Embed Size (px)
Citation preview


Scoring Health Reform: Where Economics and Health Policy Meet
Stephen T. Parente, Ph.D., M.P.H.Professor and Minnesota Insurance Industry Chair of Health FinanceDepartment of FinanceDirector, Medical Industry Leadership InstituteUniversity of MinnesotaCarlson School of Management
Heller-Hurwicz InstituteNovember 17, 2011

Agenda Level Set: The Trillion Dollar Health
Marketplace Scoring Objectives New York Health Reform/Debate Example What is the Economics that drives
simulation What are simulations projecting now? Health reform alternatives to 2009/2010 law What is on the horizon?

Physicians
Congress Main StreetMedical Technology
Courts
Federal Government
<90% Income
Insurers 99% Income 91-99% Income
Big Business
Hospitals
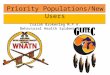
The $2.7 Trillion
HealthcareMarketplace
The $2.7 Trillion
HealthcareMarketplace

Scoring Objectives Federal/State government reform cost (1 & 10
year) Tax credits, deductions, vouchers, subsidies, system
investments, direct service provision. Federal/state government revenue generated
Taxes and fees collected – usually from change in tax law for individuals and corporations.
Change in insured/uninsured System wide impact (non-tax $$$ effects placed
upon stakeholders – positive & negative)

Scoring Challenges Inter-related set of factors that play on each
over time – dynamic simultaneous equations Little true data to be used to predict
response from comparable experiments or demonstrations
Few actual ‘levers’ to test effect based on real data
Little peer review and few colleagues that are not ‘conflicted’ or ‘private’ or ‘non-transparent’

Levers that Matter
Credits/Deductions/Subsidies Insurance Choice Set Plan Design Premiums in the Real World State-specific factors Growth rate & inflation Income-related points of inflection Out of Sample Land - Missing data
assumptions

New York Health Reform Debate:Policy ‘Influence’ Tool – The Op-Ed

Estimate plan offerings using linked data
Merge employer data
Estimate hedonic premium regression
Assign plan choices to full MEPS sample
Estimate plan choice regression
Use parameter estimates to predict plan choice probabilities for MEPSRe-scale take-up rates
Define plan design & premium
Simulate impact of proposed policies
Model Estimation
Choice set Assignment/Prediction
Policy Simulation
Economic Components for MicrosSimulation
MEPSData Sources CDHPs eHealthinsurance

Economic Model:Demand for Health Insurance Plan Choices: HMO, 3 Preferred Provider Organizations
(PPOs) (low, medium, high premiums), High Deductible health plans with Health Reimbursement/Savings Accounts
Utility-maximization assumption where Uhj = j + Zj + Xhj + ehj
Estimate a conditional logit model of plan choice using the pooled, employer data
Explanatory variables Plan attributes (Z)
Annual tax-adjusted employee premium ($1000s dollars) Savings/reimbursement account size ($1000s dollars) Donut hole: difference between annual deductible and account
size ($1000s dollars) Coinsurance rate (i.e., .10 = 10% coinsurance)
Interactions between employee and plan attributes (X) Age, female, wage income, family contract
Plan-specific constants (j )

Economic Model Data Sources Health plan choice data from several large employers
participating in a Robert Wood Johnson Foundation funded study on health insurance Employee premium, deductible, coinsurance, worker’s
age, gender, wage income, single/family coverage Federal Medical Expenditure Panel Survey (MEPS)
Household Component: All adults age 19-64 not enrolled in public insurance programs and not full-time students during Round 1 Demographic, employment, and health insurance
information Linked Insurance Component: Subset of workers offered
employer coverage and their plan choices Plan type, premiums, contributions, coinsurance,
copayments and deductibles eHealthinsurance.com
Individual health plan information

Plan Choices in the NY Simulation Direct Pay Low PPO
restrictive network high co-pay 15 percent coinsurance
Direct Pay Medium PPO Lower co-pay and coinsurance than the Low
PPO Direct Pay High PPO
lowest co-pay no coinsurance
HSA High deductible , low account contribution

Simulation Calibration Applied plan choice model estimates to predict
probabilities of plan choices for Federal MEPS sample respondents
Model Calibrations % of adults who turn down employer offers
by income quartile % of adults in the individual market who are
uninsured by income quartile Applied New York State population weights to
the calibrated model to represent the population 19-64, excluding full-time students, those enrolled in public insurance, and non-offered dependents with employer coverage through their spouse

Plan Choice – Conditional Logit (1 of 2)
Adjusted r-square: ~0.363, Reference PPO_High
StandardVariable Coefficient Error T-Statistic P-valueTax adjusted Employee Premium in $1,000 -1.7299 0.0665 -25.9996 <.0001Employee's Health Account in $1,000 0.6179 0.0974 6.3407 <.0001∆ Between Deductible and Health Account in $1,000 -0.8502 0.0272 -31.2867 <.0001Coinsurance (e.g., 15% = .15) -7.5675 0.5300 -14.2794 <.0001PPO Medium Plan Intercept=1, else=0 0.1153 0.0860 1.3404 0.1801PPO Low Plan Intercept=1, else=0 -1.0210 0.1311 -7.7887 <.0001High HRA Plan Intercept=1, else=0 -1.9816 0.1646 -12.0383 <.0001Low HRA* Plan Intercept=1, else=0 -1.7031 0.1252 -13.6042 <.0001HMO Plan Intercept=1, else=0 1.9338 0.1048 18.4506 <.0001Premium & Family Contract (0/1) Interaction 1.1067 0.0721 15.3418 <.0001PPO Medium & Age (in 100 years) Interacttion -1.5547 0.1673 -9.2926 <.0001PPO Low & Age (in 100 years) Interaction 0.5609 0.2917 1.9228 0.0545HRA & Age (in 100 years) Interaction -2.0759 0.3506 -5.9217 <.0001HSA_S/E & Age (in 100 years) Interaction -2.5626 0.2410 -10.6318 <.0001HMO & Age (in 100 years) Interaction -3.9740 0.1946 -20.4199 <.0001
N=28,737* We used Low HRA to create HSA 'predicting' coefficients for an individual version where theemployee pays all (S) and the employer offered version where the premium and the accountis heavily subsidized (E).

Plan Choice – Conditional Logit (2 of 2)
Adjusted r-square: ~0.363, Reference PPO_High
StandardVariable Coefficient Error T-Statistic P-valuePPO Medium & Income (in $1,000) Interaction -0.0005 0.0006 -0.8201 0.4122PPO Low & Income (in $1,000) Interaction 0.0038 0.0014 2.6689 0.0076HRA & Income (in $1,000) Interaction 0.0100 0.0009 11.6295 <.0001HSA_S/E & Income (in $1,000) Interaction 0.0102 0.0006 17.5883 <.0001HMO & Income (in $1,000) Interaction -0.0017 0.0007 -2.3806 0.0173PPO Medium & Female (0/1) Interaction 0.0852 0.0369 2.3100 0.0209PPOLow & & Female (0/1) Interaction -0.1566 0.0617 -2.5373 0.0112HRA & Female (0/1) Interaction -0.1665 0.0776 -2.1456 0.0319HSA_S/E & Female (0/1) Interaction -0.0278 0.0514 -0.5399 0.5893HMO & Female (0/1) Interaction -0.1892 0.0435 -4.3506 <.0001PPO Medium & Family Contract (0/1) Interaction 0.0218 0.0690 0.3154 0.7525PPO Low & Family Contract (0/1) Interaction 0.3809 0.0773 4.9275 <.0001HRA & Family Contract (0/1) Interaction -0.2979 0.1140 -2.6132 0.0090HSA_S/E & Family Contract (0/1) Interaction 0.0067 0.1144 0.0586 0.9533HMO & Family Contract (0/1) Interaction -0.3651 0.0909 -4.0175 <.0001
N=28,737

Scenarios Modeled for New York
Removing restrictions on underwriting community rating guaranteed issue
Allowing Health Savings Accounts into the market Currently, these high-deductible savings plans may
not be sold in the New York State individual market.
Allowing the purchase of policies issued by insurers based in and regulated by neighboring states.
Allow the sale of “mandate lite” plans

Micro-simulation Used - ARCOLA
ARCOLA (Adjusted Risk Choice & Outcomes Legislative Assessment)
ARCOLA is a micro-simulation model designed to estimate the impact of health policy proposals at the federal and state level
Model first used by the Office of the Assistant Secretary of Planning and Evaluation (OASPE) of the Department of Health and Human Services (DHHS)

ARCOLA’s strengths & weaknesses
Strengths Peer-reviewed in Health
Affairs & Journal of Risk & Insurance
Can be used for federal & state estimates
Is based on a microeconomic model of health insurance demand published in three journals
Is supported by consumer driven health plan choice, cost & use
Weaknesses Needs survey data from a
state to make estimates – Zogby provided data for this analysis
Has not been bench-tested with Urban or Columbia University models with state data
Works only through price effects, but that is the dominant factor affecting insurance choice

What is the Impact of Eliminating Community Rating (CR) and Guaranteed Issue (GI) and Introducing Health Savings Accounts?
New York Health Insurance Reform Options2009 Estimates
Baseline Rx New York % Rx New York % Rx New York %
Individual Market Population No GI Change No CR & GI Change No CR & GI Change
& HSAs
Direct Pay - HSA 0 0 N/A 0 N/A 35,383 N/ADirect Pay - PPO High 16,939 365,817 2060% 766,953 4428% 741,572 4278%Direct Pay - PPO Low 9,658 8,903 -8% 5,914 -39% 5,648 -42%Direct Pay - PPO Medium 7,649 31,172 308% 35,786 368% 34,259 348%Uninsured 2,107,530 1,735,884 -18% 1,333,122 -37% 1,324,915 -37%
Total Direct Pay 34,246 405,891 808,653 816,861 Total Population 2,141,776 2,141,776 2,141,776 2,141,776
The combined effect of No CR & GI is a 37% reduction in the Number of uninsured in NYS.

What is the Impact of Interstate Market Competition?
If everyone took advantage of lower premiums, therewould be a 26% reduction. A 17% reduction if ¼ buy CT,PA
New York Health Insurance Reform Options2009 Estimates
Status Quo PA & CT % PA & CT %
Individual Market Population Entry - 100% Change Entry - 25% Change
participation participation
Direct Pay - HSA 0 49,662 N/A 65,036 N/ADirect Pay - PPO High 16,939 464,498 2642% 208,108 1129%Direct Pay - PPO Low 9,658 9,108 -6% 15,828 64%Direct Pay - PPO Medium 7,649 54,511 613% 106,874 1297%Uninsured 2,107,530 1,563,997 -26% 1,745,930 -17%
Total Direct Pay 34,246 577,778 395,846 Total Population 2,141,776 2,141,776 2,141,776

What is the Impact of Reducing the Number of Mandates in New York?
If 20 mandates were removed, the impact would be a 3% reduction in the uninsured, 9% reduction if 40 mandates removed.
New York Health Insurance Reform Options2009 Estimates
Status Quo Mandate- % Mandate- %
Individual Market Population Lite Plan Change Lite Plan Change
20 Mandates 40 Mandates
Direct Pay - HSA 0 15,515 N/A 28,141 N/ADirect Pay - PPO High 16,939 53,343 215% 152,665 801%Direct Pay - PPO Low 9,658 12,041 25% 13,799 43%Direct Pay - PPO Medium 7,649 15,885 108% 29,887 291%Uninsured 2,107,530 2,044,992 -3% 1,917,284 -9%
Total Direct Pay 34,246 96,783 224,492 Total Population 2,141,776 2,141,776 2,141,776

Summary of NY Simulation Results
Removing Community Rating & Guaranteed Issue has the greatest impact on reducing the number of uninsured.
Introducing HSAs into the market reduces the uninsured, but does not have nearly the impact of removing CR & GI.
Letting New Yorkers purchase insurance across state lines can lead to up a 26% reduction in the uninsured.
Reducing the number of mandates will have an impact, but not as great as interstate competition or the removal of CR & GI.

Current Simulation Work

PPACA: Impact of Health Reform Reconciliation Bill, as of 3/15/2010
Uninsurance is reduced by 59.8% (81% if base is US citizens only) to newly cover 32 million people, 17 million of whom through State Medicaid Agencies.
CBO (Congressional Budget Office) Estimates– 3/18/2010 CBO 10 year cost: $940 billion CBO deficit savings $130 billion
My estimates – 3/19/2010 10 year cost: $1.36 trillion
My Summary: Additional costs will eliminate deficit savings and add to deficit by $287 billion
On April 22, 2010 the Medicare/CMS actuary concluded health reform would add $251 billion to the deficit.

Health Reform Goal: ExpansionUninsured Impact 2010-2019Health Reform Premium & Uninsured EstimatesHSI Network LLC, January 8, 2010Preliminary
2010 2011 2012 2013 2014 2015 2016 2017 2018 2019Uninsured Level (in millions, including non-US citizens)
Status Quo 50.0 51.5 53.0 55.2 57.4 59.7 62.7 65.8 68.4 70.5Senate 50.0 51.5 53.6 55.7 33.4 23.4 21.1 21.3 22.1 22.8House 50.0 51.5 54.1 34.1 21.5 21.0 21.7 22.7 23.7 24.6Market-Based 50.0 51.5 46.4 44.0 35.2 35.9 36.3 34.5 34.8 35.9GOP House 50.0 51.5 46.4 44.0 44.5 44.9 45.8 47.2 48.6 50.1
As of 4/22/2010, CMS Actuary forecasts uninsured in 2019 to be 22 million.

Average Annual Premiums for Single and Family Coverage, 1999-2011
* Estimate is statistically different from estimate for the previous year shown (p<.05).
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2011.

Individual/small group premiums will increase at 8% per year, minimumHealth Reform Premium & Uninsured EstimatesHSI Network LLC, April 26, 2010Priviledged
2010 2011 2012 2013 2014 2015 2016 2017 2018 2019Family Premium
Individual insurance (purchase price to consumers)Premium $16,515 $18,167 $19,983 $21,981 $24,180 $26,598 $29,257 $32,183 $35,401 $38,942Gold $14,040 $15,163 $16,376 $17,686 $19,101 $20,629 $22,280 $24,062 $25,987 $28,066Silver $11,770 $12,594 $13,475 $14,419 $15,428 $16,508 $17,664 $18,900 $20,223 $21,639Bronze $8,480 $8,989 $9,528 $10,100 $10,706 $11,348 $12,029 $12,751 $13,516 $14,327Catastrophic $6,240 $6,490 $6,749 $7,019 $7,300 $7,592 $7,896 $8,211 $8,540 $8,881D-Catastrophic $6,240 $6,490 $6,749 $8,774 $10,529 $11,160 $11,607 $12,071 $12,554 $13,056

2011: ACA Accelerated HDHP - Distribution of Health Plan Enrollment for Covered Workers, by Plan Type, 1988-2011
* Distribution is statistically different from the previous year shown (p<.05). No statistical tests were conducted for years prior to 1999. No statistical tests are conducted between 2005 and 2006 due to the
addition of HDHP/SO as a new plan type in 2006.
Note: Information was not obtained for POS plans in 1988. A portion of the change in plan type enrollment for 2005 is likely attributable to incorporating more recent Census Bureau estimates of the number of state and local government workers and removing federal workers from the weights. See the Survey Design and Methods section from the 2005 Kaiser/HRET Survey of Employer-Sponsored Health Benefits for additional
information.
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2011; KPMG Survey of Employer-Sponsored Health Benefits, 1993, 1996; The Health Insurance Association of America (HIAA),
1988.
1%
1%
1%
1%

CBO: 2010-2019 Spend ($ billion)
0
50
100
150
200
250
Other
Medicaid and CHIP Expansion
Reinsurance and High-Risk Poolsa
Small Employer Tax Credit
Exchange Premium Credits
Health Insurance Exchanges

New York Health Insurance Reform Options
Individual Market 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
Family CoverageBronze - Catastrophic $11,343 $11,983 $12,642 $13,322 $14,021 $14,742 $15,484 $16,249 $17,036 $17,847Gold - PPO/POS $14,403 $15,655 $17,008 $18,469 $20,046 $21,750 $23,590 $25,577 $27,723 $30,041Bronze - EPO $10,802 $11,767 $12,808 $13,933 $15,147 $16,459 $17,876 $19,406 $21,058 $22,843Silver PPO/POS $12,603 $13,711 $14,908 $16,201 $17,597 $19,104 $20,733 $22,491 $24,391 $26,442Platinum PPO $16,204 $17,600 $19,108 $20,737 $22,495 $24,395 $26,447 $28,662 $31,055 $33,640
Single CoverageBronze - Catastrophic $5,083 $5,536 $6,002 $6,482 $6,977 $7,486 $8,010 $8,551 $9,107 $9,681Gold - PPO/POS $6,455 $7,072 $7,737 $8,456 $9,233 $10,071 $10,977 $11,955 $13,012 $14,153Bronze - EPO $4,841 $5,329 $5,855 $6,423 $7,037 $7,700 $8,416 $9,190 $10,025 $10,927Silver PPO/POS $5,648 $6,200 $6,796 $7,440 $8,135 $8,886 $9,697 $10,572 $11,518 $12,540Platinum PPO $7,262 $7,943 $8,679 $9,473 $10,331 $11,257 $12,258 $13,338 $14,505 $15,766
Family of four with income just above 250 % of poverty(currently around $55,000): in 2014 the required premium maximum premiumcontribution will be 8.1 percent of income
Income $55,000 $56,650 $58,350 $60,100 $61,903 $63,760 $65,673 Maximum Contribution $4,675 $4,815 $4,960 $5,108 $5,262 $5,783 $6,345
Silver Premium $16,201 $17,597 $19,104 $20,733 $22,491 $24,391 $26,442Subsidy $11,526 $12,781 $14,145 $15,624 $17,230 $18,608 $20,097

CBO: 2010-2019 Tax/Save
-300
-250
-200
-150
-100
-50
02010 2011 2012 2013 2014 2015 2016 2017 2018 2019
Other Revenue Provisionsc
Community Living Assistance Services and Supports
Additional Hospital Insurance Tax
Fees on Certain Manufacturers and Insurersb
Associated Effects of Coverage Provisions on Revenues
Excise Tax on High-Premium Plans
Penalty Payments by Employers and Uninsured Individuals
Reinsurance and Risk Adjustment Collections
Other
Medicare and Medicaid DSH Payments
Medicare Advantage Rates based on Fee for Service Rates
Reductions in Annual Updates to Medicare FFS Payment Rates

CBO: Projected Savings on Vote Eve, March 21, 2010
By 2019, $122 billion deficit savings

CBO: Projected Additional Cost/Savings of Pending Changes
0
20
40
60
80
100
120
140
CLASS Act & Community Living
Excise and other tax realities
Medicare Physician Fee Fix Back In
Market Basket Updates/Advantage Fix
By 2019, $676 billion additional deficit burden

Current vs. Pending Budget Effect – CBO’s Own Numbers
Net impact: $554 billion additional deficit 2010-2019$1.4 trillion additional deficit 2020-2029

What Might be Repeal & Replace regardless of who wins 2012?

Repeal, Replace or Ration Probabilities Repeal Only: <10% probability
Requires tea party dominance of political landscape. Tea party (broadly defined) has influence but not a majority cartel of
political power.
Replace: Two versions Revise 50% – No GOP Presidential victory in 2012 but budget force
issue for GOP Congress and President Obama Replace 50% - GOP victory in 2012 in Presidency and Congress –
move to something like Market Based Reform
Ration (leave PPACA alone): 35% probability US Will go to Double A or Single A credit rating by 2014 unless
Medicare prices at Medicaid rates and starts restricting of technology.
High deductible health plans (HSAs) become the only affordable plans in insurance exchanges.

Circa 2004-6: GOP was SeriousGOP Proposal Cost per newly insured
Estimated reduction in uninsured
Total EstimatedAnnual Cost
Per CapitaCost
Administration’s Proposal (Sim#1)
2,924,949 $8,075,081,354 $2,761
Low-income Buy-In (Sim#2) 4,495,887 $12,219,668,960 $2,718
Full subsidy (Sim#3) 12,819,856 $69,214,319,880 $5,399
Full subsidy Generous HSA (Sim#3a)
23,507,540 $211,118,893,800 $8,981
Full subsidy Non-working (Sim#4)
3,143,487 $11,234,374,714 $3,574

0
4,495,887
12,819,857
23,507,540
2,924,9490
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
$0 $50 $100 $150 $200 $250
Billions
Subsidy Cost
Pre
vio
usl
y U
nin
sure
d
But, the Designs had Diminishing Subsidy Returns
Sim #1
Sim #2
Sim #3
Sim #4
Sim #3A

New Flavor: Market Based Reform Feature Set This proposal was originally discussed by moderate GOP/Dems up to
Senate Vote on 12/24/2009 – Joint Committee on Taxation Score was $480 billion over 10 years and paid for with Medicare cuts or any tax other than a ‘Buick’ tax.
Guaranteed issue insurance coverage/no pre-existing conditions etc. Insurance exchanges, interstate purchase permitted A tax on those who choose health insurance benefits greater than $6.5K for
single coverage and $13K for family coverage equal to the employee’s marginal income tax rate times the amount over those thresholds
Full subsidy up to 200% of the federal poverty line and subsidy phased down to zero at 300% of FPL (~$66,000 for a family of four).
All insurance plans must offer preventive care benefits. All plans must use modified community rating: premiums can vary only by
geographic region (to be defined), family structure, actuarial value of benefits, and age.
Start date is January 1, 2013.

Meaningful Market Based ReformFeature Set
Age Individual Family
18-34 $1,364 $3,058
35-49 $2,237 $4,615
50-64 $3,725 $6,812
An income and age-adjusted health insurance voucher with the following 2010 amounts:
An income and age-adjusted health insurance voucher with the following 2010 amounts:

2009/10 Meaningful Market-Based Health Reform Proposal Results Uninsurance is reduced by 35% (46% if base is
US citizens only) to newly cover approximately 17.6 million people
Subsidy - Tax Recovery = Net cost: $49 billion subsidy for voucher, annual 2013 $50.6 billion tax capture , annual 2013 Total cost over ten years: $435 billion Total revenue over ten years: $450 billion Net cost (surplus): -$15 billion over ten years
Private insurance crowd out: Not an issue.

Concluding ThoughtsMarket Dynamics to Watch (and Score) Hospitals
Going on physician practice buying spree to become Accountable Care Organizations
Overplay their hand and budget and start cutting back
Physicians Next generation become free agents and plug in where
needed. Will rebel against ACO control if they can and should be able
to because with docs, there is no Care in ACO.
Health Plans No subsidized health benefit left behind. Will rally to get as
much federal $$ as possible. Will enter provider market directly (buy hospitals) or
indirectly (buy bankrupt hospital’s assets).

Thank You!
Q & A
Stephen T. Parente, Ph.D.Minnesota Insurance Industry Chair of Health Finance Director, Medical Industry Leadership InstituteProfessor, Department of FinanceCarlson School of ManagementUniversity of Minnesota321 19th Ave. S. Room 3-122Minneapolis, MN 55455612-624-1391 (w), 612-281-8220 (m)[email protected]://www.tc.umn.edu/~paren010