Embed Size (px)
Citation preview

The Seated Lateral Radiograph is a Better Stress View of the
Lumbar SpineJ. Alex Sielatycki, M.D.
Tyler Metcalf, B.S.Clinton Devin, M.D. Scott Hodges, M.D.
Center for Sports Medicine and Orthopaedic SurgeryChattanooga, TN

Background
• Standing flexion/extension x-rays are widely used for dynamic assessment of the lumbar spine
• Patient effort, body habitus, and guarding may limit the ability of such films to estimate lumbar range of motion or instability

Background
• The pelvis retroverts more with sitting than with standing flexion
• Thus with sitting the lumbar spine must go into relative kyphosis to maintain forward gaze.
• We hypothesized that seated lateral x-rays would more effectively show angular range of motion in the lumbar spine compared to standing flexion

Methods
• Plain radiographs were taken of adults presenting to our outpatient clinic with lumbar complaints.
• X-Rays obtained:• Standing lateral (patients instructed to stand upright with forward gaze)• Max forward flexion (patients asked to bend forward towards floor as far as possible)• Max extension (patients asked to maximally extend the low back and look up)• Seated lateral (patients asked to sit comfortably in hard-back chair with back against the
backrest)
• Lumbar parameters and angular measurements were made in each position, and changes in angular measures were recorded compared to the standing neutral lateral image.

MethodsTable 1: Demographics (N = 70)
L1-S1 Movers L1-S1 Stiff P-Value
Male 16 (42%) 14 (44%) -
Female 22 (58%) 18 (56%) 0.89
Age 48.2 59 0.001
• 70 patient radiographs were analyzed
• Patients were excluded in cases of: prior fusion, infection, tumor, trauma, or if unable to cooperate with standing radiographs
• Patients were divided into those moving more than 20 degrees from standing to sitting (“Movers”) vs. those who showed less than 20 degrees of angular motion from L1-S1 (”Stiff”).

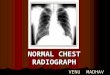
ResultsTable 2: All patients (n= 70)
Change with Sitting % Change with Flexion % P-ValueL1-S1 Lordosis -21.60 36% -15.8 26% 0.004L1-L3 Lordosis -5 56% -6.4 65% 0.3L3-4 Lordosis -5 33% -4.5 27% 0.2L4-S1 -12.5 33% -6.3 16% <0.001L4-L5 -6.7 34% -2.8 8% <0.001L5-S1 -5.8 29% -3.5 16% 0.001Pelvic Tilt 20 126% -12.7 -66% <0.001Sacral Slope -17.5 -50% -13.7 40% <0.001
• Overall, seated lateral radiographs showed greater angular range of motion as compared with standing flexion
• Global L1-S1 lordosis decreased more with sitting
• Angular range of motion from L1-L4 was minimal whether patients were seated or standing in flexion (average of 5 degrees of less motion)
• Greater angular range of motion was seen across the lower lumbar segments (L4-S1) in both groups, with larger differences in the seated x-rays

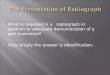
ResultsTable 3: Patients that move MORE than 20 degrees L1-S1 (n = 38)
Change with Sitting % Change with Flexion % P-ValueL1-S1 Lordosis -32 53% -20 32% <0.001L1-L3 Lordosis -7 70% -7.9 96% 0.17L3-4 Lordosis -7.4 50% -5.2 33% 0.02L4-S1 -17.8 46% -7.4 19% <0.001L4-L5 -9.9 49% -3.7 9% <0.001L5-S1 -7.9 39% -4.1 19% <0.001Pelvic Tilt 23.1 150% -11.3 -61% <0.001Sacral Slope -20.9 -61% 13.6 39% <0.001
• Among patients that moved at least 20 degrees from standing to sitting, differences in angular range of motion between standing and sitting were accentuated.
• L4-L5 showed the greatest single-level change from standing to sitting, followed by L5-S1 and L3-L4.
• Even in the more mobile group, relatively little angular motion was seen from L1-L3
• *** We did not observe a difference in amount of spondylolisthesis between standing and sitting in this patient population

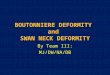
Results
• Among “stiff” patients that did not have at least 20 degrees of motion from standing to sitting, there wereno significant differences in angular range of motion between standing and sitting
• Thus a certain subset of patients have a relatively “stiff” lumbar spine even without prior fusion• On further analysis, “Stiffness” was associated with older age as expected. • There was no statistical association of stiffness with diabetes, smoking status, or BMI
Table 4: Patients that move LESS than 20 degrees L1-S1 (n = 32)Change with Sitting % Change with Flexion % P-Value
L1-S1 Lordosis -9.9 17% -12.4 20% 0.28L1-L3 Lordosis -3 28% -4.9 42% 0.29L3-4 Lordosis -2.5 17% -4 27% 0.2L4-S1 -6.5 18% -5.1 12% 0.06L4-L5 -2.8 15% -2 6% 0.14L5-S1 -3.6 19% -3.1 14% 0.19Pelvic Tilt 17.2 104% -14.4 -69% <0.001Sacral Slope -13.6 -37% 14.4 41% <0.001

Results

Conclusions:
• Seated lateral x-rays place the lumbar spine into more relative kyphosis as compared with standing flexion• Especially at the lower lumbar segments (L4-S1) where most degenerative
pathology occurs
• We recommend utilizing the seated lateral radiograph for dynamic assessment of the lumbar spine
• Future studies are underway to investigate changes in angular ROM above prior fusion

Limitations
• We did not detect a difference in spondylolisthesis between standing flexion and sitting. Out of the 70 patients reviewed, only 8 patients had any listhesis; thus, we were likely underpowered to detect such a difference.
• We did not utilize slumped-sitting or flexion in the seated posture for this analysis. We now ask patients to sit AND flex forward, which we suspect will show even greater differences in angular range of motion.

Key References
• Hey HWD, Teo AQA, Tan KA, et al. How the spine differs in standing and in sitting-important considerations for correction of spinal deformity. Spine J2017;17:799-806.
• Dennis Hey HW, Choong DAW, Lin AZ, et al. Patient and radiographer assessment of slump sitting flexion compared to conventional standing forward bending flexion. J Spine Surg 2018;4:750-6.
• Sparrey CJ, Bailey JF, Safaee M, et al. Etiology of lumbar lordosis and its pathophysiology: a review of the evolution of lumbar lordosis, and the mechanics and biology of lumbar degeneration. Neurosurg Focus2014;36:E1.