Embed Size (px)
Citation preview
Screening in Gynaecological Cancers
Prof. HYS Ngan
Department of Obstetrics & Gynaecology University of Hong Kong
Queen Mary Hospital
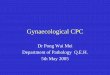
Fallopion tube
OvaryEndometrium
Cervix
Vagina
Uterus
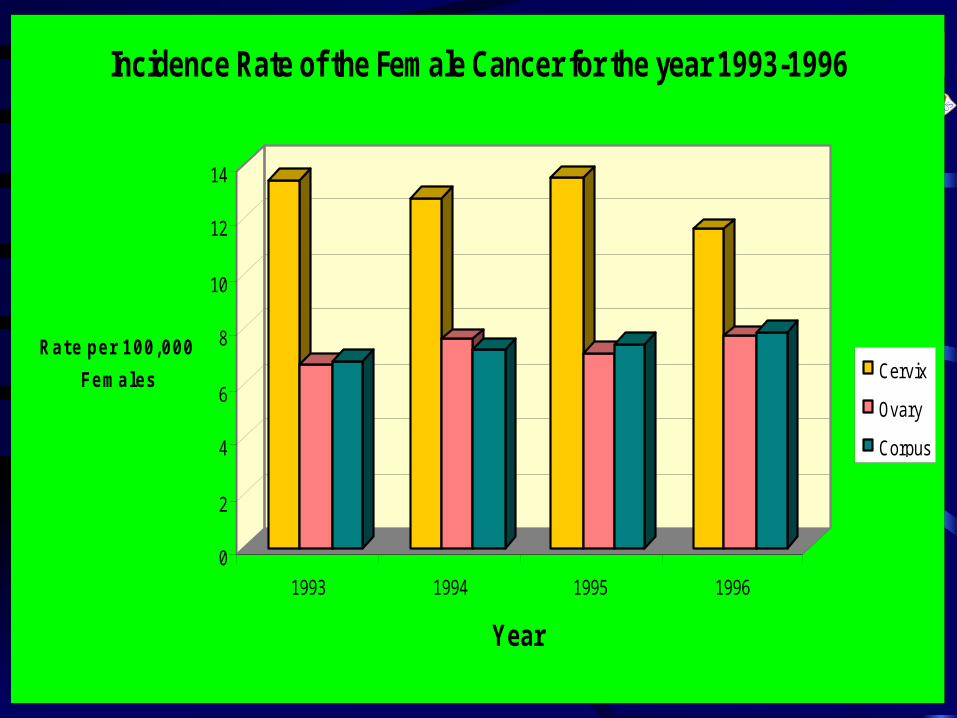
0
2
4
6
8
10
12
14
Rate per 100,000
Females
1993 1994 1995 1996
Year
Incidence Rate of the Female Cancer for the year 1993-1996
Cervix
Ovary
Corpus
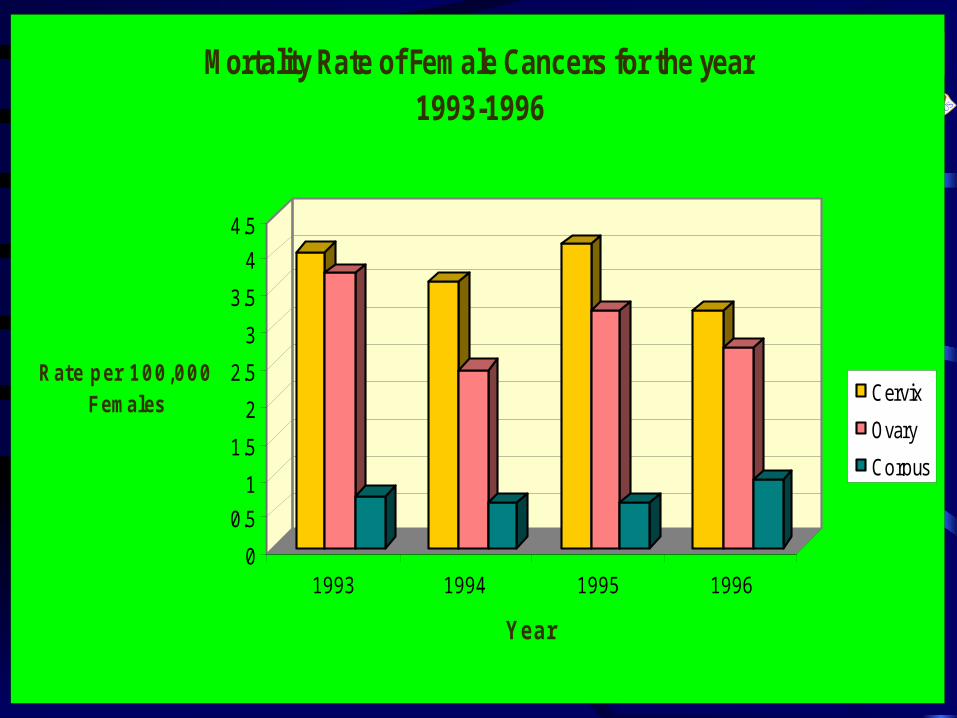
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Rate per 100,000 Females
1993 1994 1995 1996
Year
Mortality Rate of Female Cancers for the year 1993-1996
Cervix
Ovary
Corpus
Screening
• Cervical cancer
• Ovarian cancer
• Endometrial cancer
Screening
To detect disease among
healthy
population
Without symptoms of disease
Purpose: decrease mortality due to the disease screened
Disease appropriate for screening
• High prevalence of disease
• Known natural history, precursor lesion and course of progression
• Detection of early stage disease, amenable to cure
• Method used is simple, cheap, specific and sensitive, acceptable, risk-free and accessible
Carcinoma of the cervix
• commonest lower genital tract cancer
• about 500 new cases per year in HK
• about 140 deaths per year in HK
• median age: 50 years
Natural history of low-grade HPV cervical lesion
• Cervical HPV is very common, related to sexual behaviour
• High spontaneous remission rate
• lower remission rate in CIN
• LSIL progress to HSIL in 70% in 10 yrs
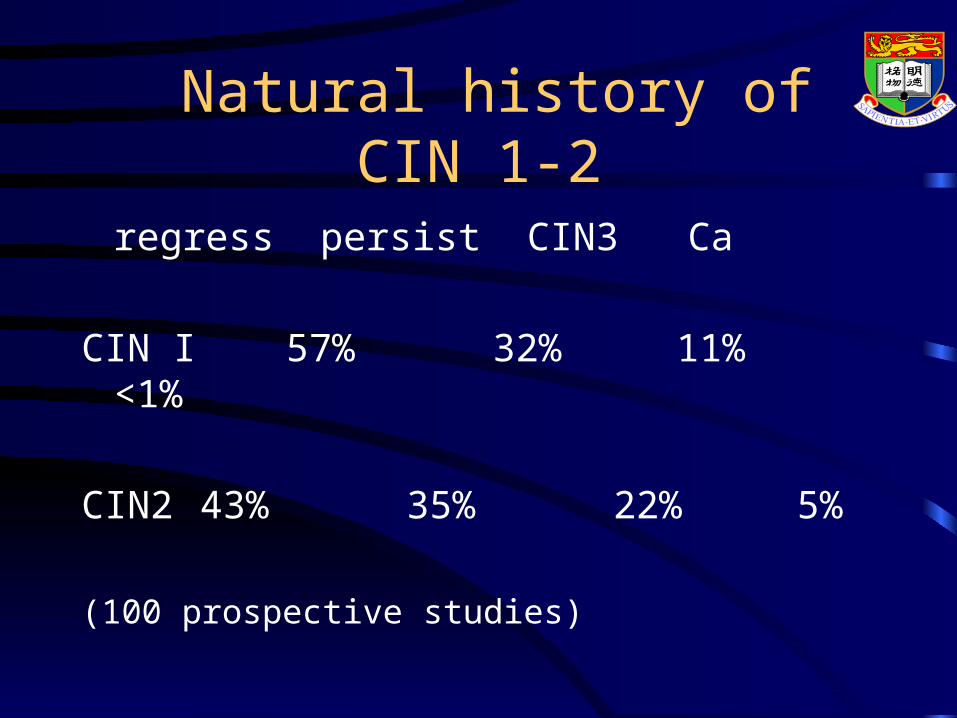
Natural history of CIN 1-2
regress persist CIN3 Ca
CIN I 57% 32% 11% <1%
CIN2 43% 35% 22% 5%
(100 prospective studies)
Cervical cytologySensitivity and Specificity
• Overall sensitivity: 61-64%, cervical cancer: 82-95%
• Overall specificity : 99 - 99.4%
Quantin.C 1992, Soost.HJ 1991
Cervical cytologyPositive predictive value
• Low-moderate dysplasia: 73-76%
• severe dysplasia : 85-90%
• Invasive cancer: 95%
Quantin.C 1992, Soost.HJ 1991
False negative rate of cervical cytology in detecting cervical
cancer
• Depends on the quality of the smear taking and the laboratory
• estimated to be 3-30%
New technology
• automation for cervical cancer screening
• liquid-based cytology - thin layer preparation
Advantages of LBC
Eliminate
• air-dried artifact
• inflammatory cells
• blood
• mucus
Increase
• detection of abnormal cytology
Cervical cancer screening - new methods under exploration
• cervicography
• polar probe
• HPV typing
HPV DNA testing - potential use
• HPV based instead of cytology based screening
• triage of patients with equivocal or ASCUS
• external quality control of cytology
• high risk HPV predicts high grade SIL in the absence of cytology abnormality
• molecular variant predicts carcinoma
Organized screening vs Opportunistic screening
• Finland and Sweden
decrease in indicence and mortality of cervical cancer
concentrate resources
wide coverage
• Policy decision
European and American recommendation
Age:
• Europe: 35-60 yrs for invasive ca
25-65 yrs for preinvasive lesions
• USA: 18 yrs old
Interval:
• Europe: 3-5 years
• USA: annual
low risk, 3 consecutive negative, space out
Hong Kong College of Obstetricians and Gynaecologists
• Age: sexually active to 65
• Interval: 2 consecutive annual normal smears, 3 yearly
How to take a cervical smear?
• Speculum
• adequate exposure
• light source
• sampling device - Ayres’ spatula, brush or broom
• transformation zone

Speculum
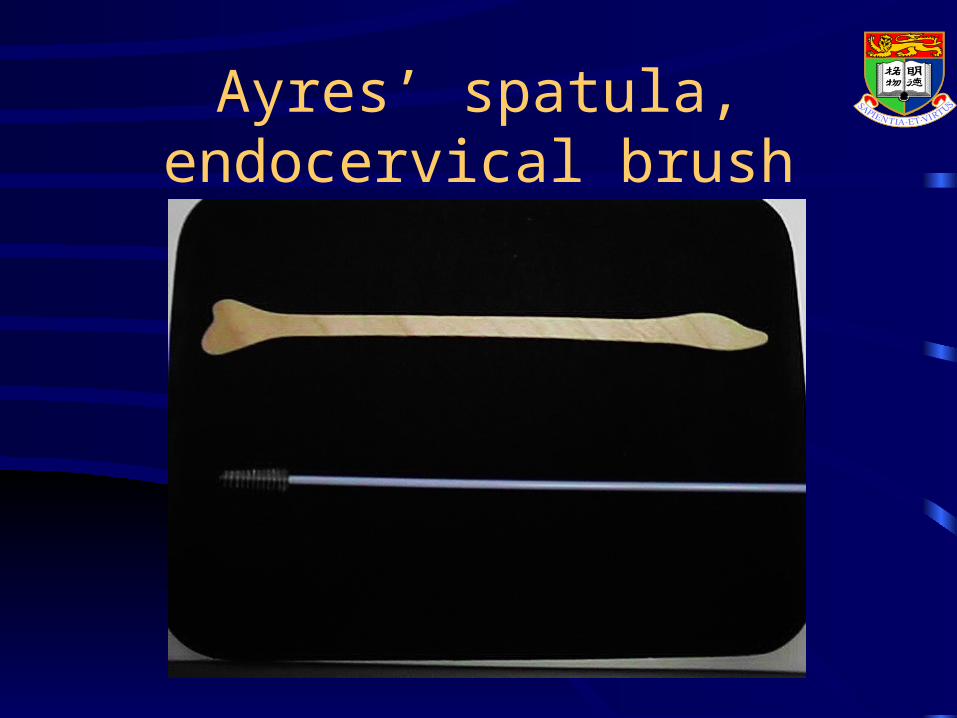
Ayres’ spatula, endocervical brush

Broom type sampler
When not to take a cervical smear
• Blood in vagina, on the cervix - usually because of menstruation
• Obvious or gross growth on the cervix - a biopsy is more appropriate
• Cervix cannot be seen
How to interpret a cytology report?
– Reports of cervical smear should be interpreted together with the clinical picture of the patient.
– Some physiological or medical conditions may lead to difficulty in the interpretation of a smear.
History on request form
– contraceptive history – menopausal status– date of last menstrual period– prior radiotherapy or current chemotherapy– hysterectomy– drugs or hormones– parity
Bethesda System 2001
• Negative
• Squamous cell - ASCUS, ASC-H (cannot exclude HSIL)
- LSIL
- HSIL, HSIL with features suspicious of invasion
- SCC
Bethesda System 2001
• Glandular cell
- Atypical : endocervical cells, endometrial cells, glandular cells
- Atypical, favor neoplastic: endocervical cells, glandular cells
- Endocervical adenocarcinoma in-situ
- Adenocarcinoma: endocervical, endometrial, extrauterine, NOS
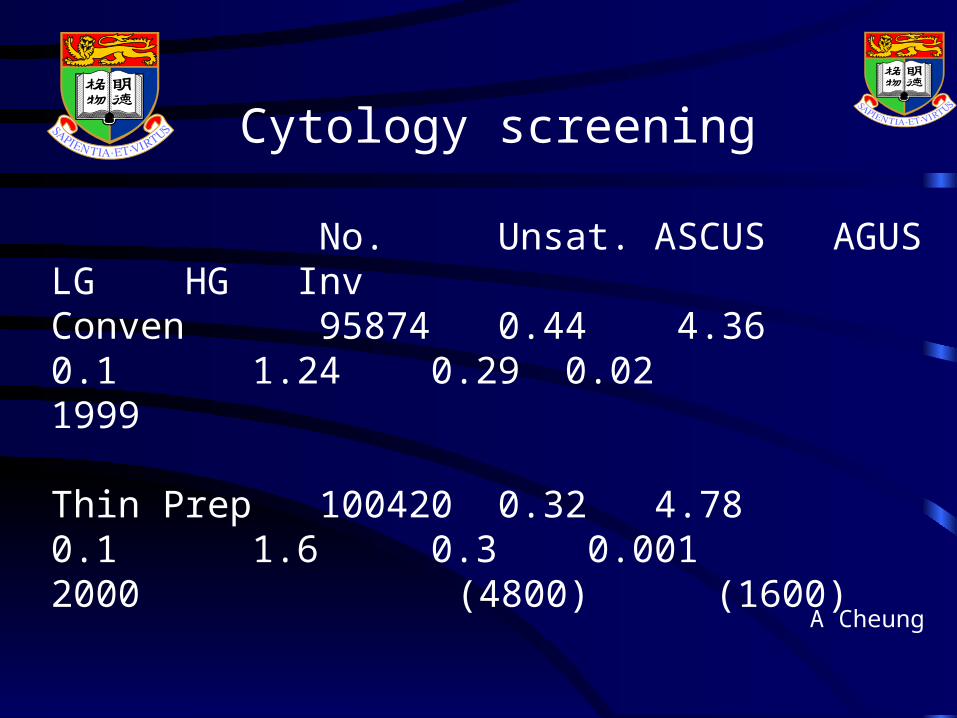
Cytology screening
No. Unsat. ASCUS AGUS LG HG InvConven 95874 0.44 4.36 0.1 1.24 0.29 0.021999
Thin Prep 100420 0.32 4.78 0.1 1.6 0.3 0.0012000 (4800) (1600)
A Cheung
How to manage abnormal smear?
Histological grading of pre-invasive cervical lesion
• Koilocytes : human papillomaviral changes
• Cervical intraepithelial neoplasia (CIN)
• 1 : dysplastic cells in lower one third of epithelium
• 2 : lower two third
• 3 : almost the whole thickness
Inflammatory changes with atypia
– could be due to vaginitis or infection such as monilia, trichomonas, herpes or condyloma.
– Treat the cause and repeat the smear 4 to 6 months later to ensure that dysplastic cells were not masked by the previous inflammatory cells.
Management of ASCUS
• 5% of smears reported as ASCUS
• Majority of ASCUS turn out to be normal or of low grade CIN
• Less than 1 % associated with cancer
Management of LSIL
• 1.5-2.5 % of smears screened were of LGIL
• 15-30% associated with HG CIN
• about 1% associated with cancer
• 2 options:
• repeat smear 4-6 months interval
• refer for colposcopic assessment (HKCOG guideline)
Management of HSIL
• Gross examination showed a growth - biopsy
• Grossly normal - refer colposcopy
Outcome of AGUS
• Normal: 19-34%
• Significant pathology: 15-37%
CIN 16-54%
AIS 3-5%
Ca cervix 2-3%
Ca corpus 1-4%
Recommendation
• AGUS- favor neoplasia, co-existing with squamous neoplasia, previous hx of cervical lesion: refer colposcopy, D&C and cone
• AGUS- favor reactive, not otherwise specified: repeat cytology with adequate endocervical sampling
Colposcopy services in Hong Kong
• Department of Obs & Gyn of major hospitals of the Hospital Authority
• Lady Helen Woo Women’s Diagnostic and Treatment Centre at Tsan Yuk Hospital
• Private gynaecologist with colposcopy training
Colposcope
Treatment of high grade CIN
• ablative therapy– cryotherapy– cold coagulation– diathermy– laser evaporisation
• excision therapy– cone (knife, laser, loop excision)
• hysterectomy is rarely indicated
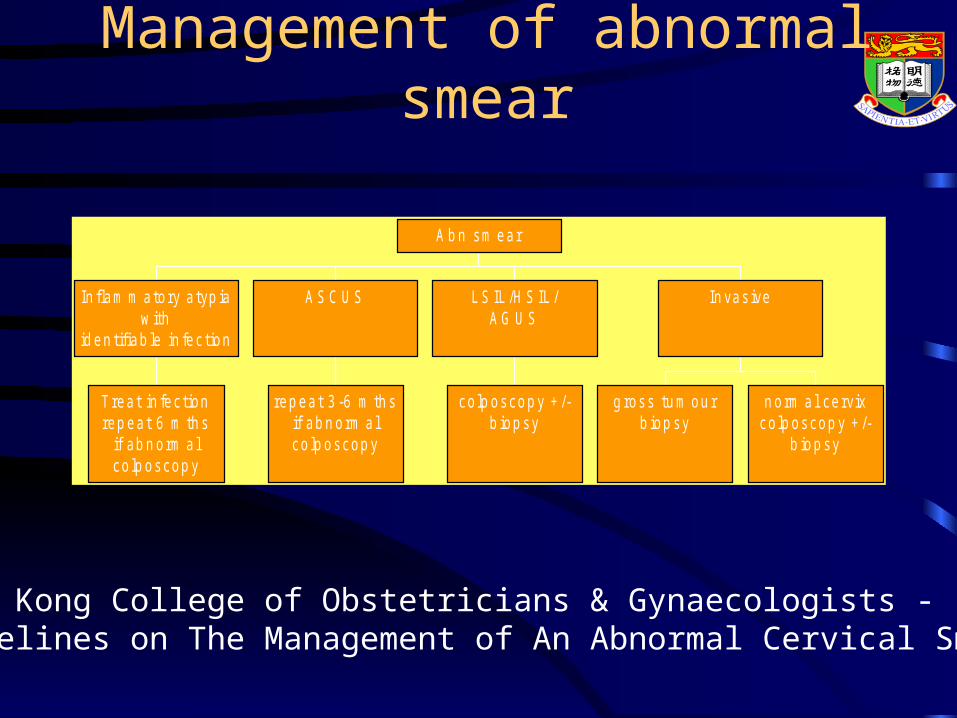
Management of abnormal smear
Trea t in fec tionrep eat 6 m th s
if ab n orm a lco lp oscop y
In flam m atory a typ iaw ith
id en tifiab le in fec tion
rep eat 3 -6 m th sif ab n orm a lco lp oscop y
A S C U S
co lp oscop y + /-b iop sy
L S IL /H S IL /A G U S
g ross tu m ou rb iop sy
n orm a l ce rvixco lp oscop y + /-
b iop sy
In vas ive
A b n sm ear
Hong Kong College of Obstetricians & Gynaecologists - Guidelines on The Management of An Abnormal Cervical Smear
Ovarian Cancer in HKNew Cases : 220
Death : 95
Median age : 51
(1992)
Ovarian cancer
• High mortality due to late diagnosis
• 75% of ca ovary at diagnosis were at late stage with a 28% 5 yr survival
• Stage I ca ovary has 95% 5 yr survival
Ovarian CancerSymptoms of ovarian cancer :• asymptomatic• Lower abdominal pain/pressure • mass• Abdominal enlargement• Vaginal bleeding• Urinary/bowel symptoms
Ovarian Cancer
Risk factors :
1) majority has no risk factor
2) family history 10%
- familial ovarian syndrome
2) nulliparous
3) racial and social
Why screening for ovarian cancer is so difficult?
• Anatomic location of the ovary, not easily accesible
• Lack well defined precursor lesion and has poorly defined natural history
• Low prevalence, need exquisite specificity to avoid unnecessary intervention
• Lack of a good method
Methods used for ovarian cancer screening
• Serum CA125
• Transvaginal ultrasonogram
• Multimodal
• New method under investigation - lysophosphatidic acid
Serum CA125
• Elevated in 82% of ovarian cancer and <1% of healthy women
• rising pattern over time preceded ovarian cancer
• limitations: lack of sensitivity in Stage I disease, poor specificity (elevated in benign and other malignant conditions)
TVS in ov ca screeningKentucky study 2000
• 14,468 postmenopausal women
• annual TVS
• total 57,214 scans
• 180 laparotomies: 17 ov ca (stage I=11, stage II=3, stage III=3)
• sensitivity 81% specificity 98.9% PPV 9.4% NPV 99.97%
• Survival at 2 yr 92.9% and at 5 yr 83.6%
Ovarian cancer screening• Jacobs et al. 1993
• 22000 women over 45 yrs
• CA125 and transvaginal ultrasound
• 125 elevated CA125, FU with CA125 and TVS
• 41 laparotomies: 11 ovarian ca vs 8 in control gp
• specificity = 99.9%
• sensitivity = 78.6%
• positive predictive value = 26.8%
Ovarian screening
• Not cost-effective
• May be considered in high risk population
• No place for population screening yet
Carcinoma of Endometrium
Incidence : third commonest malignant tumour
of genital tract
Age : 58
Endometrial Cancer in H.K.
New cases : 200
Death : 50
Median age : 60
(1992)
Risk factors
• nulliparity, anovulation, late menopause
• exogenous estrogen
• endogenous estrogen
• DM, HT, obesity
• smoking, white
• tamoxifen
• familial history
Postmenopausal Bleeding
1) carcinoma of endometrium 14%2) other gynecological malignancy 14%3) atrophic endometritis 20%4) endometrial hyperplasia 12%5) cervicitis/erosion 8%6) endometrial polyp 8%7) cervical polyp 8%
Diagnosis of Carcinoma of Endometrium
(f) D&C near 100%uterine aspirate 90%endocervical aspirate + vaginal 65%
aspiratevaginal aspirate + cervical smear 40% cervical smear 15%
Should endometrial cancer be screened?
• High prevalence in the West, low (same as ovarian ca) in Hong Kong
• precursor lesion, atypical endometrial hyperplasia
• accessibility of endometrium to sampling• high cure rate for early disease
Cons: majority detected at early stage because of abnormal bleeding esp PMB
Endometrial Cancer Screening
• Tools explored– pelvic ultrasound (>8mm endometrial thickness
in postmenopausal women) Karlsson 1995
– endometrial aspirate (inadequate sampling in menopausal women)
Endometrial aspirator
Endometrial aspirator
Endometrial aspiration
• Sensitivity for endometrial ca 94% in patient with symptoms
• sensitivity for hyperplasia 31%
Cons: discomfort to patient
lack of known efficiency in asymtomatic patients
TVS in endometrial ca screening
• Croatia study (Kurjak 1994)
• 5013 asymptomatic women
• ca endometrium 6 and hyperplasia 18, no false positive
(low prevalence of ca endometrium in asymptomatic patients, ? Advantage)
Endometrial cancer screening
• Not justified in population screening
• excellent prognosis of majority of ca endometrium unlikely will result in decreased mortality rates
Conclusions
• Cervical cancer screening is the most successful programme in gynaecological cancers
• Ovarian cancer screening is not proven to be cost-effective yet, may be considered in high risk groups
• Endometrial cancer screening may be consider in high risk groups