Embed Size (px)
DESCRIPTION
SCREENING TEST. Dr. Khanchit Limpakarnjanarat Thailand MOPH – US CDC Collaboration (TUC). SCREENING TEST. Did any one of participants experience in using screening test in your daily work? What is it?. [ANC, health check up, patient with fever, surveillance, etc] - PowerPoint PPT Presentation
Citation preview

1
SCREENING TEST
Dr. Khanchit LimpakarnjanaratThailand MOPH – US CDC Collaboration
(TUC)
2
SCREENING TEST
• Did any one of participants experience in using screening test in your daily work? What is it?
• [ANC, health check up, patient with fever, surveillance, etc]• Whenever primary prevention is possible, it is the best approach to prevent disease occurrence and/or epidemic.• Two possible approaches to early diagnosis
–Depends on awareness of warning signs–Active detection of disease in asymptomatic cases
3
Know the Seven Warning Signs of Cancer…
•Appearance of a lump in a breast or elsewhere
•A change in a mole or wart
•A sore that doesn't heal
•Indigestion or difficulty swallowing
•Nagging cough or hoarseness
•Unusual bleeding
•Persistent respiratory problems
[American Cancer Society]

4
CAGE screening for alcoholism
• Have you ever felt you should Cut down on your drinking?
• Have people Annoyed you by criticizing your drinking?
• Have you ever felt bad or Guilty about your drinking?
• Have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover (Eye-opener)?

5
The CAGE questions for alcohol abuse
Number of positive answers to the 4 CAGE questions
Alcohol abuse
YES NO
3 or 4
2, 1 or none
ac d
b
a + c
b + d
c + d
a + b
a + b + c + d
(True +)
60
(False +)
1
400
(True -)
57
(False -)117
401
518
457
61
Suckett D. A Primer on the Precision and Accuracy of the Clinical Examination. JAMA 267(19):2638-2644, May 1992
Sens. = 60/117=0.51Spec. = 400/401=0.998
PVP = 60/61 = 0.98PVN = 400/457 = 0.88
6
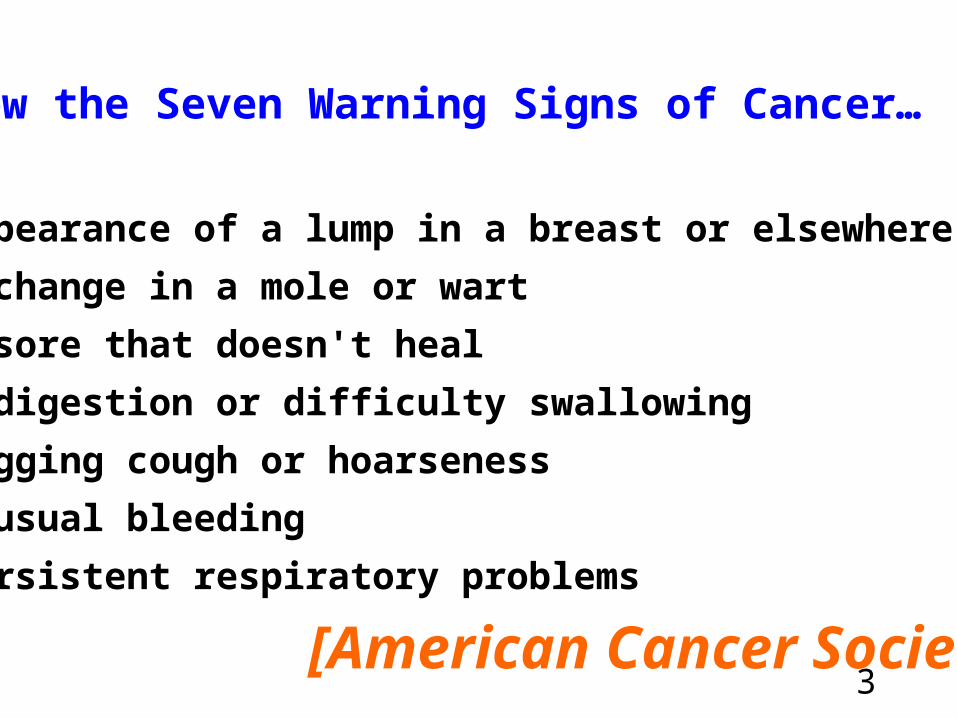
Schema relating path of detection to outcome
[Dr. Maureen Handerson]A. CURRENT SITUATION
Self referral Care for chromic
disease
Diagnosis
Surveillance Recovery
B. FUTURE PROJECTION
Self referral Care for chromic
disease
Diagnosis
Surveillance Recovery
Source: Mausner & Bahn: Epidemiology-an introductory text, Chapter9 - screening in detection of disease

7
Screening test
is the basic tool of screening program and must be thoroughly understood since screening is designed to be applied to large group of people, screening test should be easy to use, rapid and inexpensive. They should also be able to carry out largely by technicians
1.2
8
Screening Test
Definition: the PRESUMPTIVE
identification of unrecognized disease or defect by the application of tests, examinations, or other procedures which can be applied rapidly to sort out apparently well persons who probably have a disease from those who probably do not.
A screening test is not intended to be diagnostic. Persons with positive or suspicious findings must be referred to their physicians for diagnosis and necessary treatment.
[Commissioned on Chronic Illness –1951]

9
Goal of Screening Test
•To reduce morbidity or mortality from the disease among the people screened by early treatment of the cases discovered. (Clinical Medicine)
•To help guide preventive and control measures in general or specific populations. (Epidemiology and Public Health)

10Flow diagram for a mass screening test
APPARENTLY WELL POPULATION TO BE TESTED(Well persons plus those with
undiagnosed disease)
+
Negatives on test
Positives on test, no diseasePositives on test, disease present
+
++
+
Rescreen at prescribed interval
Negatives (normal)
- persons presumed to be free of disease under study
SCREENING TEST
++++
+
+++++
++
+
++DIAGNOS
TIC PROCEDURES
Positives (abnormal)
- persons presumed to have the disease or be at increased risk in future
THERAPEUTIC INTERVENTION
Disease or risk factor present
Disease or risk factor absent
Rescreen at prescribed interval

11
PURPOSES OF SCREENING
• DIAGNOSIS• IDENTIFY TOXIC CHEMICAL AGENTS• ESTIMATE MAGNITUDE OF DISEASE OR
PUBLIC HEALTH CONDITIONS• IDENTIFICATION OF PEOPLE AT HIGH RISK

12
PURPOSE OF SCREENING (1)
•DIAGNOSIS: Series of test perform on a symptomatic patient for whom a diagnosis has not yet been established.
Example: Patients with hematuria may need UA, urine culture, cystoscopy, bladder biopsy, several types of X-ray, several blood chemistry studies
13
PURPOSE OF SCREENING (2)
•IDENTIFY TOXIC CHEMICAL AGENTS: Chemical agents may be screened by means of laboratory tests or epidemiologic surveillance in order to identify those substances likely to be toxic.
Example: Pb poisoning surveillance by Pb screening among children

14
•ESTIMATE MAGNITUDE OF DISEASE OR PUBLIC HEALTH CONDITIONS: Some screening procedures can be used to estimate the prevalence of various conditions which may lead to disease control objectives. Major methodologic problem in this area is the relation between ‘detected’ prevalence and the underlying ‘true’ prevalence, e.g., sample size, sampling technics.
Example: Serologic testing, GenProbe testing, Cervical Pap’s smear, Tuberculin skin test, CXR
PURPOSE OF SCREENING (3)
15
PURPOSE OF SCREENING (4)
•IDENTIFICATION OF PEOPLE AT HIGH RISK: People at high risk may be who do not yet have the disease. The link between screening for a risk factor and a disease may not be sharp.
Example: Identify smokers, identify drinkers by MAST test, HT may be a risk factor for CVD or may be early disease detection itself
16
Types of Screening Program
• Selective screening specific disease in people at risk
• Mass screening test large number of people
17
Selective screening
• Selective screening: Tests are used to detect a specific disease among people who are at risk of having disease.– Single disease: e.g., CXR for pneumoconiosis in
coal miners or FBS for evidence of DM in diabetic patients’ relatives
– Multiphasic screening program: e.g., ANC in pregnant women

18
Mass screening
• Mass screening: Large number of people are tested for the presence of disease or condition without specific emphasis to their individual risk of having disease or condition– Single disease: e.g., cervical pathology for
cancer of cervix, mammography for breast cancer
– Multiphasic screening program: e.g., Biochemical profile in community survey

19
Lead time and screening test
• Lead time is the time interval from detection by screening test to the time at which diagnosis would have been made without that screening.
• Length of lead time interval may vary from person to person (short and long lead time)
• Importance of lead time is for disease control and by early detection and early treatment to prevent spread and disability of affected persons. Screening test is valuable in reducing severe morbidity and mortality
20
Measurements used in screening tests
• Validity – test is capable to differentiate presence or absence of disease
• Yield – brought unrecognized disease to diagnosis
• Reliability – consistent result when test more than once

21
Creation of 2 x 2 table – initial step for calculation
TEST “Screening”
+
-
Yes No
DISEASE “Gold standard”
a bc d
True pos False pos
False neg True neg
22
VALIDITY• Validity is the indication of which test is capable
of differentiating the presence or absence of a disease concerned
SENSITIVITY = ability of test to detect people who actually have the disease (True Positive)
SPECIFICITY = ability of test to identify correctly people who actually do not have the disease (True Negative)

23
1. Sensitivity = proportion of subjects with disease who have the positive test from screening
= a / a+c
or = TP / TP + FN2. Specificity = proportion of subjects without disease
who have the negative test from screening
= d / b+d
or = TN / FP + TN3. Accuracy of the test = a + d / a + b + c + d
= TP + TN / Total screened
Validity of screening test
24
YIELD
• Yield is the amount of previously unrecognized disease which is diagnosed and brought to treatment as a result of the screening
PREDICTIVE VALUE POSITIVE (PVP) is the likelihood that an individual with a positive test has the disease
PREDICTIVE VALUE NEGATIVE (PVN) is the likelihood that an individual with a negative test does not have the disease

25
Yield of screening test
• Predictive Value Positive (PVP)PVP = a / a + b
or = TP / TP + FP
• Predictive Value Negative (PVN)PVN = d / c + d
or = TN / TN + FN
9

26
RELIABILITY (Precision)
• Reliability is one that give consistent results when the test is performed more than once on the same individual under the same conditions. It is also called ‘Repeatability’
27
Reliability**Precision**Repeatability
Number of agreed positive= -------------------------------------
Number of positive either time
a= --------------
(a + b + c)

28
Trade off point
Cut off point“Criterion of Positivity”

29
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5Persons without disease
Persons with Disease
Trade off point
abc
d
Num
ber
o f p
ers o
n sReal situation of screening test
Persons with disease = a + c
Persons without disease = b + d
30
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
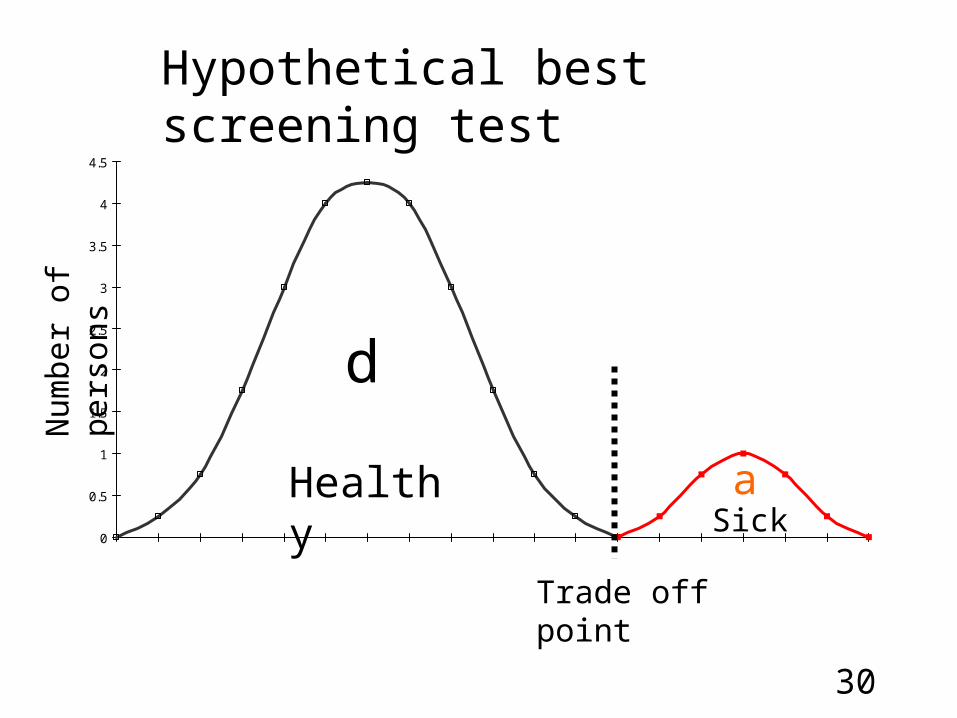
HealthySick
Trade off point
a
d
Num
ber
o f p
ers o
n sHypothetical best screening test

31
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Trade off point A
Healthy
Sick
Num
ber
of p
ers o
n sShifting of trade off point A
abc
d
X
32
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
HIV-free population
HIV-positive population
Num
ber
o f p
ers o
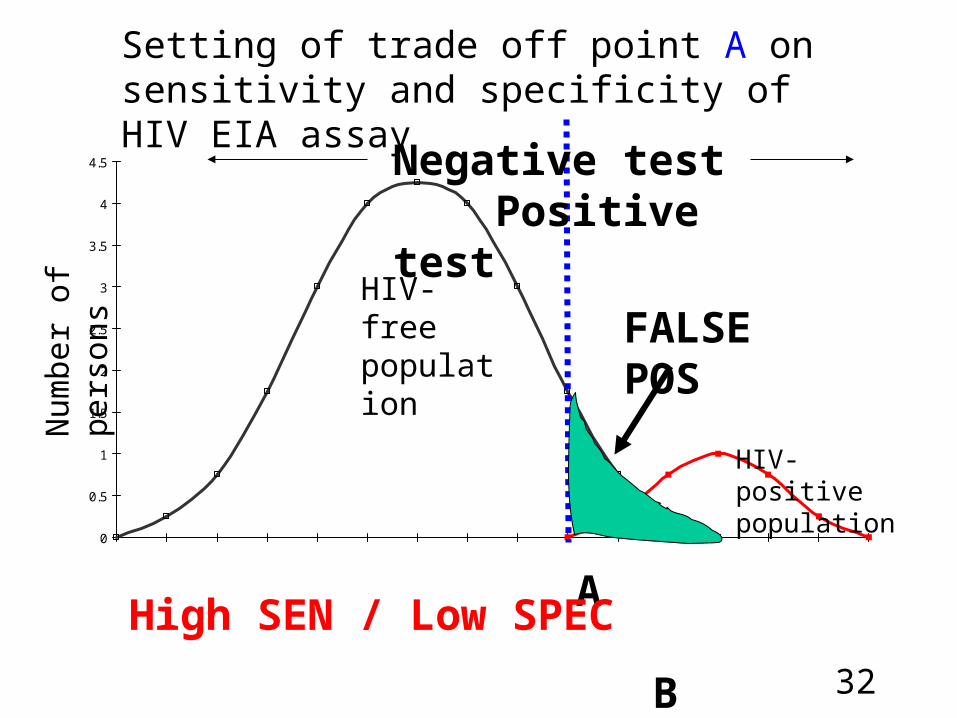
n sSetting of trade off point A on sensitivity and specificity of HIV EIA assay
c
A B
Negative test Positive test
FALSE POS
High SEN / Low SPEC
33
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
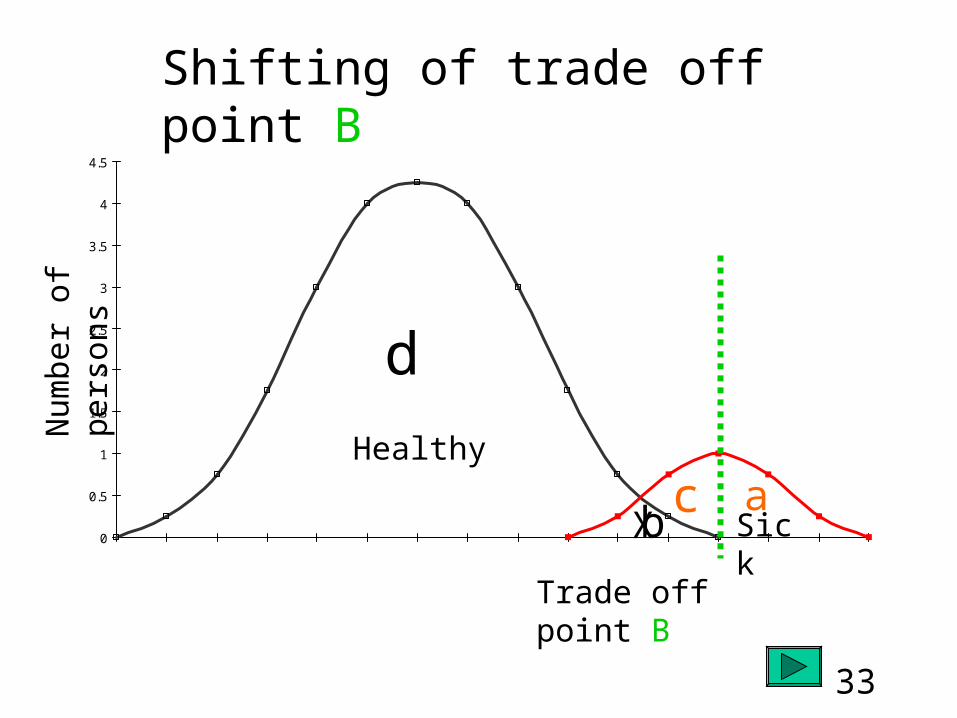
Trade off point B
Healthy
Sick
Num
ber
of p
ers o
n sShifting of trade off point B
ab
c
d
X

34
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
HIV-free population
HIV-positive population
Num
ber
o f p
ers o
n sSetting of trade off point B on sensitivity and specificity of HIV EIA assay
A B
Negative test Positive test
FALSE NEG
Low SEN / High SPEC
35
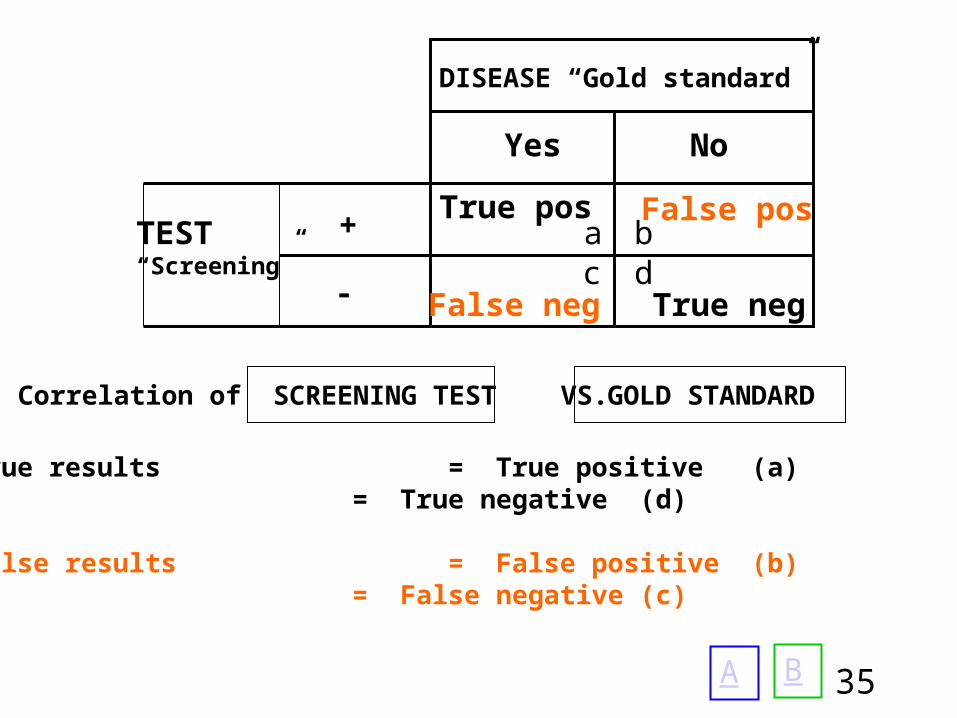
Correlation of SCREENING TEST VS.
True results = True positive (a)= True negative (d)
False results = False positive (b)= False negative (c)
GOLD STANDARD
A B
TEST “Screening”
+
-
Yes No
DISEASE “Gold standard”
a bc d
True pos False pos
False neg True neg
36
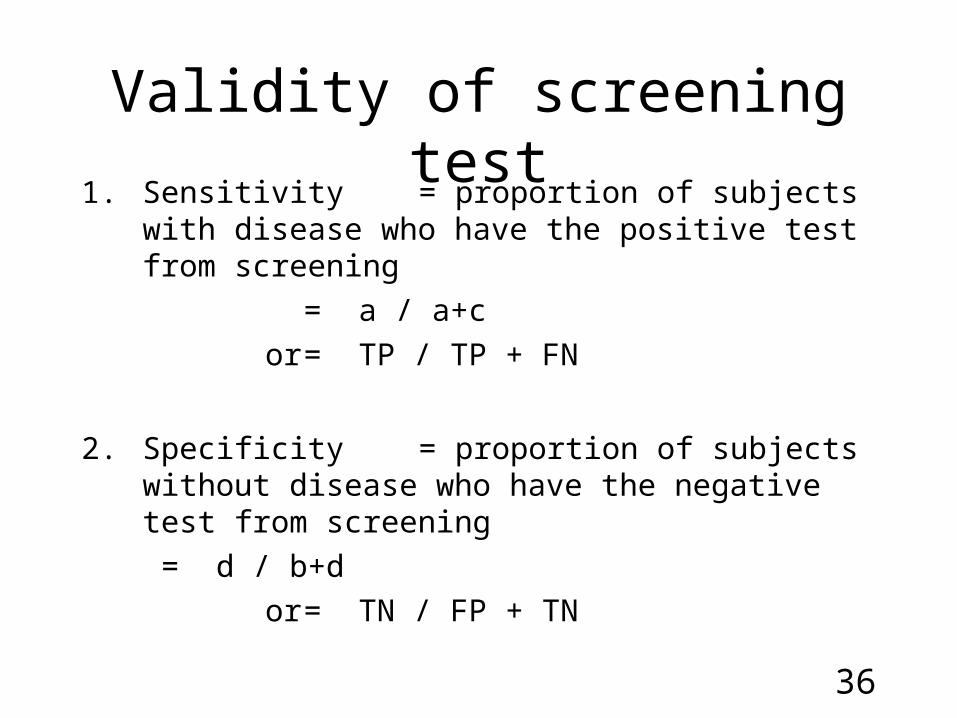
1. Sensitivity = proportion of subjects with disease who have the positive test from screening
= a / a+c
or = TP / TP + FN
2. Specificity = proportion of subjects without disease who have the negative test from screening
= d / b+d
or = TN / FP + TN
Validity of screening test

37
Specificity should be increased relative to sensitivity:
• When the false positive result can harm patient physically, emotionally, or financially, e.g., HIV infection
• When the cost or risk associated with further diagnostic technique are substantial, such as breast cancer, for which the definitive diagnostic evaluation of a positive screening test is a biopsy
38
Sensitivity should be increased at the expense of specificity:
• When the penalty associated with missing a case is high such as disease is serious and definitive treatment exist, e.g., PKU
• When the disease can spread, e.g., syphilis
• When subsequent diagnostic evaluations of positive screening tests are associated with minimal cost and risk, e.g., series of B.P. readings to ascertain HT
39
PROBLEMS WITH SCREENING TEST
1. Lack of information on negative tests : Prostate specific antigen (PSA) for
prostate cancer
2. Lack of information in the non-disease :MRI to diagnose prolapse disk
3. Lack of standards for disease• Consequence of imperfect standards : diagnosis of gall stone by U/S vs. Cholecystogram
Clinical Epidemiology - KKU
40
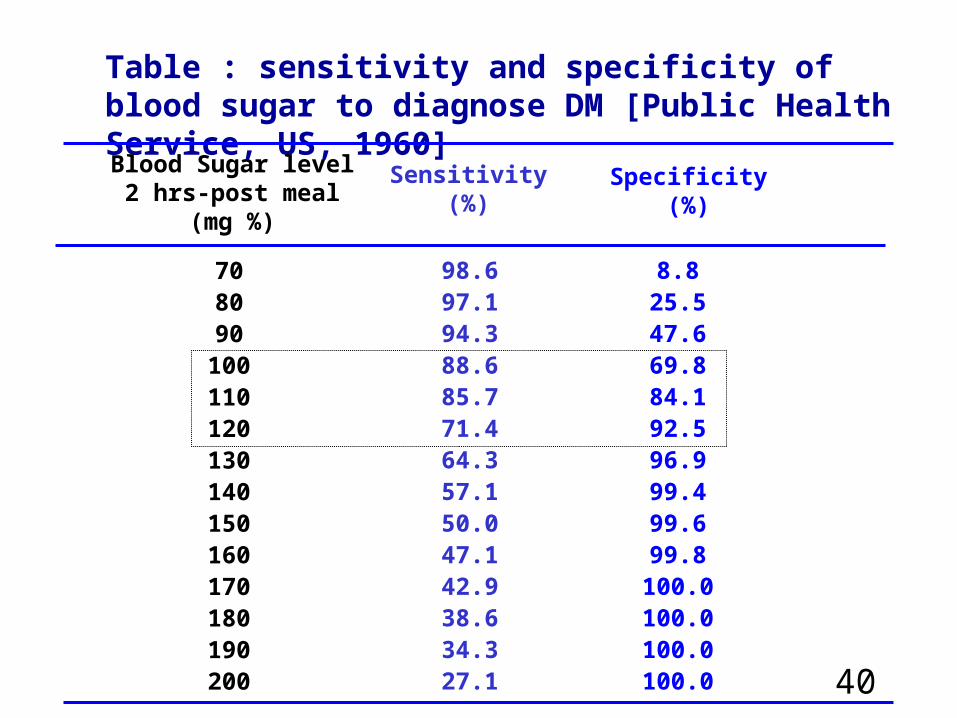
Table : sensitivity and specificity of blood sugar to diagnose DM [Public Health Service, US, 1960]
708090
100110120130140150160170180190200
98.697.194.388.685.771.464.357.150.047.142.938.634.327.1
8.825.547.669.884.192.596.999.499.699.8
100.0100.0100.0100.0
Blood Sugar level2 hrs-post meal
(mg %)
Sensitivity(%)
Specificity(%)

41
ROC of accuracy of blood sugar test (2 hours post meal) to diagnosis DM [Public Health Service, Diabetes program guide Publ. No. 506, Washington DC, US Government Printing Office, 1960]
Specificity (%)
Diagnosis point
1 -
Sen
siti
vity
(%
)
Sen
siti
vity
(%
)[T
rue
po
siti
ve]
6.5B1 - Specificity (%)

42
Combination of test
To enhance sensitivity or specificity of the screening test
• Test in series: person is called “positive” when he tests +ve to all of a series of test, “negative” if he tests –ve to any. This enhance the SPECIFICITY of the test
• Test in parallel: person is labeled “positive” if he tests +ve to any of a test, “negative” if he tests –ve to all. This enhance the SENSITIVITY of the test

43
MULTIPLE TESTS CONCEPT
Types Step of event Result
Serialtesting
Paralleltesting
sensitivity specificity
sensitivity specificity
+
+
+
A
B
C
-
-
-
A B C+ + +
6.6B
Positive = all test +ve
Positive = any test +ve

44
Perinatal HIV Outcome Monitoring System (PHOMS)
•Criteria for diagnosis of HIV status in children = uninfected–HIV antibody negative at least 1 time in any age group; (serial or parallel)
–PCR negative at least 2 times at a different interval and last test must be after 2 months old (serial or parallel)
Serial to increase specificity
Parallel to increase sensitivity

45
Perinatal HIV Outcome Monitoring System (PHOMS)
•Criteria for diagnosis of HIV status in children = infected–HIV antibody positive at least 2 times with different technic, age > 18 months; (serial or parallel)
–PCR positive at least 2 times at a different interval in any age group (serial or parallel)
Serial to increase specificity
Serial to increase specificity
46
Yield of screening test
• Predictive Value Positive (PVP) is likelihood that an individual with a positive test has the disease
PVP = a / a + b or = TP / TP + FP
• Predictive Value Negative (PVN) is likelihood that an individual with a negative test does not have the disease
PVN = d / c + d or = TN / TN + FN
This measurement is useful to M.D. especially PVP

48
Binomial Mathematical ModelIf p = prevalence of disease sens.= sensitivity of test spec.= specificity of test
Then; PVP = p(sens)
p(sens) + (1–p)(1-spec)
PVN = (1-p) spec
(1–p) spec + p(1-sens)PV or yield can be affected by Prevalence, and
Specificity and slightly affected by Sensitivity10.2
49
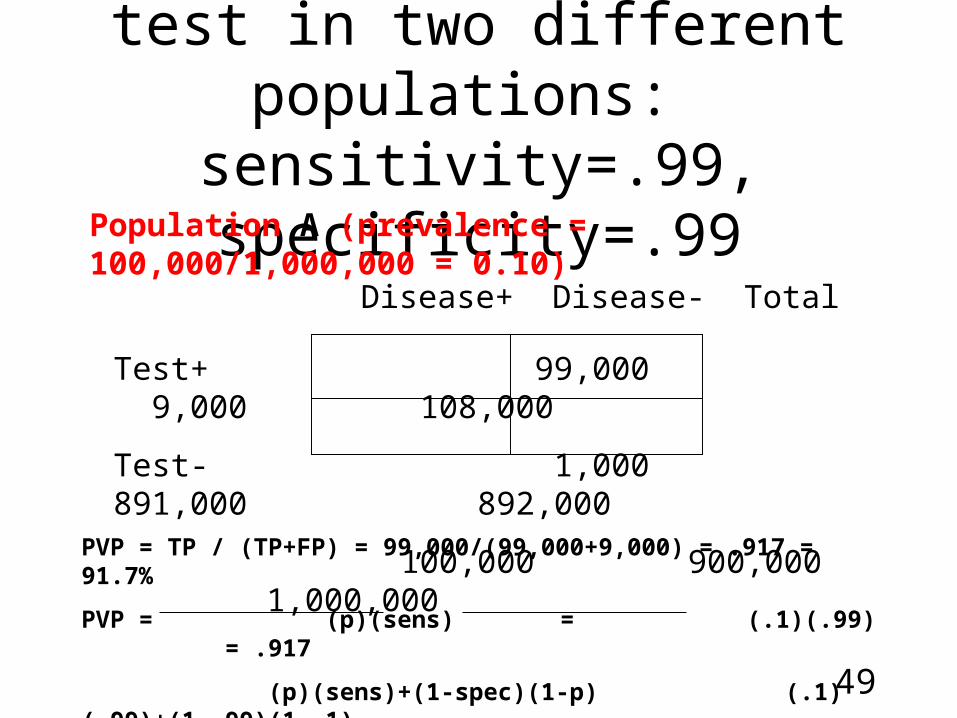
Results of screening test in two different populations:
sensitivity=.99, specificity=.99Population A (prevalence = 100,000/1,000,000 = 0.10)
Disease+ Disease- Total
Test+ 99,000 9,000 108,000
Test- 1,000 891,000 892,000
100,000 900,000 1,000,000
PVP = TP / (TP+FP) = 99,000/(99,000+9,000) = .917 = 91.7%
PVP = (p)(sens) = (.1)(.99) = .917
(p)(sens)+(1-spec)(1-p) (.1)(.99)+(1-.99)(1-.1)
50
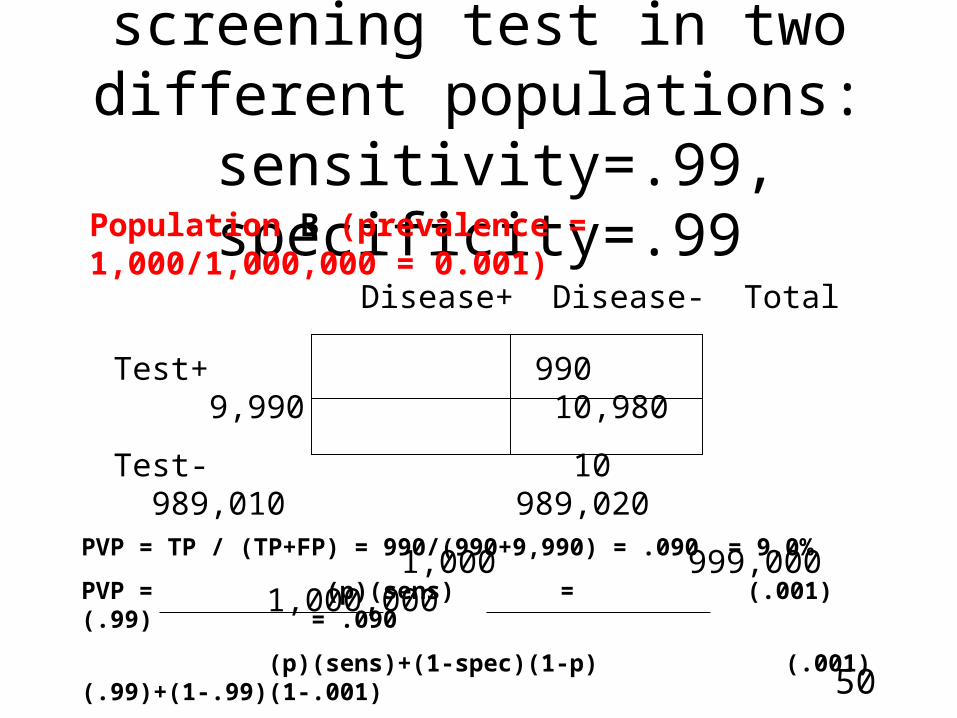
Test results of screening test in two different
populations: sensitivity=.99, specificity=.99Population B (prevalence = 1,000/1,000,000 = 0.001)
Disease+ Disease- Total
Test+ 990 9,990 10,980
Test- 10 989,010 989,020
1,000 999,000 1,000,000
PVP = TP / (TP+FP) = 990/(990+9,990) = .090 = 9.0%
PVP = (p)(sens) = (.001)(.99) = .090
(p)(sens)+(1-spec)(1-p) (.001)(.99)+(1-.99)(1-.001)
51
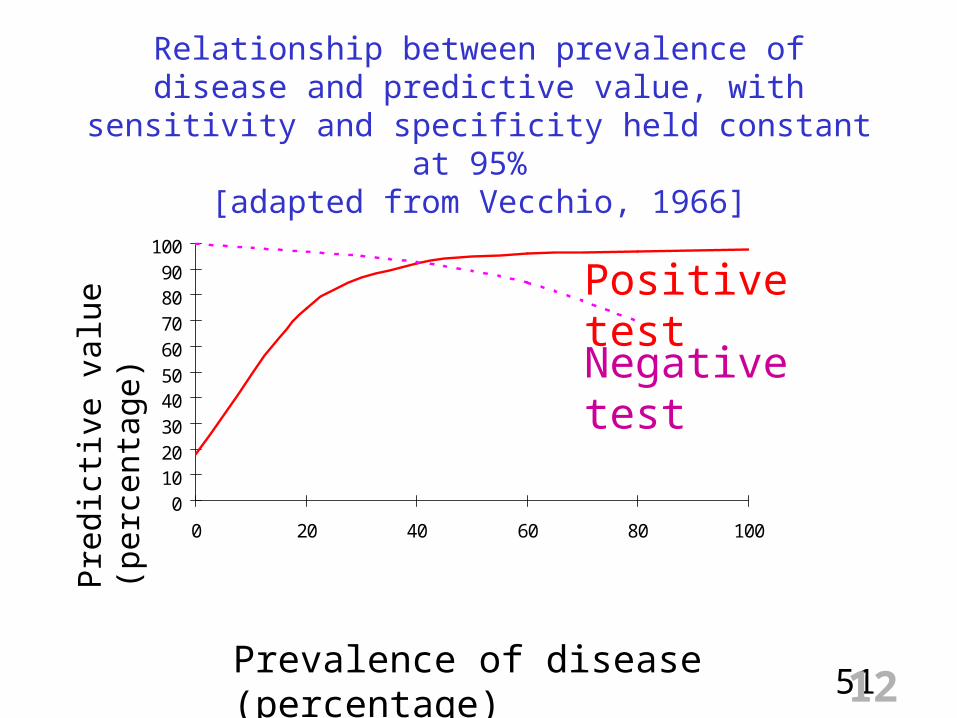
Relationship between prevalence of disease and predictive value, with sensitivity and specificity held constant at 95%
[adapted from Vecchio, 1966]
0102030405060708090
100
0 20 40 60 80 100
Positive test
Negative test
Prevalence of disease (percentage)
Pre
dict
ive
valu
e (p
erce
ntag
e)
12

52
PVP as a function of prevalence, sens = .99
0102030405060708090
100
0 10 20 40 60 80 100
Positive test
Prevalence of disease (percentage)
Pre
dict
ive
valu
e (p
erce
ntag
e) Spec = .99Spec =
.90Spec = .80

53
PVN as a function of prevalence, spec = .99
0102030405060708090
100
0 10 20 40 60 80 100
Negative test
Prevalence of disease (percentage)
Pre
dict
ive
valu
e (p
erce
ntag
e) Sens = .99Sens = .90
Sens = .80

54
Reliability**Precision**Repeatability
Number of agreed positive= -------------------------------------
Number of positive either time
a= --------------
(a + b + c)

55
Screening of breast cancer by Mammography
Cancer+ Cancer- Total
Test+ 31 108 139
Test- 24 20048 20072
65 20156 20211
Reliability = a / a+b+c = 31 / 31+24+108
= 31 / 163
= 19.0%
56
Four sources of variability
• Biological variation (specimens)
• Variation due to the test method or measurement (test)
• Intra-observer variation (examiner)
• Inter-observer variation (examiners)
57
Increase reliability can be made through:
• Standardization of procedures
• Intensive training of observers
• Periodic quality control
• Use of 2 or more observers making independent observations

58
Reliability and Validity of Instruments
A – reliable and valid C – reliable but not valid
B – not reliable but valid D – not reliable and not valid
Fre
quen
cy
A
B
C
D
True value Measurement
X

59
2X 2 table of screening test, definitions and formulas
Test
positive
negative
Diseasepresent absent
True positive
False positive
a + bc + d
False negative
True negative
a b
c da + c
b + d
a + b + c + d
+PV = a / a + b-PV = d / c + d
Sensitivity
= a / a + c
Specificity
= d / b + dAccuracy= a+d / a+b+c+d
Prevalence= a+c / a+b+c+d

60
Example 1: Screening of breast cancer by clinical examination
Clin exam
positive
negative
Breast cancerpresent absent
34
2000021
156
55 20156 20211
20021
190
Sensitivity = 34/55 X 100 = 61.3% Specificity = 20000/20156 X 100 = 99.2%
PVP = 34/190 X 100 = 17.9% PVN = 20000/20021 X 100 = 99.9%

61
Example 2: Screening of breast cancer by mammography
Mammography
positive
negative
Breast cancerpresent absent
31
2004824
108
55 20156 20211
20072
139
Sensitivity = 31/55 X 100 = 56.4% Specificity = 20048/20156 X 100 = 99.5%
PVP = 31/139 X 100 = 22.3% PVN = 20248/20072 X 100 = 99.9%

62
Example 3: Screening of breast cancer by clinical examination and follows by mammography
positive
negative
Breast cancerpresent absent
19
15515
1
34 156 190
170
20
PVP = 19/20 X 100 = 95%
Mammography
63
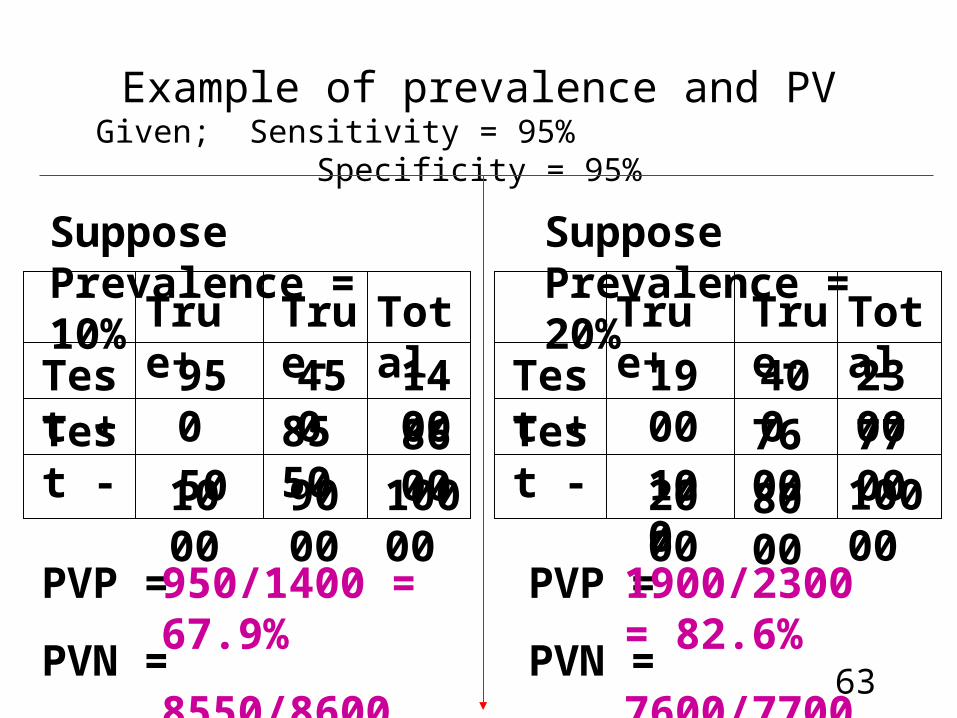
Example of prevalence and PVGiven; Sensitivity = 95% Specificity = 95%
Test +Test -
True+
True-
Total
Suppose Prevalence = 10%
Test +Test -
True+
True-
Total
Suppose Prevalence = 20%
950
450
400
1900
2000
100
76008000
2300770010000
10000
9000
1000
14008600
50
8550
PVP =
PVN =
PVP =
PVN =
950/1400 = 67.9%
8550/8600 = 99.4%
1900/2300 = 82.6%
7600/7700 = 98.7%
64
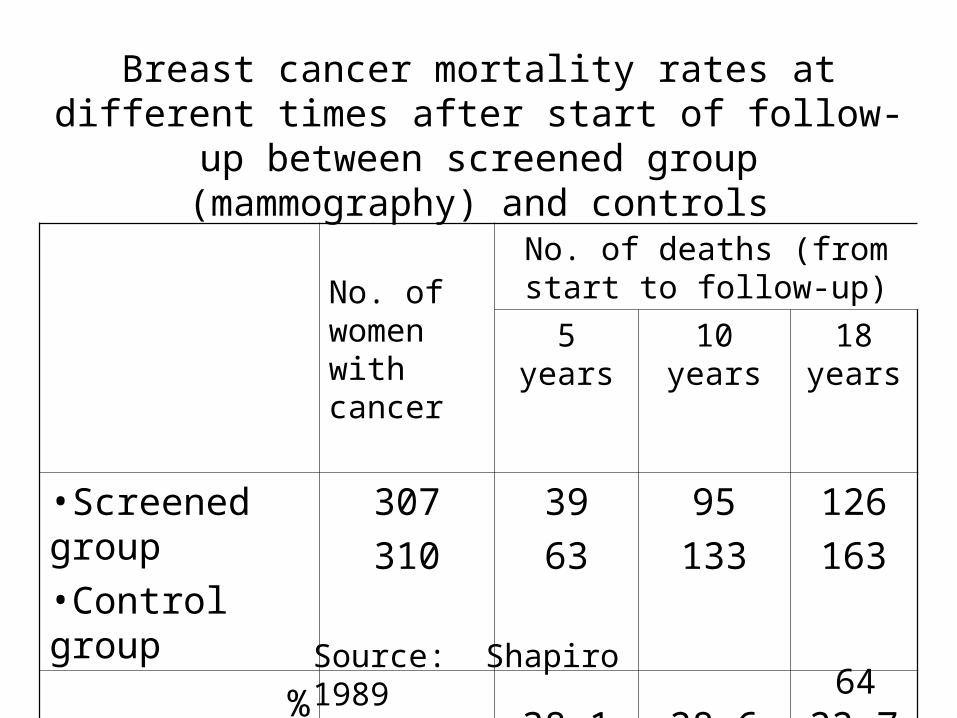
Breast cancer mortality rates at different times after start of follow-up between screened group (mammography)
and controls
No. of women with cancer
No. of deaths (from start to follow-up)
5 years 10 years 18 years
•Screened group•Control group
307
310
39
63
95
133
126
163
% difference 38.1 28.6 22.7
Source: Shapiro 1989

65
SimpliRED VS. WB and EIA VS. WB
+
-
+ -
362
1
0
2133
SimpliREDSensitivity = 100%Specificity = 99.95%
WB
Sim
pli
RE
D
+
-
+ -
362
9
0
2125
EIASensitivity = 100%Specificity = 99.58%
WB
EIA
Conclusion
66
Conclusion of SimpliRED and EIA
• SimpliRED is as sensitive and specific as EIA, but more expensive
• It had excellent correlation with the gold standard WB
• It provided rapid, accurate and on-site HIV status identification
• It required no equipment and minimal training• For this study, it saved unnecessary CD4 testing of
HIV samples

70
Principle of good screening program (1)1. The condition being sought is an important health
problem for the individual and the community. Since screening requires the commitment of large amounts of money, manpower, and other resources, screening should be undertaken only when it has the potential to lead to a significant decrease in rates of disability or death or both
2. There is an acceptable form of treatment for patients with recognizable disease. The goal of screening is to prevent disability or death or both. However, if there is no generally accepted treatment, it is premature to embark on a screening program
3. The natural history of the condition, including its development from latent to declared disease, is adequately understood. This is perhaps the most crucial of all the criteria in determining the feasibility of screening.
71
Principle of good screening program (2)
4. There is a recognizable latent or early symptomatic stage
5. There is a suitable screening test or examination for detecting the disease at the latent or early symptomatic stage, and this test is acceptable to the population
6. The facilities required for diagnosis and treatment of patients revealed by the screening program are available. Many screening programs have had little effect because planning for them did not include adequate and effective mechanisms for follow-up of positives
7. There is an agreed policy on whom to treat as patients
8. Treatment at the pre-symptomatic, borderline stage of a disease favorably influences its course and prognosis

72
Principle of good screening program (3)
9. The cost of the screening program (which would include the cost of diagnosis and treatment) is economically balanced in relation to possible expenditure on medical care as a whole
10.Case finding is a continuing process, not a “once and for all” project. Some conditions, e.g., Phenylketonuria must be screened for once, early in life. Others should be monitored repeatedly. When repeated screening is necessary, empirical studies are needed to determine the optimal interval between screenings
[Wilson and Jungner, WHO 1968]

73
Criteria for instituting screening program
Disease - Serious
- High prevalence of pre-clinical stage
- Natural history: undertood
- Long period between first signs and overt disease
Pre-test - Sensitive and specific
- Simple and cheap
- Safe and acceptable
- Reliable
Diagnosis - Facilities are adequate
and treatment - Effective, acceptable, and safe treatment available

78
Questions ?

79

80
81
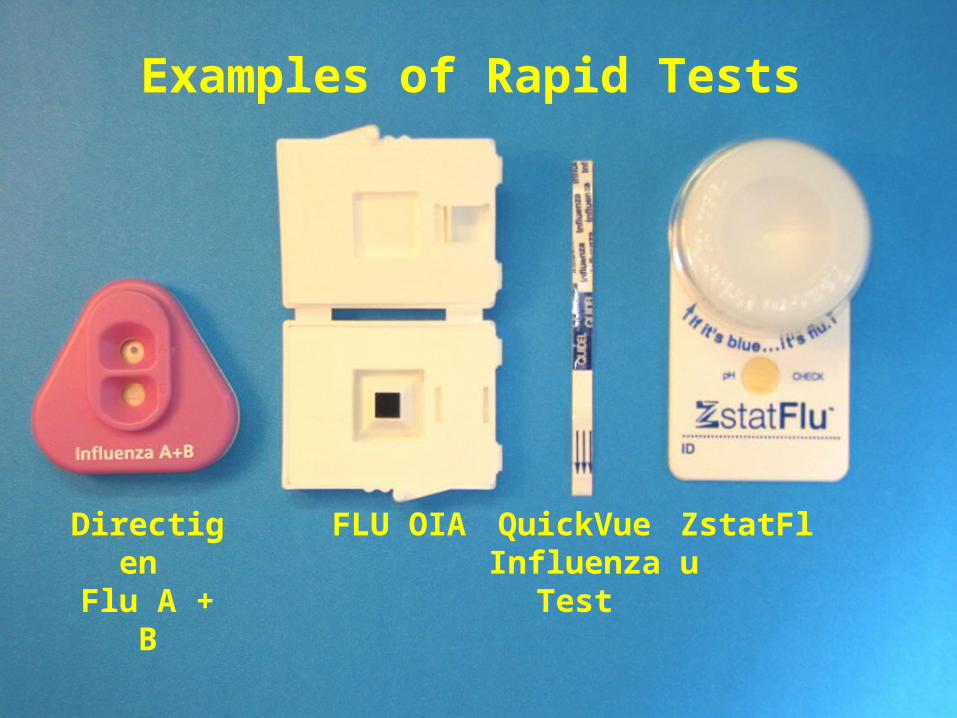
Directigen Flu A + B
FLU OIA QuickVue Influenza
Test
ZstatFlu
Examples of Rapid Tests
82
• Test Factors • Sensitivity- Proportion of positive tests by gold standard
that are also positive by screening test (true positives)
• Specificity- Proportion of negative tests by gold standard that are also negative by screening test (true negatives)
• Prevalence- Proportion of tested population with influenza
• Other factors• Type and quality of respiratory specimen• Day of illness when specimen was obtained• Compliance with test procedures• Interpretation of result
Factors Affecting Rapid Test Performance

83
• Sensitivity: median = 70-75%
• Specificity: median = 90-99%• Calculated under ideal conditions• Most data are from children with
influenza A (H1N1) or A (H3N2)• Sensitivity to detect influenza A > B• No published data on H5N1
Summary of Published Data on Performance of Rapid Influenza Tests*
*Uyeki, T. 2003. Peds Infectious Disease (22) 164-77.

84
New Uses for Rapid Tests In Thailand
• Febrile respiratory illness outbreak investigation
• Research – Outpatient disease burden– Seasonality– Cost of illness
• Expanded human influenza surveillance
• H5N1 avian influenza clinical management

85
Seasonality of Outpatient Influenza
Using Rapid Tests; 2003-2004
29%
21%
0% 0% 0%
9%13%
27%
45%40%
12%
31%
0%
10%
20%
30%
40%
50%
Aug
Sep Oct NovDec Ja
nFeb Mar Apr
May Jun Ju
l
Month
Prop
ortio
n Po
sitiv
e