due to
(1)Respiratory acidosis and coma
(2)Right-sided heart failure
(3)Massive collapse of the lungs secondary to pneumothorax.
Bronchial Asthma

Asthma is a chronic inflammatory disorder of the airways that causes recurrent episodes of wheezing, breathlessness, chest tightness, and cough, particularly at night and/or in the early morning.
These symptoms are usually associated with widespread but variable bronchoconstriction and airflow limitation that is at least partly reversible, either spontaneously or with treatment.
It is thought that inflammation causes an increase in airway responsiveness (bronchospasm) to a variety of stimuli.
Etiopathogenesis and types:
Typically, asthma is categorized into three types:
•Extrinsic (atopic, allergic) asthma —initiated by a type I hypersensitivity reaction induced by exposure to an extrinsic antigen
•Intrinsic (idiosyncratic, non-atopic) asthma —initiated by diverse, nonimmune mechanisms, including ingestion of aspirin; pulmonary infections, especially viral; cold; inhaled irritants; stress; and exercise
•Mixed type —many patients do not clearly fit into either of the above two categories and have mixed features of both.
Morphology features:
Grossly;
Overdistended --the lungs are overdistended because of overinflation, and there may be small areas of atelectasis.
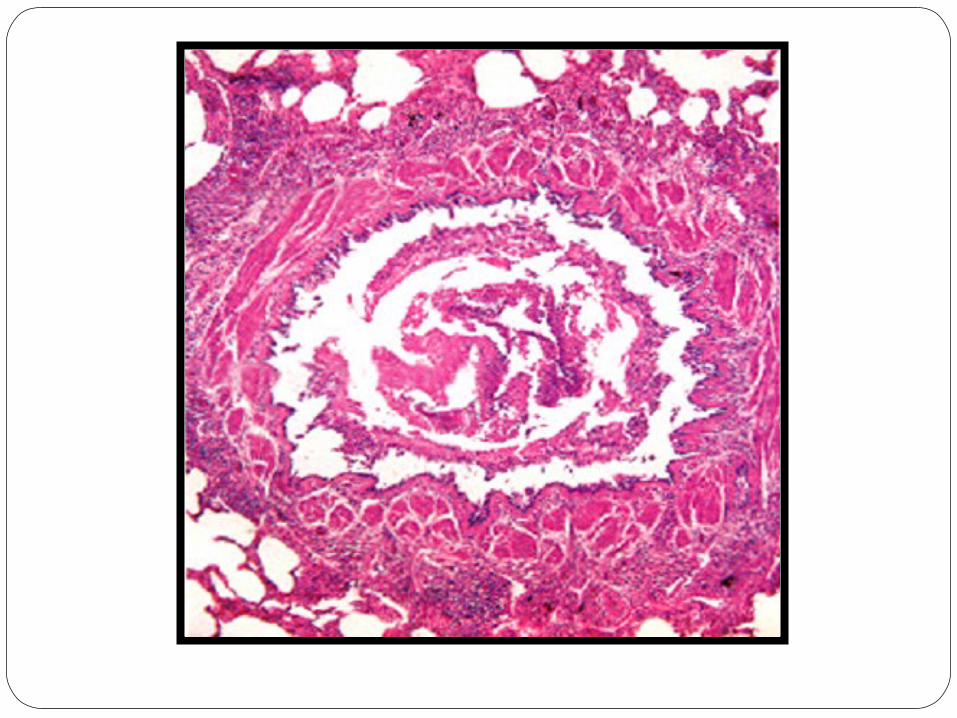
Mucous plugs --The most striking macroscopic finding is occlusion of bronchi and bronchioles by thick, tenacious mucous plugs.

Hyperinflated lungs of a patient who died with
status asthmaticus.
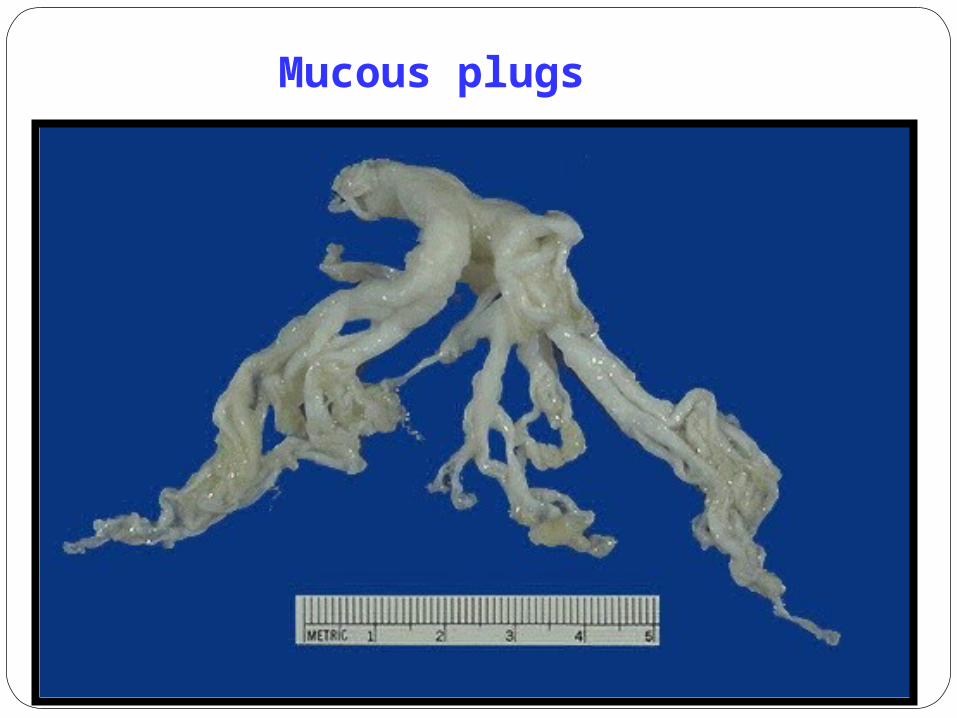
Mucous plugs
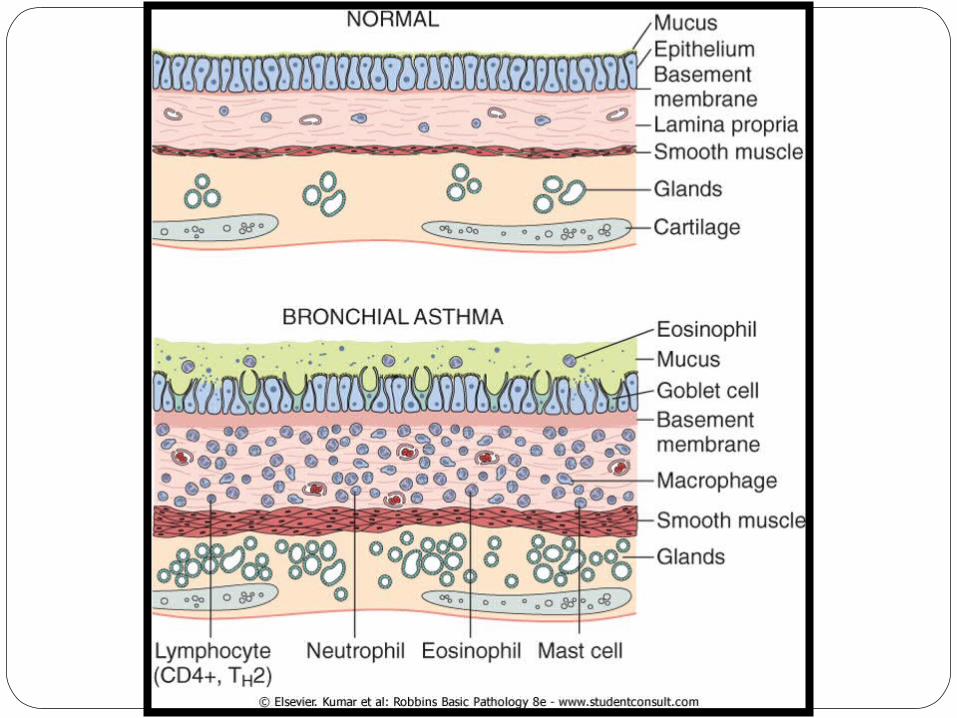
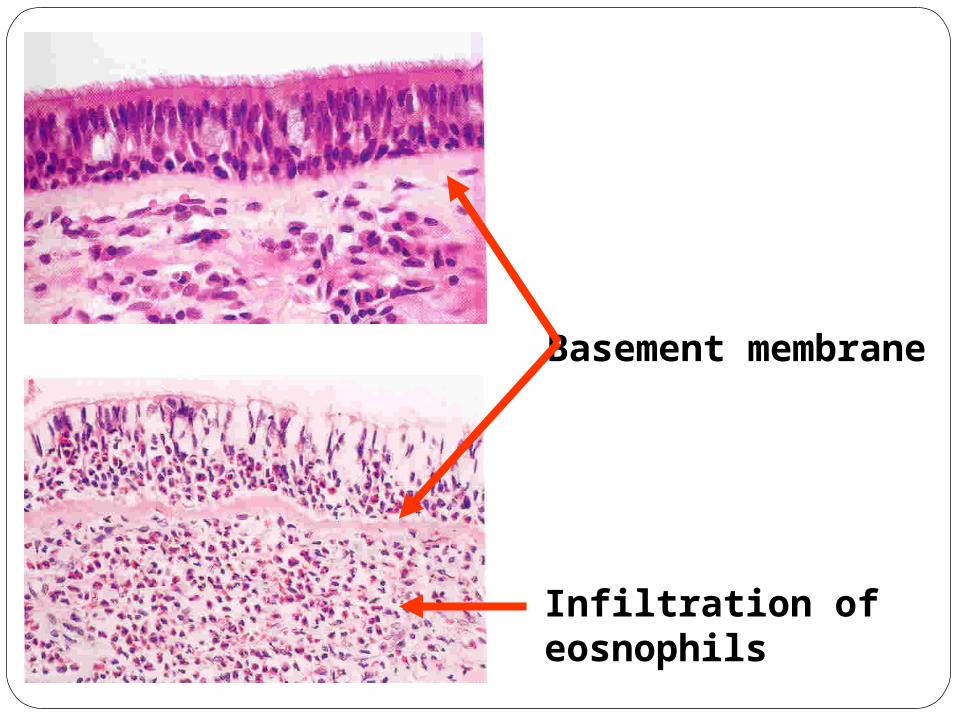
Infiltration of eosnophils
Basement membrane

Smooth muscle thickening
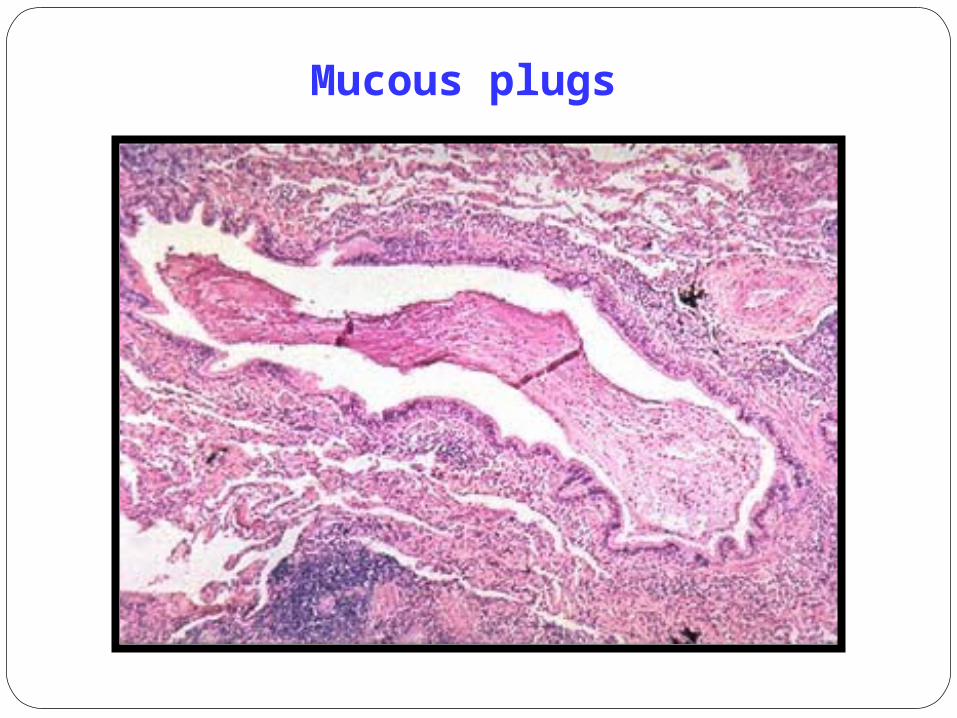
Mucous plugs
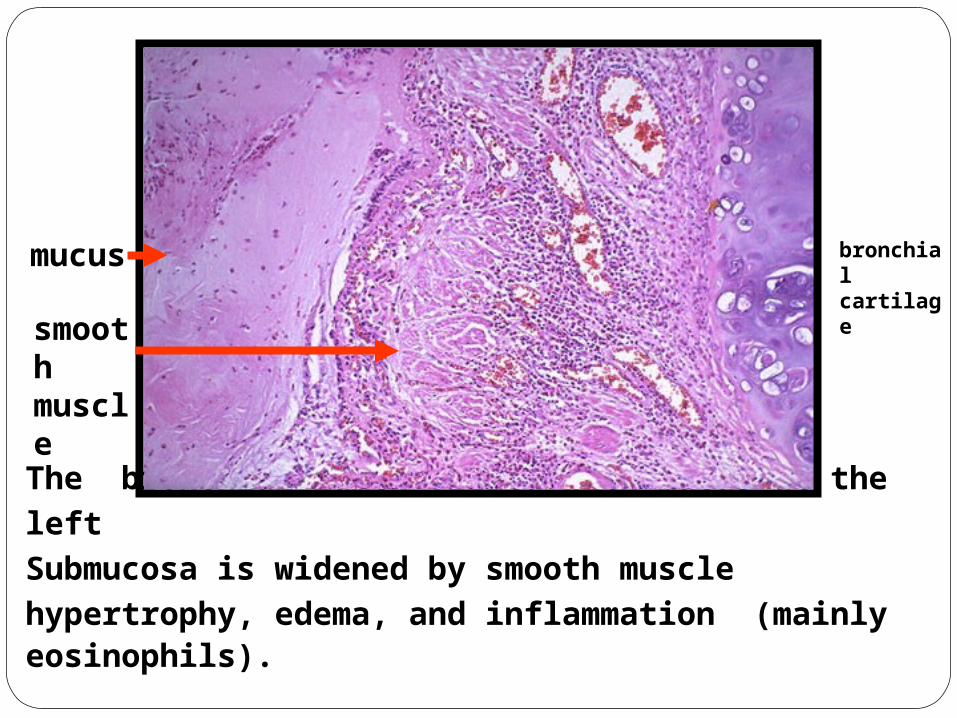
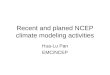
The bronchial lumen filled with mucus at the left
Submucosa is widened by smooth muscle hypertrophy, edema, and inflammation (mainly eosinophils).
bronchial cartilage
mucus
smooth muscle

At high magnification, the numerous eosinophils are
prominent from their bright red cytoplasmic granules in this case of bronchial asthma
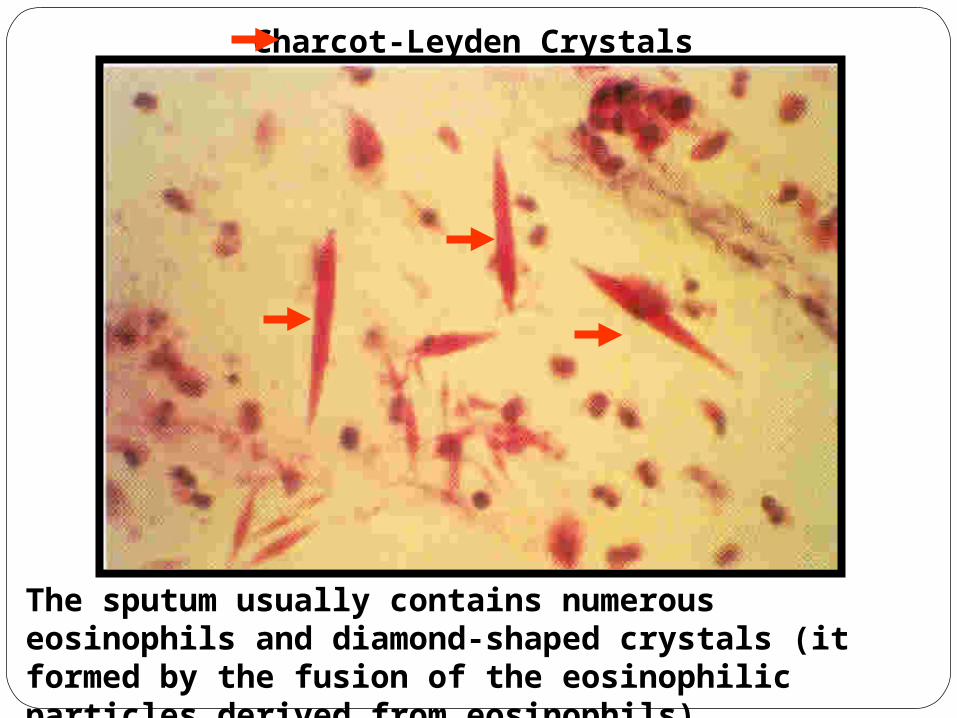
Charcot-Leyden Crystals
The sputum usually contains numerous eosinophils and diamond-shaped crystals (it formed by the fusion of the eosinophilic particles derived from eosinophils).

Clinical Term
Anatomic Site
Major Pathologic Changes Etiology
Signs/Symptoms
Chronic bronchitis
Bronchus Mucous gland hyperplasia, hypersecretion
Tobacco smoke, air pollutants
Cough, sputum production
Bronchiectasis
Bronchus Airway dilation and scarring
Persistent or severe infections
Cough, purulent sputum, fever
Asthma Bronchus Smooth muscle hyperplasia, excess mucus, inflammation
Immunologic or undefined causes
Episodic wheezing, cough, dyspnea
Emphysema
Acinus Airspace enlargement; wall destruction
Tobacco smoke
Dyspnea
The Spectrum of COPD