Embed Size (px)
Citation preview
Screening for BH and PH
Conditions
When in Process Flow to Screen &
What Screening Tools to Use?
Screening Tool Checklist
5/19/2014 11:30 AM
• Research base demonstrating construct validity
• Free
• Easy to Train Staff on Use
• Sixth Grade Reading Level
• Short and Long Versions
• Face Validity
• Widely Adopted
• Able to be coded into EMR
Screening Tools
Behavioral Health Clinic
• What tools are you currently using for Physical
Health Screening?
• What Physical Health Data do you Collect?
Primary Care Clinic
• What tools are you currently using for Behavioral
Health Screening?
Screening Workflow
5/19/2014 11:30 AM
• When, Where, Who?
• Where does the data go?
• How is the data turned into information and
leveraged?
• How are staff trained?
Solutions for Effective
Transportation Supports
Significant Barriers to
Healthcare
5/19/2014 11:30 AM
Structural • Availability • Organization •
Transportation • Financial • Insurance coverage •
Reimbursement levels • Public support Personal •
Acceptability • Cultural • Language • Attitudes •
Education/Income
Source: Institute of Medicine. Access to Health Care in America.
National Academies of Science Press, 1993
Burden of Transportation
The poorest fifth of Americans spend 42
percent of their annual household budget on
the purchase, operation, and maintenance
of automobiles, more than twice the national
average.
Source: Surface Transportation Policy Project,
http://www.transact. org/library/factsheets/poverty.asp.
Patient Navigators
• Older Asian and Hispanic youth who do what
they’ve always done for family and friends
• Educated and trained at local community
colleges – 1 year credit bearing certificate
program
• Career ladder - transferable, forward-looking
skills for non-clinical health worker members
of an integrated, culturally-competent,
patient-facing care delivery team (whew)
How we roll • Clinician refers patient for appt./consult
• Software matches patient language/time needs, texts
appropriate patient navigator (PN)
• PN meets patient, accompanies her to referral
service, checks in, interprets/explains, checks out
• App records non-clinical activities.
• After checkout, clinical supervisor reviews before
posting. Instant electronic payment.
Source: Asian Americans for Community Involvement (www.aaci.org)
Transportation Resources
• http://www.apha.org/advocacy/priorities/issues/tr
ansportation
High Performing
Interdisciplinary Teams
“Team” & “Teamwork”
means something different
to everyone…
A Continuum of
Healthcare Teams • Multi-disciplinary Team = hierarchical, each role
separate, some communication, parallel processes.
• Inter-disciplinary Team = interdependent, maintain distinct professional responsibilities & assignments, must make dramatic adjustments in their orientation to co-workers.
• Trans-disciplinary Team = shared decision making, every member can do everyone else's role if needed, one process, much communication.
Source: Cooper et al. (2003). The Interdisciplinary team in the management of chronic condition: Has its time come? RWJF.
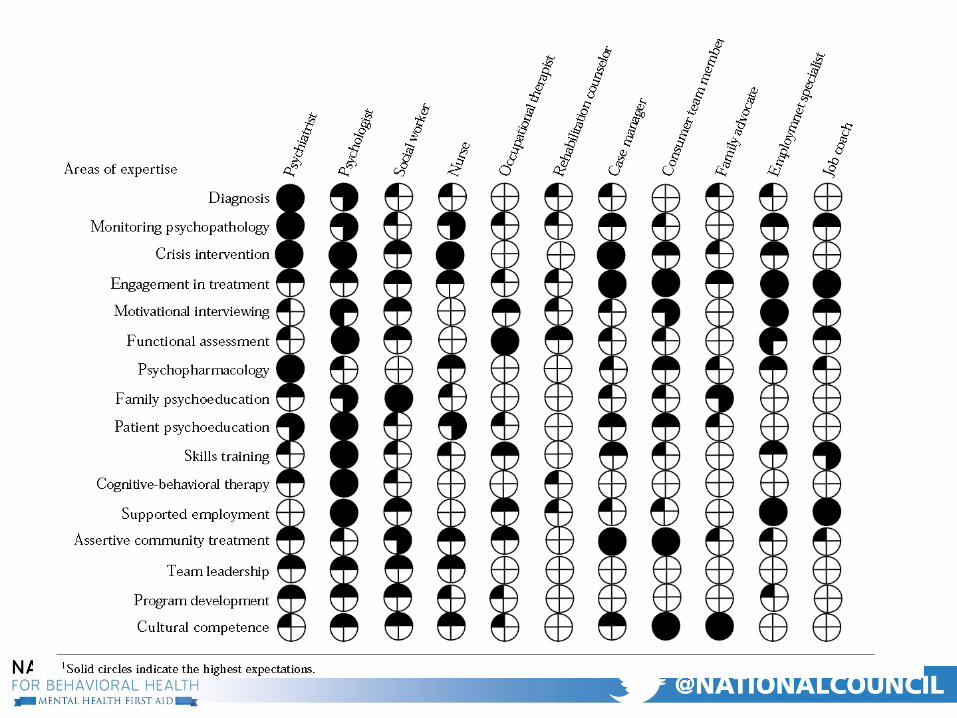
The Interdisciplinary Team:
People with distinct disciplinary training
working together for a common purpose,
as they make different, complementary
contributions to patient-focused care.
Leathard , A., ed. (1994). Going Interprofessional: Working Together for Health &
Welfare. Routledge, London.
Adaptive Reserve
• Borrill et al. (2000) found that teams with greater
occupational diversity reported higher overall
effectiveness and the innovations introduced by
these teams were more radical and had
significantly more impact both on the
organization and on patient care.
Borrill & Haynes (2000). Managers' lives. Stressed to kill. Journal of Health
Service.10;110(5691):24-5.
2007 Cochrane Review of
“Shared Care”
“Results from a few of the studies suggested that
shared care may be more effective in certain patient
groups. These include patients with depression and
other serious chronic mental health illness and those
with high levels of morbidity at baseline such as the
elderly and people with moderate to severe
congestive cardiac failure.”
Source: Effectiveness of shared care across the interface between primary and specialty care in chronic
disease management (Review) 13 Copyright © 2007 The Cochrane Collaboration., JohnWiley & Sons, Ltd
Health Outcomes Related to Interdisciplinary
Teams
A study involving >5,000 patients in 13 ICU’s found
significant patient mortality reductions in hospitals
where interdisciplinary teams worked in close
collaboration.
Source: Sommers LS, Marton KI, Barbaccia JC et al. Physician, nurse, and social worker
collaboration in primary care for chronically ill seniors. Arch Intern Med 2000;160:1825–
1833.
Interdisciplinary teamwork correlated to lower
hospital readmission rates the greatest reductions
in readmission rates occurred when physicians,
nurses, and social workers were most satisfied
with their professional relationships on the team.
Source: Knaus WA, Draper EA, Wagner DP et al. An evaluation of outcome from
intensive care in major medical centers. Ann Intern Med 1986;104:410–418.
Health Outcomes Related to Interdisciplinary
Teams
The Team as an Emerging
Standard of Care “The high-performing team is now widely
recognized as an essential tool for constructing a
more patient-centered, coordinated, and effective
health care delivery system.”
Source: Mitchell, P., M. Wynia, R. Golden, B. McNellis, S. Okun, C.E. Webb, V.
Rohrbach, & I. Von Kohorn. (2012). Core principles & values of effective team-
based health care. Discussion Paper, Institute of Medicine, Washington, DC.
www.iom.edu/tbc. P.5.
Five Components of Effective
Interdisciplinary Teams:
1. Defining appropriate team goals.
2. Clear role expectations for team members.
3. A flexible decision-making process.
4. The establishment of open communication
patterns.
5. The ability of the team to “treat” itself.
Source: Leipzig, Hyer et al. (2002). Attitudes Toward Working on Interdisciplinary
Healthcare Teams: A Comparison by Discipline J Am Geriatr Soc 50:1141–1148.
Terms Teams Must be able to
Operationalize Concepts that are
not Yet Well Operationalized
• Team based care
• Care Coordination/Care Navigation
• Patient Centered Care/Medical Home
• Population Health Management
• Treat to Target
• Bundled/Episode of Care
Defining appropriate team
goals
• Develop a team dashboard that includes
measurable, and meaningful/relevant goals.
• The goals must relate to tx plan, staff work plan
& broader organizational goals.
• Tie the goals to a quality improvement/PDSA
process.
• Incorporate discussion of the goals/measures
into every meeting.
Clear role expectations for
team members
• The more complex the task the clearer roles must
be.
• All team members have their own opinions of what
their role is and what their team member’s role is…
• If suspected or seen role ambiguity & conflict should
be discussed right away.
• Routinely, clearly state who “owns” or is
“responsible” for a task to help foster this thinking.
Staff Competencies
1. Interpersonal Communication
2. Collaboration & Teamwork
3. Screening & Assessment
4. Care Planning & Care Coordination
5. Intervention
6. Cultural Competence & Adaptation
7. Systems Oriented Practice
8. Practice Based Learning & Quality Improvement
9. Informatics
• A team is a problem-solving, decision-making mechanism. This is not to imply that an entire group must always make all decisions as a group.
• The issue is one of relevance and appropriateness; who has the relevant information and who will have to implement the decision.
A flexible decision-making
process
• Similarly, when a group faces a conflict it can
choose to (a) ignore it, (b) smooth over it, (c)
allow one person to force a decision, (d) create
a compromise, or (e) confront all the realities of
the conflict (facts & feelings) and attempt to
develop an innovative solution.
• The choices individual team members and the
team as a whole make will significantly influence
how the team functions.
A flexible decision-making
process cont.
The establishment of open
communication patterns
• Create avenues for communication (e.g., logs,
regular team meetings, use of common
language, etc.).
• Maintain regular contact with agency leadership.
• Understand how culture & training drives
language and communication styles.
• Maintain regular one-on-one supervision.
What Staff Care About/ Want from a
Leader
Practical Questions • What do you want me to keep doing?
(standardization)
• What do you want me to stop doing? (waste)
• What do you want me to do differently? (CQI)
Personal Questions • Is my job fulfilling my passion/life vision?
• Is my job fulfilling my career goals?
The ability of the team to
“treat” itself
• Include a “Team self-audit” process that is tied to
the team’s dashboard.
• Encourage questioning & the voicing of
alternative views.
• Declare team breakthroughs & team breakdowns
when necessary.
• Encourage necessary acts of leadership.
Team Norms… • Norms take on particular potency because they
influence all of the other areas previously discussed.
• Groups develop norms governing leadership, influence, communication patterns, decision-making, conflict resolution, and the like. Inherently, norms are not good or bad.
• The issue is one of appropriateness — Does
a particular norm help or hinder a group's ability to work?
Team Value Systems… • Wilmot (1995) reported that nurses valued
individualism, caring, autonomy, holism & patient
well-being, while social workers internalized
collectivity, liberty, equality & justice.
• Family practice and internal medicine medical
students and residents were found to be least
inclined to interdisciplinary practice while social
workers were most inclined. Source: Wilmot (1995). Professional values & inter-professional dialogue. Journal of Inter-professional
Care. 9(3):257–266
Take Care of Your Team… • “Transformation occurs, not at a steady & predictable
pace, but in fits & starts. After the strenuous task of
implementing a particular PCMH component, the
practice had to simultaneously manage the ripple
effects, maintain the change, & prepare for the next…”
• “…the work is daunting, exhausting & occurring in
practices that already felt as if they were running as
fast as they could. This type of transformative change,
if done too fast, can damage practices and often result
in staff burnout, turnover, & financial distress.”
Source: Nutting et al. (2010) Effect of Facilitation on Practice Outcomes in the
National Demonstration Project Model of the Patient-Centered Medical Home Annals
of Fam. Med., VOL. 8 (1). 533-544.
Team Care • Recognize teams are dynamic, emotion laden, and
need constant attention and reassurance.
• Hardwire rewards into the work flows.
• Be careful to hire team members not positions.
• Get in the habit of monitoring and responding to changes in morale/trust.
Team Tools/Scales
• ATHCT Scale: Attitudes Toward Health Care Teams
Scale
• Team Skills Scale (TSS): a self-assessment instrument
• Inter-professional Collaboration Scale (IPC): Team
function from individual team members’ perspective
specifically, effectiveness of communication,
accommodation and appearance of isolation
• Primary Health Care Team Effectiveness Survey
• Scale for Leadership Assessment & Team
Evaluation (SLATE),
Other Sources • Bosch M, Faber MJ, Cruijsberg J, et al. Effectiveness of Patient Care Teams and the Role of Clinical
Expertise and Coordination: A Literature Review. Med Care Res Rev. 2009. 66:5S-34S.
• Mitchell, P., M. Wynia, R. Golden, B. McNellis, S. Okun, C.E. Webb, V. Rohrbach, & I. Von Kohorn.
(2012). Core principles & values of effective team-based health care. Discussion Paper, Institute of
Medicine, Washington, DC. www.iom.edu/tbc. P.7.
• O’Leary KJ, Wayne DB, Haviley C, Slade ME, Lee J, Williams MV. Improving Teamwork: Impact of
Structured Interdisciplinary Rounds on a Medical Teaching Unit. J Gen Intern Med. 2010;25(8):826–32.
• Mudge A, Laracy S, Richter K, Denaro C. Controlled Trial of Multidisciplinary Care Teams for Acutely Ill
Medical Inpatients: Enhanced Multidisciplinary Care. Intern Med J. 2006. 36:558–63.
• Smith ST, Enderby S, Bessler RA. Teamwork in Leadership and Practice-Based Management. In:
McKean SC, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS, eds. Principles and Practice of Hospital
Medicine. 1st ed. New York, NY: McGraw-Hill; 2012:860-65.
• Internet Citation: Essentials Instructional Module: TeamSTEPPS® Long-Term Care Version. July 2012.
Agency for Healthcare Research and Quality, Rockville, MD.
http://www.ahrq.gov/professionals/education/curriculum-
tools/teamstepps/longtermcare/essentials/index.html
Primary Care Behavioral Health Ohio Integrated Health Learning Community Suzanne Daub, LCSW
May 15, 2014
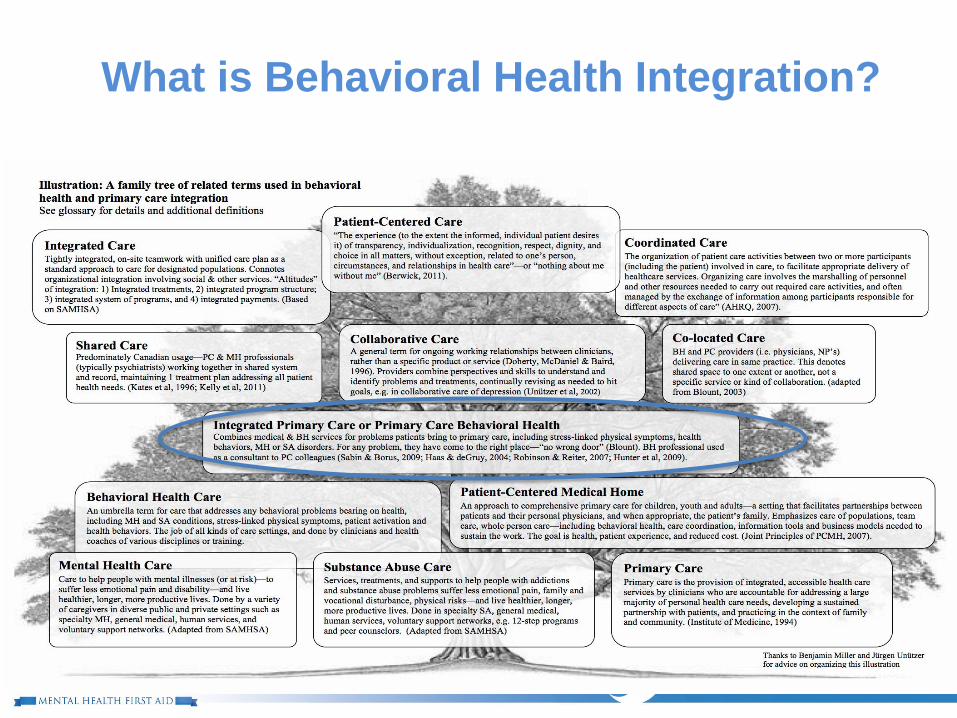
What is Behavioral Health Integration?
The Primary Care Behavioral Health
(PCBH) Model
At the simplest level, integrated behavioral and physical
health care occurs when behavioral and primary care
providers work together to address the physical and
behavioral health needs of their patients.
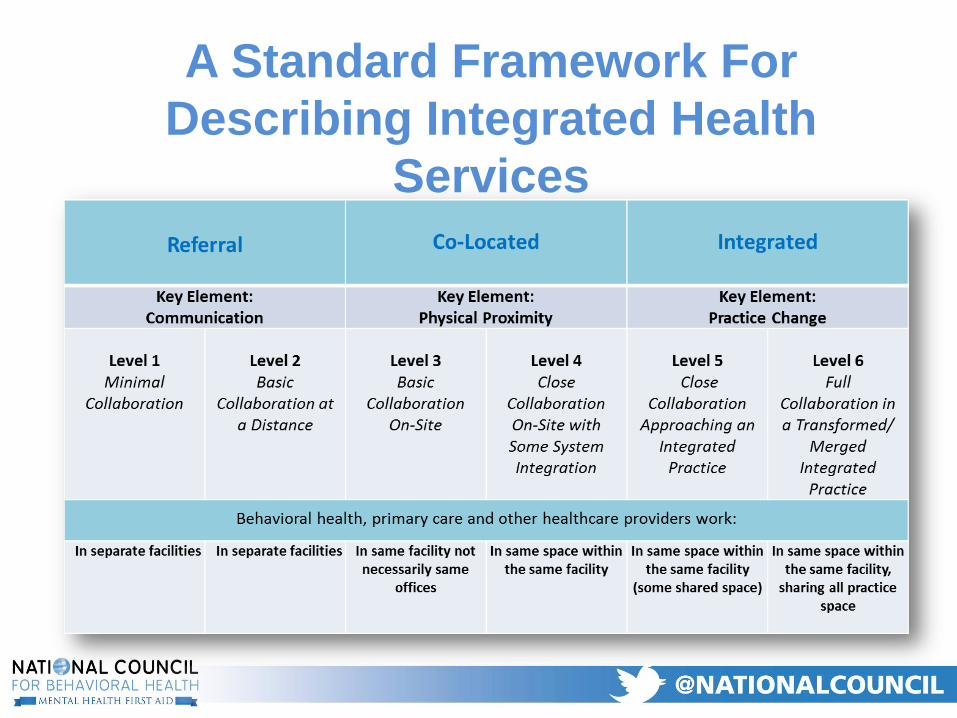
A Standard Framework For
Describing Integrated Health
Services
Integrating Behavioral Health and
Primary Care: Behavioral Health
Consultation
PCBH and Role of Primary Care
Provider
Serves as team leader
Screens for depression, anxiety and trauma
Refers a broad range of patients to behavioral health
Uses behavioral health consistently at certain types of visits (chronic pain, initial dx of diabetes, well child visits, etc.)
Conducts medication evaluation, prescribing, and monitoring
PCBH and Role of Behavioral Health
Work alongside primary care providers as Behavioral Health Consultants (BHCs)
Immediately accessible for both curbside and in-exam room consults, same-day visits (15 – 30 minute consults between 7 – 10/day)
Shared records: chart in the medical record using a Subjective, Objective, Assessment, and Plan (SOAP) note format
Reimbursement by encounter – not by time
No office, No caseload, No “no shows”
Robinson, P.J. and Reiter, J.T. (2007). Behavioral Consultation and Primary Care (pp 1-16). N.Y.: Springer Science + Business Media.
Clinical Approach of Behavioral
Health Consultant
Problem-focused and functional-contextual approach to
assessment and treatment of behavioral health
disorders
Use evidence-based instruments to develop treatment
plans, monitor patient progress, and flexibly provide
care to meet patient’s changing needs:
1. Motivational Interviewing
2. Behavioral Activation
3. Acceptance and Commitment Therapy
4. Screening, Brief Intervention, and Referral to
Treatment (SBIRT)
Robinson, P.J. and Reiter, J.T. (2007). Behavioral Consultation and Primary Care (pp 1-16). N.Y.: Springer Science + Business Media.
Role of the Behavioral Health Consultant
Address a variety of issues common to
primary care:
Affective concerns: depression;
anxiety
Response to physical illness; pain;
substance use and abuse
Health behavior change: obesity,
smoking, sleep, medication
adherence, self management of
chronic conditions
Engage in prevention activities
Hunter, C.L., Goodie, J.L., Oordt, M.S., & Dobmeyer A.C., (2009), Integrated behavioral health in primary care: Step-by-step guidance for assessment and intervention. Washington, DC: American Psychological Association
PCBH − Collaborative Approach
PCPs systematically screen and do “warm hand-offs” according to patient needs
PCPs and BHCs regularly review each other’s notes in the Electronic Medical Record
Regularly consult about patient care and change or adjust treatments if patients do not meet treatment targets
Co-monitor treatment response at each contact with valid outcome measures
Patients who are not improving are identified and targeted for move to a higher level of care
Case Example
Ms. T is a 73 year old African American woman. She is a retired teacher with chronic back pain, hypertension, and a history of multiple hospitalizations for coronary artery disease. She is depressed, has stopped going to church, misses her PCP appointments, and takes her HBP medications “on her own terms.”
To work in integrated care settings…
Basic understanding of primary care medical conditions
Screening, rapid assessment and brief intervention
Motivational interviewing, behavioral activation, self
management
Systems oriented practice including care planning
and care coordination
Primary care communication skills and
interdisciplinary care
Working knowledge of psychopharmacology
Substance use/addiction treatment
(Source: /Forthcoming/ Annapolis Coalition on Behavioral Health Workforce White Paper, “Core Competencies for Integrated Behavioral Health and Primary Care“)
Questions
Resources
SAMHSA/HRSA Center for Integrated Health Solutions (CIHS)
Field-based & Research-based Materials
Council on Social Work Education (CSWE)
Free Integrated Health Social Work Curriculums
Integrated Care Resource Center (ICRC)
Medicaid State Level Tech. Asst. for Integrated Health
AHRQ Academy for Integrating Behavioral Health & Primary Care
Great Research-based Resources
Dear State Medicaid Letters/Centers for Medicaid & Medicare
Services (CMS)
Variety of IH Directives including: Health Home Core Quality
Measures
Resources
Clinical Social Work & Behavioral Medicine Certificate Program
http://www.bu.edu/academics/ssw/programs/clinical-social-work-and-behavioral-medicine-certificate-program/
University of Michigan
Certificate in Integrated Health
http://ssw.umich.edu/offices/continuing-education/certificate-courses/integrated-behavioral-health-and-primary-care
University of Massachusetts
Two Certificate Programs in Integrated Health
http://www.umassmed.edu/cipc/
Fairleigh Dickinson University
Certificate in Integrated Primary Care
http://integratedcare.fdu.edu/
Arizona State University Doctor of Behavioral Health
http://asuonline.asu.edu/dbh





























![arXiv:0709.3025v1 [astro-ph] 19 Sep 2007 · 2018-11-15 · 10 0 52600 52700 52800 52900 53000 53100 53200 53300 53400 53500 Modified Julian Day BH: 1E 1740.7-2942 40 30 20 10 0 BH:](https://img.pdfslide.us/doc/110x75/5fa85a2b74ccc44d330b0ee8/arxiv07093025v1-astro-ph-19-sep-2007-2018-11-15-10-0-52600-52700-52800-52900.jpg)