Embed Size (px)
Citation preview
JOURNALOF
www.elsevier.com/locate/jpsychires
Journal of Psychiatric Research 40 (2006) 267–272
PSYCHIATRIC
RESEARCH
Screening for anxiety disorders in depressed patients
Mark Zimmerman *, Iwona Chelminski
Department of Psychiatry and Human Behavior, Brown University School of Medicine, Rhode Island Hospital,
235 Plain Street, Suite 501, Providence, RI 02905, USA
Received 27 July 2004; received in revised form 6 December 2004; accepted 1 March 2005
Abstract
The Psychiatric Diagnostic Screening Questionnaire (PDSQ) is a brief, psychometrically strong, questionnaire designed to screenfor common Axis I disorders. In the present report, we examine the ability of the PDSQ to identify anxiety disorders in psychiatricoutpatients with a principal diagnosis of major depressive disorder. Eight hundred patients presenting for treatment were evaluatedwith the Structured Clinical Interview for DSM-IV (SCID) after completing the PDSQ. Two hundred ninety-five patients had aprincipal diagnosis of major depressive disorder. The mean sensitivity and negative predictive value of the anxiety disorder subscaleswas 88.5% and 96.5% when all patients were considered, and 88.2% and 95.6% when only depressed patients were examined. ThePDSQ�s anxiety disorder subscales have high sensitivity and negative predictive value thereby indicating that the scale could functionwell as a screening instrument in depressed patients.� 2005 Elsevier Ltd. All rights reserved.
Keywords: Depression; Anxiety disorders; Screening; Diagnosis; Psychiatric Diagnostic Screening Questionnaire
1. Introduction
There is a long history in the mental health field ofusing paper-and-pencil questionnaires to evaluate suchconstructs as personality, temperament, mood, responsestyles, and psychosocial functioning. More than 20 yearsago the publication of specific inclusion criteria to makepsychiatric diagnoses, complemented by the develop-ment of standardized interviews to reliably assess the cri-teria, improved the reliability of psychiatric diagnosis.This development made it possible to develop a newgeneration of self-administered questionnaires thatscreen for or make provisional psychiatric diagnoses.During the past two decades several questionnaires havebeen designed to screen for or ‘‘diagnose’’ single psychi-atric disorders (e.g., Foa et al., 1993; Zimmerman et al.,1986). More recently, some scales have been developed
0022-3956/$ - see front matter � 2005 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jpsychires.2005.03.001
* Corresponding author. Tel.: +1 401 277 0724; fax: +1 401 2770726.
E-mail address: [email protected] (M. Zimmerman).
to assess multiple disorders (Broadhead et al., 1995;Spitzer et al., 1999).
The purpose of screening is to improve diagnosticrecognition. Recent research suggests that there is aproblem with the recognition of anxiety disorders inclinical practice. Shear et al. (2000) interviewed 164 psy-chiatric outpatients with the Structured Clinical Inter-view for DSM-IV (SCID) after they were evaluatedclinically, and found that in contrast to the small num-ber of patients diagnosed by clinicians with an anxietydisorder (13%), more than half (53%) of the patientsinterviewed with the SCID were diagnosed with a cur-rent anxiety disorder. Zimmerman and Mattia (1999b)examined diagnostic frequencies in two separate samplesof 500 patients drawn from the same outpatient practice,the first group diagnosed by clinicians based on anunstructured clinical evaluation and the second diag-nosed by raters administering the SCID. Panic disorder,social phobia, specific phobia, generalized anxietydisorder (GAD), obsessive-compulsive disorder (OCD),and posttraumatic stress disorder (PTSD) were all

268 M. Zimmerman, I. Chelminski / Journal of Psychiatric Research 40 (2006) 267–272
significantly less frequently diagnosed in the clinicallyevaluated patients. In a separate paper, we focused onthe diagnosis of anxiety disorders in depressed patientsbecause this is a frequent form of diagnostic comorbid-ity that has potential treatment implications (Zimmer-man and Chelminski, 2003a). In that paper, wereported that anxiety disorders are underrecognized indepressed patients evaluated in routine clinical practice,and that depressed patients usually want treatment toaddress these comorbid anxiety disorders.
Traditionally, when examining the performance ofscreening questionnaires, their performance has beenexamined in the entire sample evaluated. Such a strategywas followed in our initial report of the diagnostic per-formance of the Psychiatric Diagnostic Screening Ques-tionnaire (PDSQ) (Zimmerman and Mattia, 2001b).However, in examining the performance of screeningscales, a distinction should be made between principaland additional diagnoses. In mental health settings, diag-nostic recognition should be adequate for the principaldisorders for which patients seek treatment (i.e., the chiefcomplaint). In contrast, the recognition of comorbid dis-orders that are not the principal reason for seeking treat-ment may be problematic. Evidence of this was found inour study of clinicians� recognition of PTSD (Zimmer-man and Mattia, 1999a). When PTSD was the principaldiagnosis, then the frequency of PTSD diagnoses wassimilar according to unstructured clinical interviewsand semi-structured research evaluations. In contrast,when PTSDwas an additional, comorbid, condition thenclinicians were significantly less likely to detect its pres-ence compared to research evaluations. Because the pur-pose of screening is to improve diagnostic recognition,this suggests that when evaluating a screening scale�s per-formance in psychiatric patients the focus should be onits diagnostic properties for disorders that are not theprincipal reason for seeking treatment.
As a follow-up to our paper on clinician recognitionof anxiety disorders in depressed patients we turn to is-sue of screening for anxiety disorders in depressed pa-tients. The recognition of comorbidity is not simply ofacademic interest – it has important clinical significance.Epidemiological studies such as the National Comorbid-ity Study have demonstrated that depressed individualswith a history of anxiety disorders are at increased riskfor hospitalization, suicide attempt, and greater impair-ment from the depression (Kessler et al., 1994, 1996).The co-occurrence of anxiety disorders in depressed pa-tients has been associated with a more chronic course ofdepression in psychiatric patients, primary care patients,and epidemiological samples (Van Valkenburg et al.,1984; Coryell et al., 1988; Grunhaus, 1988; Brownet al., 2000; Sherbourne and Wells, 1997; Gayneset al., 1999).
Controlled studies of the prognostic significance ofanxiety disorders in depressed patients have also sug-
gested that the presence of comorbid anxiety disordersis associated with poorer outcome. Fava et al. (1997)treated nearly 300 depressed outpatients with fluoxetineand found that patients with a comorbid anxiety disor-der were less likely to respond than depressed patientswithout a comorbid anxiety disorder. In Brown et al.�s(1996) primary care study of nortriptyline and interper-sonal therapy, the presence of a comorbid anxiety disor-der was associated with a nonsignificantly higher rate ofpremature discontinuation from treatment, and patientswith a lifetime history of panic disorder had a lowerrecovery rate than patients without panic. Levitt et al.(1993) treated 31 depressed outpatients with seasonalaffective disorder (SAD) with light therapy and 25 pa-tients without SAD with desipramine or imipramine.The presence of a comorbid anxiety disorder did notpredict response to light therapy in the patients withSAD. In the patients without SAD who were treatedwith a TCA, the presence of a comorbid anxiety disor-der was associated with a significantly lower responserate. None of these studies, however, included a placebogroup.
There are no studies that have examined the impor-tant question of whether the treatment of depressed pa-tients with and without comorbid anxiety disordersshould differ; though clinical experience and inferencefrom the extant literature suggests that the presence ofa comorbid anxiety disorder impacts upon case formula-tion and treatment planning (Nutt, 1999; Pollack andMarzol, 2000; Roy-Byrne, 1999). For example, treat-ment planning for depressed patients with a comorbidanxiety disorder could include referral for CBT for theanxiety disorder. Choice and dosing of pharmacologicagents might also vary. Depressed patients with acomorbid panic disorder might have a benzodiazepineprescribed as well as an antidepressant at treatment on-set in order to achieve more rapid relief from the panicattacks. If an SSRI is prescribed, dosage titration mightbe more gradual (Gorman et al., 1987). The best empir-ically supported treatment decision is the preferentialselection of an SSRI over a TCA in the treatment of de-pressed patients with comorbid OCD (Hoehn-Saricet al., 2000). Depression comorbid with social phobiamight also be preferentially prescribed an SSRI. Theaddition of a benzodiazepine might be considered in de-pressed patients with comorbid GAD.
Although there is little controlled data demonstratingpreferred treatment strategies in depressed patients withcomorbid anxiety disorders, the presence of anxiety dis-order comorbidity frequently influences psychiatrists�selection of antidepressant medication (Zimmermanet al., 2004). Consequently, the detection of anxiety dis-orders in depressed patients has clinical relevance. In thepresent report from the Rhode Island Methods toImprove Diagnostic Assessment and Services (MIDAS)project we examined the ability of the PDSQ to identify
M. Zimmerman, I. Chelminski / Journal of Psychiatric Research 40 (2006) 267–272 269
anxiety disorders in psychiatric outpatients with a prin-cipal diagnosis of MDD.
2. Methods
Eight hundred patients presenting for treatment inthe Rhode Island Hospital Department of Psychiatryoutpatient practice were evaluated by a trained diagnos-tic interviewer who administered the Structured ClinicalInterview for DSM-IV (SCID) (First et al., 1995). Aspart of their initial paperwork all patients completedthe PDSQ before the SCID. The diagnostic raters didnot review patients� responses on the PDSQ. The RhodeIsland Hospital institutional review committee approvedthe research protocol, and all patients provided in-formed, written consent.
The PDSQ has undergone several rounds of studyinvolving more than 3000 primary care and psychiatricoutpatients. After each large validation study the scalewas revised based on a psychometric analysis of the sub-scales and items. The final version of the PDSQ consistsof 126 questions assessing the symptoms of 13 DSM-IVdisorders in 5 areas: eating disorders (bulimia/binge eat-ing disorder), mood disorders (MDD), anxiety disorders(panic disorder, agoraphobia, PTSD, OCD, GAD andsocial phobia), substance use disorders (alcohol abuse/dependence, drug abuse/dependence), and somatoformdisorders (somatization disorder, hypochondriasis). Inaddition, there is a six-item psychosis screen.
In the validity study of the final version of the PDSQ,994 psychiatric outpatients completed the scale (Zim-merman and Mattia, 2001a). The 13 PDSQ subscalesdemonstrated good to excellent levels of internal consis-tency. Cronbach�s alpha was greater than 0.80 for 12 ofthe 13 subscales, and the mean of the alpha coefficientswas 0.86. Test-retest reliability was examined in 185 sub-jects who completed the PDSQ two times less than aweek apart. Test-retest reliability coefficients were greaterthan 0.80 for 9 subscales, and the mean of the test-retestcorrelation coefficients was 0.83. The convergent anddiscriminant validity of the PDSQ subscales was exam-ined in 361 patients who completed a package of ques-tionnaires at home less than a week after completingthe PDSQ. The booklet included measures of symptomsrelated to each of the PDSQ symptoms domains. EveryPDSQ subscale was more highly correlated with the con-cordant validity scale assessing the same symptom do-main versus other symptoms domains. Across allsubscales, the mean correlation between the PDSQ sub-scales and their respective validity scale was 0.66, whilethe mean correlation between PDSQ subscales and mea-sures of other symptom domains was 0.25. Finally, thediagnostic performance of the PDSQ subscales wasexamined in 630 patients interviewed with the SCID.Based on cutoff scores associated with 90% sensitivity,
the mean specificity and negative predictive value ofthe PDSQ subscales was 66% and 97%, respectively(Zimmerman and Mattia, 2001b).
Depending on the scale�s purpose, cutoff scores mightbe selected to optimize the sensitivity or specificity of thescale. In our previous report of the diagnostic propertiesof the PDSQ we recommended that a cutoff resulting indiagnostic sensitivity of 90% be chosen when using thescale in clinical practice. We used the same cutoffs inthe present report to examine the diagnostic propertiesof the PDSQ anxiety disorder subscales in depressed pa-tients, and compared these results to the diagnostic per-formance of the PDSQ anxiety disorder subscales in theentire sample. We also evaluated the scales� diagnosticperformance across the range of cutoff scores by con-ducting receiver operating curve (ROC) analyses andcomputing the areas under the curve (AUC).
3. Results
The majority of the 800 patients were white (88.8%,n = 710), female (63.1%, n = 505), married (40.4%,n = 323) or single (30.8%, n = 246), and had some col-lege education (67.1%, n = 537). The mean age of thesample was 37.7 years (SD = 12.2). Two hundredninety-five patients received a principal diagnosis ofDSM-IV nonbipolar MDD. We followed the DSM-IVconvention to distinguish between principal and addi-tional diagnoses. That is, the principal diagnosis referredto the features of the disorder that the patient indicatedwas the main reason for seeking treatment; all otherdiagnoses were considered additional diagnoses.
The data in Table 1 show the diagnostic properties ofthe PDSQ anxiety disorder subscales in depressed pa-tients. For comparison purposes the results for the entiresample are also presented. In depressed patients thePDSQ subscales maintained excellent sensitivity, andcontinued to have high negative predictive value. AllAUCs were significant. The mean sensitivity and nega-tive predictive value of the anxiety disorder subscaleswas 88.5% and 96.5% when all patients were considered,and 88.2% and 95.6% when only depressed patients wereexamined. The AUC from the Receiver Operating Char-acteristic (ROC) analyses decreased from 0.84 to 0.79,but all remained significant. These results suggest thatthe anxiety disorder subscales of the PDSQ do a goodjob of identifying anxiety disorders in depressed psychi-atric outpatients (i.e. they have high sensitivity), and anexcellent job identifying individuals who are unlikely tohave an anxiety disorder (i.e., they have very high nega-tive predictive value). The specificity of the PDSQ sub-scales, however, decreased when the analysis waslimited to anxiety disorders as comorbid conditions indepressed patients. Further, when we compared theAUCs in nonoverlapping groups of patients with
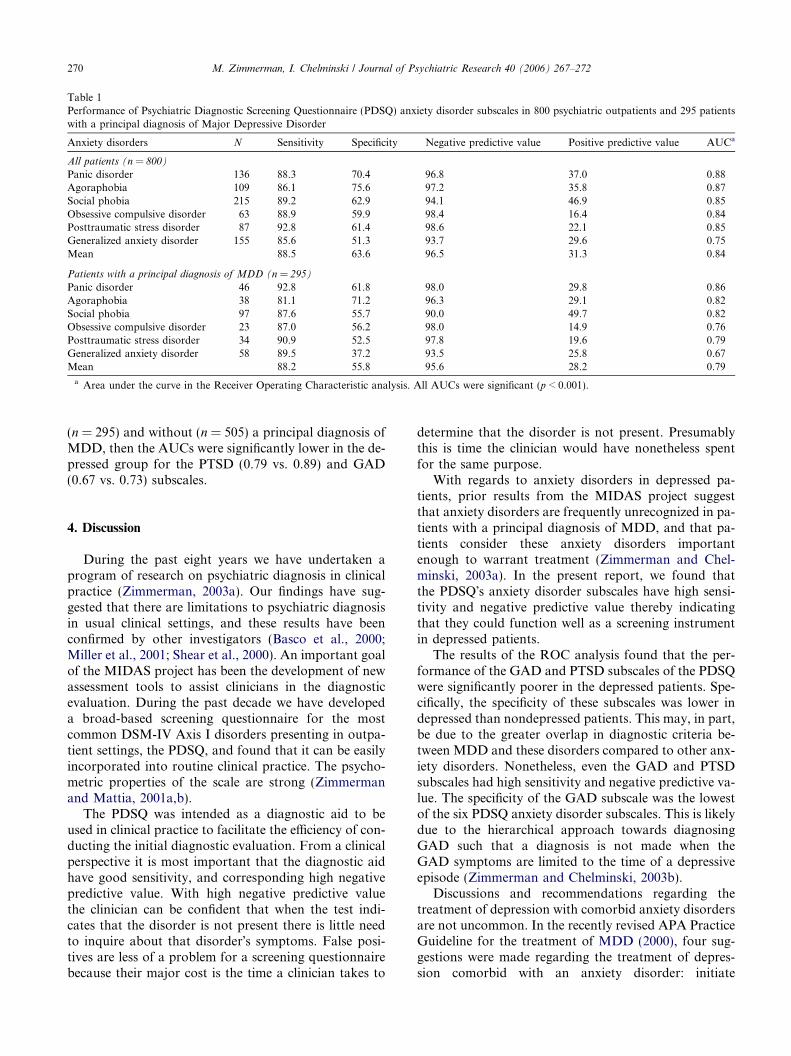
Table 1Performance of Psychiatric Diagnostic Screening Questionnaire (PDSQ) anxiety disorder subscales in 800 psychiatric outpatients and 295 patientswith a principal diagnosis of Major Depressive Disorder
Anxiety disorders N Sensitivity Specificity Negative predictive value Positive predictive value AUCa
All patients (n = 800)
Panic disorder 136 88.3 70.4 96.8 37.0 0.88Agoraphobia 109 86.1 75.6 97.2 35.8 0.87Social phobia 215 89.2 62.9 94.1 46.9 0.85Obsessive compulsive disorder 63 88.9 59.9 98.4 16.4 0.84Posttraumatic stress disorder 87 92.8 61.4 98.6 22.1 0.85Generalized anxiety disorder 155 85.6 51.3 93.7 29.6 0.75Mean 88.5 63.6 96.5 31.3 0.84
Patients with a principal diagnosis of MDD (n = 295)
Panic disorder 46 92.8 61.8 98.0 29.8 0.86Agoraphobia 38 81.1 71.2 96.3 29.1 0.82Social phobia 97 87.6 55.7 90.0 49.7 0.82Obsessive compulsive disorder 23 87.0 56.2 98.0 14.9 0.76Posttraumatic stress disorder 34 90.9 52.5 97.8 19.6 0.79Generalized anxiety disorder 58 89.5 37.2 93.5 25.8 0.67Mean 88.2 55.8 95.6 28.2 0.79
a Area under the curve in the Receiver Operating Characteristic analysis. All AUCs were significant (p < 0.001).
270 M. Zimmerman, I. Chelminski / Journal of Psychiatric Research 40 (2006) 267–272
(n = 295) and without (n = 505) a principal diagnosis ofMDD, then the AUCs were significantly lower in the de-pressed group for the PTSD (0.79 vs. 0.89) and GAD(0.67 vs. 0.73) subscales.
4. Discussion
During the past eight years we have undertaken aprogram of research on psychiatric diagnosis in clinicalpractice (Zimmerman, 2003a). Our findings have sug-gested that there are limitations to psychiatric diagnosisin usual clinical settings, and these results have beenconfirmed by other investigators (Basco et al., 2000;Miller et al., 2001; Shear et al., 2000). An important goalof the MIDAS project has been the development of newassessment tools to assist clinicians in the diagnosticevaluation. During the past decade we have developeda broad-based screening questionnaire for the mostcommon DSM-IV Axis I disorders presenting in outpa-tient settings, the PDSQ, and found that it can be easilyincorporated into routine clinical practice. The psycho-metric properties of the scale are strong (Zimmermanand Mattia, 2001a,b).
The PDSQ was intended as a diagnostic aid to beused in clinical practice to facilitate the efficiency of con-ducting the initial diagnostic evaluation. From a clinicalperspective it is most important that the diagnostic aidhave good sensitivity, and corresponding high negativepredictive value. With high negative predictive valuethe clinician can be confident that when the test indi-cates that the disorder is not present there is little needto inquire about that disorder�s symptoms. False posi-tives are less of a problem for a screening questionnairebecause their major cost is the time a clinician takes to
determine that the disorder is not present. Presumablythis is time the clinician would have nonetheless spentfor the same purpose.
With regards to anxiety disorders in depressed pa-tients, prior results from the MIDAS project suggestthat anxiety disorders are frequently unrecognized in pa-tients with a principal diagnosis of MDD, and that pa-tients consider these anxiety disorders importantenough to warrant treatment (Zimmerman and Chel-minski, 2003a). In the present report, we found thatthe PDSQ�s anxiety disorder subscales have high sensi-tivity and negative predictive value thereby indicatingthat they could function well as a screening instrumentin depressed patients.
The results of the ROC analysis found that the per-formance of the GAD and PTSD subscales of the PDSQwere significantly poorer in the depressed patients. Spe-cifically, the specificity of these subscales was lower indepressed than nondepressed patients. This may, in part,be due to the greater overlap in diagnostic criteria be-tween MDD and these disorders compared to other anx-iety disorders. Nonetheless, even the GAD and PTSDsubscales had high sensitivity and negative predictive va-lue. The specificity of the GAD subscale was the lowestof the six PDSQ anxiety disorder subscales. This is likelydue to the hierarchical approach towards diagnosingGAD such that a diagnosis is not made when theGAD symptoms are limited to the time of a depressiveepisode (Zimmerman and Chelminski, 2003b).
Discussions and recommendations regarding thetreatment of depression with comorbid anxiety disordersare not uncommon. In the recently revised APA PracticeGuideline for the treatment of MDD (2000), four sug-gestions were made regarding the treatment of depres-sion comorbid with an anxiety disorder: initiate

M. Zimmerman, I. Chelminski / Journal of Psychiatric Research 40 (2006) 267–272 271
antidepressant medication at lower than usual dosagesand slowly titrate upwards; SSRIs and clomipramineare effective for OCD and therefore should be consid-ered when treating depressed patients with comorbidobsessive features; buproprion has not been found tobe effective in the treatment of panic disorder (andalthough the guidelines do not specifically state this,the inference is that this medication should not be con-sidered a first line treatment for depressed patients withthis comorbidity); and benzodiazepines may be benefi-cial augmenting agents in the short term. Except forthe single OCD study, none of the treatment suggestionsdescribed above have been subjected to empiricaltesting.
Whether improved detection of comorbid anxiety dis-orders in depressed patients will result in improved out-come is an empirical question. It is possible that thepresence of a comorbid anxiety disorder will be associ-ated with poorer outcome even when the diagnosis isknown (Zimmerman, 2003b). Future research shouldexamine whether the information from a self-reportscale such as the PDSQ can improve clinicians� recogni-tion of anxiety disorders in depressed patients and con-sequently improve their outcome.
References
APA. Practice guideline for the treatment of patients with majordepressive disorder (Revision). Washington, DC, 2000.
Basco MR, Bostic JQ, Davies D, Rush AJ, Witte B, Hendrickse W,et al. Methods to improve diagnostic accuracy in a communitymental health setting. American Journal of Psychiatry2000;157:1599–605.
Broadhead WE, Leon AC, Weissman MM, Barrett JE, Blacklow RS,Gilbert TT, et al. Development and validation of the SDDS-PCscreen for multiple mental disorders in primary care. Archives ofFamily Medicine 1995;4:211–9.
Brown C, Schulberg HC, Madonia MJ, Shear MK, Houck PR.Treatment outcomes for primary care patients with major depres-sion and lifetime anxiety disorders. American Journal of Psychiatry1996;153:1293–300.
Brown C, Schulberg HC, Prigerson HG. Factors associated withsymptomatic improvement and recovery from major depression inprimary care patients. General Hospital Psychiatry2000;22:242–50.
Coryell W, Endicott J, Andreasen NC, Keller MB, Clayton PJ,Hirschfield RMA, Scheftner WA, Winokur G. Depression andpanic attacks: The significance of overlap as reflected in follow-upand family study data. American Journal of Psychiatry1988;145:293–300.
Fava M, Uebelacker LA, Alpert JE, Nierenberg AA, Pava JA,Rosenbaum JF. Major depressive subtypes and treatment response.Biological Psychiatry 1997;42:568–76.
First MB, Spitzer RL, Gibbon M, Williams JBW. Structured clinicalinterview for DSM-IV Axis I disorders – patient edition (SCID-I/P,version 2.0). New York: Biometrics Research Department, NewYork State Psychiatric Institute; 1995.
Foa EB, Riggs DS, Dancu CV, Rothbaum BO. Reliability and validityof a brief instrument for assessing post-traumatic stress disorder.Journal of Traumatic Stress 1993;6:459–73.
Gaynes BN, Magruder KM, Burns BJ, Wagner HR, Yarnall KSH,Broadhead WE. Does a coexisting anxiety disorder predictpersistence of depressive illness in primary care patients with majordepression. General Hospital Psychiatry 1999;21:158–67.
Gorman JM, Liebowitz MR, Fyer AJ, Goetz D, Campeas D, FyerMR, Davies SO, Klein DF. An open trial of fluoxetine in thetreatment of panic attacks. Journal of Clinical Psychopharmacol-ogy 1987;7:329–32.
Grunhaus L. Clinical and psychobiological characteristics of simulta-neous panic disorder and major depression. American Journal ofPsychiatry 1988;145:1214–21.
Hoehn-Saric R, Ninan P, Black DW, Stahl S, Greist JH,Lydiard B, McElroy S, Zajecka J, Chapman D, Clary C,Harrison W. Multicenter double-blind comparison or sertralineand desipramine for concurrent obsessive-compulsive andmajor depressive disorders. Archives of General Psychiatry2000;57:76–82.
Kessler R, McGonagle K, Zhao S, Nelson C, Hughes M, Eshleman S,Wittchen H, Kendler K. Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States. Results fromthe National Comorbidity Survey. Archives of General Psychiatry1994;51:8–19.
Kessler R, Nelson C, McGonagle K, Liu J, Swartz M, Blazer D.Comorbidity of DSM-III-R major depressive disorder in thegeneral population: results from the US National ComorbiditySurvey. British Journal of Psychiatry Supplement 1996;30:17–30.
Levitt AJ, Joffe RT, Brecher D, MacDonald C. Anxiety disorders andanxiety symptoms in a clinic sample of seasonal and non-seasonaldepressives. Journal of Affective Disorders 1993;28:51–6.
Miller PR, Dasher R, Collins R, Griffiths P, Brown F. Inpatientdiagnostic assessments: 1. Accuracy of structured vs. unstructuredinterviews. Psychiatry Research 2001;105:255–64.
Nutt DJ. Care of depressed patients with anxiety symptoms. Journal ofClinical Psychiatry 1999;60(suppl):23–7.
Pollack MH, Marzol PC. Pharmacotherapeutic options in the treat-ment of comorbid depression and anxiety. CNS Spectrums2000;5:23–30.
Roy-Byrne PP. Anxiety in primary care depression: How does it leadto poor outcomes and what can we do about it?. General HospitalPsychiatry 1999;21:151–3.
Shear MK, Greeno C, Kang J, Ludewig D, Frank E, Swartz HA, et al.Diagnosis of nonpsychotic patients in community clinics. AmericanJournal of Psychiatry 2000;157:581–7.
Sherbourne CD, Wells KB. Course of depression in patients withcomorbid anxiety disorders. Journal of Affective Disorders1997;43:245–50.
Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME MD: the PHQ primary care study.Primary Care Evaluation of Mental Disorders. Patient HealthQuestionnaire. Journal of the American Medical Association1999;282:1737–44.
Van Valkenburg C, Akiskal HS, Puzantian V, Rosenthal T. Anxiousdepressions: clinical, family history, and naturalistic outcome-comparisons with panic and major depressive disorders. Journal ofAffective Disorders 1984;6:67–82.
Zimmerman M. Integrating the assessment methods of researchersin routine clinical practice: The Rhode Island Methods toImprove Diagnostic Assessment and Services (MIDAS) project.In: First M, editor. Standardized evaluation in clinicalpractice. Washington: American Psychiatric Publishing, Inc;2003a. p. 29–74.
Zimmerman M. What should the standard of care for psychiatricdiagnostic evaluations be?. The Journal of Nervous and MentalDisease 2003b;191:281–6.
Zimmerman M, Chelminski I. Clinician recognition of anxietydisorders in depressed outpatients. Journal of Psychiatric Research2003a;37:325–33.

272 M. Zimmerman, I. Chelminski / Journal of Psychiatric Research 40 (2006) 267–272
Zimmerman M, Chelminski I. Generalized anxiety disorder in patientswith major depressive disorder: Is DSM-IV�s hierarchy correct?American Journal of Psychiatry 2003b;160:504–12.
Zimmerman M, Coryell W, Corenthal C, Wilson S. A self-report scaleto diagnose major depression disorder. Archives of GeneralPsychiatry 1986;43:1076–81.
Zimmerman M, Mattia JI. Is posttraumatic stress disorder underdi-agnosed in routine clinical settings? Journal of Nervous and MentalDisease 1999a;187:420–8.
Zimmerman M, Mattia JI. Psychiatric diagnosis in clinicalpractice: Is comorbidity being missed? Comprehensive Psychi-atry 1999b;40:182–91.
Zimmerman M, Mattia JI. The Psychiatric Diagnostic ScreeningQuestionnaire: Development, reliability and validity. Comprehen-sive Psychiatry 2001a;42:175–89.
Zimmerman M, Mattia JI. A self-report scale to help makepsychiatric diagnoses: The Psychiatric Diagnostic Screening Ques-tionnaire (PDSQ). Archives of General Psychiatry2001b;58:787–94.
Zimmerman M, Posternak M, Friedman M, Attiullah N,Baymiller S, Boland R, Berlowitz S, Rahman S, Uy K,Singer S. Which factors influence psychiatrists� selection of anantidepressant? American Journal of Psychiatry2004;161:1285–9.